
Submitted:
25 May 2023
Posted:
26 May 2023
You are already at the latest version
Abstract
Abstract
Peripartum depression (PPD) is a major complication of pregnancy and many risk factors have been
associated with its development, including dysfunctional coping strategies and insecure attachment styles, both during pregnancy and postpartum. The aim of our study was to investigate the role of coping strategies in mediating the relationship between women’s attachment style and PPD in pregnancy, and one week after childbirth, in a large cohort of women. We hypothesized that the relationship between anxious and avoidant attachment and PPD would be mediated by use of maladaptive coping strategies. The assessment instruments were Edinburgh Postnatal Depression Scale (EPDS), Brief Coping Orientation for Problem Experiences (COPE), Experiences in Close Relationship Scale (ECR). The results indicated that the effect of insecure attachment styles (anxious and avoidant attachment) on antepartum depressive symptomatology was partially mediated by dysfunctional coping styles. Anxious attachment has also an indirect significant effect on postpartum depression through emotional coping; however, avoidant attachment does not seem to be significantly related to postpartum depression. Our findings revealed that not only it is important to consider attachment in understanding PPD but also that coping plays an important role in these relationships. These findings would help a preventive coping-based intervention strategy to enhance the capacity of women with insecure attachment styles to use more adaptive coping during and after pregnancy.
Keywords:
Perinatal Depression
; Attachment Style
; Coping Strategies
; Gender Medicine
; Women Health
1. Introduction
Major depressive disorder with peripartum onset is the most common complication of childbearing. Estimates show that one in seven women can experience peripartum depression (PPD) occurring during pregnancy or after childbirth [1,2]. A wide range of factors have been consistently identified as important risk factors that interact to contribute to the development of peripartum depression, including genetic predisposition, and various environmental, social, and psychological factors including negative personality traits and ineffective coping strategies [3,4,5].
Coping is described as the cognitive and behavioural strategies that people may use to deal with stressful circumstances that are demanding, challenging, threatening and/or have a potential for harm or loss [6]. Growing evidence suggests that maladaptive coping strategies (e.g., emotional coping, denial) may be risk factors for depressive mood during both antenatal [7,8] and postnatal period; while adaptive coping strategies (e.g., acceptance, humour) tend to be protective factors for PPD [3,8,9,10]. For instance, a recent large prospective study of 1626 women reported that maladaptive coping strategies such as self-distraction, substance use, and self-blame were positively associated with major postpartum depression [11]. Contrastingly, women who have positive coping styles that involve actively solving problems and positively interpreting situations were less likely to have perinatal depressive symptoms [12,13,14,15]. In recent years, research has also shown that coping with stressful conditions to ensure proper psychological adjustment does not operate in isolation. Rather, coping strategies appeared to mediate the relationship between personality traits and depression [11,12,16].
Preparation and transition to motherhood is considered a stressful experience demanding several adjustments to a new role and new responsibilities, which clearly triggers the attachment system throughout pregnancy and beyond [17]. The attachment system is an innate behavioural system that is biologically driven to promote survival through relational closeness. According to attachment theory the infant’s early experiences with caregivers determine internal working models of attachment (a set of mental representations of the self and others) which influence the individual’s future attachment behaviours in intimate relationships, including adult romantic relationships and parenting [18,19,20,21]. When a caregiver is perceived as accessible, and trustworthy, an infant develops a secure attachment style. However, when the primary caregiver is unavailable, and/or unresponsive, an infant develops a negative internal working model and an insecure attachment style [22]. Researchers have identified two dimensions of insecure attachments in adults: anxious and avoidance attachment. Anxious attachment is characterized by a hyperactivate attachment system, which leads to a constant need to seek support and comfort. Conversely, avoidant attachment is characterized by an underactive attachment system, which leads to continual inhibition of psychological and social relationship needs, excessive self-reliance, and a negative disposition toward others [23]. Several studies have shown that insecure attachment styles are associated with depressive symptoms in adulthood. [24,25,26]. Particularly, many previous studies have consistently shown that insecure attachment styles are strong and independent predictors of depression symptomatology either in pregnancy or in the postpartum period [see for review 4, 27]. For instance, Bianciardi et al. [5] found that insecure attachment styles were associated with depressive symptoms during both antenatal and early postpartum phases. However, many scholars have questioned the direct path between attachment and depression, and instead, they argue that early attachment experiences do influence later psychological distress through different intermediate mechanisms such as coping strategies [28,29,30]. Over the past few decades research has provided extensive evidence the coping strategies that individuals employ in stressful situations are determined, at least in part, by their attachment style [29,31]. Securely attached persons tend to rely on active coping styles (e.g., support-seeking coping strategies) and to maintain acceptable psychological well-being during stressful periods [e.g., 32-34].
In contrast, individuals with avoidance or anxiety attachment styles have been found to appraise stressful events in threatening terms and report doubts about their coping abilities [35]. For instance, Schmidt et al. [36] found insecure attachment to be related to less flexible coping, with anxiously attached individuals showing more negative emotional coping (e.g., impulsivity and distortion) and avoidantly attached individuals showing more disengaging methods of coping (e.g., denial, tendency to avoid awareness of problems).
Despite many previous studies reported a significant relationship between attachment styles and coping strategies, a mediational model to explore how coping might mediate the link between attachment and perinatal depression has not been performed. The integration of findings from attachment theory and behavioral neuroscience is of more than theoretical interest in patients with perinatal depressive disorders. Identification of possible mediators such as coping strategies of the relation between attachment and depression could optimize treatment outcomes through the selection of attachment-based therapies that address either insecure attachment styles or the maladaptive coping strategies associated with them.
Coping styles have been originally categorized into two high-order dimensions: problem-focused and emotion-focused [37]. However, there are many ways to group coping responses. An important distinction is between problem-focused (e.g., active coping, planning), emotion-focused coping (e.g., support seeking, emotion regulation) and disengagement coping, which includes maladaptive coping strategies and such as avoidance, denial, and wishful thinking [38,39,40,41].However, there is not much consistency in the aggregation of coping strategies to form higher-order factors in the literature and more research was needed to determine the appropriate factor structure depending on the context [42]. Considering that higher-order strategies, such as emotion-focused coping and maladaptive coping have found to be composed of different lower-order coping strategies, it would be suitable to run separate factor analyses and determine the factor structure in the context of PPD, rather than relying on previously defined factors [29]. Thus, in the present study, two steps will be taken. First, we use exploratory and confirmatory factor analysis (CFA) to investigate the factor structure of the coping. Second, we examine the role of coping strategies in mediating the relationships between insecure attachment styles and depression in both antepartum and postpartum period. In this regard, structural equation modelling (SEM) analysis is a suitable statistical method to evaluate the extent to which a third intermediate or mediating variable (coping) explains the effect of a predictor (e.g., attachment insecurity) on an outcome (e.g., depressive symptoms) [43].
Depression is significant at each stage but most reported in the second half of pregnancy and early postnatal period [44,45] The present study aimed to examine the relationship of coping strategies, attachment styles and symptoms of depression that occur in the late pregnancy period (third trimester) and within early postpartum period (day 1–7) as previously reported [45]. Based on the literature revised we hypothesized that: (a) both anxious and avoidant attachment scores respectively would be significantly associated with dysfunctional coping strategies (b) the relationship between anxious and avoidant attachment and perinatal depression would be mediated by use of dysfunctional maladaptive coping strategies.
2. Materials and Methods
The data of this study were collected as part of a previous longitudinal study that assessed the prevalence and risk factors of perinatal depression among pregnant women attending, from July to November 2020, maternal health clinics in three major public hospitals (Ospedali Riuniti di Foggia, Ospedale Vito Fazi di Lecce and Ospedale Di Venere di Bari) of the Regione Puglia (Italy) [46]. The inclusion criteria were being a woman over the age of 18 and in the third trimester of pregnancy. The exclusion criteria included intellectual disability, unwillingness to participating in the study and poor knowledge of language which compromised the ability of the woman to perform the research protocol. All the participants were given verbal and written explanations of the purpose of the study and their informed consent was obtained prior to their participation in the study. During the study period, 1664 eligible women were enrolled and assessed in their third trimester of pregnancy (t0). The same cohort was followed up one week after delivery [47,48]. Sociodemographic characteristics, attachment styles and coping strategies were assessed during the first visit (t0). The characteristics of patients with and without depression were subjected to an analysis using descriptive analysis. T-test was applied for continuous data.
2.1. Edinburg Postnatal Depression Scale
The Italian validated version of the Edinburgh Postnatal Depression Scale (EPDS) [49] was administered twice, once during the antenatal visit and again during a postnatal follow-up. The Edinburgh Postnatal Depression Scale (EPDS) is a 10-item instrument that was developed as a screening tool for postpartum depression and is widely adopted for detection of depression in both antepartum and postpartum samples [50,51,52]. Each item is scored from 0 to 3 and total scores range from 0 to 30 with higher scores indicating a more severe depression. We administered the Italian version of the EPDS which has shown to be a valid tool for detecting maternal antenatal and postnatal episodes of major depression with acceptable internal consistency and test–retest reliability [49,53]. In many validation studies, different cut-off points have been found. It must be acknowledged that the optimal EPDS cut-off scores change considerably during different stages of peripartum period [54,55]. Many studies have suggested an optimal cut off score of the EPDS ≥12/13 in the late pregnancy [56,57]. However, as suggested by Dennis [58] a cut-off score ≥ 9 is usually adopted for identifying patients with major depression, during the early post-partum period [48,59]. Therefore, in this paper, we chose to use a cut of the EPDS ≥12 and a cut off of EPDS ≥ 9 were used, respectively, in the assessment for antepartum depression and depression in the immediate postpartum period to make our findings comparable with findings from both local and international studies. The EPDS t0 and t1 showed internal consistency (Cronbach’s alpha 0.78 and 0.79, respectively).
2.2. Experiences in Close Relationship Scale
The Experiences in Close Relationship Scale (ECR) is one of the most used self-report instruments for the assessment of adult attachment and has been widely adopted in previous studies assessing attachment as a risk factor for antenatal and postpartum depression [60,61,62]. The ECR consists of 36 items, scored on a seven-point Likert scale, with 1 indicating “disagree strongly” and 7 indicating “agree strongly”. It is composed of two subscales, namely attachment Anxiety (concerning rejection or abandonment), and attachment Avoidance (of intimacy and interdependency in close relationships [60]. We employed the Italian version of the ECR [63]. In the current study, the internal consistency was good (Cronbach’s alpha 0.78).
2.3. Coping Orientation for problem Experiences
Coping strategies were assessed with the brief Coping Orientation for Problem Experiences (COPE) which consists of 14 scales: active coping, planning, behavioural disengagement, self-distraction, seeking emotional support, seeking instrumental support, venting of emotions, positive reframing, humour, acceptance, denial, religion, substance use, and self-blame [42]. The model developed by Carver et al. [37] consists of three types of coping strategies: emotion-focused coping, problem-focused coping, and avoidant coping. Problem focused coping strategies, that are aimed at changing the stressful situation, include active coping, seeking instrumental support, planning, and positive reframing. Emotion-focused coping strategies that are aiming to regulate emotions associated with the stressful situation, include venting of emotions, seeking emotional support, humour, acceptance, self-blame, and religion. The third type of coping, avoidance-focused coping, which indicates physical or cognitive efforts to disengage from the stressors, include self-distraction, denial, substance use, and behavioural disengagement [64,65]. We employed the Italian version as provided by Conti [66]. The internal consistency of the total Brief COPE was high (Cronbach’s alpha 0.85). Statistical analyses were performed using the IBM Statistical Package for Social Sciences (SPSS), version 26.0, and AMOS, version 22.0. The data were scanned for missing values and possible multivariate outliers via the Mahalanobis distance, with a criterion of p < 0.001 to remove the participants [67]. The skewness and kurtosis were used to examine the distribution of the data. The linear relationship between independent and dependent variables was examined by Pearson’s correlation. Inflation variance (VIF) and tolerance factors were used to evaluate the multiple alignment between variables. To reduce the number of factors and create a more specific model of coping strategies, we conducted a second-order exploratory factor analysis (EFA) on the subscales of the Brief COPE in two different periods (pregnancy and postpartum). A confirmatory factor analysis (CFA) was performed to validate the results of the EFA. To test our main hypotheses, structural equation modelling (SEM) was applied to test the mediating role of the different higher order coping strategies in the relationship between attachment and perinatal depression at T0 and T1. To analyse the fit of the models, we used the criteria of the Comparative Fit Index, the Root Mean Square Error of Approximation (RMSEA), the Standardized Root Mean Square Residual (SRMR), and the minimum discrepancy per degree of freedom (CMIN/DF), following the recommendations of Schreiber et al. [68]. As recommended in SEM literature [69] alternative models were also tested to eliminate alternative explanations. To confirm the presence of mediation, bootstrapping, with 5000 bootstrap samples, was used to calculate the total, direct and indirect effects of the predictors (attachment styles) on the outcome variables (perinatal depression). The total, direct and indirect effects are reported as estimate with 95% confidence intervals. The level of statistical significance was set at p < 0.05.
3. Results
According to the EPDS score ≥12, 14.1% of the women (234/1664) suffered from depression in pregnancy and, according to the EPDS score ≥9, 18.5% (309/1664) in the postpartum period. 19.4.6% (60/309) of women who had antepartum depression were found to have postpartum depression. Missing values and cases found to be outliers were excluded from the analyses leaving the antepartum total sample in 233 and the postpartum total sample in 287/1351 participants. The descriptive statistics of the study samples are illustrated in Table 1.
Differences between women with and without major depression according to the EPDS scores in all analysed variables in the antepartum and postpartum phase are reported in the Table 2. Therefore, women with depression scored significantly higher in measurements of anxiety and avoidant attachment. The coping strategies with adaptive valence which we find the most often in non-depressed women are coping styles centered on acceptance of the situation in both antepartum and postpartum period. The coping strategies most frequently associated with depression are denial, venting of emotion, self-blame, seeking emotional support and behavioral disengagement.
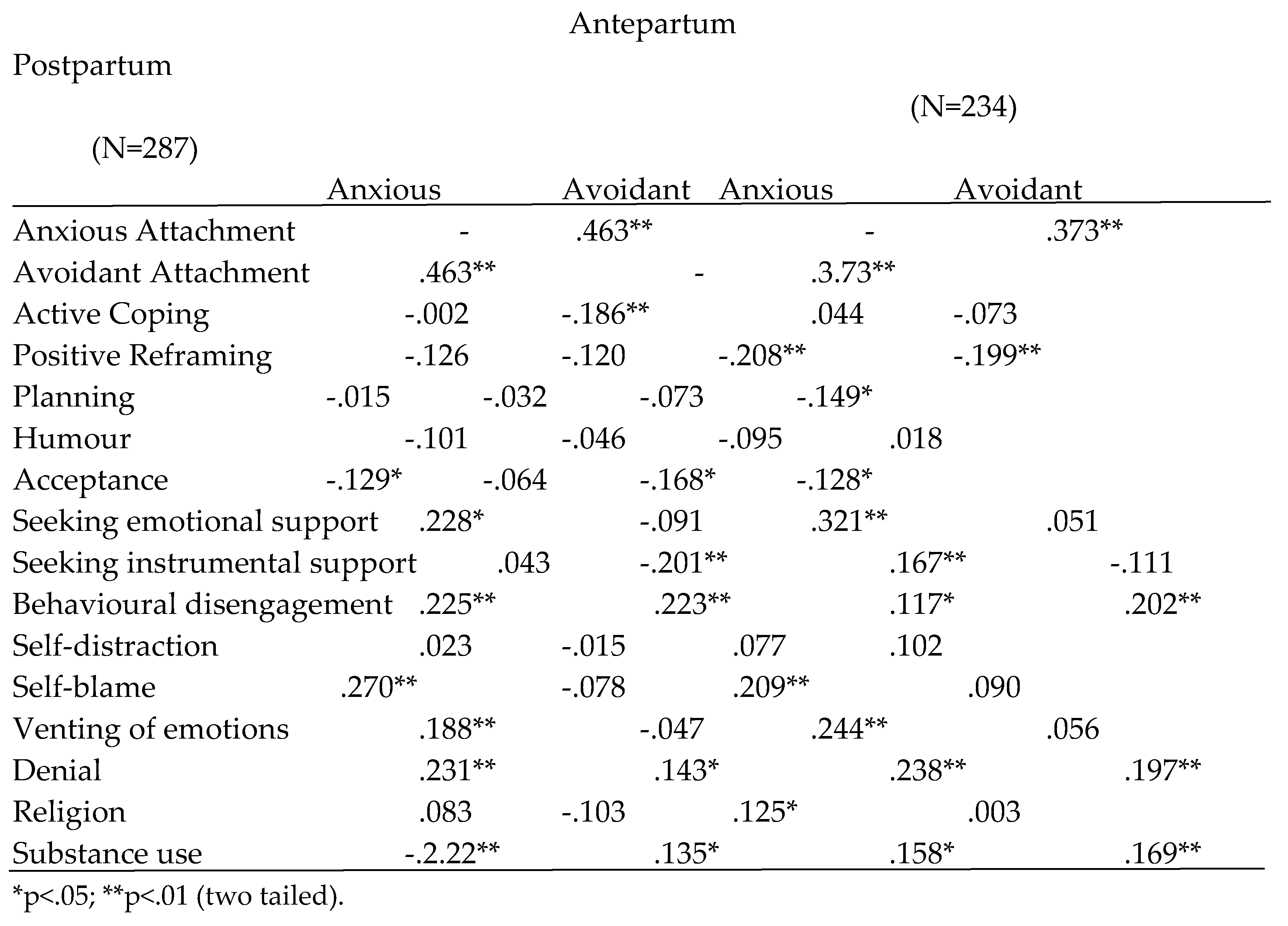
The results of Pearson’s correlations between attachment styles and coping strategies are reported in Table 3. The highest correlation was found between anxious attachment and avoidant attachment. In the prenatal phase anxious attachment was also positively correlated with seeking emotional support and dysfunctional coping strategies such as denial, self-blame, venting of emotion and behavioural disengagement; while avoidant attachment was positively correlated with seeking instrumental support, denial, behavioral disengagement, and substance use. The analysis of coping strategies in the postnatal period is also particularly informative. Anxious attachment was positively correlated with seeking emotional support, seeking instrumental support, venting of emotion, denial, behavioral disengagement, self-blame, religion and substance use; while avoidant attachment was correlated with behavioral disengagement, denial and substance use.
3.1. Exploratory Factor Analysis
An EFA on the subscales of the Brief COPE was performed in two different periods (pregnancy and postpartum) using a principal component analysis and varimax rotation. Eigenvalues of 1.0 were used to determine the number of components extracted. The minimum factor loading was set to 0.50 [70]. The factor solution derived from the EFA in participants with antenatal depression yielded three distinct second-order factors, which accounted for 59.048 per cent of variation in the data. No items showed cross-loadings of 0.50 or above on more than one factor. The Barlett’s test of Sphericity, which provides information about whether the correlations in the data are strong enough to use a dimension-reduction technique such as principal components analysis was significant (χ²(55) = 657.564; p <0.001) [71]. The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy, which indicates the appropriateness of the data for factor analysis, was 0.719 which is well above the acceptable threshold of 0.50 [72,73]. Based on the criteria of factor loadings the resulting factors consisted of the following sub-scales: Factor 1, adaptive coping, includes the scales of active coping, planning, positive reframing, acceptance, and humour. Factor 2, emotional coping, includes the scales of seeking instrumental support, seeking emotional support, venting of emotions and self-blame. Factor 3, maladaptive coping, includes the scales of denial, behavioural disengagement, and substance use. No items cross-loaded on multiple factors with loadings greater than 0.50. Self-distraction and religion did not load above 0.3 in any of the three predicted factors. Therefore, these scales were left out of the analyses. Similar results were found when confirmatory factor analysis was conducted on participants with postpartum depression. The factor structure derived from the EFA yielded three distinct second-order factors, which accounted for 57.541 per cent of variation of the data. The Barlett’s test of Sphericity was significant (χ² (66) = 450.237, p <0.001). The KMO was 0.65. The resulting factors consisted of the following sub-scales: Factor 1, adaptive coping, includes the scales of positive framing, acceptance, planning and humour. Factor 2, emotional coping, includes the scales of seeking instrumental support, seeking emotional support, venting of emotions and self-blame. Factor 3, maladaptive coping, includes the scales of denial and behavioural disengagement. No items cross-loaded on multiple factors with loadings greater than 0.50. Self-distraction and religion and active coping did not load above 0.3 in any of the three predicted factors. Therefore, these scales were excluded from the analyses.
3.2. Confirmatory Factor Analysis
To determine the reliability of the factor structure derived from the EFA, a CFA was applied. An initial test of the three-factor model, derived from the EFA in participants with antepartum depression, indicated a less than acceptable fit with the following parameters: CMIN/DF = 3.027; CFI = 0.831, RMSEA = 0.098, SRMR = 0.082, The examination of the standardized residuals and modification indices suggested to permit the correlation of errors between planning and active coping, reframing and humour; venting and self-blame, instrumental support and self-blame, denial and substance. This new model resulted in: CMIN/DF = 2.388, CFI = 0.908, RMSEA = 0.07, and SRMR = 0.064, meeting all the fitting criteria. The definitive three-factor model reached a much better fit than the three-factor model that distinguishes problem focused coping, emotional focused coping, and avoidant coping [37]: CMIN/DF = 4.559, CFI = 0.63, RMSEA = 0.125, and SRMR = 0.114. Similar results were obtained testing the three-factor model derived from the EFA in participants with postpartum depression. The initial test indicated a poor fit: CMIN/DF = 3.319, CFI = 0.804, RMSA =0.086, SRMR = 0.078. Modification indices suggested adding covariances between seeking instrumental support and seeking emotion, seeking instrumental support and self-blame, humour and acceptance, humour and positive reframing. The model reached an excellent fit index: CMIN/DF =2.040, CFI =0.95, RMSEA ==.059, SRMR = 0.053. This definitive model showed a much better fit than the three-factor model that distinguishes problem focused coping, emotional focused coping, and dysfunctional coping: CMIN/DF = 3.632, CFI = 0.71, RMSEA = 0.106, and SRMR = 0.109.
3.3. SEM Analysis
Prior to the analysis, the assumptions of SEM including normal distribution and multiple alignment were examined. We assessed the distribution of all variables and transformed those variables that showed strong non-normality. Log transformation was used of EPDS postpartum, and substance use scores. All the other variables are normally distributed [74]. There was no alignment between the variables (VIF amplitude was less than 10 and tolerance was higher than 0.1). To analyse the mediation effects of coping strategies on the relationship between attachment styles and peripartum depression the three second-order factors, identified during the CFA, were used in the structural equation modelling (SEM) analysis. Due to the complexity of the models only the higher-order coping strategies were estimated as latent factors. For all other constructs in the model the factor scores were used as manifest variables.
3.3.1. SEM Antepartum Depression
The first model, which investigated the role of coping strategies in mediating the relationship between attachment styles and ante-partum depression, consisted of two independent variables (Avoidance attachment and Anxiety attachment), three intermediate variables (adaptive, emotional, and maladaptive coping) and the dependent variable (ante-partum mood symptoms) based on EPDS score ≥12. The first model did not reach any acceptable fit indices at this point (CMIN/DF = 7.81, CFI = 0.800, RMSEA = 0.097, SRMR = 0.103). To create a more parsimonious model, non-significant paths (attachment avoidant path to the maladaptive coping and the path of anxious attachment to ante-partum depression and to active coping) were eliminated stepwise. Next, modification indices suggested to allow the error terms of instrumental support and blame, instrumental support and emotional support, substance use and denial, humour and reframing, planning and active coping to covariate. This new model reached acceptable fit indices (CMIN/DF = 2.19, CFI = 0.894, RMSEA = 0.071, SRMR = 0.065) [70,75]. All regressions were statistically significant (p<0.01). A diagrammatic representation of the structural models is presented in Figure 1. Results showed that anxious attachment was positively associate with both maladaptive coping and emotive coping strategies. Avoidant attachment was associated with ante-partum depression, and less emotive coping strategies. Emotional coping strategies were positively associated with ante-partum depressive symptoms, while active coping strategies were negatively associated with postpartum depressive symptoms. Maladaptive coping was not associated with post-partum depressive symptoms. To further confirm the specificity of coping strategies as mediators of these relations, based on existing literature findings [76] an alternative model was also tested whereby ante-partum depression was included as the mediator variable, and coping strategies as the outcome variables. This model was nonsignificant (CMIN/DF=3.224, CFI=78.1, RMSEA=0.098, SRMR=0.0874). In summary, structural equation modelling identified a significant mediational effect of emotional and maladaptive coping strategies on the relation between anxiety attachment and ante-partum depression. Results showed a significant mediational effect of emotional coping strategies on the relationship between avoidant attachment and ante-partum depression. Results from bootstrapping analysis confirmed a mediating effect of emotional and maladaptive coping strategies on the relationships between anxious attachment and ante-partum depression (two-tailed significance bias-corrected, p=0.005; 95% confidence interval 0.01 to 0.04). Moreover, results confirmed a mediating effect of maladaptive coping strategies on the relationships between avoidant attachment and ante-partum depression (95% confidence interval -0.03 to -0.04; two-tailed significance bias-corrected p=0.002.
3.3.2. SEM Postpartum Depression
The second model, which investigated the mediating role of coping strategies between attachment styles and postpartum depression consisted of two independent variables (Avoidance attachment and Anxiety attachment), three intermediate coping factors (adaptive, emotional, and passive coping) and the dependent variable (postpartum depression) based on EPDS score ≥9. An initial test of the model resulted in poor model fit (CMIN/DF =3.598, CFI = 0.805, RMSEA =0.095, SRMR = 0.073). To achieve adequate fit, all non-significant paths were eliminated one at a time from the initial model to evaluate a more parsimonious model with fewer paths. The investigation of modification indices suggested adding covariances between humour and acceptance, humour, and planning, blame and venting, seeking instrumental support and seeking emotional support. Results of the final model revealed a satisfactory fit (CMIN/DF = 2.676, CFI = 0.874, RMSEA =0.077, SRMR = 0.650). All regressions were statistically significant (p<0.01). The path coefficients are shown in Figure 2. Anxious attachment style was positively associated with emotive coping and maladaptive coping and negatively associated with active coping. Avoidant attachment style was associated with maladaptive coping. The relationships between emotional coping, active coping and postpartum depression were comparable to those found in the previous antepartum model. Results showed that emotional coping strategies were positively associated, and active coping strategies were negatively associated with post-partum depressive symptoms, respectively. Maladaptive coping was not associated with post-partum depressive symptoms indicating that it did not serve any significant mediating role in the relationship between attachment styles and post-partum depression. The alternative model with post-partum depression and coping strategies swapped (with post-partum as mediator and coping strategies as the dependent variables) was nonsignificant (CMIN =3.821, CFI = 0.784, RMSA = 0.099, SRMR = 0.945). In summary, structural equation modelling identified a significant mediational effect of emotional coping and less active coping strategies on the relation between anxiety attachment and post-partum depression. Results from bootstrapping analysis confirmed a mediating effect of emotional and active coping strategies on the relationships between anxious attachment and post-partum depression (95% confidence interval 0.0 to 0.01; two-tailed significance bias-corrected p=0.005).
4. Discussion
This study was the first to test a model whereby the relationship between attachment styles and depression are mediated by coping strategies, in both antepartum and postpartum periods. The main result of the study is that attachment characteristics had a greater predictive power on depressive symptoms when its direct and indirect statistical effects are taken into consideration. As expected, based on based on past evidence [4,26,27,77], preliminary analyse showed strong correlations between independent variables (Avoidance attachment and Anxiety attachment), intermediate variables (coping strategies) and the dependent variables (perinatal depression outcomes), laying the groundwork for mediation analysis [78]. First, we found supporting evidence of three-factor structure of the coping strategies using the Brief COPE questionnaire, identifying three groups of coping strategies (i.e., active coping, maladaptive coping, and emotional coping) in both antepartum and postpartum samples [42]. The fact that the higher-order factor that we denominated emotional coping encompassed seeking emotional and instrumental support was in line with the studies by Carver [42] and Farley et al. [79], concerning the Brief COPE. Second, we examined the role of these three high-order factors of coping in mediating the relationship between attachment dimensions and antenatal or postnatal depressive symptoms. The results of SEM analyses revealed that the hypothesized models of this study had a good fit in the study samples. Although past research has consistently identified linear relations between dimensions of insecure attachment styles and peripartum depression [5], in the current we show that coping strategies play a significant role in mediating the effect of anxious and avoidant attachment styles on depressive symptomatology. Moreover, we show that different dimensions of attachment styles and dysfunctional coping strategies were associated with either antepartum or postpartum depressive symptoms. In line with previous studies, the results indicated that, besides the direct effect of avoidant attachment on antepartum symptoms, the effect of insecure attachment styles (anxious and avoidant attachment) on antepartum depressive symptomatology was partially mediated by emotional coping styles. Anxious attachment has also an indirect significant effect on postpartum depression through emotional coping; however, avoidant attachment does not seem to be significantly related to postpartum depression [80,81,82,83].
5. Antepartum Depression
The results of mediational analyses revealed that anxious attachment style was significantly associated with antepartum depressive symptomatology through emotional and maladaptive coping strategies. These results are in line with previous literature indicating that the relation between anxious attachment and psychological distress, including depressive symptomatology, is not simply a direct linear relationship; rather, coping plays an important role in mediating this relationship [28,30]. Regarding relations between anxious attachment and coping strategies the present study shows that anxiously attached individuals use more ineffective maladaptive coping strategies (i.e., denial, substance use, behavioral disengagement) and emotional coping strategies (i.e., self-blame, seeking instrumental support, seeking emotional support, venting of emotions) compared to the effective ones. These findings are in line with previous studies revealing that those individuals with anxious attachment use emotion-focused, and maladaptive coping strategies more frequently when dealing with stresses [80,81,82]. As emotion-focused coping strategies are most often used when the individuals perceive the stressor as something that cannot be altered, and must be endured, we assume that women with anxious attachment utilized these strategies to lessen the emotional distress associated with the pregnancy and post-partum [6]. Additionally, as people with attachment anxiety reported high levels of alienation and tend to be withdrawal these individuals might also endorse increased use of a variety of coping strategies, including dysfunctional coping such as maladaptive coping strategies [83].
Avoidant attachment style showed both a direct effect on antenatal depressive symptoms and an indirect effect through emotional coping. Our findings are consistent with that of a previous study showing that attachment avoidance has both a direct effect on indices of psychological distress and an indirect effect through ineffective problem coping styles [30]. Early studies reported that attachment avoidance failed to significantly predict distress after attachment anxiety was controlled for [28,29]. However, our results, in line with previous research [30], showed that attachment avoidance predicted antenatal depression even after we controlled for the respective other attachment dimension. In considering the relationship between attachment and coping the findings of the present study indicate a strong correlation between avoidant attachment style and emotional coping. As higher levels of attachment avoidance correspond to a lesser acknowledgment of distress and are related to a more discomfort in expressing difficulties to others [84], the observed positive correlation was unexpected. However, several emotional coping strategies, specifically self-blame and venting, are intended to relieve the psychological distress, without necessarily engaging with and relying on others for support [37]. Therefore, it is possible that this unexpectedly positive correlation found between emotional coping and attachment avoidance was greatly driven by these less functional strategies. It is also possible that as those with avoidant attachment are skeptical of trust in relationships and find it difficult to depend on others, they necessarily engaged in more emotional coping strategies [85].
6. Postpartum Depression
Our findings indicate that emotional coping and less use of active coping strategies mediate the relations between anxious attachment and postpartum depression, while the effects of avoidant attachment were not significant. The results are consistent with previous studies [4,5] showing that anxious style was found to be associated with postpartum depression more frequently than avoidant style of attachment. Similarly, in the related literature, it is acknowledged that there is a significant and positive correlation between anxious attachment and perceived stress; however, avoidant attachment does not seem to be significantly related to stress symptoms [86,87,88,89]. This is in line with the observations, as discussed above, that persons with attachment avoidance tend not to acknowledge their distress [81,90]. The fact that avoidant attachment style had a significant and direct effect on antepartum depression, but it did not have any significant effect on postpartum depression may be indicative of the heterogeneous nature of the avoidant attachment style which encompasses both a positive sense and negative of self. It is also possible that those with avoidant attachment experiencing a greater level of perceived stress during postpartum period, reported greater utilization of avoidant coping strategies to distance themselves from actively processing and/or resolving the distress. It is noteworthy, indeed, that avoidant attachment style was strongly correlated with maladaptive coping, including self-distraction, behavioral disengagement, and denial. As prior research has demonstrated a significative significant association between maladaptive coping and perinatal depression [3,11], it was expected that these coping strategies would mediate the relationship between avoidant attachment and post-partum depressive symptomatology. One possible reason for this inconsistency is that structural equation modelling used in the present study is potentially more powerful and less susceptible to bias than the regression methods used in other studies. These results may be also due to a stronger conceptualization and measurement of coping strategies.
The findings regarding anxious attachment are consistent with the findings reported in previous studies showing a strong association between anxious attachment styles with postnatal depression [4,5]. We extended these original observations by providing evidence that anxious attachment has an indirect significant effect on postpartum depressive symptoms through ineffective coping strategies (e.g., emotional coping). These results confirm analyses reported in other earlier studies revealing patterns of the relationship between anxious attachment styles and way of coping with difficult situations [28,30].
There are several limitations to the study that are important to note. First, data were collected through self-assessment questionnaires, which can reduce the validity of the results. Even so, the questionnaire we used in the current study are reliable and widely accepted instrument for research purposes. Moreover, although a validated measure was used to assess attachment styles, the study could have been strengthened by the use of multiple attachment measures to operationalize insecure attachment styles. Second, the cross-sectional nature of this study also limited its ability to thoroughly interpret the relationship between attachment styles and perinatal depression outcomes through coping strategies. Longitudinal studies could provide a more rigorous evaluation of these associations. Third, although the results are based on SEM, a more complex model than previously used in the literature, the results are based on correlational data. Therefore, it is not possible to draw any firm conclusions about the causal relationships among the variables. Despite these limitations, our findings suggest that attachment styles (especially anxious attachment) associated with a greater use of ineffective coping strategies have meaningful predictor power in explaining perinatal depression. Further research is needed to continue to explore the relationships between attachment and stress reactions as mediated by coping strategies. This would help a preventive coping-based intervention strategy to enhance the capacity of women with insecure attachment styles to use more adaptive coping during and after pregnancy.
Author Contributions
Conceptualization, A.B and L.N.; methodology, A.P. and M.S; formal analysis, A.M and I.L.; investigation, A.V. and M.S.; data curation, L.D., L.F. F.G, S.B; writing—original draft preparation, A.M.; writing—review and editing, I.L.; visualization, G.M. and A.B.; supervision, G.M; funding acquisition, A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Department of Health Promotion of the Regione Puglia, Italy.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Regione Puglia with two special deliberations: “DGR n. 1392 released on 2 August 2018 and DGR n. 2294 released on 11 December 2018.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are openly available in FigShare at doi: 10.6084/m9.figshare.23100746.
Acknowledgments
The authors would like to thank dr. Giovanni Gentile for his help with statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Gavin, I.N. , Gaynes N.B, Lohr N.K, Meltzer-Brody S., Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence. Obstetrics & Gynecology. 2005; 106 (5 Part 1):1071-83. [CrossRef]
- Langan, R.; Goodbred, A.J. Identification and Management of Peripartum Depression. American family physician 2016, 93, 852–8. [Google Scholar]
- Gutiérrez-Zotes, A.; Labad, J.; Martín-Santos, R.; García-Esteve, L.; Gelabert, E.; Jover, M.; Guillamat, R.; Mayoral, F.; Gornemann, I.; Canellas, F.; et al. Coping Strategies and Postpartum Depressive Symptoms: a Structural Equation Modelling Approach. Eur. Psychiatry 2015, 30, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Warfa, N.; Harper, M.; Nicolais, G.; Bhui, K. Adult attachment style as a risk factor for maternal postnatal depression: a systematic review. BMC Psychol. 2014, 2, 56. [Google Scholar] [CrossRef] [PubMed]
- Bianciardi, E.; Vito, C.; Betrò, S.; De Stefano, A.; Siracusano, A.; Niolu, C. The anxious aspects of insecure attachment styles are associated with depression either in pregnancy or in the postpartum period. Ann. Gen. Psychiatry 2020, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R. , Folkman, S. Stress, Appraisal, and Coping. Springer. New York, 1984.
- Da Costa, D.; Larouche, J.; Dritsa, M.; Brender, W. Psychosocial correlates of prepartum and postpartum depressed mood. J. Affect. Disord. 2000, 59, 31–40. [Google Scholar] [CrossRef] [PubMed]
- de Tychey, C.; Spitz, E.; Briançon, S.; Lighezzolo, J.; Girvan, F.; Rosati, A.; Thockler, A.; Vincent, S. Pre- and postnatal depression and coping: a comparative approach. J. Affect. Disord. 2005, 85, 323–326. [Google Scholar] [CrossRef]
- Honey, K. Predicting postnatal depression. J. Affect. Disord. 2003, 76, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Faisal-Cury, A.; Tedesco, J.J.A.; Kahhale, S.; Menezes, P.R.; Zugaib, M. Postpartum depression: in relation to life events and patterns of coping. Arch. Women’s Ment. Heal. 2004, 7, 123–131. [Google Scholar] [CrossRef]
- Gutiérrez-Zotes, A.; Labad, J.; Martín-Santos, R.; García-Esteve, L.; Gelabert, E.; Jover, M.; Guillamat, R.; Mayoral, F.; Gornemann, I.; Canellas, F.; et al. Coping strategies for postpartum depression: a multi-centric study of 1626 women. Arch. Women’s Ment. Heal. 2015, 19, 455–461. [Google Scholar] [CrossRef]
- Guardino, C.M.; Schetter, C.D. Coping during pregnancy: a systematic review and recommendations. Heal. Psychol. Rev. 2013, 8, 70–94. [Google Scholar] [CrossRef]
- Ren, J.; Jiang, X.; Yao, J.; Li, X.; Liu, X.; Pang, M.; Chiang, C.L.V. Depression, Social Support, and Coping Styles among Pregnant Women after the Lushan Earthquake in Ya’an, China. PLOS ONE 2015, 10, e0135809. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Smith, A.; Rattan, S.L. Application of a stress and coping model to antenatal depressive symptomatology. Psychol. Heal. Med. 2007, 12, 266–277. [Google Scholar] [CrossRef]
- Chen, Z.; Li, Y.; Chen, J.; Guo, X. The mediating role of coping styles in the relationship between perceived social support and antenatal depression among pregnant women: a cross-sectional study. BMC Pregnancy Childbirth 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Besser, A.; Priel, B. Trait vulnerability and coping strategies in the transition to motherhood. Curr. Psychol. 2003, 22, 57–72. [Google Scholar] [CrossRef]
- Robakis, T.K.; Zhang, S.; Rasgon, N.L.; Li, T.; Wang, T.; Roth, M.C.; Humphreys, K.L.; Gotlib, I.H.; Ho, M.; Khechaduri, A.; et al. Epigenetic signatures of attachment insecurity and childhood adversity provide evidence for role transition in the pathogenesis of perinatal depression. Transl. Psychiatry 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and loss: Vol. 1. Attachment (2nd.ed.). Basic Books. New York, NY: (1969/1982).
- Bowlby, J. Attachment and loss: Vol. 2. Separation. Basic Books. New York, NY: (1973).
- Bowlby, J. Attachment and loss: Vol. 3. Loss. Basic Books. New York, NY: (1980).
- Sherman, L.J.; Rice, K.; Cassidy, J. Infant capacities related to building internal working models of attachment figures: A theoretical and empirical review. Dev. Rev. 2015, 37, 109–141. [Google Scholar] [CrossRef]
- Bretherton, I. New perspectives on attachment relations: Security, communication, and internal working models. In J. Osofsky (Ed.), Handbook of infant development. New York: Wiley. 1987 (pp. 1061-1100).
- Brennan K., A. , Clark C.L., Shaver P. R. Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships. Guilford Press. New York, NY. 1998 (pp. 46-76).
- Jinyao, Y.; Xiongzhao, Z.; Auerbach, R.P.; Gardiner, C.K.; Lin, C.; Yuping, W.; Shuqiao, Y. INSECURE ATTACHMENT AS A PREDICTOR OF DEPRESSIVE AND ANXIOUS SYMPTOMOLOGY. Depression Anxiety 2012, 29, 789–796. [Google Scholar] [CrossRef]
- Dagan, O.; Facompré, C.R.; Bernard, K. Adult attachment representations and depressive symptoms: A meta-analysis. J. Affect. Disord. 2018, 236, 274–290. [Google Scholar] [CrossRef]
- Bifulco, A.; Moran, P.M.; Ball, C.; Bernazzani, O. Adult attachment style. I: Its relationship to clinical depression. Chest 2002, 37, 50–59. [Google Scholar] [CrossRef]
- Ikeda, M.; Hayashi, M.; Kamibeppu, K. The relationship between attachment style and postpartum depression. Attach. Hum. Dev. 2014, 16, 557–572. [Google Scholar] [CrossRef]
- Lopez, F.G.; Mauricio, A.M.; Gormley, B.; Simko, T.; Berger, E. Adult Attachment Orientations and College Student Distress: The Mediating Role of Problem Coping Styles. J. Couns. Dev. 2001, 79, 459–464. [Google Scholar] [CrossRef]
- Lopez, F.G.; Mitchell, P.; Gormley, B. Adult attachment orientations and college student distress: Test of a mediational model. J. Couns. Psychol. 2002, 49, 460–467. [Google Scholar] [CrossRef]
- Wei, M.; Heppner, P.P.; Mallinckrodt, B. Perceived coping as a mediator between attachment and psychological distress: A structural equation modeling approach. J. Couns. Psychol. 2003, 50, 438–447. [Google Scholar] [CrossRef]
- Howard, M.S.; Medway, F.J. Adolescents’ attachment and coping with stress. Psychol. Sch. 2004, 41, 391–402. [Google Scholar] [CrossRef]
- Birnbaum, G.E.; Orr, I.; Mikulincer, M.; Florian, V. When Marriage Breaks Up-Does Attachment Style Contribute to Coping and Mental Health? J. Soc. Pers. Relationships 1997, 14, 643–654. [Google Scholar] [CrossRef]
- Mikulincer, M.; Florian, V.; Weller, A. Attachment styles, coping strategies, and posttraumatic psychological distress: The impact of the Gulf War in Israel. J. Pers. Soc. Psychol. 1993, 64, 817–826. [Google Scholar] [CrossRef]
- Buelow, S.A.; Lyddon, W.J.; Johnson, J.T. Client attachment and coping resources. Couns. Psychol. Q. 2002, 15, 145–152. [Google Scholar] [CrossRef]
- Mikulincer, M. , Florian V. The relationship between adult attachment styles and emotional and cognitive reactions to stressful events. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships. The Guilford Press. 1998 (pp. 143–165).
- Schmidt, S.; Nachtigall, C.; Wuethrich-Martone, O.; Strauss, B. Attachment and coping with chronic disease. J. Psychosom. Res. 2002, 53, 763–773. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Carver, C.S.; Connor-Smith, J. Personality and Coping. Annu. Rev. Psychol. 2010, 61, 679–704. [Google Scholar] [CrossRef]
- Moos, R.H. Schaefer J.A. Coping Resources and Processes: Current Concepts and Measures. In: Goldberger, L. and Breznitz, S., Eds., Handbook of Stress: Theoretical and Clinical Aspects, 2nd Edition, The Free Press, New York, 1993 (pp 234-257).
- Roth, S.; Cohen, L.J. Approach, avoidance, and coping with stress. Am. Psychol. 1986, 41, 813–819. [Google Scholar] [CrossRef]
- Skinner, E.A.; Edge, K.; Altman, J.; Sherwood, H. Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychol. Bull. 2003, 129, 216–269. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Moya, E.; Mzembe, G.; Mwambinga, M.; Truwah, Z.; Harding, R.; Ataide, R.; Larson, L.M.; Fisher, J.; Braat, S.; Pasricha, S.; et al. Prevalence of early postpartum depression and associated risk factors among selected women in southern Malawi: a nested observational study. BMC Pregnancy Childbirth 2023, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- McCauley, M.; White, S.; Bar-Zeev, S.; Godia, P.; Mittal, P.; Zafar, S.; Broek, N.v.D. Physical morbidity and psychological and social comorbidities at five stages during pregnancy and after childbirth: a multicountry cross-sectional survey. BMJ Open 2022, 12, e050287. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, A.; Severo, M.; Petito, A.; Nappi, L.; Iuso, S.; Altamura, M.; Marconcini, A.; Giannaccari, E.; Maruotti, G.; Palma, G.L.; et al. Perinatal depression screening and prevention: Descriptive findings from a multicentric program in the South of Italy. Front. Psychiatry 2022, 13, 962948. [Google Scholar] [CrossRef]
- Maliszewska, K.; Bidzan, M.; Świątkowska-Freund, M.; Preis, K. Personality type, social support and other correlates of risk for affective disorders in early puerperium. Ginekol. Polska 2016, 87, 814–819. [Google Scholar] [CrossRef]
- Dennis, C.E.; Janssen, P.A.; Singer, J. Identifying women at-risk for postpartum depression in the immediate postpartum period. Acta Psychiatr. Scand. 2004, 110, 338–346. [Google Scholar] [CrossRef]
- Benvenuti, P.; Ferrara, M.; Niccolai, C.; Valoriani, V.; Cox, J.L. The Edinburgh Postnatal Depression Scale: validation for an Italian sample. J. Affect. Disord. 1999, 53, 137–141. [Google Scholar] [CrossRef]
- Bergink, V.; Kooistra, L.; Lambregtse-van den Berg, M.P.; Wijnen, H.; Bunevicius, R.; van Baar, A.; Pop, V. Validation of the Edinburgh Depression Scale during pregnancy. J. Psychosom. Res. 2011, 70, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.; Carothers, A.D. The Validation of the Edinburgh Post-natal Depression Scale on a Community Sample. Br. J. Psychiatry 1990, 157, 288–290. [Google Scholar] [CrossRef]
- Boyd, R.C. , Le H.N., Somberg R. Review of screening instruments for postpartum depression. Arch Womens Ment Health. 2005; 8:141-53. [CrossRef]
- Cena, L.; Mirabella, F.; Palumbo, G.; Gigantesco, A.; Trainini, A.; Stefana, A. Prevalence of maternal antenatal and postnatal depression and their association with sociodemographic and socioeconomic factors: A multicentre study in Italy. J. Affect. Disord. 2020, 279, 217–221. [Google Scholar] [CrossRef]
- Su, K.-P.; Chiu, T.-H.; Huang, C.-L.; Ho, M.; Lee, C.-C.; Wu, P.-L.; Lin, C.-Y.; Liau, C.-H.; Liao, C.-C.; Chiu, W.-C.; et al. Different cutoff points for different trimesters? The use of Edinburgh Postnatal Depression Scale and Beck Depression Inventory to screen for depression in pregnant Taiwanese women. Gen. Hosp. Psychiatry 2007, 29, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Kozinszky, Z.; Dudas, R.B. Validation studies of the Edinburgh Postnatal Depression Scale for the antenatal period. J. Affect. Disord. 2015, 176, 95–105. [Google Scholar] [CrossRef]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.K.; Kim, J.J.; Park, Y.G.; Ko, H.S.; Park, I.Y.; Shin, J.C. The Simplified Edinburgh Postnatal Depression Scale (EPDS) for Antenatal Depression: Is It a Valid Measure for Pre-Screening? Int. J. Med Sci. 2012, 9, 40–46. [Google Scholar] [CrossRef]
- Dennis, C.-L. Can we identify mothers at risk for postpartum depression in the immediate postpartum period using the Edinburgh Postnatal Depression Scale? J. Affect. Disord. 2004, 78, 163–169. [Google Scholar] [CrossRef]
- Tanuma-Takahashi, A.; Tanemoto, T.; Nagata, C.; Yokomizo, R.; Konishi, A.; Takehara, K.; Ishikawa, T.; Yanaihara, N.; Samura, O.; Okamoto, A. Antenatal screening timeline and cutoff scores of the Edinburgh Postnatal Depression Scale for predicting postpartum depressive symptoms in healthy women: a prospective cohort study. BMC Pregnancy Childbirth 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Brennan, K.A. , Clark C.L., Shaver P.R. Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson &W. S. Rholes (Eds.), Attachment theory and close relationships New York: Guilford. 1998 (pp. 46–76).
- Iles, J.; Slade, P.; Spiby, H. Posttraumatic stress symptoms and postpartum depression in couples after childbirth: The role of partner support and attachment. J. Anxiety Disord. 2011, 25, 520–530. [Google Scholar] [CrossRef]
- Marques, R.; Monteiro, F.; Canavarro, M.C.; Fonseca, A. The role of emotion regulation difficulties in the relationship between attachment representations and depressive and anxiety symptoms in the postpartum period. J. Affect. Disord. 2018, 238, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Picardi, A. , Vermigli P., Toni A., D’Amico R., Bitetti D., Pasquini P. Il questionario “experiences in close relationships” (ECR) per la valutazione dell’attaccamento negli adulti: Ampliamento delle evidenze di validità per la versione italiana. Ital J Psychopathol. 2002; 8:282–94.
- Dias, C.; Cruz, J.F.; Fonseca, A.M. The relationship between multidimensional competitive anxiety, cognitive threat appraisal, and coping strategies: A multi-sport study. Int. J. Sport Exerc. Psychol. 2012, 10, 52–65. [Google Scholar] [CrossRef]
- Poulus, D.; Coulter, T.J.; Trotter, M.G.; Polman, R. Stress and Coping in Esports and the Influence of Mental Toughness. Front. Psychol. 2020, 11, 628. [Google Scholar] [CrossRef]
- Conti, L. Repertorio delle scale di valutazione in psichiatria. Firenze: SEE Firenze. (2000).
- Tabachnick, B.G. , Fidell L.S. Using multivariate statistics (7th ed.). Pearson. (2018).
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Boateng, S.L. Structural equation modelling made easy: for business and social science research using SPSS and AMOS. Washington: independently published. (2018).
- Hair, J.F. , Black W.C., Babin B.J., Anderson, R.E. Multivariate Data Analysis (7th edition). New Jersey: Prentice Hall. (2010).
- Bartlett, M.S. THE EFFECT OF STANDARDIZATION ON A χ2 APPROXIMATION IN FACTOR ANALYSIS. Biometrika 1951, 38, 337–344. [Google Scholar] [CrossRef]
- Norusis, M. SPSS 16.0 Advanced Statistical Procedures Companion; Prentice Hall Press: Upper Saddle River, NJ, USA, 2008. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage: Newcastle upon Tyne, UK, 2013. [Google Scholar]
- Byrne, B. M. Structural equation modeling with AMOS: Basic concepts, applications, and programming. New York: Routledge. (2010).
- Schumacker, R.E. , Lomax R.G. A Beginner’s Guide to Structural Equation Modeling (4th Ed.). New York: Routledge. (2016).
- Azale, T.; Fekadu, A.; Medhin, G.; Hanlon, C. Coping strategies of women with postpartum depression symptoms in rural Ethiopia: a cross-sectional community study. BMC Psychiatry 2018, 18, 41. [Google Scholar] [CrossRef] [PubMed]
- Monk, C.; Leight, K.L.; Fang, Y. The relationship between women’s attachment style and perinatal mood disturbance: implications for screening and treatment. Arch. Women’s Ment. Heal. 2008, 11, 117–129. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Farley, T.; Galves, A.; Dickinson, L.M.; Perez, M.d.J.D. Stress, Coping, and Health: A Comparison of Mexican Immigrants, Mexican-Americans, and Non-Hispanic Whites. J. Immigr. Minor. Heal. 2005, 7, 213–220. [Google Scholar] [CrossRef]
- Mikulincer, M.; Florian, V. Appraisal of and Coping with a Real-Life Stressful Situation: The Contribution of Attachment Styles. Pers. Soc. Psychol. Bull. 1995, 21, 406–414. [Google Scholar] [CrossRef]
- Vogel, D.L.; Wei, M. Adult Attachment and Help-Seeking Intent: The Mediating Roles of Psychological Distress and Perceived Social Support. J. Couns. Psychol. 2005, 52, 347–357. [Google Scholar] [CrossRef]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef] [PubMed]
- Guttmann-Steinmetz, S.; Crowell, J.A. Attachment and Externalizing Disorders: A Developmental Psychopathology Perspective. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Hazan, C.; Shaver, P. Romantic love conceptualized as an attachment process. J. Personal. Soc. Psychol. 1987, 52, 511–524. [Google Scholar] [CrossRef]
- Perrine, R.M. Stress and college persistence as a function of attachment style Journal of the First Year Experience and Students in Transition. 1: 11, 1999. [Google Scholar]
- Elwood, L.S.; Williams, N.L. PTSD–Related Cognitions and Romantic Attachment Style as Moderators of Psychological Symptoms in Victims of Interpersonal Trauma. J. Soc. Clin. Psychol. 2007, 26, 1189–1209. [Google Scholar] [CrossRef]
- Fortuna, K.; Roisman, G.I. Insecurity, stress, and symptoms of psychopathology: contrasting results from self-reports versus interviews of adult attachment. Attach. Hum. Dev. 2008, 10, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Hankin, B.L.; Kassel, J.D.; Abela, J.R.Z. Adult Attachment Dimensions and Specificity of Emotional Distress Symptoms: Prospective Investigations of Cognitive Risk and Interpersonal Stress Generation as Mediating Mechanisms. Pers. Soc. Psychol. Bull. 2005, 31, 136–151. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Nolan, R.P.; Hunter, J.J.; Tannenbaum, D.W. The relationship of attachment insecurity to subjective stress and autonomic function during standardized acute stress in healthy adults. J. Psychosom. Res. 2006, 60, 283–290. [Google Scholar] [CrossRef]
- Collins, N.L. Working models of attachment: Implications for explanation, emotion, and behavior. J. Pers. Soc. Psychol. 1996, 71, 810–832. [Google Scholar] [CrossRef]
Figure 1.
Path analysis model of the mediating role of coping in the relationship between attachment styles and antepartum depression. Hum=Humour; Refr=Reframing; Acc=Acceptance; Plan=Planning; Act=Active coping; Sub = Substance Use; Den=Denial; Dis=Behavioral Disengagement; Bla=Sefl-Blame; Instr=Seeking Instrumental Support; Emot=Seeking Emotional Support; Vent=Venting of Emotions.
Figure 1.
Path analysis model of the mediating role of coping in the relationship between attachment styles and antepartum depression. Hum=Humour; Refr=Reframing; Acc=Acceptance; Plan=Planning; Act=Active coping; Sub = Substance Use; Den=Denial; Dis=Behavioral Disengagement; Bla=Sefl-Blame; Instr=Seeking Instrumental Support; Emot=Seeking Emotional Support; Vent=Venting of Emotions.
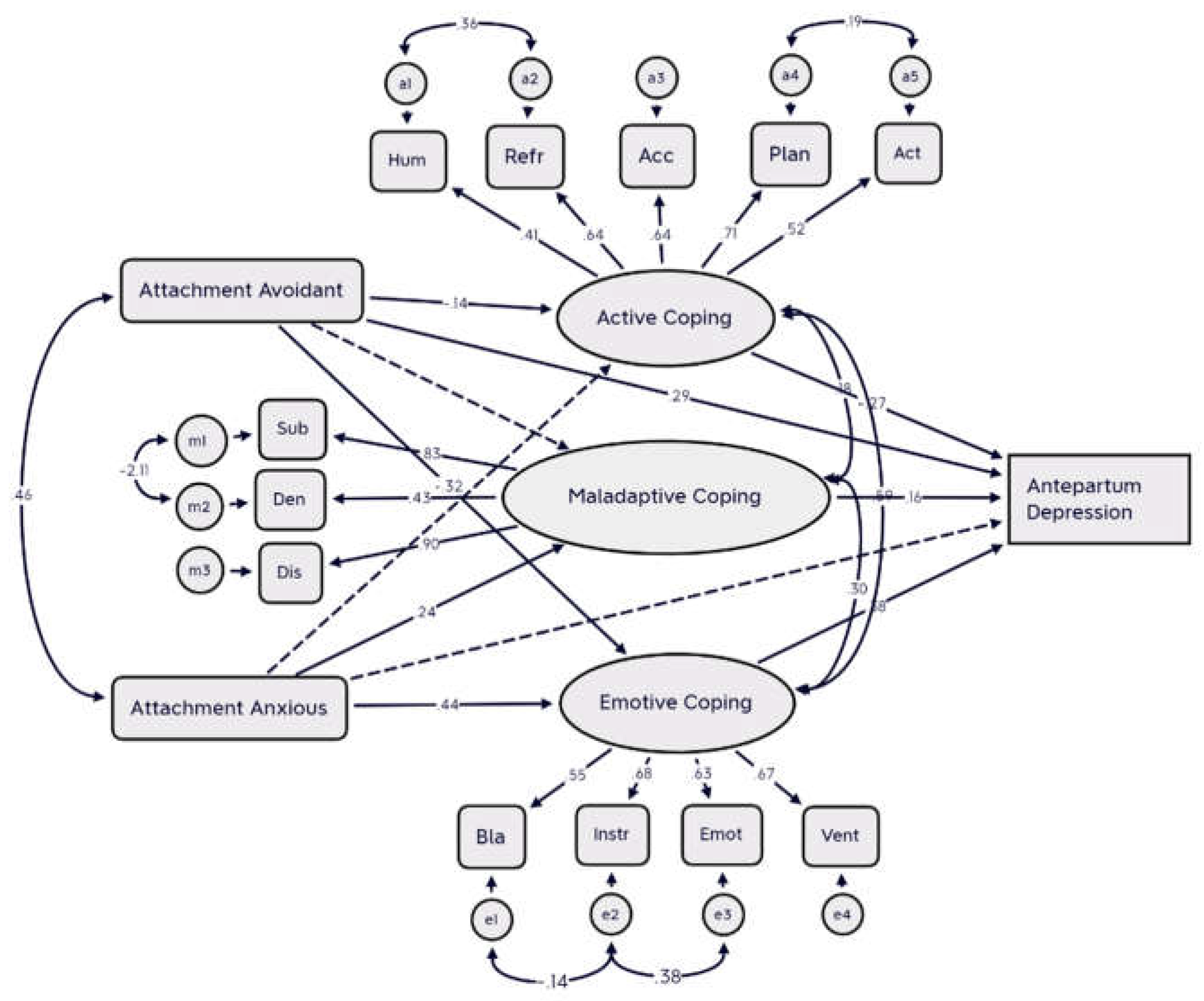
Figure 2.
Path analysis model of the mediating role of coping in the relationship between attachment styles and postpartum depression. Hum=Humour; Refr=Reframing; Acc=Acceptance; Plan=Planning; Act=Active coping; Den=Denial; Dis=Behavioral Disengagement; Bla=Sefl-Blame; Instr=Seeking Instrumental Support; Emot=Seeking Emotional Support; Vent=Venting of Emotions.
Figure 2.
Path analysis model of the mediating role of coping in the relationship between attachment styles and postpartum depression. Hum=Humour; Refr=Reframing; Acc=Acceptance; Plan=Planning; Act=Active coping; Den=Denial; Dis=Behavioral Disengagement; Bla=Sefl-Blame; Instr=Seeking Instrumental Support; Emot=Seeking Emotional Support; Vent=Venting of Emotions.
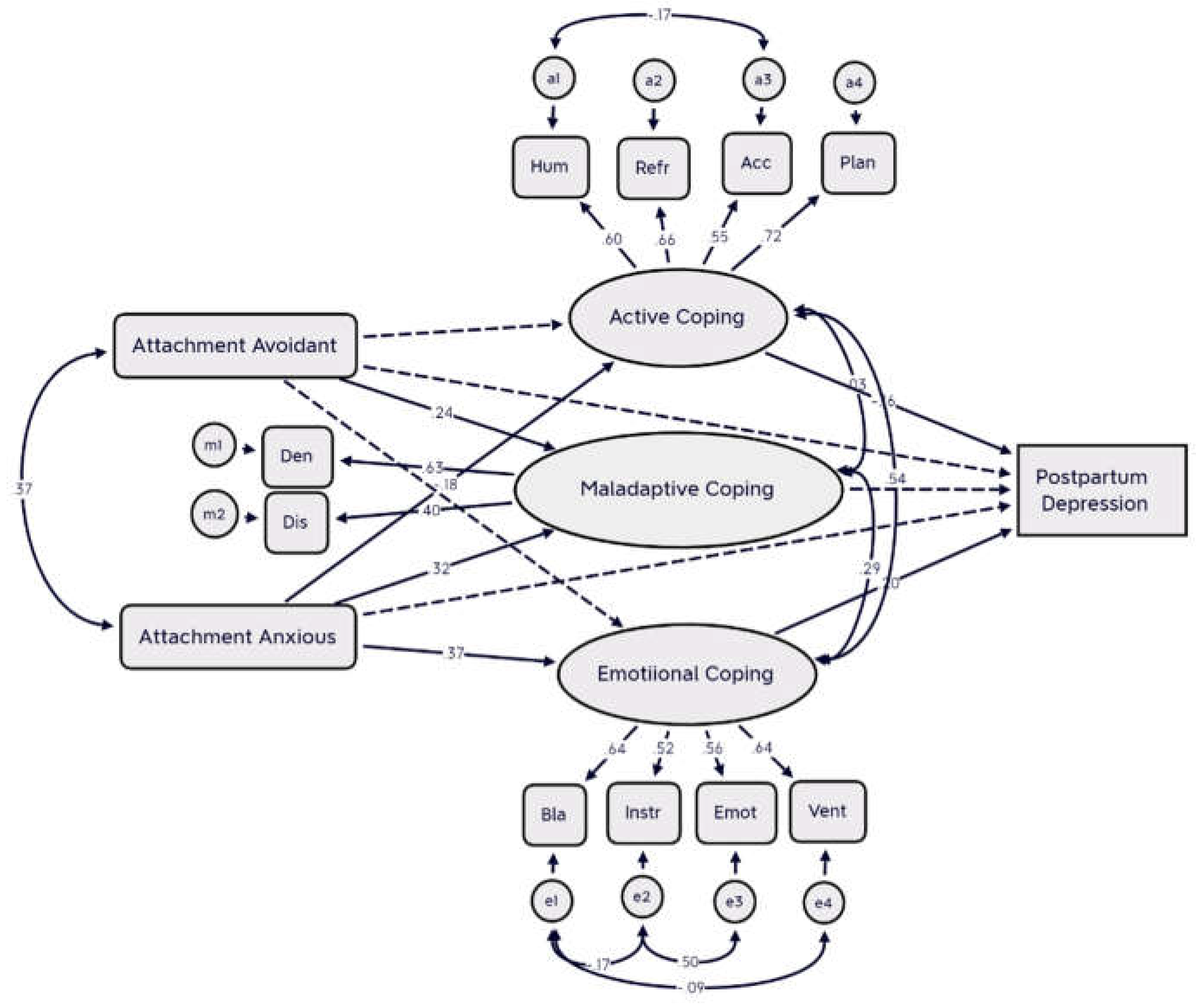

Table 1.
Characteristics of women with antepartum (N=234) and early postpartum depression (N=287).
| Antepartum depression | Postpartum depression | |
| Age (mean, SD) | 32.2 (5.9) | 32.9 (5.2) |
| Educational Level (%) | ||
| Primary school | 1 (0.42) | 1 (0.34) |
| Secondary school | 37 (15.8) | 34 (11.8) |
| Post-Secondary school | 116 (49.5) | 155 (54.0) |
| Higher education | 79 (33.7) | 96 (33.4) |
| Parity (primiparous) (%) | 111 (47.4) | 151 (52.6) |
| Marital status (%) | ||
| Married or paired | 230 (98.2) | 286 (99.6) |
| Some medical condition | ||
| during pregnancy (%) | 64 (27.3) | 85 (29.6) |
| Complication during pregnancy (%) | 154 (65.8) | 278 (96.8) |
| Family history of psychiatric | ||
| problems (%) | 147 (62.8) | 141 (49.1) |
Table 2.
Coping strategies in women with or without postpartum depression. Mean (SD).
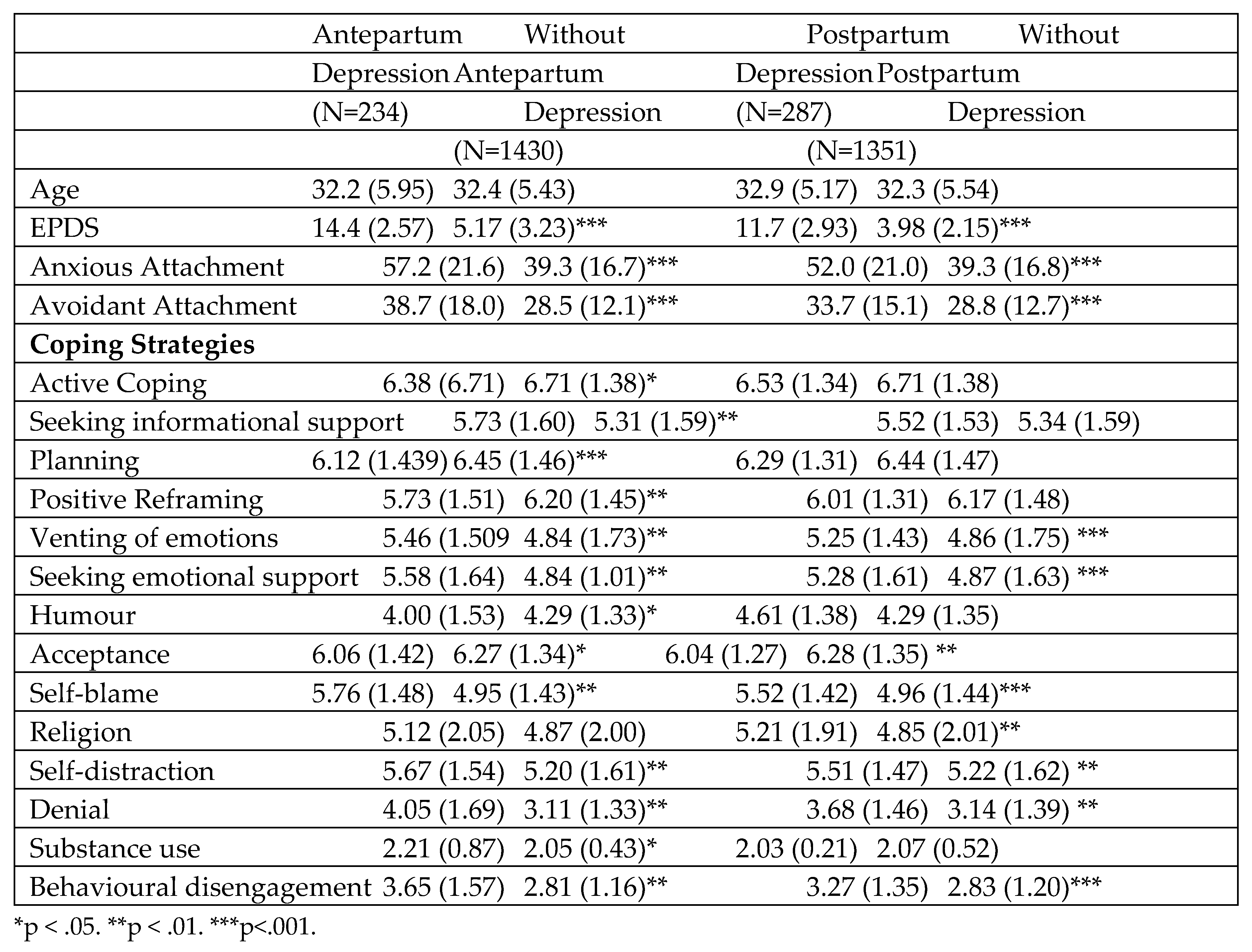 |
Table 3.
Correlation coefficients between attachment styles and stress coping strategies.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



