
Submitted:
31 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
Type 1 Diabetes mellitus (T1DM) occurs when insulin is not produced in the Pancreas due to the autoimmune destruction of the beta cells. The patients may be diagnosed after 80-90% of the beta cells are destroyed. Insulin remains the essential medicine in T1DM management, under continuous monitoring of glucose levels. T1DM management consists of a complex and precise set of self-care measures for the entire life; during this continuous process, the patients could become overwhelmed, angry, anxious, frustrated, and/or discouraged. Therefore, to be widely used and provide general benefits, new technologies for DM management must provide clinical advantages without compromising safety. The compliance of T1DM patients is also essential, thus improving their quality of life (QoL). Moreover, the accessibility of the new system for patients through healthcare coverage is critical; they must be able to buy the new devices and accessories and pay for their maintenance. In this context, our work aims to describe the most recent technologies regarding continuous glucose monitors (CGMs) and continuous subcutaneous insulin infusion (CSII) systems, correlated with psychosocial impact and capacity to improve T1DM patients' life quality.
Keywords:
Type 1 Diabetes mellitus
; Insulin
; Diabetes management
; Technology
; Continuous glucose monitoring systems
; Insulin pumps
1. Introduction
According to the World Health Organization, Diabetes mellitus (DM) represents a group of metabolic diseases characterized by high blood glucose levels when the treatment is missing [1]. It is at the top of global death causes, with more than 420 million people living with diabetes worldwide [2].
Type 1 Diabetes mellitus (T1DM) occurs when insulin is not produced in the pancreas due to the beta cells’ autoimmune destruction [3]. The patients may be diagnosed when 80-90% of the beta cells are destroyed. The classic concept is that healthy β-cells are mistakenly damaged by autoreactive T cells.
Recently, Roep et al. [4] proposed an alternative point of view in which abnormal β-cells are the main contributors to T1DM pathogenesis. Based on previously reported results of immunotherapy to delay T1DM onset [5,6,7], they showed that β-cells, with limited self-defense, are vulnerable to biosynthetic stress [4]. Thus, novel strategies for preventing and managing T1DM are investigated [8,9]. Current research is centered to beta cell recovery. This aim could be achieved through antigen vaccination (with oral insulin or peptides). Moreover, verapamil and glucagon-like peptide-1 receptor agonists could act as protective agents of beta cells in stress conditions. On the other hand, prevention approaches against autoimmune phenomena are also essential in T1DM, requiring the advent of stem cell-based replacement therapies [10]. Hence, FDA approved in November 2022 the first drug - Tzield (teplizumab-mzwv) injection - that can delay the Type 1 Diabetes outbreak [11,12,13]; thus, the treated patients could live months to years as diabetes-free [14].
Even though there are new therapeutical approaches in diabetes mellitus type 1 and opened new horizons in T1DM treatment, insulin remains the only treatment for T1DM, under continuous monitoring of glucose levels. To diminish the risks and unwanted complications of injectable insulin administration and increase the patient’s compliance, various research teams tried to incorporate it in multiple carriers for oral administration [15,16,17]: liposomes [18,19] mixed micelles [20,21], nanoparticles [22,23,24], intestinal patches [25]. Current studies also explore other access ways for insulin administration: intranasal [26,27,28], transdermal [29,30], and sublingual [31,32].
Nowadays, the most common regimens consist of subcutaneous administration of various insulin forms, as follows:
- Multiple daily injections (MDI) – A long-acting insulin administered one time daily (morning or evening) - and a rapid-acting one before meals (its dose is calculated considering the amount of carbohydrate and the blood glucose level) [35];
- Continuous subcutaneous insulin infusion (CSII) – A rapid-acting insulin administered 24 hours/day using an insulin pump. [36].
Although insulin is a life-saving medicine for T1DM patients [37], in countries with limited government expenditures for health, individuals must pay out-of-pocket for all or part of their diabetes care, including insulin and syringes, blood glucose meters, delivery devices, and necessary health education [38,39]. Some try to underuse insulin treatment without informing their clinicians about this condition [40]. However, T1DM is a debilitating chronic illness associated with high morbidity [41], work-life diminution [42], and premature mortality [43] if not correctly managed; the patients highly depend on exogenous insulin associated with substantial lifestyle adjustments to normalize lipid and protein metabolism [44]. When diabetes coexists with other diseases [45,46,47,48,49,50], the management of a patient’s condition is even more difficult.
The previously mentioned aspects have complex pathophysiological, psychological, and quality of life (QoL) implications [51]; the risk of developing psychiatric comorbidities (depressive disorders) increases with the earlier onset of T1DM [52,53]. These conditions are known as diabetes distress (DD), leading to poor compliance with diabetes care, low glycemic control, and long-term complications (Figure 1) [52,54].
Generally, younger people [55,56], women [57], and people with poor glycemic control—high glycosylated hemoglobin (HbA1c) values [58]—have an increased risk for high levels of DD. Older diabetic people have a lower DD incidence [59].
T1DM management includes complex and precise self-care measures during the patients’ entire life. This continuous process could overwhelm the patients; they could become angry, anxious, frustrated, and/or discouraged [60].
Due to the previously described conditions, the new technologies for DM management must provide clinical advantages and high usability without compromising safety [61]. The adherence and compliance of T1DM patients to prescribed therapy are also essential, thus improving their QoL [62]. Moreover, the accessibility of the new system for patients through healthcare coverage [63] is critical; they must be able to afford the new devices and accessories and their maintenance [64,65].
2. Materials and Methods
We performed a literature review searching original published articles on type 1 diabetes in humans. We used a data filter on insulin therapy, insulin pumps, and advanced technologies in medical devices for insulin infusion. The selection aimed the publications in scholarly peer-reviewed journals in the last 10 years (2013-2022) written in English (but with no country restriction). The initial selection was from Google Scholar search. Due to the high document variety, we accessed other three primary databases: PubMed®/MEDLINE, Mendeley, and Web of Science®. The following keywords were used: Type 1 Diabetes mellitus technology (3,046 journal articles), Continuous Glucose Monitoring System (4,273), Continuous insulin infusion (7,150), Automated Insulin Delivery (533), Patch insulin pump (153), Closed-loop insulin pump (874), Hybrid closed-loop insulin pump (218), Artificial Pancreas (3,389), Bionic Pancreas (76). We performed our searching only on open-access articles edited in English Language and performed the final search on April 15, 2023.
3. Continuous Glucose Monitoring Systems
Insulin administration and blood glucose monitoring systems continue to be the first-line treatment option for T1DM management [35,68,69]; the patient must have 4 measurements of blood glucose level per day. The basic technology still widely used around the world is represented by the blood glucose meters (BGM) [70]. Patients can learn to efficiently use the blood glucose meters and appropriate PC health software and to perform different changes in the day-to-day management of their diabetes [71].
The glucose level monitoring daily protocol is significantly improved through advanced technologies that offer continuous glucose monitoring (CGM) systems [72]. Two types of CGMs are described: intermittently scanned CGMs (IS-CGM) [73] and real-time ones (RT-CGM) [74].
A CGM consisting of a sensor that measures glucose levels every minute and stores data automatically every 15 min without transmitting them is known as a flash glucose monitor (FGM) [75,76].
RT-CGMs automatically measure glucose levels day and night and transmit them every 1/5 minutes to a receiver [77,78]. They have alarm systems for outstanding glucose levels and inform patients/caregivers about immediate/long-term events (hyperglycemia or hypoglycemia) [79]. Knowing glucose levels in real-time can help make more informed daily decisions about food balance, physical activity, and insulin doses [80].
3.1. Description
A CGM System consists of a few principal components: sensor, transmitter, application software, and insertion tool. For sensor insertion, the abdominal region [83] is the most common location. CGMs evaluate glucose levels in the interstitial fluid (ISF) from the subcutaneous adipose tissue [84]. The measured glucose concentrations in ISF are used, through various algorithms [85], to predict the blood glucose (BG) ones, assessed with glucometers.
The clinical utility of CGMs consists of therapeutic decisions [86] based on real-time glucose evaluation.
CGM data have the following clinical applications:
In the analytical performance of CGMs (sensors + algorithms) evaluation, the mean absolute relative difference (MARD) is a parameter expressed as percent (%), frequently used [90]. The MARD calculation involves temporally matched glucose data from CGM systems compared to BG measurements of all subjects included in a clinical study. A high-performance CGM implies MARD value < 10%. Therefore, the BG evaluation 2-4 times daily with a glucometer ensures an optimal calibration of CGM systems - even for those without mandatory calibration - avoiding significant differences between CGM data and BG values.
Each sensor lasts up to 7,10, 14, or 180 days and the patient can see glucose levels on a reader device or smartphone.
Different companies commercialize minimally invasive continuous glucose monitoring devices (MID): GlySens Incorporated, Senseonics Holdings, Inc., Abbott Laboratories, Medtronic plc, F. Hoffmann-La Roche Ltd., Dexcom, Inc., A. Menarini Diagnostics, LifeScan IP Holdings LLC, Echo Therapeutics, Inc., Johnson & Johnson, Terumo Corporation, and B. Braun Melsungen AG.
A few CGM system types are listed in the American Diabetes Association recommendations [91] and presented in Table 1.
In Table 1, the most known FDA-approved CGMs are comparatively analyzed.
Registered data show that the most complex and expensive is Eversense E3 CGM. It also has the most numerous days of sensor wearing and is suitable for over 18 years patients. The others have RT under 15 days and can be used by children.
Two MIDs have factory calibration and do not require daily calibration (Dexcom 6 and Libre 2); they also register a high accuracy. The most significant accuracy (MARD = 8.5%) is attributed to Eversense E3 CGM. Its previous version, Eversense XL, was approved in June 2018 by the U.S. Food and Drug Administration as the first implantable CGM device for people with diabetes. Furthermore, Only two GCMs received FDA approval to be used in Automatic insulin delivery (AID) systems.
The measured glucose levels are strongly influenced by numerous factors related to the insertion place [83].
Thus, measurements from the right abdominal site tend to be diminished than those from the left. Studies on CGM sensors involving sleep [93] and belt compression [94] reported a potential influence of diminished blood flow on the sensors’ measurements. Similarly, Mensh et al. [84] demonstrated that the susceptibility of CGMs to abnormal nocturnal glucose readings was related to sleeping positions. On the abdominal surface, various physiologic conditions [95,96] could be related to different CGM readings in the left versus right part. In various BMI values, the subcutaneous adipose tissue size could influence CGM measurement accuracy [97].
The sensors’ biocompatibility could determine the discrepancy between abdominal sites [98]. Sensor insertion traumatizes the afferent zone, inducing inflammatory reactions [99], which are glucose customers around [100]. Local proteolytic enzymes and reactive oxygen species [101] could negatively affect the sensors. During wound healing, capillary neoangiogenesis can supply additional glucose at the insertion site [25].
Benefits
Compared with a standard blood glucometer, every day using a CGM system can help to:
- ▪ Maintaining a constant glycemic level daily.
- ▪ Diminishing hypoglycemia emergencies.
- ▪ Reducing finger pricks number.
- ▪ Decreasing BG and HbA1c levels variability.
3.2. Limits
- ▪ CGM systems are more expensive than standard glucometers.
- ▪ The finger prick glucose test is needed twice daily for some CGM to check the accuracy.
- ▪ Readings are not trusted, and too much time is needed to use them [90].
- ▪ Invasiveness.
- ▪ Short lifespan.
- ▪ Biocompatibility.
- ▪ Calibration and prediction.
3.3. Potential adverse effects related to the insertion, removal, and wear of the sensor
- ▪ Allergies to adhesives
- ▪ Bleeding and bruising
- ▪ Infection, pain, or discomfort
- ▪ Sensor destruction during extraction
- ▪ Skin inflammation, scarring, thinning, discoloration, or redness.
Other potential unwanted effects are associated with decisions made in the case of inaccurate device measurements:
- ▪ Excessive insulin administration could increase the risk of hypoglycemia
- ▪ Inappropriate administration of carbohydrates increases the risk of hyperglycemia and acute diabetic ketoacidosis. Moreover, there could appear long-term microvascular complications of diabetes.
- ▪ Inaccurate calculation of the glucose change rate could increase the incidence of hypo or hyperglycemia.
Recently, a non-invasive CGM manufactured by Afon Technology Ltd (Caldicot, Monmouthshire, UK) is in the stage of clinical studies. It could be available soon as an alternative technology to traditional blood glucose monitoring tools. This CGM system utilizes high-frequency microwaves, a technology not used yet in this application [102]. The most important features regarding used materials, techniques, and methods are displayed in Figure 2.
4. Continuous Subcutaneous Insulin Delivery Systems (CSII)
An insulin pump is an electronic device that releases regular insulin according to the body’s daily needs [103]. Hence, the patient with T1DM does not need insulin injections [104].
Insulin pumps generally use rapid-acting insulin formulations. They deliver insulin in two primary ways:
- ▪ A continuous infusion of rapid-acting insulin throughout the day and night (basal),
- ▪ The user gives a discreet, one-time dose of rapid-acting insulin for meals or high blood glucose correction (bolus).
The ideal patient for insulin pump use is:
- People with T1DM or insulin-dependent T2DM.
- Persons with multiple-day injections of Insulin and a similar number of BG tests.
- Individuals - able to assess appropriate blood glucose control.
- Capable of performing insulin pump therapy initiation and maintenance.
- Able to maintain frequent contact with the healthcare team.
- Able to consider insulin pumps as a tool to improve diabetes care.
- Capable of accurately calculating carbohydrates and insulin bolus.
- Patients with critical clinical conditions have serious difficulties controlling glycemic targets despite intensive treatment and monitoring.
- With substantially decompensated diabetes (frequent severe hypoglycemia and/or hypoglycemia).
- Other associated conditions: extreme insulin sensitivity, gastroparesis, pregnancy, variable schedules or work shifts, significant "dawn phenomenon," high insulin doses therapy, or severe insulin resistance.
The CSII benefits and limits are displayed in Table 2.
4.1. Conventional Insulin Pumps
An insulin pump is a small digital device that ensures a continuous infusion of rapid-acting insulin. The infusion set is inserted into the subcutaneous tissue and fixed on the skin with an adhesive. In most insulin pumps, the infusion set connects to the pump by plastic tubing. Insulin infuses from the pump through the tubing to the infusion set cannula and into the subcutaneous tissue.
4.2. Insulin Patch Pumps (PP)
Some insulin pumps are directly attached to the skin (patch insulin pumps). Insulin delivery in a PP is controlled by a hand device; however, some devices also allow at least some functionality via the PP. There are 3 categories of PP: PPs with reduced features, fully equipped PPs, and PPs suitable for Automatic Insulin Delivery (AID) systems.
4.2.1. Simple insulin PPs devices
The simple forms of PPs intended for insulin therapy aim to be small and disposable, easy to handle and carry. They aim to replace insulin pen therapy with PPs. PPs use simple insulin dosing ways. To simplify insulin therapy, PPs deliver only basal insulin. V-GO (Zealand Pharma; Zealand, Denmark) is a simple PP that delivers a fixed amount of basal insulin over 24 h and has a bolus button that permits up to 36 units of prandial insulin to be given in 2-unit increments per day (Figure 3, and Table S1 from Supplementary Material).
V=Go is replaced daily, but other insulin PPs could be maintained 3 days. The Simplicity (CeQur; Luzern, Switzerland) PP holds up to 200 bolus insulin units infused in 2-unit increments or 330 units for 3 days, and admits different basal rates.
4.2.2. Full-Featured Electromechanical Patch Pumps
They have generally electromechanical structure with an electronic controller.
These are all full-featured pumps with different basal rates, individually controllable bolus amounts and fewer ways of bolus delivery.
4.2.3. PPs suitable for AID systems
PPs have small size, beying easy to use and discreet to wear. Moreover, they are able to interact with CGM system and the algorithm, in AID systems.
Other advantages of PPs and their limitations are displayed in Table 3.
4.3. Sensor Augmented Pump Therapy (SAPT)
In a SAPT system, the insulin pump is combined with a CGM system. It displays CGM data on the insulin pump’s home screen, with easy access to the recorded data.
SAPT systems reveal a higher diminution in HbA1c after 12 months than MDI therapy [109].
Exist 2 function types of SAPT (Table 4):
- ▪ With low-glucose suspend (SAPT-LGS)
- ▪ With predictive low-glucose management (SAPT-PLGM).
SAPT systems are known as open-loop systems [110]. The most known device is the MiniMed Paradigm Real-Time system (Medtronic Diabetes, Northridge, CA, USA), launched in 2006 and consists of real-time continuous glucose monitoring (CGM) integrated with an insulin delivery device (Table 4) [111].
SAPT-LGS can reduce hypoglycemia by 40–50% (< 70 mg/dL). It occurs without an increase in glycosylated hemoglobin (Table 4) [112,113].

| SAPT-LGS | SAPT-PLGM | ||
|---|---|---|---|
| Properties | |||
| When the pump users did not recognize the warning sounds, the SAPT-LGS automatically stops the basal insulin infusion (for up to 2 h) as a response to hypoglycemia detected by a sensor. Then, the basal insulin infusion is released at the rate previously programmed. | Basal insulin delivery is usually stopped when the sensor indicates a glucose level below 70 mg/dL. When the users do not exert an action, the insulin infusion returns at the last regulated rate after two hours of suspending. |
||
| SAPT-LGS system can diminish moderate-to-severe hypoglycemia, especially during nighttime. | SAPT-PLGS system reduces more effectively the frequency of hypoglycemia and the risk of developing this condition in a severe form in T1DM patients. | ||
| Devices | |||
|
RT-Paradigm® Veo™* (Medtronic, Northridge, CA, USA) |
RT-MiniMed 640G (Medtronic, Northridge, CA, USA) |
||
| MARD% | 13.6% | MARD% | 14.2% |
| Calibration | 3 days | Calibration | 3 days |
| Life of sensor | 6 days | Life of sensor | 6 days |
| Clinical studies | |||
| Studies using SAPT-LGS demonstrated a diminishing in hypoglycemic events (with 40–50%), without an A1C increase, compared to SAPT alone [112,113]. | Under real-life conditions, SAPT-PLGM decreases hypoglycemic events in patients previously treated with MDI and SAPT-LGS. It occurs without deteriorating glycemic control in SAPT-LGS patients and improves A1C in those treated with MDI [114,115]. | ||
| Ideal user | |||
| Able to permanently wear a device on the body and manage CGM data. | Able to comfortably wear an automatic device. | ||
| Able to check BG when needed. | Able to regulate the carbohydrate amount. | ||
| Able to respond and manage CGM alerts | |||
SAPT—Sensor Augmented Pump Therapy; LGS—Low Glucose Suspend; PLGM—Predictive Low Glucose Management; CGM—Continuous Glucose Monitor; MDI—Multi-Daily Injections; MARD— mean absolute relative difference; A1C —measures the amount of glycosylated hemoglobin.
4.4. Closed-loop Insulin Systems (Artificial Pancreas)
A CGM could become a part of a CSII, generating a closed-loop insulin system (Figure 4A). It is a substantially improved system, adjusting insulin delivery in response to real-time sensor glucose levels and other inputs, such as meal intake (Figure 4B). Control algorithms can modulate the insulin needs’ variability between and within individual users, considering CGM accuracy limitations and insulin delivery imprecision [116].
The glycemic control artificial maintenance requires three main components of a closed-loop system (Figure 4A):
- ▪ Glucose measuring device (CGM)
- ▪ Control device for BG analysis and insulin dosing regulation (computer/microprocessor)
- ▪ Insulin infusion device (insulin pump)
The control algorithms are continuously adapted to physiological changes with real-time adjustment of closed-loop control parameters (Figure 5).
Various control algorithms were developed [119], as follows: Model predictive iterative learning control (MPC) [120,121,122], Proportional integral derivative (PID) controllers [123,124], and Fuzzy logic control approaches [125,126].
The closed-loop system’s components function as a healthy pancreas that controls BG levels. Thus, the closed-loop insulin system is known as the Artificial Pancreas (AP) [127].
When an AP system requires counting and registering the carbohydrate amount from mealtime, it is called a "hybrid" [128] because a part of insulin is provided automatically, and another is infused based on the reported information.
In 2016, FDA approved a hybrid closed-loop system that measures the glucose level at each 5 minutes day and night through a CGM [129]. It automatically gives a suitable amount of long-acting basal insulin through a separate insulin pump. The patient still needs a glucose meter a few times daily, manually adjusting the insulin delivery at mealtimes and when it requires a dose correction.
The hybrid closed-loop system could free the patient from some actions needed to keep constant BG levels—or help him to sleep the nighttime without needing to wake for glycemia testing.
Like a healthy pancreas, an utterly automated closed-loop system does not request meal announcements; it can react to BG level variations [130].
Another artificial pancreas system is known as a hormonal Bionic Pancreas (BP) [130,131,132]. It has the next-generation technology to deliver insulin and/or glucagon automatically than standard-of-care management. Therefore, BP is more effective in maintaining blood glucose levels within the normal range in T1DM people [133]. In 2018, the Beta Bionics Inc (Boston, Massachusetts, U.S.A.) iLet bionic pancreas system [131,132,134,135,136] received FDA approval for clinical trial testing at home.
4.4.1. Benefits
- ▪ The glucose levels could be continuously monitored.
- ▪ The control algorithms improve BG control, automatically regulating the amount of insulin.
- ▪ The System helps the T1DM user avoid emerging events (hypoglycemia and hyperglycemia).
4.4.2. Limits
- ▪ The T1DM patient regularly verifies the devices to ensure that they function correctly.
- ▪ The user must continuously verify the CGM and infusion pump catheter, ensuring they are in a suitable place, and change them when needed.
- ▪ The CGM accuracy should be verified, and the CGM sensor must be regularly replaced.
- ▪ The patient must count the mealtime carbohydrates and enter them into the System.
- ▪ The control software settings must be verified to ensure that the insulin infusion has a suitable amount.
- ▪ The extreme BG levels should be regulated if the System is unable.
- ▪ The adhesive patches used with these systems may cause skin redness or irritation.
- ▪ Other medicines might also interfere with the glucose monitor.
4.4.3. Complications
- ▪ Hypoglycemia occurs when a significant basal rate of insulin is delivered due to a human error in insulin pump programming or a device malfunction.
- ▪ Hyperglycemia is caused by programming error or device malfunction, leading to a low insulin delivery rate (battery depletion or malposition, cannula occlusion, total pump failure).
- ▪ If the infusion set is not changed regularly, at 3-4 days, there is irritation and infections at the place of cannula insertion.
- ▪ Insulin pump therapy discontinuation (18-50%) is the T1DM patient choice for various reasons: unwanted interference with the lifestyle, missing improvements in glycemic control, and infection at the insertion place. It occurs with high incidence in women, younger patients, pregnancy, and when the patient has psychological comorbidities.
5. The impact of new technologies on T1DM people’s Quality of Life
5.1. Evaluation of Diabetes Distress
The T1DM adults have a self-report scale with 28 items, evidencing 7 critical points of diabetes distress.
These 7 items refer to crucial feelings of T1DM adults, according to Fisher et al. [137] (Figure 6).
Open discussions with T1DM patients represent a clinical instrument for their emotional behavior evaluation.
5.2. Satisfaction Survey for Diabetes Technology Users
The Glucose Monitors Satisfaction Survey (GMSS) [140] was conceived for T1DM patients as a 15-item self-report scale, following 3 key dimensions:
- ▪ Openness.
- ▪ Emotional and behavioral burdens.
- ▪ Trust.
Moreover, Insulin Device Satisfaction Survey (IDSS) as a self-report scale with a 14-item version for T1DM [141], following 3 key dimensions:
- ▪ Effectiveness.
- ▪ Burdensomeness.
- ▪ Inconvenience.
All these documents are available in various languages and accessible to non-profit institutions for use in clinical care and research. Concomitantly, they could be accessed as copyright with licensing fees by all for-profit companies and institutions on https://behavioraldiabetes.org/scales-and-measures/ (accessed on April 9, 2023).
5.3. Quality of Life Evaluation
Joensen et al. [142] analyzed the effect of continuous care and support in T1DM adults with insulin pump therapy. The flexible and participatory peer support approach augmented patients’ motivation and empowerment, induced a feeling of serenity about diabetes management, and demonstrated the potential to diminish diabetes distress, thus increasing their QoL. Adequate diabetes-specific social support avoids the risk of participants feeling isolated within peer support groups and allows free interactive dialogue regarding T1DM disease and all difficulties in coping with it. Evaluation of motivation, serenity in life with diabetes, awareness of own diabetes practices, diabetes empowerment, diabetes loneliness, and diabetes distress are applicable, feasible, and appropriate when measuring the effect of peer support in adults with insulin pump-treated diabetes.
Introducing technology in T1DM management in patients with 30+ year’s duration of diabetes also encounters multiple obstacles. Our team’s experience materialized in a model of the efficiency of this process. Following this model and after the treatment change, we have obtained a 1.3% reduction of HbA1c and significantly fewer hypoglycemic events RR 34% (p < 0.01). Patients’ acceptance of the new treatment increased in time by 92%. The implementation process effectively achieved this transformation, reached glycemic targets, and changed patients’ lifestyles [143].
Recently, Fanzolla et al. [144] supervised a two-section questionnaire (children/parents) to evaluate the impact of CGM on T1DM children and their families. The data show that CGM devices significantly benefited the QoL of children and their parents. Thus, 80% of children reported that the CGM subcutaneous placement is much less painful than fingertips implied in classical BG controlling. Moreover, the QoL at school and sports is significantly better: diminished anxiety, higher comfort, and better glycemic control [144]. Of parents, 90% stated that CGM devices use remarkably improved glycemic control, reducing emerging events. A similar percentage (89% of parents) are convinced that the recent technology substantially benefits their children’s QoL [144].
The use of CGM by individuals with diabetes is correlated with psychological benefits and burdens [145]. Potential benefits consist of improved QoL and diminished hypoglycemia fear. However, randomized clinical trials versus cohort studies for youth and adults show heterogeneous results. In correspondent studies, adolescents and adults have nearly universally reported substantially perceived satisfaction regarding CGM use. The specific benefits were linked to easier diabetes management and better glycemic control. In contrast, pain and body issues, communication problems, feeling awestruck by the complex glucose management, and doubts regarding the accuracy of CGM compared to glucometer readings [146]. Increased anxiety of adolescents and parents and poorer parental sleep has also been remarked [147].
Rusak et al. [148] evaluated the quality of life and satisfaction in children under 7 years of age with T1DM using the RT-CGM system integrated with an insulin pump, investigating their caregivers’ opinions. They reported high satisfaction with CGM use (68% in groups aged 5–7 years and 92% in 2–4 years). 71% of caregivers confirmed the positive effect of CGM on their sleep quality.
Polonsky et al. [149] analyzed the CGM Impact on the Quality of Life in T1DM adults. The participants completed QoL evaluation (regarding overall well-being, health status, DD, confidence, and hypoglycemic fear) and CGM Satisfaction Survey. CGM satisfaction was not considerably associated with glycemic levels. The satisfaction was directly correlated with diminishing diabetes distress and hypoglycemic fear and increasing well-being and hypoglycemic confidence [149]. Therefore, the CGM group reported higher hypoglycemic confidence and diabetes distress reduction than the SMBG, but with no statistically significant differences.
The Satisfaction survey on patients with Artificial Pancreas [150] did not yet clearly reveal a clear impact on fear of hypoglycemia, adherence, quality of life, depression and anxiety, and diabetes distress.
However, T1DM children from a summer camp [151] revealed the benefits of a Bionic Pancreas in the following:
- ▪ Reducing their fear of hypoglycemia,
- ▪ Decreasing their sense of regimen burden,
- ▪ Diminishing their worries about out-of-range blood sugar levels,
- ▪ Improving their overall freedom to engage in activities that they enjoyed.
In addition, their concerns about the BP included wishing the system responded to out-of-range blood sugar levels more quickly and the annoyance of carrying several devices around [151].
6. Discussion
BG self-monitoring is crucial to the daily routine care of T1DM patients receiving insulin therapy. However, the adherence rate is low. A recent study [152] reported a 61.6% adherence rate to the Spanish Diabetes Society protocol for SMBG. The authors identified the associated factors: the frequency of insulin injections (<3 injections daily), alcohol abstinence, peripheral vascular disease, and retrieval of the reactive strips from the pharmacy. Only 21.4% of patients had an excellent self-perception of glycemia.
Peralta et al. [153] performed a cross-sectional observational study in adults and children treated with basal-bolus therapy and CSII users, aiming at T1DM management. They observed that metabolic control (expressed as HbA1c) positively correlates with higher educational level, carbohydrate counting, more daily SMBG, and minor hypoglycemic episodes. It decreases with T1DM duration, higher insulin total dose, low adherence to diet, and a family history of DM [153].
Spaan et al. [154] reported that adherence to insulin pumps in T1DM adolescents declined with age. The transition from parental care to adolescent self-caring patients led to this. Moreover, more conditions are requested to maintain the T1DM pediatric patients’ adherence to CSII therapy. Giany et al. [155] observed that insulin pumps are underused in T1DM youths. Their study integrated the evaluation of biomedical and psychosocial factors associated with consistent and durable CGM use over time. Their results were confirmed by Trandafir et al. [156], who showed that close family members (parents) and healthcare professionals have an essential role in their adherence to insulin pump therapy, together with other determinants (Figure 8).
De Bock et al. [157] analyzed CGM adherence and contributing factors. They investigated users of sensor-augmented pumps with low-glucose insulin suspension in a 6-month clinical trial. Variable parameters were examined (patients’ age and gender, the values of HbA1c, diabetes duration, frequency of BG testing, sensor accuracy, and the frequency of insulin pump alarm) and associated with CGM adherence. CGM adherence was 75% (35% to 96%), significantly varying with age—the other variables mentioned above were not directly correlated with CGM adherence.
On the other hand, younger clinicians treated more patients using insulin pumps and CGMs, recorded more positive attitudes concerning diabetes technology [158], and identified the barriers to patient adherence: device on the body (73% pump; 63% CGM), alarms (61% CGM), and missing understanding the procedure (40% pump; 46% CGM).
Aiming to increase CGM adherence, the healthcare professionals (a diabetes specialist and a nurse clinician) improved the communication and information transmitting mode to their T1DM patients. Rizvi et al. evaluated the impact of the continuous monitorisation of patients using CGMs in a diabetes clinique. It implied virtual video visits with high frequency; moreover, the patients on intensive insulin therapy could communicate with healthcare staff through an electronic messaging system on glycemic parameters [159]. CGM data was downloaded proactively every 2 weeks from computer cloud-based device accounts in 146 patients with diabetes on multiple (2-5) daily insulin injections or insulin pump therapy. Then, the diabetes specialist analyzes and interprets the glucose profile and individually advises each patient regarding modifications in diet, behavior, and components of the insulin regimen. The communication used an electronic portal linked to email during telehealth and in-person office visits. As a result, the adherence was approximately 100%.
Insulin pumps have been developed to offer continuous glucose sensing coupled with insulin infusions [160]. However, many challenges remain regarding displayed data, including continuous glucose sensor inaccuracies and signal feedback lags [161]. Moreover, the technologies price could explain the poor adherence and early discontinuation. Shengsheng et al. [162] evaluated the monthly healthcare resource waste within the first year of traditional CGM initiation. They combined estimates of real-world nonadherence and too rapid discontinuation from the literature with the wholesale acquisition costs of the current technology in the United States (for a commercial payer and Medicare), or its equivalent in Sweden, Germany, or the Netherlands. Therefore, they found an early discontinuation rate of 27% and nonadherence rates of 13.9%–31.1% over the first 12 months following CGM initiation. In addition, the calculated values of healthcare resource waste were $220,289 (associated with early discontinuation) and $21,775 (caused by nonadherence) for every 100 patients initiating CGM in the U.S. commercial payer scenario. In the Medicare scenario, the corresponding figures were $72,648 and $5,675, respectively. In both cases, nonadherence and early discontinuation accounted for 24% of resources wasted within the first year of CGM initiation. Similar results were observed using the local costs in the other countries analyzed.
The healthcare resource waste associated with nonadherence to traditional CGM and early discontinuation justifies rigorous consideration in selecting suitable patients for these technologies.
Recent studies analyzed glucose-responsive biomaterials [163], especially for rapid and extended self-regulated insulin delivery [164]. Moreover, using chitosan hydrogels integrated with glucose-responsive microspheres for insulin delivery, Yin et al. [165] performed a synthetic artificial pancreas. However, new biomaterials or a substantial variety of composite ones are necessary to build a functional bioartificial pancreas with proper mechanical strengths and biological activities [166]. These properties can be achieved using 3D bioprinting technology. An innovative process in advanced tissue engineering aims to construct clinically applicable bioartificial pancreatic islet tissue [167] with a native tissue environment. It is expected that a 3D bio-printed Pancreas to have critical applications for future diabetes treatment.
7. Conclusions
All presented data evidence that current emerging technologies and control systems significantly improve T1DM self-management. Moreover, unconditional, continuous medical and social help is essential in increasing their self-confidence, motivation, and adherence to CSII, minimizing the impact of other factors (family incomes, requested education, and the ability for technology use). The quality of life of T1DM patients could substantially increase when the advanced devices and algorithms performances are associated with considerable support from family and healthcare providers.
However, the technological systems’ limitations and potential adverse effects and complications lead to continuous worldwide research for finding alternative approaches for T1DM therapy.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: Various Insulin PPs, adapted from [106,108].
Author Contributions
Conceptualization, V.E., V.P., E.A.O., and D.L.; methodology, V.P. and E.A.O.; software, V.P.; validation, V.E., E.A.O., and D.L.; formal analysis, V.P., A.M.M., A.C.F., E.R., and G.R.; investigation, V.P. and E.A.O.; resources, V.E.; data curation, A.M.M., A.C.F., E.R., and G.R.; writing—original draft preparation, V.P.; writing—review and editing, V.E., V.P., E.R., and G.R.; visualization, V.E., E.A.O., A.M.M., A.C.F., E.R., G.R., and D.L.; supervision, V.E., E.A.O., and D.L.; project administration, V.E., E.A.O., and D.L.; funding acquisition, V.E., E.A.O., and A.M.M. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by Carol Davila University of Medicine and Pharmacy
Institutional Review Board Statement
Not applicable
Data Availability Statement
Data are available in the MS and Supplementary Material.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Diabetes. Available online: https://www.who.int/health-topics/diabetes (accessed on 14 April 2023).
- Alam, S.; Hasan, M.K.; Neaz, S.; Hussain, N.; Hossain, M.F.; Rahman, T. Diabetes Mellitus: Insights from Epidemiology, Biochemistry, Risk Factors, Diagnosis, Complications, and Comprehensive Management. Diabetology 2021, 2, 36–50. [Google Scholar]
- Schmidt, A.M. Highlighting Diabetes Mellitus. Arterioscler. Thromb. Vasc. Biol. 2018, 38, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Roep, B.O.; Thomaidou, S.; van Tienhoven, R.; Zaldumbide, A. Type 1 diabetes mellitus as a disease of the β-cell (do not blame the immune system?). Nat. Rev. Endocrinol. 2021, 17, 150–161. [Google Scholar] [PubMed]
- Pozzilli, P.; Maddaloni, E.; Buzzetti, R. Combination immunotherapies for type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2015, 11, 289–297. [Google Scholar] [CrossRef]
- Bone, R.N.; Evans-Molina, C. Combination Immunotherapy for Type 1 Diabetes. Curr. Diab. Rep. 2017, 17, 50. [Google Scholar] [CrossRef]
- Thomas, R.; Carballido, J.M.; Wesley, J.D.; Ahmed, S.T. Overcoming Obstacles in the Development of Antigen-Specific Immunotherapies for Type 1 Diabetes. Front. Immunol. 2021, 12, 730414. [Google Scholar] [PubMed]
- von Scholten, B.J.; Kreiner, F.F.; Gough, S.C.L.; von Herrath, M. Current and future therapies for type 1 diabetes. Diabetologia 2021, 64, 1037–1048. [Google Scholar] [CrossRef]
- Felton, J.L. Timing of Immunotherapy in Type 1 Diabetes: The Earlier, the Better? ImmunoHorizons 2021, 5, 535–542. [Google Scholar]
- Niedźwiedzka-Rystwej, P.; Wołącewicz, M.; Cywoniuk, P.; Klak, M.; Wszoła, M. Crosstalk Between Immunity System Cells and Pancreas. Transformation of Stem Cells Used in the 3D Bioprinting Process as a Personalized Treatment Method for Type 1 Diabetes. Arch. Immunol. Ther. Exp. (Warsz). 2020, 68, 13. [Google Scholar] [CrossRef]
- Sims, E.K.; Bundy, B.N.; Stier, K.; Serti, E.; Lim, N.; Long, S.A.; Geyer, S.M.; Moran, A.; Greenbaum, C.J.; Evans-Molina, C.; et al. Teplizumab improves and stabilizes beta cell function in antibody-positive high-risk individuals. Sci. Transl. Med. 2021, 13, eabc8980. [Google Scholar]
- Frontino, G.; Guercio Nuzio, S.; Scaramuzza, A.; D’Annunzio, G.; Toni, S.; Citriniti, F.; Bonfanti, R. Prevention of type 1 diabetes: where we are and where we are going. Minerva Pediatr. 2021, 73, 486–503. [Google Scholar] [CrossRef]
- Perdigoto, A.L.; Preston-Hurlburt, P.; Clark, P.; Long, S.A.; Linsley, P.S.; Harris, K.M.; Gitelman, S.E.; Greenbaum, C.J.; Gottlieb, P.A.; Hagopian, W.; et al. Treatment of type 1 diabetes with teplizumab: clinical and immunological follow-up after 7 years from diagnosis. Diabetologia 2019, 62, 655–664. [Google Scholar] [PubMed]
- Kwong, S.P.; Wang, C. Review: Usnic acid-induced hepatotoxicity and cell death. Environ. Toxicol. Pharmacol. 2020, 80, 103493. [Google Scholar] [CrossRef]
- Wang, M.; Wang, C.; Ren, S.; Pan, J.; Wang, Y.; Shen, Y.; Zeng, Z.; Cui, H.; Zhao, X. Versatile Oral Insulin Delivery Nanosystems: From Materials to Nanostructures. Int. J. Mol. Sci. 2022, 23, 3362. [Google Scholar] [CrossRef] [PubMed]
- Mahameed, M.; Xue, S.; Stefanov, B.A.; Hamri, G.C. El; Fussenegger, M. Engineering a Rapid Insulin Release System Controlled By Oral Drug Administration. Adv. Sci. 2022, 9, 2105619. [Google Scholar]
- Martínez-López, A.L.; Carvajal-Millan, E.; Canett-Romero, R.; Prakash, S.; Rascón-Chu, A.; López-Franco, Y.L.; Lizardi-Mendoza, J.; Micard, V. Arabinoxylans-Based Oral Insulin Delivery System Targeting the Colon: Simulation in a Human Intestinal Microbial Ecosystem and Evaluation in Diabetic Rats. Pharmaceuticals 2022, 15, 1062. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; He, S.; Ding, Y.; Chen, C.; Cai, Q.; Zhou, W. Multivesicular liposomes for glucose-responsive insulin delivery. Pharmaceutics 2022, 14, 21. [Google Scholar] [CrossRef]
- Sarhadi, S.; Moosavian, S.A.; Mashreghi, M.; Rahiman, N.; Golmohamadzadeh, S.; Tafaghodi, M.; Sadri, K.; Chamani, J.; Jaafari, M.R. B12-functionalized PEGylated liposomes for the oral delivery of insulin: In vitro and in vivo studies. J. Drug Deliv. Sci. Technol. 2022, 69, 103141. [Google Scholar]
- Bahman, F.; Taurin, S.; Altayeb, D.; Taha, S.; Bakhiet, M.; Greish, K. Oral insulin delivery using poly (Styrene co-Maleic acid) micelles in a diabetic mouse model. Pharmaceutics 2020, 12, 1–17. [Google Scholar] [CrossRef]
- Han, X.; Lu, Y.; Xie, J.; Zhang, E.; Zhu, H.; Du, H.; Wang, K.; Song, B.; Yang, C.; Shi, Y.; et al. Zwitterionic micelles efficiently deliver oral insulin without opening tight junctions. Nat. Nanotechnol. 2020, 15, 605–614. [Google Scholar]
- Wu, H.; Guo, T.; Nan, J.; Yang, L.; Liao, G.; Park, H.J.; Li, J. Hyaluronic-Acid-Coated Chitosan Nanoparticles for Insulin Oral Delivery: Fabrication, Characterization, and Hypoglycemic Ability. Macromol. Biosci. 2022, 22, e2100493. [Google Scholar] [CrossRef]
- Li, J.; Qiang, H.; Yang, W.; Xu, Y.; Feng, T.; Cai, H.; Wang, S.; Liu, Z.; Zhang, Z.; Zhang, J. Oral insulin delivery by epithelium microenvironment-adaptive nanoparticles. J. Control. Release 2022, 341, 31–43. [Google Scholar]
- Elkhatib, M.M.; Ali, A.I.; Al-Badrawy, A.S. In vitro and in vivo comparative study of oral nanoparticles and gut iontophoresis as oral delivery systems for insulin. Biol. Pharm. Bull. 2021, 44, 251–258. [Google Scholar] [PubMed]
- Banerjee, A.; Wong, J.; Gogoi, R.; Brown, T.; Mitragotri, S. Intestinal micropatches for oral insulin delivery. J. Drug Target. 2017, 25, 608–615. [Google Scholar] [CrossRef]
- Torabi, N.; Nazari, M.; Fahanik-Babaei, J.; Eliassi, A. Long-term administration of intranasal insulin improves peripheral glucose concentration in diabetic male rats. Physiol. Pharmacol. 2020, 24, 268–275. [Google Scholar] [CrossRef]
- Roque, P.; Nakadate, Y.; Sato, H.; Sato, T.; Wykes, L.; Kawakami, A.; Yokomichi, H.; Matsukawa, T.; Schricker, T. Intranasal administration of 40 and 80 units of insulin does not cause hypoglycemia during cardiac surgery: a randomized controlled trial. Can. J. Anesth. 2021, 68, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Huang, Y.; Yang, J.; Tu, R.; Zhang, X.; He, W.W.; Hou, C.Y.; Wang, X.M.; Yu, J.M.; Jiang, G.H. Intranasal insulin ameliorates neurological impairment after intracerebral hemorrhage in mice. Neural Regen. Res. 2022, 17, 210–216. [Google Scholar]
- Jin, X.; Zhu, D.D.; Chen, B.Z.; Ashfaq, M.; Guo, X.D. Insulin delivery systems combined with microneedle technology. Adv. Drug Deliv. Rev. 2018, 127, 119–137. [Google Scholar] [CrossRef]
- Chen, S.; Miyazaki, T.; Itoh, M.; Matsumoto, H.; Moro-Oka, Y.; Tanaka, M.; Miyahara, Y.; Suganami, T.; Matsumoto, A. Temperature-Stable Boronate Gel-Based Microneedle Technology for Self-Regulated Insulin Delivery. ACS Appl. Polym. Mater. 2020, 2, 2781–2790. [Google Scholar]
- Cui, C.Y.; Lu, W.L.; Xiao, L.; Zhang, S.Q.; Huang, Y.B.; Li, S.L.; Zhang, R.J.; Wang, G.L.; Zhang, X.; Zhang, Q. Sublingual delivery of insulin: Effects of enhancers on the mucosal lipid fluidity and protein conformation, transport, and in Vivo hypoglycemic activity. Biol. Pharm. Bull. 2005, 28, 2279–2288. [Google Scholar] [CrossRef]
- Erzengin, S.; Guler, E.; Eser, E.; Polat, E.B.; Gunduz, O.; Cam, M.E. In vitro and in vivo evaluation of 3D printed sodium alginate/polyethylene glycol scaffolds for sublingual delivery of insulin: Preparation, characterization, and pharmacokinetics. Int. J. Biol. Macromol. 2022, 204, 429–440. [Google Scholar] [PubMed]
- Hermansen, K.; Fontaine, P.; Kukolja, K.K.; Peterkova, V.; Leth, G.; Gall, M.A. Insulin analogues (insulin detemir and insulin aspart) versus traditional human insulins (NPH insulin and regular human insulin) in basal-bolus therapy for patients with Type 1 diabetes. Diabetologia 2004, 47, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Lucidi, P.; Porcellati, F.; Andreoli, A.M.; Carriero, I.; Candeloro, P.; Cioli, P.; Bolli, G.B.; Fanelli, C.G. Pharmacokinetics and pharmacodynamics of NPH insulin in type 1 diabetes: The Importance of appropriate resuspension before subcutaneous injection. Diabetes Care 2015, 38, 2204–2210. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Esposito, K. Continuous glucose monitoring for patients with type 1 diabetes on multiple daily injections of insulin: pros and cons. Endocrine 2018, 59, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Ross, L.J.; Neville, K.A. Continuous subcutaneous insulin infusion versus multiple daily injections for type 1 diabetes. J. Paediatr. Child Health 2019, 55, 718–722. [Google Scholar] [PubMed]
- Savu, O.; Elian, V.; Steriade, O.; Teodoru, I.; Mihut, S.; Tacu, C.; Covic, A.; Serafinceanu, C. The impact of basal insulin analogues on glucose variability in patients with type 2 diabetes undergoing renal replacement therapy for end-stage renal disease. Int. Urol. Nephrol. 2016, 48, 265–270. [Google Scholar]
- Brown-Georgi, J.; Chhabra, H.; Vigersky, R.A. The Rising Cost of Insulin for Pump Users: How Policy Drives Prices. J. Diabetes Sci. Technol. 2020, 15, 1177–1180. [Google Scholar]
- Lawton, J.; Kirkham, J.; Rankin, D.; White, D.A.; Elliott, J.; Jaap, A.; Smithson, W.H.; Heller, S.; Gianfrancesco, C.; Gordon, V.; et al. Who gains clinical benefit from using insulin pump therapy? A qualitative study of the perceptions and views of health professionals involved in the Relative Effectiveness of Pumps over MDI and Structured Education (REPOSE) trial. Diabet. Med. 2016, 33, 243–251. [Google Scholar] [CrossRef]
- Herkert, D.; Vijayakumar, P.; Luo, J.; Schwartz, J.I.; Rabin, T.L.; Defilippo, E.; Lipska, K.J. Cost-Related Insulin Underuse Among Patients With Diabetes. JAMA Intern. Med. 2019, 179, 112–114. [Google Scholar] [CrossRef]
- Moroșan, E.; Popovici, V.; Elian, V.; Dărăban, A.M.; Rusu, A.I.; Licu, M.; Mititelu, M.; Karampelas, O. The Impact of Medical Nutrition Intervention on the Management of Hyperphosphatemia in Hemodialysis Patients with Stage 5 Chronic Kidney Disease: A Case Series. Int. J. Environ. Res. Public Health 2023, 20, 5049. [Google Scholar] [CrossRef]
- Elian, V.; Ditu, G.; Bodnarescu, M.; Calin, A.; Serafinceanu, C.; Cioca, G.; Pantea-Stoian, A. Protein-Energy Wasting and Survival in Diabetes Mellitus Hemodialysis Patients. In Proceedings of the 2nd International Conference on Interdisciplinary Management of Diabetes Mellitus and its Complications, Bucharest, Romania, 3–5 March 2016. [Google Scholar]
- Eliasson, B.; Lyngfelt, L.; Strömblad, S.O.; Franzén, S.; Eeg-Olofsson, K. The significance of chronic kidney disease, heart failure and cardiovascular disease for mortality in type 1 diabetes: nationwide observational study. Sci. Rep. 2022, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Genuth, S. Insights from the diabetes control and complications trial/epidemiology of diabetes interventions and complications study on the use of intensive glycemic treatment to reduce the risk of complications of type 1 diabetes. In Proceedings of the Endocrine Practice; 2006; Vol. 12, pp. 34–41.
- Niazi, A.K.; Kalra, S. Diabetes and tuberculosis: A review of the role of optimal glycemic control. J. Diabetes Metab. Disord. 2012, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- da Silva de Sousa, G.G.; Yamamura, M.; de Araújo, M.F.M.; Ramos, A.C.V.; Arcêncio, R.A.; de Jesus Costa, A.C.P.; Pascoal, L.M.; Santos, F.S.; de Oliveira Serra, M.A.A.; Fontoura, I.G.; et al. Vulnerable territories to tuberculosis-diabetes mellitus comorbidity in a northeastern Brazilian scenario. J. Infect. Dev. Ctries. 2022, 16, 813–820. [Google Scholar] [CrossRef]
- Kaur, N.; Bhadada, S.K.; Minz, R.W.; Dayal, D.; Kochhar, R. Interplay between type 1 diabetes mellitus and celiac disease: Implications in treatment. Dig. Dis. 2018, 36, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Kogut, M.D.; Brinegar, C.H. Addison’s disease and diabetes mellitus. J. Pediatr. 1972, 81, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Ingley, M.; Quebedeaux, P.; Schmidbauer, K.; Amghaiab, I.A.; Chan, J. PMON315 Hyperglycemia Dilemma: Concomitant Type 1 Diabetes Mellitus and Cushing’s disease. J. Endocr. Soc. 2022, 6, A624–A625. [Google Scholar] [CrossRef]
- Ilie, I.; Ciubotaru, V.; Tulin, A.; Hortopan, D.; Caragheorgheopol, A.; Purice, M.; Neamtu, C.; Elian, V.I.; Banica, A.; Oprea, L.; et al. The multifarious cushing’s – Lessons from a case series. Acta Endocrinol. (Copenh). 2019, 15, 261–269. [Google Scholar]
- Wardian, J.L.; True, M.W.; Folaron, I.; Colburn, J.; Tate, J.M.; Beckman, D.J. The Choice Should Be Yours: Diabetes-Related Distress by Insulin Delivery Method for People with Type 1 Diabetes. Diabetes Technol. Ther. 2020, 22, 42–47. [Google Scholar] [CrossRef]
- Tareen, R.S.; Tareen, K. Psychosocial aspects of diabetes management: Dilemma of diabetes distress. Transl. Pediatr. 2017, 6, 383–396. [Google Scholar]
- Barnard, K.; Crabtree, V.; Adolfsson, P.; Davies, M.; Kerr, D.; Kraus, A.; Gianferante, D.; Bevilacqua, E.; Serbedzija, G. Impact of Type 1 Diabetes Technology on Family Members/Significant Others of People with Diabetes. J. Diabetes Sci. Technol. 2016, 10, 824–830. [Google Scholar]
- Davies, M. Psychological aspects of diabetes management. Med. (United Kingdom) 2022, 50, 749–751. [Google Scholar] [CrossRef]
- Mianowska, B.; Fedorczak, A.; Michalak, A.; Pokora, W.; Barańska-Nowicka, I.; Wilczyńska, M.; Szadkowska, A. Diabetes related distress in children with type 1 diabetes before and during the covid-19 lockdown in spring 2020. Int. J. Environ. Res. Public Health 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wang, H.; Li, X.; Zhou, Z.; Valimaki, M.; Whittemore, R.; Grey, M.; Guo, J. Factors associated with diabetes distress among adolescents with type 1 diabetes. J. Clin. Nurs. 2021, 30, 1893–1903. [Google Scholar] [CrossRef]
- Schmidt, C.B.; Voorhorst, I.; Van De Gaar, V.H.W.; Keukens, A.; Potter Van Loon, B.J.; Snoek, F.J.; Honig, A. Diabetes distress is associated with adverse pregnancy outcomes in women with gestational diabetes: A prospective cohort study. BMC Pregnancy Childbirth 2019, 19, 223. [Google Scholar]
- Skinner, T.C.; Joensen, L.; Parkin, T. Twenty-five years of diabetes distress research. Diabet. Med. 2020, 37, 393–400. [Google Scholar] [CrossRef]
- De Wit, M.; Pouwer, F.; Snoek, F.J. How to identify clinically significant diabetes distress using the Problem Areas in Diabetes (PAID) scale in adults with diabetes treated in primary or secondary care? Evidence for new cut points based on latent class analyses. BMJ Open 2022, 12, e056304. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Earles, J.; Dudl, R.J.; Lees, J.; Mullan, J.; Jackson, R.A. Assessing psychosocial distress in diabetes: Development of the Diabetes Distress Scale. Diabetes Care 2005, 28, 626–631. [Google Scholar] [CrossRef]
- Rubin, R.R.; Peyrot, M. Health-related quality of life and treatment satisfaction in the sensor-augmented pump therapy for A1C reduction 3 (STAR 3) trial. Diabetes Technol. Ther. 2012, 14, 143–151. [Google Scholar]
- Klamann, M.; Majkowska, L. New technologies and metabolic control in type 1 diabetes mellitus. Clin. Diabetol. 2017, 6, 111–114. [Google Scholar] [CrossRef]
- Kimbell, B.; Lawton, J.; Boughton, C.; Hovorka, R.; Rankin, D. Parents’ experiences of caring for a young child with type 1 diabetes: a systematic review and synthesis of qualitative evidence. BMC Pediatr. 2021, 21, 160. [Google Scholar]
- Pauley, M.E.; Berget, C.; Messer, L.H.; Forlenza, G.P. Barriers to uptake of insulin technologies and novel solutions. Med. Devices Evid. Res. 2021, 14, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Pease, A.; Zomer, E.; Liew, D.; Lo, C.; Earnest, A.; Zoungas, S. Cost-effectiveness of health technologies in adults with type 1 diabetes: A systematic review and narrative synthesis. Syst. Rev. 2020, 9, 171. [Google Scholar] [PubMed]
- Prahalad, P.; Tanenbaum, M.; Hood, K.; Maahs, D.M. Diabetes technology: improving care, improving patient-reported outcomes and preventing complications in young people with Type 1 diabetes. Diabet. Med. 2018, 35, 419–429. [Google Scholar]
- Gonder-Frederick, L.A.; Shepard, J.A.; Grabman, J.H.; Ritterband, L.M. Psychology, technology, and diabetes management. Am. Psychol. 2016, 71, 577–589. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Klonoff, D.C. Diabetes technology update: Use of insulin pumps and continuous glucose monitoring in the hospital. Diabetes Care 2018, 41, 1579–1589. [Google Scholar] [CrossRef]
- Yeh, T.; Yeung, M.; Mendelsohn Curanaj, F.A. Managing Patients with Insulin Pumps and Continuous Glucose Monitors in the Hospital: to Wear or Not to Wear. Curr. Diab. Rep. 2021, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Boyle, E.; Delaney, C.; Shaw, J. A comparison of blood glucose meters in Australia. Diabetes Res. Clin. Pract. 2006, 71, 113–118. [Google Scholar]
- Apostolopoulos, A.; Apostolopoulou, D.; Tsoubeli, A. Application of health informatics in the education of diabetic patients for the improvement of self-management and reporting to specialists. J. Inf. Technol. Healthc. 2007, 5, 379–386. [Google Scholar]
- Olczuk, D.; Priefer, R. A history of continuous glucose monitors (CGMs) in self-monitoring of diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 181–187. [Google Scholar]
- Franceschi, R.; Micheli, F.; Mozzillo, E.; Cauvin, V.; Liguori, A.; Soffiati, M.; Giani, E. Intermittently Scanned and Continuous Glucose Monitor Systems: A Systematic Review on Psychological Outcomes in Pediatric Patients. Front. Pediatr. 2021, 9, 660173. [Google Scholar] [CrossRef]
- Visser, M.M.; Charleer, S.; Fieuws, S.; De Block, C.; Hilbrands, R.; Van Huffel, L.; Maes, T.; Vanhaverbeke, G.; Dirinck, E.; Myngheer, N.; et al. Comparing real-time and intermittently scanned continuous glucose monitoring in adults with type 1 diabetes (ALERTT1): a 6-month, prospective, multicentre, randomised controlled trial. Lancet 2021, 397, 2275–2283. [Google Scholar] [CrossRef] [PubMed]
- Staal, O.M.; Hansen, H.M.U.; Christiansen, S.C.; Fougner, A.L.; Carlsen, S.M.; Stavdahl, Ø. Differences between flash glucose monitor and fingerprick measurements. Biosensors 2018, 8, 93. [Google Scholar] [CrossRef]
- Fokkert, M.; Van Dijk, P.R.; Edens, M.A.; Díez Hernández, A.; Slingerland, R.; Gans, R.; Delgado Álvarez, E.; Bilo, H. Performance of the Eversense versus the Free Style Libre Flash glucose monitor during exercise and normal daily activities in subjects with type 1 diabetes mellitus. BMJ Open Diabetes Res. Care 2020, 8, e001193. [Google Scholar] [PubMed]
- Ahmed, I.; Jiang, N.; Shao, X.; Elsherif, M.; Alam, F.; Salih, A.; Butt, H.; Yetisen, A.K. Recent advances in optical sensors for continuous glucose monitoring. Sensors & Diagnostics 2022, 1, 1098–1125. [Google Scholar]
- Gaynanova, I.; Punjabi, N.; Crainiceanu, C. Modeling continuous glucose monitoring (CGM) data during sleep. Biostatistics 2022, 23, 223–239. [Google Scholar] [CrossRef]
- Urakami, T. The Advanced Diabetes Technologies for Reduction of the Frequency of Hypoglycemia and Minimizing the Occurrence of Severe Hypoglycemia in Children and Adolescents with Type 1 Diabetes. J. Clin. Med. 2023, 12, 781. [Google Scholar] [CrossRef]
- Kropff, J.; DeVries, J.H. Continuous Glucose Monitoring, Future Products, and Update on Worldwide Artificial Pancreas Projects. Diabetes Technol. Ther. 2016, 18, S253–S263. [Google Scholar] [CrossRef]
- Cappon, G.; Acciaroli, G.; Vettoretti, M.; Facchinetti, A.; Sparacino, G. Wearable continuous glucose monitoring sensors: A revolution in diabetes treatment. Electron. 2017, 6, 65. [Google Scholar] [CrossRef]
- Zafar, H.; Channa, A.; Jeoti, V.; Stojanović, G.M. Comprehensive Review on Wearable Sweat-Glucose Sensors for Continuous Glucose Monitoring. Sensors 2022, 22, 638. [Google Scholar]
- Wu, P.T.; Segovia, D.E.; Lee, C.C.; Nguyen, K.L. Consistency of continuous ambulatory interstitial glucose monitoring sensors. Biosensors 2018, 8, 49. [Google Scholar] [CrossRef]
- Mensh, B.D.; Wisniewski, N.A.; Neil, B.M.; Burnett, D.R. Susceptibility of interstitial continuous glucose monitor performance to sleeping position. J. Diabetes Sci. Technol. 2013, 7, 863–870. [Google Scholar] [CrossRef]
- Russell, S.J. , El-Khatib, F.H., Sinha, M., Magyar, K.L., Mckeon, K., Goergen, L.G., Hillard, M.A., Nathan, D.M. and Damiano, E.R. Multiday outpatient glycemic control in adolescents with type 1 diabetes using a bihormonal bionic pancreas: The barton center summer camp study. Diabetes 2014, 63, A62. [Google Scholar]
- Beck, R.W.; Riddlesworth, T.D.; Ruedy, K.; Ahmann, A.; Haller, S.; Kruger, D.; McGill, J.B.; Polonsky, W.; Price, D.; Aronoff, S.; et al. Continuous glucose monitoring versus usual care in patients with type 2 diabetes receiving multiple daily insulin injections. Ann. Intern. Med. 2017, 167, 365–374. [Google Scholar] [CrossRef]
- Vettoretti, M.; Cappon, G.; Facchinetti, A.; Sparacino, G. Advanced diabetes management using artificial intelligence and continuous glucose monitoring sensors. Sensors (Switzerland) 2020, 20, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Tagougui, S.; Taleb, N.; Rabasa-Lhoret, R. The benefits and limits of technological advances in glucose management around physical activity in patients type 1 diabetes. Front. Endocrinol. (Lausanne). 2019, 10, 818. [Google Scholar]
- Von Dem Berge, T.; Biester, S.; Biester, T.; Buchmann, A.K.; Datz, N.; Grosser, U.; Kapitzke, K.; Klusmeier, B.; Remus, K.; Reschke, F.; et al. Recommendations for Diabetes Treatment with Systems for Automated Insulin Delivery. Diabetol. und Stoffwechsel 2022, 17, 61–73. [Google Scholar]
- Shapiro, A.R. Nonadjunctive Use of Continuous Glucose Monitors for Insulin Dosing: Is It Safe? J. Diabetes Sci. Technol. 2017, 11, 833–838. [Google Scholar]
- ElSayed NA.; Aleppo G.; Aroda VR.; Bannuru RR.; Brown FM.; Bruemmer D.; Collins BS.; Hilliard ME.; Isaacs D.; Johnson EL.; Kahan S.; Khunti K.; Leon J.; Lyons SK.; Murdock L.; Perry ML.; Prahalad P.; Pratley RE.; Seley JJ.; Stanton RC.; Woodward CC.; Gabbay RA. on behalf of the American Diabetes Association. 17. Diabetes Advocacy: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S279-S280.
- https://www.diabetesnet.com/diabetes-technology/meters-monitors/compare-current-monitors/ accessed on March 14, 2023.
- Helton, K.L.; Ratner, B.D.; Wisniewski, N.A. Biomechanics of the sensor-tissue interface - Effects of motion, pressure, and design on sensor performance and foreign body response - Part II: Examples and application. In Proceedings of the Journal of Diabetes Science and Technology; 2011; Vol. 5, pp. 647–656.
- Petrofsky, J.S.; McLellan, K.; Prowse, M.; Bains, G.; Berk, L.; Lee, S. The effect of body fat, aging, and diabetes on vertical and shear pressure in and under a waist belt and its effect on skin blood flow. Diabetes Technol. Ther. 2010, 12, 153–160. [Google Scholar] [CrossRef]
- Ardilouze, J.L.; Karpe, F.; Currie, J.M.; Frayn, K.N.; Fielding, B.A. Subcutaneous adipose tissue blood flow varies between superior and inferior levels of the anterior abdominal wall. Int. J. Obes. 2004, 28, 228–233. [Google Scholar] [CrossRef]
- Cengiz, E.; Tamborlane, W. V. A tale of two compartments: Interstitial versus blood glucose monitoring. Diabetes Technol. Ther. 2009, 11, S11–6. [Google Scholar] [CrossRef]
- Weinstein, R.L.; Schwartz, S.L.; Brazg, R.L.; Bugler, J.R.; Peyser, T. a; McGarraugh, G. V Accuracy of the 5-Day FreeStyle Navigator Continuous Glucose Monitoring System. Diabetes Care 2007, 30, 1125–1130. [Google Scholar] [PubMed]
- Hoss, U.; Budiman, E.S.; Liu, H.; Christiansen, M.P. Continuous glucose monitoring in the subcutaneous tissue over a 14-day sensor wear period. J. Diabetes Sci. Technol. 2013, 7, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Borazan, A.; Binici, D.N. Relationship between insulin resistance and inflammation markers in hemodialysis patients. Ren. Fail. 2010, 32, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, M.; Jansen, J.A.; Kros, A.; Vriezema, D.M.; Sommerdijk, N.A.J.M.; Nolte, R.J.M.; Lutterman, J.A.; Van Hvell, S.W.F.M.; Van Der Gaag, A. Influence of inflammatory cells and serum on the performance of implantable glucose sensors. J. Biomed. Mater. Res. 2001, 54, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.C.; Spokane, R.B.; Homan, M.M.; Sudan, R.; Miller, M. Long-term stability of electro-enzymatic glucose sensors implanted in mice. An update. ASAIO Trans. 1988, 34, 259–265. [Google Scholar]
- https://www.diabetes.co.uk/news/2023/feb/non-invasive-blood-glucose-monitoring-wearable-launch-date-revealed.html accessed on March 14, 2023.
- Alsaleh, F.M.; Smith, F.J.; Keady, S.; Taylor, K.M.G. Insulin pumps: From inception to the present and toward the future. J. Clin. Pharm. Ther. 2010, 35, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Benkhadra, K.; Alahdab, F.; Tamhane, S.U.; McCoy, R.G.; Prokop, L.J.; Murad, M.H. Continuous subcutaneous insulin infusion versus multiple daily injections in individuals with type 1 diabetes: a systematic review and meta-analysis. Endocrine 2017, 55, 77–84. [Google Scholar]
- https://www.diabetes.co.uk/insulin-pumps/pros-cons-of-insulin-pumps.html, accessed on March 14, 2023.
- Kulzer, B.; Freckmann, G.; Heinemann, L.; Schnell, O.; Hinzmann, R.; Ziegler, R. Diabetes Research and Clinical Practice Patch Pumps : What are the advantages for people with diabetes ? Diabetes Res. Clin. Pract. 2022, 187, 109858. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, T.; Nikkel, C.; Dziengelewski, B.; Wu, S.; Chen, A.M.H. Clinical Evaluation of Basal-Bolus Therapy Delivered by the V-Go® Wearable Insulin Delivery Device in Patients with Type 2 Diabetes: A Retrospective Analysis. Pharmacy 2020, 8, 215. [Google Scholar] [CrossRef]
- Thompson, B.; Cook, C.B. Insulin Pumping Patches: Emerging Insulin Delivery Systems. J. Diabetes Sci. Technol. 2019, 13, 8–10. [Google Scholar]
- Berget, C.; Messer, L.H.; Forlenza, G.P. A clinical overview of insulin pump therapy for the management of diabetes: Past, present, and future of intensive therapy. Diabetes Spectr. 2019, 32, 194–204. [Google Scholar] [CrossRef]
- Pohar, S.L. Subcutaneous open-loop insulin delivery for type 1 diabetes: Paradigm Real-Time System. Issues Emerg. Health Technol. 2007, 1–6. [Google Scholar]
- Mastrototaro, J.; Lee, S. The integrated MiniMed Paradigm real-time insulin pump and glucose monitoring system: Implications for improved patient outcomes. Diabetes Technol. Ther. 2009, 11, S37–43. [Google Scholar]
- Danne, T.; Kordonouri, O.; Holder, M.; Haberland, H.; Golembowski, S.; Remus, K.; Bläsig, S.; Wadien, T.; Zierow, S.; Hartmann, R.; et al. Prevention of hypoglycemia by using low glucose suspend function in sensor-augmented pump therapy. Diabetes Technol. Ther. 2011, 13, 1129–1134. [Google Scholar] [CrossRef]
- Bergenstal, R.M.; Klonoff, D.C.; Garg, S.K.; Bode, B.W.; Meredith, M.; Slover, R.H.; Ahmann, A.J.; Welsh, J.B.; Lee, S.W.; Kaufman, F.R. Threshold-Based Insulin-Pump Interruption for Reduction of Hypoglycemia. N. Engl. J. Med. 2013, 369, 224–232. [Google Scholar] [CrossRef]
- Abraham, M.B.; Nicholas, J.A.; Smith, G.J.; Fairchild, J.M.; King, B.R.; Ambler, G.R.; Cameron, F.J.; Davis, E.A.; Jones, T.W. Reduction in hypoglycemia with the predictive low-Glucose management system: A long-term randomized controlled trial in adolescents with type 1 diabetes. Diabetes Care 2018, 41, 303–310. [Google Scholar]
- Forlenza, G.P.; Li, Z.; Buckingham, B.A.; Pinsker, J.E.; Cengiz, E.; Paul Wadwa, R.; Ekhlaspour, L.; Church, M.M.; Weinzimer, S.A.; Jost, E.; et al. Predictive low-glucose suspend reduces hypoglycemia in adults, adolescents, and children with type 1 diabetes in an at-home randomized crossover study: Results of the PROLOG trial. Diabetes Care 2018, 41, 2155–2161. [Google Scholar] [CrossRef]
- Boughton, C.K.; Hovorka, R. New closed-loop insulin systems. Diabetologia 2021, 64, 1007–1015. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, X.L.; Li, Z.H.; Zhu, Z.G.; Qian, S.H.; Flewitt, A.J. Current and emerging technology for continuous glucose monitoring. Sensors (Switzerland) 2017, 17, 182. [Google Scholar] [CrossRef] [PubMed]
- El Youssef, J.; Castle, J.; Ward, W.K. A review of closed-loop algorithms for glycemic control in the treatment of type 1 diabetes. Algorithms 2009, 2, 518–532. [Google Scholar]
- Quiroz, G. The evolution of control algorithms in artificial Pancreas: A historical perspective. Annu. Rev. Control 2019, 48, 222–232. [Google Scholar] [CrossRef]
- Vigersky, R.A.; Huang, S.; Cordero, T.L.; Shin, J.; Lee, S.W.; Chhabra, H.; Kaufman, F.R.; Cohen, O. Improved HBA1C, total daily insulin dose, and treatment satisfaction with insulin pump therapy compared to multiple daily insulin injections in patients with type 2 diabetes irrespective of baseline C-peptide levels. Endocr. Pract. 2018, 24, 446–452. [Google Scholar]
- Abuin, P.; Rivadeneira, P.S.; Ferramosca, A.; González, A.H. Artificial pancreas under stable pulsatile MPC: Improving the closed-loop performance. J. Process Control 2020, 92, 246–260. [Google Scholar]
- Incremona, G.P.; Messori, M.; Toffanin, C.; Cobelli, C.; Magni, L. Model predictive control with integral action for artificial Pancreas. Control Eng. Pract. 2018, 77, 86–94. [Google Scholar]
- Karpelyev, V.A.; Philippov, Y.I.; Averin, A. V.; Boyarskiy, M.D.; Gavrilov, D.A. Development and in silico validation of the pid-algorithm for the artificial Pancreas with intraperitoneal insulin delivery. Diabetes Mellit. 2018, 21, 58–65. [Google Scholar] [CrossRef]
- Chakrabarty, A.; Gregory, J.M.; Moore, L.M.; Williams, P.E.; Farmer, B.; Cherrington, A.D.; Lord, P.; Shelton, B.; Cohen, D.; Zisser, H.C.; et al. A new animal model of insulin-glucose dynamics in the intraperitoneal space enhances closed-loop control performance. J. Process Control 2019, 76, 62–73. [Google Scholar] [CrossRef]
- Soylu, S.; Danisman, K. In silico testing of optimized Fuzzy P+D controller for artificial Pancreas. Biocybern. Biomed. Eng. 2018, 38, 399–408. [Google Scholar] [CrossRef]
- Mehmood, S.; Ahmad, I.; Arif, H.; Ammara, U.E.; Majeed, A. Artificial pancreas control strategies used for type 1 diabetes control and treatment: A comprehensive analysis. Appl. Syst. Innov. 2020, 3, 1–36. [Google Scholar]
- Peyser, T.; Dassau, E.; Breton, M.; Skyler, J.S. The artificial Pancreas: Current status and future prospects in the management of diabetes. Ann. N. Y. Acad. Sci. 2014, 1311, 102–123. [Google Scholar] [CrossRef] [PubMed]
- Hybrid Closed-Loop Insulin Delivery Systems for People with Type 1 Diabetes, available online at https://www.cadth.ca/hybrid-closed-loop-insulin-delivery-systems-people-type-1-diabetes, accessed on March 14, 2023.
- De Bock, M.; Dart, J.; Roy, A.; Davey, R.; Soon, W.; Berthold, C.; Retterath, A.; Grosman, B.; Kurtz, N.; Davis, E.; et al. Exploration of the Performance of a Hybrid Closed Loop Insulin Delivery Algorithm That Includes Insulin Delivery Limits Designed to Protect Against Hypoglycemia. J. Diabetes Sci. Technol. 2017, 11, 68–73. [Google Scholar] [CrossRef]
- El-Khatib, F.H.; Russell, S.J.; Magyar, K.L.; Sinha, M.; McKeon, K.; Nathan, D.M.; Damiano, E.R. Autonomous and continuous adaptation of a bihormonal bionic pancreas in adults and adolescents with type 1 diabetes. J. Clin. Endocrinol. Metab. 2014, 99, 1701–1711. [Google Scholar]
- Elkhatib, F.; Buckingham, B.A.; Buse, J.B.; Harlan, D.M.; Magyar, K.; Ly, T.T.; Kirkman, M.S.; Malkani, S.; Thompson, M.J.; Lock, J.P.; et al. Home use of a bihormonal bionic pancreas vs. Conventional insulin pump therapy in adults with type 1 diabetes: A multicenter, randomized clinical trial. Diabetes 2016, 65. [Google Scholar]
- Rayannavar, A.; Mitteer, L.M.; Balliro, C.A.; El-Khatib, F.H.; Lord, K.L.; Hawkes, C.P.; Ballester, L.S.; Damiano, E.R.; Russell, S.J.; De Leon, D.D. The bihormonal bionic Pancreas improves glycemic control in individuals with hyperinsulinism and postpancreatectomy diabetes: A pilot study. Diabetes Care 2021, 44, 2582–2585. [Google Scholar] [CrossRef]
- Beck, R.W.; Russell, S.J.; Damiano, E.R.; El-Khatib, F.H.; Ruedy, K.J.; Balliro, C.; Li, Z.; Calhoun, P. A Multicenter Randomized Trial Evaluating Fast-Acting Insulin Aspart in the Bionic Pancreas in Adults with Type 1 Diabetes. Diabetes Technol. Ther. 2022, 24, 681–696. [Google Scholar]
- Wszola, M.; Klak, M.; Kosowska, A.; Olkowska-Truchanowicz, J.; Tymicki, G.; Berman, A.; Bryniarski, T.; Kołodziejska, M.; Uchrynowska-Tyszkiewicz, I.; Kamiński, A. Bionic Pancreas: the first results of functionality bionic tissue model with pancreatic islets. Korean J. Transplant. 2021, 35, S44–S44. [Google Scholar] [CrossRef]
- Russell, S.; Balliro, C.; Sherwood, J.; Jafri, R.; Hillard, M.; Sullivan, M.; Greaux, E.; Selagamsetty, R.; El-Khatib, F.; Damiano, E. Home use of the iLet bionic Pancreas in the bihormonal configuration using glucagon versus the insulin-only configuration in adults with type 1 diabetes. Diabetes Technol. Ther. 2020, 22, S97. [Google Scholar]
- NCT03565666 The Insulin-Only Bionic Pancreas Bridging Study 2018, available at https://clinicaltrials.gov/show/NCT03565666 , accessed on March 10, 2023. 10 March.
- Fisher, L.; Polonsky, W.H.; Hessler, D.M.; Masharani, U.; Blumer, I.; Peters, A.L.; Strycker, L.A.; Bowyer, V. Understanding the sources of diabetes distress in adults with type 1 diabetes. J. Diabetes Complications 2015, 29, 572–577. [Google Scholar]
- Hessler, D.; Fisher, L.; Polonsky, W.; Johnson, N. Understanding the areas and correlates of diabetes-related distress in parents of teens with type 1 diabetes. J. Pediatr. Psychol. 2016, 41, 750–758. [Google Scholar]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Johnson, N. Emotional distress in the partners of type 1 diabetes adults: Worries about hypoglycemia and other key concerns. Diabetes Technol. Ther. 2016, 18, 292–297. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Edelman, S. V. Development of a New Measure for Assessing Glucose Monitoring Device-Related Treatment Satisfaction and Quality of Life. Diabetes Technol. Ther. 2015, 17, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Fisher, L.; Hessler, D.; Edelman, S. V. Development of a New Measure for Assessing Insulin Delivery Device Satisfaction in Patients with Type 1 and Type 2 Diabetes. Diabetes Technol. Ther. 2015, 17, 773–779. [Google Scholar] [CrossRef]
- Joensen, L.E.; Andersen, M.M.; Jensen, S.; Nørgaard, K.; Willaing, I. The effect of peer support in adults with insulin pump-treated type 1 diabetes: A pilot study of a flexible and participatory intervention. Patient Prefer. Adherence 2017, 11, 1879–1890. [Google Scholar] [PubMed]
- Elian, V.; Musat, M.; Radulian, G.; Negoita, O. A model of efficiency on introducing technology in T1DM management process for patients with 30+year’s duration of diabetes - a single-center interventional study. Diabetes Technology and Therapeutics 2020, 22, A225–A225. [Google Scholar]
- Fanzola, V.; Riboni, S.; Cannalire, G.; Metti, M.; Bensi, G.; Granata, C.; Biasucci, G. The impact of new continuous glucose monitoring (CGM) devices versus self-management of blood glucose (SMBG) on the daily life of parents and children affected by type 1 diabetes mellitus. J. Pediatr. Neonatal Individ. Med. 2022, 11, e110111. [Google Scholar]
- Patton, S.R.; Clements, M.A. Psychological Reactions Associated with Continuous Glucose Monitoring in Youth. J. Diabetes Sci. Technol. 2016, 10, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, J.T.; Pratt, K.; Aggarwal, J.; Volkening, L.K.; Laffel, L.M.B. Psychosocial correlates of continuous glucose monitoring use in youth and adults with type 1 diabetes and parents of youth. Diabetes Technol. Ther. 2012, 14, 523–526. [Google Scholar] [PubMed]
- Landau Z, Rachmiel M, Pinhas-Hamiel O, Boaz M, Bar-Dayan Y, Wainstein J, T.R. Parental sleep quality and continuous glucose monitoring system use in children with type 1 diabetes. Diabetes Technol. Ther. 2015, 17, S18–S19.
- Rusak, E.; Ogarek, N.; Wolicka, K.; Mrówka, A.; Seget, S.; Kuźnik, M.; Jarosz-Chobot, P. The quality of life and satisfaction with continuous glucose monitoring therapy in children under 7 years of age with T1D using the rTCGM system integrated with insulin pump—a caregivers point of view. Sensors 2021, 21, 1–7. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Hessler, D.; Ruedy, K.J.; Beck, R.W. The impact of continuous glucose monitoring on markers of quality of life in adults with type 1 diabetes: Further findings from the DIAMOND randomized clinical trial. Diabetes Care 2017, 40, 736–741. [Google Scholar] [CrossRef]
- Forlenza, G.P.; Messer, L.H.; Berget, C.; Wadwa, R.P.; Driscoll, K.A. Biopsychosocial Factors Associated With Satisfaction and Sustained Use of Artificial Pancreas Technology and Its Components: a Call to the Technology Field. Curr. Diab. Rep. 2018, 18, 114. [Google Scholar] [CrossRef]
- Weissberg-Benchell, J.; Hessler, D.; Polonsky, W.H.; Fisher, L. Psychosocial Impact of the Bionic Pancreas during Summer Camp. J. Diabetes Sci. Technol. 2016, 10, 840–844. [Google Scholar]
- Vidal Florc, M.; Jansà Morató, M.; Galindo Rubio, M.; Penalba Martínez, M. Factors associated to adherence to blood glucose self-monitoring in patients with diabetes treated with insulin. The dapa study. Endocrinol. Diabetes y Nutr. 2018, 65, 99–106. [Google Scholar]
- Gómez-Peralta, F.; Menéndez, E.; Conde, S.; Conget, I.; Novials, A. Clinical characteristics and management of type 1 diabetes in Spain. The SED1 study. Endocrinol. Diabetes y Nutr. 2021, 68, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Spaans, E.A.J.M.; Kleefstra, N.; Groenier, K.H.; Bilo, H.J.G.; Brand, P.L.P. Adherence to insulin pump treatment declines with increasing age in adolescents with type 1 diabetes mellitus. Acta Paediatr. Int. J. Paediatr. 2020, 109. [Google Scholar] [CrossRef] [PubMed]
- Giani, E.; Snelgrove, R.; Volkening, L.K.; Laffel, L.M. Continuous Glucose Monitoring (CGM) Adherence in Youth with Type 1 Diabetes: Associations with Biomedical and Psychosocial Variables. J. Diabetes Sci. Technol. 2017, 11, 476–483. [Google Scholar] [CrossRef]
- Trandafir, L.M.; Moisa, S.M.; Vlaiculescu, M.V.; Butnariu, L.I.; Boca, L.O.; Constantin, M.M.L.; Lupu, P.M.; Brinza, C.; Temneanu, O.R.; Burlacu, A. Insulin Pump Therapy Efficacy and Key Factors Influencing Adherence in Pediatric Population-A Narrative Review. Medicina (Kaunas). 2022, 58, 1671. [Google Scholar] [CrossRef]
- De Bock, M.; Cooper, M.; Retterath, A.; Nicholas, J.; Ly, T.; Jones, T.; Davis, E. Continuous Glucose Monitoring Adherence: Lessons from a Clinical Trial to Predict Outpatient Behavior. J. Diabetes Sci. Technol. 2016, 10, 627–632. [Google Scholar] [CrossRef]
- Tanenbaum, M.L.; Adams, R.N.; Hanes, S.J.; Barley, R.C.; Miller, K.M.; Mulvaney, S.A.; Hood, K.K. Optimal Use of Diabetes Devices: Clinician Perspectives on Barriers and Adherence to Device Use. J. Diabetes Sci. Technol. 2017, 11, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A. IDF21-0043 Technology Trio: Continuous Glucose Monitoring, Telehealth, and Electronic Messaging for Insulin-Treated Patients. Diabetes Res. Clin. Pract. 2022, 186, 109605. [Google Scholar] [CrossRef]
- Duke, D.C.; Barry, S.; Wagner, D. V.; Speight, J.; Choudhary, P.; Harris, M.A. Distal technologies and type 1 diabetes management. Lancet Diabetes Endocrinol. 2018, 6, 143–156. [Google Scholar] [CrossRef]
- Moon, S.J.; Jung, I.; Park, C.Y. Current advances of artificial pancreas systems: A comprehensive review of the clinical evidence. Diabetes Metab. J. 2021, 45, 813–839. [Google Scholar]
- Yu, S.; Varughese, B.; Li, Z.; Kushner, P.R. Healthcare resource waste associated with patient nonadherence and early discontinuation of traditional continuous glucose monitoring in real-world settings: A multicountry analysis. Diabetes Technol. Ther. 2018, 20, 420–424. [Google Scholar] [PubMed]
- Ravaine, V.; Ancla, C.; Catargi, B. Chemically controlled closed-loop insulin delivery. J. Control. Release 2008, 132, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Volpatti, L.R.; Matranga, M.A.; Cortinas, A.B.; Delcassian, D.; Daniel, K.B.; Langer, R.; Anderson, D.G. Glucose-Responsive Nanoparticles for Rapid and Extended Self-Regulated Insulin Delivery. ACS Nano 2020, 14, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.; He, J.; Bai, M.; Huang, C.; Wang, K.; Zhang, H.; Yang, S.M.; Zhang, W. Engineering synthetic artificial pancreas using chitosan hydrogels integrated with glucose-responsive microspheres for insulin delivery. Mater. Sci. Eng. C 2019, 96, 374–382. [Google Scholar] [CrossRef]
- Wang, X. Bioartificial Organ Manufacturing Technologies. Cell Transplant. 2019, 28, 5–17. [Google Scholar]
- Parvaneh, S.; Kemény, L.; Ghaffarinia, A.; Yarani, R.; Veréb, Z. Three-dimensional bioprinting of functional β-islet-like constructs. Int. J. Bioprinting 2022, 9, 256–279. [Google Scholar] [CrossRef]
Figure 1.
Diabetes distress, a schematic presentation; adapted from [52,54].

Figure 2.
Overview of the modern non-invasive CGM approaches for intensive insulin therapy, adapted from [82].
Figure 2.
Overview of the modern non-invasive CGM approaches for intensive insulin therapy, adapted from [82].
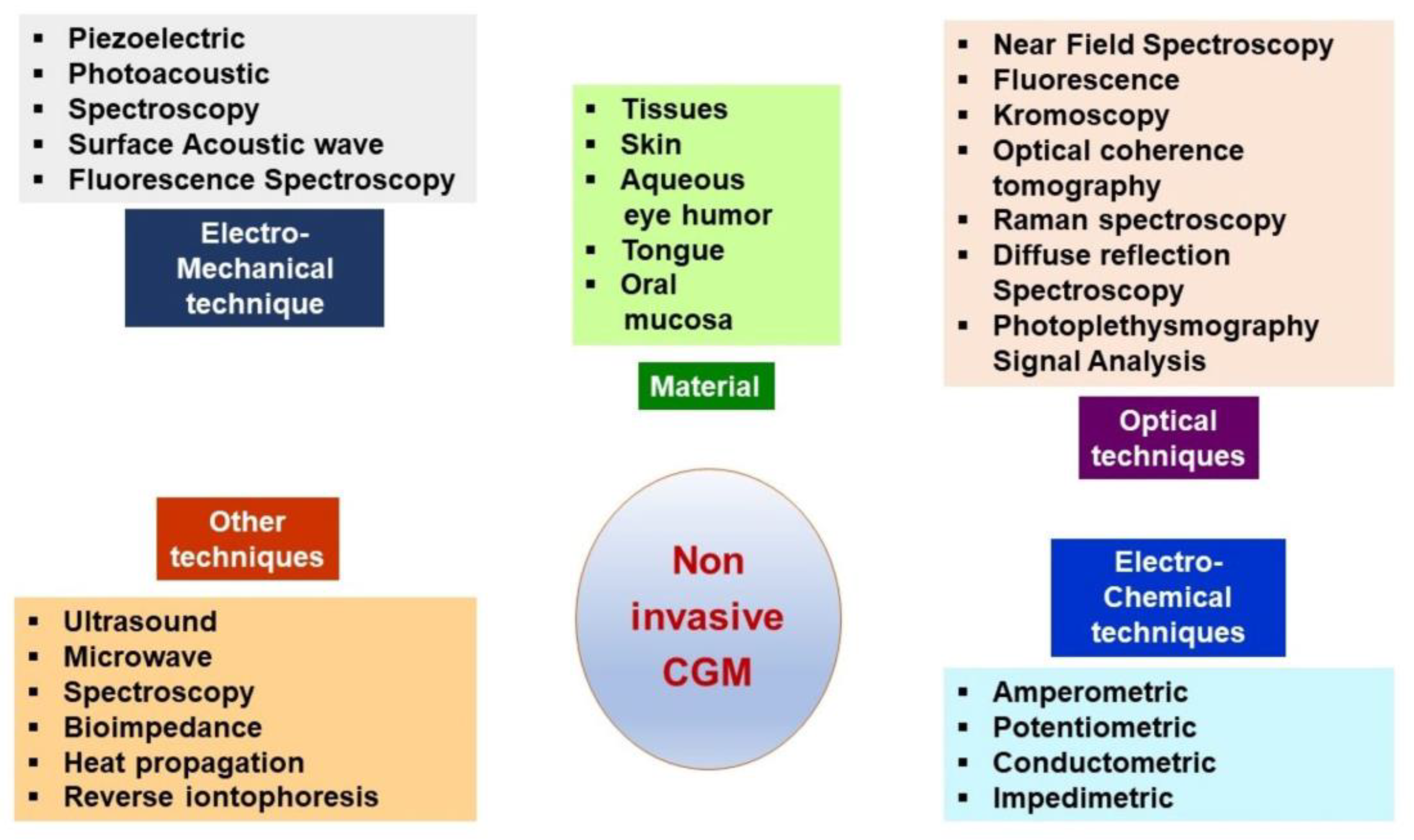
Figure 3.
V-Go - a 24 h wearable insulin PP, reproduction with permission from [107].
Figure 3.
V-Go - a 24 h wearable insulin PP, reproduction with permission from [107].
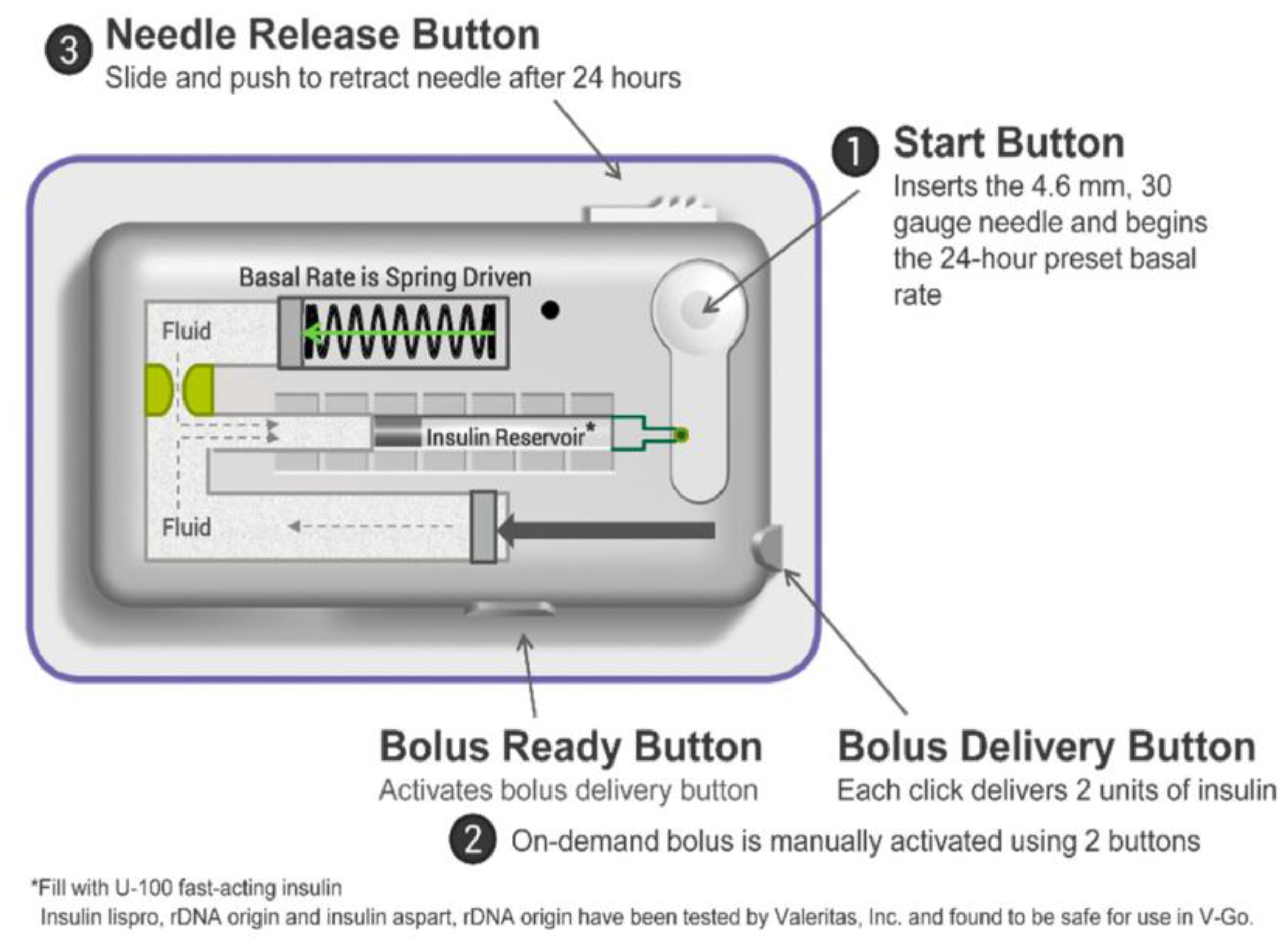
Figure 4.
A. Closed-loop glycemic management system using the ’Sense and Act’ method for optimal insulin delivery; a reproduction with permission from [117]; B. Schematic representation of closed-loop insulin delivery, adapted from [116]. A CGM wirelessly transmits the information related to interstitial glucose concentration (to a smartphone/insulin pump); the algorithm translates the received data and calculates the appropriate amount of insulin. Then, a rapid-acting insulin analog is delivered by an insulin pump. Insulin infusion is regulated in real time by the control algorithm. CSII—continuous subcutaneous insulin infusion; ISF—interstitial fluid.
Figure 4.
A. Closed-loop glycemic management system using the ’Sense and Act’ method for optimal insulin delivery; a reproduction with permission from [117]; B. Schematic representation of closed-loop insulin delivery, adapted from [116]. A CGM wirelessly transmits the information related to interstitial glucose concentration (to a smartphone/insulin pump); the algorithm translates the received data and calculates the appropriate amount of insulin. Then, a rapid-acting insulin analog is delivered by an insulin pump. Insulin infusion is regulated in real time by the control algorithm. CSII—continuous subcutaneous insulin infusion; ISF—interstitial fluid.
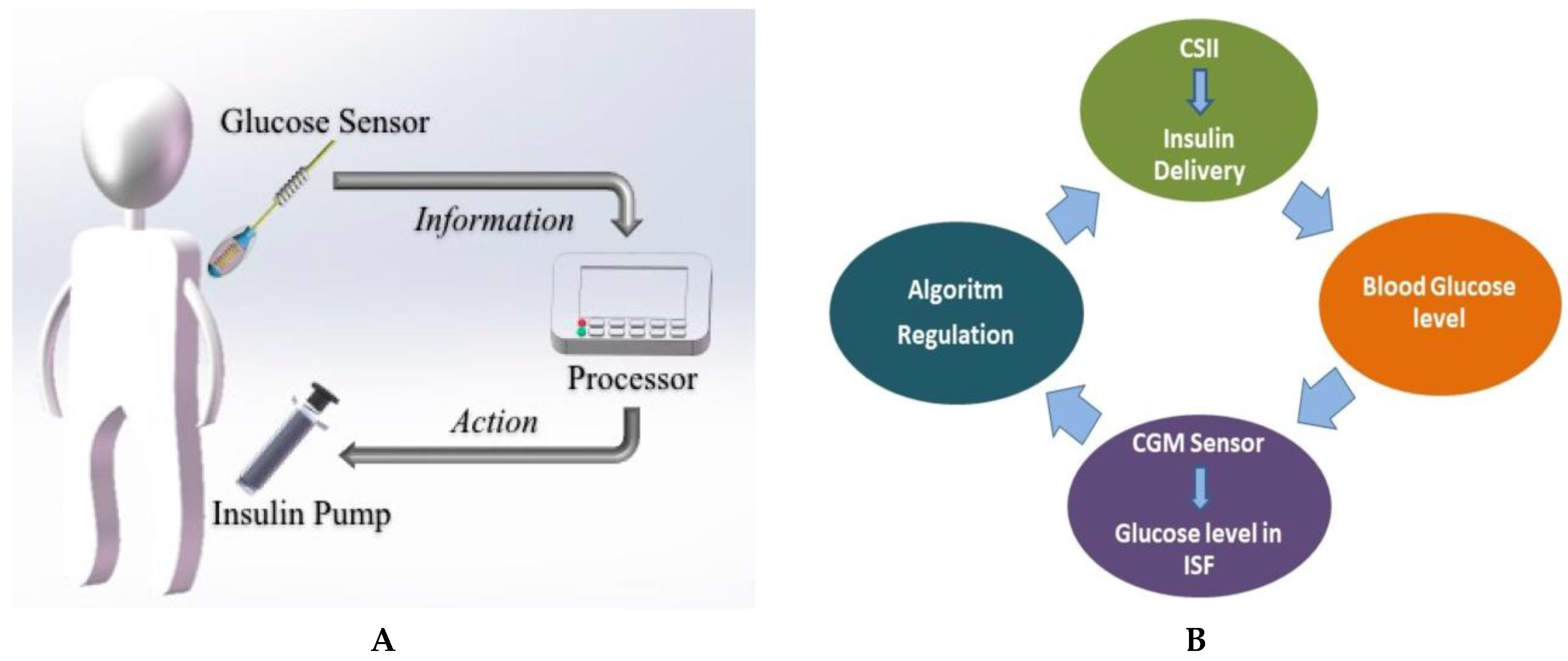
Figure 5.
Control systems’ principles applied to glycemic control; a reproduction with permission from [118].
Figure 5.
Control systems’ principles applied to glycemic control; a reproduction with permission from [118].
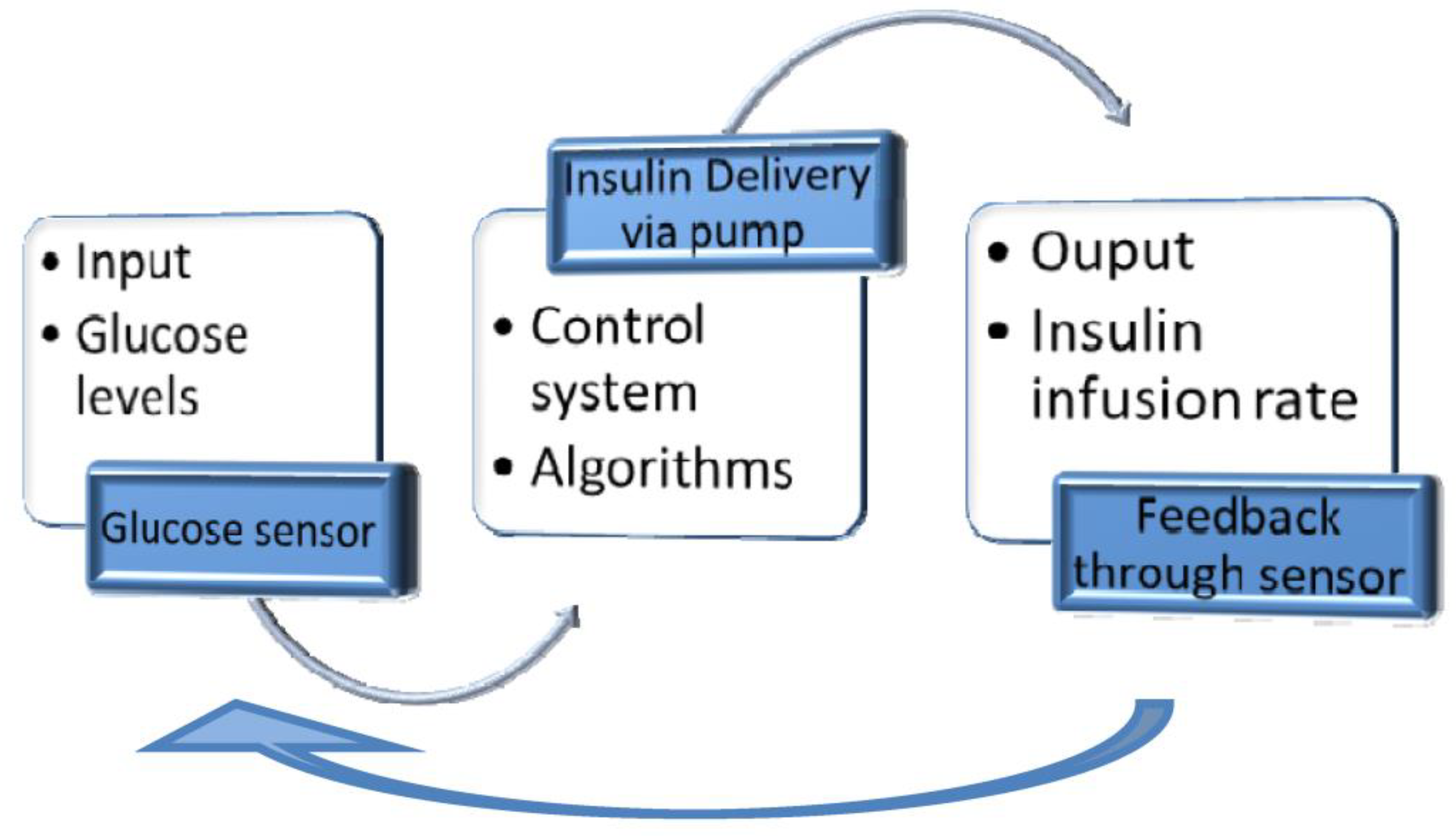
Figure 6.
The principal sources of diabetes distress in T1DM adults, adapted from [137].
Figure 6.
The principal sources of diabetes distress in T1DM adults, adapted from [137].

Figure 8.
Factors negatively impacting insulin pump adherence in pediatric patients, adapted from [156], reproduction with permission.
Figure 8.
Factors negatively impacting insulin pump adherence in pediatric patients, adapted from [156], reproduction with permission.
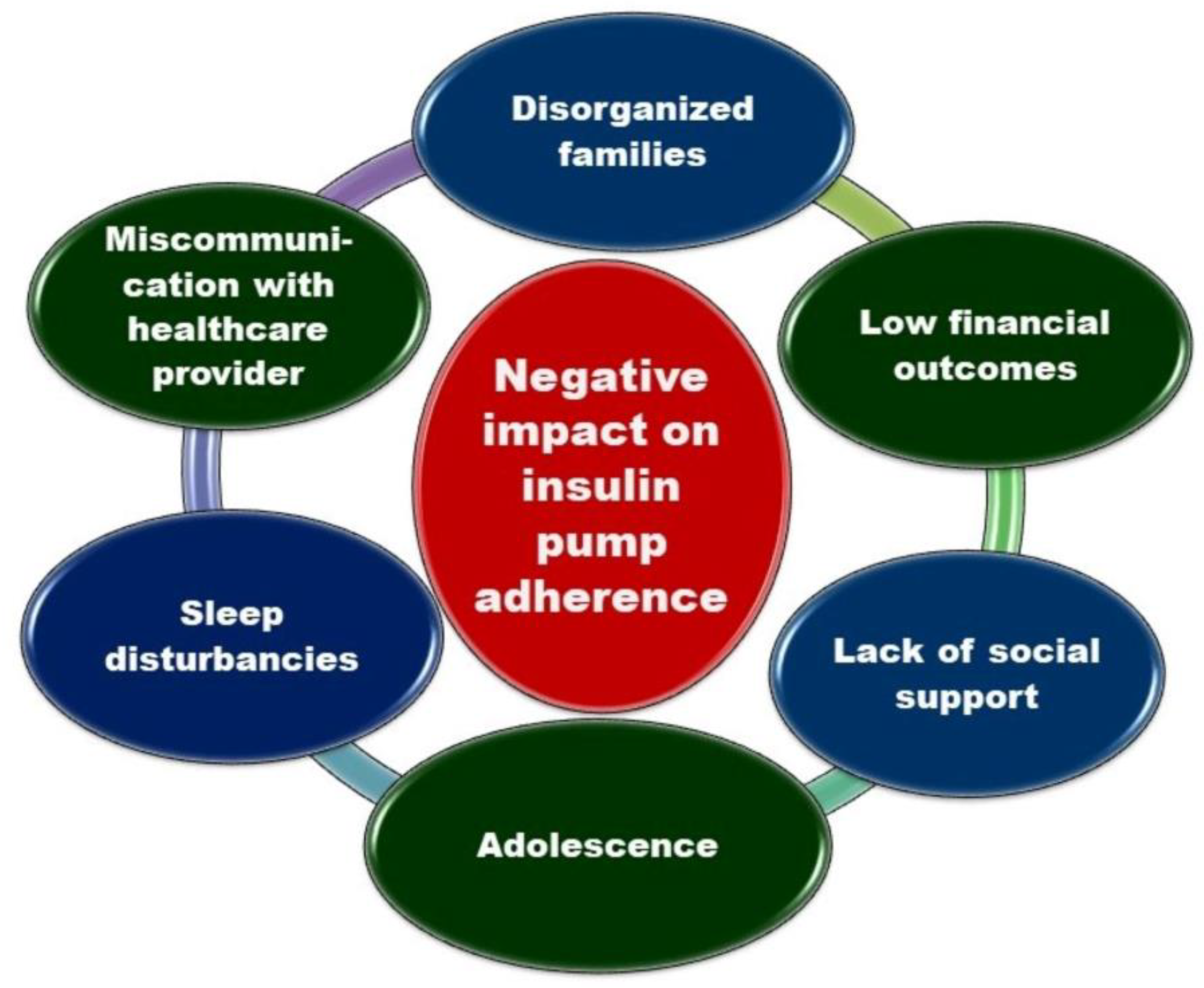
| Characteristics | Dexcom G6 | Guardian 3 | Libre 2 | Eversense E3 |
|---|---|---|---|---|
| Manufacturer [77] | DexCom, Inc, San Diego, California, USA | Medtronic, Minneapolis, Minnesota, USA |
Abbott Laboratories, Chicago, Illinois, USA |
Senseonics Holdings, Maryland, USA |
| FDA Approval [77] | March 2018 | September 2016 | September 2017 | February 2022 |
| Users [77] | Adults and children over 2 years | Adults and children over 7 years | Adults and children over 4 years | Adults over 18 years |
| Days of Sensor Wear (RT) [77] | 10 | 7 | 14 | 180 |
| Sensing molecule [77] |
Glucose-oxidase | Glucose-oxidase | Glucose-oxidase | Boronic-acid derivative |
| Technique Category [77] |
Electrochemical | Electrochemical | Electrochemical | Optique |
| Components [77] | Sensor, transmitter, app | Sensor, Transmitter, app |
Sensor, reader |
Sensor, Transmitter, app, insertion tool |
| Sensor size [77] | Unavailable | 9.5 mm long | Height: 5 mmDiameter: 35 mm | 15 mm long |
| Approved areas of sure [77] | 2-13 years - abdomen and buttocks over 14 years – abdomen and arm |
Abdomen, buttocks, and upper arm |
Back of upper arm |
Upper arm |
| Accuracy (MARD%) [77] |
9% | 10.55% | 9.7% | 8.5% |
| Daily calibration Frequency [77] |
0 (factory calibration) |
2-4 | 0 (factory calibration) |
2 (at 12 h) |
| Integration with an insulin pump [77] | Tandem t:slim Control-IQ (and older Basal-IQ) | Medtronic MiniMed 740G, 780G etc. | No | No |
| Cost [92] | - Transmitter: $300 / 3 months. - Sensors: $420 for 1 month supply. - Receiver: $380 (it is unnecessary if the patient uses a smartphone application). |
- Rechargeable Transmitter: $1100 (12 months warranty, or longer). - Sensors: $450 for a set with 5 sensors (35-day supply). |
- Sensors: $135 for 1 month (28 days supply). - Reader: $175 (it is not necessary if the patient has a smartphone application). |
- $1400 for the Sensor, Transmitter, and supplies, - In addition, the price of insertion in the doctor’s office. - Limited time Eversense Bridge program globally diminishes the price to $99 plus insertion’s cost. |
| Smartphone integration [92] | Android, iOs, Apple Watch |
Android, iOs |
Android, iOs |
Android, iOs, Apple Watch |
| Data-sharing [92] |
≤ 10 people | ≤ 4 people | ≤ 20 people | ≤ 5 people |
| A separate receiver is available [92] | Yes | No | Yes | No |
| Water Resistance [92] | 2.75 m, ≥ 24 hours | 2.5 m, 10 min | 1 m, 30 min | 1 m, 30 min |
| Skin complications | Yes | Yes | Yes | Yes |
MARD—mean absolute relative difference; CGM—Continuous Glucose Monitoring.
Table 3.
Benefits and limits of CSII, adapted from [105].
Table 3.
Benefits and limits of CSII, adapted from [105].
| Insulin Pump Therapy Benefits | Insulin Pump Therapy Limits |
|---|---|
| Better diabetes control. Fewer injections. |
The need to understand the functioning and proper management of the device. |
| Improved quality of life. | High costs, if not covered by the insurance company. |
| The flexibility of basal insulin delivery during the day and night. The flexibility of food intake and exercises. |
A device that should be worn on the body with tubing that can be caught on objects. |
| Diminished risk of hypoglycemia. | Skin allergies or infections. |
| Diminished risk of complications. | Multiple alerts. |
| Advantages | Limitations |
|---|---|
| The devices are tubeless, without request for an insulin infusion system | Waste of insulin when PPs are replaced |
| The needle could be automatically inserted; thus, their application could be less painful. | The infusion place is poorly visible, and regular inspection is complex. |
| The needle is not visible. More convenient than conventional pumps in numerous activities (showering, swimming, sweating or making exercises). |
The accuracy of insulin delivery of some PPs is often lower than that of conventional pumps, particularly at low basal doses. |
| Smaller and lighter than conventional pumps. PPs can be attached to various body parts and discreetly carried, offering more effortless movement. Technical properties are often specifically adapted to T1DM patients’ needs. Simple education and training are requested for their use. |
Its have a poor ecological balance due to waste from plastic material and batteries. Risk of infections. |
| Diminished price if certain PPs compared to conventional pumps. | Higher price than MDI. |
IIS—Insulin Infusion System; PP—Patch Pump; MDI—Multiday Injections.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



