
Submitted:
31 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
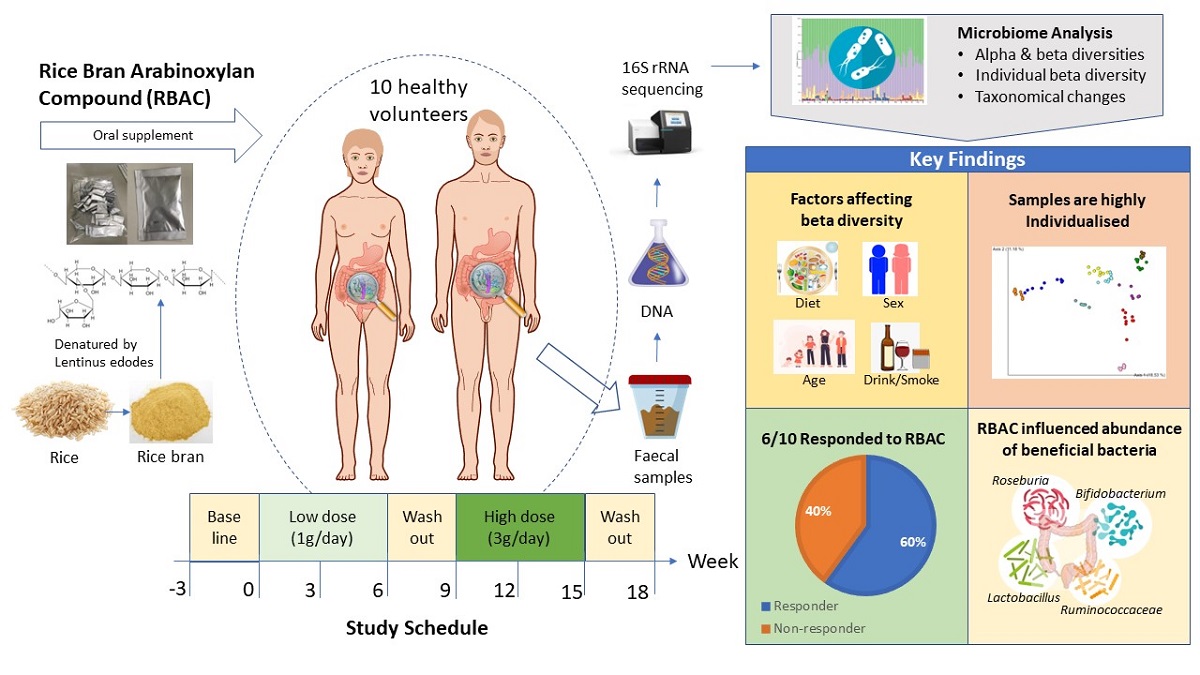
This study investigated the effects of modified rice bran arabinoxylan compound (RBAC) as a dietary supplement on the gut microbiota of healthy adults. Ten volunteers supplemented their diet with 1g of RBAC for six weeks and 3g of RBAC for another six weeks, with a three-week washout period. Faecal samples were collected every 3 weeks over 21 weeks. Microbiota from faecal samples were profiled using 16S rRNA sequencing. Assessment of alpha and beta microbiota diversity was performed using the QIIME2 platform. The results revealed that alpha and beta diversity were not associated with the experimental phase, interventional period, RBAC dosage, or time. However, statistical significance of participant was detected in alpha (p<0.002) and beta (weighted unifrac, p=0.001) diversity. Explanatory factors including age and diet were significantly associated with alpha (p<0.05) and beta (p<0.01) diversity. The individual beta diversity of six participants significantly changed (p<0.05) during the interventional period. Seven participants showed statistically significant taxonomic changes (ANCOM W≥5). These results classified four participants as responders to RBAC supplementation, with a further two participants likely responders. In conclusion, the gut microbiome is highly individualised and modulated by RBAC as a dietary supplement, dependent on lifestyle and dietary intake
Keywords:
RBAC
; Biobran/MGN-3
; microbiome
; prebiotic
; functional food
; diet
; Australian Recommended Food Score
1. Introduction
Communities of microorganisms reside within humans, with the gut being the most densely colonised site [1]. Microbial communities that cohabit the intestinal tract, known as gut microbiota, can be beneficial, neutral, or detrimental to the host. Gut microbiota can impact human health by mediating physiological homeostasis through immune function, digestion, vitamin synthesis, and pathogen colonisation [2]. The effects are exerted through interfaces between gut microbiota and intestinal epithelial cells, the immune system, and dietary intake [2,3,4]. Gut microbiota diversity and abundance is associated with health through processes such as reduced inflammation and disorders linked to inflammatory events [3].
Microbial diversity is required for healthy gut function, with a loss of diversity associated with an increased risk of disease [5]. In healthy adults, the gut microbiota comprises eight dominant phyla including Firmicutes, Bacteroidetes, Actinobacteria, Proteobacteria, Fusobacteria, and Verrucomicrobia. The Firmicutes and Bacteroidetes together represent 90% of gut microbiota [6,7]. Bacteria in these phyla perform diverse roles in regulating host health [7]. Bifidobacterium species comprise only 2% of total gut microbiota but play a significant role in the breakdown of complex carbohydrates [8,9], protecting the host against pathogens through competitive exclusion, modulating the immune system, and providing vitamins and other nutrients for the host [10]. The genus Lactobacillus includes species that produce short-chain fatty acids (SCFAs) and regulate intestinal transit [11,12]. Production of SCFAs by these bacteria can improve insulin sensitivity and protect against diet-induced obesity [9]. Other bacteria of importance to human health include Roseburia, Faecalibacterium, Ruminococcus, and Bacteroides [13,14,15].
The presence of microbes and their interaction with the host and other gut microbes in the gastrointestinal tract can lead to adverse health outcomes [1]. Metabolic products from gut microbiota have been linked to an increased risk of major adverse cardiovascular events [16] and type 2 diabetes [17]. Supporting an optimal composition of gut microbiota is vital for human health [18]. The gut microbiota in healthy individuals includes shared common microbiota, with variations across age, ethnicity, and socioeconomic status [19,20,21,22,23]. Although relatively stable throughout adulthood, variations in the common microbial genera are observed, with major shifts identified in older adults [23,24,25,26]. Composition of the gut microbiome is also affected by lifestyle [27,28]. Cigarette smoking and alcohol consumption impact the gut microbiome with changes identified with the cessation of smoking, and heavy alcohol consumption [27,28].
Diet has also been shown to be a significant factor affecting gut microbial composition [18,29]. Functional foods aim to improve health and wellbeing and have been shown to interact with gut microbiota [30,31,32]. Prebiotics are non-digestible dietary ingredients that stimulate the growth of microbes in the gut after fermentation [33]. Recent research identifies prebiotics that enhance microbial diversity to promote health and defend against dysbiosis of gut microbiota [4,5]. Arabinoxylans (AXs) are the non-digestible fibre of cereal grains, including wheat, rice, rye, maize, and sorghum [9]. The structures of AXs have been shown to influence substrate fermentation and degradation by gut microbiota [34]. Francios et al. [35] and Kjolbaek et al. [36] showed that supplementation with wheat AX/AX oligosaccharides in humans led to changes in the microbiota profile including increased beneficial bacteria such as Bifidobacterium. Lachnospiraceae have also been shown to be increased in AX-fed mice [37]. The extent and mechanism of the effects of AXs on gut microbiota differs due to variations in the chemical structure and molecular weight [38]. Recent in vivo research has focused on linear AXs due to their bioavailability and simple structures [9,39].
Rice bran arabinoxylan compound (RBAC), known as BioBran, MGN-3, and Ribraxx, is a modified AX compound [40]. RBAC consists of a water-soluble hemicellulose- fraction (degree of polymerisation approximately 200), partially decomposed by enzymes extracted from a cultured medium of Lentinula edodes (shiitake mushrooms) [40]. However, knowledge of its effect on gut microbiota, particularly in healthy adults, is lacking. Therefore, the purpose of this clinical study was to determine the changes in gut microbiota in response to dietary RBAC supplementation in healthy adults. Additional observational analysis was also performed to assess the abundance of the beneficial bacteria Bifidobacterium, Lactobacillus, Roseburia, Ruminococcaceae, and Faecalibacterium.
2. Results
2.1. Participant characteristics and dietary intake
Characteristics of the study participants and their dietary intake from the screening survey and Australian Eating Survey® (AES) are summarised in Table 1. The participant group consisted of balanced numbers of males and females (sex ratio 1:1). Ages ranged from 21 to 56 years, with most participants (n=8) being 30 years or younger (average age of 26.5 years), and two participants above 30 years (average age of 46.5 years). Nine participants did not smoke cigarettes, and six participants consumed alcohol. The dietary analysis showed that most participants did not follow a particular dietary type and were considered omnivores, however, two participants were either vegan or pescatarian. Australian Recommended Food Score (ARFS) was calculated as an average from AES results obtained before intervention commencement and at the completion of the study. For the sampling, 80 faecal samples were collected, with 3 faecal samples lost in transit. A total of 77 samples were analysed for this study.
2.2. DNA quality
There were 14,883,521 high-quality 16S rRNA sequences obtained with a mean of 173,579 forward and reverse reads per sample from 77 samples in addition to 8 repeats for quality control purposes.
2.3. Phylogenetic taxonomy of the gut microbiota
The gut microbiota taxonomy for all samples from each participant were visualised at the phylum level using taxa bar plots (Figure 1). This graph shows that Bacteroidetes (green) and Firmicutes (purple) were the two dominant phyla across all samples. Furthermore, the plot shows that the taxa of gut microbiota in participants vary from each other. However, the ratio of Firmicutes/ Bacteroidetes fluctuated over the time points and was not statistically significant.
2.4. Associations of alpha diversity of gut microbiota with explanatory factors
The rarefaction plot generated using Shannon’s index [41] showed a maximum depth of 47,647 based on the median frequency value from the frequency per sample results. This is sufficient for analysis as a levelling out on the Y-axis was observed at this depth, indicating additional sequences beyond this depth would unlikely result in additional observed features.
The association of alpha diversity metrics with explanatory factors using Kruskal-Wallis analysis was performed on sequences pooled according to explanatory factors (Table 2). These factors were participant, sex, age group, cigarette smoking, alcohol consumption, and ARFS group. Association of alpha diversity was also determined for time point (1-8), experimental phase (baseline, low dose, washout, high dose, and post-intervention), RBAC dosage (0g/day, 1g/day, and 3g/day), and interventional period (baseline to experimental period including washout and post-intervention). Participant was the only factor that showed a statistically significant effect on alpha diversity in Shannon’s evenness (p=9.66e-8) and Faith’s PD (p=0.002). Statistically significant changes in Shannon’s evenness were shown for alcohol consumption (p=7.92e-6), cigarette smoking (p=0.008), sex (p=0.003), and ARFS group (p=0.032). There were no significant changes in alpha diversity across age group, time point, experimental phase, RBAC dosage, and interventional period.
2.5. Associations of beta diversity of gut microbiota with explanatory factors
Associations of beta diversity with explanatory factors were determined using PERMANOVA (Table 3). Participant sequence data were grouped according to the explanatory factor being tested using the same technique as alpha diversity analysis. Statistically significant differences in beta diversities were found across participant (p=0.001), sex (p=0.001), alcohol consumption (p=0.001), ARFS group (p=0.001), and age group (p≤0.013). Cigarette smoking was significantly associated with all matrices (p=0.001) except weighted unifrac (p=0.1). The analysis for time point, experimental phase, RBAC dosage, and interventional period did not show statistically significant associations with any beta diversity measurements.
An EMPeror plot of Bray Curtis beta diversity showing clustering according to individual participants is demonstrated in Figure 2. These association analyses showed that participant is the major explanatory factor associated with both alpha and beta diversity patterns. This finding suggests that individuality is a critical determinant of microbial diversity.
These findings suggest the requirement to analyse beta diversity for each participant to determine whether there were statistically significant longitudinal changes from baseline across the experimental period. Individual beta diversity for each participant across samples (1-8) was calculated using weighted unifrac and Bray Curtis methods (Table 4).
The explanatory factors used for this analysis were RBAC dosage, experimental phase, and interventional period. In P02, the interventional period was significantly associated with weighted unifrac (p=0.01) and Bray Curtis (p=0.012) beta diversity methods. In P03, the experimental phase and interventional period were significantly associated with both methods (p≤0.052). P04 observed associated changes in RBAC dosage for both methods (p=0.035 and p=0.018, respectively), as well as the experimental phase with Bray Curtis (p=0.044). In P07, the experimental phase (p=0.025) and interventional period (p=0.025) were significantly associated with Bray Curtis. In P08, RBAC dosage was significantly associated with both methods (p<0.05), and experimental phase and interventional period for Bray Curtis only. P09 observed that dosage and experimental phase were significantly associated (p<0.05) with both methods. It is further noted that P05 and P10 showed marginally significant values in Bray Curtis method for the experimental phase.
The longitudinal findings are illustrated using the weighted unifrac beta diversity distance matrices across the 8 time points in EMPeror plots for selected participants (Figure 3). For P03, all timepoints after baseline (red points) show a significant change. For P03, all timepoints after baseline (red points) show a significant change. The graph for P04 illustrates an increase from baseline in the low dose interventional period (orange points), but no change in the high dose (blue points) or washout (green points) periods. P01 shows no change across any timepoints from the baseline. Technical replicates are presented on the graph and are shown on their associated time point alongside the sample. Please refer to Figure S1 of the supplementary materials for the plots for all participants.
2.6. Detection of the association of microbial diversity with interactions of explanatory factors
Further investigation was carried out to determine whether multiple variables could explain the variation in participants’ gut microbiota and reduce false positives in the beta diversity analysis. The calculated unifrac distance matrix was used to perform an Adonis PERMANOVA test on participant and other explanatory factors, including RBAC dosage, experimental phase, time point, and interventional period. The results showed that the variable participant (R2=0.796, p=0.001) explains approximately 80% of variance in the beta diversity. of the variance in the beta diversity. Regression analysis with linear models showed a statistical significance for the experimental phase (R2=0.019, p=0.026) and intervention (R2=0.012, p=0.011). Hence, after participants’ variation was accounted for, the experimental and interventional periods explain approximately 2% of the variance observed in beta diversity with the remaining 18% of variance unaccounted for.
2.7. Significant taxonomic changes from baseline to interventional period
Taxonomic changes from baseline to the interventional period were statistically assessed using ANCOM. Data for all statistically significant changes with a W value of 5 or above are listed in Table 5. Associated changes were compared from baseline to the total interventional period unless otherwise specified. These results show statistically significant taxonomic changes (from baseline) detected down to a species level for 7 participants - P01, P02, P03, P07, P08, P09 and P10.
In P01, a marked increase in the Hungatella genus with a W value of 40 was revealed and less marked changes across other genera and families were observed. In P02, decreases in Anaerococcus, Corynebacterium, and Finegoldia genera were detected with W values ranging between 48 to 64. Large declines in Dialister (W=94) and Gastranaerophilales (W=86) were observed in P03. A large decrease in Erysipelatoclostridiaceae (W=102) was displayed in P07. In P08, there was a decrease in the Eubacterium siraeum group (W=35) and lower significant changes in other bacterial genera. P09 revealed large increases in multiple bacterial genera, including Eubacterium siraeum, (W=38). This participant also showed smaller increases in Eubacterium hallii group and Stomatobaculum (W=5 for each) and further smaller increases in Anaerococcus, Ruminococcus, Megasphaera, Solobacterium (W=7-8) in either low or high RBAC doses. P10 shows a large decrease in Prevotella (W=20) and smaller changes across other groups. Some changes were only detected during the washout stage, as observed in P01.
3. Discussion
The purpose of this clinical study was to determine changes in the gut microbial composition in response to dietary RBAC supplementation in healthy adults. Our results revealed that alpha and beta diversity were not associated with experimental phase, interventional period, RBAC dosage, or time point. This suggests that the dietary supplementation did not significantly moderate the gut microbiota composition. However, the absence of supplementation effect on the gut microbiota composition should be further explicated. Firstly, the unknown species are not accounted for in alpha diversity measurements. This indicates that the true richness and evenness of the microbial environment was not fully examined in the present study. Consequently, the results on alpha diversity may be misrepresented [42]. Secondly, the finding that participant is a significant determinant for alpha and beta diversity suggests that the individual microbiome requires separate assessment alongside the explanatory factors during RBAC supplementation on gut microbiota.
The present research findings revealed differences in alpha and beta diversity of gut microbiota within individual participants. Gut microbial composition presents a profile that is distinct to the individual, with moderating factors such as genetic, environment, and lifestyle [43]. Previous research on twins has indicated heritable common gut microbiota, with cohabitating twins sharing the highest number of strains [44]. However, differences in the microbiota between twins were also shown in previous studies, indicating non-genetic factors are also at play [43,44]. Since genetics and environment are known factors influencing gut microbiota composition, it was not unexpected that the microbial composition between participants significantly differed in the present study. Compounding these factors is the individual lifestyle, which further impacts microbiota diversity among participants [45].
The present results also revealed significant association between alpha (Shannon’s evenness) and beta diversity with alcohol consumption, cigarette smoking, and diet (Australian Recommended Food Score, ARFS). Alcohol consumption has been shown to affect gut microbiota and has been linked to substantial losses in diversity, including reductions in Bacteroidetes and Firmicutes [46]. Alcohol consumption also correlates with decreased connectivity of the microbial network and subsequent alteration of gut microbiome composition [28]. Cigarette smoking causes taxonomic changes in gut microbiota, specifically decreased Bacteroidetes and increased Firmicutes, due to nicotine exposure [47]. Moreover, after smoking cessation, increased alpha diversity of gut microbiota was observed [27]. Due to the toxic effects on gut mucosa, cigarette smoking has also been linked to gut microbial dysbiosis [47]. The present study identified lifestyle including diet and subsequent ARFS, alcohol consumption, and cigarette smoking are important factors that impact gut microbiota in healthy adults.
Five of the six participants in the present study that were categorised in the highest ARFS groups revealed significant changes in beta diversity. Although there is limited research on how the ARFS is associated with the gut microbiome, Aslam et al. [48] reported that higher ARFS correlated with the consumption of a more diverse diet, with differences shown in beta diversity compared to limited diets with lower ARFS. Hence, the association of ARFS with changes in beta diversity may be explained by the differences between the consumption of core foods (e.g. grains and water) and discretionary foods (e.g. fried products and packaged sweets) in the diet [49]. The increased consumption of core foods and low discretionary foods also shows a higher proportion of complex carbohydrates that benefits gut microbiota. This may explain the significant changes observed in beta diversity for participants with a higher ARFS in the present study [49].
Age group as an explanatory factor was revealed to be associated with significant changes in beta diversity. Considerable shifts in the microbiome have previously been shown during infancy, puberty, to the later stage of life (>75 years of age) [21]. The stability of the microbiome is reached during adulthood (18-25 years of age) and remains relatively constant until approximately 75 years of age when a loss of diversity occurs [21]. However, Odamaki et al. [23] observed significant differences between adult clusters at the ages of 33 (cluster 1) and 42 (cluster 2), with higher levels of Bacteroidetes observed in the younger age group (cluster 1). This is consistent with the significant differences in beta diversity observed in the present study for participants ≤30 years and >30 years of age.
Associations between sex, and alpha and beta diversity were observed. Sex is a known modulator of the gut microbiome through the actions of sex hormones [50]. This is supported by recent studies showing that sex is a prime contributor to microbial diversity with increased alpha diversity observed in females compared to males [51,52]. Furthermore, sex has also been linked to responses of gut microbiota to diet, anti-microbial effects, and obesity [50,53]. The present findings affirm that age and sex significantly influence gut microbiota composition within healthy adults.
Dietary RBAC supplementation was shown to change the abundance of beneficial bacteria including Lactobacillus, Roseburia, and Ruminococcaceae, although these changes were not observed in all participants. Some participants exhibited trends in taxonomic changes during the interventional period. For example, participant 9 (P09) showed increases across multiple genera. These beneficial bacteria play a vital role in gut health through the production of SCFAs as essential energy sources for colonic enterocytes [12,14], the provision of vitamins [10], and possess anti-inflammatory properties [13]. This finding suggests that dietary RBAC supplementation may be used as a prebiotic for regulating these beneficial bacteria.
The increases in beneficial bacteria observed in some participants may also be associated with the ARFS. Diets with less diversity have been associated with lower bacterial variety [54]. Of the four participants who exhibited taxonomic changes in beneficial bacteria, three had the lowest ARFS. Hence, this finding suggests a potential association between RBAC supplementation responses and ARFS. This indicates that RBAC supplementation may influence the growth of beneficial gut microbiota of people with diets that are lower in core foods and higher in discretionary foods. In addition to increased beneficial bacteria, there were also reductions in bacteria known to be opportunistic pathogens, including Anaerococcus and Corynebacterium [55,56]. However, these taxonomic changes are difficult to interpret due to the difference in gut microbiota between individuals and how rapidly the gut microbiome can change in response to daily diet and lifestyle factors [45].
In six participants, significant changes in beta diversity were associated with RBAC dosage, experimental phase, and/or interventional period. Previous research has indicated that the composition and diversity of the gut microbiome can determine whether participants respond to interventions including dietary modification for health-related purposes [57]. This is further extended to other interventions such as treatments for cervical cancer and responsiveness to exercise for prediabetes treatment [57,58,59]. The present study used multiple analyses to classify participants into two groups, responders and non-responders to RBAC supplementation [60]. Four participants (P02, P03, P07, and P09) observed significant changes in all three classification criteria of individual beta diversity, weighted unifrac EMPeror plots, and taxonomic analysis, thus making them responders to RBAC supplementation. Two participants (P04 and P08) revealed changes in two criteria, hence they were probable responders to RBAC supplementation, however further supplementation and analysis is required to determine whether these participants can be classified as responders. Two participants (P01 and P10) only showed microbial taxonomic changes, therefore were unlikely to be responders to the supplementation. Further two participants (P05 and P06) showing no statistical changes across the analyses were considered non-responders to the RBAC supplementation.
Given the sample size in the present study, further research with a larger sample size is required. As demonstrated in the present study, research aiming to investigate the effects of dietary RBAC supplementation on gut microbiota may require controlling for individual characteristics as confounding factors, such as age. Also individualised doses according to body weight may be more appropriate to assess the impact of supplementation and dosage on gut microbiota. A further limitation of this study was the short timeframe of the intervention. An extended period of supplementation may reveal further changes in gut microbiota composition. Maintaining a food journal by participants to track the dietary intake and physical activity could be correlated with gut microbiota composition [45].
4. Materials and Methods
4.1. Participant recruitment and diet tracking
Ten healthy adult volunteers were recruited through University presentations and social media posts. The inclusion criteria comprised healthy adults aged 18-60 years old with informed consent. Exclusion criteria encompassed chronic health conditions and reported gut dysbiosis, ongoing medication use, history of antibiotic use in the three months prior to taking the first dietary supplement, and pregnancy or breastfeeding. Participants were required to maintain their usual diet with no major changes (e.g., changes from omnivore to vegan or vegetarian).
Baseline demographic data were collected in a screening survey before study commencement. Dietary intake was tracked by participants completing an online food frequency questionnaire, the AES, before study commencement and at study completion. Data collated from the AES detailed the participants’ macronutrient intake as well as the percentage of discretionary and core food intakes. An ARFS was obtained from survey results for each participant [61]. These scores were categorised into very low (<23), low (24-29), medium (30-33, high (34-40), and very high (>40) levels of core food intakes in the diet.
4.2. Design and intervention
The study intervention required participants to supplement their regular diet with two doses of RBAC, a low dose (1g per day for 6 consecutive weeks) and a high dose (3g per day for 6 consecutive weeks). Each RBAC sachet contained 1g of RBAC as the active ingredient plus microcrystalline cellulose (0.50g), modified starch (0.26g), dextrin (0.20g), and tricalcium phosphate (0.04g) as excipients. The net weight in each sachet amounted to 2g. Participants were instructed to take 1 sachet per day for 6 weeks (low dose), then 3 sachets per day for 6 weeks (high dose), with a washout period of 3 weeks between these doses. Two baseline faecal samples were collected to establish the individual baseline, and one post-intervention faecal sample was collected to assess for ongoing effects. Implementation of this design resulted in a total of 8 time points for faecal sample collection over 21 weeks. This interventional design was implemented as per the schedule shown in Table 6.
4.3. Faecal sample collection, preservation, and DNA extraction
Faecal samples were collected by participants using a faecal swab collection and preservation system (cat. 45670-B, Norgen Biotek Corp Thorold, Ontario, Canada). Nucleic acid within the collected swab remains stable for up to 2 years with DNA stored in the buffer at room temperature [62]. Participants were instructed to swab their faeces at the start of the sampling week as per the sample schedule and place the swab in the provided vial containing buffer. Swabs were either collected or posted from participants and stored in a -80°C freezer. Faecal samples were subjected to DNA extraction using the microbiome DNA isolation kit (cat. 64100, Norgen Biotek Corp, Thorold, Ontario, Canada). For the lysate preparation, swabs were briefly vortexed before 500 L of the sample faecal/buffer mixture was transferred to a DNAase-free microcentrifuge tube. Lysis buffers E and A were added as per product procedure and samples were incubated in a 65°C water bath for 10 minutes. Column binding and column washing were performed as per product procedure. DNA elution was completed twice to improve total yield.
4.4. Amplification and sequencing of extracted microbial DNA
The concentration and purity of the extracted DNA were determined for each sample using the Nanodrop 2000 spectrophotometer (ThermoFisher Scientific, Waltham, Massachusetts, USA). DNA concentration and purity (260/280 ratio) were noted for sequencing submission. As per MyTaq Red Mix procedure, PCRs were performed on randomly selected extractions to ensure the extracted DNA was primarily of microbial origin and suitable for downstream analysis. Primers (0341-CCTACGGGNGGCWGCAG and 0785-GACTACHVGGGTATCTAATCC 16S rRNA target primers) were diluted to a 1:5 ratio [63]. A master mix was prepared and PCR was conducted as per MyTaq Red Mix insert procedure and electrophoresis using E-Gel precast Agarose Electrophoresis System 1%. Ten (10) L of sample and 20 L of a 1-kb DNA ladder (Sigma-Aldrich-D0428) were used, two wells (10 and 11) were loaded as a positive and negative control, respectively.
Thirty (30) L of the extracted DNA samples were prepared in a round bottom 96 well microplate, sealed and transported to Ramaciotti Centre for Genomics (UNSW, Sydney, NSW, Australia). DNA amplification and sequencing were performed on the Illumina MiSeq platform, targeting the gene region 16S rRNA V3-V4 using primers 341-forward and 805-reverse.
4.5. Microbiota profiling and statistical analysis
Microbiota profiling and statistical analysis were performed using the QIIME2 platform [64]. Data were imported to QIIME2 following the Casava 1.8 paired end demultiplexed fastq instructions. The DADA2 plugin was used to find amplicon sequences, remove chimeric sequences, and minimise noise created by spurious operational taxonomic units [65]. The trim and truncating parameters (from 5’ – 3’) were run with truncating-length-forward 285 and truncating-length-reverse 220, and used for data analysis due to sequencing quality cut-offs and sequencing depths.
Phylogenetic taxonomy was assigned to the sequencing data using VSEARCH with QIIME-compatible SILVA release 138 SSURef NR99 full-length region sequences and 138 SSURef NR99 full-length region taxonomy [66]. Taxonomic changes were determined using the analysis of the composition of microbiota with bias correction (ANCOM) method, where the statistical significance was determined using a W value [67]. A one-way ANOVA was performed on the data to determine significant changes over time.
Alpha diversity (richness and evenness) and beta diversity (change in compositions over time) analyses were completed using QIIME2 q2-diversity plugin based on a phylogenetic diversity tree. This was generated with a sampling depth of 26430 determined by 56.32% of retained features in 100% of samples. Alpha diversity applying Shannon’s evenness and Faith’s phylogenetic diversity (Faith’s PD) were calculated using Kruskal-Wallis H test, with the data being pooled and ranked from smallest to largest (one-way ANOVA on ranks).
Beta diversity was calculated using four different methods: unweighted unique fraction metric (unifrac), weighted unifrac, Bray Curtis, and Jaccard. Statistical analysis of beta diversity was based on the permutational multivariate analysis of variance (PERMANOVA). Analyses were performed to identify associations of beta diversity with explanatory factors and the RBAC supplementation. The Adonis PERMANOVA test for beta diversity significance in QIIME2 was used to determine significant factors that affect beta diversity through fitting polynomial regression models [68].
Participants were classified as responders to RBAC intervention if they exhibited significant changes across three analysis methods (with p<0.05). This included individual beta diversity analysis, changes to beta diversity visualised with Earth Microbiome Project (EMPeror) plots across experimental phases, and alterations in taxonomic compositions. Multiple analyses were performed to reduce the likelihood of false positives due to the limited sample size.
5. Conclusions
Overall, the present study revealed that individual factors such as age and lifestyle significantly influence alpha and beta diversity of human gut microbiota. Dietary supplementation of RBAC was shown to influence the beta diversity of gut bacteria of most participants. Based on individual changes in the gut microbiota profile, participants were classified as responders or non-responders. RBAC supplementation was shown to influence the abundance of the beneficial bacteria, Bifidobacterium, Lactobacillus, Roseburia, Ruminococcaceae, and Faecalibacterium in five participants. These findings suggest that fermentation and degradation of RBAC by gut microbiota may be highly individualised. This evidence advocates further research controlling for participant characteristics such as age and lifestyle during dietary supplementation on the gut microbiota in healthy adults.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: EMPeror plots of weighted unifrac beta diversity distance matrix of each participant.
Author Contributions
Conceptualization, E.S., S.L.O., P.S.M., and S.C.P.; methodology, E.S., S.L.O., S.C.P., P.S.M., S.W. and T.J.; software, S.L.O.; validation, T.J. and S.W.; formal analysis, investigation, data curation, S.L.O., E.S. and T.J.; resources, S.C.P. and S.W.; writing—original draft preparation, E.S.; writing—review and editing, S.W., P.S.M., T.J., S.L.O. and S.C.P.; visualization, S.L.O. and E.S.; supervision, S.W., P.S.M. and S.C.P.; project administration, S.W. and S.C.P.; funding acquisition, S.C.P. All authors have read and agreed to the published version of the manuscript.
Funding
Funding and endowing the rice bran arabinoxylan compound for use in this research study was provided by BioMedica Nutraceuticals Pty Ltd (Sydney, NSW, Australia). The open access publication fee is partially supported by Charles Sturt University.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The Human research ethics committee at Charles Sturt University approved this research (protocol number ES03393) in compliance with the Australian National Statement on Ethical Conduct in Human Research.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding authors, (S.W. or S.C.P), upon reasonable request
Acknowledgments
The authors would like to thank the participants for volunteering their time and persistent efforts in collecting samples over the study period. The authors also wish to acknowledge the contributions of Professor Emad El-Omar and Dr Terry Golombick in conceptualising the initial research idea.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AES | Australian Eating Survey® |
| ARFS | Australian Recommended Food Score |
| DNA | Deoxyribonucleic acid |
| EMPeror | Earth Microbiome Project |
| PERMANOVA | Permutational multivariate analysis of variance |
| RBAC | Rice bran arabinoxylan compound |
| rRNA | Ribosomal ribonucleic acid |
| SCFAs | Short-chain fatty acids |
References
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the gut microbiota in nutrition and health. BMJ 2018, 361. [Google Scholar] [CrossRef]
- Malard, F.; Dore, J.; Gaugler, B.; Mohty, M. Introduction to host microbiome symbiosis in health and disease. Mucosal Immunology 2021, 14, 547–554. [Google Scholar] [CrossRef]
- Forbes, J.D.; Domselaar, G.V.; Bernstein, C.N. Microbiome survey of the inflamed and noninflamed gut at different compartments within the gastrointestinal tract of inflammatory bowel disease patients. Inflammatory Bowel Diseases 2016, 22, 817–825. [Google Scholar] [CrossRef]
- Mendis, M.; Leclerc, E.; Simsek, S. Arabinoxylans, gut microbiota and immunity. Carbohydrate Polymers 2016, 139, 159–166. [Google Scholar] [CrossRef]
- Scott, K.P.; Jean-Michel, A.; Midtvedt, T.; van Hemert, S. Manipulating the gut microbiota to maintain health and treat disease. Microbial Ecology in Health and Disease 2015, 26, 25877. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.; Gasbarrini, A.; Mele, M.C. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- King, C.H.; Desai, H.; Sylvetsky, A.C.; LoTempio, J.; Ayanyan, S.; Carrie, J.; Crandall, K.A.; Fochtman, B.C.; Gasparyan, L.; Gulzar, N.; Howell, P.; Issa, N.; Krampis, K.; Mishra, L.; Morizono, H.; Pisegna, J.R.; Rao, S.; Ren, Y.; Simonyan, V.; Smith, K.; VedBrat, S.; Yao, M.D.; Mazumder, R. Baseline human gut microbiota profile in healthy people and standard reporting template. PLOS ONE 2019, 14, e0206484. [Google Scholar] [CrossRef]
- Ventura, M.; Turroni, F.; Lugli, G.A.; van Sinderen, D. Bifidobacteria and humans: our special friends, from ecological to genomics perspectives. Journal of the Science of Food and Agriculture 2014, 94, 163–168. [Google Scholar] [CrossRef]
- Hald, S.; Schioldan, A.G.; Moore, M.E.; Dige, A.; Lærke, H.N.; Agnholt, J.; Knudsen, K.E.B.; Hermansen, K.; Marco, M.L.; Gregersen, S.; Dahlerup, J.F. Effects of arabinoxylan and resistant starch on intestinal microbiota and short-chain fatty acids in subjects with metabolic syndrome: a randomised crossover study. PLOS ONE 2016, 11, e0159223. [Google Scholar] [CrossRef]
- O’Callaghan, A.; van Sinderen, D. Bifidobacteria and their role as members of the human gut microbiota. Frontiers in Microbiology 2016, 7, 925. [Google Scholar] [CrossRef]
- Rossi, M.; Martínez-Martínez, D.; Amaretti, A.; Ulrici, A.; Raimondi, S.; Moya, A. Mining metagenomic whole genome sequences revealed subdominant but constant Lactobacillus population in the human gut microbiota. Environmental Microbiology Reports 2016, 8, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Mu, Q.; Tavella, V.J.; Luo, X.M. Role of Lactobacillus reuteri in human health and diseases. Frontiers in Microbiology 2018, 9, 757. [Google Scholar] [CrossRef]
- Tamanai-Shacoori, Z.; Smida, I.; Bousarghin, L.; Loreal, O.; Meuric, V.; Fong, S.B.; Bonnaure-Mallet, M.; Jolivet-Gougeon, A. Roseburia spp.: a marker of health? Future Microbiology 2017, 12, 157–170. [Google Scholar] [CrossRef]
- Gu, X.; Sim, J.X.Y.; Lee, W.L.; Cui, L.; Chan, Y.F.Z.; Chang, E.D.; Teh, Y.E.; Zhang, A.N.; Armas, F.; Chandra, F.; Chen, H.; Zhao, S.; Lee, Z.; Thompson, J.R.; Ooi, E.E.; Low, J.G.; Alm, E.J.; Kalimuddin, S. Low gut Ruminococcaceae levels are associated with occurrence of antibiotic-associated diarrhea. medRxiv 2021. [Google Scholar] [CrossRef]
- Neyrinck, A.M.; Possemiers, S.; Druart, C.; de Wiele, T.V.; Backer, F.D.; Cani, P.D.; Larondelle, Y.; Delzenne, N.M. Prebiotic effects of wheat arabinoxylan related to the increase in Bifidobacteria, Roseburia and Bacteroides/Prevotella in diet-induced obese mice. PLOS ONE 2011, 6, e20944. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.W.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal Microbial Metabolism of Phosphatidylcholine and Cardiovascular Risk. New England Journal of Medicine 2013, 368, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- de Mello, V.D.; Paananen, J.; Lindström, J.; Lankinen, M.A.; Shi, L.; Kuusisto, J.; Pihlajamäki, J.; Auriola, S.; Lehtonen, M.; Rolandsson, O.; Bergdahl, I.A.; Nordin, E.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Landberg, R.; Eriksson, J.G.; Tuomilehto, J.; Hanhineva, K.; Uusitupa, M. Indolepropionic acid and novel lipid metabolites are associated with a lower risk of type 2 diabetes in the Finnish diabetes prevention study. Scientific Reports 2017, 7, 46337. [Google Scholar] [CrossRef] [PubMed]
- Influence of diet on the gut microbiome and implications for human health. Journal of Translational Medicine 2017, 15, 73. [CrossRef]
- Bowyer, R.C.E.; Jackson, M.A.; Roy, C.I.L.; Lochlainn, M.N.; Spector, T.D.; Dowd, J.B.; Steves, C.J. Socioeconomic status and the gut microbiome: a TwinsUK cohort study. Microorganisms 2019, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Carson, T.L.; Wang, F.; Cui, X.; Jackson, B.E.; Pol, W.J.V.D.; Lefkowitz, E.J.; Morrow, C.; Baskin, M.L. Associations between race, perceived psychological stress, and the gut microbiota in a sample of generally healthy black and white women: a pilot study on the role of race and perceived psychological stress. Psychosomatic Medicine 2018, 80, 640–648. [Google Scholar] [CrossRef]
- Nagpal, R.; Mainali, R.; Ahmadi, S.; Wang, S.; Singh, R.; Kavanagh, K.; Kitzman, D.W.; Kushugulova, A.; Marotta, F.; Yadav, H. Gut microbiome and aging: Physiological and mechanistic insights. Nutrition and Healthy Aging 2018, 4, 267–285. [Google Scholar] [CrossRef]
- Qin, J.; Li, R.; Raes, J.; Arumugam, M.; Burgdorf, K.S.; Manichanh, C.; Nielsen, T.; Pons, N.; Levenez, F.; Yamada, T.; Mende, D.R.; Li, J.; Xu, J.; Li, S.; Li, D.; Cao, J.; Wang, B.; Liang, H.; Zheng, H.; Xie, Y.; Tap, J.; Lepage, P.; Bertalan, M.; Batto, J.M.; Hansen, T.; Paslier, D.L.; Linneberg, A.; Nielsen, H.B.; Pelletier, E.; Renault, P.; Sicheritz-Ponten, T.; Turner, K.; Zhu, H.; Yu, C.; Li, S.; Jian, M.; Zhou, Y.; Li, Y.; Zhang, X.; Li, S.; Qin, N.; Yang, H.; Wang, J.; Brunak, S.; Doré, J.; Guarner, F.; Kristiansen, K.; Pedersen, O.; Parkhill, J.; Weissenbach, J.; Antolin, M.; Artiguenave, F.; Blottiere, H.; Borruel, N.; Bruls, T.; Casellas, F.; Chervaux, C.; Cultrone, A.; Delorme, C.; Denariaz, G.; Dervyn, R.; Forte, M.; Friss, C.; van de Guchte, M.; Guedon, E.; Haimet, F.; Jamet, A.; Juste, C.; Kaci, G.; Kleerebezem, M.; Knol, J.; Kristensen, M.; Layec, S.; Roux, K.L.; Leclerc, M.; Maguin, E.; Minardi, R.M.; Oozeer, R.; Rescigno, M.; Sanchez, N.; Tims, S.; Torrejon, T.; Varela, E.; de Vos, W.; Winogradsky, Y.; Zoetendal, E.; Bork, P.; Ehrlich, S.D.; Wang, J.; Consortium, M. A human gut microbial gene catalogue established by metagenomic sequencing. Nature 2010, 464, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Odamaki, T.; Kato, K.; Sugahara, H.; Hashikura, N.; Takahashi, S.; zhong Xiao, J.; Abe, F.; Osawa, R. Age-related changes in gut microbiota composition from newborn to centenarian: a cross-sectional study. BMC Microbiology 2016, 16, 90. [Google Scholar] [CrossRef]
- Nagpal, R.; Tsuji, H.; Takahashi, T.; Kawashima, K.; Nagata, S.; Nomoto, K.; Yamashiro, Y. Sensitive quantitative analysis of the meconium bacterial microbiota in healthy term infants born vaginally or by cesarean section. Frontiers in Microbiology 2016, 7, 1997. [Google Scholar] [CrossRef]
- Claesson, M.J.; Jeffery, I.B.; Conde, S.; Power, S.E.; O’Connor, E.M.; Cusack, S.; Harris, H.M.B.; Coakley, M.; Lakshminarayanan, B.; O’Sullivan, O.; Fitzgerald, G.F.; Deane, J.; O’Connor, M.; Harnedy, N.; O’Connor, K.; O’Mahony, D.; van Sinderen, D.; Wallace, M.; Brennan, L.; Stanton, C.; Marchesi, J.R.; Fitzgerald, A.P.; Shanahan, F.; Hill, C.; Ross, R.P.; O’Toole, P.W. Gut microbiota composition correlates with diet and health in the elderly. Nature 2012, 488, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Gavini, F.; Cayuela, C.; Antoine, J.M.; Lecoq, C.; Lefebvre, B.; Membré, J.M.; Neut, C. Differences in the distribution of bifidobacterial and enterobacterial species in human faecal microflora of three different (children, adults, elderly) age groups. Microbial Ecology in Health and Disease 2001, 13, 40–45. [Google Scholar] [CrossRef]
- Biedermann, L.; Zeitz, J.; Mwinyi, J.; Sutter-Minder, E.; Rehman, A.; Ott, S.J.; Steurer-Stey, C.; Frei, A.; Frei, P.; Scharl, M.; Loessner, M.J.; Vavricka, S.R.; Fried, M.; Schreiber, S.; Schuppler, M.; Rogler, G. Smoking Cessation Induces Profound Changes in the Composition of the Intestinal Microbiota in Humans. PLOS ONE 2013, 8, e59260. [Google Scholar] [CrossRef]
- Mutlu, E.A.; Gillevet, P.M.; Rangwala, H.; Sikaroodi, M.; Naqvi, A.; Engen, P.A.; Kwasny, M.; Lau, C.K.; Keshavarzian, A. Colonic microbiome is altered in alcoholism. American Journal of Physiology-Gastrointestinal and Liver Physiology 2012, 302, G966–G978. [Google Scholar] [CrossRef]
- Leeming, E.R.; Johnson, A.J.; Spector, T.D.; Le Roy, C.I. Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Zhurlova, O.D.; Kaprelyants, L.V. The current trends and future perspectives of arabinoxylans prebiotics research: A review. Grain Products and Mixed Fodder’s 2017, 17, 4–11, https://journals.ontu.edu.ua/index.php/gpmf/article/view/760/662. Accessed: 2022-10-28. [Google Scholar]
- Ooi, S.L.; Pak, S.C.; Micalos, P.S.; Schupfer, E.; Lockley, C.; Park, M.H.; Hwang, S.J. The health-promoting properties and clinical applications of rice bran arabinoxylan modified with shiitake mushroom enzyme-a narrative review. Molecules 2021, 26. [Google Scholar] [CrossRef]
- Schupfer, E.; Pak, S.C.; Wang, S.; Micalos, P.S.; Jeffries, T.; Ooi, S.L.; Golombick, T.; Harris, G.; El-Omar, E. The effects and benefits of arabinoxylans on human gut microbiota – A narrative review. Food Bioscience 2021, 43, 101267–101267. [Google Scholar] [CrossRef]
- Tsai, Y.L.; Lin, T.L.; Chang, C.J.; Wu, T.R.; Lai, W.F.; Lu, C.C.; Lai, H.C. Probiotics, prebiotics and amelioration of diseases. Journal of Biomedical Science 2019, 26, 3. [Google Scholar] [CrossRef]
- Salden, B.N.; Troost, F.J.; Wilms, E.; Truchado, P.; Vilchez-Vargas, R.; Pieper, D.H.; Jáuregui, R.; Marzorati, M.; van de Wiele, T.; Possemiers, S.; Masclee, A.A. Reinforcement of intestinal epithelial barrier by arabinoxylans in overweight and obese subjects: A randomized controlled trial. Clinical Nutrition 2018, 37, 471–480. [Google Scholar] [CrossRef] [PubMed]
- François, I.E.J.A.; Lescroart, O.; Veraverbeke, W.S.; Marzorati, M.; Possemiers, S.; Evenepoel, P.; Hamer, H.; Houben, E.; Windey, K.; Welling, G.W.; Delcour, J.A.; Courtin, C.M.; Verbeke, K.; Broekaert, W.F. Effects of a wheat bran extract containing arabinoxylan oligosaccharides on gastrointestinal health parameters in healthy adult human volunteers: a double-blind, randomised, placebo-controlled, cross-over trial. British Journal of Nutrition 2012, 108, 2229–2242. [Google Scholar] [CrossRef]
- Kjølbæk, L.; Benítez-Páez, A.; del Pulgar, E.M.G.; Brahe, L.K.; Liebisch, G.; Matysik, S.; Rampelli, S.; Vermeiren, J.; Brigidi, P.; Larsen, L.H.; Astrup, A.; Sanz, Y. Arabinoxylan oligosaccharides and polyunsaturated fatty acid effects on gut microbiota and metabolic markers in overweight individuals with signs of metabolic syndrome: A randomized cross-over trial. Clinical Nutrition 2020, 39, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Chudan, S.; Ishibashi, R.; Nishikawa, M.; Tabuchi, Y.; Nagai, Y.; Ikushiro, S.; Furusawa, Y. Effect of Wheat-Derived Arabinoxylan on the Gut Microbiota Composition and Colonic Regulatory T Cells. Molecules 2023, 28. [Google Scholar] [CrossRef] [PubMed]
- Grootaert, C.; Delcour, J.A.; Courtin, C.M.; Broekaert, W.F.; Verstraete, W.; de Wiele, T.V. Microbial metabolism and prebiotic potency of arabinoxylan oligosaccharides in the human intestine. Trends in Food Science & Technology 2007, 18, 64–71. [Google Scholar] [CrossRef]
- Walton, G.E.; Lu, C.; Trogh, I.; Arnaut, F.; Gibson, G.R. A randomised, double-blind, placebo controlled cross-over study to determine the gastrointestinal effects of consumption of arabinoxylan-oligosaccharides enriched bread in healthy volunteers. Nutrition Journal 2012, 11, 36. [Google Scholar] [CrossRef]
- Daiwa Pharmaceutical Co., Ltd. BioBran® Rice Bran Arabinoxylan Compound. https://www.biobran.org/uploads/downloads/BioBran_guide_new.pdf?v1.1.2, 2016. Accessed: 2022-10-28.
- Shannon, C.E. A mathematical theory of communication. Bell System Technical Journal 1948, 27, 379–423. [Google Scholar] [CrossRef]
- Wagner, B.D.; Grunwald, G.K.; Zerbe, G.O.; Mikulich-Gilbertson, S.K.; Robertson, C.E.; Zemanick, E.T.; Harris, J.K. On the use of diversity measures in longitudinal sequencing studies of microbial communities. Frontiers in Microbiology 2018, 9, 1037. [Google Scholar] [CrossRef]
- Goodrich, J.; Davenport, E.; Beaumont, M.; Jackson, M.; Knight, R.; Ober, C.; Spector, T.; Bell, J.; Clark, A.; Ley, R. Genetic determinants of the gut microbiome in UK twins. Cell Host & Microbe 2016, 19, 731–743. [Google Scholar] [CrossRef]
- Koo, H.; Hakim, J.A.; Crossman, D.K.; Lefkowitz, E.J.; Morrow, C.D. Sharing of gut microbial strains between selected individual sets of twins cohabitating for decades. PLOS ONE 2019, 14, e0226111. [Google Scholar] [CrossRef]
- David, L.A.; Materna, A.C.; Friedman, J.; Campos-Baptista, M.I.; Blackburn, M.C.; Perrotta, A.; Erdman, S.E.; Alm, E.J. Host lifestyle affects human microbiota on daily timescales. Genome Biology 2014, 15, R89. [Google Scholar] [CrossRef] [PubMed]
- Capurso, G.; Lahner, E. The interaction between smoking, alcohol and the gut microbiome. Best Practice & Research Clinical Gastroenterology 2017, 31, 579–588. [Google Scholar] [CrossRef]
- Lee, S.H.; Yun, Y.; Kim, S.J.; Lee, E.J.; Chang, Y.; Ryu, S.; Shin, H.; Kim, H.L.; Kim, H.N.; Lee, J.H. Association between cigarette smoking status and composition of gut microbiota: population-based cross-sectional study. Journal of Clinical Medicine 2018, 7, 282. [Google Scholar] [CrossRef] [PubMed]
- Aslam, H.; Collier, F.; Davis, J.A.; Quinn, T.P.; O’Hely, M.; Pasco, J.A.; Jacka, F.N.; Loughman, A. Gut microbiome diversity and composition are associated with habitual dairy intakes: a cross-sectional study in men. The Journal of Nutrition 2021, 151, 3400–3412. [Google Scholar] [CrossRef] [PubMed]
- Senghor, B.; Sokhna, C.; Ruimy, R.; Lagier, J.C. Gut microbiota diversity according to dietary habits and geographical provenance. Human Microbiome Journal 2018, 7-8, 1–9. [Google Scholar] [CrossRef]
- Sinha, T.; Vila, A.V.; Garmaeva, S.; Jankipersadsing, S.A.; Imhann, F.; Collij, V.; Bonder, M.J.; Jiang, X.; Gurry, T.; Alm, E.J.; D’Amato, M.; Weersma, R.K.; Scherjon, S.; Wijmenga, C.; Fu, J.; Kurilshikov, A.; Zhernakova, A. Analysis of 1135 gut metagenomes identifies sex-specific resistome profiles. Gut Microbes 2019, 10, 358–366. [Google Scholar] [CrossRef]
- Dominianni, C.; Sinha, R.; Goedert, J.J.; Pei, Z.; Yang, L.; Hayes, R.B.; Ahn, J. Sex, body mass index, and dietary fiber intake influence the human gut microbiome. PLOS ONE 2015, 10, e0124599. [Google Scholar] [CrossRef]
- Valeri, F.; Endres, K. How biological sex of the host shapes its gut microbiota. Frontiers in Neuroendocrinology 2021, 61, 100912. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zhang, M.; Xue, J.; Huang, J.; Zhuang, R.; Zhou, X.; Zhang, H.; Fu, Q.; Hao, Y. Body mass index differences in the gut microbiota are gender specific. Frontiers in Microbiology 2018, 9, 1250. [Google Scholar] [CrossRef]
- Heiman, M.L.; Greenway, F.L. A healthy gastrointestinal microbiome is dependent on dietary diversity. Molecular Metabolism 2016, 5, 317–320. [Google Scholar] [CrossRef]
- LaButti, K.; Pukall, R.; Steenblock, K.; Rio, T.G.D.; Tice, H.; Copeland, A.; Cheng, J.F.; Lucas, S.; Chen, F.; Nolan, M.; Bruce, D.; Goodwin, L.; Pitluck, S.; Ivanova, N.; Mavromatis, K.; Ovchinnikova, G.; Pati, A.; Chen, A.; Palaniappan, K.; Land, M.; Hauser, L.; Chang, Y.J.; Jeffries, C.D.; Chain, P.; Saunders, E.; Brettin, T.; Detter, J.C.; Han, C.; Göker, M.; Bristow, J.; Eisen, J.A.; Markowitz, V.; Hugenholtz, P.; Kyrpides, N.C.; Klenk, H.P.; Lapidus, A. Complete genome sequence of Anaerococcus prevotii type strain (PC1T). Standards in Genomic Sciences 2009, 1, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Bernard, K. The genus Corynebacterium and other medically relevant Coryneform-like bacteria. Journal of Clinical Microbiology 2012, 50, 3152–3158. [Google Scholar] [CrossRef]
- Smits, S.A.; Marcobal, A.; Higginbottom, S.; Sonnenburg, J.L.; Kashyap, P.C. Individualized responses of gut microbiota to dietary intervention modeled in humanized mice. mSystems 2016, 1, e00098–16. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Y.; Ni, Y.; Cheung, C.K.; Lam, K.S.; Wang, Y.; Xia, Z.; Ye, D.; Guo, J.; Tse, M.A.; Panagiotou, G.; Xu, A. Gut microbiome fermentation determines the efficacy of exercise for diabetes prevention. Cell Metabolism 2020, 31, 77–91. [Google Scholar] [CrossRef]
- Sims, T.T.; Alam, M.B.E.; Karpinets, T.V.; Dorta-Estremera, S.; Hegde, V.L.; Nookala, S.; Yoshida-Court, K.; Wu, X.; Biegert, G.W.G.; Medrano, A.Y.D.; Solley, T.; Ahmed-Kaddar, M.; Chapman, B.V.; Sastry, K.J.; Mezzari, M.P.; Petrosino, J.F.; Lin, L.L.; Ramondetta, L.; Jhingran, A.; Schmeler, K.M.; Ajami, N.J.; Wargo, J.; Colbert, L.E.; Klopp, A.H. Gut microbiome diversity is an independent predictor of survival in cervical cancer patients receiving chemoradiation. Communications Biology 2021, 4, 237. [Google Scholar] [CrossRef]
- Bovis, F.; Carmisciano, L.; Signori, A.; Pardini, M.; Steinerman, J.R.; Li, T.; Tansy, A.P.; Sormani, M.P. Defining responders to therapies by a statistical modeling approach applied to randomized clinical trial data. BMC Medicine 2019, 17, 113. [Google Scholar] [CrossRef]
- Collins, C.; Burrows, T.; Rollo, M.; Boggess, M.; Watson, J.; Guest, M.; Duncanson, K.; Pezdirc, K.; Hutchesson, M. The Comparative Validity and Reproducibility of a Diet Quality Index for Adults: The Australian Recommended Food Score. Nutrients 2015, 7, 785–798. [Google Scholar] [CrossRef]
- Norgen Biotek Corp. Stool/faecal nucleic acid preservative safety data sheet. https://norgenbiotek.com/sites/default/files/resources/45630_45660_SDS.pdf, 2015. Accessed: 2022-10-28.
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Research 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; Bai, Y.; Bisanz, J.E.; Bittinger, K.; Brejnrod, A.; Brislawn, C.J.; Brown, C.T.; Callahan, B.J.; Caraballo-Rodríguez, A.M.; Chase, J.; Cope, E.K.; Silva, R.D.; Diener, C.; Dorrestein, P.C.; Douglas, G.M.; Durall, D.M.; Duvallet, C.; Edwardson, C.F.; Ernst, M.; Estaki, M.; Fouquier, J.; Gauglitz, J.M.; Gibbons, S.M.; Gibson, D.L.; Gonzalez, A.; Gorlick, K.; Guo, J.; Hillmann, B.; Holmes, S.; Holste, H.; Huttenhower, C.; Huttley, G.A.; Janssen, S.; Jarmusch, A.K.; Jiang, L.; Kaehler, B.D.; Kang, K.B.; Keefe, C.R.; Keim, P.; Kelley, S.T.; Knights, D.; Koester, I.; Kosciolek, T.; Kreps, J.; Langille, M.G.I.; Lee, J.; Ley, R.; Liu, Y.X.; Loftfield, E.; Lozupone, C.; Maher, M.; Marotz, C.; Martin, B.D.; McDonald, D.; McIver, L.J.; Melnik, A.V.; Metcalf, J.L.; Morgan, S.C.; Morton, J.T.; Naimey, A.T.; Navas-Molina, J.A.; Nothias, L.F.; Orchanian, S.B.; Pearson, T.; Peoples, S.L.; Petras, D.; Preuss, M.L.; Pruesse, E.; Rasmussen, L.B.; Rivers, A.; Robeson, M.S.; Rosenthal, P.; Segata, N.; Shaffer, M.; Shiffer, A.; Sinha, R.; Song, S.J.; Spear, J.R.; Swafford, A.D.; Thompson, L.R.; Torres, P.J.; Trinh, P.; Tripathi, A.; Turnbaugh, P.J.; Ul-Hasan, S.; van der Hooft, J.J.J.; Vargas, F.; Vázquez-Baeza, Y.; Vogtmann, E.; von Hippel, M.; Walters, W.; Wan, Y.; Wang, M.; Warren, J.; Weber, K.C.; Williamson, C.H.D.; Willis, A.D.; Xu, Z.Z.; Zaneveld, J.R.; Zhang, Y.; Zhu, Q.; Knight, R.; Caporaso, J.G. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nature Biotechnology 2019, 37, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nature Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Rognes, T.; Flouri, T.; Nichols, B.; Quince, C.; Mahé, F. VSEARCH: a versatile open source tool for metagenomics. PeerJ 2016, 4, e2584. [Google Scholar] [CrossRef]
- Lin, H.; Peddada, S.D. Analysis of compositions of microbiomes with bias correction. Nature Communications 2020, 11, 3514. [Google Scholar] [CrossRef]
- Oksanen, J.; Simpson, G.; Blanchet, F.G.; Kindt, R.; Legendre, P.; Minchin, P.R.; O’Hara, R.B.; Solymos, P.; Stevens, H.H.; Szoecs, E.; Wagner, H.; Barbour, M.; Bedward, M.; Bolker, B.; Borcard, D.; Carvalho, G.; Chirico, M.; Caceres, M.D.; Durand, S.; Evangelista, H.B.A.; FitzJohn, R.; Friendly, M.; Furneaux, B.; Hannigan, G.; Hill, M.O.; Lahti, L.; McGlinn, D.; Ouellette, M.H.; Cunha, E.R.; Smith, T.; Stier, A.; Braak, C.J.T.; Weedon, J. vegan: Community Ecology Package. https://cran.r-project.org/web/packages/vegan/index.html, 2022. Accessed: 2022-10-28.
Figure 1.
Taxonomy of the gut microbiota for participants across all sample time points including technical replicates. Participants are represented on the X axis with time points 1-8 within each section..
Figure 1.
Taxonomy of the gut microbiota for participants across all sample time points including technical replicates. Participants are represented on the X axis with time points 1-8 within each section..
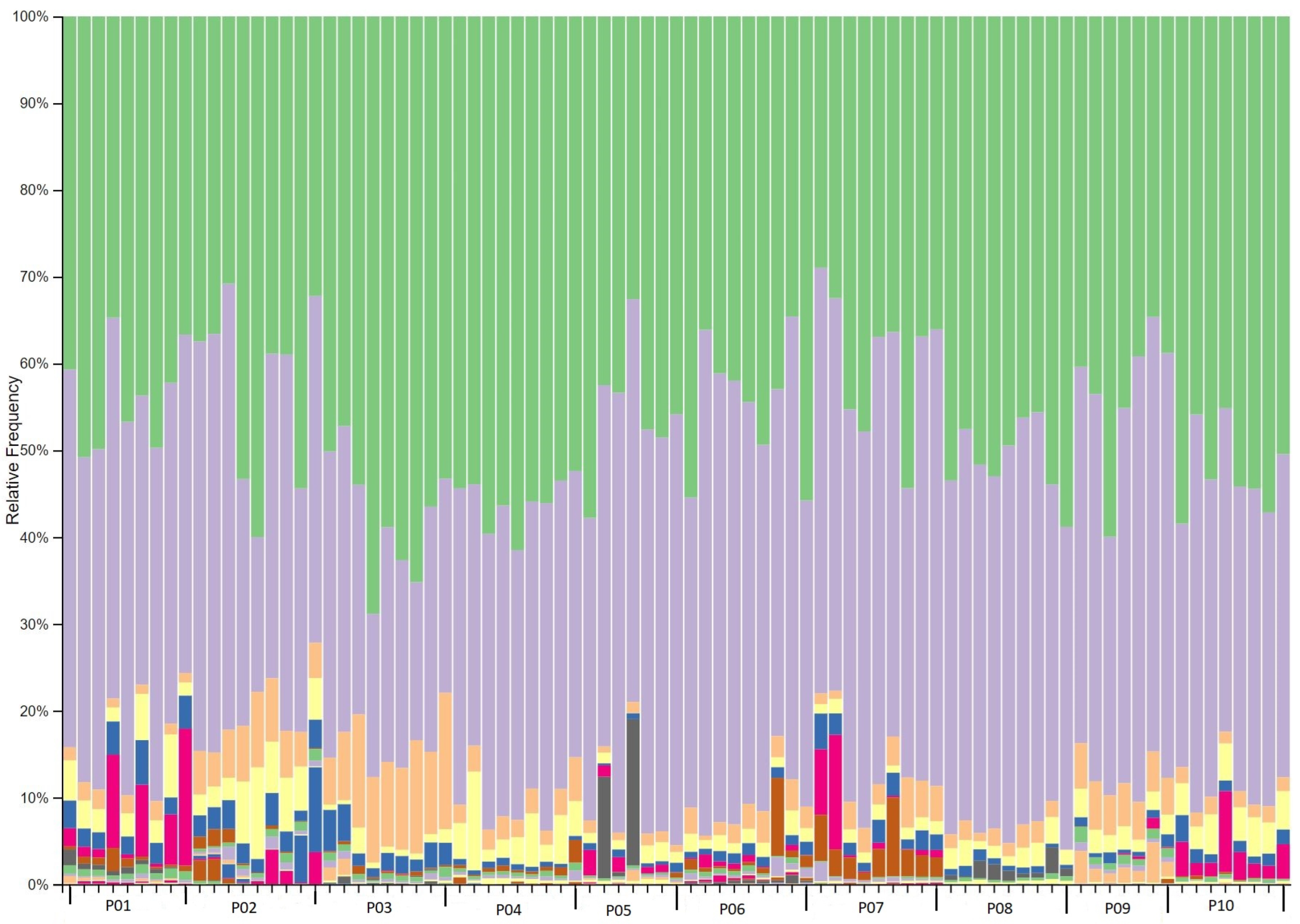
Figure 2.
Bray Curtis beta diversity EMPeror plot of all participants. Each point represents one sample from the corresponding participant and is coloured per participant for enhanced visualisation. Numbers on the axes refer to the percentage of variation explained by each axis of ordination.
Figure 2.
Bray Curtis beta diversity EMPeror plot of all participants. Each point represents one sample from the corresponding participant and is coloured per participant for enhanced visualisation. Numbers on the axes refer to the percentage of variation explained by each axis of ordination.
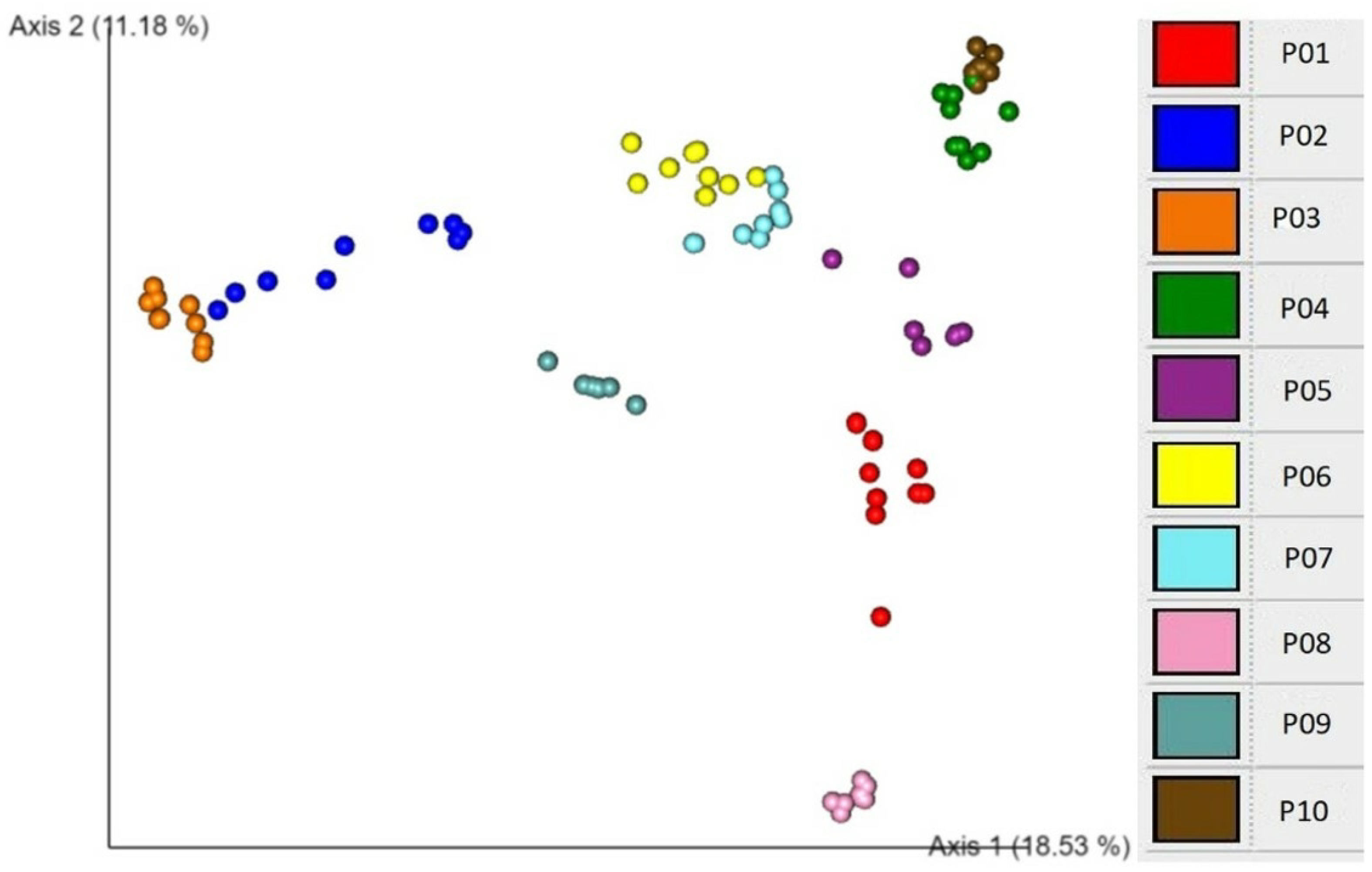
Figure 3.
EMPeror plots of weighted unifrac beta diversity distance matrix among selected participants. Axis 1 indicates the percentage of variation of the total variance between samples (alteration of microbial composition) and X-axis indicates days since experimental phase began, depicting time points 1-8. Distance on Y-axis indicates similarity of samples.
Figure 3.
EMPeror plots of weighted unifrac beta diversity distance matrix among selected participants. Axis 1 indicates the percentage of variation of the total variance between samples (alteration of microbial composition) and X-axis indicates days since experimental phase began, depicting time points 1-8. Distance on Y-axis indicates similarity of samples.
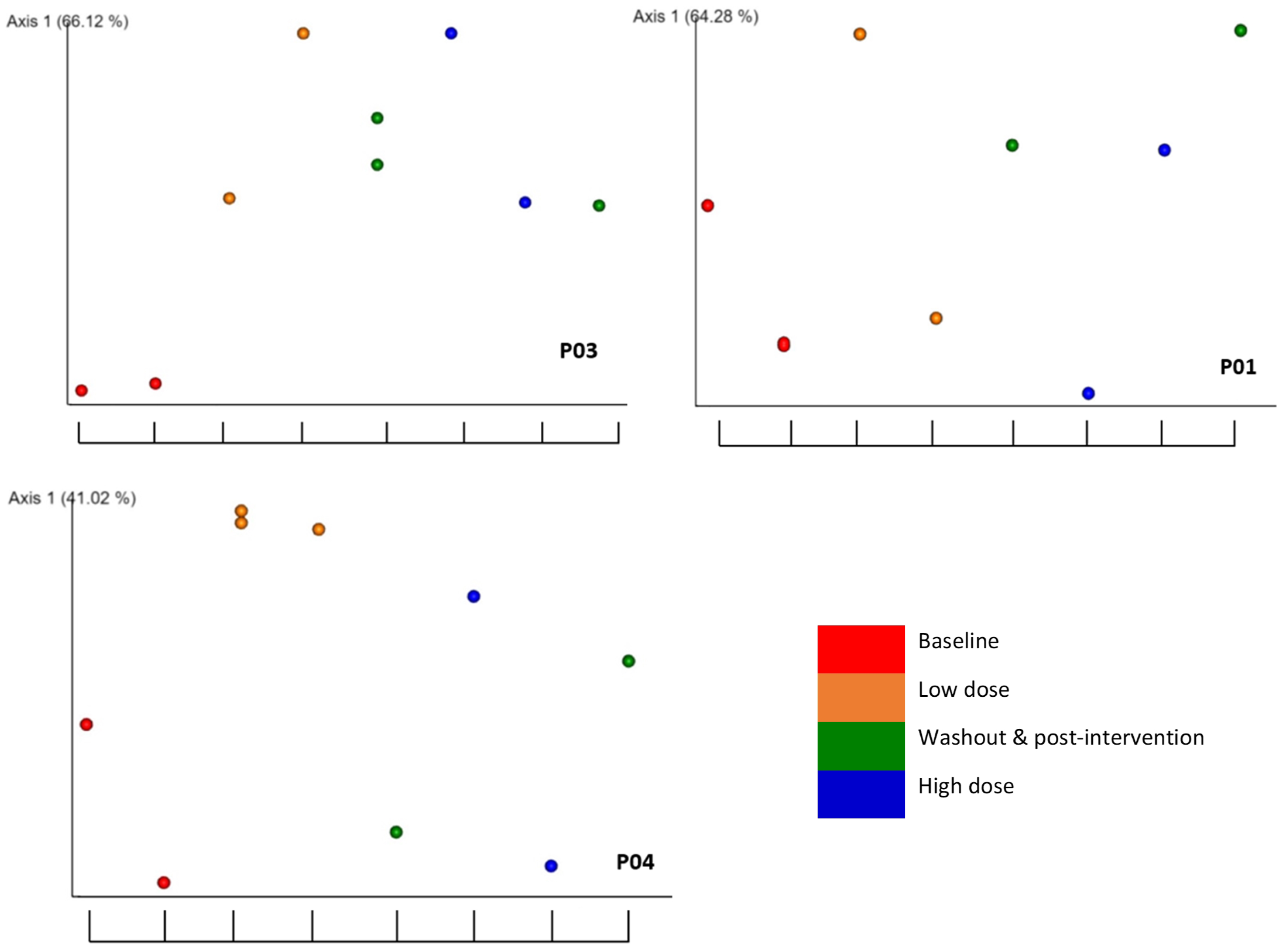

Table 1.
Participants’ characteristics and dietary intake from the screening survey and Australian Eating Survey.
Table 1.
Participants’ characteristics and dietary intake from the screening survey and Australian Eating Survey.
| Participant | Sex | Age | Age group | Cigarette smoking |
Alcohol consumption |
Diet | ARFS average |
ARFS group1 |
|---|---|---|---|---|---|---|---|---|
| P01 | F | 26 | ≤ 30 | No | No | Omnivore | 16 | Very low |
| P02 | M | 29 | ≤ 30 | No | Yes | Omnivore | 31.5 | Medium |
| P03 | M | 25 | ≤ 30 | No | No | Vegan | 42.5 | High |
| P04 | F | 26 | ≤ 30 | No | Yes | Omnivore | 29 | Low |
| P05 | F | 27 | ≤ 30 | No | Yes | Pescatarian | 28 | Low |
| P06 | M | 22 | ≤ 30 | No | Yes | Omnivore | 25.5 | Low |
| P07 | F | 56 | > 30 | Yes | No | Omnivore | 32 | Medium |
| P08 | M | 37 | > 30 | No | Yes | Omnivore | 34 | High |
| P09 | F | 28 | ≤ 30 | No | No | Omnivore | 16.5 | Very low |
| P10 | M | 30 | ≤ 30 | No | Yes | Omnivore | 22 | Very low |
1 ARFS group was classified into very low (<23), low (24-29), medium (30-33), high (34-40), and very high >40, according to ARFS average.
Table 2.
Associations of alpha diversity measured with Shannon’s evenness and Faith’s PD for explanatory factors using Kruskal-Wallis analysis. p values below 0.05 are indicated in bold.
Table 2.
Associations of alpha diversity measured with Shannon’s evenness and Faith’s PD for explanatory factors using Kruskal-Wallis analysis. p values below 0.05 are indicated in bold.
| Explanatory factor | Shannon’s evenness | Faith’s PD |
|---|---|---|
| Participant | 9.66e-8 | 0.002 |
| Alcohol consumption | 7.92-6 | 0.389 |
| Cigarette smoking | 0.008 | 0.113 |
| Sex | 0.003 | 0.165 |
| ARFS group | 0.032 | 0.494 |
| Age group | 0.390 | 0.149 |
| Interventional period1 | 0.394 | 0.602 |
| RBAC dosage2 | 0.592 | 0.442 |
| Experimental phase3 | 0.756 | 0.442 |
| Time point4 | 0.875 | 0.527 |
1 Interventional period compares baseline with the combination of low dose, washout, high dose, and post-intervention periods. 2 RBAC dosage 0g/day, 1g/day, and 3g/day. 3 Experimental phase is the comparison of baseline with low dose, washout, high dose, or post-intervention. 4 Time point includes 8 time points over 21 weeks (see Table 6).
Table 3.
Associations of beta diversity with explanatory factors determined using PERMANOVA analysis. p values under 0.05 are indicated in bold.
Table 3.
Associations of beta diversity with explanatory factors determined using PERMANOVA analysis. p values under 0.05 are indicated in bold.
| Explanatory factor | Unweighted unifrac | Weighted unifrac | Bray Curtis | Jaccard |
|---|---|---|---|---|
| Participant | 0.001 | 0.001 | 0.001 | 0.001 |
| Sex | 0.001 | 0.001 | 0.001 | 0.001 |
| Alcohol consumption | 0.001 | 0.001 | 0.001 | 0.001 |
| ARFS group | 0.001 | 0.001 | 0.001 | 0.001 |
| Age group | 0.001 | 0.013 | 0.001 | 0.001 |
| Cigarette smoking | 0.001 | 0.100 | 0.001 | 0.001 |
| Interventional Period1 | 0.826 | 0.275 | 0.866 | 0.928 |
| RBAC dosage2 | 0.936 | 0.644 | 0.997 | 0.999 |
| Experimental phase3 | 0.992 | 0.730 | 1.000 | 1.000 |
| Time point4 | 1.000 | 0.998 | 1.000 | 1.000 |
1 Interventional period compares baseline with the combination of low dose, washout, high dose, and post-intervention periods. 2 RBAC dosage 0g/day, 1g/day, and 3g/day. 3 Experimental phase is the comparison of baseline with low dose, washout, high dose, or post-intervention. 4 Time point includes 8 time points over 21 weeks (see Table 6).
Table 4.
Associations of beta diversity with explanatory factors using weighted unifrac and Bray Curtis analyses for each participant. p values equal to or lower than 0.05 are indicated in bold.
Table 4.
Associations of beta diversity with explanatory factors using weighted unifrac and Bray Curtis analyses for each participant. p values equal to or lower than 0.05 are indicated in bold.
| Weighted unifrac | Bray Curtis | |||||
| Participant | RBAC dosage1 |
Experimental phase2 |
Interventional Period3 |
RBAC dosage1 |
Experimental phase2 |
Interventional Period3 |
| P01 | 0.200 | 0.413 | 0.471 | 0.141 | 0.258 | 0.168 |
| P02 | 0.095 | 0.060 | 0.010 | 0.064 | 0.067 | 0.012 |
| P03 | 0.520 | 0.034 | 0.052 | 0.129 | 0.002 | 0.028 |
| P04 | 0.035 | 0.146 | 0.894 | 0.018 | 0.044 | 0.114 |
| P05 | 0.269 | 0.162 | 0.316 | 0.082 | 0.060 | 0.174 |
| P06 | 0.948 | 0.763 | 0.924 | 0.775 | 0.631 | 0.787 |
| P07 | 0.086 | 0.102 | 0.062 | 0.068 | 0.025 | 0.025 |
| P08 | 0.046 | 0.094 | 0.569 | 0.039 | 0.001 | 0.025 |
| P09 | 0.015 | 0.008 | 0.945 | 0.039 | 0.021 | 0.271 |
| P10 | 0.961 | 0.926 | 0.174 | 0.832 | 0.087 | 0.165 |
1 RBAC dosage 0g/day, 1g/day, and 3g/day. 2 Experimental phase is the comparison of baseline with low dose, washout, high dose, or post-intervention. 3 Interventional period compares baseline with the combination of low dose, washout, high dose, and post-intervention periods. (see Table 6).
Table 5.
Statistically significant taxonomic changes from baseline to interventional period determined using ANCOM. Data displayed only for participants showing a W≥5.
Table 5.
Statistically significant taxonomic changes from baseline to interventional period determined using ANCOM. Data displayed only for participants showing a W≥5.
| Participant | Bacteria (phylum, class, order, family, genus, and species) | W | Associated Change |
|---|---|---|---|
| P01 | Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Hungatella | 40 | increase |
| Proteobacteria; Gammaproteobacteria; Enterobacterales; Enterobacteriaceae; Citrobacter | 12 | increase (washout) | |
| Firmicutes; Bacilli; Erysipelotrichales; Erysipelatoclostridiaceae; Erysipelatoclostridium | 8 | increase (washout) | |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; unknown | 6 | decrease | |
| P02 | Firmicutes; Clostridia; Peptostreptococcales-Tissierellales; Peptostreptococcales-Tissierellales; Anaerococcus | 64 | decrease |
| Actinobacteriota; Actinobacteria; Corynebacteriales; Corynebacteriaceae; Corynebacterium; unknown | 63 | decrease | |
| Actinobacteriota; Actinobacteria; Corynebacteriales; Corynebacteriaceae; Corynebacterium; unknown | 50 | decrease | |
| Firmicutes; Clostridia; Peptostreptococcales-Tissierellales; Peptostreptococcales-Tissierellales; Finegoldia | 48 | decrease | |
| P03 | Negativicutes; Veillonellales-Selenomonadales; Veillonellaceae; Dialister | 94 | decrease |
| Cyanobacteria; Vampirivibrionia; Gastranaerophilales; Gastranaerophilales; Gastranaerophilales | 86 | decrease | |
| P07 | Firmicutes; Bacilli; Erysipelotrichales; Erysipelatoclostridiaceae | 102 | decrease |
| P08 | Firmicutes; Clostridia; Oscillospirales; Ruminococcaceae; Eubacterium siraeum group | 35 | decrease |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Eisenbergiella | 9 | decrease | |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Lachnospiraceae ND3007 group | 7 | increase | |
| Proteobacteria; Gammaproteobacteria; Enterobacterales;Enterobacteriaceae; Escherichia-Shigella | 6 | increase (low dose) | |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Frisingicoccus | 5 | increase | |
| P09 | Firmicutes; Clostridia; Oscillospirales; Ruminococcaceae; Eubacterium siraeum group | 38 | increase |
| Firmicutes; Clostridia; Peptostreptococcales-Tissierellales; Peptostreptococcales-Tissierellales; Anaerococcus | 8 | increase (low dose) | |
| Firmicutes; Clostridia; Oscillospirales;Ruminococcaceae; Ruminococcus | 8 | increase (high dose) | |
| Firmicutes; Negativicutes; Veillonellales-Selenomonadales; Veillonellaceae; Megasphaera | 8 | increase (low dose) | |
| Firmicutes; Bacilli; Erysipelotrichales; Erysipelotrichaceae; Solobacterium | 7 | increase (low dose) | |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Eubacterium hallii group | 5 | increase | |
| Firmicutes; Bacilli; Erysipelotrichales; Erysipelotrichaceae; Turicibacter | 5 | increase (high dose) | |
| Firmicutes; Clostridia; Lachnospirales; Lachnospiraceae; Stomatobaculum | 5 | increase | |
| P10 | Bacteroidota; Bacteroidia; Bacteroidales; Prevotellaceae; Prevotella | 20 | decrease |
| Firmicutes; Clostridia; Oscillospirales; Butyricicoccaceae; Butyricicoccus | 8 | increase | |
| Firmicutes; Bacilli; Lactobacillales; Carnobacteriaceae; Granulicatella | 5 | increase |
Table 6.
Dosage and schedule of RBAC supplementation with corresponding faecal sample number.
| Time point | RBAC dose | Faecal sample | Experimental |
|---|---|---|---|
| (week) | (g/day) | number | phase |
| -3 | 0 | 1 | Baseline |
| 0 | 0 | 2 | Baseline |
| 3 | 1 | 3 | Low dose |
| 6 | 1 | 4 | Low dose |
| 9 | 0 | 5 | Washout |
| 12 | 3 | 6 | High dose |
| 15 | 3 | 7 | High dose |
| 18 | 0 | 8 | Post-intervention |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



