Submitted:
21 May 2023
Posted:
23 May 2023
You are already at the latest version
Abstract
Depression and anxiety in cardiovascular disease worsen the prognosis of patients. Treatments for these disorders often provide limited improvement. The present study aimed to test, for the first time, the impact of educational technology on anxiety and depressive symptoms in patients participating in a cardiac rehabilitation program. A 12-month randomized controlled trial was conducted, in which 207 patients were randomly assigned to either the experimental (n=76) or control (n=69) groups. The intervention involved a structured patient education program provided by medical students who had undergone specially designed training in cardiac rehabilitation. The primary outcomes were death, hospitalization, heart failure, and recurrent myocardial infarction. The study also assessed anxiety and depression. A year later, the experimental group showed a statistically significant decrease in anxiety and depression on the HADS scale, with reductions of 2.0 and 1.9 points respectively (p<0.05). The control group showed reductions of 1.5 and 1.2 points (p<0.05). The difference in depression (HRDS) between the groups at 12 months was -1.29 in favor of the main group (95% CI, -0.7 to -1.88), and the standardized effect size (SMD) was 0.36 (95% CI, 0.03 to 0.69). No treatment-related adverse events were observed. The results suggest that educational interventions can have a positive impact on mental health. The study's strengths include a structured intervention, randomization, and long-term follow-up. Limitations include the lack of blinding of study participants and a relatively small sample size.
Keywords:
anxiety
; cardiac rehabilitation
; depression
; medical education
; primary care
1. Introduction
Cardiovascular disease (CVD) is the most prevalent non-communicable disease [1], and it is the leading cause of morbidity and mortality worldwide. Psychological consequences, such as anxiety and depression, affect up to one-third of people with CVD and are associated with an increased risk of coronary diseases, lower quality of life (QoL), and increased healthcare costs [2,3]. Therefore, the prevention and treatment of anxiety and depression are essential components of patient care [4]. Although several studies have evaluated the effect of antidepressants and psychotherapy on depression in CVD, their effect on depressive symptoms was negligible or small [5].
Cardiac rehabilitation (CR) has been shown to be effective in reducing depression [6]. Patients who completed the CR program reported higher levels of physical and mental QoL and lower levels of depression [7]. One accessible, well-received, and side-effect-free method for addressing the psychological and physical problems of patients is a well-organized educational program [8]. Given the growing number of patients and the shortage of nurses and doctors in many countries, trained medical students are recruited to work with patients, and this strategy has proven successful [9].
Providing patients and caregivers with good education and information about recovery is an essential aspect of chronic patient care [10,11]. A recent Cochrane review provides evidence that education improves the knowledge of cardiac patients and their relatives, increases satisfaction, and leads to a decrease in their depression rates [12]. Many patients want to receive additional knowledge about the causes and prognosis of the disease, preventive measures, the availability of public services, and informal support groups.
There is a difference between informing patients and educating them. Information refers to healthcare issues, while patient education refers to interventions that facilitate care, increase adherence to treatment, lifestyle modifications, and informed decision-making [13]. The effectiveness of teaching depends on how it is delivered [14]. This applies to both recipients and service providers, so the choice of educational interventions is crucial. Educational interventions are a wide range of technologies, methods, and training tools aimed at forming competent professionals [15]. Educational interventions provide learners with the support they need to acquire skills and should address the functional, academic, cognitive, behavioral, and social skills that directly affect educational ability [16]. New educational programs, courses, and pedagogical methods aim to reform the old practices used [14].
Efforts aimed at developing patient education skills in healthcare professionals, mainly nurses, ensure long-term success in disease management [14]. In the existing system of primary healthcare in Kazakhstan, with a shortage of personnel, a doctor-centered model of care, and a large number of medical university students, we see the prospect of involving students in working with the population. Our study aimed to evaluate the effectiveness of patient education conducted by volunteers - students of the medical university who completed a short specially designed course outside the main educational program. In this article, we attempted to assess whether visits by trained volunteers to patients with CVD reduce depression and anxiety.
2. Materials and Methods
2.1. Study design
A randomized controlled trial was conducted with two groups of patients followed up for 12 months, comparing the educational intervention group with the usual outpatient follow-up practice for CVD patients after acute conditions. Patients were recruited from the cardiology department of the university hospital, Medical Center of the Non-Commercial Joint Stock Company West Kazakhstan Marat Ospanov Medical University in the northwest of Kazakhstan. Ethical approval was obtained from the Local Ethical Committee of the West Kazakhstan Marat Ospanov Medical University. The study was conducted as part of the scientific and technical project “Building the Capacity of Medical Education Technologies and Research in Family Medicine in Kazakhstan” with a grant from the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP09260428).
2.2. Participants
All patients who met the inclusion criteria and agreed to participate in the study were randomized into intervention and control groups in a 1:1 ratio using a computer random number generator. Baseline characteristics of the study participants are presented in Table 1.
The study participants were assessed using the Russian-validated Hospital Anxiety and Depression Scale (HADS) [17] and the Hamilton Rating Scale for Depression (HDRS) [18] before the start of the study and after 12 months. The HADS measures the symptoms of anxiety (7 points) and depression (7 points). The items are rated on a 4-point (0–3) scale, and higher scores indicate increased levels of stress. Scores for each subscale range from 0 to 21 and can be classified as normal (0–7), mild (8–10), moderate (11–14), and severe (15–21). A HADS score of 8 or higher is considered the threshold for mild clinical symptoms and provides optimal sensitivity and specificity for case detection [19]. The HDRS scores of 0 to 7 are considered normal, 8-16 indicate mild depression, 17-23 indicate moderate depression, and scores greater than 24 indicate severe depression; the maximum score is 52 points on a 17-point scale [20]. A clinically significant reduction in anxiety and depression was defined as a reduction of at least 3 points on the HDRS scale, 1.7 points on the HADS scale, and/or an SMD greater than 0.3 [21,22].
2.3. Interventions
Participation in study groups does not preclude the possibility of adding treatment for severe anxiety and depression, which may be necessary and offered by mental health professionals as part of routine outpatient follow-up.
- The current practice of dispensary observation of patients receiving CR (basic/standard) care in both groups of study participants includes a mandatory amount of assistance as part of outpatient treatment at the patient’s place of residence, as prescribed by the orders of the Ministry of Health of the Republic of Kazakhstan, the clinical protocol: On approval of the rules for organizing the provision of medical care to people with chronic diseases, the frequency and timing of observation, the mandatory minimum and frequency of diagnostic studies. Order of the Minister of Health of the Republic of Kazakhstan dated October 23, 2020 No. RK HM-149 /2020 (registered in the Register of State Registration of Regulatory Legal Acts under No. 21513). Available from: https://adilet.zan.kz/rus/docs/V2000021513
- On approval of the Rules for provision of medical rehabilitation. The order of the Minister of Healthcare of the Republic of Kazakhstan dated October 7, 2020 No. KR HM- 116/2020 (registered in the Register of state registration of regulatory legal acts under No. 21381). Available from: https://adilet.zan.kz/rus/docs/V2000021381
- Clinical protocol for medical rehabilitation stage third "outpatient rehabilitation ii". profile "cardiology and cardiac surgery" (adults) Recommended by the Expert Council of the RSE on REM "Republican Center for Health Development" of the Ministry of Health and Social Development of the Republic of Kazakhstan dated December 12, 2014 Protocol No. 9. Available from: https://endovascular.kz/ru/rekomendatsii/klinicheskie-protokoly-mz-rk/tretij-etap-ambulatornaya-reabilitatsiya-ii-profil-kardiologiya-i-kardiokhirurgiya-vzroslye
Polyclinics have the necessary specialists, and schools for patients are held, with examinations and medications (antihypertensive, antiischemic, statins, antiplatelet agents) provided free of charge for insured patients. Patients subject to planned hospitalization and inpatient rehabilitation (on average 10 days) can also receive these services free of charge, in accordance with regulatory legal acts.
2.4. Educational intervention
The educational intervention consisted of a minimum of 12 weekly volunteer visits of 60 minutes or more during the first three months, followed by once-a-month visits. A detailed description of the intervention is provided in our previous article [23]. Volunteers who completed a specially designed training made home visits to patients in need of CR for education, information, support, and motivational interviews. Visits were conducted weekly during the first three months, followed by once-a-month visits, with telephone counseling available more frequently upon the patient’s request. The educational visits covered topics such as lifestyle and risk factor management, exercise, medication, symptom and laboratory control. Additionally, volunteers conducted motivational interviews and provided patient support.
Volunteers completed a 5-day training course where they were trained to assess both the physical and mental states of patients. They were also taught about technologies for conducting individual training on nutrition, physiotherapy exercises, self-management, the mechanism of action and taking medications, and conducting a motivational interview. At the end of the course, the volunteers underwent an exam to assess their newly acquired skills, received instructions on how to work with patients, communicate and receive feedback from them, and how to liaise with patients’ district doctors and mentor-curators of the research group.
2.5. Collection of information
Information was collected through two patient assessments: the baseline (pre-CR) assessment and the assessment conducted 12 months after randomization.
2.6. Statistical analysis
Sample size was calculated using WinPepi software with alpha- and beta-errors set at 5% and 20%, respectively, based on the expected clinically important differences. Numeric variables were presented as mean ± standard deviation (SD), while categorical variables were presented as absolute numbers and percentages. Mann-Whitney tests were used to compare continuous variables between independent groups, while Wilcoxon tests were used for paired observations. Pearson’s chi-squared tests were used for analyzing categorical variables, and McNemar tests were applied for paired comparisons of dichotomous data. In addition to significance testing, effect sizes were calculated for all tests performed. Standardized mean difference (SMD) was used to compare two mean values, with a value of 0.20 indicating a small effect, 0.50 indicating a medium effect, and 0.80 indicating a strong effect. All differences were considered significant at p<0.05. All calculations were performed using IBM SPSS v.25 software.
3. Results
Between April 1, 2019 and March 31, 2020, a total of 207 patients were referred for CR and screened for eligibility (Figure 1). Of these, 22 patients did not meet the inclusion criteria, 30 withdrew, and 79 were randomized to the intervention group and 76 (49%) to the control group.
Table 1 presents the demographic and clinical data for the sample at baseline. The groups were well balanced for all measured variables, including the severity of physical illness and the prevalence of mental disorders. There was no major depressive disorder in either group.
The intervention improved lifestyle measures, including reduced body mass index, waist circumference, and smoking. It also improved cardiovascular performance, indicated by SBP, DBP, HR, EF, and the 6-minute test. Furthermore, it had a positive impact on indicators of lipid metabolism, such as total cholesterol, cholesterol-LDL, and cholesterol-HDL. In addition, the intervention resulted in a decrease in hospital admissions (RR 0.18, 95%CI 0.04-0.79; NNT 8.4) as shown in Table 2 and Table 3.
The percentage of patients achieving the target SBP ≤120 mmHg and DBP ≤80 mmHg was significantly higher in the intervention group (77.6% (95% CI 68-87%) and 97.4% (95% CI 94-101%)), with an RR of 2.14 (95% CI 1.5-2.9%, NNT 2.4), compared to the control group (36.2% (95% CI 25-48%) and 65.2% (95% CI 54-76%)), with an RR of 1.4 (95% CI 1.2-1.7%) and an NNT of 3.4.
The level of total cholesterol decreased significantly in the experimental group compared to the control group (Table 2 and Table 3). However, the number of patients who reached the target LDL level <1.8 mmol/l was low in both groups, with 6 patients in the experimental group and 5 patients in the control group. The percentage of patients who achieved at least a ≥50% reduction in cholesterol levels between 1.8 and 3.5 mmol/L was statistically significantly higher in the experimental group (14.5% (95% CI 7-22%) compared to 1.4% (95% CI 1-4%)), with an RR of 9.9 (95% CI 1.3-75.3%).
In the intervention group, there was a decrease not only in BMI (Table 2 and Table 3) but also in body weight, with an average reduction of -3.3 kg (-3.9%) compared to baseline (p<0.001). Conversely, the control group experienced an increase in BMI and body weight by 2.3% (from 78.4 (12.7) kg to 79.8 (12.5) kg). Tolerance to physical activity in the experimental group increased by 24.9%, whereas in the control group, it only increased by 10.3%.
After 12 months, the number of smokers in the experimental group decreased by 32.9% (from 56.6 to 23.7%), while in the control group, it decreased by 5.8% (from 42 to 36.2%), resulting in an RR of 0.65 (95% CI 0.39-1.09). Among those who continued to smoke, there was a reduction in the number of cigarettes smoked (Table 2 and Table 3). However, the effect on death (RR 0.68, 95%CI 0.15-2.9; NNT 54.1), recurrent MI (RR 0.34, 95%CI 0.09-1.2; NNT 13.1), and stroke (RR 0.23, 95%CI 0.03-1.98; NNT 22.3) tended to decrease, although the results were not statistically significant.
The Hospital Anxiety and Depression Scale (HADS) depression scores in both groups before the intervention were statistically similar (3.04±3.7 in the intervention group versus 3.83±3.89) in the control group, p=0.07), as were the Hamilton Rating Scale for Depression (HRDS) scores (4.2±4.7 vs. 4.5±5.3, p=0.50). HADS anxiety scores also did not differ significantly (3.9±3.2 versus 4.5±3.4, p=0.35, in the intervention and control groups, respectively).
After 12 months, the mean HADS depression scores were 1.1±1.7 in the intervention group versus 2.6±2.9 in the control group, p<0.0001, the HRDS scores were 1.5±1.7 versus 3.1±4.3, p=0.0086, and the HADS anxiety scores were 1.9±1.5 versus 3.0±1.8, p=0.0002, in the intervention and control groups, respectively.
In the intervention group, the decrease in anxiety and depression on both scales exceeded the decrease in the control group, although the comparison of the differences was not statistically significant (Table 4). The group difference on the Hamilton scale at 12 months was -1.29 in favor of the intervention group (95% CI, -0.7 to -1.88); SMD 0.36±95% CI, 0.03 to 0.69). The group difference on the HADS-anxiety scale after 12 months was -0.5 in favor of the intervention group (95% CI, from -0.09 to -0.9); SMD 0.2 (95% CI, -0.13 to 0.5). The group difference on the HADS-depression scale at 12 months was -0.7 in favor of the intervention group (95% CI, from -0.22 to -1.17); SMD 0.24 (95% CI, -0.09 to 0.56).
The proportion of patients with anxiety on the HADS scale in the intervention group decreased from 18.4% to 1.3% (p=0.0002), while in the control group, it decreased from 18.8% to 5.8% (p=0.001). The proportion of patients with depression in the intervention group decreased from 15.8% to 0 (p=0.0007) and in the control group, it decreased from 14.5% to 2.6% (p=0.002), according to the HADS and HRDS scales, respectively. The development of depression during the year was observed in two patients in the control group who did not initially have depression, whereas positive dynamics were observed in 100% of cases in the intervention group. However, no significant differences were found between the changes (Table 5). Safety and adverse events associated with the intervention were monitored throughout the trial and were not observed.
4. Discussion
In this article, we report the results of an educational intervention in patients enrolled in an outpatient CR program. By the end of the study, significant effects (SMD≥0.8) were observed for BMI, WC, the number of cigarettes smoked, blood lipids other than triglycerides, and the 6-minute walk test. The weight loss reported in cardiac rehabilitation programs in the scientific literature aligns with the findings of our study [24]. Regarding smoking, our study demonstrated lower results (33% reduction) compared to those reported by other authors (53-58%) [25,26]. Based on our results, the intervention has the potential to significantly reduce LDL-C and TC levels while increasing serum HDL-C levels. Similar findings are supported by the Wu et al. [27] systematic review.
The minimum clinically significant difference for 6MWD in CAD patients after ACS is considered to be 25 meters [28]. However, recent studies have shown a substantially greater improvement in exercise tolerance, such as the study by Gao et al. [29], which reported an increase of 200 meters. In our study, we also observed a notable improvement in this indicator, with an average increase of 88 meters, representing a 25% improvement over the baseline value.
One year later, in the main group, anxiety and depression on the HADS scale decreased by 2.0 and 1.9 points respectively (p<0.05). Depression on the HDRS scale decreased by an average of 1.29 points (p<0.05), while in the control group, there was no clinically significant decrease, and 5.8% of patients remained moderately to severely depressed. The effect size for HDRS depression at 12 months (SMD) was 0.36. The results show a slight improvement in performance in the CR control group, which contrasts with a more significant improvement in the main group. Different authors consider a change in HDRS-17 by 3–6 points to be a clinically significant decrease in the level of depression [30,31]. For anxiety and depression, a decrease of 1.7 points is considered to be the minimum clinically significant difference for HADS [22].
The UK National Institute for Health and Care Excellence (NICE) considers a reduction of 3 points on the Hamilton Depression Rating Scale (HDRS) of 17 points as a criterion for the effectiveness of depression treatment [32]. Some authors recognize SMD of about 0.3 as another criterion of minimal clinical significance in comparative studies [21]. However, these criteria can be called conditional because obtaining such values is not always a threshold. For example, people with less severe depression require smaller absolute reductions in HDRS scores for a clinically meaningful difference. In addition, some of the symptoms assessed by the HDRS may be a manifestation of other patient conditions other than depression, such as medical illness, drug side effects, and may persist despite improved mental status [21]. This is supported by the observed discrepancy between the HDRS score and remission as assessed by patients [33].
Clinical relevance remains uncertain even for pharmacological antidepressants. Numerous meta-analyses show that the SMD of antidepressants in the treatment of depression is 0.3. The average reduction in HDRS scores associated with antidepressant use is 2 points [21,31]. Psychotherapy has the same clinical value as antidepressants – 0.3-0.4 on the difference in effects [34]. Overall, the Cochrane Review found that both psychological and pharmacological interventions have low certainty evidence for an effect on depression in patients with CAD due to the small number of outcome trials and the heterogeneity of study populations and interventions [35].
CR has been shown to reduce mortality and readmissions and improve QoL [36]. However, its effect on anxiety and depression has been demonstrated only in combination with CR and psychotherapy. The PATHWAY study, which added group metacognitive psychotherapy sessions to a standard CR program, showed significant improvement in both depressive and anxiety symptoms [37].
4.1. Goals of CR programs
The key goal of CR programs is to improve physical health and QoL and to equip and support people to develop the necessary skills for successful self-management [38,39,40]. Psychological components are not standardized and vary across healthcare resources. They include counseling, relaxation, meditation, stress management, cognitive psychotherapy, social support, help, and communication channels.
4.2. Psychological component in outpatient CR
In our program of outpatient CR, the psychological component included regular informative assessments of physical conditions (such as BP, heart rate, exercise tolerance, and interpretation of laboratory and instrumental examinations), training in self-management methods aimed at improving CVD risk profiles, increasing physical activity, and providing support and continuous feedback from the patient. There was no psychotherapy, psychological counseling, stress management, or consultations with a psychiatrist or a psychotherapist. Improvement in physical condition, increased physical activity, and clear patient-oriented recommendations, in our opinion, ensured the results obtained.
4.3. Strengths and limitations
Strengths of the study include a structured intervention, randomization, and the use of long-term follow-up. The sample of this study is representative of patients with CVD. For example, Choo et al. [7] reported that 74% of CR patients were male, and the mean and SD of age was 57±8.8, which is comparable to our study by sex and age. Wells et al. [37] reported that half of the patients had concomitant arterial hypertension, and 23% had diabetes mellitus, which is similar to our study in which 58% of patients had hypertension, and 23% had type 2 diabetes.
Limitations of the present study include no blinding of study participants and a small sample size. The Wells study had 332 participants in two groups, the Choo study had 194 patients, Ayasrah et al. [41] had 186 patients, while Sharif et al. had 80 participants [42]. There were 145 patients in our study.
4.4. Practical Significance
The practical significance of our study is likely to be different for different healthcare systems and medical education. In our country, students of medical HEIs and medical colleges can be potential system assistants who can interact closely with patients. However, there is not enough staff in the primary care system to better cover the population with effective medical services, not only for the rehabilitation of patients with CVD but also for patients with other chronic diseases, palliative care, and preventive activities. Our study is the only one of its kind that has evaluated the effectiveness of using students for healthcare practice.
5. Conclusions
Educational intervention in routine CR appears to be safe and effective in reducing anxiety and depression compared to conventional care. Benefits appeared to be stable over the 12-month follow-up period, and the effect size is comparable to the best existing results from research on depression. Educational interventions for cardiac rehabilitation that do not increase the incidence of adverse events are effective and safe, offering notable clinical benefits in terms of improving exercise endurance, reducing hospitalization, and managing risk factors. We believe that the intervention could be included in routine CR to significantly improve psychological outcomes in patients with CVD and offer added value over standard CR.
Author Contributions
Conceptualization, Lazzat Zhamaliyeva; Data curation, Lazzat Zhamaliyeva, Damira Zhamankulova and Nurgul Abenova; Formal analysis, Gulbakit Koshmaganbetova; Investigation, Damira Zhamankulova and Nurgul Abenova; Methodology, Nurgul Abenova; Software, Lazzat Zhamaliyeva; Supervision, Lazzat Zhamaliyeva; Writing – original draft, Damira Zhamankulova; Writing – review & editing, Lazzat Zhamaliyeva and Gulbakit Koshmaganbetova.
Funding
The study was conducted as part of the scientific and technical project “Building the Capacity of Medical Education Technologies and Research in Family Medicine in Kazakhstan” with a grant from the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP09260428). - this is written in the "Materials and Methods" section. The name of the grantor is correct.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of West Kazakhstan Marat Ospanov Medical university (protocol code 30 19.09.2019).
Informed Consent Statement
This study was approved by the local research ethics committee (protocol 4 from 29 January 2018)
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
The authors thank Bekbolat Zholdin for reviewing the study protocol, Gulnara Kurmanalina, Galina Veklenko, Gauhar Dilmagambetova, Alima Kashkinbayeva, Ziyash Tanbetova for help in the selection and training of medical students. We are grateful for statistical advice from Andrej Grjibovski.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bennett, J.E.; Stevens, G.A.; Mathers, C.D.; Bonita, R.; Rehm, J.; Kruk, M.E.; Riley, L.M.; Dain, K.; Kengne, A.P.; Chalkidou, K.; et al. NCD Countdown 2030: worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet 2018, 392, 1072–1088, doi:Doi 10.1016/S0140-6736(18)31992-5.
- Wells, A.; Reeves, D.; Heal, C.; Fisher, P.; Doherty, P.; Davies, L.; Heagerty, A.; Capobianco, L. Metacognitive therapy home-based self-help for anxiety and depression in cardiovascular disease patients in the UK: A single-blind randomised controlled trial. PLoS Med 2023, 20, e1004161. [CrossRef]
- Olsson, K.M.; Meltendorf, T.; Fuge, J.; Kamp, J.C.; Park, D.H.; Richter, M.J.; Gall, H.; Ghofrani, H.A.; Ferrari, P.; Schmiedel, R.; et al. Prevalence of Mental Disorders and Impact on Quality of Life in Patients With Pulmonary Arterial Hypertension. Front Psychiatry 2021, 12, 667602. [CrossRef]
- Aggarwal, M.; Ornish, D.; Josephson, R.; Brown, T.M.; Ostfeld, R.J.; Gordon, N.; Madan, S.; Allen, K.; Khetan, A.; Mahmoud, A.; et al. Closing Gaps in Lifestyle Adherence for Secondary Prevention of Coronary Heart Disease. Am J Cardiol 2021, 145, 1–11. [CrossRef]
- Zambrano, J.; Celano, C.M.; Januzzi, J.L.; Massey, C.N.; Chung, W.J.; Millstein, R.A.; Huffman, J.C. Psychiatric and Psychological Interventions for Depression in Patients With Heart Disease: A Scoping Review. J Am Heart Assoc 2020, 9, e018686. [CrossRef]
- Zheng, X.; Zheng, Y.; Ma, J.; Zhang, M.; Zhang, Y.; Liu, X.; Chen, L.; Yang, Q.; Sun, Y.; Wu, J.; et al. Effect of exercise-based cardiac rehabilitation on anxiety and depression in patients with myocardial infarction: A systematic review and meta-analysis. Heart Lung 2019, 48, 1–7. [CrossRef]
- Choo, C.C.; Chew, P.K.H.; Lai, S.M.; Soo, S.C.; Ho, C.S.; Ho, R.C.; Wong, R.C. Effect of Cardiac Rehabilitation on Quality of Life, Depression and Anxiety in Asian Patients. Int J Environ Res Public Health 2018, 15, 1095. [CrossRef]
- Carroll, D.L.; Malecki-Ketchell, A.; Astin, F. Non-pharmacological interventions to reduce psychological distress in patients undergoing diagnostic cardiac catheterization: a rapid review. Eur J Cardiovasc Nurs 2017, 16, 92–103. [CrossRef]
- Berg, L.J.; Arons, D.; Deng, J.; Green, A.L.; Taneja, M.; Wang, C.; Liu, S.S. Cardiac Coaches: A Student-Led Inpatient Cardiac Rehabilitation Program in the COVID-19 Era. Acad Med 2021, 96, e24. [CrossRef]
- Shi, W.; Ghisi, G.L.M.; Zhang, L.; Hyun, K.; Pakosh, M.; Gallagher, R. Systematic review, meta-analysis and meta-regression to determine the effects of patient education on health behaviour change in adults diagnosed with coronary heart disease. J Clin Nurs 2022. [CrossRef]
- Ertugrul, B.; Ozden, D. Physical Restraint Experiences of Family Caregivers of Patients With Stroke in Turkey: A Qualitative Study. Clin Nurs Res 2023, 32, 499–509. [CrossRef]
- Crocker, T.F.; Brown, L.; Lam, N.; Wray, F.; Knapp, P.; Forster, A. Information provision for stroke survivors and their carers. Cochrane Database of Systematic Reviews 2021. [CrossRef]
- Paterick, T.E.; Patel, N.; Tajik, A.J.; Chandrasekaran, K. Improving health outcomes through patient education and partnerships with patients. In Proceedings of the Baylor University Medical Center Proceedings, 2017; pp. 112–113.
- Timmers, T.; Janssen, L.; Kool, R.B.; Kremer, J.A. Educating Patients by Providing Timely Information Using Smartphone and Tablet Apps: Systematic Review. J Med Internet Res 2020, 22, e17342. [CrossRef]
- Menezes, P.; Guraya, S.Y.; Guraya, S.S. A Systematic Review of Educational Interventions and Their Impact on Empathy and Compassion of Undergraduate Medical Students. Frontiers in Medicine 2021, 8, 758377. [CrossRef]
- Meinema, J.G.; Buwalda, N.; van Etten-Jamaludin, F.S.; Visser, M.R.; van Dijk, N. Intervention descriptions in medical education: what can be improved? A systematic review and checklist. Academic Medicine 2019, 94, 281.
- Shal’nova, S.A.; Evstifeeva, S.E.; Deev, A.D.; Artamova, G.V.; Gatagonova, T.M.; Dupliakov, D.V.; Efanov, A.; Zhernakova Iu, V.; Konradi, A.O.; Libis, R.A.; et al. [The prevalence of anxiety and depression in different regions of the Russian Federation and its association with sociodemographic factors (according to the data of the ESSE-RF study)]. Ter Arkh 2014, 86, 53–60. [CrossRef]
- Santor, D.A.; Debrota, D.; Engelhardt, N.; Gelwicks, S. Optimizing the ability of the Hamilton Depression Rating Scale to discriminate across levels of severity and between antidepressants and placebos. Depress Anxiety 2008, 25, 774–786. [CrossRef]
- Wu, Y.; Levis, B.; Sun, Y.; He, C.; Krishnan, A.; Neupane, D.; Bhandari, P.M.; Negeri, Z.; Benedetti, A.; Thombs, B.D.; et al. Accuracy of the Hospital Anxiety and Depression Scale Depression subscale (HADS-D) to screen for major depression: systematic review and individual participant data meta-analysis. BMJ 2021, 373, n972. [CrossRef]
- Davies, T.; Garman, E.C.; Lund, C.; Schneider, M. Adaptation and validation of a structured version of the Hamilton Depression Rating Scale for use by non-clinicians in South Africa (AFFIRM-HDRS). J Eval Clin Pract 2020, 26, 1425–1435. [CrossRef]
- Hieronymus, F.; Jauhar, S.; Østergaard, S.D.; Young, A.H. One (effect) size does not fit at all: interpreting clinical significance and effect sizes in depression treatment trials. Journal of Psychopharmacology 2020, 34, 1074–1078.
- Lemay, K.R.; Tulloch, H.E.; Pipe, A.L.; Reed, J.L. Establishing the Minimal Clinically Important Difference for the Hospital Anxiety and Depression Scale in Patients With Cardiovascular Disease. J Cardiopulm Rehabil Prev 2019, 39, E6–E11. [CrossRef]
- Zhamankulova, D.G.; Zhamaliyeva, L.M.; Kurmanalina, G.L.; Tanbetova, Z.; Grjibovski, A.M. Public Health Rehabilition after Acute Myocardial Infarction: a Randomized Controlled Study. Human Ecology 2021, 8, 57–64.
- Hushcha, P.; Jafri, S.H.; Malak, M.M.; Parpos, F.; Dorbala, P.; Bousquet, G.; Lutfy, C.; Sonis, L.; Cabral, L.; Mellett, L.; et al. Weight Loss and Its Predictors During Participation in Cardiac Rehabilitation. Am J Cardiol 2022, 178, 18–25. [CrossRef]
- Sestayo Fernandez, M.; Alonso Vazquez, M.; Gonzalez Maestro, A.; Gonzalez Salvado, V.; Diaz Balboa, E.; Neiro Rey, M.; Gonzalez Juanatey, J.; Pena Gil, C. Changes in smoking status after a cardiac rehabilitation program in Spain: description of a smoker’s profile. European Heart Journal 2022, 43, ehac544. 2382.
- Sadeghi, M.; Shabib, G.; Masoumi, G.; Amerizadeh, A.; Shahabi, J.; Heidari, R.; Roohafza, H. A Systematic Review and Meta-analysis on the Prevalence of Smoking Cessation in Cardiovascular Patients After Participating in Cardiac Rehabilitation. Curr Probl Cardiol 2021, 46, 100719. [CrossRef]
- Wu, G.; Hu, Y.; Ding, K.; Li, X.; Li, J.; Shang, Z. The Effect of Cardiac Rehabilitation on Lipid Levels in Patients with Coronary Heart Disease. A Systematic Review and Meta-Analysis. Glob Heart 2022, 17, 83. [CrossRef]
- Akowuah, E.; Mathias, A.; Bardgett, M.; Harrison, S.; Kasim, A.S.; Loughran, K.; Ogundimu, E.; Trevis, J.; Wagnild, J.; Witharana, P. Prehabilitation in elective patients undergoing cardiac surgery: a randomised control trial (THE PrEPS TRIAL)–a study protocol. BMJ open 2023, 13, e065992.
- Gao, Y.; Yue, L.; Miao, Z.; Wang, F.; Wang, S.; Luan, B.; Hao, W. The Effect and Possible Mechanism of Cardiac Rehabilitation in Partial Revascularization Performed on Multiple Coronary Artery Lesions. Clin Interv Aging 2023, 18, 235–248. [CrossRef]
- Rush, A.J.; South, C.; Jain, S.; Agha, R.; Zhang, M.; Shrestha, S.; Khan, Z.; Hassan, M.; Trivedi, M.H. Clinically Significant Changes in the 17- and 6-Item Hamilton Rating Scales for Depression: A STAR*D Report. Neuropsychiatr Dis Treat 2021, 17, 2333–2345. [CrossRef]
- Hengartner, M.P.; Ploderl, M. Estimates of the minimal important difference to evaluate the clinical significance of antidepressants in the acute treatment of moderate-to-severe depression. BMJ Evid Based Med 2022, 27, 69–73. [CrossRef]
- Kirsch, I.; Deacon, B.J.; Huedo-Medina, T.B.; Scoboria, A.; Moore, T.J.; Johnson, B.T. Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med 2008, 5, e45. [CrossRef]
- Zimmerman, M.; Chelminski, I.; Posternak, M. A review of studies of the Hamilton depression rating scale in healthy controls: implications for the definition of remission in treatment studies of depression. J Nerv Ment Dis 2004, 192, 595–601. [CrossRef]
- Cuijpers, P.; Quero, S.; Dowrick, C.; Arroll, B. Psychological Treatment of Depression in Primary Care: Recent Developments. Curr Psychiatry Rep 2019, 21, 129. [CrossRef]
- Tully, P.J.; Ang, S.Y.; Lee, E.J.; Bendig, E.; Bauereiss, N.; Bengel, J.; Baumeister, H. Psychological and pharmacological interventions for depression in patients with coronary artery disease. Cochrane Database Syst Rev 2021, 12, CD008012. [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol 2022, 19, 180–194. [CrossRef]
- Wells, A.; Reeves, D.; Capobianco, L.; Heal, C.; Davies, L.; Heagerty, A.; Doherty, P.; Fisher, P. Improving the Effectiveness of Psychological Interventions for Depression and Anxiety in Cardiac Rehabilitation: PATHWAY-A Single-Blind, Parallel, Randomized, Controlled Trial of Group Metacognitive Therapy. Circulation 2021, 144, 23–33. [CrossRef]
- Rathore, S.; Kumar, B.; Tehrani, S.; Khanra, D.; Duggal, B.; Chandra Pant, D. Cardiac rehabilitation: Appraisal of current evidence and utility of technology aided home-based cardiac rehabilitation. Indian Heart J 2020, 72, 491–499. [CrossRef]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019, 140, e69–e89.
- Ruivo, J.; Moholdt, T.; Abreu, A. Overview of Cardiac Rehabilitation (OCRE) Following Post-Acute Myocardial Infarction in European Society of Cardiology (ESC) Member Countries. Eur J Prev Cardiol 2023, zwad024. [CrossRef]
- Ayasrah, S.M.; Ahmad, M.M. Educational Video Intervention Effects on Periprocedural Anxiety Levels Among Cardiac Catheterization Patients: A Randomized Clinical Trial. Research and Theory for Nursing Practice 2016, 30, 70–84, doi:Doi 10.1891/1541-6577.30.1.70.
- Sharif, F.; Shoul, A.; Janati, M.; Kojuri, J.; Zare, N. The effect of cardiac rehabilitation on anxiety and depression in patients undergoing cardiac bypass graft surgery in Iran. BMC Cardiovasc Disord 2012, 12, 40. [CrossRef]
Figure 1.
Trend follow diagram of a randomized controlled trial for educational intervention effects on depression and anxiety in patients after myocardial infarction.
Figure 1.
Trend follow diagram of a randomized controlled trial for educational intervention effects on depression and anxiety in patients after myocardial infarction.
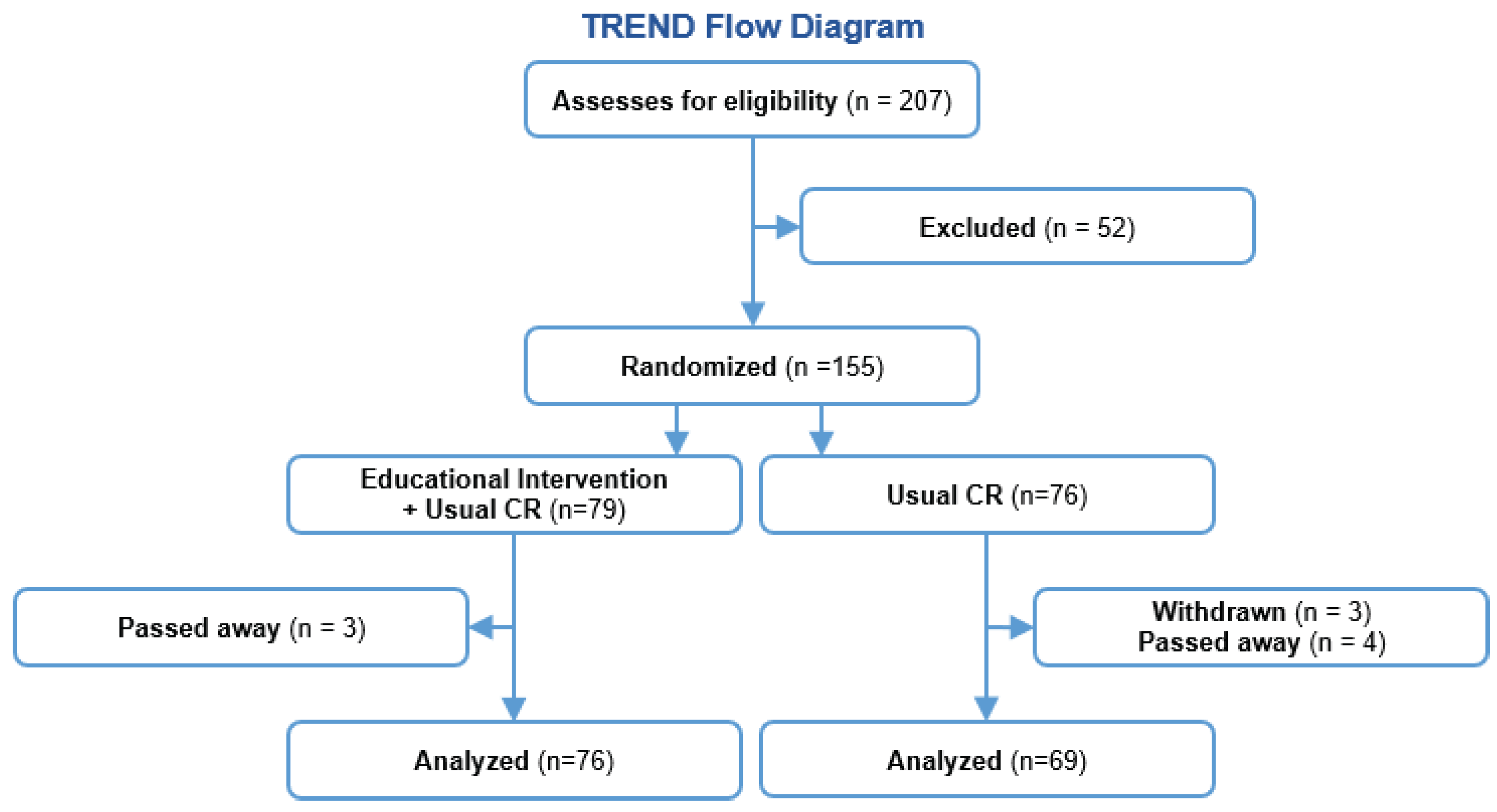

Table 1.
Demographic and clinical indicators of patients in a randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction.
Table 1.
Demographic and clinical indicators of patients in a randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction.
| Indices | Experimental group (n=76) | Control group (n=69) | P-value |
|---|---|---|---|
| Age, years (range) | 58 (52-68) | 59 (54.5-69) | 0.24 |
| SBP, mmHg (range) | 140 (130-150) | 130 (120-150) | 0.37 |
| DBP, mmHg (range) | 85 (80-90) | 80 (80-90) | 0.40 |
| Heart rate, bpm (range) | 75 (68-85) | 78 (70-80) | 0.44 |
| Cholesterol, mmol/L (range) | 5.6 (4.6-6.5) | 5.1 (4.2-6.5) | 0.15 |
| Triglycerides, mmol/L (range) | 1.2 (0.9-1.8) | 1.2 (0.9-1.8) | 0.82 |
| HDL, mmol/L (range) | 1.1 (0.9-1.3) | 1.2 (1.1-1.2) | 0.79 |
| LDL, mmol/L (range) | 3.5 (2.9-4.1) | 3.2 (2.5-4.2) | 0.44 |
| Glucose, mmol/L (range) | 6.7 (5.5-8.9) | 6.5 (5.2-7.9) | 0.15 |
| Creatinine, µmol/L (range) | 73 (66-89) | 79 (67.6-92.9) | 0.37 |
| Smoked, n (%) | 43 (56.6%) | 29 (42.0%) | 0.08 |
| Hypertension Grade 3, n (%) | 44 (57.9%) | 44 (63.8%) | 0.82 |
| Recurrent MI, n (%) | 12 (15.8%) | 17 (24.6%) | 0.18 |
| Stroke / TIA, n (%) | 7 (9.2%) | 8 (11.6%) | 0.57 |
| Diabetes mellitus, n (%) | 18 (23.7%) | 13 (18.8%) | 0.47 |
| Ejection fraction by echocardiography, n (%) | 50 (46-54) | 50 (45-53) | 0.50 |
| 6-minute walk test, n (%) | 365 (335-400) | 370 (330-440) | 0.62 |
| Gender | 0.12 | ||
| Male, n (%) | 58 (73.42%) | 61 (83.56%) | |
| Female, n (%) | 21 (26.58%) | 12 (16.44%) | |
| Place of residence | 0.44 | ||
| City, n (%) | 47 (59.49%) | 42 (57.53%) | |
| Rural area, n (%) | 19 (24.05%) | 23 (31.51%) | |
| Suburb, n (%) | 13 (16.46%) | 8 (10.96%) | |
| Marital status | 0.50 | ||
| Married, n (%) | 61 (77.22%) | 60 (82.19%) | |
| Divorced/Widower, n (%) | 16 (20.25%) | 10 (13.70%) | |
| Single, n (%) | 2 (2.53%) | 3 (4.11%) | |
| Education | 0.57 | ||
| Secondary, n (%) | 36 (45.57%) | 37 (51.39%) | |
| Vocational, n (%) | 22 (27.85%) | 21 (29.17%) | |
| Higher, n (%) | 21 (26.58%) | 14 (19.44%) | |
| Employment | 0.70 | ||
| Unemployed, n (%) | 34 (43.04%) | 34 (46.58%) | |
| Manual labor, n (%) | 31 (39.24%) | 24 (32.88%) | |
| Mental labor, n (%) | 14 (17.72%) | 15 (20.55%) | |
| HADS, anxiety, n (%) | 14 (18.42%) | 13 (18.84%) | 0.98 |
| Subclinical anxiety, n (%) | 9 (11.84%) | 8 (11.59%) | |
| Clinical anxiety, n (%) | 5 (6.58%) | 5 (7.25%) | |
| HADS, depression, n (%) | 12 (15.78%) | 10 (14.48%) | 0.97 |
| Subclinical depression, n (%) | 6 (7.89%) | 5 (7.24%) | |
| Clinically significant depression, n (%) | 6 (7.89%) | 5 (7.24%) | |
| Hamilton, depression, n (%) | 11 (14.47%) | 10 (14.49%) | 0.66 |
| Mild depressive disorder, n (%) | 5 (6.58%) | 5 (7.25%) | |
| Moderate depressive disorder, n (%) | 3 (3.95%) | 1 (1.45%) | |
| Severe depressive disorder, n (%) | 3 (3.95%) | 3 (4.35%) |
Table 2.
Mean ± standard deviation (SD) of characteristics of the patients after 12 months in the experimental and control groups of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction
Table 2.
Mean ± standard deviation (SD) of characteristics of the patients after 12 months in the experimental and control groups of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction
| Indices | Experimental (n=76) |
Control (n=69) |
P-value |
|---|---|---|---|
| BMI, kg/m2 | 27.1±4.8 | 28.3±3.8 | 0.00 |
| WC, sm | 97.2±13.1 | 102.2±12.2 | 0.01 |
| Cigarettes smoked per day, n | 1.9±4.2 | 6.2±8.9 | 0.00 |
| Systolic blood pressure, mmHg | 119.0±8.3 | 132.2±15.7 | 0.00 |
| Diastolic blood pressure, mmHg | 75.9±5.9 | 82.2±8.6 | 0.00 |
| Heart rate, bpm | 63.1±3.4 | 68.6±7.4 | 0.00 |
| Cholesterol, mmol/L | 4.1±0.8 | 4.9±1.2 | 0.00 |
| Triglycerides, mmol/L | 1.4±0.5 | 1.5±0.7 | 0.10 |
| HDL, mmol/L | 1.2±0.2 | 1.0±0.2 | 0.00 |
| LDL, mmol/L | 2.5±0.8 | 3.1±0.9 | 0.00 |
| Ejection fraction by echocardiography, % | 53.6±6.5 | 49.7±6.9 | 0.00 |
| 6-minute walk test, m | 442.6±71.8 | 372.2±101.4 | 0.00 |
| Death, n (%) | 3.0±3.8% | 4.0±5.4% | 0.62 |
| Recurrent MI, n (%) | 3.0±3.80% | 8.0±10.9% | 0.08 |
| Stroke / TIA, n (%) | 1.0±1.2% | 4.0±5.4% | 0.14 |
| Hospitalization, n (%) | 2.0±2.5% | 10.0±13.7% | 0.01 |
Table 3.
Mean ± standard deviation (SD) of the differences between the values after 12 months and at the initiation of the study in the experimental and control groups of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction.
Table 3.
Mean ± standard deviation (SD) of the differences between the values after 12 months and at the initiation of the study in the experimental and control groups of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction.
| Indices | Intervention group | Control group | P-value | Effect size (95%CI) |
|---|---|---|---|---|
| Body mass index, kg/m2 | -1.1±1.0 | 0.4±1.1 | <0.001 | -1.49 (96%CI -1.8; -1.12) |
| Waist circumference, cm | -3.4±2.4 | 1.8±2.7 | <0.001 | -2.08 (96%CI -2.5; -1.7) |
| Number of cigarettes a day, n | -10.6±11.2 | -2.6±7.2 | <0.001 | -0.8 (-1.18; -0.5) |
| Systolic blood pressure, mmHg | -18.7±18.4 | -4.9±25.5* p=0.11 |
<0.001 | -0.63 (96%CI -0.96; -0.3) |
| Diastolic blood pressure, mmHg | -8.16±9.4 | -1.3±12.4* p=0.39 |
<0.001 | -0.63 (96%CI -0.96; -0.3) |
| Heart rate, bpm | -12.9±11.9 | -8.2±11.2 | 0.01 | -0.4 (95%CI -0.7; -0.07) |
| Cholesterol, mmol/L | -1.57±1.2 | -0.39±1.2 | <0.001 | -0.98 (95%CI -1.3; -0.6) |
| Triglycerides, mmol/L | -0.08±0.7* p=0.38 |
0.13±0.7* p=0.16 |
0.10 | -0.3 (95%CI -0.6; 0.03) |
| HDL, mmol/L | 0.08±0.3 | -0.05±0.2* p=0.15 |
0.006 | 0.46 (95%CI 0.13; 0.8) |
| LDL, mmol/L | -0.9±1.1 | -0.2±0.9* p=0.07 |
<0.001 | -0.7 (95%CI -1.02; -0.36) |
| Ejection fraction by echocardiography, % | 4.2±4.9 | 0.7±4.6* p=0.19 |
<0.001 | 0.72 (95%CI 0.39; 1.06) |
| 6-minute walk test, m | 88.1±28.9 | 34.8±28.0 | <0.001 | 1.9 (95%CI 1.5; 2.3) |
*Changes were not statistically significant.
Table 4.
Mean ± standard deviation (SD) of categorical characteristics in the experimental and control groups at the beginning and end of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction, as well as their changes.
Table 4.
Mean ± standard deviation (SD) of categorical characteristics in the experimental and control groups at the beginning and end of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction, as well as their changes.
| Characteristics | Experimental group, n=76 | P-value1 | Control group, n=69 | P-value1 | Experimental group changes | Control group changes | P-value2 | ||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | ||||||
| HADS anxiety | 3.9±3.2 | 1.9±1.5 | 0.0002 | 4.5±3.4 | 3.0±1.8 | <0.001 | -2.0 | -1.5 | 0.24 |
| HADS depression | 3.0±3.7 | 1.1±1.7 | <0.0001 | 3.8±3.9 | 2.6±2.9 | <0.001 | -1.9 | -1.2 | 0.21 |
| HDRS depression | 4.2±4.7 | 1.5±1.7 | 0.008 | 4.5±5.3 | 3.1±4.3 | <0.001 | -2.7 | -1.4 | 0.23 |
1 According to the Wilcoxon test for paired populations. 2 According to the Mann-Whitney test for unpaired populations
Table 5.
Frequency of categorical features (outcome – yes / no) in the experimental and control groups at the beginning and end of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction, as well as their changes
Table 5.
Frequency of categorical features (outcome – yes / no) in the experimental and control groups at the beginning and end of the randomized controlled trial for educational intervention effects on depression and anxiety after myocardial infarction, as well as their changes
| Characteristics | Experimental group | Control group | P-value 2 | |||||
| Before, Positive outcome | Before, Negative outcome | P-value 1 | Before, Positive outcome | Before, Negative outcome | P-value 1 | |||
| HADS anxiety | <0.001 | 0.008 | 0.19 | |||||
| After, Negative outcome | 13 | 62 | 9 | 56 | ||||
| After, Positive outcome | 1 | 0 | 4 | 0 | ||||
| HADS depression | 0.002 | 0.04 | 0.07 | |||||
| After, Negative outcome | 12 | 64 | 8 | 58 | ||||
| After, Positive outcome | 0 | 0 | 2 | 1 | ||||
| HDRS depression | 0.008 | 0.68 | 0.06 | |||||
| After, Negative outcome | 9 | 65 | 4 | 57 | ||||
| After, Positive outcome | 2 | 0 | 6 | 2 | ||||
1 Comparison using the McNemar test for paired populations. 2 Comparison using Pearson’s chi-square test for unpaired populations
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



