
Submitted:
31 May 2023
Posted:
02 June 2023
You are already at the latest version
Abstract
Citation: Lastname, F.; Lastname, F.; Last-name, F. Title. Phar-maceuticals 2022, 15, x. https://doi.org/10.3390/xxxxx
Academic Editor: Firstname Lastname
Received: date
Accepted: date
Published: date
Publisher’s Note: MDPI stays neutral with regard to jurisdic-tional claims in pub-lished maps and insti-tutional affiliations.
Copyright: © 2023 by the authors. Submitted for possible open access publication under the terms and conditions of the Creative Commons
1Olga Gumkowska-Sroka, 2Kacper Kotyla, 3Ewa Mojs, 2Klaudia Palka, 1,2*Przemysław Kotyla
1. Department of Rheumatology and Clinical Immunology Voivodeship Hospital No5 in Sosnowiec Medical University of Silesia Katowice, Poland
2. Department of Internal Medicine Rheumatology and Clinical Immunology Medical University of Silesia Katowice , Poland
3. 3. Department of Clinical Psychology, Poznan University of Medical Sciences Poznan, Poland
*Correspondence: Prof Przemysław Kotyla Department of Internal Medicine Rheumatology and Clinical Immunology Medical University of Silesia, Katowice, Poland-
Summary
Systemic sclerosis is a connective tissue disease of unknown origin and unpredictable course, with both cutaneous and internal organ manifestations. In spite of enormous progress in rheumatology and clinical immunology, the background of diseases is largely unknown and no specific therapy exists.
The therapeutic approach to the disease is aimed to treat and preserve the function of internal organs, and this approach is commonly referred to as an organ-based treatment. However, in modern times data from the other branches of medicine may help to treat disease-related complications, making it possible to find a group of drugs to be utilized in the treatment of the disease. In this review, we present possible therapeutic options aiming to stop the progression of fibrotic processes, restore aberrant immune response, stop improper signalling from proinflammatory cytokines, and halt the production of disease-related autoantibodies.
Keywords:
Systemic sclerosis
; treatment
; Janus kinase inhibitors
; fibrosis
; anti-cytokine treatment
Introduction
Systemic sclerosis (SSc) is a connective tissue disease of autoimmune background characterized by dysregulation of immune response, manifested as altered T- and B-lymphocyte function, autoantibody synthesis, and vascular bed damage, leading to peripheral tissue hypoxia and massive tissue fibrosis [1]. As the result patients with systemic sclerosis experience progressive endothelial injury with abundant collagen deposition in the skin and internal organs resulting in terminal organ dysfunction. With a prevalence of 7.2–33.9 and 13.5–44.3 per 100,000 individuals in Europe and North America, respectively and annual incidence of 0.6-5,6 per 100000 individuals, SSc is recognized as a rare disease [2]. The disease is characterized by high clinical heterogeneity varying from no skin lesions (scleroderma sine scleroderma) to massive skin involvement ( generalized systemic sclerosis). Several subtypes of disease have been described. The most common classification is one proposed by Le Roy who distinguished generalized and limited subsets o systemic sclerosis on the base of skin involvement. In limited systemic sclerosis, ski fibrosis is restricted to hands, face, and feet. In contrast, in the generalized form skin sclerosis extending proximal to elbows and knees is seen and may involve truncal areas [3].
The cause of the disease is still a topic of debate among scientists, with many potential mechanisms being suggested. Patients with systemic sclerosis (SSc) almost universally have antinuclear antibodies in their blood, along with specific autoantibodies based on the type of disease subset [4]. This autoantibody presence is observed in 95% of cases at the initial diagnosis [5], which is used to assess preclinical stages of the disease known as VEDOSS (very early diagnosis of SSc). ANA positivity is one of three red flags, along with puffy fingers and Raynaud phenomenon [6]. The disease has two major subtypes based on the extent of skin involvement, as well as other types such as CREST syndrome, overlap syndrome, and systemic sclerosis without skin involvement.
First attempts to systematically assess the utility of dozens of various compounds for SSc treatment started in the 1960s. Since that time it was apparent that currently no specific drug able to halt disease progression exists. Therefore special emphasis was put on treating scleroderma-related internal organ involvement and this philosophy is currently used for the treatment. The organ-based treatment is aimed to stop the progression of internal organ damage and preserve their function.
EULAR recommendation for treatment patients with SSc
EULAR recommendations for treatment of systemic sclerosis published in 2017 address the therapeutic approaches in several SSc-related organ complications such as vascular disease (Raynaud's phenomenon, digital ulcers ) pulmonary arterial hypertension (PAH), skin fibrosis, interstitial lung disease, scleroderma renal crisis and gastrointestinal involvement. However, an unmet need remains to identify a systemic treatment that may at least partially stop the progression of the disease [7]. Decades after being promised progress was on the way, SSc researches started taking tangible steps towards testing findings from laboratory studies in clinical settings. Based on the advances in rheumatology and clinical immunology the therapeutic approaches may be focused on several areas of activity aimed to reduce the disease activity as a whole not solely preventing only one cells line damage.
Reduction /halting the activity of fibrotic processes
Restoration of the proper functioning of immunocompetent cells
Targeting the specific cytokines
Reduction of antibody synthesis
Skin and visceral organ fibrosis
Fibrosis of skin and internal organs is a hallmark of systemic sclerosis. The precise mechanism leading to uncontrolled fibrosis is only partially understood and many theories exist. However, none of them are universal and satisfactorily explain all phenomena occurring in the course of the disease. At the current level of understanding, the fibrotic process is the direct result of aberrant immunocompetent cell function, however, this process is directly mediated by several “fibrotic messengers“ and cytokines activating a plethora of profibrotic pathways.
There are several fibrogenic factors, among them platelet-derived growth factor (PDGF), tumour necrosis factor-α (TNF-α), and transforming growth factor-beta (TGF-β) which are believed to be the most important ones.
TGF-β is a pleiotropic cytokine involved in promoting wound repair and suppressing inflammation. Having potent profibrotic properties TGF-β activity is linked with several fibrosis -related disorders as pulmonary fibrosis, glomerulosclerosis, renal interstitial fibrosis, cirrhosis, Crohn's disease, cardiomyopathy, scleroderma, and chronic graft-vs-host disease [8,9]. TGF-β exists in three isoforms: TGF-β1, TGF-β2, and TGF-β3. They share a similar biologically active region and use the same type I and type II TGF-β receptor complex for signalling. The most abundant isoform seen in humans is TGF-β1 expressed by most human cells. However, it seems that the main source of TGF is platelets, which have a moderate concentration of TGF but are present in the blood in high numbers [10]. TGF-β exerts a potent stimulatory effect on fibroblasts and matrix synthesis thus it is commonly recognized as a pivotal cytokine responsible for driving the fibrotic process [11]. After binding the ligand to the TGF receptor which is formed by type II receptors homodimer (TbRII, ACTRII,AMHRII or BMPRII) coupled with type I receptor (Aktivin -like kinase 1-7) and stabilized by co-receptor (also known as type III receptor -Betaglycan and Endoglin) phosphorylation of SMAD molecules occurs leading directly to the activation of the SMAD4 molecule which translocates to the nucleus and regulates the expression of targeted genes. Apart from this canonical way of signalling, TGF-β can activate several mitogen activated protein pathways such as c-Jun N terminal kinase (JNK) and extracellular signal-regulated kinase (ERK) with subsequent activation of Ras, Raf, ERK and mitogen-activated protein kinase 1/2 which eventually activate SMAD and transcription factors in the nucleus. This leads to many pathophysiological consequences. As established recently, there is a close association between GF-β /Ras-ERK1/2 signalling and activation of the second main player in SSc pathogenesis namely endothelin -1 (ET-1). The role of TGF-β was intensively studied in various SSc models. At the current level of knowledge it is speculated that TGF acts locally rather than systemically. A recent study in patients with SSc showed that all three isoforms of TGF-β were present in lower concentrations in SSc patients than in healthy subjects, but the cytokine was shown to be hyperexpressed in dermal fibroblasts [9]. On the other hand TGF-β is a potent stimulator of epithelial-mesenchymal transition in vitro [12]. Several key questions remain open. How will these findings translate to the development of novel therapeutic strategies? Is TGF blockade a proper way to stop fibrosis? How can it be realized?
Reduction of TBF beta signalling can be realized by modulation of at least four ways of TGF beta activity.
Blocking TGF synthesis
Blocking ligand
Blocking latent activation
Blocking intracellular signalling
Several studies addressed those pathways in in-vitro and preclinical studies with promising results. A topical application of a peptide inhibitor of TGFβ1(P144) in a mouse model of systemic sclerosis revealed the remarkable suppression of connective tissue growth factor expression, fibroblast SMAD2/3 phosphorylation, and α-smooth muscle actin positive myofibroblast development [13]. Recently in the similar animal model LG283, a curcumin derivate, suppressed fibrosis in mice as well as in cultured human fibroblasts antagonizing TGF-β/SMAD3 pathway [14]. Parallel to this a Chinese group addressed the potential of Iguratimod (T-614), a novel DMARD currently tested in rheumatoid arthritis in China and Japan [15,16]. According to the results obtained from the study Iguratimod negatively regulated the TGF-β1/Smad pathway and inhibited TGF-β1-induced dermal fibroblast proliferation [17]. Another therapeutic approach has recently been proposed by Jiang et al. They tested polyporus polysaccharide (PPS) Chinese herb derivates on the TGF-β1/ Smad2/3 pathway. They showed that PPS exerts potent antifibrotic effects by inhibiting fibroblast-to-myofibroblast transition, halting ECM deposition, and modulating lung fibroblast proliferation and migration [18]. Unfortunately, these promising results have not been fully confirmed in human studies.
The first study testing recombinant human anti-transforming growth factor β1 antibody in patients with systemic sclerosis completed in 2007 did not show evidence of efficacy [19]. More promising data came from the study of Rice et al, which showed that fresolimumab, a high-affinity neutralizing antibody targeting all 3 TGF-β isoforms significantly improved skin disease with concomitant reduction of dermal myofibroblast infiltration and lowering the expression of genes thrombospondin-1 (THBS1), a biomarker of SSc skin disease highly upregulated by TGF-β Figure 1.
TGF-β is believed to play a key role in driving the fibrotic process in systemic sclerosis. Amelioration of its activity may translate to the halting of fibrotic process in the disease. It can be realized by the use of P144 which is able to block the interaction of TGF-β with its membrane receptors, or blocking the TGF molecule (fresolimumab) With the use of Iguratimod the blockade of SMAD activation can be achieved. Direct activation of targeted genes in the nucleus can be stopped by interuption of SMAD signalling with the use of novel molecules as LG283 or PP5
Immunocompetent cells in systemic sclerosis
B cells in systemic sclerosis
The role of B cells in the pathogenesis of autoimmune diseases has been conclusively confirmed. In systemic sclerosis dysregulation of the immune system and breaking the tolerance towards nuclear antigens is currently recognized as a hallmark of the disease [21]. The role of B cells is not however restricted to the production of scleroderma-related antibodies [22]. B cells are a rich source of potent proinflammatory cytokines, they may act as antigen presenting cells, co-stimulate T cells and synthesize profibrotic agents [23]. Thus targeting the B cell population seems to be a reasonable therapeutic approach [24].
With many therapeutic approaches targeting B cells anti-CD20, therapies targeting of specific B cell populations (anti-CD38, anti-CD22), modulation of intracellular B cell signalling pathways, co-stimulation blockade (anti-CD40), targeting of B cell survival factors (anti-BAFF), or more recently introduced cellular immunotherapy approaches (anti-CD19 CAR T cells) attract the special attention [24].
Rituximab (RTX), a chimeric anti-CD20 monoclonal antibody is one of the best studied therapeutic compound in systemic sclerosis. It targets the CD20 molecule expressed on cells of pre-B to pre-plasma cell stages. As the result treatment with RTX results in long lasting therapeutic effect. The role of RTX in the treatment for SSc has been reported in two small randomized controlled trials, in 16 patients versus placebo and in 60 patients versus cyclophosphamide with early SSc duration(<2 years). They showed improvement in FVC and reduction mRSS in the RTX group. However, these results should be interpreted with caution as the small number of patients included may be linked with statistical bias [25,26] The results from all small trials, non-controlled and controlled studies were recently summarized by Goswani et al. [27]. In their meta-analysis they showed significant improvement of lung function in systemic sclerosis related lung fibrosis. Additionally RTX was characterized by good safety profile with less infection adverse events observed in patients treated [27]. Discussing the role of anti-B cell therapy, a key question remains open, whether results from small pilot studies will be confirmed in larger phase III trials?
T cells
The second main player in the field of systemic sclerosis is the T cell. T cells have been shown to modulate and drive the development of autoimmunity, inflammatory response and fibrosis. In the course of disease, alteration of the frequencies of lymphocytes is observed suggesting the pivotal role of these cells in progression of the disease [28]. The role of T cells in a pathophysiological context in systemic sclerosis is recognized as T cells interact with B cells to produce specific autoantibodies as well as a source of potent proinflammatory cytokines [29]. T helper (Th) cells are involved both in the early and late phase of the disease. Taking into consideration the concept of Th cells polarisation toward Th1 or Th2 response is worth to note that Th1 but also Th17 related cytokines as TNFα, IFN, IL-1,IL-12, IL17 act predominantly at early stages of the disease being responsible for driving the inflammation [30]. With progression of the disease inflammation is less active and Th2 cytokines (IL-4, IL-13, IL-5, IL-6, and IL-10) become more prominent [31,32].
Modulation of T cell function may also be realized indirectly by interaction with cell-to cell signalling (co-stimulation). Essential molecules involved in this process are the inducible T cell costimulator ICOS and the CD 28 molecule that bind ICOS ligand and CD80/86 ligands respectively. Acazicolcept a double ICOS and CD28 antagonist has been tested in a mouse model of systemic sclerosis. Treatment with Acazicolcept induced a significant reduction in dermal thickness, collagen content, myofibroblast number, and immunocompetent cells number (B cells, T cells, neutrophils, and macrophages) in the Fra-2 Tg mouse model. Additionally acazicolcept treatment reduced lung fibrosis and right ventricular systolic pressure (RVSP). Moreover treatment with acazicolcept resulted in reduction of frequency of CD4+ and T effector memory cells and an increase in the percentage of CD4+ T naïve cells in spleen and lung animals treated [33].
The other therapeutic option is targeting CD30. The CD30 molecule, also known as Ki-1 or TNFRSF8, was first identified in 1982 in patients with Hodgkin (HL) lymphoma. The expression of this molecule is however not restricted to Hodgkin and Reed Stenberg cells. CD30 is expressed on a small subset of activated T and B lymphocytes, and a variety of lymphoid neoplasms, with the highest expression in classical HL and anaplastic large cell lymphoma. Subsequent studies demonstrated that CD30 expression was not uniform across all activated lymphocytes, instead being limited to subpopulations of CD4+/CD45RO+and CD8+T cells in lymph nodes and the thymic medulla. CD30 expression appears higher in CD4+ and CD8+ cells producing a Th2-type cytokines [34,35,36]. Soluble CD30 molecule has been found in high concentrations in sera of patients with systemic sclerosis that indirectly suggests the pathogenic role of this molecule and in wider context the Th2 response in the development of the disease [37,38,39,40,41,42]. At the moment two clinical trials are ongoing to test the safety and efficacy of Brentuximab vedotin (BV), a CD30-directed antibody-drug conjugate, which is already approved by US FDA for treatment of classic Hodgkin lymphoma (cHL). The first results in patients with SSc will be available in 2023 (NCT03222492 and NTC03198689).
Full activation of T cells is a multi-step process that requires not only the recognition of antigens by T cells but, also a second co-stimulatory signal, provided by binding of the CD28 receptor on T cells to CD80 and/or CD86 molecules on the surface of antigen-presenting cells. [43]. At the time of T cell activation the CD4 cell may express a regulatory molecule namely CD152 or Cytotoxic T lymphocyte-associated protein-4 (CTLA-4), an inhibitory receptor expressed constitutively on CD4+CD25+ T regulatory lymphocytes (Treg) and transiently on activated CD4+ and CD8+ T lymphocytes. With very high affinity to CD28 (150 times more than CD80/86), CD152 is able to halt activation of T cells preventing an uncontrolled immune response [44]. That was a theoretical background for synthesis and introduction of the fusion protein composed from a soluble form of the extracellular domain of CTLA-4 linked to immunoglobulin G1Fc part (Abatacept, Orencia) [45]. It showed its safety and efficacy in rheumatoid arthritis and is still intensively tested in various autoimmune diseases [46,47,48,49,50,51,52,53]. In systemic sclerosis, which is characterised by a pivotal role of T cell orchestrating immune response [54] blocking the T cell activation seems to be a reasonable approach. Indeed, data from a small retrospective multicentre study with 27 patients showed the potential utility of abatacept in the treatment of systemic sclerosis, where reduction of skin involvement as well as improvement in tender and swollen join count were observed [55]. Following these promising data the ASSET trial (A Study of Subcutaneous Abatacept to Treat Diffuse Cutaneous Systemic Sclerosis), which is a phase 2, double-blind, placebo-controlled trial of weekly subcutaneous abatacept over 12 months in patients with early diffuse cutaneous systemic sclerosis (≤36 months of disease) has been started .The ASSET trial showed only moderate (statistically non-significant) improvement with abatacept in the primary endpoint of mean change from baseline to month 12 in skin score [56]. An open label extension phase of this study confirmed the good safety profile of abatacept, however again the primary endpoint of change in mRSS has not been reached [57]. In spite of not reaching a significant improvement in skin score abatacept remains a potential candidate as a disease modifying drug in systemic sclerosis and more trials are needed to confirm the role of this drug in the treatment of the disease.
Targeting the specific cytokines
Skin fibrosis, vasculopathy and inflammation are three crucial elements of disease background. Each process is precisely orchestrated by cytokines, and chemokines activity, thus the rationale approach is to block or (rarely) enhance function of a given cytokine. Among many cytokines already identified only few of them participate in the beginning and the progression of SSc.Keeping in mind many limitations of pure categorisation of autoimmune diseases as Th1 or Th2 dependent condition. SSc may be categorised as at least partially,Th2 dependent disease with the prominent Th2 immune response and the subsequent release of Th2-dependent cytokines such as IL-4, IL-5, and IL-13, which are able to control the fibrotic process [58].
In the early stages of scleroderma however, Th1 cells and Th17 cells are suggested to dominate the immune profile [59] later shifting to Th2 [60] and this may explain why patients with SSc are characterized by overexpression of IFNα at the early stages of the disease, which than translates to the disease’s development [61,62]. It shows clearly that both arms of the immune response – cellular and humoral are involved into pathogenesis of SSc however their role depends on the stage of the disease. This may bring several therapeutic consequences suggesting that direct therapeutic targeting of a cytokine should be done in the proper phase of the disease.
Several studies have shown that IL-4, a typical representative of Th2 dependent response plays an important role as a profibrotic cytokine that stimulates collagen synthesis by fibroblasts. This was proven in laboratory studies where IL-4 stimulated human dermal fibroblasts to synthesize types I and III collagen and fibronectin [63,64]. High levels of IL-4 were reported in patients with systemic sclerosis, where it plays a pathogenetic role inducing the formation of the extracellular matrix [65,66].
Even more studies refer to the other typical profibrotic cytokine IL-13. IL-13 has several similarities to IL-4 at the amino acid level and both cytokines display 20-30% homology [67]. Moreover they show similar biological activity since they signal through receptor heterodimers built with combinations of three possible subunits: IL-4Rα, the common gamma chain (γc), and IL-13Rα1 common receptor chain [68]. In detail, IL-4 and IL-13 share common type I cytokine receptor composed with IL-4α and gamma chain (γc) receptor alpha (IL-4Rα), coupled with the Janus kinase/signal transducer and activator of transcription protein 6 (JAK/STAT6) signaling pathway.
The other receptor, IL-13 may bind to is the IL-13Rα2. IL-13 preferentially binds to this type of the receptor with very high affinity. Binding of the cytokine however does not exert any physiological response as this type of receptor is commonly considered a “decoy” receptor as it has a short cytoplasmic tail with no recognizable signalling motifs [69]. Finally IL-4 and Il-13 may signal through type II cytokine receptor composed with IL-4Rα and Il-13Rα2. IL-4 and Il-13 are commonly recognized as leading cytokines driving the fibrotic process [70,71]. Keeping in mind that both cytokines signal through type I or type II cytokine receptor attached to protein kinases, commonly referred as Janus kinase, with subsequent activation of JAK/STAT pathway and finally to control several gene expression, resulting in cytokine synthesis and escalation of the fibrotic process [72,73]. This finding may potentially open new therapeutic approaches. Type I and II cytokines attached to Janus kinases may be simply blocked with the use of small synthetic compounds – Janus kinase inhibitors [74].With large profibrotic potential both IL-4 and IL-13 are natural targets to inhibit, aiming to ameliorate the fibrotic process [75,76]. Indeed, targeting IL-4, and IL-13 has been tested in various fibrotic diseases including systemic sclerosis [70]. The main concept of targeting IL-4/IL-13 is based on the fact that these cytokines represent a Th2 response. The reasonable approach for SSc treatment is therefore to shift the immune response toward Th1. The IL-4, IL-13signalling pathway can be stopped at various levels: (1) by ameliorating the soluble cytokine activity, (2) targeting and inhibiting their receptors on cell surfaces or (3) blocking the intracellular signalling pathways. The first approach may be easily done by simply blocking IL-4/IL-13 activity with the use of monoclonal antibodies targeting either IL-4 or IL-13 activity. Quite recently data on a randomised, double-blind, placebo-controlled, 24-week, phase II, proof-of-concept study of romilkimab (SAR156597) in early diffuse cutaneous systemic sclerosis became available. In the study romilkimab, a humanised, bispecific immunoglobulin-G4 antibody that binds and neutralises IL-4/IL-13 has been tested in patients with diffuse type of SSc. In this study romilkimab demonstrated a significant effect on the skin changes in early dsSSc [77]. However the results of the study should be interpreted cautiously as they referred to a relatively small group of patients that obviously requires confirmation in a future phase III study.
The second possibility is to block the receptor function with the use of a monoclonal antibody. As far as this approach is concerned dupilumab, a monoclonal humanized antibody targeting subunit IL-4Rα, recently commercialized for atopic dermatitis and asthma seems to be a reasonable approach [78,79]. At the moment however dupilumab has not been tested in systemic sclerosis.
The last approach is to block the signalling pathway with the use of JAK inhibitors [74]. Cytokines are small molecular weight transmitters essential in cell to cell interaction to modulate innate and acquired immune response. Based on the similar structure they are typically divided into several cytokines families. Cytokines signal via typical receptors which can be categorized into several receptor superfamilies. Cytokines interact with the extracellular domain of the receptor, which when activated can transmit the signal via long chains of transmission molecules to activate specific genes in the nucleus. Among them cytokines belonging to class I and class II receptors family utilize receptors which lack intracellular enzymatic domain and require specific kinases to fully activate the receptor and enable to transmit the signal into the nucleus [80]. The Janus kinase (JAK) family enzymes are non-receptor tyrosine kinases that phosphorylate cytokine receptors enabling them to start signalling through the JAK-STAT signalling pathway. Considering that JAK-STAT signal transduction is initiated by the binding of ligands, such as cytokines to their receptors, proper JAK activity in the JAK-STAT pathway is a key element to orchestrate immune response and dysfunctional JAKs are directly responsible for cancers, immune system-related diseases, and autoimmune disorders [81]. These enzymes referred as Janus kinases or simply JAK kinases are an essential element for the transmission of cytokine signals for such important cytokines as IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21 which transmit their signals via gamma chain receptors (γc) [82], since GM-CSF, IL-3, and IL-5 signalling is via the beta type of receptor [83]. Another class of receptor is the heterodimer composed of the gp 130 protein (or its homologue) which is responsible for signalling from IL- 6, IL-11, IL-31, IL-35, and IL-27 [84]. Finally, the class I receptor subfamily which has a common p40 subunit interacts with IL-12 and IL-23 [85]. The second group of receptors called class II receptors is responsible for transmitting signals from interferons and the IL-10 cytokine family (IL-10, IL-19, IL-20, IL-22, IL-24, and IL-26) [86].
All types of receptor utilize a combination of the four known JAK kinases (JAK1, JAK2, JAK3 and TYK2). This makes it possible to stop or at least modulate cytokine signalling by blocking JAK activity. This was a theoretical background for the development of JAK inhibitors. Contrary to the large and high molecular weight biologics targeting one specific cytokine, JAK inhibitors are small synthetic compounds easy to synthetize and handle. This group of cytokine modulators showed their safety and efficacy in several rheumatological, dermatological and haematological conditions and are intensively tested in many others including connective tissue diseases and the other autoimmune disorders [87,88,89,90,91].
The role of JAK kinase inhibition in SSc patients can be explained again in the context of the activity of the typical Th2-dependent cytokines IL-4 and IL-13, which are responsible for driving the profibrotic process in the body. It is worth noticing however, that blocking one JAK may also result in the inhibition of other potentially proinflammatory and profibrotic cytokines, so creating a strong antifibrotic milieu.
The other players in this field are the IL-12 family of cytokines. Since the disease is characterized by the activation of IL-12 cytokine family members responsible for driving the profibrotic effect, JAK inhibition signalling from IL-12 specific receptors may block IL-12, IL-23 and IL-27 thus ameliorating a significant profibrotic effect. The role of the IL-6 cytokine was already mentioned in the light of biologics (tocilizumab) tested in SSc. IL-6 activity amelioration may alternatively be blocked by JAK inhibitors. Again, with a single compound we are to block all IL-6 family members simply due to the similarities in IL-6 receptor family, where all types of IL-6 receptors are coupled with the JAK kinases.
The role of blocking a cytokine class II receptor in systemic sclerosis is less clear. From a theoretical point of view class II cytokines (IL-10 family cytokines and interferons) are able to transmit both pro and anti-inflammatory signals. In detail IL-10 is mainly produced by Bregs that was able to suppress skin fibrosis [92]. It has also been shown that IL-10–producing Bregs have been found to be reduced in patients with SSc and correlated with disease activity, suggesting the anti-inflammatory potential of IL-10 in the disease [93,94]. Less is known on the role of the other IL-10 family cytokines such as IL-20 or IL-23 in the development of systemic sclerosis. Data from the literature suggests the reduced expression of IL-20 or dysregulated IL-23 signalling [92,95]. It remains an open question whether these findings are clinically important. In line with this, it is not clear if blocking this part of cytokine signalling may benefit patients with systemic sclerosis.
The therapeutic potential of JAKi may also be explained in another way. Systemic sclerosis is characterized by overexpression of interferon type 1 [61,96,97]. This pathophysiological phenomenon commonly referred to as an interferon signature is characterized by overexpression of several proinflammatory – Interferon- related genes. Type 1 of interferons comprises a group of five classes of interferons namely: α, β, ω, ε and κ. All types of INT T1 classes signal through the same type 1 IFN heterodimeric receptor complex coupled with the JAK kinases. This brings novel therapeutic possibilities as blocking JAK with its inhibitor can block the whole interferons’ signalling. Blocking the interferon signalling seems to be relatively safe. According to a phase I study, administration of MEDI-546, ahuman immunoglobulin G1 kappa monoclonal antibody directed against IFNAR1, resulted in sustained inhibition of the type I IFN gene signature [98]. Followed this promising results the study with Anifrolumab (anti-IFNAR1 monoclonal antibody) showed the reduced suppression of the IFN signature and TGFβ signalling in SSc skin [99]. This shows that blocking the IFN receptor might be a promising way to reduce disease activity in subjects with SSc or other IFN-related inflammatory diseases. Whether this finding translates to the inhibition of IFN signalling via JAK inhibitors should be elucidated.
Recent analysis of case reports and small uncontrolled trials showed the clinical benefit of JAK inhibitors in interstitial lung diseases associated with SSc. Keeping in mind many limitations from these studies, the results may indicate that targeting several cytokines with one drug may be a promising way to halt the progression of fibrosis and inflammation [100].
Autoantibody -targeted therapy
The prevalence of antinuclear antibodies (ANA) in SSc is almost universal as ANA can be detected in sera of more than 90% patients with the disease [29]. Among them the specific antibodies identified as anti-centromeric protein antibodies (CENP) topoisomerase I (SCl-70) and anti RNA polymerase III are commonly used for classification and prognosis staging and are linked with specific organ involvement [101].
Other targets for autoantibodies in SSc are endothelial cells, vascular smooth cells and fibroblasts. Interaction between specific autoantibodies and the targeted group of cells results in activation, damage, and expression of a pro fibrotic and pro adhesive phenotype [102,103]. Indeed, specific autoantibodies have been identified and their activity was likened to a pathogenic process such as myofibroblasts transformation and direct endothelial damage that leads to vascular injury [104,105,106,107].
Presence of antinuclear and more general autoantibodies is a hallmark of the disease linked pathogenetically with disease subtype course and prognosis. Therefore therapeutic strategies aimed to reduce the generation of autoantibodies ( currently tested in the other autoimmune diseases) seem to be reasonable approaches in the treatment of SSc.
The first choice to reduce autoantibody formation is to target a source of antibodies- B cell. This approach was addressed in detail in the chapter on role of B cells in systemic sclerosis.
There are however plenty of opportunities that are beyond the structure and function of B cells.
The fate and function of B cells is precisely regulated at the level of B cell regulatory factors. Among many cytokines, chemokines, and stimulatory factors affecting the structure and function of B cell, BAFF, also called B lymphocyte stimulator (BLyS), and APRIL which is a homologous factor to BAFF, are recognized as key elements to regulate B cell activity. BAFF is expressed by monocytes, macrophages, and activated T cells. BAFF can interact with three receptors, the BAFF-R, BCMA, or TACI, and regulates B cell survival, differentiation, maturation, immunoglobulin class switching, and antibody production [108] Following understanding of the function of BAFF/APRIL, a phase II study investigating the effects of belimumab and mycophenolic acid combination in 20 patients with dcSSc was performed. Unfortunately, patients who received belimumab did not benefit from an improvement in skin thickness compared to the placebo group. [109]
B cell targeting therapy is currently licensed in the treatment of RA and ANCA vasculitis but is also successfully used off-label in other immune mediated diseases [110,111,112,113]. Unfortunately most B cell depleting therapies target the CD20 molecule expressed on the surface of the majority of B cells. With the progress of B cells maturation, expression of this molecule reduces and finally CD20 is absent on the surface of the most differentiated B cell populations making impossible to reduce the fully differentiated B cell population. To overcome this, plasma cells, a main site of autoantibody synthesis, can be affected from “inside”. This strategy is currently realized with the use of proteasome inhibitors, a class of drug which is able to stop the proteasome activity that results in accumulation of defective immunoglobulin chains, misfolded proteins, overflow of the endocytoplasmatic reticulum and directly leads to plasma cell apoptosis [114,115,116].
In in-vitro studies proteasome inhibitors showed a potential towards the reduction of collagen synthesis by human fibroblasts. So far this mechanism was not confirmed in a mouse model of SSc which showed no effect on skin and lung fibrosis [117].
Data from current phase II studies assessing a combination of bortezomib, a protease inhibitor, and mycophenolate mofetil in patients with Ssc suggested that combination therapy was superior over bortezomib alone (NCT02370693).A second generation proteasome inhibitor ixazonib is about to be tested in the other trial (NCT04837131).
Bruton’s kinase inhibitors
Bruton’s tyrosine kinases (BTK) are members of the Tec kinases family of tyrosine protein kinases. TBK is a component of multiple signalling pathways and plays an important role in the B-cell receptor (BCR) signalling, the development and activation of B cells [118,119].
The idea to use BTK inhibitors in systemic sclerosis is generally based on the observation of the role of B cells (and myeloid cells) in the development of SSC [24,28]
In a murine model of systemic sclerosis BTKB66 (a new BTK inhibitor) treatment resulted in reduction of skin fibrosis, collagen deposition, and decreased inflammatory cell infiltration in the skin of animals [120]. In the other ex-vivo study testing the influence of ibrutinib a first-in-class, irreversible inhibitor of BTK was able to reduce the release of proinflammatory IL-6 and TNF-α. At the concentrations studied ibrutinib also reduced concentration of profibrotic cytokines without any significant influence on IL-1- and IFN-γ [121]
Currently 13 BTK inhibitor drug candidates are being evaluated in clinical trials (phase II or higher) in autoimmune diseases. Unfortunately, the studies started so far focused mainly on SLE, RA and multiple sclerosis [122].
Targeting CD38 molecule
The other therapeutic approach aimed to reduce concentration and formation of autoantibodies in SSc might be the targeting of plasma cells, and memory B cells. Moreover, recent data showed an elevated expression of CD38 in peripheral blood plasmablasts and plasma cells of SSc, suggesting a pathogenic role of this molecule in the development of the disease as well as suggesting CD38 as a potential molecule to target to reverse immunological abnormalities in the disease [123]. Taking into account that short-lived plasmablasts and plasma cells and long-lived plasma cells are important sources of autoantibodies generated upon activation, targeting the population of antibody producing cells might be reasonable approach [124,125,126].
Targeting the CD38 molecule may also bring other therapeutic effects in systemic sclerosis. The CD38 molecule represents NADase enzyme, a type II plasma membrane protein expressed on both immune and non-immune cells [127]. CD38 shows hydrolytic activity against nicotinamide adenine dinucleotide (NAD+) and its main role is to breakdown the NAD and reduce its level in the tissues. In the course of SSc CD38 expression is elevated and correlates with disease activity and skin involvement, thus negative modulation of CD38 function may translate to restoration of NAD+ homeostasis in fibroblasts, affect myofibroblast activation, halt profibrotic cellular signalling, supress the fibrotic gene, and restore endothelial function [128,129].
Mechanical removal of autoantibodies
This term refers to many procedures where circulating autoantibodies are mechanically removed from the blood. The most commonly used procedures are therapeutic plasma exchange, plasmapheresis rheoperesis and immunoadsorption. Data on the therapeutic potential of these procedures come from small studies and case reports, generally reporting favourable therapeutic effect on skin fibrosis, musculoskeletal symptoms, Raynaud’s phenomenon, healing of digital ulcers and organ manifestation. These techniques are reviewed in detail elsewhere [130].
Finally the other approach that has been proposed recently is epigenetic modulation of DNA methylation, histone modifications and non-coding RNAs in SSc [131]. Obviously the role of this sophisticated approach in the real world SSc clinic should be elucidated.
Conclusions
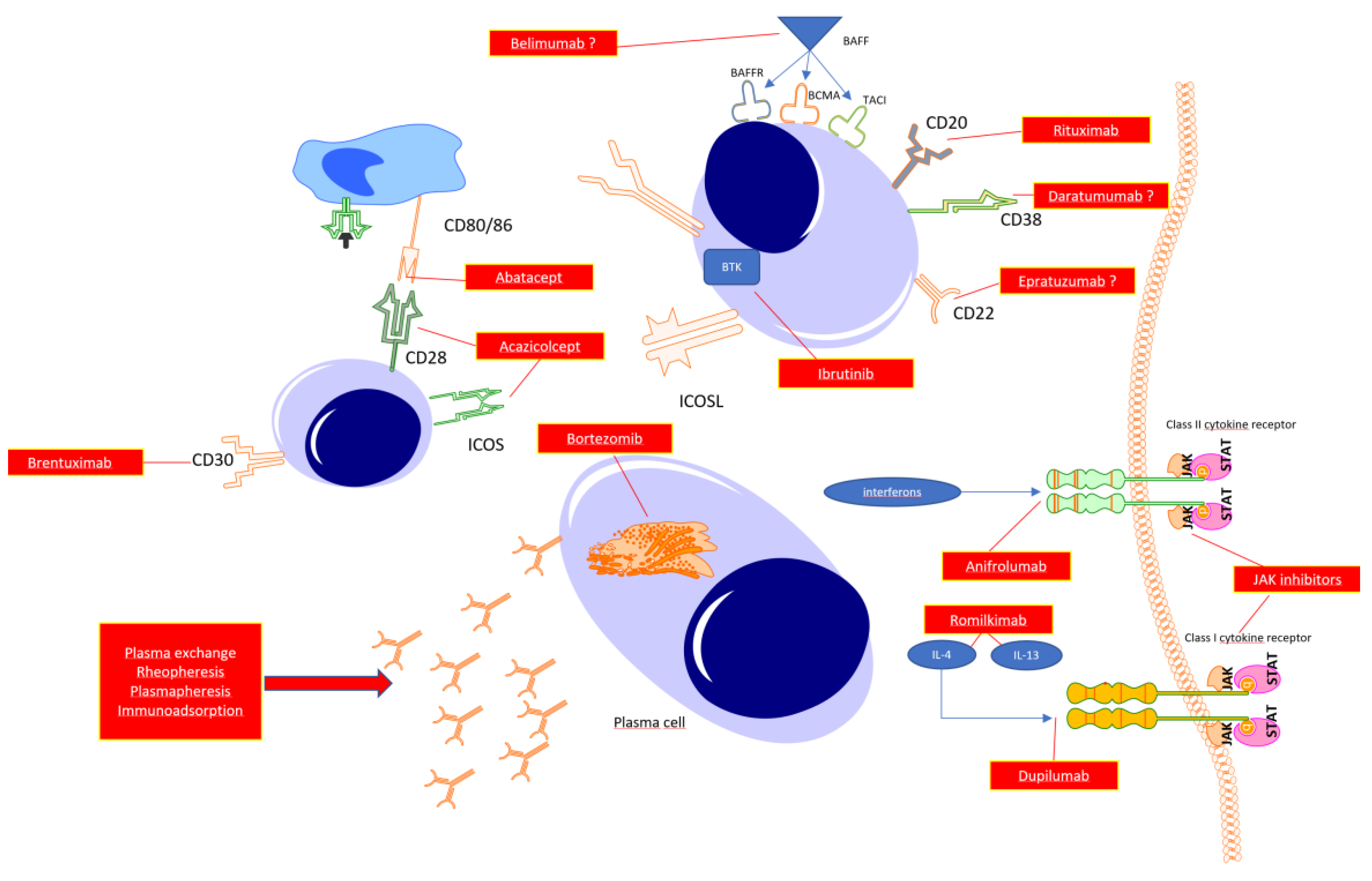
For many years SSc was a disease without any treatment, however the development of rheumatology and clinical immunology is translating to understanding the key mechanisms responsible for driving the inflammation and fibrosis in SSc. In line with this several targets for novel drugs have been proposed. Figure 2.
Abatacept Acazicolcept and Brentuximab act in the early phase of immunocompetent cell cross-talks resulting in immune tolerance or immunosuppression Targeting directly B cell function with anti-CD20 (Rituximab), antiCD22 (Epratuzumab) anti-CD38(Daratumumab) antibodies promotes B cell apoptosis, halting transformation to mature plasmablasts thus prevent autoantibody synthesis. With the use of Janus kinase inhibitors reduction of the whole spectrum of cytokine class I and class II is observed that potentially translates to halting the inflammatory response (early phase of disease) or fibrosis (late stage of the disease). The same may be achieved with the use of specific antagonists of selected cytokines or its receptors (potent profibrotic IL-4 and IL-13 or interferons),Finally targeting plasma cells with proteasome inhibitors results with reduction of autoantibody synthesis. Finally, the reduction of autoantibody levels can achieved by mechanically removing circulating antibodies with the use of total plasma exchange, rheopheresis, plasmapheresis or antibody absorption.
With the heterogeneity of pathophysiological background and clinical presentation at the moment it seems impossible to discover one drug working sufficiently in all patients with SSc. However detailed assessment of the clinical course may translate to administration of a sufficient drug. It seems to be a reasonable approach to distinguish between early (inflammation) and late phases (fibrosis) of the disease and try to match disease presentation with the required therapeutic procedure.
Author Contributions
Conceptualization P.K, K.K., O.G-S Methodology K.P, E.M., Resources P.K, O.G-S Original draft preparation P.K. O.G-S K.P, Writing-Review and Editing P.K, K.K., E.M, Visualisation K.P. K.K, Supervision O.G-S, K.K. Founding acquisition P.K.
Funding
This paper received no external funding. The APC was funded by Medical University of Silesia, Katowice, Poland.
Acknowledgments
The Authors acknowledge Dr Laura Coates University of Oxford UK for English editing the manuscript.
Conflicts of Interest
The Authors declare no conflict of interest.
References
- Rosendahl, A.-H.; Schönborn, K.; Krieg, T. Pathophysiology of systemic sclerosis (scleroderma). The Kaohsiung journal of medical sciences 2022, 38, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Bergamasco, A.; Hartmann, N.; Wallace, L.; Verpillat, P. Epidemiology of systemic sclerosis and systemic sclerosis-associated interstitial lung disease. Clinical epidemiology 2019, 11, 257–273. [Google Scholar] [CrossRef] [PubMed]
- LeRoy, E.C.; Black, C.; Fleischmajer, R.; Jablonska, S.; Krieg, T.; Medsger, T.A., Jr.; Rowell, N.; Wollheim, F. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. The Journal of rheumatology 1988, 15, 202–205. [Google Scholar] [PubMed]
- Mehra, S.; Walker, J.; Patterson, K.; Fritzler, M.J. Autoantibodies in systemic sclerosis. Autoimmunity reviews 2013, 12, 340–354. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.G.; Fritzler, M.J. Update on autoantibodies in systemic sclerosis. Current opinion in rheumatology 2007, 19, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Bellando-Randone, S.; Matucci-Cerinic, M. Very early systemic sclerosis. Best Practice & Research Clinical Rheumatology 2019, 33, 101428. [Google Scholar]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.; Cutolo, M.; Czirjak, L.; et al. Update of eular recommendations for the treatment of systemic sclerosis. Annals of the rheumatic diseases 2017, 76, 1327–1339. [Google Scholar] [CrossRef]
- Prud'homme, G.J. Pathobiology of transforming growth factor β in cancer, fibrosis and immunologic disease, and therapeutic considerations. Laboratory Investigation 2007, 87, 1077–1091. [Google Scholar] [CrossRef]
- Lomelí-Nieto, J.A.; Muñoz-Valle, J.F.; Baños-Hernández, C.J.; Navarro-Zarza, J.E.; Godínez-Rubí, J.M.; García-Arellano, S.; Ramírez-Dueñas, M.G.; Parra-Rojas, I.; Villanueva-Pérez, A.; Hernández-Bello, J. Transforming growth factor beta isoforms and tgf-βr1 and tgf-βr2 expression in systemic sclerosis patients. Clinical and experimental medicine 2022. [Google Scholar] [CrossRef]
- Grainger, D.J.; Mosedale, D.E.; Metcalfe, J.C. Tgf-β in blood: A complex problem. Cytokine & Growth Factor Reviews 2000, 11, 133–145. [Google Scholar]
- Biernacka, A.; Dobaczewski, M.; Frangogiannis, N.G. Tgf-β signaling in fibrosis. Growth factors 2011, 29, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Zavadil, J.; Böttinger, E.P. Tgf-β and epithelial-to-mesenchymal transitions. Oncogene 2005, 24, 5764–5774. [Google Scholar] [CrossRef] [PubMed]
- Santiago, B.; Gutierrez-Cañas, I.; Dotor, J.; Palao, G.; Lasarte, J.J.; Ruiz, J.; Prieto, J.; Borrás-Cuesta, F.; Pablos, J.L. Topical application of a peptide inhibitor of transforming growth factor-β1 ameliorates bleomycin-induced skin fibrosis. Journal of Investigative Dermatology 2005, 125, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Utsunomiya, A.; Chino, T.; Kasamatsu, H.; Hasegawa, T.; Utsunomiya, N.; Luong, V.H.; Matsushita, T.; Sasaki, Y.; Ogura, D.; Niwa, S.-i.; et al. The compound lg283 inhibits bleomycin-induced skin fibrosis via antagonizing tgf-β signaling. Arthritis Res Ther 2022, 24, 94. [Google Scholar] [CrossRef]
- Mu, R.; Li, C.; Li, X.; Ke, Y.; Zhao, L.; Chen, L.; Wu, R.; Wu, Z.; Zuo, X.; Xie, Y.; et al. Effectiveness and safety of iguratimod treatment in patients with active rheumatoid arthritis in chinese: A nationwide, prospective real-world study. The Lancet regional health. Western Pacific 2021, 10, 100128. [Google Scholar] [CrossRef]
- Nozaki, Y. Iguratimod: Novel molecular insights and a new csdmard for rheumatoid arthritis, from japan to the world. Life (Basel, Switzerland) 2021, 11. [Google Scholar] [CrossRef]
- Xie, X.; Gan, H.; Tian, J.; Li, F.; Chen, J.; Wang, J.; Liao, J.; Li, S. Iguratimod inhibits skin fibrosis by regulating tgf-β1/smad signalling pathway in systemic sclerosis. European journal of clinical investigation 2022, 52, e13791. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Wang, F.; Luo, A.; Lin, S.; Feng, X.; Yan, W.; Shi, Y.; Zhang, Q.; Gu, X.; Cui, G.; et al. Polyporus polysaccharide ameliorates bleomycin-induced pulmonary fibrosis by suppressing myofibroblast differentiation via tgf-β/smad2/3 pathway. Frontiers in pharmacology 2020, 11, 767. [Google Scholar] [CrossRef]
- Denton, C.P.; Merkel, P.A.; Furst, D.E.; Khanna, D.; Emery, P.; Hsu, V.M.; Silliman, N.; Streisand, J.; Powell, J.; Akesson, A.; et al. Recombinant human anti-transforming growth factor beta1 antibody therapy in systemic sclerosis: A multicenter, randomized, placebo-controlled phase i/ii trial of cat-192. Arthritis and rheumatism 2007, 56, 323–333. [Google Scholar] [CrossRef]
- Rice, L.M.; Padilla, C.M.; McLaughlin, S.R.; Mathes, A.; Ziemek, J.; Goummih, S.; Nakerakanti, S.; York, M.; Farina, G.; Whitfield, M.L.; et al. Fresolimumab treatment decreases biomarkers and improves clinical symptoms in systemic sclerosis patients. J Clin Invest 2015, 125, 2795–2807. [Google Scholar] [CrossRef]
- Sanges, S.; Guerrier, T.; Launay, D.; Lefèvre, G.; Labalette, M.; Forestier, A.; Sobanski, V.; Corli, J.; Hauspie, C.; Jendoubi, M. Role of b cells in the pathogenesis of systemic sclerosis. La Revue de médecine interne 2017, 38, 113–124. [Google Scholar] [CrossRef]
- Steen, V.D. In Autoantibodies in systemic sclerosis, Seminars in arthritis and rheumatism, 2005; Elsevier: pp 35-42.
- Liem, S.I.E.; Neppelenbroek, S.; Fehres, C.M.; Wortel, C.; Toes, R.E.M.; Huizinga, T.W.J.; Scherer, H.U.; de Vries-Bouwstra, J.K. Autoreactive b cell responses targeting nuclear antigens in systemic sclerosis: Implications for disease pathogenesis. Seminars in arthritis and rheumatism 2023, 58, 152136. [Google Scholar] [CrossRef] [PubMed]
- Merino-Vico, A.; Frazzei, G.; van Hamburg, J.P.; Tas, S.W. Targeting b cells and plasma cells in autoimmune diseases: From established treatments to novel therapeutic approaches. European journal of immunology n/a.
- Boonstra, M.; Meijs, J.; Dorjée, A.L.; Marsan, N.A.; Schouffoer, A.; Ninaber, M.K.; Quint, K.D.; Bonte-Mineur, F.; Huizinga, T.W.; Scherer, H.U. Rituximab in early systemic sclerosis. RMD open 2017, 3, e000384. [Google Scholar] [CrossRef] [PubMed]
- Sircar, G.; Goswami, R.P.; Sircar, D.; Ghosh, A.; Ghosh, P. Intravenous cyclophosphamide vs rituximab for the treatment of early diffuse scleroderma lung disease: Open label, randomized, controlled trial. Rheumatology 2018, 57, 2106–2113. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.P.; Ray, A.; Chatterjee, M.; Mukherjee, A.; Sircar, G.; Ghosh, P. Rituximab in the treatment of systemic sclerosis–related interstitial lung disease: A systematic review and meta-analysis. Rheumatology 2021, 60, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Gumkowska-Sroka, O.; Jagoda, K.; Owczarek, A.; Helbig, G.; Giemza-Stokłosa, J.; Kotyla, P.J. Cytometric characterization of main immunocompetent cells in patients with systemic sclerosis: Relationship with disease activity and type of immunosuppressive treatment. Journal of clinical medicine 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Stochmal, A.; Czuwara, J.; Trojanowska, M.; Rudnicka, L. Antinuclear antibodies in systemic sclerosis: An update. Clinical reviews in allergy & immunology 2020, 58, 40–51. [Google Scholar]
- Wynn, T.A. Fibrotic disease and the th1/th2 paradigm. Nature Reviews Immunology 2004, 4, 583–594. [Google Scholar] [CrossRef]
- Baraut, J.; Farge, D.; Jean-Louis, F.; Kesmandt, H.; Durant, C.; Verrecchia, F.; Michel, L. Cytokines in systemic sclerosis. Pathologie-biologie 2010, 60, 127–139. [Google Scholar] [CrossRef]
- Guo, R.H.; Cheng, H.; Zhang, X.Y.; Yu, Z.; Wang, G.H.; Hao, S.Y.; Gao, X.P.; Wen, H.Y. Changes in peripheral t-lymphocyte subsets and serum cytokines in patients with systemic sclerosis. Frontiers in pharmacology 2022, 13, 986199. [Google Scholar] [CrossRef]
- Orvain, C.; Cauvet, A.; Prudent, A.; Guignabert, C.; Thuillet, R.; Ottaviani, M.; Tu, L.; Duhalde, F.; Nicco, C.; Batteux, F.; et al. Acazicolcept (alpn-101), a dual icos/cd28 antagonist, demonstrates efficacy in systemic sclerosis preclinical mouse models. Arthritis Res Ther 2022, 24, 13. [Google Scholar] [CrossRef] [PubMed]
- Ellis, T.; Simms, P.; Slivnick, D.; Jäck, H.; Fisher, R. Cd30 is a signal-transducing molecule that defines a subset of human activated cd45ro+ t cells. The Journal of Immunology 1993, 151, 2380–2389. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, B.; Reddish, M.; Longenecker, B.M. Cd30 expression on human cd8+ t cells isolated from peripheral blood lymphocytes of normal donors. Journal of immunology (Baltimore, Md. : 1950) 1996, 157, 3229–3234. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, G.; De Carli, M.; D'Elios, M.M.; Daniel, K.C.; Almerigogna, F.; Alderson, M.; Smith, C.A.; Thomas, E.; Romagnani, S. Cd30-mediated signaling promotes the development of human t helper type 2-like t cells. J Exp Med 1995, 182, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Ihn, H.; Yazawa, N.; Kubo, M.; Yamane, K.; Sato, S.; Fujimoto, M.; Kikuchi, K.; Soma, Y.; Tamaki, K. Circulating levels of soluble cd30 are increased in patients with localized scleroderma and correlated with serological and clinical features of the disease. The Journal of rheumatology 2000, 27, 698–702. [Google Scholar] [PubMed]
- Nagy, Z.; Czirják, L. Increased levels of amino terminal propeptide of type iii procollagen are an unfavourable predictor of survival in systemic sclerosis. Clinical and experimental rheumatology 2005, 23, 165–172. [Google Scholar] [PubMed]
- Amedei, A.; Pimpinelli, N.; Grassi, A.; Bella, C.D.; Niccolai, E.; Brancati, S.; Benagiano, M.; D'Elios, S.; Bosi, A.; D'Elios, M.M. Skin cd30(+) t cells and circulating levels of soluble cd30 are increased in patients with graft versus host disease. Auto- immunity highlights 2014, 5, 21–26. [Google Scholar] [CrossRef]
- Giacomelli, R.; Cipriani, P.; Lattanzio, R.; Di Franco, M.; Locanto, M.; Parzanese, I.; Passacantando, A.; Ciocci, A.; Tonietti, G. Circulating levels of soluble cd30 are increased in patients with systemic sclerosis (ssc) and correlate with serological and clinical features of the disease. Clinical and experimental immunology 1997, 108, 42–46. [Google Scholar] [CrossRef]
- Higashioka, K.; Kikushige, Y.; Ayano, M.; Kimoto, Y.; Mitoma, H.; Kikukawa, M.; Akahoshi, M.; Arinobu, Y.; Horiuchi, T.; Akashi, K.; et al. Generation of a novel cd30(+) b cell subset producing gm-csf and its possible link to the pathogenesis of systemic sclerosis. Clinical and experimental immunology 2020, 201, 233–243. [Google Scholar] [CrossRef]
- Mavalia, C.; Scaletti, C.; Romagnani, P.; Carossino, A.M.; Pignone, A.; Emmi, L.; Pupilli, C.; Pizzolo, G.; Maggi, E.; Romagnani, S. Type 2 helper t-cell predominance and high cd30 expression in systemic sclerosis. The American journal of pathology 1997, 151, 1751–1758. [Google Scholar]
- Walker, L.S.K.; Sansom, D.M. The emerging role of ctla4 as a cell-extrinsic regulator of t cell responses. Nature Reviews Immunology 2011, 11, 852–863. [Google Scholar] [CrossRef] [PubMed]
- Linsley, P.S.; Greene, J.L.; Brady, W.; Bajorath, J.; Ledbetter, J.A.; Peach, R. Human b7-1 (cd80) and b7-2 (cd86) bind with similar avidities but distinct kinetics to cd28 and ctla-4 receptors. Immunity 1994, 1, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Lingel, H.; Brunner-Weinzierl, M.C. Ctla-4 (cd152): A versatile receptor for immune-based therapy. Seminars in Immunology 2019, 42, 101298. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Becker, J.-C.; Schiff, M.; Luggen, M.; Sherrer, Y.; Kremer, J.; Birbara, C.; Box, J.; Natarajan, K.; Nuamah, I. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor α inhibition. New England Journal of Medicine 2005, 353, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; Connolly, S.E.; Jabado, O.; Ye, J.; Kelly, S.; Maldonado, M.A.; Westhovens, R.; Nash, P.; Merrill, J.T.; Townsend, R.M. Identification of biomarkers of response to abatacept in patients with sle using deconvolution of whole blood transcriptomic data from a phase iib clinical trial. Lupus Sci Med 2017, 4, e000206. [Google Scholar] [CrossRef] [PubMed]
- Hosoda, T.; Hashimoto, S.; Sato, R.; Fujita, M.; Aizawa, T.; Tsugawa, K.; Tanaka, H. Abatacept as an alternative therapy for the treatment of drug-intolerant lupus nephritis: A case of underlying monosomy 1p36 deletion syndrome. Clinical nephrology 2022, 97, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Zhu, M.; Lin, Y.; Zhong, H.; Cai, L.; He, L.; Chou, K.C. The preliminary efficacy evaluation of the ctla-4-ig treatment against lupus nephritis through in-silico analyses. Journal of theoretical biology 2019, 471, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, M.; Bird, P.; Pachai, C.; Du, S.; Wu, C.; Landis, J.; Fuerst, T.; Ahmad, H.A.; Connolly, S.E.; Conaghan, P.G. Implementation of the omeract psoriatic arthritis magnetic resonance imaging scoring system in a randomized phase iib study of abatacept in psoriatic arthritis. Rheumatology (Oxford, England) 2022, 61, 4305–4313. [Google Scholar] [CrossRef]
- Tang, Q.; Ramsköld, D.; Krystufkova, O.; Mann, H.F.; Wick, C.; Dastmalchi, M.; Lakshmikanth, T.; Chen, Y.; Mikes, J.; Alexanderson, H.; et al. Effect of ctla4-ig (abatacept) treatment on t cells and b cells in peripheral blood of patients with polymyositis and dermatomyositis. Scandinavian journal of immunology 2019, 89, e12732. [Google Scholar] [CrossRef]
- Tjärnlund, A.; Tang, Q.; Wick, C.; Dastmalchi, M.; Mann, H.; Tomasová Studýnková, J.; Chura, R.; Gullick, N.J.; Salerno, R.; Rönnelid, J.; et al. Abatacept in the treatment of adult dermatomyositis and polymyositis: A randomised, phase iib treatment delayed-start trial. Annals of the rheumatic diseases 2018, 77, 55–62. [Google Scholar] [CrossRef]
- Toussirot, E.; Michaud, M.; Wendling, D.; Devauchelle, V. Abatacept as adjunctive therapy in refractory polymyalgia rheumatica. The Journal of rheumatology 2021, 48, 1888–1889. [Google Scholar] [CrossRef]
- Jin, W.; Zheng, Y.; Zhu, P. T cell abnormalities in systemic sclerosis. Autoimmunity reviews 2022, 21, 103185. [Google Scholar] [CrossRef] [PubMed]
- Elhai, M.; Meunier, M.; Matucci-Cerinic, M.; Maurer, B.; Riemekasten, G.; Leturcq, T.; Pellerito, R.; Von Mühlen, C.A.; Vacca, A.; Airo, P. Outcomes of patients with systemic sclerosis-associated polyarthritis and myopathy treated with tocilizumab or abatacept: A eustar observational study. Annals of the rheumatic diseases 2013, 72, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Spino, C.; Johnson, S.; Chung, L.; Whitfield, M.L.; Denton, C.P.; Berrocal, V.; Franks, J.; Mehta, B.; Molitor, J. Abatacept in early diffuse cutaneous systemic sclerosis: Results of a phase ii investigator-initiated, multicenter, double-blind, randomized, placebo-controlled trial. Arthritis & rheumatology 2020, 72, 125–136. [Google Scholar]
- Chung, L.; Spino, C.; McLain, R.; Johnson, S.R.; Denton, C.P.; Molitor, J.A.; Steen, V.D.; Lafyatis, R.; Simms, R.W.; Kafaja, S.; et al. Safety and efficacy of abatacept in early diffuse cutaneous systemic sclerosis (asset): Open-label extension of a phase 2, double-blind randomised trial. The Lancet. Rheumatology 2020, 2, e743–e753. [Google Scholar] [CrossRef] [PubMed]
- Katsumoto, T.R.; Whitfield, M.L.; Connolly, M.K. The pathogenesis of systemic sclerosis. Annual review of pathology 2011, 6, 509–537. [Google Scholar] [CrossRef] [PubMed]
- Kurzinski, K.; Torok, K.S. Cytokine profiles in localized scleroderma and relationship to clinical features. Cytokine 2011, 55, 157–164. [Google Scholar] [CrossRef]
- Boin, F.; De Fanis, U.; Bartlett, S.J.; Wigley, F.M.; Rosen, A.; Casolaro, V. T cell polarization identifies distinct clinical phenotypes in scleroderma lung disease. Arthritis & Rheumatism 2008, 58, 1165–1174. [Google Scholar]
- Skaug, B.; Assassi, S. Type i interferon dysregulation in systemic sclerosis. Cytokine 2020, 132, 154635. [Google Scholar] [CrossRef]
- Brkic, Z.; van Bon, L.; Cossu, M.; van Helden-Meeuwsen, C.G.; Vonk, M.C.; Knaapen, H.; van den Berg, W.; Dalm, V.A.; Van Daele, P.L.; Severino, A. The interferon type i signature is present in systemic sclerosis before overt fibrosis and might contribute to its pathogenesis through high baff gene expression and high collagen synthesis. Annals of the rheumatic diseases 2016, 75, 1567–1573. [Google Scholar] [CrossRef]
- Gillery, P.; Fertin, C.; Nicolas, J.F.; Chastang, F.; Kalis, B.; Banchereau, J.; Maquart, F.X. Interleukin-4 stimulates collagen gene expression in human fibroblast monolayer cultures. Potential role in fibrosis. FEBS letters 1992, 302, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Postlethwaite, A.E.; Holness, M.A.; Katai, H.; Raghow, R. Human fibroblasts synthesize elevated levels of extracellular matrix proteins in response to interleukin 4. J Clin Invest 1992, 90, 1479–1485. [Google Scholar] [CrossRef]
- Hasegawa, M.; Fujimoto, M.; Kikuchi, K.; Takehara, K. Elevated serum levels of interleukin 4 (il-4), il-10, and il-13 in patients with systemic sclerosis. The Journal of rheumatology 1997, 24, 328–332. [Google Scholar] [PubMed]
- Makhluf, H.A.; Stepniakowska, J.; Hoffman, S.; Smith, E.; LeRoy, E.C.; Trojanowska, M. Il-4 upregulates tenascin synthesis in scleroderma and healthy skin fibroblasts. Journal of investigative dermatology 1996, 107, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Chomarat, P.; Banchereau, J. Interleukin-4 and lnterleukin-13: Their similarities and discrepancies. International reviews of immunology 1998, 17, 1–52. [Google Scholar] [CrossRef]
- McCormick, S.M.; Heller, N.M. Commentary: Il-4 and il-13 receptors and signaling. Cytokine 2015, 75, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Chiaramonte, M.G.; Mentink-Kane, M.; Jacobson, B.A.; Cheever, A.W.; Whitters, M.J.; Goad, M.E.; Wong, A.; Collins, M.; Donaldson, D.D.; Grusby, M.J. Regulation and function of the interleukin 13 receptor α 2 during a t helper cell type 2–dominant immune response. The Journal of experimental medicine 2003, 197, 687–701. [Google Scholar] [CrossRef]
- Nguyen, J.K.; Austin, E.; Huang, A.; Mamalis, A.; Jagdeo, J. The il-4/il-13 axis in skin fibrosis and scarring: Mechanistic concepts and therapeutic targets. Archives of dermatological research 2020, 312, 81–92. [Google Scholar] [CrossRef]
- O'Reilly, S. Role of interleukin-13 in fibrosis, particularly systemic sclerosis. Biofactors 2013, 39, 593–596. [Google Scholar] [CrossRef]
- Wohlfahrt, T.; Usherenko, S.; Englbrecht, M.; Dees, C.; Weber, S.; Beyer, C.; Gelse, K.; Distler, O.; Schett, G.; Distler, J.H.; et al. Type 2 innate lymphoid cell counts are increased in patients with systemic sclerosis and correlate with the extent of fibrosis. Annals of the rheumatic diseases 2016, 75, 623–626. [Google Scholar] [CrossRef]
- Fuschiotti, P.; Medsger Jr, T.A.; Morel, P.A. Effector cd8+ t cells in systemic sclerosis patients produce abnormally high levels of interleukin-13 associated with increased skin fibrosis. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology 2009, 60, 1119–1128. [Google Scholar]
- Kotyla, P.; Gumkowska-Sroka, O.; Wnuk, B.; Kotyla, K. Jak inhibitors for treatment of autoimmune diseases: Lessons from systemic sclerosis and systemic lupus erythematosus. Pharmaceuticals (Basel, Switzerland) 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.L.; Wang, Y.J.; Yan, J.W.; Wan, Y.N.; Chen, B.; Li, B.Z.; Yang, G.J.; Wang, J. Role of anti-inflammatory cytokines il-4 and il-13 in systemic sclerosis. Inflammation research : official journal of the European Histamine Research Society... [et al.] 2015, 64, 151–159. [Google Scholar] [CrossRef]
- Gasparini, G.; Cozzani, E.; Parodi, A. Interleukin-4 and interleukin-13 as possible therapeutic targets in systemic sclerosis. Cytokine 2020, 125, 154799. [Google Scholar] [CrossRef] [PubMed]
- Allanore, Y.; Wung, P.; Soubrane, C.; Esperet, C.; Marrache, F.; Bejuit, R.; Lahmar, A.; Khanna, D.; Denton, C.P. A randomised, double-blind, placebo-controlled, 24-week, phase ii, proof-of-concept study of romilkimab (sar156597) in early diffuse cutaneous systemic sclerosis. Annals of the rheumatic diseases 2020, 79, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Brusselle, G.; Quirce, S.; Papi, A.; Kuna, P.; Chipps, B.E.; Hanania, N.A.; Blaiss, M.; Msihid, J.; Jacob-Nara, J.A.; Deniz, Y.; et al. Dupilumab efficacy in patients with uncontrolled or oral corticosteroid-dependent allergic and non-allergic asthma. The journal of allergy and clinical immunology. In practice, 2022. [Google Scholar]
- Kamphuis, E.; Boesjes, C.M.; Loman, L.; Bakker, D.S.; Poelhekken, M.; Zuithoff, N.P.A.; Kamsteeg, M.; Romeijn, G.L.E.; van Wijk, F.; de Bruin-Weller, M.S.; et al. Dupilumab in daily practice for the treatment of pediatric atopic dermatitis: 28-week clinical and biomarker results from the bioday registry. Pediatric allergy and immunology : official publication of the European Society of Pediatric Allergy and Immunology 2022, 33, e13887. [Google Scholar] [CrossRef]
- Hu, X.; Li, J.; Fu, M.; Zhao, X.; Wang, W. The jak/stat signaling pathway: From bench to clinic. Signal transduction and targeted therapy 2021, 6, 402. [Google Scholar] [CrossRef]
- Agashe, R.P.; Lippman, S.M.; Kurzrock, R. Jak: Not just another kinase. Mol Cancer Ther 2022, 21, 1757–1764. [Google Scholar] [CrossRef]
- Waickman, A.T.; Park, J.-Y.; Park, J.-H. The common γ-chain cytokine receptor: Tricks-and-treats for t cells. Cellular and molecular life sciences 2016, 73, 253–269. [Google Scholar] [CrossRef]
- Pant, H.; Hercus, T.R.; Tumes, D.J.; Yip, K.H.; Parker, M.W.; Owczarek, C.M.; Lopez, A.F.; Huston, D.P. Translating the biology of β common receptor-engaging cytokines into clinical medicine. The Journal of allergy and clinical immunology 2022. [Google Scholar] [CrossRef]
- Rose-John, S. Interleukin-6 family cytokines. Cold Spring Harbor perspectives in biology 2018, 10, a028415. [Google Scholar] [CrossRef] [PubMed]
- Vignali, D.A.; Kuchroo, V.K. Il-12 family cytokines: Immunological playmakers. Nat Immunol 2012, 13, 722–728. [Google Scholar] [CrossRef]
- Ni, S.; Shan, F.; Geng, J. Interleukin-10 family members: Biology and role in the bone and joint diseases. International immunopharmacology 2022, 108, 108881. [Google Scholar] [CrossRef] [PubMed]
- Kotyla, P.J. Are janus kinase inhibitors superior over classic biologic agents in ra patients? BioMed research international 2018, 2018, 7492904. [Google Scholar] [CrossRef] [PubMed]
- Fiorentini, E.; Bonomi, F.; Peretti, S.; Orlandi, M.; Lepri, G.; Matucci Cerinic, M.; Bellando Randone, S.; Guiducci, S. Potential role of jak inhibitors in the treatment of systemic sclerosis-associated interstitial lung disease: A narrative review from pathogenesis to real-life data. Life (Basel, Switzerland) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.H.; Chung, W.H.; Wu, P.C.; Chen, C.B. Jak-stat signaling pathway in the pathogenesis of atopic dermatitis: An updated review. Frontiers in immunology 2022, 13, 1068260. [Google Scholar] [CrossRef]
- Hutton, J.; Mease, P.; Jadon, D. Horizon scan: State-of-the-art therapeutics for psoriatic arthritis. Best practice & research. Clinical rheumatology, 2022; 101809. [Google Scholar]
- Nash, P. Jak inhibitors: New indication and emerging safety data in 2022. Nature reviews. Rheumatology 2022. [Google Scholar] [CrossRef] [PubMed]
- Sawamura, S.; Jinnin, M.; Inoue, K.; Yamane, K.; Honda, N.; Kajihara, I.; Makino, T.; Masuguchi, S.; Fukushima, S.; Ihn, H. Regulatory mechanisms of collagen expression by interleukin-22 signaling in scleroderma fibroblasts. Journal of dermatological science 2018, 90, 52–59. [Google Scholar] [CrossRef]
- Matsushita, T.; Hamaguchi, Y.; Hasegawa, M.; Takehara, K.; Fujimoto, M. Decreased levels of regulatory b cells in patients with systemic sclerosis: Association with autoantibody production and disease activity. Rheumatology 2016, 55, 263–267. [Google Scholar] [CrossRef]
- Mavropoulos, A.; Simopoulou, T.; Varna, A.; Liaskos, C.; Katsiari, C.G.; Bogdanos, D.P.; Sakkas, L.I. Breg cells are numerically decreased and functionally impaired in patients with systemic sclerosis. Arthritis & rheumatology 2016, 68, 494–504. [Google Scholar]
- Aydoğdu, E.; Pamuk, Ö.N.; Dönmez, S.; Pamuk, G.E. Decreased interleukin-20 level in patients with systemic sclerosis: Are they related with angiogenesis? Clinical rheumatology 2013, 32, 1599–1603. [Google Scholar] [CrossRef] [PubMed]
- Kakkar, V.; Assassi, S.; Allanore, Y.; Kuwana, M.; Denton, C.P.; Khanna, D.; Del Galdo, F. Type 1 interferon activation in systemic sclerosis: A biomarker, a target or the culprit. Current opinion in rheumatology 2022, 34, 357–364. [Google Scholar] [CrossRef]
- Wu, M.; Assassi, S. Dysregulation of type i interferon signaling in systemic sclerosis: A promising therapeutic target? Current Treatment Options in Rheumatology 2021, 7, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.; Geppert, T.; Schiopu, E.; Frech, T.; Hsu, V.; Simms, R.W.; Peng, S.L.; Yao, Y.; Elgeioushi, N.; Chang, L.; et al. Dose-escalation of human anti-interferon-α receptor monoclonal antibody medi-546 in subjects with systemic sclerosis: A phase 1, multicenter, open label study. Arthritis Res Ther 2014, 16, R57. [Google Scholar] [CrossRef]
- Guo, X.; Higgs, B.W.; Bay-Jensen, A.C.; Karsdal, M.A.; Yao, Y.; Roskos, L.K.; White, W.I. Suppression of t cell activation and collagen accumulation by an anti-ifnar1 mab, anifrolumab, in adult patients with systemic sclerosis. Journal of Investigative Dermatology 2015, 135, 2402–2409. [Google Scholar] [CrossRef]
- Moriana, C.; Moulinet, T.; Jaussaud, R.; Decker, P. Jak inhibitors and systemic sclerosis: A systematic review of the literature. Autoimmunity reviews 2022, 21, 103168. [Google Scholar] [CrossRef] [PubMed]
- Kranenburg, P.; van den Hombergh, W.M.; Knaapen-Hans, H.K.; van den Hoogen, F.H.; Fransen, J.; Vonk, M.C. Survival and organ involvement in patients with limited cutaneous systemic sclerosis and anti-topoisomerase-i antibodies: Determined by skin subtype or auto-antibody subtype? A long-term follow-up study. Rheumatology 2016, 55, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.I.; Howat, S.; Abraham, D.J.; Pearson, J.D.; Lawson, C. Agonistic anti-icam-1 antibodies in scleroderma: Activation of endothelial pro-inflammatory cascades. Vascular pharmacology 2013, 59, 19–26. [Google Scholar] [CrossRef]
- Tamby, M.C.; Humbert, M.; Guilpain, P.; Servettaz, A.; Dupin, N.; Christner, J.J.; Simonneau, G.; Fermanian, J.; Weill, B.; Guillevin, L. Antibodies to fibroblasts in idiopathic and scleroderma-associated pulmonary hypertension. European Respiratory Journal 2006, 28, 799–807. [Google Scholar] [CrossRef]
- Hysa, E.; Campitiello, R.; Sammorì, S.; Gotelli, E.; Cere, A.; Pesce, G.; Pizzorni, C.; Paolino, S.; Sulli, A.; Smith, V.; et al. Specific autoantibodies and microvascular damage progression assessed by nailfold videocapillaroscopy in systemic sclerosis: Are there peculiar associations? An update. Antibodies (Basel, Switzerland) 2023, 12. [Google Scholar]
- Jerjen, R.; Nikpour, M.; Krieg, T.; Denton, C.P.; Saracino, A.M. Systemic sclerosis in adults. Part i: Clinical features and pathogenesis. J Am Acad Dermatol 2022, 87, 937–954. [Google Scholar] [CrossRef] [PubMed]
- Liem, S.I.E.; Neppelenbroek, S.; Fehres, C.M.; Wortel, C.; Toes, R.E.M.; Huizinga, T.W.J.; Scherer, H.U.; de Vries-Bouwstra, J.K. Autoreactive b cell responses targeting nuclear antigens in systemic sclerosis: Implications for disease pathogenesis. Seminars in arthritis and rheumatism 2023, 58, 152136. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Denton, C.P. Scleroderma autoantibodies in guiding monitoring and treatment decisions. Current opinion in rheumatology 2022, 34, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Nakayamada, S.; Tanaka, Y. Baff- and april-targeted therapy in systemic autoimmune diseases. Inflammation and Regeneration 2016, 36, 6. [Google Scholar] [CrossRef]
- Gordon, J.K.; Martyanov, V.; Franks, J.M.; Bernstein, E.J.; Szymonifka, J.; Magro, C.; Wildman, H.F.; Wood, T.A.; Whitfield, M.L.; Spiera, R.F. Belimumab for the treatment of early diffuse systemic sclerosis. Arthritis & Rheumatology 2018, 70, 308–316. [Google Scholar]
- Ly, S.; Nedosekin, D.; Wong, H.K. Review of an anti-cd20 monoclonal antibody for the treatment of autoimmune diseases of the skin. American journal of clinical dermatology 2023, 1–27. [Google Scholar] [CrossRef]
- Merino-Vico, A.; Frazzei, G.; van Hamburg, J.P.; Tas, S.W. Targeting b cells and plasma cells in autoimmune diseases: From established treatments to novel therapeutic approaches. European journal of immunology 2023, 53, e2149675. [Google Scholar] [CrossRef]
- van den Hoogen, L.L.; Bisoendial, R.J. B-cells and baff in primary antiphospholipid syndrome, targets for therapy? Journal of clinical medicine 2022, 12. [Google Scholar] [CrossRef]
- Zhen, C.; Hou, Y.; Zhao, B.; Ma, X.; Dai, T.; Yan, C. Efficacy and safety of rituximab treatment in patients with idiopathic inflammatory myopathies: A systematic review and meta-analysis. Frontiers in immunology 2022, 13, 1051609. [Google Scholar] [CrossRef]
- Alexander, T.; Cheng, Q.; Klotsche, J.; Khodadadi, L.; Waka, A.; Biesen, R.; Hoyer, B.F.; Burmester, G.R.; Radbruch, A.; Hiepe, F. Proteasome inhibition with bortezomib induces a therapeutically relevant depletion of plasma cells in sle but does not target their precursors. European journal of immunology 2018, 48, 1573–1579. [Google Scholar] [CrossRef]
- Adams, J. The proteasome: A suitable antineoplastic target. Nature reviews. Cancer 2004, 4, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Hideshima, T.; Richardson, P.G.; Anderson, K.C. Mechanism of action of proteasome inhibitors and deacetylase inhibitors and the biological basis of synergy in multiple myeloma. Molecular Cancer Therapeutics 2011, 10, 2034–2042. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, S.; Bongiovanni, M.; Donati, Y.; Djaafar, S.; Naso, F.; Goffin, L.; Barazzone Argiroffo, C.; Pache, J.-C.; Dayer, J.-M.; Ferrari-Lacraz, S. In vivo investigations on anti-fibrotic potential of proteasome inhibition in lung and skin fibrosis. American journal of respiratory cell and molecular biology 2008, 39, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Duan, W.; Cu, X.; Liang, C.; Xin, M. Bruton’s tyrosine kinase (btk) inhibitors in treating cancer: A patent review (2010-2018). Expert Opinion on Therapeutic Patents 2019, 29, 217–241. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.N. Regulation of b lymphocyte development and activation by bruton's tyrosine kinase. Immunologic research 2001, 23, 147–156. [Google Scholar] [CrossRef]
- Du, Y.; Lei, L.; Ding, H.; Chen, Y.; Pathak, S.; Hicks, J.; Tran, P.T.; Wu, M.; Chang, B.; Wirtz, U.; et al. Targeting multiple end organs in lupus and other systemic rheumatic diseases by inhibiting bruton's tyrosine kinase. Frontiers in immunology 2022, 13, 893899. [Google Scholar] [CrossRef] [PubMed]
- Einhaus, J.; Pecher, A.-C.; Asteriti, E.; Schmid, H.; Secker, K.-A.; Duerr-Stoerzer, S.; Keppeler, H.; Klein, R.; Schneidawind, C.; Henes, J.; et al. Inhibition of effector b cells by ibrutinib in systemic sclerosis. Arthritis Res Ther 2020, 22, 66. [Google Scholar] [CrossRef] [PubMed]
- Ringheim, G.E.; Wampole, M.; Oberoi, K. Bruton's tyrosine kinase (btk) inhibitors and autoimmune diseases: Making sense of btk inhibitor specificity profiles and recent clinical trial successes and failures. Frontiers in immunology 2021, 12, 662223. [Google Scholar] [CrossRef]
- Agarbati, S.; Benfaremo, D.; Viola, N.; Paolini, C.; Svegliati Baroni, S.; Funaro, A.; Moroncini, G.; Malavasi, F.; Gabrielli, A. Increased expression of the ectoenzyme cd38 in peripheral blood plasmablasts and plasma cells of patients with systemic sclerosis. Frontiers in immunology 2022, 13, 1072462. [Google Scholar] [CrossRef]
- Peclat, T.R.; Shi, B.; Varga, J.; Chini, E.N. The nadase enzyme cd38: An emerging pharmacological target for systemic sclerosis, systemic lupus erythematosus and rheumatoid arthritis. Current opinion in rheumatology 2020, 32, 488–496. [Google Scholar] [CrossRef]
- Benfaremo, D.; Gabrielli, A. Is there a future for anti-cd38 antibody therapy in systemic autoimmune diseases? Cells 2019, 9. [Google Scholar] [CrossRef]
- Cole, S.; Walsh, A.; Yin, X.; Wechalekar, M.D.; Smith, M.D.; Proudman, S.M.; Veale, D.J.; Fearon, U.; Pitzalis, C.; Humby, F.; et al. Integrative analysis reveals cd38 as a therapeutic target for plasma cell-rich pre-disease and established rheumatoid arthritis and systemic lupus erythematosus. Arthritis Res Ther 2018, 20, 85. [Google Scholar] [CrossRef] [PubMed]
- De Flora, A.; Guida, L.; Franco, L.; Zocchi, E. The cd38/cyclic adp-ribose system: A topological paradox. The international journal of biochemistry & cell biology 1997, 29, 1149–1166. [Google Scholar]
- Shi, B.; Wang, W.; Korman, B.; Kai, L.; Wang, Q.; Wei, J.; Bale, S.; Marangoni, R.G.; Bhattacharyya, S.; Miller, S.; et al. Targeting cd38-dependent nad(+) metabolism to mitigate multiple organ fibrosis. iScience 2021, 24, 101902. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.A.; Boslett, J.; Varadharaj, S.; De Pascali, F.; Hemann, C.; Druhan, L.J.; Ambrosio, G.; El-Mahdy, M.; Zweier, J.L. Depletion of nadp (h) due to cd38 activation triggers endothelial dysfunction in the postischemic heart. Proceedings of the National Academy of Sciences 2015, 112, 11648–11653. [Google Scholar] [CrossRef]
- Graßhoff, H.; Fourlakis, K.; Comdühr, S.; Riemekasten, G. Autoantibodies as biomarker and therapeutic target in systemic sclerosis. Biomedicines 2022, 10, 2150. [Google Scholar] [CrossRef]
- Tsou, P.-S.; Varga, J.; O’Reilly, S. Advances in epigenetics in systemic sclerosis: Molecular mechanisms and therapeutic potential. Nature Reviews Rheumatology 2021, 17, 596–607. [Google Scholar] [CrossRef]
Figure 1.
Fibrotic pathways to be blocked in systemic sclerosis.
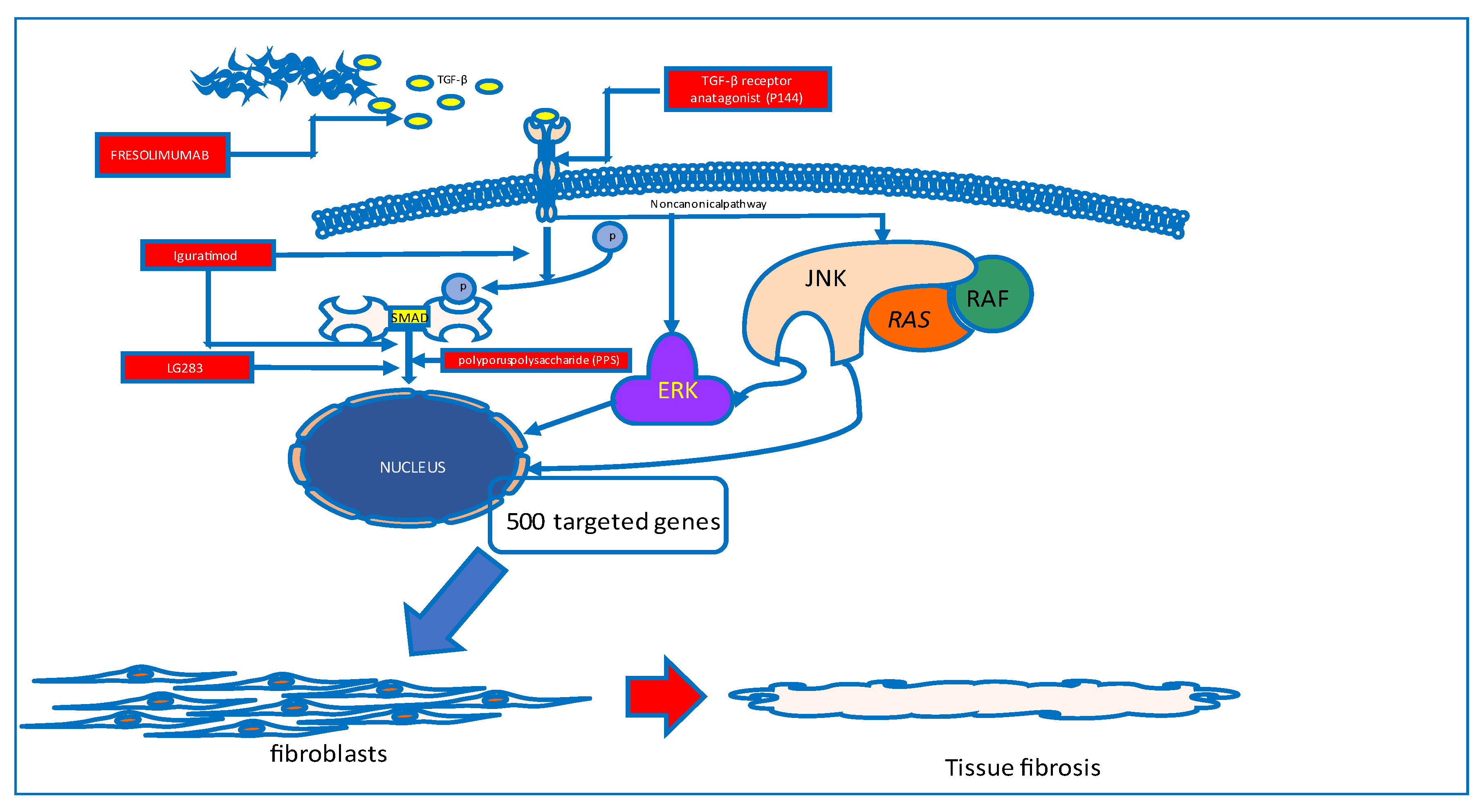
Figure 2.
Possible therapeutic targets in the treatment of systemic sclerosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



