
Submitted:
21 May 2023
Posted:
23 May 2023
You are already at the latest version
Abstract
Aim: Evaluation of role of supplementation of omega-3 polyunsaturated fatty acids on endothelial function in patients with metabolic syndrome.
Methods: Total of 80 patients with metabolic syndrome were enrolled to two groups. We evaluated endothelial function in subjects before and after three-month treatment with omega-3 polyunsaturated fatty acids in dose 2.4g daily (800mg 3 times a day) vs placebo. Using the Endo-PAT2000 device (Itamar Medical Ltd. Caesarea, Israel), reactive hyperemia index – a parameter of endothelial function and augmentation index– a parameter of arterial stiffness were measured. Plasmatic level of glutation peroxidase, homocysteine, apolipoprotein B and lipoprotein (a) were also evaluated.
Results: The average values of reactive hyperemia index before the treatment with n-3PUFA was 1.62 ± 0.42 , whereas 1.96 ± 0.62 at the end of the study (p<0.005). Augmentation index changed from 14.66 ± 19.55 to 9.21 ± 15.64 after the treatment (p=0.003). We also observed statistically significant decrease of apolipopotein B (0.94 ± 0.36 vs 1.13 ± 0.35, p = 0.001) and homocysteine (19.31 ± 5.29 vs. 13.78 ± 3.05, p = 0.001) and increase of the glutathion perxidase plasma levels (41.65 ± 8.90 vs. 45.20 ± 8.01), p=0.001.
Conclusion: We have observed significant improvement of the endothelial function in subjects with metabolic syndrome treated with omega-3 polyunsaturated fatty acids in dose 2.4g daily.
Keywords:
metabolic syndrome
; endothelial dysfunction
; omega-3 fatty acid
Background
Despite advances in preventive cardiology, the cardiovascular (CV) mortality remains high. Metabolic syndrome (MS) is defined as simultaneous presence of lipid and non-lipid related CV and cardio-metabolic risk factors that significantly increase the risk of CV disorders, as well as type 2 diabetes. A common trait of these risk factors is the fact that they cause endothelial dysfunction (ED). ED plays a significant role in the development and clinical manifestation of atherosclerosis.
Omega-3 poly-unsaturated fatty acids (n-3 PUFA) used for primary and secondary prevention of CV disorders are currently associated with a wide range of evidence within the framework of evidence-based medicine. Their anti-inflammatory, anti-thrombotic, anti-arrhythmic and triglyceride-reducing effects (at high doses) are well established, often associated with increase of HDL cholesterol. The objective of the work is to assess the possible effect on n-3 PUFA on endothelial function in MS patients.
First evidence of the benefits of n-3 PUFA originated in 1970-s, with the publication of reports on reduced prevalence of ischemic heart disease and diabetes in Eskimos – Inuits, who live in Greenland, who were found to have high n-3 PUFA levels thanks to excessive intake of fish fat that contains n-3 PUFA [1]. These reports have been expanded over the recent decades, extended, supplemented and analyzed in additional clinical studies. The results of GISSI Prevenzione and DART studies present an explanation for several effects of n-3 PUFA [2,3]
Clinical data supporting the reduction of the progression of atherosclerosis with n-3 PUFA originate from SCIMO (Study on Prevention of Coronary Atherosclerosis by Intervention with Marine Omega-3 fatty acids), where quantitative analysis of the progression/regression of plaque in coronary arteries has been performed [4].
Based on extensive evidence-based medicine data, in the primary and secondary prevention of CV diseases, n-3 PUFA have their role in the recommendations by international and global organizations [5].
The aim of this trial was to evaluate the role of n-3 PUFA supplementation on endothelial function in patients with metabolic syndrome compare to placebo
Methodology
Study Population
80 patients with MS were enrolled in the study (40 patients on n-3 PUFA and 40 patients on corresponding placebo). In n-3 PUFA group there were 56,5% (23) male and 43,5% (17) females with the mean age of 60,5 years, range 31-81 years. MS was classified according to the definition of IDF (2005) (International Diabetes Federation), with discriminating factor being the presence of abdominal obesity [6]. Figure 1 presents the prevalence of the presence of IDF criteria for MS and Table 1 presents the patient medication at start and at the end of trial in n3 PUFA group of patients. Following Table 1, statins were most used – representing up to 90% and Figure 2 presents the use of individual statins at various doses.
Figure 1.
Representation of components of metabolic syndrome in n3 PUFA group of patients.
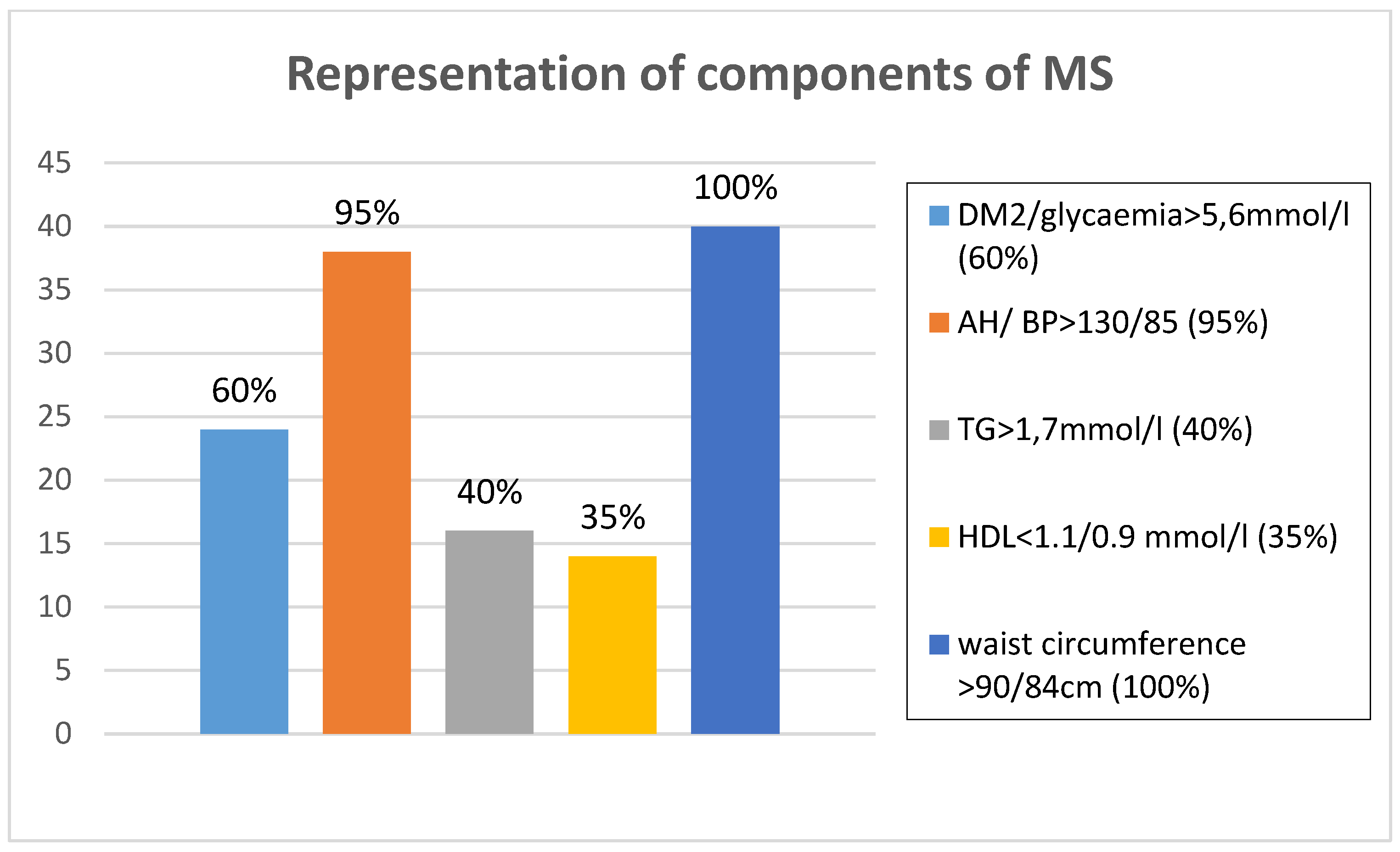
Figure 2.
Representation of statin therapy (%) in n3 PUFA group of patients.
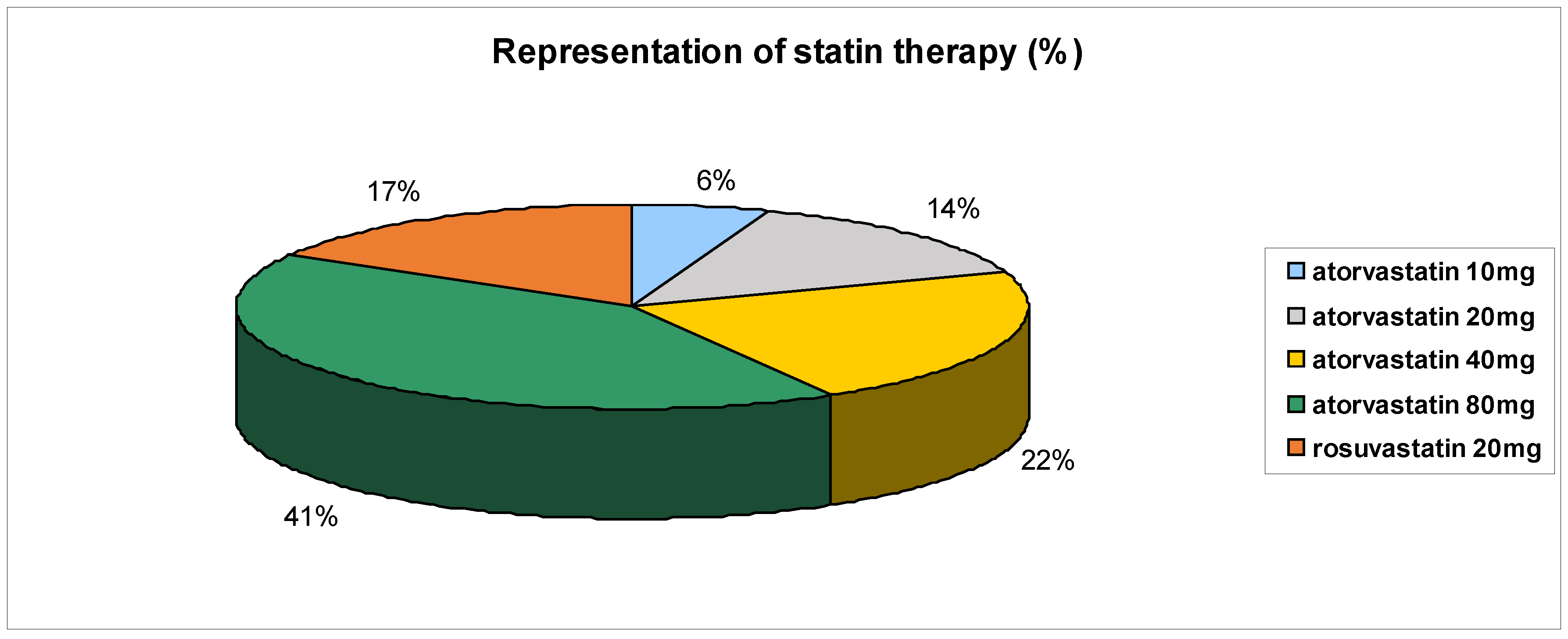
Figure 3.
Normal endothelial function (vasodilatation).
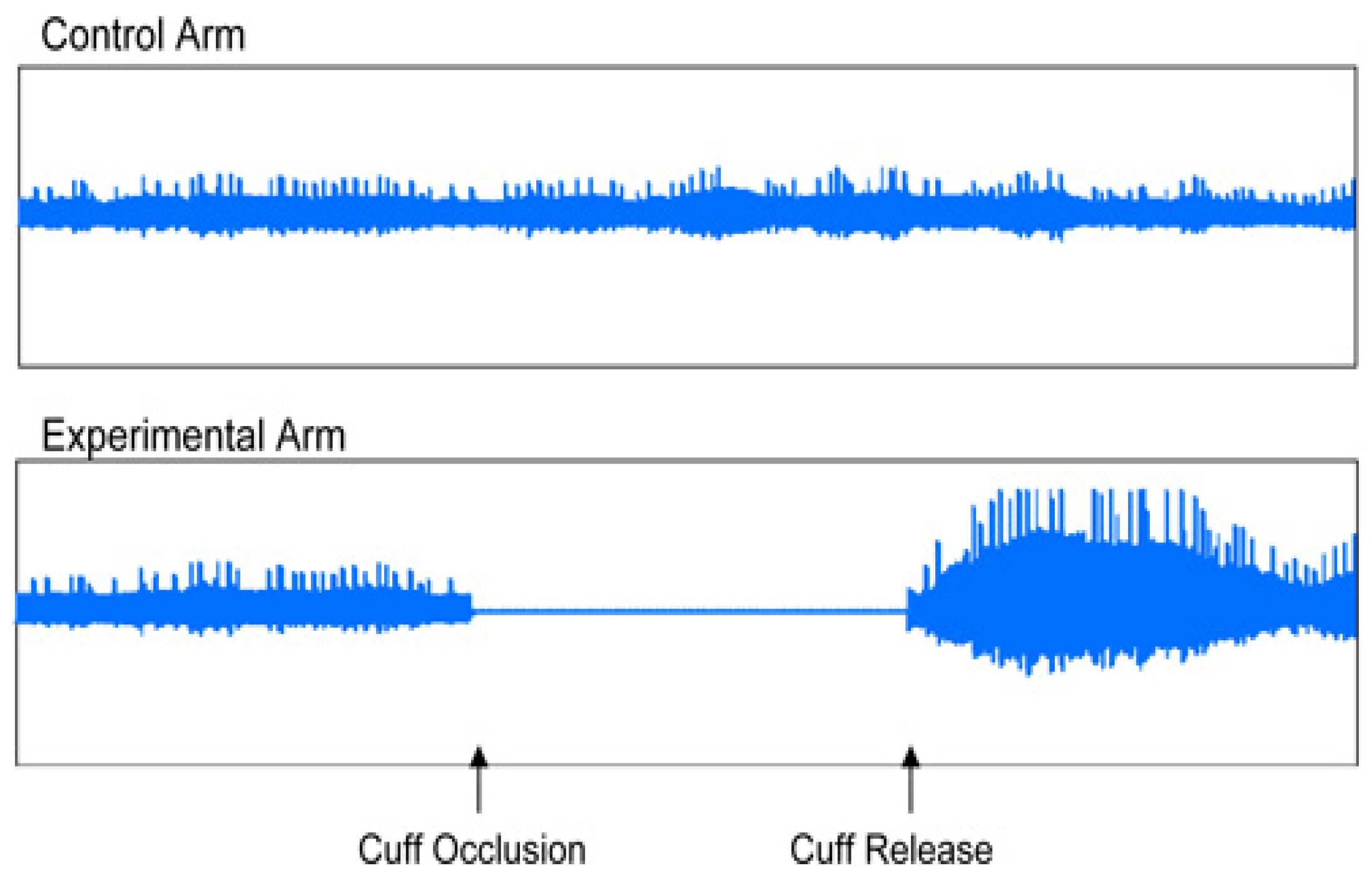
Figure 4.
Endothelial dysfunction.
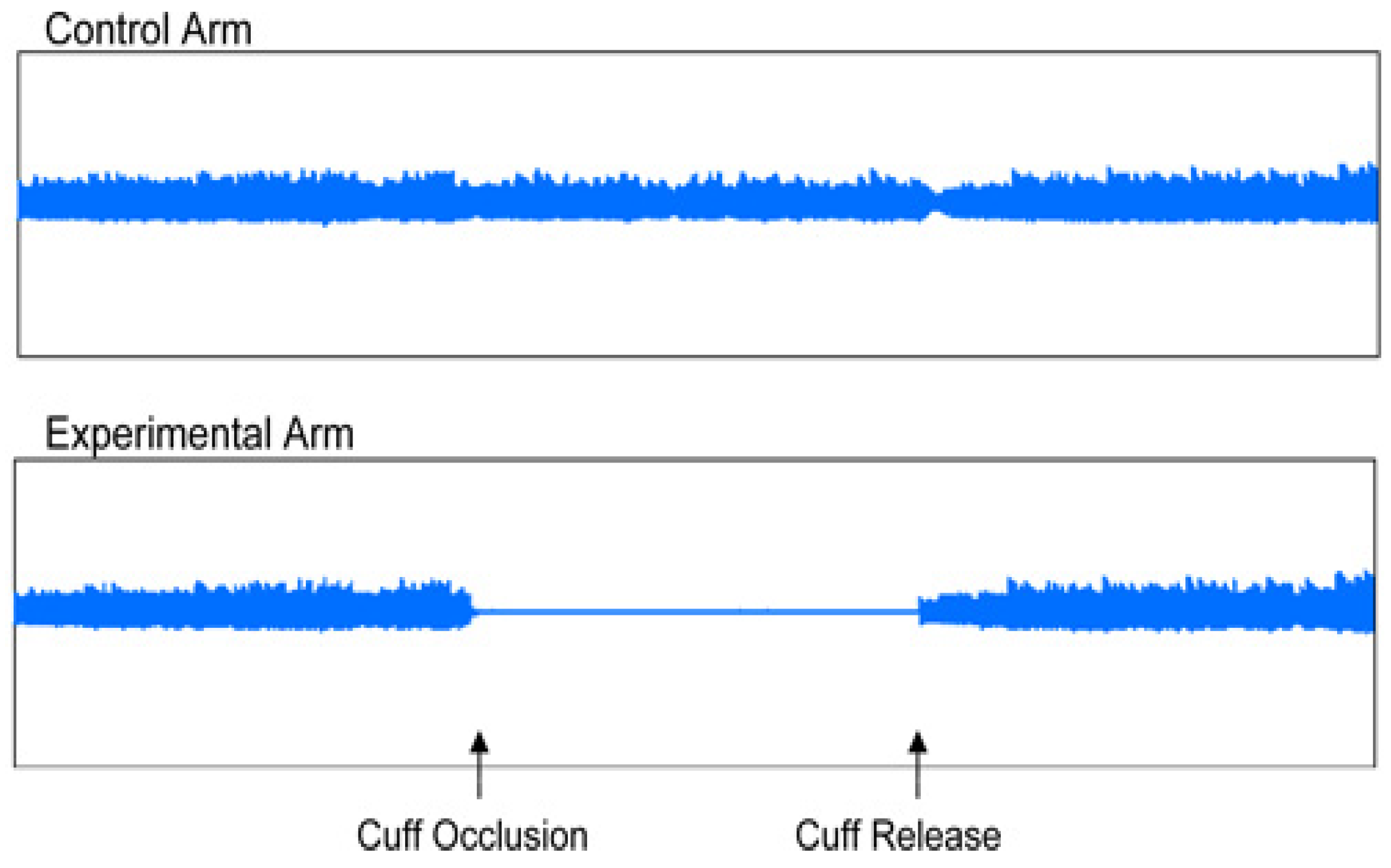

Table 1.
Medication in n-3 PUFA group of evaluated patients.
| Medication | N. of Patients at Start | N. of Patients at End | p | % |
|---|---|---|---|---|
| ACEi | 25 | 22 | NS | 62.50 |
| Beta-blocker | 32 | 32 | NS | 80.00 |
| Calcium channel blocker | 14 | 14 | NS | 35.00 |
| Sartans-AT1 Blockers | 12 | 12 | NS | 30.00 |
| Alfa-blocker | 12 | 12 | NS | 30.00 |
| Diuretics | 30 | 28 | NS | 75.00 |
| Acetylsalicylic acid | 15 | 15 | NS | 37.00 |
| Trimetazidin | 18 | 18 | NS | 45.00 |
| Insulin | 6 | 6 | NS | 15.00 |
| Oral Antidiabetics | 12 | 12 | NS | 30.00 |
| Nitrates | 10 | 10 | NS | 25.00 |
| Clopidogrel | 7 | 7 | NS | 17.00 |
| Allopurinol | 8 | 8 | NS | 20.00 |
| Proton pump inhibitors | 2 | 2 | NS | 5.00 |
| Warfarin | 3 | 3 | NS | 7.50 |
| Dabigatran | 1 | 1 | NS | 2.50 |
| Rivaroxaban | 2 | 2 | NS | 5.00 |
| Ivabradine | 4 | 4 | NS | 10.00 |
| Propaphenone | 1 | 1 | NS | 2.50 |
| Amiodarone | 1 | 1 | NS | 2.50 |
| Digoxin | 2 | 2 | NS | 5.00 |
| L-thyroxine | 3 | 3 | NS | 7.50 |
| Prasugrel | 1 | 1 | NS | 2.50 |
| Statin | 36 | 34 | NS | 90.00 |
| Fibrat | 8 | 8 | NS | 20.00 |
| Ezetimibe | 6 | 6 | NS | 15.00 |
Patient population was based on patients examined at the out-patient cardiology office (academic based) Kosice as well as the patients referred by cooperating cardiologists. Patients who took any nutrition supplements containing n-3 PUFA in the course of the last 6 months were not enrolled. When enrolling the patients, we focused especially on clinically stable patients who were not expected to have their pharmacotherapy or lifestyle changed in the course of the observed study period.
Upon signing the informed consent form, all patients had physical checkup, including blood pressure measurement, waist and hip circumference measurements, body height and body weight. Laboratory tests were performed, and the patient was evaluated using EndoPAT device. At the beginning of the study, the patients initially received n-3 PUFA (ZenixX Vital) at the dose of 2.4 grams per day, divided in three daily doses of 800 mg. All tests were performed before starting the study therapy and at the end of the subject period after three months (± 1 week). The effect of treatment with n-3 PUFA on ED was assessed on the following basis:
1. selected laboratory markers and ED risk factors: glutathione-peroxidase (GPX), homocysteine (Hcy), lipoprotein (a) (Lp(a)), apo-lipoprotein B (ApoB)
2. markers of arterial stiffness – augmentation index (AI) and index of reactive hyperemia (RHI) – endothelium function parameter – examined using EndoPAT 2000 device
Laboratory Markers Evaluation
Of the assessed parameters, upon sample collection the Lp(a), ApoB and Hcy were processed by local laboratory, specific ED markers such as GPX were sent in vials with heparine to the Department of Experimental Medicine, Pavol Jozef Safarik University, Kosice, Slovakia where centrifuged plasma was frozen (-80°C) until individual tests were to be performed. Upon thawing, 50 ul of heparinized blood was added to 2 ml of dilution solution. Upon measurement of Hb concentration in the resulting hemolysate, the GPX activity was determined using RANSEL kit (RANDOX, Great Britain) using automatic analyzer Daytona. GPX activity in control samples was determined with each measurement series [7].
Assessment of Endothelial Dysfunction Using EndoPAT 2000
EndoPAT 2000 is a simple method for non-invasive measurement of ED. The method involves the measurement of the changes of vascular tone in peripheral vascular bed (PAT – peripheral arterial tone), using plethysmography, i.e. the measurement is independent of the investigator. EndoPAT assessment involves vasodilation – hyperemia following previous application of tourniquette on the extremity. EndoPAT measures the signal from the vascular bed of the entire finger, including microcirculation. The test enables differentiation between systemic and endothel-induced vaso-reactivity, the measurement is performed simultaneously on both upper extremities and the resulting curves are compared. The assessment needs to be performed in a separate, quiet and warm room. Patient preparation before the assessment is required – the patient should be fasting for at least 4 hours, avoiding caffeine, nicotine, vitamins or any other medication for 8 hours, as these may affect the vascular tone [8]. During the test, usually taking about 20 minutes, the patient is in supine or semi-sitting position, most commonly with closed eyes, no talking and no movement of upper extremities to avoid interference with the electrode signals. The sensing electrodes were placed on both index fingers, subsequently they were inflated, and signal check was carried out. The signal was recorded by the computer and observed by investigator in the form of 2 curves throughout the test. During the first 5 minutes the upper extremity was left without occlusion, subsequently the cuff was inflated using pressure gauge to the pressure of at least 200 mmHg for at least 5 minutes, after that the cuff was deflated and the signal after occlusion was observed for at least additional five minutes. The outcome of the test was automatically assessed using the system software, using two parameters: reactive hyperemia index (RHI) and augmentation index (AI) [8].
Statistical Analysis
To describe the population, basic description statistics was used for continuous variable – number, mean value, standard deviation, minimum and maximum values and 95% confidence interval for mean value. For categorical values, absolute and relative frequency was used. To compare the mean values of continuous parameters for two and more groups, scatter analysis was used. Chi-square test was used to compare to categorical variables. Pair t-test was used to determine the effect of treatment, comparing the parameter values at the beginning and at the end of the therapy. When testing hypotheses, we considered significance value of 0.05.
Results
Supplementation with n 3-PUFA significantly affected the decrease of ApoB (0.94 ± 0.36 vs. 1.13 ± 0.35, p = 0.001), homocysteine (13.78 ± 3.05 vs. 19.3 ±5.29, p = 0,001) and increase of GPX (41.65 ± 8.90 vs. 45.20 ± 8.01, p=0.001). Lp(a) did not changed during this stort pilot trial (0.30 ± 0.29 vs. 0.29 ± 0.33, p=NS) (Table 2). Among all observed subjects, 3 patients (7,5%) failed to come to the follow-up visit after 3 months due to voluntary discontinuation of the study treatment in the active group of patients. We did not observed any significant changes in laboratory biomarkers in placebo group of patients
Very interesting results were observed upon testing the ED using EndoPAT 2000. Of the total number, in 37 subjects there was a statistically significant difference in reactive hyperemia index (RHI), which reflects endothelial function, and augmentation index (AI), which provides an indication of arterial stiffness. RHI increased from baseline values of 1.62 ± 0.42 to 1.96 ± 0.62 after treatment, p=0.005, AI decreased from 14.66 ± 19.55 to 9.21 ± 15.64 (p = 0,002) after three months of treatment. No significant changes or improvement was visible in placebo group of patients during the trial. (Table 3). Statistical significance was observed even between the groups of patients during the trial (Table 4).
Discussion
Based not only from evidence based medicine data but also from our pilot trial we could conclude that n-3 PUFA represent a benefit for MS patients due to the lipid-lowering effect – through positive effect on atherogenic dyslipidemia. We have also demonstrated that the supplementation with n-3 PUFA leads to the improvement of endothelial dysfunction in the MS patients, therefore we can assume the effect on atherogenic process at this level, as well as the potential use of n-3 PUFA in comprehensive treatment of MS, since ED represent the basic common denominator in the pathogenesis of all components of MS.
ED occurs in the early stages of atherosclerosis, where disorders in the reactivity of blood vessels precede the structural changes of the vascular wall, resulting from the joint action of all atherogenic and athero-protective factors. All known risk factors of atherosclerosis, such as dyslipidemy, hypertension, diabetes, smoking, age, menopause are associated with ED. In the recent 10 years, attention has been focused on additional important risk factors of atherosclerosis, i.e. also ED, including: ApoB, ApoA, triglycerides, triglyceride-rich lipoproteins, small dense LDL particles, oxidized LDL, oxidized LDL antibodies, Lp(a), Hcy, C-reactive protein measured using high-sensitivity method (hsCRP) [9]. Further below we shall discuss the risk factors and markers of ED that we observed.
Measurement of ApoB in MS patients is very important. These patients sometimes have normal levels, but in reality their LDL consist of the population of so-called “small dense LDL particles”, with very high atherogenic potential. These small dense LDLD-particles contain greater percentage of Apob and the measurement of ApoB helps us to better estimate the proportion of this high-risk population of LDL. The AMORIS study (Apolipoprotein MOrtality RISk study), as well as the large international study INTERHEART have shown that apoprotein B levels as well as the apoB/apoA-I ratio significantly improve the estimate of cardiovascular risk [10]. In our work we have shown, that supplementation of n-3 PUFA in patients with MS has lead to significant decrease of ApoB. Similar results have been shown also by multicenter randomized study MARINE [11]. Even though it has to be admitted that only EPA (eicosapentaenoic acid) was supplemented in this study – as compared to our study where a combination of EPA+DHA (deoxyhexaenic acid) was used), (EPA at the dose of at least 155g, DHA at least 520g). However, the observation period was 12 weeks as well.
Another risk factor of ED is hyperhomocysteinemia (HHcy), even though its causal relation to CV risk is subject to controversial discussion, as even large randomized studies such as NORVIT, HOPE-2, SEARCH failed to show that the reduction of Hcy would lead to decrease of CV risk [12]. Although the multicenter, randomized, placebo-controlled, double blind study SU.FOL.OM3 (Supplémentation en Folates et Omega-3) has shown significant decrease of Hcy following the treatment with n-3 PUFA, surprisingly, this has not resulted in the reduced CV morbidity [13]. In our study, following the supplementation with n-3 PUFA, we observed significant decrease of Hcy levels, but to demonstrate the effect of CV morbidity, longer observation is needed as well as larger patient population would be required, possible also higher dosage of n-3 PUFA than that used in SU.FOL.OM3, this could therefore be the objective of future clinical studies. However, an interesting finding involves the fact that Hcy, probably through increased vascular oxidative stress and atherothrombosis – partially suppresses the expression go GPX-1 gene, located at the 3p21.3 chromosome. Among many factors that contribute to the risk of atherosclerosis in plasma, great emphasis is placed on GPX-3, basic extracellular peroxidase, that plays a significant role in the modulation of oxidative stress. Lack of GPX-3 is associated with reduced biological availability of the nitric oxide and increased activation of platelets [14,15]. In our study, following the treatment with n-3 PUFA, we have shown significant increase of GPX, thus confirming the parallel antioxidant effect of n-3 PUFA, that significantly affects the ED and the process of atherogenesis.
Another independent risk factors of development of CV disorders is the increased level of Lp(a), as shown by currently available meta-analyses of epidemiological studies. Lp(a) increases the risk of stroke and death associated with vascular events in elderly males – independently of LDL-cholesterol levels. Reduction of Lp(a) is the secondary priority, following the reduction of LDL cholesterol and total cholesterol [16]. In our population n-3 PUFA did not significantly decreased the Lp(a), but enrolling plasma levels in our observed patients did not reach significant values at all.
Endothelial dysfunction plays important role in Long Covid syndrome as well reported by recent papers, where COVID-19 could impair ED directly as viral effect or via cytokines inflammatory response (17) on endothelial cells reducing nitric oxid bioavailability. More common in patients with non-respiratory symptoms, Long Covid-19 symptoms could be persistent due to ED, that’s why better care for the patients could be done by n-3 PUFFA supplementation. These conclusions need to be confirmed by another pilot, placebo controlled trial.
In addition to laboratory assessment of AD, non-invasive measurement of ED using EndoPAT 2000 is currently coming to the center of attention. This method involves the measurement of the changes of vascular tone in the peripheral vascular bed (PAT – peripheral arterial tone) using plethysmography. The common principle for EndoPAT 2000 and flow mediated dilation (FMD) is the vasodilation-hyperemia, following the previous occlusion of the extremity. A significant advantage compared to FMD is the fact that EndoPAT 2000 is also a measure for arterial stiffness. Arterial stiffness is increased in various pathological conditions, such as ischemic heart disease, MS, chronic kidney disease and others [1]. In our work, we assessed the endothelial function using EndoPAT 2000, based on the values of two parameters – RHI and AI. There are no official reference values available for RHI, but in general, RHI values under 1,67 are classified as ED, while the higher values of RHI are considered normal or represent the improvement of the endothelial function. Normal range of AI is between -30% and -10%, the limit value of AI is between -10% and 10% and abnormal values of AI are above 10% [19,20]. This method was used to demonstrate the improvement of the parameters of ED and arterial stiffness in our population of MS patients after 3 months of n-3 PUFA supplementation vs placebo group of patients.
Limitations of the Study
The study was limited by the low number of subjects, affecting the results of the effect on ED. Another limitation is the duration of observation period – a 3-month observation is not necessarily sufficient to assess the change of endothelial function. Additionally, it has to be said, that our study did not involve a homogenous population of subjects (the subjects took statins at various doses, in monotherapy as well as in combination with other agents, and for different length of time before the start of the combination therapy), possibly affecting the results due to their known pleiotropic effects. Another source of possible errors involved the assessment using the highly sensitive device – EndoPAT 2000, despite our effort to ensure strict observation of the requirements and procedures.
Conclusions
Our three-month observation has shown that n-3 PUFA improved ED in MS patients, as assessed by two selected markers, using two different methods (laboratory and plethysmography measurements using ENDOPAT 2000). n-3 PUFA supplementation (2.4 g per day) was associated with significant reduction of ApoB and Hcy and significant increase of GPX anti-oxidant enzyme. At the same time there was a significant improvement of arterial stiffness, as assessed by significant reduction of AI and improvement of ED – assessed by significant increase of RHI. We did not observed positive changes of placebo group of patients.
Effect on individual components of MS on the basis the possible positive effect of supplementation of n-3 PUFA on ED appears to be one of the promising alternatives available to modify the atherogenic process at the level that should be investigated by future clinical studies.
Acknowledgments
This publication was supported by grant AKARDIO COVID-19, ITMS: 313011AUB1, Operational Program Integrated Infrastructure, co-founded by European Regional Development Fund.Acknowledgement also applies to PLEURAN, s.r.o.- distributor of ZenixX Vital for the Slovak Republic, for providing n-3 PUFA.
References
- Bang HO, Dyerberg J, Nielsen A. Plasma lipid and lipoprotein pattern in Greenlandic west-coast Eskimos. Lancet. 1971; June 5:1143-1145.
- Burr ML, Fehily AM. Gilbert JF et al. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: Diet and Reinfarction Trial (DART). Lancet 1989; 2: 757-761.
- GISSI-Prevenzione Investigators. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Lancet 1999; 354: 447-455.
- Von Schacky C, Angerer P, Kothny W, Theisen K, Mudra H. Study on Prevention of Coronary Atherosclerosis with Marine Omega-3 fatty acids (SCIMO)—first results of a randomized double blind study. Can J Cardiol 1997;13(suppl):42B.
- Mori TA.: Dietary n-3 PUFA and CVD –a review of the evidence. Proc Nutr Soc. 2014 Feb;73(1):57-64.
- Alberti KGM.M, Zimmet PZ, Shaw JE. The metabolic syndrome-a new world-wide definition from the International Diabetes Federation consensus. Lancet. 2005;366:1059- 62.
- Šipulová, Rácz : Hodnotenie a modifikácia metódy Ransod. Lab. Diagnostika, 2, 1997: 144-148.
- Axtell AL, Gomari FA, Cooke JP. Assessing Endothelial Vasodilator Function with the Endo-PAT 2000. J. Vis. Exp. (44), e2167. [CrossRef]
- Ganz P, Vita JA. Testing endothelial vasomotor function. Nitric oxide, a multipotent molecule. Circulation 2003;108:2049–2053.
- Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART Study): case control study. Lancet 2004;364:937−952.
- Bays HE, Ballantyne CM, Kastelein JJ, et al. Eicosapentaenoic acid ethyl ester (AMR101) therapy in patients with very high triglyceride levels (from the multi-center, placebo-controlled, randomized, double-blind, 12-week study with an open-label extension [MARINE] trial). Am J Cardiol 2011; 108:682-690.
- Mori TA, et al. Omega-3 fatty acids and cardiovascular disease: epidemiology and effects on cardiometabolic risk factors. Food Funct. 2014 Sep;5(9):2004-19.
- Blacher J, Czernichow S, et. al. Homocysteine, folic acid, group B vitamins and cardiovascular risk. Arch Mal Coeur Vaiss. 2005 Feb;98(2):145-52.
- Blankenberg S, Rupprecht HJ, Bickel C, Torzewski M, Hafner G, Tiret L, et al. Glutathione peroxidase 1 activity and cardiovascular events in patients with coronary artery disease. N Engl J Med. 2003;349:1605–13.
- Prabhakar R, Morokuma K, Musaev DG. Peroxynitrite reductase activity of selenoprotein glutathione peroxidase: A computational study. Biochemystry. 2006; 45: 6967-77.
- Riche DM., East HE, Priest HM.: Practical management of dyslipidaemia with elevated lipoprotein (a). J Am Pharm Assoc 2008; 48(6): 803-7.
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418.
- Charfeddine S, Ibn Hadi Amor H, Jdidi et al. Long COVID 19 Syndrome: Is It Related to Microcirculation and Endothelial Dysfunction? Insights From TUN-EndCOV Study. Front. Cardiovasc. Med. 8:745758.
- Nichols WW., Singh B.M.: Augmentation index as a measure of peripheral vascular disease state. Curr Opin Cardiol. 2002 Sep.; 17(5):543-55.
- Jedlickova L, Merkovska L, Jackova Stovkova L et al. Effect of Ivabradine on Endothelial Function in Patients with Stabile Angina Pectoris: Assessement with EndoPAT 2000 Device. In Advances in Therapy 32(10). Nov2015.
Table 2.
Comparison of selected laboratory markers and risk factors of endothelial dysfunction. before and after 3-month treatment with n-3 PUFA.
Table 2.
Comparison of selected laboratory markers and risk factors of endothelial dysfunction. before and after 3-month treatment with n-3 PUFA.
| Number | Before Treatment | After Treatment | p | |
|---|---|---|---|---|
| Lp(a) | 37 | 0,30 ± 0,29 | 0,29 ± 0,33 | NS |
| ApoB | 37 | 1,13 ± 0,35 | 0,94 ± 0,36 | 0,001 |
| HCYS | 37 | 19,31 ± 5,29 | 13,78 ± 3,05 | 0,001 |
| GPX | 37 | 41,65 ± 8,90 | 45,20 ± 8,01 | 0,001 |
Table 3.
Comparison of results of ENDOPAT 2000 before and after 3-months supplementation with n-3 PUFA vs placebo group.
Table 3.
Comparison of results of ENDOPAT 2000 before and after 3-months supplementation with n-3 PUFA vs placebo group.
| N3 PUFA Group | N | Before Treatment | After Treatment | p |
|---|---|---|---|---|
| RHI | 37 | 1.62 ± 0.42 | 1.96 ± 0.62 | 0.005 |
| AI | 37 | 14.66 ± 19.55 | 9.21 ± 15.64 | 0.003 |
| Placebo group | ||||
| RHI | 40 | 1.51 ± 0.38 | 1.51 ± 0.38 | NS |
| AI | 40 | 16.46 ± 17.43 | 18.89 ± 13.49 | NS |
RHI- reactive hyperemia index, AI- augmentation index.
Table 4.
Comparison of results of ENDOPAT 2000 before and after 3-months supplementation with n-3 PUFA vs placebo group (between groups).
Table 4.
Comparison of results of ENDOPAT 2000 before and after 3-months supplementation with n-3 PUFA vs placebo group (between groups).
| Before Treatment N3 PUFA |
Before Treatment Placebo |
p | After Treatment N3 PUFA |
After Treatment Palcebo |
p | |
|---|---|---|---|---|---|---|
| RHI | 1.62 ± 0.42 | 1.51 ± 0.38 | NS | 1.96 ± 0.62 | 1.58 ± 0.42 | 0.001 |
| AI | 14.66 ± 19.55 | 16.46 ± 17.43 | NS | 9.21 ± 15.64 | 18.89 ± 13.49 | 0.001 |
RHI- reactive hyperemia index, AI- augmentation index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



