
Submitted:
26 May 2023
Posted:
29 May 2023
You are already at the latest version
Abstract
Diabetic nephropathy (DN), one of the primary consequences of diabetes mellitus, affecting many people worldwide. Diabetes affects yearly 463 million adults globally between the ages of 20 and 79, and is the main cause of death under the age of 60. ROS production rises during hyperglycemia and is crucial to the development of diabetic complications. Advanced glycation end products (AGEs) are produced excessively in a diabetic state and accumulate in the kidney, where they change renal architecture and impair renal function. Another important targeted pathway for the formation of DN includes NF-B, Nrf2, NLRP3, Akt/mTOR, and autophagy. About 40% of individuals with diabetes eventually acquire diabetic kidney disease and end stage renal disease that needs hemodialysis, peritoneal dialysis, or kidney transplantation, to survive. The current state of acceptable therapy for this kidney ailment is limited. The studies revealed that some naturally occurring bioactive substances might shield the kidney by controlling oxidative stress, renal fibrosis, inflammation, and autophagy. In order to provide new potential therapeutic lead bioactive compounds for contemporary drug discovery and clinical management of DN, this review was designed to examine the various mechanistic pathways by which current conventional plants derive phytocompounds that are effective for the control and treatment of DN.
Keywords:
Diabetic nephropathy
; Hyperglycemia
; Phytocompounds
; End stage renal disease
; Oxidative stress
; Inflammation
1. Introduction
A disorder with catastrophic repercussions known as diabetes mellitus (DM) and hyperglycemia, oxidative stress, inflammation, the creation of advanced glycation end products, and cytokine overexpression are merely some of the symptoms of this high-impact disease. The most frequent microvascular consequence of diabetes and the main cause of chronic kidney disease worldwide is Diabetic Nephropathy (DN). Uncontrolled DM in patients can lead to protracted hyperglycemia and the emergence of chronic consequences that fall under the macrovascular (peripheral, coronary artery and cerebral vascular disease) and microvascular (retinopathy, nephropathy, and neuropathy) categories [1]. The progression to chronic kidney disease and end stage renal disease (ESRD) is frequently accompanied by the development of macro albuminuria [2]. Glomerular enlargement, glomerular excessive filtration, raised urinary albumin release, thickness of basement membrane, expandsion of mesangial matrix and nodule development, tubulointerstitial inflammation, glomerulosclerosis, & interstitial fibrosis are all signs of a pathological condition in the kidneys.
By releasing vasoactive mediators like prostaglandin, insulin-like growth factor 1 (IGF-1), vascular endothelial growth factor (VEGF) and prostaglandin, as well as by upregulating sodium-glucose co-transporter 2 (SGLT2) in the proximal tubules, high blood glucose levels increase afferent arteriolar enhancement. As a result, the transport of NaCl to the macula densa of distal tubules is reduced. As an outcome, tubuloglomerular feedback leads the afferent and efferent arterioles to dilate and constrict, respectively [3,4]. High glucose levels directly caused the kidney to release renin through a paracrine signalling mechanism. As seen in the kidney sections of rat, mouse, and rabbit, the signalling cascade involves the local buildup of succinate and activating kidney-specific G protein-coupled metabolic receptor (GPR91) within glomerular endothelium. Endothelial Ca2+, prostaglandin and NO synthesis, and their paracrine effects on nearby cells producing renin are components of signal transduction. Through renal hyperfiltration, this GPR91 transduction cascade may affect kidney function and aid in the removal of metabolic waste products. According to [5] long-term hyperfiltration causes renal failure and it has been linked to metabolic illnesses like diabetes and metabolic syndrome, overactivation of RAS, systemic hypertension, and destruction of organ. Angiotensin II’s (Ang II) primary vasoconstrictor peptide is produced in greater quantities when the RAAS is activated. Through the suppression of insulin signal transduction, a decline in glucose uptake, resistance to insulin, & destruction of the beta cells of the pancreas by producing oxidative stress, Ang II impacts glucose homeostasis, which is involved in the development of DM. Activation of RAAS in the renal cells that help to stimulate aldosterone secretion and retention of sodium and water which lead to development of systematic hypertension, proteinuria, glomerular sclerosis [6]. DM conditions trigger mechanistic target of rapamycin (mTOR) and release ERK/beta catenin, TGFβ1/Smad which involved develop extracellular matrix deposition by epithelial-mesenchymal transition due to the adenosine monophosphate-activated protein kinase (AMPK) activity inhibition in renal tubular cells, thereby increasing matrix protein synthesis and tubular hypertrophy [7]. The mTORC1 hyper activated mTORC damaged podocytes cell which involved acute & chronic renal failure [8]. The creation of novel, improved therapeutic approaches is currently essential for the management and prevention of DN-related issues (Figure 1) [9]. The best source of remedies or traditional medicines has always been plant sources. Numerous plant compounds, such as terpenoids, alkaloids, flavonoids, poly-phenols, quinones, saponins etc have been thoroughly studied for their many pharmacological applications, including antidiabetic and nephroprotective properties [10]. This focus has grown as more extensive research on alternative medicine’s relationship to modern medicine has been conducted. The best source of herbal remedies or traditional medicines has always been plants. Numerous plant chemicals, such as terpenoids, flavonoids, alkaloids, poly-phenols, quinones, currently, plant-derived chemicals or their derivatives are utilised as the first-line oral therapy for treating kidney-related problems, with about 50% of pharmaceuticals that have received approval from the Food and Drug Administration (FDA) falling into this category. Natural plant-derived medicines have fewer adverse effects and are more inexpensive and available than conventional treatments. Numerous physiological characteristics, including anti- carcinogenic, anti- allergenic, anti- microbial, anti-inflammatory, antioxidant, anti-renal, anti-diabetic, and cardio protective, can be found in them [11]. Recent research has indicated that certain natural substances can effectively treat DN by reducing blood sugar levels, blood lipid levels, and oxidative stress. This review’s objective is to look at the numerous mechanistic pathways by which current conventional plants create the phytocompounds used to treat DN.
2. Epidemiological Scenario in Diabetic Nephropathy
Diabetes now affects 463 million adults globally between the ages of 20 and 79, and under the age of 60, it is the main cause of death [12]. About 40% of people with diabetes develop diabetic kidney disease (DKD), which is a frequent and significant consequence of the condition [13]. The prevalence of diabetes among adults in their middle adult years is predicted to be 79.4% in middle-income nations as a result of globalisation and epidemiological change. The most severe effect is ESRD, which necessitates renal replacement treatment (RRT) such hemodialysis, peritoneal dialysis, or kidney transplantation for affected people to survive [14]. About 20%-40% of patients with diabetes are developed DKD, which is the primary contributor to chronic renal disease and ESRD. It is significant to remember that DKD advances even when risk variables such blood sugar, blood pressure, and body weight are strictly controlled [15]. The International Diabetes Federation estimates that as of 2022, 536 million adults (20-79 years) in India had diabetes, and that figure is expected to increase in 784 millions by 2045 [16]. A clinical survey in India to found 34.4% prevalence of DKD [17]. T2D patients in India have been found to have a 2% prevalence of overt nephropathy, a 27% prevalence of microalbuminuria, and a 58.75% patient awareness of DN [18,19].
3. Role of phytocompounds in diabetes nephropathy
Plants contain a variety of biologically active chemical molecules called phytocompounds. These naturally occurring bioactive substances, which include xanthophylls, alkaloids, phenols, flavonoids, phenylpropanoids, terpenoids, and sulfur-containing compounds like allyl isothiocyanates, are derived from primary metabolism and primarily serve ecological functions like defence, adaptation, and chemo-attraction. Plant-based foods have historically been linked to preventing numerous ailments in humans [20].
3.1. Berberine
In pharmacology and medical chemistry, berberine, an alkaloid, is an important compound. Long used as an oriental medicine to treat gastroenteritis and secretory diarrhoea, berberine is an isolated compound from the roots plants Coptidis, Cortex phellodendri, and Berberis vulgaris. A growing body of research has shown that berberine has a variety of pharmacological actions, including effects against oxidative stress, inflammation, tumours, microbes, and fibrosis. Furthermore, it has been widely shown that berberine has renoprotective effects on the development of DN [21,22]. By primarily restricting the enzyme activity of dipeptidyl peptidase-4 and protein tyrosine phosphatase-1B (PTP-1B), treatment with berberine significantly lower levels of inflammatory markers, C reactive protein, free fatty acids, and triacylglycerols in bloodstreams of streptozotocin (STZ) induced animal model of diabetes. According to [23] berberine improved insulin sensitivity and reduced high blood glucose levels. Liver inflammation may result from abnormally raised level of blood sugar. Reactive oxygen species (ROS), Tumor necrosis factor (TNF-α), and other pro-inflammatory mediators are produced by the Kupffer cells, that are found in the hepatic sinusoids of the liver. Because they can cause a range of cellular responses, including proliferation, survival, and death, TNF- α and Interleukin-6 (IL-6) are significant mediators of liver-specific intracellular damage. In comparison to patients with diabetes who do not have overt nephropathy, patients with DN have higher levels of pro-inflammatory cytokines, such as Th1 cytokines and chemokines, in their plasma and urine. This finding suggests that pro-inflammatory cytokines are involved in the inflammation of the kidneys in diabetics. In the diabetic group, Interleukin-10 (IL-10)/TNF-α levels fell, although relative mRNA expression levels for TNF-α, IL-6, and IL-10 were elevated in the kidney. In comparison to the control group, IL-6/IL-10 (pro-/anti-inflammatory cytokines) mRNA expression levels were considerably lower after 14 weeks of berberine therapy. Evidently, non-obese diabetic mice’s spontaneous renal inflammation was reduced after 14 weeks of berberine therapy. By controlling the expression of pro- or anti-inflammatory (TNF-α, IL-1b, and IL-6/IL-10) or Th1/Th2 cytokines in non-obese mice with diabetes, berberine provided protection against uncontrolled persistent inflammation in liver, kidneys and spleen [24]. The first and most significant inflammatory cytokine released by the body after exposure to pathogenic stimuli, TNF-α takes role in localised inflammation and endothelial cells activation. Both high and low doses of berberine drastically decreased renal inflammatory damage and the production of IL-1, IL6, IL-18, and TNF-α in DN kidney tissues (Figure 2) [25].
The nuclear translocation of nuclear factor kappa B (NF-kB) p65 as well as elevated glucose-induced c-jun phosphorylation can both be greatly reduced by berberine. Additionally, berberine has the ability to inhibit the transcriptional and DNA-binding functions of activator protein-1 (AP-1) as well as the increased glucose-induced tissue growth factor-1 (TGF-1) gene expression. The mRNA expression levels of intracellular adhesion molecule-1(ICAM-1), TGF-1, fibronectin, and downstream inflammatory mediators in the fibrotic responses in the diabetic kidney are decreased as a result of its ability to prevent these alterations in critical signalling pathway variables. Additionally, this decreases the production of extracellular matrix (ECM), inflammatory mediators, and other pro-fibrogenic components. As a result, less ECM is deposited and there are fewer inflammatory responses, which eventually lessens the severity of renal fibrosis and glomerulosclerosis [26].
Cellular redox is predominantly managed by nuclear transcription factor and nuclear factor E2-related factor-2 (Nrf2). The antioxidant response element and NQO1 transcription can cooperate to protect downstream cells by preventing oxidative stress-related cell damage. Studies show that Nrf2 regulates oxidative stress and that excessive glucose levels inhibit its expression. Studies was shown that berberine can upregulate the expression of Nrf2 in both high and low doses, indicating that Nrf2 activation may be necessary for berberine to reduce oxidative stress and regulate the pyroptosis of DN kidney cells [27].
Previous study has demonstrated that nucleotide binding domain, leucine rich containing family, pyrin domain containing-3 (NLRP3) inflammasome with a nucleotide binding oligomeric domain regulated renal inflammation, which contributed for the progression of DN. Targeting the NLRP3 may therefore be an effective and future DN treatment [28]. It was feasible to evaluate the effects of berberine on inflammasome expression in high glucose-induced HK-2 cells by evaluating levels of expression of NLRP3 inflammasome protein and mRNA using western blotting and RT-PCR. However, the dose-dependent effects of berberine treatment decreased the expression of Caspase-1, NLRP3 and IL-1b. These biomarkers had significantly higher protein and mRNA levels in the hyperglycemia-induced condition comparing to the glucose control group. The results of a cell experiment supported those obtained in the animal experiment, which showed that berberine might prevent the Epithelial-Mesenchymal Transition (EMT) brought on by the NLRP3 inflammasome [29].
3.2. Resveratrol
Resveratrol is a well-known polyphenol produced as a secondary metabolite by plants, has been examined in numerous animal models of human diseases, including diabetes and coronary heart disease. It can be found in nature in both trans- and cis-forms and is commonly found in grapes, mulberries, red wines, and peanut skins [30]. Resveratrol treatment (5 mg/(kg/d)) reduced renal impairment in a DM rat model as evidenced by a noticeably lower level of serum creatinine, urine protein, and urinary TGF-1 expression. Additionally, a subsequent mRNA study showed that the expressions of the proteins TGF-1, Nrf2, fibronectin, sirtuin 1 (SIRT1), NF-kB/p65, and forkhead box O (FOXO) 1 in the kidney had normalised (Hussein & Mahfouz, 2016). Mammalian sirtuins are NAD+-dependent enzymes and data indicate a direct connection between SIRT1 activity and metabolic disorders like diabetes. By direct binding or deacetylation, SIRT1 can control FOXO transcription. Mesangial cells in high-glucose cultures released more ROS, produced more mitochondrial superoxide, and had higher manganese superoxide dismutase (MnSOD) activity. Resveratrol pretreatment, however, attenuated these hyperglycemia-induced states by activating SIRT1 in the cells. The protective effect of resveratrol against oxidative damage under hyperglycemic circumstances was decreased by SIRT1 suppression using a small interfering RNA targeting EX-527, demonstrating the function of SIRT1 [31]. In diabetic conditions, FOXO1 activity was markedly reduced along with the expression of FOXO1-targeted genes, reduced superoxide dismutase (SOD) activity, downregulation of FOXO1 was linked to increased type IV collagen & fibronectin protein expression in the renal cortex. These findings indicate FOXO1’s involvement in the development of oxidative stress. This emphasises the importance of the antioxidative properties of resveratrol in delivering its renoprotection in DM also the role of the SIRT1/FOXO1 pathways in this effect [32]. Under various pathophysiological circumstances, previous research found a correlation between autophagy and insulin resistance. Research examined the relative expression of autophagy-related proteins (Beclin1, LC3 II/I), finding that resveratrol treatment results in higher levels of Beclin1 and LC3 II/I than in the group using DN models. Additionally, as compared to the DN model group, resveratrol therapy decreased pmTOR/mTOR and p-ULK1 S757/ULK1 rate while dramatically increasing p-AMPK/AMPK and p-ULK1 S777/ULK1 rate. According to recent studies, resveratrol activated the AMPK/mTOR pathway in DN rats to induce autophagy. These results imply that resveratrol may represent a possible therapeutic strategy for the management of DN and type 2 DN [33].
3.3. Ellagic acid
Ellagic acid, often referred to as trihydroxy acid, is a result of the hydrolysis of tannins and is present in significant amounts in a number of foods, such as nuts, tea, berries, oak wine, and other foods. On a range of ailments such ulcerative colitis, colon cancer, hepatopathy, diabetes, and Alzheimer’s disease, it has anti-inflammatory, anti-cancer, antioxidant, and anti-atheroclerotic actions [34,35].
The innate immune system’s main component is called the toll-like receptor (TLR), particularly TLR4, are crucial for controlling inflammatory reactions. Several inflammatory pathways are triggered by TLR4, which has been linked to progressive renal fibrosis in a number of well-established experiments. Important TLR transcription factors initiate the creation of ROS and proteins associated with inflammation during this process by activating downstream transcriptional regulators including NF-kB [36]. Results of the ellagic acid inhibitory effect on lipopolysaccharide (LPS)-induced TLR4 elevation showed that ellagic acid could decrease the elevated levels of LPS-induced TLR4 and restrict the expression of downstream proteins like IRAK1, P-IRAK1, and p65 proteins, suggesting that ellagic acid could reduce a variety of inflammation-related responses by inhibiting TLR4 and TLR4/NF-kB pathways [37].
Growth factor receptor and the G protein coupled receptor families activate both downstream and upstream signalling molecules, respectively. Numerous extracellular signals, including fibroblast growth factor, VEGF, and human growth factor, can activate phosphoinositide 3-kinase (PI3K). Phosphorylated Akt operates as the second messenger to mediate a variety of cell processes [38]. This is made possible by activated PI3K. Ellagic acid and high glucose increase PI3K/Akt signalling in mesangial cells in a similar manner, ellagic acid prevented PI3K and Akt from becoming phosphorylated. Mammalian nuclei contain FOXO3a, and phosphorylated Akt can cause it to move from the nucleus to the cytoplasm, inactivating it and increasing the expression of SOD2, which lowers ROS generation. Additionally, in DN, ellagic acid suppressed NF-kB and decreased renal tissue damage. It prevented the PI3K/Akt signalling pathway, which was activated by high glucose levels in mesangial cells, and then controlled the nuclear transcription activities of FOXO3 and NF-kB, which in turn prevented cell division, oxidative stress, the release of inflammatory factors, and the production of ECM. The current study offered an experimental theoretical foundation for the process by which ellagic acid lessened the harm that elevated glucose levels induced to mesangial cells [39].
3.4. Epigallocatechin gallate
A type of catechin known as epigallocatechin gallate, sometimes known as epigallocatechin-3-gallate, is the ester of epigallocatechin and gallic acid. Epigallocatechin-3-gallate, a kind of green tea extract, is the primary polyphenolic component of green tea. Its anti-inflammatory, hypoglycemic, and anti-oxidative qualities have all been suggested. Han et al. hypothesised that Nrf2, an effective regulator of oxidative stress & inflammation, was activated by high glucose stimulation [40,41]. Oxidative stress promotes constitutive and active Nrf2 molecule production. These molecules then flood into the cytoplasm by creating a Nrf2 pool & move towards nucleus. Despite oxidative stress, the reason why Nrf2 was unable to cross the nuclear membrane could be predicted. Alternatively, the cysteine residues in Nrf2 may have changed, preventing the protein via binding with the antioxidant response element (ARE) & causing it to be expelled into the cytoplasm instead, leading to accumulation and altered chemistry of the inducer-cysteine code that links Keap1 and Nrf2, which has not been studied. Both scenarios could have affected the nuclear acquire machinery that is responsible for nuclear import of Nrf2. The extent of Nrf2’s functioning in the nucleus was revealed by electrophoretic mobility shift assay (EMSA) investigations that revealed increased levels of the Nrf2/ARE complex in mice given epigallocatechin gallate. In addition to altering the stoichiometric relationship between Nrf2 & its negative regulators, epigallocatechin gallate administration improves the system of antioxidant defence in diabetic rats by keeping Nrf2 inside the nucleus by increasing its affinity to ARE. Epigallocatechin gallate enhances nuclear Nrf2 levels and stimulates the Nrf2/ARE signalling pathway, according to in vitro research employing NRK-52E cells. The analysis of the Nrf2 mRNA gene expression profiles in cells fed with high glucose (30 mM) media for different periods of time reveals that the Nrf2 mRNA levels increase gradually up to 24 hours, then again at 48 hours, but the amounts do not remain constant after 72 hours. Similar findings were found in kidney biopsy specimens of diabetes patients [42,43].
Renal fibrosis was caused by excessive Notch expression, suggesting Notch might be a target for anti-fibrotic treatment. Notch receptors are modular, single-pass transmembrane proteins that detect signals from transmembrane ligands on neighbouring cells. Epigallocatechin gallate treatment might reduce Notch1 activation and attenuate Notch1 expression in HEK293 cells after high-glucose stimulation boosted Notch expression. Notch bind to TGFβ has been considered an intermediary in renal fibrosis by activating its downstream Smad signalling pathway [44]. In accordance with multiple studies, the TGF/Smad3 signalling pathway may be crucial in the progression of renal fibrosis in diabetic rats. According to some studies, suppressing Notch expression can reduce kidney fibrosis by preventing the activation of TGF/Smad3 signalling pathway. It was revealed that Notch serves as a receptor for epigallocatechin gallate, and that treatment with the compound reduces NICD expression. A potential mechanism of epigallocatechin gallate for treating renal fibrosis brought on by high glucose concentrations is revealed by the possibility that it works by targeting Notch to suppress the TGF/Smad3 pathway (Figure 3) [45,46].
3.5. Ursolic acid
One of the most potent components of herbal compounds is ursolic acid, which is extensively dispersed throughout plants and naturally present in fruits like apples, cranberries, and blueberries as well as herbs like rosemary, plantain, and thyme. It has a number of therapeutically relevant pharmacological effects, including as antibacterial, anti-inflammatory, anti-tumor, and anti-hepatitis. It is the ideal drug to treat infectious hepatitis because of its low level of toxicity and minimal adverse effects. It has been shown that ursolic acid reduces oxidative stress and increases the expression of inflammation-related mediators in DN [47,48].
High blood sugar causes inflammation of the glomerular mesangial cells, which is essential for DN. TNF-α, IL-6, and IL-1 are just a few examples of the several cellular inflammatory factors that are produced when there is inflammation, which can also affect tissue homoeostasis. These cytokines play a part in regulating the immune system’s inflammatory response, and are a significant contributor to inflammation of the kidneys [49]. TNF-α is a cytokine that is generated by macrophages and monocytes and has negative effects on mesangial & epithelial cells. It can also increase macrophage activity. It has been demonstrated that IL-6 is connected to an abnormal rise in glomerular epithelial cells permeability, glomerular mesangial proliferation, and glomerular basement membrane thickness. It has been demonstrated that the autocrine growth factor IL-1 aids in the rapid growth of mesangial cells. The above-mentioned pro-inflammatory factors are activated and induced by the P38MAPK pathway, and inhibitors of this system have also been found to be beneficial in treating a variety of inflammatory illnesses. Ursolic acid decreased P38 mRNA as well as protein expression while inhibiting the increase of TNF-α, IL-6, and IL-1 expression. Ursolic acid can reduce kidney inflammation brought on by DN, which may also be connected to the P38MAPK signalling pathway’s suppression [50,51].
NF-kB play an important role in gene regulation during apoptosis and inflammation and a recent investigation discovered that it is directly linked to the origin and progression of DN [52]. NF-kB can be triggered by a variety of physiological and non-physiological stimuli. TLR4 is the most important receptor for NF-kB activation. Findings indicate that NF-kB can be triggered by various diabetes factors and it can cause it to start numerous DN-related genes from transcription. Moreover, research indicates that NF-kB activation may, through a downstream effect, increase the risk of renal interstitial fibrosis [53]. Ursolic acid suppresses the development of breast cancer cells through PI3K/AKT and NF-kB signalling pathways. Additionally, TLR4 suppression improved the anti-inflammatory effects of ursolic acid in rats with diabetes-induced nephropathy via the TLR4 pathway [54].
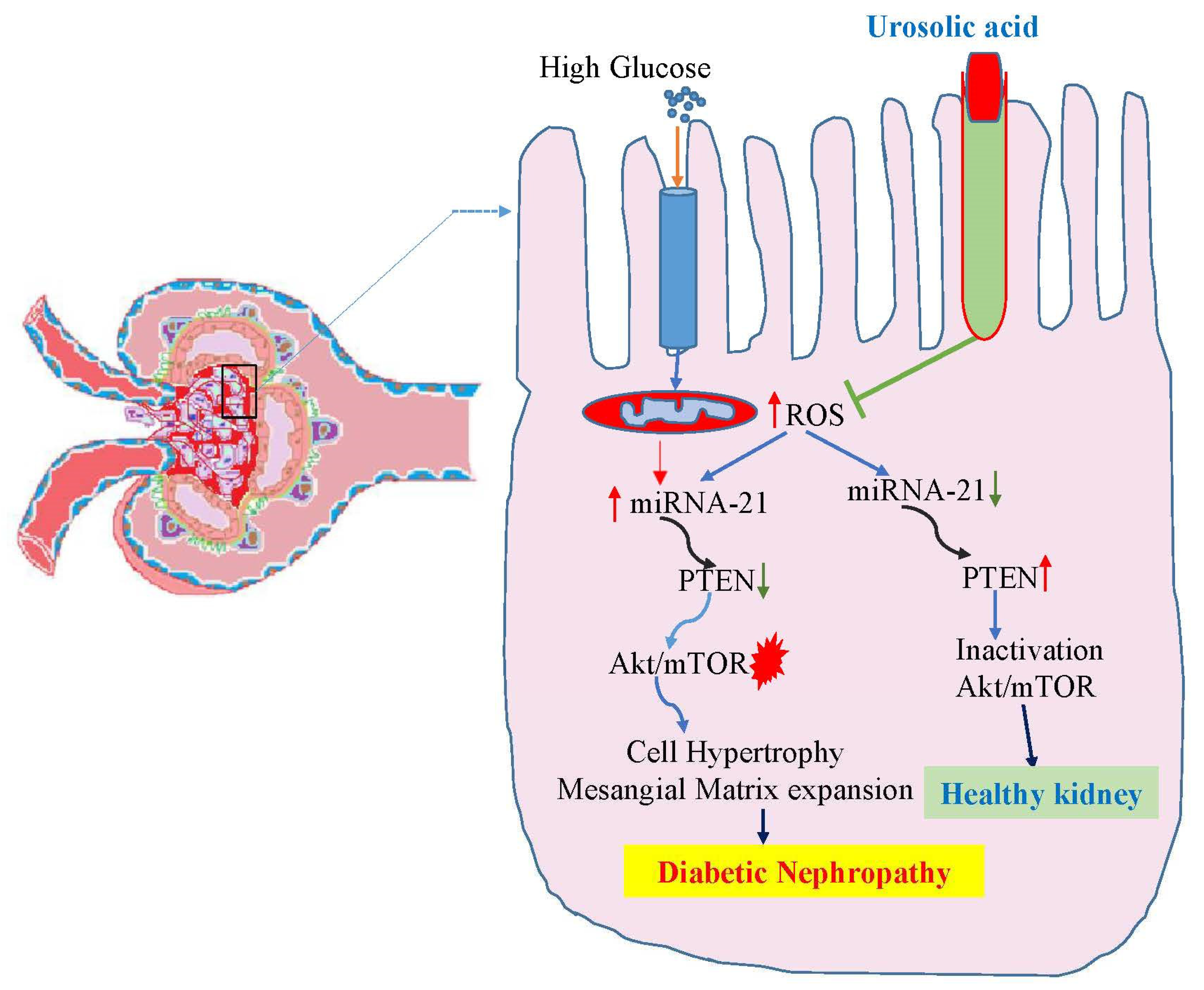
It was demonstrated that high glucose treatment and TGF boost the synthesis of microRNA (miRNA)-21, whereas miRNA-21 targets the 3′-UTR of Phosphatase and Tensin Homolog (PTEN) mRNA to decrease PTEN protein expression. Mesangial cell hypertrophy and the enlargement of the mesangial matrix are caused by overexpression of miRNA-21, which also suppresses PTEN expression while triggering the Akt/mTOR signalling pathway. On the other hand, Akt phosphorylation and PTEN down-regulation caused by excessive hyperglycemia are prevented by reducing endogenous miRNA-21 expression. By increasing the activity of the Akt/mTOR pathway and decreasing the amount of the target protein PTEN, miRNA-21 aids in the development of significant pathogenic defects in DN [55]. By regulating inappropriate activation of the Akt/mTOR pathways and reducing mesangial cell damage brought on by high glucose, ursolic acid boosted PTEN mRNA as well as protein expression [56]. Ursolic acid has the potential to be a promising treatment for DN because it reduces podocyte damage and restores improper autophagy through a miR-21 and PTEN-dependent mechanism (Figure 4).
3.6. Ferulic acid
Ferulic acid is an organic substance called hydroxycinnamic acid. The genus Ferula, which provides plants including Ferula asafoetida L., Anthemis nobilis L., and Equisetum hyemale L., offers a variety of pharmacological qualities and is less poisonous. It effectively reduces diabetes problems and their effects. Recent research has demonstrated that ferulic acid protects the kidneys of DN rats by minimuizing oxidative stress, inflammation & fibrosis [57].
A cellular process called autophagy rids the body of macromolecules and damaged organelles, which in turn makes it possible for cells to regenerate normally. Numerous disease-related pathogenic processes include autophagy. DN results in a dysregulated inflammatory response in the body, which aggravates kidney failure [58]. It has been proposed that autophagy, which may be related to its regulating influence on the NLRP3 inflammasome signalling pathway, can reduce excessive immune-inflammatory responses. According to recent research, there are two primary phases involved in the stimulation of the inflammasome signalling pathway. First, when cells are triggered by negative signals, TLRs become active and start the transcription and production of precursor proteins including pro-IL-1 and NLRP3 through the NF-kB pathway. Both the cytoplasm and the nucleus of the glomerular and renal tubular epithelial cells were the primary sites of NF-kB p65 expression, while the cytoplasmic renal tubular epithelial cells was the primary site for TNF-α expression. Both NF-kB p65 and TNF-α expressions were raised in STZ-induced diabetic kidney disease group of rats, but both upregulated expressions could be downregulated by ferulic acid treatments. During the evolution of DN, ferulic acid has a renoprotective effect, and its potential mechanism may be connected to anti-inflammation, anti-fibrosis, and a reduction in podocyte damage. Following this, the NLRP3 inflammasome is assembled, and activated caspase-1 processes and modifies downstream inflammatory components to prepare them for mature secretion [59]. In DN mice generated by a high-fat diet mixed with STZ, which involves the occurrence of fibrosis and kidney inflammation, NLRP3 and IL-1 levels were drastically elevated. By preventing the activation of the NLRP3 inflammasome, DN mice’s renal fibrosis and inflammation can be reduced. Ma et al. found that ferulic acid therapy greatly reduced a rise in NLRP3 and IL-1 expression of mice. By reducing the expression of the proteins NLRP3 and IL-1, ferulic acid may reduce the renal inflammation-related process in mice with diabetes and protect the kidneys [29,60]. Another study found that oral administration of ferulic acid for 8 weeks at a dose of 50 mg/kg significantly reduced renal cell inflammation, apoptosis, and impaired autophagy in diabetic rats by modifying advanced glycation end products (AGEs), MAPKs protein 38 (P38), c-Jun N-terminal kinase (JNK), NF-kB, and extracellular signal-regulated kinase 1/2 (Erk1/2) signalling pathways [61].
3.7. Quercetin
One of the six categories of the flavonoid chemicals, known as “bioflavonoids,” contains quercetin, the primary polyphenolic flavonoid found in a variety of plants, including lovage, berries, cilantro,capers, dill, and apples. Quercetin exhibits a number of pharmacological effects, including lowering the risk of cardiovascular and kidney disorders, anti-tumor activity, anti-oxidation, anti-inflammatory properties. The ability of quercetin to limit cell proliferation has been demonstrated in a number of recent studies, but the majority of these investigations involved tumours. According to studies, quercetin can prevent liver tumours by regulating the cell cycle to decrease cell growth and promote apoptosis [62]. EMT is a physiological phenomenon linked to tissue remodelling, wound healing, and embryogenesis. EMT, however, has a role in the pathophysiology of many illnesses. Tubular epithelial cells in DN undergo a trans differentiation process that causes them to evolve into myofibroblasts, which are the main extracellular matrix producers in cells of renal kissues and leads to the onset of renal fibrosis. One of the most crucial aspects of renal fibrosis is the thickening of the tubular basement membrane. According to Lu et al., high glucose treatment promoted deposition of glycogen & laminin expression across tubular basement membrane in NRK-52E & HK-2 cells. The development of renal fibrosis caused by diabetes was delayed by quercetin treatment because it considerably decreased the amount of collagen that built up in the glomerular and kidney interstitial areas in addition to the thicknesses of the tubular basement membrane. Quercetin is a potent chemical to stop and treat these processes, and diabetes is one of the main causes that contributes to decline in kidney function & chronic renal fibrosis. It is believed that quercetin enhances kidney function and reduces renal fibrosis in diabetic rats by suppressing EMT of renal tubular epithelial cells due to its protective impact on EMT in tubular cells [63]. The maturation of IL-1β & IL-18 depends on the activation of caspase-1, which is regulated by the multiprotein complex NLRP3 inflammasome. Recent studies have linked kidney illness to the NLRP3 inflammasome-caspase-1-IL-1β/IL-18 axis. In rats with DN, STZ caused aberrant renal expression of genes and proteins associated to urate transport and lipid metabolism, resulting in hyperuricemia and dyslipidaemia. Additionally, STZ-treated rats showed renal NLRP3 inflammasome activation, which led to a rise in IL-1b, IL-18 and a worsening of kidney damage. There is some evidence that connects renal inflammasome activation of NLRP3 and a disturbance of lipid metabolism to the occurrence of STZ-induced renal toxicity and hyperuricemia in rats. Quercetin’s anti-hyperuricemic and anti-dyslipidemic properties may be employed to treat the hypernephrotoxicity that STZ-induced diabetic rats experience [64,65].
Cholesterol generation and absorption are important processes which is required for cell maintenance since cholesterol is a crucial lipid that controls raft formation, membrane fluidity, and the synthesis of steroid and bile acids. 3-hydroxy-3-methyl-glutaryl-coenzyme the low-density lipoprotein receptor (LDLr), a mediator of cholesterol uptake, & hydroxymethylglutaryl-coenzyme a reductase inhibitor (HMGCR), a crucial enzyme for cholesterol production, are two important proteins that are mostly regulated by SREBP-2. Two additional proteins, SREBP-2 and SREBP SCAP, strictly control the negative feedback system that mediates the upward or downward regulation of HMGCR and LDLr when cells lack or have too much cholesterol compared to what is required for their physiological requirements, which is crucial for maintaining a balance of cholesterol at the level of both the cell and the system. The buildup of cholesterol in the kidneys of diabetic rats has also been linked to elevated levels of LDLr-mediated absorption of cholesterol and HMGCR-mediated cholesterol production. Along with quercetin’s antioxidant properties, it has been proposed that reducing HMGCA may help mitigate the negative effects of LDL-C and VLDL-C [66]. After receiving quercetin medication for 10 weeks, db/db mice’s levels of cholesterol, serum triglycerides, & LDL-C significantly decreased as compared to diabetic controls, which coincided with a decrease in renal HMGCR expression. According to clinical research, statins (HMGCA reductase inhibitors) protect against both non-diabetic and diabetic kidney damage by inhibiting cholesterol biosynthesis to lower cholesterol synthesis [67].
3.8. Baicalin
One of the main bioactive flavonoids known as baicalin, which is found in many medicinal hrbs, that shown to have a number of pharmacological advantages, including anti-diabetic, anti-inflammatory, antioxidant, & anti-cancer effects. Baicalin has been shown in studies to protect against DN by preventing increasing renal fibrosis, & the underlying mechanisms were linked to the suppression of NF-kB signalling. In the context of the antioxidant defence system, Nrf2 is crucial. Activated Nrf2 moves into the nucleus in response to oxidative damage, which causes the production of genes that are directed by antioxidant response elements, like heme oxygenase-1. In DN mice, there was a clear inhibition of both the levels of the antioxidant enzymes (HO-1, NQO-1) and the activation of Nrf2 signalling. Baicalin activates the Nrf2-mediated antioxidant system to reduce oxidative stress in DN [68,69].
MicroRNAs (miRNAs) are a class of short (21 nucleotides or less) non-coding RNAs that have the ability to control post-transcriptional levels of gene expression. Furthermore, it has been discovered that accumulating miRNAs have an important role in the onset and development of kidney disorders such as DN and renal fibrosis. In the renal tissues of STZ-induced DN mice along with high glucose-induced HK-2 cells, baicalin increases the expression of miR-124 [70]. Overexpression of the miR-124 gene improved mouse survival rates, reduced the expression of the pro-inflammatory cytokines TNF-, IL-1, and IL-6, and reduced the severity of acute renal damage [71]. Without changing the amount of total NF-kB, baicalin significantly reduced the nuclear translocation of NF-kB in reaction to 1 hour of hyperglycemia as well as hyperglycemia with AGE and TNF-α. Baicalin reduced the amount of JAK2 and STAT3 phosphorylation in HK-2 cells that had been treated to high glucose. By reducing oxidative stress and inflammation-induced inhibition of NF-kB phosphorylations & JAK2 phosphorylation, baicalin protects against renal fibrosis. As a result, NF-kB and STAT3 activation was seen in human renal proximal tubular cells [72].
4. Conclusion
Persistent hyperalbuminuria, an incomplete reduction in renal function, and glomerular disease are the hallmarks of the syndrome referred to as DN. In the therapy of DN, numerous natural plant compounds have been employed extensively and exhibit good pharmacological effect. Bioactive phytocompounds, which are found naturally in many plants and fruits which have been shown to offer a variety of health benefits in the modern period. Present studies focous on the anti-oxidative and anti-inflammatory actions of bioactive phytocompounds, which are correlated with apoptosis, glomerular protection, and kidney fibrosis, are particularly important for DN therapy. Additionally, the protective effects of bioactive phytocompounds against DN point to the potential for treating DN, and because there aren’t any relevant clinical trials, more investigation is necessary in this area.
Author Contributions
Conceptualization, supervision, validation, formal analysis, funding acquisition, writing—review and editing, S.R; formal analysis, methodology, investigation, resources, writing—original draft preparation, visualization, methodology, investigation, project administration, P.M. and S.J. All authors have read and agreed to the published version of the manuscript.
Funding
This review work do not received any external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors grateful to Dr. Pradip Ghosh, Director, Midnapore City College for essential support, a well-organized work environment and laboratory facilities for conducting related research work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lee, W. J.; Sobrin, L.; Lee, M. J.; Kang, M. H.; Seong, M.; Cho, H. The relationship between diabetic retinopathy and diabetic nephropathy in a population-based study in Korea (KNHANES V-2, 3). Invest. Ophthalmol. Vis. Sci. 2014, 55, 6547–6553. [Google Scholar] [CrossRef] [PubMed]
- de Boer, I. H.; Rue, T. C.; Hall, Y. N.; Heagerty, P. J.; Weiss, N. S.; Himmelfarb, J. (2011). Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA. 2011, 305, 2532–2539. [Google Scholar] [CrossRef] [PubMed]
- Cianciolo, G.; De Pascalis, A.; Gasperoni, L.; Tondolo, F.; Zappulo, F.; Capelli, I.; Cappuccilli, M.; La Manna, G. The Off-Target Effects, Electrolyte and Mineral Disorders of SGLT2i. Molecules. 2020, 25, 2757. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, K. R. Back to the future: glomerular hyperfiltration and the diabetic kidney. Diabetes. 2017, 66, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Toma, I.; Kang, J. J.; Sipos, A.; Vargas, S.; Bansal, E.; Hanner, F.; Meer, E.; Peti-Peterdi, J. Succinate receptor GPR91 provides a direct link between high glucose levels and renin release in murine and rabbit kidney. J. Clin. Invest. 2008, 118, 2526–2534. [Google Scholar] [CrossRef]
- Rahimi, Z.; Moradi, M.; Nasri, H. A systematic review of the role of renin angiotensin aldosterone system genes in diabetes mellitus, diabetic retinopathy and diabetic neuropathy. J. Res. Med. Sci. 2014, 19, 1090. [Google Scholar]
- Sun, H. J.; Wu, Z. Y.; Cao, L.; Zhu, M. Y.; Liu, T. T.; Guo, L.; Lin, Y.; Nie, X. W.; Bian, J. S. Hydrogen Sulfide: Recent Progression and Perspectives for the Treatment of Diabetic Nephropathy. Molecules. 2019, 24, 2857. [Google Scholar] [CrossRef]
- Yasuda-Yamahara, M.; Kume, S.; Maegawa, H. Roles of mTOR in diabetic kidney disease. Antioxidants (Basel). 2021, 10, 321. [Google Scholar] [CrossRef]
- Parveen, A.; Jin, M.; Kim, S. Y. Bioactive phytochemicals that regulate the cellular processes involved in diabetic nephropathy. Phytomedicine. 2018, 39, 146–159. [Google Scholar] [CrossRef]
- Bacanli, M.; Dilsiz, S. A.; Başaran, N.; Başaran, A. A. Effects of phytochemicals against diabetes. Adv. Food Nutr. Res. 2019, 89, 209–238. [Google Scholar]
- Shahidi, F.; Yeo, J. Bioactivities of phenolics by focusing on suppression of chronic diseases: A review. Int. J. Mol. Sci. 2018, 19, 1573. [Google Scholar] [CrossRef]
- Zuckerman Levin, N.; Cohen, M.; Phillip, M.; Tenenbaum, A.; Koren, I.; Tenenbaum-Rakover, Y.; Admoni, O.; Hershkovitz, E.; Haim, A.; Mazor Aronovitch, K.; Zangen, D., Strich, D.; Brener, A.; Yeshayahu, Y.; Schon, Y.; Rachmiel, M.; Ben-Ari, T.; Levy-Khademi, F.; Tibi, R.; Weiss, R.; Shehadeh, N. Youth-onset type 2 diabetes in Israel: A national cohort. Pediatr. Diabetes. 2022, 23, 649–659.
- de Boer, I. H.; Rue, T. C.; Cleary, P. A.; Lachin, J. M.; Molitch, M. E.; Steffes, M. W.; Sun, W.; Zinman, B.; Brunzell, J. D.; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study Research Group, White, N. H.; Danis, R. P.; Davis, M. D.; Hainsworth, D.; Hubbard, L. D.; Nathan, D. M. Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Arch. Intern. Med. 2011, 171, 412–420.
- Webster, A. C.; Nagler, E. V.; Morton, R. L.; Masson, P. Chronic kidney disease. Lancet. 2017, 389, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Kocak, M. Z.; Aktas, G.; Duman, T. T.; Atak, B. M.; Savli, H. Is Uric Acid elevation a random finding or a causative agent of diabetic nephropathy? Rev. Assoc. Med. Bras. 2019, 65, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Sethuram, L.; John, T.; Mukherjee, A.; Natarajan, C. A review on contemporary nanomaterial-based therapeutics for the treatment of diabetic foot ulcers (DFUs) with special reference to the Indian scenario. Nanoscale Adv. 2022, 4, 2367–2398. [Google Scholar] [CrossRef]
- Hussain, S.; Habib, A.; Najmi, A. K. Limited knowledge of chronic kidney disease among type 2 diabetes mellitus patients in India. Int. J. Environ. Res. Public Health. 2019, 16, 1443. [Google Scholar] [CrossRef]
- Unnikrishnan, R.; Rema, M.; Pradeepa, R.; Deepa, M.; Shanthirani, C. S.; Deepa, R.; Mohan, V. Prevalence and risk factors of diabetic nephropathy in an urban South Indian population: the Chennai Urban Rural Epidemiology Study (CURES 45). Diabetes Care. 2007, 30, 2019–2024. [Google Scholar] [CrossRef]
- Bansal, C.; Kaushik, R.; Kaushik, R. M. Awareness of diabetic nephropathy in patients with type 2 diabetes mellitus: the Indian scenario. J. of Nephro. 2018, 7, 90–97. [Google Scholar] [CrossRef]
- Khan, A.; Siddiqui, S.; Husain, S. A.; Mazurek, S.; Iqbal, M. A. Phytocompounds targeting metabolic reprogramming in cancer: an assessment of role, mechanisms, pathways, and therapeutic relevance. J Agric Food Chem. 2021, 69, 6897–6928. [Google Scholar] [CrossRef]
- Zhu, L.; Han, J.; Yuan, R.; Xue, L.; Pang, W. Berberine ameliorates diabetic nephropathy by inhibiting TLR4/NF-κB pathway. Biol. Res. 2018, 51, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Neag, M. A.; Mocan, A.; Echeverría, J.; Pop, R. M.; Bocsan, C. I.; Crişan, G.; Buzoianu, A. D. Berberine: Botanical occurrence, traditional uses, extraction methods, and relevance in cardiovascular, metabolic, hepatic, and renal disorders. Front. Pharmacol. 2018, 9, 557. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Y.; Zhang, J.; Sun, C.; Lopez, A. Berberine improves glucose homeostasis in streptozotocin-induced diabetic rats in association with multiple factors of insulin resistance. ISRN Endocrinol. 2011, 2011, 519371. [Google Scholar] [CrossRef] [PubMed]
- Chueh, W. H.; Lin, J. Y. Protective effect of isoquinoline alkaloid berberine on spontaneous inflammation in the spleen, liver and kidney of non-obese diabetic mice through downregulating gene expression ratios of pro-/anti-inflammatory and Th1/Th2 cytokines. Food Chemistry. 2012, 131, 1263–1271. [Google Scholar] [CrossRef]
- Sun, J.; Chen, X.; Liu, T.; Jiang, X.; Wu, Y.; Yang, S.; Hua, W.; Li, Z.; Huang, H.; Ruan, X.; Du, X. Berberine Protects Against Palmitate-Induced Apoptosis in Tubular Epithelial Cells by Promoting Fatty Acid Oxidation. Med. Sci. Monit. 2018, 24, 1484–1492. [Google Scholar] [CrossRef]
- Ni, W. J.; Ding, H. H.; Tang, L. Q. Berberine as a promising anti-diabetic nephropathy drug: An analysis of its effects and mechanisms. Eur. J. Pharmacol. 2015, 760, 103–112. [Google Scholar] [CrossRef]
- Ding, B.; Geng, S.; Hou, X.; Ma, X.; Xu, H.; Yang, F.; Liu, K.; Liang, W.; Ma, G. Berberine Reduces Renal Cell Pyroptosis in Golden Hamsters with Diabetic Nephropathy through the Nrf2-NLRP3-Caspase-1-GSDMD Pathway. Evid Based Complement Alternat Med. 2021, 2021, 5545193. [Google Scholar] [CrossRef]
- Wen, L.; Yang, H.; Ma, L.; Fu, P. The roles of NLRP3 inflammasome-mediated signaling pathways in hyperuricemic nephropathy. Mol. Cell Biochem. 2021, 476, 1377–1386. [Google Scholar] [CrossRef]
- Ma, Z.; Zhu, L.; Wang, S.; Guo, X.; Sun, B.; Wang, Q.; Chen, L. Berberine protects diabetic nephropathy by suppressing epithelial-to-mesenchymal transition involving the inactivation of the NLRP3 inflammasome. Ren. Fail. 2022, 44, 923–932. [Google Scholar] [CrossRef]
- Thapa, S. B.; Pandey, R. P.; Park, Y. I.; Sohng, J. K. Biotechnological advances in resveratrol production and its chemical diversity. Molecules. 2019, 24, 2571. [Google Scholar] [CrossRef]
- Wang, X.; Meng, L.; Zhao, L.; Wang, Z.; Liu, H.; Liu, G.; Guan, G. Resveratrol ameliorates hyperglycemia-induced renal tubular oxidative stress damage via modulating the SIRT1/FOXO3a pathway. Diabetes Res Clin Pract. 2017, 126, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Gowd, V.; Kang, Q.; Wang, Q.; Wang, Q.; Chen, F.; Cheng, K. W. Resveratrol: evidence for its nephroprotective effect in diabetic nephropathy. Adv. Nutr. 2020, 11, 1555–1568. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y. H.; Fan, Y. J. Resveratrol improves lipid metabolism in diabetic nephropathy rats. Front Biosci (Landmark Ed). 2020, 25, 1913–1924. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, O. D.; Kulkarni, Y. A. Mini-review of analytical methods used in quantification of ellagic acid. Rev. Ana. Chem. 2020, 39, 31–44. [Google Scholar] [CrossRef]
- Zhou, B. H.; Qiu, Z. P.; Yi, H. L.; Zhou, D. S.; Wang, J.; Wu, Y. [Research progress of ellagitannin intestinal metabolite urolithins]. Zhongguo. Zhong. Yao. Za. Zhi. 2016, 41, 2968–2974. [Google Scholar]
- Liu, Y.; Yin, H.; Zhao, M.; Lu, Q. TLR2 and TLR4 in autoimmune diseases: a comprehensive review. Clin. Rev. Allergy. Immunol. 2014, 47, 136–47. [Google Scholar] [CrossRef]
- Zhou, B.; Li, Q.; Wang, J.; Chen, P.; Jiang, S. Ellagic acid attenuates streptozocin induced diabetic nephropathy via the regulation of oxidative stress and inflammatory signaling. Food. Chem. Toxicol. 2019, 123, 16–27. [Google Scholar] [CrossRef]
- Zhang, M.; Zhang, X. The role of PI3K/AKT/FOXO signaling in psoriasis. Arch. Dermatol. Res. 2019, 311, 83–91. [Google Scholar] [CrossRef]
- Lin, W.; Liu, G.; Kang, X.; Guo, P.; Shang, Y.; Du, R.; Wang, X.; Chen, L.; Yue, R.; Kong, F.; Zhu, Q. Ellagic acid inhibits high glucose-induced injury in rat mesangial cells via the PI3K/Akt/FOXO3a signaling pathway. Exp. Ther. Med. 2021, 22, 1017. [Google Scholar] [CrossRef]
- Han, S. G.; Han, S. S.; Toborek, M.; Hennig, B. EGCG protects endothelial cells against PCB 126-induced inflammation through inhibition of AhR and induction of Nrf2-regulated genes. Toxicol. Appl. Pharmacol. 2012, 261, 181–8. [Google Scholar] [CrossRef]
- Sun, W.; Liu, X.; Zhang, H.; Song, Y.; Li, T.; Liu, X.; Liu, Y.; Guo, L.; Wang, F.; Yang, T.; Guo, W.; Wu, J.; Jin, H.; Wu, H. Epigallocatechin gallate upregulates NRF2 to prevent diabetic nephropathy via disabling KEAP1. Free. Radic. Biol. Med. 2017, 108, 840–857. [Google Scholar] [CrossRef]
- Suzuki, T.; Yamamoto, M. Stress-sensing mechanisms and the physiological roles of the Keap1–Nrf2 system during cellular stress. J. Biol. Chem. 2017, 292, 16817–16824. [Google Scholar] [CrossRef] [PubMed]
- Mohan, T.; Narasimhan, K. K. S.; Ravi, D. B.; Velusamy, P.; Chandrasekar, N.; Chakrapani, L. N.; Srinivasan, A.; Karthikeyan, P.; Kannan, P.; Tamilarasan, B.; Johnson, T.; Kalaiselvan, P.; Periandavan, K. Role of Nrf2 dysfunction in the pathogenesis of diabetic nephropathy: Therapeutic prospect of epigallocatechin-3-gallate. Free. Radic. Biol. Med. 2020, 160, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y. W.; Zhu, Q. Q.; Yang, X. Y.; Xu, H. H.; Sun, B.; Wang, X. J.; Sheng, J. Wound healing can be improved by (—)-epigallocatechin gallate through targeting Notch in streptozotocin-induced diabetic mice. FASEB J. 2019, 33, 953–964. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Xiang, Z.; Wang, Y.; Li, X.; Fang, C.; Song, S.; Li, C.; Yu, H.; Wang, H.; Yan, L.; Hao, S.; Wang, X.; Sheng, J. (-)-Epigallocatechin Gallate Targets Notch to Attenuate the Inflammatory Response in the Immediate Early Stage in Human Macrophages. Front. Immunol. 2017, 8, 433. [Google Scholar] [CrossRef]
- Zhu, Q. Q.; Yang, X. Y.; Zhang, X. J.; Yu, C. J.; Pang, Q. Q.; Huang, Y. W.; Wang, X. J.; Sheng, J. EGCG targeting Notch to attenuate renal fibrosis via inhibition of TGFβ/Smad3 signaling pathway activation in streptozotocin-induced diabetic mice. Food. Funct. 2020, 11, 9686–9695. [Google Scholar] [CrossRef]
- López-Hortas, L.; Pérez-Larrán, P.; González-Muñoz, M. J.; Falqué, E.; Domínguez, H. Recent developments on the extraction and application of ursolic acid. A review. Food. Res. Int. 2018, 103, 130–149. [Google Scholar] [CrossRef]
- Xu, H. L.; Wang, X. T.; Cheng, Y.; Zhao, J. G.; Zhou, Y. J.; Yang, J. J.; Qi, M. Y. Ursolic acid improves diabetic nephropathy via suppression of oxidative stress and inflammation in streptozotocin-induced rats. Biomed. Pharmacother. 2018, 105, 915–921. [Google Scholar] [CrossRef]
- Su, L.; Cao, P.; Wang, H. Tetrandrine mediates renal function and redox homeostasis in a streptozotocin-induced diabetic nephropathy rat model through Nrf2/HO-1 reactivation. Ann. Transl. Med. 2020, 8, 990. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhu, C.; Yang, H.; Deng, J.; Fan, D. Protective effect of ginsenoside Rg5 against kidney injury via inhibition of NLRP3 inflammasome activation and the MAPK signaling pathway in high-fat diet/streptozotocin-induced diabetic mice. Pharmacol. Res. 2020, 155, 104746. [Google Scholar] [CrossRef]
- Wu, X.; Li, H.; Wan, Z.; Wang, R.; Liu, J.; Liu, Q.; Zhao, H.; Wang, Z.; Zhang, H.; Guo, H.; Qi, C.; Jiao, X.; Li, X. The combination of ursolic acid and empagliflozin relieves diabetic nephropathy by reducing inflammation, oxidative stress and renal fibrosis. Biomed. Pharmacother. 2021, 144, 112267. [Google Scholar] [CrossRef] [PubMed]
- Tang, S. T.; Su, H.; Zhang, Q.; Tang, H. Q.; Wang, C. J.; Zhou, Q.; Wei, W.; Zhu, H. Q.; Wang, Y. Sitagliptin inhibits endothelin-1 expression in the aortic endothelium of rats with streptozotocin-induced diabetes by suppressing the nuclear factor-κB/IκBα system through the activation of AMP-activated protein kinase. Int. J. Mol. Med. 2016, 37, 1558–66. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, D.; Fan, L.; Xiao, Q.; Zuo, H.; Li, Z. CAPE-pNO2 ameliorated diabetic nephropathy through regulating the Akt/NF-κB/iNOS pathway in STZ-induced diabetic mice. Oncotarget. 2017, 8, 114506–114525. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, N.; Yan, S.; Liu, M.; Sun, B.; Lu, Y.; Shao, Y. Ursolic acid alleviates inflammation and against diabetes-induced nephropathy through TLR4-mediated inflammatory pathway. Mol. Med. Rep. 2018, 18, 4675–4681. [Google Scholar] [CrossRef] [PubMed]
- Dey, N.; Ghosh-Choudhury, N.; Kasinath, B. S.; Choudhury, G. G. TGFβ-stimulated microRNA-21 utilizes PTEN to orchestrate AKT/mTORC1 signaling for mesangial cell hypertrophy and matrix expansion. PLoS One. 2012, 7, e42316. [Google Scholar] [CrossRef]
- Lu, X.; Fan, Q.; Xu, L.; Li, L.; Yue, Y.; Xu, Y.; Su, Y.; Zhang, D.; Wang, L. Ursolic acid attenuates diabetic mesangial cell injury through the up-regulation of autophagy via miRNA-21/PTEN/Akt/mTOR suppression. PLoS One. 2015, 10, e0117400. [Google Scholar] [CrossRef]
- Bento-Silva, A.; Patto, M. C. V.; do Rosário Bronze, M. Relevance, structure and analysis of ferulic acid in maize cell walls. Food Chem. 2018, 246, 360–378. [Google Scholar] [CrossRef]
- Choi, M. E. Autophagy in kidney disease. Annu. Rev. Physiol. 2020, 82, 297–322. [Google Scholar] [CrossRef]
- Yang, Y.; Klionsky, D. J. Autophagy and disease: unanswered questions. Cell Death Differ. 2020, 27, 858–871. [Google Scholar] [CrossRef]
- Li, F.; Chen, Y.; Li, Y.; Huang, M.; Zhao, W. Geniposide alleviates diabetic nephropathy of mice through AMPK/SIRT1/NF-κB pathway. Eur. J. Pharmacol. 2020, 886, 173449. [Google Scholar] [CrossRef]
- Li, X.; Wu, J.; Xu, F.; Chu, C.; Li, X.; Shi, X.; Zheng, W.; Wang, Z.; Jia, Y.; Xiao, W. Use of Ferulic Acid in the Management of Diabetes Mellitus and Its Complications. Molecules. 2022, 27, 6010. [Google Scholar] [CrossRef] [PubMed]
- Lei, D.; Chengcheng, L.; Xuan, Q.; Yibing, C.; Lei, W.; Hao, Y.; Xizhi, L.; Yuan, L.; Xiaoxing, Y.; Qian, L. Quercetin inhibited mesangial cell proliferation of early diabetic nephropathy through the Hippo pathway. Pharmacol. Res. 2019, 146, 104320. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Ji, X. J.; Zhou, Y. X.; Yao, X. Q.; Liu, Y. Q.; Zhang, F.; Yin, X. X. Quercetin inhibits the mTORC1/p70S6K signaling-mediated renal tubular epithelial–mesenchymal transition and renal fibrosis in diabetic nephropathy. Pharmacol. Res. 2015, 99, 237–47. [Google Scholar] [CrossRef] [PubMed]
- Shigeoka, A. A.; Mueller, J. L.; Kambo, A.; Mathison, J. C.; King, A. J.; Hall, W. F.; Correia, J.daS.; Ulevitch, R. J.; Hoffman, H. M.; McKay, D. B. An inflammasome-independent role for epithelial-expressed Nlrp3 in renal ischemia-reperfusion injury. J. Immunol. 2010, 185, 6277-85.
- Wang, C.; Pan, Y.; Zhang, Q. Y.; Wang, F. M.; Kong, L. D. Quercetin and allopurinol ameliorate kidney injury in STZ-treated rats with regulation of renal NLRP3 inflammasome activation and lipid accumulation. PLoS One. 2012, 7, e38285. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Gurung, P.; Wang, T.; Li, L.; Zhang, R.; Li, H.; Guo, R.; Han, Q.; Zhang, J.; Lei, S.; Liu, F. The relationship between the thickness of glomerular basement membrane and renal outcomes in patients with diabetic nephropathy. Acta. Diabetol. 2018, 55, 669–679. [Google Scholar] [CrossRef]
- Jiang, X.; Yu, J.; Wang, X.; Ge, J.; Li, N. Quercetin improves lipid metabolism via SCAP-SREBP2-LDLr signaling pathway in early stage diabetic nephropathy. Diabetes Metab. Syndr. Obes. 2019, 12, 827–839. [Google Scholar] [CrossRef]
- Lee, D.; Ko, W.K.; Hwang, D.S.; Heo, D.N.; Lee, S.J.; Heo, M.; Lee, K.S.; Ahn, J.Y.; Jo, J.; Kwon, I.K. Use of baicalin-conjugated gold nanoparticles for apoptotic induction of breast cancer cells. Nanoscale Res. Lett. 2016, 11, 381. [Google Scholar]
- Ma, L.; Wu, F.; Shao, Q.; Chen, G.; Xu, L.; Lu, F. Baicalin alleviates oxidative stress and inflammation in diabetic nephropathy via Nrf2 and MAPK signaling pathway. Drug Des. Devel. Ther. 2021, 15, 3207–3221. [Google Scholar] [CrossRef]
- Zhang, S.; Xu, L.; Liang, R.; Yang, C.; Wang, P. Baicalin suppresses renal fibrosis through microRNA-124/TLR4/NF-κB axis in streptozotocin-induced diabetic nephropathy mice and high glucose-treated human proximal tubule epithelial cells. J. Physiol. Biochem. 2020, 76, 407–416. [Google Scholar] [CrossRef]
- Ou, Y.; Zhang,W.; Chen, S.; Deng, H. Baicalin improves podocyte injury in rats with diabetic nephropathy by inhibiting PI3K/Akt/mTOR signaling pathway. Open Med. (Wars). 2021, 16, 1286–1298. [CrossRef] [PubMed]
- Nam, J. E.; Jo, S. Y.; Ahn, C. W.; & Kim, Y. S.; & Kim, Y. S. Baicalin attenuates fibrogenic process in human renal proximal tubular cells (HK− 2) exposed to diabetic milieu. Life Sci. 2020, 254, 117742. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pathophysiology of experimentally induced diabetic nephropathy. VEGF, vascular endothelial growth factor; IGF-1, insulin-like growth factor 1; SGLT2, sodium-glucose co-transporter 2; GPR91, kidney-specific G protein-coupled metabolic receptor; PGE2, prostaglandin; NO, nitric oxide; Ang II, Angiotensin II's; RAAS, renin-angiotensin-aldosterone system; mTOR, mechanistic target of rapamycin; TGFT-β, transforming growth factor beta; Smad, Suppressor of mothers against decapentaplegic; AMPK, adenosine monophosphate-activated protein kinase; mTOR, mammalian target of rapamycin.
Figure 1.
Pathophysiology of experimentally induced diabetic nephropathy. VEGF, vascular endothelial growth factor; IGF-1, insulin-like growth factor 1; SGLT2, sodium-glucose co-transporter 2; GPR91, kidney-specific G protein-coupled metabolic receptor; PGE2, prostaglandin; NO, nitric oxide; Ang II, Angiotensin II's; RAAS, renin-angiotensin-aldosterone system; mTOR, mechanistic target of rapamycin; TGFT-β, transforming growth factor beta; Smad, Suppressor of mothers against decapentaplegic; AMPK, adenosine monophosphate-activated protein kinase; mTOR, mammalian target of rapamycin.
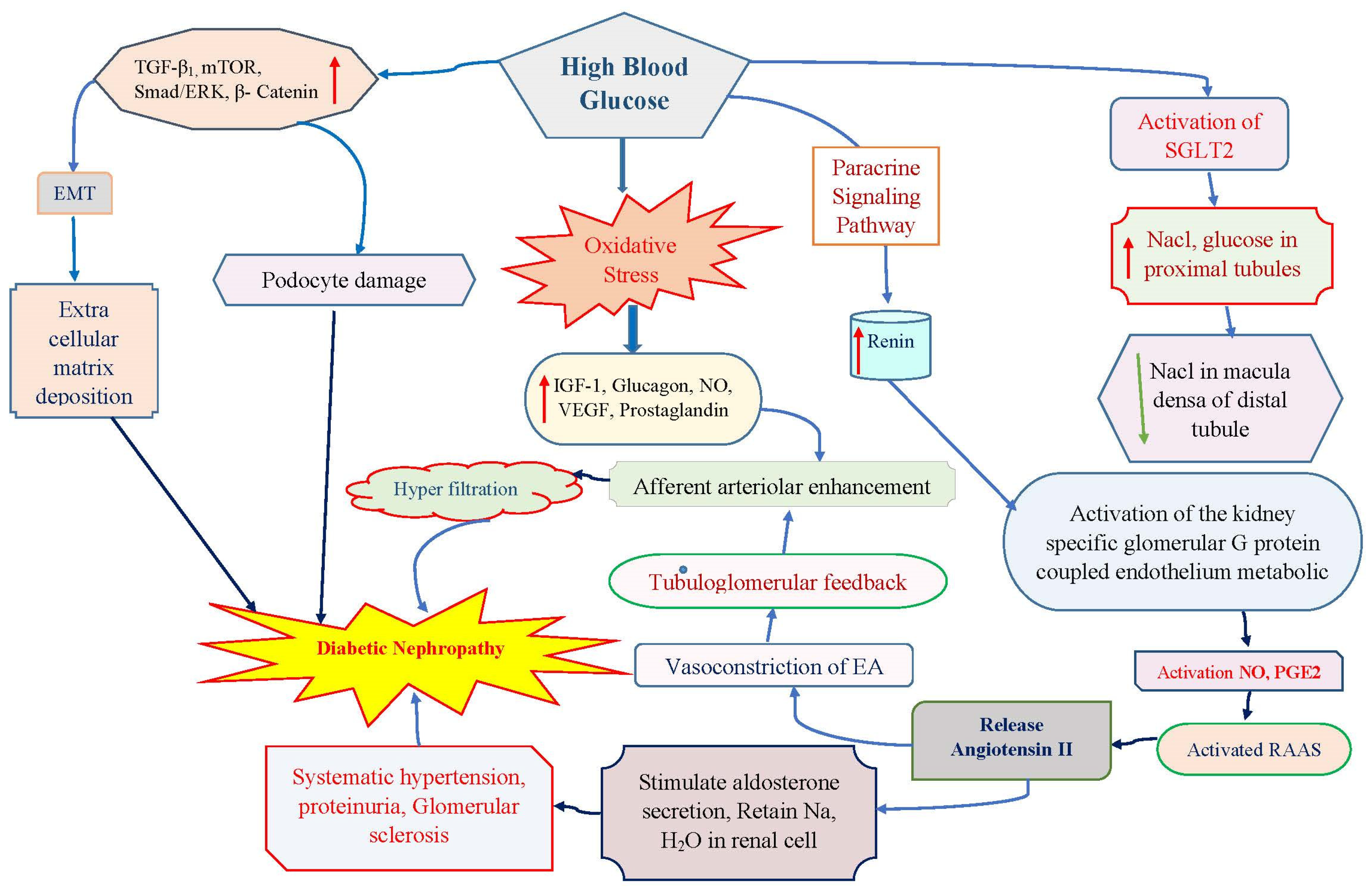
Figure 2.
Berberine can reduces glomerular injury in diabetic nephropathy in rats by preventing ROS generation and reduced extracellular matrix deposition in renal cell. TNF-α, Tumor necrosis factor alpha; IL-1β, Interleukin-1 beta; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; ICAM, Inter Cellular Adhesion Molecule; ECM, extracellular matrix.
Figure 2.
Berberine can reduces glomerular injury in diabetic nephropathy in rats by preventing ROS generation and reduced extracellular matrix deposition in renal cell. TNF-α, Tumor necrosis factor alpha; IL-1β, Interleukin-1 beta; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; ICAM, Inter Cellular Adhesion Molecule; ECM, extracellular matrix.
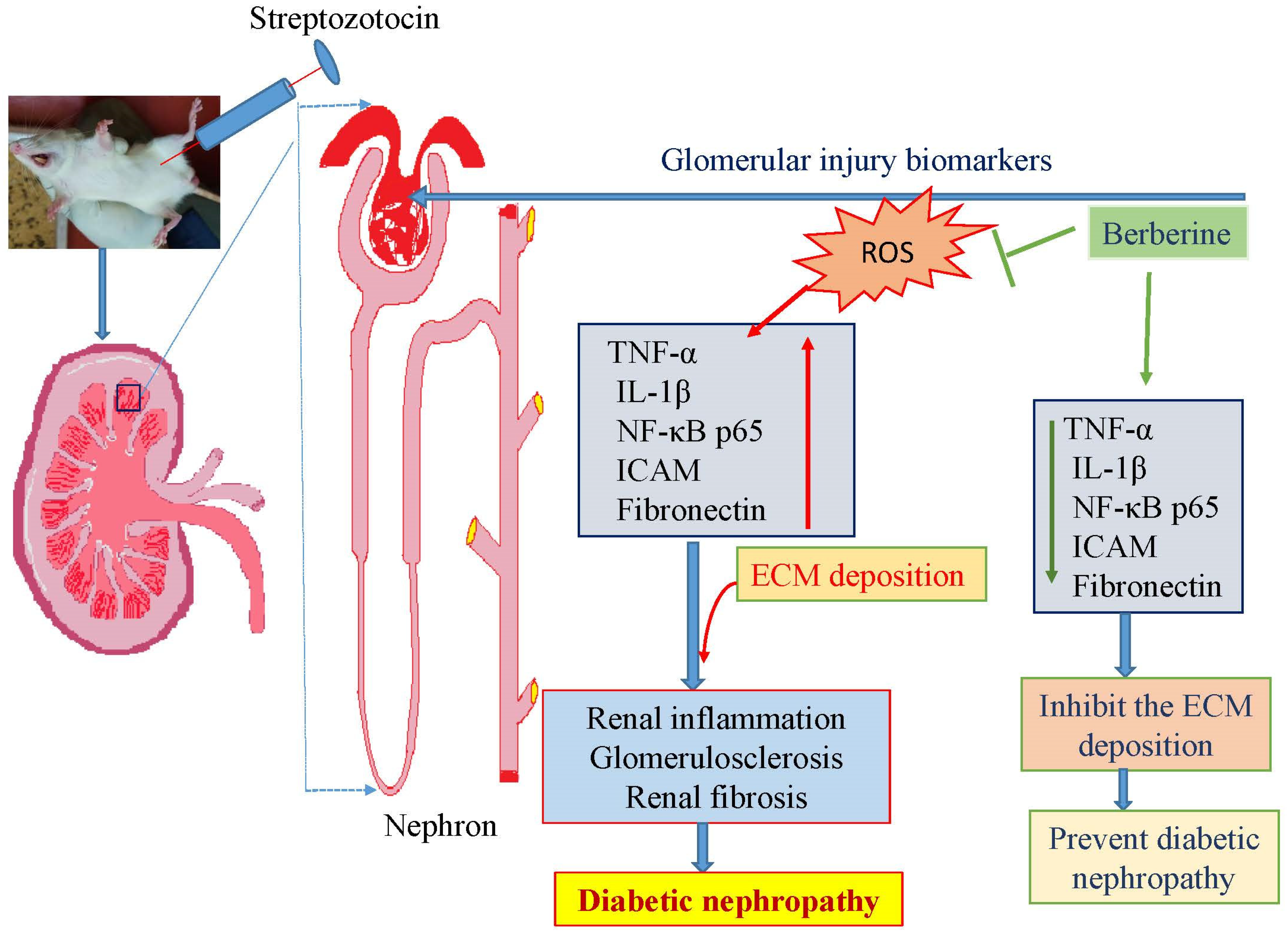
Figure 3.
A potential mechanism of epigallocatechin gallate for treating renal fibrosis brought on by high glucose concentrations is revealed by the possibility that it works by targeting Notch to suppress the TGF/Smad3 pathway. Notch, neurogenic locus notch homolog protein; TGFβ transforming growth factor-beta. Smad, suppressor of mothers against decapentaplegic.
Figure 3.
A potential mechanism of epigallocatechin gallate for treating renal fibrosis brought on by high glucose concentrations is revealed by the possibility that it works by targeting Notch to suppress the TGF/Smad3 pathway. Notch, neurogenic locus notch homolog protein; TGFβ transforming growth factor-beta. Smad, suppressor of mothers against decapentaplegic.
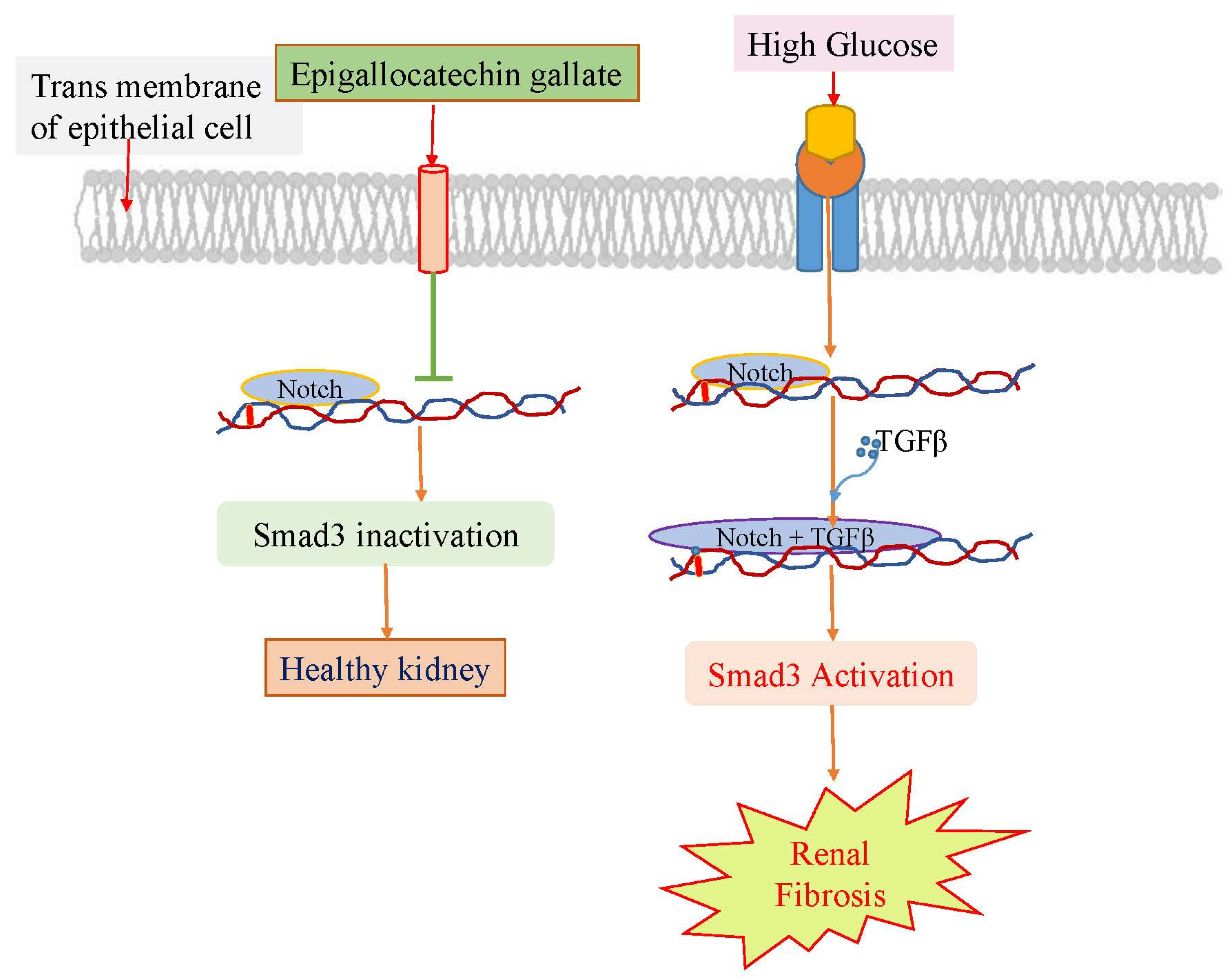
Figure 4.
Urosolic acid protects kidneys from diabetic nephropathy by inactivation of Akt/mTOR that involved in the downregulation of mi-RNA-21 and results upregulated PTEN expression of the glomerulus. ROS, reactive oxygen spices; miRNA-21, micro ribonucleic acid; PTEN, Phosphatase and tensin; Akt, Ak strain transforming; mTOR, mammalian target of rapamycin.
Figure 4.
Urosolic acid protects kidneys from diabetic nephropathy by inactivation of Akt/mTOR that involved in the downregulation of mi-RNA-21 and results upregulated PTEN expression of the glomerulus. ROS, reactive oxygen spices; miRNA-21, micro ribonucleic acid; PTEN, Phosphatase and tensin; Akt, Ak strain transforming; mTOR, mammalian target of rapamycin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



