
Submitted:
28 May 2023
Posted:
31 May 2023
You are already at the latest version
Abstract
Considering the relevance of the pathogenesis research of different liver diseases, in our study we investigated the possible activity of IL-23/IL-17 axis on the im-munohepatotoxicity of two etiologically different CLD. A total of patients with CHC infection, 19 with NASH and 20 healthy controls (CG) were recruited. After histological verification from liver tissue obtain by liver biopsy, patients with CHC were divided into two groups: CHC-NSF (F0/F1/F2)-non-significant fibrosis, 20 patients, and CHC-SF (F3/F4)-significant fibrosis/cirrhosis, 16 patients. All anthropometric, biochemical, immunological cytokines (IL-6, IL-10, IL-17 and IL-23) tests were performed accordance to standard procedure. The plasma levels of IL-6, Il-17A and IL-23 were significantly higher in CHC-SF and NASH in compared with CG. Also, plasma levels of IL-23/IL-17A were significantly higher in NASH in compared to CHC-SF. In CHC-SF we had significantly lowest IL-10 level in compared with all three groups. Liver tissue levels of IL-17A and IL-23 in CHC-NSF were significantly lower in compared with NASH. IN CHC-SF and NASH, IL17-A and IL-23 in liver tissue were significantly higher in compare to plasma levels. In conclusan, proinflammatory response of IL-23/17A axis is dominant in plasma and liver tissue in CHC with higher levels of liver fibrosis and in NASH patients.
Keywords:
chronic hepatitis C
; nonalcoholic steatohepatitis
; IL-23/IL-17 axis
; immunohepatotoxicity
1. Introduction
The most common chronic liver diseases (CLD) nowadays have been attributed to nonalcoholic fatty liver disease (NAFLD) (59%), followed by hepatitis B virus (HBV) (29%), hepatitis C virus (HCV) (9%) and alcoholic liver disease (ALD) (2%). Other liver diseases account for 1%, including primary biliary cholangitis, primary sclerosing cholangitis, alpha-1-antitrypsin deficiency, Wilson’s disease and autoimmune hepatitis. Historically, viral hepatitis has been the leading etiology for CLD, but improved prevention strategies in the case of hepatitis B and treatment in the case of hepatitis C, have led to changing CLD trends [1] . The absolute number of CLD cases (inclusive of any stage of disease severity) is estimated at 1.5 billion worldwide [2] . CLD caused 1.32 million deaths in 2017, approximately two-thirds among men and one-third among women [1] . In 2019 CLD and cirrhosis was the ninth leading cause for males (1.9% of deaths), but it was not in the top 10 for females. For those aged 25–44, CLD and cirrhosis were among the leading causes of mortality [3]. The role of immune system in CLD has been recognized a decades ago [4,5], but not all immunological mechanisms of liver damage, which could be potential therapeutic targets, have been clarified to date. Interleukin-23 (IL-23) and its downstream factor IL-17 are described as the key cytokines involved in immunopathogenesis in CLD [6] . Its role is very well known in other chronic diseases, sach as rheumatic diseases, inflammatory bowel diseases, chronic skin diseases, chronic lymphocitic leukemia [7,8,9,10] . In chronic inflammation, antigen-stimulated dendritic cells and macrophages produce IL-23, which promotes the development of Th17/ThIL-17 cells. Th17/ThIL-17 cells produce IL-17, which enhances T cell priming and triggers potent inflammatory responses by inducing the production of a variety of inflammatory mediators. IL-23 also acts on dendritic cells and macrophages in an autocrine/paracrine manner to stimulate the generation of proinflammatory cytokines, such as IL-1, IL-6, IL-17 and TNF-α. IL-12–stimulated Th1 cells produce IFN-γ and suppress the differentiation of Th17/ThIL-17 cells. Th1 cells may play an immunoregulatory, protective, role in the development of chronic inflammation [11,12] . Numerous studies have described the influence of the IL-23/17 axis on the development of liver fibrosis with heterogeneous results. [13,14] . The results point not only to pathophysiology but also to potential immunotherapeutic options [15,16] . The most contradictory results are related to chronic hepatitis C (CHC) and NASH, so the aim of this study was to describe if there are differences in the effect of this axis in two chronic liver diseases with different etiopathogenesis – CHC and NASH.
2. Results
All demographic, anthropometric and biochemical characteristics are showed in Table1. Some values of metabolic syndrome (MS) parameters (body mass index (BMI), body mass (BM), cholesterol, low-density lipoprotein cholesterol (LDL) and triglycerides) are significantly higher in NASH in comparison with all the other groups, as well as high-density lipoprotein cholesterol (HDL) levels were significantly lower in all of the liver diseases groups compared to control group (CG). In chronic hepatitis C group with significant fibrosis (CHC-SF) albumins and platelets (PLT) levels were statistical lower in comparison with chronic hepatitis C group with non significant fibrosis (CHC-NSF), NASH and CG. Also, in CHC-SF group alpha fetoprotein (AFP) was statistical higher compared to the other three groups. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were significantly higher in all liver diseases groups in comparison with CG, as well as in CHC-SF group with CHC-NSF and NAFLD.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
The levels of IL-6 in the plasma was not significantly different between the compared groups (p=0.075), but significant difference was noted in liver tissue (p=0.043). CG had the lowest measured plasma levels (median 3.91 pg/ml), with 8 out of 20 samples having levels below LOD. Median levels of plasma IL-6 were 12.60; 7.30 and 10.11 pg/ml and median liver tissue IL-6 were 49.35, 23.06, 43.63 pg/ml for NASH, CHC-NSF and CHC-SF group, respectively. Post-hock analysis showed that CHC-SF and NASH had significantly higher levels in comparison with CG. The liver tissue levels were significantly higher in comparison than plasma IL-6 levels in CHC-SF and NASH groups (Figure 1).
Median concentration of IL-10 in the plasma showed a clear decreasing trend from healthy controls to NASH, as well as from hepatitis without significant fibrosis to liver cirrhosis. The differences between the groups were statistically significant (p<0.0001), while the post-test revealed the difference between CG and both CHC-NSF and CHC-SF groups, as well as between NASH and both CHC-NSF and CHC-SF groups. Also, levels in CHC-SF were statistically lower compared to CHC-NSF group. The levels of IL-10 in the liver tissue was not significantly different between the compared groups (p=0.162), but post-test showed significantly higher median value in CHC-NSF compared to NASH (p<0.05). Median plasma levels were: 162.6, 137.5, 79.44, and 59.39 pg/ml for CG, NAFLD, CHC-NSF and CHC-SF groups, respectively. Also, median tissue levels were: 61.96, 43.26, and 46.85 pg/ml for NAFLD, CHC-NSF and CHC-SF groups, respectively. The liver tissue levels were significantly lower compared to plasma IL-10 levels in CHC-NSF and NASH groups (Figure 2).
The plasma concentrations of IL-17A were different between the groups (p=0.000). Median plasma level in CHC-SF group was 17.79 pg/ml, while median concentration in NASH group was 26.56 pg/ml. Majority of patients from the CHC-NSF as well as CG, had measured levels below the lower limit of detection and were thus median serum levels were considered as 0. Plasma levels of IL-17A in the group of patients with liver cirrhosis and CHC-NSF were lower compared to the group of patients with NASH (p=0.0035, p=0.000, respectively). In comparison with CG and CHC-NSF, plasma levels of IL-17A were higher in CHC-SF and NASH (p=0.000, p=0.000, p=0.000, respectively) (Figure 3). Median tissue levels were: 49.35, 23.06, 43.63, 0 pg/ml for NASH, CHC-NSF, CHC-SF and CG group, respectively. The differences between the groups were statistically significant (p=0.017), while the post-test revealed the differences between CHC-NSF and CHC-SF, as well as CHC-NSF and NASH groups (p= 0.050, for all). The liver tissue levels were significantly higher compared to plasma IL-17A levels in CHC-SF and NASH groups (Figure 3).
Plasma concentrations of IL-23 were different between the groups (p=0.0105) (Figure 4). Control samples had the lowest median value (66.15 pg/ml), median for CHC-SF group was 88.72 pg/ml, for CHC-NSF group 92.64 pg/ml, while patients with NASH had the highest plasma concentrations of IL-23 - 131.80 pg/ml. In addition, the difference in levels in CG and all three groups (CHC-NSF, CHC-SF, NASH), as well as NASH and CHC-SF were significant (p<0.05). The levels of IL-23 in the liver tissue was not significantly different between the compared groups (p=0.093), but there was post-test significant difference in liver tissue in CHC-NSF and NASH (p=0.042). . The liver tissue levels of IL-23 were significantly higher in comparison with plasma in CHC-SF and NASH groups. Median liver tissue for NASH group was 49.35 pg/ml, for CHC-NSF 23.06 pg/ml, and for CHC-SF was 43.63 pg/ml.
3. Discussion
Considering the relevance of the pathogenesis research of different liver diseases, in our study we investigated the possible activity of IL-23/IL-17 axis on the immunohepatotoxicity of two etiologically different CLD. NAFLD, recently renamed as metabolic (dysfunction)-associated fatty liver disease (MAFLD) is a complex, multifactorial disease that includes one or more components of the MS like systemic hypertension, dyslipidaemia, visceral obesity, insulin resistance, or diabetes [17,18] . Disease progresses from non-alcoholic fatty liver (NAFL) characterized by macrovesicular hepatic steatosis that may be accompanied by mild inflammation to NASH which is additionally characterized by the presence of inflammation and cellular injury (ballooning), with or without fibrosis. The last stage of disease is cirrhosis, which is characterized by bands of fibrous septa leading to the formation of cirrhotic nodules, and further progression leads to irreversible damage, decompensation of liver function and hepatocellular carcinoma. The prevalence of NASH has risen rapidly worldwide. In the last three decades these rates have increased from 25% to 38%, and is likely to become the main indication for liver transplantation in the near future [19,20,21,22] .
On the other hand, CHC is caused by HCV infection. The acute infection with HCV frequently does not resolve spontaneously. Approximately 80% of the infected individuals become chronic carriers, of which 10%-20% of patients will develop liver cirrhosis and 1%-5% will develop hepatocellular carcinoma (HCC) within 20-30 years. [23].
Both of these liver diseases, as one of the first laboratory abnormality, show elevated levels of ALT and AST as the indicators of liver damage. NASH determines asymptomatic elevation of ALT and AST levels in up to 90% of cases, once other liver disease causes are excluded [24]. Numerous of study have showed that in CHC patient with different stages of disease, serum levels of ALT and AST are elevated. [25,26] . In our study, AST and ALT levels were significantly higher in all liver diseases groups compared with CG, and statistical higher values in CHC-SF group compared with CHC-NSF and NASH group which is expected because of the higher levels of liver fibrosis and necrosis of hepatocytes in this group (F3/F4 in CHC-SF compared with F0/F1/F2 in CHC-NSF and NASH groups). Some values of MS parameters such as BM, BMI, cholesterol, LDL and triglycerides are significantly higher in NASH compared with all the other groups, as well as HDL levels were significantly lower in all of the liver diseases groups compared with CG. These results are expected and in correlation with previous studies. [27,28] . Patients from CHC-SF group have showed statistical lower levels of albumins and PLT compared with CHC-NSF, NASH and CG, which is an indicator of the weakened synthetic function of the liver in the advanced stage of the disease. Also this group of patients have showed statistical higher levels of AFP in absents of HCC, compared with other liver diseases groups, which is all in correlation with the other authors [29,30,31,32]. All the other biochemical parameters didn’t show statistical significance.
From the immunopathogenic aspects, in the literature there are controversial results about both of these chronic liver diseases. In liver diseases, before cirrhosis is established, multiple pathways of fibrogenesis are activated as a result of continuous interaction between pathogen-related factors, the host genetic such as certain HLA haplotypes and cytokines gene polymorphisms, liver resident cells and the immune system. [33,34,35,36]. In our focus was IL23/IL17 axis, which is one of the important proinflammatory response on chronic stimulation. The role of these axis in the pathogenesis of liver disease has been extensively evaluated in multiple mouse models of liver injury. Yan et al. have showed that genetic deletion of IL-17RA or IL-17A, or antibody-mediated neutralization of IL-17A can protect from induced hepatitis, as well as the increased levels of IL-17 and IL/6 parallel with the severity of liver injury reflected by ALT and histological assay [15]. In our study, CHC-SF patients as well as NASH patients, had significant higher plasma levels of IL-17A and IL-23 compared to CHC-NSF and CG, as well as CHC-NSF patients had statistically higher levels of IL23 compared with CG, but there was no difference in IL17A level between these two groups. In our study, IL-17A plasma levels in CHC-NSF and CG were below level of detection, so in these two groups we used 0 pg/ml for mediana. Previous study which investigated systemic sclerosis, also in CG and lower severity diseases group had below level of IL-17A detection and also used 0 pg/ml as mediana for these groups. [37]. Previous studies have showed that patient with CHC have increased levels of IL17A and IL23 compared to healthy group, but these studies did not include the degree of liver fibrosis in the analysis [38]. Also, recent studies have showed that levels of these cytokines are increased in NASH patients compared with healthy group [39,40] which is all in correlation with our results. Statistical higher levels of IL-17A and IL-23 were detected in NASH group compared to CHC-SF group, regardless of the higher level of fibrosis in CHC-SF, which is one of the proof that NASH is a reflection of the systemic inflammatory response with inflammation as one of the main pathogenic factors.
Plasma levels of IL-6 were statistically higher in CHC-SF and NASH group compared with CG, whereas CHC-NSF have not showed statistical significance with any of the other groups. Some of the previous studies have showed that the serum levels of proinflammatory cytokines such as IL-6 and IL-17, are statistically higher in CHC patient with sever liver fibrosis (F3/F4) [41], as well as one of the previous study has showed that in NASH patients levels of IL-6 is increased compared with healthy group [42], which is both confirmed by our results. In our study we have not found statistical differences of IL-6 and IL-23 plasma levels between our two groups with CHC, but levels of IL-17A was statistically higher in CHC-SF than in CHC-NSF group. The importance of increased levels of IL-17 in the different stages of CHC was previously recognized [43,44], and seems to play an important role even in the progression of CHC to HCC [45].
The only anti-inflammatory cytokine in our study, IL-10, was statistically higher in CG in compared with both of the CHC groups, whereas the level is higher in CHC-NSF compared with CHC-SF group. One of the previous study has showed decreased levels of IL-10 in healthy group compared with chronic hepatitis group [46] which is not in correlation with our results. On the other hand, Dorcas et al. have showed that twenty-five percent (41/163) of the anti-HCV positive participants had recovered from HCV and had significantly higher concentration of IL-10 compared to those with active HCV infection [47]. Our results can be explained by an increased anti-inflammatory response in healthy controls and CHC without significant fibrosis, because it is obvious that in advanced fibrosis and cirrhosis, the dominant component of the immune response becomes more proinflammatory. In NASH group levels of IL-10 were statistically higher compared with both groups of CHC, but there was no difference between NASH and CG in our study. One of the previous studies on rats has showed higher serum levels of IL-10 in NASH-induced group compared with control group [48], but Vonghia el al. [27] have showed there is no statistical difference in serum IL-10 levels in NASH and CG which is in correlation with our study.
We have measured and the liver tissue levels of all of these cytokines in CLD groups, where we have found statistically higher tissue levels of IL-6 and IL-17A in CHC-SF compared with CHC-NSF group. As we previous showed, plasma levels of IL-17A were statistically higher in CHC-SF compared with CHC-NSF group, whereas the levels of IL-6 have not showed differences between these two group. Aboushousha et al. demonstrated a positive correlation between IL-17 liver tissue expression with marked grades of hepatitis activity and high scores of liver fibrosis compared to lower ones [49]. Also Tan et al. reported that intrahepatic IL-17 expression was positively correlated with serum indices of hepatic fibrosis [50] . Gomes et al. suggested that IL-17 in CHC may initiate steatohepatitis progressing to HCC [51]. All of these results are in correlation with the results of our study, so we can conclude that IL-17A contribute to chronic hepatitis-induced liver fibrosis.
We have found statistically lower tissue levels of IL-6, IL-17A, IL-23 and IL-10 in CHC-NSF compared with NASH group, despite the same level of fibrosis into these two groups (F0/F1/F2). Between these two groups we have not found differences of plasma IL-6 and IL-23 levels. In the literature we have not found comparation between these groups, but we can conclude that local liver immunopathogenetic response in NASH patient leads to stronger local proinflammation and probably faster liver damage with consequently cirrhosis, compared with CHC patients.
We have analyzed difference between plasma and liver tissue cytokines levels in each of the liver diseases groups. In CHC-NSF there is no significant difference between plasma and liver tissue levels of IL-6, IL-17A and IL-23, whereas tissue level of IL-10 is lower in compared to plasma level. On the other hand, in CHC-SF group as well as in NASH group, there were increased liver tissue levels of IL-6, IL-17A and IL-23 compared with plasma levels, which is the sign of the higher local immunology than systemic response in these CLD. Previous studies have showed that the liver IL-6 expression is correlated positively with the severity of inflammation and the degree of fibrosis observed in NASH patients, with the fact that saturated FFA have been demonstrated to induce IL-6 production by hepatocytes in vitro [52] . Beihui et al. have demonstrated that the levels of Th17 cell-related cytokines [IL-6, IL-17 and IL-23) in serum and in liver tissue were increased in mice NASH-induced disease compared with healthy group, but they have not analyzed differences between serum and liver tissue levels. [53]. In CHC patient recent studies have described increased proportions of both, circulating and liver-infiltrating Th17 cells compared to healthy individuals, and both measures of Th17 cells were correlated with severity of liver inflammation [54]. Macek Jilkova et al. in their study have concluded that in chronic hepatitis the number of IL-17(+) neutrophils in fibrotic septa and portal areas is strongly correlated with the stages of fibrosis, contributing significantly to total IL-17 production in liver tissue [55].
4. Materials and Methods
4.1. Subjects
A total of 75 subjects were included in this study. 36 patients with CHC infection and 19 patients with NASH were recruited from the Clinic for infectious and tropical diseases, University Clinical Center of Serbia (UCCS) from October 2018 to December 2019. Diagnosis for CHC patients was made using the European Association for the Study of the Liver (EASL) Clinical Practice Guidelines: Management of hepatitis C virus infection [56], and included anti-HCV antibodies during at least 6 months with positive real-time polymerase chain reaction (PCR) assays for quantifying HCV RNA. After histological verification from liver tissue obtain by liver biopsy, patients with CHC were divided into two groups – group with non-significant fibrosis- CHC-NSF (F0/F1/F2) with 20 patients, and the group with significant fibrosis/cirrhosis- CHC-SF (F3/F4) with 16 patients.
Diagnosis of NASH was made using EASL Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease [57]. After histological verification from liver tissue obtain by liver biopsy in NASH group were included 19 patients. 20 age and sex-matched healthy donors were used as controls. Peripheral blood samples were collected from all healthy controls, patients with CHC and NASH, while fine needle liver biopsy was done in patients with CHC and NASH. Participants with the following conditions were excluded:
- pregnancy
- presence of decompensated cirrhosis;
- co-infection with human immunodeficiency virus (HIV) and co-infection with hepatitis A, B, or D virus for CHC group of patients; infection with HIV, hepatitis A, B, C or D for NASH and control group of patients;
- other chronic or acute liver disease (autoimmune/toxic);
- presence of any of an immunocompromised state
- patients with HCC.
Written informed consent was obtained from all of the patients. The study protocol was approved by the ethics committees of Clinic for Infectious and Tropical Diseases, University Clinical Center of Serbia. Our research was subject to ethical standards that promote and ensure respect for all human subjects and protect their health and rights by the Declaration of Helsinki.
4.2. Pathohistological analysis of liver tissue
Using Menghini needles, liver biopsies were done in the Clinic for Infectious and Tropical Diseases, after that processed by the Institute of Pathology at University of Belgrade. Liver biopsy specimens are fixed in formalin to form cross-links and prevent degradation. The METAVIR score was used to classify the liver fibrosis in CHC patients: F0- No fibrosis; F1- Portal fibrosis without septa; F2- Portal fibrosis with few septa; F3- Numerous septa without cirrhosis; F4- Cirrhosis [58]. In NAFLD patients, we used American Association for the Study of Liver Diseases (AASLD) scoring system [59]:
- Steatosis was graded as follows: <5% of liver parenchyma- 0; 5–33%- 1; >33–66%- 2; >66%- 3;
- Fibrosis was staged: none- 0; perisinusoidal or periportal- 1; perisinusoidal and portal/periportal- 2; bridging fibrosis- 3; cirrhosis- 4;
- Inflammation: lobular, portal (0-3);
- Hepatocellular ballooning degenaration (0-2)
4.3. Detection of HCV Antibody, Viral Load and Genotypes of HCV
Virological analyses were done in Virology Laboratory of Clinic for Infectious and Tropical diseases. Anti-HCV antibodies were detected by ELISA test (Roche, NJ, USA), HCV genomic RNA test (HCV-RNA) was performed in the Amplicor RT-PCR (Roche, NJ, USA), that presents a sensitivity of 50 IU/mL. Samples with detectable HCV-RNA were further genotyped throughout in-house RT-nested PCR and RFLP analysis and viral load determined by RT-PCR (Amplicor HCV Monitor, Roche, NJ, USA) with data expressed as IU/mL.
4.4. Biochemical Assays
Biochemical analyses (Erythrocytes (cells/ml), Hemoglobin (g/L), Leucocytes (cells/ml), Thrombocytes (cells/ml), Glucose (mmol/l), Uric acide (µmol/l), Creatinine (µmol/l), Total cholesterol (mmol/l), Triglycerides (mmol/l), Total proteins (g/l), Albumin (g/l), Total bilirubin (mg/dl), Direct bilirubin (mg/dl), Fibrinogen (mg/dl), Aspartate aminotransferase (U/l), Alanine aminotransferase (U/l), γ-glutamyl transpeptidase (U/l); Alkaline phosphatase (U/l); Alpha fetoprotein (ng/ml); Thyroid-stimulating hormone (microU/ml); Low-density lipoprotein cholesterol (mmol/l); High-density lipoprotein cholesterol (mmol/l); INR indicates international normalized ratio; C-reactive protein (mg/dl)) were observed in Biochemical Laboratory of Clinic for Infectious and Tropical diseases by standard methodes.
4.5. Measurement of Plasma and Tissue Cytokines (IL-6, IL-10, IL-17A and IL-23)
Previously collected plasma from CG, NASH, CHC-NSF and CHC-SF was used for the measurement of IL-6, IL-10, IL-17 and IL-23 using Human ELISA kits from Elabscience (#E-EL-H0102, #E-EL-H0103, # E-EL-H0105, # E-EL-H0107, respectively). The same cytokines were measured in liver biopsy tissues in NASH, CHC-NSF and CHC-SF. Upon liver biopsy the tissues were weighted and snap frozen. Each sample was mechanically homogenized in lysis buffer for the extraction of proteins (150 mM NaCl, 25 mM Tris-HCl pH 7.6, 1% IGEPAL, 0.1% SDS, 1% sodium deoxycholate, 1 mM EDTA), through repeated freeze-thaw cycles. The samples were centrifuged at 14 000 g at 4 C for 15 minutes and supernatants used for ELISA. The assays were performed according to manufacturers' instructions (Elabscience). In short, ELISA plates are pre-coated with specific antibody biotinylated antibody for specific cytokine is used for detection, and avidin-horseradish peroxidase conjugate is used to convert the substrate color into blue. The enzyme-substrate reaction is terminated by the addition of stop solution. The intensity of the developed blue color is directly proportional to the concentration of measured cytokine. The absorbance (optical density, O.D.) was measured at wavelength of 450 nm on an automated plate reader (Tecan, Dorset, UK). The concentrations of the cytokines were calculated by comparing O.D. values of samples with standards using four-parameter logistic curve in GraphPad Prism. The results for sera are expressed as pg/ml while the results for tissues are expressed as pg/ml/mg of wet tissue weight. Standard curves and lower level of detection for each measured parameter can be found in supplementary material. All of these measurement was done in Biochemical Institute, Faculty of Medicine, University of Belgrade.
4.6. Anthropometric measurements
BM was measurement under standard procedure on Tanita body analyzer (In body 970, South Korea). SECA – 217 stadimeter was used for BH (Hamburg, Germany). BMI was calculated as BM in kg/(BH in m)2.
4.7. Statistical Analysis
The data obtained are presented as mean (± S.E.M.) or median (interquartile range). Shapiro-Wilk test was used for an assessment of the normality of continuous data. The differences between the groups were assessed using ANOVA parametric test for multiple group comparison with post-hock Bonferroni for all parameters with normal continuous data. For nonparametric data, the differences between the groups were assessed using Kruskal-Wallis nonparametric test for multiple group comparison with post-hock Mann-Whitney. p values are reported as Gaussian approximation.
5. Conclusions
In our study, anthropometric and biochemical characteristics were all in correlation with etiology as well as the stage of liver disease. Proinflammatory response is dominant in plasma and liver tissue in CHC with higher levels of liver fibrosis and in NASH patients. In NASH patients there are increased plasma levels of proinflammatory cytokines compared to CHC with same stage of liver fibrosis as well as CHC with significant fibrosis and cirrhosis, which could be confirmation of systemic multifactorial inflammation in NASH. On the other hand, in this group of patients as well as in CHC with significant fibrosis and cirrhosis, local liver inflammation is increased compared to systemic proinflammatory response. We can conclude that proinflammation in CLD such as CHC and NASH, is one of important factors that lead in progression of disease and can be potential therapeutic option which will reduce the need for liver transplantation and mortality.
Author Contributions
A.V., M.Dj., and I.M. Writing—original draft preparation: A.V., M.Dj., and I.M. Immunology measurements: A.I. and S.M.D. Writing—review and final editing: A.V., M.Dj., and I.M. Collection and transport of samples: J.J. and M.M. Funding acquisition and critical reading: M.Dj. and I.M. initiated and supervised the whole work.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study, which is approved by Ethical committee of Faculty of Medicine University of Belgrade.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cheemerla, S.; Balakrishnan, M. Global Epidemiology of Chronic Liver Disease. Clin. Liver Dis. 2021, 17, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clin. Gastroenterol. Hepatol. 2019, 18, 2650–2666. [Google Scholar] [CrossRef] [PubMed]
- CDC National Vital Statistics Reports, July, 2021. https://www.cdc.gov/nchs/nvss/leading-causes-of-death.htm.
- Sherlock, S. The immunology of liver disease. Am. J. Med. 1970, 49, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Vierling, J.; Gershwin, M.E.; Milich, D.; Chisari, F.V.; Hoofnagle, J.H. Immunology and the liver. Hepatology 1991, 13, 977–994. [Google Scholar] [CrossRef] [PubMed]
- Meng, P.; Zhao, S.; Niu, X.; Fu, N.; Su, S.; Wang, R.; Zhang, Y.; Qiao, L.; Nan, Y. Involvement of the Interleukin-23/Interleukin-17 Axis in Chronic Hepatitis C Virus Infection and Its Treatment Responses. Int. J. Mol. Sci. 2016, 17, 1070. [Google Scholar] [CrossRef]
- Li, H.; Tsokos, G.C. IL-23/IL-17 Axis in Inflammatory Rheumatic Diseases. Clin. Rev. Allergy Immunol. 2020, 60, 31–45. [Google Scholar] [CrossRef]
- Cătană, C.-S.; Neagoe, I.B.; Cozma, V.; Magdaş, C.; Tăbăran, F.; Dumitraşcu, D.L. Contribution of the IL-17/IL-23 axis to the pathogenesis of inflammatory bowel disease. World J. Gastroenterol. 2015, 21, 5823–5830. [Google Scholar] [CrossRef]
- Menter, A.; Krueger, G.G.; Paek, S.Y.; Kivelevitch, D.; Adamopoulos, I.E.; Langley, R.G. Interleukin-17 and Interleukin-23: A Narrative Review of Mechanisms of Action in Psoriasis and Associated Comorbidities. Dermatol. Ther. 2021, 11, 385–400. [Google Scholar] [CrossRef]
- Bankir, M.; Acik, D.Y. IL-17 and IL-23 levels in patients with early-stage chronic lymphocytic leukemia. North. Clin. Istanb. 2020, 8, 24–30. [Google Scholar] [CrossRef]
- Kolls, J.K.; Lindén, A. Interleukin-17 Family Members and Inflammation. Immunity 2004, 21, 467–476. [Google Scholar] [CrossRef]
- Iwakura, Y.; Ishigame, H. The IL-23/IL-17 axis in inflammation. J. Clin. Investig. 2006, 116, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Meng, P.; Zhao, S.; Niu, X.; Fu, N.; Su, S.; Wang, R.; Zhang, Y.; Qiao, L.; Nan, Y. Involvement of the Interleukin-23/Interleukin-17 Axis in Chronic Hepatitis C Virus Infection and Its Treatment Responses. Int. J. Mol. Sci. 2016, 17, 1070. [Google Scholar] [CrossRef] [PubMed]
- Heredia, J.E.; Sorenson, C.; Flanagan, S.; Nunez, V.; Jones, C.; Martzall, A.; Leong, L.; Martinez, A.P.; Scherl, A.; Brightbill, H.D.; et al. IL-23 signaling is not an important driver of liver inflammation and fibrosis in murine non-alcoholic steatohepatitis models. PLOS ONE 2022, 17, e0274582. [Google Scholar] [CrossRef]
- Yan, S.; Wang, L.; Liu, N.; Wang, Y.; Chu, Y. Critical role of interleukin-17/interleukin-17 receptor axis in mediating Con A-induced hepatitis. Immunol. Cell Biol. 2011, 90, 421–428. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Hwang, S.; Ahmed, Y.A.; Feng, D.; Li, N.; Ribeiro, M.; Lafdil, F.; Kisseleva, T.; Szabo, G.; Gao, B. Immunopathobiology and therapeutic targets related to cytokines in liver diseases. Cell. Mol. Immunol. 2020, 18, 18–37. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; on behalf of theInternational Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef]
- Dixon, J.B.; Bhathal, P.S.; O’Brien, P.E. Nonalcoholic Fatty Liver Disease: Predictors of Nonalcoholic Steatohepatitis and Liver Fibrosis in the Severely Obese. Gastroenterology 2001, 121, 91–100. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- Kountouras, J. Innate immunity and nonalcoholic fatty liver disease. Ann. Gastroenterol. 2023, 36, 244–256. [Google Scholar] [CrossRef]
- Yuan, L.; Hanlon, C.L.; Terrault, N.; Alqahtani, S.; Tamim, H.; Lai, M.; Saberi, B. Portrait of Regional Trends in Liver Transplantation for Nonalcoholic Steatohepatitis in the United States. Am. J. Gastroenterol. 2022, 117, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, G.; Gkouvatsos, K.; Pantopoulos, K. Chronic hepatitis C and liver fibrosis. World J. Gastroenterol. 2014, 20, 11033–53. [Google Scholar] [CrossRef] [PubMed]
- Edmison, J.; McCullough, A.J. Pathogenesis of Non-alcoholic Steatohepatitis: Human Data. Clin. Liver Dis. 2007, 11, 75–104. [Google Scholar] [CrossRef] [PubMed]
- Afify, M.; Hamza, A.H.; Alomari, R.A. Correlation Between Serum Cytokines, Interferons, and Liver Functions in Hepatitis C Virus Patients. J. Interf. Cytokine Res. 2017, 37, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F.; Klinker, H.; Boeker, K.H.W.; Merle, U.; Link, R.; Buggisch, P.; Hüppe, D.; Cornberg, M.; Sarrazin, C.; Wedemeyer, H.; et al. Elevated liver enzymes predict morbidity and mortality despite antiviral cure in patients with chronic hepatitis C: Data from the German Hepatitis C-Registry. Hepatol. Commun. 2022, 6, 2488–2495. [Google Scholar] [CrossRef]
- Vonghia, L.; Magrone, T.; Verrijken, A.; Michielsen, P.; Van Gaal, L.; Jirillo, E.; Francque, S. Peripheral and Hepatic Vein Cytokine Levels in Correlation with Non-Alcoholic Fatty Liver Disease (NAFLD)-Related Metabolic, Histological, and Haemodynamic Features. PLOS ONE 2015, 10, e0143380. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Stewart, A.G.; Woodman, O.L.; Ritchie, R.H.; Qin, C.X. Non-Alcoholic Steatohepatitis: A Review of Its Mechanism, Models and Medical Treatments. Front. Pharmacol. 2020, 11. [Google Scholar] [CrossRef]
- Castro-Narro, G.; Moctezuma-Velázquez, C.; Male-Velázquez, R.; Trejo-Estrada, R.; Bosques, F.J.; Moreno-Alcántar, R.; Rodríguez-Hernández, H.; Bautista-Santos, A.; Córtez-Hernández, C.; Cerda-Reyes, E.; et al. Position statement on the use of albumin in liver cirrhosis. Ann. Hepatol. 2022, 27, 100708. [Google Scholar] [CrossRef]
- Rawi, S.; Wu, G.Y. Pathogenesis of Thrombocytopenia in Chronic HCV Infection: A Review. J. Clin. Transl. Hepatol. 2020, 8, 184–191. [Google Scholar] [CrossRef]
- Manuc, D.; Preda, C.M.; Sandra, I.; Baicus, C.; Cerban, R.; Constantinescu, I.; Olteanu, A.O.; Ciora, C.A.; Manuc, T.; Chiriac, D.E.; et al. Signification of Serum Alpha-Fetoprotein Levels in Cases of Compensated Cirrhosis and Hepatitis C Virus without Hepatocellular Carcinoma. J. Med. Life 2020, 13, 68–74. [Google Scholar] [CrossRef]
- Chu, C.-W.; Hwang, S.-J.; Luo, J.-C.; Lai, C.-R.; Tsay, S.-H.; Li, C.-P.; Wu, J.-C.; Chang, F.-Y.; Lee, S.-D. Clinical, Virologic, and Pathologic Significance of Elevated Serum Alpha-fetoprotein Levels in Patients with Chronic Hepatitis C. J. Clin. Gastroenterol. 2001, 32, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Falleti, E.; Fabris, C.; Toniutto, P.; Fontanini, E.; Cussigh, A.; Bitetto, D.; Fumolo, E.; Fornasiere, E.; Bragagnini, W.; Pinato, D.J.; et al. Interleukin-6 Polymorphisms and Gender: Relationship with the Occurrence of Hepatocellular Carcinoma in Patients with End-Stage Liver Disease. Oncology 2009, 77, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Barrett, S.; Collins, M.; Kenny, C.; Ryan, E.; Keane, C.; Crowe, J. Polymorphisms in tumour necrosis factor-α, transforming growth factor-β, interleukin-10, interleukin-6, interferon-γ, and outcome of hepatitis C virus infection. J. Med Virol. 2003, 71, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Dolganiuc, A.; Norkina, O.; Kodys, K.; Catalano, D.; Bakis, G.; Marshall, C.; Mandrekar, P.; Szabo, G. Viral and Host Factors Induce Macrophage Activation and Loss of Toll-Like Receptor Tolerance in Chronic HCV Infection. Gastroenterology 2007, 133, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Wang, K.; Aoyama, T.; Grivennikov, S.I.; Paik, Y.; Scholten, D.; Cong, M.; Iwaisako, K.; Liu, X.; Zhang, M.; et al. Interleukin-17 Signaling in Inflammatory, Kupffer Cells, and Hepatic Stellate Cells Exacerbates Liver Fibrosis in Mice. Gastroenterology 2012, 143, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Robak, E.; Gerlicz-Kowalczuk, Z.; Dziankowska-Bartkowiak, B.; Wozniacka, A.; Bogaczewicz, J. Serum concentrations of IL-17A, IL-17B, IL-17E and IL-17F in patients with systemic sclerosis. Arch. Med Sci. 2019, 15, 706–712. [Google Scholar] [CrossRef]
- Meng, P.; Zhao, S.; Niu, X.; Fu, N.; Su, S.; Wang, R.; Zhang, Y.; Qiao, L.; Nan, Y. Involvement of the Interleukin-23/Interleukin-17 Axis in Chronic Hepatitis C Virus Infection and Its Treatment Responses. Int. J. Mol. Sci. 2016, 17, 1070. [Google Scholar] [CrossRef]
- Belinchón-Romero, I.; Bellot, P.; Romero-Pérez, D.; Herraiz-Romero, I.; Marco, F.; Frances, R.; Ramos-Rincón, J.-M. Non-alcoholic fatty liver disease is associated with bacterial translocation and a higher inflammation response in psoriatic patients. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Tang, Y.; Bian, Z.; Zhao, L.; Liu, Y.; Liang, S.; Wang, Q.; Han, X.; Peng, Y.; Chen, X.; Shen, L.; et al. Interleukin-17 exacerbates hepatic steatosis and inflammation in non-alcoholic fatty liver disease. Clin. Exp. Immunol. 2011, 166, 281–290. [Google Scholar] [CrossRef]
- de Souza-Cruz, S.; Victória, M.B.; Tarragô, A.M.; da Costa, A.G.; Pimentel, J.P.D.; Pires, E.F.; Araújo, L.d.P.; Coelho-Dos-Reis, J.G.; Gomes, M.d.S.; Amaral, L.R.; et al. Liver and blood cytokine microenvironment in HCV patients is associated to liver fibrosis score: a proinflammatory cytokine ensemble orchestrated by TNF and tuned by IL-10. BMC Microbiol. 2016, 16, 1–12. [Google Scholar] [CrossRef]
- Rau, M.; Schilling, A.-K.; Meertens, J.; Hering, I.; Weiss, J.; Jurowich, C.; Kudlich, T.; Hermanns, H.M.; Bantel, H.; Beyersdorf, N.; et al. Progression from Nonalcoholic Fatty Liver to Nonalcoholic Steatohepatitis Is Marked by a Higher Frequency of Th17 Cells in the Liver and an Increased Th17/Resting Regulatory T Cell Ratio in Peripheral Blood and in the Liver. J. Immunol. 2016, 196, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Cachem, F.C.O.F.; Dias, A.S.; Monteiro, C.; Castro, J.R.; Fernandes, G.; Delphim, L.; Almeida, A.J.; Tavares, F.; Maciel, A.M.A.; Amendola-Pires, M.M.; et al. The proportion of different interleukin-17-producing T-cell subsets is associated with liver fibrosis in chronic hepatitis C. Immunology 2017, 151, 167–176. [Google Scholar] [CrossRef]
- Cachem, F.C.; Dias, A.S.; Monteiro, C.; Fernandes, G.; Delphim, L.; Tavares, F.; Maciel, A.M.; Amendola-Pires, M.M.; Brandão-Mello, C.E.; Andrade, R.M.; et al. Different core-specific T cell subsets are expanded in chronic hepatitis C with advanced liver disease. Cytokine 2018, 124, 154456. [Google Scholar] [CrossRef] [PubMed]
- Askoura, M.; Abbas, H.A.; Al Sadoun, H.; Abdulaal, W.H.; Abu Lila, A.S.; Almansour, K.; Alshammari, F.; Khafagy, E.-S.; Ibrahim, T.S.; Hegazy, W.A.H. Elevated Levels of IL-33, IL-17 and IL-25 Indicate the Progression from Chronicity to Hepatocellular Carcinoma in Hepatitis C Virus Patients. Pathogens 2022, 11, 57. [Google Scholar] [CrossRef] [PubMed]
- El-Emshaty, H.M.; Nasif, W.A.; Mohamed, I.E. Serum Cytokine of IL-10 and IL-12 in Chronic Liver Disease: The Immune and Inflammatory Response. Dis. Markers 2015, 2015, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Owusu, D.O.; Phillips, R.; Owusu, M.; Sarfo, F.S.; Frempong, M. Increased levels of circulating IL-10 in persons recovered from hepatitis C virus (HCV) infection compared with persons with active HCV infection. BMC Res. Notes 2020, 13, 1–7. [Google Scholar] [CrossRef]
- Tsujimoto, T.; Kawaratani, H.; Kitazawa, T.; Yoshiji, H.; Fujimoto, M.; Uemura, M.; Fukui, H. Immunotherapy for nonalcoholic steatohepatitis using themultiple cytokine production modulator Y-40138. World J. Gastroenterol. 2009, 15, 5533–40. [Google Scholar] [CrossRef]
- Aboushousha, T.; Emad, M.; Rizk, G.; Ragab, K.; Hammam, O.; Fouad, R.; Helal, N.S. IL-4, IL-17 and CD163 Immunoexpression and IL-6 Gene Polymorphism in Chronic Hepatitis C Patients and Associated Hepatocellular Carcinoma. Asian Pac. J. Cancer Prev. 2021, 22, 1105–1113. [Google Scholar] [CrossRef]
- Tan, Z.; Qian, X.; Jiang, R.; Liu, Q.; Wang, Y.; Chen, C.; Wang, X.; Ryffel, B.; Sun, B. IL-17A Plays a Critical Role in the Pathogenesis of Liver Fibrosis through Hepatic Stellate Cell Activation. J. Immunol. 2013, 191, 1835–1844. [Google Scholar] [CrossRef]
- Gomes, A.L.; Teijeiro, A.; Burén, S.; Tummala, K.S.; Yilmaz, M.; Waisman, A.; Theurillat, J.-P.; Perna, C.; Djouder, N. Metabolic Inflammation-Associated IL-17A Causes Non-alcoholic Steatohepatitis and Hepatocellular Carcinoma. Cancer Cell 2016, 30, 161–175. [Google Scholar] [CrossRef]
- Wieckowska, A.; Papouchado, B.G.; Li, Z.; Lopez, R.; Zein, N.N.; Feldstein, A.E. Increased Hepatic and Circulating Interleukin-6 Levels in Human Nonalcoholic Steatohepatitis. Am. J. Gastroenterol. 2008, 103, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Wu, L.; Xie, W.; Shao, Y.; Jiang, J.; Zhao, Z.; Yan, M.; Chen, Z.; Cui, D. The imbalance of Th17/Treg cells is involved in the progression of nonalcoholic fatty liver disease in mice. BMC Immunol. 2017, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chang, Q.; Wang, Y.; Zhao, Q.; Wang, C.; Hu, Y.; Wu, B. Th17 cells are increased with severity of liver inflammation in patients with chronic hepatitis C. J. Gastroenterol. Hepatol. 2011, 27, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Macek Jilkova, Z.; Afzal, S.; Marche, H.; Decaens, T.; Sturm, N.; Jouvin-Marche, E.; Huard, B.; Marche, P.N. Progression of fibrosis in patients with chronic viral hepatitis is associated with IL-17(+) neutrophils. Liver Int. Off. J. Int. Assoc. Study Liver 2016, 36, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Negro, F. ; European Association for the Study of the Liver EASL Clinical Practice Guidelines: Management of hepatitis C virus infection. J. Hepatol. 2014, 60, 392–420. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
Figure 1.
Median level of IL-6 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF, ¥ p<0.05plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16 .
Figure 1.
Median level of IL-6 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF, ¥ p<0.05plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16 .
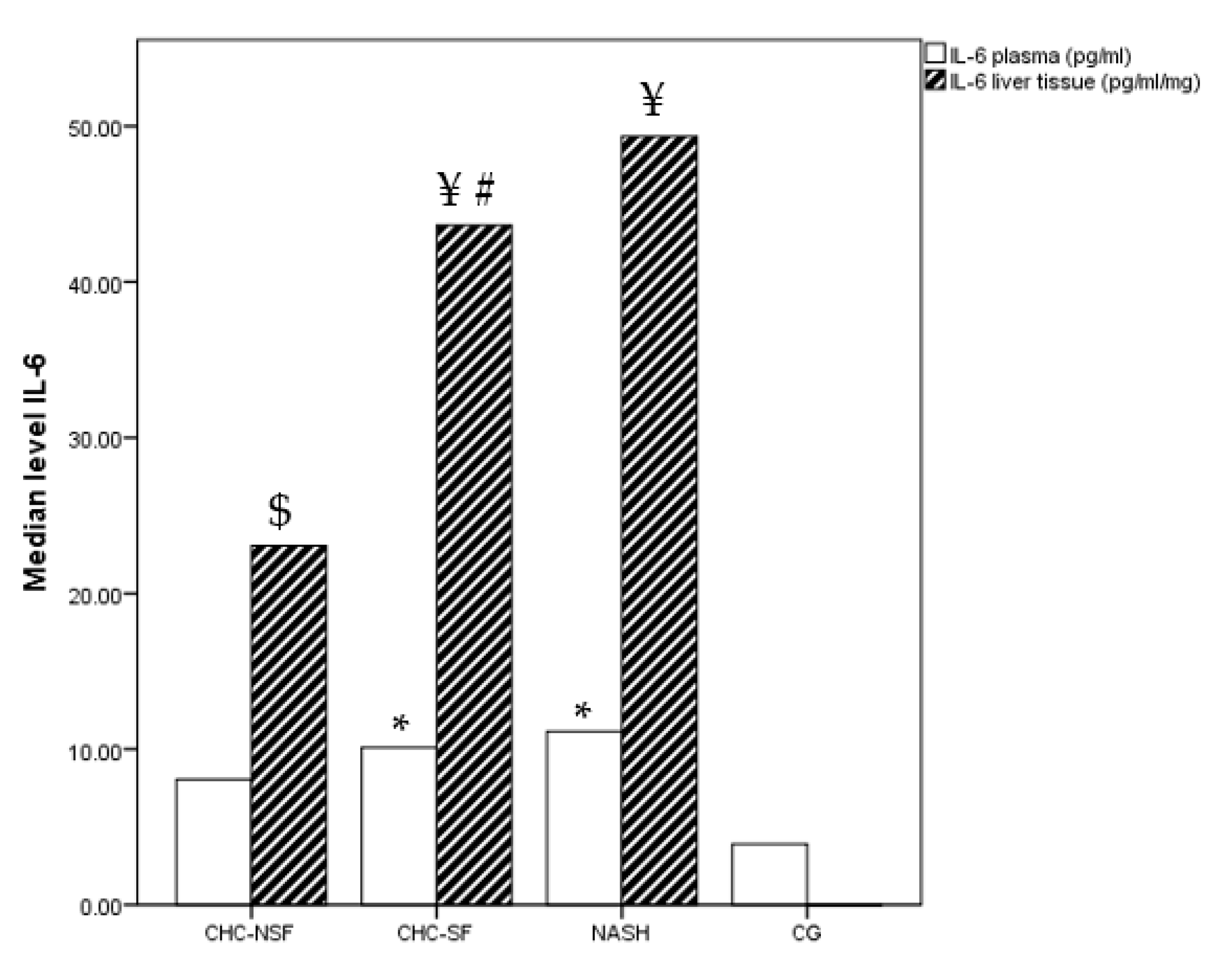
Figure 2.
Median level of IL-10 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
Figure 2.
Median level of IL-10 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
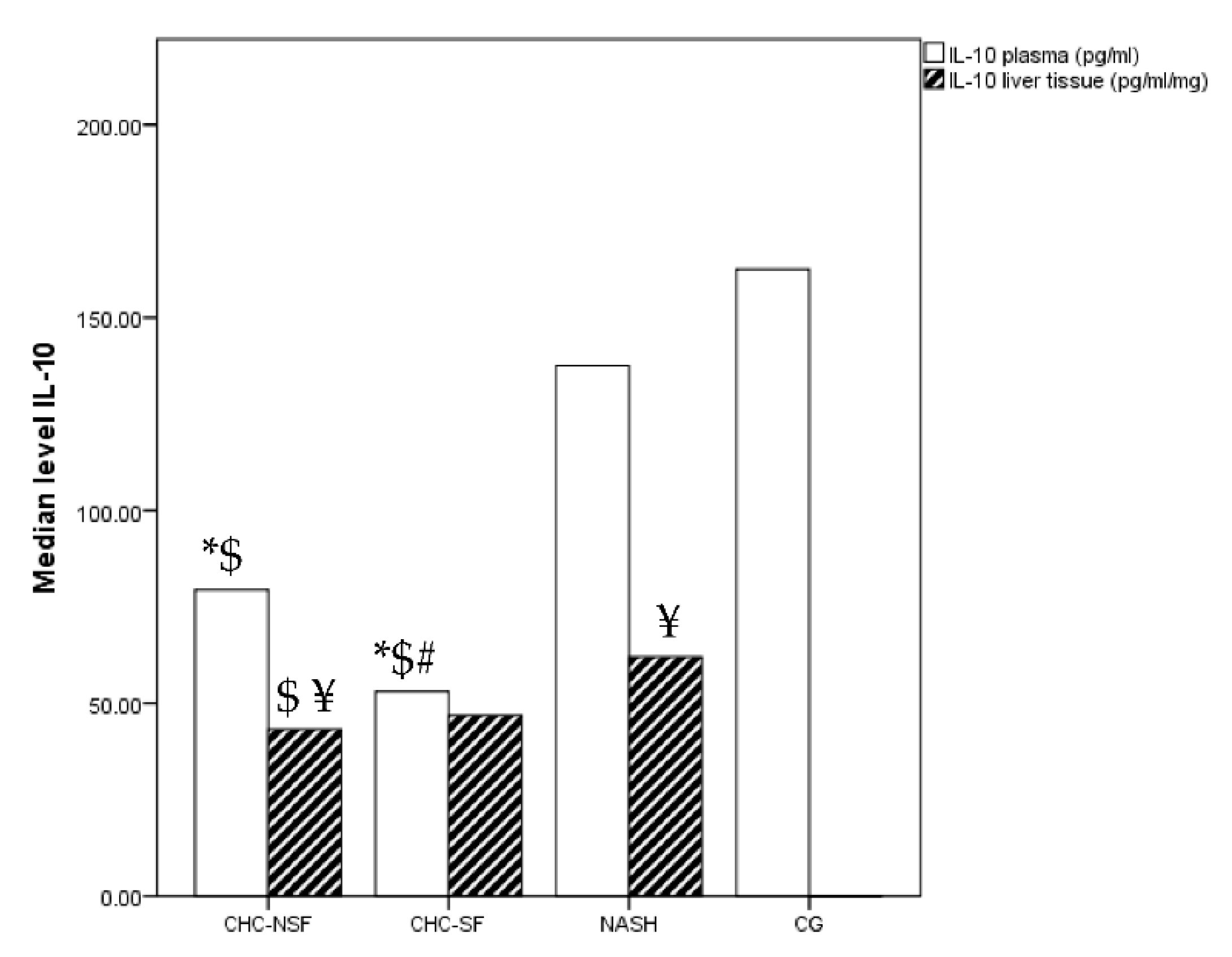
Figure 3.
Median level of IL-17A in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Withney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
Figure 3.
Median level of IL-17A in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; # p<0.05 in comparison with CHC-NSF; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Withney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
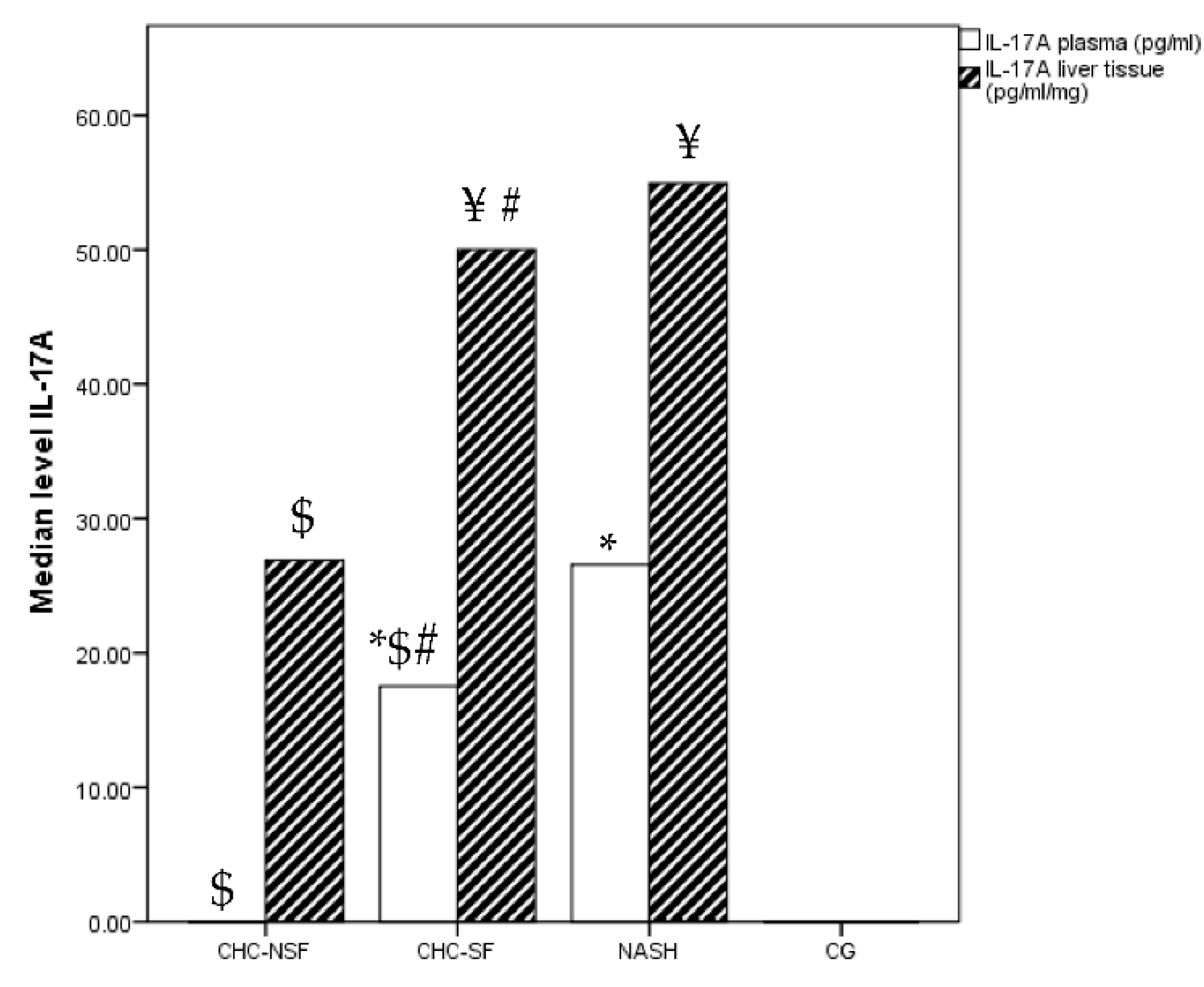
Figure 4.
Median level of IL-23 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
Figure 4.
Median level of IL-23 in plasma and liver tissue of healthy controls and patients with liver diseases. Statistical difference was assessed using Kruskal-Wallis test. *p<0.05 in comparison with CG; $ p<0.05 in comparison with NASH; ¥ p<0.05 plasma levels in comparison with liver tissue levels (Post-hock statistical difference using Mann-Whitney test); n (CG) = 20, n (NASH) = 19, n (CHC-NSF) = 20, n (CHC-SF) =16.
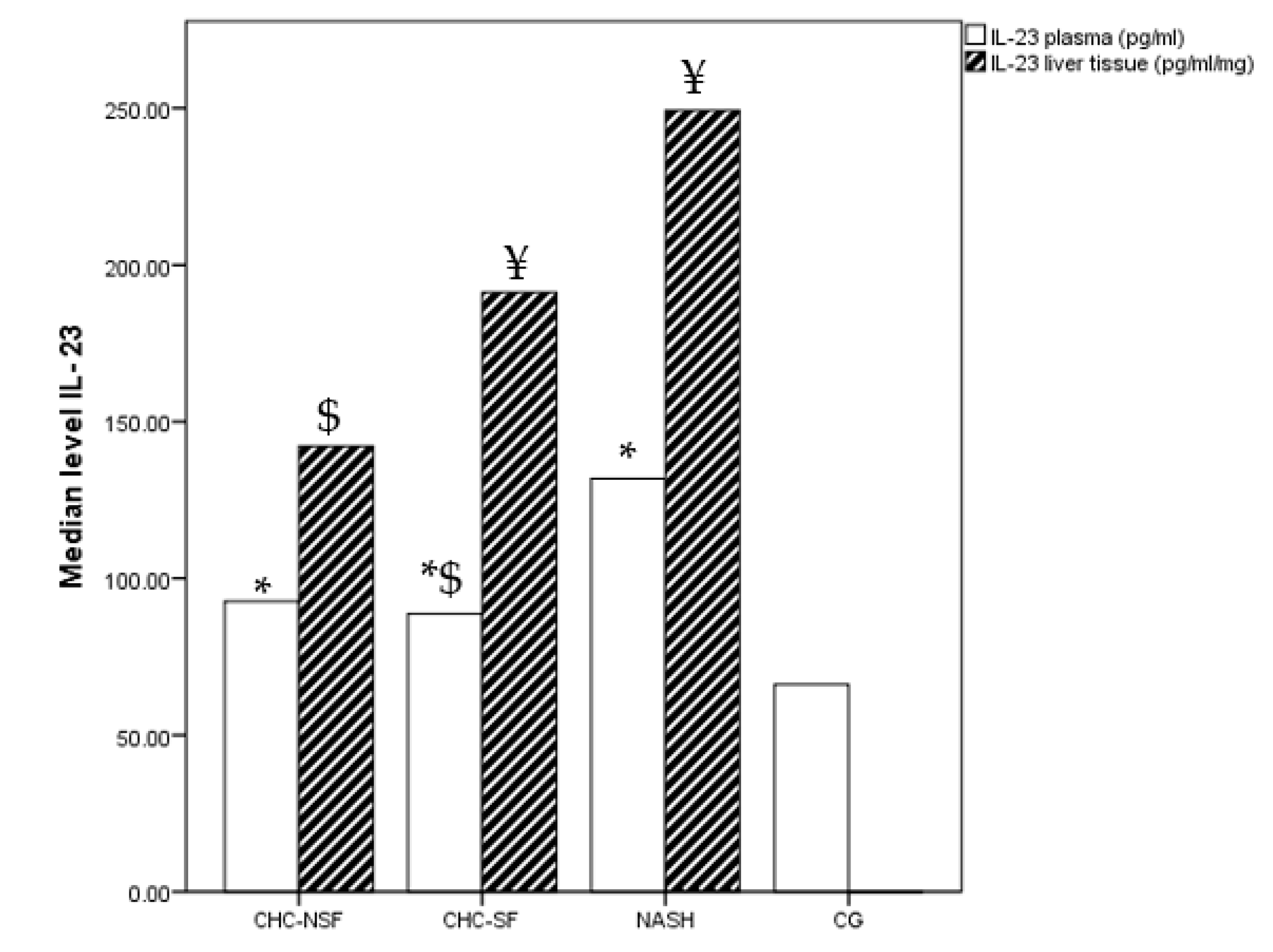

Table 1.
Demographic, anthropometric, biochemical characteristic in all groups.
| Variable | CHC-NSF (n=20) |
CHC-SF (n=16) |
NASH (n=19) |
CG (n=20) |
p value |
|---|---|---|---|---|---|
| Age (years) | 46.3 ± 13.6 | 54.2 ± 16.3 | 43.9 ± 9.2 | 42.5 ± 13.3 | ns |
| GenderFemale/ Male (%) | 49/51 | 52/48 | 34/66 | 47/53 | ns |
| Body mass (kg) | 70.0±9.6 | 70.1±9.5 | 96.7±19.4 *#$ | 67.8±11.1 | 0.000 |
| Body hight (cm) | 177.8±10.9 | 176.4±11.6 | 179.0±7.9 | 176.6±11.6 | ns |
| BMI (kg/cm2) | 22.0±0.9 | 22.4±0.8 | 30.1±5.5*#$ | 21.5±1.2 | 0.000 |
| Erythrocytes (cells/ml) | 4.9 ± 0.5 | 4.8 ± 0.6 | 5.0 ± 0.5 | 4.4 ±0.5 | ns |
| Hemoglobin (g/L) | 147.7 ± 13.7 | 142.1 ± 19.3 | 144.3 ± 14.2 | 137.8 ± 7.6 | ns |
| Leucocytes (cells/ml) | 7.8 ± 2.5 | 6.5 ± 2.2 | 6.6 ± 1.6 | 5.6 ± 1.4 | ns |
| PLT (cells/ml) | 230.6 ± 63.2 | 182.2 ± 57.4*# | 220.1 ± 41.0 | 263.7 ±66.7 | 0.000 |
| AST (U/l) | 41.3 ± 39.9* | 104.5 ± 38.8*# | 50.1 ±15.7*& | 22.5 ± 5.6 | 0.000 |
| ALT (U/l) | 61.1 ± 28.7* | 157.1 ± 29.9*# | 88.8 ± 44.2*& | 33.9 ± 11.1 | 0.000 |
| γGTP (U/l) | 67.8 ± 94.0 | 81.0 ± 82.8 | 61.1 ± 45.9 | 24.3 ± 5.1 | ns |
| AF (u/L) | 66.6 ± 24.9 | 80.0 ± 53.9 | 67.1 ± 17.5 | 71.4 ± 14.3 | ns |
| AFP (ng/ml) | 4.4 ± 2.4 | 11.8 ± 8.2*# | 2.9 ± 1.1& | 1.9 ± 0.6 | 0.000 |
| TSH (microU/ml) | 1.5 ± 0.8 | 1.6 ± 0.6 | 1.7 ± 0.9 | 2.5 ± 0.5 | ns |
| Glucose (mmol/l) | 5.7 ± 1.5 | 5.8 ± 1.1 | 5.4 ± 0.7 | 4.7 ± 0.5 | ns |
| Uric acide (µmol/l) | 5.3 ± 2.1 | 6.2 ± 1.6 | 5.6 ± 1.5 | 4.7 ± 1.2 | ns |
| Creatinine (µmol/l) | 79.8 ± 19.6 | 76.6 ± 17.2 | 81.5 ± 14.6 | 67.4 ± 10.8 | ns |
| Total cholesterol (mmol/l) | 4.7 ± 1.1 | 4.2 ± 1.0 | 7.1 ± 0.8*#& | 3.6 ± 0.7 | 0.000 |
| LDL (mmol/l) | 2.6 ± 1.0 | 2.4 ± 0.8 | 4.7 ± 0.8*#& | 2.5 ± 0.5 | 0.000 |
| HDL (mmol/l) | 1.5 ± 0.5* | 1.4 ± 0.3* | 1.3 ± 0.7* | 2.0 ± 0.5 | 0.000 |
| Triglycerides (mmol/l) | 1.25±0.8 | 1.20±0.8 | 4.13±1.13*#& | 1.14±0.2 | 0.000 |
| Total proteins (g/l) | 76.6 ± 6.5 | 75.1 ± 7.6 | 76.3 ± 7.7 | 75.9 ± 6.1 | ns |
| Albumin (g/l) | 38.9 ± 3.1* | 31.1 ± 2.4*# | 43.3 ± 5.5& | 42.6 ± 3.9 | 0.000 |
| Total bilirubin (mg/dl) | 10.6 ± 4.5 | 10.9 ± 2.7 | 13.7 ± 9.3 | 10.5 ± 3.3 | ns |
| Direct bilirubin (mg/dl) | 3.9 ± 1.8 | 4.6 ± 1.4 | 3.9 ± 1.5 | 2.1 ± 1.5 | ns |
| INR | 1.0 ± 0.2 | 1.1 ± 0.2 | 1.0 ± 0.1 | 1.0 ± 0.1 | ns |
| Fibrinogen (mg/dl) | 2.9 ± 0.5 | 2.8 ± 0.5 | 3.1 ± 0.4 | 2.6 ± 0.4 | ns |
| CRP (mg/dl) | 2.5 ± 2.0 | 3.7 ± 2.0 | 3.8 ± 2.3 | 1.3 ± 0.6 | ns |
Data are given as mean ± SD; BMI: body mass index, PLT: platelets, AST: aspartate aminotransferase, ALT: alanine aminotransferase, γGTP: γ-glutamyl transpeptidase; AP: alkaline phosphatase; AFP: alpha fetoprotein; TSH: thyroid-stimulating hormone; LDH: lactate dehydrogenase; CK: creatine kinase; LDL: low-density lipoprotein cholesterol; HDL: high-density lipoprotein cholesterol; INR: indicates international normalized ratio; CRP: c-reactive protein; ns: not significant. Statistical difference was assessed using ANOVA test. *p<0.05 in comparison with CG; # p<0.05 in comparison with CHC-NSF; & p<0.05 in comparison with CHC-SF (Post-hock statistical difference using Bonferroni test).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



