
Submitted:
29 May 2023
Posted:
31 May 2023
You are already at the latest version
Abstract
Carbapenemase resistance in Enterobacterales is a global public health problem and rapid and effective methods to detect resistance mechanisms are needed urgently. Our aim was to evaluate the performance of a MALDI-TOF MS based KPC detection protocol from patients’ positive blood cultures, short-term cultures and colonies at health care settings. Bacterial identification and KPC detection were achieved after protein extraction with organic solvents and target spot loading with suitable organic matrices. Confirmation of KPC production was performed by susceptibility tests, blaKPC amplification by PCR and sequencing. KPC direct detection (KPC-peak at approximately 28.681 Da) from patients’ positive blood cultures, short-term cultures and colonies, once bacterial identification was achieved, showed an overall sensibility and specificity of 100% (CI95: [95%,100%] and CI95: [99%, 100%], respectively). Concordance between hospital routine bacterial identification protocol and identification with this new methodology from the same extract used for KPC detection was ≥92%. This study represents the pioneering effort to directly detect KPC using MALD-TOF MS technology, conducted on patient-derived samples obtained at the hospitals for validation purposes, in a multi-resistance global context that requires concrete actions to preserve available therapeutic options and reduce the spread of antibiotic resistance markers.
Keywords:
KPC
; blood culture
; short-term culture
; MALDI-TOF MS
1. Introduction
Carbapenem resistance in Enterobacterales (CRE) is a worldwide public health problem, whose magnitude was enlarged after the SARS-CoV-2 pandemic [1,2]. Klebsiella pneumoniae carbapenemase (KPC), the most prevalent variants being KPC-2 and KPC-3, is by now the most commonly reported carbapenemase around the world, and is associated with high morbidity and mortality rates. Its location on self-conjugative plasmids and frequent association with K. pneumoniae, are some of the factors that contributed to its global dissemination [3].
KPC detection at clinical laboratories is usually achieved by traditional phenotypic methods, being the most common ones, the disk diffusion tests and synergy approaches [4]. Also, colorimetric assays, like Blue Carba test [5] and Carba-NP [6] can be performed, and even though they are operator-friendly, they do not define the enzyme involved in the resistance mechanism and may not be attainable for every clinical laboratory. These culture-based methodologies are easy to perform but require the isolation of the pathogen on solid culture media after at least a 18-24 incubation period, and their sensibilities and specificities range from 84-100% and 91-100%, respectively [4]. Also, lateral flow immunoassays are available with high sensitivity and specificity, but are generally expensive for most clinical laboratories [4]. Carbapenemase genotypic detection (like Polymerase Chain Reaction- PCR- assays or Whole Genome Sequencing-WGS-) is highly sensitive but not commonly available in most clinical laboratories because its elevated cost [7] and trained personnel necessity. Matrix-assisted laser desorption ionization – time of flight mass spectrometry (MALDI-TOF MS) hydrolysis assays to detect carbapenemases have been described, but they are not commonly implemented at clinical laboratories [4,8]. Therefore, there is an ongoing effort to develop and validate new molecular and immunological methods for KPC detection in clinical settings.
Blood stream infection with CRE is associated with high mortality rates [9,10] and, as previously stated by Kumar et al. [11], rapid instauration of adequate antibiotic therapy for bacteremia is crucial for patients’ prognosis, raising the need for new rapid methodologies for resistance detection to be developed. Colorimetric assays to detect carbapenemase activity, along with bacterial identification, have also been tested from short-term cultures (STC) obtained from positive blood culture (BC) bottles showing good results [12,13], but no protocol has been evaluated directly from positive patients’ BC bottles.
Carbapenemase-producing K. pneumoniae is the most commonly isolated pathogen from rectal swabs, when the surveillance of carbapenemase carriers in hospital closed units is carried out [14]. Screening is usually made using chromogenic culture media, where carbapenem-resistant bacteria is recovered from the patients’ sample [15,16] and KPC confirmation is made afterwards by phenotypic synergy tests. KPC producers are also commonly isolated from other types of clinical specimens, like respiratory and urine samples [3,17].
MALDI-TOF MS technology is nowadays widely used for microbial identification (ID) of bacteria and fungi around the world [18,19], and antibiotic resistance detection is one of the current challenges to face [20].
Based on investigations performed by Camara et al. [21] and Papagiannitsis et al. [22], we formerly developed a methodology for CMY [23] and KPC [24] detection using MALDI-TOF MS from isolated colonies (COL), showing high sensibility and specificity results. The aim of this study was to evaluate the performance of a fast and easy bacterial identification and KPC detection protocol using MALDI-TOF MS from patients´ positive blood cultures, short-term cultures and colonies at health care settings, testing its concordance with the results obtained in each hospital.
2. Materials and Methods
2.1. Control strains
Recombinant strains (E. coli TOP10/pKPC-2 and E. coli TOP10/pKPC-3) [24,25] expressing the most prevalent KPC variants were used as controls, to establish the m/z value of the enzyme in the spectrum as a reference. Receptor strains (E. coli TOP10 and E. coli TOP10/pK19) not expressing the enzymes, were evaluated as negative control spectra. Protein extraction with formic acid—isopropyl alcohol—water, 17:33:50 (v/v) (FA-ISO) was performed from isolated colonies (COL) on solid culture media [24]. K. pneumoniae ATCC 700603 was also used as a negative control strain.
2.2. KPC detection from simulated positive blood cultures, short-term cultures and colonies using previously characterized isolates
We evaluated a panel of 93 Enterobacterales (60 K. pneumoniae, 33 Escherichia coli) for bacterial identification and KPC detection from simulated positive blood cultures and short-term cultures, and 118 Enterobacterales (60 K. pneumoniae, 28 E. coli, 12 Enterobacter cloacae complex, 3 Citrobacter braakii, 15 Serratia marcescens) for bacterial identification and KPC detection form colonies (Table 1).
All isolates were previously characterized phenotypically by identification, disk diffusion tests and sinergy tests [26], and genotypically by PCR and sequencing [27] at Laboratorio de Resistencia Bacteriana (Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires).
Sample processing from simulated positive BC and COL was performed as previously described by Figueroa-Espinosa et al. [24]. Sample processing from STC was performed the same way as from isolated colonies [24].
We evaluated bacterial identification results and calculated KPC detection sensibility and specificity from visual inspection of KPC producing and non-KPC producing isolates’ spectra for every type of sample.
2.3. Clinical samples
A total of 193 samples, collected during a 7 months period between 2022 and 2023, were included in this study: 78 positive BC bottles, 78 STC and 37 COL samples. Samples showing positive growth for members of Enterobacterales, were included for direct processing from positive BC bottles (49 were analyzed at Hospital Alemán and 29 at Hospital de Clínicas). Bacterial identification and KPC detection were evaluated directly form positive BC bottles (n = 78) and from the corresponding STC (n = 78).
In addition, 37 carbapenem resistant isolates recovered from rectal swabs (n = 25) and other clinical specimens (n = 12) were included. To test bacterial identification and KPC detection from solid culture media, we selected blue colonies grown on CHROMagarTM KPC supplemented with meropenem (CHROMagar, France) recovered from rectal swabs, and isolates obtained from urine cultures grown on Mueller Hinton Agar (Laboratorio Argentino, Argentina) showing resistance to carbapenems. All samples from colonies were analyzed at Hospital Alemán.
As patients´ personal information was encrypted, this study was exempted from the requirement of written informed consent. Also, it was approved by the Ethics Committee of Facultad de Farmacia y Bioquímica (Universidad de Buenos Aires) (RESCD-2020-134-E-UBA-DCT_FFYB, August 20th, 2020).
2.4. Hospitals´ bacterial routine identification
Bacterial routine identification at both hospitals was performed by the standard direct MALDI-TOF MS protocol [18] from STC obtained from positive BC bottles, and from isolated colonies for COL samples. A loopfull of bacteria from the STC/colonies was laid onto a steel target plate with a wooden stick and then, 1 µL of α-cyano-4-hydroxycinnamic acid (HCCA) was deposited on the spot. After drying at room temperature, automatic analysis with MALDI-TOF MS´s flexAnalysis software was performed.
2.5. Protein extraction from patients´ positive blood culture bottles
As described previously [24], protein extraction was performed using organic solvents. Briefly, 1.4 mL of positive blood culture was transferred to an eppendorf tube, which was centrifuged at 1.4 rpm for 5 min. One milliliter of the supernatant was collected and centrifuged at 13.000 for 2 min; then the pellet was washed once with 1 mL of distilled water, vortexed for 30 s, and centrifuged at 13.000 rpm for 2 min. The bacterial pellet was re-suspended in 300 mL of distilled water and vortexed for 30 s at room temperature. Then, 900 mL of absolute ethanol (Sigma-Aldrich, USA) was added, vortexed for 30 s, and centrifuged at 13.000 rpm for 2 min. The supernatant was discarded, and the pellet was re-suspended in 100 mL of extraction solvent (FA-ISO) (Sigma-Aldrich, USA). The suspension was vortexed for 30 s and centrifuged for 2 min at 13.000 rpm. The supernatant extract was used both for bacterial identification and KPC detection with MALDI-TOF MS.
2.6. Protein extraction from short-term cultures
In addition to processing samples directly from BC bottles, protein extraction was also performed from the corresponding STC. Two drops (approximately 100 µL) of positive BC were plated on Blood Agar plates and incubated at 37°C for 4-5 hours, in a 5% CO2 atmosphere. Protein extracts from STC were obtained with FA-ISO extraction method as previously described by Figueroa-Espinosa et al. [24] from isolated colonies, but after a shorter incubation period (4-5 hours instead of 18-24 hours). The supernatant extract was used both for bacterial identification and KPC detection with MALDI-TOF MS.
2.7. Protein extraction from colonies
Protein extraction was performed according to Figueroa-Espinosa et al. [24] protocol (FA-ISO extraction method) from isolated colonies on CHROMagarTM KPC supplemented with meropenem and lawns grown on Mueller Hinton Agar after 18-24 hours incubation at 37°C. Supernatant extracts were used both for bacterial identification and KPC detection with MALDI-TOF MS.
2.8. Target spot loading for bacterial identification and KPC detection
For bacterial identification, 1 µL of protein extract was co-crystallized with 1 µL of HCCA matrix and analyzed after drying at room temperature (one spot per sample).
For KPC detection, protein extracts obtained from patients´ positive BC, STC and COL, were spotted onto the steel target plate using a double-layer sinapinic acid (SA) method, as follows: first, a layer of 0.7 µL of SA-saturated solution (10 mg/mL SA in absolute ethanol) (Sigma-Aldrich, USA) was laid on the spot; after drying at room temperature, a second layer of 1 µL of SA solution in acetonitrile (30:70 v/v) (Sigma-Aldrich, USA) and 0.1% trifluoroacetic acid (Sigma-Aldrich, USA) in water was deposited above the first one, and finally, 1 µL of protein extract was added in the final step. The samples were left to dry at room temperature and then analyzed by MALDI-TOF MS. For KPC detection, each extract was analyzed in duplicate.
2.9. Spectra acquisition
For bacterial identification in the low molecular weight range, spectra were obtained in the linear positive ion mode of a Microflex LT mass spectrometer (Bruker Daltonics, Germany) with flexControl 3.4 software (Bruker Daltonics, Germany), using the automatic MBT_FC.par method with default parameters. Before each run, the spectrometer was calibrated using Bacterial Test Standard (Bruker Daltonics, Germany).
For high molecular weight range analysis (KPC detection), spectra were obtained in the linear positive ion mode of the Microflex LT mass spectrometer (Bruker Daltonics, Germany) with flexControl 3.4 software, using the LP44_44kDa.par method.
At Hospital Alemán, parameters were configured as follows: mass range: 10,000 Da to 50,000 Da; spectrometer ion source 1: 19.99 kV; ion source 2: 17.94 kV; lens: 5.99 kV; pulsed ion extraction: 650 ns; and detection gain: 3017 V; laser frequency was 60 Hz and laser power was set at 90%. Each spectrum was obtained after 1000-1200 shots per spot.
At Hospital de Clínicas, parameters were configured as follows: mass range: 10,000 Da to 50,000 Da; spectrometer ion source 1: 19.94 kV; ion source 2: 17.78 kV; lens: 5.95 kV; pulsed ion extraction: 650 ns; and detection gain: 2745 V; laser frequency was 60 Hz and laser power was set at 90%. Each spectrum was obtained after 1000-1200 shots per spot.
Data were manually acquired using autoXecute mode at both hospitals. Before each run, the spectrometer was calibrated using Protein Standard II Calibration Mix (Bruker Daltonics, Germany), containing a mixture of Protein A and Trypsinogen.
2.10. Bacterial identification concordance calculation
Bacterial identification concordance between the hospital routine method (direct MALDI-TOF MS protocol from STC or isolated colonies [18]) and protein extraction using FA-ISO method was calculated according to the following formula [30]:
Concordance = (No. of result matches/total tests) x 100
When different species belonged to E. cloacae complex, the group as a hole (the complex) was considered for the concordance analysis, regardless species names, as recommended by the Argentinian National Network for Microbiological Identification by Mass Spectrometry [31].
2.11. Visual spectra analysis and statistics for KPC detection
Spectra obtained directly from patients’ positive BC, STC and COL were analyzed visually using flexAnalysis 3.4 software (Bruker Daltonics, Germany). We searched for the visual presence/absence of the KPC peak in every spectrum after baseline substraction and smoothing, considering the expected size of the enzyme observed when analyzing the control strains as reference. In addition, we evaluated intensity in the y axis (arbitrary units) for every spectrum in the expected KPC m/z position.
We also visually searched for a ~11.109 Da peak, previously reported to be associated to a common KPC dissemination platform [32,33,34] on spectra acquired for bacterial identification with HCCA.
Only those samples for which bacterial identification with FA-ISO extraction method was achieved, were included for KPC detection statistical analysis with ClinPro Tools, as we considered that failed identification is indicative of low efficiency in the protein extraction process, that could lead to false negative results when detecting KPC for a producing culture.
Spectra of each protein extract were analyzed after automatic calibration and normalization with the software ClinPro Tools 3.0 (Bruker Daltonics) [35]. Statistical analysis was performed using the full raw spectra (10,000 to 50,000 Da) of duplicates with the “Peak Statistic Calculation” tool. The area under the curve (AUC) of the ROC curve was evaluated for the selected peak between KPC producing and non-producing strains to determine discriminative power and Genetic Algorithm (GA) was used to calculate sensitivity and specificity.
2.12. Antimicrobial susceptibility testing and genetic characterization of isolates
All isolates were characterized phenotypically by disk diffusion tests according to the Clinical and Laboratory Standards Institute (CLSI) guidelines [36] at the hospitals. Production of carbapenemases was investigated by sinergy tests using boronic acid (BOR), EDTA and carbapenems [26] at both hospitals. Blue Carba Test (bioMérieux, France) [5] was performed at Hospital de Clínicas from most STC obtained from positive BC bottles when requested by physicians, and an immunochromatographic assay (Britania, Argentina) [4] for carbapenemase detection was performed for two isolates at Hospital Alemán. The results obtained from hospitals remained blinded and were not shared until the conclusion of the study, ensuring a double-blind approach.
Genotypic characterization was carried out at Laboratorio de Resistencia Bacteriana (Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires) by PCR amplification performed on total DNA using primers and conditions described previously [27]. We searched for carbapenemase encoding genes usually found in Enterobacterales (blaKPC and blaNDM), and blaKPC amplicons were sequenced on both strands using an ABI3730XL DNA Sequencer (Macrogen, Seoul).
3. Results
3.1. KPC-producing recombinant strains spectra analysis
KPC m/z observed in control strains spectra obtained by using SA as matrix was 28.679 Da for KPC-2 (Figure 1.a) and 28.703 Da for KPC-3 (Figure 1.b), both peaks absent in the receptor strains, and they were considered as reference for visual evaluation of clinical samples. KPC variants m/z values were similar when analyzed at both hospitals.
3.2. Bacterial identification and KPC detection from simulated positive blood cultures, short-term cultures and colonies evaluated with previously characterized isolates
Bacterial identification performed using FA-ISO extraction method showed complete concordance with previous characterization results for all the isolates evaluated (93 Enterobacterales from simulated positive BC and STC and 118 from colonies).
For visual detection of KPC (peak ~28.680 Da) from simulated positive BC and STC, both sensitivity and specificity were 100% (CI95%: [90%; 100%] for sensibility, CI95%: [93%; 100%] for specificity).
Regarding KPC visual detection from isolated colonies, the sensitivity and specificity were also 100% (CI95%: [93%; 100%] for sensibility; CI95%: [94%; 100%] for specificity).
3.3. Bacterial identification from clinical samples
Bacterial ID from patients’ positive BC bottles with FA-ISO extraction method was achieved in 71/78 samples. Seven BC samples rendered a not reliable identification (NRI) result, probably due to a low efficiency in the protein extraction process.
Considering the samples for which a successful ID was achieved from patients´ BC bottles (n = 71): 41 samples were identified as K. pneumoniae by the hospital protocol, whereas ID results using FA-ISO extraction method were K. pneumoniae (n = 39) and K. variicola (n = 2); 1 sample identified as K. variicola by the hospital was identified as K. pneumoniae by the FA-ISO protocol; E. coli was concordantly identified in every case (n = 24) as well as S. marcescens (n = 5), E. cloacae complex (n =1) and Proteus mirabilis (n =1) (Table 2). The concordance rate for bacterial identification directly from patients´positive BC bottles reached 98% when considering the samples for which a successful ID was achieved.
Regarding bacterial identification from STC (n = 78), 45 samples identified by the hospital as K. pneumoniae were identified as K. pneumoniae (n = 40) and K. variicola (n = 5) by the FA-ISO extraction method. E. coli (n = 24), E. cloacae complex (n = 2), K. variicola (n =1) and P. mirabilis (n =1) were concordantly identified by both methods. Five samples were identified as S. marcescens by the hospital, whereas the FA-ISO method ID result was S. marcescens (n = 4) and S. ureilytica (n = 1) (Table 3). Concordance for bacterial identification from STC was 92%.
When comparing bacterial identification from COL samples (n = 37) between direct MALDI-TOF MS method from isolated colonies (hospital routine identification) and FA-ISO extraction method, there was 100% concordance. Specifically, 36 isolates were identified as K. pneumoniae, and one of them was identified as Proteus mirabilis (Table 4).
3.4. KPC detection from patients’ positive BC bottles
KPC producers (7 K. pneumoniae) evaluated directly from patients’ positive BC bottles showed a peak between 28.655 Da and 28.740 Da (median = 28.722, CI95: [28.655 Da, 28.740 Da]) (Figure 2.a). This peak was absent in non-KPC producers’ spectra (n = 64), although some intensity at KPC m/z range was observed in some cases (background noise), but did not constitute a clear peak (Table 2). Intensities ranged from 221 a.u. to 1095 a.u. for KPC producers (median = 610 a.u.) and from 0 a.u. to 176 a.u. (median = 27,5 a.u) for non-KPC producing strains (Figure 3.a).
For statistical parameters calculation we considered only the samples for which bacterial identification was achieved by FA-ISO extraction method, indicating an efficient protein extraction process (see Section 2.11).
Statistical analysis with ClinPro Tools showed a significant difference (p-value < 0.001) between KPC producers and non-KPC producers for a selected peak at 28.724 Da. The AUC of the ROC curve for this specific peak was 0,98, indicating a great discrimination power between the groups. Sensibility and specificity for KPC detection from positive BC bottles, calculated by the GA tool, was 100% for both parameters (CI95%: [77%; 100%] for sensibility; CI95%: [97%; 100%] for specificity) (Table 5).
3.5. KPC detection from STC samples
KPC producers (8 K. pneumoniae) evaluated from STC obtained from positive BC bottles showed a peak between 28.660 Da and 28.728 Da (median = 28.676 Da, CI95%: [28.660 Da, 28.728 Da]) (Figure 2.b). This peak was absent in non-KPC producers’ spectra (n = 70), although some intensity at KPC m/z range was observed in some of them but did not constitute a clear peak (Table 3). Intensities ranged from 261 a.u. to 1283 a.u. for KPC producers (median = 835,5 a.u.) and from 0 a.u. to 520 a.u. (median = 48,5 a.u.) for non-KPC producing strains (Figure 3.b).
Statistical analysis with ClinPro Tools showed a significant difference (p-value < 0.001) between KPC producers and non-KPC producers for a selected peak at 28.679 Da. The AUC of the ROC curve for this specific peak was 0,97, indicating a great discrimination power between the groups. Sensibility and specificity for KPC detection from STC calculated by GA tool, was 100% for both parameters (CI95%: [79%; 100%] for sensibility; CI95%: [97%; 100%] for specificity) (Table 5).
3.6. KPC detection from COL samples
All K. pneumoniae KPC producers evaluated from COL (n = 18) showed a peak between 28.662-28.716 Da (median = 28.683 Da, CI95%: [28.676 Da; 28.698 Da]) (Figure 2.c), and intensities ranged from 727- 3949 a.u (median = 1503,5 a.u.) (Figure 3.c). This peak was not present in non-KPC producers´ spectra (n = 19). When evaluating intensities at the KPC m/z range for COL for non-KPC producers, values ranging 4 - 519 a.u. were observed (median = 67 a.u.) (Table 4).
Statistical analysis with ClinPro Tools showed a significant difference (p-value < 0.001) between KPC producers and non-KPC producers for a selected peak at 28.686 Da. The AUC of the ROC curve for this specific peak was 0,97, indicating a great discrimination power between the groups. Sensibility and specificity for KPC detection from COL, calculated by GA tool, was 100% for both parameters (CI95%: [90%; 100%] for sensibility; CI95%: [91%; 100%] for specificity) (Table 5).
A comparison of KPC m/z median, intensity median for samples containing KPC producers and non-KPC producers, sensibility and specificity for each type of sample evaluated in this study is shown in Table 5. The median m/z value for KPC in all KPC-producing samples (7 BC, 8 STC and 18 COL) was 28.681 Da (CI95%: [28.676 Da; 28.687 Da]), with a median intensity of 1095 a.u. In contrast, the median intensity for non-KPC producers was only 45 a.u. The overall sensibility and specificity for KPC detection were 100%, [CI95%: 95%; 100% and CI95%: 99%; 100%, respectively].
3.7. Peak at m/z ~11.109 Da visual detection
Considering all the samples included in this study (BC, STC and COL) a ~11.109 Da peak, corresponding to the P019 protein associated to Tn4401a transposon carried by some KPC-producing K. pneumoniae strains, was visually detected on 21/33 KPC producers´ spectra, ranging from 11.100-11.117 Da (median: 11.109 Da, [CI95%: 11.106 Da; 11.110 Da]), and it was not detected in non-KPC producing isolates (Table 2, Table 3 and Table 4). This biomarker was successfully detected in KPC producers from 3/7 positive BC bottles, 3/8 STC samples, and 15/18 COL samples and its overall sensibility and specificity were 63% and 100%, respectively.
3.8. Ferulic acid matrix performance for KPC detection
Spectra acquired after FA target spot loading for all protein extracts (BC bottles, STC and COL) showed similar results to those obtained with SA. Additionally, successful KPC peak detection was achieved when FA was used as a co-crystallization matrix. Even if some background noise was observed when analyzing some non-KPC producing isolates spectra, no clear peaks in KPC m/z range were observed when the FA matrix was used (Figure 4).
3.9. Antimicrobial susceptibility testing and carbapenemase gene detection by PCR
Twenty-six K. pneumoniae STC (18 K. pneumoniae, 5 S. marcescens, 2 E. coli and 1 E. cloacae complex) were tested by Blue Carba test at Hospital de Clínicas, and 12 of them rendered a positive result for carbapenemase production. When analyzed by PCR amplification, 4 of them were blaKPC carriers, and 8 were blaNDM carriers. Two samples (1HC15 and 1HC16) rendered a Blue Carba test negative result and blaNDM was amplified by PCR afterwards. The 2 isolates tested by immunochromatography at Hospital Alemán (HC64 and HC65), rendered a blaKPC positive result by PCR.
All KPC-producing isolates (8 BC/STC samples and 18 COL samples), showed cephalosporin and carbapenem resistance by disk diffusion tests. In addition, positive amplification for blaKPC was obtained by PCR assay. Thirty-four samples (10 BC/10 STC samples and 24 COL samples) showed positive amplification only for blaNDM and 7 isolates (COL) were co-carriers of blaKPC and blaNDM (Table 2, Table 3 and Table 4). Two clinical isolates were positive for blaIMP amplification (Table 4). Regarding KPC variants, 21 isolates (8 BC/8 STC samples and 13 COL samples) carried blaKPC-2 and 5 isolates (COL samples) carried blaKPC-3 (Table 2, Table 3 and Table 4). Non-carbapenem resistant isolates rendered a negative result for carbapenemase genes amplification, as expected.
4. Discussion
Previous studies evaluated KPC detection from isolated colonies and simulated positive blood cultures using MALDI-TOF MS [24,37,38]. This is the first study including patients’ samples and performed in the health care setting. Bacterial identification and KPC detection were successfully achieved from liquid culture media (BC broth) as well as from different solid culture media (Blood Agar, chromogenic media and Mueller Hinton Agar).
Moreira et al. reported a sensibility of 98,09% and a specificity of 97,9% for KPC detection from isolated colonies [37] and a sensibility of 94,9% and a specificity of 95,3% for KPC detection from simulated positive blood cultures [38]. However, it is worth noting that these statistical parameters are slightly lower than the ones reported in this study when evaluating isolates previously characterized isolates from our strain collection.
Regarding patients’ samples, KPC detection from BC bottles and STC can be achieved during the first hours once the BC bottle is positive, reducing the turnaround time (TAT) of traditional KPC phenotypic verification methods for 24-48 hours (Figure 5). We strongly recommend performing KPC detection only after successful bacterial identification has been achieved from the protein extract in the first place. This serves as a “check-point” to ensure the efficiency of the protein extraction process before proceeding with KPC detection. If bacterial identification is unsuccessful, we suggest repeating the protein extraction protocol if some sample is still available.
MALDI-TOF MS KPC-peak detection from rectal swab isolates as well as isolates recovered from other clinical specimens, can significantly reduce the TAT of commonly used phenotypic synergy tests. This accelerated approach can assist in the clinical decision-making process of isolating patients with KPC fecal carriage in hospital closed units (Figure 5).
For KPC-2 producers, a KPC-peak at approximately 28.681 Da was consistently detected after visual analysis of spectra of KPC-producing samples, compared to reference m/z observed in control strains (E. coli TOP10/pKPC-2), with the exception of 1HD19, HC63, HC64, HD65 and POR15 (KPC-2 carriers). For these samples, the observed m/z values in the spectra were higher than the control strain spectrum. Given the potential variation in the m/z value of the KPC-peak, it is advisable to consider a m/z range for detection instead of a fixed peak value.
The slight difference between KPC-peak median values calculated manually and KPC-peak values selected by ClinPro Tools program may be attributed to software parameters.
Previous studies reported different KPC m/z values. Yoon et al. [39] estimated a KPC m/z of 28.718 Da when analyzing transformant strains, after protein extraction with a lysis buffer from colonies grown in MacConkey Agar. Regarding the spectrometer parameters, this research group used a pulse ion extraction of 1200 ns. Moreira et al. [37] evaluated different pulse ion extraction settings, using the FA-ISO extraction method [24], finding different KPC m/z at each scenario. Performing different protein extraction methodologies and different acquisition parameters could then lead to different KPC m/z values. Nonetheless, Moreira et al. [37,38] reported a similar KPC-peak range when analyzing isolated colonies and artificial positive BC as the one we observed for the samples included in this study.
While a direct comparison between both KPC detection approaches was not performed, it is clear that KPC confirmation through KPC-peak detection demonstrated higher sensitivity compared to the biomarker approach (which relied on detection of a ~11.109 Da peak). High sensitivity and specificity values for KPC prediction were reported for this peak in the United States [32,40] and Europe [33]. We previously observed a low sensitivity for KPC prediction using this biomarker in our region [24], which might be attributed to a different scenario for the circulation of the genetic platform responsible for its presence (Tn4401a). Undoubtedly, KPC-peak detection strategy shows a much higher sensitivity than the ~11.109 Da peak approach, at least for the set of samples evaluated in this study.
Additionally, we observed that while some samples contained non-KPC producing bacteria and exhibited spectra with background noise at the KPC m/z position, a clear visual distinction could still be made between these spectra and spectra with a clear KPC-peak. Although KPC m/z intensity could be used as a parameter to differentiate KPC producers from non-KPC producers [24,26], we believe visual inspection of spectra is still necessary, as automated softwares may not be able to distinguish between background noise and a true KPC-peak.
Unfortunately, NDM enzyme cannot yet be detected applying this methodology, probably due its inefficiency to extract membrane-anchored proteins [41].
As previously mentioned by Moreira et al. [38], it is important to highlight that equipment parameters should be tested and optimized in every MALDI-TOF spectrometer for KPC detection before analyzing patients´ samples. For this purpose, it would be ideal to evaluate control strains beforehand. In this study, we demonstrated successful detection of the KPC-peak using two different spectrometers, in two different hospitals. To obtain reproducible results, training of clinical laboratory staff would be relevant. We also recommend performing replicates of target spot loading, as results may vary between spots, due to possible differential protein co-crystallization.
We highlight the capacity of this protocol both to detect KPC presence and to identify the ethological agent from the same protein extract obtained with FA-ISO from BC, STC and COL. Protein extracts can be used for bacterial identification and detecting the ~11.109 Da peak by analyzing the low molecular weight range, as well as detecting the KPC-peak in the high molecular weight range, selecting the appropriate organic matrices and acquisition parameters. Also, this protocol can be implemented with commonly used chemical reagents and simple centrifugation and separation steps, making it an easy to perform methodology.
Ferulic acid matrix, previously reported for high molecular weight protein detection [32,33], could be used as an alternative organic matrix to detect KPC-peak at the high molecular weight range, as its performance was similar to sinapinic acid, giving more options to clinical laboratories in terms of available chemical reagents.
Clinical laboratories can incorporate this new rapid and simple methodology for KPC detection in selected samples, on a daily basis, based on local epidemiology. The method is easily implementable and can be used to test any bacterial culture suspected of carbapenemase production, thus expanding the already established utility of MALDI-TOF MS.
5. Conclusions
MALDI-TOF MS technology has significant potential in clinical settings for detecting antibiotic resistance, particularly in a multi-resistance global context. Once the spectrometer is acquired by the hospital or institution, this fast and effective MALDI-TOF MS protocol can quickly confirm KPC production, reducing the turnaround time compared to traditional phenotypic methods, optimizing the use of available antibiotics and improving patients´ prognosis. Healthcare settings could benefit from faster detection of resistance markers, thereby preserving available therapeutic options and reducing the spread of antibiotic resistance. In conclusion, this study represents the pioneering effort to directly detect KPC using MALD-TOF MS technology, conducted on patient-derived samples obtained at the hospitals for validation purposes.
Author Contributions
Conceptualization: A.C., R.F., G.G. and J.D.C.; methodology: A.C., R.F. and J.A.M.; formal analysis, data curation, writing—original draft preparation: A.C.; writing—review and editing: A.C.; R.F., G.G. and J.D.C.; funding acquisition: J.D.C. and G.G.; bacterial isolation from clinical samples: L.F.C, M.I.M., S.A.B., A.E.S., C.V., C.H.R. and M.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Agencia Nacional de Promoción Científica y Tecnológica PICT 2019-1879 to JDC, and PIP 2021 GI11220200102588CO to GG.
Institutional Review Board Statement
The study was approved by the Ethics Committee of Facultad de Farmacia y Bioquímica (Universidad de Buenos Aires) (RESCD-2020-134-E-UBA-DCT_FFYB, August 20th, 2020) for studies involving bacteria recovered from human clinical samples.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sulayyim, H.J.A.; Ismail, R.; Hamid, A.A.; Ghafar, N.A. Antibiotic Resistance during COVID-19: A Systematic Review. Int J Environ Res Public Health 2022, 19, 11931. [Google Scholar] [CrossRef]
- Livermore, D.M. Antibiotic resistance during and beyond COVID-19. J Antimicrob Chemother 2021, 3, i5–i16. [Google Scholar] [CrossRef] [PubMed]
- Halat, D.H.; Moubareck, C.A. The Current Burden of Carbapenemases: Review of Significant Properties and Dissemination among Gram-Negative Bacteria. Antibiotics 2020, 9, 186. [Google Scholar] [CrossRef]
- Tamma, P.D.; Simner, P.J. Phenotypic detection of carbapenemase producing organisms from clinical isolates. J Clin Microbiol 2018, 56, e01140–18. [Google Scholar] [CrossRef]
- Pires, J.; Novais, A.; Peixe, L. Blue-carba, an easy biochemical test for detection of diverse carbapenemase producers directly from bacterial cultures. J Clin Microbiol 2013, 51, 4281. [Google Scholar] [CrossRef] [PubMed]
- Osterblad, M.; Hakanen, a.J.; Jalava, J. Evaluation of the Carba NP test for carbapenemase detection. Antimicrob Agents Chemother 2014, 58, 7553–7556. [Google Scholar] [CrossRef]
- Maugeri, G.; Lychko, I.; Sobral, R.; Roque, A.C.A. Identification and Antibiotic-Susceptibility Profiling of Infectious Bacterial Agents: A Review of Current and Future Trends. Biotechnol J 2019, 14, e1700750. [Google Scholar] [CrossRef] [PubMed]
- Oviaño, M.; Bou, G. Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry for the Rapid Detection of Antimicrobial Resistance Mechanisms and Beyond. Clin Microbiol Rev 2019, 32. [Google Scholar] [CrossRef]
- Perez, F.; Bonomo, R.A. Carbapenem-Resistant Enterobacteriaceae: Global Action Required. Lancet Infect. Dis. 2019, 19, 561–562. [Google Scholar] [CrossRef]
- Lespada, M.I.; Córdova, E.; Roca, V.; Gómez, N.; Badía, M.; Rodriguez, C. Bacteremia caused by Klebsiella pneumoniae carbapenemase (KPC)-producing K. pneumoniae. A retrospective study of 7 years. Rev Esp Quimioter 2019, 32, 15–21. [Google Scholar]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; Gurka, D.; Kumar, A.; Cheang, M. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006, 34, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, A.T.A.; Wong, A.Y.W.; Özenci, V. The impact of delayed analysis of positive blood cultures on the performance of short-term culture followed by MALDI-TOF MS. J. Microbiol. Methods 2020, 177, 106027. [Google Scholar] [CrossRef] [PubMed]
- Nastro, M.; Ayora, M.; García, S.; Vay, C.; Famiglietti, A.; Rodriguez, C.H. Rapid Blue-Carba test: reduction in the detection time of carbapenemases performed from a 4-hour bacterial lawn. Journal of Chemotherapy 2017, 29, 150–153. [Google Scholar] [CrossRef]
- Liu, Q.; Liu. L.; Li. Y.; Chen, X.; Yan, Q.; Liu, W. Fecal Carriage and Epidemiology of Carbapenem-Resistant Enterobacteriaceae Among Hospitalized Patients in a University Hospital. Infection and Drug Resistance 2019, 12, 3935–3942. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Mangold, K.A.; Wyant, K.; Schora, D.M.; Voss, B.; Kaul, K.L.; Hayden, M.K.; Chundi, V.; Peterson, L.R. Rectal Screening for Klebsiella pneumoniae Carbapenemases: Comparison of Real-Time PCR and Culture Using Two Selective Screening Agar Plates. J Clin Microbiol 2012, 50, 2596–2600. [Google Scholar] [CrossRef]
- Moubareck, C.A.; Halat, D.H.; Sartawi, M.; Lawlor, K.; Sarkis, D.K.; Alatoom, A. Assessment of the performance of CHROMagar KPC and Xpert Carba-R assay for the detection of carbapenem-resistant bacteria in rectal swabs: First comparative study from Abu Dhabi, United Arab Emirates. J Global Antimicrob Res 2020, 20, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Mathema, B.; Chavda, K.D.; DeLeo, F.R.; Bonomo, R.A.; Kreiswirth, B.N. Carbapenemase-producing Klebsiella pneumoniae: molecular and genetic decoding. Trends Microbiol 2014, 22, 686–696. [Google Scholar] [CrossRef]
- Clark, A. E.; Kaleta, E.J.; Arora, A.; Wolk, D.M. Matrix-assisted laser desorption ionization-time of flight mass spectrometry: a fundamental shift in the routine practice of clinical microbiology. Clin Microbiol Rev 2013, 26, 547–603. [Google Scholar] [CrossRef]
- Li, D.; Yi, J.; Han, G.; Qiao, L. MALDI-TOF Mass Spectrometry in Clinical Analysis and Research. ACS Meas Sci Au 2022, 2, 385–404. [Google Scholar] [CrossRef]
- Torres-Sangiao, E.; Leal Rodriguez, C.; García-Riestra, C. Application and Perspectives of MALDI–TOF Mass Spectrometry in Clinical Microbiology Laboratories. Microorganisms 2021, 9, 1539. [Google Scholar] [CrossRef]
- Camara, J. E.; Hays, F. A. Discrimination between wild-type and ampicillin-resistant Escherichia coli by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Anal Bioanal Chem 2007, 389, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Papagiannitsis, C. C.; Kotsakis, S.D.; Tuma, Z.; Gniadkowski, M.; Miriagou, V.; Hrabak, J. Identification of CMY-2-type cephalosporinases in clinical isolates of Enterobacteriaceae by MALDI-TOF MS. Antimicrob Agents Chemother 2014, 58, 2952–2957. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, R. F.; Rumi, V.; Marchisio, M.; Cejas, D.; Radice, M.; Vay, C.; Barrios, R.; Gutkind, G.; Di Conza, J. Fast and easy detection of CMY-2 in Escherichia coli by direct MALDI-TOF mass spectrometry. J. Microbiol. Methods 2018, 148, 20–28. [Google Scholar] [CrossRef]
- Figueroa-Espinosa, R.; Costa, A.; Cejas, D.; Barrios, R.; Vay, C.; Radice, M.; Gutkind, G.; Di Conza, J. MALDI-TOF MS based procedure to detect KPC-2 directly from positive blood culture bottles and colonies. J. Microbiol. Methods 2019, 159, 120–127. [Google Scholar] [CrossRef]
- Figueroa-Espinosa, R.; Costa, A.; Cejas, D.; Magariños, F.; Nicola, F.; Rodriguez, C.H.; Vay, C.; Radice, M., Gutkind, G.; Di Conza, J. Ensayo preliminar para la detección de variantes de KPC- (KPC-2, KPC-3, KPC-8 y KPC-31) por espectrometría de masas MALDI-TOF a partir de aislamientos clínicos. In Proceedings of the Sociedad Argentina de Infectología Congress, Buenos Aires, Argentina, 25–27 October 2021.
- Tsakris, A.; Kristo, I.; Poulou, A.; Themeli-Digalaki, K.; Ikonomidis, A.; Petropoulou, D.; Pournaras, S.; Sofianou, D. Evaluation of boronic acid disk tests for differentiating KPC-possessing Klebsiella pneumoniae isolates in the clinical laboratory. J Clin Microbiol 2009, 47, 362–367. [Google Scholar] [CrossRef]
- Dominguez, J.E.; Redondo, L.M.; Figueroa Espinosa, R.A.; Cejas, D.; Gutkind, G.O.; Chacana, P.A.; Di Conza, J.A.; Fernandez Miyakawa, M.E. Simultaneous carriage of mcr-1 and other antimicrobial resistance determinants in Escherichia coli from poultry. Front Microbiol 2018, 9, 1679. [Google Scholar] [CrossRef] [PubMed]
- Madonna, A.J.; Basile, F.; Ferrer, I.; Meetani, M.A.; Rees, J.C.; Voorhees, K.J. On-probe sample pretreatment for the detection of proteins above 15 KDa from whole cell bacteria by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Rapid Commu. Mass Spectrom 2000, 14, 2220–2229. [Google Scholar] [CrossRef]
- Meetani, M.A.; Voorhees, K.J. MALDI Mass Spectrometry Analysis of High Molecular Weight Proteins from Whole Bacterial Cells: Pretreatment of Samples with Surfactants. J Am Soc Mass Spectrom 2005, 16, 1422–1426. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.B.; Lewinski, M.A.; Loeffelholz, M.J.; Tibbets, R.J. Verification and Validation of Procedures in the Clinical Microbiology Laboratory. Coordinating ed., S.E. Sharp. ASM Press, Washington, DC, United States of America, 2009; Cumitech31A.
- Red Nacional de Espectrometría de Masas aplicada al Laboratorio de Microbiología Clínica. Available online: http://www.anlis.gov.ar/renaem/ (accessed on 20 May 2023).
- Youn, J.H.; Drake, S.K.; Weingarten, R.A.; Frank, K.M.; Dekker, J.P.; Lau, A.F. Clinical performance of a matrix-assisted laser desorption ionization-time of flight mass spectrometry method for detection of certain blaKPC-containing plasmids. J. Clin. Microbiol. 2016, 54, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Gaibani, P.; Galea, A.; Fagioni, M.; Ambretti, S.; Sambri, V.; Landini, M.P. Evaluation of matrix-assisted laser desorption ionization-time of flight mass spectrometry for identification of KPC-producing Klebsiella pneumoniae. J. Clin. Microbiol. 2016, 54, 2609–2613. [Google Scholar] [CrossRef]
- Centonze, A.R.; Bertoncelli, A.; Savio, C.; Orza, P.; Bedenic, B.; Mazzariol, A. Evaluation of rapid KPC carbapenemase detection method based on MALDI-TOF VITEK MS spectra analysis. J. Med. Microbiol. 2018, 67, 1474–1479. [Google Scholar] [CrossRef] [PubMed]
- Ketterlinus, R.; Hsieh, S.; Teng, S.; Lee, H.; Pusch, W. Fishing for biomarkers: analyzing mass spectrometry data with the new ClinProTools software. Biotechniques 2005, 38, 37–40. [Google Scholar] [CrossRef]
- CLSI, 2023. Performance standards for antimicrobial susceptibility testing. In: 33rd Informational Supplement M100. USACLSI, Wayne, PA 2023.
- Moreira, N.K.; Wilhelm, C.M.; Wink, P.L.; Barth, A.L.; Caierão. MALDI-TOF mass spectrometry for direct KPC detection among Enterobacterales. Brazilian Jour of Microbiol published online. 2022. [CrossRef]
- Moreira, N.K.; Wilhelm, C.M.; Echevarria, A.D.; Volpato, F.C.Z.; Wink, P.L.; Barth, A.L.; Caierão, J. Direct Detection of KPC Peak from Positive Blood Cultures Using MALDI-TOF MS: Are We There Yet? Antibiotics 2023, 12, 601. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E-J.; Lee, E. H.; Hwang, D. H.; Lee, H.; Baek, J-H.; Jeong, S. H. Direct detection of intact Klebsiella pneumoniae carbapenemases produced by Enterobacterales using MALDI-TOF MS. J Antimicrob Chemother 2020, 75, 1174–1181. [CrossRef]
- Lau, A. F.; Wang, H.; Weingarten, R.A.; Drake, S. K.; Suffredini, A. F; Garfield, M. K.; Chen, Y.; Gucek, M.; Youn, J-H.; Stock, F.; Tso, H.; DeLeo, J.; Cimino, J. J.; Frank, K. M.; Dekker, J. P. A Rapid Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry-Based Method for Single-Plasmid Tracking in an Outbreak of Carbapenem-Resistant Enterobacteriaceae. J. Clin. Microbiol. 2014, 52, 2804–2812. [CrossRef]
- González, L.J.; Bahr, G.; Nakashige, T.G.; Nolan, E.M.; Bonomo, R.A.; Vila, A.J. Membrane-anchoring stabilizes and favors secretion of New Delhi Metallo-β-lactamase. Nat Chem Biol 2016, 12, 516–522. [Google Scholar] [CrossRef]
Figure 1.
Control strains spectra. Recombinant strains spectra expressing (a) KPC-2 or (b) KPC-3 are shown in red and receptor strains spectra are shown in blue (E. coli TOP10) and green (E. coli TOP10+pK19).
Figure 1.
Control strains spectra. Recombinant strains spectra expressing (a) KPC-2 or (b) KPC-3 are shown in red and receptor strains spectra are shown in blue (E. coli TOP10) and green (E. coli TOP10+pK19).
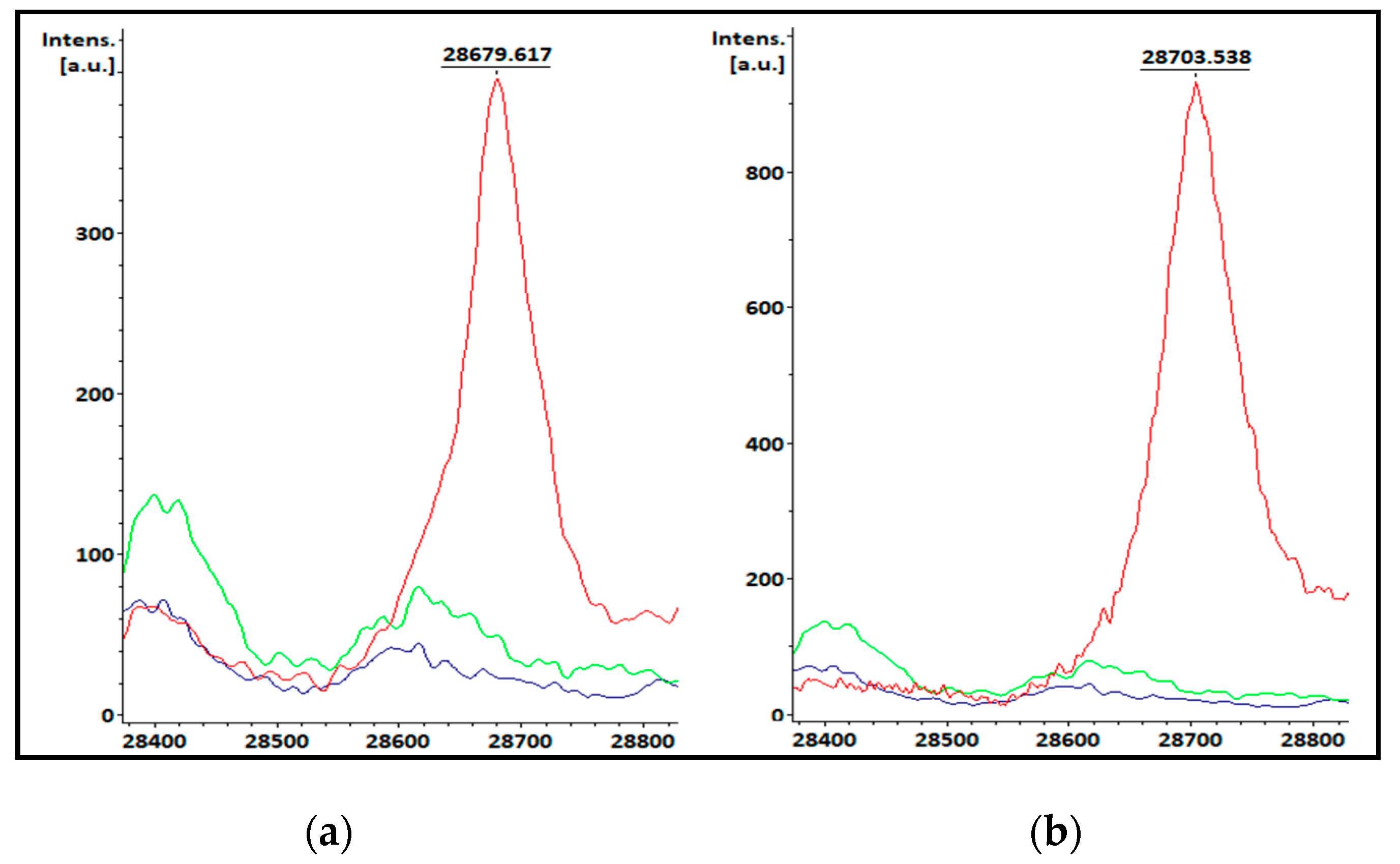
Figure 2.
Spectra obtained from (a) patients’ positive BC bottles; (b) STC, (c) COL. KPC peaks on KPC producers’ spectra are shown in red and spectra from samples containing non-KPC producing bacteria are shown in blue. The KPC m/z value of one spectrum is displayed as an example.
Figure 2.
Spectra obtained from (a) patients’ positive BC bottles; (b) STC, (c) COL. KPC peaks on KPC producers’ spectra are shown in red and spectra from samples containing non-KPC producing bacteria are shown in blue. The KPC m/z value of one spectrum is displayed as an example.
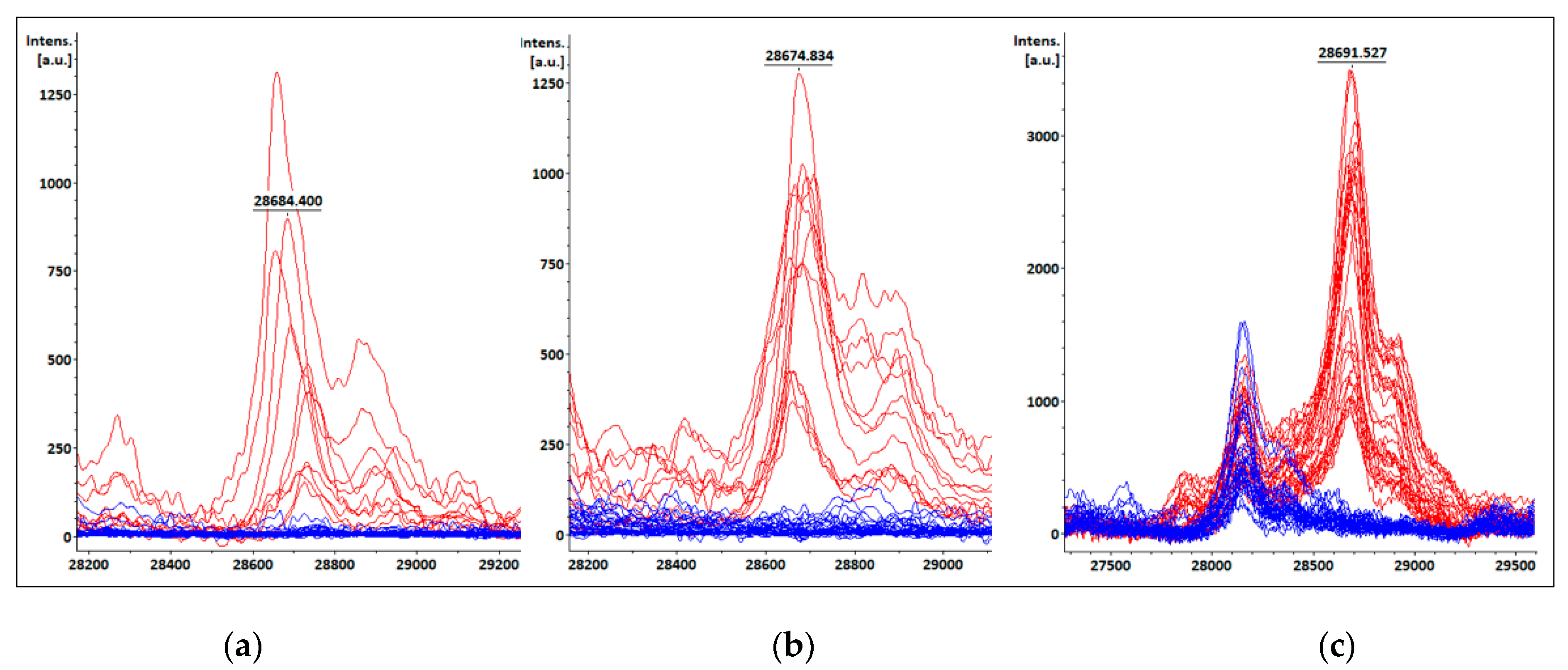
Figure 3.
Box plots showing median and interquartile range 95% for spectra intensities at KPC m/z obtained from (a) BC, (b) STC and (c) COL. Intensities for KPC m/z of spectra obtained from samples containing KPC producers and non-KPC producers are shown in red and blue boxes, respectively. KPC m/z shown value corresponds to the median calculated for every type of sample.
Figure 3.
Box plots showing median and interquartile range 95% for spectra intensities at KPC m/z obtained from (a) BC, (b) STC and (c) COL. Intensities for KPC m/z of spectra obtained from samples containing KPC producers and non-KPC producers are shown in red and blue boxes, respectively. KPC m/z shown value corresponds to the median calculated for every type of sample.
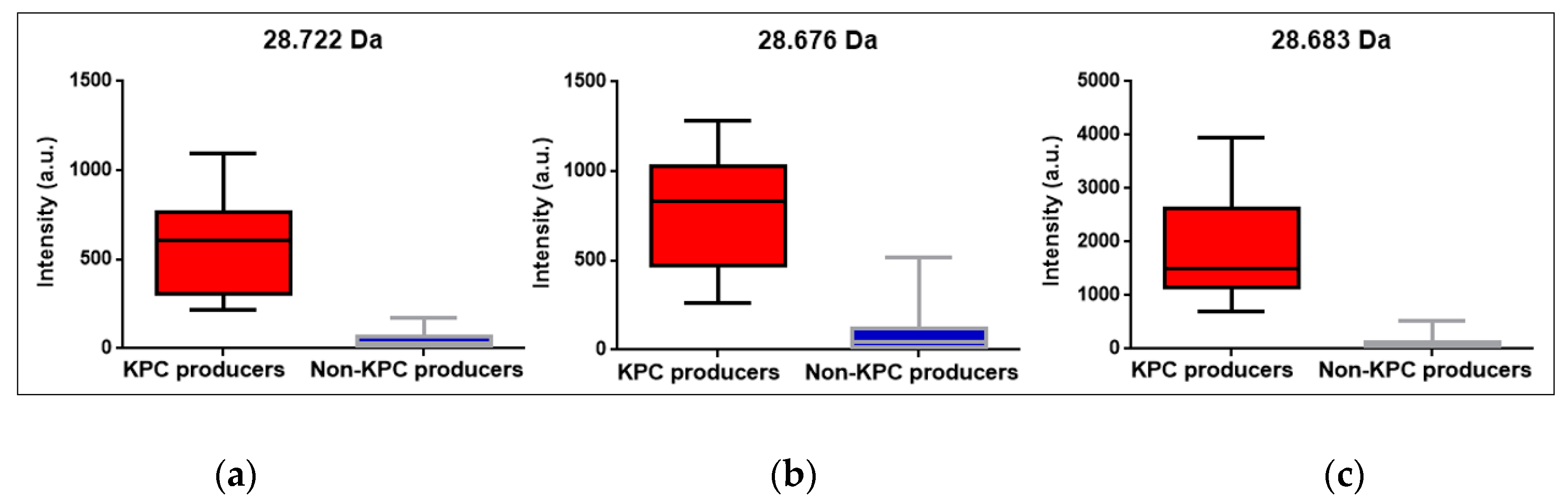
Figure 4.
Comparison of spectra after target spot loading with (a) SA and (b) FA. KPC-producers’ spectra are shown in red (red) and non-KPC producers’ spectra are shown in blue. The KPC m/z value of one spectrum is displayed as an example.
Figure 4.
Comparison of spectra after target spot loading with (a) SA and (b) FA. KPC-producers’ spectra are shown in red (red) and non-KPC producers’ spectra are shown in blue. The KPC m/z value of one spectrum is displayed as an example.
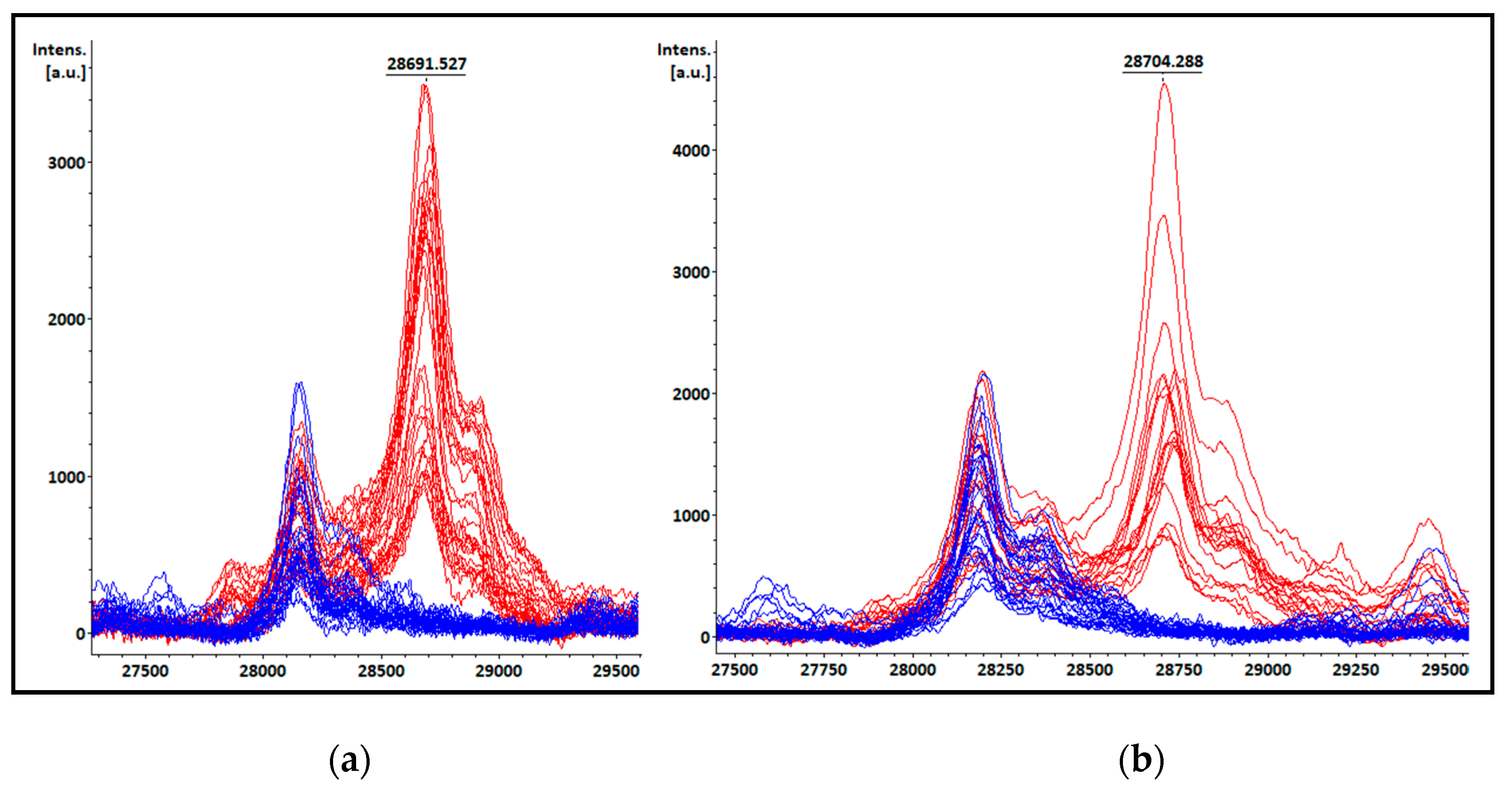
Figure 5.
Comparison of turnaround time for phenotypic KPC confirmation methodologies (black lines) and MALDI-TOF MS detection with FA-ISO extraction method (blue lines) from positive blood culture bottles, short-term cultures and colonies.
Figure 5.
Comparison of turnaround time for phenotypic KPC confirmation methodologies (black lines) and MALDI-TOF MS detection with FA-ISO extraction method (blue lines) from positive blood culture bottles, short-term cultures and colonies.
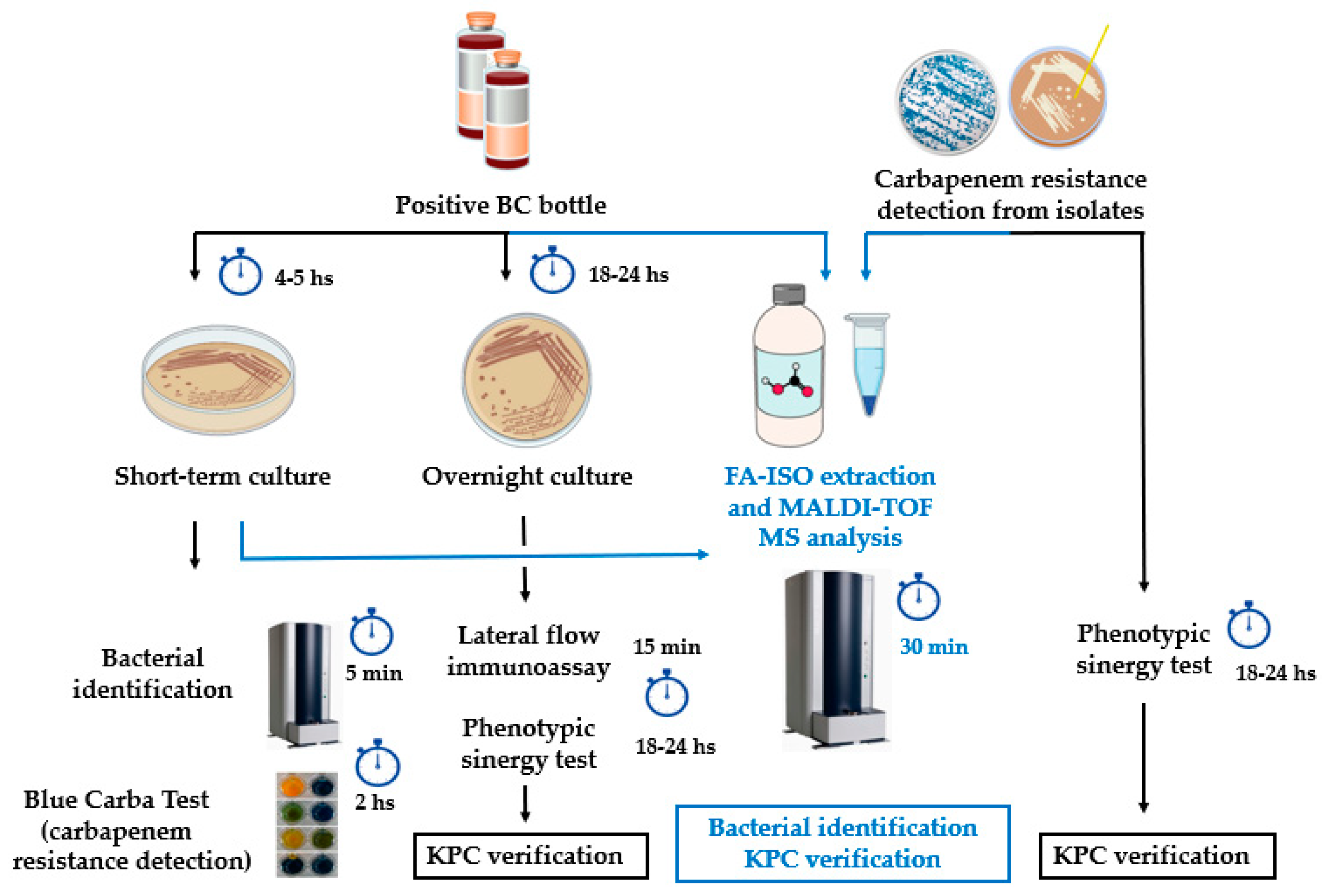

Table 1.
Bacterial isolates evaluated from simulated positive blood cultures, short-term cultures and isolated colonies.
Table 1.
Bacterial isolates evaluated from simulated positive blood cultures, short-term cultures and isolated colonies.
| Species | Total isolates | KPC producing isolates | Non-KPC producing isolates |
|---|---|---|---|
| Simulated positive blood cultures and short-term cultures | |||
| K. pneumoniae | 60 | 32 | 28 |
| E. coli | 33 | 5 | 28 |
| TOTAL | 93 | 37 | 56 |
| Isolated colonies | |||
| K. pneumoniae | 60 | 39 | 21 |
| E. coli | 28 | 4 | 24 |
| E. cloacae complex | 12 | 7 | 5 |
| C. braakii | 3 | 1 | 2 |
| S. marcescens | 15 | 4 | 11 |
| TOTAL | 118 | 55 | 63 |
Table 2.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from patients´ positive BC bottles. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
Table 2.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from patients´ positive BC bottles. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
| Sample | Hospital routine ID | ID from BC | KPC peak m/z from BC (Da) |
Intensity (a.u.) |
Peak at m/z ~11.109 Da |
Resistance markers |
|---|---|---|---|---|---|---|
| 1HD02 | K. pneumoniae | K. pneumoniae | 28.687 | 762 | (+) | blaKPC-2 |
| 1HD19 | K. pneumoniae | K. pneumoniae | 28.722 | 221 | Absent | blaKPC-2 |
| 1HD21 | K. pneumoniae | K. pneumoniae | 28.655 | 1095 | (+) | blaKPC-2 |
| 1HD22 | K. pneumoniae | K. pneumoniae | 28.660 | 613 | (+) | blaKPC-2 |
| HD63 | K. pneumoniae | K. pneumoniae | 28.736 | 355 | Absent | blaKPC-2 |
| HD64 | K. pneumoniae | K. pneumoniae | 28.725 | 311 | Absent | blaKPC-2 |
| HD65 | K. pneumoniae | K. pneumoniae | 28.740 | 610 | Absent | blaKPC-2 |
| 1HD03* | K. pneumoniae | NRI | NA | NA | NA | blaKPC-2 |
| HD01 | K. pneumoniae | K. pneumoniae | Absent | 27 | Absent | NCD |
| HD02 | K. pneumoniae | K. pneumoniae | Absent | 130 | Absent | NCD |
| HD03 | K. pneumoniae | K. pneumoniae | Absent | 50 | Absent | NCD |
| HD04 | K. pneumoniae | K. pneumoniae | Absent | 40 | Absent | NCD |
| HD06 | K. pneumoniae | K. pneumoniae | Absent | 11 | Absent | NCD |
| HD07 | K. pneumoniae | K. pneumoniae | Absent | 0 | Absent | NCD |
| HD08 | E. coli | E. coli | Absent | 0 | Absent | NCD |
| HD10 | E. coli | E. coli | Absent | 30 | Absent | NCD |
| HD11 | E. coli | E. coli | Absent | 33 | Absent | NCD |
| HD12 | E. coli | E. coli | Absent | 28 | Absent | NCD |
| HD14 | E. coli | E. coli | Absent | 80 | Absent | NCD |
| HD15 | K. pneumoniae | K. pneumoniae | Absent | 154 | Absent | NCD |
| HD16 | E. coli | E. coli | Absent | 24 | Absent | NCD |
| HD18 | E. coli | E. coli | Absent | 143 | Absent | NCD |
| HD20* | E. coli | NRI | NA | NA | NA | NCD |
| HD21 | E. coli | E. coli | Absent | 62 | Absent | NCD |
| HD22 | E. coli | E. coli | Absent | 69 | Absent | NCD |
| HD23 | K. pneumoniae | K. variicola | Absent | 0 | Absent | NCD |
| HD24 | K. pneumoniae | K. pneumoniae | Absent | 20 | Absent | NCD |
| HD25* | K. pneumoniae | NRI | NA | NA | NA | NCD |
| HD26* | E. coli | NRI | NA | NA | NA | NCD |
| HD27* | K. pneumoniae | NRI | NA | NA | NA | NCD |
| HD28 | E. coli | E. coli | Absent | 34 | Absent | NCD |
| HD29 | E. coli | E. coli | Absent | 78 | Absent | NCD |
| HD30 | E. coli | E. coli | Absent | 8 | Absent | NCD |
| HD33 | K. pneumoniae | K. variicola | Absent | 106 | Absent | NCD |
| HD35 | P. mirabilis | P. mirabilis | Absent | 88 | Absent | NCD |
| HD36 | E. coli | E. coli | Absent | 125 | Absent | NCD |
| HD40 | K. pneumoniae | K. pneumoniae | Absent | 65 | Absent | NCD |
| HD42 | E. coli | E. coli | Absent | 33 | Absent | NCD |
| HD43 | E. coli | E. coli | Absent | 122 | Absent | NCD |
| HD44 | E. coli | E. coli | Absent | 68 | Absent | NCD |
| HD45 | E. coli | E. coli | Absent | 6 | Absent | NCD |
| HD47 | K. pneumoniae | K. pneumoniae | Absent | 71 | Absent | NCD |
| HD48 | K. pneumoniae | K. pneumoniae | Absent | 55 | Absent | NCD |
| HD49 | K. pneumoniae | K. pneumoniae | Absent | 69 | Absent | NCD |
| HD50 | K. pneumoniae | K. pneumoniae | Absent | 29 | Absent | NCD |
| HD51 | K. pneumoniae | K. pneumoniae | Absent | 87 | Absent | NCD |
| HD52* | K. pneumoniae | NRI | NA | NA | NA | NCD |
| HD53 | E. coli | E. coli | Absent | 29 | Absent | NCD |
| HD54 | K. variicola | K. pneumoniae | Absent | 15 | Absent | NCD |
| HD56 | K. pneumoniae | K. pneumoniae | Absent | 97 | Absent | NCD |
| HD57 | K. pneumoniae | K. pneumoniae | Absent | 64 | Absent | NCD |
| HD59 | E. cloacae complex | E. hormaechei | Absent | 176 | Absent | NCD |
| HD61 | E. coli | E. coli | Absent | 21 | Absent | NCD |
| HD62 | E. coli | E. coli | Absent | 24 | Absent | NCD |
| 1HD01* | E. cloacae complex | NRI | NA | NA | NA | NCD |
| 1HD04 | S. marcescens | S. marcescens | Absent | 7 | Absent | NCD |
| 1HD05 | S. marcescens | S. marcescens | Absent | 20 | Absent | NCD |
| 1HD06 | K. pneumoniae | K. pneumoniae | Absent | 2 | Absent | NCD |
| 1HD07 | K. pneumoniae | K. pneumoniae | Absent | 7 | Absent | NCD |
| 1HD08 | K. pneumoniae | K. pneumoniae | Absent | 7 | Absent | blaNDM |
| 1HD09 | E. coli | E. coli | Absent | 7 | Absent | NCD |
| 1HD10 | E. coli | E. coli | Absent | 8 | Absent | NCD |
| 1HD11 | K. pneumoniae | K. pneumoniae | Absent | 7 | Absent | blaNDM |
| 1HD12 | K. pneumoniae | K. pneumoniae | Absent | 5 | Absent | blaNDM |
| 1HD13 | K. pneumoniae | K. pneumoniae | Absent | 6 | Absent | blaNDM |
| 1HD14 | K. pneumoniae | K. pneumoniae | Absent | 5 | Absent | blaNDM |
| 1HD15 | K. pneumoniae | K. pneumoniae | Absent | 47 | Absent | blaNDM |
| 1HD16 | K. pneumoniae | K. pneumoniae | Absent | 55 | Absent | blaNDM |
| 1HD17 | S. marcescens | S. marcescens | Absent | 11 | Absent | NCD |
| 1HD18 | S. marcescens | S. marcescens | Absent | 46 | Absent | NCD |
| 1HD20 | K. pneumoniae | K. pneumoniae | Absent | 14 | Absent | NCD |
| 1HD23 | K. pneumoniae | K. pneumoniae | Absent | 9 | Absent | NCD |
| 1HD24 | K. pneumoniae | K. pneumoniae | Absent | 12 | Absent | blaNDM |
| 1HD25 | K. pneumoniae | K. pneumoniae | Absent | 4 | Absent | blaNDM |
| 1HD26 | K. pneumoniae | K. pneumoniae | Absent | 12 | Absent | blaNDM |
| 1HD27 | S. marcescens | S. marcescens | Absent | 11 | Absent | NCD |
| 1HD28 | K. pneumoniae | K. pneumoniae | Absent | 6 | Absent | NCD |
| 1HD29 | K. pneumoniae | K. pneumoniae | Absent | 9 | Absent | NCD |
*Samples not included in statistical analysis for KPC peak detection due to failed identification result, indicating a low efficiency in protein extraction process. Samples beginning with “1HD” and “HD” were analyzed at Hospital de Clínicas and Hospital Alemán, respectively. ID: bacterial identification, BC: blood culture, NRI: not reliable identification (score<1,4), a.u.: arbitrary units, NA: not applicable, NCD: no carbapenemase genes detected (blaKPC/blaNDM).
Table 3.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from STC. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
Table 3.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from STC. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
| Sample | Hospital routine ID | ID from STC | KPC peak m/z from STC (Da) |
Intensity (a.u.) |
Peak at m/z ~11.109 Da |
Resistance markers |
|---|---|---|---|---|---|---|
| 1HC02 | K. pneumoniae | K. pneumoniae | 28.686 | 1031 | (+) | blaKPC-2 |
| 1HC03 | K. pneumoniae | K. pneumoniae | 28.679 | 1013 | (+) | blaKPC-2 |
| 1HC19 | K. pneumoniae | K. pneumoniae | 28.728 | 1283 | Absent | blaKPC-2 |
| 1HC21 | K. pneumoniae | K. pneumoniae | 28.675 | 823 | (+) | blaKPC-2 |
| 1HC22 | K. pneumoniae | K. pneumoniae | 28.675 | 848 | Absent | blaKPC-2 |
| HC63 | K. pneumoniae | K. pneumoniae | 28.660 | 637 | Absent | blaKPC-2 |
| HC64 | K. pneumoniae | K. pneumoniae | 28.662 | 415 | Absent | blaKPC-2 |
| HC65 | K. pneumoniae | K. pneumoniae | 28.676 | 261 | Absent | blaKPC-2 |
| HC01 | K. pneumoniae | K. pneumoniae | Absent | 49 | Absent | NCD |
| HC02 | K. pneumoniae | K. pneumoniae | Absent | 102 | Absent | NCD |
| HC03 | K. pneumoniae | K. pneumoniae | Absent | 117 | Absent | NCD |
| HC04 | K. pneumoniae | K. pneumoniae | Absent | 70 | Absent | NCD |
| HC06 | K. pneumoniae | K. pneumoniae | Absent | 427 | Absent | NCD |
| HC07 | K. pneumoniae | K. pneumoniae | Absent | 18 | Absent | NCD |
| HC08 | E. coli | E. coli | Absent | 149 | Absent | NCD |
| HC10 | E. coli | E. coli | Absent | 24 | Absent | NCD |
| HC11 | E. coli | E. coli | Absent | 103 | Absent | NCD |
| HC12 | E. coli | E. coli | Absent | 50 | Absent | NCD |
| HC14 | E. coli | E. coli | Absent | 45 | Absent | NCD |
| HC15 | K. pneumoniae | K. pneumoniae | Absent | 121 | Absent | NCD |
| HC16 | E. coli | E. coli | Absent | 47 | Absent | NCD |
| HC18 | E. coli | E. coli | Absent | 37 | Absent | NCD |
| HC20 | E. coli | E. coli | Absent | 23 | Absent | NCD |
| HC21 | E. coli | E. coli | Absent | 124 | Absent | NCD |
| HC22 | E. coli | E. coli | Absent | 39 | Absent | NCD |
| HC23 | K. pneumoniae | K. variicola | Absent | 405 | Absent | NCD |
| HC24 | K. pneumoniae | K. variicola | Absent | 445 | Absent | NCD |
| HC25 | K. pneumoniae | K. variicola | Absent | 192 | Absent | NCD |
| HC26 | E. coli | E. coli | Absent | 48 | Absent | NCD |
| HC27 | K. pneumoniae | K. variicola | Absent | 63 | Absent | NCD |
| HC28 | E. coli | E. coli | Absent | 45 | Absent | NCD |
| HC29 | E. coli | E. coli | Absent | 334 | Absent | NCD |
| HC30 | E. coli | E. coli | Absent | 112 | Absent | NCD |
| HC33 | K. pneumoniae | K. variicola | Absent | 22 | Absent | NCD |
| HC35 | P. mirabilis | P. mirabilis | Absent | 158 | Absent | NCD |
| HC36 | E. coli | E. coli | Absent | 311 | Absent | NCD |
| HC40 | K. pneumoniae | K. pneumoniae | Absent | 329 | Absent | NCD |
| HC42 | E. coli | E. coli | Absent | 163 | Absent | NCD |
| HC43 | E. coli | E. coli | Absent | 116 | Absent | NCD |
| HC44 | E. coli | E. coli | Absent | 106 | Absent | NCD |
| HC45 | E. coli | E. coli | Absent | 330 | Absent | NCD |
| HC47 | K. pneumoniae | K. pneumoniae | Absent | 52 | Absent | NCD |
| HC48 | K. pneumoniae | K. pneumoniae | Absent | 157 | Absent | NCD |
| HC49 | K. pneumoniae | K. pneumoniae | Absent | 60 | Absent | NCD |
| HC50 | K. pneumoniae | K. pneumoniae | Absent | 103 | Absent | NCD |
| HC51 | K. pneumoniae | K. pneumoniae | Absent | 93 | Absent | NCD |
| HC52 | K. pneumoniae | K. pneumoniae | Absent | 15 | Absent | NCD |
| HC53 | E. coli | E. coli | Absent | 3 | Absent | NCD |
| HC54 | K. variicola | K. variicola | Absent | 10 | Absent | NCD |
| HC56 | K. pneumoniae | K. pneumoniae | Absent | 111 | Absent | NCD |
| HC57 | K. pneumoniae | K. pneumoniae | Absent | 265 | Absent | NCD |
| HC59 | E. cloacae complex | E hormaechei | Absent | 520 | Absent | NCD |
| HC61 | E. coli | E. coli | Absent | 13 | Absent | NCD |
| HC62 | E. coli | E. coli | Absent | 30 | Absent | NCD |
| 1HC01 | E. cloacae complex | E. cloacae | Absent | 13 | Absent | NCD |
| 1HC04 | S. marcescens | S. marcescens | Absent | 4 | Absent | NCD |
| 1HC05 | S. marcescens | S. ureilytica | Absent | 11 | Absent | NCD |
| 1HC06 | K. pneumoniae | K. pneumoniae | Absent | 2 | Absent | NCD |
| 1HC07 | K. pneumoniae | K. pneumoniae | Absent | 3 | Absent | NCD |
| 1HC08 | K. pneumoniae | K. pneumoniae | Absent | 5 | Absent | blaNDM |
| 1HC09 | E. coli | E. coli | Absent | 16 | Absent | NCD |
| 1HC10 | E. coli | E. coli | Absent | 9 | Absent | NCD |
| 1HC11 | K. pneumoniae | K. pneumoniae | Absent | 7 | Absent | blaNDM |
| 1HC12 | K. pneumoniae | K. pneumoniae | Absent | 13 | Absent | blaNDM |
| 1HC13 | K. pneumoniae | K. pneumoniae | Absent | 0 | Absent | blaNDM |
| 1HC14 | K. pneumoniae | K. pneumoniae | Absent | 13 | Absent | blaNDM |
| 1HC15 | K. pneumoniae | K. pneumoniae | Absent | 94 | Absent | blaNDM |
| 1HC16 | K. pneumoniae | K. pneumoniae | Absent | 62 | Absent | blaNDM |
| 1HC17 | S. marcescens | S. marcescens | Absent | 38 | Absent | NCD |
| 1HC18 | S. marcescens | S. marcescens | Absent | 9 | Absent | NCD |
| 1HC20 | K. pneumoniae | K. pneumoniae | Absent | 34 | Absent | NCD |
| 1HC23 | K. pneumoniae | K. pneumoniae | Absent | 25 | Absent | NCD |
| 1HC24 | K. pneumoniae | K. pneumoniae | Absent | 46 | Absent | blaNDM |
| 1HC25 | K. pneumoniae | K. pneumoniae | Absent | 91 | Absent | blaNDM |
| 1HC26 | K. pneumoniae | K. pneumoniae | Absent | 83 | Absent | blaNDM |
| 1HC27 | S. marcescens | S. marcescens | Absent | 31 | Absent | NCD |
| 1HC28 | K. pneumoniae | K. pneumoniae | Absent | 9 | Absent | NCD |
| 1HC29 | K. pneumoniae | K. pneumoniae | Absent | 16 | Absent | NCD |
Samples beginning with “1HC” and “HC” were analyzed at Hospital de Clínicas and Hospital Alemán, respectively. ID: bacterial identification, STC: short-term culture, a.u.: arbitrary units, NCD: no carbapenemase genes detected (blaKPC/blaNDM).
Table 4.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from COL. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
Table 4.
Bacterial identification, KPC peak m/z and intensity of spectra after visual analysis from COL. KPC mass value and intensities correspond to the average m/z for both spectra duplicates. Spectra intensities for KPC non-producing isolates were calculated considering the position of KPC-peak m/z for KPC producing isolates median.
| Sample | Hospital routine ID | ID from COL | KPC peak m/z from COL (Da) |
Intensity (a.u.) |
Peak at m/z ~11.109 Da |
Resistance markers |
|---|---|---|---|---|---|---|
| POR02 | K. pneumoniae | K. pneumoniae | 28.662 | 1734 | (+) | blaKPC-2, blaNDM |
| POR03 | K. pneumoniae | K. pneumoniae | 28.685 | 1203 | (+) | blaKPC-2, blaNDM |
| POR06 | K. pneumoniae | K. pneumoniae | 28.712 | 735 | (+) | blaKPC-3 |
| POR08 | K. pneumoniae | K. pneumoniae | 28.679 | 1158 | (+) | blaKPC-2 |
| POR09 | K. pneumoniae | K. pneumoniae | 28.710 | 1227 | (+) | blaKPC-3 |
| POR11 | K. pneumoniae | K. pneumoniae | 28.686 | 3184 | (+) | blaKPC-2, blaNDM |
| POR14 | K. pneumoniae | K. pneumoniae | 28.716 | 2567 | (+) | blaKPC-3 |
| POR15 | K. pneumoniae | K. pneumoniae | 28.704 | 2829 | (+) | blaKPC-2, blaNDM |
| POR16 | K. pneumoniae | K. pneumoniae | 28.676 | 3949 | (+) | blaKPC-2, blaNDM |
| POR17 | K. pneumoniae | K. pneumoniae | 28.681 | 2386 | (+) | blaKPC-2, blaNDM |
| POR18 | K. pneumoniae | K. pneumoniae | 28.687 | 2555 | (+) | blaKPC-3 |
| POR21 | K. pneumoniae | K. pneumoniae | 28.706 | 2963 | (+) | blaKPC-3 |
| POR23 | K. pneumoniae | K. pneumoniae | 28.685 | 1086 | (+) | blaKPC-2 |
| POR29 | K. pneumoniae | K. pneumoniae | 28.675 | 727 | Absent | blaKPC-2, blaNDM |
| UC16 | K. pneumoniae | K. pneumoniae | 28.668 | 1321 | (+) | blaKPC-2 |
| UC24 | K. pneumoniae | K. pneumoniae | 28.677 | 1095 | Absent | blaKPC-2 |
| UC75 | K. pneumoniae | K. pneumoniae | 28.675 | 1546 | (+) | blaKPC-2 |
| COL65 | K. pneumoniae | K. pneumoniae | 28.680 | 1461 | Absent | blaKPC-2 |
| POR01 | K. pneumoniae | K. pneumoniae | Absent | 120 | Absent | blaNDM |
| POR04 | K. pneumoniae | K. pneumoniae | Absent | 211 | Absent | blaNDM |
| POR07 | K. pneumoniae | K. pneumoniae | Absent | 4 | Absent | blaNDM |
| POR10 | K. pneumoniae | K. pneumoniae | Absent | 29 | Absent | blaNDM |
| POR19 | K. pneumoniae | K. pneumoniae | Absent | 519 | Absent | blaNDM |
| POR20 | K. pneumoniae | K. pneumoniae | Absent | 72 | Absent | blaNDM |
| POR22 | K. pneumoniae | K. pneumoniae | Absent | 403 | Absent | blaNDM |
| POR26 | K. pneumoniae | K. pneumoniae | Absent | 17 | Absent | blaNDM |
| POR27 | K. pneumoniae | K. pneumoniae | Absent | 105 | Absent | blaNDM |
| POR28 | K. pneumoniae | K. pneumoniae | Absent | 74 | Absent | blaNDM |
| POR30 | K. pneumoniae | K. pneumoniae | Absent | 27 | Absent | blaNDM |
| UC20 | K. pneumoniae | K. pneumoniae | Absent | 65 | Absent | blaNDM |
| UC40 | K. pneumoniae | K. pneumoniae | Absent | 58 | Absent | blaIMP |
| UC42 | K. pneumoniae | K. pneumoniae | Absent | 60 | Absent | blaNDM |
| UC47 | K. pneumoniae | K. pneumoniae | Absent | 140 | Absent | blaNDM |
| UC76 | K. pneumoniae | K. pneumoniae | Absent | 20 | Absent | blaNDM |
| UC104 | K. pneumoniae | K. pneumoniae | Absent | 67 | Absent | blaIMP |
| UC105 | K. pneumoniae | K. pneumoniae | Absent | 73 | Absent | blaNDM |
| UC107 | P. mirabilis | P. mirabilis | Absent | 18 | Absent | blaNDM |
All COL samples were analyzed at Hospital Alemán. ID: bacterial identification, COL: isolated colonies, a.u.: arbitrary units.
Table 5.
Overall statistical results and comparison of calculated parameters for each type of sample (BC, STC and COL).
Table 5.
Overall statistical results and comparison of calculated parameters for each type of sample (BC, STC and COL).
| Parameter | Positive BC | STC | COL | Overall |
|---|---|---|---|---|
| KPC m/z median |
28.722 Da CI95%: [28.655 Da; 28.740 Da] |
28.676 Da CI95%: [28.660 Da; 28.728 Da] |
28.683 Da CI95%: [28.676 Da; 28.698 Da] |
28.681 Da CI95%: [28.676 Da; 28.687 Da] |
|
KPC m/z intensity median and range (KPC producers) |
610 a.u. (221 a.u. - 1095 a.u.) |
835,5 a.u. (261 a.u. - 1283 a.u.) |
1503,5 a.u. (727 a.u. - 3949 a.u.) |
1095 a.u. (221 a.u. - 3949 a.u.) |
|
KPC m/z intensity median and range (non-KPC producers) |
27,5 a.u. (0 a.u. - 176 a.u.) |
48,5 a.u. (0 a.u. - 520 a.u.) |
67 a.u. (4 a.u. - 519 a.u.) |
46 a.u. (0 a.u. - 520 a.u.) |
| KPC detection sensibility |
100% CI95%: [77%; 100%] |
100% CI95%: [79%; 100%] |
100% CI95%: [90%; 100%] |
100% CI95%: [95%; 100%] |
| KPC detection specificity |
100% CI95%: [97%; 100%] |
100% CI95%: [97%; 100%] |
100% CI95%: [91%; 120%] |
100% CI95%: [99%; 100%] |
BC: blood culture, STC: short-term culture, COL: isolated colonies, a.u.: arbitrary units.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



