
Submitted:
23 May 2023
Posted:
24 May 2023
You are already at the latest version
Abstract
Background and Aim. Recently made analysis for anti-HBcor prevalence within Kazakhstan blood donors population concluded 17.2% rate. Considering these data are among the highest of infectivity results worldwide, an objective of this study was to define an association of positive Hepatitis B serology markers with risk and behavior factors.
Methods. The blood donors’ samples were tested for anti-HBcore total (IgG/IgM) and anti-HBs, by CLIA on the Architect i2000SR platform (Abbott). Surrogate alanine transferase (ALT) markers for all blood donors were tested by kinetic method on the Biosystems A25 analyzer. A questionnaire was developed for socio-demographic characteristics, donors’ nutrition habits, cholesterol levels and history of smoking, alcohol consumption. Informed consent was obtained from all study participants. Statistics was calculated using the R software program (version 4.1.1, USA, 2021).
Results. A group of 5709 blood donors participated in the study. Participants with positive anti-HBcore scores were on average older (41.8 vs 34.4 years, p<0.001), Kazakh (88.7% vs 83.0%, p<0.001), married (74.0% vs 55.6%, p<0.001), had a secondary education (70.1% vs. 59.4%, p=0.03), smoked (27.9% vs. 24.3%, p=0.05), had a longer smoking history (13.6±9.5 years vs. 9.8±8.5 years, p<0.001), and various hypercholestesterolaemia (6.2% vs 3.9%, p=0.02). Predominantly their main meal was dinner (17.0% vs 14.2%, p=0.03).
Analysis for associations of socio-demographics characteristics, risk factors, nutrition with anti-HBs, showed that those who have secondary education level (70.1%) were more likely to be anti-HBs-positive (p=0.03). No other significant correlations for anti-HBs were observed.
Conclusions. The risk factors and behavior analysis highlighted the blood donors’ overall health status. Positive Hepatitis B markers associated with statistically significant characteristics from socio-demography, nutrition habits or risk factors could support further pathogenesis studies looking for HBV treatment guides fulfilling the existing gaps.
Keywords:
hepatitis B
; anti HBcore
; risk factors
; blood donors
1. Introduction
According to the World Health Organization (WHO) approximately 1.5 million people become infected HBV each year [1], with around 240 million chronic carriers worldwide [2,3]. Kazakhstan is ranked as one of the countries with medium endemicity (2-7%) [4]. In terms of the prevalence of HBV, the peak incidence in 2020 was defined in West Kazakhstan, Kyzylorda region and in the city of Nur-Sultan than the national average prevalence [5].
Anti-HBc is considered being a detectable marker produced in all those who get HBV infection, in chronic carrier state and at the end of an acute resolving infection [6].
The results of Croatian study [7] showed that the anti-HBc prevalence among blood donors is 1.32.%. The study by Meffre C. et al [8] showed that the overall anti-HBc prevalence was 7.3% among metropolitan residents in France. In Germany population the anti-HBc prevalence of whole population was defined as 8.71% [9].
Considering these data are among the highest of infectivity results worldwide, another study of known risk and behavior factors and their association with positive HBV markers was performed in parallel. It was observed that tobacco smokers are most often developing HBV infection and also are involved in the development of hepatocellular carcinoma [10,11]. Alcohol is estimated as the main cause for alcoholic liver disease, including development of chronic viral hepatitis [12]. Also, patients with HBV-associated liver failure are suffering of insufficient nutrition with high risk for the impairment of intestinal function [13]. Although HBV risk factors have been widely studied in Western countries, they are less analyzed and documented in Kazakhstan.
An objective of this study was to define an association of positive Hepatitis B serology markers with risk and behavior factors.
2. Materials and Methods
2.1. Study design
A cross-sectional study aimed at investigating anti-HBc was initiated in 2021 at the Scientific-Production Center of Transfusiology, Ministry of Healthcare, in Kazakhstan. An approval for the study was obtained from Ethics Commission (Decision of EC #5 from 20 August 2020). A specific questionnaire was created for the study purposes to obtain information from blood donors’ socio-demographic characteristics, their nutrition style (eating vegetables and fruits), diet (main meal), risky habits (smoking, alcohol consumption, dyslipidemia, family members, blood transfusion, intravenous or intramuscular procedures, tattooing or skin piercing, surgical interventions).
2.2. Inclusion criteria
The study included blood donors who satisfied the donation criteria, which encompassed individuals aged 18 and above, with no history of blood donation within the past 3 months, weighing more than 50 kg, and testing negative for Hepatitis B, Hepatitis C, HIV, syphilis, gonorrhea, and other relevant laboratory parameters as per the stipulated requirements for blood donation.
2.3. Exclusion criteria
Potential blood donors were not engaged to participate in the study if did not meet inclusion criteria.
2.4. Laboratory analysis
The samples initially were tested for anti-HBcore total (IgG/IgM). If found to be positive of anti-HBcore, further were tested for anti-HBs. All reagents for hepatitis B screening were used for Architect i2000SR, Abbott system.
ALT markers were tested using Biosystems A25 analyzer. The confirmatory tests for infectious markers were evaluated by NAT in pools of six samples by Cobas TaqScreen MPX Test v.2.0
2.5. Statistical analysis
Statistical analysis was conducted by the R software (version 4.1.1, USA, 2021) [14]. Descriptive statistics were reported as proportions (%) for categorical variables and as means±standard deviations for continuous variables. The normality of the distribution was assessed using the Kolmogorov-Smirnov test. Categorical variables were analyzed using Chi-square or Fisher’s exact tests, while continuous independent variables were evaluated using Student’s t-test or Mann-Whitney U test, depending on appropriateness. Adjusted odds ratios were utilized to present the associations between the risk factors and the prevalence of outcomes, specifically anti-HBcore and anti-HBs results, while controlling for certain variables. Statistical significance was considered at p≤0.05.
3. Results
5709 participants were enrolled in this study in the period between June 1 to July 22, 2021. The sample consisted of 68.17% (3139) males and 31.83% (1466) females. The average age of the participants engaged into the study was 35.69±10.57 year.
The most participants were of Kazakh nationality (84%), mainly having secondary education (68%), married (58.8%), non-smokers (75%) and denied alcohol consumption (71,2%).
Regarding nutrition of donors, the main meal was lunch (54.0%), most often the participants prefer to eat 3 or more times a day (90.7%), having fruits and vegetables every day (68.4%) and for the majority (48.0%) meat and meat products were essential parts of the diet.
15.3% of the participants had surgical interventions (including cosmetic surgery or organ removal). A total of 5.2% of the participants reported receiving intravenous or intramuscular treatments such as injections, acupuncture, tattoos, or piercings within the previous 4 months.
Recently made analysis for anti-HBcore prevalence within Kazakhstan blood donors population concluded 17.2% (983) rate [15]. Results of anti-HBcore positive samples presenting antibodies of HBsAg demonstrated that, 90.2% (887 from 983) have anti-HBs positive markers.
Participants with positive anti-HBcore scores were smoked (27.9% vs. 24.3%, p≤0.05), had a longer smoking history (13.6±9.5 years vs. 9.8±8.5 years, p<0.001), had a history of cholesterol problems (6.2% vs 3.9%, p≤0.05), and their main meal was dinner (17.0% vs 14.2%, p≤0.05) than participants found be negative by anti-HBcore results respectively (Table 1).
Results demonstrated that those who have secondary education level (70.1%) were more likely to be anti-HBs-positive (p≤0.05). No difference in anti-HBs prevalence was observed by other risk factors, nutrition (Table 2).
It was also showed that age (p<0.001), ethnicity (p<0.05), marital status (p<0.05) were statistically associated with anti-HBcore positivity (Table 3). Statistical analysis done to compare gender, nationality, education, marital status, family history of hepatitis, blood transfusion history, injections or surgical interventions, with a one-year increase in age (adjOR=1.06, 95%CI:1.05-1.07), showed a 6% growth in odds found to be anti-HBcore positive. Blood donors with Russian ethnicity (adjOR=0.65, 95%CI:0.46-0.93) and representatives of other nationality (adjOR=0.56, 95%CI:0.37-0.85) found to have lower odds with positive anti-HBcore results when compared to Kazakhs. Among singles, the odds ratio of positive anti-HBcore results were lower by 29% (adjOR = 0.71, 95%CI:0.57-0.89) compared to married participants when adjusting for other variables. (Figure 1)
Analysis adjusting for gender, nationality, education, marital status, family history of hepatitis, blood transfusions, injections and surgery, showed that those who represented other nationality groups (adjOR=0.36, 95%CI:0.18-0.72) had lower odds of having anti-HBs comparing to the Kazakhs. Those reporting to have secondary level had lower odds of having anti-HBs result by 50% when compared to who had vocational level (adjOR=0.50, 95%CI:0.28-0.89) (Table 3).
4. Discussion
Evaluating the study results, correlation of HBV positive markers with participants’ age, ethnicity, education level and marital status do not compromise further discussions as all these mentioned categories are overall majorities within Kazakh population and shows the total estimated picture of real situation [16,17].
Antibodies against HBs also develop in a person being successfully vaccinated against hepatitis B virus [7]. These correlations explain our results found within age group of 30-39 years old for the highest prevalence of anti-HBcore while anti-HBcore positive samples for the presence of anti-HBs demonstrated 89% positivity for the marker, which aligns with vaccination starting process in Kazakhstan [4] and most active blood donors age group.
The study conducted by Shaha et al. [18] found no significant association of positive anti-HBs markers with age, gender, socioeconomic status. Meanwhile, it was observed a significant decrease in the development of anti-HBs, either through natural immunity or vaccination, among individuals who reported smoking [18]. This finding contrasts with our earlier results regarding anti-HBcore positivity and its association with this high-risk behavior. Prabina P et al. [19] demonstrated that cigarette smoking was seen in 52% of the HBV-infected patients. Developing of different antibodies against HBV might be reduced or elevated due to the mechanisms of the pathogenesis affected by viral nucleic acid and host intracellular or humoral response, which needs further investigation [20]. Assuming the fact, that nicotine is metabolized by the liver enzymes, subsequent involvement of hepatocytes within various signaling pathways may play direct role to liver affinity of viral infection and indirect further development of malignancies as it relevant to lung cancer biochemistry [21]. Known protective role of anti-HBs in the structure of hepatitis B immunoglobulins (HBIG) was confirmed to be highly effective for perinatal HBV [22] suggest of intrahepatic production of immunoglobulins are working for the chain of immune response cascade [23].
According to the survey results, we found that participants with positive anti-HBcore scores had hypercholestesterolaemia disorders, and their main meal was dinner. We didn’t find other published studies confirmed our results. It is known that HBV induces multiple changes in hepatic lipid metabolism, at the same time increasing both lipid synthesis and lipolysis [23], which may contribute to our findings. Another study indicated that HBV is able to induce the expression of TLR2 gene, developing hepatic lipid accumulation involving genes related to cholesterol absorption and metabolism [24]. Lipid homeostasis manifesting as dyslipidemia and initially observed obesity found affected by lipoprotein receptors damage in the liver which are considering the main players for regulation of hepatic lipolysis [25]. Identification of target genes analyzing whole genome expression profile in the high-fat dietary can bring clearer picture of glucose and lipid metabolism [20], with possible interactions of the same pathways affected by HBV [26].
We found that positive anti-HBcore markers were determined in 23% participants with elevated ALT, and even in 17% of donors with normal levels of ALT [15]. The discussions around the ALT value as surrogate marker for hepatitis diagnostics in early stage are still on debate. The only one clear statement that elevated ALT levels definitely show dysfunction of hepatocytes or their response to any other aggressive interaction which could be either infection or toxically acting substance [27,28].
The main challenge today is global burden of Hepatitis B. Scientists are developing an effective control of HBV replication in early stage [29]. The main outcomes of insufficient treatment of HBV resulting patients’ death with hepatocellular carcinoma, cirrhosis or liver failure are suggesting where the limits or gaps of knowledge are.
One of the key strengths is the inclusion of a large sample size, which provided increased statistical power for accurately estimating prevalence rates and assessing risk factors with greater precision. However, independent risk factors 1 3 were obtained using self-reported information could be biased and missed and HBV vaccination status was not assessed.
5. Conclusions
The comprehensive analysis of risk factors and behaviors in this study shed light on the overall health status of blood donors. The identification of statistically significant associations between positive Hepatitis B markers and various socio-demographic factors, nutritional habits, and other risk factors provides valuable insights. These findings can serve as a foundation for further research into the pathogenesis of Hepatitis B, aiming to address existing gaps in HBV treatment guidelines. Additionally, the identification of high-risk groups for screening expansion and the development of fundamental testing approaches are crucial steps in filling the current knowledge gaps.
Author Contributions
All authors were equally involved. All authors have read and approved the final version of the manuscript. Corresponding author had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
This research was supported by reagents from Abbott Laboratories, Chicago. Company participated in the decision to submit the report for publication.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article its supplementary materials.
Declaration of conflicting interests
The authors declare that there is no conflict of interest in the present study.
Abbreviations
| ALT | Alanine aminotransferase |
| Anti-HBs | Antibody to Hepatitis B surface |
| Anti-HBcore | Antibody to hepatitis B core antigen |
| CHB | Chronic hepatitis B infection |
| HBV | Hepatitis B infection |
| HBsAg | Hepatitis B surface antigen |
| HBV DNA | Hepatitis B infection DNA |
| HCV | Hepatitis C infection |
| HIV | Human immunodeficiency virus |
| WHO | The World Health Organization |
References
- Available online: https://www.hepb.org/what-is-hepatitis-b/what-is-hepb/facts-and-figures/.
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update 2009. Hepatology 2009, 50, 661–662. [Google Scholar] [CrossRef]
- Aliya, K. Epidemiology aspects of the chronic HBV with HDV infection in Kazakhstan. Eurasian Journal of Clinical Sciences 2019, 2, 4–5. [Google Scholar] [CrossRef]
- Jumabayeva, A.; Nersesov, A.; Kulzhanov, M.; Nefedova, M.; Nuraliyeva, G.; Rakhimbekova, G.; Tanabayeva, S.; Fakhradiyev, I. Prevalence of Viral Hepatitis B, C, and D in Kazakhstan. The Scientific World Journal 2022, 2022, 9102565. [Google Scholar] [CrossRef] [PubMed]
- Debra, A.; Kessler, R.N.; Alexandra Jimenez, M.D. In Transfusion Medicine and Hemostasis, 3rd ed.; 2019.
- Miletić, M.; Bingulac-Popović, J.; Stojić Vidović, M.; Hećimović, A.; Berendika, M.; Babić, I.; Đogić, V.; Samardžija, M.; Barišić, K.; Jukić, I.; et al. Anti-HBc prevalence among Croatian blood donors in a 14-year period (2004-2017): Assessment of trends, risks and need for implementing routine testing. Transfus Clin Biol. 2019, 26, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Meffre, C.; Le Strat, Y.; Delarocque-Astagneau, E.; Dubois, F.; Antona, D.; Lemasson, J.M.; Warszawski, J.; Steinmetz, J.; Coste, D.; Meyer, J.F.; et al. Prevalence of hepatitis B and hepatitis C virus infections in France in 2004: Social factors are important predictors after adjusting for known risk factors. J Med Virol. 2010, 82, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Jilg, W.; Hottenträger, B.; Weinberger, K.; Schlottmann, K.; Frick, E.; Holstege, A.; Schölmerich, J.; Palitzsch, K.D. Prevalence of markers of hepatitis B in the adult German population. J Med Virol. 2001, 63, 96–102. [Google Scholar] [CrossRef]
- Liu, X.; Baecker, A.; Wu, M.; Zhou, J.Y.; Yang, J.; Han, R.Q.; Wang, P.H.; Jin, Z.Y.; Liu, A.M.; Gu, X.; et al. Interaction between tobacco smoking and hepatitis B virus infection on the risk of liver cancer in a Chinese population. Int J Cancer 2018, 142, 1560–1567. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, S.M.; Asgharpour, A. Smoking and Liver Disease. Gastroenterol Hepatol (N Y) 2020, 16, 617–625. [Google Scholar] [PubMed]
- Le, T.V.; Vu, T.T.T.; Dang, A.K.; Vu, G.T.; Nguyen, L.H.; Nguyen, B.C.; Tran, T.H.; Tran, B.X.; Latkin, C.A.; Ho, C.S.S.; et al. Understanding Risk Behaviors of Vietnamese Adults with Chronic Hepatitis B in an Urban Setting. Int J Environ Res Public Health 2019, 16, 570. [Google Scholar] [CrossRef]
- Chang, Y.; Liu, Q.Y.; Zhang, Q.; Rong, Y.M.; Lu, C.Z.; Li, H. Role of nutritional status and nutritional support in outcome of hepatitis B virus-associated acute-on-chronic liver failure. World J Gastroenterol. 2020, 26, 4288–4301. [Google Scholar] [CrossRef] [PubMed]
- R.Core, version 4.1.1, USA, 2021.
- Savchuk, T.; Grinvald, Y.; Ali, M.; Sepetiene, R.; Saussakova, S.; Zhangazieva, K.; Imashpayev, D.; Abdrakhmanova, S. Antibodies to Hepatitis B core antigen prevalence study in Kazakhstan. Immun Inflamm Dis. 2023, 11, e793. [Google Scholar] [CrossRef] [PubMed]
- Eschment, B.; De Cordier, B. Introduction: Ethnic, Civic, or Both? The Ethnicities of Kazakhstan in Search of an Identity and Homeland. Central Asian Affairs 2021, 8, 315–318. [Google Scholar] [CrossRef]
- Gulis, G.; Aringazina, A.; Sangilbayeva, Z.; Zhan, K.; de Leeuw, E.; Allegrante, J.P. Population Health Status of the Republic of Kazakhstan: Trends and Implications for Public Health Policy. Int J Environ Res Public Health 2021, 18, 12235. [Google Scholar] [CrossRef]
- Shaha, M.; Hoque, S.A.; Ahmed, M.F.; Rahman, S.R. Effects of Risk Factors on Anti-HBs Development in Hepatitis B Vaccinated and Nonvaccinated Populations. Viral Immunol. 2015, 28, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Prabina, P.; Jayanthi, S.; Krishna Murthy, C.; Kumar, S.B.; Banu, A.S.; Sakunthala, S.R.; Perumal, J. A Study on Hepatitis B Viral Seromarkers and Associated Risk Factors among the Patients Suffering from Acute and Chronic Hepatitis B Infection. International Journal of Applied and Basic Medical Research 2019, 9, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Ciupe, S.M.; Ribeiro, R.M.; Perelson, A.S. Antibody responses during hepatitis B viral infection. PLoS Comput Biol. 2014, 10, e1003730. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.E. Biochemistry of nicotine metabolism and its relevance to lung cancer. J Biol Chem. 2021, 296, 100722. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.H.; Chang, M.H.; Huang, L.M.; et al. Hepatitis B virus infection in children and adolescents in a hyperendemic area: 15 years after mass hepatitis B vaccination. Ann. Intern. Med. 2001, 135, 796–800. [Google Scholar] [CrossRef]
- Elsner, R.A.; Shlomchik, M.J. Germinal center and extrafollicular B cell responses in vaccination, immunity, and autoimmunity. Immunity 2020, 53, 1136–1150. [Google Scholar] [CrossRef]
- Zhang, J.; Ling, N.; Lei, Y.; Peng, M.; Hu, P.; Chen, M. Multifaceted Interaction Between Hepatitis B Virus Infection and Lipid Metabolism in Hepatocytes: A Potential Target of Antiviral Therapy for Chronic Hepatitis B. Front Microbiol. 2021, 12, 636897. [Google Scholar] [CrossRef]
- Li, T.; Yan, H.; Geng, Y.; Shi, H.; Li, H.; Wang, S.; Wang, Y.; Xu, J.; Zhao, G.; Lu, X. Target genes associated with lipid and glucose metabolism in non-alcoholic fatty liver disease. Lipids Health Dis. 2019, 18, 211. [Google Scholar] [CrossRef]
- Akbar, S.; Pinçon, A.; Lanhers, M.C.; Claudepierre, T.; Corbier, C.; Gregory-Pauron, L.; Malaplate-Armand, C.; Visvikis, A.; Oster, T.; Yen, F.T. Expression profile of hepatic genes related to lipid homeostasis in LSR heterozygous mice contributes to their increased response to high-fat diet. Physiol Genomics 2016, 48, 928–935. [Google Scholar] [CrossRef]
- Zeng, Z. Human genes involved in hepatitis B virus infection. World J Gastroenterol. 2014, 20, 7696–7706. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, D.; Sugawa, M.; Kawahara, K. Study on Evaluation of Alanine Aminotransferase (ALT) as Surrogate Marker in Hepatitis Virus Test. J Med Dent Sci. 2016, 63, 45–52. [Google Scholar] [CrossRef]
- Ali, N.; Moiz, B.; Moatter, T. Evaluation of elevated alanine aminotransferase and hepatitis B virus DNA in healthy seronegative blood donors. BMC Res Notes 2012, 5, 272. [Google Scholar] [CrossRef]
- Suk-Fong Lok, A. Hepatitis B Treatment: What We Know Now and What Remains to Be Researched. Hepatol Commun. 2018, 3, 8–19. [Google Scholar] [CrossRef]
Figure 1.
Risk factors statistical evaluation, α = 1 – p.
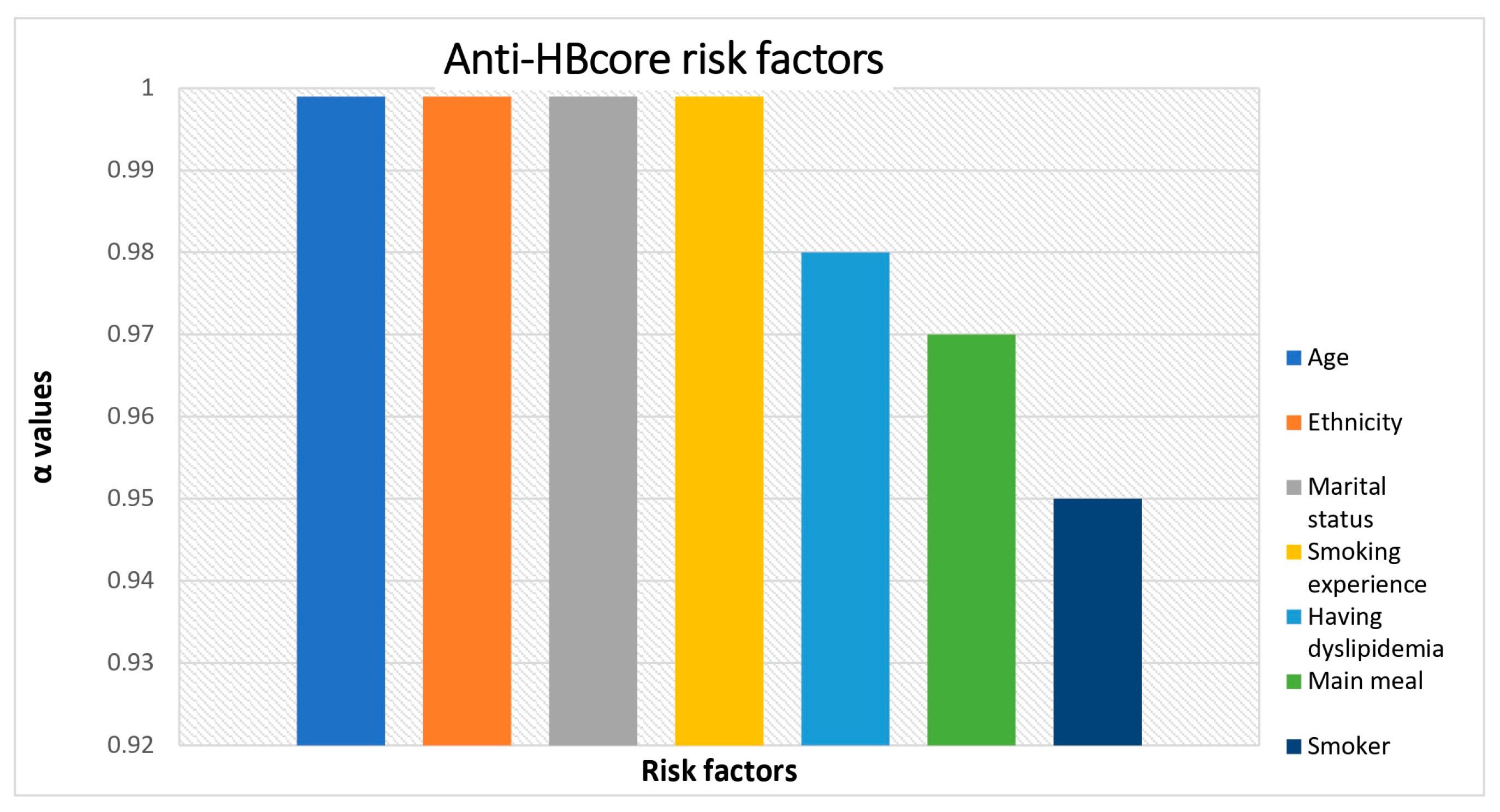

Table 1.
Risk factors and anti-HBcore positive data.
| Variables | Total N=5709 |
anti-HBcore | p-value | |
|---|---|---|---|---|
| Negative | Positive | |||
| n=4726 | n=983 | |||
| Age (mean (SD)) | 35.69 (10.57) | 34.42 (10.33) | 41.75 (9.54) | <0.001 |
| Gender, n (%) | 0.46 | |||
| Females | 1466 (31.8) | 1220 (32.1) | 246 (30.7) | |
| Males | 3139 (68.2) | 2583 (67.9) | 556 (69.3) | |
| Ethnicity, n (%) | <0.001 | |||
| Kazakh | 3855 (84.0) | 3146 (83.0) | 709 (88.7) | |
| Russian | 415 (9.0) | 364 (9.6) | 51 (6.4) | |
| Other ethnicities | 320 (7.0) | 281 (7.4) | 39 (4.9) | |
| Education level, n (%) | 0.48 | |||
| Secondary level | 2753 (68.0) | 2269 (67.8) | 484 (69.1) | |
| Vocational level | 549 (13.6) | 464 (13.9) | 85 (12.1) | |
| University level | 745 (18.4) | 614 (18.3) | 131 (18.7) | |
| Married, n (%) | <0.001 | |||
| Yes | 2354 (58.8) | 1845 (55.6) | 509 (74.0) | |
| Not | 1651 (41.2) | 1472 (44.4) | 179 (26.0) | |
| Smoker, n (%) | 0.05 | |||
| Yes | 1041 (25.0) | 836 (24.3) | 205 (27.9) | |
| Not | 3130 (75.0) | 2600 (75.7) | 530 (72.1) | |
| Smoking experience (mean (SD)) | 10.56 (8.79) | 9.83 (8.47) | 13.62 (9.46) | <0.001 |
| Alcohol consumption in the last 48 hours, n (%) | 0.16 | |||
| Yes | 1160 (18.8) | 972 (19.3) | 188 (16.6) | |
| Not | 2866 (71.2) | 2346 (70.7) | 520 (73.4) | |
| Main meal, n (%) | 0.03 | |||
| All | 515 (12.7) | 417 (12.5) | 98 (13.8) | |
| Breakfast | 754 (18.6) | 645 (19.3) | 109 (15.4) | |
| Lunch | 2187 (54.0) | 1805 (54.0) | 382 (53.8) | |
| Dinner | 595 (14.7) | 474 (14.2) | 121 (17.0) | |
| Meals per day, n (%) | 0.10 | |||
| 1-2 times | 386 (9.3) | 330 (9.6) | 56 (7.6) | |
| 3 or more times | 3770 (90.7) | 3091 (90.4) | 679 (92.4) | |
| Eating vegetables and fruits, n (%) | 0.68 | |||
| Several times a day | 581 (14.5) | 487 (14.7) | 94 (13.6) | |
| Every day | 2737 (68.4) | 2254 (68.1) | 483 (69.7) | |
| Sometimes | 683 (17.1) | 567 (17.1) | 116 (16.7) | |
| The percentage of food with meat and meat products, n (%) | 0.37 | |||
| ≤ 25% | 1113 (27.3) | 935 (27.8) | 178 (25.1) | |
| 26%-50% | 1953 (48.0) | 1606 (47.8) | 347 (48.9) | |
| 51%-75% | 726 (17.8) | 597 (17.8) | 129 (18.2) | |
| > 76% | 279 (6.9) | 223 (6.6) | 56 (7.9) | |
| Having dyslipidemia, n (%) | 0.02 | |||
| Yes | 150 (4.3) | 113 (3.9) | 37 (6.2) | |
| Not | 3359 (95.7) | 2797 (96.1) | 562 (93.8) | |
| Have family members had hepatitis in the last 6 months? n (%) | 0.41 | |||
| Yes | 68 (1.6) | 59 (1.7) | 9 (1.2) | |
| Not | 4096 (98.4) | 3367 (98.3) | 729 (98.8) | |
| Having transfusion of donated blood or its components in the last 12 months, n (%) | 0.57 | |||
| Yes | 56 (1.2) | 44 (1.1) | 12 (1.4) | |
| Not | 4653 (98.8) | 3835 (98.9) | 818 (98.6) | |
| Having intravenous or intramuscular injections, acupuncture, tattoos or piercings in the last 4 months | 0.71 | |||
| Yes | 247 (5.2) | 201 (5.2) | 46 (5.6) | |
| Not | 4458 (94.8) | 3678 (94.8) | 780 (94.4) | |
| Having surgical interventions (including cosmetic surgery or organ removal), n (%) | 0.18 | |||
| Yes | 722 (15.3) | 608 (15.7) | 114 (13.7) | |
| Not | 3989 (84.7) | 3273 (84.3) | 716 (86.3) | |
*Number (percent) of participants missing answer for gender - 1104 (19.3%); missing answer for ethnicity - 1119 (19.6%), missing answer for education level – 1662 (29.1%), missing answer for marital status – 1704 (29.8%), missing answer for smoking–1538 (26,9%), missing answer for alcohol consumption – 1683 (29.5%), missing answer for main meal – 1658 (29%), missing answer for meals per day – 1553 (27.2%), missing answer for eating vegetables and fruits – 1708 (29.9%), missing answer for the percentage of food with meat and meat products – 1638 (28.7%), missing answer for having cholesterol disorder – 2200 (38.5%), missing answer for family history of hepatitis – 1545 (27.1%), missing answer for blood transfusions – 1000 (17,5%), missing answer for Intravenous or intramuscular injections, acupuncture, tattoos or piercings – 1004 (17,6%), missing answer for surgical interventions – 998 (17.5%).
Table 2.
Risk factors and anti-HBs positive data.
| Variables | anti-HBs | p-value | |
|---|---|---|---|
| Negative | Positive | ||
| n=211 (19.22%) | n=887 (80,78%) | ||
| Age (mean (SD)) | 40.02 (10.43) | 41.27 (9.50) | 0.117 |
| Gender, n (%) | 0.795 | ||
| Male | 62 (22.5) | 223 (21.1) | |
| Female | 129 (67.5) | 493 (68.9) | |
| Ethnicity, n (%) | 0.094 | ||
| Kazakh | 161 (84.3) | 629 (88.2) | |
| Russian | 12 (6.3) | 47 (6.6) | |
| Other ethnicities | 18 (9.4) | 37 (5.2) | |
| Education level, n (%) | 0.031 | ||
| Secondary level | 92 (59.4) | 439 (70.1) | |
| Vocational level | 27 (17.4) | 73 (11.7) | |
| University level | 36 (23.2) | 114 (18.2) | |
| Married, n (%) | 0.627 | ||
| Yes | 105 (70.9) | 454 (73.3) | |
| Not | 43 (29.1) | 165 (26.7) | |
| Smoker, n (%) | 0.366 | ||
| Yes | 40 (24.2) | 184 (28.1) | |
| Not | 125 (75.8) | 470 (71.9) | |
| Smoking experience (mean (SD)) | 15.18 (8.86) | 13.15 (9.57) | 0.306 |
| Alcohol consumption in the last 48 hours, n (%) | 1.00 | ||
| Yes | 43 (26.4) | 168 (26.7) | |
| Not | 120 (73.6) | 461 (73.3) | |
| Main meal, n (%) | 0.382 | ||
| All | 22 (13.9) | 87 (13.7) | |
| Breakfast | 31 (19.6) | 100 (15.8) | |
| Lunch | 85 (53.8) | 335 (52.8) | |
| Dinner | 20 (12.7) | 112 (17.7) | |
| Meals per day, n (%) | 0.062 | ||
| 1-2 times | 6 (3.6) | 54 (8.3) | |
| 3 or more times | 159 (96.4) | 600 (91.7) | |
| Eating vegetables and fruits, n (%) | 0.081 | ||
| Several times a day | 26 (17.1) | 81 (13.0) | |
| Every day | 110 (72.4) | 433 (69.7) | |
| Sometimes | 16 (10.5) | 107 (17.2) | |
| The percentage of food with meat and meat products, n (%) | 0.507 | ||
| ≤ 25% | 39 (24.8) | 160 (25.2) | |
| 26%-50% | 80 (51.0) | 311 (48.9) | |
| 51%-75% | 31 (19.7) | 115 (18.1) | |
| > 76% | 7 (4.5) | 50 (7.9) | |
| Having cholesterol disorder, n (%) | 0.838 | ||
| Yes | 7 (5.2) | 33 (6.2) | |
| Not | 127 (94.8) | 503 (93.8) | |
| Have family members had hepatitis in the last 6 month? n (%) | 1.00 | ||
| Yes | 2 (1.2) | 8 (1.2) | |
| Not | 163 (98.8) | 648 (98.8) | |
| Having transfusion of donated blood or its components in the last 12 months, n (%) | 0.126 | ||
| Yes | 5 (3.0) | 8 (1.1) | |
| Not | 162 (97.0) | 736 (98.9) | |
| Having intravenous or intramuscular injections, acupuncture, tattoos or piercings in the last 4 months | 0.856 | ||
| Yes | 8 (4.8) | 41 (5.5) | |
| Not | 158 (95.2) | 699 (94.5) | |
| Having surgical interventions (including cosmetic surgery or organ removal), n (%) | 0.166 | ||
| Yes | 31 (18.6) | 104 (14.0) | |
| Not | 136 (81.4) | 640 (86.0) | |
| ALT level, n (%) | 0.479 | ||
| Normal | 196 (94.2) | 819 (95.7) | |
| Elevated | 12 (5.8) | 37 (4.3) | |
*Number (percent) of participants missing answer for gender – 20 (9.5%); missing answer for ethnicity – 20 (9.5%); missing answer for education level – 56 (26.5%); missing answer for marital status – 63 (29.9%); missing answer for smoking–46 (21.8%); missing answer for alcohol consumption – 48 (22.7%); missing answer for main meal – 53 (25.1%); missing answer for meals per day – 46 (21.8%); missing answer for eating vegetables and fruits – 59 (28%); missing answer for the percentage of food with meat and meat products – 54 (25.6%); missing answer for having cholesterol disorder – 77 (36.5%); missing answer for family history of hepatitis – 46 (21.8%); missing answer for blood transfusions – 44 (20.9%); missing answer for Intravenous or intramuscular injections, acupuncture, tattoos or piercings – 45 (21.3%); missing answer for surgical interventions – 44 (20.9%); missing answer for ALT level – 106 (50.2%).
Table 3.
Risk factors for anti-HBcore and anti-HBs positivity: Multivariable logistic regression analysis.
Table 3.
Risk factors for anti-HBcore and anti-HBs positivity: Multivariable logistic regression analysis.
| Variables | anti-HBcore | anti-HBs | ||
|---|---|---|---|---|
| Adjusted OR (95%CI) |
p-value | Adjusted OR (95%CI) |
p-value | |
| Age | 1.06 (1.05; 1.07) | <0.001 | 1.02 (1.00; 1.04) | 0.09 |
| Gender | 0.32 | 0.64 | ||
| Females | Ref. | Ref. | ||
| Males | 1.11 (0.90; 1.38) | 1.11 (0.71; 1.72) | ||
| Ethnicity | ||||
| Kazakh | Ref. | Ref. | ||
| Russian | 0.65 (0.46; 0.93) | 0.03 | 0.80 (0.39; 1.63) | 1.00 |
| Other ethnicities | 0.56 (0.37; 0.85) | 0.01 | 0.36 (0.18; 0.72) | <0.01 |
| Education level | ||||
| Secondary level | Ref. | Ref. | ||
| Vocational level | 0.77 (0.57; 1.04) | 0.18 | 0.50 (0.28; 0.89) | 0.04 |
| University level | 1.02 (0.79; 1.31) | 1.00 | 0.78 (0.47; 1.30) | 0.70 |
| Married | <0.01 | 0.74 | ||
| Yes | Ref. | Ref. | ||
| No | 0.71 (0.57; 0.89) | 0.92 (0.58; 1.46) | ||
| Have family members had hepatitis in the last 6 months? | 0.61 | 0.74 | ||
| Yes | Ref. | Ref. | ||
| No | 1.23 (0.55; 2.71) | 1.31 (0.26; 6.53) | ||
| Having transfusion of donated blood or its components in the last 12 months | 0.92 | 0.07 | ||
| Yes | Ref. | Ref. | ||
| No | 0.96 (0.44; 2.10) | 3.31 (0.89; 12.3) | ||
| Having intravenous or intramuscular injections, acupuncture, tattoos or piercings in the last 4 months | 0.21 | 0.89 | ||
| Yes | Ref. | Ref. | ||
| No | 0.79 (0.55; 1.15) | 0.89 (0.40; 1.99) | ||
| Having surgical interventions (including cosmetic surgery or organ removal) | 0.07 | 0.19 | ||
| Yes | Ref. | Ref. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



