Submitted:
30 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
Cognitive biases towards disorder-specific stimuli are suggested to be crucial in the development and maintenance of symptoms in adults with functional gastrointestinal disorders (FGID). Functional abdominal pain disorders (FAPD), a subtype of FGID, are common in children and adolescents, but the influence of cognitive biases is sparsely examined. The aim of this study was to 1) develop a new experimental design for assessing cognitive biases towards gastrointestinal stimuli in children and adolescents (age 8-17 years) and 2) test its feasibility on a healthy sample exploring potential sex- and age-related differences. The online experimental design – BY-FAP (Bias in Youth with Functional Abdominal Pain) includes a word task and a picture task. Stimuli in both tasks are related to general and gastrointestinal symptoms and the design includes three phases: 1) encoding, 2) free recall and 3) recognition. Results from 96 healthy participants (Mage = 12.3, 47.9% female) found no significant difference between sex or age groups in recall and recognition of either words or pictures. The results support that the design is feasible for children and adolescents. In the future, BY-FAP can be used to explore possible cognitive biases in children and adolescents with FAPD.
Keywords:
Adolescent
; children
; cognitive bias
; functional abdominal pain disorder
; functional gastrointestinal disorders
; interpretation bias
; memory bias
1. Introduction
Cognitive biases refer to abnormalities in attention, interpretation and memory of specific stimuli, for instance showing selective attention to negative information [1]. These biases are suggested to influence the development, maintenance and recurrence of symptoms in various disorders, such as anxiety, depression and functional disorders (FD) [1-3]. The latter is an umbrella term for disorders characterized by certain patterns of unspecific somatic symptoms that cannot be explained by a well-defined organic or psychiatric disorder [4, 5]. The aetiological mechanisms of FD are suggested to be multi-factorial involving both the body and brain [4, 5] including a symptom-focused attentional bias [3] and a lower threshold for detection of symptoms [6].
Cognitive biases can be explored in experimental studies, where participants' attention, interpretation or memory of specific stimuli, e.g. pictures or words, are assessed. A range of tasks using these principles exist, for example the dot probe task [7], the Health Norms Sorting Task (HNST) [8] or the Implicit Association Task [9]. In patient populations, biases are often present for disorder-specific stimuli [10]. For instance, patients with irritable bowel syndrome (IBS), a subtype of FD, show attentional biases specifically towards gastrointestinal-related words, whereas patients with anxiety show attentional bias for threat-related words [2, 11]. Not only the theme of the stimuli is important, but the best type of stimuli may also depend on the disorder being explored. In chronic fatigue syndrome (CFS), another subtype of FD, studies have found attentional bias for word stimuli, but not for pictorial stimuli [10]. In contrast, pictorial stimuli have been suggested to be more favourable for assessing cognitive biases in studies on health anxiety [12, 13].
A common limitation in most prior studies is that biases in attention, interpretation or memory are examined separately although it has been suggested that they interact. Hirsch et al. proposed the combined bias hypothesis, suggesting that cognitive biases at different levels interact to maintain symptoms of a disorder [14]. Thus, examining cognitive biases together, rather than in isolation, may mimic how these processes unfold in everyday life and inform how the combined effect of these biases influence the development or maintenance of disorders [1, 14].
So far, most experimental studies on cognitive biases in FD have been performed on adults, and have for example demonstrated cognitive biases for health-related or negative stimuli in adults with IBS and functional neurological disorder [11, 15-17]. In contrast, the research on cognitive biases in children and adolescents is scarce, although FD are also prominent in these age groups. One of the most prevailing FD in youth is Functional Abdominal Pain Disorder (FAPD) [18], in which IBS is included, with an estimated prevalence of more than 10% [19]. For now, the most evidence based treatment for FAPD is cognitive behavioural therapy (CBT), but the effects of CBT are mostly small to moderate [20, 21]. Thus, increased understanding of cognitive biases in these disorders may be crucial to further optimize psychological treatment. To date, only a few studies focusing on abdominal pain and cognitive biases in children and adolescents have been performed. Results from these studies, point towards an attentional bias for pain-related stimuli being associated with abdominal pain [22-25]. However, it is difficult to draw more general conclusions as the studies differ with regard to clinical group (both functional abdominal pain and organic abdominal pain), control group and use of stimuli.
The present study introduces a novel experimental design overcoming the limitations of prior studies by including both word and picture stimuli to examine interpretation and memory biases for gastrointestinal stimuli in children and adolescents. Further, this new design includes the potential to assess the interplay of biases in interpretation and memory. Specifically, the aims are: 1) to develop a new experimental design: "Bias in Youth with Functional Abdominal Pain" (BY-FAP) for assessing cognitive biases towards gastrointestinal stimuli in children and adolescents and 2) to test its feasibility on a healthy sample exploring potential sex- and age-related differences. The data from this study can also be used as comparison data for later studies on children with FAPD.
2. Materials and Methods
2.1. Study design and procedure
This is a cross-sectional study collecting data online using REDCap (Research Electronic Data Capture) [26, 27]. The data collection was carried out from April 2022 to April 2023. Potential participants, i.e. healthy children and adolescents were recruited through social media, school intranets and word of mouth. Information regarding eligibility according to predefined study in-/exclusion criteria was provided by a parent and/or the participant (if age ≥ 15 years) in a telephone interview. All children and adolescents who completed the study took part in a lottery to win a tablet or Bluetooth headphones.
Inclusion criteria were age between 8 and 17 years and Danish language proficiency. Exclusion criteria were 1) chronic physical diseases or disabilities demanding treatment or follow-up in a hospital-setting, 2) a psychiatric diagnosis, 3) current psychological treatment, or 4) experiencing abdominal pain more than twice during the past two weeks [23].
2.2. Experimental design
BY-FAP included a word task and a picture task both developed to assess the possible interplay of cognitive biases in interpretation and memory for each type of stimuli. BY-FAP consisted of three phases: 1) encoding, 2) free recall and 3) recognition. The order of presentation of the phases was: word encoding, picture encoding, word free recall, picture free recall, word recognition and picture recognition. The order ensured a short time interval between each phase concerning the same stimuli. Hence, the picture tasks served as filler tasks for the word tasks and vice versa. Both word stimuli and picture stimuli were included because they had different targets. The words targeted specific gastrointestinal symptoms, while the pictures showed different situations that typically can be affected when children and adolescents experience abdominal pain (e.g. social situations with peers) [28]. For an overview of the BY-FAP design see Figure 1. BY-FAP was pilot tested on five children and five adolescents, which resulted in minor changes of the set-up to shorten test-time (i.e. removal of a task to describe each picture in the encoding phase).
2.2.1. Word task
The word task was inspired by the HNST [8], which has previously been used to assess cognitive biases in children and adults [30, 31]. In the encoding phase, participants were presented with a list of physical symptoms and asked to attend to one symptom at a time while imagining developing that symptom. For each word, they indicated whether they would perceive themselves as healthy or no longer healthy, if they developed the symptom. Two categories of symptoms were included in the present study: 1) general symptoms (e.g. coughing, headache) and 2) gastrointestinal symptoms (e.g. nausea, constipation), each comprising 10 words. General symptoms were selected from the Children's Somatic Symptom Inventory (CSSI) and the HNST, while the gastrointestinal symptoms were selected from the Pediatric Quality of Life Inventory (PEDsQL) Gastrointestinal Symptom Scale (for a list of all included words, see Table S1) [32, 33]. In the free recall phase, participants wrote down as many symptoms as they remembered from the encoding phase. In the recognition phase, participants were presented with all symptoms from the encoding phase alongside 20 new symptoms not previously presented. The new symptoms were 10 general symptoms (from the CSSI and HNST) and 10 gastrointestinal symptoms (determined by the author group). The symptoms, both previously presented and new, were split in two lists corresponding to their category (general or gastrointestinal) and presented on separate pages. For each word (original and new), participants indicated if they had seen the symptom before or not. Further, they rated the difficulty of making this choice and the confidence in their answer on a scale from 1-7 (1 = not at all, 7 = a lot) for each of the two lists of symptoms.
2.2.2. Picture task
The design of the picture task followed previous studies [34, 35], but was adjusted to be suitable to a younger age group by simplifying the task. The stimuli were 15 pictures from the PiSCES database [29]. Pictures from the database have previously been used in a study on children [36]. The pictures represented three categories of social contexts (i.e. school, fun and play, food) with five pictures in each category (see Table S2 for a description of each picture and reference number in the PiSCES database). In the encoding phase, participants saw one picture at a time and had to rate the picture on three dimensions before they could move on to the next picture, in line with previous studies [34, 35]. Participants rated each picture on 1) whether it was positive or negative (emotional valence, 0 = negative, 100 = positive), 2) if they experienced any bodily symptoms when seeing the picture (physical arousal, 1 = not at all, 7 = a lot) and 3) if the picture reminded them of something from their own life (self-relevance, 1 = not at all, 7 = a lot). In the free recall phase, participants were instructed to describe as many pictures as they could remember from the encoding phase. Each remembered picture was described and rated separately on emotional valence and physical arousal using the same questions as in the encoding phase. In the recognition phase, participants were presented with all pictures from the encoding phase along with the picture's mirror image. Each original picture and mirror image pair was presented separately. Participants indicated which of the two pictures they had seen in the encoding phase, rated how difficult it was to choose between them (difficulty; 1 = not at all, 7 = a lot) and how confident they were in their decision (confidence; 1 = not at all, 7 = a lot).
2.3. Additional measures
Parents provided information on sociodemographic background, i.e. their education, employment and cohabitant status. The demographics of the participants (age and sex) was obtained when signing up for the study. After completing the experimental tasks, participants answered three questionnaires on unspecific somatic complaints, illness-related anxiety and quality of life (see below).
1) The Children's Somatic Symptoms Inventory (CSSI-24), formerly known as the Children Somatization Inventory, consists of 24 items assessing unspecific somatic symptom complaints in children [32]. The questionnaire is rated on a 5-point scale from 0 "Not at all" to 4 "A whole lot".
2) The Childhood Illness Attitudes Scale (CIAS) assesses symptoms of health anxiety in school children [37]. The CIAS is a modified version of the Illness Attitudes Scales and has 35 items. sThe CIAS is rated on a 3 point Likert-scale ranging from 1 "None of the time to 3 "A lot of the time" with a higher score indicating a higher level of health anxiety. In the present study only the subscale "fears" (11 items) was included [38].
3) The Pediatric Quality of Life Inventory, Gastrointestinal Symptom Scale (PEDsQL (GSS)) measures symptoms related to functional gastrointestinal disorder (FGID) [33]. The scale has nine items rated on a 5-point Likert-scale from 0 "Never a problem", 1 "Almost never a problem", 2 "Sometimes a problem", 3 "Often a problem" to 4 "Almost always a problem". Items are reversed scored, thus a higher score indicates a better quality of life [33].
2.4. Power analysis
The parameters for the power analysis are based on a previous study by Jungmann & Witthöft [30]. We assumed a power (β) of 0.8 and α = 0.05 comparing 60 patients in a clinical group with 100 healthy controls. Based on these parameters, a power analysis using the effect of two independent means gives a minimal detectable effect size of Cohens d = 0.46. Since a Cohens d = 0.4 is a typical effect size in psychological research, the estimated effect size of 0.46 was deemed adequate [39]. Thus, we aimed for recruiting approximately 100 healthy participants in the current study to obtain comparison data for future studies on children and adolescents with FAPD.
2.5. Data analysis
Participants' descriptions of words and pictures in the free recall phase were coded according to their correspondence to the individual words and pictures in the encoding phase as well as their correspondence to a category (words: general symptoms, gastrointestinal symptoms; pictures: school, fun and play, food). If a description did not match an individual picture or word or did not match a category, it was coded as "other". Responses from the first 20 individuals (only 19 for pictures), who completed the experimental tasks, were coded by two independent raters (1st author and 3rd author) with high interrater agreement for both words (individual words: 95%, word category: 98%) and pictures (individual pictures: 98%, picture category: 100%). Disagreements between the two coders were resolved through discussion under supervision of an experienced rater (4th author). The remaining responses were coded by the first author. The statistical analyses were performed using STATA version 17.0 MP—Parallel Edition [40]. We used Student's t-test and Wilcoxon rank-sum test to explore potential sex- and age-related differences in the outcomes of the encoding, recall and recognition phases.
3. Results
203 records were assessed for eligibility, and the final sample consisted of 51 children (8-12 years) and 47 adolescents (13-17 years). For more details, see Figure 2. Characteristics of participants and their parents can be found in Table 1.
3.1. Word task
Table 2 shows the descriptive statistics for the three phases in the word task. In the encoding phase, participants evaluated that they would still be "Healthy", if they developed the majority of the symptoms in the task (Median (Mdn) = 12.5, IQR = 5.0). The symptom most often evaluated as "No longer healthy" was "Vomiting". There was no significant difference between sex or age groups. In the recall phase, the median for recalled words was 7.0 (IQR = 6.00, possible range 0-20). The most often recalled word was "Stomachache", which was recalled by 81.3% of the participants followed by "Headache" which was recalled by 72.9% of the participants. For the number of overall recalled words, there was no significant difference between sex or age groups, but adolescents were significantly better at recalling general words (Mdn = 3.0 vs. 4.0, p-value <0.01). In the recognition phase, the median for correctly recognized words was 37.0 (IQR = (2.00, possible range 0-40) with no significant difference between sex or age groups. This was above chance level, which would have been 20 words.
3.2. Picture task
Table 3 shows the descriptive statistics for the three phases in the picture task. In the encoding phase the total sample evaluated the pictures as slightly positive (Mdn = 69.0, IQR = 11.40, range 0-100) with no significant difference between sex or age groups in the rating of emotional valence. In both the encoding phase and the free recall phase, there was a significant difference between children and adolescents' evaluation of physical reaction as children had a higher median in both phases compared to adolescents (p-value = 0.04). In the recall phase, the median for recalled pictures was 3.0 (IQR = 2.00, range 0-15) with no significant difference in sex or age groups. The most often recalled picture depicted a birthday, which was recalled by 54.17% of the participants followed by a picture depicting people in a library, which was recalled by 51.04% of the participants. There was a significant difference between girls and boys on the rating of emotional valence, where boys evaluated the recalled pictures as more positive than girls (Mdn = 64.5 vs. 74.4, p-value = 0.01). In the recognition phase, almost all 15 pictures were correctly recognized by the participants (median = 15, IQR = 0.00). There was no significant difference in sex or age groups.
4. Discussion
To our knowledge, the BY-FAP is the first experimental design, specifically developed for children and adolescents, to assess cognitive biases of interpretation and memory and their interplay towards gastrointestinal stimuli. Only one out of 97 participants did not complete the BY-FAP once started. Additionally, 98% of participants recalled at least one word or picture and for both the recognition phases the participants performed above chance level. Further, we found few significant differences between sex and age groups across the three phases in both the word task and the picture task. Together, these results support the feasibility of BY-FAP within the age group (8-17 years).
The word task was designed to target biases specific for gastrointestinal stimuli in line with other studies exploring cognitive biases for disorder-specific stimuli [41, 42]. In the encoding phase, the participants on average evaluated 37% of the symptoms as "No longer healthy". This was lower than Jungmann & Witthöft, who found that children and adolescents on average rated 56% of symptoms as "No longer healthy" in their version of the HNST. This may be explained by our sample being healthy while 80% of the sample in the Jungmann & Witthöft study had at least one medically unexplained symptom within the last six months [30]. For the recall phase, the adolescents recalled significantly more general words than the children. Also, for the recognition phase, the adolescents were significantly better at correctly recognizing gastrointestinal words than the children. For gastrointestinal and general words in total, there was no significant differences between children and adolescents in either the recall or recognition phase. For the recognition task, our results depicted a ceiling effect as the participants recognized 91% of the symptoms correct. Such a ceiling effect is a standard detection and confirms that the participants payed attention in the encoding phase and thus, it supports the feasibility of BY-FAP.
The design of the picture task was inspired by prior studies on adults, that also used phases of encoding, recall and recognition to assess cognitive biases [34, 35], however our design was simplified to be adapted to a sample of children and adolescents. For the encoding phase, the overall emotional valence of the pictures was evaluated as slightly positive (Mdn = 69.0, IQR = 11.40, range: 0-100) in line with the original ratings in the PiSCES database [29]. The rating on physical reaction was significantly different in children and adolescents in both the encoding and the recall phase, since the children tended to rate their physical reaction higher than adolescents. For the recall phase, we found significant differences between girls' and boys' rating of emotional valence on recalled pictures. The mean emotional valence of the recalled pictures was lower for the girls compared to the boys. This may be explained by the categories of pictures that the girls and boys recalled. The girls recalled more pictures within the "Food" and "School" categories, which included both positive, neutral and negative pictures (as attributed in the PiSCES database [29]). In contrast, the boys recalled more pictures within the "Fun and play" category, which only contained positive pictures. In the recognition phase, we saw a clear ceiling effect, as >99% of all pictures were recognized correctly. As for the word task, ceiling effects are also a standard finding in pictorial recognition tasks, and thus the results underpin the feasibility of the BY-FAP design.
The results of both the word task and picture task indicated that the different phases interacted with each other. The recall of words and pictures and the ceiling effects in the recognition phases confirmed that participants payed attention in the encoding phase. The participants performed better in some phases depending on the stimuli. For the recall phase, more words than pictures were recalled (35% vs. 22%), however for the recognition phase more pictures than words were correctly recognized (90% vs. 99%). Based on our results, it was not possible to conclude whether word stimuli were preferable over picture stimuli or vice versa. The study included both word and pictorial stimuli as each category displayed different targets. The word stimuli target specific symptoms related to FAPD, such as nausea and stomach ache. Prior studies on adults with IBS have found evidence for cognitive biases specifically for IBS-related words [11, 42]. In contrast, the pictorial stimuli target the effects of the symptoms on daily life, for instance the fear of having stomach ache at a birthday party if you eat cake. A prior study from Heathcote et al. found that youth who catastrophized about pain and who had recent experiences of pain had more negative interpretations of ambiguous situations, not only related to pain and bodily threat, but also towards social situations [43].
With the inclusion of three phases in BY-FAP, we aimed for a design that could assess the interplay of different cognitive biases. For conclusions on the interplay of biases, our results must be compared with future clinical samples using the BY-FAP. In future studies potential associations between recall and recognition of the different stimuli categories should be explored. For instance, do children with FAPD falsely recognize new gastrointestinal words as having been previously presented? A prior study on adults with IBS found that the IBS group had a high false-positive score for recognizing negative words [17]. Additionally, Witthöft et al. also found that individuals with pathological health anxiety had a response bias for illness and symptom words in a recognition task compared to depressed and healthy control groups [41].
4.1. Strengths and limitations
Compared to other studies on cognitive biases in children and adolescents both our sample size and age span was bigger [22, 25, 30]. Though the sample was not completely even in age, overall all ages between 8-17 years were represented in both sexes. Further, BY-FAP included three phases (encoding, recall and recognition) making it possible to explore the potential interplay of biases in interpretation and memory.
The study also had limitations. First, our study population was healthier and more socioeconomically advantaged than the general population. All participants were screened for current physical and mental disorders to limit the possibility of cognitive biases in relation to the employed stimuli. It was essential to screen our participants as a prior study found evidence of a negative interpretation bias in a general school population [43]. The parents of the participants differed from the general population in regard to education, employment, civil status and yearly household income. For the majority of the participants, their parents: lived together, had a higher education, were employed and had a yearly household income above average. Thus, our results may reflect a higher feasibility of BY-FAP as children of resourceful parents tend to perform better than the average child. Further, the study was conducted as an online study to make participation more easy. This might be a limitation, since participants completed BY-FAP and questionnaires at home. Though, parents and participants >15 years were clearly instructed, that the participant should complete the survey as independent as possible. It was not possible to rule out that some (preferably children) received too much help from their parents.
5. Conclusions
BY-FAP is a novel experimental design to assess biases of interpretation and memory towards gastrointestinal stimuli in children and adolescents. This was a first test of the feasibility on a healthy sample and exploration of potential sex- and age-related differences. We found only few significant differences between sex and age groups. Overall, the results support the BY-FAP to be feasible across the age-span. In the future, the BY-FAP could be used to assess cognitive biases in children and adolescent with FAPD with results from the present study as comparison material. Further, BY-FAP could be used as a framework to assess cognitive biases in children and adolescents with other clinical disorders by exchanging the present stimuli (words and pictures) with disorder-specific stimuli for other conditions..
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Symptom words used in encoding and recognition phases and Table S2: Description of pictures from encoding and recognition phases.
Author Contributions
Conceptualization, EBN, KHK, ESN, TBG, LF and CUR; methodology, EBN, KHK, ESN, TBG, LF and CUR; formal analysis, EBN, ESN and TBG; investigation, EBN; data curation, EBN; writing—original draft preparation, EBN.; writing—review and editing, EBN, KHK, ESN, TBG, LF and CUR; supervision, KHK, TBG and CUR; project administration, ESN and CUR; funding acquisition, EBN. All authors have read and agreed to the published version of the manuscript.
Funding
First author received a scholarship from Lundbeckfonden, grant number F-61171-19-27, for this research project. The project was further funded by Dagmar Marshalls Fond, grant number 86/2022, Frimodt-Heineke Fonden, grant number 1-16-2-3-23 and Else og Mogens Wedell – Wedellsborgs Fond, grant number 20-22-3. The APC was funded by Dagmar Marshalls Fond.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study was reported to the Regional Ethics Committee for the Central Region Denmark and found exempt from full review (1-10-72-1-22). The study was registered at the Internal Register of Research Projects in Central Region Denmark (1-16-02-86-22).
Informed Consent Statement
Written informed consent was obtained from both parents or one parent and the participant, if the participant was ≥ 15 years. The informed consent form was sent through a secure and personal email system (DigitalPost) and stored in REDCap [44].
Data Availability Statement
The data used in the present study contain sensitive personal information and therefore cannot be shared freely due to Danish data protection laws. All data are stored in REDCap, and access can only be granted through approval from the Central Region Denmark, which has legal responsibility for data as the data manager. If access is granted, the principal investigator and last author (Charlotte Ulrikka Rask, charrask@rm.dk) will make data available. The General Data Protection Regulation (GDPR) and the Danish Data Protection Act prohibit any other forms of data sharing.
Acknowledgments
Thank you to all the participating children and adolescents and their parents. Thank you to statistician Anders Helles Carlsen for statistical support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Everaert, J., E.H. Koster, and N. Derakshan, The combined cognitive bias hypothesis in depression. Clin Psychol Rev, 2012. 32(5): p. 413-24. [CrossRef]
- Craske, M.G. and D.C. Pontillo, Cognitive biases in anxiety disorders and their effect on cognitive-behavioral treatment. Bull Menninger Clin, 2001. 65(1): p. 58-77. [CrossRef]
- Brown, R.J., Psychological mechanisms of medically unexplained symptoms: an integrative conceptual model. Psychol Bull, 2004. 130(5): p. 793-812. [CrossRef]
- Burton, C., et al., Functional somatic disorders: discussion paper for a new common classification for research and clinical use. BMC Med, 2020. 18(1): p. 34. [CrossRef]
- Fink, P. and M. Rosendal, Functional Disorders and Medically Unexplained Symptoms: Assessment and Treatment, ed. P. Fink and M. Rosendal. 2015, Aarhus, Denmark: Aarhus University Press.
- Deary, V., T. Chalder, and M. Sharpe, The cognitive behavioural model of medically unexplained symptoms: a theoretical and empirical review. Clin Psychol Rev, 2007. 27(7): p. 781-97. [CrossRef]
- MacLeod C Fau - Mathews, A., P. Mathews A Fau - Tata, and P. Tata, Attentional bias in emotional disorders. (0021-843X (Print)). [CrossRef]
- Barsky, A.J., et al., Hypochondriacal patients' beliefs about good health. Am J Psychiatry, 1993. 150(7): p. 1085-9. [CrossRef]
- Greenwald, A.G., J.L. McGhee De Fau - Schwartz, and J.L. Schwartz, Measuring individual differences in implicit cognition: the implicit association test. (0022-3514 (Print)). [CrossRef]
- Hughes, A.M., et al., Maximizing potential impact of experimental research into cognitive processes in health psychology: A systematic approach to material development. (2044-8287 (Electronic)). [CrossRef]
- Phillips, K., B.J. Wright, and S. Kent, Irritable bowel syndrome and symptom severity: evidence of negative attention bias, diminished vigour, and autonomic dysregulation. J Psychosom Res, 2014. 77(1): p. 13-9. [CrossRef]
- Witthoft, M., et al., Neuronal and behavioral correlates of health anxiety: results of an illness-related emotional Stroop task. Neuropsychobiology, 2013. 67(2): p. 93-102. [CrossRef]
- Lees, A., K. Mogg, and B.P. Bradley, Health anxiety, anxiety sensitivity, and attentional biases for pictorial and linguistic health-threat cues. Cogn Emot, 2005. 19(3): p. 453-62. [CrossRef]
- Hirsch, C.R., D.M. Clark, and A. Mathews, Imagery and interpretations in social phobia: support for the combined cognitive biases hypothesis. Behav Ther, 2006. 37(3): p. 223-36. [CrossRef]
- Keynejad, R.C., et al., Attentional Processing and Interpretative Bias in Functional Neurological Disorder. Psychosom Med, 2020. 82(6): p. 586-592. [CrossRef]
- Lam, N.C., et al., Cognitive impairment in Irritable Bowel Syndrome (IBS): A systematic review. Brain Res, 2019. 1719: p. 274-284. [CrossRef]
- Gomborone, J.E., et al., Selective affective biasing in recognition memory in the irritable bowel syndrome. Gut, 1993. 34(9): p. 1230-3. [CrossRef]
- Vernon-Roberts, A., I. Alexander, and A.S. Day, Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). J Clin Med, 2021. 10(21). [CrossRef]
- Cordeiro Santos, M.L., et al., Non-pharmacological management of pediatric functional abdominal pain disorders: Current evidence and future perspectives. World J Clin Pediatr, 2022. 11(2): p. 105-119. [CrossRef]
- Abbott, R.A., et al., Recurrent Abdominal Pain in Children: Summary Evidence From 3 Systematic Reviews of Treatment Effectiveness. (1536-4801 (Electronic)). [CrossRef]
- Bonvanie, I.J., et al., Psychological Interventions for Children with Functional Somatic Symptoms: A Systematic Review and Meta-Analysis. (1097-6833 (Electronic)). [CrossRef]
- Boyer, M.C., et al., Attentional Biases to Pain and Social Threat in Children with Recurrent Abdominal Pain. Journal of Pediatric Psychology, 2005. 31(2): p. 209-220. [CrossRef]
- Beck, J.E., et al., Attentional bias to pain and social threat in pediatric patients with functional abdominal pain and pain-free youth before and after performance evaluation. PAIN, 2011. 152(5): p. 1061-1067. [CrossRef]
- van der Veek, S.M., et al., Attentional bias to activity of different parts of the body in children with functional abdominal pain: an experimental study. J Pediatr Psychol, 2014. 39(4): p. 438-49. [CrossRef]
- Hermann, C., et al., Cortical correlates of an attentional bias to painful and innocuous somatic stimuli in children with recurrent abdominal pain. PAIN, 2008. 136(3): p. 397-406. [CrossRef]
- Harris, P.A., et al., The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 2019. 95: p. 103208. [CrossRef]
- Harris, P.A., et al., Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 2009. 42(2): p. 377-381. [CrossRef]
- Roth-Isigkeit, A., et al., Pain among children and adolescents: restrictions in daily living and triggering factors. (1098-4275 (Electronic)). [CrossRef]
- Teh, E.J., M.J. Yap, and S.J.R. Liow, PiSCES: Pictures with social context and emotional scenes with norms for emotional valence, intensity, and social engagement. Behav Res Methods, 2018. 50(5): p. 1793-1805. [CrossRef]
- Jungmann, S.M. and M. Witthöft, Medically unexplained symptoms in children and adolescents: Illness-related self-concept and parental symptom evaluations. J Behav Ther Exp Psychiatry, 2020. 68: p. 101565. [CrossRef]
- Weck, F. and M. Witthöft, Context effects in the evaluation of bodily symptoms: Comparing three versions of the Health Norms Sorting Task. Journal of Experimental Psychopathology, 2017. 8(3): p. 241-251. [CrossRef]
- Walker, L.S., et al., Children's Somatization Inventory: psychometric properties of the revised form (CSI-24). (1465-735X (Electronic)). [CrossRef]
- Varni, J.W., et al., Health-related quality of life in pediatric patients with irritable bowel syndrome: a comparative analysis. J Dev Behav Pediatr, 2006. 27(6): p. 451-8. [CrossRef]
- Niziurski, J.A. and D. Berntsen, Involuntary versus voluntary episodic memories: The effects of encoding factors and emotion. Psychology of Consciousness: Theory, Research, and Practice, 2019. [CrossRef]
- Gehrt, T.B., et al., Encoding and retrieval biases for health-related scenes in patients with severe health anxiety(.). Memory, 2019. 27(8): p. 1110-1121. [CrossRef]
- Teh, E.J., M.J. Yap, and S.J. Rickard Liow, Emotional Processing in Autism Spectrum Disorders: Effects of Age, Emotional Valence, and Social Engagement on Emotional Language Use. (1573-3432 (Electronic)). [CrossRef]
- Wright, K.D. and G.J.G. Asmundson, Health Anxiety in Children: Development and Psychometric Properties of the Childhood Illness Attitude Scales. Cognitive Behaviour Therapy, 2003. 32(4): p. 194-202. [CrossRef]
- Thorisdottir, A.S., et al., Measurement invariance across Genders on the Childhood Illness Attitude Scales (CIAS). J Psychosom Res, 2017. 98: p. 34-39. [CrossRef]
- Brysbaert, M. and M. Stevens, Power Analysis and Effect Size in Mixed Effects Models: A Tutorial. J Cogn, 2018. 1(1): p. 9. [CrossRef]
- StataCorp. 2021. Stata Statistical Software: Release 17. College Station, T.S.L. 2021.
- Witthöft, M., et al., Cognitive biases in pathological health anxiety: The contribution of attention, memory, and evaluation processes. Clinical Psychological Science, 2016. 4(3): p. 464-479. [CrossRef]
- Afzal, M., et al., Selective processing of gastrointestinal symptom-related stimuli in irritable bowel syndrome. Psychosom Med, 2006. 68(5): p. 758-61. [CrossRef]
- Heathcote, L.C., et al., Negative Interpretation Bias and the Experience of Pain in Adolescents. (1528-8447 (Electronic)). [CrossRef]
- Lawrence, C.E., et al., A REDCap-based model for electronic consent (eConsent): Moving toward a more personalized consent. Journal of Clinical and Translational Science, 2020. 4(4): p. 345-353. [CrossRef]
Figure 1.
Overview of the experimental word task and picture task design in BY-FAP. Pictures are from the PiSCES database [29].
Figure 1.
Overview of the experimental word task and picture task design in BY-FAP. Pictures are from the PiSCES database [29].
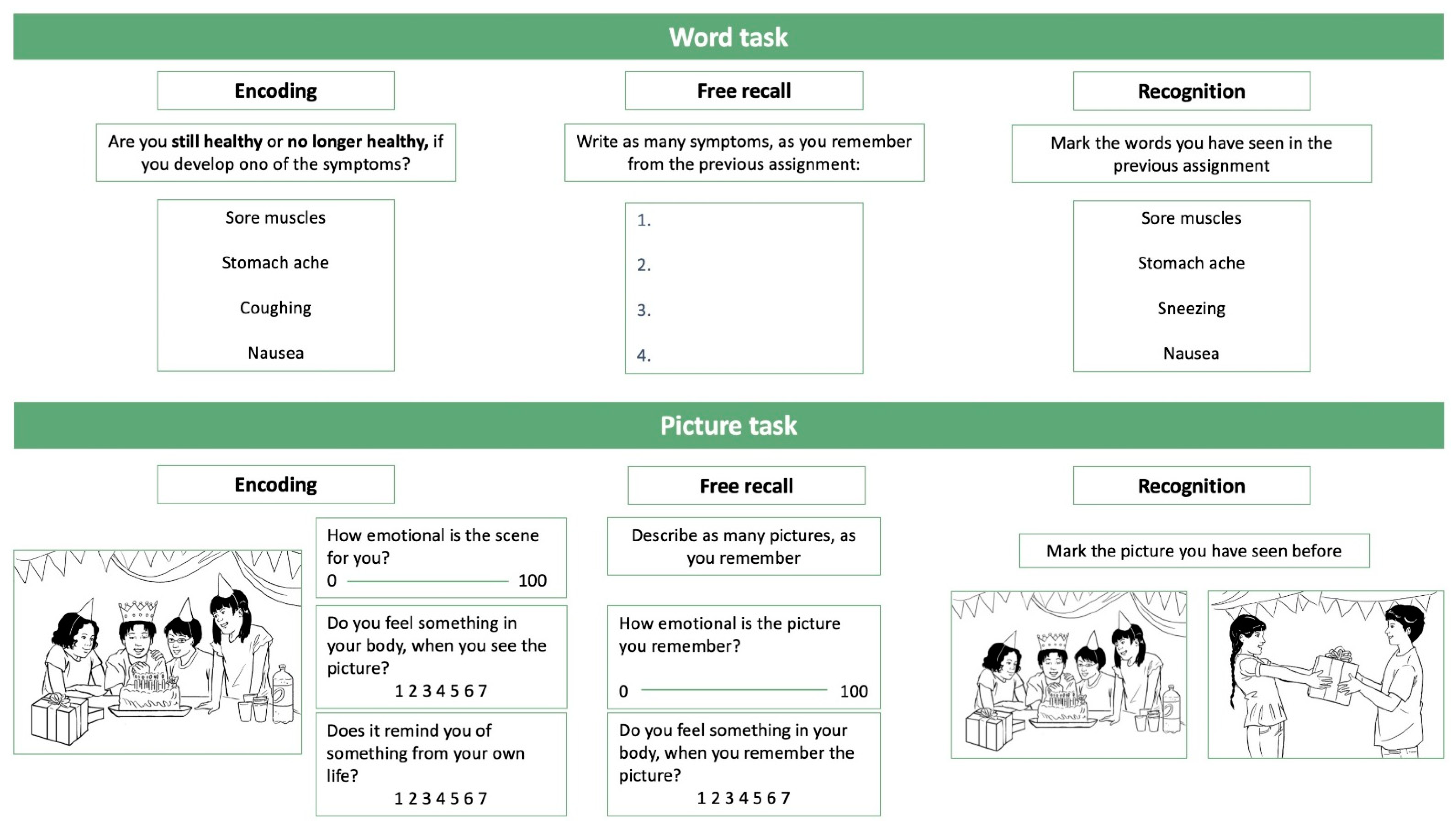
Figure 2.
Flowchart of the recruiting and inclusion process. Pictures are from the PiSCES database [29].
Figure 2.
Flowchart of the recruiting and inclusion process. Pictures are from the PiSCES database [29].
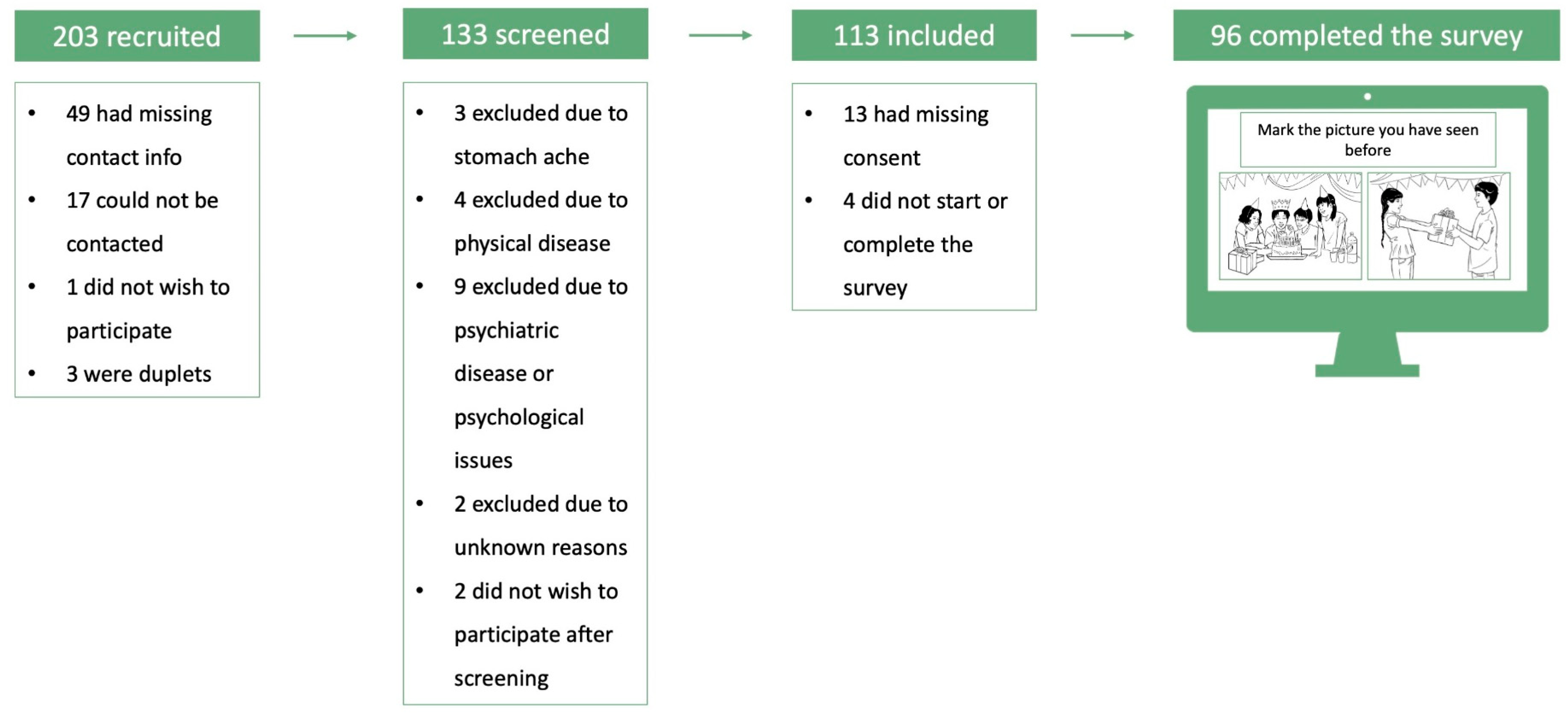

Table 1.
Sample characteristics of participants and their parents.
| Participants | Possible Range | Total | Children (8-12 years) |
Adolescents (13-17 years) |
|---|---|---|---|---|
| N (% female) | 96 (47.9%) | 51 (49.0%) | 45 (46.7%) | |
| Age (mean (SD)) | 12.3 (2.6) | 10.3 (1.4) | 14.6 (1.2) | |
| Scores on questionnaires (median (IQR)) | ||||
| Children's Somatic Symptoms Inventory1 (CSSI) | 0-96 | 8.0 (11.0) | 8.0 (11.0) | 11.0 (10.0) |
| Childhood Illness Attitude Scale2 (CIAS) | 11-33 | 15.0 (5.0) | 14.0 (6.0) | 16.0 (4.0) |
| Pediatric Quality of Life Inventory1, Gastrointestinal symptom scale (PEDsQL (GSS)) | 0-100 | 86.1 (19.4) | 91.7 (19.4) | 86.1 (16.7) |
| Parents | ||||
| Education | ||||
| High school, % (n)3 | <5 | 0.0 (0) | <5 | |
| Vocational education, % (n) | 13.5 (13) | 11.8 (6) | 15.6 (7) | |
| Continuing education, % (n)3 | 8.3 (8) | < 5 | 11.1 (5) | |
| Higher education, % (n) | 77.1 (74) | 82.3 (42) | 71.1 (32) | |
| Employment | ||||
| Full or part time employment, % (n) | 92.7 (89) | 88.2 (45) | 97.8 (44) | |
| Unemployed, % (n)3 | <5 | <5 | 0.0 (0) | |
| Other (e.g. sick leave, maternity leave), % (n)3 | 6.3 (6) | 9.8 (5) | <5 | |
| Marital status | ||||
| Living together, % (n) | 85.5 (85) | 90.2 (46) | 86.7 (39) | |
| Living apart, % (n) | 10.4 (10) | 7.8 (4) | 13.3 (6) | |
| Other, % (n)3 | <5 | <5 | 0.0 (0) | |
| Yearly household income | ||||
| Low income (< 500.000 DKK), % (n)3 | 5.2 (5) | <5 | <5 | |
| Middle income (500.000-1.000.000 DKK), % (n) | 49.0 (47) | 47.1 (24) | 51.1 (23) | |
| High income (>1.000.000) % (n) | 45.8 (44) | 45.1 (23) | 46.7 (21) |
1 Only 94 participants answered the CSSI and PedsQL (GSS) questionnaires. 2Only 95 participants answered the CIAS questionnaire. 3 Numbers between 0 and 5 are showed as "<5" due to data protection rules in Denmark. There was no significant difference between children and adolescents for Children's Somatic Symptoms Inventory1 (CSSI), Childhood Illness Attitude Scale (CIAS) and Pediatric Quality of Life Inventory Gastrointestinal symptom scale (PEDsQL(GSS)) and no significant differences in education, employment, marital status or yearly household income between children and adolescents (all p-values > 0.05) (Wilcoxon rank sum test). DKK = Danske kroner (Danish currency). IQR = Interquartile Range. SD = Standard deviation.
Table 2.
Median (IQR) scores within the three phases for the word task.
| Possible range | Total (N = 96) |
Girls (N = 46) |
Boys (n = 50) |
Test statisticb |
P-value |
Children (n = 51) |
Adolescents (n = 45) |
Test statisticb | P-value |
|
|---|---|---|---|---|---|---|---|---|---|---|
| Encoding | ||||||||||
| Healthy | 12.50 (5.00) | 13.00 (4.00) | 12.00 (6.00) | 0.45 | 0.65 | 12.00 (6.00) | 13.00 (4.00) | -1.59 | 0.11 | |
| No longer healthy | 7.50 (5.00) | 7.00 (4.00) | 8.00 (6.00) | -0.45 | 0.65 | 8.00 (6.00) | 7.00 (4.00) | 1.59 | 0.11 | |
| Free recall | ||||||||||
| Number of words recalled | 0-20 | 7.00 (6.00) | 8.00 (6.00) | 6.50 (5.00) | 0.85 | 0.40 | 6.00 (4.00) | 8.00 (4.00) | -2.17 | 0.03 |
| Number of gastrointestinal words recalled | 0-10 | 3.00 (3.00) | 3.00 (3.00) | 3.00 (3.00) | 0.28 | 0.78 | 3.00 (3.00) | 3.00 (3.00) | -0.42 | 0.67 |
| Number of general words recalled | 0-10 | 4.00 (3.00) | 4.00 (4.00) | 3.00 (4.00) | 1.16 | 0.25 | 3.00 (3.00) | 4.00 (5.00) | -3.31 | <0.01 |
| Recognition | ||||||||||
| Words correctly recognized in total | 0-40 | 37.00 (2.00) | 37.00 (2.00) | 37.00 (2.00) | 1.01 a | 0.31 | 37.00 (2.00) | 37.00 (3.00) | -0.75 a | 0.45 |
| General words correctly recognized | 0-20 | 19.00 (2.00) | 19.00 (1.00) | 19.00 (2.00) | 1.60 a | 0.11 | 19.00 (1.00) | 19.00 (2.00) | 1.28 a | 0.20 |
| Difficulty | 1-7 | 2.00 (2.50) | 2.50 (2.00) | 2.00 (3.00) | 0.49 a | 0.63 | 2.00 (2.00) | 2.00 (3.00) | 0.59 a | 0.55 |
| Confidence | 1-7 | 5.00 (2.00) | 5.00 (2.00) | 5.00 (2.00) | -0.23 a | 0.82 | 5.00 (1.00) | 5.00 (2.00) | 1.91 a | 0.06 |
| Gastrointestinal words correctly recognized | 0-20 | 18.00 (2.00) | 18.00 (2.00) | 18.50 (2.00) | -0.16 a | 0.87 | 18.00 (3.00) | 19.00 (2.00) | -2.17 a | 0.03 |
| Difficulty | 1-7 | 3.00 (2.00) | 3.00 (1.00) | 3.00 (2.00) | -0.39 a | 0.70 | 3.00 (2.00) | 3.00 (1.00) | 1.14 a | 0.26 |
| Confidence | 1-7 | 5.00 (2.00) | 5.00 (2.00) | 5.00 (2.00) | -0.19 a | 0.85 | 5.00 (2.00) | 5.00 (2.00) | 0.53 a | 0.60 |
a Wilcoxon rank-sum test used due to non-normal distribution. bFor Students ttest "t-value" is reported. For Wilcoxon rank sum test "z-value" is reported.
Table 3.
Median (IQR) scores within the three phases for the picture task.
| Possible range | Total n = 96 |
Girls (n = 46) |
Boys (n = 50) |
Test statisticb | P- value | Children (n = 51) |
Adolescents (n = 45) |
Test statisticb | P- value |
|
|---|---|---|---|---|---|---|---|---|---|---|
| Encoding | ||||||||||
| Emotional valence | 1-100 | 69.00 (11.40) | 69.60 (10.06) | 68.50 (10.33) | -1.30 | 0.20 | 67.93 (13.00) | 70.00 (8.80) | -1.02 | 0.31 |
| Physical reaction | 1-7 | 1.27 (0.93) | 1.40 (1.07) | 1.20 (0.93) | 1.22a | 0.22 | 1.47 (1.33) | 1.20 (0.46) | 2.05a | 0.04 |
| Self-relevance | 1-7 | 4.37 (1.30) | 4.13 (1.27) | 4.43 (1.27) | -0.49 | 0.63 | 4.20 (1.27) | 4.40 (1.33) | -1.01 | 0.31 |
| Free recall | ||||||||||
| Number of pictures recalled | 0-15 | 3.00 (2.00) | 3.00 (2.00) | 3.00 (3.00) | 0.30 | 0.76 | 3.00 (2.00) | 3.00 (2.00) | -0.74 | 0.46 |
| Number of fun pictures recalled | 0-5 | 1.00 (2.00) | 1.00 (2.00) | 1.00 (2.00) | -0.43 | 0.67 | 1.00 (2.00) | 1.00 (1.00) | 0.18 | 0.86 |
| Number of school pictures recalled | 0-5 | 1.00 (2.00) | 1.00 (2.00) | 1.00 (2.00) | 0.39 | 0.70 | 1.00 (2.00) | 1.00 (2.00) | -1.11 | 0.27 |
| Number of food pictures recalled | 0-5 | 1.00 (1.50) | 1.00 (1.00) | 1.00 (2.00) | 0.54 | 0.59 | 1.00 (2.00) | 1.00 (1.00) | -0.33 | 0.75 |
| Emotional valence of recalled picture | 1-100 | 68.20 (20.76) | 64.50 (16.25) | 74.38 (19.75) | -2.43 | 0.01 | 68.40 (24.64) | 68.00 (20.00) | -0.41 | 0.68 |
| Physical reaction of recalled pictures | 1-7 | 1.20 (1.00) | 1.45 (1.25) | 1.00 (1.00) | 1.43 a | 0.15 | 1.60 (1..71) | 1.10 (0.50) | 2.05 a | 0.04 |
| Recognition | ||||||||||
| Number of pictures correctly recognized | 0-15 | 15.00 (0.00) | 15.00 (0.00) | 15.00 (0.00) | 1.95 a | 0.05 | 15.00 (0.00) | 15.00 (0.00) | 0.11 a | 0.92 |
| Difficulty | 1-7 | 1.07 (0.27) | 1.07 (0.13) | 1.20 (0.33) | -1.34 a | 0.18 | 1.07 (0.33) | 1.07 (0.20) | 1.32 a | 0.19 |
| Confidence | 1-7 | 6.93 (3.00) | 6.97 (0.47) | 6.93 (0.20) | 0.02 a | 0.98 | 6.93 (0.73) | 6.93 (0.13) | -1.32 a | 0.19 |
a Wilcoxon rank-sum test used due to non-normal distribution. bFor Students ttest "t-value" is reported. For Wilcoxon rank sum test "z-value" is reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



