Submitted:
25 May 2023
Posted:
29 May 2023
You are already at the latest version
Abstract
Cardiovascular diseases (CVD) account for about 17.3 million annual deaths worldwide. 85% of these deaths occurred as a result of myocardial infarction (MI) and stroke. Chronic heart diseases, such as arterial hypertension (AH), coronary heart disease, various cerebrovascular diseases, dilated and hypertrophic cardiomyopathies are widespread, with a fairly high incidence of mortality and disability. Most of these diseases are characterized by cardiac arrhythmias, conduction and contractility disorders. Additionally, interruption of the electrical activity of the heart, the appearance of extensive ectopic foci and heart failure are all symptoms of a number of severe hereditary diseases.
The molecular mechanisms leading to the development of CVD are associated with impaired permeability and excitability of cell membranes and mainly caused by dysfunction of cardiac Ca2+ channels.
Acquired channelopathies are caused by metabolic disorders, increased tone of the sympathetic nervous system, age-related changes that lead to deterioration of coronary blood flow and hemodynamics. Currently known channelopathies, such as the long or short QT syndromes, Brugada and Lenegre syndromes, catecholaminergic polymorphic ventricular tachycardia, etc., are congenital and genetic disorders caused by mutations of genes "responsible" for the conductive properties of certain channel-forming proteins, including pore-forming subunits of Ca2+ channels.
Over the past 50 years, more than 100 varieties of ion channels have been found in the cardiovascular system cells. The relationship between the activity of these channels and cardiac pathology, as well as the general cellular biological function, has been intensively studied on several cell types and experimental animal models in vivo и in situ.
In this review, we discuss the origin of Ca2+ channelopathies and the role of Ca2+ channels of various types: L- R-, T-types voltage-gated calcium channels, RyR2, non-selective hyperpolarization-activated cyclic nucleotide-gated (HCN) channels, transient receptor potential (TRPC, TRPM7, TRPA1) channels in the development of cardio-vascular pathology.
Keywords:
cardiac calcium channels
; gene regulation
; cardiac arrhythmias
; calcium channelopathies
; cardiovascular diseases
1. Introduction
From the vast majority of ion channels involved in cardiovascular diseases (CVD), Ca2+ channels of cardiomyocytes (CM) should be highlighted as the most important structural components of not only transport, but also signaling systems that are necessary for normal cardiac functions [1]. Cardiac Ca2+ channels are classified into different types based on their structure, electrophysiological and pharmacological characteristics. Condition of these channels is regulated by: 1) changes in the membrane potential effecting their gate mechanism(voltage-gated channels, VGCC) [2]; 2) depletion of Ca2+ stores (store-operated Ca2+ channels) [3]; 4), mechanical stretch of cell membrane (transient receptor potential channels, TRPC1-6 channels) [4], 5) hyperpolarization and cyclic nucleotides (non-selective HCN channels that conduct a pacemaker, "fanny" current) [5], and some others [6,7,8,9]. Impairment of the physiological functions of Ca2+ channels leads to mitochondrial Ca2+ overload, damage to CM, apoptosis and heart pathology. Currently, significant progress has been made in the understanding of the function of Ca2+ channels in a healthy heart, but there is still a limited amount of data on cytoarchitectonics and physiology of Ca2+ channels in the cardiovascular system cells associated with heart diseases. The problems of the origin and treatment of congenital and acquired Ca2+ channelopathies, the influence of Ca2+ channel mutations on the pathogenesis of chronic heart diseases, and associated multisystem disorders are also far from being fully understood. In addition, the contribution of posttranslational modifications of Ca2+ channels and defects of Ca2+ handling proteins to the development of potentially lethal heart diseases is still poorly understood [10, 11, 12, etc].
2. Cardiac voltage-gated calcium channels (VGCCs)
Cardiomyocytes contain three types (L-, R- и T-) of voltage-gated calcium channels (Cav channels) that activate upon membrane depolarization. They differ in their properties, functions, and distribution in different compartments of the heart. Most importantly, these channels differ in the activation threshold, which is essential for ensuring the cellular specialization of cardiomyocytes [13, 14, 15, etc.].
2.1. L-type Cav channels (Cav1)
The main cardiac Cav channels are L-type Cav channels (LTCC - long-lasting large-capacity). These are high-threshold (HVA) ion channels, the activation threshold of which is significantly higher than the resting potential (RP) [14]. It should be noted that Cav1 channels electrophysiological properties are characterized with high conductivity and very slow inactivation kinetics [16]. These properties of the channels ensure generation of the action potential (AP), maintenance of normal sinus rhythm and excitation-contraction coupling (ECC) of cardiac cells in depolarization phase of AP. In the cardiovascular system, Cav1 channels are mainly localized in contractile cardiomyocytes, in pacemaker cells of the cardiac conduction system, and in vascular smooth muscle cells, where they function as Ca2+-activated signaling receptors [1,2,17,18]. Dysfunction of Cav1 channels leads to the development of severe hereditary or acquired chronic heart diseases [17,18,19,20].
Cav1 channels are heterooligomeric protein complexes consisting of five subunits: α1, α2, δ, β and γ. The α1 pore-forming subunit is the main component of the channel and remaining four subunits are auxiliary components. However, the functioning of the channel and its positioning on the membrane require the participation of all protein subunits [16]. Moreover, a few other effectors and regulatory proteins directly associated with α1-subunit are required to regulate Сa2+ transport and gating. These proteins (small and large GTPases, calmodulin, etc.) forming supramolecular signal complexes with α1-subunit of Cav1 channel significantly expand the repertoire of mechanisms that regulate the Ca2+ channel influx.
The α1-subunit includes four homologous transmembrane (TM) domains (D1–D4), each of which consists of six α-helices (S1–S6). S5 and S6 together with the linker peptide (linker S5–S6) form a selective pore permeable to Ca2+ ions. The voltage-sensing module (voltage sensor) of the channel is formed by positively charged arginine/lysine-rich S4 segments. The β-subunit is involved in the inactivation and closure of the channel. Together with the α-subunit, they can control the gating by interacting with the pore-forming transmembrane segment S6 of domain I [16, Figure 1].
Voltage-gated calcium channels LTCC exist in three Cav1.1, Ca1.2, and Cav1.3 (Cav1.1-1.3) isoforms, two of which, Cav1.2 and Cav1.3, are found in СM and slightly differing in structure of α-subunits encoded by the CACNA1C, -D genes, respectively [16,21]. Cav 1.2 and Cav 1.3 channels possess high conductivity (25 pSm), very slow inactivation kinetics (τ > 500 ms), and the ability to activate at high membrane potentials (over -10 mV).
The Cav1 channels form multi-subunit protein complexes comprising the Cavα1 pore-forming subunit co-assembly with one of four α2δ subunits and one of four β subunits (Figure 2).
Under physiological conditions, Cav 1.2 and Cav 1.3 channels are modulated by small G-proteins, PKA and other signaling molecules, while conformational changes of channels, their activation kinetics, and a decrease in "tail currents", are well studied [14,15,22].
In adult cardiac myocytes, calcium flow through Cav1.2 channel forms the main type of internal current during the plateau phase of the cardiac AP, and Cav1.2 is the dominant channel involved in ECC. Calcium currents also influence the electrical properties of cardiomyocytes, and channel mutations are associated with various cardiac arrhythmias. Ventricular myocytes have only Cav1.2 channels, whereas both Cav1.2 and Cav1.3 channels are expressed in atrial myocytes, the Gis-Purkinje conducting system, SA and AV node pacemaker cells, and in smooth muscle cells of blood vessels. Nowadays, alternative LTCC splicing has attracted attention as an instrument of tissue specificity, which revealed that the dominant variant of Cav1.2 channel in smooth muscle cells differs from one in heart cells [12,16,21]. The activation threshold of Cav1.2 channels is less negative (-30 mV) than in Cav1.3 channels (-50 mV), which is essential to ensure the sequence of electrical activity in the myocardium [12,17]. The role of Cav1.3 channels is not limited only to their participation in generation of diastolic depolarization in pacemaker cells. The opening of these channels contributes to the generation of local diastolic intracellular Ca2+ releases (LCRs) and is required for the coupled-clock system that drives the automaticity of human sinoatrial nodal pacemaker cells [20]. Unsurprisingly, malfunction of these channels leads to SAN dysfunction, atrioventricular conduction disorders, arrhythmias, and heart failure [23].
Mutations found in genes encoding Cav1 channels determine a wide range of diseases called calcium channelopathies, and all four genes encoding α- and β-subunits carry such mutations [19]. Cav1-channelopathies include muscular, neurological, cardiac and visual syndromes. Among them is Timothy's syndrome, manifested by prolongation of the QT interval and congenital heart defects [24]. This condition is associated with a high risk of sudden cardiac death (SCD) and is caused by defects in the CACNA1C gene encoding the α1-subunit of Cav1.2 channel [14,24,25]. Mutations in the CACNA1C gene change the structure of α-subunits and the conformation of Cav1.2 channels. As a result of these mutations, these channels remain open longer than usual, which leads to excessive intake of Ca2+ into the heart cells, increase in cellular excitability, and increased risk of life-threatening cardiac arrhythmias. The CACNA1C gene is located on the short arm of chromosome 12 (12p13.3) [25].
There are two molecular genetic variants of Timothy syndrome. The most common one is named "classic variant". It is caused by a mutation in exon 8a of the CACNA1C gene and is characterized by polymorphism of clinical manifestations associated with the expression of this gene site in various tissues of the body. The "atypical" variant is less common and caused by mutations in exon 8 of the CACNA1C gene, leading to more pronounced prolongation of the QT and QTc interval and ventricular arrhythmias, most of which are drug-induced or associated with the use of anesthesia [24]. The "atypical" variant of Timothy syndrome is characterized by the maximum expression of the CACNA1C gene in exon 8 in the heart and brain (80% CACNA1C mRNA) [24].
QT syndrome type V (SQT5) is another genetic heterogeneous disease associated with impaired functioning of Cav1.2 channels. It is characterized by a decrease in QT interval ≤ 300 ms and the appearance of a high symmetrical peak-shaped T wave. Mutations leading to a shortening of the AP, which are pathological for this syndrome, were found in the genes encoding K+ channels and CaCNB2b gene (locus 10p12.33) encoding the β2-subunit of Cav1.2 [26,27].
CACNB2b gene encodes 660 amino acids of the β2-subunit Cav1.2 [28]. This gene is mainly expressed in heart cells. The influx of Ca2+ ions into the cytosol is reduced in the channels with defective β2-subunits, which leads to a decrease in the IL,Ca current. Phenotypically, mutations in the CACNB2b gene can lead to not only shortening of the QT interval (SQT5), but also to Brugada syndrome (BS) or combination of both [29].
Brugada syndrome is known as a form of cardiac channelopathy associated with a high risk of SCD. It is believed that BS accounts for 20% of mortality in young people and in men aged 30-40 years without structural pathology of the myocardium. The diagnostic hallmark of the syndrome are distinctive changes in electrocardiogram (ECG) in the form of right bundle branch block and elevation of the ST segment in the right pericardial leads (V1-V3) [19,29]. This pathology is associated with mutations of the CACNA1C and CACNB2b genes encoding α- and β2-subunits of the Cav1.2 channel, respectively. In patients with mutations of these genes, the bandwidth of Cav1.2 is reduced and the IL,Ca current is decreased [26].
The role of Cav1.3 in rhythmogenesis and heart rate modulation has been established only recently [14]. Compared to other calcium channels, Cav1.3 channels are activated faster and at more hyperpolarized voltages, which is important in maintaining the pacemaking, and regulation of heart automaticity [20].
In humans, the first channelopathy involving CACNA1D gene encoding Cav1.3 protein was identified in 2011 [14]. Initially, a loss-of-function mutation in an alternatively spliced exon was associated with congenital deafness. Further observations showed that patients with this pathology had bradycardia and SA node dysfunction (sinus node weakness syndrome) with preserved normal QRS and QT in ECG. In the experimental conditions on mice, the CACNA1D gene knockout was shown to lead to the appearance of viable and fertile offspring, but with deafness, bradycardia, and dysfunction of SA and AV nodes, resulting in pathological functional disorders close to their human counterparts [14]. Experimental data suggest that the C-terminus of Cav1.3 protein can function as a transcription regulator in atrial CM and modulate the expression of the myosin II light chain and small conductance calcium-activated K+ channel [14].
In ventricular CM, the Cav1.2 and Cav1.3 channels are the main structures maintaining myocardial contractility. Genetic or posttranslational modifications of Cavα1- and Cavβ2-subunits can lead to significantly reduced left-ventricular contractility and development of ventricular tachycardia [30]. Defects in these channels lead to an increase in duration of their open state. As a result, the mechanism of Ca2+-induced Ca2+ release (CICR) from the sarcoplasmic reticulum (SR), which is the trigger for the onset of contraction, becomes disrupted. The Cav1.2 and Cav1.3 channel activity in the ventricular CM are usually transient and beneficial, but chronic irritation can become pathological [31]. To restore the functions of the CM associated with the malfunction of Cav1.2 and Cav1.3 channels, a method of targeted mobilization of a pre-synthesized pool of subsarcolemmal Cav1.2 channel-containing vesicles/endosomes into the CM sarcolemma has been developed [32].
2.2. R-type Ca2+ channels (Cav2.3)
R-type Ca2+ channels (Cav2.3) are encoded by the CACNA1A gene and are intermediate in electrophysiological properties between L- and T-type Cav channels. Their structure has not been sufficiently studied. These channels are known to be blocked by Ni2+ and sensitive to Zn2+ and pharmacological regulators of store-operated Ca2+ channels, in particular, to isoproterenol [33]. In the Cav 2.3-deficient mouse model, Cav2.3 channels contribute to the automatism and atrioventricular conduction [13,34].
Like other HVA Сa2+ channels, Cav2.3 channels form multi-subunit complexes consisting of pore-forming α1- and α2-subunits, one of several cytoplasmic β-subunits and extracellular δ-subunits. The Cavα1-subunit is a pseudotetrameric protein with four homologous repeats (I–IV), which consist of six spiral segments penetrating the membrane (S1-S6). Four segments (S1-S4) in each repetition form a voltage sensor module, while the remaining two segments (S5-S6) of all repeats make up the majority of the pore domain (PD) and activation gates. The pore and the selective filter possessing a conserved Ca(2+)-selectivity filter motif ([T/S]x[D/E]xW) are formed by re-enterable pore loops (p-loops) between segments S5 and S6, which partially re-enter the pore region. Three inter-domain linkers and phosphorylation sites in the cytoplasmic domain of the channel are involved in inactivation, association of auxiliary Cavß-subunits, and intracellular modulation [35,36].
It is known that changes in the kinetics and expression of HVA calcium channels caused in particular by mutations in the CACNA1E gene, lead to various pathological conditions and chronic diseases, primarily to the appearance of hereditary cardiac arrhythmia syndromes, such as short QT syndrome (SQTS) and early repolarization (ERS) [19]. People with the CACNA1E gene mutations suffer from arrhythmia and are at risk of SCD [37].
2.3. T-type Ca2+ channels
T-type Са2+ channels (Cav3.1, Cav3.2) - («transient», «short-term» - meaning the opening time of the channel).
Unlike HVA, which open at -20 mV, Cav3 channels are low-threshold, since their activation happens near -40 mV (in SAN cells, the channel activation threshold is -55 mV) [17,21]. The Cav3 channels are characterized by high sensitivity to the blocking action of Ni2+, low sensitivity to dihydropyridines, amiloride, as well as low conductivity (~8 pSm). The activity of the channels is regulated by G-protein-coupled receptors (GPCR), which are blocked by mibefradil, Ni2+ (especially Cav3.2) and curtoxin [38].
T-type calcium channels consist of a single pore-forming α1-subunit that has two key structural determinants of Cav channel gating as well as ion selectivity and permeability. The Cav3 pore-forming α1-subunit is a relatively large plasma membrane protein of about 260 kDa organized into four hydrophobic domains (DI - DIV), each of which consists of six transmembrane helices (S1 - S6) (Figure 3).
Similar to L-type Са2+ channels, the voltage-sensitive channel module (S4) is formed by positively charged rich arginine/lysine, while the selectivity and channel ion conductivity depend on the re-entrant linkers connecting S5 and S6 modules and forming P-loop. The four TM modules are linked together by several intracellular loops connecting S6 module of the upstream domain to S1 module of the downstream domain, which in combination with the NH2- and COOH-termini provide a site/center for channel regulation by various signaling molecules and other protein partners, including the βγ-dimer of the GPCR, PKA, calcineurin, CaMKII, syntaxin-1A, stac1, CACHD1, spectrin α/β and ankyrin B, etc. Furthermore, T-type channels undergo several posttranslational modifications, such as phosphorylation, glycosylation, and ubiquitination that contribute to the expression and activity of the channel [39].
T-type calcium channels exhibit variations in their electrophysiological and pharmacological properties that can be explained by existence of several channel splice variants [39]. These variants include Cav3.1, Cav3.2, and Cav3.3, which are encoded by the genes CACNA1G, CACNA1H, and CACNA1I, respectively in humans [21,40].
T-type channels are formed by numerous variants of α1-subunits, among which the Cav3.1 channels made of (α1G) and (α1H) subunits are found in heart. These channels are expressed mainly in sinoatrial and atrioventricular nodes cells, where along with Cav1.3 channels (α1D), they play an important role in generating spontaneous excitation of pacemaker cells. T-type channelopathies that drastically impair cardiac automaticity are considered rare. They are associated with severe hereditary diseases that lead to sudden cardiac death. One of such diseases is myotonic dystrophy type I (DM1), known as Steinert disease, associated with a DMPK gene defect and channelopathy caused by mutations in genes associated with cardiac function (i.e., TNNT, TNNT2, TTN, TPM1, SYNE1, MTMR1, NEBL, and TPM1), including CACNA1A and CACNA1H [41].
Patients with DM1 suffer from defects in conductivity and atrial or ventricular tachyarrhythmia. The disease progresses with aging and becomes complicated by second- and third-degree heart blockage and left ventricular hypertrophy [42]. Histopathological analysis of the affected hearts from patients with DM1 showed fibrosis and multifocal disintegration of myofibrils [42].
The Cav3.1 channel dysfunction was detected in patients with sinus node weakness and heart blockage caused by congenital autoimmune disease of the cardiac conduction system [20].
In ventricular myocytes, the population of Cav3.1 and Cav3.2 channels is uncommon. Therefore, their role in the regulation of myocardial contractility is insignificant. Transient expression of T-type Ca2+ channels occur in the embryonic heart [43]. In a mouse model, it was demonstrated that the Cav3.2 channels are predominantly expressed in the embryonic heart from 9.5 to 18 days of embryonic development. At the same time, Cav3.1 channels are also expressed, but their expression level is significantly lower than that of Cav3.2 [43]. The functional role of these channels in the embryonic heart remained unknown. The T-type Ca2+ channels was suggested to be involved not only in the regulation of cell proliferation of prenatal CM, but may also be included in the processes of cell growth in the differentiated heart [43]. Indeed, it turned out that Cav3.1 and Cav3.2 channels can be re-expressed in ventricular myocytes with pathological hypertrophy and myocardial infarction [44]. However, the increased expression of Ca3.2 channels is limited to the myocardial lesion zone and has a regional and temporary nature [44]. The hypertrophic overloads of the heart from α1G-transgenic mice demonstrated that the mice were resistant to pressure overload, isoproterenol and cardiac hypertrophy caused by physical exertion. These mice also had no cardiac pathology, despite a significant increase in the influx of Ca2+ into CM. Unlikely, α1G-/-mice showed enhanced hypertrophic reactions after cardiac overload by pressure or infusion of isoproterenol. Pathological hypertrophy in a1G-/-transgenic mice was reversed using the a1G-transgene, which proves the importance of Cav3.1 channels in cardio protection and prevention of cell remodeling [44].
3. Store-operated calcium Ca2+ channels
Ca2+ ions play an important role in many physiological processes, including pacemakering, contraction, release of neurotransmitters, ECC, gene expression, etc. Unsurprisingly, that with a relatively low [Ca(2+)]i, a significant amount of Ca2+ is preserved by cells in intracellular Ca2+ stores. In CM and vascular smooth muscle cells (VSMCs), Ca2+ is stored mainly in SR and mitochondria. Calcium levels in cells are precisely regulated by various transporters and ion channels. Reduction in the intracellular concentration of Ca2+ serves as a signal to refill the Ca2+ stores through store-operated calcium entry mechanism (SOCE).
3.1. Cardiac ryanodine receptor (RyR2)
Ryanodine receptors (RyR2s) are Ca2+-permeable ion channels in the membrane of the SR. These channels are responsible for local Ca2+-induced Ca2+ release from SR. The Ca2+ released (Ca2+ sparks) activates contraction, pacemakering, ECC, and affects other Ca2+-dependent intracellular processes.
RyRs are found in both atrial and ventricular CM, as well as in vascular smooth muscle cells (VSMCs) [45].
Currently, three isoforms of the RyRs have been characterized, one of which is the type 2 ryanodine receptor (RyR2) has been found in CM. Modern innovations in cryo-electron microscopy have made possible to obtain a number of near-atomic RyRs structures that have contributed to a better understanding of the RyRs architecture [46]. The RyR2 consists of 4 subunits combined into a homotetramer and the FC-binding protein calstabin 2 in a stoichiometric ratio of 1:4 [47].
The distinctive feature of the channels formed by RyR2 is that they are activated by an extracellular influx of Ca2+ as a result of the Cav1-RyR2 interaction that triggers local Ca2+ release [46].
Coupling between the Ca2+ entry and intracellular Ca2+ store in CM and VSMCs is mainly mediated by stromal interaction molecule STIM1 located in the endoplasmic reticulum and ORAI1 membrane protein. These proteins are the primary components of the calcium-release activated calcium (CRAC) channel (Figure 4) [46,48,49]. In response to a decrease in the concentration of Ca2+ in SR, STIM1 is homooligomerized and translocated to the SR-PM contact sites, where it colocalizes with Ca2+-ATPase (SERCA), IP3R, and Orai1 forming the Ca2+ selective Orai1 pore [48]. However, it is still unclear how such a close arrangement of proteins is conducted [49].
STIM1 domains include the ER luminal domains that have the SAM and EF hands. These domains function as the Ca2+ sensor of SR store content. Cytosolic oriented STIM1 contains regions critical for Orai channel gained within the CC domains. Additional domains include the ERM and lysine rich regions. The first protein, STIM1, is the ER-Ca2+ sensor protein involved in activation of SOCE. The second protein, Orai1, is the pore-forming component of the CRAC channel.
The STIM1 protein contains specific sequences localized in the transmembrane and cytoplasmic domains responsible for modular protein-protein interactions, as well as two Ca2+-binding EF-hand motifs facing the CP lumen. These Ca2+-binding sites are the primary detectors of the Ca2+ level. Over the last years, studies there have been demonstrated evidences of the involvement of STIM1 in the growth of the heart in response to signals of development and pathology [50].
RyR2s are part of the pacemaker molecular mechanism that ensures the heart automaticity. The contribution of the RyR2-dependent Ca2+ releases (Ca2+ sparks) to the automaticity is currently interpreted within the framework of a model dubbed "calcium clock". [51]. According to the coupled-clock pacemaker cell system concept, the “clock” in pacemaker cells forms two competing oscillators: "Ca2+-clock" mechanism based on the spontaneous release of Ca2+ from SR and "membrane clock" ("M-clock") which includes surface membrane cation channels to ignite an AP [51]. The phenomenon of Ca2+ oscillations, underlying the “Ca2+-clock”, is associated with the local diastolic intracellular Ca2+ releases (LCRs), and it is independent of the membrane potential (MP). Indeed, spontaneous LCRs can be observed in the absence of changes in MP and are a distinctive feature of the "Ca2+-clock" [52]. RyRs act as a gear in a "Ca2+-clock" inducing rhythmically discharges of LCRs, which, in turn, activate an inward current (INCX1) that prompts the "M-clock" to start an AP [51]. This electrogenic transport mechanism generates an internal ion current, which contributes to the onset of diastolic depolarization. In the final phase of diastolic depolarization, Cav channels cooperate with Na+/Ca2+-exchanger (NCX) to raise MP to the threshold value of the AP [51]. During the AP phase, the intake of Ca2+ through LTCC channels refills the leakage of Ca2+ from SR allowing new diastolic intracellular Ca2+ release to occur in the next cycle. Consequently, under the normal physiological conditions, the "Ca2+-clock" and the "M-clock" synchronize the pacemaker activity of the heart cells and create a reliable basis for the heart automaticity [51,53].
Considering the importance of the RYR2 in providing of the heart automaticity, it seems quite obvious that mutations of genes encoding these receptors or proteins interacting with RYR2 in the CICR, would lead to catastrophic consequences for the organism [54]. Indeed, studies using a mouse model have shown that a RYR2 mutation with a locus in the CaM-binding site (reducing receptor inactivation) causes cardiac hypertrophy, heart failure, and early sudden death [55,56].
Clinical studies suggest that enhancing the interaction of CаM-RyR2 may represent an effective therapeutic strategy for the treatment of cardiac arrhythmias and heart failure. In support of this idea, the mutation of GOF CаM-M37Q and reinforcement of the CаM-RyR2 interaction have been demonstrated to be able to suppress the spontaneous release of Ca2+ from SR and catecholaminergic polymorphic ventricular tachycardia.
In chronic heart diseases accompanied by cardiac arrhythmias, there is an increase in the activity of Cav1.2 channels, which leads to an increase in their permeability to Ca2+ and, as a result, to CM calcium overload. At the same time, spontaneous Ca2+ releases induced by more frequent RYR2 openings form "pathological" calcium waves that are abolished removed under physiological conditions with the participation of NCX1 and other molecular determinants of Ca2+ homeostasis (CASQ2, FKBP12, SERCA2a, ect.) [46]. It was found that NCX1 dysfunction and changes in its expression profile during arrhythmia lead to changes in atrial cell morphology and calcium handling together with dramatic alterations in the function of SAN [58,59].
Recent studies have shown that spontaneous arrhythmogenic "calcium waves" can result from genetic mutations of RyR2, but more often due to an increase in the time of its open state [60,61,62,63,64,65]. Defects in its modular coupling with regulatory proteins of the cytosol, such as CaM, Epacl, PDE, FKBP12.6, PKA, PP1, calstabin, etc., or with Ca2+-binding proteins localized in the lumen of the SR (junctin, triadin and calsequestrin) and forming temporary macromolecular complexes with it, can lead to a disruption of the RyR2 gate function [61,66,67,68,69]. Mechanisms of interaction of the partner molecules with RyR2 are built on a structural basis, while regulatory proteins (predominantly kinases) use RyR2 as a scaffold protein to form functional signal complexes that can modify a large number of other Ca2+-dependent molecules involved in the cascade signal transmission. The structure of these RyR2-multi-domain complexes and mechanisms of regulation of their activity are still far from being fully understood [65,69].
It is noted that point mutations of RyR2-associated proteins or changes in their expression can dramatically affect the development of cardiac arrhythmias [70]. In particular, the expression level of serine/threonine protein phosphatases plays an important role in the pathogenesis of arrhythmias [71]. Serine/threonine protein phosphatases (PP1, PP2A, and PP2B) control dephosphorylation of numerous cardiac proteins, including a variety of ion channels (Cav1.2, NKA, NCX, ect.), calcium-handling proteins (SERCA, junctin and PLB), contractile proteins MLC2, TnI and MyBP-C [71,72], thereby providing post-translational regulation of ECC and other heart functions. Accordingly, dysfunction of this regulation can contribute to the development of cardiac arrhythmias. Atrial fibrillation (AF) is the most common heart rhythm disorder, and it is characterized by electrical and structural cardiac remodeling that among other factors includes changes in the phosphorylation status of a wide range of proteins, such as the RyR2 [71]. It was found that a decrease in the concentration of PP1 caused by an increase in the level of PP1-regulatory proteins like inhibitor-1 (I-1), inhibitor-2 or heat-shock protein -20 in the sarcoplasm of ventricular CM lead to the rapid development of tachycardia and could cause sudden death [63,72], although an experimental increase in the concentration of PP1 in sarcoplasm prevented the development of arrhythmia, which was proven in experiments on mice overexpressing Ang II [73]. Mice characterized with a highly phosphorylated RyR2-S2808 site (S2808A+/+) demonstrated an increased sensitivity of RyR2 to Ca2+ during dephosphorylation of PP-1 [74].
СaM kinase II is another enzyme that plays an important pathogenetic role in diseases accompanied by cardiac arrhythmia [52,54,75]. Effect of CaM kinase II on RyR2 is controversial. In pharmacological experiments using the method of embedding proteins in an artificial bilayer, some authors revealed the activating effect of this kinase on RyR2. On the other hand, others demonstrated its’ inhibitory effect [76]. Using molecular genetic methods (transgenic overexpression), more recent studies have found that СаМ kinase II by binds RyR2 and causes its phosphorylation at serine 2814 (RYR2-S2814). This, in turn, increases the frequency of Ca2+ spikes and the spontaneous local diastolic subsarcolemmal Ca2+ releases in the process of ECC [52]. It was noted that an increase in the level of phosphorylation of RYR-S2814 in SAN pacemaker cells led to the alteration of the "Ca2+-clock" regulation and the development of heart failure (HF) [77].
Inhibition of CaM kinase II by a specific blocker KN93 reduced the release of Ca2+ from SR and a slowed in heart rate [52]. In vitro studies have shown the possibility of using this blocker to relieve ventricular tachycardia caused by oxidative stress, which opens up prospects for the therapeutic use of KN-93 and its’ functional analogues in the treatment of arrhythmias [52].
In addition, an increase in the basal level of CaMKII through phosphorylation of histone deacetylases (HDACs) activates myocyte-enhancer factor 2 (MEF2), which initiates the CaMKII/MEF-2 signaling pathway and hypertrophic remodeling of ventricular myocytes [78]. Among endogenous biologically active molecules that have arrhythmogenic effects, the most studied are neurohormones, such as endothelin-1 (ET-1), aldosterone, epinephrine, which act through Gαq-associated GPCRs and cAMP-dependent protein kinase A (PKA) [79,80,81]. Increased hormonal stimulation of these receptors leads to hyperphosphorylation of RyR2 and dissociation of calstabin 2 (FKBP12.6) from it. RyR2, deprived of this protein, loses its locking function, which leads to an increase in the time of its open state, leakage of Ca2+, an increase in [(Ca2+)]i, to afterdepolarization and can cause "fatal arrhythmia", heart attack, and SCD [82]. To date, two genetic diseases associated with mutations in ventricular RyR2 have been described: catecholaminergic polymorphic ventricular tachycardia (CPVT), or familial polymorphic ventricular tachycardia and arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) type 2 [83]. In patients with CPVT, the affinity of calstabin 2 to RyR2 is reduced due to a defect in RyR2 at its binding site to calstabin [82]. The use of molecular approaches in the strategy of the targeted therapy of CVD emerged new drugs that suppress hyperphosphorylation of p-RyR2 (Ser2808) and p-RyR2 (Ser2814), thereby, stabilizing RyR2 and normalizing heart rate and contractility of ventricular myocytes [84,85]. The ClinVar database describes 165 variants of pathogenic mutations of the RYR2 gene. The most common mutations associated with CPVT are: Ser2246Leu, Arg2474Ser, Asn4104Lys, Arg4497Cys, Pro2328Ser, 1.1-KB DEL, EX3. Most of these mutations lead to amino acid substitution or to the appearance of a premature stop codon and disruption of the formation of a functional protein [86].
In addition to the RYR2 gene, encoding ryanodine receptor calcium release channel, mutations in 5 genes encoding proteins from the SR calcium-release complex are involved in pathogenesis of CPVT: CASQ2 (encoding cardiac calsequestrin), TRDN (encoding triadin), CALM1, CALM2 and CALM3 (encoding identical protein calmodulin) [87].
The development of arrhythmogenic dysplasia of the right ventricle is also associated with mutations in the RYR2 gene. The ARVD2 locus was mapped to chromosome 1q42--q43 [88]. This disease is characterized by partial fatty or fibrous degeneration of the myocardium of the right ventricle, electrical instability, and sudden death [88]. The detection of RyR2 mutations causing CPVT and ARVD2 opens the way to pre-symptomatic detection of carriers of the disease in childhood, thus enabling early monitoring and treatment [87,88].
3.2. Ion channels with transient receptor potential (TRPC, TRPM7, TRPA1)
Transient receptor potential channels are nonselective cation channels of the TRP channel superfamily, uniting the related receptor proteins capable of being activated by the potential originating from binding of the ligand to the receptor. This superfamily is divided into a family of canonical TRP channels (TRPC) and several families whose names come from the name of the receptor, binding to which initiates the potential. Most TRPs are polymodal channels, so-called «coincidence detectors» that are activated by both physical and chemical stimuli [89]. TRP channels vary degrees of selectivity and permeability to ions. TRPV1 - TRPA1 and TRPM6/7 channels are more selective for Ca2+ ions. In CM, they are localized in the sarcolemma adjacent mainly to intercalated disks and are activated by phospholipase C (PLC) via Gaq-associated G protein-coupled receptors [90].
The common structural features of these channels are: four N-terminal ankyrin repeats, six short TM domains and pore-forming region localized between transmembrane domains 5 and 6. Like the other previously described channels, TRP channels with partner proteins and kinases form signaling complexes that can be involved in the pathogenesis of various cardiovascular diseases [91,92,93,94].
The existing data suggest that several types of TRP channel (TRPC3, TRPC6, TRPV1, TRPV3, TRPV4, TRPA1, TRPM6 and TRPM7) may play a central role in the progression of fibroproliferative disorders in the heart and blood vessels and contribute to both acute and chronic inflammatory processes involved in them [95].
The family of canonical TRP channels consists of proteins closely related to the Drosophila channel proteins of the same name involved in photoreception [96]. This family includes seven subfamilies (TRPC1 – TRPC7), of which proteins of the TRPC1, -3, -4, -6 and -7 subfamilies were found in CM [97]. To date, the greatest interest is focused on mechanosensitive TRPC channels. In case of their molecular «breakdown», these channels begin to pass an increased flow of Ca2+ ions, and, thereby, activate processes involving pathological remodeling of CM [91,93,98]. In addition, TRPC7 also mediate apoptosis, thereby contributing to the process of heart failure [99].
All TRPC channels are dependent on receptors associated with PLC, since they are directly or indirectly activated by phospholipid products formed due to activation of this enzyme and induction of hydrolysis of membrane phospholipids. TRPV1, -2 and -5 channels are activated by binding IP3 to the receptors and responsible for SOCE. In this case, the interaction of TRPC with Orai protein and stromal interacting molecule 1 (STIM1) is noted [100]. The mechanism of Ca2+ store filling with the participation of these proteins is as follows. After Ca2+ store depletion, the STIM1 protein located in the ER undergoes a complex conformational rearrangement which results in STIM1 translocation into discrete ER-plasma membrane junctions, where it directly interacts with the plasma membrane protein Orai1. Orai 1 in its turn triggers recruitment of TRPC1 into the plasma membrane where it is activated by STIM1 then. TRPC1 and Orai1 form discrete STIM1-gated channel for the entry of Ca2+ into the lumen of the ER [101,102]. In addition, STIM1 can also activate TRPC1 through its C-terminal polybasic domain, a distinct from its Orai1-activating domain, SOAR [101].
TRPM2 is the second member of the TRPM subfamily that includes eight members, specifically TRPM1-8. TRPM2 is widely expressed in СM, where it forms a Ca2+-permeable cation channel and serves as a cellular sensor for oxidative stress or inflammatory response [103,104,105].
The N-terminus is composed of four melastatin homology regions and homology region pre-S1 (melastatin homology regions (MHR) and homology regions (HR). The channel domain contains six TM (S1–S6), corresponding to a voltage-sensor-like domain; the pore is formed by the loop between the S5 and S6. The C-terminus is composed of TRP and the coiled-coil domain (CC) (Figure 5).
Trpm2 monomer is depicted as having 6 TM (S1 to S6) with the putative pore-forming loop situated between S5 and S6. Four monomers associate to form a Trpm2 channel. Both N- and C-termini are in the cytosol. The N-terminus contains 4 modules of Trpm subfamily melastatin homology domain (MHD). In the second MHD, there is an IQ-like motif which binds Ca2+-calmodulin. The C-terminus contains a Trp box (TRP), a coiled-coil domain (CC), and the adenosine diphosphate ribose (ADPR) pyrophosphatase homolog domain. Trpm2 is a non-specific cation-permeable channel which allows entry of Ca2+, Na+, and K+.
TRPM2 channels are activated by ADPR, Ca2+, H2O2 and other reactive oxygen species (ROS). They serve as a cellular sensor for oxidative stress, mediating oxidative stress-induced [Ca(2+)]i increase and contributing to pathological processes in many cell types, including CM. Overexpression of Trpm2 induces cell injury and death by Ca2+ overload or enhanced inflammatory response [103,105].
Mutations in genes encoding closely related TRPM4 channels lead to impaired automatism, conduction, and the appearance of hereditary progressive familial heart block type I (PFHBI) [106,107]. It is also assumed that some forms of provoked cardiac arrhythmia may occur due to a single gain-of-function mutation in TRPM4. To date, 47 mutations of TRPM4 channel have been registered in the Human Gene Mutation Database [108,109].
TRPM7 channel mutations are especially dangerous in the prenatal period, as they can lead to intrauterine fatal arrhythmia and fetal death or to a change in the myocardial transcription profile in adulthood, deterioration of ventricular contractile function, conduction and repolarization [110,111].
There is evidence of a wide involvement of TRP channels in the pathogenesis of CVD caused by hypoxia and oxidative stress, as well as ischemia-reperfusion (I/R) [90,104,112,113,114].
It is known that during hypoxia and I/R, there is formation of ROS and accumulation of lipid peroxidation products, including unsaturated aldehydes such as acrolein and 4-hydroxynonenal, which are TRPA1 agonists, in cardiac tissue [115]. The mechanism of toxic action of unsaturated aldehydes on CM is associated with their high electrophilicity and the ability to covalently bind to cysteine residues in the TRPA1 molecule, leads to the opening of these channels and an increase sarcoplasmic reticulum Ca2+ release flux into the cytosol [116]. Overexpression of TRPС1 channels also contributes to Ca2+ leakage from SR [117]. As a result, Ca2+ overload of СM, leading to impaired contractility, heart failure and myocardial infarction occurs [117].
The pathogenic significance of TRP channels in the development of heart failure, coronary artery disease, arterial and pulmonary hypertension, as well as coronary microvascular dysfunction and atherosclerosis is no less [6,90,118,119,120].
TRPA1, TRPV1-4 and TRPC1-6 are expressed on the surface of endothelial cells and ensure the pass of Ca2+ ions into cells, regulating endothelial-dependent vasodilation in response to a number of signaling molecules, such as endothelial derived hyperpolarizing factor (EDHF), NO, and prostacyclin [90,113,119,123]. In mice with TRPV1 and TRPC3 channel knockout, there was a decrease in aortic vasodilation in response to carbachol, which proves the involvement of these channels in endothelium-dependent vasodilation [119,124]. In experiments on three animal models (dog, rat and mouse), it was demonstrated that i.v. administration of the TRPV4 agonist, GSK1016790A, stimulated endothelial derived EDHF-dependent vasodilation, and led to a subsequent decrease in blood pressure [125]. The TRPV4 channels have been noted to participate in the coupling of endothelial-dependent vasodilation and relaxation of VSMCs through interaction with RyR2 and the big conduction KCa channel [126]. TRPV4/7, TRPC1/5/6/7 and TRPV1/2/4 are expressed in VSMCs and participate in myogenic regulation of vascular tone [119,120,127]. Electrophysiological experiments demonstrated that the TRPM4 knockout mice had increased vascular tone and developed hypertension [90,128], while inhibition of TRPC6 reduced VSMCs contraction [127]. TRPV1 channels are involved in the progression of the atherosclerotic process in the apolipoprotein E gene knockout mice [129]. Further studies have shown that other mechanosensitive TRP channels may also play a role in the development of atherosclerosis and coronary heart disease (CHD) [6,130,131]. In addition, disruption of the TRP channel expression or function may explain the observed increased cardiovascular risk in patients with metabolic syndrome [132].
Thus, TRP channels have broad cardiovascular plasticity. TRPC3, TRPC5, TRPC6, TRPV1, and TRPM7 are involved in vasoconstriction and regulation of blood pressure and can be considered as potential therapeutic targets for the treatment of chronic CVD, including cardiometabolic diseases and myocardial atrophy [6,119,132,133,134].
4. Hyperpolarization-activated cyclic nucleotide-gated (HCN) channels
HCN channels are non-selective cationic channels that are involved in the generation of pacemaker activity in heart and brain cells [135,136]. They belong to the family of channels operated by cyclic nucleotides, which is part of the superfamily of potential-operated potassium channels, the regulation of which is under the control of the autonomic nervous system [137]. There are 4 isoforms of HCN channels (HCN1-4) encoded by the same genes [138]. The function of HCN channels is to generate a pacemaker current (If) during the hyperpolarization phase of the AP [139,140].
HCN channels are expressed differentially. HCN4 is the dominant form found in the SAN. HCN2 is found in the His-Purkinje system. HCN1 is also expressed in the SAN but it is less optimal for pacemaker targeting [139], HCN1 and HCN2 transcripts are predominantly found in ventricular CM [140,141].
HCN channels are primarily selective to Na+ and K+, but their functioning directly affects the influx of Ca2+ ions into CM and has a regulatory effect on diastolic depolarization under physiological conditions [142,143,144,145]. Electrophysiological experiments using the patch-clamp technique revealed that the influx of Ca2+ through HCN2 channels is enhanced by increasing the time of their open state with an increase in the concentration of сAMP and is inhibited by the specific If-blocker ivabradine [102].
HCN channels consist of 4 subunits, which can be either the same or different from each other [138,139]. However, in vivo channels consisting of subunits of the same type are more common [146] (Figure 6).
Each α-subunit contains six TM (S1—S6), including a positively charged potential sensor (S4), and P-region located between the pore-forming S5 and S6 segments and carrying a GYG motif of Kv channels, as well as a cyclic nucleotide-binding domain (CNBD) located on the C-terminus. C-terminus contain two conserved structured regions: the C-linker contributing to tetramerization and the CNBD which allows for modulation by cAMP, followed by a non-conserved region. Besides, HCN1 contains a di-arginine ER retention signal in the intrinsically disordered region of the C-terminus of HCN1. This signal controls the trafficking of HCN1 and negatively regulates surface expression of HCN1 [148,149]. Deletion of the entire N terminus (residues 1-185) also prevented surface expression HCN2 [147].
HCN isoforms (1-4) are highly conserved relative to TM and the binding site for cyclic nucleotides (80-90% identity), but have differences in activation and reactivation kinetics, depending on voltage and cAMP modulation [151]. For example, HCN4 exhibits the slowest activation and reactivation kinetics and opens at more negative potentials than other isoforms [152]. On the contrary, HCN1 demonstrates the fastest kinetics and opens at more positive potentials [152]. HCN4 is the most sensitive to cAMP, while the HCN1 subtype is faintly affected by cAMP and other cyclic nucleotides [139,153,154].
Cardiac activity is under hormonal control and modulated by mechanisms mediated by small proteins, β-adrenoreceptors and сAMP [155,156]. An uncontrolled increase in the concentration of сAMP (sympathicotonia), or other non-canonical cyclic nucleotides, an increase in membrane expression and activation rate of HCN channels in the SAN can lead to modulation of the cAMP-dependent activation profiles, an increase in heart rate and SCD [155,157].
HCN channel dysfunction, decreased levels of connexin 40, connexin 43, myocyte-enhancer factor-2C and components of gap junction were noted in the hearts of transgenic mice with overexpression of calreticulin [158]. The complex of these disorders underlies the development of arrhythmia, dilated cardiomyopathy and SCD [158]. Age-related conduction disorders are also associated with HCN channel dysfunction [159].
Recent studies have shown the existence of four HCN channelopathies associated with different types of arrhythmia [146,153]. The mutation in exon 5 of the HCN4 gene is functionally associated with a truncated protein that is unable to bind cAMP and, therefore, has a dominant negative effect on channel function. Missense-mutations of the same gene have been found in families at patients with the SAN dysfunction. The presence of these mutations led to recurrent syncopes, severe bradycardia (39 beats per minute), prolonged QT interval and polymorphic ventricular tachycardia [153]. Dysfunction of HCN channels, mainly HCN4, is associated with the sick sinus syndrome and other arrhythmias, such as atrial fibrillation, ventricular tachycardia and atrioventricular block. In recent years, several data have also shown that dysfunctional HCN channels (HCN1, HCN2, and HCN4) may play an important role in the pathogenesis of epilepsy [146]. Myocardial involvement is frequent in patients affected by neuromuscular disorders and is the main cause of death in some conditions (Table 1).
Currently, there are ongoing studies on the directed transport of recombinant genes directly into the heart [160]. In experiments on mice, adenoviral constructs expressing the HCN2 gene were delivered by epicardial injection into the root of the appendage of the left atrial appendage. Four days after the targeted delivery of the HCN2 gene, spontaneous beats occurring at the injection site were detected. The heart rate in experimental mice was under the control of the autonomic nervous system, which was proved by stimulation of the heart rate with catecholamines and a decrease in heart rate because of stimulation of the left vagus nerve. Cells localized at the injection site showed increased expression of HCN2 channels and increased If -currents [161].
These studies show the effectiveness of a targeted approach in the treatment of arrhythmias and congenital cardiac HCN channelopathies in humans [146,160,161].
However, for successful gene therapy of HCN channelopathies in humans, additional mutant or chimeric HCN channel constructs will be required, which will have more positive activation and increased reactivity, as well as optimization of the method of delivery of therapeutic genes to the target cells of the heart. Research in this direction is underway [160,162].
5. Prospects of using the achievements of molecular biology in the treatment of chronic heart diseases
The cornerstone in the strategy of targeted molecular therapy is the idea of using drugs that act on subcellular structures involved in the mechanism of disease development. Currently, such drugs are mainly used for the treatment of certain types of cancer. In the therapy of cardiac diseases, the use of substances targeting certain molecular substrates has not become common yet. The most well-known drugs that can be attributed to this drug group are calcium channel blockers (CCBs). They have been used since the 70s of the last century and have proven to be effective and reliable means in the treatment of CVD accompanied by rhythm disorders and decreased myocardial contractility. The broad use of CCBs in clinical practice was facilitated by their high anti-ischemic and antianginal efficacy, as well as by good tolerability, established during large clinical studies [163]. Over the past years, more than one generation of drugs of this group has changed. Modern CCBs (amlodipine, lacidipine, etc.) are substances that differ from their predecessors (verapamil, nifedipine, diltiazem, etc.) by prolongation of action, and a higher safety profile [164,165]. Drugs of this group have a cardioprotective effect by improving myocardial perfusion, reducing myocardial oxygen demand, reducing the formation of free radicals and mitochondrial Ca2+ overloading of CM [164,165,166]. The disadvantages of CCBs as drugs are their rather wide range of action and low selectivity with respect to their molecular targets directly in the myocardium. Moreover, the use of these drugs is associated with an increased risk of developing proarrhythmia, systemic toxicity, an increase in the defibrillation threshold and, in some cases, an increase in mortality [167]. Such significant disadvantages of CCBs make it necessary to search for novel alternative drugs, the targets of therapeutic action of which are not the channel proteins themselves, but the molecules modulating their activity. Such proteins can be fully attributed to CaM kinase II, which is, on the one hand, a key modulating enzyme of Ca2+ metabolism in chronic heart pathology and on the other hand, a widespread protein found in other vertebrates, making possible to study the effect of CaM kinase II blockers initially in vivo experiments and in situ [168,169].
It is obvious that other regulatory proteins that exert their cardiotropic effect through interaction with Ca2+ channels or their modulators can become targets for pharmacological strategy in the treatment of chronic heart diseases. We mentioned some of them previously [84,85]. Currently, the most promising are studies aimed at finding blockers of the NCX1 [170], various isoforms of phosphodiesterases [171], subunits of voltage-operated channels of various types, including nonselective HCN1-4 and TRP channels [172,173]. The use of these, in fact, "molecular tools" to influence the mechanisms of Ca2+ signaling in heart failure and other chronic heart diseases is the first step towards making new drugs whose therapeutic targets are small fragments of specialized molecules or their specific isoforms. The recent progress in the studies of the structure and properties of Ca2+ channels and Ca2+ handling proteins, as well as modern technologies using targeted nanoparticles and targeted gene delivery directly to the heart allow us to hope that significant progress will be made in the treatment of severe CVD associated with heart rate and contractility disorders in the near future [160,174].
Funding
This research received no external funding. This work was carried out using the state budget funds under the state task № АААА-А18-118012290142-9.
Conflicts of Interest
The author declare no conflict of interest.
Abbreviations
| ADPR | ADP-ribose |
| AP | action potential |
| ARVC/D | arrhythmogenic right ventricular cardiomyopathy/dysplasia type 2 |
| AVN | atrioventricular node |
| BS | Brugada syndrome |
| Ca2+ | calcium |
| [Ca(2+)]i | intracellular Ca2+ concentration |
| CAD | сoronary artery disease |
| СаМ | calmodulin |
| Cav channels | voltage-gated calcium channels |
| Cav1 | L-type Cav channels |
| CCB | calcium channel blockers |
| CCs | calcium channelopathies |
| CHD | coronary heart disease |
| CIRC | Ca2+-induced Ca2+ release |
| CM | cardiomyocyte |
| CNBD | cyclic nucleotide-binding domain |
| CPVT | catecholaminergic polymorphic ventricular tachycardia |
| CRAC | calcium-release activated calcium channel |
| CVD | сardiovascular diseases |
| DADs | afterdepolarizations |
| DM1 | myotonic dystrophy type I |
| ECC | excitation-contraction coupling |
| ECG | electrocardiogram |
| EDHF | endothelial derived hyperpolarizing factor |
| GPCR | G-protein-coupled receptors |
| HF | heart failure |
| HR | heart rate |
| HVA | high voltage-activated voltage-gated calcium channels |
| IHD | ischemic heart disease |
| I/R | ischemia/reperfusion |
| LCRs | local diastolic intracellular Ca2+ release |
| LTCC | L-type Cav channels (Cav1) |
| MI | myocardial infarction |
| MP | membrane potential |
| NCX1 | Na+/Ca2+ exchange |
| PDE | phosphodiesterase |
| PFHBI | progressive familial heart block type I |
| PKA | cAMP-dependent protein kinase A |
| PLC | phospholipase C |
| PM | plasma membrane |
| PP | resting potential |
| ROS | reactive oxygen species |
| RP | resting potential |
| RyR2 | ryanodine receptor type 2 |
| SAN | sinus node |
| SOCE | store-operated calcium entry |
| SQTS | Short QT syndrome |
| SR | sarcoplasmic reticulum |
| STIM1 | stromal interacting molecule 1 |
| ТМ | transmembrane domain |
| TS | Timothy syndrome |
| TRP | transient receptor potential (canonical, vallinoid-related, melastatin-related) |
| SCD | Sudden Cardiac Death |
| SMC | smooth muscle cells |
| VGCC | voltage-gate calcium channel |
| VSMCs | vascular smooth muscle cells |
References
- Atlas, D. Voltage-gated calcium channels function as Ca2+-activated signaling receptors. Trends Biochem. Sci. 2014, 39, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Landstrom, A.P.; Dobrev, D.; Wehrens, X.H.T. Calcium Signaling and Cardiac Arrhythmias. Circ. Res. 2017, 120, 1969–1993. [Google Scholar] [CrossRef] [PubMed]
- Collins, H.E.; Zhang, D; Chatham, J. C. STIM and Orai Mediated Regulation of Calcium Signaling in Age-Related Diseases. Front. Aging. 2022, 3, 876785. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, J.; Tong, X. Cross-Talk between Mechanosensitive Ion Channels and Calcium Regulatory Proteins in Cardiovascular Health and Disease. Int. J. Mol. Sci. 2021, 22, 8782. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, A.S.; Peigneur, S.; Tytga,t. J. Review: HCN Channels in the Heart. Curr. Cardiol. Rev. 2022, 18, e040222200836. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; D'Amato, A.; Pucci, M.; Infusino, F.; Adamo, F.; Birtolo, L.I.; Netti, L.; Montefusco, G.; Chimenti, C.; Lavalle, C.; Maestrini, V.; Mancone, M.; Chilian, W.M.; Fedele, F. Ischemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation to Microvascular Dysfunction. Int. J. Mol. Sci. 2020, 21, 8118. [Google Scholar] [CrossRef] [PubMed]
- Weisbrod, D. Small and Intermediate Calcium Activated Potassium Channels in the Heart: Role and Strategies in the Treatment of Cardiovascular Diseases. Front. Physiol. 2020, 11, 590534. [Google Scholar] [CrossRef]
- Kim, J.; Gupta, R.; Blanco, L.P.; Yang, S.; Shteinfer-Kuzmine, A.; Wang, K.; Zhu, J.; Yoon, H.E.; Wang, X.; Kerkhofs, M.; Kang, H.; Brown, A.L.; Park, S.J.; Xu, X.; Zandee van Rilland, E.; Kim, M.K.; Cohen, J.I.; Kaplan, M.J.; Shoshan-Barmatz, V.; Chung, J.H. VDAC oligomers form mitochondrial pores to release mtDNA fragments and promote lupus-like disease. Science. 2019, 366, 1531–1536. [Google Scholar] [CrossRef]
- Rosenberg, P. VDAC2 as a novel target for heart failure: Ca2+ at the sarcomere, mitochondria and SR. Cell Calcium. 2022, 104, 102586. [Google Scholar] [CrossRef]
- Martin, C.A.; Huang, C.L.; Matthews, G.D. The role of ion channelopathies in sudden cardiac death: implications for clinical practice. Ann Med. 2013, 45, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, C.T.; Owen, T.; Lawal, S.; Cao, S.; Pandey, S.S.; Yang, H.Y.; Song, W.; Wilkinson, R.; Alvarez-Laviada, A.; Gehmlich, K.; Marston, S.B.; MacLeod, K.T. Age- and strain-related aberrant Ca2+ release is associated with sudden cardiac death in the ACTC E99K mouse model of hypertrophic cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H1213–H1226. [Google Scholar] [CrossRef] [PubMed]
- Striessnig, J. Voltage-Gated Ca2+/ Channel α1-Subunit de novo Missense Mutations: Gain or Loss of Function - Implications for Potential Therapies. Front. Synaptic Neurosci. 2021, 13, 634760. [Google Scholar] [CrossRef] [PubMed]
- Galetin, T.; Tevoufouet, E.E.; Sandmeyer, J.; Matthes, J.; Nguemo, F.; Hescheler, J.; Weiergräber, M.; Schneider,T. Pharmacoresistant Cav2·3 (E-type/R-type) voltage-gated calcium channels influence heart rate dynamics and may contribute to cardiac impulse conduction. Cell Biochemistry Funct. 2013, 31, 434–449. [Google Scholar] [CrossRef] [PubMed]
- Priest, B.T.; McDermott, J.S. Cardiac ion channels. Channels (Austin). 2015, 9, 52–359.
- Fernández-Quintero, M.L.; El Ghaleb, Y.; Tuluc, P.; Campiglio, M.; Liedl, K.R.; Flucher, B.E. Structural determinants of voltage-gating properties in calcium channels. Elife. PMCID: PMC8099428. 2021, 10, e64087. [Google Scholar] [CrossRef] [PubMed]
- Catterall, W.A. Signaling complexes of voltage-gated sodium and calcium channels, 486,107–16. Neurosci Lett.
- Mangoni, M.E.; Couette, B.; Marger, L.; Bourinet, E.; Striessnig, J.; Nargeot, J. Voltage-dependent calcium channels and cardiac pacemaker activity: from ionic currents to genes. Prog. Biophys. Mol. Biol. 2006, 90, 38–63. [Google Scholar] [CrossRef] [PubMed]
- Harraz, O.F.; Jensen, L.J. Vascular calcium signalling and ageing. J. Physiol. 2021, 599, 5361–5377. [Google Scholar] [CrossRef]
- Betzenhauser, M.J.; Pitt, G.S.; Antzelevitch, C. Calcium Channel Mutations in Cardiac Arrhythmia Syndromes. Curr. Mol. Pharmacol. 2015, 8, 133–142. [Google Scholar] [CrossRef]
- Torrente, A.G.; Mesirca, P.; Bidaud, I.; Mangoni, M.E. Channelopathies of voltage-gated L-type Cav1.3/α1D and T-type Cav3.1/α1G Ca2+channels in dysfunction of heart automaticity. Pflugers Arch. 2020, 472, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Baudot, M.; Louradour, J.; Torrente, A.G.; Fossier, L.; Talssi, L.; Nargeot, J.; Barrère-Lemaire, S.; Mesirca, P.; Mangoni, M.E. Concomitant genetic ablation of L-type Cav1.3 (α1D) and T-type Cav3.1 (α1G) Ca2+ channels disrupts heart automaticity. Sci Rep. 2020, 10, 18906. [Google Scholar] [CrossRef]
- Harvey, R.D.; Hell, J.W. Cav1.2 signaling complexes in the heart. J. Mol. Cell Cardiol. 2013, 58, 143–152. [Google Scholar] [CrossRef]
- Varró, A.; Tomek, J.; Nagy, N.; Virág, L.; Passini, E.; Rodriguez, B.; Baczkó, I. Cardiac transmembrane ion channels and action potentials: cellular physiology and arrhythmogenic behavior. Physiol. Rev. 2021, 101, 1083–1176. [Google Scholar] [CrossRef] [PubMed]
- Tester, D.J.; Ackerman, M.J. Genetics of long QT syndrome. Methodist Debakey Cardiovasc. J. 2014, 10, 29–33. [Google Scholar] [CrossRef]
- Gakenheimer-Smith, L.; Meyers, L.; Lundahl, D.; Menon, S.C.; Bunch, T.J.; Sawyer, B.L.; Tristani-Firouzi, M.; Etheridge, S.P. Expanding the phenotype of CACNA1C mutation disorders. Mol. Genet. Genomic. Med. 2021, 9, e1673. [Google Scholar] [CrossRef]
- Harrell, D.T.; Ashihara, T.; Ishikawa, T.; Tominaga, I.; Mazzanti, A.; Takahashi, K.; Oginosawa, Y.; Abe, H.; Maemura, K.; Sumitomo, N.; Uno, K.; Takano, M.; Priori, S.G.; Makita, N. Genotype-dependent differences in age of manifestation and arrhythmia complications in short QT syndrome. Int. J. Cardiol. 2015, 190, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Zhong, R.; Zhang, F.; Yang. Z.; Li, Y.; Xu, Q.; Lan, H.; Cyganek, L.; El-Battrawy, I.; Zhou X.; Akin, I.; Borggrefe, M. Epigenetic mechanism of L-type calcium channel β-subunit downregulation in short QT human induced pluripotent stem cell-derived cardiomyocytes with CACNB2 mutation. Europace. 2022, 24, 2028–2036. [Google Scholar] [CrossRef] [PubMed]
- Van Petegem, F.; Clark, K.A.; Chatelain, F.C.; Minor, D.L. Structure of a complex between a voltage-gated calcium channel beta-subunit and an alpha-subunit domain. Nature. 2004, 429, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Alings; M. ; Wilde, A. “Brugada” syndrome: clinical data and suggested pathophysiological mechanism. Circulation. 1999, 99, 666–673. [Google Scholar] [CrossRef]
- Ednie, A.R.; Bennett, E.S. Intracellular O-linked glycosylation directly regulates cardiomyocyte L-type Ca(2+) channel activity and excitation-contraction coupling. Basic Res. Cardiol. 2020, 115, 59. [Google Scholar] [CrossRef]
- Angelini, M.; Pezhouman, A.; Savalli, N.; Chang, M.G.; Steccanella, F.; Scranton, K.; Calmettes, G.; Ottolia, M.; Pantazis, A.; Karagueuzian, H.S.; Weiss, J.N; Olcese, R. Suppression of ventricular arrhythmias by targeting late L-type Ca2+ current. J. Gen. Physiol. 2021, 153, e202012584. [Google Scholar] [CrossRef]
- Ito, D.W.; Hannigan, K.I.; Ghosh, D.; Xu, B.; Del Villar, S.G.; Xiang, Y.K; Dickson, E.J.; Navedo, M.F.; Dixon, R.E. β-adrenergic-mediated dynamic augmentation of sarcolemmal CaV1.2 clustering and co-operativity in ventricular myocytes. J. Physiol, 2019; 597, 2139–2162, PMCID: PMC6462464. [Google Scholar] [CrossRef] [PubMed]
- Neumaier, F.; Schneider, T.; Albanna, W. Cav2.3 channel function and Zn2+induced modulation: potential mechanisms and (patho)physiological relevance. Channels (Austin). 2020, 14, 362–379. [Google Scholar] [CrossRef]
- Tevoufouet, E.E.; Nembo, E.N.; Distler, F.; Neumaier, F.; Hescheler, J.; Nguemo, F.; Schneider, T. Multiple nickel-sensitive targets elicit cardiac arrhythmia inisolated mouse hearts after pituitary adenylate cyclase-activatingpolypeptide-mediated chronotropy. Pharmacol Res. 2017, 117, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.; Alpdogan, S.; Hescheler, J.; Neumaier, F. In vitro and in vivo phosphorylation of the Cav2.3 voltage-gated R-type calcium channel. Channels (Austin). 2018, 12, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Wang, Y.; Wang, Z.; Fan, X.; Wu, D.; Huang, J.; Mueller, A.; Gao, S.; Hu, M.; Robinson, C.V.; Yu, Y.; Gao, S.; Yan, N. Structures of the R-type human Cav2.3 channel reveal conformational crosstalk of the intracellular segments. Nat. Commun. 2022, 13, 7358. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.; Neumaier, F.; Hescheler, J.; Alpdogan, S. Cav2.3 R-type calcium channels: from its discovery to pathogenic de novo CACNA1E variants: a historical perspective. Pflugers Arch. 2020, 472, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Vassort, G.; Talavera, K.; Alvarez, J.L. Role of T-type Ca2+ channels in the heart. Cell Calcium. 2006, 40, 205–220. [Google Scholar] [CrossRef] [PubMed]
- Weiss, N.; Zamponi, G.W. Genetic T-type calcium channelopathies. J. Med. Genet. 2020, 57, 1–10. [Google Scholar] [CrossRef]
- Cribbs, L.L.; Lee, J.H.; Yang, J.; Satin, J.; Zhang, Y.; Daud, A.; Barclay, J.; Williamson, M.P.; Fox, M.; Rees, M.; Perez-Reyes, E. Cloning and characterization of alpha1H from human heart, a member of the T-type Ca2+ channel gene family. Circ. Res. 1998, 83, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Dastidar, S.; Majumdar, D.; Tipanee, J.; Singh, K.; Klein, A.F.; Furling, D.; Chuah, M.K.; VandenDriessche, T. Comprehensive transcriptome-wide analysis of spliceopathy correction of myotonic dystrophy using CRISPR-Cas9 in iPSCs-derived cardiomyocytes. Mol. Ther., 2022, 30, 75–91. [Google Scholar] [CrossRef]
- Petri, H.; Vissing, J.; Witting, N.; Bundgaard, H.; Køber, L. Cardiac manifestations of myotonic dystrophy type 1. Int. J. Cardiol. 2012, 160, 82–88. [Google Scholar] [CrossRef]
- Yasui, K.; Niwa, N.; Takemura, H.; Opthof, T.; Muto, T.; Horiba, M.; Shimizu, A.; Lee, J.K.; Honjo, H.; Kamiya, K.; Kodama, I. Pathophysiological significance of T-type Ca2+ channels: expression of T-type Ca2+ channels in fetal and diseased heart. J. Pharmacol. Sci. 2005, 99, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Bodi, I.; Correll, R.N.; Chen, X.; Lorenz, J.; Houser, S.R.; Robbins, J. α1G-dependent T-type Ca2+ current antagonizes cardiac hypertrophy through a NOS3-dependent mechanism in mice. J. Clin. Invest. 2009, 119, 3787–3796. [Google Scholar] [CrossRef] [PubMed]
- Kushnir, A.; Wajsberg, B.; Marks, A.R. Ryanodine receptor dysfunction in human disorders. Biochim. Biophys. Acta Mol. Cell Res. 2018, 1865, 1687–1697. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Kurebayashi, N.; Yamazawa, T.; Murayama, T. Regulatory mechanisms of ryanodine receptor/Ca2+release channel revealed by recent advancements in structural studies. J. Muscle Res. Cell Motil. 2021, 42, 291–304. [Google Scholar] [CrossRef]
- Hamilton, S.L.; Serysheva, II. Ryanodine receptor structure: progress and challenges. J. Biol. Chem. 2009, 284, 4047–4051. [Google Scholar] [CrossRef] [PubMed]
- Correll, R.N.; Goonasekera, S.A.; van Berlo, J.H.; Burr, A.R.; Accornero, F.; Zhang, H.; Makarewich, C.A.; York, A.J.; Sargent, M.A.; Chen, X.; Houser, S.R.; Molkentin, J.D. STIM1 elevation in the heart results in aberrant Ca2+ handling and cardiomyopathy. J. Mol. Cell Cardiol. 2015, 87, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhou, M.Y.; Kuang SJ, Qin, X. Y.; Cai, Y.J.; Chen, S.Z.; Li, S.M.; Rao, F.; Yang, H.; Deng, C.Y. Differential role of STIM1 in calcium handling in coronary and intrarenal arterial smooth muscles. Eur. J. Pharmacol. 2022, 937, 175386. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.; Katz, D.; Bryson, V. SOCE and STIM1 signaling in the heart: Timing and location matter. Cell Calcium. 2019, 77, 20–28. [Google Scholar] [CrossRef]
- Lakatta, E.G.; Vinogradova, T.M.; Maltsev, V.A. The missing link in the mystery of normal automaticity of cardiac pacemaker cells. Ann. N. Y. Acad. Sci. 2008, 1123, 41–57. [Google Scholar] [CrossRef]
- Xue, J.B.; Val-Blasco, A.; Davoodi, M.; Gómez, S.; Yaniv, Y.; Benitah, J.P.; Gómez, A.M. Heart failure in mice induces a dysfunction of the sinus node associated with reduced CaMKII signaling. J. Gen. Physiol. 2022, 154, e202112895. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Mesirca, P.; Marqués-Sulé, E.; Zahradnikova, A. Jr.; Villejoubert, O.; D'Ocon, P.; Ruiz, C.; Domingo, D.; Zorio, E.; Mangoni, M.E.; Benitah, J.P.; Gómez, A.M. RyR2R420Q catecholaminergic polymorphic ventricular tachycardia mutation induces bradycardia by disturbing the coupled clock pacemaker mechanism. JCI Insight. 2017, 2, e91872. [Google Scholar] [CrossRef]
- Wei, J.; Yao, J.; Belke, D.; Guo, W.; Zhong, X.; Sun, B.; Wang, R.; Paul Estillore, J.; Vallmitjana, A.; Benitez, R.; Hove-Madsen, L.; Alvarez-Lacalle, E.; Echebarria, B.; Chen, S.R.W. Ca2+-CaM Dependent Inactivation of RyR2 Underlies Ca2+ Alternans in Intact Heart. Circ. Res. 2021, 128, e63–e83. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Guo, T.; Oda, T.; Chakraborty, A.; Chen, L.; Uchinoumi, H.; Knowlton, A.A.; Fruen, B.R.; Cornea, R.L.; Meissner, G.; Bers, D.M. Cardiac myocyte Z-line calmodulin is mainly RyR2-bound, and reduction is arrhythmogenic and occurs in heart failure. Circ. Res. 2014, 114, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, N.; Takahashi, N.; Xu, L.; Smithies, O.; Meissner, G. Early cardiac hypertrophy in mice with impaired calmodulin regulation of cardiac muscle Ca2+ release channel. J. Clin. Invest. 2007, 117, 1344–1353. [Google Scholar] [CrossRef]
- Liu, B.; Walton, S.D.; Ho, H.T.; Belevych, A.E.; Tikunova, S.B.; Bonilla, I.; Shettigar, V.; Knollmann, B.C.; Priori, S.G.; Volpe, P.; Radwański, P.B.; Davis, J.P.; Györke, S. Gene Transfer of Engineered Calmodulin Alleviates Ventricular Arrhythmias in a Calsequestrin-Associated Mouse Model of Catecholaminergic Polymorphic Ventricular Tachycardia. J. Am. Heart Assoc. 2018, 7, e008155. [Google Scholar] [CrossRef] [PubMed]
- Yue, X.; Hazan, A.; Lotteau, S.; Zhang, R.; Torrente, A.G.; Philipson, K.D.; Ottolia, M.; Goldhaber, J.I. Na/Ca exchange in the atrium: Role in sinoatrial node pacemaking and excitation-contraction coupling. Cell Calcium. 2020, 87, 102167. [Google Scholar] [CrossRef]
- Li, M.C.H.; O'Brien, T.J.; Todaro, M.; Powell, K.L. Acquired cardiac channelopathies in epilepsy: Evidence, mechanisms, and clinical significance. Epilepsia. 2019, 60, 1753–1767. [Google Scholar] [CrossRef] [PubMed]
- Humphries, E.S.A.; Kamishima, T.; Quayle, J.M.; Dart, C. Calcium/calmodulin-dependent kinase 2 mediates Epac-induced spontaneous transient outward currents in rat vascular smooth muscle. J. Physiol. 2017, 595, 6147–6164. [Google Scholar] [CrossRef]
- Ezeani, M.; Prabhu, S. PI3K(p110α) as a determinant and gene therapy for atrial enlargement in atrial fibrillation. Mol. Cell Biochem. 2022, 478, 471–490. [Google Scholar] [CrossRef]
- Potenza, D.M.; Janicek, R.; Fernandez-Tenorio, M.; Camors, E.; Ramos-Mondragón, R.; Valdivia, H.H.; Niggli, E. Phosphorylation of the ryanodine receptor 2 at serine 2030 is required for a complete β-adrenergic response. J. Gen. Physiol. 2019, 151, 131–145. [Google Scholar] [CrossRef]
- Sirenko, S.T., Zahanich, I.; Li, Y.; Lukyanenko, Y.O.; Lyashkov, A.E.; Ziman, B.D.; Tarasov, K.V.; Younes, A.; Riordon, D.R.; Tarasova, Y.S.; Yang, D.; Vinogradova, T.M.; Maltsev, V.A.; Lakatta EG. Phosphoprotein Phosphatase 1 but Not 2A Activity Modulates Coupled-Clock Mechanisms to Impact on Intrinsic Automaticity of Sinoatrial Nodal Pacemaker Cells. Cells PMCID: PMC8623309. 2021, 10, 3106. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Kushner, J.; Marx, S.O. Adrenergic Regulation of Calcium Channels in the Heart. Annu Rev Physiol. 2022, 84, 285–306. [Google Scholar] [CrossRef] [PubMed]
- Hulsurkar, M.M.; Lahiri, S.K.; Karch, J.; Wang, M.C.; Wehrens, X.H.T. Targeting calcium-mediated inter-organellar crosstalk in cardiac diseases. Expert Opin, Ther, Targets. 2022, 26, 303–317. [Google Scholar] [CrossRef]
- Chopra, N.; Knollmann, B.C. Triadin regulates cardiac muscle couplon structure and microdomain Ca(2+) signalling: a path towards ventricular arrhythmias. Cardiovasc. Res. 2013, 98, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Mirza, S.; Richardson, S.J.; Gallant, E.M.; Thekkedam, C.; Pace, S.M.; Zorzato, F.; Liu, D.; Beard, N.A.; Dulhunty, A.F. A new cytoplasmic interaction between junctin and ryanodine receptor Ca2+ release channels. J. Cell Sci. 2015, 128, 951–963, PMCID: PMC4342579. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Wang, L.; Han, L.; Wang, Y.; Zhou, Y.; Li, Q.; Wu, Y.; Talabieke, S.; Hou, Y.; Wu, L.; Liu, R.; Fu, Z.; You, H.; Li, B.Y.; Zheng, Y.; Luo, D. Functional Calsequestrin-1 Is Expressed in the Heart and Its Deficiency Is Causally Related to Malignant Hyperthermia-Like Arrhythmia. Circulation. 2021, 144, 788–804. [Google Scholar] [CrossRef] [PubMed]
- Brandenburg, S.; Pawlowitz, J.; Steckmeister, V.; Subramanian, H.; Uhlenkamp, D.; Scardigli, M.; Mushtaq, M.; Amlaz, S.I.; Kohl, T.; Wegener, J.W.; Arvanitis, D.A.; Sanoudou, D.; Sacconi, L.; Hasenfub, G.; Voigt, N.; Nikolaev, V.O.; Lehnart, S.E. A junctional cAMP compartment regulates rapid Ca2+signaling in atrial myocytes. J. Mol. Cell Cardiol. 2022, 165, 141–157. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Liu, X.; Gong, Y.; Zhang, P.; Qiang, S.; Zhao, Q.; Guo, R.; Qian, Y.; Wang, L.; Zhu, L.; Wang, R.; Hao, Z.; Wen, H.; Zhang, J.; Tang, K.; Zang, W.F.; Yuchi, Z.; Chen, H.; Chen, S.R.W.; Zheng, W.; Wang, S.Q.; Xu, Y.W.; Liu, Z. Pathogenic mechanism of a catecholaminergic polymorphic ventricular tachycardia causing-mutation in cardiac calcium release channel RyR2. J. Mol. Cell Cardiol. 2018, 117, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Heijman, J.; Ghezelbash, S.; Wehrens, X.H.; Dobrev, D. Serine/Threonine Phosphatases in Atrial Fibrillation. J. Mol. Cell Cardiol. 2017, 103, 110–120. [Google Scholar] [CrossRef]
- Klapproth, E.; Kämmerer, S.; El-Armouche, A. Function and regulation of phosphatase 1 in healthy and diseased heart. Cell Signal. 2022, 90, 110203. [Google Scholar] [CrossRef] [PubMed]
- Sovari, A.A.; Iravanian, S.; Dolmatova, E.; Jiao, Z.; Liu, H.; Zandieh, S.; Kumar, V.; Wang, K.; Bernstein, K.E.; Bonini, M.G.; Duffy, H.S.; Dudley, S.C. Inhibition of c-Src tyrosine kinase prevents angiotensin II-mediated connexin-43 remodeling and sudden cardiac death. J. Am. Cell Cardiol. 2011, 58, 2332–2339. [Google Scholar] [CrossRef]
- Potenza, D.M.; Janicek, R.; Fernandez-Tenorio, M.; Niggli, E. Activation of endogenous protein phosphatase 1 enhances the calcium sensitivity of the ryanodine receptor type 2 in murine ventricular cardiomyocytes. J. Physiol. 2020, 598, 1131–1150. [Google Scholar] [CrossRef] [PubMed]
- Said, M.; Becerra, R.; Valverde, C.A.; Kaetzel, M.A.; Dedman, J.R.; Mundiña-Weilenmann, C.; Wehrens, X.H.; Vittone, L.; Mattiazzi, A. Calcium-calmodulin dependent protein kinase II (CaMKII): a main signal responsible for early reperfusion arrhythmias. J. Mol. Cell Cardiol. 2011, 51, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Bers, D.M.; Grandi, E. Calcium/calmodulin-dependent kinase II regulation of cardiac ion channels. J. Cardiovasc. Pharmacol. 2009, 54, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.L.; Chuang, H.L.; Chen, Y.C.; Kao, Y.H.; Lin, Y.K.; Yeh, Y.H.; Chen, S.A.; Chen, Y.J. Heart failure modulates electropharmacological characteristics of sinoatrial nodes. Exp. Ther. Med. 2017, 13, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, J.; Liu, Y.; Zhang, J.; Zheng, X.; Sun, X.; Lei, S.; Kang, Z.; Chen, X.; Lei, M.; Hu, H.; Zeng, X.; Hao, L. Distinct roles of calmodulin and Ca2+calmodulin-dependent protein kinase II in isopreterenol-induced cardiac hypertrophy. Biochem. Biophys. Res. Commun. 2020, 526, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Q.; Wang, L.P.; Gong, Y.Y.; Fan, X.X.; Zhu, S.Y.; Wang, X.T.; Wang, Y.P.; Li, L.L.; Xing, X.; Liu, X.X.; Ji, G.S.; Hou, T.; Zhang, Y.; Xiao, R.P.; Wang, S.Q. β2-Adrenergic Stimulation Compartmentalizes β1- Signaling Into Nanoscale Local Domains by Targeting the C-Terminus of β1-Adrenoceptors. Circ. Res. 2019, 124, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- Demydenko, K.; Sipido, K.R.; Roderick, H.L. Ca2+ release via InsP3Rs enhances RyR recruitment during Ca2+ transients by increasing dyadic [Ca2+] in cardiomyocytes. J. Cell Sci. 2021, 134, jcs258671. [Google Scholar] [CrossRef]
- Jin, X.; Amoni, M.; Gilbert, G.; Dries, E.; Doñate Puertas, R.; Tomar, A.; Nagaraju, C.K.; Pradhan, A.; Yule, D.I.; Martens, T.; Menten, R.; Vanden Berghe, P.; Rega, F.; Sipido, K.; Roderick, H.L. InsP3R-RyR Ca2+ channel crosstalk facilitates arrhythmias in the failing human ventricle. Basic. Res. Cardiol. 2022, 117. [Google Scholar] [CrossRef] [PubMed]
- Wehrens, X.H.; Lehnart, S.E.; Huang, F.; Vest, J.A.; Reiken, S.R.; Mohler, P.J.; Sun, J.; Guatimosim, S.; Song, L.S.; Rosemblit, N.; D'Armiento, J.M.; Napolitano, C.; Memmi, M.; Priori, S.G.; Lederer, W.J.; Marks, A.R. FKBP12.6 deficiency and defective calcium release channel (ryanodine receptor) function linked to exercise-induced sudden cardiac death. Cell. 2003, 113, 829-840. [CrossRef] [PubMed]
- Taur, Y.; Frishman, W.H. The cardiac ryanodine receptor (RyR2) and its role in heart disease. Cardiol. Rev. 2005, 13, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Dridi, H.; Kushnir, A.; Zalk, R.; Yuan, Q.; Melville, Z.; Marks, A.R. Intracellular calcium leak in heart failure and atrial fibrillation: a unifying mechanism and therapeutic target. Nat. Rev. Cardiol. 2020, 17, 732–747. [Google Scholar] [CrossRef]
- Chen, L.; Liu, R.; Wang, W.; Tang, C.; Ran, J.; Huang, W.; Li, S.; Liu, J. Chai-Hu-San-Shen Capsule Ameliorates Ventricular Arrhythmia Through Inhibition of the CaMKII/FKBP12.6/RyR2/Ca2+ Signaling Pathway in Rats with Myocardial Ischemia. Evid. Based Complement. Alternat. Med. 2022, 3, 2670473. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, C.; Mazzanti, A.; Priori, S.G. Genetic risk stratification in cardiac arrhythmias. Curr. Opin. Cardiol. 2018, 33, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Wleklinski, M.J.; Kannankeril, P.J.; Knollmann, B.C. Molecular and tissue mechanisms of catecholaminergic polymorphic ventricular tachycardia. J. Physiol. 2020, 598, 2817–2834. [Google Scholar] [CrossRef] [PubMed]
- Tiso, N.; Stephan, D.A.; Nava, A.; Bagattin, A.; Devaney, J.M.; Stanchi, F.; Larderet, G.; Brahmbhatt, B.; Brown, K.; Bauce, B.; Muriago, M.; Basso, C.; Thiene, G.; Danieli, G.A; Rampazzo, A. Identification of mutations in the cardiac ryanodine receptor gene in families affected with arrhythmogenic right ventricular cardiomyopathy type 2 (ARVD2). Hum. Mol. Genet. 2001, 10, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Koivisto, A.P.; Belvisi, M.G.; Gaudet, R.; Szallasi, A. Advances in TRP channel drug discovery: from target validation to clinical studies. Nat. Rev. Drug Discov. 2022, 21, 41–59. [Google Scholar] [CrossRef] [PubMed]
- Falcón, D.; Galeano-Otero, I.; Martín-Bórnez, M.; Fernández-Velasco, M.; Gallardo- Castillo, I.; Rosado, J.A.; Ordóñez, A.; Smani, T. TRPC Channels: Dysregulation and Ca2+/Mishandling in Ischemic Heart Disease. Cells. 2020, 9, 173. [Google Scholar] [CrossRef] [PubMed]
- Eder, P.; Molkentin, J.D. TRPC channels as effectors of cardiac hypertrophy. Circ. Res. 2011, 108, 265–272. [Google Scholar] [CrossRef] [PubMed]
- He, R.; Zhang, J.; Luo, D.; Yu, Y.; Chen, T.; Yang, Y.; Yu, F.; Li, M. Upregulation of Transient Receptor Potential Canonical Type 3 Channel via AT1R/TGF-iβ/i1/Smad2/3 Induces Atrial Fibrosis in Aging and Spontaneously Hypertensive Rats. Oxid. Med. Cell Longev. 2019, 23, 4025496, PMCID: PMC6906806. [Google Scholar] [CrossRef] [PubMed]
- Bogdanova, E.; Beresneva, O.; Galkina, O.; Zubina, I.; Ivanova, G.; Parastaeva, M.; Semenova, N.; Dobronravov, V. Myocardial Hypertrophy and Fibrosis Are Associated with Cardiomyocyte Beta-Catenin and TRPC6/Calcineurin/NFAT Signaling in Spontaneously Hypertensive Rats with 5/6 Nephrectomy. Int. J. Mol. Sci. 2021, 22, 4645. [Google Scholar] [CrossRef]
- Yan, J.; Honglei, Y.; Yun, W.; Sheng, D.; Yun, H.; Anhua, Z.; Na, F.; Min, L.; Dandan, S.; Jing, W.; Junming, T.; Wenjun, Z.; Xiju, H. Puerarin ameliorates myocardial remodeling of spontaneously hypertensive rats through inhibiting TRPC6-CaN-NFATc3 pathway. Eur. J. Pharmacol. 2022, 933, 175254. [Google Scholar] [CrossRef] [PubMed]
- Inoue, R.; Kurahara, L.H.; Hiraishi, K. TRP channels in cardiac and intestinal fibrosis. Semin. Cell Dev. Biol. 2019, 94, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalamo, K.; Montell, C. TRP channels. Annu Rev. Biochem. 2007, 76, 387–417. [Google Scholar] [CrossRef] [PubMed]
- Numaga-Tomita, T.; Nishida, M. TRPC Channels in Cardiac Plasticity. Cells. 2020, 9, 454. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Wilkin, B.J.; Bodi, I.; Molkentin, J.D. Calcineurin-dependent cardiomyopathy is activated by TRPC in the adult mouse heart. FASEB J. 2006, 20, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Satoh, S.; Tanaka, H.; Ueda, Y.; Oyama, J.; Sugano, M.; Sumimoto, H.; Mori, Y.; Makino, N. Transient receptor potential (TRP) protein 7 acts as a G protein-activated Ca2+channel mediating angiotensin II-induced myocardial apoptosis. Mol. Cell Biochem. 2007, 294, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Plummer, N.W.; George, M.D.; Abramowitz, J.; Zhu, M.X.; Birnbaumer, L. A role for Orai in TRPC-mediated Ca2+ entry suggests that a TRPC: Orai complex may mediate store and receptor operated Ca2+ entry. Proc. Natl. Acad. Sci U S A. 2009, 106, 3202–3206. [Google Scholar] [CrossRef]
- Ambudkar, I.S.; de Souza, L.B.; Ong, H.L. TRPC1, Orai1, and STIM1 in SOCE: Friends in tight spaces. Cell Calcium. 2017, 63, 33–39. [Google Scholar] [CrossRef]
- Dyrda, A.; Koenig, S.; Frieden, M. STIM1 long and STIM1 gate differently TRPC1 during store-operated calcium entry. Cell Calcium. 2020, 86, 102134. [Google Scholar] [CrossRef] [PubMed]
- Kühn, F.J.; Heiner, I.; Lückhoff, A. TRPM2: a calcium influx pathway regulated by oxidative stress and the novel second messenger ADP-ribose. Pflugers Arch. 2005, 451, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Ru, X.; Yao, X. TRPM2: a multifunctional ion channel for oxidative stress sensing. Sheng Li Xue Bao. 2014, 66, 7–15. [Google Scholar] [PubMed]
- Cheung, J.Y.; Miller, B.A. Transient Receptor Potential-Melastatin Channel Family Member 2: Friend or Foe. Trans. Am. Clin. Climatol. Assoc. 2017, 128, 308–329. [Google Scholar]
- Kruse, M.; Schulze-Bahr, E.; Corfield, V.; Beckmann, A.; Stallmeyer, B.; Kurtbay, G.; Ohmert, I.; Schulze-Bahr, E.; Brink, P.; Pongs, O. Impaired endocytosis of the ion channel TRPM4 is associated with human progressive familial heart block type I. J. Clin. Invest. 2009, 119, 2737–44. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Zong, P.; Yan, J.; Yue, Z.; Li, X.; Smith, C.; Ai, X.; Yue, L. Upregulation of transient receptor potential melastatin 4 (TRPM4) in ventricular fibroblasts from heart failure patients. Pflugers Arch. 2021, 473, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Du, R.; Fan, L.L.; Jin, J.Y.; Huang, H.; Chen, Y.Q.; Bi, D.D.; Xiang, R. Whole-Exome Sequencing Identifies a Novel TRPM4 Mutation in a Chinese Family with Atrioventricular Block. Biomed. Res. Int. 2021, 17, 9247541. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y,; Li, Q. ; Kurahara, L.H.; Shioi, N.; Hiraishi, K.; Fujita, T.; Zhu, X.; Inoue, R. An Arrhythmic Mutation E7K Facilitates TRPM4 Channel Activation via Enhanced PIP2 Interaction. Cells. 2021, 10, 983. [Google Scholar] [CrossRef] [PubMed]
- Sah, R.; Mesirca, P.; Mason, X.; Gibson, W.; Bates-Withers, C.; Van den Boogert, M.; Chaudhuri, D.; Pu, W.T.; Mangoni, M.E.; Clapham, D.E. Timing of myocardial trpm7 deletion during cardiogenesis variably disrupts adult ventricular function, conduction, and repolarization. Circulation. 2013, 128, 101–114. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, J.H.; Aziz, Q.; Harmer, S.C.; Thayyil, S.; Tinker, A.; Munroe, P.B. Genetic variants in TRPM7 associated with unexplained stillbirth modify ion channel function. Hum. Mol. Genet. 2020, 29, 1797–1807. [Google Scholar] [CrossRef]
- Conklin, D.J.; Guo, Y.; Nystoriak, M.A.; Jagatheesan, G.; Obal, D.; Kilfoil, P.J.; Hoetker, J.D.; Guo, L.; Bolli, R.; Bhatnagar, A. TRPA1 channel contributes to myocardial ischemia-reperfusion injury. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H889–H899. [Google Scholar] [CrossRef]
- Martín-Bórnez, M.; Galeano-Otero, I.; Del Toro, R.; Smani, T. ; TRPC and TRPV Channels' Role in Vascular Remodeling and Disease. Int. J. Mol. Sci. 2020, 21, 6125. [Google Scholar] [CrossRef]
- Üstünel, L.; Özgüler, I.M. The effects of iloprost and beta3 receptor agonist on TRPA1 and TRPC1 immunreactivity in an experimental lower extremty ischemia-reperfusion injury model. Turk. J. Med. Sci. 2021, 51, 2763–2770. [Google Scholar] [CrossRef]
- Uchida, K.; Kanematsu, M.; Sakai, K.; Matsuda, T.; Hattori, N.; Mizuno, Y.; Suzuki, D.; Miyata, T.; Noguchi, N.; Niki, E.; Osawa, T. Protein-bound acrolein: potential markers for oxidative stress. Proc. Natl. Acad. Sci U S A. 1998, 95, 4882–4887. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, L.J.; Dubin, A.E.; Evans, M.J.; Marr, F.; Schultz, P.G.; Cravatt, B.F.; Patapoutian, A. Noxious compounds activate TRPA1 ion channels through covalent modification of cysteines. Nature. 2007, 445, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q. , Ahmad, A.A.; Seidel, T.; Hunter, C.; Streiff, M.; Nikolova, L.; Spitzer, K.W.; Sachse, F.B. Location and function of transient receptor potential canonical channel 1 in ventricular myocytes. J. Mol. Cell Cardiol. 2020, 139, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Firth, A.L.; Remillard, C.V.; Yuan, J.X. TRP channels in hypertension. Biochim. Biophys. Acta. 2007, 1772, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Yue, Z.; Xie, J.; Yu, A.S.; Stock, J.; Du, J.; Yue, L. ; Role of TRP Channels in the Cardiovascular System. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H157–H182. [Google Scholar] [CrossRef] [PubMed]
- Andriulė, I.; Pangonytė, D.; Gwanyanya, A.; Karčiauskas, D.; Mubagwa, K.; Mačianskienė, R. Detection of TRPM6 and TRPM7 Proteins in Normal and Diseased Cardiac Atrial Tissue and Isolated Cardiomyocytes. Int. J. Mol. Sci. 2022, 23, 14860. [Google Scholar] [CrossRef]
- Hong, K.S.; Lee, M.G. Endothelial Ca2+ signaling-dependent vasodilation through transient receptor potential channels. Korean J. Physiol. Pharmacol. 2020, 24, 287–298. [Google Scholar] [CrossRef]
- Kochukov, M.Y.; Balasubramanian, A.; Noel, R.C.; Marrelli, S.P. Role of TRPC1 and TRPC3 channels in contraction and relaxation of mouse thoracic aorta. J. Vasc. Res. 2013, 50, 11–20. [Google Scholar] [CrossRef]
- Willette, R.N.; Bao, W.; Nerurkar, S.; Yue, T.L.; Doe, C.P.; Stankus, G.; Turner, G.H. , Ju, H.; Thomas, H.; Fishman, C.E.; Sulpizio, A.; Behm, D.J.; Hoffman, S.; Lin, Z.; Lozinskaya, I.; Casillas, L.N.; Lin, M.; Trout, R.E.; Votta, B.J.; Thorneloe, K.; Lashinger, E.S.; Figueroa, D.J.; Marquis, R.; Xu, X. Systemic activation of the transient receptor potential vanilloid subtype 4 channel causes endothelial failure and circulatory collapse: Part 2. J. Pharmacol. Exp. Ther. 2008, 326, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Earley, S.; Heppner, T.J.; Nelson, M.T.; Brayden, J.E. TRPV4 forms a novel Ca2+ signaling complex with ryanodine receptors and BKCa channels. Circ. Res. 2005, 97, 1270–1279. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Miguel, I.; Cidad, P.; Pérez-García, M.T.; López-López, J.R. Differences in TRPC3 and TRPC6 channels assembly in mesenteric vascular smooth muscle cells in essential hypertension. J. Physiol. 2017, 595, 1497–1513. [Google Scholar] [CrossRef]
- Mathar, I.; Vennekens, R.; Meissner, M.; Kees, F.; Van der Mieren, G.; Camacho Londoño, J.E.; Uhl, S.; Voets, T.; Hummel, B.; van den Bergh, A.; Herijgers, P.; Nilius, B.; Flockerzi, V.; Schweda, F.; Freichel, M. Increased catecholamine secretion contributes to hypertension in TRPM4-deficient mice. J. Clin. Invest. 2010, 120, 3267–3279. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Ching, L.C.; Zhao, J.F.; Shyue, S.K.; Lee, H.F.; Kou, Y.R.; Lee, T.S. Essential Role of Transient Receptor Potential Vanilloid Type 1 in Evodiamine-Mediated Protection Against Atherosclerosis. Acta Physiol. 2013, 207, 299–307. [Google Scholar] [CrossRef]
- Nishida, M.; Tanaka, T.; Mangmool, S.; Nishiyama, K.; Nishimura, A. Canonical Transient Receptor Potential Channels and Vascular Smooth Muscle Cell Plasticity. J. Lipid Atheroscler. 2020, 9, 124–139. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.; Rahaman, S.G.; Goswami, R.; Dutta, B.; Mahanty, M.; Rahaman, S.O. Role of mechanosensitive channels/receptors in atherosclerosis. Am. J. Physiol. Cell Physiol. 2022, 322, C927–C938. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhu, Z.; Tepel, M. The role of transient receptor potential channels in metabolic syndrome. Hypertens Res. 2008, 31, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, K.; Tanaka, T.; Nishimura, A.; Nishida, M. TRPC3-Based Protein Signaling Complex as a Therapeutic Target of Myocardial Atrophy. Curr. Mol. Pharmacol. 2021, 14, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Hiraishi, K.; Kurahara, L.H.; Ishikawa, K.; Go, T.; Yokota, N.; Hu, Y.; Fujita, T.; Inoue, R.; Hirano, K. Potential of the TRPM7 channel as a novel therapeutic target for pulmonary arterial hypertension. J. Smooth Muscle Res. 2022, 58, 50–62. [Google Scholar] [CrossRef]
- Lüthi, A.; McCormick, D.A. H-current: properties of a neuronal and network pacemaker. Neuron. 1998, 21, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, A.S.; Peigneur, S.; Tytgat, J. Review: HCN Channels in the Heart. Curr. Cardiol. Rev. 2022, 18, e040222200836. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, A.; Bauer, D.; Giese, M.H.; Swuec, P.; Porro, A.; Gasparri, F.; Sharifzadeh, A.S.; Chaves-Sanjuan, A.; Alberio, L.; Parisi, G.; Cerutti, G.; Clarke, O.B.; Hamacher, K.; Colecraft, H.M.; Mancia, F.; Hendrickson. W.A.; Siegelbaum, S.A.; DiFrancesco, D.; Bolognesi, M.; Thiel, G.; Santoro, B.; Moroni, A. Gating movements and ion permeation in HCN4 pacemaker channels. Mol. Cell. 2021, 81, 2929–2943. [Google Scholar] [CrossRef] [PubMed]
- Santoro, B.; Tibbs, G.R. The HCN gene family: molecular basis of the hyperpolarization-activated pacemaker channels. Ann. N. Y. Acad. Sci. 1999, 868, 741–764. [Google Scholar] [CrossRef] [PubMed]
- Biel, M.; Schneider, A.; Wahl, C. Cardiac HCN channels: Structure, function, and modulation. Trends Cardiovasc. Med. 2002, 12, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Cohen, I.S.; Robinson, R.B. Pacemaker current and automatic rhythms: toward a molecular understanding. Handb. Exp. Pharmacol. 2006, 171, 41–71. [Google Scholar] [CrossRef] [PubMed]
- Farraha, M; Kumar, S. ; Chong, J.; Cho, H.C.; Kizana, E. Gene Therapy Approaches to Biological Pacemakers. J. Cardiovasc. Dev. Dis. 2018, 5, 50, PMCID: PMC6306875. [Google Scholar] [CrossRef] [PubMed]
- Van Wagoner, D.R.; Lindsay, B.D. Phosphodiesterase-4 activity: a critical modulator of atrial contractility and arrhythmogenesis. J. Am. Coll. Cardiol. 2012, 59, 2191–2192. [Google Scholar] [CrossRef]
- Yu, X.; Chen, X.W.; Zhou, P.; Yao, L.; Liu, T.; Zhang, B.; Li, Y.; Zheng, H.; Zheng, L.H.; Zhang, C.X.; Bruce, I.; Ge, J.B.; Wang, S.Q.; Hu, Z.A.; Yu, H.G.; Zhou, Z. Calcium influx through If channels in rat ventricular myocytes. Am. J. Physiol Cell Physiol. 2007, 292, C1147–C1155. [Google Scholar] [CrossRef]
- Michels, G.; Brandt, M.C.; Zagidullin, N.; Khan, I.F.; Larbig, R.; van Aaken, S.; Wippermann, J.; Hoppe, U.C. Direct evidence for calcium conductance of hyperpolarization-activated cyclic nucleotide-gated channels and human native If at physiological calcium concentrations. Cardiovasc. Res. 2008, 78, 466–475. [Google Scholar] [CrossRef]
- Ide, T.; Ohtani, K.; Higo, T.; Tanaka, M.; Kawasaki, Y.; Tsutsui, H. Ivabradine for the treatment of cardiovascular diseases. Circ. J. 2019, 83, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Rivolta, I.; Binda, A.; Masi, A.; DiFrancesco, J.C. Cardiac and neuronal HCN channelopathies. Pflugers Arch. 2020, 472, 931–951. [Google Scholar] [CrossRef] [PubMed]
- Proenza, C.; Tran, N.; Angoli, D.; Zahynacz, K.; Balcar, P.; Accili, E.A. Different roles for the cyclic nucleotide binding domain and amino terminus in assembly and expression of hyperpolarization-activated, cyclic nucleotide-gated channels. J. Biol. Chem. 2002, 277, 29634–29642. [Google Scholar] [CrossRef]
- Pan, Y.; Laird, J.G.; Yamaguchi, D.M.; Baker, S.A. An N-terminal ER export signal facilitates the plasma membrane targeting of HCN1 channels in photoreceptors. Invest. Ophthalmol. Vis. Sci. 2015, 56, 3514–3521. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Blanco, I.; Hayoz, S.; Brelidze, T.I. The HCN domain is required for HCN channel cell-surface expression and couples voltage- and cAMP-dependent gating mechanisms. J. Biol. Chem. 2020, 295, 8164–8173. [Google Scholar] [CrossRef] [PubMed]
- Baruscotti, M.; Bucchi, A.; Difrancesco, D. Physiology and pharmacology of the cardiac pacemaker ("funny") current. Pharmacol. Ther. 2005, 107, 59–79. [Google Scholar] [CrossRef] [PubMed]
- Hennis, K.; Rötzer, R.D.; Piantoni, C.; Biel, M.; Wahl-Schott, C.; Fenske, S. Speeding Up the Heart? Traditional and New Perspectives on HCN4 Function. Front Physiol. 2021, 12, 669029. [Google Scholar] [CrossRef] [PubMed]
- Wahl-Schott, C.; Biel, M. HCN channels: structure, cellular regulation and physiological function. Cell. Mol. Life Sci. 2009, 66, 470–494. [Google Scholar] [CrossRef] [PubMed]
- Scicchitano, P.; Carbonara, S.; Ricci, G.; Mandurino, C.; Locorotondo, M.; Bulzis, G.; Gesualdo. M.; Zito, A.; Carbonara, R.; Dentamaro, I.; Riccioni, G.; Ciccone, M.M. HCN channels and heart rate. Molecules. 2012, 17, 4225–4235. [Google Scholar] [CrossRef]
- Hummert, S.; Thon, S.; Eick, T.; Schmauder, R.; Schulz, E.; Benndorf, K. Activation gating in HCN2 channels. PLoS Comput. Biol. 2018, 14, e1006045. [Google Scholar] [CrossRef]
- VanSchouwen, B.; Melacini, G. Regulation of HCN Ion Channels by Non-canonical Cyclic Nucleotides. Handb. Exp. Pharmacol. 2017, 238, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.H.; Singh, R.K.; Bankston, J.R.; Proenza, C. Regulation of HCN Channels by Protein Interactions. Front. Physiol. 2022, 13, 928507. [Google Scholar] [CrossRef]
- Erlenhardt, N.; Kletke, O.; Wohlfarth, F.; Komadowski, M.A.; Clasen, L.; Makimoto, H; Rinné, S. ; Kelm, M.; Jungen, C.; Decher, N.; Meyer, C.; Klöcker, N. Disease-associated HCN4 V759I variant is not sufficient to impair cardiac pacemaking. Pflugers Arch. 2020, 472, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Hattori, K.; Nakamura, K.; Hisatomi, Y.; Matsumoto, S.; Suzuki, M.; Harvey, R.P.; Kurihara, H.; Hattori, S.; Yamamoto, T.; Michalak, M.; Endo, F. Arrhythmia induced by spatiotemporal overexpression of calreticulin in the heart. Mol. Genet. Metab. 2007, 91, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Saeed, Y.; Temple, I.P.; Borbas, Z.; Atkinson, A.; Yanni, J.; Maczewski, M.; Mackiewicz, U.; Aly, M.; Logantha, S.J.R.J.; Garratt, C.J.; Dobrzynski, H. Structural and functional remodeling of the atrioventricular node with aging in rats: The role of hyperpolarization-activated cyclic nucleotide-gated and ryanodine 2 channels. Heart Rhythm. 2018, 15, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Farraha, M.; Kumar, S.; Chong, J.; Cho, H.C.; Kizana, E. Gene Therapy Approaches to Biological Pacemakers. J. Cardiovasc. Dev. Dis. 2018, 5, 50. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Plotnikov, A.N.; Danilo, P.; Shlapakova, I.; Cohen, I.S.; Robinson, R.B.; Rosen, M.R. Expression and function of a biological pacemaker in canine heart. Circulation. 2003, 107, 1106–1109. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Jin, K.; Zhou, J.; Gu. J.; Gu, X.; Dong, L.; Sun, X. G9a inhibition promotes the formation of pacemaker-like cells by reducing the enrichment of H3K9me2 in the HCN4 promoter region. Mol. Med. Rep. 2023, 27, 21. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.; Lin, L.Y.; Tsai, T.F. Use of calcium channel blockers in dermatology: a narrative review. Expert. Rev. Clin. Pharmacol. 2021, 14, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Kokilambigai, K.S.; Kavitha, J.; Seetharaman, R.; Lakshmi, K.S.; Sai Susmitha, A. Analytical and Bioanalytical Techniques for the Quantification of the Calcium Channel Blocker - Amlodipine: A Critical Review. Crit. Rev. Anal. Chem. 2021, 51, 754–786. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, D.A.; Ozer, L.Y.; Al Haj Zen, A. A Novel High Content Angiogenesis Assay Reveals That Lacidipine, L-Type Calcium Channel Blocker, Induces In Vitro Vascular Lumen Expansion. Int. J. Mol. Sci. 2022, 23, 4891. [Google Scholar] [CrossRef]
- Rabah, F.; El-Naggari, M.; Al-Nabhani, D. Amlodipine: The double edged sword. J. Paediatr. Child Health. 2017, 53, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Kung, J.Y.; Mitchelmore, B.; Cave, A.; Banh, H.L. Comparative peripheral edema for dihydropyridines calcium channel blockers treatment: A systematic review and network meta-analysis. J. Clin. Hypertens. (Greenwich). 2022, 24, 536–554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liang, R.; Wang, K.; Zhang, W.; Zhang, M.; Jin, L.; Xie, P.; Zheng, W.; Shang, H.; Hu, Q.; Li, J.; Chen, G.; Wu, F.; Lan, F.; Wang, L.; Wang, S.Q.; Li, Y.; Zhang, Y.; Liu, J.; Lv, F.; Hu, X.; Xiao, R.P.; Lei, X.; Zhang, Y. Novel CaMKII-δ Inhibitor Hesperadin Exerts Dual Functions to Ameliorate Cardiac Ischemia/Reperfusion Injury and Inhibit Tumor Growth. Circulation. 2022, 145, 1154–1168. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Li, F.; Zhang, M.; Jin, L.; Xie, P.; Liu, D.; Zhang, J.; Hu, X.; Lv, F.; Shang, H.; Zheng W, Sun X, Duanmu J, Wu F, Lan F, Xiao RP, Zhang Y. Targeting CaMKII-δ9 Ameliorates Cardiac Ischemia/Reperfusion Injury by Inhibiting Myocardial Inflammation. Circ. Res. 2022, 130, 887–903. [Google Scholar] [CrossRef] [PubMed]
- Xia, H.; Zahra, A.; Jia, M.; Wang, Q.; Wang, Y.; Campbell, S.L.; Wu, J. Na+/H+ Exchanger 1, a Potential Therapeutic Drug Target for Cardiac Hypertrophy and Heart Failure. Pharmaceuticals (Basel). 2022, 15, 875. [Google Scholar] [CrossRef] [PubMed]
- Kamel, R.; Leroy, J.; Vandecasteele, G.; Fischmeister, R. Cyclic nucleotide phosphodiesterases as therapeutic targets in cardiac hypertrophy and heart failure. Nat. Rev. Cardiol. 2023, 20, 90–108. [Google Scholar] [CrossRef] [PubMed]
- Mengesha, H.G.; Tafesse, T.B.; Bule, M.H. If Channel as an Emerging Therapeutic Target for Cardiovascular Diseases: A Review of Current Evidence and Controversies. Front. Pharmacol. 2017, 8, 874. [Google Scholar] [CrossRef]
- Ma, S.; Jiang, Y.; Huang, W.; Li, X.; Li, S. Role of Transient Receptor Potential Channels in Heart Transplantation: A Potential Novel Therapeutic Target for Cardiac Allograft Vasculopathy. Med. Sci Monit. 2017, 23, 2340–2347. [Google Scholar] [CrossRef]
- Cheraghi, M.; Negahdari, B.; Daraee, H.; Eatemadi, A. Heart targeted nanoliposomal/nanoparticles drug delivery: An updated review. Biomed. Pharmacother. 2017, 86, 316–323. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic representation of the pore-forming channel α1-subunit Cav1. (Modified by [16]).
Figure 1.
Schematic representation of the pore-forming channel α1-subunit Cav1. (Modified by [16]).
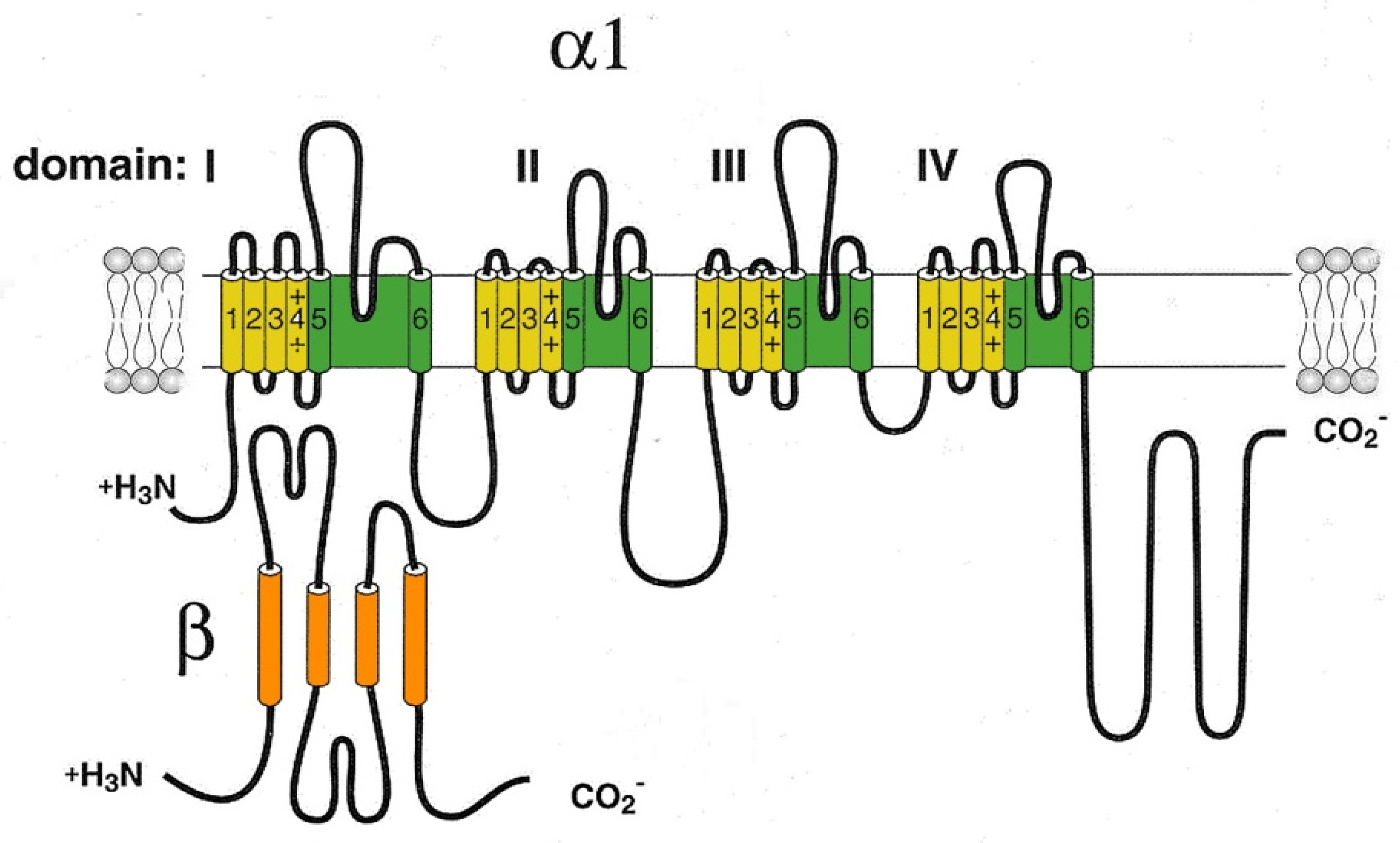
Figure 2.
The cardiac CaV1.2 channel signaling complex. ABD, AKAP15 binding domain; DCRD, distal C-terminal regulatory domain; PCRD, proximal C-terminal regulatory domain; scissors, site of proteolytic processing. (Modified by [16]).
Figure 2.
The cardiac CaV1.2 channel signaling complex. ABD, AKAP15 binding domain; DCRD, distal C-terminal regulatory domain; PCRD, proximal C-terminal regulatory domain; scissors, site of proteolytic processing. (Modified by [16]).
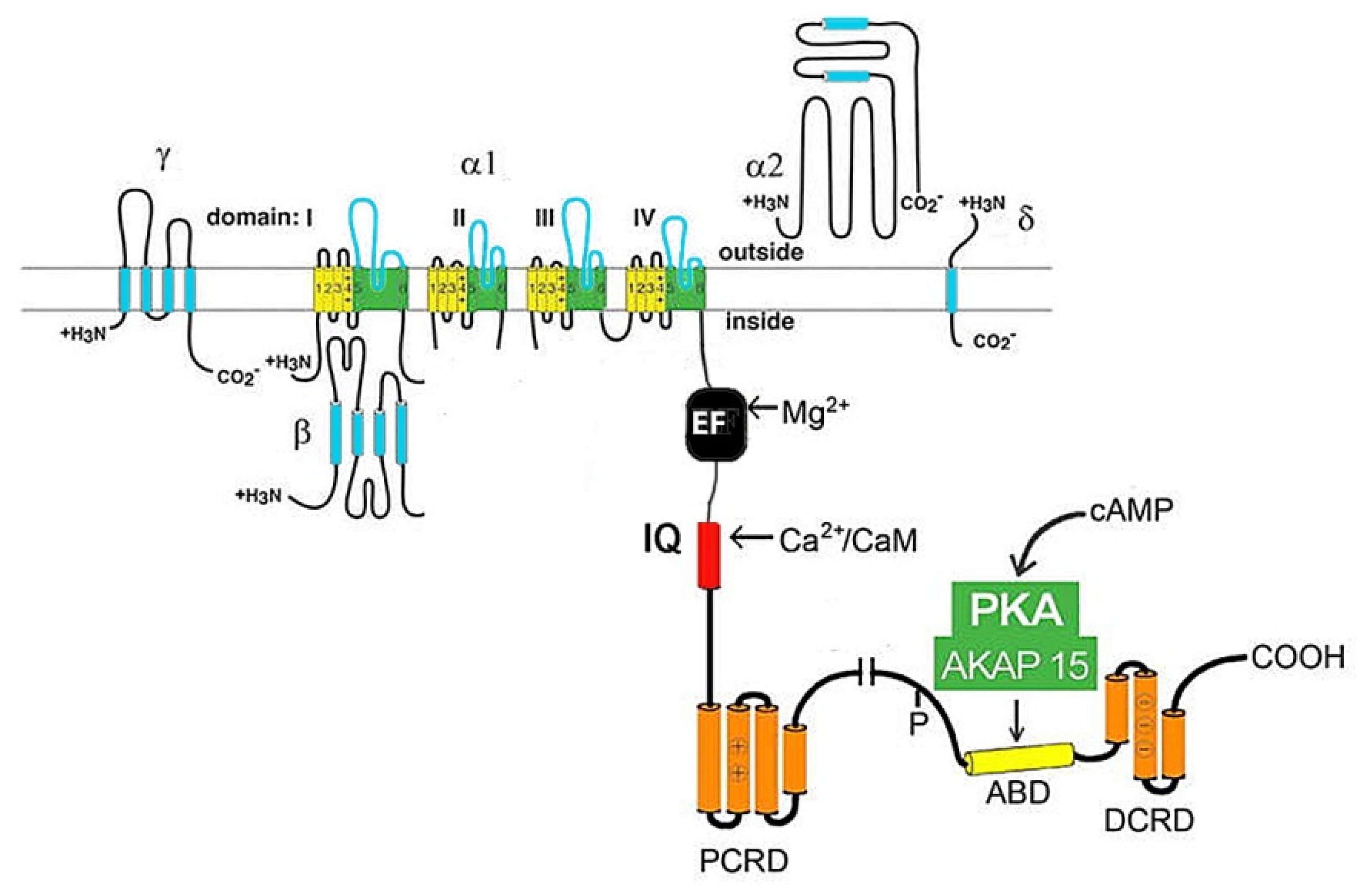
Figure 3.
Schematic representation of Cav3 α1-subunit. (Modify by [39]).
Figure 3.
Schematic representation of Cav3 α1-subunit. (Modify by [39]).
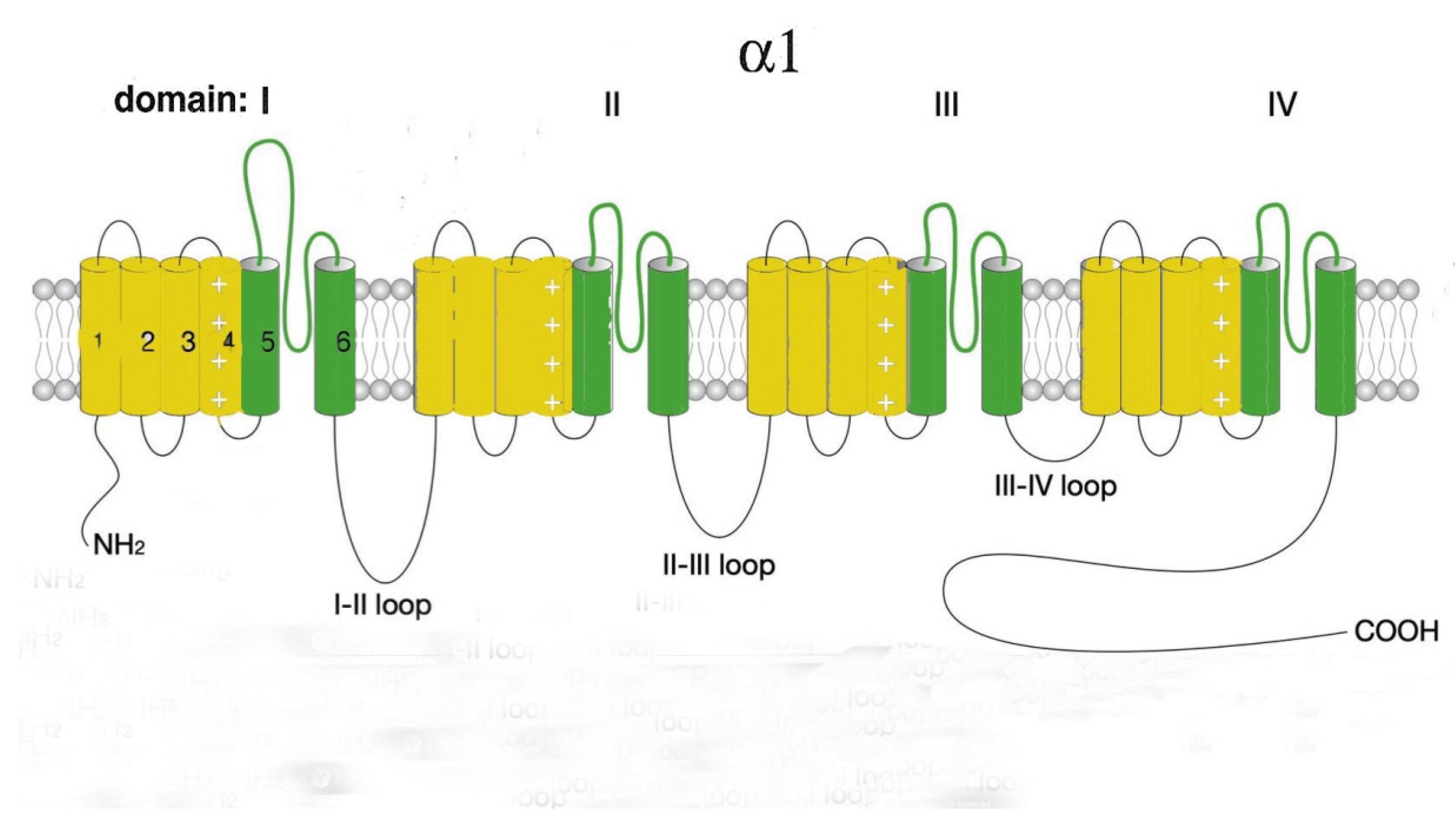
Figure 4.
Structural features of STIM1 (A) and Orai1 (B) proteins. Functional domains of proteins are enclosed in rectangles: EF – Ca(2+)-binding motif "EF-hands"; SAM – so-called "sterile"-α-motif (sterile-α-motif); TM – transmembrane domain; ERM – protein binding domain of the ERM complex; S/P-domain enriched with serine and proline; C-C – domain enriched with lysine; CAD – domain responsible for channel activation; SOAR, STIM1-Orai – activation region; PR domain enriched with proline and arginine; TM1-4 – transmembrane domains.
Figure 4.
Structural features of STIM1 (A) and Orai1 (B) proteins. Functional domains of proteins are enclosed in rectangles: EF – Ca(2+)-binding motif "EF-hands"; SAM – so-called "sterile"-α-motif (sterile-α-motif); TM – transmembrane domain; ERM – protein binding domain of the ERM complex; S/P-domain enriched with serine and proline; C-C – domain enriched with lysine; CAD – domain responsible for channel activation; SOAR, STIM1-Orai – activation region; PR domain enriched with proline and arginine; TM1-4 – transmembrane domains.
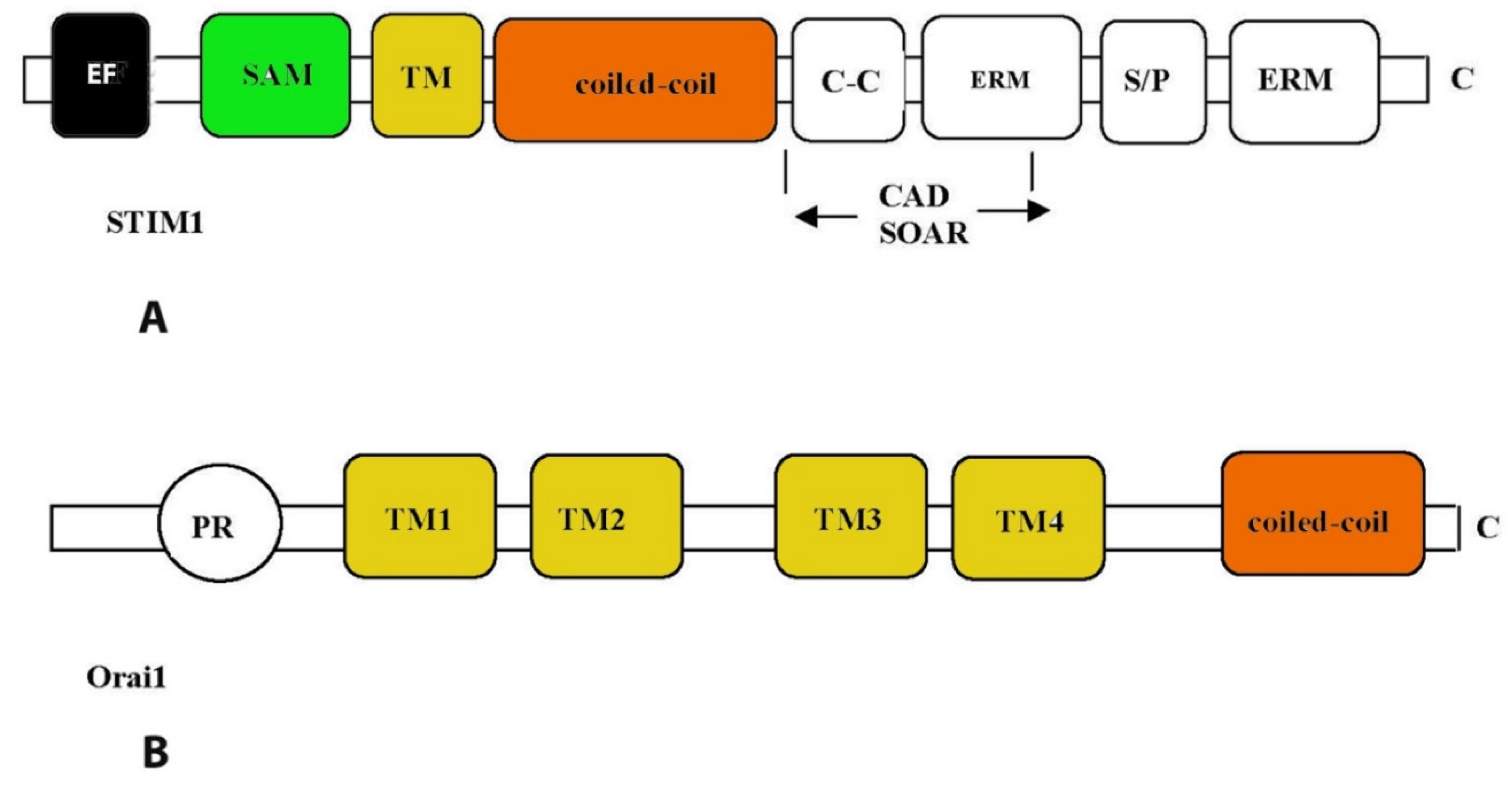
Figure 5.
Schematic representation of Trpm2 monomer structure. (Modify by [105]).
Figure 5.
Schematic representation of Trpm2 monomer structure. (Modify by [105]).
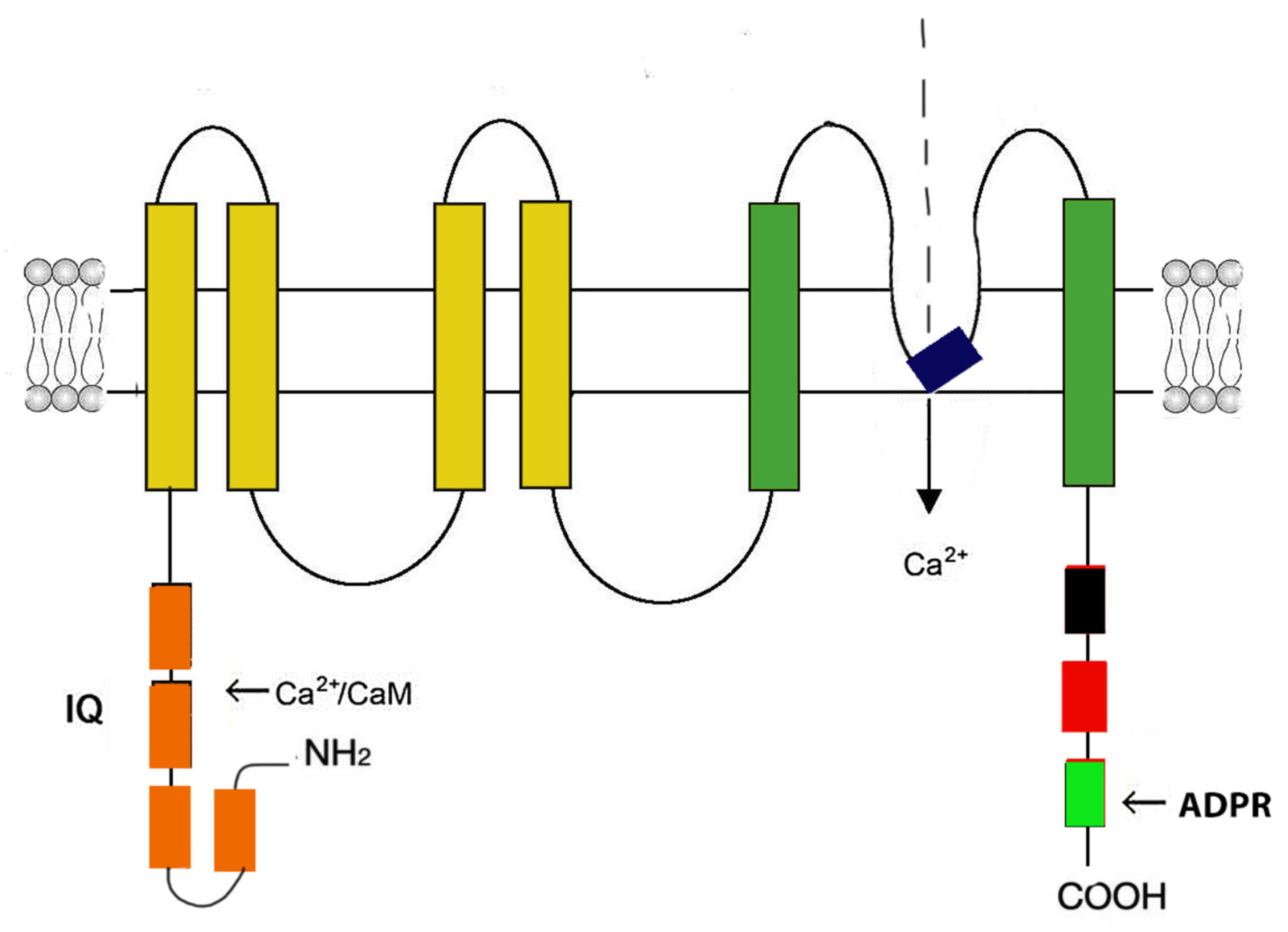
Figure 6.
Schematic representation of the HCN channel.
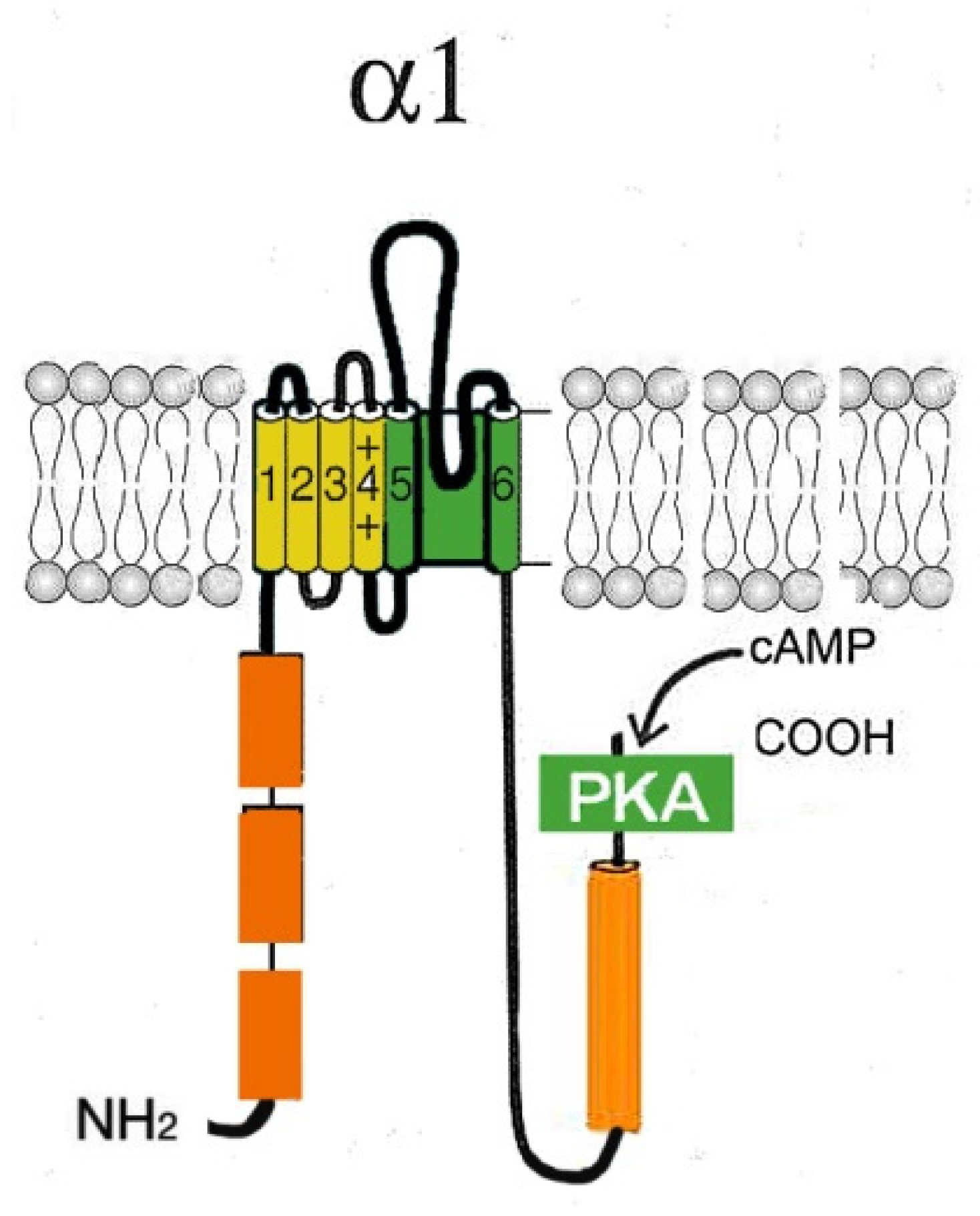

Table 1.
Са2+ channels and associated channelopathies. (Based on OMIM, Online Mendelian Inheritance in Man database).
Table 1.
Са2+ channels and associated channelopathies. (Based on OMIM, Online Mendelian Inheritance in Man database).
| Са2+ channel | Gene | Channelopathy, syndromes | OMIM |
|---|---|---|---|
| Cav | |||
| Cav1.1 | CACNA1S | Hypokalemic Periodic Paralysis Type 1 Normokalemic Periodic Paralysis Malignant Hypothermia Susceptibility 5 |
170400 170600 601887 |
| Cav1.2 | CACNA1C | Timothy Syndrome Long QT Syndrome 8 (LQT8) Brugada Syndrome 3 |
601005 618447 611875 |
| Cav1.3 | CACNA1D | Sinoatrial Node Dysfunction and Deafness Syndrome Primary aldosteronism, seizures, and neurologic abnormalities Autism spectrum disorder (with or without more severe manifestations including intellectual disability, neurological abnormalities, primary aldosteronism and/or congenital hyperinsulinism |
614896 615474 Not listed in OMIM |
| Cav1.4 | CACNA1F | Aldosterone producing adenomas Congenital Stationary Night Blindness Type 2 X-linked Cone-Rod Dystrophy 3 Aland Island Eye Disease |
Not listed in OMIM 300071 300476 300600 |
| Cav2.1 | CACNA1A | Familial and Sporadic Hemiplegic Migraine Type 1 with or without progressive cerebellar ataxia Episodic Ataxia Type 2 Spinocerebellar Ataxia Type 6 Early Infantile Epileptic Encephalopathy 42 Congenital Ataxia |
141500 108500 183086 617106 Not listed in OMIM |
| CACNA1B | Neurodevelopmental disorder with seizures and non-epileptic hyperkinetic movements | 618497 | |
| Cav2.3 | CACNA1E | Early Infantile Epileptic Encephalopathy 69 | 618285 |
| Cav3.1 | CACNA1G | Spinocerebellar Ataxia Type 42 Spinocerebellar Ataxia Type 42 early-onset, with neurodevelopmental deficits (Childhood-Onset Cerebellar Atrophy) |
616795 618087 |
| Cav3.2 | CACNA1H | Familial Hyperaldosteronism type IV Aldosterone producing adenomas |
617027 Not listed in OMIM |
| Cav3.3 | CACNA1I | Neurodevelopmental disorder with epilepsy and intellectual disability | Not listed in OMIM |
| RyR | |||
| RyR2 | RYR2 | Arrhythmogenic right ventricular dysplasia/cardiomyopathy type 2 Stress-induced polymorphic ventricular tachycardia (Catecholaminergic polymorphic ventricular tachycardia 1) |
600996 604772 |
| TRP | |||
| TRPC3 | TRPC3 | Spinocerebellar ataxia | 602345 |
| TRPC6 | TRPC6 | Glomerulosclerosis, focal segmental, 2 | 603965 |
| TRPV3 | TRPV3 | Olmsted Syndrome | 614594 |
| TRPV4 | TRPV4 | Brachyolmia type 3 | 113500 |
| Digital arthropathy-brachydactyly, familial | 606835 | ||
| Hereditary motor and sensory neuropathy, type IIc | 606071 | ||
| Metatropic dysplasia | 156530 | ||
| Parastremmatic dwarfism | 168400 | ||
| Scapuloperoneal spinal muscular atrophy | 181405 | ||
| SED, Maroteaux type | 184095 | ||
| Spinal muscular atrophy, distal, congenital nonprogressive | 600175 | ||
| Spondylometaphyseal dysplasia, Kozlowski type | 184252 | ||
| TRPM1 | TRPM1 | Night blindness, congenital stationary (complete), 1C, autosomal recessive | 613216 |
| TRPM4 | TRPM4 | Progressive familial heart block, type IB | 604559 |
| TRPM6 | TRPM6 | Hypomagnesemia 1, intestinal | 602014 |
| TRPA1 | TRPA1 | Episodic pain syndrome, familial | 615040 |
| TRPML1 | TRPML1 | Mucolipidosis IV | 252650 |
| PKD2 (TRPP1) | PKD2 | Autosomal dominant polycystic kidney disease | 613095 |
| HCN | |||
| HCN1 | HCN1 | Dravet syndrome | Not listed in OMIM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



