
Submitted:
30 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
Patients with polycythemia vera (PV) are at increased risk of thrombosis and hemorrhages. Although hydroxyurea (HU) has been the frontline therapy for patients at high-risk of vascular complications, about 25% of patients develop resistance/intolerance to this therapy. The aim of this non-interventional, multicenter cohort study was to understand the clinical characteristics and HU treatment response of Portuguese PV patients. HU resistance/intolerance was defined according to adjusted European LeukemiaNet (ELN) criteria. 134 PV patients with a mean disease duration of 4.8±5.0 years were included and followed up for 2 years. At baseline, most patients were ≥60 years old (83.2%), at high risk for thrombotic events (87.2%), and receiving HU therapy (79.1%). A total of 10 thrombotic events and 8 hemorrhagic events were reported, resulting in a 5-year probability of thrombo-hemorrhagic events of 17.2%. Hematocrit (p=0.007), hemoglobin (p=0.012) and MPN10 symptom score (12.0±11.6 vs 10.3±9.1; p=0.041) decreased significantly at the 24-month visit compared to baseline. Overall, 75.9% of patients met at least one of the adjusted ELN criteria for HU resistance. 14.4% of patients remained on HU throughout the study. The results from this real-world study may help identify the subset of patients at higher risk of disease sequelae who may benefit from earlier second-line treatment.
Keywords:
disease management
; hemorragic events
; hydroxyurea
; resistance
; symptomatic evaluation
; patient-reported outcomes
; thrombotic events
; polycythemia vera
1. Introduction
Polycythemia vera (PV) is a chronic myeloproliferative neoplasm (MPN) character-ised by a somatic activating mutation in the JAK2 gene that drives abnormal erythrocytosis, resulting in an abnormal increase in red blood cell mass [1,2]. The incidence of PV is around 2 per 100,000 per year, which results in an overall prevalence of 44-57 per 100,000 individuals [3,4].
Patients with PV have an increased risk of thrombosis and hemorrhages, with an associated risk of disease progression to myelofibrosis (MF) or acute myeloid leukaemia (AML) [4,5]. Such clinical outcomes reduce patients’ quality of life and increase their morbidity and mortality. Thus, symptomatic relief and prevention of thrombotic and hemorrhagic events represent primary goals in PV treatment [6,7].
The risk of thrombosis in PV patients is associated with the patients’ age and the likelihood of recurrent thrombosis. Accordingly, PV patients can be stratified into high-risk (age >60 years or thrombosis history) or low-risk (absence of both risk factors) [8]. The risk of thrombotic events is reduced by maintaining a haematocrit level below 45% [9]. Typical management is accomplished with cytoreductive therapy in high-risk or selected patients and with phlebotomies and low-dose aspirin in all PV patients [6,10].
The first-line cytoreductive therapy of choice is hydroxyurea (HU), which may still require the concomitant use of phlebotomy [11]. However, a Spanish study reported that 12% and 13% of patients developed resistance and intolerance to HU, respectively. HU was also associated with an increased risk of death or haematological transformation [12]. Therefore, clinicians must monitor the response to HU and its side effects in order to decide whether the patient should be switched to second-line therapy.
Clinical characterisation of Portuguese PV patients is scarce. So, the main goal of this study was to characterise the clinical profile, symptomatic burden, and treatment response of Portuguese PV patients. A better understanding of the clinical characteristics of these patients, especially those with an inadequate response or intolerance to HU, is of paramount importance for an optimal treatment approach and the best possible clinical outcomes.
2. Materials and Methods
2.1. Study Design and Population
This is a descriptive, non-interventional, prospective, and multicenter cohort study of adult Portuguese patients diagnosed with PV and registered in the Portuguese Oncology Nursing Association (AEOP) database, which includes patients with all Philadelphia-negative myeloproliferative neoplasms (PV, MF, and ET) from 8 participating centers that geographically represent the country. This database was initially established for the assessment and monitoring of symptoms in MPN patients using the MPN-Symptom Assessment Form Total Symptom Score (MNP-10) [13]. With the exception of the MNP10 scale, all clinical information was collected by healthcare professionals from patients’ medical records as part of routine care (secondary use of data). The AEOP database index date was March 21, 2017. This corresponded to the first patient entry and assessment of symptom burden using the MNP10 questionnaire.
The study period was one year (1 November 2020 to 20 October 2021), during which patient data were collected from the first registry up to a maximum of 24 months. The patient’s first registry into the database was defined as the baseline visit, and the data collected at 12 and 24 months after study initiation were considered the two follow-up visits. The observation period spanned from the index date until death, loss to follow-up, or the end of the study at month 24.
Adult patients (>18 years) with a confirmed diagnosis of PV according to the hospital medical record (patient diary) and registered in the AEOP database were included in the study.
2.2. Study Endpoints
The characterisation of PV patients’ demographics, clinical profile, treatment patterns and symptom burden (assessed through the MNP10 score) were considered primary endpoints.
Secondary endpoints included the description of thrombotic and hemorrhagic events, the proportion of patients with resistance/intolerance to HU and the assessment of the association between potential risk factors and key clinical outcomes.
The evaluation of resistance/intolerance to HU was performed based on adjusted ELN criteria [14,15], which were adapted to this study’s characteristics. These criteria were applied to all patients on any HU dosage for at least 9 months, instead of considering the maximum tolerated HU dose. Resistance was defined in patients meeting at least one of the following criteria: need for phlebotomy, platelet count >400×109/L and leukocyte count >10×109/L and neutrophil count <1.0×109/L or platelet count <100×109/L or hemoglobin <10.0 g/dL. Symptoms were evaluated through the MPN10 score and considered when the MPN10 total score ≥20 or an individual symptom score >5 [16].
Intolerance was considered whenever any unacceptable HU-related non-haematological toxicities occurred.
2.3. Data collection
Demographic data (age and sex) were collected at baseline. Clinical data (disease duration, therapy, haematocrit level, platelet count, leukocyte count, hemoglobin level, and neutrophil count) were collected at baseline and at the 12- and 24-month follow-up visits.
As recommended by the NCCN guidelines, PV patients' symptoms were assessed and monitored using the MPN-SAF total symptom score, also known as the MPN10 scale [17]. During the course of their treatment, patients self-evaluated 10 of the most clinically significant symptoms, with a total score ranging from 0 to 100 points [13].
Clinician-reported cases of MF progression, AML transformation, non-haematological toxicities, and resistance/intolerance to HU were also recorded.
2.4. Statistical analysis
Categorical variables were summarised by providing absolute and relative frequencies. Continuous variables were summarised considering the mean, standard deviation (SD) and median.
The normality of the distribution of continuous variables was assessed using histograms, Q-Q plots, and the Shapiro-Wilk’s test. The comparison of paired observations, from baseline to 12 and 24 months, for continuous variables was performed using the non-parametric Wilcoxon test for paired samples. The Bonferroni method was used to adjust the significance level for the multiple comparisons.
For the symptom scale, the significance level was adjusted when comparing the results of each symptom. Kaplan-Meier analysis was performed to estimate the time to thrombotic and hemorrhagic events since PV diagnosis (maximum registered time of 240 months).
A significance level of 5% was considered. Two-sided 95% confidence intervals (CIs) for the mean and for percentages were provided for the main results. Statistical analysis was conducted using the R® software version 4.1.2.
3. Results
3.1. Demographic and clinical profile of PV patients
A total of 134 PV patients registered in the AEOP database were included at baseline. Twelve-month follow-up data was available for 65 patients, and 24-month follow-up data was available for 37 patients.
At baseline, patients had a mean age of 70.6 ± 11.7 years, with the majority being female (71, 53%). Still, a considerable number (22, 16.8%) of patients <60 years were included. The mean disease duration was 4.8 ± 5.0 years, with a total of 21 (17.2%) patients with a PV diagnosis for ≥10 years. Based on the classical risk stratification for thrombotic events in PV patients (age > 60 years or thrombotic history), 104 participants (83.2%) were considered high-risk PV patients at the time of study initiation (Table 1). No differences were observed between the group of patients classified as low-risk and those classified as high-risk with respect to mean disease duration (5.2 years vs. 4.7 years, respectively; p=0.524). nor with respect to the female-to-male ratio between the groups (p=0.157) (Table S1).
3.2. Treatment characteristics
At enrolment, the majority of patients (n=106, 79.1%) were already receiving pharmacological therapy (Table 2), with HU being the most frequent treatment (106, 79.1%), administered for a median (P25-P75) of 1.9 (0.2-3.4) years. HU was taken either alone (66, 49.2%) or in combination with other drugs (40, 29.8%), mainly acetylsalicylic acid (ASA; 38, 28.4%). Phlebotomy was added to HU therapy in 35 patients (26.1%). Pharmacological treatment options other than HU were ASA alone (6, 4.5%), ASA with interferon (1, 0.7%), ruxolitinib (5, 3.7%), or busulfan (1, 0.7%). Of note, the percentage of individuals receiving HU remained relatively consistent across all follow-up visits, ranging from 79.1% at baseline to 75.7% at the 24-month follow-up visit. The same tendency was observed regarding the use of other medications. The percentage of patients who did not receive any pharmacological treatment ranged from 10.8% to 12.3% throughout the study.
In high-risk patients, HU was the cytoreductive therapy of choice (89, 81.6%), combined or not with other modalities (phlebotomy: 29, 26.6%; ASA: 30, 27.5%; warfarin: 1, 0.9%; clopidogrel: 1, 0.9%). Four (3.7%) of the high-risk patients received ruxolitinib; another four took ASA; and one (0.9%) was on busulfan. Eleven (10.1%) patients had no pharmacological treatment, of whom 3 (2.8%) received phlebotomy (data not shown).
Of the 81 participants who had information on the number of phlebotomies performed prior to study initiation, 44 (54.3%) had a record of having undergone this procedure. Twelve patients (30.0%) had between 1 and 2 phlebotomies during the first 12 months of follow-up. In the second year, this number was reduced to 8 (25.8%) patients. A total of 4 (10.0%) and 3 (9.7%) PV patients received 3 or more phlebotomies during the first and second year of follow-up, respectively. The percentage of individuals who did not receive phlebotomy increased from 45.7% at baseline to 74.2% at 24 months. Of note that a substantial number of patients had missing data regarding phlebotomies (Table 2).
3.3. Clinical outcomes and hematological response
Over a median of 4.9 years since PV diagnosis, 9 (6.9%) patients reported a total of 10 thrombotic events (3 arterial and 7 venous) and 5 (6.0%) patients reported a total of 8 events (Table S2). This results in 1-, 2-, and 5-year probabilities of thrombo-hemorrhagic events of 5.0%, 8.0% and 17.2%, respectively, when considering data from the first 5 years after PV diagnosis (Figure 1, Table S3).
Throughout the study, clinicians reported 2 cases of progression to MF in patients whose PV was diagnosed 16.5 years and 25 months prior to baseline. AML transformation was not reported. Non-haematological toxicity was recorded in 2 patients, namely tinnitus and bradycardia (Table S4). The patient with bradycardia was on HU treatment throughout the entire study period.
Analysis of the hematological data (Table 3) revealed significant differences between the baseline and 24-month mean values for hematocrit and hemoglobin (p=0.007 and p=0.012, respectively). Specifically, the mean hematocrit percentage decreased from 45.2±6.8 at baseline to 42.2±5.2 at 24 months. For hemoglobin, the mean value decreased from 14.6±2.6 at baseline to 13.5±1.8 at 24 months.
In addition to these parameters, the data suggest that patients in this cohort experienced a slight decrease in the platelet and neutrophil counts during the 24 months of follow-up, while their white blood cell counts remained relatively stable.
3.4. Resistance to HU
The evaluation of resistance to HU was based on the modified ELN criteria [14,15], adapted to the conditions of this study. The modified ELN criteria consider resistance to occur when there is the need for phlebotomy, uncontrolled myeloproliferation, or failure to reduce splenomegaly in patients treated with 2g of HU per day for at least 3 months or the maximum tolerated dose, or the occurrence of cytopaenia at the lowest dose. In addition, according to the same criteria, intolerance to HU is recognised in case of unacceptable HU-related non-haematological toxicity. However, in this study, data on the maximum tolerated dose of HU were not recorded, and non-hematological toxicities were only reported in about half the patients. Therefore, resistance to HU was analysed cautiously in patients receiving HU for at least 9 months while using the MPN10 scale to assess symptomatic burden. HU intolerance could not be determined.
Overall, 83 patients had been treated with HU for at least 9 months. Of these, 63 patients (75.9%) met at least one ELN criterion, defining resistance to HU. At the time of study enrolment, 45 (76.3%) of the 59 patients treated with HU for ≥9 months met at least one of these criteria: 9 patients required phlebotomy, 4 had elevated platelet and leukocyte counts, 18 developed cytopaenia, and 37 had an MPN10 score ≥20 or an individual symptom score of >5. Information on splenomegaly was not available for 86% of the patients. At the 24-month follow-up, 15 (62.5%) of the 24 patients on HU for ≥9 months met the same criteria (Table 4). Among patients receiving HU for ≥9 months, 9 (15.3%) maintained resistance to HU from baseline to the end of the study period, in agreement with the adjusted ELN criteria (Table S5). At the 12-month follow-up, 6 of these patients (66.7%) remained on the initial HU dose. No HU dose-related information was available for the remaining 3 patients.
The majority of patients relied solely on HU treatment for hematocrit control at baseline, although a substantial number of individuals also received phlebotomies either in combination with HU or as a standalone approach. Specifically, among the 46 patients who had controlled hematocrit levels (<45%) at baseline, the treatment patterns were as follows: 3 patients (6.5%) received only phlebotomies before or up to the baseline; 12 patients (26.1%) underwent both phlebotomies and hydroxyurea (HU) treatment; 25 patients (54.3%) received HU treatment alone; and 6 patients (13.0%) did not receive HU or phlebotomies (Table S6).
The analysis of patients with controlled hematocrit levels at 24 months (n=20) revealed variations in treatment patterns over time, with some patients transitioning from or combining HU with phlebotomies.
The number of phlebotomies performed before and after HU initiation is shown in Table 5. Of note, only patients with at least 12 months of follow-up (and up to 24 months) were included in the analysis. Prior to the initiation of the cytoreductive therapy, only 8 patients (14.3%) had performed phlebotomies. However, following the initiation of HU treatment, there was a significant increase (p=0.005) in the number of patients requiring phlebotomies for disease control, with a total of 17 patients undergoing the procedure at least once (30.7% vs 14.3% before HU).
1Distribution of patients (n=56) in both groups (before and after HU) was compared using the Wilcoxon test for paired samples: p=0.005.
3.5. Patient-reported symptom burden
Self-evaluation of the 10 most clinically significant symptoms was conducted using the MPN10 scale (Table 6). At baseline, the mean MPN10 total score was 12.0 ± 11.6. Among the reported symptoms, fatigue (3.0 ± 2.9), itching (2.0 ± 2.8), and inactivity (1.7 ± 2.6) exhibited the highest burden. Moreover, these 3 symptoms consistently remained the most heavy throughout the study, without statistically significant alterations compared to baseline. Yet, there was a significant decrease in the total MPN10 score after 24 months of study initiation (p=0.041).
1Comparison of scores between baseline and the 24-month follow-up visit was performed considering the Wilcoxon test for paired samples. For the score of each symptom, the p-value was adjusted by the Bonferroni method: p=0.005. N/A: not applicable.
4. Discussion
This real-world study provides an extensive clinical characterization of Portuguese PV patients, enabling a better understanding of the patient demographics, risk profiles, symptomatology, treatment patterns, and clinical outcomes associated with this condition. This knowledge has the potential to inform clinical decision-making, improve patient management strategies, and facilitate the development of personalized and more effective therapeutic interventions for PV patients in the future.
The baseline characteristics of the study cohort align with previous observations in PV patients, with the majority of patients being older than 60 years and classified as high-risk based on age or thrombotic history. These factors are known to increase the risk of thrombotic events in these patients [18], underscoring the urgent need for effective treatment management strategies to mitigate these complications.
Hydroxyurea (HU) was the frontline therapy for the majority of patients at the time of study initiation, consistent with its recommendation as the first-line cytoreductive therapy for high-risk PV patients. However, the challenges associated with its inaccurate management should not be overlooked [8,12]. Resistance and intolerance to this drug can reach significant numbers, with HU resistance posing a heighthened risk of mortality and disease transformation to acute leukaemia or MF [12]. Indeed, a significant number of patients met at least one of the adjusted ELN criteria defining HU resistance, with 14% of patients maintaining HU resistance throughout the study period without discontinuing the treatment. These results are consistent with previous clinical experience indicating that a large proportion of patients (20-60%) remain on HU therapy despite lack of response or intolerance [19]. The prevalence of resistance to HU has been reported in various studies, ranging from 11% to 21% of patients [12,15,17,20]. Our study found a similar rate of 15% for patients receiving HU for ≥9 months and maintaining at least one criterion for HU resistance from baseline to the end of the study period. Unfortunately, the assessment of HU intolerance was not possible due to a lack of information on non-hematologic toxicities. Taken together, these findings highlight the lack of standard therapeutic approaches and the need to monitor treatment response and consider second-line therapies for non-responders.
Analysis of treatment patterns in the population with controlled hematocrit levels at baseline showed that while the majority of patients received HU alone, a substantial proportion also received phlebotomy, either in combination with HU or as a stand-alone approach. However, the analysis of patients with hematocrit levels <45% at 24 months revealed variations in treatment patterns over time, with some patients switching from HU to other interventions or combining HU with phlebotomy. In addition, a significant increase in the number of patients requiring phlebotomy for disease control after initiation of HU treatment was observed, further supporting the poor management of these patients in routine practice.
The thrombotic and hemorrhagic events reported in this study illustrate the ongoing risk faced by Portugese PV patients, despite treatment. The projected 5-year probability of thrombo-hemorrhagic events was 17.2%, similar to previous studies [7,17]. The fact that approximately one-sixth of the study sample was under the age of 60, and more than half was under the age of 74, underscores the importance of maintaining ongoing vigilance and implementing appropriate management strategies to prevent such complications, especially in patients with a relatively long life expectancy.
The MPN10 scale, which assesses the 10 most clinically important symptoms experienced by PV patients, was used to assess symptom burden. Fatigue, itching, and inactivity were the most burdensome symptoms reported at baseline, and their severity remained relatively unchanged throughout the study. Even though the observed total MPN10 scores were relatively lower than those reported for other cohorts (18.8 ± 15.5) [21], fatigue, itching, and inactivity were the symptoms with the highest burden, consistent with previous studies [21]. The overall decrease in the total MPN10 score at 24 months suggests a potential improvement in symptom burden, although the clinical significance of this finding should be interpreted with caution.
Furthermore, PV patients may experience HU-related non-hematological toxicity and symptoms that must be recognized and adjusted to fit the therapeutic plan. In this cohort, one patient developed tinnitus and another bradycardia. Still, only the latter was on HU treatment.
A major limitation of this study pertained to the use of secondary data. Patient information was occasionally incomplete, particularly their maximum tolerated HU dose, which was not documented in this study, and there were missing data for certain evaluated criteria. These limitations affected the assessment of predictive factors for thrombotic and hemorrhagic events and other clinical outcomes in this Portuguese cohort. Moreover, they hindered the accurate determination of the frequency of patients who developed resistance to HU, which was cautiously focused on patients who had been treated with HU for at least 9 months and based on the MPN10 symptom scale.
5. Conclusions
This real-world study provides the first clinical characterisation of Portuguese PV patients. The results show that a significant proportion of PV patients meet HU resistance criteria, with an alarming number of HU-treated patients maintaining resistance throughout the study without treatment change. The lack of standardised management of PV highlights the importance of establishing a consensus on optimal treatment strategies. This also has an impact on the quality of life of these patients, as evidenced by their symptom burden. Overall, this study underlines the importance of identifying patients with HU resistance and implementing a standardised approach to ensure optimal treatment and management of PV, ultimately improving patient clinical outcomes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, J.F., I.C., and D.B.; methodology, J.F., I.C., and D.B.; ; investigation, M.S, M.D., J.S., S.P., D.R., L.F., M.J.M.S., J.P., G.F., J.F., I.C., and D.B.; resources, I.C. and D.B.; writing—review and editing, M.S, M.D., J.S., S.P., D.R., L.F., M.J.M.S., J.P., G.F., J.F., I.C., and D.B.; project administration, I.C. and D.B.; funding acquisition, I.C. and D.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This project was partially funded by Novartis through a research collaboration between the Portuguese Oncology Nurse Association (AEOP) and Novartis.
Institutional Review Board Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by each site ethics’ commission. Prior to study inclusion, all patients gave their informed consent.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank Joana Melo and Carla Gomes (W4Research) for the writing support in the preparation of this manuscript and Adriana Belo (W4Research) for the biostatistics analysis, which the AEOP and Novartis partnership funded, according to the Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Conflicts of Interest
IC and DB are employees of Novartis Farma. Remaining authors have no relevant financial or non-financial interests to disclose.
References
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Ugo, V.; Le Couédic, J.-P.; Staerk, J.; Delhommeau, F.; Lacout, C.; Garçon, L.; Raslova, H.; Berger, R.; Bennaceur-Griscelli, A.; et al. A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature 2005, 434, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.; Wang, H.; Iqbal, S.U.; Mesa, R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk. Lymphoma 2014, 55, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Moulard, O.; Mehta, J.; Fryzek, J.; Olivares, R.; Iqbal, U.; Mesa, R.A. Epidemiology of myelofibrosis, essential thrombocythemia, and polycythemia vera in the European Union. Eur. J. Haematol. 2014, 92, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Cerquozzi, S.; Tefferi, A. Blast transformation and fibrotic progression in polycythemia vera and essential thrombocythemia: a literature review of incidence and risk factors. Blood Cancer J. 2015, 5, e366. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Barosi, G.; Birgegard, G.; Cervantes, F.; Finazzi, G.; Griesshammer, M.; Harrison, C.; Hasselbalch, H.C.; Hehlmann, R.; Hoffman, R.; et al. Philadelphia-Negative Classical Myeloproliferative Neoplasms: Critical Concepts and Management Recommendations From European LeukemiaNet. J. Clin. Oncol. 2011, 29, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Larrán, A.; Pérez-Encinas, M.; Ferrer-Marín, F.; Hernández-Boluda, J.C.; Ramírez, M.J.; Martínez-López, J.; Magro, E.; Cruz, Y.; Mata, M.I.; Aragües, P.; et al. Risk of thrombosis according to need of phlebotomies in patients with polycythemia vera treated with hydroxyurea. Haematologica 2017, 102, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Barbui, T. Polycythemia vera and essential thrombocythemia: 2021 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2020, 95, 1599–1613. [Google Scholar] [CrossRef]
- Marchioli, R.; Finazzi, G.; Specchia, G.; Cacciola, R.; Cavazzina, R.; Cilloni, D.; De Stefano, V.; Elli, E.; Iurlo, A.; Latagliata, R.; et al. Cardiovascular Events and Intensity of Treatment in Polycythemia Vera. New Engl. J. Med. 2013, 368, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Landolfi, R.; Marchioli, R.; Kutti, J.; Gisslinger, H.; Tognoni, G.; Patrono, C.; Barbui, T.; for the European Collaboration on Low-Dose Aspirin in Polycythemia Vera Investigators. Efficacy and Safety of Low-Dose Aspirin in Polycythemia Vera. N. Engl. J. Med. 2004, 350, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Marchioli, R. , et al., The CYTO-PV: A Large-Scale Trial Testing the Intensity of CYTOreductive Therapy to Prevent Cardiovascular Events in Patients with Polycythemia Vera. Thrombosis, 2011. 2011: p. 794240.
- Alvarez-Larrán, A.; Pereira, A.; Cervantes, F.; Arellano-Rodrigo, E.; Hernández-Boluda, J.-C.; Ferrer-Marín, F.; Angona, A.; Gómez, M.; Muiña, B.; Guillén, H.; et al. Assessment and prognostic value of the European LeukemiaNet criteria for clinicohematologic response, resistance, and intolerance to hydroxyurea in polycythemia vera. Blood 2012, 119, 1363–1369. [Google Scholar] [CrossRef]
- Emanuel, R.M.; Dueck, A.C.; Geyer, H.L.; Kiladjian, J.-J.; Slot, S.; Zweegman, S.; Te Boekhorst, P.A.W.; Commandeur, S.; Schouten, H.C.; Sackmann, F.; et al. Myeloproliferative Neoplasm (MPN) Symptom Assessment Form Total Symptom Score: Prospective International Assessment of an Abbreviated Symptom Burden Scoring System Among Patients With MPNs. J. Clin. Oncol. 2012, 30, 4098–4103. [Google Scholar] [CrossRef]
- Barosi, G.; Birgegard, G.; Finazzi, G.; Griesshammer, M.; Harrison, C.; Hasselbalch, H.; Kiladijan, J.; Lengfelder, E.; Mesa, R.; Mc Mullin, M.F.; et al. A unified definition of clinical resistance and intolerance to hydroxycarbamide in polycythaemia vera and primary myelofibrosis: results of a European LeukemiaNet (ELN) consensus process. Br. J. Haematol. 2010, 148, 961–963. [Google Scholar] [CrossRef] [PubMed]
- Demuynck, T.; Verhoef, G.; Delforge, M.; Vandenberghe, P.; Devos, T. Polycythemia vera and hydroxyurea resistance/intolerance: a monocentric retrospective analysis. Ann. Hematol. 2019, 98, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Scherber, R. , et al. in Haematologica. 2016.
- Alvarez-Larrán, A.; Kerguelen, A.; Hernández-Boluda, J.C.; Pérez-Encinas, M.; Ferrer-Marín, F.; Bárez, A.; Martínez-López, J.; Cuevas, B.; Mata, M.I.; García-Gutiérrez, V.; et al. Frequency and prognostic value of resistance/intolerance to hydroxycarbamide in 890 patients with polycythaemia vera. Br. J. Haematol. 2016, 172, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Finazzi, G. A prospective analysis of thrombotic events in the European collaboration study on low-dose aspirin in polycythemia (ECLAP). Pathol. Biol. 2004, 52, 285–288. [Google Scholar] [CrossRef]
- Griesshammer, M.; Gisslinger, H.; Mesa, R. Current and future treatment options for polycythemia vera. Ann. Hematol. 2015, 94, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Devos, T.; Beguin, Y.; Noens, L.; Van Eygen, K.; Zachée, P.; Mineur, P.; Knoops, L.; Doyen, C.; Theunissen, K.; Benghiat, F.S.; et al. Disease and treatment characteristics of polycythemia vera patients in Belgium: Results from a scientific survey. Eur. J. Haematol. 2018, 100, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Mesa, R.; Boccia, R.V.; Grunwald, M.R.; Oh, S.T.; Colucci, P.; Paranagama, D.; Parasuraman, S.; Stein, B.L. Patient-Reported Outcomes Data From REVEAL at the Time of Enrollment (Baseline): A Prospective Observational Study of Patients With Polycythemia Vera in the United States. Clin. Lymphoma Myeloma Leuk. 2018, 18, 590–596. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan-Meier curve for the time between PV diagnosis and the occurrence of thrombo-hemorrhagic events. Only patients diagnosed with PV within up to 5 years of the index date were included.
Figure 1.
Kaplan-Meier curve for the time between PV diagnosis and the occurrence of thrombo-hemorrhagic events. Only patients diagnosed with PV within up to 5 years of the index date were included.
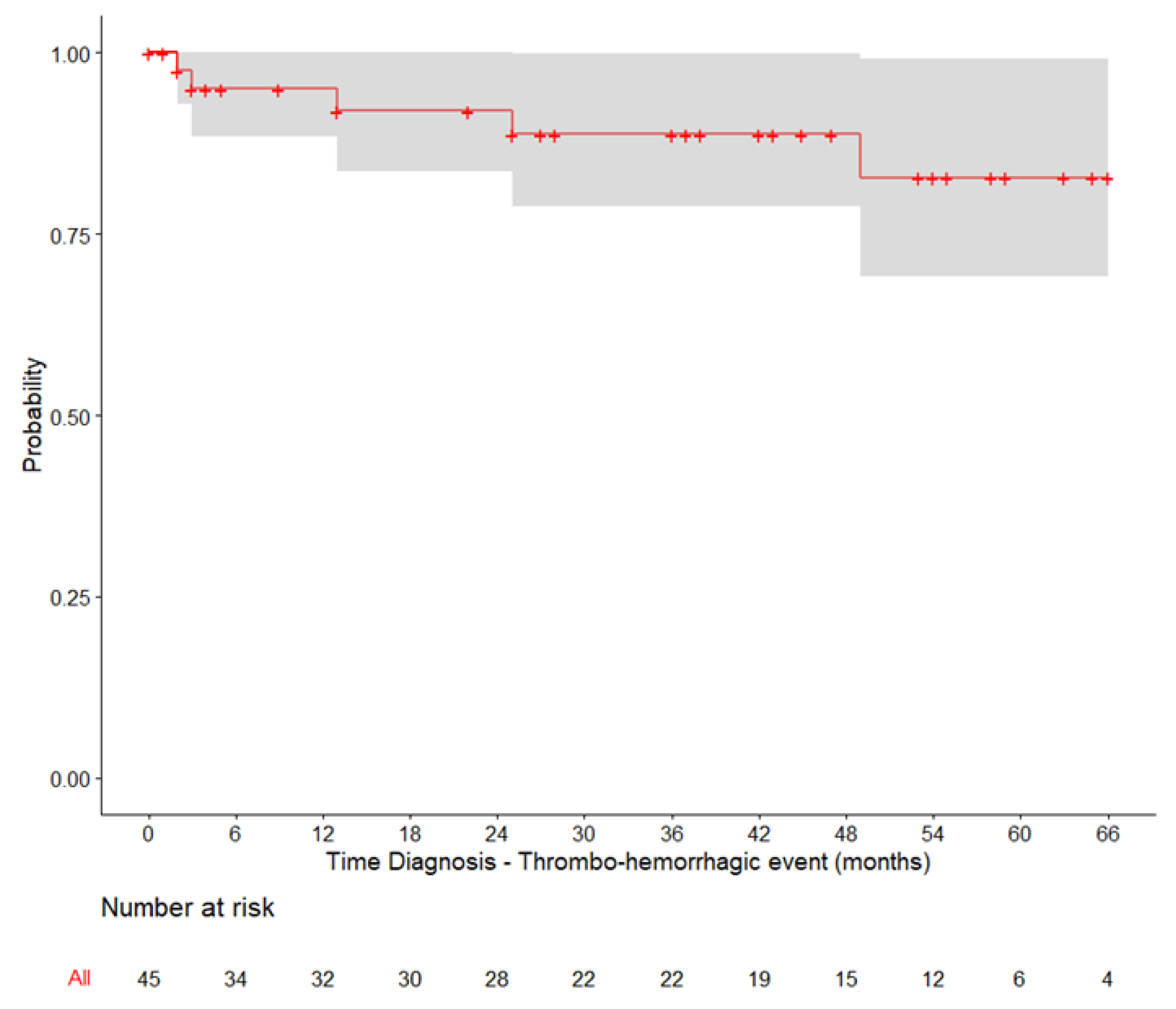

Table 1.
Characteristics of PV patients at baseline.
| Baseline characteristics | Overall (n=134) |
| Age, years | n=131 |
| 18 - 34 | 2 (1.5%) |
| 35 - 59 | 20 (15.3%) |
| 60 - 74 | 55 (42.0%) |
| ≥75 | 54 (41.2%) |
| Mean [95% CI] ± SD | 70.6 [69.0, 72.2] ± 11.7 |
| Missing | 3 (2.2%) |
| Gender | n=134 |
| Male | 63 (47.0%) |
| Female | 71 (53.0%) |
| Disease duration, years | n=122 |
| <1 year | 33 (27.0%) |
| 1 - 4 years | 40 (32.8%) |
| 5 - 9 years | 28 (23.0%) |
| 10 - 14 years | 11 (9.0%) |
| ≥15 years | 10 (8.2%) |
| Mean [95% CI] ± SD | 4.8 [4.1, 5.5] ± 5.0 |
| Missing | 12 (9.0%) |
| PV risk status | n=125 |
| Low | 21 (16.8%) |
| High | 104 (83.2%) |
| Missing | 9 (6.7%) |
| Thrombotic event history | n=78 |
| Prior thrombotic event | 5 (6.4%) |
Table 2.
Treatment profile of PV patients.
| Treatment profile | Baseline | 12 months | 24 months |
| Pharmacological treatment | n=134 | n=65 | n=37 |
| HU | 106 (79.1%) | 52 (80.0%) | 28 (75.7%) |
| [72.2%, 86.0%] | [70.3%, 89.7%] | [61.9%, 89.5%]) | |
| Alone | 66 (49.2%) | 33 (50.8%) | 18 (48.6%) |
| With acetylsalicylic acid (ASA) | 38 (28.4%) | 17 (26.2%) | 8 (21.6%) |
| With clopidogrel | 1 (0.7%) | 1 (1.5%) | 1 (2.7%) |
| With warfarin | 1 (0.7%) | 1 (1.5%) | 0 (0.0%) |
| With triflusal | 0 (0.0%) | 0 (0.0%) | 1 (2.7%) |
| With phlebotomy | 35 (26.1%) | 15 (23.1%) | 11 (29.7%) |
| Other | 13 (9.7%) | 5 (7.7%) | 4 (10.8%) |
| Without pharmacological treatment | 15 (11.2%) | 8 (12.3%) | 4 (10.8%) |
| Phlebotomy | n=81 | n=40 | n=31 |
| No | 37 (45.7%) | 24 (60.0%) | 23 (74.2%) |
| [34.8%, 56.5%] | [44.8%, 75.2%] | [58.8%, 89.6%] | |
| Yes | 44 (54.3%) | 16 (40.0%) | 8 (25.8%) |
| [43.5%, 65.1%] | [24.8%, 55.2%] | [10.4%, 41.2%] | |
| Number phlebotomies | |||
| 1-2 | 30 (37.0%) | 12 (30.0%) | 5 (16.1%) |
| [26.5%, 47.5%] | [15.8%, 44.2%] | [3.2%, 29%] | |
| ≥3 | 10 (12.3%) | 4 (10.0%) | 3 (9.7%) |
| [5.1%, 19.5%] | [0.7%, 19.3%] | [0.0%, 20.1%] | |
| Unknown | 4 (4.9%) | 0 (0.0%) | 0 (0.0%) |
| [0.2%, 9.6%] | |||
| Missing | 53 (39.6%) | 25 (38.5%) | 6 (16.2%) |
Table 3.
Hematological data of PV patients throughout the study.
| Baseline | 12 months | 24 months | |
| Haematocrit (%) | n=100 | n=44(1) | n=31(2) |
| Mean ± SD | 45.2 ± 6.8 | 43.7 ± 4.2 | 42.2 ± 5.2 |
| Median | 45.5 | 43.5 | 43.0 |
| Hemoglobin (g/dL) | n=118 | n=44(3) | n=31(4) |
| Mean ± SD | 14.6 ± 2.0 | 14.2 ± 1.5 | 13.5 ± 1.8 |
| Median | 14.7 | 14.4 | 13.6 |
| Platelets (x109/L) | n=100 | n=45(5) | n=31(6) |
| Mean ± SD | 350.2 ± 194.2 | 303.6 ± 131.5 | 325.2 ± 130.8 |
| Median | 298.0 | 260.0 | 327.0 |
| Neutrophils (x109/L) | n=29 | n=16(7) | n=13(8) |
| Mean ± SD | 6.69 ± 4.14 | 6.61 ± 5.34 | 5.37 ± 3.31 |
| Median | 5.2 | 4.9 | 3.7 |
| Leukocytes (x109/L) | n=72 | n=34(9) | n=30(10) |
| Mean ± SD | 8.8 ± 4.2 | 9.2 ± 5.2 | 9.2 ± 5.4 |
| Median | 7.5 | 7.0 | 7.4 |
Multiple comparisons of hematological data between baseline and each follow-up visit were performed considering Wilcoxon test for paired samples and a significance level adjusted by the Bonferroni method: 0.050/2=0.025: (1)p=0.056; (2)p=0.007; (3)p=0.202; (4)p=0.012; (5)p=0.492; (6)p=0.493; (7)p=0.847; (8)p=0.108; (9)p=0.424; (10)p=0.814.
Table 4.
Number of PV patients on HU for ≥9 months meeting at least one of the adjusted ELN criteria.
Table 4.
Number of PV patients on HU for ≥9 months meeting at least one of the adjusted ELN criteria.
| Number of patients | Baseline (n=134) |
12 months (n=65) |
24 months (n=37) |
| HU | |||
| No | 28 (20.9%) | 13 (20.0%) | 9 (24.3%) |
| [14.9%, 28.5%] | [12.1%, 31.3%] | [13.4%, 40.1%] | |
| Yes | 106 (79.1%) | 52 (80.0%) | 28 (75.7%) |
| [71.5%, 85.1%) | [68.7%, 87.9%] | [13.4%, 40,1%] | |
| On HU for <9 months or no info about HU date | 47 (44.3%) [35.2%, 53.8%] |
3 (5.8%) [2.0%, 15.6%] |
4 (14.3%) [5.7%, 31.5%] |
| On HU for ≥9 months | 59 (55.7%) | 49 (94.2%) | 24 (85.7%) |
| [46.2%, 64.8%] | [84.4%, 98.0%] | [68.5%, 94.3%] | |
| Meeting at least 1 of the adjusted ELN criteria | 45 (76.3%) [65.4%, 87.2%] |
29 (59.2%) [45.4%, 73.0%] |
15 (62.5%) [43.1%, 81.9%] |
| Meeting no adjusted ELN criteria | 5 (8.5%) [1.4%, 15.6%] |
12 (24.5%) [12.4%, 36.5%] |
0 (0.0%) |
| No information available | 9 (15.3%) [6.1%, 24.5%] |
8 (16.3%) [6.0%, 26.6%] |
9 (37.5%) [18.1%, 56.9%] |
Table 5.
Number of patients who performed phlebotomies before and after starting HU.
| Number of phlebotomies1 | Before HU | After HU |
| 0 | 48 (85.7%) | 39 (69.6%) |
| 1 | 7 (12.5%) | 9 (16.1%) |
| 2 | 0 (0.0%) | 2 (3.6%) |
| 3 | 1 (1.8%) | 2 (3.6%) |
| 4 | 0 (0.0%) | 2 (3.6%) |
| 9 | 0 (0.0%) | 1 (1.8%) |
| 17 | 0 (0.0%) | 1 (1.8%) |
Table 6.
Self-assessment of the most clinically significant symptoms by PV patients.
| Symptoms (Mean ± SD) | Baseline (n=123) |
24 months (n=29) |
p-value1 |
| Fatigue | 3.0 ± 2.9 | 2.0 ± 2.5 | 0.065 |
| Early satiety | 0.8 ± 1.9 | 0.4 ± 0.9 | 0.125 |
| Abdominal discomfort | 0.8 ± 1.9 | 0.9 ± 2.0 | 0.354 |
| Inactivity | 1.7 ± 2.6 | 2.0 ± 2.6 | 0.809 |
| Concentration problems | 1.1 ± 2.4 | 1.1 ± 1.8 | 0.844 |
| Night sweats | 1.0 ± 2.0 | 0.4 ± 1.0 | 0.195 |
| Itching | 2.0 ± 2.8 | 1.7 ± 1.9 | 0.010 |
| Bone pain | 1.2 ± 2.2 | 1.4 ± 2.3 | 0.203 |
| Fever (≥37.8°C) | 0.0 ± 0.1 | 0.0 ± 0.0 | N/A |
| Weight loss | 0.5 ± 1.6 | 0.3 ± 1.0 | 0.182 |
| MPN10 score | 12.0 ± 11.6 | 10.3 ± 9.1 | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



