
Submitted:
01 June 2023
Posted:
02 June 2023
You are already at the latest version
Abstract
Background. Minimally invasive surgery via right mini-thoracotomy has become the standard of care for the treatment of mitral valve disease worldwide, particularly at high volume centers. In recent years, the spectrum of indications has progressively shifted and extended to fragile and higher risk patients, also addressing more complex mitral valve disease and ultimately including patients with native or prosthetic infective endocarditis. The rationale for the adoption of the minimally invasive approach is to minimize the surgical trauma, promote an earlier postoperative recovery and reduce the incidence of surgical wound infection and other nosocomial infections. The aim of this retrospective observational study is to evaluate the effectiveness and the early and late outcome in patients undergoing minimally invasive surgery for mitral valve infective endocarditis.
Methods. Prospectically collected data regarding minimally invasive surgery in patients with mitral valve infective endocarditis were entered into a dedicated database for the period between January 2007 and December 2022 and retrospectively analyzed. All comers during the study period underwent a preoperative evaluation based upon clinical history and anatomy for the allocation to the most appropriate surgical strategy. Selection for the mini-thoracotomy approach was primarily driven by a thorough transthoracic and especially transesophageal echocardiographic evaluation, coupled with total body and vascular imaging.
Results. During the study period, 92 patients underwent right mini-thoracotomy to treat native (80/92, 87%) or prosthetic (12/92, 13%) mitral valve endocarditis at our institution, representing 5% of the patients undergoing minimally invasive mitral surgery. Twenty-six (28%) patients had undergone previous cardiac operations, whereas 18 (20%) presented preoperatively with complications related to endocarditis, most commonly systemic embolization. Sixty-nine and 23 patients, respectively, underwent early surgery (75%) or were operated on after the completion of targeted antibiotic treatment (25%). A conservative procedure was feasible in 16/80 (20%) patients with native valve endocarditis. Conversion to standard sternotomy was necessary in a single case (1.1%). No cases of intraoperative iatrogenic aortic dissection were reported. Four patients died perioperatively, accounting for a thirty-day mortality of 4.4%. Causes of death were refractory heart or multiorgan failure and/or septic shock. New onset stroke was observed postoperatively in one case (1.1%). Overall actuarial survival rate at 1 and 5 years after operation was 90.8% and 80.4%, whereas freedom from mitral valve reoperation at 1 and 5 years was 96.3% and 93.2%, respectively.
Conclusions. The present study shows good early and long-term results in higher-risk patients undergoing minimally invasive surgery for mitral valve infective endocarditis. Total body, vascular and echocardiographic screening represent the key points to select the optimal approach and allow the extension of indications for minimally invasive surgery to sicker patients, including active endocarditis and sepsis.
Keywords:
mitral valve
; infective endocarditis
; minimally invasice cardiac surgery
; mini-thoracotomy
; cardiac reoperation
; prosthetic valve endocarditis
; systemic embolization
1. Introduction
Minimally invasive surgery has become the standard of care for the treatment of mitral valve (MV) disease at many institutions worldwide. Compared to traditional median full sternotomy, equivalence in terms of safety, efficacy, and durability of operations carried out via the right mini-thoracotomy has been widely documented with increasing favor for this approach by the cardiac surgical community. Non-inferiority of the former aspects are coupled by a better outcome in terms of postoperative pain, a lower rate of transfusions and reoperation for bleeding, improved cosmesis, shorter hospital length of stay and time to return to normal activity or work, and a lower need for rehabilitation resources at discharge [1–5]. As a consequence, especially at high volume institutions, the spectrum of indications has progressively shifted toward more fragile and higher risk patients allowing to apply the minimally invasive approach also to MV disease of increasing complexity, ultimately including patients with MV infective endocarditis (IE).
Surgical treatment in patients with IE is required in more than 50% of cases to prevent severe complications, most typically heart failure, uncontrolled infection, and systemic embolism [6,7]. US and European guidelines strongly recommend early intervention when surgery is needed. The evolution in the planning of an earlier surgical procedure, coupled with advances in intensive care and postoperative management have dramatically improved outcomes in these patients. However, the rate of perioperative mortality and morbidity are still consistently high [6,7].
The rationale for the adoption of the minimally invasive approach in these higher risk patients is to minimize the surgical trauma, thus promoting a quicker recovery after the operation, and reduce the rate of surgical wound infection and other hospital-related infections.
The aim of this retrospective observational study is to evaluate effectiveness and the early and late outcome in patients undergoing minimally invasive MV surgery for IE.
2. Methods
2.1. Study design and patients’ selection
Data regarding minimally invasive surgery in patients with MV IE were prospectively entered into a dedicated database for the period between January 2007 and December 2022. All patients described in our series met the modified Duke criteria for IE [8]. All comers during the study period underwent a preoperative evaluation based upon clinical history and anatomy for the allocation to the most appropriate surgical setting.
Selection for the mini-thoracotomy approach was primarily driven by a thorough transthoracic and especially transesophageal echocardiographic evaluation. Although less invasive approaches have been extended to treat multiple left sided valve disease in recent years, any suspicion of even minimal aortic valve involvement by the IE mandates a contraindication for the minimally invasive approach at our institution. Hence, in this clinical scenario, patients were scheduled for conventional full sternotomy to allow, if indicated, treatment of associated lesions and extensive inspection of the aortic valve and aorto-mitral curtain. Besides, more than mild aortic valve regurgitation and severe or extreme pleural adhesions of the right lung following prior thoracic operations are to be considered major if not absolute exclusion criteria for the minimally invasive approach, irrespective of IE. Finally, patients operated on an emergency basis with cardiogenic shock were addressed via median sternotomy.
In case of previous cardiac surgical procedures the endoaortic balloon setting was used in most cases to avoid tedious and near-blind dissection of adhesions to free the ascending aorta for cross-clamping. However, this was not always feasible, most typically in the case of a dilated ascending aorta, i.e., with a maximum diameter above 40 mm, or in the presence of moderate or severe tortuosity of the infrarenal aorta and ileofemoral axes. A small caliber of the common femoral vessels (<7 mm) also renders impractical the use of the endoballon, which requires the insertion of a 21F of 23F arterial perfusion cannula with a side branch for the insertion of the balloon itself, implying in these cases transthoracic clamping with a Chitwood or, more recently, a Cygnet type aortic clamp (see below). Besides, in case of severe tortuous and/or atheromatous abdominal aortoiliac and femoral vessels, the antegrade perfusion via the axillary artery with transthoracic clamping was predominantly preferred to minimize the hazards of systemic embolization and stroke related to retrograde perfusion. In this respect, a rigorous peripheral vascular screening with computerized tomography scan or aortography and ileofemoral angiography or a combination of imaging techniques became routine in our clinical practice since 2009 [9,10].
The selection of one setting with respect to the others was patient oriented and independent from the learning curve. Long-term outcomes were obtained through regular postoperative follow-up at the outpatient clinic, telephone interviews, or both. Early surgery relates to the course of IE and, more specifically, to operations carried out at any time during the course of antibiotic treatment [11]. Postoperative stroke was defined as clinical signs persisting at the time of discharge from the hospital and/or in the presence of localized ischemic infarcts detectable by conventional neuroimaging techniques. In relation to late follow-up, adverse events analyzed as primary outcomes in the present study were death from any cause and MV reoperation. The cause of reoperation, i.e., recurrent IE or not was also analyzed as a secondary outcome.
2.2. Surgical technique
The right mini-thoracotomy approach, perfusion strategies and aortic clamping techniques used for patients undergoing MV surgery have been described previously Figure 1 [9,10,12–15]. Briefly, a right anterolateral mini-thoracotomy in the fourth intercostal space is performed and double lumen endotracheal tube intubation for the single left lung ventilation is provided in all patients. More posteriorly, a secondary port is prepared for the endoscope and for carbon dioxide insufflation. An additional sixth intercostal space port is created for pump suction. After the institution of cardiopulmonary bypass, core temperature is lowered to 30 °C. Arterial perfusion is gained with a peripheral femoral or axillary cannulation. The latter is usually preferred to provide antegrade systemic perfusion in the case of severe atherosclerotic burden [12]. Venous drainage is obtained via double femoral and jugular cannulation. All cannulae are inserted with a Seldinger technique, either under direct vision in case of vascular surgical exposure or percutaneously. The ascending aorta is clamped using the endoaortic balloon or a trans-thoracic clamp. In the endoaortic clamping setting, aortic occlusion and cardioplegia delivery are gained with a balloon catheter inserted through the sidearm of a femoral arterial cannula (21F or 23F Intraclude®, Edwards Lifesciences, Irvine, CA, USA). In the trans-thoracic clamping setting the clamp is addressed towards the ascending aorta through the first intercostal space with a Chitwood clamp or through the main port with a Cygnet® flexible clamp. Cardioplegia is delivered with a 7F cardioplegia needle (CalMed Technologies, Santa Inez, CA, USA) placed into the proximal ascending aorta. Antegrade myocardial protection is provided with St. Thomas (PlegisolTM, Hospira Inc., Lake Forest, IL, USA) or Custodiol (Bretschneider histidine, tryptophan, ketoglutarate solution, Köhler Chemie, Bensheim, Germany) cold crystalloid cardioplegia [14]. Superior and inferior vena cava snaring is obtained by placing tourniquets around the vessels or by placing endovascular balloons to provide a temporary mini right atriotomy to drain the cardioplegic solution and in patients requiring associated right atrial procedures, most commonly tricuspid valve repair. The MV is exposed through a standard left atriotomy, parallel and posterior to the interatrial septum. The extension of vegetations, leaflet involvement and the chances of valve repair are assessed. Clamp release is obtained at a core temperature above 33 ◦C during rewarming. Intraoperative transesophageal echocardiography is mandatory and was used in all patients to guide the correct positioning of the cannulae before the onset of cardiopulmonary bypass and to assess cardiac function, residual MV regurgitation in case of MV repair, paravalvular leaks, and prosthetic valve gradients after the intracardiac phase of the operation.
2.3. Statistical analysis
Categorical and continuous, either normally distributed or skewed, variables are reported as n (%), mean ± standard deviation or median [interquartile range] as appropriate. The probability of adverse events over time was analyzed with the Kaplan-Meier method. Factors affecting a different probability of an adverse event were assessed with the log-rank test. P values <0.05 were considered statistically significant. SPSS® software package was used for statistical computations.
3. Results
During the study period, 1847 patients underwent minimally invasive MV surgery at our institution. Ninety-two (5%) the diagnosis and indication for operation was IE. Among these, 80/92 (87%) were native MV IE whereas the remaining 12/92 (13%) were prosthetic valve IE. Patients’ characteristics are summarized in Table 1. Mean age was 61.1 ± 12.7 years, and 34 patients were female (37%). Twenty-six patients (28%) had undergone one or more previous cardiac operations. Eighteen patients (20%) reported preoperative IE-related complications, namely, systemic embolic events in 13 cases, and heart failure in 5 cases. Sixty-nine (75%) patients underwent early MV surgery, whereas 13 (25%) patients were operated after the completion of antibiotic treatment. Overall, the estimated operative mortality applying the logistic EuroSCORE was 14.9%. Micro-organisms were identified on excised tissues at the time of surgery in 71 (77%) patients and were almost invariably Gram positive bacteria (Table 2).
Intraoperative and postoperative variables are reported in Table 3. Isolated MV surgery was performed in most of the cases (82/92, 89,%). Although IE most often precludes or renders MV repair unwise, a conservative procedure was possible in 16/80 (20%) patients with IE on the native MV. Retrograde systemic arterial perfusion via the femoral artery was performed in the vast majority of cases (85/92, 92%), whereas aortic cross-clamping was obtained with the endoluminar balloon in 40/92 (43%) and with a trans-thoracic clamp in 51 (55%) cases, respectively. The procedure was carried out without cardioplegic arrest on the fibrillating heart in one patient with multiple prior operations. Conversion to standard full sternotomy was necessary in a single patient (1.1%). No cases of iatrogenic intraoperative aortic dissection were observed.
Four patients died perioperatively, accounting for an operative thirty-day mortality of 4.4%. The causes of death were worsening heart or multiorgan failure, refractory sepsis or a combination of these conditions. Postoperative stroke was reported in a single case (1.1%).
Clinical follow-up was concluded in April 2023 and was 100% completed. Median follow-up was 98.1 months. Overall, Kaplan-Meier survival analysis outlined an actuarial survival rate at 1 and 5 years was 90.8% and 80.4%, respectively (Figure 2). Eight patients underwent redo MV surgery during follow-up. Surgical MV replacement was performed in 7 cases, whereas 1 patient received transcatheter valve-in-valve implantation to address bioprosthetic structural deterioration. Despite being an interventional procedure, the latter was considered an adverse MV event and was included in the reoperations. Recurrent IE was the indication for reoperation in 5 of 8 cases, with reoperations being performed respectively at 1, 10, 13, 23 and 85 months after the primary operation. Overall, the probability of freedom from reoperation at 1 and 5 years was 96.3% and 93.2%, respectively. Although only a single patient underwent reoperative surgery early (<6 months) after the primary operation, the probability of reoperation over time was significantly different in relation to the recurrence of infection or not (log-rank p < 0.0001). In fact, patients reoperated on for recurrent MV IE were treated significantly earlier than the remaining.
4. Discussion
Minimally invasive cardiac surgery has consistently evolved during the last years. To date, also complex valve diseases and high-risk subgroups of patients, such as those with IE, are routinely enrolled for operations through a right mini-thoracotomy approach in experienced heart valve centers [12,15].
According to current guidelines, early surgery for IE is essentially recommended in case of valve defects causing haemodynamic impairment, i.e., severe regurgitation, in the presence of uncontrolled infection and to prevent embolic events [6,7]. More in particular, early surgery has shown to be able to avoid progression of heart failure, to prevent irreversible structural valve damage that reduces or precludes the chances of successful repair on the MV, and to reduce the risks of IE recurrence and overall postoperative adverse events [16,17].
However, evidence in the literature highlights how, to date, a strict adherence to the recommendations is poorly applied in real-world clinical scenarios, and only one out of four patients with IE and a potential surgical indication is actually addressed surgically or evaluated for operation [6,18]. This low rate of referral to surgery can be partially explained when considering the poor prognosis in this kind of surgical subpopulation. Despite advances in prevention strategies, antimicrobial therapies, and surgical management, IE still remains associated with substantial mortality which ranges between 10% and 20% even in recent reports from high volume centers [6,19–21].
The right mini-thoracotomy approach is able to minimize the surgical trauma, to reduce the risk of re-entry injuries in case of IE in previous cardiac surgeries, to accelerate patient’s recovery and to reduce the rate of wounds and other hospital-related infections in this subgroup of high-risk patients. After 15-year experience, the right mini-thoracotomy approach has become the standard of care for treating mitral and tricuspid IE in selected patients at our center. Previously, we reported worthy results in terms of feasibility and safety of the minimally invasive setting in case of MV IE [22]. The present study, on nearly 100 high-risk patients – mean logistic EuroSCORE 14.5%, almost 30% of redo procedures, and nearly 20% of patients with preoperative IE-related complications, namely, embolic events or heart failure – highlights good early and long-term outcomes with a 4.4% 30-day mortality, a 1% of stroke rate and a median intensive care unit and hospital length of stay of 1 and 7 days respectively. Our mortality rate and postoperative outcomes are lower than estimated with the EuroSCORE and, more importantly, below recent data reported in the current literature. A recent systematic review on minimally invasive surgery for MV IE reports an average in-hospital mortality of 9.4%, a stroke rate of 2.3%, and an average length of hospital stay of 21.6 days, whereas reoperation during follow-up was required in 9.3% of cases [23,24].
At follow-up, reoperation was dictated by recurrent IE in 5 (5.4%) cases for, but only 1 patient was reoperated on very early, 2 months after the primary operation, indicating that eradication of the primary infection was carried out in virtually all patients (91/92, 98,9%). Consequently, in carefully selected patients the minimally invasive approach dose not jeopardize the essence of surgical treatment of IE which imposes radical excision of all infected tissues. In this series the etiology of IE was most commonly related to Gram positive bacteria with a substantially equal prevalence of staphylococci and streptococci accounting for almost 50% of the population and a lower prevalence of enterococci. The pathogen could not be isolated and sterile cultures were observed in 21 (22.8%) patients, most likely indicating sensitivity to first line blind antibiotic therapy and, possibly, less virulent agents. Consequently, a potential bias versus patients’ selection for minimally invasive MV surgery might be hypothesized and eventually correlate with the favorable outcomes observed. Actually, staphylococcal IE, which typically presents with more severe sepsis and valve destruction, represented only one quarter of the population. Conversely, the prevalence of streptococcal culture negative IE and the related lower virulence may correlate with some probability to indicate MV repair in a subgroup of patients with native IE.
Admittedly, although we were able to address the majority of patients with MV IE, the minimally invasive approach was not employed in all cases, since patients with a suspicion of more extensive IE or operated on with an emergent or salvage indication, most commonly cardiogenic or septic shock, were addressed with conventional sternotomy. In parallel, the timing of the operation is of utmost importance. Despite a somewhat more aggressive timing is now recommended by the current guidelines, fixed indications are lacking. The severity of valve dysfunction, the ongoing infection and the hazards (or consequences) of embolization should always be balanced with the benefits of immediate surgery. Patients with systemic embolization represent a special challenge with respect to optimal timing. Embolic stroke, in particular, may be a true dilemma in relation to the hazards of heparinization and cerebral hemorrhage. In this respect, however, operations on cardiopulmonary bypass have been carried out with a relatively low risk of hemorrhagic infarction, anecdotally comprising conditions requiring deep hypothermia and circulatory arrest, such as aortic dissection complicated by cerebral malperfusion [25]. Thus, even in case of cerebral embolization, IE should be managed as early as possible, reserving a “wait and see” approach to patients with very large brain infarcts, ongoing intracranial hemorrhage and a very compromised cognitive or near comatose state. Conversely, in case of embolization to the visceral vessels, the most commonly involved site is the splenic territory. In the presence of very large and recent infarcts, prophylactic splenectomy, although not indicated per se, may be associated during surgery for IE. In this series, this scenario occurred in 2 cases. Besides, although the minimally invasive approach has been criticized with respect to the potential hazards of embolization and subtle cerebral emboli may be detected with high resolution neuroimaging techniques [26], the presence of IE does not appear a clinically relevant additional risk factor in our experience. In fact postoperative stroke was observed in a single case, indicating a very low incidence which is most likely unrelated to IE.
On the contrary, however, the uniqueness of the IE state is characterized by the derangement determined by the systemic infection itself, which includes acute or subacute cardiac dysfunction, a prolonged inflammatory state and additional toxicity related to antibiotic therapy with a consequently reduced multiorgan, especially hepatic and renal, functional reserve. In this scenario, it might be speculated that a minimally invasive approach, which may inherently reduce not only surgical trauma, but also additional activation of systemic inflammatory pathways, could possibly mitigate the hazards of intraoperative end-organ damage. In fact, despite this aspect is beyond the scope of this report and the sickest patients were excluded, the incidence of acute kidney injury necessitating postoperative dialysis was surprisingly low in this series (5/92, 5.5%). This could be explained by a relatively early timing of the operation in most of the cases and to near routine use of hemofiltration during cardiopulmonary bypass. Besides, particularly in case of reoperations, similar considerations may apply to the unnecessary and possibly harmful dissection of previous pericardial adhesions to minimize inflammation caused by surgical manipulation. In this respect, the usefulness of the endoaortic balloon for clamping and of filtration of the cardioplegic solution to avoid bicaval dissection and snaring cannot be overemphasized.
The favorable results reported in the present study outline how our current practice, based on long-standing experience with different and evolving modalities of minimal access settings for MV surgery, allows us to reach a satisfactory outcome while guiding the patient toward the safest approach [9,13]. A careful selection of the patient before skin incision is required: transoesophageal echocardiography is a mandatory tool to estimate the risk of embolization in relation to the size and, even more importantly, the mobility of the vegetations characterizing the IE process, to exclude aortic valve involvement, to define the likelihood of a conservative MV procedure and to exclude the involvement of perivalvular structures and abscesses. Angiography or vascular computerized tomography scan or both are mandatory for the diagnosis of peripheral vascular disease.
Despite encouraging outcome reported in the literature and recognized advantages, minimally invasive surgery for IE is currently still not widely adopted. Concerns have been expressed in relation to the challenges of the surgical learning curve which may compromise the effectiveness of the procedure or even the ability to achieve adequate valve repair, when feasible. Definitely, this should be taken into consideration when approaching more complex valve diseases in a program of minimally invasive surgery. Thus, we recommend to address increasingly demanding patients after a first phase of the learning curve to reach the encouraging results reported in the current literature.
5. Limitations
Apart from the inherent limitation of a retrospective observational study, the main drawbacks of our study are essentially the relatively small sample size and the lack of a comparison group. However, a comparative study with a standard sternotomy cohort at a single center with an advanced program of minimally invasive MV cardiac surgery is difficult if not impossible to realize because virtually all patients selected for the sternotomy approach present concomitant disease, e.g., in this clinical scenario associated aortic valve IE or coronary artery disease. Consequently, even a comparison with a historical group would be biased by changes in perioperative management and surgical experience occurring from a time period to another, and thus of little value.
6. Conclusions
The present study depicts encouraging early and long-term results in higher risk patients undergoing minimally invasive MV surgery for IE. Mandatory key points for a successful outcome are thorough echocardiographic assessment and peripheral vascular screening to optimize the selection of patients for the mini-thoracotomy approach and the timing of the operation to eradicate IE in the most favorable risk to benefit condition.
Author Contributions
Conceptualization, Cristina Barbero and Marco Pocar; Data curation, Dario Brenna, Barbara Parrella, Sara Baldarelli, Valentina Aloi, Alessandro Vairo and Gianluca Alunni; Formal analysis, Marco Pocar, Dario Brenna and Andrea Costamagna; Methodology, Cristina Barbero and Marco Pocar; Project administration, Mauro Rinaldi; Supervision, Cristina Barbero and Mauro Rinaldi; Validation, Marco Pocar; Visualization, Anna Trompeo and Stefano Salizzoni; Writing – original draft, Cristina Barbero; Writing – review & editing, Marco Pocar. All authors have read and agreed to the published version of the manuscript.
References
- Vollroth, M.; Seeburger, J.; Garbade, J.; Pfannmueller, B.; Holzhey, D.; Misfeld, M.; Borger, MA.; Mohr, FW. Minimally invasive mitral valve surgery is a very safe procedure with very low rates of conversion to full sternotomy. Eur. J. Cardiothorac. Surg. 2012, 42, e13-e16. [CrossRef]
- Modi, P.; Rodriguez, E.; Hargrove, WC III.; Hassan, A.; Szeto, WY.; Chitwood, WR Jr. Minimally invasive video-assisted mitral valve surgery: a 12-year, 2-center experience in 1178 patients. J. Thorac. Cardiovasc. Surg. 2009, 137, 1481-87.
- Seeburger, J.; Borger, MA.; Falk, V.; Kuntze, T.; Czesla, M.; Walther, T.; Doll, N.; Mohr, FW. Minimal invasive mitral valve repair for mitral regurgitation: results of 1339 consecutive patients. Eur. J. Cardiothorac. Surg. 2008, 34, 760-65. [CrossRef]
- Gammie, JS.; Zhao, Y.; Peterson, ED.; O’Brien, SM.; Rankin, JS.; Griffith, BP. J. Maxwell Chamberlain Memorial Paper for adult cardiac surgery. Less-invasive mitral valve operations: trends and outcomes from the Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2010, 90, 1401-08. [CrossRef]
- Toscano, A.; Barbero, C.; Capuano, P.; Costamagna, A.; Pocar, M.; Trompeo, A.; Pasero, D.; Rinaldi, M.; Brazzi, L. Chronic postsurgical pain and quality of life after right minithoracotomy mitral valve operations. J. Card. Surg. 2022, 37, 1585-90. [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, MJ.; Bongiorni, MG.; Casalta, JP.; Del Zotti, F.; et al. 2015 ESC Guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio- Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart. J. 2015, 36, 3075-128.
- Nishimura, RA.; Otto, CM.; Bonow, RO.; Carabello, BA.; Erwin, JP.; Guyton, RA.; et al. 2014 AHA/ACC guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and the Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2014, 63, e57-e185.
- Li, JS.; Sexton, DJ.; Mick, N.; Nettles, R.; Fowler, VG.; Ryan, T.; et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 2000, 30, 633-8. [CrossRef]
- Barbero, C.; Marchetto, G.; Ricci, D.; El Qarra, S.; Attisani, M.; Filippini, C.; et al. Minimal access mitral valve surgery: impact of tailored strategies on early outcome. Ann. Thorac. Surg. 2016, 102, 1989-94.
- Barbero, C.; Marchetto, G.; Ricci, D.; Cura Stura, E.; Clerici, A.; El Qarra, S.; et al. Steps forward in minimally invasive cardiac surgery: 10-year experience. Ann. Thorac. Surg. 2019, 108, 1822-9. [CrossRef]
- Thuny, F.; Grisoli, D.; Collart, F.; Habib, G.; Raoult, D. Management of infective endocarditis: challenges and perspectives. Lancet. 2012, 379, 965-75. [CrossRef]
- Barbero, C.; Pocar, M.; Marchetto, G.; Cura Stura, E.; Calia, C.; Boffini, M.; Rinaldi, M.; Ricci, D. Antegrade perfusion for mini-thoracotomy mitral valve surgery in patients with atherosclerotic burden. Heart. Lung. Circ. 2022, 31, 415-9. [CrossRef]
- Barbero, C.; Ricci, D.; El Qarra, S.; Marchetto, G.; Boffini, M.; Rinaldi, M. Aortic cannulation system for minimally invasive mitral valve surgery. J. Thorac. Cardiovasc. Surg. 2015, 149, 1669-72.
- Barbero, C.; Pocar, M.; Marchetto, G.; Cura Stura, E.; Calia, C.; Dalbesio, B.; Filippini, C.; Salizzoni, S.; Boffini, M.; Rinaldi, M.; et al. Single-dose St. Thomas versus Custodiol® cardioplegia for right mini-thoracotomy mitral valve surgery. J. Cardiovasc. Transl. Res. 2022, 16, 192-8.
- Barbero, C.; Spitaleri, A.; Pocar, M.; Parrella, B; Santonocito, A.; Bozzo, E.; Depaoli, A.; Faletti, R.; Rinaldi, M. Handling extensive mitral annular calcification via a minimally invasive right mini-thoracotomy approach. Appl. Sci. 2023, 13, 2563. [CrossRef]
- Funakoshi, S.; Kaji, S.; Yamamuro, A.; Tani, T.; Kinoshita, M.; Okada, Y.; et al. Impact of early surgery in the active phase on long term outcomes in left-sided native valve infective endocarditis. J. Thorac. Cardiovasc. Surg. 2011, 142, 836-42.
- Lalani, T.; Cabell, CH.; Benjamin, DK.; Lasca, O.; Naber, C.; Fowler, VG.; et al. Analysis of the impact of early surgery on in-hospital mortality of native valve endocarditis. Use of propensity score and instrumental variable methods to adjust for treatment-selection bias. Circulation. 2010, 121, 1005-13.
- Chu, VH.; Park, LP.; Athan, E.; Delahaye, F.; Freiberger, T.; Lamas, C.; et al. Association between surgical indications, operative risk, and clinical out- come in infective endocarditis: a prospective study from the international collaboration on endocarditis. Circulation. 2015, 131, 131-40.
- Perrotta, S.; Fröjd, V.; Lepore, V.; Schersten, H.; Jeppsson, A.; Svensson, G. Surgical treatment for isolated mitral valve endocarditis: a 16-year single-centre experience. Eur. J. Cardiothorac. Surg. 2018, 53, 576-81. [CrossRef]
- van der Merwe, J.; Casselman, F.; Stockman, B.; Roubelakis, A.; Vermeulen, Y.; Degrieck, I.; Van Praet, F. Endoscopic port access surgery for isolated atrioventricular valve endocarditis. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 487-93. [CrossRef]
- Folkmann, S.; Seeburger, J.; Garbade, J.; Schon, U.; Misfeld, M.; Mohr, FW.; Pfannmueller, B. Minimally invasive mitral valve surgery for mitral valve infective endocarditis. J. Thorac. Cardiovasc. Surg. 2018, 66, 525-9. [CrossRef]
- Barbero, C.; Marchetto, G.; Ricci, D.; Mancuso, S.; Boffini, M.; Cecchi, E.; De Rosa, FG.; Rinaldi, M. Minimal access surgery for mitral valve endocarditis. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 241-5. [CrossRef]
- Shih, E.; Squiers, JJ.; DiMaio, JM. Systematic review of minimally invasive surgery for mitral valve infective endocarditis. Innovations. 2021, 16, 244-8. [CrossRef]
- He, K.; Song, J.; Luo, H.; Su, H.; Liang, W.; Bian, L.; Yue, H.; Wu, Z. Valve replacement or repair in native mitral valve infective endocarditis – Which is better? A meta-analysis and systematic review. J. Card. Surg. 2022, 37, 1004-15. [CrossRef]
- Pocar, M.; Passolunghi, D.; Moneta, A.; Mattioli, R.; Donatelli, F. Coma might not preclude emergency operation in acute aortic dissection. Ann. Thorac. Surg. 2006, 81, 1348-51. [CrossRef]
- Barbero, C.; Rinaldi, M.; Marchetto, G.; Valentini, M.C.; Cura Stura, E.; Bosco, G.; Pocar, M.; Filippini, C.; Boffini, M.; Ricci, D. Magnetic resonance imaging for cerebral micro-embolizations during minimally invasive mitral valve surgery. J. Cardiovasc. Transl. Res. 2022, 15, 828-33. [CrossRef]
Figure 1.
Exposure of the mitral valve through a right mini-thoracotomy and endoscopic view. a. Example of a large vegetation on scallop A2 with leaflet perforation. b. Extensive resection of the anterior leaflet around the infected tissue. c. Mitral valve repair with patch on the anterior leaflet and ring annuloplasty.
Figure 1.
Exposure of the mitral valve through a right mini-thoracotomy and endoscopic view. a. Example of a large vegetation on scallop A2 with leaflet perforation. b. Extensive resection of the anterior leaflet around the infected tissue. c. Mitral valve repair with patch on the anterior leaflet and ring annuloplasty.
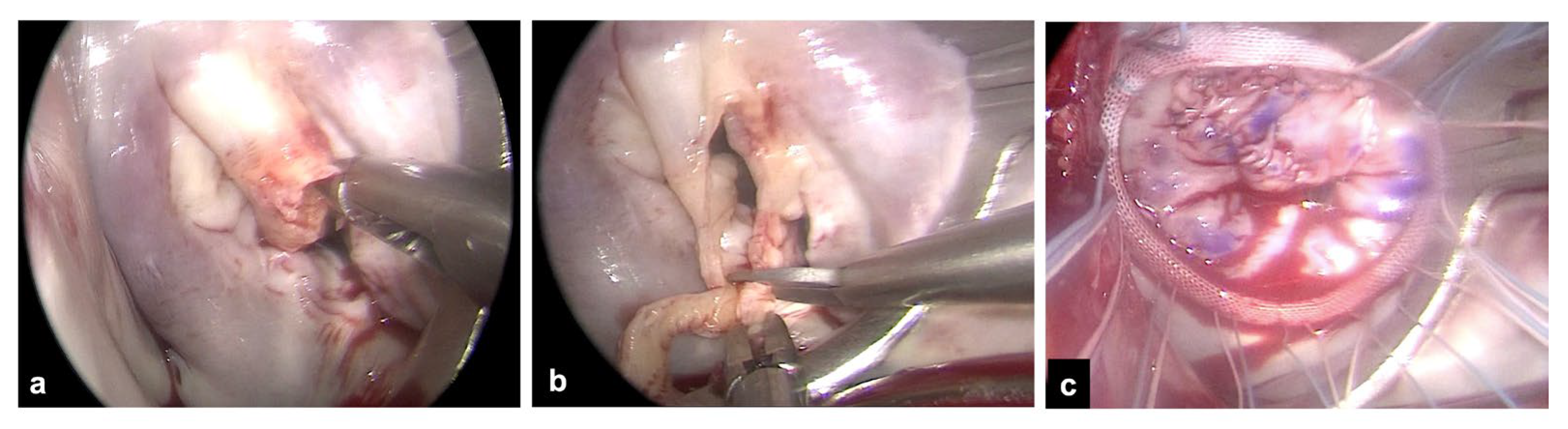
Figure 2.
a. Kaplan–Meier curve of survival probability. b. Freedom from MV reoperation according to diagnosis.
Figure 2.
a. Kaplan–Meier curve of survival probability. b. Freedom from MV reoperation according to diagnosis.
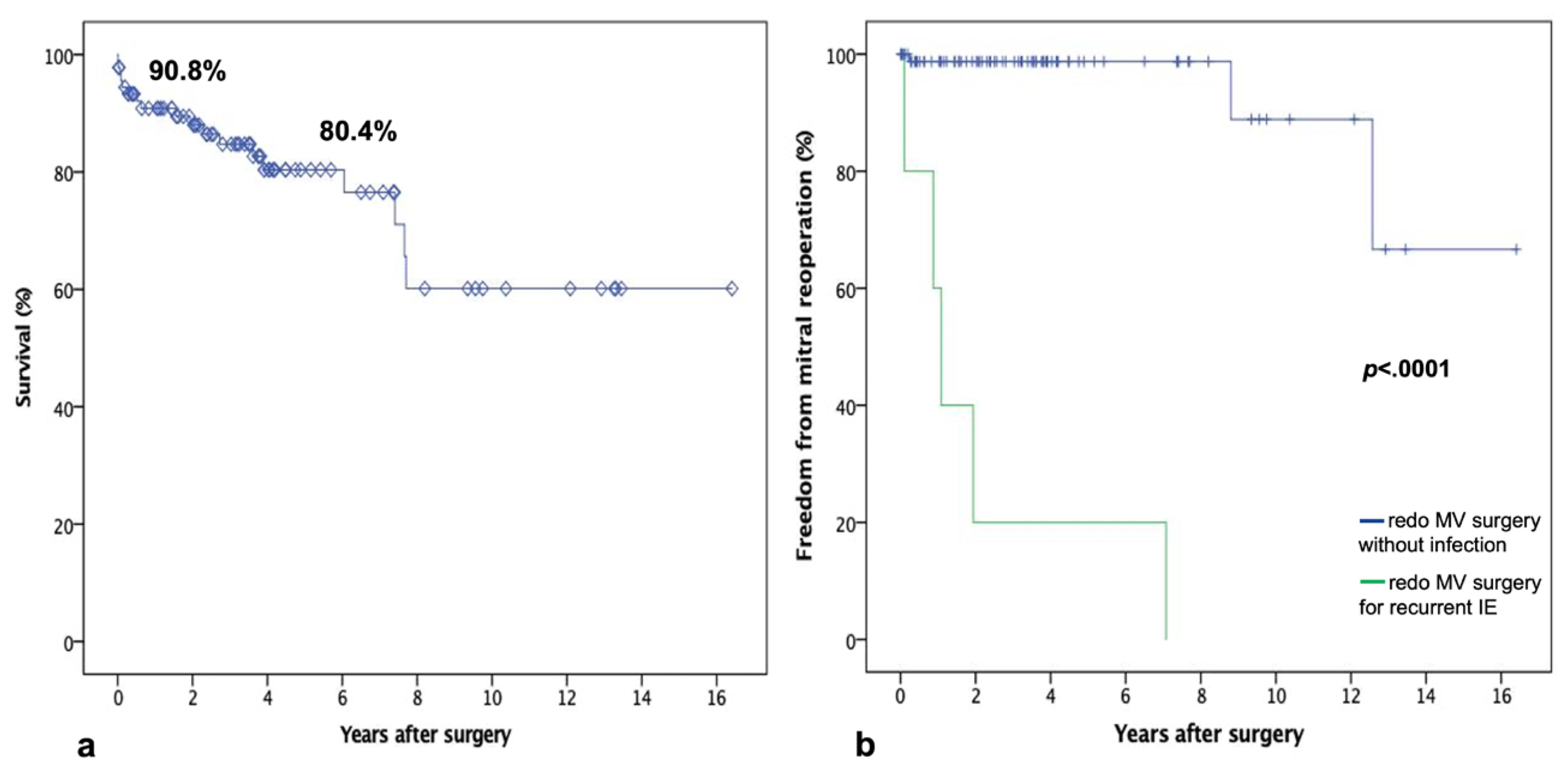

Table 1.
Baseline patients’ characteristics (n=92).
| Age (yrs) | 61.1 ± 12.7 |
| Female | 34 (37%) |
| BMI (Kg/m2) | 24.6 ± 5.4 |
| Hypertension | 44 (48%) |
| Diabetes | 18 (20%) |
| Atrial fibrillation | 21 (23%) |
| COPD | 7 (7.6%) |
| Chronic kidney disease | 12 (13%) |
| Peripheral vascular disease | 2 (2.2%) |
| NYHA class ≥3 | 20 (22%) |
| IE native | 80 (87%) |
| prosthetic | 12 (13%) |
| Heart Failure | 5 (5.4%) |
| Cerebral embolization | 13 (14%) |
| Redo | 26 (28%) |
| Ejection fraction (%) | 59 ± 9 |
| PAPs (mmHg) | 38 ± 14 |
| Log EuroSCORE | 15 ± 16 |
| Early Surgery | 69 (75%) |
BMI: body mass index; COPD: chronic obstructive pulmonary disease; NYHA: New York Heart Association;.IE: infective endocarditis; MV: mitral valve; PAPs: systolic pulmonary artery pressure.
Table 2.
Bacteriological analysis (n=92).
| Streptococcus | 22 (24%) |
| viridans | 3/22 |
| sanguis | 4/22 |
| mitis | 8/22 |
| haemoliticus | 3/22 |
| gallolyticus | 4/22 |
| Staphylococcus | 23 (25%) |
| aureus | 16/25 |
| epidermidis | 5/25 |
| lugdunensis | 2/25 |
| Entereococcus faecalis | 14 (15%) |
| Other | 12 (13%) |
| Culture-negative | 21 (23%) |
Table 3.
Operative data and perioperative outcomes (n=92).
| Isolated MV surgery | 82 (89%) |
| MV repair (native) | 16/80 (20%) |
| MV/MP replacement | 76 (83%) |
| TV surgery | 5 (5.4%) |
| ASD closure | 5 (5.4%) |
| Retrograde arterial perfusion (femoral) | 85 (92.4%) |
| Endo-aortic clamp | 40 (43%) |
| Trans-thoracic clamp | 51 (55%) |
| Fibrillating heart, | 1 (1.1) |
| CPB time (mins) | 143 ± 34 |
| Cross-clamp time (mins) | 105 ± 27 |
| Conversion to sternotomy | 1 (1.1%) |
| Aortic dissection | - |
| Stroke | 1 (1.1%) |
| Acute kidney injury | 5 (5.5%) |
| Re-exploration for bleeding | 5 (5.5%) |
| Mechanical ventilation >72 hrs | 7 (7.7%) |
| Reintubation | 4 (4.4%) |
| Permanent pacemaker | 3 (3.3%) |
| ICU length-of-stay (days) | 1 [1,2] |
| Hospital length-of-stay (days) | 7 [6–11] |
| 30-day mortality | 4 (4.4%) |
| Follow-up (months) | 98.1 [36.9-164.5] |
MV: mitral valve; MP: mitral prosthesis; TV: tricuspid valve; ASD: atrial septal defect; CPB: cardiopulmonary bypass; ICU: intensive care unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



