
Submitted:
20 May 2023
Posted:
26 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Globally 703 000 people commit suicide (4th leading cause of mortality among 15-29 year-olds, 1.4% of all deaths globally) every year, which have a negative effect on families, colleagues, and societies. India accounts for 36.6 percent of global suicide in women and 24.3 percent among men, while having only 17.8 percent of the global population, also remarkable fact is that the suicide ratio for female is 14.7 per 100,000 compared to 21.2 per 100,000 of male which is 2.1 times the global average in female, while 1.4 times higher for men. COVID-19 (coronavirus disease-2019) pandemic has certainly affected the physical, mental, economical and social well being of global population directly or indirectly in different ways. Deteriorating physical, mental, economical and social health of an individual could increase the suicidal tendency, leading to accidents and suicide. This study tried to find out the COVID-19 pandemic situation impact on accidental death as well as suicide rates in India. The study period is from 1st January 1967 to 31st December 2021, to assess the effect of the COVID-19 pandemic situation on suicide and accidental death rates. This study revealed that the suicide deaths percentage among males increased significantly in comparison to females in COVID-19 era and actual count and incidence also increased. This study revealed that the mean accidental death and suicide both increased during COVID period of study as compared to pre-pandemic whole period from 1967 by 25.47 % and 30.61% respectively. Alternatively we can say that the accidental death and suicides increased significantly in India, which is largely preventable.
Keywords:
COVID-19
; suicide
; accident
; pandemic
; impact
1. Background:
Globally 703 000 people commit suicide (4th leading cause of mortality among 15-29 year-olds, 1.4% of all deaths globally) every year, which have a negative effect on families, colleagues, and societies [1]. LMICs (low- and middle-income countries) account for 77% of global suicides most commonly by ingestion of pesticide (20% of global suicides) in rural agricultural areas in low- and middle-income countries; hanging and firearms [2]. Suicide is serious public health issue in India which can be prevented by low-cost interventions [3]. In 2016 the suicidal death rate in India per lakh population was 16.5, whereas the global average in 2016 was 10.5 per 100 000 [4]. India accounts for 36.6 percent of global suicide in women and 24.3 percent among men, while having only 17.8 percent of the global population, also remarkable fact is that the suicide ratio for female is 14.7 per 100,000 compared to 21.2 per 100,000 of male which is 2.1 times the global average in female, while 1.4 times higher for men [5].
COVID-19 (coronavirus disease-2019) pandemic has certainly affected the physical, mental, economical and social well being of global population directly or indirectly in different ways [6]. The COVID-19 distress is no more a PHEIC (public health emergency of international concern) as declared by WHO (World Health Organization) International Health Regulations (2005) (IHR) Emergency Committee 15th meeting, held on Thursday 4 May 2023 [7]. The global researcher community is yet calculating and analyzing the devastating impact of this pandemic on various aspect of life. Undoubtedly the situations have provoked mental health issues globally. Numerous factors originating due to the pandemic situation like fear, anxiety, reduced access-utilization of routine health services, forced social distancing, lockdowns, loss of job, hiked treatment costs, social boycott of infected individuals, an increase of domestic violence could deteriorate the physical, mental, economical and social health of an individual [8]. Deteriorating physical, mental, economical and social health of an individual could increase the suicidal tendency, leading to accidents and suicide [9]. Several Studies have reported that COVID-19 pandemic is associated with increased stress, depression, insomnia, and narcotics abuse [10]. Research on exploring association/impact of the pandemic with suicide and accident are abundant in developed countries, where there is narrow gap in different samples. In countries like India where there are extreme rich and extreme poor individuals such studies will provide a better insight about the impact of pandemic situation on such explorations [11]. Of course limited public data availability and lack of funds to eminent poor researchers of countries like India for carrying out field survey of situation might interfere with the output of such studies on the COVID-19 impact on suicide and accidental death in developing countries. One study done by, Pirikis et al. found that the suicidal death has not increased in twenty two high-income countries, whereas in LMICs, COVID-19 attributed as a prominent cause of suicidal death [12]. The impact of the pandemic on suicide and accidental death could be country- exclusive depending on individual country specific factors like the prevalence of physical, mental, economical and social co morbidities, and the country specific public health actions imposed by governments to contain the pandemic. Some studies found gender variation in suicide rates with a high rate for males, whereas some have reported mental health worsening related to the pandemic is higher in females [13,14,15].
The COVID-19 pandemic has had deleterious effects on the food system, economy and social life globally as well as it has disrupted transportation across the world [16]. Globally governments imposed travel restrictions (closed borders, restricted flights, and lockdowns) which may have reduced the risk of collisions and accidental deaths [17]. Two major waves of the COVID-19 pandemic distressed the world in 2020 and 2021, leading to the death of about 06 million (real count may be more) people worldwide by 2021end [18]. The first confirmed case of COVID-19 in India, was from southern state Kerala on 30th January 2020 [19], India imposed nationwide lockdown and stopped flights, Railways and roadways from 25thMarch disrupting several routine services except for essential services like food, health, etc [20,21,22,23]. The lockdown increased fear and feeling of isolation, which was more aggravated by the loss of relatives, and social stigma [24]. Added to this lockdown caused loss of employment, financial crisis, uncertain future to students who could not attend schools and colleges [25]. Females became more exposed to domestic violence at home while older ones feel neglected leading to depression [26].
This study tried to find out the COVID-19 pandemic situation impact on accidental death as well as suicide rates in India. This study may help policy and decision makers in devising appropriate programs for reducing the future pandemic or any similar disaster responses to minimize harm. This study also aims to create awareness among health professionals and readers in general by doing comparative study of suicidal deaths and accidents during the pre-COVID-19 and COVID-19 periods.
2. Aim and Objective
The aim of this study is to compare the accidental and suicidal deaths, (incidence, prevalence, rate, numbers, percentage, gender, etc.) in the pandemic (COVID-19 period) with non-pandemic periods (pre-COVID-19 period), in India. The key objective is to assess the COVID-19 impact on accidental and suicidal mortality in terms of epidemiological indicators like rate, proportions, etc.
Methodology
This is an observational, comparative and retrospective study for analyzing the COVID-19 impact on suicide and accidental death count in India. The study period is from 1st January 1967 to 31st December 2021, to assess the effect of the COVID-19 pandemic situation on suicide and accidental death rates. We define 1st January 1967 to 31st December 2019 as the pre-pandemic period and 1st January 2020 to 31st December 2021 as the pandemic period (based on identification of first COVID-19 confirmed case in India). Of course two similar periods is also compared to avoid bias i.e. 2018-2019 is compared to 2020-2021. A larger period is studied to know the longer trends in suicide and accidental death count in India.
Study setting and data
The annual suicide and accidental death counts by gender for India were obtained from NCRB (NATIONAL CRIME RECORDS BUREAU), Government of India [27]. The cause of death is investigated by the Indian Police department of 36 states and union territories of India as required by established law. The nature of death is usually based on the certified medical and autopsy reports. The population estimate by gender was obtained from World Bank, Population data [28]. Table 1 presents the data collected during the study period.
Statistical analysis
We calculated the suicide and accidental death rates for each year during the study period by dividing the number of suicide and accidental death by the population exposed (considering whole population exposed). Then incidence rate per lakh population is calculated for each year during the pandemic era by utilizing the data.
The data was collected from NCRB records. The same period was also taken to address any bias due to seasonal factors as well as the whole data collected was also analyzed to present the previous background. The data is presented as tables, graph, etc. with appropriate statistical analysis. The incidence rate ratio (IRR) is calculated as the ratio of incidence of suicide and accidental death out of total deaths during the study period and two period separately (NOT AVAILABLE IN PREPRINT). Table 2 presents the statistical analysis of the data collected during the study period.
3. Results
Suicidal deaths - accidental deaths – 2018-2019-2020-2021
Table 3-A shows that during the pre-COVID-19 era of this study, 1106567 suicidal and accidental deaths were reported, of which 83298 (75.27 %) were accidental deaths and 273639 (24.73 %) were suicidal death. During the COVID-19 epoch of this study, 1089012 suicidal and accidental deaths were reported of which 771927 (70.88 %) were accidental and 317085 (29.12 %) were suicidal.
This research study revealed that out of two study period the accidental death were reduced by 4.39 % during the COVID-19 epoch of this study whereas the suicidal death increased by 4.39% during the COVID-19 epoch. This study also revealed that the total suicidal and accidental deaths reduced during COVID-19 epoch by 1.59%.
Table 3-B shows that out of total 1604855 accidental death during above study period 832928 (51.90%) accidental deaths were reported during the pre-COVID-19 era of this study, whereas 771927 (48.10 %) were reported during COVID-19 epoch. During the pre-COVID-19 epoch of this study, 273639 (46.32%) suicidal deaths whereas 317085 (53.68%) were reported during the COVID-19 epoch out of total 590724 suicide during above study period.
This research study revealed that out of individual category of total suicide and accidental death, the accidental death were reduced by 3.80 % during the COVID-19 epoch of this study whereas the suicidal death increased by 7.35% during the COVID-19 epoch.
Mean Suicidal deaths vs. accidental deaths – 1967-2021
The whole study period i.e. from 1967 to 2021 mean comparison of two periods is presented in Table 3-C and D. The mean accidental death and suicides increased to a great extent during the COVID period as compared to pre- COVID period of study. This study revealed that the mean accidental death and suicide both increased during COVID period of study as compared to pre-pandemic whole period from 1967 by 25.47 % and 30.61% respectively. Alternatively we can say that the accidental death and suicides increased significantly in India, which is largely preventable.
To reduce the bias a similar previous period of pre- COVID period is compared in Table3-A and B.
Test of independence is not applied here between cause of death during pre-COVID-19 and COVID-19 era as this is not a sample survey, instead the whole population is taken into account for this study.
Gender-Wise Yearly variation in suicides and accidental death
Table 1,Table 2, Table 4 and Figure 1 and Figure 2 presents the Gender-Wise Yearly variation in suicides and accidental death during the study period.
A monthly data of suicides will provide a better insight in suicides and accidental deaths during the COVID period, particularly to assess the impact of the lockdown period on, the number of accidental and Suicidal deaths. The data is not available to us but we are trying to get data from an accredited source.
Gender Variation- accidental deaths
Tables 1, 2, 4-A and Figure 1 shows that during the total pre-COVID-19 period (1967-2019), there were 12149833 [95% C.I. - 198716.8 -259767.4] total accidental deaths, out of which 8905209 were male[95% C.I. - 142066 -193979.6], and 3220020 female[95% C.I. - 55866.3 -65643.9], whereas, for the COVID-19 period, there were total 771927 accidental deaths [95% C.I. - 238997.2- 532929.8] out of which 625556 were males[95% C.I. -168270.3 -457285.7], and 146281 were females[95% C.I. -71037.6 -75243.4]. This study revealed that compared to immediate previous i.e. 2018-2019 pre-pandemic era a decrease in percentage and annual incidence of accidental deaths is observed in both the genders with male preponderance during the COVID-19 period (2020-2021) of the study.
Male
Table 1, 2, 4-A and Figure 1 shows that for the pre-COVID period 2018-2019, accidental deaths percentage among males out of total accidental deaths (411824-421104) were 80.4%-80.8% respectively for 2018-2019 whereas for the COVID period 2020-2021(374397-397530), accidental deaths among males as a percentage of total accidental deaths was 80.5%-81.5% respectively for 2018-2019. The accidental deaths among males percentage increased slight in comparison to females in COVID-19 era but actual count and incidence decreased.
Female
Table 1, 2, 4-A and Figure 1 shows that for the pre-COVID period 2018-2019, accidental deaths percentage among females out of total accidental deaths (411824-421104) were 19.6%-19.2% respectively for 2018-2019 whereas for the COVID period 2020-2021(374397-397530), accidental deaths among females as a percentage of total accidental deaths was 19.5%-18.4% respectively for 2018-2019. The accidental deaths among females percentage decreased slight in comparison to males in COVID-19 era but actual count and incidence decreased.
Gender Variation- Suicide
Table 1, 2, 4-B and Figure 2 shows that during the total pre-COVID-19 period (1967-2019), there were 4464299 [95% C.I. - 74052.4- 94411.8] total suicide deaths, out of which 2797739 were male[95% C.I. - 45719.6 -59855.4], and 1666479 female[95% C.I. - 28207.7- 34678.3], whereas, for the COVID-19 period, there were total 317085 suicide deaths [95% C.I. - 88779.1 -228305.9] out of which 227511 were males[95% C.I. -47384.6 -180126.4], and 89524 were females[95% C.I. -41407.6- 48116.4]. This study revealed that compared to immediate previous i.e. 2018-2019 pre-pandemic era, an increase in percentage and annual incidence of suicide deaths is observed in both the genders with male preponderance during the COVID-19 period (2020-2021) of the study.
Male
Table 1, 2, 4-B and Figure 2 shows that for the pre-COVID period 2018-2019, suicide deaths percentage among males out of total suicide deaths (134516-139123) were 68.5%-70.2% respectively for 2018-2019 whereas for the COVID period 2020-2021(153052-164033), suicide deaths among males as a percentage of total suicide deaths was 70.9%-72.5% respectively for 2018-2019. This study revealed that the suicide deaths percentage among males increased significantly in comparison to females in COVID-19 era and actual count and incidence also increased.
Female
Table 1, 2, 4-B and Figure 2 shows that for the pre-COVID period 2018-2019, suicide deaths percentage among females out of total suicide deaths (134516-139123) were 31.5%-29.8% respectively for 2018-2019 whereas for the COVID period 2020-2021(153052-164033), suicide deaths among females as a percentage of total suicide deaths was 29.1%-27.4% respectively for 2018-2019. This study revealed that the suicide deaths among females percentage increased in COVID-19 era and actual count and incidence also increased.
Table 1, 2, 3 and 4 shows that during this 55 year observational retrospective study between 1st January 1967 and 31st December 2021, 1, 29, 21,760 accidental deaths occurred of which 71.0% were male and 28.6% were female and 47, 81,384 people committed suicide in India, of which 61.9% were male and 38.1% were female. The annual average accidental death and suicide incidence (including both gender) during 55 years of the study is 24.6 and 9.1 per 100,000 respectively. This study revealed that males had a significantly higher mean annual incidence of accidental deaths of 32.7 per 100,000 compared to female of 13.4 per 100,000. Furthermore males had a significantly higher mean annual incidence of suicidal deaths of 10.5 per 100,000 compared to female of 06.8 per 100,000. Furthermore mean male and female suicide percent out of total suicides during whole period of study is 61.9% and 38.1%, whereas for accidental deaths it is 71.0 and 28.6 respectively.
The statistical analysis of suicide in India from 1st January-1967 to 31st December 2021 showed a substantial variation with annual suicide numbers ranging from 38217 to 164033 [Min, Max],( Obs, Mean, Std. Dev., [95% Conf. Interval], Std. Err., Total, - 55,86934.3, 38879.9, 76423.5 -97444.9, 5242.6, 4781384,) respectively.
The statistical analysis of accidental deaths in India from 1st January-1967 to 31st December 2021 showed a substantial variation with annual accidental deaths ranging from 105601 to 451757, [Min, Max],( Obs, Mean, Std. Dev., [95% Conf. Interval], Std. Err., Total, - 55, 234941.1, 112658.5, 204485.2 -265397, 15190.9, 12921760,) respectively.
Gender-wise statistical analysis is presented in Table 2-A-B-C-D. The lowest suicides were recorded in 1979 in all 55 years, whereas the highest suicides were recorded in 2021 of the COVID-19 era. In the accidental death category lowest count were recorded in 1971 in all 55 years, whereas the highest count were recorded in 2014 of the pre-COVID-19 era. During the whole study period, the highest suicides incidence/lakh population were observed in males during the COVID-19 era 2021 while in 1999 highest suicides incidence/lakh population were observed in females.
Table 4 presents the gender-wise annual suicide and accidental death counts with annual incidence rates in different years at the country level. The annual increase/decrease in suicide and accidental death can be seen in this table.
Over the entire pandemic period, this study found an overall increase in annual suicide rates of males compared to female population. The increase in suicide rate is significant among males.
4. Discussion
Suicide and accidents are significant preventable public health problem especially in LMICs like India due to several factors like population density, illiteracy and a multitude of socio-economic as well as political-administrative issues [29]. Majority of these can be prevented with specific, timely, research-based low-cost interventions. A comprehensive multisectoral co-ordination for suicide and accident prevention is needed to reduce the mortality. Suicides are absolutely preventable cause of death by creating awareness in individual, community and national levels [30]. The prevention of accidents and suicide can be addressed by creating awareness in the societies to openly discuss it. A novel robust but flexible national suicide and accident prevention framework needs to be drafted for countrywide implementation in order to improve the data and situation.
Globally, the data of suicides and accidents availability and quality is poor [31,32]. This problem of poor-quality data is likely due to under-reporting and lack of proper classification. Improved surveillance and monitoring is needed for making accident and suicide prevention strategies. Faulty registration of accidental death and suicide in hospital- register and nationally-representative surveys may occur like COVID-19 death registration [33]. Furthermore a large percentage of mortality is not medically certified in India; hence the mortality counts may represent only the iceberg of deaths from accidents and suicides [34].
Risk assessment should be done at national level. Several research found well established link between suicide, accidental death and psychiatric illness (mostly depression and substance use dependency) [35,36]. Furthermore situations of crisis like COVID-19 leading to a breakdown in the normal ability to deal with life stresses, like financial crisis, fear, conflict, violence, abuse, discrimination, sense of isolation, relationship break-up, and illness can increase the vulnerability for suicides and accidental death [37].
The National Mental Health Act AND accident prevention strategy- NOT AVAILABLE IN PREPRINT
Limitations and strength
There are several studies done on the title mentioned research question but this study is very unique study as we have also explored the pandemic impact on accidents together with suicide (considering the fact that the COVID-19 led mental issues may have increased the accidents due to poor concentration while driving etc). One of the major limitations is the data which is obtained solely from the NCRB in our study. In India there is lack of any accredited other public health agencies, to collect and report these data. The NCRB is dependent on the 36 states and union territories for this data which lacks robust data collection systems hence prone to error due to utilizing methods like paper- recording and document transfer of data. Hence there could be data quality issues. Despite this limitation, the data utilized for this study is the most accredited available data and most of the studies have utilized this data source. The data we utilized was yearly aggregated data hence we were cannot explore finer variation in less time intervals (e.g. days or weeks) or age standardized variations like age or cause of accident and suicide. Furthermore, the study can only adjust for seasonality (by comparing equal annual periods), but the geographical-temporal trends could not be calculated specific to pandemic periods or pre- COVID-19 era. This is the first study in our knowledge analyzing the accidental death and suicide together in India in the context of the COVID-19 in the whole population, and by gender.
5. Conclusion
COVID-19 is having an indirect impact on accidental death and suicide, positive impact on accidental death while negative impact on suicide. The present quantitative data study on the accidental and suicidal deaths in both genders is intended to present a brief answer to the title mentioned query. The accident rate decreased while the suicide rates significantly increased in males of India during the COVID-19 pandemic, whereas in females the suicide rates increased slightly with significant decrease in accident rate. Epidemiological studies with better data input and more analysis is needed to better understand and control the drivers of accident and suicide with more exploration related to gender and other differences like existing co-morbidities. Future version of this research will try to explore these differential impacts of the COVID-19 pandemic in different states and union territories of India.
Prevention and control of suicides (accident already reduced hence not emphasized here)
Suicides are largely preventable. Measures should be taken at national, state/UTs and individual levels to reduce suicide and suicide attempts. WHO’s approach and recommendation for suicide prevention is given below which is based on evidence-based interventions [38]:
- Stop the access to instrument of suicide (e.g. firearms, pesticides, certain medications);
- Improve the media for appropriate-responsible reporting of suicide events;
- Encourage socio-emotional life skills;
- Early identification, assessment, management and follow up of individuals with suicidal behaviours.,
These interventions need situation analysis with multisectoral collaboration, financing, awareness raising, surveillance and monitoring, capacity building, and evaluation. Suicide prevention require multisectoral coordination with collaboration among individuals of society, including the health and other sectors like agriculture, business, education, politics, labour, justice, law, defence, and the media. These efforts need to be comprehensive and integrated as individual approach for an issue as complex as suicide is not sufficient.
Recommendations for reducing suicides in distress like COVID-19 (accident already reduced)
- A national robust, flexible and scientifically-technically sound, multisectoral primordial preventive strategy is needed to mitigate the suicidal morbidity and mortality.
- Creating mass awareness by government bodies, national/local media, NGO-social organizations, health care facilities-providers, and increasing budgetary allocation for mental health.
- More investment on research and analysis to better understand the COVID-19 impact on suicides in different regions.
- Financial stability programs to decreased suicide in times of poverty.
- Promoting BCC through online portals with community approach.
Ethical Issues
None, Not applicable. This study has not involved any human or animals in real or for experiments. The submitted work does not contain any identifiable patient/participant information.
Sources of Funding
None
Author Contributions
Project proposal, data collection, compilation and analysis; Drafting project report; Writing final project report and proofreading – by author and co-author.
Funding
The author declares that no funds are taken from any individual or agency-institution for this study.
Acknowledgments
I am thankful to Advocate Anupama my wife and daughters Aathmika-Atheeva for cooperation.
Conflicts of Interest
There are no conflicts of interest.
Abbreviations
COVID-19- Coronavirus Disease 2019; UTs- union territories; World Health Organization (WHO); LMICs (lower-middle-income countries); GoI (Government of India)
References
- WHO (World Health Organization) - Home/Newsroom/Fact sheets/Detail/Suicide – Available at - https://www.who.int/news-room/fact-sheets/detail/suicide.
- Renaud, J., MacNeil, S. L., Vijayakumar, L., Spodenkiewicz, M., Daniels, S., Brent, D. A., & Turecki, G. (2022). Suicidal ideation and behavior in youth in low- and middle-income countries: A brief review of risk factors and implications for prevention. Frontiers in psychiatry, 13, 1044354. [CrossRef]
- Thippaiah, S. M., Nanjappa, M. S., & Math, S. B. (2019). Suicide in India: A preventable epidemic. The Indian journal of medical research, 150(4), 324–327. [CrossRef]
- WHO (World Health Organization) - Home/Health topics/Suicide– Available at - https://www.who.int/india/health-topics/suicide#:~:text=The%20suicide%20mortality%20rate%20per,relief%20to%20those%20attempting%20it.
- Ramesh, P., Taylor, P. J., McPhillips, R., Raman, R., & Robinson, C. (2022). A Scoping Review of Gender Differences in Suicide in India. Frontiers in psychiatry, 13, 884657. [CrossRef]
- WHO (World Health Organization) - Home/Newsroom/Feature stories/Detail/The impact of COVID-19 on mental health cannot be made light of– Available at - https://www.who.int/news-room/feature-stories/detail/the-impact-of-covid-19-on-mental-health-cannot-be-made-light-of.
- WHO (World Health Organization) - Home/News/Statement on the fifteenth meeting of the IHR (2005) Emergency Committee on the COVID-19 pandemic -Available at - https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic. 2023.
- Lu, X., & Lin, Z. (2021). COVID-19, Economic Impact, Mental Health, and Coping Behaviors: A Conceptual Framework and Future Research Directions. Frontiers in psychology, 12, 759974. [CrossRef]
- Brådvik L. (2018). Suicide Risk and Mental Disorders. International journal of environmental research and public health, 15(9), 2028. [CrossRef]
- . Kohli, S., Diwan, S., Kumar, A., Kohli, S., Aggarwal, S., Sood, A., Sachdeva, H. C., & Usha, G. (2022). Depression, Anxiety, Stress, and Insomnia amongst COVID Warriors across Several Hospitals after Second Wave: Have We Acclimatized? A Cross-sectional Survey. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine, 26(7), 825–832. [CrossRef]
- Surjit S Bhalla, Karan Bhasin and Arvind Virmani. Pandemic, Poverty and Inequality: Evidence from India – Available at- https://www.elibrary.imf.org/downloadpdf/journals/001/2022/069/001.2022.issue-069-en.xml.
- Knipe, D., John, A., Padmanathan, P., Eyles, E., Dekel, D., Higgins, J. P. T., Bantjes, J., Dandona, R., Macleod-Hall, C., McGuinness, L. A., Schmidt, L., Webb, R. T., & Gunnell, D. (2022). Suicide and self-harm in low- and middle- income countries during the COVID-19 pandemic: A systematic review. PLOS global public health, 2(6), e0000282. [CrossRef]
- Pieh, C., Budimir, S., & Probst, T. (2020). The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. Journal of psychosomatic research, 136, 110186. [CrossRef]
- Proto, E., & Quintana-Domeque, C. (2021). COVID-19 and mental health deterioration by ethnicity and gender in the UK. PloS one, 16(1), e0244419. [CrossRef]
- Moghanibashi-Mansourieh A. (2020). Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian journal of psychiatry, 51, 102076. [CrossRef]
- WHO (World Health Organization) - Home/News/Impact of COVID-19 on people's livelihoods, their health and our food systems-Available at - https://www.who.int/news/item/13-10-2020-impact-of-covid-19-on-people's-livelihoods-their-health-and-our-food-systems.
- Yasin, Y.J., Grivna, M. & Abu-Zidan, F.M. Global impact of COVID-19 pandemic on road traffic collisions. World J Emerg Surg 16, 51 (2021). [CrossRef]
- COVID-19 Excess Mortality Collaborators (2022). Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21. Lancet (London, England), 399(10334), 1513–1536. [CrossRef]
- Andrews, M. A., Areekal, B., Rajesh, K. R., Krishnan, J., Suryakala, R., Krishnan, B., Muraly, C. P., & Santhosh, P. V. (2020). First confirmed case of COVID-19 infection in India: A case report. The Indian journal of medical research, 151(5), 490–492. [CrossRef]
- Piyush Kumar, (2022). What Impact Have SARS-CoV-2/Covid-19 Pandemic induced lockdown on the number of OPD patients of Diabetes, Hypertension, Stroke (CVA), Acute Heart Disease, Mental Illness, Epilepsy, Ophthalmic, Dental and oncology in India during the lockdown months (April-May-2020)?Observational Research Analysis?. Int J Cancer Res Ther, 7(2), 51-62. [CrossRef]
- Piyush Kumar. (2022). What Impact Have SARS-CoV-2/Covid-19 Pandemic on Domestic Violence against Women in India across Different States and Union Territories from the Beginning of Lockdown Due To covid-19 pandemic in March 2020 till 20th September 2020?. J Cli Ped Chi Res, 3(1), 78-83. 20 March. [CrossRef]
- Piyush Kumar, Habib Hasan Farooqui. (2022). What is the Impact of Covid-19 Pandemic on the RCH (Reproductive and Child Health) Programme in Rajasthan, because of nationwide lockdown (April 2020 to June 2020)?. J Cli Ped Chi Res, 3(1), 26-41. 20 April. [CrossRef]
- Dr. Piyush Kumar (2022), Impact of Covid-19 Induced Lockdown on The opd Patients Of Diabetes, Hypertension, Stroke (cva), Acute Heart Disease, Mental Illness, Epilepsy, Ophthalmic, Dental and Oncology In India- A Cross-Sectional Research Study, Int J Diabetes Metab Disord, 2022, 7(1),10-22. [CrossRef]
- Singh, S., Roy, D., Sinha, K., Parveen, S., Sharma, G., & Joshi, G. (2020). Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry research, 293, 113429. [CrossRef]
- Chatterji, S., McDougal, L., Johns, N., Ghule, M., Rao, N., & Raj, A. (2021). COVID-19-Related Financial Hardship, Job Loss, and Mental Health Symptoms: Findings from a Cross-Sectional Study in a Rural Agrarian Community in India. International journal of environmental research and public health, 18(16), 8647. [CrossRef]
- Usher, K., Bradbury Jones, C., Bhullar, N., Durkin, D. J., Gyamfi, N., Fatema, S. R., & Jackson, D. (2021). COVID-19 and family violence: Is this a perfect storm?. International journal of mental health nursing, 30(4), 1022–1032. [CrossRef]
- NCRB (NATIONAL CRIME RECORDS BUREAU), Government of India- Available at - https://ncrb.gov.in/en/ADSI-2021.
- The World Bank, Population data - Available at - https://data.worldbank.org/indicator/SP.POP.TOTL.FE.ZS?locations=IN.
- Thippaiah, S. M., Nanjappa, M. S., & Math, S. B. (2019). Suicide in India: A preventable epidemic. The Indian journal of medical research, 150(4), 324–327. [CrossRef]
- Vijayakumar L. (2010). Indian research on suicide. Indian journal of psychiatry, 52(Suppl 1), S291–S296. [CrossRef]
- Bachmann S. (2018). Epidemiology of Suicide and the Psychiatric Perspective. International journal of environmental research and public health, 15(7), 1425. [CrossRef]
- halla, K., Harrison, J. E., Shahraz, S., Fingerhut, L. A., & Global Burden of Disease Injury Expert Group (2010). Availability and quality of cause-of-death data for estimating the global burden of injuries. Bulletin of the World Health Organization, 88(11), 831–838C. [CrossRef]
- Piyush K and Anupama. What can be Impact of Civil Authorities’ Faulty Mortality Registration on COVID-19 Mortality Count in the State of Bihar, India- Evidence from NFHS (National Family Health Survey -5). Public H Open Acc 2022, 6(2): 000212. [CrossRef]
- Piyush K and Anupama. What Percentage of Mortality were Medically Certified among Total Registered Mortality in 36 States & UTs of India During 2018-2020 and COVID-19 Mortality AgeSex Distribution Pattern in India: A Cross Sectional Observational Research Study. Public H Open Acc 2022, 6(2): 000214. [CrossRef]
- Brådvik L. (2018). Suicide Risk and Mental Disorders. International journal of environmental research and public health, 15(9), 2028. [CrossRef]
- Alavi, S. S., Mohammadi, M. R., Souri, H., Mohammadi Kalhori, S., Jannatifard, F., & Sepahbodi, G. (2017). Personality, Driving Behavior and Mental Disorders Factors as Predictors of Road Traffic Accidents Based on Logistic Regression. Iranian journal of medical sciences, 42(1), 24–31.
- Sripad, M. N., Pantoji, M., Gowda, G. S., Ganjekar, S., Reddi, V. S. K., & Math, S. B. (2021). Suicide in the context of COVID-19 diagnosis in India: Insights and implications from online print media reports. Psychiatry research, 298, 113799. [CrossRef]
- WHO (World Health Organization) - National suicide prevention strategies Progress, examples and indicators – Available at - https://apps.who.int/iris/bitstream/handle/10665/279765/9789241515016-eng.pdf.
Figure 1.
Gender-wise comparison of annual accidental death in India from 1st January-1967 to 31st December 2021.
Figure 1.
Gender-wise comparison of annual accidental death in India from 1st January-1967 to 31st December 2021.
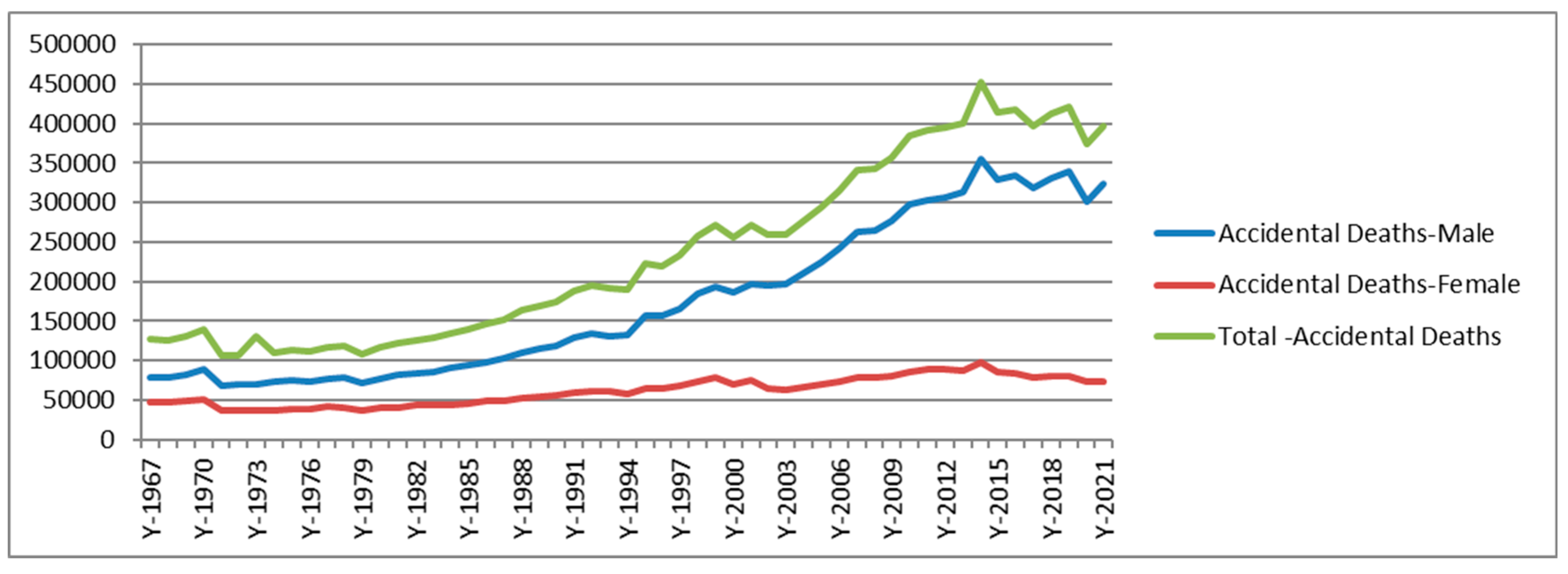
Figure 2.
Gender-wise comparison of annual suicide in India from 1st January-1967 to 31st December 2021.
Figure 2.
Gender-wise comparison of annual suicide in India from 1st January-1967 to 31st December 2021.
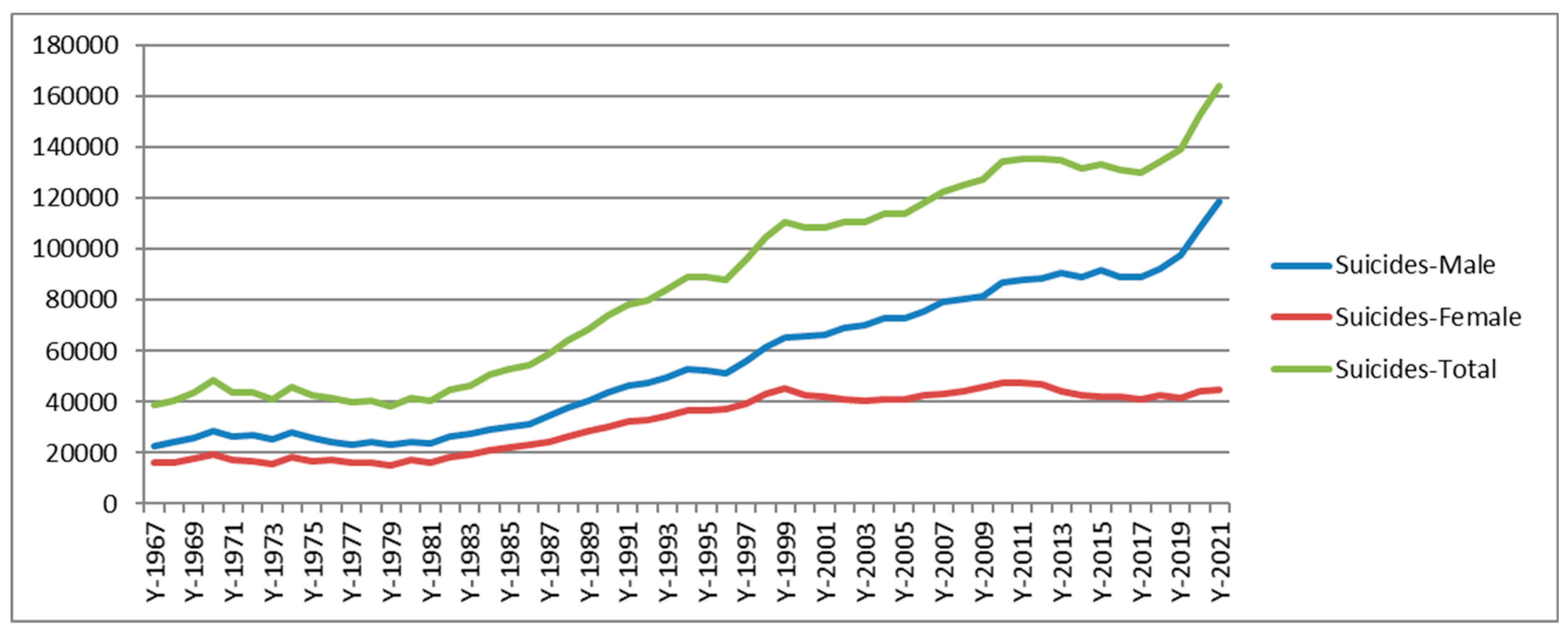

Table 1.
Gender-wise suicide and accidental death in India from 1967 to 2021*.
| Year | Accidental Deaths-Male | Accidental Deaths-Female | Accidental Deaths-Bisexual | Total -Accidental Deaths | Suicides-Male | Suicides-Female | Suicides-Bisexual | Suicides-Total |
| 1967 | 79131 | 47631 | N/A** | 126762 | 22637 | 16192 | N/A | 38829 |
| 1968 | 79159 | 47073 | N/A | 126232 | 24464 | 16224 | N/A | 40688 |
| 1969 | 82105 | 48650 | N/A | 130755 | 25947 | 17686 | N/A | 43633 |
| 1970 | 89210 | 50542 | N/A | 139752 | 28846 | 19582 | N/A | 48428 |
| 1971 | 68344 | 37257 | N/A | 105601 | 26326 | 17349 | N/A | 43675 |
| 1972 | 69838 | 36346 | N/A | 106184 | 26923 | 16678 | N/A | 43601 |
| 1973 | 69613 | 36741 | N/A | 130654 | 25231 | 15576 | N/A | 40807 |
| 1974 | 73580 | 37044 | N/A | 110624 | 27791 | 18217 | N/A | 46008 |
| 1975 | 74987 | 38029 | N/A | 113016 | 26074 | 16816 | N/A | 42890 |
| 1976 | 73098 | 38513 | N/A | 111611 | 24042 | 17373 | N/A | 41415 |
| 1977 | 76013 | 41325 | N/A | 117338 | 23453 | 16265 | N/A | 39718 |
| 1978 | 78352 | 40242 | N/A | 118594 | 24137 | 16070 | N/A | 40207 |
| 1979 | 72448 | 36539 | N/A | 108987 | 22980 | 15237 | N/A | 38217 |
| 1980 | 76293 | 40619 | N/A | 116912 | 24188 | 17475 | N/A | 41663 |
| 1981 | 82328 | 39893 | N/A | 122221 | 23864 | 16381 | N/A | 40245 |
| 1982 | 82977 | 43016 | N/A | 125993 | 26520 | 18212 | N/A | 44732 |
| 1983 | 85577 | 42999 | N/A | 128576 | 27260 | 19319 | N/A | 46579 |
| 1984 | 90636 | 43992 | N/A | 134628 | 29296 | 21275 | N/A | 50571 |
| 1985 | 93568 | 46089 | N/A | 139657 | 30460 | 22351 | N/A | 52811 |
| 1986 | 98480 | 48543 | N/A | 147023 | 31271 | 23086 | N/A | 54357 |
| 1987 | 103727 | 48587 | N/A | 152314 | 34292 | 24276 | N/A | 58568 |
| 1988 | 110235 | 53287 | N/A | 163522 | 37755 | 26515 | N/A | 64270 |
| 1989 | 114953 | 54113 | N/A | 169066 | 40212 | 28532 | N/A | 68744 |
| 1990 | 117932 | 56469 | N/A | 174401 | 43451 | 30460 | N/A | 73911 |
| 1991 | 129142 | 58861 | N/A | 188003 | 46324 | 32126 | N/A | 78450 |
| 1992 | 133977 | 60933 | N/A | 194910 | 47481 | 32668 | N/A | 80149 |
| 1993 | 130499 | 61858 | N/A | 192357 | 49851 | 34393 | N/A | 84244 |
| 1994 | 132241 | 58194 | N/A | 190435 | 52752 | 36443 | N/A | 89195 |
| 1995 | 157219 | 65268 | N/A | 222487 | 52357 | 36821 | N/A | 89178 |
| 1996 | 156106 | 63988 | N/A | 220094 | 51206 | 37035 | N/A | 88241 |
| 1997 | 164876 | 69027 | N/A | 233903 | 56281 | 39548 | N/A | 95829 |
| 1998 | 185520 | 72889 | N/A | 258409 | 61686 | 43027 | N/A | 104713 |
| 1999 | 193652 | 78266 | N/A | 271918 | 65488 | 45099 | N/A | 110587 |
| 2000 | 186324 | 69559 | N/A | 255883 | 66032 | 42561 | N/A | 108593 |
| 2001 | 196129 | 74890 | N/A | 271019 | 66314 | 42192 | N/A | 108506 |
| 2002 | 194850 | 65272 | N/A | 260122 | 69332 | 41085 | N/A | 110417 |
| 2003 | 197285 | 62340 | N/A | 259625 | 70221 | 40630 | N/A | 110851 |
| 2004 | 210190 | 67073 | N/A | 277263 | 72651 | 41046 | N/A | 113697 |
| 2005 | 224806 | 69369 | N/A | 294175 | 72916 | 40998 | N/A | 113914 |
| 2006 | 241210 | 73494 | N/A | 314704 | 75702 | 42410 | N/A | 118112 |
| 2007 | 262918 | 77876 | N/A | 340794 | 79295 | 43342 | N/A | 122637 |
| 2008 | 263809 | 78500 | N/A | 342309 | 80544 | 44473 | N/A | 125017 |
| 2009 | 276333 | 80688 | N/A | 357021 | 81471 | 45680 | N/A | 127151 |
| 2010 | 298262 | 86387 | N/A | 384649 | 87180 | 47419 | N/A | 134599 |
| 2011 | 302420 | 88464 | N/A | 390884 | 87839 | 47746 | N/A | 135585 |
| 2012 | 306061 | 88921 | N/A | 394982 | 88453 | 46992 | N/A | 135445 |
| 2013 | 312670 | 87847 | N/A | 400517 | 90543 | 44256 | N/A | 134799 |
| 2014 | 354573 | 97078 | 106 | 451757 | 89129 | 42521 | 16 | 131666 |
| 2015 | 328241 | 85169 | 47 | 413457 | 91528 | 42088 | 7 | 133623 |
| 2016 | 333804 | 84372 | 45 | 418221 | 88997 | 41997 | 14 | 131008 |
| 2017 | 318316 | 78234 | 34 | 396584 | 89019 | 40852 | 16 | 129887 |
| 2018 | 330925 | 80864 | 35 | 411824 | 92114 | 42391 | 11 | 134516 |
| 2019 | 340267 | 80800 | 37 | 421104 | 97613 | 41493 | 17 | 139123 |
| 2020 | 301405 | 72975 | 17 | 374397 | 108532 | 44498 | 22 | 153052 |
| 2021 | 324151 | 73306 | 33 | 397530 | 118979 | 45026 | 28 | 164033 |
| Total | 9530765 | 3366301 | 354 | 12921760 | 3025250 | 1756003 | 131 | 4781384 |
*Source of data – NCRB, Government of India- Available at - https://ncrb.gov.in/en/ADSI-2021 ** N/A – Not Available.
Table 2.
Statistical analysis of the data collected during the study period.
| A-Gender-wise statistical analysis of suicide and accidental death in India from 1st January-1967 to 31st December 2021 | ||||||||
| Variable | Obs | Mean | Std. Dev. | [95% Conf. Interval] | Std. Err. | Total | Min | Max |
| Accidental Deaths-Male | 55 | 173286.6 | 96397.1 | 147226.9 -199346.4 | 12998.2 | 9530765 | 68344 | 354573 |
| Accidental Deaths-Female | 55 | 61205.5 | 17561.7 | 56457.9 -65953.1 | 2368.0 | 3366301 | 36346 | 97078 |
| Accidental Deaths-Bisexual | 8 | 44.3 | 26.5 | 22.1 -66.4 | 9.4 | 354 | 17 | 106 |
| Total -Accidental Deaths | 55 | 234941.1 | 112658.5 | 204485.2 -265397 | 15190.9 | 12921760 | 105601 | 451757 |
| Suicides-Male | 55 | 55004.6 | 27692.1 | 47518.3 -62490.7 | 3734.0 | 3025250 | 22637 | 118979 |
| Suicides-Female | 55 | 31927.3 | 11789.9 | 28740.1- 35114.6 | 1589.8 | 1756003 | 15237 | 47746 |
| Suicides-Bisexual | 8 | 16.4 | 6.4 | 10.9 -21.8 | 2.3 | 131 | 7 | 28 |
| Suicides-Total | 55 | 86934.3 | 38879.9 | 76423.5 -97444.9 | 5242.6 | 4781384 | 38217 | 164033 |
| B-Gender-wise statistical analysis of suicide and accidental death in India during pre-COVID-19 period from 1st January 1967 to 31st December 2019 | ||||||||
| Variable | Obs | Mean | Std. Dev. | [95% Conf. Interval] | Std. Err. | Total | Min | Max |
| Accidental Deaths-Male | 53 | 168022.8 | 94171.1 | 142066 -193979.6 | 12935.4 | 8905209 | 68344 | 354573 |
| Accidental Deaths-Female | 53 | 60755.1 | 17736.6 | 55866.3 -65643.9 | 2436.3 | 3220020 | 36346 | 97078 |
| Accidental Deaths-Bisexual | 6 | 50.7 | 27.6 | 21.7 -79.7 | 11.3 | 304 | 34 | 106 |
| Total -Accidental Deaths | 53 | 229242.1 | 110745.8 | 198716.8 -259767.4 | 15212.1 | 12149833 | 105601 | 451757 |
| Suicides-Male | 53 | 52787.5 | 25642.4 | 45719.6 -59855.4 | 3522.3 | 2797739 | 22637 | 97613 |
| Suicides-Female | 53 | 31443 | 11737.6 | 28207.7- 34678.3 | 1612.3 | 1666479 | 15237 | 47746 |
| Suicides-Bisexual | 6 | 13.5 | 3.8 | 9.5- 17.5 | 1.6 | 81 | 7 | 17 |
| Suicides-Total | 53 | 84232.1 | 36931.9 | 74052.4- 94411.8 | 5072.9 | 4464299 | 38217 | 139123 |
| C-Gender-wise statistical analysis of suicide and accidental death in India during COVID-19 period from 1st January 2020 to 31st December 2021 | ||||||||
| Variable | Obs | Mean | Std. Dev. | [95% Conf. Interval] | Std. Err. | Total | Min | Max |
| Accidental Deaths-Male | 2 | 312778 | 16083.9 | 168270.3 -457285.7 | 11373 | 625556 | 301405 | 324151 |
| Accidental Deaths-Female | 2 | 73140.5 | 234.1 | 71037.6 -75243.4 | 165.5 | 146281 | 72975 | 73306 |
| Accidental Deaths-Bisexual | 2 | 25 | 11.3 | -76.6- 126.6 | 8 | 50 | 17 | 33 |
| Total -Accidental Deaths | 2 | 385963.5 | 16357.5 | 238997.2- 532929.8 | 11566.5 | 771927 | 374397 | 397530 |
| Suicides-Male | 2 | 113755.5 | 7387.1 | 47384.6 -180126.4 | 5223.5 | 227511 | 108532 | 118979 |
| Suicides-Female | 2 | 44762 | 373.4 | 41407.6- 48116.4 | 264 | 89524 | 44498 | 45026 |
| Suicides-Bisexual | 2 | 25 | 4.2 | -13.1- 63.1 | 3 | 50 | 22 | 28 |
| Suicides-Total | 2 | 158542.5 | 7764.7 | 88779.1 -228305.9 | 5490.5 | 317085 | 153052 | 164033 |
| D-Gender-wise statistical analysis of suicide and accidental death in India during Pre-COVID-19 period from 1st January 2018 to 31st December 2019 – NOT AVAILABLE IN PREPRINT | ||||||||
Table 3.
Cause of death during COVID-19 and pre-COVID-19 periods.
| Table 3A: Cause of death during COVID and pre-COVID periods Manner of death (same period percent of accidents and deaths) | Pre-COVID period 2018-2019 | COVID period 2020-2021 | Total 2018-2021 |
| Total Accidental Death | 832928(75.27%) | 771927(70.88%) | 1604855 |
| Total Suicide | 273639(24.73%) | 317085(29.12%) | 590724 |
| Total | 1106567(100%) | 1089012(100%) | 2195579 |
| Table 3B: Cause of death during COVID and pre-COVID periods Manner of death(Two study period percent of accidents and deaths) | Pre-COVID period 2018-2019 | COVID period 2020-2021 | Total 2018-2021 |
| Total Accidental Death | 832928 (51.90%) | 771927(48.10%) | 1604855(100%) |
| Total Suicide | 273639(46.32%) | 317085(53.68%) | 590724(100%) |
| Total | 1106567 | 1089012 | 2195579 |
| Table 3C: Cause of death during COVID and pre-COVID periods Manner of death (Two study period percent of accidents and deaths) | Mean Pre-COVID period 1967-2019 | Mean COVID period 2020-2021 | Mean Total 1967-2021 |
| Mean Accidental Death | 229242.1(37.26%) | 385964(62.74%) | 615206.1(100%) |
| Mean Suicide | 84232.06(34.70%) | 158543(65.30%) | 242775.1(100%) |
| Mean Total | 313474.2 | 544507 | 857981.2 |
| Table 3D: Cause of death during COVID and pre-COVID periods Manner of death (same period percent of accidents and deaths) | Mean Pre-COVID period 1967-2019 | Mean COVID period 2020-2021 | Mean Total 1967-2021 |
| Mean Accidental Death | 229242.1(73.13%) | 385964(70.88%) | 615206.1 |
| Mean Suicide | 84232.06(26.87%) | 158543(29.12%) | 242775.1 |
| Mean Total | 313474.2(100%) | 544507(100%) | 857981.2 |
Table 4A-.
Gender-wise comparison of accidental death in India from 1st January-1967 to 31st December 2021.
Table 4A-.
Gender-wise comparison of accidental death in India from 1st January-1967 to 31st December 2021.
| Year | Accidental Deaths-Male | Population male | Male-Annual Incidence per 100000 | Accidental Deaths-Female | Population female | Female-Annual Incidence per 100000 | Total -Accidental Deaths | Male-% of Total | Female-%of total | Accidental Deaths-Bisexual* |
| Y-1967 | 79131 | 269770979 | 29.3 | 47631 | 252216091 | 18.9 | 126762 | 62.4 | 37.6 | N/A** |
| Y-1968 | 79159 | 275736482 | 28.7 | 47073 | 257695427 | 18.3 | 126232 | 62.7 | 37.3 | N/A |
| Y-1969 | 82105 | 281934206 | 29.1 | 48650 | 263380464 | 18.5 | 130755 | 62.8 | 37.2 | N/A |
| Y-1970 | 89210 | 288292405 | 30.9 | 50542 | 269208897 | 18.8 | 139752 | 63.8 | 36.2 | N/A |
| Y-1971 | 68344 | 294818942 | 23.2 | 37257 | 275180236 | 13.5 | 105601 | 64.7 | 35.3 | N/A |
| Y-1972 | 69838 | 301529376 | 23.2 | 36346 | 281308597 | 12.9 | 106184 | 65.8 | 34.2 | N/A |
| Y-1973 | 69613 | 308465459 | 22.6 | 36741 | 287642024 | 12.8 | 130654 | 53.3 | 28.1 | N/A |
| Y-1974 | 73580 | 315584063 | 23.3 | 37044 | 294137889 | 12.6 | 110624 | 66.5 | 33.5 | N/A |
| Y-1975 | 74987 | 322800952 | 23.2 | 38029 | 300723268 | 12.6 | 113016 | 66.4 | 33.6 | N/A |
| Y-1976 | 73098 | 330077580 | 22.1 | 38513 | 307373867 | 12.5 | 111611 | 65.5 | 34.5 | N/A |
| Y-1977 | 76013 | 337496325 | 22.5 | 41325 | 314189303 | 13.2 | 117338 | 64.8 | 35.2 | N/A |
| Y-1978 | 78352 | 345069608 | 22.7 | 40242 | 321198151 | 12.5 | 118594 | 66.1 | 33.9 | N/A |
| Y-1979 | 72448 | 352826329 | 20.5 | 36539 | 328422054 | 11.1 | 108987 | 66.5 | 33.5 | N/A |
| Y-1980 | 76293 | 360875327 | 21.1 | 40619 | 335953058 | 12.1 | 116912 | 65.3 | 34.7 | N/A |
| Y-1981 | 82328 | 369149846 | 22.3 | 39893 | 343719452 | 11.6 | 122221 | 67.4 | 32.6 | N/A |
| Y-1982 | 82977 | 377542519 | 22.0 | 43016 | 351626946 | 12.2 | 125993 | 65.9 | 34.1 | N/A |
| Y-1983 | 85577 | 386102269 | 22.2 | 42999 | 359724278 | 12.0 | 128576 | 66.6 | 33.4 | N/A |
| Y-1984 | 90636 | 394865497 | 23.0 | 43992 | 368029660 | 12.0 | 134628 | 67.3 | 32.7 | N/A |
| Y-1985 | 93568 | 403766421 | 23.2 | 46089 | 376475662 | 12.2 | 139657 | 67.0 | 33.0 | N/A |
| Y-1986 | 98480 | 412811682 | 23.9 | 48543 | 385067312 | 12.6 | 147023 | 67.0 | 33.0 | N/A |
| Y-1987 | 103727 | 421960524 | 24.6 | 48587 | 393755601 | 12.3 | 152314 | 68.1 | 31.9 | N/A |
| Y-1988 | 110235 | 431194389 | 25.6 | 53287 | 402535292 | 13.2 | 163522 | 67.4 | 32.6 | N/A |
| Y-1989 | 114953 | 440551295 | 26.1 | 54113 | 411461378 | 13.2 | 169066 | 68.0 | 32.0 | N/A |
| Y-1990 | 117932 | 449984059 | 26.2 | 56469 | 420468106 | 13.4 | 174401 | 67.6 | 32.4 | N/A |
| Y-1991 | 129142 | 459463492 | 28.1 | 58861 | 429478264 | 13.7 | 188003 | 68.7 | 31.3 | N/A |
| Y-1992 | 133977 | 469046096 | 28.6 | 60933 | 438527953 | 13.9 | 194910 | 68.7 | 31.3 | N/A |
| Y-1993 | 130499 | 478735976 | 27.3 | 61858 | 447615320 | 13.8 | 192357 | 67.8 | 32.2 | N/A |
| Y-1994 | 132241 | 488535405 | 27.1 | 58194 | 456726553 | 12.7 | 190435 | 69.4 | 30.6 | N/A |
| Y-1995 | 157219 | 498432465 | 31.5 | 65268 | 465846665 | 14.0 | 222487 | 70.7 | 29.3 | N/A |
| Y-1996 | 156106 | 508349160 | 30.7 | 63988 | 474932057 | 13.5 | 220094 | 70.9 | 29.1 | N/A |
| Y-1997 | 164876 | 518303618 | 31.8 | 69027 | 484031612 | 14.3 | 233903 | 70.5 | 29.5 | N/A |
| Y-1998 | 185520 | 528287413 | 35.1 | 72889 | 493147162 | 14.8 | 258409 | 71.8 | 28.2 | N/A |
| Y-1999 | 193652 | 538244360 | 36.0 | 78266 | 502255693 | 15.6 | 271918 | 71.2 | 28.8 | N/A |
| Y-2000 | 186324 | 548223581 | 34.0 | 69559 | 511410095 | 13.6 | 255883 | 72.8 | 27.2 | N/A |
| Y-2001 | 196129 | 558291332 | 35.1 | 74890 | 520679574 | 14.4 | 271019 | 72.4 | 27.6 | N/A |
| Y-2002 | 194850 | 568334873 | 34.3 | 65272 | 529978166 | 12.3 | 260122 | 74.9 | 25.1 | N/A |
| Y-2003 | 197285 | 578236241 | 34.1 | 62340 | 539178882 | 11.6 | 259625 | 76.0 | 24.0 | N/A |
| Y-2004 | 210190 | 587990365 | 35.7 | 67073 | 548274218 | 12.2 | 277263 | 75.8 | 24.2 | N/A |
| Y-2005 | 224806 | 597477666 | 37.6 | 69369 | 557161047 | 12.5 | 294175 | 76.4 | 23.6 | N/A |
| Y-2006 | 241210 | 606611392 | 39.8 | 73494 | 565762395 | 13.0 | 314704 | 76.6 | 23.4 | N/A |
| Y-2007 | 262918 | 615506279 | 42.7 | 77876 | 574185530 | 13.6 | 340794 | 77.1 | 22.9 | N/A |
| Y-2008 | 263809 | 624242020 | 42.3 | 78500 | 582492785 | 13.5 | 342309 | 77.1 | 22.9 | N/A |
| Y-2009 | 276333 | 632892402 | 43.7 | 80688 | 590747758 | 13.7 | 357021 | 77.4 | 22.6 | N/A |
| Y-2010 | 298262 | 641566029 | 46.5 | 86387 | 599047591 | 14.4 | 384649 | 77.5 | 22.5 | N/A |
| Y-2011 | 302420 | 650244390 | 46.5 | 88464 | 607376801 | 14.6 | 390884 | 77.4 | 22.6 | N/A |
| Y-2012 | 306061 | 658839435 | 46.5 | 88921 | 615647779 | 14.4 | 394982 | 77.5 | 22.5 | N/A |
| Y-2013 | 312670 | 667322883 | 46.9 | 87847 | 623809180 | 14.1 | 400517 | 78.1 | 21.9 | N/A |
| Y-2014 | 354573 | 675549357 | 52.5 | 97078 | 631697152 | 15.4 | 451757 | 78.5 | 21.5 | 106 |
| Y-2015 | 328241 | 683543213 | 48.0 | 85169 | 639323292 | 13.3 | 413457 | 79.4 | 20.6 | 47 |
| Y-2016 | 333804 | 691623419 | 48.3 | 84372 | 647012921 | 13.0 | 418221 | 79.8 | 20.2 | 45 |
| Y-2017 | 318316 | 699587889 | 45.5 | 78234 | 654607791 | 12.0 | 396584 | 80.3 | 19.7 | 34 |
| Y-2018 | 330925 | 707149230 | 46.8 | 80864 | 661854076 | 12.2 | 411824 | 80.4 | 19.6 | 35 |
| Y-2019 | 340267 | 714325057 | 47.6 | 80800 | 668786993 | 12.1 | 421104 | 80.8 | 19.2 | 37 |
| Y-2020 | 301405 | 720997448 | 41.8 | 72975 | 675389679 | 10.8 | 374397 | 80.5 | 19.5 | 17 |
| Y-2021 | 324151 | 726503429 | 44.6 | 73306 | 681060412 | 10.8 | 397530 | 81.5 | 18.4 | 33 |
| Mean | 173286.6 | 493012045 | 32.7 | 61205.5 | 460355243.8 | 13.4 | 234941.091 | 71.0 | 28.6 | 44.3 |
*Due to less available data further analysis of this category is not done but it is included in total count. ** N/A – Not Available
Table 4B-.
Gender-wise comparison of suicide in India from 1st January-1967 to 31st December 2021.
| Year | No. of Suicides-Male | Population of male | Male-Annual Incidence of suicide in male per 100000 | No. of Suicides-Female | Population of female | Female-Annual Incidence of suicide in female per 100000 | Total No. of Suicides- | Male-% of Total suicide | Female-%of total suicide | Suicides-Bisexual* |
| Y-1967 | 22637 | 269770979 | 8.4 | 16192 | 252216091 | 6.4 | 38829 | 58.3 | 41.7 | N/A** |
| Y-1968 | 24464 | 275736482 | 8.9 | 16224 | 257695427 | 6.3 | 40688 | 60.1 | 39.9 | N/A |
| Y-1969 | 25947 | 281934206 | 9.2 | 17686 | 263380464 | 6.7 | 43633 | 59.5 | 40.5 | N/A |
| Y-1970 | 28846 | 288292405 | 10.0 | 19582 | 269208897 | 7.3 | 48428 | 59.6 | 40.4 | N/A |
| Y-1971 | 26326 | 294818942 | 8.9 | 17349 | 275180236 | 6.3 | 43675 | 60.3 | 39.7 | N/A |
| Y-1972 | 26923 | 301529376 | 8.9 | 16678 | 281308597 | 5.9 | 43601 | 61.7 | 38.3 | N/A |
| Y-1973 | 25231 | 308465459 | 8.2 | 15576 | 287642024 | 5.4 | 40807 | 61.8 | 38.2 | N/A |
| Y-1974 | 27791 | 315584063 | 8.8 | 18217 | 294137889 | 6.2 | 46008 | 60.4 | 39.6 | N/A |
| Y-1975 | 26074 | 322800952 | 8.1 | 16816 | 300723268 | 5.6 | 42890 | 60.8 | 39.2 | N/A |
| Y-1976 | 24042 | 330077580 | 7.3 | 17373 | 307373867 | 5.7 | 41415 | 58.1 | 41.9 | N/A |
| Y-1977 | 23453 | 337496325 | 6.9 | 16265 | 314189303 | 5.2 | 39718 | 59.0 | 41.0 | N/A |
| Y-1978 | 24137 | 345069608 | 7.0 | 16070 | 321198151 | 5.0 | 40207 | 60.0 | 40.0 | N/A |
| Y-1979 | 22980 | 352826329 | 6.5 | 15237 | 328422054 | 4.6 | 38217 | 60.1 | 39.9 | N/A |
| Y-1980 | 24188 | 360875327 | 6.7 | 17475 | 335953058 | 5.2 | 41663 | 58.1 | 41.9 | N/A |
| Y-1981 | 23864 | 369149846 | 6.5 | 16381 | 343719452 | 4.8 | 40245 | 59.3 | 40.7 | N/A |
| Y-1982 | 26520 | 377542519 | 7.0 | 18212 | 351626946 | 5.2 | 44732 | 59.3 | 40.7 | N/A |
| Y-1983 | 27260 | 386102269 | 7.1 | 19319 | 359724278 | 5.4 | 46579 | 58.5 | 41.5 | N/A |
| Y-1984 | 29296 | 394865497 | 7.4 | 21275 | 368029660 | 5.8 | 50571 | 57.9 | 42.1 | N/A |
| Y-1985 | 30460 | 403766421 | 7.5 | 22351 | 376475662 | 5.9 | 52811 | 57.7 | 42.3 | N/A |
| Y-1986 | 31271 | 412811682 | 7.6 | 23086 | 385067312 | 6.0 | 54357 | 57.5 | 42.5 | N/A |
| Y-1987 | 34292 | 421960524 | 8.1 | 24276 | 393755601 | 6.2 | 58568 | 58.6 | 41.4 | N/A |
| Y-1988 | 37755 | 431194389 | 8.8 | 26515 | 402535292 | 6.6 | 64270 | 58.7 | 41.3 | N/A |
| Y-1989 | 40212 | 440551295 | 9.1 | 28532 | 411461378 | 6.9 | 68744 | 58.5 | 41.5 | N/A |
| Y-1990 | 43451 | 449984059 | 9.7 | 30460 | 420468106 | 7.2 | 73911 | 58.8 | 41.2 | N/A |
| Y-1991 | 46324 | 459463492 | 10.1 | 32126 | 429478264 | 7.5 | 78450 | 59.0 | 41.0 | N/A |
| Y-1992 | 47481 | 469046096 | 10.1 | 32668 | 438527953 | 7.4 | 80149 | 59.2 | 40.8 | N/A |
| Y-1993 | 49851 | 478735976 | 10.4 | 34393 | 447615320 | 7.7 | 84244 | 59.2 | 40.8 | N/A |
| Y-1994 | 52752 | 488535405 | 10.8 | 36443 | 456726553 | 8.0 | 89195 | 59.1 | 40.9 | N/A |
| Y-1995 | 52357 | 498432465 | 10.5 | 36821 | 465846665 | 7.9 | 89178 | 58.7 | 41.3 | N/A |
| Y-1996 | 51206 | 508349160 | 10.1 | 37035 | 474932057 | 7.8 | 88241 | 58.0 | 42.0 | N/A |
| Y-1997 | 56281 | 518303618 | 10.9 | 39548 | 484031612 | 8.2 | 95829 | 58.7 | 41.3 | N/A |
| Y-1998 | 61686 | 528287413 | 11.7 | 43027 | 493147162 | 8.7 | 104713 | 58.9 | 41.1 | N/A |
| Y-1999 | 65488 | 538244360 | 12.2 | 45099 | 502255693 | 9.0 | 110587 | 59.2 | 40.8 | N/A |
| Y-2000 | 66032 | 548223581 | 12.0 | 42561 | 511410095 | 8.3 | 108593 | 60.8 | 39.2 | N/A |
| Y-2001 | 66314 | 558291332 | 11.9 | 42192 | 520679574 | 8.1 | 108506 | 61.1 | 38.9 | N/A |
| Y-2002 | 69332 | 568334873 | 12.2 | 41085 | 529978166 | 7.8 | 110417 | 62.8 | 37.2 | N/A |
| Y-2003 | 70221 | 578236241 | 12.1 | 40630 | 539178882 | 7.5 | 110851 | 63.3 | 36.7 | N/A |
| Y-2004 | 72651 | 587990365 | 12.4 | 41046 | 548274218 | 7.5 | 113697 | 63.9 | 36.1 | N/A |
| Y-2005 | 72916 | 597477666 | 12.2 | 40998 | 557161047 | 7.4 | 113914 | 64.0 | 36.0 | N/A |
| Y-2006 | 75702 | 606611392 | 12.5 | 42410 | 565762395 | 7.5 | 118112 | 64.1 | 35.9 | N/A |
| Y-2007 | 79295 | 615506279 | 12.9 | 43342 | 574185530 | 7.5 | 122637 | 64.7 | 35.3 | N/A |
| Y-2008 | 80544 | 624242020 | 12.9 | 44473 | 582492785 | 7.6 | 125017 | 64.4 | 35.6 | N/A |
| Y-2009 | 81471 | 632892402 | 12.9 | 45680 | 590747758 | 7.7 | 127151 | 64.1 | 35.9 | N/A |
| Y-2010 | 87180 | 641566029 | 13.6 | 47419 | 599047591 | 7.9 | 134599 | 64.8 | 35.2 | N/A |
| Y-2011 | 87839 | 650244390 | 13.5 | 47746 | 607376801 | 7.9 | 135585 | 64.8 | 35.2 | N/A |
| Y-2012 | 88453 | 658839435 | 13.4 | 46992 | 615647779 | 7.6 | 135445 | 65.3 | 34.7 | N/A |
| Y-2013 | 90543 | 667322883 | 13.6 | 44256 | 623809180 | 7.1 | 134799 | 67.2 | 32.8 | N/A |
| Y-2014 | 89129 | 675549357 | 13.2 | 42521 | 631697152 | 6.7 | 131666 | 67.7 | 32.3 | 16 |
| Y-2015 | 91528 | 683543213 | 13.4 | 42088 | 639323292 | 6.6 | 133623 | 68.5 | 31.5 | 7 |
| Y-2016 | 88997 | 691623419 | 12.9 | 41997 | 647012921 | 6.5 | 131008 | 67.9 | 32.1 | 14 |
| Y-2017 | 89019 | 699587889 | 12.7 | 40852 | 654607791 | 6.2 | 129887 | 68.5 | 31.5 | 16 |
| Y-2018 | 92114 | 707149230 | 13.0 | 42391 | 661854076 | 6.4 | 134516 | 68.5 | 31.5 | 11 |
| Y-2019 | 97613 | 714325057 | 13.7 | 41493 | 668786993 | 6.2 | 139123 | 70.2 | 29.8 | 17 |
| Y-2020 | 108532 | 720997448 | 15.1 | 44498 | 675389679 | 6.6 | 153052 | 70.9 | 29.1 | 22 |
| Y-2021 | 118979 | 726503429 | 16.4 | 45026 | 681060412 | 6.6 | 164033 | 72.5 | 27.4 | 28 |
| Mean | 55004.545 | 493012045 | 10.5 | 31927.3 | 460355243.8 | 6.8 | 86934.3 | 61.9 | 38.1 | 16.4 |
*Due to less available data further analysis of this category is not done but it is included in total count. ** N/A – Not Available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



