
Submitted:
23 May 2023
Posted:
25 May 2023
You are already at the latest version
Abstract
Abstract
Introduction
Minimally invasive approaches to oncological liver resection is common in many hepatobiliary centres. This study aims to compare the key oncological and survival outcomes of patients with colorectal liver metastases (CRLM) undergoing laparoscopic or open resections using propensity score matching (PSM).
Methods
A single-centre retrospective study was performed using a prospective database of patients undergoing liver resection for CRLM between January 2016 and December 2019. Different co-variates were selected for matching using PSM. Pre-matching and post-matching analyses were compared. Surgical and survival outcomes were analysed.
Results
In total, 303 patients who met the inclusion criteria were identified: 214 underwent open liver resection (OLR) and 91 laparoscopic liver resection (LLR). LLR had a significantly reduced length of intensive treatment unit (ITU) and overall in-patient stay but longer pringle and operative times. In the unmatched cohort, the median overall and disease-free survival time was significantly longer in patients undergoing laparoscopic compared with open surgery. A PSM model demonstrated significantly reduced blood loss and length of hospital stay, with a significantly greater Pringle and operative time in the LLR group. Differences seen in overall and disease-free survival were lost with propensity score matching, possibly due to lack of bi-lobar disease within the minimally invasive group.
Conclusion
In selected patients with CRLM, LLR presents similar survival and oncological outcomes with the advantages of the short-term results associated with the laparoscopic approach.
Keywords:
liver surgery
; colorectal cancer
; laparoscopy
; survival
1. Introduction
The GLOBOCAN 2020 study (1) estimates
that colorectal cancer is the third most common cancer globally, making up 10%
of total cases in the world, whilst being the second most common cause of
cancer death in both males and females (9.4% of all cancer deaths).
Due to characteristics of
colorectal cancer, the most common non-nodal site of metastatic tumour spread
in these patients is the liver. At time of diagnosis, 15-20% of patients may
present with synchronous colorectal liver metastases (CRLM) and up to 25% of
patients develop metachronous CRLM (2). At the initial time of diagnosis,
approximately 20% of patients with liver metastases are resectable (2). While a
high proportion of patients present with initially unresectable CRLM, advances
in chemotherapy and the advent of targeted therapies have enabled initially
non-resectable disease to become resectable with a subsequently improved
prognosis. However, despite the improvements and advances in the different
therapeutic modalities, liver resection is the only potential curative treatment
providing long-term survival, with 5- and 10-year overall survival (OS) rates
being 33%–58% and 23%–39%, respectively (3-5).
Since the benefit in survival
outcomes of CRLM surgery was established, the operative approach to CRC
metastases has traditionally been open liver resection (OLR). However, since
the introduction of laparoscopic liver resection (LLR) in the early 1990s
(6-7), improvements in surgical devices and minimally invasive techniques have
led to an increasingly common laparoscopy approach in the operative management
of benign and malignant liver lesions, including CRLM (8). During the past
decade a large number of studies have reported on the safety, feasibility, and
oncological efficacy of the LLR in the management of primary and secondary liver
lesions (9-10). Studies have highlighted the benefits of LLRs compared with
conventional OLR, including less intraoperative blood loss, decreased
postoperative pain, lower postoperative morbidity rates, shorter postoperative
length of hospital stay and earlier return to functional activities (11-14).
Although some studies have
reported superior oncological results with the laparoscopic approach (15),
these results have to be interpreted with caution owing to the potential role
of selection bias and its effect on outcomes. Evidence on laparoscopic approach
to CRLM resection is most commonly based on retrospective analyses of
case-matched studies or meta-analyses of non-randomized studies. To date, only
one randomized controlled study (OSLO-COMET) has been conducted showing
benefits for minimal-invasive hepatectomies (MIH) in CRLM resection (16).
The propensity-score matching
(PSM) analysis has gained popularity in recent years as a statistical method to
adjust for known confounding factors and thus reduce the impact of selection
bias in retrospective studies (17,18). For that reason, PSM has been often used
for the comparison of surgical techniques, to create comparable treatment
groups. The aim of this study was to evaluate and compare surgical outcomes of
overall survival and disease-free survival in OLR and LLR, with and without
using a PSM.
2. Methods
Patients undergoing resection of
colorectal liver metastasis between January 2016 and December 2019 at the
Aintree University Hospital NHS Trust (Liverpool) were identified by review of
a prospectively-maintained database. All patients underwent pre-operative
computed tomography (CT) chest/abdomen/pelvis, magnetic resonance imaging (MRI)
liver and
fluorodeoxyglucose -
positron emission tomography
(FDG-PET) scan discussed
at the multidisciplinary team meeting. Patients received 6-monthly CT
chest/abdomen/pelvis for the first two years following surgery and yearly
thereafter for 5 years.
Overall survival is defined as the
time between surgery and death or censoring and liver-specific and disease-free
survival are defined as the time between surgery and hepatic or any recurrence,
as documented on cross-sectional imaging.
Age, body mass index (BMI),
neoadjuvant chemotherapy, synchronicity and side of primary (right colon versus
left or rectum), colonic nodal disease, synchronous lung metastases, major
resection number and size of largest metastasis were considered possible
confounders of the association between operative approach and outcomes. Differences
between baseline confounders were assessed using chi-squared tests for
categorical variables. Normality of continuous variables was assessed using
Shapiro-Wilks tests. Median and inter-quartile range were reported for skewed
continuous confounders and differences were compared using Wilcoxon Rank tests.
The association between type of
surgery and each outcome was first assessed in an unadjusted analysis. Survival
analysis methods were used to assess time-to-event outcomes. Kaplan-Meier
curves were used to visually inspect difference in recurrence free survival,
and Log-rank tests to statistically assess differences. Cox-proportional
hazards models were used to assess the association between surgery type and
risk of recurrence. Logistic regression was used to assess the binary margin
outcome.
Since the association between
surgery type and surgery outcome may have been confounded by a number of
baseline covariates, we first adjusted for these covariates in a regression
model for each outcome. We then used PSM to further investigate potential
confounding and particularly the contribution of selection bias to differences
in outcome between the laparoscopic and open approaches. Propensity scores were
generated using a logistic regression model including surgery type as the
outcome and the full list of possible confounders as explanatory variables. The
propensity scores were used in two ways. Firstly, we performed PSM using a
nearest-neighbour method and a caliper of 0.25. Propensity score matches for
each laparoscopic case were selected without replacement, and each regression
model was estimated on the propensity matched dataset.
3. Results
We identified 303 patients who met
the inclusion criteria, of whom 214 underwent hepatectomy by the open approach
and 91 laparoscopically. Demographic, operative and outcome details of these
patients are demonstrated in Table 1.
Patients who underwent laparoscopic surgery were significantly less likely to
have bi-lobar liver metastasis and when compared with the open approach, had a
significantly smaller number of metastases. Laparoscopic patients had a
significantly longer operation and Pringle time but less blood loss and a
significantly reduced length of ITU and overall in-patient stay. The median
overall and disease-free survival time was significantly longer in patients
undergoing laparoscopic compared with open surgery (Figure 1). Comparing margin status, although
there was no difference in absolute R1 status, laparoscopic surgery provided a
significantly greater distance between tumour and resection edge.
Given the evident selection bias
with regards operative approach, as demonstrated by the significantly reduced
burden of disease demonstrated in patients undergoing laparoscopic surgery, we
performed PSM to balance the cohorts based on pre-operative and biological
variables (see methods for co-variate selection). This resulted in two cohorts,
each containing 82 patients which demonstrated good matching (Table 2).
The PSM model demonstrated a
significantly greater Pringle and operative time in the laparoscopic group in
addition to significantly reduced blood loss and length of hospital stay (Table 2). However, after PSM there was no
significant difference in either overall or disease-free survival between the
laparoscopic or open approaches (Figure 2,
Table 3).
4. Discussion
In recent years the laparoscopic approach for benign and malignant liver tumours has been increasing in frequency and complexity (major hepatectomies or one-stage surgery for CRLM). On the whole, the uptake of minimally invasive approaches in hepatobiliary surgery has been more gradual when compared to other operative subspecialties, primarily due to complexity of procedures and anatomy, difficulties with potential uncontrolled haemorrhage, and psychologically demanding learning curves (19). Currently, CRLM are the most common indication for laparoscopic liver resection in the Western world (20).
The present study reports a single institution’s experience with patients diagnosed of CRLM, treated during a 3-year time period, before and after applying the PSM method. PSM analysis has been introduced aiming to overcome treatment or selection bias in retrospective studies by assembling patient cohorts with minimal differences in clinicopathological features allowing for a meaningful comparison (17, 18). In our study, we observed that those patients who underwent LLR were statistically less likely to have bilobar liver metastasis (46.2% vs 26.4%, p=0.002) and a significantly smaller number of liver metastases (2 vs 1, p=0.002) when compared with the OLR, in a manner similar to other studies (21-23).
Previous series from the literature (10,21-25) have highlighted the benefits of LLR for CRLM in terms of less intraoperative blood loss, lower morbidity rates, shorter postoperative length of hospital stay and superiority in functional recovery compared with OLR. Most of these reports were case series, case–control studies or meta-analyses of non-randomized studies (10, 21-27), and results have therefore been evaluated with caution due to the lack of randomized controlled trials (RCTs). So far, there are only a few RCTs that have been completed evaluating MIH for CRLM, the OSLO-COMET (16) and LapOpHuva (28), while another (ORANGE II Trial) had to be stopped prematurely owing to poor recruitment (29).
Regarding the benefits of LLR for CRLM, our analysis shows similar results to other studies. Operation time, intraoperative blood loss and Pringle time show statistically significant differences between the LLR and OLR groups, in agreement with Cipriani et. al (21) and Ratti et. al (24). Concerns regarding intraoperative haemorrhage could explain why the Pringle time is longer in the LLR group and this, combined with increased pneumoperitoneum pressures during LLR could lead to reduced operative blood loss.
In most surgical subspecialties, laparoscopy has been associated with decreased postoperative morbidity and mortality (30). Although there are no significant differences in our study in terms of complications and mortality, the postoperative ITU and hospital stay was significantly shorter after laparoscopic surgery, similar to other studies (11-14).
During the initial uptake of laparoscopic approaches in hepatobiliary surgery, early concerns were raised around ability to achieve robust oncological outcomes. However, well-designed randomized controlled trials (16,28) and meta-analyses (27) have shown its noninferiority to open surgery. In the present series, LLR appeared to be effective in terms of oncologic outcomes. Laparoscopic surgery provided a significantly greater distance between tumour and resection edge in comparison with open surgery (5mm vs 2mm, respectively). However, comparing margin status there was no significant difference in R1 status with or without PSM. The median overall survival (OS) and disease-free survival (DFS) show no significant differences between LLR and OLR groups with PSM.
Once different studies have determined the validity of the LLR for CRLM in terms of oncological outcomes, it cannot be ignored that some studies have even reported better oncological results in patients operated by laparoscopic approach (15,26,27,31).
One of the key points related to those differences in morbidity and mortality that had been demonstrated by Fretland et al (32) in the context of a substudy within the OsloCoMet study (16), which shows that LLR of CRLMs reduced the inflammatory response compared with open resection. Our study shows similar results and although statistical significance is lost after PSM, there are obvious differences in both survival curves. In this context, a possible explanation for the possible better oncological results of LLR could be a reduced inflammatory response (32), lower morbidity and better early functional recovery compared to the OLR; allowing a shorter interval to postoperative chemotherapy as it is reported in a recent study from Tohme et al (33).
While that fact that this study is based only in a single centre could be considered a limitation, this characteristic also provides advantages such as a high degree of standardization of diagnostics, patient selection, surgical technique and postoperative care, all based in a high-volume hepatobiliary centre with extensive open and laparoscopic experience. Additionally, it must be borne in mind that study sample size decreased after PSM, which could have affected the accuracy of overall and survival-estimated data. Another limitation is that this study is not an RCT. However, use of a well-designed PSM analysis allows critical consideration of this available data, bearing in mind the caveat of possible confounding factors potentially affecting results.
5. Conclusions
LLR is a beneficial alternative to OLR in selected patients with CRLM, providing favourable short-term outcomes such as reduced blood loss, shorter length of ITU and hospital stay. LLR does not compromise oncological outcomes including surgical margin, overall-survival and disease-free survival. Our results support that LLR should be preferred for patients presenting with resectable CRLM.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin [Internet]. 2021, 71, 209–49. [CrossRef]
- Leporrier J, Maurel J, Chiche L, Bara S, Segol P, Launoy G. A population-based study of the incidence, management and prognosis of hepatic metastases from colorectal cancer. Br J Surg 2006, 93, 465–474. [CrossRef]
- Choti MA, Sitzmann JV, Tiburi MF, Sumetchotimetha W, Rangsin R, Schulick RD, et al. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann Surg. 2002, 235, 759–66. [CrossRef]
- Mann CD, Metcalfe MS, Leopardi LN, Maddern GJ. The clinical risk score: emerging as a reliable preoperative prognostic index in hepatectomy for colorectal metastases. Arch Surg. 2004, 139, 1168–72. [CrossRef]
- Cummings LC, Payes JD, Cooper GS. Survival after hepatic resection in metastatic colorectal cancer: a population-based study. Cancer 2007, 109, 718–26. [CrossRef]
- Reich, H.; McGlynn, F.; DeCaprio, J.; Budin, R. Laparoscopic excision of benign liver lesions. Obstet. Gynecol. 1991, 78 Pt 2, 956–958. 1: PMID, 1833. [Google Scholar]
- Katkhouda, N.; Fabiani, P.; Benizri, E.; Mouiel, J. Laser resection of a liver hydatid cyst under videolaparoscopy. Br. J. Surg. 1992, 79, 560–561. [Google Scholar] [CrossRef] [PubMed]
- Koffron, A. , Geller, D. , Gamblin, T. C. & Abecassis, M. Laparoscopic liver surgery: Shifting the management of liver tumors. Hepatology 2006, 44, 1694–1700. [Google Scholar] [CrossRef]
- Jackson NR, Hauch A, Hu T, Buell JF, Slakey DP, Kandil E. The safety and efficacy of approaches to liver resection: a meta-analysis. JSLS 2015, 19, e2014⋅00186. [CrossRef]
- Schiffman SC, Kim KH, Tsung A, Marsh JW, Geller DA. Laparoscopic versus open liver resection for metastatic colorectal cancer: a metaanalysis of 610 patients. Surgery 2015, 157, 211–222. [CrossRef]
- Koffron AJ, AuffenbergG,Kung R,Abecassis M. Evaluation of 300 minimally invasive liver resections at a single institution: less is more. Ann Surg. 2007, 246, 385–92. [CrossRef]
- Simillis C, Constantinides VA, Tekkis PP, Darzi A, Lovegrove R, Jiao L, et al. Laparoscopic versus open hepatic resections for benign and malignant neoplasm meta-analysis. Surgery. 2007, 141, 203–11. [CrossRef]
- Nguyen KT, Marsh JW, Tsung A, Steel JJ, Gamblin TC, Geller DA. Comparative benefits of laparoscopic vs open hepatic resection: a critical appraisal. Arch Surg. 2011, 146, 348–56. [CrossRef]
- Rao A, Rao G, Ahmed I. Laparoscopic or open liver resection? Let systematic review decide it. Am J Surg. 2012, 204, 222–31. [CrossRef]
- Castaing D, Vibert E, Ricca L, Azoulay D, Adam R, Gayet B. Oncologic results of laparoscopic versus open hepatectomy for colorectal liver metastases in two specialized centers. Ann Surg 2009, 250, 849–855. [CrossRef]
- Fretland, A.A.; Dagenborg, V.J.; Bjornelv, G.M.W.; Kazaryan, A.M.; Kristiansen, R.; Fagerland, M.W.; Hausken, J.; Tonnessen, T.I.; Abildgaard, A.; Barkhatov, L.; et al. Laparoscopic versus open resection for colorectal liver metastases: The OSLO-COMET randomized controlled trial. Ann. Surg. 2018, 267, 199–207. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the eects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Adamina, M.; Guller, U.; Weber, W.P.; Oertli, D. Propensity scores and the surgeon. Br. J. Surg. 2006, 93; 389–394. [CrossRef]
- Tzanis D, Shivathirthan N, Laurent A, Abu Hilal M, Soubrane O, Kazaryan AM, et al. European experience of laparoscopic major hepatectomy. J Hepatobiliary Pancreat Sci 2013, 20, 120–124. [CrossRef]
- Ciria R, Cherqui D, Geller DA, et al. Comparative short-term benefits of laparoscopic liver resection: 9000 cases and climbing. Ann Surg. 2016, 263, 761–77. [CrossRef]
- Cipriani F, Rawashdeh M, Stanton L, et al. Propensity score–based analysis of outcomes of laparoscopic versus open liver resection for colorectal metastases. Br J Surg. 2016, 103, 1504–1512. [CrossRef]
- Montalti R, Berardi G, Laurent S, Sebastiani F, Ferdinande L, Libbrecht LJ et al. Laparoscopic liver resection compared to open approach in patients with colorectal liver metastases improves further resectability: oncological outcomes of a case–control matched-pairs analysis. Eur J Surg Oncol 2014, 40, 536–544. [CrossRef]
- Untereiner X, Cagniet A, Memeo R, Tzedakis S, Piardi T, Severac F, et al. Laparoscopic hepatectomy versus open hepatectomy for colorectal cancer liver metastases: comparative study with propensity score matching. Hepatobiliary Surg Nutr [Internet]. 2016, 5, 290–9. [CrossRef]
- Ratti F, Fiorentini G, Cipriani F, Catena M, Paganelli M, Aldrighetti L. Laparoscopic vs open surgery for colorectal liver metastases. JAMA Surg [Internet]. 2018, 153, 1028–35. [CrossRef]
- Beppu T, Wakabayashi G, Hasegawa K, Gotohda N, Mizuguchi T, Takahashi Y, et al. Long-term and perioperative outcomes of laparoscopic versus open liver resection for colorectal liver metastases with propensity score matching: a multi-institutional Japanese study. J Hepatobiliary Pancreat Sci [Internet]. 2015, 22, 711–20. [CrossRef]
- Kazaryan AM, Marangos IP, Røsok BI, Rosseland AR, Villanger O, Fosse E et al. Laparoscopic resection of colorectal liver metastases: surgical and long-term oncologic outcome. Ann Surg 2010, 252, 1005–1012. [CrossRef]
- Zhang X-L, Liu R-F, Zhang D, Zhang Y-S, Wang T. Laparoscopic versus open liver resection for colorectal liver metastases: A systematic review and meta-analysis of studies with propensity score-based analysis. Int J Surg [Internet]. 2017, 44, 191–203.
- Robles-Campos R, Lopez-Lopez V, Brusadin R, Lopez-Conesa A, Gil-Vazquez PJ, Navarro-Barrios Á, et al. Open versus minimally invasive liver surgery for colorectal liver metastases (LapOpHuva): a prospective randomized controlled trial. Surg Endosc [Internet]. 2019, 33, 3926–36. [CrossRef]
- Wong-Lun-Hing EM, van Dam RM, van Breukelen GJP, Tanis PJ, Ratti F, van Hillegersberg R, et al. Randomized clinical trial of open versus laparoscopic left lateral hepatic sectionectomy within an enhanced recovery after surgery programme (ORANGE II study). Br J Surg [Internet]. 2017, 104, 525–35. [CrossRef]
- Berardi G, Van Cleven S, Fretland ÅA, et al. Evolution of laparoscopic liver surgery from innovation to implementation to mastery: perioperative and oncologic outcomes of 2,238 patients from 4 European specialized centers. J Am Coll Surg. 2017, 225, 639–649. [Google Scholar] [CrossRef]
- Parks KR, Kuo YH, Davis JM, O’ Brien B, Hagopian EJ. Laparoscopic versus open liver resection: a meta-analysis of long-term outcome. HPB (Oxford). 2014, 16, 109–18. [CrossRef]
- Fretland AA, Sokolov A, Postriganova N, Kazaryan AM, Pischke SE, Nilsson PH, et al. Inflammatory response after laparoscopic versus open resection of colorectal liver metastases: Data from the Oslo-CoMet trial. Medicine (Baltimore) [Internet]. 2015, 94, e1786. [CrossRef]
- Tohme S, Goswami J, Han K, et al. Minimally invasive resection of colorectal cancer liver metastases leads to an earlier initiation of chemotherapy compared to open surgery. J Gastrointest Surg. 2015, 19, 2199–2206. [CrossRef]
Figure 1.
Overall (A) and Disease-free (B) survival curves in the unmatched cohorts demonstrating laparoscopic (red) and open (blue) approaches. Pink and blue shaded areas represent 95% confidence intervals respectively.
Figure 1.
Overall (A) and Disease-free (B) survival curves in the unmatched cohorts demonstrating laparoscopic (red) and open (blue) approaches. Pink and blue shaded areas represent 95% confidence intervals respectively.
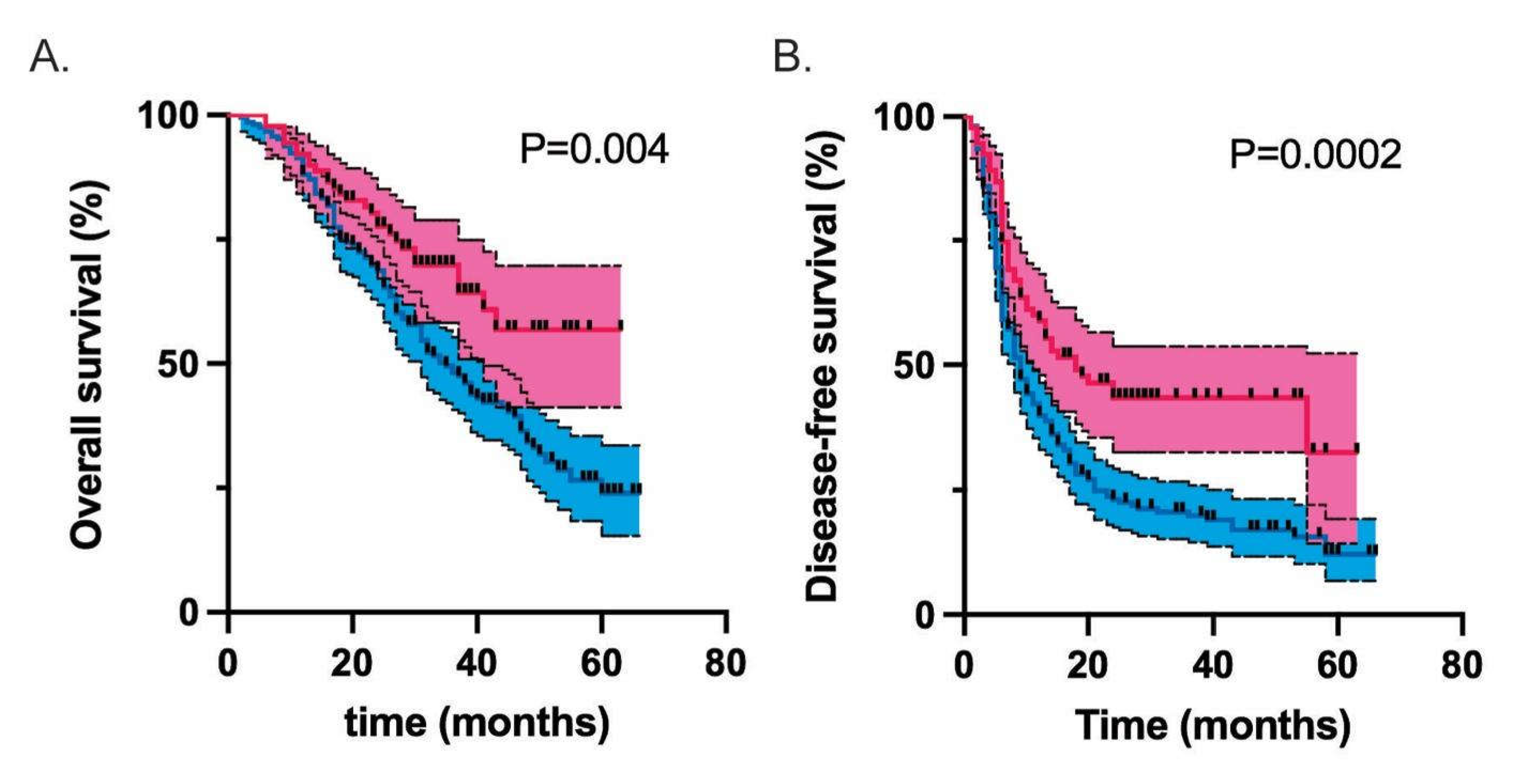
Figure 2.
Overall (A) and Disease-free (B) survival curves in the PSM cohorts demonstrating laparoscopic (red) and open (blue) approaches. Pink and blue shaded areas represent 95% confidence intervals respectively.
Figure 2.
Overall (A) and Disease-free (B) survival curves in the PSM cohorts demonstrating laparoscopic (red) and open (blue) approaches. Pink and blue shaded areas represent 95% confidence intervals respectively.
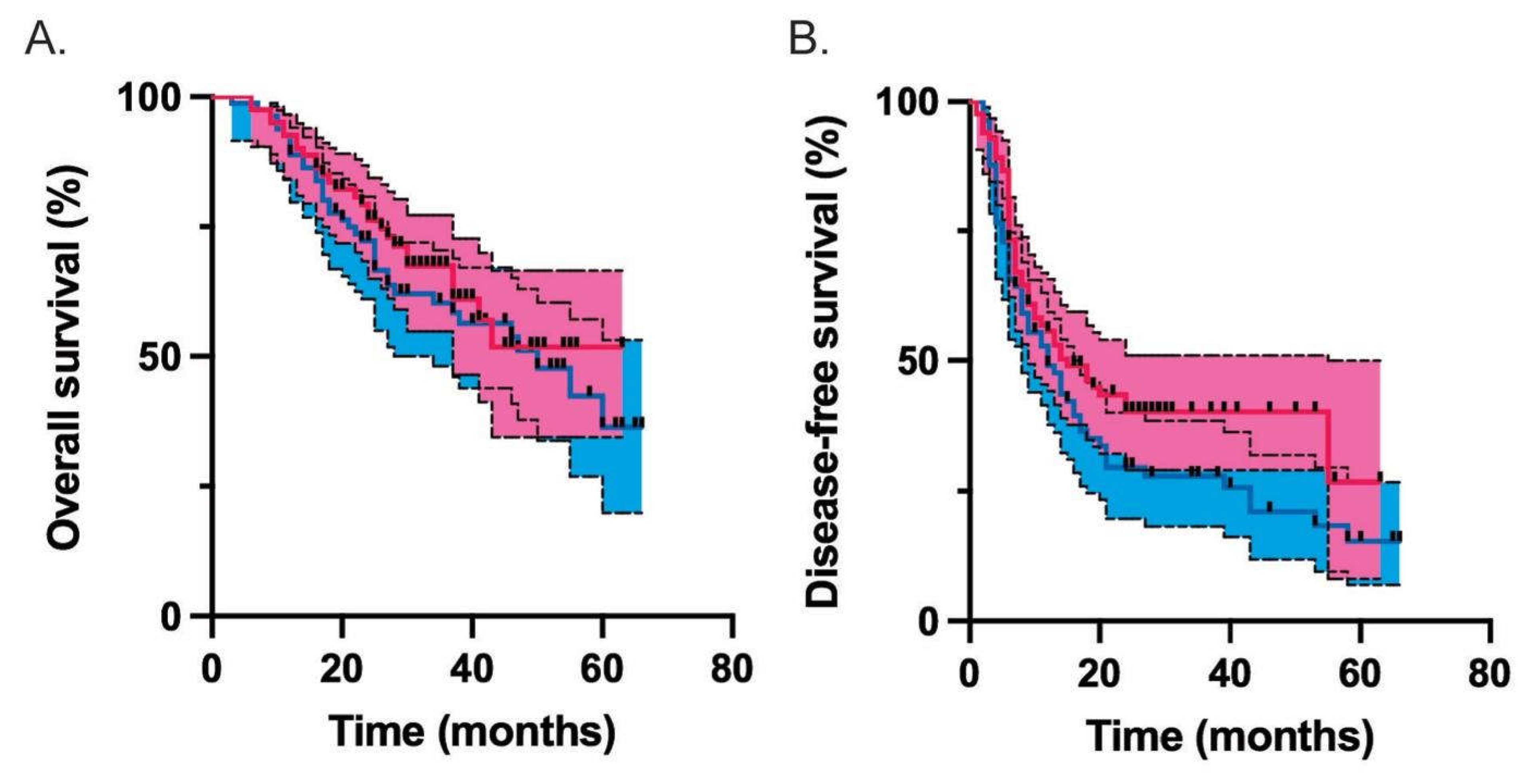

Table 1.
Demographics of laparoscopic and open hepatectomy patients. *median (IQR), $mean (±SD), major hepatectomy defined as >3 liver segments, + includes any hepatic or extrahepatic metastasis.
Table 1.
Demographics of laparoscopic and open hepatectomy patients. *median (IQR), $mean (±SD), major hepatectomy defined as >3 liver segments, + includes any hepatic or extrahepatic metastasis.
| Open | Laparoscopic | P | |
|---|---|---|---|
| N (%) | 212 | 91 | |
| Demographics | |||
| Age (years)* | 66 (57-72) | 69 (61.5-74) | 0.054 |
| Sex (male) | 134 (63.2) | 54 (59.3) | 0.891 |
| BMI (kg/m2)* | 27.1 (24.1-30.4) | 26.1 (23.4-29.4) | 0.054 |
| American Society of Anesthesiologists (ASA) scale 1 2 3 4 |
15 (7.1) 146 (68.9) 50 (23.6) 1 (0.5) |
9 (9.9) 69 (75.8) 13 (14.3) 0 (0.0) |
0.246 |
| Anaerobic threshold$ (ml/min/kg) | 11.5 (±3.3) | 12.0 (±2.7) | 0.283 |
| Hemoglobin (Hb)$ (g/L) | 134 (±15.3) | 134 (±15.4) | 0.848 |
| White Cell Count (WCC)$ (109/L) | 7.39 (±5.05) | 6.95 (±1.73) | 0.415 |
| Tumour biology | |||
| Carcinoembryonic antigen (CEA)* (ng/mL) | 5.4 (2.4-18.7) | 5.3 (2.4-14.4) | 0.094 |
| Neoadjuvant chemotherapy | 134 (63.2) | 46 (50.5) | 0.054 |
| Synchronous primary | 121 (57.1) | 49 (53.8) | 0.694 |
| Right-sided primary | 157 (74.1) | 69 (75.8) | 0.857 |
| Node positive primary | 133 (62.7) | 53 (58.2) | 0.543 |
| Synchronous lung metastasis | 36 (17.0) | 10 (11.0) | 0.247 |
| Bilobar liver metastasis | 98 (46.2) | 24 (26.4) | 0.002 |
| Number of metastases* | 2 (1-4) | 1 (1-3) | 0.002 |
| Largest metastasis (mm)* | 30 (20-50) | 30 (20-40) | 0.579 |
| Major hepatectomy | 91 (42.9) | 30 (33.0) | 0.135 |
| Outcomes | |||
| Pringle time (min) * | 25 (7-43) | 37 (9-55) | 0.042 |
| Highest intra-operative lactate* | 2.3 (1.5-3.3) | 2.5 (1.5-3.5) | 0.511 |
| Intraoperative blood loss (ml) * | 450 (200-920) | 300 (100-500) | 0.002 |
| Operation time (min) * | 190 (150-270) | 240 (180-300) | 0.002 |
| ITU stay (days) * | 1 (0-2) | 1 (0-1) | 0.091 |
| Hospital stay (days) * | 6 (5-9) | 5 (3-6) | 0.0008 |
| Complication >grade II | 30 (14.2) | 9 (9.9) | 0.354 |
| R1 (any metastasis+) | 76 (35.9) | 22 (24.2) | 0.060 |
| Closest margin (mm) * | 2 (0.2-6) | 5 (1-10) | 0.002 |
| 30-day mortality | 2 (0.94) | 0 (0) | 1.0 |
| Median overall survival (months) | 35 | Undefined | 0.004 |
| Median disease-free survival (months) | 9 | 18 | 0.0003 |
Table 2.
Demographics and outcomes of propensity score-matched laparoscopic and open hepatectomy patients. *median (IQR), $mean (±SD), major hepatectomy defined as >3 liver segments, + includes any hepatic or extrahepatic metastasis.
Table 2.
Demographics and outcomes of propensity score-matched laparoscopic and open hepatectomy patients. *median (IQR), $mean (±SD), major hepatectomy defined as >3 liver segments, + includes any hepatic or extrahepatic metastasis.
| Open | Laparoscopic | P | |
| Total N (%) | 82 (50.0) | 82 (50.0) | |
| Demographics | |||
| Age (years)* | 68 (61-75) | 69 (59-74) | 0.856 |
| Sex (male) | 48 (58.5) | 51 (62.2) | |
| BMI (kg/m2)* | 25.9 (23.5-28.7) | 26.5 (24.0-29.8) | 0.302 |
| ASA 1 2 3 |
9 (11.0) 58 (70.7) 15 (18.3) |
9 (11.0) 60 (73.2) 13 (15.9) |
0.915 |
| Anaerobic threshold$ (ml/min/kg) | 12.0 (±2.9) | 11.8 (±2.8) | 0.680 |
| Hb$ (g/L) | 133 (±15.1) | 133 (±15.9) | 0.994 |
| WCC$ (109/L) | 6.82 (±1.6) | 6.86 (±1.13) | 0.907 |
| Tumour biology | |||
| CEA* (ng/mL) | 5.5 (2.8-17.8) | 5.0 (2.3-14.1) | 0.269 |
| Neoadjuvant chemotherapy | 49 (59.8) | 44 (53.7) | 0.528 |
| Synchronous primary | 51 (62.2) | 43 (52.4) | 0.269 |
| Right-sided primary | 61 (74.4) | 62 (75.6) | 1.0 |
| Node positive primary | 55 (67.1) | 48 (58.5) | 0.332 |
| Synchronous lung metastases | 13 (15.9) | 10 (12.2) | 0.653 |
| Bilobar metastases | 30 (36.6) | 24 (29.3) | 0.406 |
| Number of metastases* | 2 (1-3) | 1 (1-3) | 0.492 |
| Largest metastasis (mm)* | 30 (20-45) | 30 (22-41.5) | 0.789 |
| Major hepatectomy | 28 (34.1) | 29 (35.4) | 1.0 |
| Outcomes | |||
| Pringle time (min) * | 21.5 (2.0-40.5) | 40 (12-55.5) | 0.005 |
| Highest intra-operative lactate* | 2.23 (1.6-3.1) | 2.5 (1.5-3.5) | 0.499 |
| Intraoperative blood loss (ml) * | 400 (150-738) | 300 (100-500) | 0.026 |
| Operation time (min) * | 160 (120-240) | 240 (180-300) | <0.0001 |
| ITU stay (days) * | 1 (0-2) | 1 (0-1) | 0.912 |
| Hospital stay (days) * | 6 (5-8) | 5 (3-6) | 0.014 |
| Complication >grade II | 6 (7.3) | 7 (8.5) | 1.0 |
| R1 (any metastasis+) | 29 (35.4) | 21 (25.6) | 0.235 |
| Closest margin (mm) * | 2 (0-6) | 5 (1-10) | 0.008 |
| 30-day mortality | 1 (1.2) | 0 (0) | 1.0 |
| Median overall survival (months) | 50 | undefined | 0.442 |
| Median disease-free survival (months) | 12 | 15 | 0.096 |
Table 3.
Comparison of overall and disease-free survival represented at hazard ratios and 95% confidence intervals in the laparoscopic and open cohorts in the unadjusted and PSM cohorts. .
Table 3.
Comparison of overall and disease-free survival represented at hazard ratios and 95% confidence intervals in the laparoscopic and open cohorts in the unadjusted and PSM cohorts. .
| Model | Overall survival | Disease-free survival | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-value | Hazard Ratio (95% CI) | p-value | |
| Unadjusted | 0.59 (0.42-0.85) | 0.004 | 0.55 (0.41-0.76) | <0.001 |
| Propensity score matched | 0.83 (0.51-1.36) | 0.442 | 0.74 (0.5-1.09) | 0.129 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



