
Submitted:
22 May 2023
Posted:
24 May 2023
You are already at the latest version
Abstract
The human respiratory syncytial virus (hRSV) poses a serious risk to global public health and is a significant cause of severe lower respiratory infections. There are currently only a few therapies available to treat RSV infections, as well as no RSV vaccinations. Therefore, there is an urgent demand for clinically feasible, safe, and affordable RSV prevention and treatment alternatives. In this study, an ion-activated in situ gel comprising broad-spectrum antiviral 18β-glycyrrhetinic acid (GA) for antiviral action on RSV was developed. In this content, mechanical properties, sprayability, drug content, pH, ex vivo mucoadhesive strength, in vitro drug release pattern, and stability were all examined. Rheological properties were also tested by utilizing in vitro gelation capacity and rheological synergism tests. Finally, the optimized in situ gel's cytotoxic and antiviral activities on RSV cultured in human laryngeal epidermoid carcinoma (HEP-2) cell line were evaluated. In conclusion, the optimized in situ gel prepared with a combination of 0.5%w/w gellan gum and 0.5%w/w sodium carboxymethylcellulose demonstrated good gelation capacity and sprayability (weight deviation between T0 and T14: 0.34%), desired rheological synergism (mucoadhesive force (Fb): 9.53), mechanical characteristics (adhesiveness: 0.300 mJ ± 0.05), ex vivo bioadhesion force (19.67 g ± 1.90), drug content uniformity (RSD%: 0.494), and sustained drug release over period of 168 h (101.57% ± 0.53). The antiviral activity test results showed that the optimized in situ gel had strong anti-HRSV activity (EC50 simultaneous = 0.05 µg/ml, SI = 306; EC50 preinfection = 0.154 µg/ml, SI= 100) which was significantly higher than that of ribavirin (EC50 =4.189 µg/ml; SI= 28) used as a positive control against hRSV. In conclusion, this research has demonstrated the formulation of an effective antiviral nasal spray that has the ability to possess both prophylactic and virucidal activity.
Keywords:
in situ gel
; intranasal delivery
; gellan gum
; mucoadhesion
; 18β-glycyrrhetinic acid
; respiratory syncytial virus
; common cold
; antiviral activity
1. Introduction
Respiratory viruses lead to the majority of respiratory tract infections, which are the primary cause of morbidity and mortality for humans [1]. As the most frequent source of symptoms-based illness that results in a substantial financial burden from an increase in sick days, respiratory virus infections are a concern for global public health [2,3]. Additionally, among the leading causes of death in emerging nations is respiratory disorders [4]. The most common viruses involved are adenoviruses, respiratory syncytial virus (RSV), parainfluenza types 1, 2, and 3, and influenza A and B [5]. The viruses that cause the majority of these infections are seasonal, and they can affect both the upper and lower respiratory tracts. Nevertheless, unfavorable outcomes, such as the development of pneumonia, respiratory failure, and elevated mortality rates, are far more common in immunocompromised patients than in non-immunocompromised people [6,7,8]. According to the literature, it is emphasized that the rates of progression to lower respiratory tract infections and death due to common respiratory viral infections are high in immunocompromised patients, with the highest incidence in RSV [9]. Influenza (A and B) viruses and RSV are two of the primary risk factors that cause respiratory viral infection [10].
RSV, a non-segmented negative-strand, enveloped virus, is a member of the Paramyxoviridae family of RNA viruses. In terms of the number of genes and proteins, RSV is the most sophisticated member of the family [11]. Infection with RSV poses a considerable risk to the elderly and is one of the main causes of serious respiratory disease in newborns and young children globally [12]. RSV is a virus that can potentially lead to the common cold [13]. People of all ages can develop upper respiratory tract disease as a result of RSV infection [14]. RSV has been reported to be responsible for 160,000 annual death and 64 million infections worldwide, according to the World Health Organization [15]. RSV was first identified in chimpanzees who had cold-like symptoms in 1955 [16]. In the years that followed, the virus was also isolated from newborns suffering from serious lower respiratory tract disease [17]. Since that time, research has established that RSV is a common disease that affects almost all children with half of them acquiring two infections during this time [18]. RSV was found in 43%, 25%, 11%, and 10% of pediatric hospitalizations for bronchiolitis, pneumonia, bronchitis, and croup, respectively, in a 13-year prospective study of newborns and children in the United States (US) [19]. RSV has been additionally linked to chronic respiratory diseases include idiopathic pulmonary fibrosis, asthma, chronic bronchitis, and obstructive pulmonary disease. Furthermore, it can have a major negative impact on the elderly, particularly those with weakened immune systems, chronic bronchitis, and other medical conditions including chronic obstructive pulmonary disease [20]. RSV has a similar impact to the non-pandemic influenza virus in terms of morbidity and mortality in the elderly [21]. RSV has a significant fatality rate in immunocompromised people, especially those who have received allogeneic bone marrow transplants. RSV also has a negative impact on people who have long-term conditions such chronic heart and lung illness, particularly asthma [22]. RSV has been identified to be responsible for 14,000 annual deaths and 177,000 hospital admissions among US people over the age of 65 [23].
RSV infections are typically transferred through intimate contact, however they can also be conveyed through aerosolized droplets into the environment. RSV infection may move to the tiny bronchioles or alveoli of the lower respiratory tract following an initial replication period in the epithelial tissue of the nasopharynx and upper respiratory tract. Host immunological reactions to RSV infection are brought on by an increase in mucus production, inflammation, airway narrowing that results in bronchiolitis in young children, and acute respiratory illness in older persons or those with underlying chronic diseases [24]. Few methods for preventing or treating RSV infection have been established, despite years of continuous work. Since RSV was discovered to be a human infection more than 60 years ago, disappointingly no approved vaccine has yet to be discovered [24]. The inadequate immunological response of humans to RSV primarily is one explanation for this. For instance, 2 months after a prior infection, adult participants may be infected with RSV again [12]. The possibility of disease enhancement by vaccines is another obstacle to vaccine development. When a formalin-inactivated RSV vaccination was examined in the 1960s, those who received it were more seriously ill the following RSV season than those who received a placebo [25,26]. The mechanism behind this is still unclear, however mice immunized with formalin-inactivated RSV exhibit preferential stimulation of the Th2 subtype of helper T cells. When infected with RSV, this in turn causes more inflammatory reactions in the lungs [27]. In addition to these obstacles, the frequent mutation of RSV, like that of the influenza virus, makes the development of vaccines particularly challenging [28]. Only two RSV antiviral medications have been given the FDA's approval to treat or prevent serious RSV-related respiratory tract infections: aerosolized ribavirin for treatment and palivizumab (Synagis®) for prophylaxis [10]. A broad-spectrum antiviral drug having efficacy against RSV and other RNA viruses including hepatitis C and the Zika virus is the guanosine analog ribavirin [29,30,31]. A number of studies have shown that this medication has a positive impact on preventing RSV replication. Infected cotton rats with RSV lung titers were treated with ribavirin, which demonstrated antiviral efficacy against RSV [32]. Similar to adults, children treated with aerosolized ribavirin early in infection have shown considerable clinical improvements [33]. However, ribavirin's nonspecific anti-RSV efficacy, high potential for toxicity, and relatively expensive cost limit its use in practice [34]. Additionally, many institutions can no longer afford this due to recent changes in the pricing structure [35]. Additionally, ribavirin has not had a significant effect on clinically important outcomes like mortality, hospital stay length, need for mechanical breathing, or admission to an intensive care unit [36,37,38]. In high-risk newborns and young children, RSV immunoprophylaxis is particularly helpful in preventing life-threatening RSV infections [37]. The only FDA-approved immunoprophylaxis for severe RSV lower respiratory tract infection in certain high-risk pediatric populations, such as infants born at or below 35 weeks' gestational age (wGA), children with hemodynamically serious congenital heart disease, and children with chronic lung disease of prematurity, is palivizumab, a humanized monoclonal antibody (mAb) [37]. Palivizumab is solely advised for usage as a preventative measure; it is not recommended for the management of RSV infection. Data show that once RSV infection has occurred, it has had no impact on the results [39]. Palivizumab has been shown to be both effective and safe for preventing RSV infection in high-risk pediatric groups in randomized, placebo-controlled trials and post-licensure efficacy studies [40,41]. Nevertheless, high cost, a short half-life requiring monthly injections, and a tight RSV immunoprophylaxis guideline from the American Academy of Pediatrics are a few obstacles preventing palivizumab use in compliance with its license [42]. RSV infection cannot be prevented by a vaccination at the moment [38]. The demand for clinically viable, safe, and cost-effective RSV prevention and treatment alternatives is therefore paramount.
Herbal antiviral agents may be a potential alternative to humans for respiratory viruses for therapeutic or prophylactic purposes. “18β-glycyrrhetinic acid (GA)”, a broad-spectrum potent antiviral herbal agent, is a pentacyclic triterpenoid that is the key metabolite of glycyrrhizic acid, the main water-soluble component of licorice root. GA and its derivatives are components of natural origin with a wide spectrum of bioactivity, including antitumor [43,44,45], antiviral [46], antimicrobial [47], anti-ulcer [48], antidiabetic [49], hepatoprotective [50], cardioprotective and neuroprotective effects [51]. Hardy et al. demonstrated that GA therapy prevented rotavirus replication that most likely took place after virus entry. When GA was applied to infected cultures after viral adsorption, it was discovered that the yields of rotavirus were reduced by 99%. The viral proteins VP2, VP6, and NSP2 were significantly downregulated [52]. Additionally, strong hRSV activity of GA was shown. It largely prevented viral attachment, stimulated interferon (IFN) secretion, and inhibited HRSV internalization. In addition to blocking viral attachment, GA also inhibits viral replication and boosts host cell activity [53].
The viral loads in symptomatic and asymptomatic patients are comparable, and the nasal cavity and nasopharynx have some of the highest viral loads in the body. Given that nasal secretions contain a virus that might transmit and that contagiousness seems to be at its peak before or immediately after symptom start, these "silent spreaders" may accidentally contribute to the exponential expansion of disease. In order to accomplish these goals, intranasal delivery of antiviral medications or agents may present an additional choice for limiting the spread of disease, treating the nasal disease, and supplying perioperative antisepsis [54].
One of the most significant barriers to successful active substance delivery through the nose is mucociliary clearance, as it reduces the residence time of the drug in the zone of action. In nasal applications, the effectiveness can be increased by prolonging the contact time between the nasal mucosa and the formulation. For this purpose, mucoadhesive carrier systems are being developed. Increasing the viscosity using mucoadhesive polymers may be beneficial to avoid the formulation draining and to extend the contact time between the nasal mucosa and the drug [55]. The adherence of a polymer to a mucus layer is referred to as mucoadhesion. The mucus layer is a sticky and viscous layer composed primarily of mucin and water [56,57]. The ability of a polymer to bind to the mucus layer depends on several factors such as swelling, molecular weight and flexibility of polymer chains, as well as chemical bond formation [58,59]. Compared to conventional liquid nasal formulations, mucoadhesive systems form a gel following contact with the nasal mucosa, thanks to its polymer structure. Therefore, they not only extend the contact time between the nasal mucosa and the active substance, but also the release of the active substance takes place in a prolonged manner [60,61]. However, because of the high consistency of the formulation, nasal application of typical mucoadhesive gels can be technically difficult and problematic to provide precise medication dosing. On the other hand, due to the challenging manufacturing method and high manufacturing costs, mucoadhesive powders are not a widely demanded product. Additionally, they might make the tissue feel gritty and irritate the nasal mucosa [62]. Due to these factors, in situ gels (also known as environmentally sensitive gels), a novel dosage form employed in nasal medication applications, have recently grown to be quite appealing [63]. Compared to nasal formulations in liquid form, nasal in situ gels are low viscous fluids prior to administration and form a gel by changing the polymer structure after contact with the nasal mucosa. Therefore, in situ gels not only extend the contact time between the nasal mucosa and the drug, but also the drug release occurs slowly and continuously. Transition from solution form to gel form (sol-gel phase transition) can occur with a change in pH (eg. cellulose acetate phthalate), a change in temperature known as thermogelling (eg. poloxamer 407), or the presence of cations (eg. gellan gum) [55]. In situ gels not only have the benefits of a solution such as ease of application, simplicity of preparation, no foreign body feeling and complete dosing, but also an increased residence time in the nasal mucosa like a gel. These advantages improve treatment efficacy and patient compliance [62].
A deacetylated, anionic, exocellular bacterial polymer called gellan gum was first identified in 1978. The tetrasaccharide repeating unit of 1-L-rhamnose, 1-D-glucuronic acid, and 2-D-glucose is released by Sphigomonas paucimobilis, formerly known as Pseudomonas elodea. The development of double-helical junction zones is the first step in the mechanism of gelation. Next, the double-helical segments are aggregated to create a 3-D network by complexing with cations and forming hydrogen bonds with water [64]. The type of cations in gellan gum solutions affects their ability to gel, and divalent cations work significantly better than monovalent cations to facilitate gelation. Deacetylated gellan gum (DGG) is sold under the trade names Gelrite® or Kelcogel® and is permitted for use in food products in the USA and EU as a gelling, stabilizing, and suspending ingredient. Therefore, gellan gum is recommended to be used safely in pharmaceuticals. Furthermore, gellan gum can be used in bio-medical technology, including drug delivery systems and protein immobilization media, and is one of the most intriguing in situ gelling polymers for human body [55,64,65].
In the current study, a nasal mucoadhesive spray formulation of an ion-activated in situ gel containing GA with broad-spectrum antiviral activity for antiviral effect on RSV was developed and rheological characteristics with in vitro gelation capacity and rheological synergism, mechanical characteristics, sprayability, drug content, pH, ex vivo mucoadhesive strength, in vitro drug release pattern and stability analyses were investigated. Finally, cytotoxic and antiviral effects of the optimized in situ gel on RSV cultured in human laryngeal epidermoid carcinoma (HEP-2) cell line were tested.
2. Materials and Methods
2.1. Materials
18β-glycyrrhetinic (GA) 97%, dexpanthenol, benzalkonium chloride, and porcine gastric mucin (type II) were purchased from Sigma-Aldrich (St. Louis, MO), Kelcogel® CG-LA (deacetylated gellan gum, DGG) was kindly provided by Azelis (Istanbul, Türkiye), VANZAN® NF (xanthan gum) was kinly obtained from Vanderbilt Minerals, LLC (Norwalk, CT), Blanose™ (sodium carboxymethylcellulose, Na-CMC) and Benecel™ E10M (hydroxypropyl methycellulose, HPMC) were kindly gifted by Ashland (Istanbul, Türkiye), Carbopol® 974P NF was obtained as a gift from Lubrizol (OH, USA), Methanol ≥ 99.9% for liquid chromatography and ortho-phosphoric acid 85% were supplied from Isolab Chemicals (Istanbul, Türkiye). Fetal bovine serum (FBS), Dulbecco`s Phosphate Buffered Saline (DPBS), Antibiotic‒antimycotic solution (100×), Ribavirin, Minimum essential medium (MEM) were purchased from Sigma-Aldrich (St. Louis, MO), 0.25% Trypsin-EDTA (1×) solution was provided from (Diagnovum, Germany), Trypan blue dye was purchased from NutriCulture (UK), XTT [2,3-Bis- (2-Methoxy-4-Nitro-5-Sulfophenyl)-2H-Tetrazolium-5-Carboxanilide] kit was obtained from (Biological Industries Ltd., Kibbutz Beit Haemek, Israel). All other chemicals and reagents used in the study were of analytical grade.
2.2. Methods
2.2.1. Preparation of GA Loaded In Situ Gel Formulations
Formulation of In Situ Gelling Systems Using Only Gellan Gum
The Morsi et al. method was used to prepare GA-loaded in situ gels. [66]. In order to prepare a clear DGG solution, various concentrations of DGG (0.2% - 1%, w/v) were dispersed into distilled water and fully dissolved with moderate stirring for 20 minutes at 500 rpm on a 90 °C hot magnetic stirrer. Thereafter, the cooled DGG solution was then blended thoroughly with GA powders to get the final formulations. Then, other excipients including the isotonicity agent glycerin, the mucous moisturizer dexpanthenol, and the preservative benzalkonium chloride were added while being continuously stirred. Finally, the mixture was kept stirring for 24 hours. The process for producing GA-loaded in situ gels using only DGG is shown in Figure 1 below.
Formulation of In Situ Gelling Systems Using Combined Polymers
DGG was combined with four different mucoadhesive polymers (xanthan gum, HPMC, Na-CMC, or Carbopol® 974P NF) to prepare in situ gelling systems. The polymers were dissolved in deionized water in the DGG/xanthan, DGG/HPMC, and DGG/Na-CMC systems by heating at 90 °C for 20 minutes, then allowing to cool at room temperature. In order to prepare the systems that contain Carbopol® 974P NF, the polymer was sprinkled in cold deionized water, allowed to hydrate, and then mixed with DGG solution. The polymer solution was then continuously stirred with GA and additional formulation excipients to achieve a final polymer concentration of 0.5% w/w (xanthan gum, HPMC, Na-CMC, or Carbopol® 974P NF) together with DGG (0.4, 0.5, or 0.6% w/w). Finally, the mixture was kept stirring for 24 hours. The chemical compositions of different in situ gelling systems are shown in Table 1.
GA-loaded in situ gels were prepared using combined polymers, as shown in Figure 2 below.
2.2.2. Characterization of GA Loaded In Situ Gel Formulations
Gelatin Capacity of In Situ Gel Formulations with/without Mucoadhesive Polymers
Formulations (1.0 ml) were mixed with simulated nasal fluid (SNF) (0.5 ml), which contains 7.45 mg/ml NaCl, 1.29 mg/ml KCl, and 0.32 mg/ml CaCl2.2H2O in the transparent glass vials to measure the gelatin capacity of in situ gels. These transparent glass vials were then placed in a water bath set at 34 °C. İnverting the vial after 20 seconds, in situ gelation was observed by visual inspection [67,68]. An in situ gelation of formulation was also demonstrated by the rheological analysis using a cone-plate viscometer (Brookfield HA DV3T, Brookfield, UK). Each sample was examined in the viscometer, which had a spindle 52 suitable for gelled systems, at shear rates ranging from 20 to 100 rpm. All measurements were carried out in triplicates [66].
Rheological Evaluation
The same cone and plate viscometer was used to determine the rheological properties of the prepared in situ gels. The viscometer was equipped with a cone spindle 40 for the liquid in situ gels prior to gelation with SNF solution. For the case of gelled systems, the viscometer was equipped with spindle 52, and each sample was tested at shear rates ranging from 20 to 100 rpm (keeping a period of 10 seconds at each rpm). Each measurements were performed in triplicates [66].
In Situ Gel-Mucin Interaction Study
A straightforward approach was used to assess the 'rheological synergism' that results from mixing mucoadhesive in situ gels containing DGG with mucoadhesive polymer and mucin dispersions in order to measure the mucoadhesive force of the gels [69]. In specifically, it demonstrates a more than additive increase in the mixture's viscosity that results from the interactions between the chains of the two macromolecular species when mucoadhesive polymers and mucin dispersions are mixed. Mucin type II (8%, w/v) was dissolved in SNF and allowed to equilibrate for at least 2 hours. All mucin suspensions were used within 4 hours after preparation to prevent mucin degradation. The dispersion was then heated to 34 °C and after that, mixed with the in situ gels that had also been heated to the same temperature [70,71]. The viscosities of the mucin disperison, the in situ gels and the in situ gel–mucin mixture were estimated in triplicate using the Brookfield viscometer. Eq. (1) was used to calculate the viscosity component of the mucoadhesion.
where ηb is the viscosity due to the mucoadhesion, ηt is the viscosity of the mixture, ηm is the viscosity of mucin and ηp is the viscosity of the in situ gel formulation. Eq. (2) was used to calculate the mucoadhesive force.
where γ represents the shear rate at which the viscosity value was calculated [70].
ηb = ηt – (ηm + ηp)
Fb = ηb × γ
Mechanical Characteristics of In Situ Gels
The texture profile analyses of the produced in situ gels were examined using CT3 Texture Analyser (Brookfield, UK) in order to evaluate the mechanical parameters such as hardness, adhesiveness, cohesiveness and compressibility. With a set recovery period of 15 seconds between the end of the first compression and the start of the second, an analytical probe with a diameter of 12.7 cm was immersed twice into each sample to a defined depth of 10 mm and at a defined rate of 2 mm/s. Applied trigger force was 0.01 N. Triplicate analyzes were performed for each sample at 34 ± 1°C. TexturePro CT V1.6 Build was used for the calculations and data collection. Hardness (the amount of force necessary to cause a particular deformation), compressibility (the work required to deform the product during the probe's initial pass), adhesiveness (the work required to overcome the attractive forces between the sample's surface and the probe's surface), cohesiveness (the ratio of the area under the curve for the second compression cycle of the forcetime curve to the area under the curve for the first compression cycle) can all be determined from the force-time plots that result [62].
Ex Vivo Mucoadhesive Strength Test
A tensile test was utilized to assess the ex vivo mucoadhesion of ion-activated in situ gels using the same texture analyzer and probe as for texture profile analysis. The impact of changing the contact time (1, 2, 3, and 5 minutes) was examined in order to optimize the first contact time between in situ gels and nasal mucosa. In order to measure contact time and mucoadhesive force, formulations were allowed to come into contact with nasal mucosa. The contact time that yielded the maximum strength was chosen to be the optimum contact time required for sufficient adhesion.
Fresh sheep nasal mucosa was provided from the local slaughterhouse and cleaned with SNF solution. A thin layer of clean mucosa was placed on the instrument's test holder [72,73]. Prior to analysis, a thin layer of the respective formulation was formed around the cylindrical probe's (12.7 mm-diameter) surface by immerging it for 10 seconds in a beaker containing in situ gel formulations. After being touched the mucosal surface for 2 minutes with a compressive energy of 0.5 N, the probe was separated at a speed of 1 mm/s with a triggering force of 3 g. The force required to separate the contact between the mucosa and the formulation-containing probe was examined using the Texture Pro CT V1.3 Build 15 software [72].
Sprayability Analysis
Control of content uniformity and mass uniformity is crucial for ensuring dosage homogeneity in nasal spray treatments. The regulatory framework requires exact controls on dosage content or mass consistency [74]. With this aim, sprayability analysis was performed on the selected in situ gel formulations according to the literature [75]. According to Ph.Eur. recommendations, spray bottle pumps had to be primed five times at intervals of five seconds (or "priming") before measurements could be taken. After that, a single dose of 2 puffs was administered, and their unique masses were calculated using different flask weights. This process was also done at 7- and 14-day intervals to assess the mass homogeneity of the various in situ gels at various times of use.
Quantitative Determination of 18β-glycyrrhetinic Acid
A validated RP-HPLC method was used to analyze GA quantitatively, in accordance with a previously reported method. [76].
HPLC conditions: Chromatography analysis was carried out on a CTO-20A type Shimadzu high performance liquid chromatography (HPLC) with SPD-20A and LC-20AT unit, CTO-20AC column oven and a Nucleosil® C18 column (5 µm, 250x4.6 mm). The mobile phase was delivered via isocratic elution at a flow rate of 1.0 mL/min. The mobile phase, which contained methanol and 0.4% phosphoric acid (85:15), was passed through a 0.45 m membrane before usage.The injection volume was 20 μL. The temperature of the column was set at 35 °C, and a wavelength of 251 nm was used.
Preparation of solutions: The solutions were prepared by dissolving GA in methanol to obtain 500 ng/mL stock solutions for the HPLC method. The stock solution was then diluted with methanol to prepare standard working solutions (0.1, 0.5, 1, 2.5, 5, 10, 15, 20, 30 μg/ml).
Active Substance Content Determination
Drug content of the optimized in situ gel formulation was determined after mixing the in situ gel containing 0.5 mg GA with the solvent mixture (methanol and distilled water containing 0.4% phosphoric acid (85:15, v/v)) in a falcon tube volume up to 25 ml. The mixture was homogenized by vortexing for 5 minutes. After that, it was sonicated for 1 hour and then centrifuged at 4000 rpm for 10 minutes [77]. The supernatant was filtered (0.45 m) and the HPLC method described in section Quantitative determination of 18β-glycyrrhetinic acid was used to determine the concentration of GA.
Fourier Transform Infrared Spectrometry (FTIR) Studies
Drug–excipient interactions were further assessed using FTIR spectroscopy (Cary 630 FTIR Spectrometer - Agilent). The spectra for GA pure substance, physical mixtures of GA with DGG and Na-CMC (1:1) were analysed. Powder samples were scanned for IR spectra from 4000 to 600 cm−1.
In Vitro Release Study
In vitro release study was performed using dialysis bag method, as previously described, for the optimized in situ gel and the plain in situ gel (used as a control). [62]. In situ gel formulation with a known amount of GA (6 mg) was sealed inside a cellulosic dialysis membrane (Spectra-Por4 dialysis tubing, cut-off 12–14 kDa, Spectrum Laboratories Inc., USA) and then put into a beaker with 100 ml of SNF solution pH 5.5 (to mimic the pH of the nasal interstitial fluid). The tests were conducted at a temperature of 34± 1 °C, while the system was continuously shaken at 100 rpm in a water bath. 1 ml of the release medium was removed and replaced, at specified time intervals, with an equal volume of fresh, pre-warmed release solution. The GA content in the collected samples was examined using the validated HPLC-UV method described in section 2.2.2.7. Quantitative determination of 18β-glycyrrhetinic acid.
Physicochemical Stability
A sufficient quantity of in situ gel in amber glass bottles was stored at three different storage conditions for a period of 3 months: 25 ± 2 °C and 60% RH, 40 ± 2 °C and 75% RH, and 5 ± 3 °C. Formulations were evaluated for physical appearance, drug content, pH and viscosity, and in situ gelation at predetermined time intervals. All experiments were performed in triplicate [62].
2.2.3. Cell Culture Studies
Cells and Virus
Human respiratory syncytial virus (hRSV Long strain: ATCC VR-26) was cultured using human larynx epidermoid carcinoma cells [HEp-2; ATCC (the American Type Culture Collection) CCL 23]. Cells were cultured at 37 °C with 5% CO2 in MEM enriched with 10% FBS, 25 μg/ml amphotericin B, 10 mg/ml streptomycin and 10000 U/ml penicillin. ATCC-VR-26 coded HRSV was purchased from ATCC and reproduced in Virology Laboratory of Science Faculty of Selçuk University. The virus was propagated, as described above, on a 90% confluent cell monolayer in MEM with antibiotics and 2% FBS. The virus titer was calculated using the 50% tissue culture infectious dose (TCID50) method and then represented as TCID50 per 0.1 ml [78]. The virus was kept at -80 °C prior to use. Ribavirin is used as a positive control for hRSV inhibition. A ribavirin stock solution (1000 g/ml) was prepared using MEM without FBS and kept at -80 °C until use.
Cytotoxicity Assay
XTT-based cell proliferation kit (Catalog no. 20-300-1000) developed by the company of Biological Industries (Kibbutz Beit Haemek, Israel) was used to determine the cytotoxic effects of ribavirin, GA, the in situ gel containing GA and placebo in situ gel on HEp-2 cells. Tests were conducted according to the manufacturer's instructions as follows; two-fold decreasing serial dilutions were prepared according to log2 base from the stock solution of GA using MEM. 50 µl HEp-2 cell suspensions containing 2.5 × 105 cells per ml were added onto GA dilutions to making the final concentrations of the GA dilutions in the wells as 133.3 - 1.04 µg/ml. The same processes were applied for ribavirin, the in situ gel containing GA and placebo in situ gel using another microplate. The final concentrations of ribavirin in the wells were 500 - 0.98 µg/ml while the final concentrations of GA in situ gel formulation in the wells were 33.33 – 0.26 µg/ml. The microplates were also included cells control (CC) and media control (MC). The microplates were incubated for 2 days at 37 °C in a humidified incubator with 5% CO2. Then, 50 µl of a mixture of 5 ml XTT reagent and 0.1 ml PMS activator were added to each well. Microplates were incubated for an additional 3 hours to form the XTT formazan product. The average optical densities (OD) from the wells were recorded using an ELISA reader (Multiskan EX, Labsystems) at a test wavelength of 490 nm and a reference wavelength of 630 nm. The experiment was performed in triplicate, and the results were presented as the ratio of the average cytotoxicity to the cell control.
The percentage of cytotoxicity of test samples on HEp-2 cells was calculated using the following formula [79].
A: The OD of cell control
B: The OD for the cells treated with GA, in situ gels or ribavirin.
The calculated percentages of cytotoxic effects were graphed against the corresponding concentrations of the tested samples (GA, in situ gels and ribavirin). The GraphPad Prism 5.03 program was used to analyze the sample concentration that allowed 50% survival of HEp-2 cells (CC50) [80]. These determined CC50 values were used to assess the antiviral activity of GA, in situ gels and ribavirin. The maximum non-toxic concentrations (MNTCs) of GA, in situ gels and ribavirin were also determined by comparing OD with CC.
3. Results and Discussion
3.1. Optimization and Characterization of GA Loaded In Situ Gel Formulations
3.1.1. Gelatin Capacity of In Situ Gel Formulations
Ideally, an in-situ gelling system should contain a low viscous fluid to allow a nasal reproducible administration but go through an in-situ phase transition to create a gel that can tolerate shear stresses in the nasal passages and maintain drug release under physiological conditions [82]. As a result, the longer residence time in the nasal cavity and less mucociliary clearance would result from the increased viscosity [83]. However, nasal liquid has the potential to dilute DGG and influence the in situ gel's ability to gel [67]. To accomplish the necessary ion-sensitive sol-gel transition, DGG concentration had to be optimized. Therefore, preliminary attempts were undertaken to choose the DGG concentration that provides optimal gelation. Gelation capacity test were carried out by blending DGG with SNF. The findings showed that the DGG solution with a concentration more than 0.3% might quickly transform into a colorless and transparent gel. Accordingly, the sol-gel phase change is more favorable the greater the concentration of DGG, suggesting that the gelation characteristics were favorably associated with polymer concentration. However, the increased viscosity at the higher DGG concentration made it difficult to administer. Therefore, a DGG concentration below 0.7% was ideal to avoid discomfort with swelling of the gel after application and to prevent patient non-compliance. When the DGG concentration was lower than 0.4%, the in situ gel was so easily diluted by mucus present in nasal cavities that it would be challenging to ensure gel formation. This is because nasal fluid dilution has an impact on the gelation capacity. DGG concentration in in situ gel should therefore not be less than 0.4%. Taken together, due to their desirable gelling capabilities and adequate viscosity, DGG concentrations in the range of 0.4-0.6% w/w are chosen when optimizing the formulation of the intranasal in situ gel for further studies. These results were in good agreement with Hao et al. [68] and Cai et al. [67].
3.1.2. Rheological Evaluation
The most crucial aspects to consider when assessing the effectiveness of in situ gelling systems are viscosity and gelling capacity [66]. The formulation needs to have the ideal viscosity under storage conditions for simple administration into the nasal cavity, and it must quickly convert from sol to gel upon contact with SNF in order to maintain an extended residence time at the administration site.
By comparing the rheograms of several DGG formulations in the sol state, it was determined that a concentration-dependent increases in viscosity was seen, which was compatible with the findings of Morsi et al. (Figure 3) [66]. Due to the liquid state of the gel formulations, mixtures containing 0.2% to 0.6% DGG had low viscosity values at room temperature. However, the formulations transformed to a low viscous gel texture, and their viscosity increased as the DGG concentration increased to 0.7% or higher (Figure 3). In this case, it is considered that the sprayability of the in situ gels containing DGG at 0.7% and higher concentrations into the nasal passage and the homogeneous spreadability of the formulation on the nasal mucosa may be adversely affected. Therefore, for further research, DGG concentrations in the range of 0.4-0.6% w/w are preferable due to their appropriate viscosity values.
On the other hand, the addition of SNF to all formulations led to a significant increase in viscosity as a result of gelation (Figure 4). These ionic sensitive in situ gels behave as a non-Newtonian pseudo-plastic fluid with a typical shear thinning feature since the viscosity of mixtures of the DGG solutions and SNF at 34 °C rapidly decreased with regard to the applied shear rate. The potential intranasal use of in situ gels may benefit greatly from this condition. A pseudo-plastic system generally demonstrates an increase in viscosity after it enters the nasal cavity and comes into touch with the ions in the nasal fluid, extending the nasal residence time [68]. These results agree with the findings of other studies [66,67,84].
Different polymers are frequently combined to improve the characteristics of in situ gelling and mucoadhesive compositions. This method can result in improved mucoadhesion or superior gelling characteristics by reducing the amount of polymer in the system [85]. Despite the fact that DGG has mucoadhesive characteristics, these are inadequate to extend mucosal residence time as they are dependent on relatively weak forces like hydrogen bonds and van der Waals forces [86]. Therefore, the optimized selected concentrations of DGG (0.4-0.6%) were combined with four different mucoadhesive polymers (xanthan gum, HPMC, Na-CMC, or Carbopol® 974P NF), in order to investigate the potential synergistic effects brought on by the polymer combinations and to enhance the in situ gel compositions' mucoadhesive characteristics. As a result, by comparing viscosity values of in situ gels containing combined polymers with that containing only DGG, a significant increase in viscosity could be detected. It was found that according to the type of combined polymer, the increase in viscosity can be ranked in the order Carbopol > HPMC > xanthan gum > Na-CMC. The increase in viscosity for the cellulose derivatives could be explained by their ability to form in situ gels when their aqueous solutions are heated [87]. For Na-CMC, the transition temperature is in the range of 40 to 50 °C, and for HPMC, it is between 75 and 90 °C. The gelation temperature of MC is reported to be lowered to 32–34 °C by adding sodium chloride, while the transition temperature of HPMC can be lowered to around 40 °C by reducing the hydroxypropyl molar substitution [88]. The significant high viscosity of xanthan gum, on the other hand, can be linked to its anionic character and is known as an ion driven in situ gelling polymer. Its molecules become extended due to the electrostatic repulsions caused by the charged groups on the side chains [89]. In turn, this causes the molecules to align and join together through hydrogen bonds to form a weakly organized helical conformation that would immobilize free water and enhance viscosity [89]. A well-known polymer that induces in situ gelling due to pH is carbopol. It is a polyacrylic acid polymer that, when the pH is raised above its pK of around 5.5, exhibits a sol-gel phase transition in aqueous solution [90]. At low pH values and high pH values, the carboxylic groups of PAA receive and release protons, respectively. The electrostatic repulsion of the negatively charged groups causes the PAA to swell and expand up to 1000 times its initial volume at high pH [91]. In our study, the combination of carbopol with different DGG concentrations showed the highest increase in viscosity when mixed with SNF at 0.5% carbopol concentration. However, in situ gels containing carbopol are too viscous and their consistency is not uniform. Therefore, they are excluded from further studies as they are thought to cause discomfort in the nasal cavity and cannot ensure dose homogeneity in the application site. Data on the comparison of viscosity values of in situ gels containing combined polymers except carbopol with those containing only DGG are given in Figure 5.
3.1.3. In Situ Gel-Mucin Interaction Study
The current experiment relies on the hypothesis that rheological synergism results via chemical interactions and entanglements between components of the formulation and glycoproteins in mucus [69]. Commercial mucin, the primary component of mucus, was used in this test to assess the in situ gels' mucoadhesion. When mucoadhesive polymers and mucin dispersions are combined, depending on the interactions between the chains of the two macromolecular species, a rheological synergism could be seen that indicates a more than additive growth of the mixture viscosity. In other words, the equation [ηmixture − (ηpolymer + ηmucin)] > 0 denotes the additional viscosity-enhancing effect of the mucin-polymer interaction relative to the value predicted on the basis of simple additivity of the polymer and mucin contributions [92].
As can be shown in Table 2, at the examined shear rate (34 s-1), the viscosity values (cP) of the mixes were greater than the total of the values of mucin and the corresponding in situ gel formulation. This would suggest rheological synergism between the in situ gels and mucin dispersions rather than additive growth. One explanation might be the development of secondary chemical interactions and molecular entanglements between gel solutions and the mucus glycoproteins [69]. The in situ gels containing Na-CMC demonstrated a substantial synergism and it was determined that as the DGG concentration increased, the mucoadhesive strength (Fb) values increased proportionally. This was possibly anticipated because the greatest mucoadhesive qualities are found in the large families of hydrophilic polymers that include the carboxylic group [93].
In the subsequent study, it was investigated whether different concentrations of Na-CMC as a selected mucoadhesive polymer have an effect on the mucoadhesive force of the in situ gel. For this purpose, in situ gels containing different concentrations of Na-CMC (0.1, 0.3, 0.5 and 0.7% w/v) and DGG (0.5% w/v) were prepared and in situ gel-mucin interaction was observed. On the basis of the results, it was observed that all the in situ gels containing Na-CMC showed positive synergism values; this means that the viscosity measured for the mixtures with mucin is higher than the sum of the viscosities of the in situ gel and the mucin solution. The degree of synergism increase was related to concentration of Na-CMC (Table 3). The synergism of formulation increased along with the increase in Na-CMC concentration.
3.1.4. Mechanical Characteristics of In Situ Gels
The development of topical intranasal formulations faces a considerable difficulty in achieving a number of anticipatory properties, such as improved spreadability, good mucoadhesion, and appropriate viscosity, which support comfortable administration and patient compliance [94]. By examining the physical gel structure, TPA enables the evaluation of the mechanical properties of semi-solid formulations. The mechanical properties of in situ gels using mixed polymers (hardness, compressibility, adhesiveness, and cohesiveness) were determined from the force-time curve that resulted from TPA diagrams.
One of the important mechanical parameters is adhesiveness because it provides optimal gel contact and retention at the mucosal surface, resulting in increased medication bioavailability [62]. When compared to neutral polymers, anionic polyelectrolytes have been found to generate stronger adhesions with the mucus layer's glycoprotein chains because the presence of charged functional groups in the polymer chain significantly affects the bioadhesion's strength [95]. Similar results were obtained in this study. The mucoadhesive polymers could be arranged based on their adhesiveness at 0.5% concentration of DGG and mucoadhesive polymer as follows: Na-CMC (0.300 ± 0.05 mJ) > xanthan gum (0.100 ± 0.00 mJ) > HPMC (0.050 ± 0.05 mJ). This may clarify the relatively low mucoadhesive strength of nonionic HPMC compared to anionic Na-CMC and xanthan gum [66]. Furthermore, the hardness and compressibility values were quite similar between different mucoadhesive polymers and observed that the hardness of the in situ gels was directly related to their viscosity since an increase in gel viscosity was accompanied by an increase in hardness. This is consistent with the in situ gel's extent of crosslinking. Greater crosslink quantity per unit volume result in higher gel strength values and, consequently, higher viscosities in the resulting gels [96]. On the other hand, lower values for cohesiveness denote better spreadability [68]. In this study, cohesiveness at 0.5% concentration of DGG and mucoadhesive polymer as follows: HPMC (0.915 ± 0.05) > xanthan gum (0.410 ± 0.06) > Na-CMC (0.140 ± 0.05).
3.1.5. Ex Vivo Mucoadhesive Strength Test
Considering all the data so far, the in situ gel containing 0.5% DGG + Na-CMC polymers is in clear liquid form at room temperature and was considered as having a sprayable viscosity compared to 0.6% DGG + Na-CMC in situ gel. When mixed with SNF at 34°C, 0.5% DGG + Na-CMC in situ gel’s viscosity increased significantly (before gelation: 74.23 cP; after gelation: 269.55 cP) and formed a clear gel. As a result of TPA analysis, it was found to have high adhesiveness value (0.300 mJ) compared to other in situ gels containing HPMC and xanthan gum polymers. Also, the mucoadhesive force (9.39 Pa) was determined to be superior than that of the other in situ gels in the rheological synergism study. Considering all data, it was decided to continue further studies with the formulation containing a 0.5% DGG + CMC combination.
3.1.6. Sprayability
The findings of the spray uniformity tests are displayed in Table 5. While the weight deviations (%) of the mean values of T7 and T14 from the target values (mean values of T7) remained below 2% for all in situ gel formulations. These deviations are found to be in accordance with the Ph.Eur. and the FDA draft guidelines. The Ph.Eur. criteria state that no more than two values may vary from the mean value by more than 25%, and no more than 35%. According to recently proposed guidelines from the FDA, the weight of each spray should not exceed 15% of the target weight, and the mean weight should not exceed 10% of the target weight [75]. Considering usage at 7-day and 14-day intervals, all in situ gels meet these specifications. Although the formulation containing 0.7% Na-CMC was found to comply with the sprayability standards, the spreadability of the in situ gel droplets during spraying was less compared to other in situ gels. Therefore, the formulation prepared with 0.7% Na-CMC was not found suitable for administration as a nasal spray and was eliminated from the study.
3.1.7. Quantitative Determination of 18β-glycyrrhetinic Acid
The quantitative determination of GA was accomplished using the validated HPLC-UV method in accordance with ICH recommendations for the active substance content determination and in vitro release study. Without interference from impurities in the analyzed matrices, GA was eluted at 10.7 minutes. The response of the detector was linear throughout a range of 0.10 – 30 g/mL. The method showed excellent accuracy (recovery% ranged from 101.16 – 103.67%), intraday and interday precision (RSD% values were 0.44% and 0.35%, respectively) (n = 6). The regression equation obtained was y = 0.1237x + 0.0021 and the coefficient of determination was R² = 0.9993. Figure 6 shows a plot of the findings from the linearity study.
3.1.8. Active Substance Content Determination
Each unit in a batch should have a drug substance amount that is tightly confined to the label claim in order to guarantee the uniformity of dosing units. One dose or a portion of a dose of a drug substance is found in each dosage unit, which are also known as dosage forms. The term “uniformity of dosage unit” is defined as the degree of uniformity in the amount of the drug substance among dosage units. Testing for uniformity of dosage units is specified by USP, Section <905>. If the amount of the drug substance is between 85.0% and 115.0% of the label claim, no unit is outside of the range of 75.0% to 125.0% of the label claim, and the RSD of the 10 dosage units is less than or equal to 6.0%, the dosage uniformity standards are met [97]. In our study, the percent active substance content and the RSD of the samples for the optimized in situ gel was found to be satisfactory in the range of 100.46– 101.78% and equal to 0.49%, respectively.
3.1.9. Fourier Transform Infrared Spectrometry (FTIR) Studies
This analysis was carried out to determine whether the active ingredient molecule has undergone any chemical alteration as a result of the excipients. The characteristic absorption bands linked to the stretching vibration of the carbonyl group in carboxyl groups and ketone groups, respectively, showed at 1704 and 1664 cm-1 in the FTIR spectra of GA (Figure 7). The results revealed that the FTIR spectra of GA in the physical mixtures were identically the same as those seen for pure GA, proving that the excipients utilized had no impact on the chemical stability of GA.
3.1.10. In Vitro Release Study
Nasal sprays form a cornerstone therapy for the prevention of virus transmission [98]. However, the physiological mechanism most closely associated with the lowering of the drug residence time in the nasal environment is mucociliary clearance. This self-clearing mechanism is in charge of the rapid removal of the active substance from the nasal cavity, which shortens the time it takes for the active substance to exert its therapeutic effects [99]. In order to prevent rapid drainage of drugs and extend their residence time in the nasal cavity when administered as simple aqueous solutions, a viscosity-increasing approach has been proposed: nasal in situ gelling formulations appear to be a more effective alternative to nasal liquid ones [100]. Such formulations are simple to administer as low-viscosity polymeric solutions, allowing ideal nasal deposition. When these solutions come into touch with the mucosa, they transform into gels. The development of a polymeric network in vivo ensures a continuous release of medicinal substances as well as extending the amount of time that the drug is in contact with the site of action or absorption [55].
To identify the GA release pattern from the optimized in situ gel and to predict the formulation's capacity for controlled release after application to the nasal cavity, in vitro drug release study was performed. As seen in Figure 8 after 168 hours, GA release from the formulation reached 101.57% ± 0.53, indicating the controlled GA release of the optimized in situ gel over time.
3.1.11. Physicochemical Stability
The optimized in situ gel underwent accelerated stability testing for three months at 4, 25, and 40 °C. Every month, samples underwent examinations for their appearance, active substance content, pH, viscosity, and in situ gelation. It was determined that the optimized in situ gel's physical appearance was unaffected by time or temperature since it remained clear liquid at different storage conditions for three months.
The systemic approach to stability evaluation includes information on the stability of the active substance as a key component. The minimum permissible potency level is typically accepted to be 90% of the labeled potency according to Food and Drug Administration (FDA) Drug Stability Guidelines [101]. With respect to drug content, the obtained results (96.44 ± 0.06% for 4 °C, 98.37 ± 0.13 for 25 °C and 94.14 ± 0.15 for 40 °C) at the end of the third month was almost constant compared to initial drug content. A neutral to slightly acidic pH is well tolerated because the nasal mucosa has a pH of approximately 5 - 6.5 [102]. With respect to pH, the in situ gel did not exhibit any notable alterations during the study's duration (initial pH value: 6.47 ± 0.01; pH values after the third month: 6.46 ± 0.01, 6.47 ± 0.01 and 6.45 ± 0.01 at 4, 25 and 40 °C, respectively).
An in situ nasal gel should have the ideal viscosity for simple nasal administration as a liquid that transforms into a gel under physiological conditions in the nose. Additionally, the gel should maintain its form to allow for longer contact between the medication and the absorptive sites in the nasal cavity and to limit formulation drainage to enable continuous release of the active substance [62]. From viscosity and in situ gelation studies, it was demonstrated that all samples were in liquid form at storage conditions and were converted into gel after mixing with SNF at 34 °C, consistent with the initial viscosity values) (data not shown).
3.2. Cell Culture Studies
3.2.1. Cytotoxicity Assay
The cytotoxic effect of GA, the in situ gel containing GA, placebo in situ gel and ribavirin on Hep-2 cells were evaluated by colorimetric cell viability test. In the experiments, the non-toxic dose of the test samples and ribavirin on HEp-2 cells was determined. The obtained MNTCs and CC50 values of the test samples and ribavirin against HEp-2 cells are shown in Table 6.
The CC50 and MNTC values of GA, the in situ gel containing GA, placebo in situ gel and ribavirin were determined as 47.59, 15.29, 14.84, 117.00 µg/ml and 8.33, 4.16, 4.16, 0.98 µg/ml, respectively.
3.2.2. Virus Titration
In the titration of RSV in HEp-2 cell culture by the microtitration method, virus titres was determined as TCID50 = 10-4.5/0.1 ml at the end of the 3rd day.
Figure 9.
a) View of HEp-2 cells; b) CPE view of RSV in HEp-2 cells (Original).

3.2.3. Antiviral Activity Assay
The EC50 and selectivity index (SI) values of the test samples and ribavirin obtained as a result of the antiviral assays are shown in Table 7.
As a result of the antiviral activity tests, it was determined that GA and GA containing in situ gel have significant antiviral activity at higher level than ribavirin (used as positive control). Furthermore, it can be seen that (Table 7) GA and in situ gel formulations are less toxic than ribavirin on HEp-2 cells, and CC50 values of GA, in situ gel formulations and ribavirin are higher than EC50 values.
Chattopadhyay et al. (2009) reported that if the SI value obtained according to the antiviral result is 10 or greater than 10, substances may have potential antiviral activity [103]. Considering this, it has seen that the antiviral activity of the in situ gel developed using 18 β-GA is high in the protection of cells before active infection of hRSV and especially in the prevention of hRSV entry into the cell. The binding glycoprotein (G) and fusion (F) glycoprotein on the surface of the virion control the first stage of hRSV infections [104]. G glycoprotein interacts with host cell receptors and allows adsorption to the cell surface [105]. G glycoprotein targets receptors in ciliated cells of the airways, while F glycoprotein causes the virion membrane to fuse with a target cell membrane [104,105]. Therefore, it is thought that both 18 β-GA and the in situ gel containing 18 β-GA can significantly inhibit the binding and adsorption of hRSV to the host cell.
5. Conclusions
The nasal cavity has a macroscopic surface area of 150–180 cm2 and a volume ranging from 15 to 19 ml, but the existence of microstructures such microvilli on the columnar significantly increases this surface area to over 96,000 cm2 [106,107]. While this ensures a substantial area for filtration, it also offers a wide target for viral infiltration [108]. Although emerging technologies appear to support the preservation of this area [109,110,111], suitable devices are still needed to prevent the spread of airborne viruses and stop further spread. One option for such a device is a spray dosage form administered directly to the nasal cavity to support the innate antiviral function of the nasal mucosa [112]. In this study, the developed situ gelling system has shown to be a potential platform for effective GA nasal delivery. A well-tailored formulation with good sprayability, gelling ability, mucoadhesion, and drug release capabilities was produced by combining the strategies of incorporating an in situ gelling polymer (DGG) and a mucoadhesive polymer (Na-CMC) into an in situ gelling system for optimum nasal delivery.
The widespread persistence of RSV infection (common cold) requires novel medical devices such as nasal sprays to prevent viral infection and transmission [108]. A promising candidate for new antiviral formulations against RSV is GA, a triterpene derived from licorice root. In our study, antiviral activity of GA and the optimized in situ gel containing GA has been shown to be highly effective as a prophylactic and virucidal activity against hRSV. It was considered that both the pure substance and the GA loaded in situ gel primarily inhibited hRSV attachment, induced interferon (IFN) secretion, and reduced internalization of the virus, consistent with the results of literature related to antiviral activity study of pure substance (GA) [53]. Therefore, it is considered that the developed in situ gelling formulation is a promising non-invasive, cost-effective, easy-to-use, and self-administrable drug delivery system that has great potential to be used as an alternative antiviral formulation against RSV infection.
Author Contributions
“Conceptualization, B.Ö. and E.A.; methodology, B.Ö., E.A., Ü.Ü. and H.H.D.; software, B.Ö. and E.A..; validation, B.Ö. and E.A.; formal analysis, B.Ö., E.A., Ü.Ü. and H.H.D.; investigation, B.Ö., E.A., H.H.D., Ü.Ü.; resources, B.Ö., E.A., Y.,O. and R.Ç.K.; data curation, B.Ö., E.A., Y.,O. and R.Ç.K.; writing—original draft preparation, B.Ö. and E.A.; writing—review and editing, B.Ö., E.A., Y.,O. and R.Ç.K..; visualization, B.Ö. and E.A. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Scientific Research Projects Coordination Unit of Istanbul University, Grant number: TSA-2021-37684 and TUBITAK (The Scientific & Technological Research Council of Turkey), Grant number: 222S866.
Data Availability Statement
Not applicable
Acknowledgments
We would like to thank Çağla Kazaz (Pharmaceutical R&D Supervisor, MSc.) and Serdar Ünlü (R&D Director) of the Ali Raif Pharmaceutical Industry Company for their support by enabling the FTIR measurements to be taken in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Liu, Q.; et al. Antivirals for respiratory viral infections: Problems and prospects. In Seminars in Respiratory and Critical Care Medicine; Thieme Medical Publishers: New York, NY, USA, 2016. [Google Scholar]
- Borchardt, R.A.; Rolston, K.V. Respiratory tract infections: Emerging viral pathogens. JAAPA 2012, 25, 19–20. [Google Scholar] [CrossRef]
- Kim, Y.I.; et al. The antiviral effects of RSV fusion inhibitor, MDT-637, on clinical isolates, vs its achievable concentrations in the human respiratory tract and comparison to ribavirin. Influenza Other Respir. Viruses 2017, 11, 525–530. [Google Scholar] [CrossRef]
- Ferkol, T.; Schraufnagel, D. The global burden of respiratory disease. Ann. Am. Thorac. Soc. 2014, 11, 404–406. [Google Scholar] [CrossRef]
- Yeolekar, L.R.; et al. Respiratory viruses in acute respiratory tract infections in Western India. Indian J. Pediatr. 2008, 75, 341–345. [Google Scholar] [CrossRef]
- Corti, M.; Palmero, D.; Eiguchi, K. Respiratory infections in immunocompromised patients. Curr. Opin. Pulm. Med. 2009, 15, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Englund, J.; Feuchtinger, T. Viral infections in immunocompromised patients. Biol. Blood Marrow Transplant. 2011, 17, S2. [Google Scholar] [CrossRef] [PubMed]
- Gainer, S.M.; et al. Increased mortality of solid organ transplant recipients with H1N1 infection: A single center experience. Clin. Transplant. 2012, 26, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Shahani, L.; Ariza-Heredia, E.J.; Chemaly, R.F. Antiviral therapy for respiratory viral infections in immunocompromised patients. Expert Rev. Anti-Infect. Ther. 2017, 15, 401–415. [Google Scholar] [CrossRef]
- Behzadi, M.A.; Leyva-Grado, V.H. Overview of current therapeutics and novel candidates against influenza, respiratory syncytial virus, and Middle East respiratory syndrome coronavirus infections. Front. Microbiol. 2019, 10, 1327. [Google Scholar] [CrossRef]
- Collins, P.L.; Fearns, R.; Graham, B.S. Respiratory syncytial virus: Virology, reverse genetics, and pathogenesis of disease. Challenges and opportunities for respiratory syncytial virus vaccines.
- Shafique, M.; et al. Hurdles in vaccine development against respiratory syncytial virus. In The Burden of Respiratory Syncytial Virus Infection in the Young; IntechOpen: London, UK, 2019. [Google Scholar]
- Wat, D. The common cold: A review of the literature. Eur. J. Intern. Med. 2004, 15, 79–88. [Google Scholar] [CrossRef]
- Hall, C.B.; Long, C.E.; Schnabel, K.C. Respiratory syncytial virus infections in previously healthy working adults. Clin. Infect. Dis. 2001, 33, 792–796. [Google Scholar] [CrossRef]
- Collins, P.L.; Graham, B.S. Viral and host factors in human respiratory syncytial virus pathogenesis. J. Virol. 2008, 82, 2040–2055. [Google Scholar] [CrossRef]
- Morris, J.; Blount, R., Jr.; Savage, R. Recovery of cytopathogenic agent from chimpanzees with goryza. Proc. Soc. Exp. Biol. Med. 1956, 92, 544–549. [Google Scholar] [CrossRef]
- Chanock, R.; Finberg, L. Recovery from Infants with Respiratory Illness of a Virus related to Chimpanzee Coryza Agent (CCA). II. Epidemiologie Aspects of Infection in Infants and Young Children. Am. J. Hyg. 1957, 66, 291–300. [Google Scholar]
- Glezen, W.P.; et al. Risk of primary infection and reinfection with respiratory syncytial virus. Am. J. Dis. Child. 1986, 140, 543–546. [Google Scholar] [CrossRef]
- Murphy, B.R.; et al. Current approaches to the development of vaccines effective against parainfluenza and respiratory syncytial viruses. Virus Res. 1988, 11, 1–15. [Google Scholar] [CrossRef]
- Britto, C.J.; et al. Respiratory viral infections in chronic lung diseases. Clin. Chest Med. 2017, 38, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; et al. Respiratory syncytial virus infection in elderly and high-risk adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Long, S.S., C. G. Prober, and M. Fischer, Principles and practice of pediatric infectious diseases E-Book. 2022, Elsevier Health Sciences.
- Walsh, E.; et al. RSV-associated hospitalization in adults in the USA: A retrospective chart review investigating burden, management strategies, and outcomes. Health Sci. Rep. 2022, 5, e556. [Google Scholar] [CrossRef]
- Peebles, R.S., Jr.; Graham, B.S. Pathogenesis of respiratory syncytial virus infection in the murine model. Proc. Am. Thorac. Soc. 2005, 2, 110–115. [Google Scholar] [CrossRef]
- Kapikian, A.Z.; et al. An epidemiologic study of altered clinical reactivity to respiratory syncytial (RS) virus infection in children previously vaccinated with an inactivated RS virus vaccine. Am. J. Epidemiol. 1969, 89, 405–421. [Google Scholar] [CrossRef]
- Kim, H.W.; et al. Respiratory syncytial virus disease in infants despite prior administration of antigenic inactivated vaccine. Am. J. Epidemiol. 1969, 89, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Alwan, W.; Kozlowska, W. Distinct types of lung disease caused by functional subsets of antiviral T cells. J. Exp. Med. 1994, 179, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.; Drews, S.J.; Marchant, D.J. Respiratory syncytial virus: Infection, detection, and new options for prevention and treatment. Clin. Microbiol. Rev. 2017, 30, 277–319. [Google Scholar] [CrossRef] [PubMed]
- Antonini, T.M.; et al. Sofosbuvir-based regimens in HIV/HCV coinfected patients after liver transplantation: Results from the ANRS CO23 CUPILT study. Transplantation 2018, 102, 119–126. [Google Scholar] [CrossRef]
- Kim, J.-A.; et al. Favipiravir and ribavirin inhibit replication of Asian and African strains of Zika virus in different cell models. Viruses 2018, 10, 72. [Google Scholar] [CrossRef]
- Zhurilo, N.I.; et al. Isosteric ribavirin analogues: Synthesis and antiviral activities. Bioorganic Med. Chem. Lett. 2018, 28, 11–14. [Google Scholar] [CrossRef]
- Bonavia, A.; et al. Identification of broad-spectrum antiviral compounds and assessment of the druggability of their target for efficacy against respiratory syncytial virus (RSV). Proc. Natl. Acad. Sci. 2011, 108, 6739–6744. [Google Scholar] [CrossRef]
- Devincenzo, J.P. Therapy of respiratory syncytial virus infection. Pediatr. Infect. Dis. J. 2000, 19, 786–790. [Google Scholar] [CrossRef]
- Sun, Z.; et al. Respiratory syncytial virus entry inhibitors targeting the F protein. Viruses 2013, 5, 211–225. [Google Scholar] [CrossRef]
- Chemaly, R.; et al. Aerosolized ribavirin: The most expensive drug for pneumonia. Transpl. Infect. Dis. 2016, 18, 634–636. [Google Scholar] [CrossRef] [PubMed]
- Trang, T.P.; et al. Comparative effectiveness of aerosolized versus oral ribavirin for the treatment of respiratory syncytial virus infections: A single-center retrospective cohort study and review of the literature. Transpl. Infect. Dis. 2018, 20, e12844. [Google Scholar] [CrossRef] [PubMed]
- Simoes, E.A.; et al. Past, present and future approaches to the prevention and treatment of respiratory syncytial virus infection in children. Infect. Dis. Ther. 2018, 7, 87–120. [Google Scholar] [CrossRef] [PubMed]
- Domachowske, J.B.; Anderson, E.J.; Goldstein, M. The future of respiratory syncytial virus disease prevention and treatment. Infect. Dis. Ther. 2021, 10, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Geskey, J.M.; Thomas, N.J.; Brummel, G.L. Palivizumab: A review of its use in the protection of high risk infants against respiratory syncytial virus (RSV). Biol. Targets Ther. 2007, 1, 33–43. [Google Scholar]
- Anderson, E.J.; et al. Effectiveness of palivizumab in high-risk infants and children: A propensity score weighted regression analysis. Pediatr. Infect. Dis. J. 2017, 36, 699. [Google Scholar] [CrossRef] [PubMed]
- Blanken, M.O.; et al. Respiratory syncytial virus and recurrent wheeze in healthy preterm infants. N. Engl. J. Med. 2013, 368, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Resch, B. Product review on the monoclonal antibody palivizumab for prevention of respiratory syncytial virus infection. Hum. Vaccines Immunother. 2017, 13, 2138–2149. [Google Scholar] [CrossRef]
- Yamaguchi, H.; et al. Novel effects of glycyrrhetinic acid on the central nervous system tumorigenic progenitor cells: Induction of actin disruption and tumor cell-selective toxicity. Eur. J. Med. Chem. 2010, 45, 2943–2948. [Google Scholar] [CrossRef]
- Kong, S.-Z.; et al. The protective effect of 18β-Glycyrrhetinic acid against UV irradiation induced photoaging in mice. Exp. Gerontol. 2015, 61, 147–155. [Google Scholar] [CrossRef]
- Pugalendi, K. Protective effect of 18β-glycyrrhetinic acid on lipid peroxidation and antioxidant enzymes in experimental diabetes. J. Pharm. Res. 2011, 4, 107–111. [Google Scholar]
- Zhao, C.-H.; et al. Inhibition of human enterovirus 71 replication by pentacyclic triterpenes and their novel synthetic derivatives. Chem. Pharm. Bull. 2014, 62, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.-R.; et al. 18β-Glycyrrhetinic acid derivatives possessing a trihydroxylated A ring are potent gram-positive antibacterial agents. J. Nat. Prod. 2016, 79, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Aly, A.M.; Al-Alousi, L.; Salem, H.A. Licorice: A possible anti-inflammatory and anti-ulcer drug. Aaps Pharmscitech 2005, 6, E74–E82. [Google Scholar] [CrossRef] [PubMed]
- Pugalendi, K.V. Antihyperglycemic effect of 18β-glycyrrhetinic acid, aglycone of glycyrrhizin, on streptozotocin-diabetic rats. Eur. J. Pharmacol. 2009, 606, 269–273. [Google Scholar]
- Jeong, H.G.; et al. Hepatoprotective effects of 18β-glycyrrhetinic acid on carbon tetrachloride-induced liver injury: Inhibition of cytochrome P450 2E1 expression. Pharmacol. Res. 2002, 46, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Pastorino, G.; et al. Liquorice (Glycyrrhiza glabra): A phytochemical and pharmacological review. Phytother. Res. 2018, 32, 2323–2339. [Google Scholar] [CrossRef] [PubMed]
- Hardy, M.E.; et al. 18 β-glycyrrhetinic acid inhibits rotavirus replication in culture. Virol. J. 2012, 9, 1–7. [Google Scholar] [CrossRef]
- Yeh, C.F.; et al. Water extract of licorice had anti-viral activity against human respiratory syncytial virus in human respiratory tract cell lines. J. Ethnopharmacol. 2013, 148, 466–473. [Google Scholar]
- Higgins, T.S.; et al. Intranasal antiviral drug delivery and coronavirus disease 2019 (COVID-19): A state of the art review. Otolaryngol. Head Neck Surg. 2020, 163, 682–694. [Google Scholar] [CrossRef]
- Cao, S.-l.; et al. In situ gel based on gellan gum as new carrier for nasal administration of mometasone furoate. Int. J. Pharm. 2009, 365, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.P.; Laverty, T.; Jones, D.S. Mucoadhesive polymeric platforms for controlled drug delivery. Eur. J. Pharm. Biopharm. 2009, 71, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, M.; et al. The gastric mucus layers: Constituents and regulation of accumulation. Am. J. Physiol. -Gastrointest. Liver Physiol. 2008, 295, G806–G812. [Google Scholar] [CrossRef]
- Salamat-Miller, N.; Chittchang, M.; Johnston, T. The use of mucoadhesive polymers in buccal drug delivery. Adv. Drug Deliv. Rev. 2005, 57, 1666–1691. [Google Scholar] [CrossRef]
- Hagesaether, E.; Hiorth, M.; Sande, S.A. Mucoadhesion and drug permeability of free mixed films of pectin and chitosan: An in vitro and ex vivo study. Eur. J. Pharm. Biopharm. 2009, 71, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, T.; Bonaccorso, A.; Puglisi, G. Epilepsy disease and nose-to-brain delivery of polymeric nanoparticles: An overview. Pharmaceutics 2019, 11, 118. [Google Scholar] [CrossRef]
- Sosnik, A.; Neves, J.D.; Sarmento, B. Mucoadhesive polymers in the design of nano-drug delivery systems for administration by non-parenteral routes: A review. Prog. Polym. Sci. 2014, 39, 2030–2075. [Google Scholar] [CrossRef]
- Altuntaş, E.; Yener, G. Formulation and evaluation of thermoreversible in situ nasal gels containing mometasone furoate for allergic rhinitis. AAPS PharmSciTech 2017, 18, 2673–2682. [Google Scholar] [CrossRef]
- Shinde, J.V.; et al. In situ mucoadhesive nasal gels of metoclopramide hydrochloride: Preformulation and formulation studies. J Pharm Res 2008, 1, 88–96. [Google Scholar]
- Salunke, S.R.; Patil, S.B. Ion activated in situ gel of gellan gum containing salbutamol sulphate for nasal administration. Int. J. Biol. Macromol. 2016, 87, 41–47. [Google Scholar] [CrossRef]
- Jansson, B.; et al. The influence of gellan gum on the transfer of fluorescein dextran across rat nasal epithelium in vivo. Eur. J. Pharm. Biopharm. 2005, 59, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Morsi, N.; et al. Nanoemulsion-based electrolyte triggered in situ gel for ocular delivery of acetazolamide. Eur. J. Pharm. Sci. 2017, 104, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; et al. Formulation and evaluation of in situ gelling systems for intranasal administration of gastrodin. Aaps Pharmscitech 2011, 12, 1102–1109. [Google Scholar] [CrossRef]
- Hao, J.; et al. Fabrication of an ionic-sensitive in situ gel loaded with resveratrol nanosuspensions intended for direct nose-to-brain delivery. Colloids Surf. B Biointerfaces 2016, 147, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Hassan, E.E.; Gallo, J.M. A simple rheological method for the in vitro assessment of mucin-polymer bioadhesive bond strength. Pharm. Res. 1990, 7, 491–495. [Google Scholar] [CrossRef]
- Mayol, L.; et al. A novel poloxamers/hyaluronic acid in situ forming hydrogel for drug delivery: Rheological, mucoadhesive and in vitro release properties. Eur. J. Pharm. Biopharm. 2008, 70, 199–206. [Google Scholar] [CrossRef]
- Callens, C.; et al. Rheological study on mucoadhesivity of some nasal powder formulations. Eur. J. Pharm. Biopharm. 2003, 55, 323–328. [Google Scholar] [CrossRef]
- Gadhave, D.; et al. Nose-to-brain delivery of amisulpride-loaded lipid-based poloxamer-gellan gum nanoemulgel: In vitro and in vivo pharmacological studies. Int. J. Pharm. 2021, 607, 121050. [Google Scholar] [CrossRef]
- Gadhave, D.; et al. Intranasal teriflunomide microemulsion: An improved chemotherapeutic approach in glioblastoma. J. Drug Deliv. Sci. Technol. 2019, 51, 276–289. [Google Scholar] [CrossRef]
- Spray, N.; Solution, I. Suspension, and Spray Drug Products; Chemistry, Manufacturing and Controls Documentation. US Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER).
- Grobuschek, N.; et al. Mass uniformity of nasal sprays. Sci. Pharm. 2003, 71, 151–164. [Google Scholar] [CrossRef]
- Zhou, N.; et al. A simple method for evaluation pharmacokinetics of glycyrrhetinic acid and potential drug-drug interaction between herbal ingredients. Sci. Rep. 2019, 9, 11308. [Google Scholar] [CrossRef] [PubMed]
- Nodilo, L.N.; et al. In situ gelling nanosuspension as an advanced platform for fluticasone propionate nasal delivery. Eur. J. Pharm. Biopharm. 2022, 175, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Francis, T. Diagnostic procedures for virus and rickettsial diseases. 1956, American Public Health Association.
- Andrighetti-Fröhner, C.; et al. Cytotoxicity and potential antiviral evaluation of violacein produced by Chromobacterium violaceum. Memórias Do Inst. Oswaldo Cruz 2003, 98, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.S.; et al. Antiviral activity of daphnoretin isolated from Wikstroemia indica. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2010, 24, 657–661. [Google Scholar] [CrossRef]
- Doğan, H.H.; Duman, R. The Anti Hrsv Activity of Ferula Halophila Peşmen Aqueous and Methanol Extract by Mtt Assay. Trak. Univ. J. Nat. Sci. 2021. [Google Scholar] [CrossRef]
- Abdulla, N.A.; et al. Intranasal delivery of Clozapine using nanoemulsion-based in-situ gels: An approach for bioavailability enhancement. Saudi Pharm. J. 2021, 29, 1466–1485. [Google Scholar] [CrossRef]
- Qian, S.; Wong, Y.C.; Zuo, Z. Development, characterization and application of in situ gel systems for intranasal delivery of tacrine. Int. J. Pharm. 2014, 468, 272–282. [Google Scholar] [CrossRef]
- Galgatte, U.C.; Kumbhar, A.B.; Chaudhari, P.D. Development of in situ gel for nasal delivery: Design, optimization, in vitro and in vivo evaluation. Drug Deliv. 2014, 21, 62–73. [Google Scholar] [CrossRef]
- Zahir-Jouzdani, F.; et al. In situ gelling and mucoadhesive polymers: Why do they need each other? Expert Opin. Drug Deliv. 2018, 15, 1007–1019. [Google Scholar] [CrossRef]
- Jelkmann, M.; et al. A gellan gum derivative as in-situ gelling cationic polymer for nasal drug delivery. Int. J. Biol. Macromol. 2020, 158, 1037–1046. [Google Scholar] [CrossRef]
- Wu, Y.; et al. Research progress of in-situ gelling ophthalmic drug delivery system. Asian J. Pharm. Sci. 2019, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Paulson, A.T.; Rousseau, D. Biopolymers in controlled-release delivery systems. In Modern biopolymer science; Elsevier: Amsterdam, The Netherlands, 2009; pp. 519–557. [Google Scholar]
- Khouryieh, H.; et al. Intrinsic viscosity and viscoelastic properties of xanthan/guar mixtures in dilute solutions: Effect of salt concentration on the polymer interactions. Food Res. Int. 2007, 40, 883–893. [Google Scholar] [CrossRef]
- Lin, H.-R.; Sung, K. Carbopol/pluronic phase change solutions for ophthalmic drug delivery. J. Control. Release 2000, 69, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.; et al. In situ gelling systems: A strategy to improve the bioavailability of ophthalmic pharmaceutical formulations. Drug Discov. Today 2014, 19, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Fini, A.; Bergamante, V.; Ceschel, G.C. Mucoadhesive gels designed for the controlled release of chlorhexidine in the oral cavity. Pharmaceutics 2011, 3, 665–679. [Google Scholar] [CrossRef]
- Madhav, N. Oral mucoadhesive drug delivery systems: A review. JBI 2011, 2229, 7499. [Google Scholar]
- Jones, D.S.; Woolfson, A.D.; Brown, A.F. Textural, viscoelastic and mucoadhesive properties of pharmaceutical gels composed of cellulose polymers. Int. J. Pharm. 1997, 151, 223–233. [Google Scholar] [CrossRef]
- Peppas, N.A.; Buri, P.A. Surface, interfacial and molecular aspects of polymer bioadhesion on soft tissues. J. Control. Release 1985, 2, 257–275. [Google Scholar] [CrossRef]
- Draget, K.; et al. Gel strength of Ca-limited alginate gels made in situ. In in Fourteenth International Seaweed Symposium: In Proceedings of the Fourteenth International Seaweed Symposium, Brest, France, 16–21 August 1992. [Google Scholar]
- Senderak, E.T. Content uniformity acceptance limit for a validation batch—Suppositories, transdermal systems, and inhalations. Drug Dev. Ind. Pharm. 2009, 35, 735–737. [Google Scholar] [CrossRef]
- Sharma, M. Mucoadhesive nanoformulations and their potential for combating COVID-19. Nanomedicine 2021, 16, 2497–2501. [Google Scholar]
- Vigani, B.; et al. Recent advances in the development of in situ gelling drug delivery systems for non-parenteral administration routes. Pharmaceutics 2020, 12, 859. [Google Scholar] [CrossRef] [PubMed]
- Karavasili, C.; Fatouros, D.G. Smart materials: In situ gel-forming systems for nasal delivery. Drug Discov. Today 2016, 21, 157–166. [Google Scholar] [CrossRef]
- Food, U.; Administration, D. Guidance for industry: Drug stability guidelines; USFDA: Theodore Roosevelt, WA, USA, 2008. [Google Scholar]
- Pires, P.C.; et al. Strategies to improve drug strength in nasal preparations for brain delivery of low aqueous solubility drugs. Pharmaceutics 2022, 14, 588. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, D.; et al. Recent advancements for the evaluation of anti-viral activities of natural products. New Biotechnol. 2009, 25, 347–368. [Google Scholar] [CrossRef]
- Faber, T.E. Immunity to respiratory syncytial virus: A clinical perspective; Utrecht University: Utrecht, The Netherlands, 2017. [Google Scholar]
- Proença-Módena, J.L.; et al. Respiratory Viral Infections. Tropical Infectious Diseases: Principles, Pathogens and Practice 2011, 378.
- Dhakar, R.C.; et al. A review on factors affecting the design of nasal drug delivery system. Int. J. Drug Deliv. 2011, 3, 194. [Google Scholar]
- Gizurarson, S. Anatomical and histological factors affecting intranasal drug and vaccine delivery. Curr. Drug Deliv. 2012, 9, 566–582. [Google Scholar] [CrossRef]
- Robinson, T.E.; Moakes, R.J.; Grover, L.M. Low acyl gellan as an excipient to improve the sprayability and mucoadhesion of iota carrageenan in a nasal spray to prevent infection with SARS-CoV-2. Front. Med. Technol. 2021, 3, 687681. [Google Scholar] [CrossRef] [PubMed]
- Takeda, Y.; et al. Acidic electrolyzed water potently inactivates SARS-CoV-2 depending on the amount of free available chlorine contacting with the virus. Biochem. Biophys. Res. Commun. 2020, 530, 1–3. [Google Scholar] [CrossRef]
- de Vries, R.D.; et al. Intranasal fusion inhibitory lipopeptide prevents direct-contact SARS-CoV-2 transmission in ferrets. Science 2021, 371, 1379–1382. [Google Scholar] [CrossRef]
- Mann, B.J.; et al. TaffiX nasal powder forms an effective barrier against SARS-CoV-2. Biomed J Sci Tech Res 2021, 33, 25483–25485. [Google Scholar] [CrossRef]
- Moakes, R.J.; et al. Formulation of a Composite Nasal Spray Enabling Enhanced Surface Coverage and Prophylaxis of SARS-COV-2. Adv. Mater. 2021, 33, 2008304. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Diagrammatic representation of the fabrication process of GA loaded in situ gel using only DGG.
Figure 1.
Diagrammatic representation of the fabrication process of GA loaded in situ gel using only DGG.
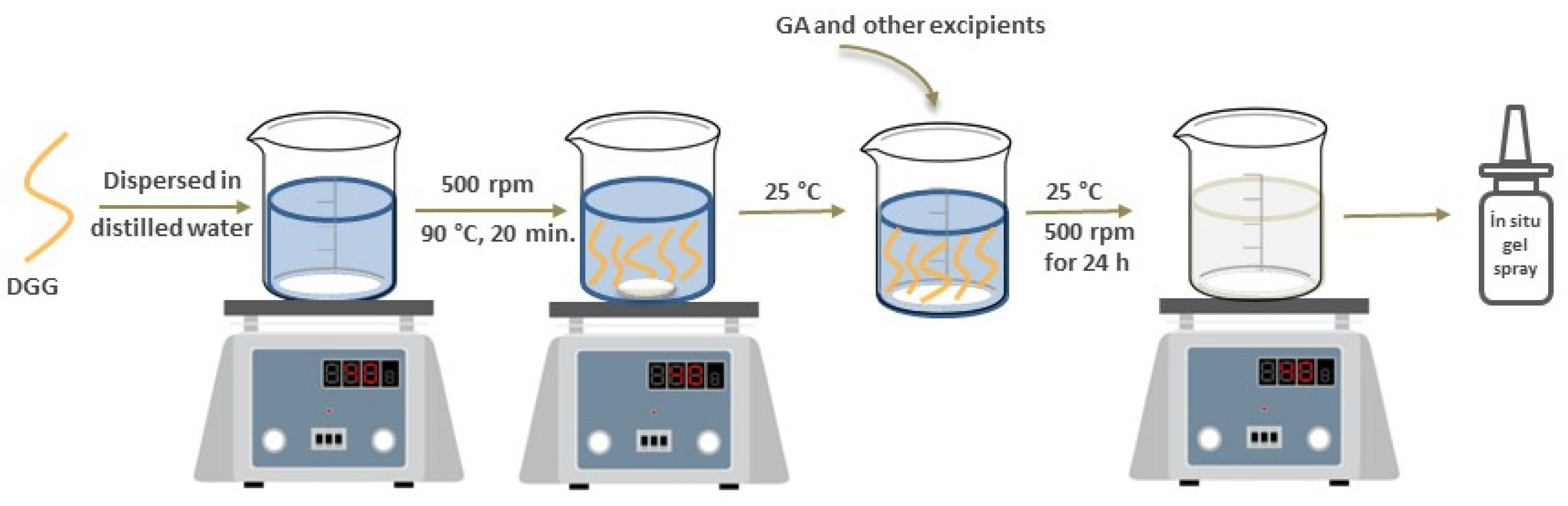
Figure 2.
Diagrammatic representation of the fabrication process of GA loaded in situ gel using combined polymers.
Figure 2.
Diagrammatic representation of the fabrication process of GA loaded in situ gel using combined polymers.
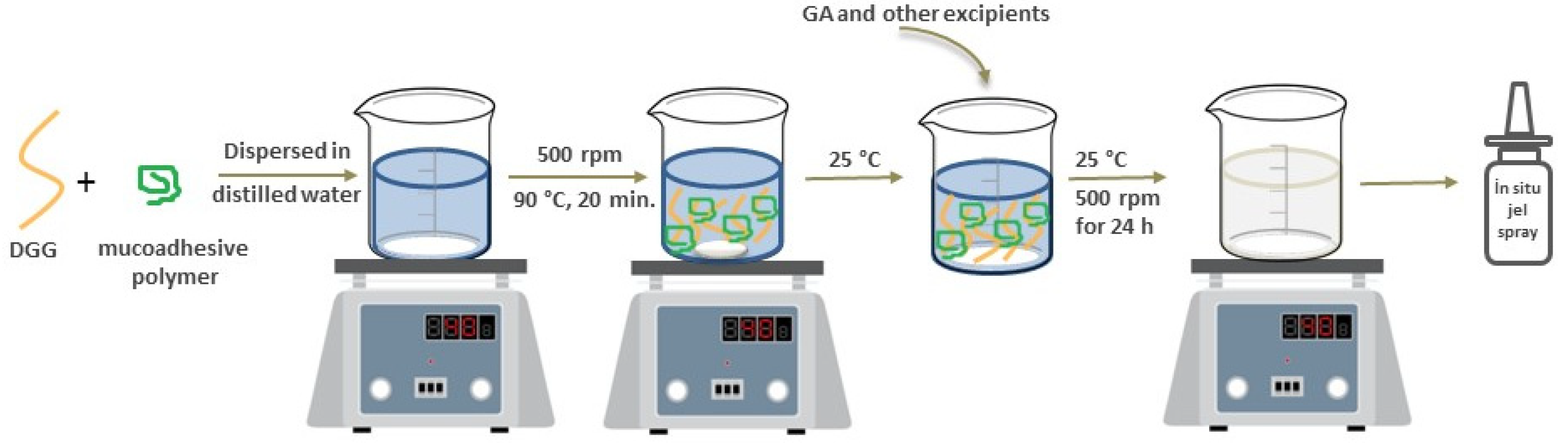
Figure 3.
The viscosity values of in situ gels containing different DGG concentrations at room temperature (values are expressed as mean ± SD) (n = 3).
Figure 3.
The viscosity values of in situ gels containing different DGG concentrations at room temperature (values are expressed as mean ± SD) (n = 3).
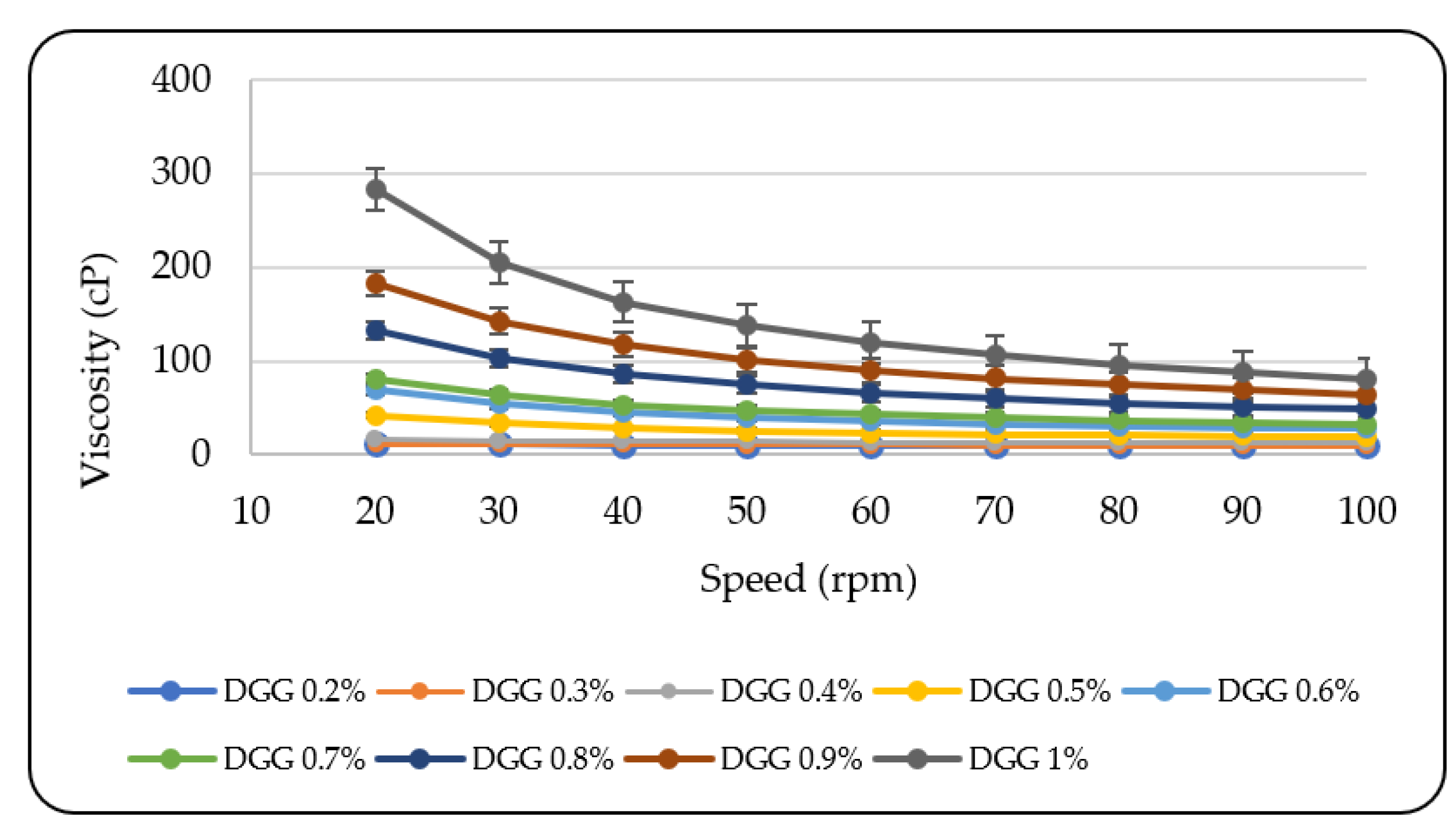
Figure 4.
The viscosity values of in situ gels containing different DGG concentrations at room temperature (values are expressed as mean ± SD) (n = 3).
Figure 4.
The viscosity values of in situ gels containing different DGG concentrations at room temperature (values are expressed as mean ± SD) (n = 3).
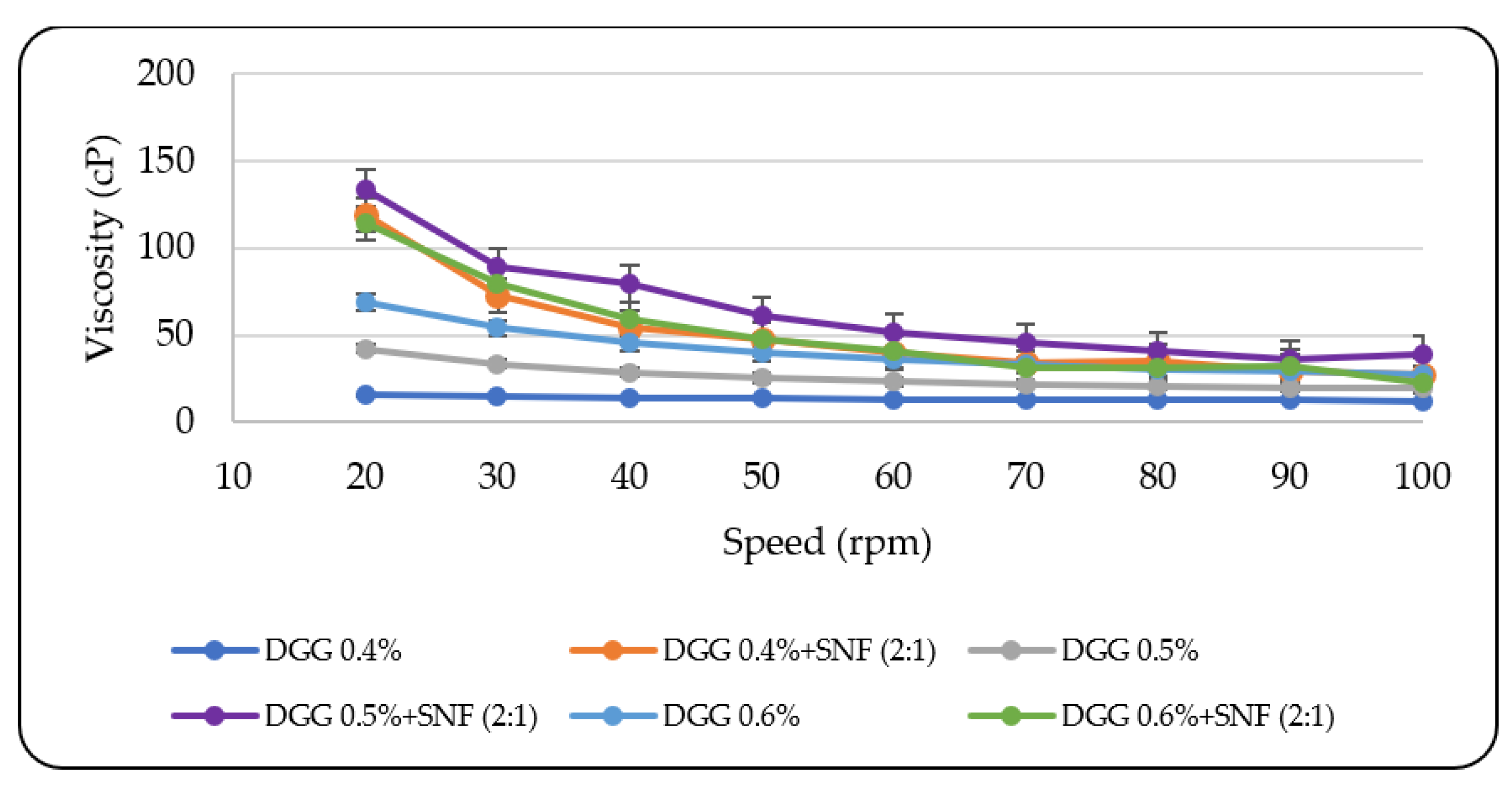
Figure 5.
Comparison of the viscosity values of DGG-only and combined in situ gel mixtures after mixing with SNF (1:2 v/v), (a) 0.4% DGG in situ gels; (b) 0.5% DGG in situ gels; (c) 0.6% DGG in situ gels (n = 3).
Figure 5.
Comparison of the viscosity values of DGG-only and combined in situ gel mixtures after mixing with SNF (1:2 v/v), (a) 0.4% DGG in situ gels; (b) 0.5% DGG in situ gels; (c) 0.6% DGG in situ gels (n = 3).
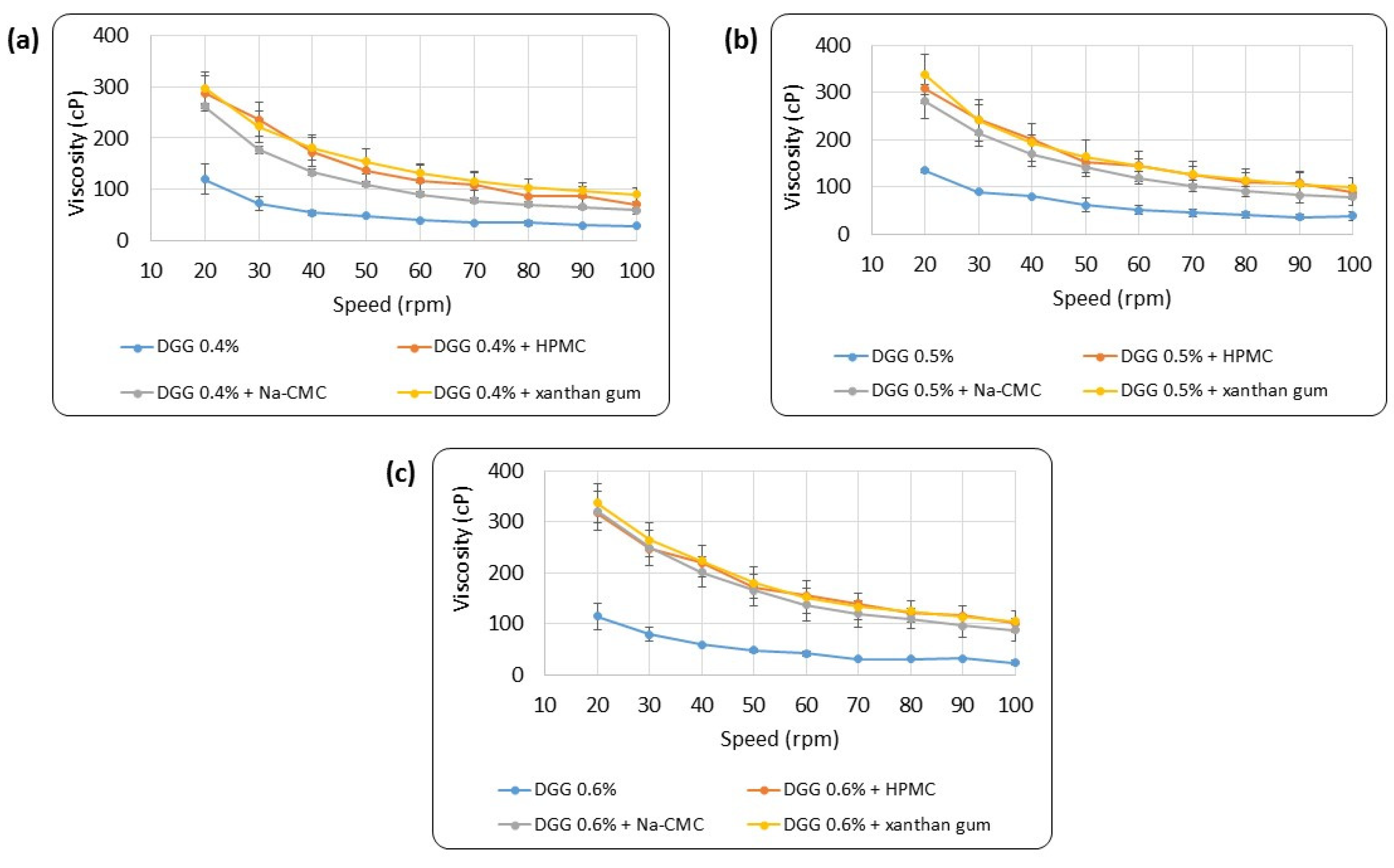
Figure 6.
Calibration curve of GA (means ± SD, n = 6).

Figure 7.
FTIR spectra of pure GA, physical mixtures of DGG and Na-CMC with pure GA.
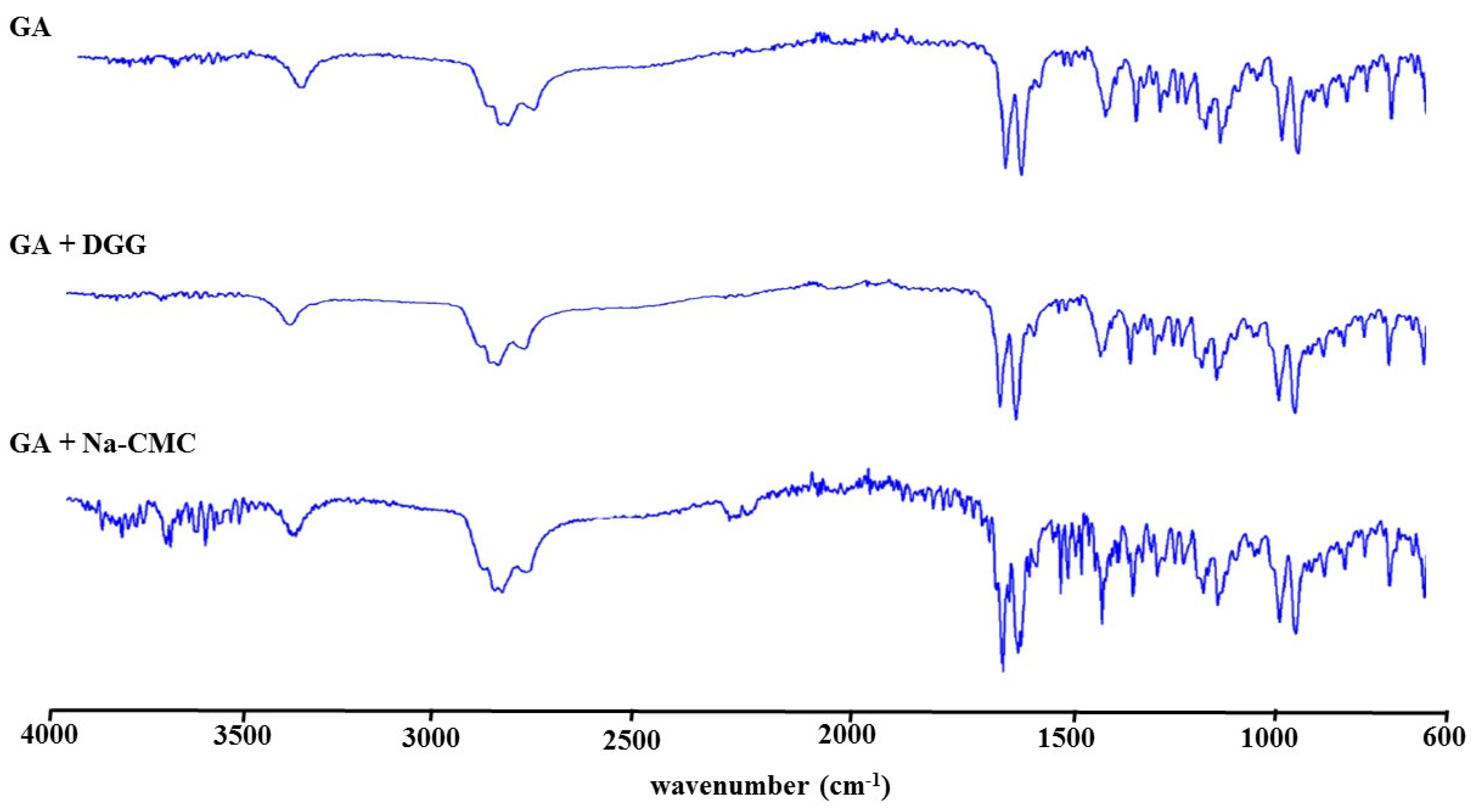
Figure 8.
In vitro GA release study of the optimized in situ gel. Data is reported as mean ± SD, (n = 3).
Figure 8.
In vitro GA release study of the optimized in situ gel. Data is reported as mean ± SD, (n = 3).
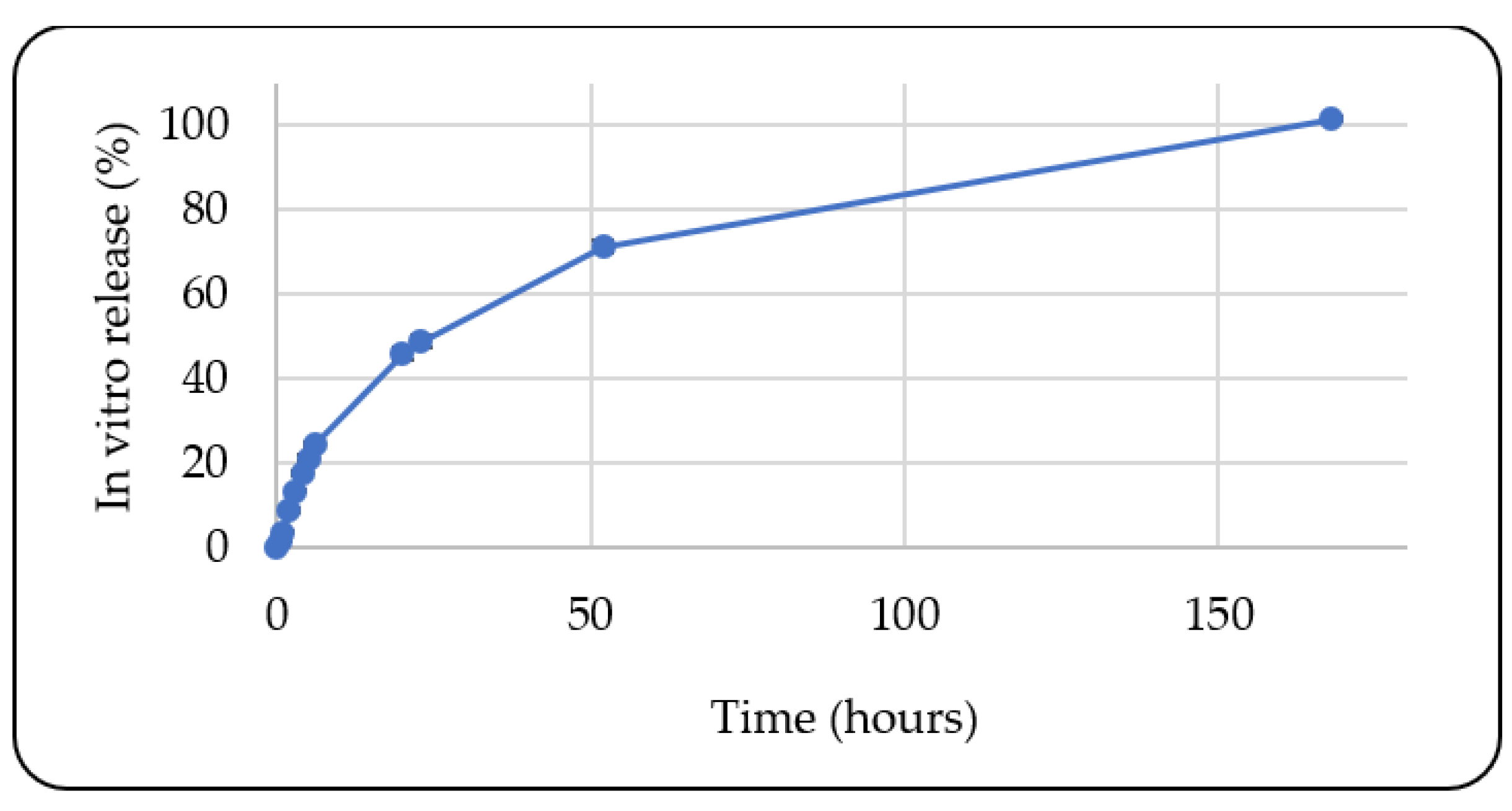

Table 1.
Composition of different in situ gel formulations.
| Ingredients | Composition (%w/w) | ||
|---|---|---|---|
| DGG | 0.40 | 0.50 | 0.60 |
| GA | 0.10 | 0.10 | 0.10 |
| Xanthan gum, HPMC, Na-CMC or Carbopol® 974P NF |
0.50 | 0.50 | 0.50 |
| Dexpanthenol | 0.20 | 0.20 | 0.20 |
| Glycerin | 1.00 | 1.00 | 1.00 |
| Benzalkonium chloride | 0.02 | 0.02 | 0.02 |
| Distilled water | 97.88 | 97.78 | 97.68 |
Table 2.
Viscosity (ηp, ηm, ηt, ηb) and mucoadhesive force (Fb) values of the combined in situ gels calculated at a shear rate value equal to 34 s-1 (n = 3).
Table 2.
Viscosity (ηp, ηm, ηt, ηb) and mucoadhesive force (Fb) values of the combined in situ gels calculated at a shear rate value equal to 34 s-1 (n = 3).
| Formulation | Ƞp | Ƞm | Ƞt | Ƞb | Fb (Pa) |
|---|---|---|---|---|---|
| DGG 0.4% - HPMC | 125.68 | 13.95 | 238.13 | 98.50 | 3.94 |
| DGG 0.5% - HPMC | 168.68 | 13.95 | 294.35 | 111.73 | 4.47 |
| DGG 0.6% - HPMC | 251.36 | 13.95 | 343.96 | 78.65 | 3.15 |
| DGG 0.4% - Na-CMC | 55.59 | 13.95 | 191.82 | 122.28 | 4.89 |
| DGG 0.5% - Na-CMC | 72.48 | 13.95 | 321.08 | 234.65 | 9.39 |
| DGG 0.6% - Na-CMC | 74.01 | 13.95 | 327.43 | 239.46 | 9.58 |
| DGG 0.4% - xanthan gum | 99.22 | 13.95 | 317.51 | 204.34 | 8.17 |
| DGG 0.5% - xanthan gum | 148.83 | 13.95 | 317.04 | 154.26 | 6.17 |
| DGG 0.6% - xanthan gum | 188.52 | 13.95 | 317.51 | 115.04 | 4.60 |
Table 3.
Viscosity (ηp, ηm, ηt, ηb) and mucoadhesive force (Fb) values of the in situ gels containing different concentrations of Na-CMC calculated at a shear rate value equal to 34 s-1 (n = 3).
Table 3.
Viscosity (ηp, ηm, ηt, ηb) and mucoadhesive force (Fb) values of the in situ gels containing different concentrations of Na-CMC calculated at a shear rate value equal to 34 s-1 (n = 3).
| Formulation | Ƞp | Ƞm | Ƞt | Ƞb | Fb(Pa) |
|---|---|---|---|---|---|
| DGG 0.5% - Na-CMC 0.1% | 20.28 | 16.51 | 298.84 | 262.06 | 8.91 |
| DGG 0.5% - Na-CMC 0.3% | 54.28 | 16.51 | 315.03 | 244.23 | 8.30 |
| DGG 0.5% - Na-CMC 0.5% | 74.23 | 16.51 | 371.08 | 280.34 | 9.53 |
| DGG 0.5% - Na-CMC 0.7% | 116.41 | 16.51 | 371.37 | 238.44 | 8.11 |
Table 4.
Mucoadhesive strength values of in situ gels containing different Na-CMC concentrations (n = 3).
Table 4.
Mucoadhesive strength values of in situ gels containing different Na-CMC concentrations (n = 3).
| Formulation | Adhesion strength (g) | |
|---|---|---|
| DGG 0.5% - Na-CMC 0.1% | 14.33 ± 8.40 | |
| DGG 0.5% - Na-CMC 0.3% | 15.67 ± 5.20 | |
| DGG 0.5% - Na-CMC 0.5% | 19.67 ± 5.90 | |
| DGG 0.5% - Na-CMC 0.7% | 27.67 ± 6.80 |
Table 5.
Average variation in weight (weight in mg) and weight deviations (%) with weekly application (n=3).
Table 5.
Average variation in weight (weight in mg) and weight deviations (%) with weekly application (n=3).
| Formulation | T1 | T7 | T14 | ||
|---|---|---|---|---|---|
| Mean ± SD |
Mean ± SD |
Weight deviation (%) |
Mean ± SD | Weight deviation (%) |
|
| DGG 0.5% - Na-CMC 0.1% |
0.323 ± 0.003 | 0.319 ± 0.002 | 1.24 | 0.320 ± 0.003 | 0.93 |
| DGG 0.5% - Na-CMC 0.3% |
0.319 ± 0.002 | 0.326 ± 0.001 | 2.19 | 0.323 ± 0.002 | 1.25 |
| DGG 0.5% - Na-CMC 0.5% |
0.306 ± 0.001 | 0.299 ± 0.002 | 2.29 | 0.302 ± 0.001 | 1.30 |
| DGG 0.5% - Na-CMC 0.7% |
0.299 ± 0.003 | 0.287 ± 0.001 | 4.01 | 0.294 ± 0.001 | 1.67 |
Table 6.
The cytotoxicity results for GA, in situ gels and ribavirin.
| Cytotoxicity | ||
|---|---|---|
| Sample Type | MNTC (µg/mL) |
CC50 (µg/mL) |
| GA | 8.33 | 47.59 |
| GA in situ gel | 4.16 | 15.29 |
| Placebo in situ gel | 4.16 | 14.84 |
| Ribavirin | 0.98 | 117.00 |
Table 7.
The antiviral activity results for GA, in situ gels and ribavirin.
| Sample Type | Simultaneous | Pre-infection | ||
|---|---|---|---|---|
| EC50 (µg/mL) |
SI | EC50 (µg/mL) |
SI | |
| GA | 0.435 | 109.65 | 0.115 | 415.00 |
| GA in situ gel | 0.050 | 306.00 | 0.154 | 100.00 |
| Placebo in situ gel | 0.790 | 18.83 | 2.005 | 7.40 |
| Ribavirin | 4.189 | 28.00 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



