
Submitted:
23 May 2023
Posted:
25 May 2023
You are already at the latest version
Abstract
The advent of immunotherapy and specifically of immune checkpoint inhibitors (ICIs) for the treatment of solid tumors has deeply transformed therapeutic algorithms in medical oncology. Approximately one third of patients treated with ICIs may develop immune-related adverse events, being the gastrointestinal tract often affected with different grades of mucosal inflammation. Checkpoint inhibitors colitis (CIC) presents with watery or bloody diarrhoea and in case of severe activity requires ICIs discontinuation. The pathogenesis of CIC is multifactorial and still partially unknow: anti-tumor activity that collaterally effects the colonic tissue and the upregulation of specific systemic inflammatory pathways (i.e., CD8+ cytotoxic and CD4+ T lymphocytes) are mainly involved. Many open issues remain on treatment timing and options, and biological treatment, above all with anti-TNF alpha, can be offered to these patients aiming to rapidly resume the oncological therapies. This review aims to summarize the pathogenetic mechanisms underlying CIC and to discuss evidenced-based management including the role of biological therapy.
Keywords:
checkpoint inhibitors
; colitis
; immune-related adverse events
; enterocolitis
; diarrhea
1. Introduction
Cancer is the second leading cause of death, after heart disease, in Europe and United States [1]. The advent of immunotherapy has completely revolutionized cancer treatment in the last decade, representing a novel opportunity for patients who failed standard treatments [2]. Basically, immunotherapy aims to boost natural defences to eradicate malignant cells [3].
Indeed, the adaptive and natural immune systems play an essential role in the surveillance and suppression of tumors [4]. However, cancer cells and their microenvironment can evade the immune system by inducing a hypofunctional state of the immune cells, especially of the T-cells, and promoting the survival of the tumor itself. One established mechanism is represented by cancer cells’ activation of the immune checkpoints, proteins that usually down-regulate and limit the immune response, by maintaining the T-cells inactivated and thus escaping immune surveillance [5].
Immune checkpoint inhibitors (ICIs) represent one of the most important categories of immunotherapy and are composed of monoclonal antibodies that aim to strength and reinvigorate the immune system, by binding to these co-inhibitory receptors, inducing immune-mediated tumoral cell death [4]. Since their first approval in 2011 [6], they showed promising results [7,8] and were approved by the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of different neoplasms such as melanoma, non-small cell lung carcinoma (NSCLC), renal cell carcinoma, urothelial carcinoma, breast cancer, gastro-intestinal (GI) cancers and lately Hodgkin lymphoma. Their indication is summarized in Table 1.
At present, approved ICIs are directed against cytotoxic T-lymphocyte associated protein-4 (CTLA-4) (i.e., Ipilimumab), programmed death protein-1 (PD-1) (i.e., Nivolumab, Pembrolizumab, Cemiplimab) and PD-ligand 1 (PD-L1), (i.e., Atezolizumab, Durvalumab, Avelumab). PD-1 and PD-L1 are co-inhibitory proteins expressed by lymphocytes and antigen-presenting cells (APC) that induce self-tolerance and autoimmunity control, while CTLA-4 is expressed on T and B cells and functions to negatively regulate lymphocyte activation [9].
On the other hand, immune checkpoints are relevant in balancing pro and anti-inflammatory responses and their inhibition may lead to an overactive immune response and humoral autoimmunity which can lead to a large spectrum of immune-related adverse events (irAEs) [10]. This inflammatory toxicity can affect any organ; most frequently the skin, the GI, endocrine, and respiratory systems, and more rarely the nerves and the heart [11].
Skin and GI irAEs represent the principal leading causes of ICIs’ discontinuation, presenting in up to 50% of the patients [12].
To date, irAEs pathogenesis and management are still unclear. This review aims to summarize the current mechanisms underlying immune checkpoint inhibitors colitis (CIC) and evidence-based management, focusing on the unclear pathogenesis aspects, the role of biological therapy and the similarity with inflammatory bowel disease (IBD).
2. Epidemiology
ICIs-IrAEs have a wide variability of organs involvement, time of onset and association with the type of tumor and ICI [13].
Aside from the most common constitutional symptoms such as fever, pruritus and fatigue, anti-CTLA-4 is more associated with diarrhea (36%), colitis (8%) and hypophysitis (4%), while anti PD-1 and PD-L1 can lead more frequently to thyroiditis (8%) and pneumonitis (4%) [14,15]. Furthermore, tissue-related factors and the tumoral microenvironment could play a major role in determining the autoimmune response profile. For example, a recent systematic review reported that patients affected by melanoma were more likely at risk of developing skin and GI irAEs, while pneumonitis, thyroiditis or hypophysitis were more associated with non small cell lung cancer (NSCLC) or renal cell carcinoma [14].
Major AEs (grade ≥3) are more frequent in patients treated with an anti-CTLA-4 alone (34%), while adverse events were reported in 14% and 20% of the patients treated with PD-L1 and PD-1 inhibitors monotherapy respectively. Immunotherapy combination was related to major adverse events (55%) [16]. Higher toxicity related to anti-CTLA-4 therapy may be due to a more generalized immune response by producing a massive T-cell proliferation, compared to anti-PD1/PD-L1 [17].
Besides, anti-PD-1 and PD-L1 did not show a dose-toxicity relationship while irAEs’ severity and frequency associated with ipilimumab are dose-related. [18]
Generally, irAEs can appear within 2-16 weeks from ICIs’ introduction with precocious dermatological (i.e., 2-3 weeks) and GI manifestations (i.e., 5-6 weeks) for both CTLA-4 and PD-1 inhibitors, while endocrine adverse events usually occur later and are associated with a slower resolution, needing a long hormonal substitutive therapy [19].
Regarding GI adverse events, the lower GI tract is the most affected. Diarrhoea is the leading adverse event, involving nearly 36% (31-41) of the patients treated with ipilimumab, 11% (9-14) with PD-L1 inhibitors and 44% (39-49) for combination therapy [16,20].
The evidence of colitis, defined as the presence of mucosal inflammation, is less common. Recent systematic reviews reported an incidence of 8.6% of colitis, higher than the one evaluated during clinical trials [12,16].
No study reported a statistically significant correlation between sex, tumor type and the severity of immune-mediated colitis [21]. Colitis could occur at any time after the commencement of ICIs, with an earlier occurrence with PD-1 inhibitors [22], but a greater severity with anti-CTLA-4 and, especially, with combination therapy [12,16,21,23]. Its clinical manifestation includes diarrhoea as the main symptom, associated with abdominal pain, bloody stools and fever. Nausea, weight loss and oral aphthous ulcers were reported with a lower frequency [24]. Diffuse enteritis could be present alone or, more frequently, in association with colitis in 25% of patients [23]. Although rare (0.3-1.3%), fatal adverse events related to ICIs are mostly represented by colitis and toxic megacolon with colonic perforation, especially with anti CTLA-4 [25]. Isolated upper gastrointestinal inflammation (gastritis, gastroenteritis, or enteritis) can also occur with a frequency above 10%. [26,27,28]
Furthermore, irAEs can affect also the liver inducing hepatitis although in a lower proportion in comparison with the lower GI tract. In a recent Phase 3 study evaluating the safety of nivolumab and ipilimumab for melanoma, monotherapy-related hepatitis was identified in 4% of patients, with severe hepatitis (5-20 x ULN transaminases) in 1% and in 2% of patients treated with nivolumab and ipilimumab, respectively; ALT elevations were reported in 19% of patients treated with combination therapy [29]. Clinical manifestations may range from asymptomatic elevations of liver enzymes, jaundice alone, and more rarely, coagulopathy and hepatic failure [23]. In addition, even the pancreatic gland could be affected by immune-mediated mechanisms; generally, irAEs lead to an asymptomatic rise of blood amylases/lipases in 2.7% of cases, while in only 15% of these patients long-term adverse outcomes, including chronic pancreatitis, recurrence, type 1 diabetes and exocrine insufficiency, are observed, mostly related to CTLA-4 target therapy and in patients affected by melanoma cancer [30].
3. Pathogenesis of checkpoint inhibitors colitis (CIC)
T cells are physiologically responsible for the selective targeting and destruction of tumor cells and are activated by two pathways: direct stimulation of the antigen mediated by the T cell receptor (TCR) and by the MHC class II on APCs and a co-stimulation between the CD28 receptor on T cells and the CD80/86 on APCs. Activated T lymphocytes proliferate, produce cytokines and express CTLA4 and PD1, with regulatory functions [35,36].
CTLA-4 is constitutively expressed on the surface of FOXP3 CD4+ T regulatory (Treg) lymphocytes and has the task of terminating the co-stimulation between T lymphocytes and APCs, binding competitively to CD80/86 with respect to CD28 [37,38]. Furthermore, CTLA-4-mediated inhibitory interaction leads to the production of immunosuppressive cytokines such as IL-10 and TGF-b by Treg cells, which also inhibit other T cells’ activation and proliferation [39].
On the other hand, PD-1 is expressed on the surface of T cells and other immune cells, while PD-L1 is expressed on APCs. The PD-1/PD-L1 interaction suppresses the signaling downstream of the TCR, with a reduction of the transcriptional activity underlying the production of proinflammatory cytokines [40].
Under normal conditions, CTLA-4 and PD-1/PD-L1 act as negative regulators, maintaining “the balance” of the immune system [41]. Nevertheless, tumor cells often acquire the ability to escape immune response, expressing PD-L1 and PD-1 whom combine on the surface of cells, with downregulation of the T-cell response [42].
ICIs’ inhibition of regulatory mechanisms is associated with the loss of control over autoreactivity, resulting in a higher incidence of irAEs during treatment with these agents [43]. However, this assumption alone is reductive and the mechanisms governing irAEs, in particular for CIC, are very complex, involving many actors such as: cellular autoimmunity, autoantibodies, complement activation, cytokines-chemokines release, genetics and alterations of the gut microbiome [44].
While research is focusing on this issue, the specific mechanisms are still poorly understood.
Briefly, we can categorize 3 main domains of mechanisms:
- on target effects: anti-tumor activity that collaterally affects normal tissue
- off-target effects: upregulation of some systemic inflammatory pathways
- host-related factors (e.g., microbiome)
3.1. On target effects
ICI-induced overactivation of T lymphocytes generates a response against tumor antigens. However, normal and tumor cells display many common antigens (“epitope sharing”), and cell lysis mediated by CD8+ cytotoxic T lymphocytes induces the release of tumor antigens and, collaterally, self-antigens from normal tissue. This phenomenon, called “epitope diffusion or spreading”, promotes diversification of the T cell repertoire, reducing immune tolerance, which is also strengthened by inhibition of Treg lymphocytes. These events result in activated T cells targeting non-tumor antigens or self-peptides [45,46].
The collateral presence of autoreactive T cell clones in healthy tissues during treatment with ICIs is documented in different types of irAEs, in particular in case of myocarditis, myositis and skin toxicity [47,48,49].
As regards CIC, evidence indicates that a high bowel infiltration of CD4+ T and CD8+ T lymphocytes correlates with the severity of the disease [50,51].
Specifically, the increase of CD4+ T lymphocytes is usually found in subjects treated with anti-CTLA-4, while the increase of CD8+ is associated with anti-PD-1 colitis [52].
Studies in animal models support this hypothesis: in CTLA-4 knock-out mice a widespread infiltration of immune cells was found in various organs and also in the intestinal tissues [53,54]. Furthermore, spontaneous development of colitis occurs also in B7 (CD80/86) double knock-out transgenic mice due to poor stimulation of CTLA-4, with also a decrease in the number of FOXP3 Treg cells [55].
Similarly, humans with germline mutations in CTLA-4 develop immune dysregulation syndromes with early-onset diarrhea and colic inflammation [56,57].
Moreover, another class of T cells appears to play a key role in irAEs, in particular those affecting mucous layers, and tumor response to ICIs: the tissue-resident memory T (Trm) cells [58].
Louma et al. conducted a comprehensive single-cell analysis of immune cell populations in CIC, reporting a pathological accumulation of cytotoxic CD8+ T cells: TCR sequence analysis suggested that the majority of those colitis-associated CD8+ T cells arose directly from the Trm population, explaining the higher frequency and early onset of colitis symptoms after initiation of treatment. The activation of resident CD8+ T cells induces subsequent recruitment of additional CD8+ and CD4+ T-cell populations from blood [50].
Additionally, Sasson et al. highlighted that CD8+ Trm cells are the most represented activated T cell subset in CIC and their activation level is related to colitis clinical and endoscopic severity. Furthermore, RNA sequencing indicates that these cells express high levels of transcripts for checkpoint inhibitors and INFγ. The authors proposed this INF-producing cell as a pathological hallmark of CIC and as a novel target for therapy [59,60].
Increased infiltration of CD8+ lymphocytes is recognized as a specific feature of CIC and increased CD8+/CD4+ ratio have been proposed as a simple biomarker and discriminator with respect to other forms of colitis [61]. On the other hand, it is not clear if Treg cells infiltration could be another hallmark of CIC, as their presence can be either increased or decreased [50,62,63].
Although CTLA-4 appears to play a more central role than PD-1 or PD-L1 in intestinal homeostasis, it is important to note that PD-1 plays a key role in the developmental process of innate lymphoid cells, which are central effectors of the GI mucosa [64].
It seems that the severity of CIC is related to the increasing number of innate group 3 lymphoid cells in the mucosa, which control homeostatic functions of the tissue barrier and regulate host-commensal flora mutualism [65].
Antibody-mediated autoimmunity may also be involved in the pathogenesis of irAEs [44]. According to a recent systematic review, autoantibodies are present in about 50% of patients with ICI-induced endocrinopathies, skin and muscle diseases. Instead, they are rarer in rheumatologic affections (11-30%), liver disease (18%, ANA+) and colitis (19%, pANCA+) [66]. However, their utility as biomarkers is unclear, due to the fact that they are often detected after the onset of irAEs without a baseline comparison [67].
Complement involvement is assumed, particularly in ICI-induced hypophysitis. Indeed, it has been reported that endogenous autoantibodies and/or exogenous IgG1 anti-CTLA-4 (such as ipilimumab) activate the classic complement pathway [68]. As far as colitis is concerned, there is no such data in the literature.
3.2. Off target effects
During treatment with ICIs the disproportionate increase of inflammatory cytokines is well documented [69]. Moreover, some cases of cytokine release syndrome were recently reported [70].
Regarding CIC, some cytokines are upregulated, such as tumor necrosis factor α (TNFα) and interferon γ (IFN-γ) [50,52], TNF-like cytokine 1A (TL1A) and its receptor DR3 [71], and interleukine 17 (IL-17), with activation of T helper (Th) 1 and Th17 T lymphocytes [72].
Furthermore, a small study in CIC patients reported a significant decreased in granulocyte colony-stimulating factor (GCS-F) compared to controls [73], and recent evidences suggest also a role of the IL-23/INF- axis, as the predominant aspect of cytotoxic lymphocyte response and regulation [74] and a systemic upregulation of IL-6 which determines a myeloid infiltration in colonic mucosa [75].
High concentrations of T cell chemotactic chemokines (i.e., CXCL9 and CXCL10) are generally associated with irAEs [76], but differences in gene expression of chemokines and their receptors have been reported in CIC patients. Indeed, CXCR3 and CXCR6 chemokine receptor (CXCR9/10 and CXCR16, respectively) genes show high-level expression on T-cell population, upregulating T-cell activity [50,77].
Furthermore, in T-cell clusters associated with colitis, the increased expression of genes coding integrin receptors is reported. This upregulation of integrin receptors could lead to lymphocyte retention in the intestinal mucosa [78].
3.3. Host-related factors
The role of demographic factors was evaluated in an analysis of 455 anti-PD-1-treated melanoma patients: total irAEs rate did not vary between younger and older subjects, however serious events were more frequent in younger people, in particular colitis and hepatitis, even if reported mortality was low. No link was found between gender or seasonality and irAEs [79]. Also tumor kind and type of treatment seems to be involved, since colitis and skin irAEs are generally more common in patients with underling melanoma, treated with anti CTLA-4 therapy [14]. Moreover, concomitant use of NSAIDs is associated with increased risk of CIC [24]; conversely vitamin D seems to be protective [80]. Genetic susceptibility is supported by clinical and preclinical studies in mice with loss of function of checkpoint inhibitors genes, as previously discussed [54]. In addition, some clinical studies have correlated certain human leukocyte antigens or polygenic profile with an increased-risk of developing of immune-mediated diseases and irAEs as well (e.g., HLA-DRB1*04:05 is associated with ICI-induced arthritis and HLA-DR4 to ICI-induced diabetes) [81,82].
The gut microbiota is a complex ecological system which plays a key role in both maintaining homeostasis and in determining the risk of development of certain diseases, such as infections and IBD [83]. The influence of the microbiome on ICIs’ response is well established and evidences suggest that it plays also a key role in determining the onset of irAEs and, especially of CIC [84].
In a prospective study on melanoma patients, gut microbiome’s analysis was performed at baseline and at the onset of GI toxicity: treatment did not modify the microbiome, but those patients with prevalence of Faecalibacterium prausnitzii and other firmucutes, compared to Bacteroides fragilis, were more likely to develop colitis, probably due to an upregulation of dendritic cells and APCs, with proliferation of T cells and recruitment of cytotoxic cells in colonic mucosa [85].
Coherently, elevated levels of Bacteroides (B fragilis and B phylum) seem protective, hindering the blocking effect of certain ICIs through stimulation of T-reg differentiation, making CIC less likely to develop. Similarly, Bifidobacterium is reported to be associated with a lower risk of CIC, while Clostridia and Escherichia may carry a higher risk [86,87].
Integrative analysis of gut microbiome and host transcriptomes reveals associations between favorable therapeutic responses to ICIs and GI irAEs with Enterobacteriaceae, related to ribonucleoprotein complex biogenesis, cytokine-mediated signaling pathway, tRNA metabolic process, and ribonucleoprotein complex assembling in the colon [88].
Furthermore, other studies hypothesized that the reduction in microbiome diversity could lead to irAEs [89,90,91].
Therefore, the manipulation of gut microbiome to obtain better response to ICI-therapy or to treat irAEs may be an option. In a study, probiotics Lactobacillus reuteri‘s administration in mice led to resolution of CIC through an inhibitory mechanism of group 3 innate lymphoid cells, strengthening the gut barrier function and modulating cytokine production [92]. The role of Lactobacillus reuteri in suppressing effect of intestinal inflammation in humans is well known [93].
Again, the combination of Burkholderia cepacia and Bacteroides fragilis or the administration of Bacteroides thetaiotaomicron in germ-free mice has been shown to reduce intestinal toxicity while stimulating the antitumor response [94,95]. Additionally Bifidobacterium species seem to mediate antitumor efficacy while attenuating intestinal inflammation [96,97].
To complete this topic, it should be noted that the microbiome is a dynamic system that is continuously modified also on the basis of nutrition or antibiotic treatments [98]. For example, it is proven that short-chain fatty acids (mainly butyrate and propionate) can modulate the microbiome and T reg cells proliferation and activation [99].
Some recent works are therefore focusing on personalized strategies to diversify the microbiome, in order to improve the response to oncological treatments and prevent or mitigate side effects [100].
3.4. CIC and IBD: shared pathogenesis
Beyond the similar clinical and endoscopic manifestations, CIC and IBD share some pathogenetic aspects. Both diseases exhibit upregulation of regulatory cytokines (such as IL-10, INF-γ and IL-17) at the mucosa level [71,72]. Furthermore, also CTLA-4, PD-1/PD-L1 and the gut microbiome display a key role in the intestinal immunity of both IBD and CIC [101].
Indeed, in mouse model of IBD, PD-1 protein administration was protective against colitis [102]. In humans affected by Crohn disease, intestinal APCs do not express PD-L1 [103]. On the other hand, some CTLA-4 polymorphisms are known to increase the susceptibility of developing both Crohn’s (CD) disease and ulcerative colitis (UC) [104].
A significant difference in the composition of the inflammatory infiltrate between IBD and CIC involves CD20+ cells (B cells) which are common in IBD but not in CIC [105].
A reduction in microbial diversity is typical of IBD patients compared to healthy individuals [106] and in particular a significative lower proportion of Bacteroides and higher proportion of Proteobacteria phyla are reported [107,108].
Figure 1.
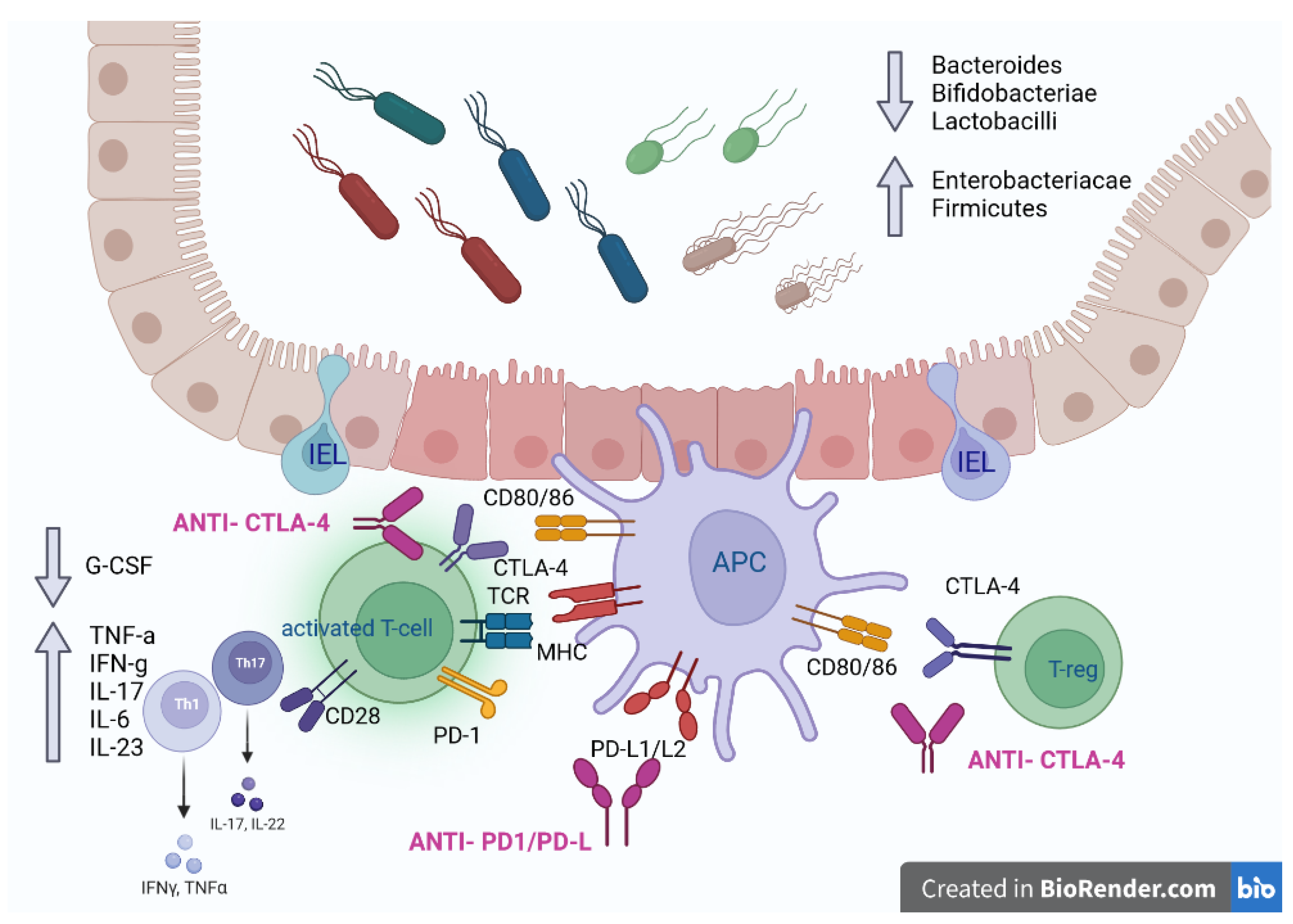
Therapy with ICIs modifies the ability of the immune system to self-regulate, in particular by interfering in the bonds between T cells and APCs. This results in an increased activity and number of activated T cells (effectors) in the intestinal epithelium, and a concomitant decreased of regulatory T cells (at least functionally). Moreover, a systemic pro-inflammatory state is associated, which is characterized by an increased concentration of cytokines such as TNF-α, IFN-γ, IL-17, IL-6 and IL-23, and a decrease of G-CSF. Furthermore, the composition of the intestinal microbiota plays an important role in the homeostasis and maintenance of the integrity of the gut epithelial barrier: higher proportions of Enterobacteriaceae and Firmicutes are associated with CIC, while higher proportions of Bacteroides, Bifidobacteriae and Lactobacilli seem to be protective. APC antigen presenting cell; IEL intraepithelial lymphocyte; T-reg T regulatory cell; Th T helper cell.
Figure 1.
Therapy with ICIs modifies the ability of the immune system to self-regulate, in particular by interfering in the bonds between T cells and APCs. This results in an increased activity and number of activated T cells (effectors) in the intestinal epithelium, and a concomitant decreased of regulatory T cells (at least functionally). Moreover, a systemic pro-inflammatory state is associated, which is characterized by an increased concentration of cytokines such as TNF-α, IFN-γ, IL-17, IL-6 and IL-23, and a decrease of G-CSF. Furthermore, the composition of the intestinal microbiota plays an important role in the homeostasis and maintenance of the integrity of the gut epithelial barrier: higher proportions of Enterobacteriaceae and Firmicutes are associated with CIC, while higher proportions of Bacteroides, Bifidobacteriae and Lactobacilli seem to be protective. APC antigen presenting cell; IEL intraepithelial lymphocyte; T-reg T regulatory cell; Th T helper cell.
4. Diagnosis
4.1. Diagnostic work up
ICI-induced GI diseases are pathological entities that can manifest with a wide range of clinical patterns and symptoms. For this reason, the final diagnosis should arise in a multidisciplinary context which must consider the clinical aspects and an accurate differential diagnosis, with exclusion of other etiologies such as infections, medications, other irAEs and IBDs [109].
CIC can mimic an infectious gastroenteritis, with an acute onset, usually in proximity to the infusion of ICI [23], so the suspect is usually oriented by temporal correlation. Only in small minority of cases an underlying infectious cause is demonstrated (<5%); however, excluding infective etiology is important when starting a treatment with immunosuppressants is planned [110].
Guidelines recommend to perform stool culture, clostridium difficile and parasitological search in all patients under ICIs treatment who develop symptoms such as moderate to severe diarrhea (interfering with daily activities), abdominal pain, nausea, vomiting, anorexia, fever or GI bleeding [110,111,112,113].
Furthermore, coexistence of infective cause and CIC is possible, with frequent encountered pathogens such as Clostidium difficile, cytomegalovirus (CMV), Salmonella and Candida [22,114–116].
To exclude other irAEs as cause of diarrhea, thyroid functionality, fecal elastase and celiac disease serology should be investigated [31,117,118].
Blood tests are not specific in the course of CIC. High C-reactive protein (CRP) level is frequent in all the irAEs types (42%) [119] and anemia, due to digestive bleeding, is a common finding in CIC [24].
Many markers have been proposed, such as leukocytosis (in particular neutrophils and eosinophils), increased inflammatory indices and low serum albumin level [120,121,122,123], but they are common to other irAEs and in general may depend on the underlying neoplastic pathology [22].
More sophisticate markers are increased IL-17 [72] and decreased baseline GCS-F, which appears to be a common finding in patients with CIC but actually not used in the normal clinical practice [73], [124].
The usefulness of fecal inflammatory markers (lactoferrin and calprotectin) is suggested by some authors. Lactoferrin was validate in a cohort of 71 patients with ICI-induced diarrhea, with sensitivity (Sn) for detecting macroscopic colitis of 70% and histological colitis of 90%. Regarding fecal calprotectin, a concentration >150 mcg/g achieved a sensitivity of 68% for detection of macroscopic colitis and of 86% for detecting microscopic inflammation [125].
In addition, fecal calprotectin may be also used as a surrogate for endoscopic and histologic remission. Indeed, in a retrospective analysis by Zou et al., its concentrations significantly decreased from onset to end of treatment (p<0.001). Furthermore, high concentrations were statistically associated with the presence of endoscopic inflammation, correlating positively with the Mayo Endoscopic Subscore. The authors identified a cut-off for predicting endoscopic remission of ≤116 μg/g and ≤80 μg/g for histological remission with specificity (Sp) of 94% and 85%, respectively [126].
Endoscopy with biopsies is the cornerstone of diagnosis, but it is needed also for staging the severity of the disease, as clinical presentation may not strictly correlate with the endoscopic-radiological findings and with the outcomes [111,127]. It is suggested in all cases of suspected ICI induced colitis or at least in patients with diarrhea/colitis grade ≥ 2, also to exclude CMV infection [22].
The typology of the examination (ileo-colonoscopy vs rectosigmoidoscopy, with or without esophagogastroduodenoscopy) and the biopsy protocol are as well not standardized. Guidelines suggest that examination of the left colon is sufficient in most of the cases of colitis [22] as literature reports a prevalent presentation of left-sided colitis (31%–43%) or pancolitis (23%–40%), while exclusive right-sided colitis and isolated ileitis are rare (2,7% and 6%–14% respectively) [125,128,129].
However, two recent expert consensus suggested that a total ileo-colonoscopy is preferred as it allows a better detection rate and precise description in consideration of the possible irregular distribution of the disease [130,131].
If unavailable or dangerous for perforation risk, flexible sigmoidoscopy is acceptable and complete ileo-colonscopy could be performed as second line if initial assessment is inconclusive.
Esophagogastroduodenoscopy is usually considered in cases where the ileo-colonscopy is negative and/or extracolonic involvement is suspected [132].
Endoscopic presentation can space from severe presentations (acute colitis) to normal mucosa appearance. Diffuse inflammatory patterns of presentation, mimicking UC, are more common (75%) rather than segmental or patchy distribution resembling Crohn’s disease [111,125].
Ulcerative and non-ulcerative forms have similar incidence, where the latter is characterized by a range of lesions such as erythema, exudate, erosion, friability, loss of vascular pattern, and edematous or granular mucosa [133,134].
In a retrospective study of 2018 analyzing a cohort of 58 patients with CIC, 40% of patients presented ulcerations, while 42% had non-ulcerative inflammation [127].
Interestingly, it is important to note that a subgroup of patients (20-30%) had a normal macroscopic endoscopic appearance [20,135] with evidence of microscopic colitis on histological evaluation [136,137].
Endoscopic features have a prognostic value, since colonic ulcerations, in particular those larger than 1 cm and/or deeper than 2 mm, and extensive colitis delineate a high risk group of patients, with lower rate of steroid response, frequent need of biologics [125] and more severe course (longer hospital stays, disease recurrence, requirements for repeat endoscopy) and symptoms.
Indeed, the endoscopic Mayo score is the most used for grading the severity of the endoscopic features: higher scores are associated with a more frequent need of infliximab (p=0.008) [138].
4.2. Histological diagnosis and histological variants
Generally, histologic changes can precede the onset of clinical symptoms. Indeed, in a study involving patients with ipilimumab induced-colitis, histologic changes appeared 1-2 weeks after treatment, while symptoms occurred 3 weeks later [52]. The main histopathological features for the diagnosis of CIC are acute or chronic inflammation, increased apoptosis, increased intra-epithelial lymphocytes and chronic changes (such as Paneth cells or pseudo-pyloric metaplasia and crypt structural distortion). Furthermore, overlapping of multiple phenotypes is possible and frequent [22,127]. These histologic characteristics result in various pathological patterns such as active colitis, chronic colitis, microscopic-like colitis (collagenous and lymphocytic), ischemic-like colitis, non-specific inflammatory reactive changes [139,140,141].
Acute inflammation, which is the most common finding, includes ulceration, neutrophilic and eosinophilic infiltration of superficial epithelium or crypts and crypt abscess formation [111]. In a systematic review, inflammatory cell infiltration and cryptitis and/or crypt abscesses were the most frequently reported pathological features of CIC (50% and 33.3%, respectively) [22]. Increased apoptotic activity is reported in 20-40% of the cases, till crypt atrophy and dropout [97,112].
Chronic inflammation is characterized by the presence in the lamina propria of lymphocytes, eosinophils and plasma cells [127,142]. Granulomas have been described but are rare [143].
There are no histological differences between anti-CTLA-4 and anti-PD-1/PD-L1 induced colitis [144], except for a more frequent presentation with active colitis and a higher presence of crypt atrophy in patient treated with anti PD-1 [142].
Among microscopic-like phenotypes, an increased presence of intra-epithelial lymphocytes, mimicking lymphocytic colitis, is reported in a minority of cases (10-12%) especially in patients treated with anti-CTLA-4 antibodies [136,145]; conversely a collagenous colitis-like phenotype is rarer and associated with anti-PD-1 anti-PD-L1 [137,146].
Usually in microscopic phenotype the crypt structure is preserved and the acute inflammatory component is reduced [147,148], even if an overlap with acute neutrophilic inflammation is also reported in literature [149]. Moreover, microscopic CIC is associated with a higher rate of hospitalization and a more aggressive disease course compared to idiopathic microscopic colitis [136].
Ischemic-like colitis is a rare pattern of CIC, characterized by atrophic crypts, reactive epithelial changes, and lamina propria fibrosis [150].
Uncommonly isolated increased apoptosis, without concurrent other pathological features of active or chronic inflammatory manifestations, can configure a scenery like graft-versus-host disease [140].
A differential diagnosis at the microscopic level between CIC and IBD can be tough, being their endoscopic and histological manifestations very similar and in some circumstances nearly superimposable [151]. Indeed, clinical features should sustain the diagnosis of CIC, in particular as regard the temporal relationship between the onset of symptoms and infusion timing [28]. Broadly, we can affirm that CIC is usually characterized by active colitis, where IBD usually shows chronicity signs [152]. In a study of 2018, compared with UC, ipilimumab-associated colitis presented less basal plasmacytosis (14% vs. 92%), less crypt distortion (23% vs. 75%), and more apoptotic bodies (17.6 vs. 8.2) [105]. Anyway, approximately 40-60% of patients with CIC present features of chronic inflammation in pathological samples [127,150], and some forms of chronic active colitis, which strictly resemble the pathological pattern of IBD, have also been reported [144,153]. Moreover, some differences can be found in the immunological profile of biopsy samples: in a study in patients with CIC induced by anti-CTLA-4, a higher prevalence of CD4+ T cells was reported, compared to IBD patients samples, where Treg cells were more frequent [52].
More consistent data could derive from the analysis of the surgical specimens, which, however have only been analyzed in very few studies in consideration of the small number of patients needing surgery. In those studies, common findings were an extensive acute severe colitis with transmural inflammation and necrosis, and a demarcated transition between normal and ulcerated mucosa [24,154].
Furthermore, to date there are no precise indications on sampling protocol, biopsies processing and criteria applied to formulate the diagnosis. In this regard, a recent expert consensus proposed that sampling should be guided by endoscopic appearance, with targeted biopsies of the most abnormal area or random biopsies in case of normal appearance (taking 2-3 samples per segment), ideally before starting treatments. Processing encompasses samples orientation for visualization of the long axis of the crypts, use of hematoxylin and eosin staining, application of immunohistochemistry to rule out CMV infection. The panel also concluded that existing scores for the assessment of histopathological activity, such as the Geboes score and Nancy indexes, are uncertain in the context of CIC, therefore it would be appropriate to develop a new specific tool [130].
On the other side, a dual center retrospective study on 134 patients who developed CIC demonstrated a correlation between higher Nancy index score (3 and 4) and the likelihood of infliximab treatment [155].
4.3. Imaging
Computered tomography (CT) scan is essential in CIC when serious complication such as megacolon, perforation, ischemia or hemorrhage is suspected [22]. However, the usefulness of imaging, and in particular of abdominal CT (possibly with contrast fluid) as a diagnostic tool is controversial and variable in literature.
Two main imaging presenting phenotypes are recognized: diffuse and segmental colitis. Atypical presentations include diffuse colonic dilation or isolated recto-sigmoid colitis. Most common features are bowel walls thickening, presence of liquid in the intestinal lumen (with air/fluid levels) and stranding of peri-colonic-mesenteric fat [156,157,158].
A retrospective analysis on 48 patients reported thickening of the intestinal wall in 97% of the cases and fluid-filled colon in the 82%, with widespread diffusion in the 61.8%. [159].
In a retrospective cohort study of 34 melanoma patients treated with ipilimumab, abdominal CT scan was highly predictive of colitis with a Sn, Sp, positive predictive value (PPV) and negative predictive value (NPV) of 85%, 75%, 96% and 43%, respectively [158].
Conversely, another retrospective cohort study of 138 patients who underwent both CT and endoscopy within 3 days, showed lower rates of accuracy of CT scan with a Sn of only 50%, Sp of 74%, PPV and NPV of 73% and 52% respectively [160].
Furthermore, authors elaborated a radiological score of severity based on different features: multiple (i.e ≥3) involved colonic segments, mural thickening, moderate or marked mural/mucosal hyperenhancement, mesenteric hyperemia, fluidfilled bowel loops, pericolonic fat stranding, and small bowel involvement. The presence of each feature corresponded to a score of 1, with a maximum of 7 points. The score was capable of predicting intravenous steroid use (OR 10.3), length of stay > 7 days (OR 9.0) and endoscopic mucosal ulceration (OR 4.7) [161].
Data are heterogeneous, however it can be suggested that, if CT scan alterations are present in a patient with history of ICI assumption, colitis is likely to be present, conversely negative scan is insufficient to exclude colitis.
Figure 2.
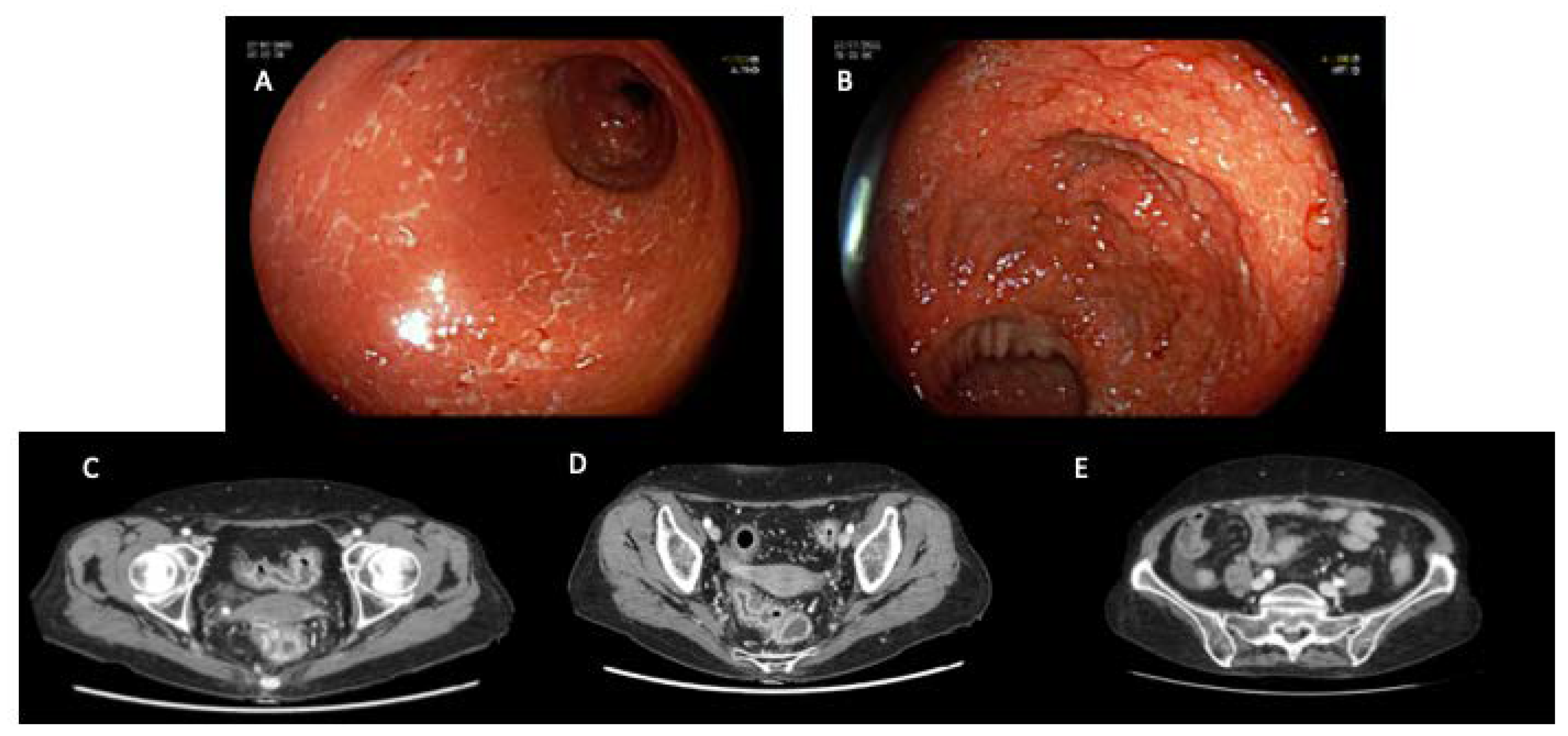
Clinical case: a 62 years old female patient affected by metastatic colorectal cancer, previously failure to traditional chemotherapy, was treated with Pembrolizumab. No personal or family history of IBD was reported in her clinical records. After one month of therapy she developed a severe gastrointestinal adverse event (diarrhea, CTCAE grade 3) requiring hospitalization. Therapy with metilprednisolone (40 mg x 2/die) was started on admission based on clinical suspicious of immune-mediated adverse event. After five days of intravenous steroid therapy the patient was still symptomatic and second level exams were required. In the first endoscopic image (A) the mucosa appears edematous, fragile, eroded and with serpiginous ulcers. The second image (B) shows the ileo-colic anastomosis: the mucosa of the ileum is spared. Endoscopic and CT evaluation revealed a severe colonic inflammation. In CT scans (images (C) and (D)) the thickening of the colonic wall can be appreciated. Because of clinical failure of high dose intravenous steroid treatment, proven also by endoscopic and radiological findings, a single dose of intravenous Infliximab 5mg/kg was administrated. Soon after Infliximab administration a complete regression of clinical symptoms and signs was observed. Considering the complete clinical remission and the advanced oncologic stage, the endoscopic examination was not repeated. The CT scan confirmed the healing, indeed in image (E) the thickness of the colonic wall is in normal range.
Figure 2.
Clinical case: a 62 years old female patient affected by metastatic colorectal cancer, previously failure to traditional chemotherapy, was treated with Pembrolizumab. No personal or family history of IBD was reported in her clinical records. After one month of therapy she developed a severe gastrointestinal adverse event (diarrhea, CTCAE grade 3) requiring hospitalization. Therapy with metilprednisolone (40 mg x 2/die) was started on admission based on clinical suspicious of immune-mediated adverse event. After five days of intravenous steroid therapy the patient was still symptomatic and second level exams were required. In the first endoscopic image (A) the mucosa appears edematous, fragile, eroded and with serpiginous ulcers. The second image (B) shows the ileo-colic anastomosis: the mucosa of the ileum is spared. Endoscopic and CT evaluation revealed a severe colonic inflammation. In CT scans (images (C) and (D)) the thickening of the colonic wall can be appreciated. Because of clinical failure of high dose intravenous steroid treatment, proven also by endoscopic and radiological findings, a single dose of intravenous Infliximab 5mg/kg was administrated. Soon after Infliximab administration a complete regression of clinical symptoms and signs was observed. Considering the complete clinical remission and the advanced oncologic stage, the endoscopic examination was not repeated. The CT scan confirmed the healing, indeed in image (E) the thickness of the colonic wall is in normal range.
5. Management
IrAEs are generally evaluated using the Common Terminology Criteria for Adverse Events (CTCAE) from the National Cancer Institute, attributing ascending severity grade from 1 to 5 (mild, moderate, severe, life-threatening, or death) [13].
To date, CIC treatment is based on expert consensus and on the severity of symptoms, due to the absence of prospective clinical trials defining the management of GI toxicity [12,110]. Therapy should start within five days from the commencement of symptoms since it is associated with a faster resolution [162]. As mentioned above, pre-emptive exclusion of infectious diseases and blood testing (blood count, CRP, celiac disease serology, metabolic panel, electrolyte levels etc) are mainly important to assess colitis etiology and severity [21].
The diagnostic value of faecal calprotectin and lactoferrin is still debated [131], however, only the American Gastroenterological Association (AGA) guidelines suggest the early use of fecal markers in patients with grade ≥ 2 diarrhea/colitis in order to identify who need endoscopic assessment [110], conversely the British Society of Gastroenterology (BSG) did not produce any specific statement [113] and in a recent Belgian consensus no significant agreement was reached on the value of fecal markers [131]. Nevertheless, some authors consider faecal calprotectin a useful non-invasive bio-marker to assess colitis severity at the onset and during follow-up, in particular after reaching clinical remission [163].
To present, there is no evidence of prophylactic use of locally acting corticosteroids, such as budesonide, to prevent the onset of CIC [164]. Furthermore, present guidelines do not recommend the use of antibiotic therapy unless high suspicion of infectious etiology. Indeed, a retrospective study showed a negative association between anaerobic antibiotic therapy and colitis’ severity and survival rates, strengthening the hypothesis of a remarkable role of the gut microbiome and dysbiosis in CIC pathogenesis [165].
For grade 1 diarrhea/colitis (< 4 stools/d over baseline), the AGA (2021) and the ASCO (2021) guidelines recommend against the discontinuation of ICI and suggest supportive treatment as hydration and low-fiber diet [110,112] Anti-motility agents (loperamide, atropine/diphenoxylate) can be helpful after ruling out infectious etiology and in case of diarrhea only and no evidence of colitis [112]. Generally, hospitalization and endoscopic evaluation are not required, [131].
Grade 2 diarrhea/colitis (an increase of 4-6 stools/d over baseline and/or abdominal pain, mucus or bloody stool) requires systemic corticosteroids (CS) (prednisone 1-2 mg/kg/daily) until symptoms improve to grade 1 or less; afterward, it is reasonable starting corticosteroid taper over a period of 4-6 weeks. Furthermore, ICI should be temporarily suspended until improvement or, preferably, resolution of symptoms [110,112]. Generally, grade 2 diarrhea/colitis requires only an outpatient management, however, hospitalization could be considered if systemic symptoms (es fever, tachycardia, dizziness etc) are present [131]. Locally acting CS are not recommended given the lack of evidence. A single-center retrospective study reported a statistically significant positive correlation between ICIs microscopic colitis treatment with budesonide compared to the one with systemic CS [26]. Another retrospective study showed a notably efficacy of budesonide in the treatment of CIC relapses, but more prospective studies are needed to confirm these results [166].
Prompt endoscopic evaluation has to be strongly considered. Abu Sbeih et al. reported a shorter steroid treatment and less recurrence in patients who underwent endoscopic evaluation within 30 days, especially within a week after the onset of symptoms [125]. Early endoscopic assessment enables to recognize the features of high risk group (presence of deep ulcers and extensive colonic involvement), who are more likely to develop refractory steroid colitis [125,167].
Patients with grade 3 or 4 diarrhea/colitis (an increase of ≥7 stools/d or severe increase in stomy output compared with baseline, or presence of severe or persistent abdominal pain-fever-ileus-peritoneal signs; life-threatening consequences, urgent intervention is indicated) should be admitted to the hospital for management and monitoring. International guidelines recommend intravenous systemic CS treatment (i.e., methylprednisolone 1-2 mg/kg/daily), fluid replacement, and electrolyte balance. Intravenous steroids are particularly recommended in case of upper GI involvement. Moreover, ICI should be discontinued permanently [110,112].
Generally, clinical response can be observed within 72 hours after CS administration [40]. A recent meta-analysis (data not published yet) described a pool rate of 42% (95%CI=28%-56%) steroid refractory diarrhoea/colitis on a total of 1101 patients affected by CIC. Immunosuppressant second-line therapy such as biologics was necessary. The overall response to biological therapy was 96% (95%CI=87%−100%) with high heterogeneity between low-quality and high-quality studies, 64% and 97% respectively. Patients affected by melanoma appear to be more at risk of developing CS refractory colitis [168].
Moreover, patients were seven times more likely to receive biological therapy (42.86% vs 6.25%, P <0.05) if they suffered from a deteriorated or recurrent episode of CIC rather than a favourable outcome, such as improved or resolved colitis [22].
Additionally, high-risk patients could be considered for biologics as early treatment (alone or in combination with CS) and not only as an escalation after no response to CS. A recent single-center retrospective study conducted on 179 patients, demonstrated that the early introduction of infliximab (IFX) or Vedolizumab (VDZ) was greatly associated with fewer hospitalizations and steroid treatment duration. Selecting high-risk patients was based mainly on the severity of CIC and response to CS therapy, high levels of CF, presence of large and deep mucosal ulcerations and extensive inflammation beyond left colon [125,163,169].
To date, the choice of biological treatment and its posology is based on the experience and knowledge achieved with IBDs [170]. Thus, current guidelines recommend IFX as the first-line therapy for high-risk patients and refractory CS colitis. VDZ could be a valid alternative [110,112,113,131].
IFX (5 mg/kg) is a chimeric monoclonal antibody directed against TNF-α, a pro-inflammatory cytokine underlying several auto-immune diseases. Ibraheim et al. reported a clinical remission in the 81% of patients with CIC (95% CI 73-87%) treated with IFX. Furthermore, its administration could lead to a reduction at least of one-third of the duration of colitis symptoms [171]. Usually standard induction infusion at 0-2-6 weeks, as for IBDs, is preferred; however, a single-administration can be sufficient [113], reducing infectious and oncological progression risk [172].
In contrast, a retrospective study showed that at least three administrations were associated with less recurrence if compared to single- drug-shot [169].
In case of CS refractoriness or persistent/relapsing symptoms, endoscopic second look is considered in order to exclude CMV infection [112] since CMV colitis is also associated with higher risk of recurrence and colectomy [173].
VDZ is an anti-α4β7 integrin humanised monoclonal antibody that aim at hindering T-lymphocytes homing in the bowel mucosa and inducing inflammation. Given its gut specificity, its clinical use could lead to fewer systemic side effects and immunosuppression. To date, there is limited evidence in literature comparing VDZ and IFX in CIC. A retrospective study conducted on 28 patients with CIC treated VDZ (300 mg IV) after failure to CS and/or IFX, reported a percentage of 86% of sustained clinical remission. Response to VDZ was higher in patients naïve-to-biological therapy (95% vs 67%) [174]. Additionally, an observational cohort study comparing VDZ and IFX in CIC reported a similar response rate between the two monoclonal antibodies, but a longer time of clinical remission in VDZ group. Furthermore, VDZ was associated with shorter hospitalization and CS exposure. Secondly, patients who received VDZ monotherapy had more favorable outcomes and a less cancer progression rate compared to IFX monotherapy. The safety profile was similar; however, a notable rise of infection rate was observed in the IFX group [175].
In conclusion, both VDZ and IFX shared similar efficacy and safety in ICI’s colitis. In patients without response to a first biological therapy, considering the other molecule could be reasonable. Nevertheless, more studies and clinical evidence are needed. Thus, biological therapy should be critically pondered case-by-case by a multidisciplinary committee (oncologist, gastroenterologist, surgeon etc) [110,112,113].
Due to the irAEs’ complexity and unclear pathogenesis, other immunotherapies are currently under evaluation as potential alternatives to VDZ and IFX, such as calcineurin inhibitors [176], anti-IL-23 and anti-IL-12 blockade [177], Janus kinase (JAK) inhibitors as tofacitinib [178].
Given the crucial role that dysbiosis plays in CIC, the faecal microbiome transplantation (FMT) has been evaluated as a potential treatment in selected patients. Indeed, FMT can restore normal intestinal microbiome, reducing mucosal inflammation. To date, it is currently approved by international guidelines for the management of recurrent C. difficile colitis, but there is a lack of clinical evidence evaluating its use in CIC management. Several case series and reports described a high rate of success of refractory and severe CIC treated by FMT, however, no data provides information about timing and complications, such as infections [179,180] Thus, more evaluations and prospective studies are warranted.
Lastly, colectomy is a rare potential treatment indicated in life-threatening colitis not responding to medical therapies, especially in the case of colonic perforation which occurs mostly with anti-CTLA-4 [25,113]. Nevertheless, there is no consensus on its timing, indications or implications on cancer therapies, therefore current guidelines recommend it in selected cases after multidisciplinary discussion [181].
Figure 3.
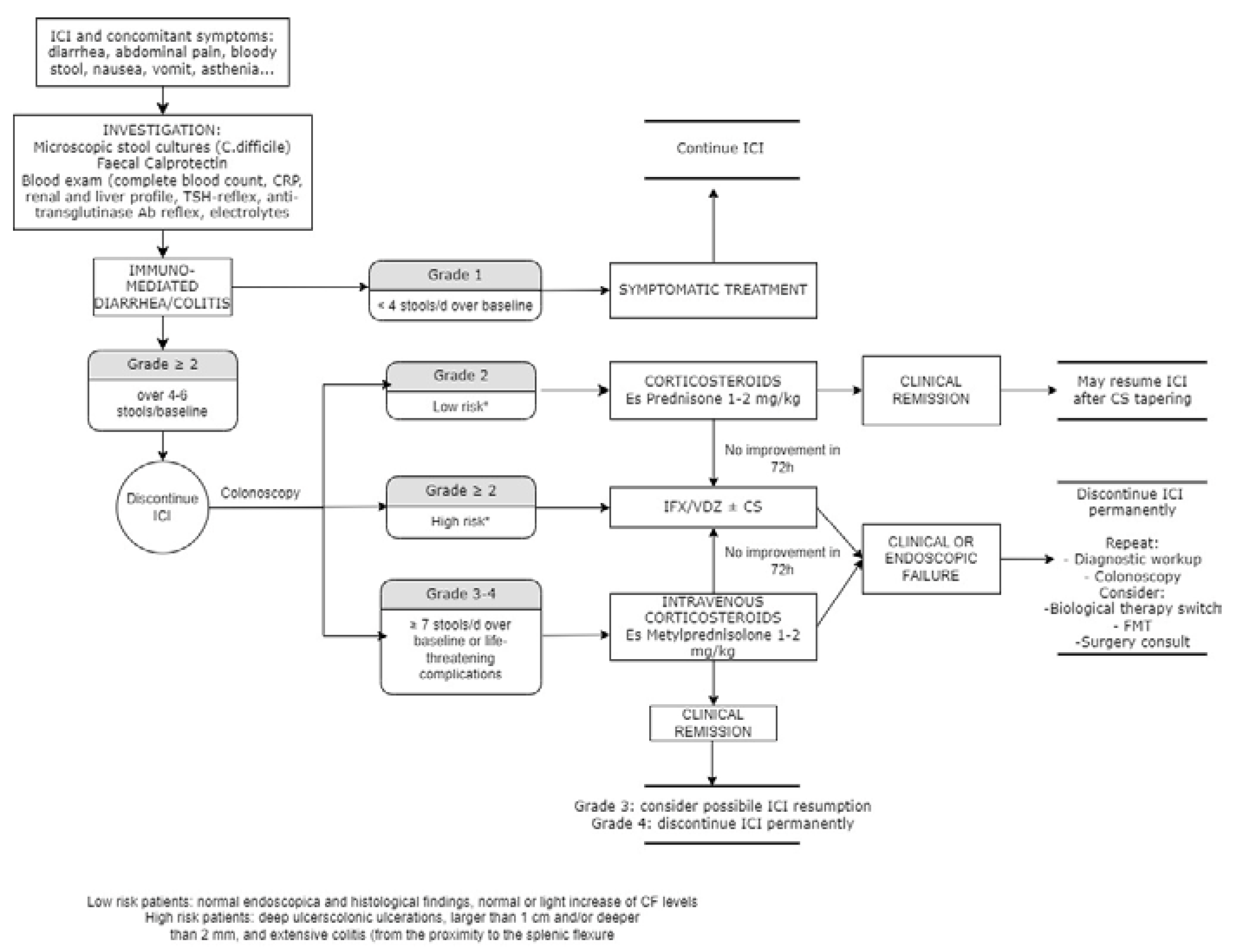
CIC management based on CTCAE grade. Adapted from AGA, ASCO and BSG guidelines [110,112,113].
Figure 3.
CIC management based on CTCAE grade. Adapted from AGA, ASCO and BSG guidelines [110,112,113].
5.1. Rechallenge of ICIs and risk of relapse
ICIs’ rechallenge and relapse risk are hot topics in the oncological field. To date, current guidelines consider safe to reintroduce ICI in case of diarrhoea/colitis grade 1, while irAEs grade 4 of any type is a strong contraindication to resumption [110,112,113]. A cohort study conducted by Doladille et al. observed that 25.2% of irAEs are associated with an ICI’s rechallenge. Moreover, the recurrence rate was higher after an anti-CTLA-4 monotherapy resumption (47.4%; 95% CI, 24.8%-69.9%) rather than after combination and anti-PD-1/PD-L1 monotherapy resumption, respectively 43.5% (95% CI, 29.1%57.8%) and 28.6% (95% CI, 24.0%-33.2%) [182].
Another cohort study focused on rechallenge with anti-PD-1/PD-L1, reporting a recurrence rate of 55%, but the second irAE was not more severe than the previous one. Most importantly, if the first irAE onset time was precocious, the risk of recurrence was noticeably higher [183]. In a recent meta-analyses and systematic review, Zhao et al. confirmed this last data and demonstrated a non-different disease control rate compared to initial ICI treatment; thus ICIs rechallenge shares similar efficacy and safety compared to initial therapy [184].
Regarding CIC, a retrospective study of 167 patients who experienced ICI resumption, 32% had recurrence. Anti-CTLA-4 rechallenge was associated with earlier and more frequent CIC recurrence compared to anti-PD-1/L1. No difference in severity was reported between the two groups. In addition, advanced stage cancer, immunosuppressive therapy, IFX or VDZ requirement, and higher grade and longer intercourse of first episode of colitis were associated with higher risk of recurrence [185].
A second endoscopic evaluation seems to have a role in patients who achieve remission, before resuming ICIs in order to confirm endoscopic and, possibly, histologic healing [130,131].
In conclusion, current clinical evidence does not discourage ICI rechallenge given the comparable risk of severity irAEs to the first treatment. Hence, ICI could be resumed after a critical evaluation on a patient basis, with particular caution to anti-CTLA-4 and high- risk factors.
5.2. ICIs treatment in IBD patients
ICIs safety in patients affected by autoimmune diseases, especially IBDs, is debated. Currently, there is a lack of clinical evidence, given the general exclusion of patients affected by IBD from ICIs’ clinical trials, assuming the presence of higher risks of developing GI toxicity. In addition, it is not clear if pre-existing GI disease’s activity and colonic involvement or pre-exposition to immunosuppressive therapy could represent ICI’s contraindications or identifying patients with higher risk to develop irAEs.
Abu Sbeih et al. reported that IBD patients own a 4-time higher risk of developing GI adverse events than patients without IBD. CIC seemed associated mostly to anti-CTLA-4 [186].
A subsequent meta-analysis involving 193 patients, reported IBD flares in the 39.8% (95% CI, 26.1–54.5) after a median time of 2-5 months, leading to ICIs discontinuation in the 35.4% (95% CI, 16.8–56.7). Combination therapy was associated with more frequent GI toxicity events [187]. Furthermore a retrospective study demonstrated a shorter time to-CIC in IBD patients, even if no worse overall survival (OS) was observed [188].
In support of these findings, a recent meta-analysis evaluating 1298 patients reported an overall incidence of IBD exacerbations after cancer treatment of 30%, with a significant increased risk of GI toxicity from ICIs (RR = 3.62). Also in this study, exacerbations were manageable in most of the cases [189].
Facing these data, on general expert consensus, the majority of patients with IBD on clinical remission could be treated with ICIs with the precautions of avoiding combination therapy and after a complete endoscopic and biomarkers evaluation of disease activity. Maintenance treatment in inactive IBD could be suspended or adapted according to the oncological progression risk, while the decision of pursuing IBD treatment in case of active disease and concomitant ICI treatment should be evaluated case-by-case by a multidisciplinary committee. Strict follow-up is mandatory in order to prompt intervention to ensure successful outcomes [190].
In conclusion, oncological and IBD patients require a personalized and multidisciplinary approach. Future studies able to assess specific oncological and toxicity risks, timing and type of immunosuppressive management are warranted.
6. Conclusions
CIC is one of the most frequent irAEs with different epidemiology according to the type of administered ICI and type of the underlying treated tumor [9,14]. CIC represents one of the leading cause of ICI discontinuation, requiring prompt recognition and treatment [22]. This novel disease is characterised by a complex and partially unclear pathogenesis, which includes multiple inflammatory pathways, molecules and the gut microbiome [44]. CIC lacks of pathognomonic features and standardized diagnostic criteria (histologic and endoscopic), therefore the diagnosis is generally based on the exclusion of other aetiologies. Early endoscopy seems to play an important prognostic role, selecting high risk patients with lower rate of steroid response [125]. A multidisciplinary approach between gastroenterologists and oncologists is fundamental to rapidly select patients with refractory/complicated CIC. Involved physicians’ shared management should carefully balance risks and benefits of introducing a biologic treatment and/or continuing ICI therapy [110,112,113].
Although CIC can have serious consequences, mortality is low [25]. Therefore, in our opinion the decision-making process should always place the oncological prognosis at the center of the therapeutic choice.
Author Contributions
MT and GM performed the research and wrote the manuscript. ADB, RG, EM, AQ, AR and AS critically reviewed the content of the paper. AA conceived the subject of the paper, contributed to the critical interpretation and supervised the project. All authors approved the final version of the manuscript.
Funding
this work received no external founding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable. No new data were created or analyzed in this study.
Conflicts of Interest
A Armuzzi has received consulting fees from: Abb-Vie, Allergan, Amgen, Arena, Biogen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, Lionhealth, MSD, Mylan, Nestlé, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, Takeda; speaker’s fees from: AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, MSD, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, Takeda, Tigenix; research support from: MSD, Takeda, Pfizer, Biogen. R Gabbiadini has received speaker’s fees from Pfizer. A Dal Buono has received speaker’s fees from Abb-vie. A Repici has received consulting fees from: Medtronic, Fujifilm. A. Santoro is an advisory board member: BMS, Servier, Gilead, Pfizer, Eisai, Bayer, MSD; has received consulting fees from: Arqule, Sanofi, Incyte; speaker’s bureau: Takeda, BMS, Roche, Abb-Vie, Amgen, Celgene, Servier, Gilead, Astrazeneca, Pfizer, Arqule, Lilly, Sandoz, Eisai, Novartis, Bayer, MSD. M Terrin, G Migliorisi, E Mastrorocco, A Quadarella declare no conflict of interests. The funders had no role in the writing of the manuscript.
References
- F. Bray, M. Laversanne, E. Weiderpass, and I. Soerjomataram. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer 2021, 127. [Google Scholar]
- Herbst Daniel Morgensztern & Chris Boshoff Roy, S. The biology and management of non-small cell lung cancer. Nature 2018.
- Y. Zhang and Z. Zhang. The history and advances in cancer immunotherapy: understanding the characteristics of tumor-infiltrating immune cells and their therapeutic implications. Cellular and Molecular Immunology 2020, 17. [Google Scholar]
- H. Raskov, A. Orhan, J. P. Christensen, and I. Gögenur. Cytotoxic CD8+ T cells in cancer and cancer immunotherapy. British Journal of Cancer 2021, 124, 359–367. [Google Scholar] [CrossRef]
- D. Hanahan and R. A. Weinberg. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar]
- H. Ledford. Melanoma drug wins US approval. Nature 2011, 471. [Google Scholar]
- F. S. Hodi et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- R. J. Motzer et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- S. Bagchi, R. S. Bagchi, R. Yuan, and E. G. Engleman. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. 2021.
- J. R. Brahmer et al. Society for immunotherapy of cancer (sitc) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J. Immunother. Cancer 2021, 9. [Google Scholar]
- M. Ramos-Casals et al. Immune-related adverse events of checkpoint inhibitors. Nature Reviews Disease Primers 2020, 6. [Google Scholar]
- A. N. Tran et al. Immune Checkpoint Inhibitor-associated Diarrhea and Colitis: A Systematic Review and Meta-analysis of Observational Studies.” 2021.
- N. C. Institute. Common Terminology Criteria for Adverse Events (CTCAE).” 2017.
- L. Khoja, D. Day, T. Wei-Wu Chen, L. L. Siu, and A. R. Hansen. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: A systematic review. Annals of Oncology 2017, 28. [Google Scholar]
- J. J. Wright, A. C. Powers, and D. B. Johnson. Endocrine toxicities of immune checkpoint inhibitors. Nature Reviews Endocrinology 2021, 17, 389–399. [Google Scholar] [CrossRef] [PubMed]
- P. Arnaud-Coffin et al. A systematic review of adverse events in randomized trials assessing immune checkpoint inhibitors. International Journal of Cancer 2019, 145, 639–648. [Google Scholar] [CrossRef]
- J. A. Seidel, A. Otsuka, and K. Kabashima. Anti-PD-1 and anti-CTLA-4 therapies in cancer: Mechanisms of action, efficacy, and limitations. Frontiers in Oncology 2018.
- A. Tarhini. Immune-Mediated Adverse Events Associated with Ipilimumab CTLA-4 Blockade Therapy: The Underlying Mechanisms and Clinical Management. Scientifica (Cairo). 2013, 2013, 1–19. [Google Scholar]
- J. S. Weber, K. C. Kähler, and A. Hauschild. Management of immune-related adverse events and kinetics of response with ipilimumab. Journal of Clinical Oncology 2012, 30, 2691–2697. [Google Scholar] [CrossRef] [PubMed]
- K. E. Beck et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J. Clin. Oncol. 2006, 24. [Google Scholar]
- H. Abu-Sbeih, F. S. Ali, and Y. Wang. Immune-checkpoint inhibitors induced diarrhea and colitis: A review of incidence, pathogenesis and management. Current Opinion in Gastroenterology 2020, 36, 25–32. [Google Scholar]
- L. Tang et al. Immune Checkpoint Inhibitor-Associated Colitis: From Mechanism to Management. Frontiers in Immunology 2021, 12. [Google Scholar]
- F. Martins et al. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nature Reviews Clinical Oncology 2019, 16. [Google Scholar]
- L. Marthey et al. Cancer immunotherapy with anti-CTLA-4 monoclonal antibodies induces an inflammatory bowel disease. J. Crohn’s Colitis 2016, 10. [Google Scholar]
- D. Y. Wang et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef]
- M. S. Hughes et al. Budesonide treatment for microscopic colitis from immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7. [Google Scholar]
- A. Haryal et al. Immune checkpoint inhibitor gastritis is often associated with concomitant enterocolitis, which impacts the clinical course. Cancer 2023, 129, 367–375. [Google Scholar]
- A. Som et al. Immune checkpoint inhibitor-induced colitis: A comprehensive review. World Journal of Clinical Cases 2019, 7. [Google Scholar]
- E. De Martin et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef]
- M. Porcu et al. Immune Checkpoint Inhibitor-Induced Pancreatic Injury: Imaging Findings and Literature Review. Targeted Oncology 2020, 15, 25–35. [Google Scholar] [CrossRef]
- R. Barroso-Sousa et al. Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens a systematic review and meta-analysis. JAMA Oncology 2018, 4. [Google Scholar]
- J. J. Koldenhof and K. P. M. Suijkerbuijk. Diarrhoea during checkpoint blockade, not always colitis. European Journal of Cancer 2017, 87. [Google Scholar]
- “Immunomodulators - Cancer Research Institute (CRI).”.
- L. Spain, S. Diem, and J. Larkin. Management of toxicities of immune checkpoint inhibitors. Cancer Treatment Reviews 2016, 44, 51–60. [Google Scholar]
- C. Li, P. Jiang, S. Wei, X. Xu, and J. Wang. Regulatory T cells in tumor microenvironment: New mechanisms, potential therapeutic strategies and future prospects. Molecular Cancer 2020, 19. [Google Scholar]
- D. Nagorsen, C. Scheibenbogen, F. M. Marincola, A. Letsch, and U. Keilholz. Natural T cell immunity against cancer. Clin. Cancer Res. 2003, 9, 4296–4303. [Google Scholar]
- O. S. Qureshi et al. Trans-endocytosis of CD80 and CD86: A molecular basis for the cell-extrinsic function of CTLA-4. Science 2011, 332. [Google Scholar]
- K. Wing et al. CTLA-4 control over Foxp3+ regulatory T cell function. Science 2008, 322. [Google Scholar]
- J. M. Moreau, M. Velegraki, C. Bolyard, M. D. Rosenblum, and Z. Li. Transforming growth factor-β1 in regulatory T cell biology. Science immunology 2022, 7. [Google Scholar]
- A. H. Sharpe and K. E. Pauken. The diverse functions of the PD1 inhibitory pathway. Nature Reviews Immunology 2018, 18. [Google Scholar]
- E. I. Buchbinder and A. Desai. CTLA-4 and PD-1 pathways similarities, differences, and implications of their inhibition. American Journal of Clinical Oncology: Cancer Clinical Trials 2016, 39. [Google Scholar]
- D. S. Thommen and T. N. Schumacher. T Cell Dysfunction in Cancer. Cancer Cell 2018, 33. [Google Scholar]
- C. H. June, J. T. Warshauer, and J. A. Bluestone. Is autoimmunity the Achilles’ heel of cancer immunotherapy? Nature Medicine 2017, 23. [Google Scholar]
- R. Poto et al. Holistic Approach to Immune Checkpoint Inhibitor-Related Adverse Events. Frontiers in Immunology 2022, 13. [Google Scholar]
- T. Passat, Y. Touchefeu, N. Gervois, A. Jarry, C. Bossard, and J. Bennouna. Physiopathological mechanisms of immune-related adverse events induced by anti-CTLA-4, anti-PD-1 and anti-PD-L1 antibodies in cancer treatment. Bulletin du Cancer 2018, 105. [Google Scholar]
- A. G. Solimando et al. Immune checkpoint inhibitor-related myositis: From biology to bedside. International Journal of Molecular Sciences 2020, 21. [Google Scholar]
- D. B. Johnson et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375. [Google Scholar]
- L. Flatz et al. Association of Checkpoint Inhibitor-Induced Toxic Effects with Shared Cancer and Tissue Antigens in Non-Small Cell Lung Cancer. JAMA Oncol. 2019, 5. [Google Scholar]
- K. C. Williams et al. Immune-related adverse events in checkpoint blockade: Observations from human tissue and therapeutic considerations. Frontiers in Immunology 2023, 14. [Google Scholar]
- A. M. Luoma et al. Molecular Pathways of Colon Inflammation Induced by Cancer Immunotherapy. Cell 2020, 182. [Google Scholar]
- T. N. A. I. E. S. S. K. K.Yoshino. Severe colitis after PD-1 blockade with nivolumab in advanced melanoma patients: Potential role of Th1-dominant immune response in immune-related adverse events: Two case reports. BMC Cancer 2019, 19. [Google Scholar]
- C. Coutzac et al. Colon immune-related adverse events: Anti-CTLA-4 and anti-PD-1 blockade induce distinct immunopathological entities. J. Crohn’s Colitis 2017, 11. [Google Scholar]
- K. Klocke, S. Sakaguchi, R. Holmdahl, and K. Wing. Induction of autoimmune disease by deletion of CTLA-4 in mice in adulthood. Proc. Natl. Acad. Sci. U. S. A. 2016, 113. [Google Scholar]
- E. A. Tivol, F. Borriello, A. N. Schweitzer, W. P. Lynch, J. A. Bluestone, and A. H. Sharpe. Loss of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity 1995, 3. [Google Scholar]
- G. Kim et al. Spontaneous Colitis Occurrence in Transgenic Mice with Altered B7-Mediated Costimulation. J. Immunol. 2008, 181. [Google Scholar]
- D. Tegtmeyer, M. Seidl, P. Gerner, U. Baumann, and C. Klemann. Inflammatory bowel disease caused by primary immunodeficiencies—Clinical presentations, review of literature, and proposal of a rational diagnostic algorithm. Pediatric Allergy and Immunology 2017, 28. [Google Scholar]
- C. Schwab et al. Phenotype, penetrance, and treatment of 133 cytotoxic T-lymphocyte antigen 4–insufficient subjects. J. Allergy Clin. Immunol. 2018, 142. [Google Scholar]
- K. Okla, D. L. Farber, and W. Zou. Tissue-resident memory T cells in tumor immunity and immunotherapy. Journal of Experimental Medicine 2021, 218. [Google Scholar]
- S. C. Sasson et al. Mucosal-associated invariant T (MAIT) cells are activated in the gastrointestinal tissue of patients with combination ipilimumab and nivolumab therapy-related colitis in a pathology distinct from ulcerative colitis. Clin. Exp. Immunol. 2020, 202. [Google Scholar]
- S. C. Sasson et al. Interferon-Gamma–Producing CD8+ Tissue Resident Memory T Cells Are a Targetable Hallmark of Immune Checkpoint Inhibitor–Colitis. Gastroenterology 2021, 161. [Google Scholar]
- Y. Takahashi et al. CD8+ Lymphocyte Infiltration Is a Specific Feature of Colitis Induced by Immune Checkpoint Inhibitors. Dig. Dis. Sci. 2023, 68. [Google Scholar]
- A. Sharma et al. Anti-CTLA-4 immunotherapy does not deplete Foxp3 þ regulatory T cells (Tregs) in human cancers. Clin. Cancer Res. 2019, 25. [Google Scholar]
- M. Iglesias-Escudero, N. Arias-González, and E. Martínez-Cáceres. Regulatory cells and the effect of cancer immunotherapy. Molecular Cancer 2023, 22. [Google Scholar]
- F. R. Mariotti, L. Quatrini, E. Munari, P. Vacca, and L. Moretta. Innate lymphoid cells: Expression of PD-1 and other checkpoints in normal and pathological conditions. Frontiers in Immunology 2019, 10. [Google Scholar]
- R. G. Domingues and M. R. Hepworth. Immunoregulatory Sensory Circuits in Group 3 Innate Lymphoid Cell (ILC3) Function and Tissue Homeostasis. Frontiers in Immunology 2020, 11. [Google Scholar]
- N. Ghosh, K. K. Chan, B. Jivanelli, and A. R. Bass. Autoantibodies in Patients with Immune-Related Adverse Events from Checkpoint Inhibitors: A Systematic Literature Review. Journal of Clinical Rheumatology 2022, 28. [Google Scholar]
- I. Les et al. Association of immune-related adverse events induced by nivolumab with a battery of autoantibodies. Ann. Med. 2021, 53. [Google Scholar]
- S. Iwama, A. De Remigis, M. K. Callahan, S. F. Slovin, J. D. Wolchok, and P. Caturegli. Pituitary expression of CTLA-4 mediates hypophysitis secondary to administration of CTLA-4 blocking antibody. Sci. Transl. Med. 2014, 6. [Google Scholar]
- J. H. Kang, J. A. Bluestone, and A. Young. Predicting and Preventing Immune Checkpoint Inhibitor Toxicity: Targeting Cytokines. Trends in Immunology 2021, 42. [Google Scholar]
- A. Ceschi, R. Noseda, K. Palin, and K. Verhamme. Immune Checkpoint Inhibitor-Related Cytokine Release Syndrome: Analysis of WHO Global Pharmacovigilance Database. Front. Pharmacol. 2020, 11. [Google Scholar]
- G. Bamias et al. Immunological Characteristics of Colitis Associated with Anti-CTLA-4 Antibody Therapy. Cancer Invest. 2017, 35. [Google Scholar]
- A. A. Tarhini et al. Baseline circulating IL-17 predicts toxicity while TGF-β1 and IL-10 are prognostic of relapse in ipilimumab neoadjuvant therapy of melanoma. J. Immunother. cancer 2015, 3, 39. [Google Scholar]
- K. Tyan et al. Cytokine changes during immune-related adverse events and corticosteroid treatment in melanoma patients receiving immune checkpoint inhibitors. Cancer Immunol. Immunother. 2021, 70. [Google Scholar]
- J. Lo et al. P001 Immune checkpoint inhibitor-induced colitis is mediated by polyfunctional lymphocytes and is dependent on the IL23/IFNg axis. J. Crohn’s Colitis 2022, 16. [Google Scholar]
- Y. Zhou et al. Intestinal toxicity to CTLA-4 blockade driven by IL-6 and myeloid infiltration. J. Exp. Med. 2023, 220. [Google Scholar]
- S. Khan et al. Immune dysregulation in cancer patients developing immune-related adverse events. Br. J. Cancer 2019, 120. [Google Scholar]
- R. Tokunaga et al. CXCL9, CXCL10, CXCL11/CXCR3 axis for immune activation – A target for novel cancer therapy. Cancer Treatment Reviews 2018, 63. [Google Scholar]
- M. F. Neurath. Targeting immune cell circuits and trafficking in inflammatory bowel disease. Nature Immunology 2019, 20. [Google Scholar]
- K. P. Shah et al. Demographic factors associated with toxicity in patients treated with anti-programmed cell death-1 therapy. Cancer Immunol. Res. 2020, 8. [Google Scholar]
- K. Tyan et al. Association of vitamin D intake with decreased risk of immune checkpoint inhibitor-induced colitis. J. Clin. Oncol. 2020, 38. [Google Scholar]
- H. K. Akturk, D. Kahramangil, A. Sarwal, L. Hoffecker, M. H. Murad, and A. W. Michels. Immune checkpoint inhibitor-induced Type 1 diabetes: a systematic review and meta-analysis. Diabetic Medicine 2019, 36. [Google Scholar]
- J. Luo et al. Immunotherapy-Mediated Thyroid Dysfunction: Genetic Risk and Impact on Outcomes with PD-1 Blockade in Non–Small Cell Lung Cancer. Clin. Cancer Res. 2021, 27. [Google Scholar]
- C. Campbell, M. R. Kandalgaonkar, R. M. Golonka, B. S. Yeoh, M. Vijay-Kumar, and P. Saha. Crosstalk between Gut Microbiota and Host Immunity: Impact on Inflammation and Immunotherapy. Biomedicines 2023, 11. [Google Scholar]
- W. Li, Y. Deng, Q. Chu, and P. Zhang. Gut microbiome and cancer immunotherapy. Cancer Letters 2019, 447. [Google Scholar]
- N. Chaput et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann. Oncol. 2017, 28. [Google Scholar]
- K. Dubin et al. Intestinal microbiome analyses identify melanoma patients at risk for checkpoint-blockade-induced colitis. Nat. Commun. 2016, 7. [Google Scholar]
- O. Oey, Y.-Y. Liu, A. F. Sunjaya, D. M. Simadibrata, M. A. Khattak, and E. Gray. Gut microbiota diversity and composition in predicting immunotherapy response and immunotherapy-related colitis in melanoma patients: A systematic review. World J. Clin. Oncol. 2022, 13. [Google Scholar]
- T. Sakurai et al. Integrative analysis of gut microbiome and host transcriptomes reveals associations between treatment outcomes and immunotherapy-induced colitis. Mol. Oncol. 2022, 16. [Google Scholar]
- M. Yuksel et al. A novel ‘humanized mouse’ model for autoimmune hepatitis and the association of gut microbiota with liver inflammation. Hepatology 2015, 62. [Google Scholar]
- M. Saresella et al. Immunological and clinical effect of diet modulation of the gut microbiome in multiple sclerosis patients: A pilot study. Front. Immunol. 2017, 8. [Google Scholar]
- X. Liu et al. Role of the Gut Microbiome in Modulating Arthritis Progression in Mice. Sci. Rep. 2016, 6. [Google Scholar]
- T. Wang et al. Probiotics Lactobacillus reuteri Abrogates Immune Checkpoint Blockade-Associated Colitis by Inhibiting Group 3 Innate Lymphoid Cells. Front. Immunol. 2019, 10. [Google Scholar]
- Q. Mu, V. J. Tavella, and X. M. Luo. Role of Lactobacillus reuteri in human health and diseases. Frontiers in Microbiology 2018, 9. [Google Scholar]
- M. Vétizou et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 2015, 350. [Google Scholar]
- S. Dasgupta, D. Erturk-Hasdemir, J. Ochoa-Reparaz, H. C. Reinecker, and D. L. Kasper. Plasmacytoid dendritic cells mediate anti-inflammatory responses to a gut commensal molecule via both innate and adaptive mechanisms. Cell Host Microbe 2014, 15. [Google Scholar]
- A. Sivan et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350. [Google Scholar]
- F. Wang, Q. Yin, L. Chen, and M. M. Davis. Bifidobacterium can mitigate intestinal immunopathology in the context of CTLA-4 blockade. Proc. Natl. Acad. Sci. U. S. A. 2018, 115. [Google Scholar]
- B. Routy, V. Gopalakrishnan, R. Daillère, L. Zitvogel, J. A. Wargo, and G. Kroemer. The gut microbiota influences anticancer immunosurveillance and general health. Nature Reviews Clinical Oncology 2018, 15. [Google Scholar]
- N. Arpaia et al. Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature 2013, 504. [Google Scholar]
- H. R. Wardill, R. J. Chan, A. Chan, D. Keefe, S. P. Costello, and N. H. Hart. Dual contribution of the gut microbiome to immunotherapy efficacy and toxicity: supportive care implications and recommendations. Supportive Care in Cancer 2022, 30. [Google Scholar]
- A. Shirwaikar Thomas, S. Hanauer, and Y. Wang. Immune Checkpoint Inhibitor Enterocolitis vs Idiopathic Inflammatory Bowel Disease. Clinical Gastroenterology and Hepatology 2023.
- M. Y. Song et al. Protective effects of Fc-fused PD-L1 on two different animal models of colitis. Gut 2015, 64. [Google Scholar]
- J. Robertson et al. Intestinal APCs of the endogenous nanomineral pathway fail to express PD-L1 in Crohn’s disease. Sci. Rep. 2016, 6. [Google Scholar]
- M. Zhang et al. Association of CTLA-4 variants with susceptibility to inflammatory bowel disease: A meta-analysis. Human Immunology 2014, 75. [Google Scholar]
- B. L. Adler et al. Histopathological and immunophenotypic features of ipilimumab-associated colitis compared to ulcerative colitis. J. Intern. Med. 2018, 283. [Google Scholar]
- X. C. Morgan et al. Dysfunction of the intestinal microbiome in inflammatory bowel disease and treatment. Genome Biol. 2012, 13. [Google Scholar]
- A. Swidsinski, J. Weber, V. Loening-Baucke, L. P. Hale, and H. Lochs. Spatial organization and composition of the mucosal flora in patients with inflammatory bowel disease. J. Clin. Microbiol. 2005, 43. [Google Scholar]
- D. Knights et al. Complex host genetics influence the microbiome in inflammatory bowel disease. Genome Med. 2014, 6. [Google Scholar]
- H. Li, Z. Y. Fu, M. E. Arslan, H. Lee, and D. Cho. Differential diagnosis and management of immune checkpoint inhibitor-induced colitis: A comprehensive review. World Journal of Experimental Medicine 2021, 11. [Google Scholar]
- M. Dougan, Y. Wang, A. Rubio-Tapia, and J. K. Lim. AGA Clinical Practice Update on Diagnosis and Management of Immune Checkpoint Inhibitor Colitis and Hepatitis: Expert Review. Gastroenterology 2021, 160. [Google Scholar]
- M. H. Geukes Foppen et al. Immune checkpoint inhibition-related colitis: Symptoms, endoscopic features, histology and response to management. ESMO Open 2018, 3. [Google Scholar]
- B. J. Schneider et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. Journal of Clinical Oncology 2021, 39. [Google Scholar]
- N. Powell et al. British Society of Gastroenterology endorsed guidance for the management of immune checkpoint inhibitor-induced enterocolitis. Lancet Gastroenterol. Hepatol. 2020, 5, 679–697. [Google Scholar] [CrossRef]
- J. Ni, X. Zhang, and L. Zhang. Opportunistic bowel infection after corticosteroid dosage tapering in a stage IV lung cancer patient with tislelizumab-related colitis. Thorac. Cancer 2020, 11. [Google Scholar]
- C. Zhou, Y. Klionsky, M. E. Treasure, and D. S. Bruno. Pembrolizumab-Induced Immune-Mediated Colitis in a Patient with Concurrent Clostridium Difficile Infection. Case Rep. Oncol. 2019, 12. [Google Scholar]
- C. Vuillamy et al. Clostridium difficile infection and immune checkpoint inhibitor–induced colitis in melanoma: 18 cases and a review of the literature. Melanoma Res. 2023, 33, 192–198. [Google Scholar]
- A. Hoadley, N. Sandanayake, and G. V. Long. Atrophic exocrine pancreatic insufficiency associated with anti-PD1 therapy. Annals of Oncology 2017, 28. [Google Scholar]
- Y. R. Badran et al. Immune checkpoint inhibitor-associated celiac disease. J. Immunother. Cancer 2020, 8. [Google Scholar]
- A. R. Abolhassani, G. Schuler, M. C. Kirchberger, and L. Heinzerling. C-reactive protein as an early marker of immune-related adverse events. J. Cancer Res. Clin. Oncol. 2019, 145. [Google Scholar]
- Y. Fujisawa et al. Fluctuations in routine blood count might signal severe immune-related adverse events in melanoma patients treated with nivolumab. J. Dermatol. Sci. 2017, 88. [Google Scholar]
- Y. Nakamura et al. Correlation between blood cell count and outcome of melanoma patients treated with anti-PD-1 antibodies. Jpn. J. Clin. Oncol. 2019, 49. [Google Scholar]
- G. Manson, J. Norwood, A. Marabelle, H. Kohrt, and R. Houot. Biomarkers associated with checkpoint inhibitors. Ann. Oncol. 2016, 27. [Google Scholar]
- K. Schindler et al. Correlation of absolute and relative eosinophil counts with immune-related adverse events in melanoma patients treated with ipilimumab. J. Clin. Oncol. 2014, 32. [Google Scholar]
- S. Meshkibaf, A. J. Martins, G. T. Henry, and S. O. Kim. Protective role of G-CSF in dextran sulfate sodium-induced acute colitis through generating gut-homing macrophages. Cytokine 2016, 78, 69–78. [Google Scholar] [CrossRef]
- H. Abu-Sbeih, F. S. Ali, W. Luo, W. Qiao, G. S. Raju, and Y. Wang. Importance of endoscopic and histological evaluation in the management of immune checkpoint inhibitor-induced colitis. J. Immunother. Cancer 2018, 6. [Google Scholar]
- F. Zou et al. Fecal calprotectin concentration to assess endoscopic and histologic remission in patients with cancer with immune-mediated diarrhea and colitis. J. Immunother. Cancer 2021, 9. [Google Scholar]
- Y. Wang et al. Endoscopic and Histologic Features of Immune Checkpoint Inhibitor-Related Colitis. Inflamm. Bowel Dis. 2018, 24. [Google Scholar]
- A. P. Wright, M. S. Piper, S. Bishu, and R. W. Stidham. Systematic review and case series: flexible sigmoidoscopy identifies most cases of checkpoint inhibitor-induced colitis. Alimentary Pharmacology and Therapeutics 2019, 49. [Google Scholar]
- J. D. Herlihy et al. Flexible Sigmoidoscopy Rather than Colonoscopy Is Adequate for the Diagnosis of Ipilimumab-Associated Colitis. South. Med. J. 2019, 112. [Google Scholar]
- C. Ma et al. Recommendations for standardizing biopsy acquisition and histological assessment of immune checkpoint inhibitor-associated colitis. J. Immunother. Cancer 2022, 10. [Google Scholar]
- V. Desmedt et al. Position statement on the management of the immune checkpoint inhibitor-induced colitis via multidisciplinary modified Delphi consensus. Eur. J. Cancer 2023, 187, 36–57. [Google Scholar] [CrossRef]
- J. A. Thompson et al. Management of immunotherapy-related toxicities, version 1.2020 featured updates to the NCCN guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2020, 18. [Google Scholar]
- K. Kubo, M. Kato, and K. Mabe. Nivolumab-Associated Colitis Mimicking Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2017, 15. [Google Scholar]
- E. Bellaguarda and S. Hanauer. Checkpoint Inhibitor–Induced Colitis. Am. J. Gastroenterol. 2020, 115, 202–210. [Google Scholar] [CrossRef]
- L. Spain et al. Patterns of steroid use in diarrhoea and/or colitis (D/C) from immune checkpoint inhibitors (ICPI). Ann. Oncol. 2016, 27. [Google Scholar]
- K. Choi et al. Can Immune Checkpoint Inhibitors Induce Microscopic Colitis or a Brand New Entity? Inflamm. Bowel Dis. 2019, 25. [Google Scholar]
- B. Baroudjian et al. Anti-PD1-induced collagenous colitis in a melanoma patient. Melanoma Res. 2016, 26. [Google Scholar]
- M. J. Mooradian et al. Mucosal inflammation predicts response to systemic steroids in immune checkpoint inhibitor colitis. J. Immunother. Cancer 2020, 8. [Google Scholar]
- P. A. Patil and X. Zhang. Pathologic manifestations of gastrointestinal and hepatobiliary injury in immune checkpoint inhibitor therapy. Arch. Pathol. Lab. Med. 2021, 145. [Google Scholar]
- M. L. Zhang, A. Neyaz, D. Patil, J. Chen, M. Dougan, and V. Deshpande. Immune-related adverse events in the gastrointestinal tract: diagnostic utility of upper gastrointestinal biopsies. Histopathology 2020, 76. [Google Scholar]
- U. N. Shivaji et al. Immune checkpoint inhibitor-associated gastrointestinal and hepatic adverse events and their management. Therapeutic Advances in Gastroenterology 2019, 12. [Google Scholar]
- D. M. Karamchandani and R. Chetty. Immune checkpoint inhibitor-induced gastrointestinal and hepatic injury: Pathologists’ perspective. J. Clin. Pathol. 2018, 71. [Google Scholar]
- S. Sakellariou, D. N. Zouki, D. C. Ziogas, D. Pouloudi, H. Gogas, and I. Delladetsima. Granulomatous colitis in a patient with metastatic melanoma under immunotherapy: a case report and literature review. BMC Gastroenterol. 2021, 21. [Google Scholar]
- J. H. Chen, M. K. Pezhouh, G. Y. Lauwers, and R. Masia. Histopathologic features of colitis due to immunotherapy With Anti-PD-1 antibodies. Am. J. Surg. Pathol. 2017, 41. [Google Scholar]
- P. Bavi, M. Butler, S. Serra, and R. Chetty. Immune modulator-induced changes in the gastrointestinal tract. Histopathology 2017, 71. [Google Scholar]
- R. A. Isidro et al. Medication-specific variations in morphological patterns of injury in immune check-point inhibitor-associated colitis. Histopathology 2021, 78. [Google Scholar]
- A. García-Varona, R. D. Odze, and F. Makrauer. Lymphocytic colitis secondary to ipilimumab treatment. Inflammatory Bowel Diseases 2013, 19. [Google Scholar]
- P. E. S. Romain, A. K. S. Salama, N. Lynn Ferguson, and R. A. Burbridge. Ipilimumab-Associated lymphocytic colitis: A case report. Transl. Gastroenterol. Hepatol. 2016, 5. [Google Scholar]
- A. Gallo et al. Collagenous colitis and atezolizumab therapy: an atypical case. Clin. J. Gastroenterol. 2021, 14. [Google Scholar]
- R. S. Gonzalez, S. N. Salaria, C. D. Bohannon, A. R. Huber, M. M. Feely, and C. Shi. PD-1 inhibitor gastroenterocolitis: case series and appraisal of ‘immunomodulatory gastroenterocolitis. Histopathology 2017, 70. [Google Scholar]
- R. Del Sordo, V. Lougaris, G. Bassotti, A. Armuzzi, and V. Villanacci. Therapeutic agents affecting the immune system and drug-induced inflammatory bowel disease (IBD): A review on etiological and pathogenetic aspects. Clin. Immunol. 2022, 234, 108916. [Google Scholar] [CrossRef]
- V. Villanacci et al. Histopathology of IBD colitis. A practical approach from the pathologists of the Italian group for the study of the gastrointestinal tract (GIPAD). Pathologica 2021, 113. [Google Scholar]
- R. Yamauchi et al. The characteristics of nivolumab-induced colitis: An evaluation of three cases and a literature review. BMC Gastroenterol. 2018, 18. [Google Scholar]
- R. Celli, H. M. Kluger, and X. Zhang. Anti-PD-1 Therapy-Associated Perforating Colitis. Case Rep. Gastrointest. Med. 2018, 2018. [Google Scholar]
- V. T. F. Cheung et al. Immune checkpoint inhibitor-related colitis assessment and prognosis: can IBD scoring point the way? Br. J. Cancer 2020, 123. [Google Scholar]
- B. Gosangi et al. Imaging features of toxicities associated with immune checkpoint inhibitors. Eur. J. Radiol. Open 2022, 9. [Google Scholar]
- A. R. Barina, M. R. Bashir, B. A. Howard, B. A. Hanks, A. K. Salama, and T. A. Jaffe. Isolated recto-sigmoid colitis: a new imaging pattern of ipilimumab-associated colitis. Abdom. Radiol. 2016, 41. [Google Scholar]
- M. Garcia-Neuer et al. Diagnostic comparison of CT scans and colonoscopy for immune-related colitis in ipilimumab-treated advanced melanoma patients. Cancer Immunol. Res. 2017, 5. [Google Scholar]
- A. C. Shieh et al. Imaging and clinical manifestations of immune checkpoint inhibitor-related colitis in cancer patients treated with monotherapy or combination therapy. Abdom. Radiol. 2020, 45. [Google Scholar]
- S. M. Durbin et al. Diagnostic utility of CT for suspected immune checkpoint inhibitor enterocolitis. J. Immunother. cancer 2020, 8. [Google Scholar]
- N. Pisuchpen et al. Multi-detector computed tomography (MDCT)–based severity score as a prognostic tool in patients with suspected immune checkpoint inhibitor therapy associated colitis. Eur. Radiol. 2021, 31. [Google Scholar]
- M. H. G. Foppen et al. Immune checkpoint inhibition-related colitis: Symptoms, endoscopic features, histology and response to management. ESMO Open 2018, 3. [Google Scholar]
- Z. Gong and Y. Wang. Immune Checkpoint Inhibitor-Mediated Diarrhea and Colitis: A Clinical Review.” 2020.
- J. Weber et al. A randomized, double-blind, placebo-controlled, phase II study comparing the tolerability and efficacy of ipilimumab administered with or without prophylactic budesonide in patients with unresectable stage III or IV melanoma. Clin. Cancer Res. 2009, 15, 5591–5598. [Google Scholar]
- H. Abu-Sbeih et al. Impact of antibiotic therapy on the development and response to treatment of immune checkpoint inhibitor-mediated diarrhea and colitis. J. Immunother. Cancer 2019, 7. [Google Scholar]
- J. L. Alexander et al. Oral beclomethasone dipropionate is an effective treatment for immune checkpoint inhibitor induced colitis. J. Immunother. Cancer 2022, 10. [Google Scholar]
- J. Burla et al. Retrospective Analysis of Treatment and Complications of Immune Checkpoint Inhibitor-Associated Colitis: Histological Ulcerations as Potential Predictor for a Steroid-Refractory Disease Course. Inflamm. Intest. Dis. 2020, 5. [Google Scholar]
- M. Ding et al. Treatment and outcomes of immune checkpoint inhibitors-associated colitis/diarrhea: A systematic review and meta-analysis. Digestive and Liver Disease. Elsevier B.V., 2023.
- H. Abu-Sbeih et al. Early introduction of selective immunosuppressive therapy associated with favorable clinical outcomes in patients with immune checkpoint inhibitor-induced colitis. J. Immunother. Cancer 2019, 7. [Google Scholar]
- H. Abu-Sbeih and Y. Wang. Management Considerations for Immune Checkpoint Inhibitor-Induced Enterocolitis Based on Management of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2020, 26, 662–668. [Google Scholar] [CrossRef] [PubMed]
- D. H. Johnson et al. Infliximab associated with faster symptom resolution compared with corticosteroids alone for the management of immune-related enterocolitis. J. Immunother. Cancer 2018, 6. [Google Scholar]
- Y. Wang et al. Immune-checkpoint inhibitor-induced diarrhea and colitis in patients with advanced malignancies: Retrospective review at MD Anderson. J. Immunother. Cancer 2018, 6. [Google Scholar]
- S. T. van Turenhout et al. Cytomegalovirus in Steroid-Refractory Immune Checkpoint Inhibition–Related Colitis. Journal of Thoracic Oncology 2020, 15, e15–e20. [Google Scholar] [CrossRef]
- H. Abu-Sbeih et al. Outcomes of vedolizumab therapy in patients with immune checkpoint inhibitor-induced colitis: A multi-center study. J. Immunother. Cancer 2018, 6. [Google Scholar]
- F. Zou et al. Efficacy and safety of vedolizumab and infliximab treatment for immune-mediated diarrhea and colitis in patients with cancer: A two-center observational study. J. Immunother. Cancer 2021, 9. [Google Scholar]
- E. Zhang, C. Kiely, N. Sandanayake, and S. Tattersall. Calcineurin inhibitors in steroid and anti-TNF-alpha refractory immune checkpoint inhibitor colitis. JGH Open 2021, 5, 558–562. [Google Scholar] [CrossRef]
- A. S. Thomas, W. Ma, and Y. Wang. Ustekinumab for Refractory Colitis Associated with Immune Checkpoint Inhibitors. N. Engl. J. Med. 2021, 384, 581–583. [Google Scholar] [CrossRef] [PubMed]
- R. B. Holmstroem et al. Tofacitinib and faecal microbiota transplantation in treating checkpoint inhibitor-induced enterocolitis: case report. BMJ Open Gastroenterol. 2022, 9, e000989. [Google Scholar] [CrossRef] [PubMed]
- M. Chen et al. Fecal Microbiota Transplantation Effectively Cures a Patient With Severe Bleeding Immune Checkpoint Inhibitor-Associated Colitis and a Short Review. Frontiers in Oncology 2022, 12. [Google Scholar]
- Y. Wang et al. Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis. Nat. Med. 2018, 24, 1804–1808. [Google Scholar] [CrossRef] [PubMed]
- T. K. T. T. T. N. Keiichi Mitsuyama Ryosuke Yamauchi. Characteristic of Immune Checkpoint Inhibitor-Induced Colitis: A Systematic review. Kurume Med. Jounal 2021.
- C. Dolladille et al. Immune Checkpoint Inhibitor Rechallenge after Immune-Related Adverse Events in Patients with Cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef]
- A. Simonaggio et al. Evaluation of Readministration of Immune Checkpoint Inhibitors after Immune-Related Adverse Events in Patients with Cancer. JAMA Oncol. 2019, 5, 1310–1317. [Google Scholar] [CrossRef]
- Q. Zhao et al. Safety and Efficacy of the Rechallenge of Immune Checkpoint Inhibitors After Immune-Related Adverse Events in Patients With Cancer: A Systemic Review and Meta-Analysis. Frontiers in Immunology 2021, 12.
- H. Abu-Sbeih et al. Resumption of Immune Checkpoint Inhibitor Therapy After Immune-Mediated Colitis. J Clin Oncol 2019, 37, 2738–2745. [Google Scholar] [CrossRef]
- H. Abu-Sbeih et al. Immune Checkpoint Inhibitor Therapy in Patients With Preexisting Inflammatory Bowel Disease. J Clin Oncol 2019, 38, 576–583. [Google Scholar]
- J. Meserve, A. Facciorusso, A. K. Holmer, V. Annese, W. J. Sandborn, and S. Singh. Systematic review with meta-analysis: safety and tolerability of immune checkpoint inhibitors in patients with pre-existing inflammatory bowel diseases. Alimentary Pharmacology and Therapeutics 2021, 53, 374–382. [Google Scholar] [CrossRef] [PubMed]
- J. Sleiman, W. Wei, R. Shah, M. S. Faisal, J. Philpott, and P. Funchain. Incidence of immune checkpoint inhibitor-mediated diarrhea and colitis (imDC) in patients with cancer and preexisting inflammatory bowel disease: A propensity score-matched retrospective study. J. Immunother. Cancer 2021, 9. [Google Scholar]
- S. Grimsdottir, M. Attauabi, E. Kristine Dahl, J. Burisch, and J. B. Seidelin. Systematic Review with Meta-analysis: The Impact of Cancer Treatments on the Disease Activity of Inflammatory Bowel Diseases. J. Crohn’s Colitis 2023.
- A. Amiot et al. Management of immune checkpoint inhibitor in patients with cancer and pre-existing inflammatory bowel disease: Recommendations from the GETAID. Digestive and Liver Disease 2022, 54. [Google Scholar]

Table 1.
Indications and common immune related adverse events of immune checkpoint inhibitors.
| Immune checkpoint inhibitor | Target | Date of Approval (year) | Indications (by FDA/EMA) [33] | Immune-related Adverse events [16,34] | Colitis [12,16,34] |
|---|---|---|---|---|---|
| Ipilimumab | CTLA-4 | 2010 | In combination with nivolumab: Previously treated MSI-H/dMMR Metastatic CRC, HCC, intermediate and poo-risk advanced RCC, malignant pleural mesothelioma, Mycosis fungoides, Sezary Syndrome, NSCLC Alone: late-stage melanoma |
Diarrhea 36% (31-41) Rash 23% Hepatitis 5% Hyperthiroidism 4% Hypophisitis 4% Hypothiroidism 3% Pneumonitis 1% |
All grade: 8% (6-10) Grade 3-4: 5% (4-6) |
| Nivolumab | PD-1 | 2015 | In combination with ipilimumab: late-stage melanoma, NSCLC, RCC, CRC, malignant pleural mesothelioma, HCC Alone: late-stage melanoma, NSCLC, RCC, HNCC, Classic Hodgkin Lymphoma, Esophageal Cancer, gastroesophageal cancer, urothelial carcinoma |
Diarrhea 11% Rash 10% Hypothyroidism 8% Hepatitis 5% Hyperthyroidism 5% Pneumonitis 4% Hypohysitis 1% |
All grade: 1% Grade 3-4: 1% |
| Pembrolizumab | PD-1 | 2016 | Late-stage melanoma, NSCLC, CRC, HCC, RCC, HNCC, Cervical Cancer, endometrial cancer, Classic Hodgkin lymphoma, large B-cell lymphoma, Esophageal Cancer, Gastric cancer, urothelial carcinoma, MSI-H/dMMR/TMB-H cancers, CSCC, Merkel Cell Carcinoma, BC | ||
| Cemiplimab | PD-1 | 2018 | CSCC, BCC, NSCLC | ||
| Atezolizumab | PD-L1 | 2016 | Melanoma, NSCLC, SCLC, HCC, Urothelial carcinoma, BC | ||
| Durvalumab | PD-L1 | 2016 | HCC, biliary tract, NSCLC, SCLC, urothelial carcinoma | ||
| Avelumab | PD-L1 | 2017 | RCC, Urothelial carcinoma, Merkel Cell carcinoma |
BC-Breast Cancer, BCC-Basal Cell Carcinoma, CRC-Colon Rectal Cancer, CSCC- Cutaneous squamous Cell Carcinoma, HCC-Hepatocellular Carcinoma, HNSCC-Head and Neck carcinoma, MSI-H/dMMR/TMB-H-microsatellite instability-high/mismatch deficient repair, tumor mutational burden-high, NSCLC- Non small cell Lung cancer, RCC-Renal cell carcinoma, SCLC- Small cell lung cancer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



