
Submitted:
01 June 2023
Posted:
02 June 2023
You are already at the latest version
Abstract
Viral Encephalitis is a significant public health concern globally, especially west Africa. There are more than 500 known arboviruses with over 100 of them identified to cause encephalitic diseases in humans and animals, giving rise to a tremendous burden of the diseases, and socioeconomic strains in tropical and subtropical regions worldwide. Despite their importance, few effective preventive and control measures in form of vaccines and therapeutics are available and where they are, usage is limited. These limitations are largely hinged on the paucity of information about the molecular epidemiology and transmission patterns of VE in west Africa. Here, we reviewed the transmission dynamics, ecological drivers, and molecular epidemiology of VE in the region. Collectively, timely and accurate interventions are essential for encephalitic viral disease control. Moreover, the integrated health system approach, combining surveillance, vaccination, vector control, and community engagement could be effective in preventing viral encephalitis globally.
Keywords:
Viral Encephalitis
; Transmission Dynamics
; Epidemiology
; One Health
1. Introduction
With numerous emerging and re-emerging zoonotic viral infections which cause serious neurological consequences recently gaining global attention, viral encephalitis (VE) has particularly become a significant public health concern in West Africa (1,2,3). It is essential to develop a thorough understanding of the molecular inter-relatedness and the transmission dynamics of these infections in order to properly address future danger. There are several crucial elements which potentiates the establishment and transmission cycle of these plethora of pathogens causing VE in West Africa (4). First, depending on the particular infection, different viruses that cause encephalitis ideally have arthropod or animal reservoirs (5,6). For instance, arthropod-borne viruses (arboviruses) like Chikungunya virus (CHIKV), West Nile virus (WNV), Rift Valley fever virus (RVFV), and Yellow fever virus (YFV) predominantly exploit infected animals, including birds, livestock, and wild mammals, as the virus's amplification hosts (7,8). Furthermore, zoonotic viruses like the Lassa virus have particular animal reservoirs, including the Mastomys rat, which helps transmit Lassa fever with the accompanying encephalitis (9). Ticks and mosquitoes are important carriers of arboviruses like WNV and CHIKV (10). Aedes mosquitoes, especially Aedes aegypti and Aedes albopictus, are well established carriers of these viruses (11). In most West African countries (Figure 1), especially Nigeria and Ghana, these mosquitoes typically reproduce primarily in urban and peri-urban environments where people use artificial water storage containers (12). By feeding on cattle and animals, ticks, especially those from the genus Hyalomma, contribute to the spread of encephalitis-causing viruses like the Crimean-Congo hemorrhagic fever virus (CCHFV) (13). Secondly, there is a substantial role humans play in the VE transmission cycle. Through the bites of infected ticks or mosquitoes, which act as hosts for the viruses, humans get infected (14). Working in the veterinary, agricultural, or healthcare industries puts some occupational groups at a higher risk of contracting zoonotic viruses like the Lassa virus through contact with infected animals or their bodily fluids (15). Thirdly, environmental factors are also important in the transmission dynamics of VE. Peak transmission occurs during the rainy season, when mosquito populations are at their highest, and climate and seasonality have a significant impact on tick and mosquito populations (16). Rapid urbanization and changes in land use encourage mosquito breeding, which amplifies the spread of viruses that cause encephalitis. The spread of Aedes mosquitoes in urban settings is further aided by poor waste management procedures (17). Successful implemention targeted remedies requires an understanding of these intricate drivers of VE transmission in West Africa. Here, we propose an effective and unbiased application of the one health concept to bolster existing preventive and control strategies in West African nations.
2. Transmission Dynamics of Major Viral Encephalitis in West Africa
Generally, VE can either be caused by arboviruses or non-arboviruses (2,18). For arboviruses, there are several players involved in the transmission cycle of these viruses, and a robust knowledge of these is vital for the development of efficient preventative and control strategies (3). The maintenance and spread of various viral encephalitic pathogens depend on specific reservoirs in West Africa as aforementioned (6). YFV is a major viral disease in West Africa. Non-human primates, notably monkeys and apes prevalent in forested settings, have been implicated as the main source of YFV (19). The virus is acquired by mosquitoes, specifically Aedes aegypti, when they feed on infected primates, and it is then transmitted to humans through blood feeding (19). For ZIKV, there is still much to learn about the viral reservoir in West Africa, even though some evidence points to non-human primates, notably monkeys, as potential hosts (20). In addition, as ZIKV can remain in bodily fluids like semen and be sexually transmitted, infected people can serve as reservoirs for the virus (21). Another virus-causing encephalitis disease of concern in West Africa is dengue fever caused by dengue viruses. Humans, particularly those who have symptomatic or asymptomatic infections, make up the majority of the viral reservoir for dengue viruses (22). The virus is spread to more people by mosquitoes, continuing the cycle of transmission. Furthermore, other viral infection that causes encephalitis in West Africa is CHIKV. Although non-human primates and other vertebrates may possibly help maintain the CHIKV virus in some ecological contexts, humans are the virus' principal reservoir (23). The presence of CHIKV-infected people in the population allows the virus to survive and spread. Aedes aegypti and Aedes albopictus mosquitoes, in particular, pick up the virus when they feed on infected people and pass it on to other people when they feed on blood (23). There are also other arboviruses in the region that have been largely under-investigated which have the potential of causing an outbreak in either human or animal population, like Usutu virus (24). More importantly, in West Africa, certain non-arboviruses cause encephalitis with grave outcomes. For instance, Enteroviruses, such as coxsackieviruses and enterovirus 71 (EV71). Enteroviruses are largely spread by humans, and humans make up most of the reservoir for these diseases (25). Person-to-person transmission is a factor in their persistence and spread, especially in crowded settings and among young people (25). The transmission cycle is further aided by environmental contamination brought on by the virus being shed in feces (26). Furthermore, Ebola Viral Hemorrhagic disease (EVD) which was first reported in Guinea, Liberia, and Sierra Leone about a decade ago has since become a major highlight as regards major encephalitic disease outbreak in West Africa (27). Ebola virus was introduced into the human population via contact with blood, organs, or other bodily fluids of an infected animal. For example, the first human EVD case in the West Africa outbreak was presumably infected via exposure to bats. Asides bats, EVD has also been reported in individuals exposed to infected wild animals like chimpanzees, antelopes, and gorillas in places like Gabon, Cote d’Ivoire, and the Republic of the Congo (28). Also, Rabies caused by rabies virus, a lyssavirus, is a neglected though preventable zoonotic encephalitic disease that predominantly affects the most vulnerable populations living in remote rural areas of resource-limited countries like West African countries (29). There are two possible transmission routes for rabies, either via bats or dog-mediated (30). Currently, most country in Africa is considered endemic for dog-mediated rabies with an estimated 20,000 or more death annually (31).
3. Molecular Epidemiology of Major Viral Encephalitis in West Africa
A phylogenetic analysis of the sequences of isolated arthropod-borne and non-arthropod-borne viruses causing encephalitis from various countries in West Africa (Figure 2) shows the genetic evolution and inter-relatedness of these viruses, regardless of their route of transmission (2, 32). Six (6) arthropod-borne viruses causing encephalitis such as WNV, Japanese encephalitis virus, ZIKV, CHIKV, YFV, and Rift Valley fever virus were considered across seventeen (17) West African countries. Also, twelve (12) non-arthropod-borne viruses such as Herpes simplex virus types 1 and 2, Varicella-zoster virus, Enteroviruses, La Crosse virus, St. Louis virus, Equine viruses, Powassan virus, Epstein-Barr virus, Rabies virus, Cytomegalovirus, Ebola virus, and Lassa virus were considered (32). Based on the limited molecular-based network in Africa, few of these viruses' molecular signatures are available on GenBank, considering the countries that isolated the whole genome of the viruses. Only twenty-four arboviral sequences and twenty-five non-arthropod borne viral sequences were available across West Africa. This shows the need for more molecular surveillance networks across Africa. Importantly, the level of clustering of these sequences highlights the need for an integrated approach in preventing viral encephalitis across the region (33).
4. Ecological Factors Potentiating the Spread of Viral Encephalitis in West Africa
Per the epidemiological triad (37), three factors are normally required for the transmission, maintenance, and propagation of most infectious diseases: the pathogen (virus), the vector (mosquito or tick, for example), and a suitable virus-replicating host (bird, monkey, for example). All three factors must have adequate and frequent interaction within the environment for the virus to survive and make progress along the next pathway in the cycle, otherwise local infection and, eventually, the species of the virus will die off. Oftentimes the virus finds alternate routes for other direct transmissions, such as directly between people via sperm or blood transfusion, as for Zika. However, this is an exception. Sometimes mosquitoes transfer the virus to a dead-end host, as seen in West Nile infections, where humans are incidental infections that play no vital role in the virus's normal cycle and maintenance but have huge consequences since they cause sickness or death in people. Infected humans do not develop a high enough viraemia to re-infect other mosquitos, which would allow the environmental spread of the virus and thus increase dissemination opportunity and survival possibilities, which does not lead to further spread (20). Environmental and human factors seem to have a role in the rising prevalence of vector-borne illnesses. Changes in the climate, urbanization (particularly in altered urban environments), human actions, large-scale gathering events, human and animal movement, expansion of air travel, and large-scale farming have all been implicated in the swiftly expanding world epidemic of vector-borne illnesses (38). Finally, growing human population density, widespread land use change, and the emergence of human commensal vectors may exert selection pressure on viruses to develop to take advantage of novel habitats (38).
Some of the ecological factors are briefly overviewed below:
4.1. Climate: Climatic Factors and Climate Change
Changes in climate such as increases in temperature and rainfall can create more favourable conditions for the survival, reproduction and spread of arthropods, which increase their population and the risk of disease transmission. Climate change, according to the 2014 Climate Change Report, can promote the propagation of vector-borne infections by modifying the biology of the vectors, their level of abundance and distribution over space, including territorial expansion into new areas, and changes in the infectious agents' extrinsic incubation period. Environmental modifications aimed to offset the consequences of climate change, such as flood protection and more urban green space, might raise the risk of illnesses spread by vectors (39).
The temperature has for a long time, influences virus replication rates and West Nile Virus (WNV) transmission by influencing the period of extrinsic incubation, the seasonal characteristics of mosquito vector populations, and regional variance in human case occurrence [40, 41,42). Increased ambient temperatures boost vector population rise (43), shorten the time between blood feeds, and hasten viral development (40,42). Several experimental discoveries have demonstrated a link between temperature changes and the survival and competency of WNV mosquito vectors. Despite that the quantity of precipitation (rain) might alter disease prevalence patterns, the response may vary across vast geographic regions due to changes in mosquito vector ecology (44). Above-average rainfall may enhance mosquito numbers as well as the risk for epidemics of diseases (45). For Instance, the frequency of WNV in the tropics should be highest during the rainy season, when mosquitoes are most prevalent (46), but published data on the epidemiology of WNV in the tropical regions are scarce. While precipitation promotes mosquito population emergence in temperate regions (47), increasing rainfall in a humid environment may have minimal effect if undeveloped mosquito habitats are already numerous. Nevertheless, mosquitoes in dry regions, such as the climate of the Mediterranean type, may benefit from more rain because it increases the number of undeveloped habitats, particularly when heavy rainfall during the spring promotes stagnant reservoirs at the start of the hot season (43). The ecologies of the numerous possible mosquito vectors of the Rift Valley Fever (RVF) virus contribute to the link between these severe rains and epidemic incidents (48). Over four years, researchers discovered that above-average rainfall for 85-152 days preceded RVF epidemics in seven of nine locations in South Africa (49). Human outbreaks caused by the CHIKV occur at unpredictable intervals ranging from 3 to 20 years and frequently coincide with extremely wet times. Outbreaks in rural areas are typically on a limited scale and are reliant on sylvatic mosquito numbers, which rise during periods of intense precipitation (49). In contrast, certain epidemics in coastal East Africa in 2004 were linked to drought and poor socioeconomic development. In these situations, it is thought that infrequent replenishing of water reserves and mosquito hatching in storage containers near humans potentiate CHIKV transmission (50).
4.2. Human Population Growth and Global Travel
The substantial expansion of the human population in West Africa has resulted in greater urbanization and expanding agriculture, potentially creating a new medium for the transmission of disease. Particularly in urban settings, the more populous and the closer together they are distributed, the more hosts and easier accessibility available for blood-feeding mosquitoes. Higher population numbers also indicate more garbage, which produces habitat for receptacle breeders like Aedes, or dirty pools and streams for Culex, typically in the poorer and less hygienic metropolitan regions where family finances do not afford effective personal mosquito protection. Rapid and huge population expansion is being accompanied by rising urbanization and global migration (51). Most Sub-Saharan African populations are expected to expand twice the current size (52), resulting in greater human mobility into ancient, wooded regions to get access to more land and hence exposure to the many arboviruses that exist in wild cycles. It is obvious that increased population, greater urbanization, and increased worldwide travel will create a huge opportunity for the transmission and expansion of mosquitoes, viruses, and related arboviral illnesses. Furthermore, the travel and relocation of humans and animals have accelerated the spread of arthropod-borne viruses to new territories. Transnational and intercontinental movement of infectious vector mosquitoes or their eggs are one of the most significant mechanisms for fast geographical shifts in arbovirus populations. Transport of Aedes aegypti in ships centuries ago to transmit yellow fever from Africa to South America, which is happening till today (53), and Aedes albopictus principally through the used-car tyre export trade (54). Dengue, chikungunya, Zika, and other viruses have all become major threats to global public health due to this characteristic of global spread through human-facilitated means (55), which has elevated Aedes aegypti and Aedes albopictus to their current status as arguably the two most significant disease carriers on the planet. West Nile virus, a Culex-associated arbovirus that uses birds as an amplifying host, also made the journey to North America (56), possibly from Africa or the Middle East, as genetic evidence suggests, and is thought to have arrived by mosquitoes on board airplanes (56). Such disease movement is not limited to trade and tourism, as there is a growing amount of people visiting friends and relatives, pilgrimages, humanitarian and other volunteer work, and large numbers of politically and economically affected refugees, all of which contribute to the potential for infected people to carry infectious agents to other locations and infect native vectors (57).
4.3. Land Use Change
Several land use activities such as deforestation or urbanisation alter arthropod habitats and create new avenues and opportunities for increased arthropod-human contact, which ultimately facilitate the spread of diseases and increase the risk. The effect of man on the planet, such as modern infrastructure, irrigation, and vast solid waste generation, favors vector growth. Finally, urbanization in impoverished areas with an insufficient water supply and rubbish disposal might encourage mosquito breeding (38, 58). The processes of JEV propagation are linked to changes in land use and agricultural activities (59). Increased chances for mosquito breeding arise when the economy develops and the rice sector thrives at the price of deforestation, as rice paddy areas are regarded as an excellent condition for mosquito reproduction and growth. Furthermore, rice fields entice migrating birds, further complicating the intricate interplay of elements that characterize JEV propagation and dissemination (59).
4.5. Animal Reservoirs
Most arthropod-borne encephalitis viruses have animal reservoirs and perhaps amplifying hosts which can serve as a source of infection for vectors and in turn humans. RVF virus has been demonstrated in experiments to multiply in a wide range of species of mammals, however, the response to environmental infections varies greatly. Sheep, cattle, goats, and camels are the most commonly connected with severe epizootics, partly because they outnumber other possible hosts in disease-affected areas. There is now strong convincing proof that WNV spreads widely and is largely unharmful among humans, birds, horses, and a variety of other animals in Africa, Europe, many parts of Asia, and Australasia. This is based on serological investigations, virus isolation, and Polymerase Chain Reaction-sequencing using samples taken from healthy birds, horses, mosquitoes, and ticks (60). Pigs serve as the amplifying host for JEV (59). In addition to pigs and birds, several domesticated animals that may be sub-clinically ill but are not likely to aid in the spread of JEV include horses and other equids (donkeys), cattle, sheep, goats, dogs, cats, chickens, ducks, wild mammals, reptiles, and amphibians (61). However, further studies are required to rule out alternative host animal roles in the JEV transmission cycle (62).
4.6. Vertical Viral Transmission and Desiccation-Resistant Eggs
Horizontal transmission of the virus occurs between mosquitos, birds, humans, and other vertebrates, but there is also a trans-generational, vertical transfer of viruses within some vector species, allowing the infectious virus to travel from adult mosquitos to offspring (63). Vertical viral transmission from one generation of mosquitos to the next appears to be unusual in mosquito-borne Alphaviruses, but widespread in Flaviviruses and prevalent in Bunyaviruses (64). Having the capacity to pass the virus on from one mosquito generation to the next via infected eggs (vertical transmission) is a significant adaptive benefit that helps enhance the probability of virus survival in the environment, reducing the chances of local extinction of the virus at a specific geographical focus. However, a mix of this ability with eggs that are also desiccation tolerant or resistant adds a truly strong dual framework not only for virus survival but also for spatiotemporal spread. The ability of some mosquitoes to lay eggs that can withstand varying amounts of complete drying out and hatch when the next surges of rain, flood, or human irrigation of a garden occur, or even have staggered hatching events spread over multiple rainfall surges, is likely the most significant biological trait of all that contributed to the efficient transcontinental dissemination of Ae. aegypti and Ae. albopictus, as well as other viruses such as Dengue virus (DENV), CHIKV, Yellow Fever virus (YFV), and others that have been linked therewith (38). How the RVF virus continues to exist between epidemics that may have more than a decade between such occurrences has long been a mystery. It has been hypothesized that transovarially infected Aedes eggs that are drought-resistant and thrive for several decades may be to blame or assist such inter-epidemic existence (63,64).
5. Integrated Health System: Plausible Preventive and Control Measures
The integrated health system approach, combining surveillance, vaccination, vector control, and community engagement, has been proposed severally to be effective in preventing most diseases. A concerted effort combining these factors could prove to be a solution going forward.
5.1. Robust Surveillance
As shown in Figure 3, Surveillance is a cornerstone of integrated health systems in preventing viral encephalitis in West Africa. Timely detection, reporting of suspected cases and outbreaks are crucial for prompt response and control measures. Surveillance systems, such as the Integrated Disease Surveillance and Response (IDSR) strategy implemented by the World Health Organization (WHO), facilitate the collection, analysis, and dissemination of data on disease patterns, which inform public health actions. Surveillance activities for different diseases involve similar functions (detection, reporting, analysis, feedback, action) and often use the same structures, processes and personnel (38). Through robust surveillance, health authorities can identify potential hotspots, monitor disease transmission dynamics, and implement interventions to prevent the spread of VE. Disease surveillance, either through passive case detection or syndromic surveillance with laboratory confirmation, is a pillar for arboviral monitoring [5]. However, arboviral infections result in a spectrum of clinical outcomes, which can be mild with only non-specific flu-like symptoms, and often managed in outpatient clinics without testing for arboviral infections. Consequently, increased virus transmission activity would be missed since not all symptomatic infections are tested for arboviral etiology (40).
5.2. Vaccination
Vaccines have been proven to be effective in preventing viral encephalitis diseases which are prevalent in West Africa (65). Vaccination campaigns, including routine immunization, are essential components of integrated health systems to ensure high vaccine coverage in vulnerable populations (40). Vaccination campaigns for vaccine-preventable diseases, such as polio, have also been integrated into routine immunization programs in West Africa (41). Vaccination, when combined with other preventive measures, can contribute to the reduction of VE cases (42).
5.3. Vector Control
Vector control is critical to prevent viral encephalitis in West Africa as many VE diseases are transmitted by vectors, which the climate favors vector population and made arthropod borne VE prevalent. Sub-Saharan Africa hosts multiple vector-borne diseases due to the environmental conditions and high diversity of vector species (66). For many vector-borne diseases, vector control (targeting the arthropods transmitting the disease) is highly effective in reducing transmission. For some diseases, such as dengue disease, vector control is the only approach currently available (43). Previous successes indicate that thorough vector control can reduce disease incidence (67). Unsuccessful interventions are typically attributed to several factors, including inadequate responses to the virus’ strength of transmission, insecticide resistance, expanding vector populations, expanding urban centers with poor sanitation, inadequate vector control infrastructure, and so on. (68). To strengthen vector control, the WHO endorsed the integrated vector management (IVM) strategy as a platform for combating vector-borne diseases. IVM is a comprehensive approach to optimally use resources for sustained evidence-based vector control with the collaboration of the health sector, various agencies, and communities (44, 45). In 2004, the WHO adopted IVM globally for the control of all vector-borne diseases and has been implemented in various countries to reduce the burden of the diseases, including viral encephalitis (46). Community engagement is also a critical component of vector control, where communities identify and eliminate vector breeding sites, use insecticide-treated bed nets, and adopt other preventive measures. The simultaneous use of multiple methods is now the preferred vector control strategy and forms a cornerstone of integrated vector management, a best practice framework for sustainable and cost-effective vector control.
5.4. Health System Strengthening
Strengthening health systems is essential in the prevention of viral encephalitis in West Africa. Weak health systems with inadequate infrastructure, limited resources, and workforce shortages can hinder effective disease prevention and control efforts (47). Integrated health systems require providing diagnostic testing, treatment, and supportive care. Building laboratory diagnostics capacity, training healthcare workers, and improving healthcare infrastructure are critical components of the strengthening. In addition, strengthening supply chains, improving data management, and ensuring availability of medical supplies and drugs are crucial in West Africa.
5.5. Collaboration and Coordination
Collaboration and coordination among different stakeholders are essential in integrated health systems for the prevention of viral encephalitis in West Africa. Viral encephalitis is a complex public health issue that requires a multisectoral approach involving health authorities, government agencies, non-governmental organizations, community-based organizations, and other relevant partners (48). Collaborative efforts can lead to coordinated actions, resource sharing, and efficient implementation of preventive measures. Adapting the One Health approach among different sectors can help address the underlying risk factors for VE. Collaboration is essential in ensuring a unified approach to preventing VE in West Africa.
6. Conclusion and Recommendations
Despite the potential benefits of integrated health systems in preventing viral encephalitis in West Africa, there are several challenges that need to be addressed. Limited resources, including financial, human, and infrastructure, can hinder the effective implementation of integrated health systems. Inadequate funding for surveillance, vaccination campaigns, vector control, and health system strengthening can limit the capacity to prevent viral encephalitis outbreaks. Additionally, workforce shortages, particularly in remote and underserved areas, can limit the delivery of essential health services. Weak health information systems and data management can also impede the timely and accurate collection, analysis, and dissemination of disease data, hampering effective response measures.
To overcome these challenges, several solutions can be implemented. Strengthening health systems through increased investment in infrastructure, workforce training, and supply chain management can improve the capacity to prevent viral encephalitis outbreaks. Enhancing surveillance systems by investing in surveillance infrastructure, training healthcare workers, and improving data management can improve early detection and response to outbreaks. Increasing funding for vaccination campaigns, vector control, and community engagement programs can ensure high vaccine coverage and effective vector control measures. Promoting collaboration among different stakeholders through multi sectoral partnerships and resource sharing can enhance the implementation as well. Additionally, advocacy and policy engagement can be employed to highlight the importance of integrated health systems in preventing VE and advocate for increased funding and support from government, donors, and other stakeholders.
Author Contributions
OCA conceptualized the study. ROA, OCA, and AH made the figures. OCA, ROA, VA, AH, and IPO wrote and reviewed the final draft of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Klein, R.S. Encephalitic Arboviruses of Africa: Emergence, Clinical Presentation and Neuropathogenesis. Front. Immunol. 2021, 12, 769942. [Google Scholar] [CrossRef]
- Rezaei, S.J.; Mateen, F.J. Encephalitis and meningitis in Western Africa: a scoping review of pathogens. Trop. Med. Int. Health 2020, 26, 388–396. [Google Scholar] [CrossRef]
- Mencattelli, G.; Ndione, M.H.D.; Rosà, R.; Marini, G.; Diagne, C.T.; Diagne, M.M.; Fall, G.; Faye, O.; Diallo, M.; Faye, O.; et al. Epidemiology of West Nile virus in Africa: An underestimated threat. PLOS Neglected Trop. Dis. 2022, 16, e0010075. [Google Scholar] [CrossRef]
- Venkatesan, A. Advances in Infectious Encephalitis: Etiologies, Outcomes, and Potential Links with Anti-NMDAR Encephalitis. Curr. Infect. Dis. Rep. 2013, 15, 594–599. [Google Scholar] [CrossRef]
- Michelitsch, A.; Wernike, K.; Klaus, C.; Dobler, G.; Beer, M. Exploring the Reservoir Hosts of Tick-Borne Encephalitis Virus. Viruses 2019, 11, 669. [Google Scholar] [CrossRef] [PubMed]
- Tomori, O.; Oluwayelu, D.O. Domestic Animals as Potential Reservoirs of Zoonotic Viral Diseases. Annu. Rev. Anim. Biosci. 2023, 11, 33–55. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Reisen, W.K. Present and future arboviral threats. Antivir. Res. 2010, 85, 328–345. [Google Scholar] [CrossRef]
- Agboli, E.; Zahouli, J.B.Z.; Badolo, A.; Jöst, H. Mosquito-Associated Viruses and Their Related Mosquitoes in West Africa. Viruses 2021, 13, 891. [Google Scholar] [CrossRef] [PubMed]
- Sattler, R.A.; Paessler, S.; Ly, H.; Huang, C. Animal Models of Lassa Fever. Pathogens 2020, 9, 197. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Barrett, A.D.T. Transmission cycles, host range, evolution and emergence of arboviral disease. Nat. Rev. Microbiol. 2004, 2, 789–801. [Google Scholar] [CrossRef]
- Ogunlade, S.T.; Meehan, M.T.; Adekunle, A.I.; Rojas, D.P.; Adegboye, O.A.; McBryde, E.S. A Review: Aedes-Borne Arboviral Infections, Controls and Wolbachia-Based Strategies. Vaccines 2021, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- De Silva, P.M.; Marshall, J.M. Factors Contributing to Urban Malaria Transmission in Sub-Saharan Africa: A Systematic Review. J. Trop. Med. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Portillo, A.; Palomar, A.M.; Santibáñez, P.; Oteo, J.A. Epidemiological Aspects of Crimean-Congo Hemorrhagic Fever in Western Europe: What about the Future? Microorganisms 2021, 9, 649. [Google Scholar] [CrossRef] [PubMed]
- Colpitts, T.M.; Conway, M.J.; Montgomery, R.R.; Fikrig, E. West Nile Virus: Biology, Transmission, and Human Infection. Clin. Microbiol. Rev. 2012, 25, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Akhmetzhanov, A.R.; Asai, Y.; Nishiura, H. Quantifying the seasonal drivers of transmission for Lassa fever in Nigeria. Philos. Trans. R. Soc. B: Biol. Sci. 2019, 374, 20180268. [Google Scholar] [CrossRef] [PubMed]
- Caminade, C.; McIntyre, K.M.; Jones, A.E. Impact of recent and future climate change on vector-borne diseases. Ann. N. Y. Acad. Sci. 2018, 1436, 157–173. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.J.; Carlson, C.J.; Mordecai, E.A.; Johnson, L.R. Global expansion and redistribution of Aedes-borne virus transmission risk with climate change. PLoS Negl. Trop. Dis. 2019, 13, e0007213. [Google Scholar] [CrossRef] [PubMed]
- Salimi, H.; Cain, M.D.; Klein, R.S. Encephalitic Arboviruses: Emergence, Clinical Presentation, and Neuropathogenesis. Neurotherapeutics 2016, 13, 514–534. [Google Scholar] [CrossRef]
- Monath, T.P.; Vasconcelos, P.F. Yellow fever. J. Clin. Virol. 2015, 64, 160–173. [Google Scholar] [CrossRef]
- Braack, L.; De Almeida, A.P.G.; Cornel, A.J.; Swanepoel, R.; De Jager, C. Mosquito-borne arboviruses of African origin: review of key viruses and vectors. Parasites Vectors 2018, 11, 1–26. [Google Scholar] [CrossRef]
- Counotte, M.J.; Kim, C.R.; Wang, J.; Bernstein, K.; Deal, C.D.; Broutet, N.J.N.; Low, N. Sexual transmission of Zika virus and other flaviviruses: A living systematic review. PLOS Med. 2018, 15, e1002611. [Google Scholar] [CrossRef]
- Trivedi, S.; Chakravarty, A. Neurological Complications of Dengue Fever. Curr. Neurol. Neurosci. Rep. 2022, 22, 515–529. [Google Scholar] [CrossRef]
- Thiberville, S.-D.; Moyen, N.; Dupuis-Maguiraga, L.; Nougairede, A.; Gould, E.A.; Roques, P.; de Lamballerie, X. Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy. Antivir. Res. 2013, 99, 345–370. [Google Scholar] [CrossRef]
- Akinsulie, O.C.; Adesola, R.O.; Bakre, A.; Adebowale, O.O.; Adeleke, R.; Ogunleye, S.C.; Oladapo, I.P. Usutu virus: An emerging flavivirus with potential threat to public health in Africa: Nigeria as a case study. Front. Veter- Sci. 2023, 10, 1115501. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.-S.; Lee, H.-C.; Lee, K.-M.; Gong, Y.-N.; Shih, S.-R. Enterovirus and Encephalitis. Front. Microbiol. 2020, 11, 261. [Google Scholar] [CrossRef] [PubMed]
- Greening, G.E.; Cannon, J.L. Human and Animal Viruses in Food (Including Taxonomy of Enteric Viruses). Viruses in Foods 2016, 5–57. [Google Scholar] [CrossRef]
- Mbonye, A.; Wamala, J.; Nanyunja, M.; Opio, A.; Makumbi, I.; Aceng, J. Ebola Viral Hemorrhagic Disease Outbreak in West Africa- Lessons from Uganda. Afr. Heal. Sci. 2014, 14, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Buseh, A.G.; Stevens, P.E.; Bromberg, M.; Kelber, S.T. The Ebola epidemic in West Africa: Challenges, opportunities, and policy priority areas. Nurs. Outlook 2014, 63, 30–40. [Google Scholar] [CrossRef] [PubMed]
- E Rohde, R.; E Rupprecht, C. Update on lyssaviruses and rabies: will past progress play as prologue in the near term towards future elimination? Fac. Rev. 2020, 9. [Google Scholar] [CrossRef]
- Fooks, A.R.; Cliquet, F.; Finke, S.; Freuling, C.; Hemachudha, T.; Mani, R.S.; Müller, T.; Nadin-Davis, S.; Picard-Meyer, E.; Wilde, H.; et al. Rabies. Nat. Rev. Dis. Prim. 2017, 3, 17091. [Google Scholar] [CrossRef]
- Rupprecht, C.E.; Mani, R.S.; Mshelbwala, P.P.; Recuenco, S.E.; Ward, M.P. Rabies in the Tropics. Curr. Trop. Med. Rep. 2022, 9, 28–39. [Google Scholar] [CrossRef]
- Johns Hopkins Medicine. Encephalitis. Available online: https://www.hopkinsmedicine.org/health/conditions-and-diseases/encephalitis#:~:text=The%20most%20common%20causes%20of,enteroviruses%2C%20which%20cause%20gastrointestinal%20illness (accessed on 7 May 2023).
- Perlejewski, K.; Bukowska-Ośko, I.; Rydzanicz, M.; Pawełczyk, A.; Cortѐs, K.C.; Osuch, S.; Paciorek, M.; Dzieciątkowski, T.; Radkowski, M.; Laskus, T. Next-generation sequencing in the diagnosis of viral encephalitis: sensitivity and clinical limitations. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K. Estimation of the number of nucleotide substitutions when there are strong transition-transversion and G+C-content biases. Mol. Biol. Evol. 1992, 9, 678–687. [Google Scholar] [CrossRef]
- Saitou, N.; Nei, M. The neighbor-joining method: a new method for reconstructing evolutionary trees. Mol. Biol. Evol. 1987, 4, 406–425. [Google Scholar] [CrossRef]
- Felsenstein, J. Confidence limits on phylogenies: An approach using the bootstrap. Evolution 1985, 39, 783–791. [Google Scholar] [CrossRef]
- Kumari, R.; Sharma R., S.; Raina V., K.; Chauhan, L. Role of integrated vector management for prevention and control of Japanese encephalitis/acute encephalitis syndrome (JE/AES) – a review. J. Commun. Dis. 2014, 46, 93–108. [Google Scholar]
- Kilpatrick, A.M.; Randolph, S.E. Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. Lancet 2012, 380, 1946–1955. [Google Scholar] [CrossRef] [PubMed]
- Medlock, J.M.; Leach, S.A. Effect of climate change on vector-borne disease risk in the UK. Lancet Infect. Dis. 2015, 15, 721–730. [Google Scholar] [CrossRef]
- Paz, S.; Malkinson, D.; Green, M.S.; Tsioni, G.; Papa, A.; Danis, K.; Sirbu, A.; Ceianu, C.; Katalin, K.; Ferenczi, E.; et al. Permissive Summer Temperatures of the 2010 European West Nile Fever Upsurge. PLOS ONE 2013, 8, e56398. [Google Scholar] [CrossRef]
- Kinney, R.M.; Huang, C.Y.-H.; Whiteman, M.C.; Bowen, R.A.; Langevin, S.A.; Miller, B.R.; Brault, A.C. Avian virulence and thermostable replication of the North American strain of West Nile virus. J. Gen. Virol. 2006, 87, 3611–3622. [Google Scholar] [CrossRef]
- Kilpatrick, A.M.; Meola, M.A.; Moudy, R.M.; Kramer, L.D. Temperature, Viral Genetics, and the Transmission of West Nile Virus by Culex pipiens Mosquitoes. PLOS Pathog. 2008, 4, e1000092. [Google Scholar] [CrossRef]
- Paz, S.; Albersheim, I. Influence of Warming Tendency on Culex pipiens Population Abundance and on the Probability of West Nile Fever Outbreaks (Israeli Case Study: 2001–2005). Ecohealth 2008, 5, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Landesman, W.J.; Allan, B.F.; Langerhans, R.B.; Knight, T.M.; Chase, J.M. Inter-Annual Associations Between Precipitation and Human Incidence of West Nile Virus in the United States. Vector-Borne Zoonotic Dis. 2007, 7, 337–343. [Google Scholar] [CrossRef]
- Takeda, T.; A Whitehouse, C.; Brewer, M.; Gettman, A.D.; Mather, T.N. Arbovirus surveillance in Rhode Island: assessing potential ecologic and climatic correlates. J. Am. Mosq. Control Assoc. 2003, 19, 179–189. [Google Scholar] [PubMed]
- Campbell, G.L.; A Marfin, A.; Lanciotti, R.S.; Gubler, D.J. West Nile virus. Lancet Infect. Dis. 2002, 2, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Trawinski, P.; MacKay, D. Meteorologically Conditioned Time-Series Predictions of West Nile Virus Vector Mosquitoes. Vector-Borne Zoonotic Dis. 2008, 8, 505–522. [Google Scholar] [CrossRef]
- Meegan, J.M.; Bailey, C.L. Rift Valley fever. In The Arboviruses: Epidemiology and Ecology; Monath, T.P., Ed.; CRC Press: Boca Raton, FL, USA, 1988; Volume 4, pp. 51–76. [Google Scholar]
- Glancey, M.M.; Anyamba, A.; Linthicum, K.J. Epidemiologic and Environmental Risk Factors of Rift Valley Fever in Southern Africa from 2008 to 2011. Vector-Borne Zoonotic Dis. 2015, 15, 502–511. [Google Scholar] [CrossRef]
- Chretien, J.-P.; Sergon, K.; Sang, R.; Breiman, R.F.; Anyamba, A.; Bedno, S.A.; Linthicum, K.J.; Tucker, C.J.; Small, J.; Onyango, C.O.; et al. DROUGHT-ASSOCIATED CHIKUNGUNYA EMERGENCE ALONG COASTAL EAST AFRICA. Am. J. Trop. Med. Hyg. 2007, 76, 405–407. [Google Scholar] [CrossRef]
- Bongaarts, J.; John, B.; R, J.; A, D.; A, B.; H, G.; T, G.; W, L.; S, K.; J, S.; et al. Human population growth and the demographic transition. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 2985–2990. [Google Scholar] [CrossRef]
- United Nations. World Population Prospects, the 2012 revision. United Nations Department of Economic & Social Affairs, Population Division, New York, 2013. p. xxi + 94.
- Bryant, J.E.; Holmes, E.C.; Barrett, A.D.T. Out of Africa: A Molecular Perspective on the Introduction of Yellow Fever Virus into the Americas. PLOS Pathog. 2007, 3, e75. [Google Scholar] [CrossRef]
- Gratz, N.G. Critical review of the vector status of Aedes albopictus. Med Veter- Èntomol. 2004, 18, 215–227. [Google Scholar] [CrossRef]
- Benedict, M.Q.; Levine, R.S.; Hawley, W.A.; Lounibos, L.P. Spread of The Tiger: Global Risk of Invasion by The MosquitoAedes albopictus. Vector-Borne Zoonotic Dis. 2007, 7, 76–85. [Google Scholar] [CrossRef]
- Brown, C.R.; O'Brien, V.A. Are Wild Birds Important in the Transport of Arthropod-borne Viruses? Ornithol. Monogr. 2011, 71, 1–64. [Google Scholar] [CrossRef]
- Charrel, R.N.; de Lamballerie, X.; Raoult, D. Chikungunya Outbreaks — The Globalization of Vectorborne Diseases. N. Engl. J. Med. 2007, 356, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Poulakou, G.; Plachouras, D. Planet’s population on the move, infections on the rise. Intensiv. Care Med. 2016, 42, 2055–2058. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T. Control of Japanese Encephalitis — Within Our Grasp? N. Engl. J. Med. 2006, 355, 869–871. [Google Scholar] [CrossRef] [PubMed]
- Buckley, A.; Dawson, A.; Moss, S.R.; Hinsley, S.A.; Bellamy, P.E.; Gould, E.A. Serological evidence of West Nile virus, Usutu virus and Sindbis virus infection of birds in the UK. J. Gen. Virol. 2003, 84, 2807–2817. [Google Scholar] [CrossRef] [PubMed]
- OIE Technical Disease Cards. Japanese encephalitis. 2013. http://www.oie.int/fileadmin/Home/eng/Animal_Health_in_the_World/docs/pdf/Disease_cards/JAPANESE_ENCEPHALITIS.pdf.
- Oliveira, A.R.S.; Cohnstaedt, L.W.; Cernicchiaro, N. Japanese Encephalitis Virus: Placing Disease Vectors in the Epidemiologic Triad. Ann. Èntomol. Soc. Am. 2018, 111, 295–303. [Google Scholar] [CrossRef]
- Rosen, L. Further Observations on the Mechanism of Vertical Transmission of Flaviviruses by Aedes Mosquitoes. Am. J. Trop. Med. Hyg. 1988, 39, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Leake, C. Arbovirus-mosquito interactions and vector specificity. Parasitol. Today 1992, 8, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Reisen, W.K.; Fang, Y.; Martinez, V.M. Effects of temperature on the transmission of west nile virus by Culex tarsalis (Diptera: Culicidae). J. Med. Entomol. 2006, 43, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.C.; Maharaj, P.D.; Reisen, W.K.; Brault, A.C. North American West Nile virus genotype isolates demonstrate differential replicative capacities in response to temperature. J. Gen. Virol. 2011, 92, 2523–2533. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R.P.; Hardy, J.L.; Reisen, W.K. Diel Changes in Adult Mosquito Microhabitat Temperatures and Their Relationship to the Extrinsic Incubation of Arboviruses in Mosquitoes in Kern County, California. J. Med. Èntomol. 1990, 27, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.O.; Chaves, L.F.; Hamer, G.L.; Sun, T.; Brown, W.M.; Walker, E.D.; Haramis, L.; Goldberg, T.L.; Kitron, U.D. Local impact of temperature and precipitation on West Nile virus infection in Culex species mosquitoes in northeast Illinois, USA. Parasites Vectors 2010, 3, 19. [Google Scholar] [CrossRef]
Figure 1.
Map of Africa showing the percentage distribution of Viral Encephalitis in West African countries (Benin, Burkina Faso, Ghana, Guinea, Ivory coast, Mali, Nigeria, Senegal, Sierra Leone, The Gambia, and Togo) between 2014-2022. Six arboviruses causing encephalitis such as WNV, JEV, ZIKV, CHIKV, YFV, and RVFV and twelve non-arboviruses such as Herpes simplex virus types 1 and 2, Varicella-zoster virus, Enteroviruses, La Crosse virus, St. Louis virus, Equine viruses, Powassan virus, Epstein-Barr virus, Rabies virus, Cytomegalovirus, Ebola virus, and Lassa virus were considered were considered across seventeen (17) West African countries. Adapted from (32).
Figure 1.
Map of Africa showing the percentage distribution of Viral Encephalitis in West African countries (Benin, Burkina Faso, Ghana, Guinea, Ivory coast, Mali, Nigeria, Senegal, Sierra Leone, The Gambia, and Togo) between 2014-2022. Six arboviruses causing encephalitis such as WNV, JEV, ZIKV, CHIKV, YFV, and RVFV and twelve non-arboviruses such as Herpes simplex virus types 1 and 2, Varicella-zoster virus, Enteroviruses, La Crosse virus, St. Louis virus, Equine viruses, Powassan virus, Epstein-Barr virus, Rabies virus, Cytomegalovirus, Ebola virus, and Lassa virus were considered were considered across seventeen (17) West African countries. Adapted from (32).
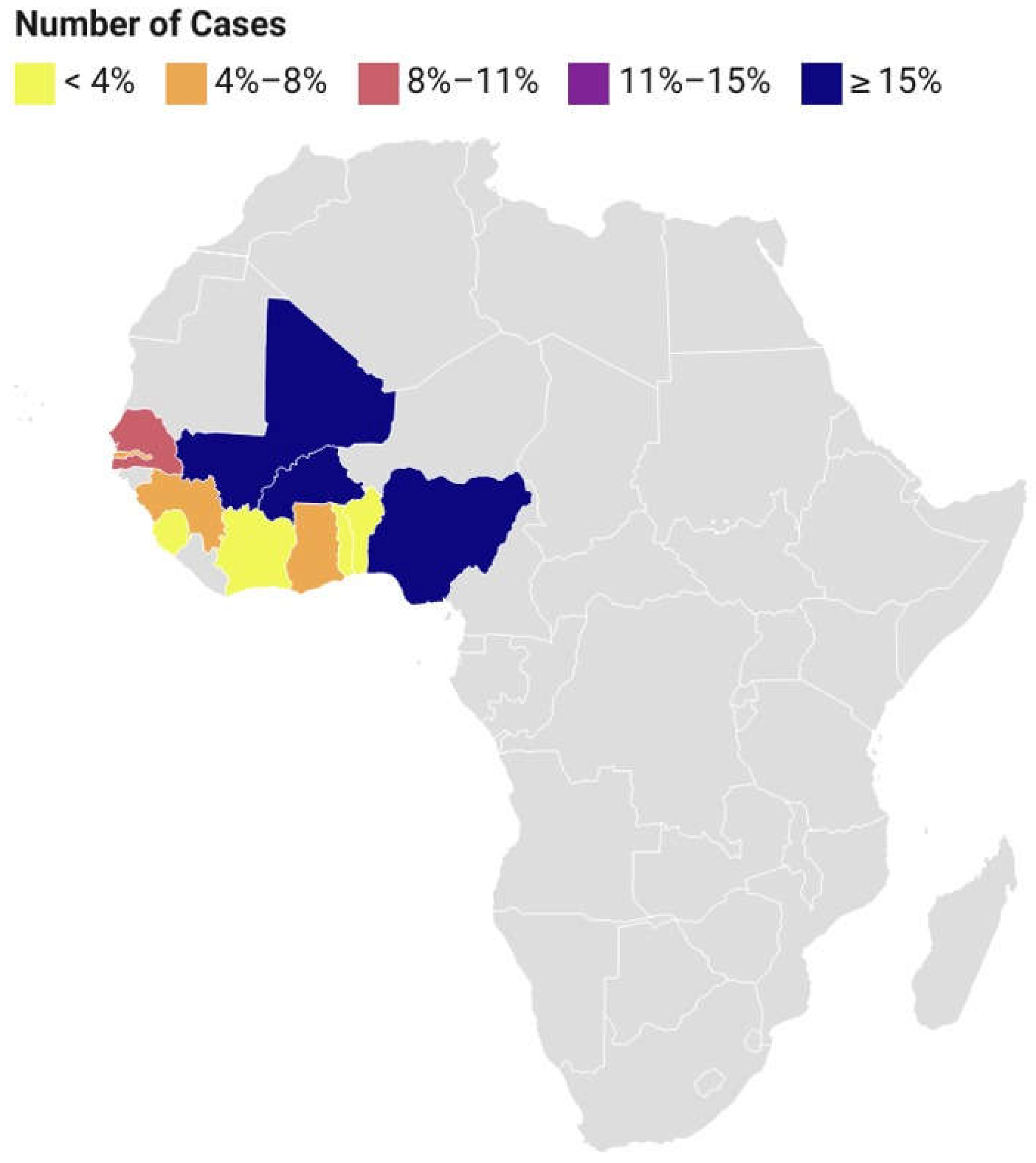
Figure 2.
Phylogenetic trees showing the relatedness of Athropod borne (A) and Non-arthropod-borne (B) Viral Encephalitis in West Africa. Whole genome sequence of the viruses was downloaded from the GenBank across the countries in West Africa. Countries with partial sequences were not considered, hence excluding some countries from the tree. FASTA files of all the sequences were downloaded and aligned using BioEdit 7.2 software. The phylogenetic tree was constructed using MEGA 11 software. Based on the Tamura 3-parameter model, the evolutionary history of each virus was determined using the Maximum Likelihood technique (34). The corresponding taxa’s number of clustered trees is displayed next to the branches. The process of creating the trees involved applying the neighbor-joining (35) and BioNJ algorithms to pairwise distance matrices calculated using the Maximum Composite Likelihood (MCL) technique (36), and then choosing the topology with the highest log likelihood value. About 1000 repeats of bootstrap values were used to evaluate the phylogenetic groupings' robustness (36). With branch lengths calculated as the number of substitutions per site, trees were scaled in their representation. Data garnered from (32) .
Figure 2.
Phylogenetic trees showing the relatedness of Athropod borne (A) and Non-arthropod-borne (B) Viral Encephalitis in West Africa. Whole genome sequence of the viruses was downloaded from the GenBank across the countries in West Africa. Countries with partial sequences were not considered, hence excluding some countries from the tree. FASTA files of all the sequences were downloaded and aligned using BioEdit 7.2 software. The phylogenetic tree was constructed using MEGA 11 software. Based on the Tamura 3-parameter model, the evolutionary history of each virus was determined using the Maximum Likelihood technique (34). The corresponding taxa’s number of clustered trees is displayed next to the branches. The process of creating the trees involved applying the neighbor-joining (35) and BioNJ algorithms to pairwise distance matrices calculated using the Maximum Composite Likelihood (MCL) technique (36), and then choosing the topology with the highest log likelihood value. About 1000 repeats of bootstrap values were used to evaluate the phylogenetic groupings' robustness (36). With branch lengths calculated as the number of substitutions per site, trees were scaled in their representation. Data garnered from (32) .
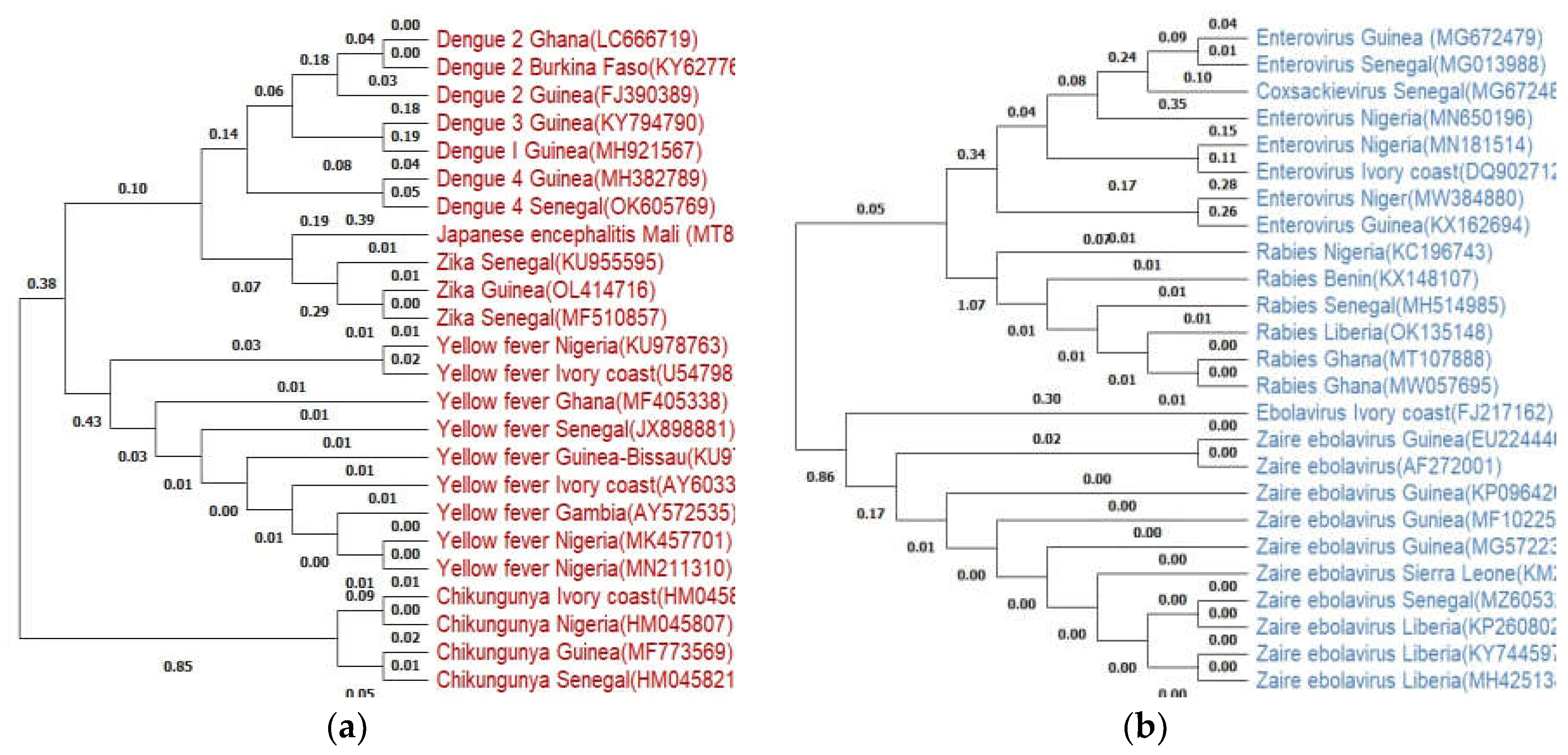
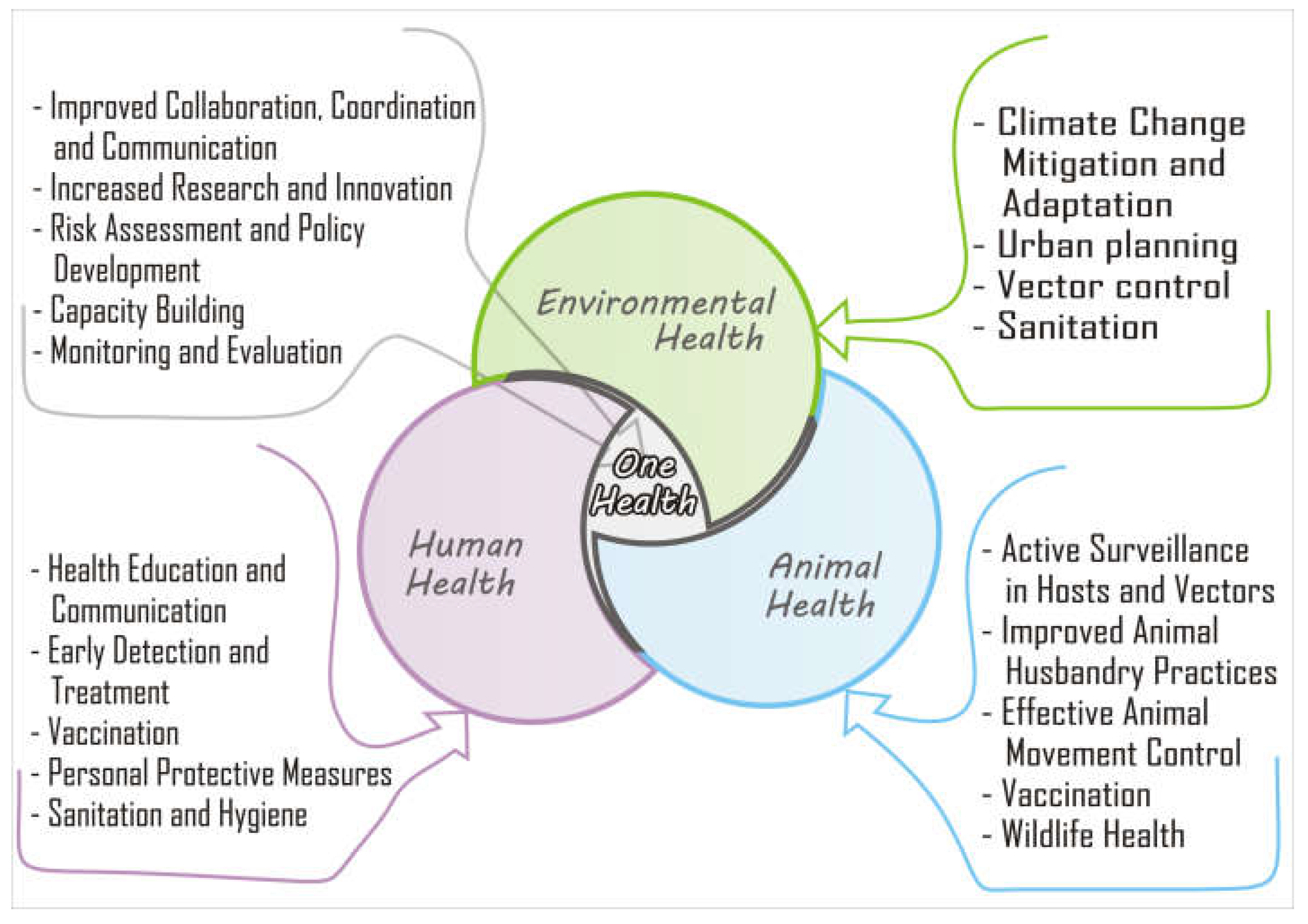
Figure 3.
A schematic description of the One-Health triad including human, animal, and environmental health. The integrated “One” health system approach, combining surveillance, vaccination, vector control, and community engagement, could be effective in preventing viral encephalitis in West Africa.
Figure 3.
A schematic description of the One-Health triad including human, animal, and environmental health. The integrated “One” health system approach, combining surveillance, vaccination, vector control, and community engagement, could be effective in preventing viral encephalitis in West Africa.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



