
Submitted:
26 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
Super-high (x400) magnification dermoscopy (D400) is a new non-invasive imaging technique that has been shown to add information for the differential diagnosis of melanocytic lesions in a pilot study. Our study aimed to confirm if D400 can add details for the discrimination of clinically atypical nevus and melanoma. This is a retrospective observational, multicentric study enrolling patients who received an x20 (D20) and x400 (D400) magnification dermoscopic examination of pigmented skin lesions. Dermoscopic images were retrospectively evaluated by three observers for the presence/absence of nine D20 and twenty D400 dermoscopic features defined in the previous pilot study. Univariate and multivariate analyses were carried out to find predictors of benign and malignant behaviors. At D20 atypical pigment network, blue-whitish veil, atypical vascular pattern, regression, and homogenous pattern were more frequent in melanoma than in nevi (p<0.001). At D400 melanoma showed more frequently than benign lesions melanocytes with an irregular arrangement and irregular in shape and size (p<0.001). Network with edged papillae was more frequent in benign lesions than melanomas (p<0.001). Our study confirms that D400 can identify melanocytes with an irregular arrangement and irregular in shape and size in melanomas, adding information to the conventional D20 examination.
Keywords:
Dermoscopy
; high magnification
; super-high magnification
; keratinocyte
; melanocyte
; melanoma.
1. Introduction
Melanoma (MM) is a malignant tumor that arises from melanocytes and primarily involves the skin, but can also arise in the eye (uvea, conjunctiva, and ciliary body), meninges and on various mucosal surfaces.[1] Cutaneous melanoma represents a public health issue, due to its high morbidity and mortality. [2-4]. The incidence and mortality rates of cutaneous melanoma differ widely by country.[5] The incidence of melanoma is increasing worldwide in particular among white populations, especially where fair-skinned people have excessive sun exposure. Earlier diagnosis of melanoma (MM) improves the survival rates but the clinical presentation can be subtle and varied.[6]
Four main different subtypes of melanomas can be identified clinically and histologically. Superficial spreading melanoma (SSM) begins with an intraepidermal, horizontal or radial growth phase, appearing first as a macule that slowly evolves into a plaque, often with multiple colours and pale areas of regression. Secondary nodular areas may also develop. A characteristic histologic feature is the presence of an epidermal lateral component with pagetoid spread of clear malignant melanocytes throughout the epidermis. Nodular MM in contrast is a primarily nodular, exophytic brown-black, often eroded or bleeding tumour, which is characterised by an aggressive vertical phase, with a short or absent horizontal growth phase. Thus, an early identification in an intraepidermal stage is challenging. Lentigo maligna melanoma often arises after many years from a lentigo maligna (melanoma in situ) located predominantly in sun-damaged faces of elderly individuals. It is characterised histologically by a lentiginous proliferation of atypical melanocytes at the dermo-epidermal junction and histological features of chronic sun exposure (solar elastosis). Acral lentiginous melanoma is typically palmoplantar or subungual. In its early intraepidermal phase, there is an irregular, poorly circumscribed pigmentation; later a nodular region reflects the invasive growth pattern. In addition to these main types, there are several rarer variants of melanoma, such as desmoplastic, amelanotic and polypoid melanomas, which constitute less than 5% of cases.[1]
Clinically atypical nevi span a continuum from minimally abnormal nevi to markedly abnormal nevi that clinically cannot be distinguished from MM.[7] For this reason, diagnosis of MM is based on histopathology, with subsequent treatment decisions being based on histological classification and risk calculation.[8]
In addition to visual evaluation, supportive imaging techniques have been shown to improve clinical diagnostic accuracy. The most routinely used non-invasive imaging technique for the skin is dermoscopy, also known as epiluminescence microscopy, a magnifying handheld optical device that uses a light source to inspect skin lesions unobscured by skin surface reflections. Use of dermoscopy requires training, but when appropriately used, this method substantially enhances the diagnosis of unclear or doubtful lesions that are suspected to be MM, reducing the number of skin lesions that should be excised to find a MM.[9] With dermoscopy, MM detection proportion can be increased to up to 90%, instead of 70% with only clinical inspection.[10] In addition, other non-invasive imaging procedures such as reflectance confocal microscopy (RCM) and fluorescence advance dermoscopy can be used to improve the clinical diagnostic accuracy.[11,12]
Recently, a pilot study has shown that x400 dermoscopy (D400 or super-high magnification dermoscopy) can also aid the non-invasive diagnosis of MM by observing single pigmented cells.[13,14] Compared with naevi, MMs had a higher frequency of scattered, large, irregular (in shape and size) dendritic/roundish cells corresponding to atypical melanocytes, and violet/blue pigmented cells corresponding to melanophages under D400. The current study aimed to confirm if D400 can add details for the discrimination of clinically atypical melanocytic lesions.
2. Materials and Methods
2.1. Study Design
Retrospective observational, multicentric study.
2.2. Setting
Data were collected on patients who came to the Dermatology Department of the University Hospital of Siena (Italy) and Saint-Etienne (France), to the Department of Dermatology of the Skin Center of Senigallia (Italy), and to a Dermatology Private Practice of Genoa (Italy) for a dermatological examination between the 1st January 2018 and 31st December 2020. Data were analysed from March 2022 to April 2022. The study was conducted according to the criteria set by the Declaration of Helsinki. All data were de-identified before use. The patients in this manuscript gave written informed consent to publication of their case details
2.3. Participants
We enrolled non-consecutive patients with pigmented skin lesions of the body (except the face, palm and sole) that needed to be removed or followed up for their atypical clinical and/or x20 dermoscopy (D20) features according to a skin imaging expert dermatologist (E.C., J.L.P., R.R., M.G.).
2.4. Data Sources
For this study, we selected only patients who received a D20 and D400 magnification dermoscopic examination of lesions that needed follow-up or excision due to their atypical dermoscopic features. These lesions were recorded with the videodermoscope Fotofinder Medicam 1000 (Fotofinder System, Bad Birnbach, Germany).
To perform D400, we used the same camera as D20 and we changed the terminal lens. Specialists in skin imaging (E.C. and J.L.P.), acquired at least seven images for each lesion, for a total of 1400 images of 190 skin lesions, as D400 does not show an entire lesion (D400 field of view -FOV- of 1 mm x 0.5625 mm). We included cases with histological diagnosis or lesions unmodified at clinical and dermoscopic follow-up of at least 12 months.
2.5. Variables
For the clinical variables, we evaluated the patient’s sex and age. A group of three dermatologists (E.C. with >10 years of experience in skin imaging, G.C. with 5 years of experience in skin imaging, and V.C. with 2 years of experience in skin imaging) belonging to the University Departure of Dermatology of the Hospital-University of Siena evaluated together the images.
The D20 dermoscopy variables included: general dermoscopic pattern (homogenous, globular, network) and 7-point checklist parameters (atypical pigment network, blue-white veil, atypical vascular pattern, irregular streaks, regression structures, blotches irregularly distribute, and irregular dots/globules).
The D400 variables were those described in the previous pilot study [7,8]: the presence of the pigmented cells and their features, out-of-focus blue or grey/brown structureless areas, vessels, angled nests, and network with or without edged papillae. Pigmented cells were differentiated into keratinocytes (seen as regular polygonal brown mostly in focus cells, evenly spread and/or inside a network), roundish melanocytes (seen as large roundish brown-to-violet/blue scattered cells; cells were defined as “large” when they were larger than keratinocytes), dendritic melanocytes (dendritic brown-to-violet/blue scattered cells), and melanophages (large blue-to-violet non in focus cells with a not defined polymorphous shape). Considered cell features were cell colour (violet and blue colours are difficult to differentiate with D400 and were considered together; light and dark brown were also considered together because brown is often present with multiple shades in the same structure), shape and size irregularity of melanocytes, and irregular arrangement of single melanocytes.
2.6. Statistical Analysis
Descriptive statistics were performed: absolute frequencies and percentages were calculated for qualitative variables and mean and standard deviations for the quantitative ones. The association between qualitative variables and the outcome (i.e., MM/nevus) and D20 or D400 was evaluated by Fisher exact test. T-test was carried out if the variables were normally distributed (normal distribution evaluated by Kolmogorov Smirnov test) and there was homoscedasticity between variances evaluated by Bartlett test, otherwise Mann-Whitney test was used. Logistic regression was later performed to evaluate variables that were statistically significant in the previous univariate analysis (p-value <0.05). The best subset of variables was selected by a stepwise procedure based on Akaike’s criterion. Odds ratio (OR) and 95% confidence intervals (CI) were estimated by logistic regression. The analyses were carried out by R software version 3.6.2.
3. Results
3.1. Participants and Lesion Data
In this study 190 patients, 91 (48%) women and 99 (52%) men (range 9–97 years) with a single atypical skin lesion of the body (except the face), were selected. The 190 skin lesions included 73 MMs and 117 benign lesions (including 17 Reed-Spitz nevi) (Table 1).
A statistically significant (p<0,001) correlation between the presence of benign lesions in young patients and melanomas in elderly patients has been demonstrated [(48.79 (19.19%) vs 64.98 (16.70%)].
There was no association between sex and benign or malignant skin lesions.
3.2. x20 Dermoscopy
The D20 data are reported in Table 2.
Concerning malignant benchmarks, the atypical pigment network [in 59 MMs (80.8%) and 57 nevi (48.7%) p<0.001, Table 1], blue-whitish veil [in 49 MMs (67.1%) and 18 nevi (15.4%) p<0.001, Table 2], atypical vascular pattern [in 12 MMs (16.4%) and 1 nevus (0.9%) p<0.001, Table 2], irregular streaks [in 22(30.1%) MMs and 11(9.4%) nevi, p=0.001], and regression structures [in 49 MMs (67.1%) and 33 (28.2%) p<0.001, Table 2] were more frequent in MM than in the benign lesions. As for dermoscopy general patterns, the homogenous pattern was more frequent in MM [43 MMs (58.9%) and 32 nevi (27.4%); p<0.001, Table 2] than in the other lesions, whereas the globular pattern was more frequent in benign lesions [in 7 MMs (9.6%) and 41 nevi (35.0%); p<0.001, Table 2] (Figure 1).
3.3. x400 Dermoscopy
The D400 features data are reported in Table 3.
MMs more frequently showed roundish [36 (49.3%) vs 35 (29.9%); p=0.011], dendritic [22 (30.1%) vs 19 (16.2%); p=0.037], irregularly arranged [30 (41.1%) vs 19 (16.2%); p <0.001)], and irregular in shape and size melanocytes [38 (52.1%) vs 21 (17.9%) ; p<0.001], and angled nests [16 (22.2%) vs 9 (7.7%); p=0.008] than nevi (Figure 2). Benign lesions more frequently revealed network with edged papillae than MMs [30 (25.6%) vs 3 (4.1%); p <0.001] (Figure 3). Cell colour [black 13 (11.1%) vs 7 (9.6%), brown 107 (91.5%) vs 66 (90.4%), violet/blue 45 (38.5%) vs 29 (39.7%)], out-of-focus bluish [36 (30.8%) vs 24 (32.9%)] or grey/brown [23 (19.7) vs 11 (15.1%)] structureless areas and vessel presence [26 (22.2%) vs 23 (31.5%)] were not statistically significant for the differential diagnosis between MM and benign lesions. The observation of benign lesions pointed out a higher visibility of keratinocytes [109 (93.2%) vs 64 (87.7%)] and roundish nests [42 (35.9%) vs 22 (30.1%)] and a lower presence of melanophages [19 (16.2%) vs 17 (23.3%)] with no statistically significant difference.
3.4. Multivariate Analysis
The multivariate regression considered the following variables: clinical features (age, sex and location), D20 (7-point checklist, general dermoscopic pattern) and D400 (cell presence, cell colour, melanocyte irregularity in shape and size, irregular melanocyte arrangement, roundish nests, out of focus structureless areas, vessels, network with edged papillae and angled nests) (Table 4).
According to the stepwise procedure, older age and irregular melanocyte arrangement at D400 were more indicative of malignant lesions (OR 1.05, 95% CI 1.03-1.09, p<0.001 and OR 4.69, 95% CI 1.58-15.45, p<0,001, respectively), and network with edged papillae at D400 was more indicative of benign lesion (OR 0.16, 95% CI 0.03-0.57, p = 0.009).
4. Discussion
Conventional dermoscopy provides images that are at 10-30x magnification. Since its development there has been also an interest in exploring higher magnifications. Higher magnification has been mainly applied to a better identification of parasites like Sarcoptes scabies, that is seen as a barely visible dark triangle in conventional dermoscopy and as a well-defined oval body with possible near droppings and eggs at 70x. [15]
In 1993 x400 images of melanocytic lesions were published, but their resolution was low, and their interpretation remained vague.[16] Lower magnification at 10-30x had the advantage of giving an image of an entire skin tumor in most of the cases, and this is probably the reason of the selection of this magnification in the clinical practice, with terminology, diagnostic algorithms and scores that have been based on this magnification. In 2018 the Italian group of Renato Rossi published amazing images of nevi that compared x20 and x400 dermoscopy, highlighting the potentiality of high magnification.[17] In the following year Jean Luc Perrot had the patience to explore entire skin lesions with D400 and handheld RCM to find the exact same area under both techniques.[18] Professor Perrot showed the same pigmented keratinocytes and pigmented atypical melanocytes with both techniques in a solar lentigo and a MM, respectively. This was the first demonstration of the possibility of observing single cells with a dermoscope device.
Subsequently, D400 also showed the possibility of observing filaments and conidia in a case of tinea nigra, highlighting how high magnification could have an impact on the identification of specific pigmented structures.[19] In addition, our group demonstrated that even non pigmented structures could be observed under D400, such as demodex. Demodex folliculorum can be observed as elongated body similar to what can be seen by RCM due to the similar size of the field of view (FOV) of these two imaging techniques.[20]
There are few videodermoscopes that provide super high magnification images and the most studied are the Fotofinder described in the present work (FOV 1 mm x 0.5625 mm) and the Horus device (Horus system, Trapani, Italy, FOV 1.7mm x 1.3 mm). Their magnification has been called super high magnification to distinguish it from high magnification (70x-100x) already used in the past. The Horus device has also the possibility of producing fluorescence dermoscopy images using a monochromatic light emitting source with a wavelength of 405 nm (±5 nm) and a fixed angle of incidence. [11,21] The latter images are in a greyscale and with a FOV of 340 µm.
Our study confirmed that D400 can identify single pigmented cells in the skin, being able to reveal them in quite all cases. Three main pigmented cell populations seem to be identifiable under D400: keratinocytes, melanocytes and melanophages. Keratinocytes are seen as small and polygonal cells, whereas melanocytes can be identified as dendritic cells or as roundish cells larger than keratinocytes. Like RCM, it seems that is not possible to identify non-activated melanocytes that have the same size as the surrounding keratinocytes. This probably explains why melanocytes were more frequently seen in MMs than nevi.
Interestingly, we confirmed that the presence of melanocytes with the irregular arrangement (scattered) and irregular in shape and size had a higher frequency in MMs than in nevi (Table 3, p<0.001). Cell distribution seems to be a fundamental parameter for the detection of MM at D400 because in nevi we could see homogeneously distributed keratinocytes or melanocytes organized in nests, whereas in MMs we had a higher frequency of scattered melanocytes. Based on our experience (data unpublished) these scattered cells correlate with pagetoid cells in the upper layers of the epidermis under RCM and are usually more abundant than in RCM images because they correspond to cells contained in a superposition of layers and not to a single focal plane.
The presence of edged papillae was associated with benignity, similar to what is seen under RCM, due to the lack of atypical melanocyte proliferation that alters the dermo-epidermal junction. Differently from the previous pilot study [9], blue out-of-focus structureless areas, violet/blue pigmented cells, and melanophages were not associated with MMs, and therefore these features seem to be related to other conditions such as regression rather than malignancy.
The main limitation of D400 seems to be the poor image penetration in case of hyperkeratotic or heavily pigmented lesions or clinically bluish lesions; in these cases, it is possible to recognize only scales or heavily pigmented keratinocytes that mask the underlying structures or a bluish homogeneous colour with no visible cells. If we compare D400 to RCM, D400 has less concern about false-positive results given by the presence of dendritic Langerhans cells in the epidermis possibly mistaken for melanocytes under RCM and has a lower cost. However, D400 can miss atypical melanocytes that are not heavily pigmented or deeper located and can show large cells suggestive of atypical melanocytes when multiple keratinocytes are superposed due to the lack of confocal sections.
Notably, nevi of our series were clinically and dermoscopically atypical, as demonstrated by the high percentage of cases with a 7-point checklist score ≥3 (49/117 benign lesions—41.9%). As expected, some parameters of the 7-point checklist (atypical pigment network, blue-whitish veil, atypical vascular pattern, and regression structures) were more frequently linked to MM diagnosis (70/73 malignant lesions—95.9%) (p<0,001).[10] It is possible that if we consider less atypical nevi, the differences between nevi and MMs would be even more marked at D400.
The main limitation of this study was represented by the fact that the acquisition of the images was dependent on the expertise of the investigators. Differently from D20, D400 does not allow to provide an image of the entire lesions and the selection of the areas to be imaged is operator-dependent. Interestingly the videodermoscope that acquires the D400 images, can progressively increase the magnification and therefore it can be useful to target an area of interest at D20 and to progressively zoom in. Moreover, there is no automatic focus and the operator needs to adjust the focus when acquiring the images. Another limitation of this study is the lack of correlation between histopathological images and images of other new non-invasive imaging techniques such as RCM. Moreover, our study did not include lentigo maligna and acral MM because of their peculiar features.
In conclusion, our study about the use of D400 for the diagnosis of lesions confirmed that D400 can reveal melanocytes irregular in arrangement and in shape and size in MMs, more frequently than in nevi and that can help the diagnosis of MM together with conventional dermoscopy data. Moreover, we could assume that D400 could help to direct the choice of the more representative site to perform a biopsy in case of large lesions and could help the identification of the anatomic structures observed under conventional x20 dermoscopy.
Author Contributions
Conceptualization, Elisa Cinotti; methodology, Elisa Cinotti; validation, Elisa Cinotti; formal analysis, Alessandra Cartocci; investigation, Giulio Cortonesi and Vittoria Cioppa; resources, Elisa Cinotti; data curation, Giulio Cortonesi, Vittoria Cioppa, Elisa Cinotti, Jean Luc Perrot, Renato Rossi and Matteo Gnone ; writing—original draft preparation, Vittoria Cioppa and Giulio Cortonesi; writing—review and editing, Elisa Cinotti; visualization, Elisa Cinotti and Linda Tognetti; supervision, Pietro Rubegni; project administration, Pietro Rubegni. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Garbe, C.; Peris, K.; Hauschild, A.; Saiag, P.; Middleton, M.; Spatz, A.; Grob, J.J.; Malvehy, J.; Newton-Bishop, J.; Stratigos, A.; et al. Diagnosis and treatment of melanoma: European consensus-based interdisciplinary guideline. Eur J Cancer 2010, 46, 270–283. [Google Scholar] [CrossRef] [PubMed]
- Sacchetto, L.; Zanetti, R.; Comber, H.; Bouchardy, C.; Brewster, D.H.; Broganelli, P.; Chirlaque, M.D.; Coza, D.; Galceran, J.; Gavin, A.; et al. Trends in incidence of thick, thin and in situ melanoma in Europe. Eur J Cancer 2018, 92, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015, 136, E359–386. [Google Scholar] [CrossRef] [PubMed]
- Iannacone, M.R.; Youlden, D.R.; Baade, P.D.; Aitken, J.F.; Green, A.C. Melanoma incidence trends and survival in adolescents and young adults in Queensland, Australia. Int J Cancer 2015, 136, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; van Akkooi, A.C.J.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet (London, England) 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Jerant, A.F.; Johnson, J.T.; Sheridan, C.D.; Caffrey, T.J. Early detection and treatment of skin cancer. American family physician 2000, 62, 357–368. [Google Scholar] [PubMed]
- Kittler, H.; Pehamberger, H.; Wolff, K.; Binder, M. Follow-up of melanocytic skin lesions with digital epiluminescence microscopy: patterns of modifications observed in early melanoma, atypical nevi, and common nevi. Journal of the American Academy of Dermatology 2000, 43, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: implications for melanoma treatment and care. Expert review of anticancer therapy 2018, 18, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Chuchu, N.; Ferrante di Ruffano, L.; Matin, R.N.; Thomson, D.R.; Wong, K.Y.; Aldridge, R.B.; Abbott, R.; Fawzy, M.; et al. Dermoscopy, with and without visual inspection, for diagnosing melanoma in adults. The Cochrane database of systematic reviews 2018, 12, Cd011902. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, M.E.; Macaskill, P.; Holt, P.E.; Menzies, S.W. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol 2008, 159, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Cortonesi, G.; Rubegni, P. High magnification and fluorescence advanced videodermoscopy for hypomelanotic melanoma. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI) 2020, 26, 766–768. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Labeille, B.; Debarbieux, S.; Carrera, C.; Lacarrubba, F.; Witkowski, A.M.; Moscarella, E.; Arzberger, E.; Kittler, H.; Bahadoran, P.; et al. Dermoscopy vs. reflectance confocal microscopy for the diagnosis of lentigo maligna. J Eur Acad Dermatol 2018, 32, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Rossi, R.; Ferrara, G.; Tognetti, L.; Rubegni, P.; Perrot, J.L. Image Gallery: Super-high magnification dermoscopy can identify pigmented cells: correlation with reflectance confocal microscopy. Br J Dermatol 2019, 181, e1. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Tognetti, L.; Campoli, M.; Liso, F.; Cicigoi, A.; Cartocci, A.; Rossi, R.; Rubegni, P.; Perrot, J.L. Super-high magnification dermoscopy can aid the differential diagnosis between melanoma and atypical naevi. Clinical and experimental dermatology 2021, 46, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Perrot, J.L.; Labeille, B.; Cambazard, F. [Diagnosis of scabies by high-magnification dermoscopy: the “delta-wing jet” appearance of Sarcoptes scabiei]. Annales de dermatologie et de venereologie 2013, 140, 722–723. [Google Scholar] [CrossRef] [PubMed]
- Puppin, D., Jr.; Salomon, D.; Saurat, J.H. Amplified surface microscopy. Preliminary evaluation of a 400-fold magnification in the surface microscopy of cutaneous melanocytic lesions. Journal of the American Academy of Dermatology 1993, 28, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Dusi, D.; Rossi, R.; Simonacci, M.; Ferrara, G. Image Gallery: the new age of dermoscopy: optical super-high magnification. British Journal of Dermatology 2018, 178, e330–e330. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Rossi, R.; Ferrara, G.; Tognetti, L.; Rubegni, P.; Perrot, J.L. Image Gallery: Super-high magnification dermoscopy can identify pigmented cells: correlation with reflectance confocal microscopy. 2019, 181, e1-e1. [CrossRef]
- Cinotti, E.; Ekinde, S.; Labeille, B.; Raberin, H.; Tognetti, L.; Rubegni, P.; Perrot, J.L. Image Gallery: Pigmented hyphae can be identified in vivo by high and super-high magnification dermoscopy. Br J Dermatol 2019, 181, e4. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, E.; Bertello, M.; Donelli, C.; Rossi, R.; Tognetti, L.; Perrot, J.L.; Rubegni, P. Super-high magnification dermoscopy can detect Demodex folliculorum. Journal of the European Academy of Dermatology and Venereology : JEADV 2023, 37, e96–e97. [Google Scholar] [CrossRef] [PubMed]
- Scarfì, F.; Gori, A.; Topa, A.; Trane, L.; Dika, E.; Broganelli, P.; Massi, D.; De Giorgi, V. Image Gallery: In vivo fluorescence-advanced videodermatoscopy for the characterization of skin melanocytic pigmented lesions. Br J Dermatol 2019, 180, e104. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
x20 dermoscopy evaluation of a nevus with a regular dermoscopic aspect (a.), a dermoscopically atypical nevus (b.) and a melanoma (c.).
Figure 1.
x20 dermoscopy evaluation of a nevus with a regular dermoscopic aspect (a.), a dermoscopically atypical nevus (b.) and a melanoma (c.).
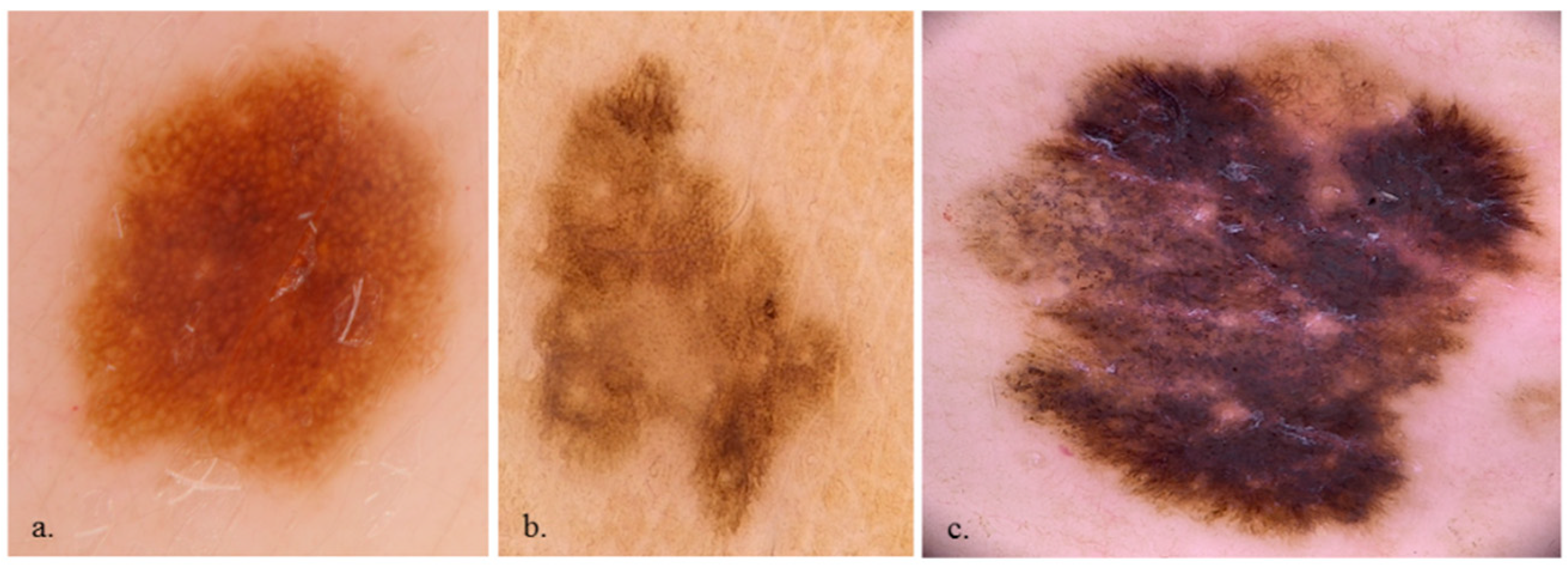
Figure 2.
x400 dermoscopy shows pleomorphic roundish and dendritic melanocytes (a.), homogeneous keratinocytes (b.) and a cluster of melanocytes (c.).
Figure 2.
x400 dermoscopy shows pleomorphic roundish and dendritic melanocytes (a.), homogeneous keratinocytes (b.) and a cluster of melanocytes (c.).
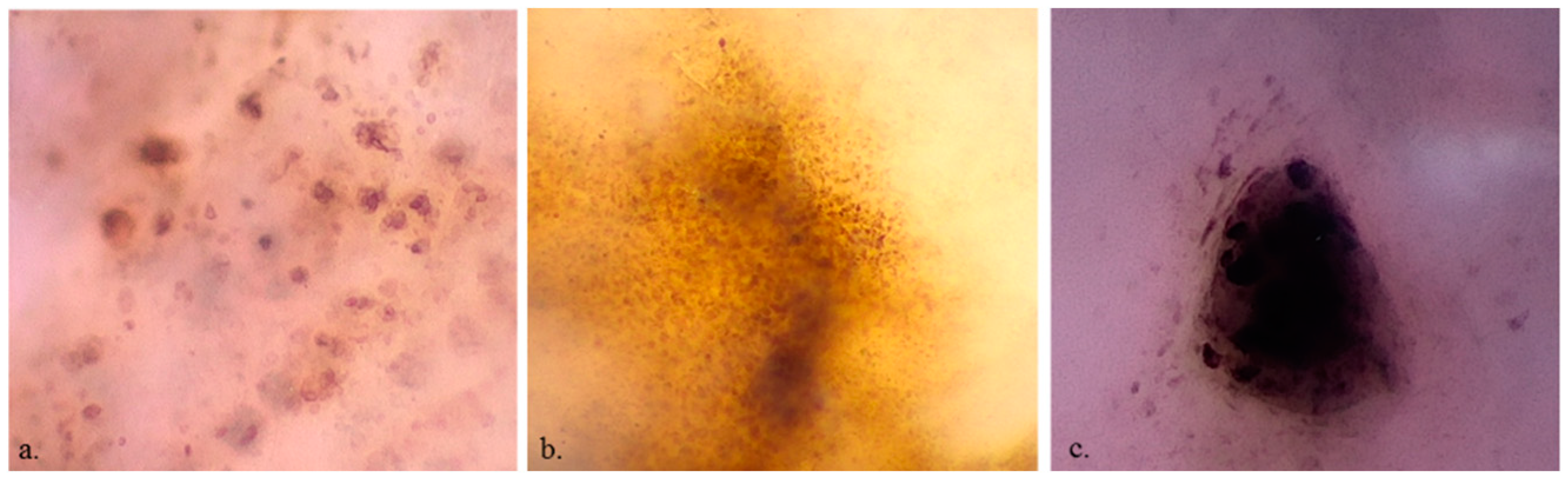
Figure 3.
x400 dermoscopy shows edged papillae (a.), vessels (b.) and out-of-focus structureless areas (c.).
Figure 3.
x400 dermoscopy shows edged papillae (a.), vessels (b.) and out-of-focus structureless areas (c.).
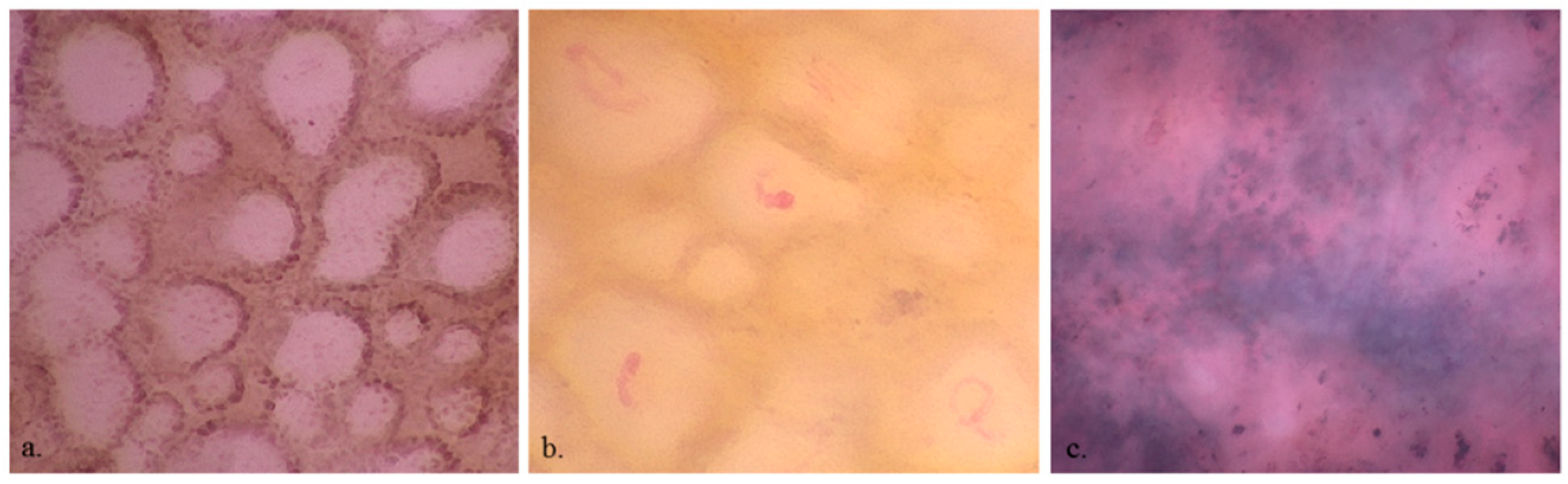

Table 1.
Clinical features of the evaluated cases.
| Benign lesions n = 117 |
Malignant lesions n = 73 |
p-value | |
|---|---|---|---|
| Age (years; SD) | 48.79 (19.19%) | 64.98 (16.70%) | <0.001 |
| Male | 68 (61.3%) | 31 (56.4%) | 0.846 |
| Female | 49 (38.7%) | 42 (43.6%) |
SD: standard deviation
Table 2.
x20 dermoscopy features.
| Benign lesions | Malignant lesions | p-value | |
|---|---|---|---|
| 7-point checklist | |||
| Atypical pigment network | 57 (48.7%) | 59 (80.8%) | <0.001 |
| Blue-whitish veil | 18 (15.4%) | 49 (67.1%) | <0.001 |
| Atypical vascular pattern | 1 (0.9%) | 12 (16.4%) | <0.001 |
| Irregular streaks | 11 (9.4%) | 22 (30.1%) | 0.001 |
| Regression structures | 33 (28.2%) | 49 (67.1%) | <0.001 |
| Irregular pigmentations | 40 (34.2%) | 23 (31.5%) | 0.823 |
| Irregular dots/globules | 36 (30.8%) | 18 (24.7%) | 0.457 |
| General pattern | |||
| homogeneous | 32 (27.4%) | 43 (58.9%) | <0.001 |
| globular | 41 (35.0%) | 7 (9.6%) | <0.001 |
| network | 67 (57.3%) | 41 (56.2%) | 1.000 |
Table 3.
x400 dermoscopy features.
| Benign lesions | Malignant lesions | p-value | |
|---|---|---|---|
| Cell presence | 113 (96.6%) | 72 (98.6%) | 0.695 |
| Keratinocytes | 109 (93.2%) | 64 (87.7%) | 0.304 |
| Roundish melanocytes | 35 (29.9%) | 36 (49.3%) | 0.011 |
| Dendritic melanocytes | 19 (16.2%) | 22 (30.1%) | 0.037 |
| Melanophages | 19 (16.2%) | 17 (23.3%) | 0.310 |
| Cell colour | |||
| Black | 13 (11.1%) | 7 (9.6%) | 0.929 |
| Brown | 107 (91.5%) | 66 (90.4%) | 1.000 |
| violet/blue | 45 (38.5%) | 29 (39.7%) | 0.983 |
| Cell irregularity in shape and size | 21 (17.9%) | 38 (52.1%) | <0.001 |
| Cell distribution: irregular arrangement | 19 (16.2%) | 30 (41.1%) | <0.001 |
| Roundish nests | 42 (35.9%) | 22 (30.1%) | 0.510 |
| Out-of-focus structureless areas | |||
| bluish | 36 (30.8%) | 24 (32.9%) | 0.886 |
| grey/brown | 23 (19.7%) | 11 (15.1%) | 0.543 |
| Vessels | 26 (22.2%) | 23 (31.5%) | 0.210 |
| Network | |||
| with edged papillae | 30 (25.6%) | 3 (4.1%) | <0.001 |
| without edged papillae | 18 (15.4%) | 19 (26.0%) | 0.107 |
| Angled nest | 9 (7.7%) | 16 (22.2%) | 0.008 |
Table 4.
Multivariate analysis.
| OR | p-value | |
|---|---|---|
| Age | 1.05 (1.03-1.09) | <0.001 |
| Irregular melanocyte distribution | 4.69 (1.58-15.45) | 0.007 |
| Network with edged papillae | 0.16 (0.03-0.57) | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



