Submitted:
02 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
The first half of the 20th century was noteworthy for the introduction of a unique group of drugs – antibiotics. It drastically changed concepts of infectious diseases treatment, which for centuries remained a scourge of the human population. With improvement of the antibiotic treatment efficacy, humanity has faced the problem of a dramatic increase in antibiotic resistance in bacteria. The COVID-19 pandemic has only exacerbated the problem and posed a new challenge to the medical community in finding solutions, both clinical and organizational and methodological, to fight antibiotic resistance widespread all over the globe. This publication covers some aspects of evolutionary processes in either pathogens or diseases, including ethical perspective.
Keywords:
antibiotics
; antibiotic therapy
; antibiotic resistance
; evolutionary medicine
; ethics
1. Introduction
In recent decades, healthcare professionals have more frequently referred to such a term as evolutionary medicine. Obviously, the majority associate it with the Darwin’s theory of evolution. On the one hand, that is as it should be; on the other hand, to narrow the meaning exclusively to the works of the century before last is somewhat naive and short-sighted in general. Evolution, even sometimes turning into something revolutionary, is an ongoing process in medicine. Evolutionary medicine or Darwinian medicine is the use of modern evolutionary theory for understanding health and disease. Human activities as a geological factor have caused a dramatic change in all fauna and flora, the whole image of the planet, which is of direct concern to the ethics issues. The founders of environmental ethics are a German doctor Albert Schweitzer (1875-1965) and an American ecologist Aldo Leopold (1887-1948). In a bid for ecologically harmonious biosphere, a human being is, of course, the power on which we can count. It undoubtedly implies a wise attitude towards ecology, the biosphere as a whole, a positive impact on the ongoing processes in ecology related to evolution [1,2].
It is worth noting that changes of the disease clinical picture under various factors are important to assess against the evolution [3,4,5]. And in this perspective, drugs are important in changing the disease clinical picture. Now we are using groups of drugs that have a visual name – disease-modifying drugs. It is clear that in most cases such terminology is used in the characterization of drugs for the treatment of non-communicable diseases, but in some cases we can use it to describe the effect of antibiotics on the pathway of bacterial infections.
A number of scientists introduced the term “drug-induced pathomorphosis” which refers to a persistent and significant change in the clinical picture, pathogenetic mechanisms and pathomorphological features of diseases under various interventions compared to their classical manifestations. In 1929, a German scientist Willy Hellpach used the term “pathomorphosis” in the treatment of syphilis. However, we should be careful with this term to avoid its broad interpretation. Only a sufficiently long-term follow-up of groups of patients receiving drug therapy can bring us closer to understanding this phenomenon [6]. The time aspect is of fundamental importance from the evolution point of view. Mutation is a source of population genetic variation. The estimated mutation rate in humans is about 10-4-10-6/gene per generation. Thirty nucleotide mutations would be expected in each human gamete per generation [7]. The steady growth of human life expectancy leads to additional risks of malignant neoplasms because of the increased probability of somatic mutations [8,9]. But in any case, infectious diseases pathogens mutate much more frequently and evolve faster than humans, adapting to new environment (including the effects of drug therapy) significantly better than humans who “evolve” much slower and, in this regard, are at a disadvantage [10].
2. Antibiotic Therapy, Antibiotic Resistance
In this context, drugs that have been long and widely used in real clinical practice, in particular those used for the treatment of infectious diseases that have undergone significant evolutionary processes over the past century, are of interest in the first place [11].
And here our attention is turned to antibiotics which have been known to mankind for almost a century. In 1928, Alexander Fleming isolated the first antibiotic, and today this group of drugs has become one of the most commonly prescribed ones for a wide variety of diseases.
With regard to antibiotic therapy, it is clear that changes in the antibiotic resistance of the leading bacterial pathogens are mostly cited. The term antibiotic resistance crisis has become commonly used. However, this is also a relatively simplified approach. We focus mainly on antibiotic resistance data from various limited patient populations and try to understand the overall situation. In this regard, the real-world clinical practice studies which have been developing in recent years are probably better for understanding the overall picture.
Antibiotics, by all accounts, are a unique group of drugs. Recently, the attitude towards this group of drugs has been changing. They actively affect not only the individual patient to whom they are prescribed, but others around as well. And if before the rapid supermigration of the population at the end of the 20th/beginning of the 21st century, we were focused on the patient’s inner circle, now we are talking about the “instantaneous” spread of dangerous strains of pathogens with different resistance phenotypes. Antibiotic resistance leads to an increase in the number of adverse outcomes, including deaths, treatment costs, etc. [12,13].
The link between the use of antibiotics and resistance development was noted almost immediately after the start of the antibiotic era. Let’s have a look at the data from the Fleming’s period.
The doctors at Boston Hospital reported 50% resistance in staphylococci detected in patients on admission to the hospital while they had never used penicillin. And in patients to whom penicillin had been previously prescribed, the level of resistance to penicillin in staphylococci was up to 80% [14]. Besides, a fairly high incidence of great resistance in staphylococci among the clinical staff was noted at that time.
Skin reactions, stomatitis, gastrointestinal disorders, liver, renal and CNS function abnormalities – these are just few of adverse reactions to antibiotics, which were clearly reported by our senior colleagues in the 1950s [15].
Despite all this knowledge and warnings about caution when prescribing antibiotics, starting with the famous Fleming’s Nobel Prize speech [16], they had little impact on the general public understanding of antibiotic resistance and the reasonableness of antibiotic therapy.
In the mid-2010th, a report by a group of British economists headed by J. O’Neill [17] who predicted a sharp increase in mortality associated with antibiotic resistance caused a heated debate. Some critics were concerned about the predicted figures [18,19], but the past years, according to most experts, have only confirmed the worst fears. And the phrase “post-antibiotic era” no longer seems exaggeratory. In 2019, another analysis of data on antibiotic resistance and its impact on healthcare in 204 countries was conducted [20], which identified 4.95 million deaths associated with bacterial AMR in 2019, including 1.27 million attributable outcomes. In 2019, the top six pathogens causing deaths due to antibiotic resistance (Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa) were attributed to 929,000 deaths and associated with 3.57 million deaths. One pathogen-drug combination – methicillin-resistant S. aureus (MRSA) – directly caused more than 100,000 deaths associated with antibiotic resistance in 2019.
According to recent data, 1 child dies every 2 to 3 minutes from antimicrobial resistance worldwide. And the situation is especially “tragic” in neonatal intensive care units, where outbreaks of multidrug-resistant infections have a mortality rate of 50% [21].
Of course, some attempts to introduce systemic solutions to control antibiotic resistance have been made. We can also mention the principle of division into nosocomial and community-onset infections [22,23,24,25], the principles of the formulary system [26,27,28,29,30,31,32], and the creation of an infection control team, with a special role for clinical pharmacologists and epidemiologists. Moreover, it is not just an epidemiologist, it is a hospital epidemiologist, because we realize that the out-of-hospital and in-hospital environment are completely different ecosystems, and the infection progression in these cases has its own peculiarities. And, indeed, we should note the “Antimicrobial stewardship” system [33]: attempts to actively implement it have been and are being made in many countries, although with a varying level of effectiveness [34,35,36].
Separate isolation of nosocomial infections confirmed the unique approaches to the management of these patients [37]. We need to acknowledge that the course of these infections changes over time as well. There is an increasing number of elderly patients with chronic diseases, organ transplant patients [38,39], immunosuppressed, including iatrogenic immunosuppression [40,41], who are more exposed to “attacks” of critical infectious agents compared to other population groups. More and more patients receive biological therapy, corticosteroids, for quite a long time, which alone significantly changes the body’s response to infections and the course of the infectious disease itself [42,43,44,45].
We should also remember the “opposite” age group − children, with such a growing specific subgroup as premature infants whose underdeveloped and immature body systems, including the immune system, significantly affect the occurrence and course of the infection, its severity and prognosis [46].
We already distinguish patients with a severe infection; there is evidence that the prognosis in these patients is worse than in patients with a relatively non-severe disease. At the same time, the benefits of, for example, combination antibiotic therapy have not been fully identified [47,48,49,50]. Patients in intensive care units are considered separately, and we recognize that this may not be the severe course of the infection itself, but simply patients in a severe condition by their baseline status, and the infection only makes its own special contribution to the severity of the condition and, of course, to the efficacy of treatment and prognosis. Respiratory support, catheter-based component of intensive care, extracorporeal methods are found by some authors as separate areas of medical care [51,52].
At the same time, intensivists admit the need to prescribe antibiotics in critical patients, either for therapeutic or prophylactic purposes, in almost all cases.
Outpatient practice has its own problem: the need for antibiotic therapy as being vital is discussed in many clinical cases [53,54,55]. On the one hand, there is an understanding that the prognosis is quite good in most cases, on the other hand, more antibiotics are administered in the outpatient setting rather than in the inpatient setting.
Some pathogens that were not given serious clinical significance a few decades ago are coming to the fore, in particular Acinetobacter spp. [56,57,58].
Changes in therapy, especially initial empiric therapy, can have a specific impact on the microflora structure of hospital departments, which is important in terms of prognosis and costs of treatment of inpatients [59]. A change of empiric antibacterial therapy from third-generation cephalosporins to piperacillin/tazobactam was effective in reducing the incidence of K.pneumoniae and P.mirabilis and the frequency of ventilator-associated pneumonia. The authors emphasized that no other intervention was used during the study to reduce the frequency of this event. In addition, it also resulted in a significant decrease in the frequency of detection of ceftazidime-resistant K.pneumoniae isolates.
Sometimes we observe controversy: on the one hand, there is evidence that antibiotic resistance impacts the disease severity and outcomes. But at the same time, there is evidence to the contrary – antibiotic resistance itself has no effect on the outcome of the infectious process.
A recent study conducted in Vietnam [60] confirms the remaining problems of the rationality of antibacterial drugs in real practice. Of 1,747 patients enrolled in the ICU, 1,112 (63.6%) patients started empiric therapy with antibiotics, but 31.5% of patients were prescribed antibiotics without a diagnosis of infection. The most frequently prescribed antibiotics were cefotaxime (22.3%), levofloxacin (19%), and ceftazidime (10.8%). According to the new WHO concept [61], antibiotics in the Watch and/or Reserve groups were prescribed to 87.3% of patients and were significantly associated with the patient’s age and presence of a systemic inflammatory response syndrome upon admission to the hospital.
The most progressive part of the medical community has been talking for a long time about the need to increase medical professionals’ attention to the problem of antibiotic resistance, starting active work in this area from their student days. One publication [62] evaluated the effect of an elective course on antibiotic prescribing etiquette in clinical practice, both in terms of increasing the level of pure knowledge and raising the awareness of the problem of antibiotic resistance in general. We would like to quote the authors of this paper: “Medical students’ knowledge, perceptions, and attitudes towards antimicrobial prescription have been improved after the elective antibiotic prescribing etiquette course. Elective courses could offer a great opportunity to enable the students to understand the extent of the problem, stand on the facts, and take responsibility for the antibiotic resistance crisis.” It all starts with education of medical professionals as well.
Today, there is more focus on the treatment of a specific disease, namely the correction of symptoms caused by the pathophysiological response of a human body to the infectious agent’s penetration and development. There are more and more guidelines [63] devoted to “fighting” specific pathogens or a group of so-called problematic pathogens.
The rapid and sometimes avalanche-like appearance of new drugs in clinical practice [64,65,66] gives clinicians the impression, often deceptive, that we can cope with any challenge of nature (in a general sense).
We are unable to note changes in biological processes in long-term dynamics, we do not learn from the lessons of history, we do not see prospects, we work today and now. Only old medical professionals can grumble that it used to be different. Perhaps this old man’s view is not productive. But it really used to be different. And we are talking here not only about changing our approaches to treatment, but also about changing the course and manifestations of diseases. Both evolutionary changes of pathogens and macroorganisms should be taken into account.
There is also increasing evidence of “collateral damage” [67] due to the use of antibiotics. And these are not only the well-known allergies, gut dysbiosis, respiratory problems, but also, for example, the association with the development of Parkinson’s disease (PD). In a Finnish study [68], which analyzed a population of 13,976 PD cases and 40,697 controls, the strongest association with PD risk was found for oral exposure to macrolides and lincosamides. The authors also noted that exposure to antianaerobics and tetracyclines 10 to 15 years before the analysis, sulfonamides and trimethoprim 1 to 5 years, and antifungal medications 1 to 5 years were positively associated with PD risk.
Many authors believe that this and other adverse long-term effects of antibiotics are primarily mediated by the effect of antibiotic therapy on the gut flora [69], the biological significance of which is not fully understood and is probably underestimated.
On the other hand, in a study [70] examining 1407 preterm infants <32 weeks gestational age, antibiotics were administered to 911/1407 (64.7%) infants during their first postnatal week. Screening-targeted pathogens were detected in 547/1407 (38.9%). Early antibiotic exposure did not increase the risk of colonization with these pathogens. The only independent risk factor for colonization with potential pathogens was their staying in the hospital. Interestingly, longer antibiotic therapy (> 7 days) decreased the risk for acquiring pathogens with increased epidemic potential. Thus, early antibiotic exposure did not impact the risk for colonization with MDRO (multi-drug-resistant organism) or highly epidemic pathogens in preterm infants.
Such sort of conflicting data bring up a burning issue of the reliability and practicality of the vast amount of information now available to doctors and the validity of specific decisions in real clinical practice.
Here, we can also talk about changes in pathogens themselves, their genetic potential, their ability to generate, for example, certain toxins, etc., as well as changes in the response of the human body.
Another crucial point is the change in the macroorganism response to the infectious agent. Obviously, the role of the immune system should be discussed here. The human population is changing. First of all, it is getting older.
Nowadays, and for a long time, β-lactam antibiotics remain the main and most frequently used drugs both in outpatient and inpatient settings. In vitro studies showed that some β-lactam antibiotics, namely third-generation cephalosporins and ampicillin, inhibit metallo-β-lactamase proteins SNM1 (sensitive to nitrogen mustard) A & B and SNM1C/Artemis protein complex. The authors of the publication [71] claim that β-lactam antibiotics (cephalosporins, ampicillin) can block the SNM1C/Artemis protein in humans, causing transient immunodeficiency.
The authors note that this is probably most important in patients requiring long-course antibiotic therapy, particularly in infections of the bones/joints, central nervous system, and cardiovascular system.
Moreover, if β-lactam antibiotics confer immunocompromised states and favour opportunistic infections, candida infections should be actively sought and routinely reported in the event of fever under these antibiotics.
Anti MP-65 (β-glucan-associated protein MP65) antibodies were associated with survival in patients with severe disseminated infection [72].
The authors of another study [73] found that the anti-MP65, but not the anti-β1,6-glucan antibodies, of candidemic patients had higher titers in survivors than in non-survivors, particularly in those subject categories with the highest mortality (>65-years old, diabetic, or septic shock patients). Thus, candidemic patients are capable of boosting anti-candida immune responses upon infection, and some of these responses might be associated with the production of protective immunity in patients with candidemia.
In light of such data, the authors suggest using anti-MP65 antibodies as some kind of indicator of higher survival in such severe patients.
3. Evolutionary Medicine
During last decades, the number and ratio of the main risk factors of such an important nosology as infective endocarditis, which is directly related to the understanding of evolutionary changes in both pathogens and the disease itself, have increased and changed. Injection drug use, cardiac surgery, and invasive medical procedures (long-term venous catheterization, hemodialysis) have become the most important risk factors, leading to a change in the main pathogen, which, according to most studies, is Staphylococcus aureus [74].
Along with an increase in the number of heart defects associated with infective endocarditis, the incidence of acute rheumatic fever and the prevalence of chronic rheumatic heart disease stemming from group A β-hemolytic streptococcus has significantly decreased [75]. According to the World Health Organization, over 616 million cases of streptococcal pharyngitis are reported annually in the world [76]. Group A streptococcus (GAS) is the most common cause of morbidity and mortality in infectious diseases and one of the major human pathogens. The prevalence of severe cases of GAS infections amounted to 18.1 million people worldwide. The epidemiological situation with the spread of streptococcal infection and post-streptococcal diseases in the world has remained tense in recent decades. According to many researchers, it is directly related to the rational antibiotic therapy of streptococcal infections at the outpatient stage.
Since the middle of the last century, the medical community around the world had a persistent idea of a steady decline in the incidence of rheumatism (acute rheumatic fever), which naturally reduced the number of patients with rheumatic heart defects and the number of patients with heart failure for this reason. Actually, this did not mean that we had defeated this pathology. According to some authors, acute rheumatic fever and rheumatic heart disease are completely preventable diseases and have been practically eliminated in developed countries, but they claim about 320,000 lives worldwide every year [77,78]. It should be emphasized that the positive dynamics had a distinct dependence on the level of well-being of states. In developing countries, rheumatic “problems” remain important to this day, especially for the child population [79,80].
We are “moving away” from the classic variants of streptococcal infections and classic complications of this pathology, but we are beginning to encounter other manifestations of the effects of streptococci on the macroorganism. Cases of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (pediatric autoimmune neuropsychiatric disorders associated with streptococcal (group A beta-hemolytic streptococcal [GABHS]) - PANDAS) after pharyngitis have been described [81].
We reassure ourselves with data on the continued 100% sensitivity of pyogenic streptococci to natural penicillins, but the amazing genetic mobility of bacteria is manifested even in such “stable” microbes.
As shown in some experimental studies, streptococci can penetrate into human cells, becoming an intracellular pathogen [82,83].
And if in some cases streptococci can survive, persist in human cells, remaining immune to the effects of antibiotics [84], then we can see other symptoms of banal streptococcal infections.
We are changing human biology; we must be aware of this fact. From the point of view of the theory of natural selection, a deadly pathogen causes a condition incompatible with a particular body capability. We help the body to cope with conditions that could be handled quite rarely in the past.
As Herman J. [85] proposed - “By creating an environment both mutagenic and protective, we have altered the balance between the two great driving forces of evolution, through increasing the frequency of mutations and reducing the need for adaptation.”
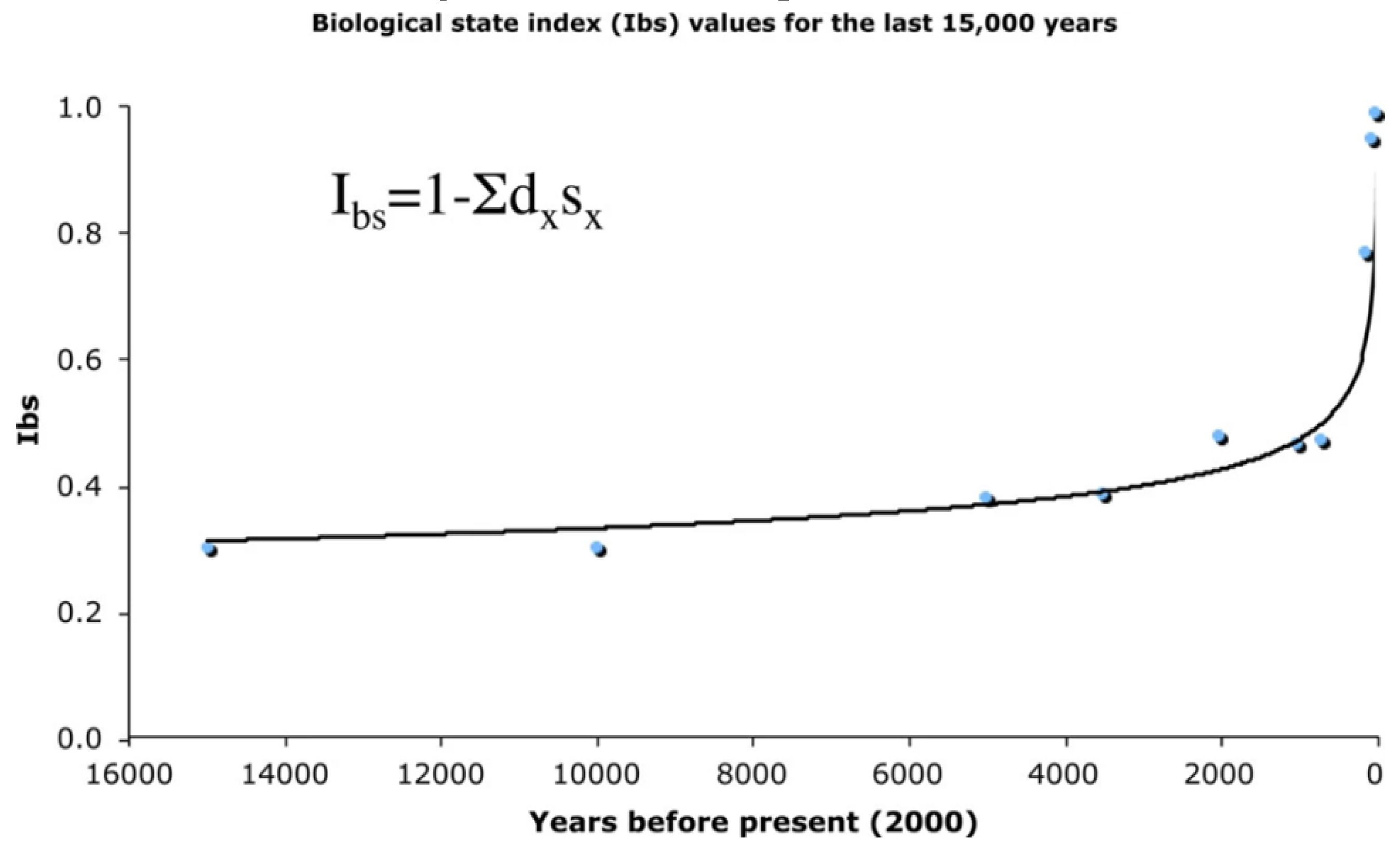
The figure shows the changes in the Biological State Index over the last 15,000 years of human evolution. The index value is a probability that an average person will be able to fully participate in reproduction of the next generation. The lower the index value is, the greater is the opportunity for natural selection [86]. Largely thanks to antibiotics, human life expectancy has increased, and the Biological State Index has increased, which presents a certain bioethical challenge to humanity.
Bauduer F. [87] emphasized the importance of evolutionary medicine - “It includes the initial Darwin’s view, its actualization in the light of progress in genetics and also dissident theories (i.e., non gene-based) particularly epigenetics. This approach enables us to reconsider the pathophysiology of numerous diseases, as, for instance, infection, and our so-called diseases of civilization, especially obesity, type 2 diabetes, allergy, or cancer. Evolutionary medicine may also improve our knowledge regarding inter-individual variation in susceptibility to disease or drugs. Furthermore, it points out the impact of our behavior and environment on the genesis of a series of diseases.”
At the genetic level, alleles do not have an absolute adaptive or maladaptive value, they assume it by interaction with the rest of the genome, and the epigenetics determines their Darwinian fitness. A gene causing pathological effects in the past (for example, predisposition to type I diabetes mellitus) may not be considered maladaptive in an environment where there is an effective treatment for diabetes [86]. But epigenetic influence and the use of modern advanced therapy drugs can perpetuate the accumulated changes in the human genome over the long term.
Infectious diseases are always an evolution of both the microorganism, which can occur under the influence of natural causes and antibiotics, and of the disease itself. Moreover, we mean such interactions between an infectious pathogen and the human body that we previously had no idea about. In particular, today we talk a lot about the antibiotic resistance of such a pathogen as Helicobacter pylori; the medical community is especially concerned about the growth of resistance to metronidazole and clarithromycin [88]. As for metronidazole, we can say that it has long been out of widespread use in eradication therapy regimens, but clarithromycin remains the standard initial therapy for many medical practitioners. At the same time, some experts argue that clarithromycin as a drug in the standard eradication regimen is past its prime now [89,90]. It is known that helicobacter is defined by the WHO as a carcinogen, and therefore during eradication, we save patients not only from complications of peptic ulcer disease and chronic gastritis, but also from gastric cancer. This only confirms the contingency of pathomorphosis of the infectious process and malignant growth. It has been noted that H.pylori infection increases the risk of gastric cancer associated with hereditary pathogenic variants in homologous-recombination genes [91]. We can suggest the influence of antibiotic use on the evolution of individual cancers at least in certain populations. And this should eventually lead to the widespread use of personalized medicine, particularly in subpopulations of the highest risk.
4. Conclusions
Thus, from the viewpoint of evolutionary medicine, long-term risk-benefit balance and widespread use of antibiotics should be under strict human control. This presents certain bioethical issues. From a utilitarian point of view, the use of a drug for a particular patient on medical indications is perfectly justified. But population risks with wide medicalization can have long-term consequences, which have not been systematized yet and do not fit into the generally accepted classifications of adverse reactions. Good pharmacovigilance practices are undoubtedly a prerequisite in the study of drugs, but they are not sufficient enough. The following actions seem to be of key importance: monitoring of antibiotic resistance, fight against polypragmasy, development of personalized medicine, further development of long-term observational studies, development of the biological collection (biobanking) and phenotyping (“mapping” of symptoms and disease syndromes) system.
It should be emphasized that the use of drugs, especially antibiotics and other biological medicines, requires strict regulation not only at the national level, but also at the international level, which demands international cooperation in this field that is vital for the mankind.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vernadsky, V. I. The Biosphere./Forward by Linn Margulis and colleagues; introduction by Jacques Grinevald; translated by David B. Langmuir; revised and annotated by Mark A. S. McMenamin. New York, Copernicus, 1998.
- Vernadsky, V. I. Thoughts of the Naturalist. Moscow, Nauka, 1977, 18.
- Wells, J.C.K.; Nesse, R.M.; Sear, R.; A Johnstone, R.; Stearns, S.C. Evolutionary public health: introducing the concept. Lancet 2017, 390, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Grunspan, D.Z.; Nesse, R.M.; Barnes, M.E.; E Brownell, S. Core principles of evolutionary medicine. Evol. Med. Public Heal. 2017, 2018, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P. , Beedle A., Buklijas T., Low FHM (2016) Principles of evolutionary medicine, 2nd ed. Oxford University Press.
- Tiganov, A.S. The pathomorphosis of schizophrenia. Zhurnal Nevrol. i psikhiatrii im. S.S. Korsakova 2015, 115, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Scott, W. Piraino, Simon J. Furney et al. Mutations: Driver Versus Passenger. In Encyclopedia of Cancer (Third Edition), 2019. Editors-in-Chief: Paolo Boffetta, Pierre Hainaut. eBook ISBN: 9780128124857. Hardcover ISBN: 9780128124840.
- Berger, M.F.; Mardis, E.R. The emerging clinical relevance of genomics in cancer medicine. Nat. Rev. Clin. Oncol. 2018, 15, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Potievskii, M.B.; Shegai, P.V.; Kaprin, A.D. Prospects for the Application of Methods of Evolutionary Biology in Oncology. J. Evol. Biochem. Physiol. 2022, 58, 318–330. [Google Scholar] [CrossRef]
- VanSteelandt, A. , Stone A.C. Genetics, Evolutionary Medicine, and the Evolution of Human Pathogens. In: A Companion to Anthropological Genetics. Dennis H. O’Rourke (Editor), 19, Wiley-Blackwell, 496 Pages. ISBN: 978-1-118-76899-0. 20 March.
- Ewald, P.W. Evolutionary biology and the treatment of signs and symptoms of infectious disease. J. Theor. Biol. 1980, 86, 169–176. [Google Scholar] [CrossRef]
- Global antimicrobial resistance and use surveillance system (GLASS) report: 2022 (who.int)). Available online: https://www.who.int/publications/i/item/9789240062702.
- Friedman, N.; Temkin, E.; Carmeli, Y. The negative impact of antibiotic resistance. Clin. Microbiol. Infect. 2015, 22, 416–422. [Google Scholar] [CrossRef]
- Spread of Antibiotic-Resistant Staphylococci. New Engl. J. Med. 1953, 249, 711–713. [CrossRef]
- Finland, M.; Weinstein, L. Complications Induced by Antimicrobial Agents. New Engl. J. Med. 1953, 248, 220–226. [Google Scholar] [CrossRef]
- Sir Alexander Fleming – Banquet speech. NobelPrize.org. Available online: https://www.nobelprize.org/prizes/medicine/1945/fleming/speech/.
- O’Neill, J. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. London: Review on Antimicrobial Resistance, 2014.
- Abat, C.; Fournier, P.-E.; Jimeno, M.-T.; Rolain, J.-M.; Raoult, D. Extremely and pandrug-resistant bacteria extra-deaths: myth or reality? Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1687–1697. [Google Scholar] [CrossRef]
- Abat, C.; Rolain, J.-M.; Dubourg, G.; Fournier, P.-E.; Chaudet, H.; Raoult, D. Evaluating the Clinical Burden and Mortality Attributable to Antibiotic Resistance: The Disparity of Empirical Data and Simple Model Estimations. Clin. Infect. Dis. 2017, 65, S58–S63. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022; 399: 629–55 Published Online January 20, 2022. [Google Scholar]
- Antimicrobial Resistance Requires a Manifold Response - Medscape - Apr 07, 2023.
- Johnson, ET. Nosocomial infection: update. J Natl Med Assoc. 1983 Feb;75(2):147-54. PMID: 6827607; PMCID: PMC2561458.
- Miles, A.A. OBSERVATIONS ON THE CONTROL OF HOSPITAL INFECTION. Br. Med Bull. 1944, 2, 276–281. [Google Scholar] [CrossRef]
- Dixon, R.E. Nosocomial infection a continuing problem. Postgrad. Med. 1977, 62, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, R. Nosocomial Infection Update. Emerg. Infect. Dis. 1998, 4, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Therapeutic evaluation of National Formulary drugs. Bull Am Pharm Assoc. 1946 Sep-Oct;14(9-10):161-204. [PubMed]
- Boetzkes, H. [The drug list of the American Hospital Formulary Service]. . 1961, 7, 114–7. [Google Scholar] [PubMed]
- Letourneau, CU. The hospital drug formulary. I. Hosp Manage. 1961 Apr;91:38-9. [PubMed]
- Deuster, S.; Roten, I.; Muehlebach, S. Implementation of treatment guidelines to support judicious use of antibiotic therapy. J. Clin. Pharm. Ther. 2010, 35, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Sermet, C.; Andrieu, V.; Godman, B.; Van Ganse, E.; Haycox, A.; Reynier, J.-P. Ongoing pharmaceutical reforms in France. Appl. Heal. Econ. Heal. Policy 2010, 8, 7–24. [Google Scholar] [CrossRef]
- Deuster, S.; Roten, I.; Muehlebach, S. Implementation of treatment guidelines to support judicious use of antibiotic therapy. J. Clin. Pharm. Ther. 2010, 35, 71–78. [Google Scholar] [CrossRef]
- Gastine, S.; Hsia, Y.; Clements, M.; Barker, C.I.; Bielicki, J.; Hartmann, C.; Sharland, M.; Standing, J.F. Variation in Target Attainment of Beta-Lactam Antibiotic Dosing Between International Pediatric Formularies. Clin. Pharmacol. Ther. 2021, 109, 958–970. [Google Scholar] [CrossRef]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Yousuf, S.; Rzewuska, M.; Duncan, E.; Ramsay, C. Identification of outcomes reported for hospital antimicrobial stewardship interventions using a systematic review of reviews. JAC-Antimicrobial Resist. 2022, 5, dlac127. [Google Scholar] [CrossRef] [PubMed]
- Garwan, Y.M.; Alsalloum, M.A.; Thabit, A.K.; Jose, J.; Eljaaly, K. Effectiveness of antimicrobial stewardship interventions on early switch from intravenous-to-oral antimicrobials in hospitalized adults: A systematic review. Am. J. Infect. Control. 2023, 51, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Sobalvarro, J.V.; Júnior, A.A.P.; Pereira, L.B.; Baldoni, A.O.; Ceron, C.S.; dos Reis, T.M. Antimicrobial stewardship for surgical antibiotic prophylaxis and surgical site infections: a systematic review. Pharm. Weekbl. 2021, 44, 301–319. [Google Scholar] [CrossRef] [PubMed]
- Selwyn, S. Hospital infection: the first 2500 years. J. Hosp. Infect. 1991, 18, 5–64. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.J.; Ali, M.; Rana, M.; Patel, G.; Sullivan, T.; Murphy, J.; Pinney, S.; Anyanwu, A.; Huprikar, S.; Taimur, S. Infections due to multidrug-resistant organisms following heart transplantation: Epidemiology, microbiology, and outcomes. Transpl. Infect. Dis. 2019, 22, e13215. [Google Scholar] [CrossRef] [PubMed]
- Qiao, B.; Wu, J.; Wan, Q.; Zhang, S.; Ye, Q. Factors influencing mortality in abdominal solid organ transplant recipients with multidrug-resistant gram-negative bacteremia. BMC Infect. Dis. 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Da Silva, R.; Casella, T. Healthcare-associated infections in patients who are immunosuppressed due to chemotherapy treatment: a narrative review. J. Infect. Dev. Ctries. 2022, 16, 1784–1795. [Google Scholar] [CrossRef]
- Kreitmann, L.; Gaudet, A.; Nseir, S. Ventilator-Associated Pneumonia in Immunosuppressed Patients. Antibiotics 2023, 12, 413. [Google Scholar] [CrossRef]
- Navarro-Zarza, J.; Álvarez-Hernández, E.; Casasola-Vargas, J.; Estrada-Castro, E.; Burgos-Vargas, R. Prevalence of community-acquired and nosocomial infections in hospitalized patients with systemic lupus erythematosus. Lupus 2009, 19, 43–48. [Google Scholar] [CrossRef]
- Restrepo-Escobar, M.M.; Granda-Carvajal, P.A.M.; Aguirre-Acevedo, D.C.M.; Jaimes, F.M.; Vásquez, G.M. Predictive Factors of Hospital-Acquired Bacterial Infections in Patients With Systemic Lupus Erythematosus. Am. J. Clin. Oncol. 2023, 29, 240–244. [Google Scholar] [CrossRef]
- Hamilton, F.; Evans, R.; Ghazal, P.; MacGowan, A. Patients with transplantation have reduced mortality in bacteraemia: Analysis of data from a randomised trial. J. Infect. 2022, 85, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Wan, Q.; Ye, Q.; Zhou, J. Mortality Predictors of Bloodstream Infections in Solid-Organ Transplant Recipients. Transplantation 2013, 11, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Elward, A.M.; Fraser, V.J. Risk Factors for Nosocomial Primary Bloodstream Infection in Pediatric Intensive Care Unit Patients: A 2-Year Prospective Cohort Study. Infect. Control. Hosp. Epidemiology 2006, 27, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Lode, H. Combination versus monotherapy for nosocomial pneumonia. Eur. Respir. Rev. 2007, 16, 50–55. [Google Scholar] [CrossRef]
- Tang, S.Y.; Zhang, S.W.; Wu, J.D.; Wu, F.; Zhang, J.; Dong, J.T.; Guo, P.; Zhang, D.L.; Yang, J.T.; Zhang, W.J. Comparison of mono- and combination antibiotic therapy for the treatment of Pseudomonas�aeruginosa bacteraemia: A cumulative meta-analysis of cohort studies. Exp. Ther. Med. 2018, 15, 2418–2428. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Silov, N.; Jukić, M.; Baloević, S.E.; Peričić, T.P.; Jerončić, A. Ertapenem Monotherapy versus Gentamicin Plus Metronidazole for Perforated Appendicitis in Pediatric Patients. Surg. Infect. 2019, 20, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Feigin, E.; Samuk, I.; Kravarusic, D.; Baazov, A.; Levy, I.; Livni, G.; Freud, E.; Dreznik, Y. Dual versus Triple Antibiotics Regimen in Children with Perforated Acute Appendicitis. Eur. J. Pediatr. Surg. 2017, 28, 491–494. [Google Scholar] [CrossRef]
- Marino’s The ICU Book International Edition (Paperback, Fourth, International Edition, LWW; Fourth, North American edition (, 2013). 5 November.
- Liu, X.; Long, Y.; Greenhalgh, C.; Steeg, S.; Wilkinson, J.; Li, H.; Verma, A.; Spencer, A. A systematic review and meta-analysis of risk factors associated with healthcare-associated infections among hospitalized patients in Chinese general hospitals from 2001 to2022. J. Hosp. Infect. 2023, 135, 37–49. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/antibiotic-use/sinus-infection. html#:~:text=Most%20sinus%20infections%20usually%20get,to%20more%20serious%20health%20problems.
- Available online: https://www.mayoclinic.org/diseases-conditions/acute-sinusitis/diagnosis-treatment/drc-20351677.
- Rosenfeld, R.M. Acute Sinusitis in Adults. New Engl. J. Med. 2016, 375, 962–970. [Google Scholar] [CrossRef]
- Maraki, S.; Mantadakis, E.; Mavromanolaki, V.E.; Kofteridis, D.P.; Samonis, G. A 5-year Surveillance Study on Antimicrobial Resistance ofAcinetobacter baumanniiClinical Isolates from a Tertiary Greek Hospital. Infect. Chemother. 2016, 48, 190–198. [Google Scholar] [CrossRef]
- Hafiz, T.A.; Alghamdi, S.S.; Mubaraki, M.A.; Alghamdi, S.S.; Alothaybi, A.; Aldawood, E.; Alotaibi, F. A two-year retrospective study of multidrug-resistant Acinetobacter baumannii respiratory infections in critically Ill patients: Clinical and microbiological findings. J. Infect. Public Heal. 2023, 16, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-J.; Xiao, Z.-G.; Lv, X.-J.; Huang, H.-T.; Liao, C.; Hui, C.-Y.; Xu, Y.; Li, H.-F. Drug-resistant Acinetobacter baumannii: From molecular mechanisms to potential therapeutics (Review). Exp. Ther. Med. 2023, 25, 209. [Google Scholar] [CrossRef] [PubMed]
- Elisa, M. Jukemura, Marcelo N. Burattini. Control of Multi-Resistant Bacteria and Ventilator-Associated Pneumonia: Is It Possible with Changes in Antibiotics? The Brazilian Journal of Infectious Diseases 2007;11(4):418-422.
- Dat, V.Q.; Dat, T.T.; Hieu, V.Q.; Giang, K.B.; Otsu, S. Antibiotic use for empirical therapy in the critical care units in primary and secondary hospitals in Vietnam: a multicenter cross-sectional study. Lancet Reg. Heal. - West. Pac. 2021, 18, 100306. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization; 2019. The 2019 WHO AWaRe classification of antibiotics for evaluation and monitoring of use. Geneva. 2019. Contract No.: WHO/EMP/IAU/2019.11.
- Rehab, H. El-sokkary, Shahenda G. Badran, Omnia S. El Seifi, Yara M. El-Fakharany, Rehab M. Elsaid Tash, El-sokkary et al. Antibiotic prescribing etiquette” an elective course for medical students: could we recruit potential physicians to fight resistance? BMC Medical Education (2023) 23:8).
- Tiseo, G.; Brigante, G.; Giacobbe, D.R.; Maraolo, A.E.; Gona, F.; Falcone, M.; Giannella, M.; Grossi, P.; Pea, F.; Rossolini, G.M.; et al. Diagnosis and management of infections caused by multidrug-resistant bacteria: guideline endorsed by the Italian Society of Infection and Tropical Diseases (SIMIT), the Italian Society of Anti-Infective Therapy (SITA), the Italian Group for Antimicrobial Stewardship (GISA), the Italian Association of Clinical Microbiologists (AMCLI) and the Italian Society of Microbiology (SIM). Int. J. Antimicrob. Agents 2022, 60, 106611. [Google Scholar] [CrossRef] [PubMed]
- Kish, T. New Antibiotics in Development Target Highly Resistant Gram-Negative Organisms. 2018, 43, 116–120. [Google Scholar] [PubMed]
- Karvouniaris, M.; Almyroudi, M.P.; Abdul-Aziz, M.H.; Blot, S.; Paramythiotou, E.; Tsigou, E.; Koulenti, D. Novel Antimicrobial Agents for Gram-Negative Pathogens. Antibiotics 2023, 12, 761. [Google Scholar] [CrossRef] [PubMed]
- Provenzani, A.; Hospodar, A.R.; Meyer, A.L.; Vinci, D.L.; Hwang, E.Y.; Butrus, C.M.; Polidori, P. Multidrug-resistant gram-negative organisms: a review of recently approved antibiotics and novel pipeline agents. Pharm. Weekbl. 2020, 42, 1016–1025. [Google Scholar] [CrossRef]
- Paterson, D.L. “Collateral Damage” from Cephalosporin or Quinolone Antibiotic Therapy. Clin. Infect. Dis. 2004, 38, S341–S345. [Google Scholar] [CrossRef]
- Mertsalmi, T.H.; Pekkonen, E.; Scheperjans, F. Antibiotic Exposure and Risk of Parkinson’s Disease in Finland: A Nationwide Case-Control Study. Mov. Disord. 2019, 35, 431–442. [Google Scholar] [CrossRef]
- Maier, L.; Goemans, C.V.; Wirbel, J.; Kuhn, M.; Eberl, C.; Pruteanu, M.; Müller, P.; Garcia-Santamarina, S.; Cacace, E.; Zhang, B.; et al. Unravelling the collateral damage of antibiotics on gut bacteria. Nature 2021, 599, 120–124. [Google Scholar] [CrossRef]
- Bubser, C.; Liese, J.; Serna-Higuita, L.M.; Müller, A.; Vochem, M.; Arand, J.; Karck, U.; Gross, M.; Poets, C.F.; Härtel, C.; et al. Impact of early antibiotic exposure on the risk of colonization with potential pathogens in very preterm infants: a retrospective cohort analysis. Antimicrob. Resist. Infect. Control. 2022, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Melenotte, C.; Pontarotti, P.; Pinault, L.; Mège, J.-L.; Devaux, C.; Raoult, D. Could β-Lactam Antibiotics Block Humoral Immunity? Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Atamna, A.; Eliakim-Raz, N.; Mohana, J.; Ben-Zvi, H.; Sorek, N.; Shochat, T.; Bishara, J. Predicting candidemia in the internal medicine wards: a comparison with gram-negative bacteremia—a retrospectives study. Diagn. Microbiol. Infect. Dis. 2019, 95, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Torosantucci, A.; Tumbarello, M.; Bromuro, C.; Chiani, P.; Posteraro, B.; Sanguinetti, M.; Cauda, R.; Cassone, A. Antibodies against a β-glucan-protein complex of Candida albicans and its potential as indicator of protective immunity in candidemic patients. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Danilov, A.I. , Alekseeva I.V., Asner T.V., Vlasova E.E., Danilova E.M., Dehnich A.V. i soavt. Jetiologija infekcionnogo jendokardita v Rossii. Klin Mikrobiol Antimikrob Khimioter. 2015; 17 (1): 4–10.
- Belov, B.S. Acute rheumatic fever and chronic rheumatic heart disease. From: Rational Pharmacotherapy of Cardiovascular Diseases: Guide for Practitioners / edited by E.I. Chazov, Yu.A. Karpov - 2nd ed., amended and suppl. M, Litterra, 2017. 623-632.
- Carapetis, J.R.; Steer, A.C.; Mulholland, E.K.; Weber, M. The global burden of group A streptococcal diseases. Lancet Infect. Dis. 2005, 5, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Watkins, D.A.; Johnson, C.O.; Colquhoun, S.M.; Karthikeyan, G.; Beaton, A.; Bukhman, G.; Forouzanfar, M.H.; Longenecker, C.T.; Mayosi, B.M.; Mensah, G.A.; et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990–2015. New Engl. J. Med. 2017, 377, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Dooley, L.M.; Ahmad, T.B.; Pandey, M.; Good, M.F.; Kotiw, M. Rheumatic heart disease: A review of the current status of global research activity. Autoimmun. Rev. 2020, 20, 102740. [Google Scholar] [CrossRef]
- Guan, C.; Xu, W.; Wu, S.; Zhang, J. Rheumatic heart disease burden, trends, and inequalities in Asia, 1990–2019. Glob. Heal. Action 2023, 16, 2215011. [Google Scholar] [CrossRef]
- Arvind, B.; Ramakrishnan, S. Rheumatic Fever and Rheumatic Heart Disease in Children. Indian J. Pediatr. 2020, 87, 305–311. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leonard, H.L.; Garvey, M.A.; Mittleman, B.B.; Allen, A.J.; Dow, S.; Zamkoff, J.; Dubbert, B.K.; Lougee, L.; Colvin, M.K.; et al. Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections: Clinical Description of the First 50 Cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef]
- LaPenta, D.; Rubens, C.; Chi, E.; Cleary, P.P. Group A streptococci efficiently invade human respiratory epithelial cells. Proc. Natl. Acad. Sci. 1994, 91, 12115–12119. [Google Scholar] [CrossRef] [PubMed]
- Greco, R.; De Martino, L.; Donnarumma, G.; Conte, M.; Seganti, L.; Valenti, P. Invasion of cultured human cells by Streptococcus pyogenes. Res. Microbiol. 1995, 146, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Rohde M, Cleary PP. Adhesion and invasion of Streptococcus pyogenes into host cells and clinical relevance of intracellular streptococci. 2022 Sep 4 [updated 2022 Oct 4]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd ed. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 17. [PubMed]
- Herman, J. Medicine and evolution: time for a new paradigm? Med Hypotheses 1997, 48, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Rühli, F.J.; Henneberg, M. New perspectives on evolutionary medicine: the relevance of microevolution for human health and disease. BMC Med. 2013, 11, 115–7. [Google Scholar] [CrossRef] [PubMed]
- Bauduer, F. La médecine évolutionniste : un nouveau regard sur la santé et les maladies. La Rev. de Médecine Interne 2017, 38, 195–200. [Google Scholar] [CrossRef]
- Katelaris, P.; Hunt, R.; Bazzoli, F.; Cohen, H.; Fock, K.M.; Gemilyan, M.; Malfertheiner, P.; Mégraud, F.; Piscoya, A.; Quach, D.; et al. Helicobacter pylori World Gastroenterology Organization Global Guideline. J. Clin. Gastroenterol. 2022, 57, 111–126. [Google Scholar] [CrossRef]
- Mégraud, F.; Graham, D.Y.; Howden, C.W.; Trevino, E.; Weissfeld, A.; Hunt, B.; Smith, N.; Leifke, E.; Chey, W.D. Rates of Antimicrobial Resistance in Helicobacter pylori Isolates From Clinical Trial Patients Across the US and Europe. Am. J. Gastroenterol. 2022, 118, 269–275. [Google Scholar] [CrossRef]
- Time to Ditch Clarithromycin for H pylori? - Medscape – Oct 21, 2022.
- Usui, Y.; Taniyama, Y.; Endo, M.; Koyanagi, Y.N.; Kasugai, Y.; Oze, I.; Ito, H.; Imoto, I.; Tanaka, T.; Tajika, M.; et al. Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer. New Engl. J. Med. 2023, 388, 1181–1190. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



