
Submitted:
04 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
The aim of this study was to evaluate the effects of autologous microfragmented adipose tissue (MFAT), obtained by mechanical fragmentation, on radiographic bone healing in dogs subjected to tibial plateau levelling osteotomy (TPLO). Twenty dogs with unilateral cranial cruciate disease were enrolled and randomly assigned to the treatment group (MFAT) or the control group (NT). The MFAT group underwent TPLO and autologous MFAT intra-articular administration while the NT group underwent TPLO alone. The adipose tissue was collected from the thigh region and MFAT was obtained by mechanical fragmentation at the end of the surgery. The patients were subjected to X-ray exam preoperatively, immediately postoperatively (T0) and at 4 (T1) and 8 (T2) weeks postoperatively. Two radiographic scores that had previously been described for the evaluation of bone healing after TPLO were used. A 12-point scoring system (from 0 = no healing to 12= complete remodelling) was used at T0, T1 and T2, while a 5-point scoring system (from 0 = no healing to 4 = 76%–100% of healing) was used at T1 and T2. The median healing scores were significantly higher at T1 and T2 for the MFAT group compared with the NT group for the 12-point (p < 0.05) and 5-point (p < 0.05) scoring systems. The intra-articular injection of autologous microfragmented adipose tissue can accelerate bone healing after TPLO without complications.
Keywords:
microfragmented adipose tissue
; regenerative medicine
; bone healing
; osteotomy
; cranial cruciate ligament
1. Introduction
Cranial cruciate ligament rupture (CCLR) is the most acquired cause of pelvic limb lameness in dog [1,2]. The aetiology is not entirely clear, but degenerative or conformational causes (such as excessive inclination of tibial plateau, intercondylar notch stenosis, insufficient nutritive supply core of ligament) are most commonly associated with a traumatic event [3,4,5,6]. Since 1952, several surgeries have been described for the treatment of CCLR in dogs; they can be subdivided into intra- or extracapsular reconstruction of the ligament and corrective osteotomies [7,8,9,10]. The latter are the most recent conception: they aim to modify the stifle joint biomechanics by neutralising the cranial tibial thrust (CTT) [11,12]. Among these procedures, tibial levelling plateau osteotomy (TPLO) is one of the most used and shows satisfactory outcomes [13,14,15,16].
Although it is a standardised surgery with a high clinical success rate, TPLO is not without its complications; among these are reported mechanical failure with loss of reduction prior to attainment of bone union and delayed or bone non-union [17,18,19,20]. Strategies to treat these consolidation delays are continuously being evaluated. Because TPLO is a relatively standardised procedure, it can be used when studying the efficacy of new therapies that could promote bone healing in a clinical setting [19,21,22,23,24].
Numerous studies have highlighted the osteogenic power of adipose stem cells (ADSCs) and their use, alone or in association with biomaterials, in the repair of bone defects or to increase the speed bone healing [25,26,27]. Based on in vivo and in vitro studies, the induction of ADSCs leads to several changes: increased expression of osteogenic genes, including runt-related transcription factor 2 (RUNX2) and osterix (OSX); increased alkaline phosphatase activity and calcium phosphate mineralised extracellular matrix; and increased osteocalcin, osteopontin and collagen type I protein [28,29]. In general, mesenchymal stem cells have a fundamental role in primary and secondary bone healing differentiating into osteoblasts and chondrocytes to complete the repair of bone [30,31,32].
In clinical practice, autologous ADSCs are often not administered as a pure isolate but rather as a constituent of the stromal vascular fraction (SVF) [33,34]. The advantages of SVF include its abundant stem cells, ease of extraction, the availability of tissue and minimal invasiveness of the harvest [35,36]. Some articles have reported promising results regarding the application of SVF in bone healing [37,38]. Saxer et al. [38] demonstrated that SVF cells, without expansion or exogenous priming, can spontaneously form bone tissue and vessel structures within a fracture microenvironment. In addition, Kim et al. [39] highlighted the osteogenic potential of SVF in vitro and the increase in bone healing with scaffold seeded with SVF compared with treatment with scaffold alone in a rabbit model.
SVF isolation involves the use of enzymatic digestion of adipose tissue, a process that is expensive, time consuming and strictly regulated by the Good Manufacturing Procedure of European Parliament (EC regulation no. 1394/2007). Therefore, it can only be performed in specialised laboratories [40,41]. In this scenario, companies have developed automatic closed devices that allow mechanically processing adipose tissue [42,43]. Mechanical disaggregation of fat results in microfragmented adipose tissue (MFAT), sometimes referred to as SVF from MFAT [36,43]. MFAT contains all the cells found in adipose tissue, including adipocytes, and preserves the microenvironment of perivascular niche. For this reason, it has a more paracrine and immunomodulatory effect then enzymatic SVF, however, with fewer stem cells [44,45,46].
In human medicine, studies have shown the potentiality of MFAT administration in aesthetic medicine, wound and fistula healing and in management of degenerative chronic diseases (osteoarthrosis and diabetes) [47,48,49,50,51]. On the other hand, the scientific literature concerning the use of MFAT in veterinary medicine is very limited [52,53,54,55]. To our knowledge there has been no research evaluating the effect of MFAT on bone healing in both human and veterinary medicine. The aim of this study was to evaluate the effects of autologous adipose micrograft, obtained by mechanical fragmentation, on radiographic bone healing in dog subjected to TPLO.
2. Materials and Methods
2.1. Ethics Statement
This clinical study was approved by the Ethics Committee for Clinical Study in Animal Patients of the University of Camerino. Informed consent was obtained from the owners of all the dogs.
2.2. Animals
Twenty mixed breed dogs with unilateral naturally occurring CCL disease were prospectively enrolled in the study. The diagnosis of complete CCL rupture was based on orthopaedic examination, and it was confirmed by radiographic evaluation. Each dog was subjected to general, orthopaedic and neurological physical examination, in order to exclude other orthopaedic or neurological pathologies. In addition, blood cell count and biochemistry profile were obtained. Dogs with concurrent orthopaedic, neurological or metabolic disease were excluded from the study, including dogs with contralateral CCL disease. Only dogs with body condition scores between 4 and 6 (on a scale of 1–9) were considered. Ten dogs were randomly assigned to the treatment group (MFAT) and the other 10 to the control group (NT).
2.3. Surgical Procedures
Each TPLO was performed by the same expert orthopaedic surgeon as described previously [13].
The subjects were positioned in dorsolateral recumbency. The affected limb and surgical field were aseptically prepared. A craniomedial surgical approach to the proximal tibia was performed with sartorius muscle dissection and popliteus muscle detachment from bone caudal aspect. Cefazoline (Teva s.r.l., Italy) was administered intravenously (22 mg/kg) approximately 30 minutes before the skin incision and a second administration was given after 90 minutes.
The plate and radial saw blade were selected by the surgeon according to the reported surgical technique indications and her experience [56]. DePuy Synthes TPLO Locking Plates (DePuy Synthes, Switzerland) were used. All osteotomies were compressed with placement of two conventional screws in compression. During the osteotomy and drilling, a saline solution lavage were used to prevent the thermal bone necrosis. The surgical site was then sutured routinely using USP 2/0 adsorbable monofilament thread (polydioxanone). Arthrotomy or arthroscopy was not performed in any dog. At the end of surgery, a soft padded bandage was applied for 48 hours in order to reduce postoperative oedema. Rescue analgesia was administrated if needed. In the postoperative period, the dogs received antibiotic therapy for 6 days (Cefadroxil 20 mg/kg BID OS, Cefa-Cure Tabs, MSD Animal Health, USA) and non-steroidal anti-inflammatory therapy for 10 days (carprofen 3 mg/kg SID OS; Rymadil, Zoetis, Italy).
2.4. Isolation, Preparation and Inoculation of MFAT
During TPLO, about 4 g of thigh subcutaneous fat were harvested from dogs of the MFAT group. The fat was processed with the Rigenera® (HBW, Italy) system, a mechanical disruptor of biological tissue. It consists of a motorised apparatus that allows a sterile and disposable capsule (Rigeneracons®) to mechanically disrupt the tissue placed inside. Each Rigeneracons® is made up of a helical blade controlled by an electric motor that makes it rotate at 80 rpm, thus allowing a precise, uniform and constant cut. Furthermore, at the end of each helix there is a metal filter containing 100 holes of about 50 µm, each of which has six micro-scalpels. The desegregated and filtered tissue is collected at the bottom of the capsule, and thanks to a syringe connector it is possible to aspirate and use the preparation. About 1 mL of the obtained MFAT was inoculated intra-articularly in dogs of the MFAT group; the dogs of the NT group did not receive an inoculation. Intra-articular inoculation of the stifle joint was performed with medial para-patellar approach and an 18G needle.
2.5. Radiographic Evaluations
The patients were subject to an X-ray exam preoperatively, immediately after surgery (T0) and at 4 (T1) and 8 (T2) weeks after surgery. Radiographs of the stifle joint were taken in mediolateral and caudocranial view with the animal sedated. Only patients that showed good compression (no visible gap) on postoperative X-ray were included in the study. The mediolateral view was performed with the stifle and tarsus joints flexed at 90° and femoral condyles superimposed over each other. The caudocranial view involved that the medial cortex of calcaneus intersected the middle of the tibial trochlear with patella superimposed centrally between the femoral condyles.
Two radiographic scores, described previously [21] for the evaluation of bone healing after TPLO, were adopted by an expert (>20 years of experience) blinded orthopaedic surgeon. A 12-point scoring system (from 0 = no healing to 12 = complete remodelling) was used at T0, T1 and T2 (Table 1), while a 5-point scoring system (from 0 = no healing to 4 = 76%–100% healing) was used at T1 and T2 (Table 2).
2.6. Statistical Analysis
Statistical analysis was performed using MedCalc software version 9.2.10. All data were tested for normality with the Shapiro–Wilk test and are reported as mean ± standard deviation. Parametric data were analysed with two-way analysis of variance (ANOVA) for repeated measurements. A p-value < 0.05 was considered to be statistically significant.
3. Results
3.1. Enrolled Patients
The following patients were enrolled: four American Staffordshire Terriers, two American Pit Bull Terriers, two German Shepherds, three Labrador Retrievers, one Golden Retriever, one Rottweiler, two Cane Corso Italiano, two Deutscher Boxer and three mixed breed dogs. The mean weight was 30.37 ± 8.25 kg (31.98 ± 7.38 kg for the MFAT group; 28.75 ± 9.13 kg for the NT group; p = 0.396) and the mean age was 4 ± 1.74 years (3.9 ± 2.2 year for the MFAT group; 4.1 ± 1.52 years for the NT group; p = 0.806) at the time of surgery. The mean preoperative tibial plateau angle (TPA) was 27° ± 2.06° (range 23°–30°) and the mean postoperative TPA was 4.8° ± 1.4° (range 2°–7°). There were not differences in preoperative and postoperative TPA between MFAT and NT group (p = 0.92 and p = 0.789, respectively). Eighteen 3.5-mm TPLO plates (six 3.5-mm broad plates, eight 3.5-mm standard plates and four 3.5-mm small plates) and two 2.7-mm TPLO plates were used. The mean surgical time was 70 ± 2.31 minutes in the MFAT group and 64 ± 3.97 in the NT group. The average preparation time for MFAT was 5 minutes (range 4–6 minutes).
3.2. Radiographic Examination
All subjects showed satisfying radiographic compression of tibial osteotomy immediately after surgery (T0). Radiographic evaluation was also performed at 4 and 8 weeks after surgery (T1 and T2, respectively) for all patients. Bone healing was significantly (p < 0.05) increased at T1 and T2 compared with T0 in both the MFAT and NT groups (Figure 1). At T1, the 12- and 5-point scores were significantly (p < 0.05) higher for MFAT group (7.28 ± 0.75 and 3 ± 0.57, respectively) compared with the NT group (5.71 ± 1.38 and 2.14 ± 0.69, respectively). At T2, the MFAT group showed greater bone healing based on higher 12- and 5-point scores (10.85 ± 1.77 and 3.85 ± 0.37, respectively) than the NT group (9.71 ± 1.6 and 3.28 ± 0.48, respectively) (p < 0.05) (Figure 2 and Figure 3).
There were significant differences (p < 0.05) in the subjective degree of callus formation and the degree of rounding of the distal step at the osteotomy site between the MFAT group (2.6 ± 0.51 and 1.3 ± 0.48, respectively) and the NT group (1.6 ± 0.69 and 1 ± 0.66 respectively) at T1. At T2, the differences in the subjective degree of callus formation and degree of rounding of the distal step at the osteotomy site were significantly different (p < 0.05) between the MFAT group (3.6 ± 0.51 and 1.8 ± 0.42, respectively) and the NT group (2.9 ± 0.73 and 1.6 ± 0.51, respectively) (Figure 4 and Figure 5). In addition, there were significant differences (p < 0.05) in the 12-point score, the 5-point score, the subjective degree of callus formation and the degree of rounding of the distal step at the osteotomy site in the same group between T1 and T2.
4. Discussion
Although some studies have demonstrated the potentiality of ADSCs to promote bone healing in some bone segments, this is the first study to evaluate the efficacy of adipose autologous micrograft on acute bone healing in subjects undergoing TPLO. Our results show a significantly superior osteogenic response already after 30 days compared with the untreated group. These results can be attributed to the effectiveness of the complex heterogeneous mixture of cells in MFAT: ADSCs, endothelial progenitor cells, smooth muscle cells, pericytes, fibroblasts, preadipocytes, myeloid cells, haematopoietic cells, monocytes, lymphocytes and granulocytes, as described previously [57,58].
The stem cells contained in MFAT are directly involved in the bone remodelling process. Specifically, they can differentiate into osteoblasts to promote bone formation and to secrete various cytokines to stimulate the differentiation of progenitor cells into endothelial cells to promote neoangiogenesis, with a beneficial effect on bone healing. In particular, ADSCs upregulate the expression of angiogenic (hepatocyte growth factor [HGF] and vascular endothelial growth factor [VEGF]), haematopoietic (granulocyte colony-stimulating factor [G-CSF]) and bone-formation-promoting (bone morphogenetic protein 2 [BMP-2] and transforming growth factor beta [TGF-β]) cytokines [59]. In other words, ADSCs favour the deposition of bone tissue by stimulating osteogenesis and angiogenesis. The literature mostly describes the use of pure stem cells together with autologous or synthetic scaffolds. The results are good especially in the treatment of bone defects; however, Topleau et al. [60] recently reported that SVF can also induce osteogenesis without invasive techniques involving bone grafting or alloplastic scaffolds. Even Saxer et al. [38] demonstrated that SVF can form vascular structures and bone tissue within a fracture, without expansion or exogenous priming. MFAT increase TGF-β1 expression in rats with fractures and large bone defects. TGF-β1 is a growth factor that modulates bone healing primarily through the stimulation of undifferentiated mesenchymal cells by inducing osteoblast proliferation [61,62,63].
In our experience, the preparation of the autologous subcutaneous tissue by mechanical disaggregation was simple and fast: it took no more than 6 minutes in total. Compared with bone marrow–derived mesenchymal stem cells, MFAT is an easily accessible and rich source of stem cells that can be prepared intraoperatively with minimal manipulation and no expansion. Overall, there are several characteristics of adipose tissue that have made it the most promising and appreciated source of stem cells: less painful sampling and a stem cell yield 500 times higher than that obtained from bone marrow (only 0.001%–0.01% of the harvested bone marrow cells are mesenchymal stem cells), especially in elderly subjects [64,65,66,67]. In clinical routine, MFAT is often used rather than pure stem cells from bone marrow, due to the ease of isolation and legislative restrictions on the use of enzymes to isolate stem cells from fat or marrow [68]. Among other factors, MFAT has produced better therapeutic results than ADSCs in comparative studies on animal models because it has a heterogeneous composition that promotes more paracrine activity, cellular interactions and immunomodulation [44,69]
Several techniques, alone or in combination, have been described for nonenzymatic isolation of SVF, including filtration, centrifugation, vibration, disruption, shearing and vortexing. Using a mechanical disruptor to obtain MFAT was easy, affordable (relatively low cost of the equipment and consumables) and relatively quick [70]. Mechanical procedures for isolating SVF from adipose tissue represent a valid alternative to the enzymatic method, bypassing the ‘minimal manipulation’ limits strictly regulated by European laws. Consistent with the human literature [71], in a recent study involving dogs [42] the researchers sampled adipose tissue from the thigh. Subcutaneous adipose tissue is a more accessible and abundant source of stem cells than visceral adipose tissue [72]. Conversely, it is a less suitable sampling site in older or emaciated subjects [73,74]. In our case there were no difficulties in fat collection, which was performed at the same time as the TPLO surgical approach.
Fat excision could give a much higher number of nucleated cells compared with liposuction [75]. Liposuction involves the use of vacuum pressure that is more traumatic for the tissue, leading to adipocyte structural disruption [76]. On the contrary, direct excision represents a more delicate harvesting technique and creates large fat particles that preserve stromal constituents, providing structural support for adipocytes and proliferating stem cells [77]. In addition, tumescent solution used for liposuction can reduce ADSC survival [78]. The fragmentation of adipose tissue represents a suitable mechanical approach with cell yield and viability that are comparable to enzymatic procedures. According to the literature, we think that to date, MFAT is the way to go in clinical regenerative applications involving adipose tissue due to processing time and legislative restrictions [79].
MFAT was inoculated intra-articularly immediately after surgery. As reported by Taroni et al. [24], after TPLO surgery, mesenchymal stem cells and their secreted substances contained in the synovial fluid come into contact with the osteotomy site. This route of administration is minimally invasive (only one injection with an 18G needle) and does not intervene directly at the osteotomy site. Therefore, this simple procedure lends itself to being used easily and speedily in a clinical setting.
In our study, the majority of subjects in both groups showed >70% radiographic bone healing with at least three continuous cortices 8 weeks after TPLO. However, the MFAT group showed increased bone healing and callus density compared with the NT group at both T1 and T2. In particular, the MFAT group showed acceleration of bone healing at the first follow-up (4 weeks after TPLO). Callus formation, a ‘step’ distal to the osteotomy, and reduced visibility of the osteotomy line were significantly increased in the MFAT group at the latest follow-up (T2). The T1 results agree with a similar study evaluating the effect of ADSCs on bone healing in dogs undergoing tibial tuberosity advancement surgery; however, the authors did not show significant differences between the treated group and the control group in the subsequent follow-up (60 days) [80]. Franco et al. [81] reported that the use of minimally invasive plate osteosynthesis (MIPO) in association with ADSC administration stimulated bone healing after a tibia fracture. They had promising results because, in their study, clinical bone healing occurred on average 28.5 and 70.3 days after treatment, respectively, in the stem cell and control groups. The use of a minimally invasive surgical approach in fracture repair preserves soft tissue blood supply (especially from muscle structures), periosteal vasculature, and early fracture haematoma. The MIPO technique and ADSC administration play a key role in promoting and accelerating callus formation, maturation and remodelling by protecting the vascular network and enhancing neoangiogenesis. These two techniques in combination could certainly yield very interesting results and above all fully embrace the goal of minimally invasiveness if MFAT is use as source of ADSCs.
In contrast to some previous studies [22,82], which evaluated radiographic bone healing after TPLO using nonspecific scales, we assessed radiographic assessment by using two radiographic scores that have been described for the evaluation of bone healing after TPLO with more accurate results and minimising the margin of error. For this reason, radiographic exam included two orthogonal TPLO views (mediolateral and caudocranial view). We chose to assess bone healing with X-ray examination because it is widely available and has great practicality.
Among the limitations of the study, we can include the lack of a second-level diagnostic technique such as computed tomography and a histology that could characterise the formation of the bone callus. However, according to Italian legislation, clinical patients cannot be subjected to radiation or a bone biopsy if they do not need it (i.e. if it is only for research purposes). Other limitations of this study include the small number of cases enrolled, the lack of an intermediate time between T1 and T2 and it is difficult to control all factors affecting bone healing.
In the future it might be interesting to evaluate the progression of osteoarthritis in the knee joint treated with MFAT after TPLO surgery compared with a control group.
5. Conclusions
In conclusion, we can state that the mechanical disaggregation of adipose tissue represents a rapid and easy-to-perform method to prepare autologous MFAT that accelerates bone healing after an osteotomy or an acute fracture without complications. Additional studies are needed to truly understand the effect of MFAT on bone healing in pathological conditions that can lead to delayed union or non-union.
Author Contributions
Conceptualisation, L. P. and A.P.P..; methodology, L.P. and C.D.B.; formal analysis, L.P., A.S., F.R. and S.S.; investigation, L.P., A.S., F.R., S.S., and A.P.P.; resources, L.P., and A.P.P.; data curation, L.P. and C.D.B.; writing – original draft preparation, L.P., writing – review and editing, A.P.P..; visualisation, C.D.B.; supervision, A.P.P.; project administration, A.P.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Animal Welfare Body of the University of Camerino and received formal institutional approval in accordance with national and European law.
Informed Consent Statement
Not applicable.
Data Availability Statement
The clinical data used to support the findings of this study are included within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Witsberger, T. H.; Villamil, J. A.; Schultz, L. G.; Hahn, A. W.; Cook, J. L. Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. J. Am. Vet. Med. Ass. 2008, 232(12), 1818–1824. [CrossRef]
- Sellon, D. C.; Marcellin-Little, D. J. Risk factors for cranial cruciate ligament rupture in dogs participating in canine agility. BMC Vet. Res. 2022, 18(1), 39. [CrossRef]
- Griffon, D. J. A review of the pathogenesis of canine cranial cruciate ligament disease as a basis for future preventive strategies. Vet. Surg. 2010, 39(4), 399–409. [CrossRef]
- Comerford, E. J.; Smith, K.; Hayashi, K. Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Vet. Comp. Orthop. Traumatol. 2011, 24(2), 91–98. [CrossRef]
- Terhaar, H. M.; Muir, P.; Baker, L. A.; Binversie, E. E.; Chi, J.; Sample, S. J. Contribution of habitual activity to cruciate ligament rupture in Labrador retrievers. Vet. Comp. Orthop. Traumatol. 2020, 33(2), 82–88. [CrossRef]
- Kyllar, M.; Čížek, P. Cranial cruciate ligament structure in relation to the tibial plateau slope and intercondylar notch width in dogs. J. Vet. Sci. 2018, 19(5), 699–707. [CrossRef]
- Bergh, M. S.; Sullivan, C.; Ferrell, C. L.; Troy, J.; Budsberg, S. C. Systematic review of surgical treatments for cranial cruciate ligament disease in dogs. J. Am. An. Hosp. Ass. 2014, 50(5), 315–321. [CrossRef]
- Moore, K. W.; Read, R. A. Cranial cruciate ligament rupture in the dog—a retrospective study comparing surgical techniques. Austr. Vet. J. 1995, 72(8), 281–285. [CrossRef]
- Arnoczky, S. P. The over-the-top procedure: a technique for anterior cruciate ligament substitution in the dog. J. Am. Anim. Hosp. Assoc. 1979, 15, 283–290.
- Geels, J. J.; Roush, J. K.; Hoskinson, J. J.; McLaughlin, R. M. Evaluation of an intracapsular technique for the treatment of cranial cruciate ligament rupture. Vet. Comp. Orthop. Traumatol. 2000, 13(4), 197-203. [CrossRef]
- Kim, S. E.; Pozzi, A.; Kowaleski, M. P.; Lewis, D. D. Tibial osteotomies for cranial cruciate ligament insufficiency in dogs. Vet. Surg. 2008. 37(2), 111–125. [CrossRef]
- Gordon-Evans, W. J.; Griffon, D. J.; Bubb, C.; Knap, K. M.; Sullivan, M.; Evans, R. B. Comparison of lateral fabellar suture and tibial plateau leveling osteotomy techniques for treatment of dogs with cranial cruciate ligament disease. J. Am. Vet. Med. Ass. 2013, 243(5), 675–680. [CrossRef]
- Slocum, B.; Slocum T.D. Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Vet. Clin. North Am. Small Anim. Pract. 1993, 23(4), 777–795. [CrossRef]
- Hans, E. C.; Barnhart, M. D.; Kennedy, S. C.; Naber, S. J. Comparison of complications following tibial tuberosity advancement and tibial plateau levelling osteotomy in very large and giant dogs 50 kg or more in body weight. Vet. Comp. Orthop. Traumatol. 2017, 30(4), 299–305. [CrossRef]
- Krotscheck, U.; Nelson, S. A.; Todhunter, R. J.; Stone, M.; Zhang, Z. Long term functional outcome of tibial tuberosity advancement vs. tibial plateau leveling osteotomy and extracapsular repair in a heterogeneous population of dogs. Vet. Surg. 2016, 45(2), 261–268. [CrossRef]
- Corr, S. A.; Brown, C. A comparison of outcomes following tibial plateau levelling osteotomy and cranial tibial wedge osteotomy procedures. Vet. Comp. Orthop. Traumatol. 2007, 20(4), 312–319. [CrossRef]
- Fitzpatrick, N.; Solano, M.A. Predictive variables for complications after TPLO with stifle inspection by arthrotomy in 1000 consecutive dogs. Vet. Surg. 2010, 39(4), 460–474. [CrossRef]
- Conkling, Amanda L.; Bennett Fagin, R.; Daye, M. Comparison of tibial plateau angle changes after tibial plateau leveling osteotomy fixation with conventional or locking screw technology. Vet. Surg. 2010, 39(4), 475–481.
- Franklin, S. P.; Burke, E. E.; Holmes, S. P. The effect of platelet-rich plasma on osseous healing in dogs undergoing high tibial osteotomy. PLoS One. 2017, 12(5), e0177597. [CrossRef]
- Bergh, M. S.; Peirone, B. Complications of tibial plateau levelling osteotomy in dogs. Vet. Comp. Orthop. Traumatol. 2012, 25(5), 349–358. [CrossRef]
- Kieves, N. R.; MacKay, C. S.; Adducci, K.; Rao, S.; Goh, C.; Palmer, R. H.; Duerr, F. M. High energy focused shock wave therapy accelerates bone healing. Vet. Comp. Orthop. Traumatol. 2015, 28(6), 425–432. [CrossRef]
- Kieves, N. R.; Canapp, S. O.; Lotsikas, P. J.; Christopher, S. A.; Leasure, C. S.; Canapp, D.; Gavin, P. R. Effects of low-intensity pulsed ultrasound on radiographic healing of tibial plateau leveling osteotomies in dogs: a prospective, randomized, double-blinded study. Vet. Surg. 2018, 47(5), 614–622.
- Stewart, S. K. Fracture non-union: a review of clinical challenges and future research needs. Malays. Orthop. J. 2019, 13(2), 1. [CrossRef]
- Taroni, M.; Cabon, Q.; Fèbre, M.; Cachon, T.; Saulnier, N.; Carozzo, C.; Maddens, S.; Labadie, F.; Robert, C.; Viguier, E. Evaluation of the effect of a single intra-articular injection of allogeneic neonatal mesenchymal stromal cells compared to oral non-steroidal anti-inflammatory treatment on the postoperative musculoskeletal status and gait of dogs over a 6-month period after tibial plateau leveling osteotomy: a pilot study. Front. Vet. Sci. 2017, 4, 83. [CrossRef]
- Akpancar, S.; Tatar, O.; Turgut, H.; Akyildiz, F.; Ekinci, S. The current perspectives of stem cell therapy in orthopedic surgery. Arch. Traum. Res. 2016, 5(4). [CrossRef]
- Yoshida, Y.; Matsubara, H.; Fang, X.; Hayashi, K.; Nomura, I.; Ugaji, S.; Hamada, T.; Tsuchiya, H. Adipose-derived stem cell sheets accelerate bone healing in rat femoral defects. PLoS One. 2019, 14(3) e0214488. [CrossRef]
- Rada, T.; Reis, R. L.; Gomes, M. L. Adipose tissue-derived stem cells and their application in bone and cartilage tissue engineering. Tiss. Eng. 2009, 15(2), 113–125. [CrossRef]
- Tapp, H.; Hanley Jr, E. N.; Patt, J. C.; Gruber, H. E. Adipose-derived stem cells: characterization and current application in orthopaedic tissue repair. Exp. Biol. Med. 2009, 234(1), 1–9.
- Qomi, R. T.; Sheykhhasan, M. Adipose-derived stromal cell in regenerative medicine: a review. World J. Stem Cells. 2017, 9(8), 107. [CrossRef]
- Wang, X.; Wang, Y.; Gou, W.; Lu, Q.; Peng, J.; Lu, S. Role of mesenchymal stem cells in bone regeneration and fracture repair: a review. Intern. Orthop. 2013, 37, 2491–2498. [CrossRef]
- Ghiasi, M. S.; Chen, J.; Vaziri, A.; Rodriguez, E. K.; Nazarian, A. Bone fracture healing in mechanobiological modeling: a review of principles and methods. Bone Rep. 2017, 6, 87–100. [CrossRef]
- Zhu, H.; Liu, Y. L.; Chen, J. D.; Li, H.; Liu, Y. X.; Xu, F. F.; Jang, X.X.; Zhang, Y.; Mao, N. Effect of osteogenically and adipogenically differentiated bone mesenchymal stem cells from mouse on osteoclast formation. Zhongguo shi yan xue ye xue za zhi. 2012, 20(5), 1187–1190.
- Han, S.; Sun, H. M.; Hwang, K. C.; Kim, S. W. Adipose-derived stromal vascular fraction cells: update on clinical utility and efficacy. Crit. Rev. Euk. Gen. Exp. 2015, 25(2). [CrossRef]
- Gentile, P.; Sterodimas, A.; Pizzicannella, J.; Dionisi, L.; De Fazio, D.; Calabrese, C.; Garcovich, S. Systematic review: allogenic use of stromal vascular fraction (SVF) and decellularized extracellular matrices (ECM) as advanced therapy medicinal products (ATMP) in tissue regeneration. Int. J. Mol Sci. 2020, 21(14), 4982. [CrossRef]
- Mehranfar, S.; Rad, I.A.; Mostafav, E.; Akbarzadeh, A. The use of stromal vascular fraction (SVF), platelet-rich plasma (PRP) and stem cells in the treatment of osteoarthritis: an overview of clinical trials. Artif. Cells Nanomedicine Biotechnol. 2019, 47(1), 882–890. [CrossRef]
- Palumbo Piccionello, A.; Riccio, V.; Senesi, L.; Volta, A.; Pennasilico, L.; Botto, R.; Rossi, G.; Tambella, A.M.; Galosi, L.; Marini, C.; Vullo, C.; Gigante, A.; Zavan, B.; De Francesco, F.; Riccio, M. Adipose micro-grafts enhance tendinopathy healing in ovine model: An in vivo experimental perspective study. Stem Cells Transl. Med. 2021, 10(11), 1544–1560. [CrossRef]
- Rhee, S. C.; Ji, Y. H.; Gharibjanian, N. A.; Dhong, E. S.; Park, S. H.; Yoon, E. S. In vivo evaluation of mixtures of uncultured freshly isolated adipose-derived stem cells and demineralized bone matrix for bone regeneration in a rat critically sized calvarial defect model. Stem Cells Develop. 2011, 20(2), 233–242. [CrossRef]
- Saxer, F.; Scherberich, A.; Todorov, A.; Studer, P.; Miot, S.; Schreiner, S.; Guven, S.; Tchang, L.A.H.; Haugh, M.; Heberer, M.; Schaefer, D.J.; Rikli, D.; Martin, I.; Jakob, M. Implantation of stromal vascular fraction progenitors at bone fracture sites: from a rat model to a first-in-man study. Stem Cells. 2016, 34(12), 2956–2966. [CrossRef]
- Kim, A.; Kim, D. H.; Song, H. R.; Kang, W. H.; Kim, H. J.; Lim, H. C.; Cho, D.G.; Bae, J. H. Repair of rabbit ulna segmental bone defect using freshly isolated adipose-derived stromal vascular fraction. Cytotherapy. 2012, 14(3), 296–305. [CrossRef]
- François, P.; Rusconi, G.; Arnaud, L.; Mariotta, L.; Giraudo, L.; Minonzio, G.; Veran, J.; Bertrand, B.; Dumoulin, C.; Grimaud, F.; Lyonnet, L.; Casanova, D.; Giverne, C.; Cras, A.; Magalon, G.; Dignat-George, F.; Sabatier, F.; Magalon, J.; Soldati, G. Inter-center comparison of good manufacturing practices-compliant stromal vascular fraction and proposal for release acceptance criteria: a review of 364 productions. Stem. Cell. Res. Ther. 2021, 12, 1–11. [CrossRef]
- De Francesco, F.; Mannucci, S.; Conti, G.; Dai Prè, E.; Sbarbati, A.; Riccio, M. A non-enzymatic method to obtain a fat tissue derivative highly enriched in adipose stem cells (ASCs) from human lipoaspirates: preliminary results. Intern. J. Mol. Sci. 2018, 19(7), 2061. [CrossRef]
- De Francesco, F.; Riccio, V.; Biswas, R.; Busato, A.; Di Bella, C.; Serri, E.; Sbarbati, A.; Zavan, B.; Riccio, M.; Palumbo Piccionello, A. In Vitro characterization of canine microfragmented adipose tissue non-enzymatically extracted from the thigh and lumbar regions. Animals. 2021, 11(11), 3231. [CrossRef]
- Tremolada, C. Microfractured Adipose Tissue Graft (lipogems) and Regenerative Surgery. J. Orthop. Re.s Ther. 2022, 7, 1210.
- Vezzani, B.; Shaw, I.; Lesme, H.; Yong, L.; Khan, N.; Tremolada, C.; Péault, B. Higher pericyte content and secretory activity of microfragmented human adipose tissue compared to enzymatically derived stromal vascular fraction. Stem Cells Transl. Med. 2018, 7(12), 876–886. [CrossRef]
- Copcu, H.E. A new classification for adipose-derived stromal-cell systems. Plast. Recon. Surg. 2022, 10(12), e4712. [CrossRef]
- Trivisonno, A., Alexander, R. W., Baldari, S., Cohen, S. R., Di Rocco, G., Gentile, P., Magalon, G., Magalon, J., Miller, R.B., Womack, H., Toietta, G. Intraoperative strategies for minimal manipulation of autologous adipose tissue for cell-and tissue-based therapies: concise review. Stem Cells Transl. Med. 2019, 8(12), 1265–1271. [CrossRef]
- Raffaini, M.; Tremolada, C. Micro fractured and purified adipose tissue graft (Lipogems®) can improve the orthognathic surgery outcomes both aesthetically and in postoperative healing. CellR4. 2014, 2(4), e1118.
- Striano, R. D.; Battista, V.; Bilboo, N. Non-responding knee pain with osteoarthritis, meniscus and ligament tears treated with ultrasound guided autologous, micro-fragmented and minimally manipulated adipose tissue. Open J. Regene. Med. 2017, 6(2), 17–26. [CrossRef]
- Lonardi, R.; Leone, N.; Gennai, S.; Trevisi Borsari, G.; Covic, T.; Silingardi, R. Autologous micro-fragmented adipose tissue for the treatment of diabetic foot minor amputations: a randomized controlled single-center clinical trial (MiFrAADiF). Stem Cell Res. Ther. 2019, 10(1), 1–9. [CrossRef]
- Cattaneo, G.; De Caro, A.; Napoli, F.; Chiapale, D.; Trada, P., Camera, A. Micro-fragmented adipose tissue injection associated with arthroscopic procedures in patients with symptomatic knee osteoarthritis. BMC Musculoskelet. Disord. 2018, 19(1), 1–7. [CrossRef]
- Giori, A.; Tremolada, C.; Vailati, R.; Navone, S. E.; Marfia, G.; Caplan, A. I. Recovery of function in anal incontinence after micro-fragmented fat graft (Lipogems®) injection: two years follow up of the first 5 cases. CellR4. 2015, 3(2), e1544.
- Botto, R.; Riccio, V.; Galosi, L.; Rossi, G.; Vincenzetti, S.; Tambella, A. M.; De Francesco, F.; Pennasilico, L.; Riccio, M.; Salvaggio, A.; Sassaroli, S.; Palumbo Piccionello, A. Effects of intra-articular autologous adipose micrograft for the treatment of osteoarthritis in dogs: A prospective, randomized, controlled study. Animals. 2022, 12(14), 1844. [CrossRef]
- Pennasilico, L.; Di Bella, C.; Botto, R.; Murgia, E.; Riccio, V.; Piccionello, A. P. Use of micro-grafts in a chronic infected open wound after limb amputation in a cat. Vet. Med. 2021, 66(10), 448–455. [CrossRef]
- Zeira, O.; Scaccia, S.; Pettinari, L.; Ghezzi, E.; Asiag, N.; Martinelli, L.; Zahirpour, D.; Dumas, M.P.; Konar, M.; Lupi, D.V.; Fiette, L.; Pascucci, L.; Leonardi, L.; Cliff, A.; Alessandri, G.; Pessina, A.; Spaziante, D.; Aralla, M. Intra-articular administration of autologous micro-fragmented adipose tissue in dogs with spontaneous osteoarthritis: safety, feasibility, and clinical outcomes. Stem Cells Transl. Med. 2018, 7(11), 819–828. [CrossRef]
- Pavarotti, G. S.; Hivernaud, V.; Brincin, M.; Roche, R.; Barreau, P.; Festy, F.; Gauthier, O. Evaluation of a single intra-articular injection of autologous adipose tissue for the treatment of osteoarthritis: a prospective clinical study in dogs. Vet Comp. Orthop. Traumatol. 2020, 33(4), 258–266. [CrossRef]
- Fujino, H., Honnami, M.; Mochizuki, M. Preoperative planning for tibial plateau leveling osteotomy based on proximal tibial width. J. Vet. Med. Sci. 2020, 82(5), 661–667. [CrossRef]
- Nguyen, A.; Guo, J.; Banyard, D. A.; Fadavi, D.; Toranto, J. D.; Wirth, G. A.; Payadar, K.J.; Evans, G.R.D.; Widgerow, A. D. Stromal vascular fraction: a regenerative reality? Part 1: current concepts and review of the literature. J. Plast. Reconstr. Aesthet. Surg. 2016, 69(2), 170–179. [CrossRef]
- Busato, A.; De Francesco, F.; Biswas, R.; Mannucci, S.; Conti, G.; Fracasso, G.; Conti, F.; Riccio, V.; Riccio, M.; Sbarbati, A. Simple and rapid non-enzymatic procedure allows the isolation of structurally preserved connective tissue micro-fragments enriched with SVF. Cells. 2020, 10(1), 36. [CrossRef]
- Trzyna, A.; Banaś-Ząbczyk A. Adipose-derived stem cells secretome and its potential application in “stem cell-free therapy”. Biomolecules. 2021, 11(6), 878. [CrossRef]
- Toplu, G.; Ozcelik, D.; Serin, M.; Erdem, H.; Topacoglu, A. T. Adipose tissue-derived stromal vascular fraction increases osteogenesis in an experimental design zygomatic bone defect model. J. Craniof. Surgery. 2017, 28(8), 2179–2182. [CrossRef]
- Poniatowski, Ł. A.; Wojdasiewicz, P.; Gasik, R.; Szukiewicz, D. Transforming growth factor Beta family: insight into the role of growth factors in regulation of fracture healing biology and potential clinical applications. Mediators Inflamm. 2015, 2015. [CrossRef]
- Sarahrudi, K.; Thomas, A.; Mousavi, M.; Kaiser, G.; Köttstorfer, J.; Kecht, M.; Hajdu, S.; Aharinejad, S. Elevated transforming growth factor-beta 1 (TGF-β1) levels in human fracture healing. Injury. 2011, 42(8), 833–837. [CrossRef]
- Sananta, P.; Dradjat, R. S.; Rosandi, R. D.; Siahaan, L. D. TGF-1 biomarker level evaluation on fracture healing in a murine model with a bone defect after stromal vascular fraction application. Med. Glas. 2022, 19(1), 63–67. [CrossRef]
- Bukowska, J.; Szóstek-Mioduchowska, A. Z.; Kopcewicz, M.; Walendzik, K.; Machcińska, S.; Gawrońska-Kozak, B. Adipose-derived stromal/stem cells from large animal models: from basic to applied science. Stem Cell Rev. Rep. 2021, 17, 719–738. [CrossRef]
- Strioga, M.; Viswanathan, S.; Darinskas, A.; Slaby, O.; Michalek, J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Develop. 2012, 21(14), 2724-2752. [CrossRef]
- Tsuji, W.; Rubin, J. P.; Marra, K. G. Adipose-derived stem cells: implications in tissue regeneration. World J. Stem Cells. 2014, 6(3), 312. [CrossRef]
- El-Badawy, A.; Amer, M.; Abdelbaset, R.; Sherif, S. N.; Abo-Elela, M.; Ghallab, Y. H.; Abdelhamid, H.; Ismail, Y.; El-Badri, N. Adipose stem cells display higher regenerative capacities and more adaptable electro-kinetic properties compared to bone marrow-derived mesenchymal stromal cells. Sci. Rep. 2016, 6(1), 37801. [CrossRef]
- Yoshimura, K.; Shigeura, T.; Matsumoto, D.; Sato, T.; Takaki, Y.; Aiba-Kojima, E.; Sato, K.; Inoue, K.; Koshima, I.; Gonda, K. Characterization of freshly isolated and cultured cells derived from the fatty and fluid portions of liposuction aspirates. J. Cell. Phys. 2006, 208(1), 64–76. [CrossRef]
- Guo, J.; Nguyen, A.; Banyard, D. A.; Fadavi, D.; Toranto, J. D.; Wirth, G. A.; Paydar, K.Z.; Evans, G.R.D.; Widgerow, A. D. Stromal vascular fraction: a regenerative reality? Part 2: mechanisms of regenerative action. J. Plast. Reconstr Aesthet Surg. 2016, 69(2), 180–188. [CrossRef]
- Oberbauer, E.; Steffenhagen, C.; Wurzer, C.; Gabriel, C.; Redl, H.; Wolbank, S. Enzymatic and non-enzymatic isolation systems for adipose tissue-derived cells: current state of the art. Cell Regen. 2015, 4(1), 1–14. [CrossRef]
- Dai Prè, E.; Busato, A.; Mannucci, S.; Vurro, F.; De Francesco, F.; Riccio, V.; Sbarbati, A. In vitro characterization of adipose stem cells non-enzymatically extracted from the thigh and abdomen. Int. J. Mol. Sci. 2020, 21(9), 3081. [CrossRef]
- Neupane, M.; Chang, C. C.; Kiupel, M.; Yuzbasiyan-Gurkan, V. Isolation and characterization of canine adipose–derived mesenchymal stem cells. Tiss. Eng. 2008, 14(6), 1007–1015.
- Hendawy, H.; Uemura, A.; Ma, D.; Namiki, R.; Samir, H.; Ahmed, M. F.; El-Husseiny, H.M.; Chieh-Jen, C.; Tanaka, R. Tissue harvesting site effect on the canine adipose stromal vascular fraction quantity and quality. Animals. 2021, 11(2), 460. [CrossRef]
- Astor, D. E.; Hoelzler, M. G.; Harman, R.; Bastian, R. P. Patient factors influencing the concentration of stromal vascular fraction (SVF) for adipose-derived stromal cell (ASC) therapy in dogs. Can. J. Vet. Res.. 2013, 77(3), 177–182.
- Yaylacı, S.; Kaçaroğlu, D.; Hürkal, Ö.; Ulaşlı, A. M. An enzyme-free technique enables the isolation of a large number of adipose-derived stem cells at the bedside. Sci. Rep. 2023, 13(1), 8005.
- Fontes, T.; Brandão, I.; Negrão, R.; Martins, M. J.; Monteiro, R. Autologous fat grafting: harvesting techniques. Ann. Med. Surg. 2018, 36, 212–218. [CrossRef]
- Gause, T. M.; Kling, R. E.; Sivak, W. N.; Marra, K. G.; Rubin, J. P.; Kokai, L. E. Particle size in fat graft retention: a review on the impact of harvesting technique in lipofilling surgical outcomes. Adipocyte. 2014, 3(4), 273–279. [CrossRef]
- Francis, A.; Wang, W. Z.; Goldman, J. J.; Fang, X. H.; Williams, S. J.; Baynosa, R. C. Enhancement of viable adipose-derived stem cells in lipoaspirate by buffering tumescent with sodium bicarbonate. Plas. Reconstr. Surg. Glob. Op. 2019, 7(3). [CrossRef]
- Aronowitz, J.A.; Lockhart R.A.; Cloe S. Hakakian. Mechanical versus enzymatic isolation of stromal vascular fraction cells from adipose tissue. Springerplus. 2015, 4(1), 1–9. [CrossRef]
- Rocha dos Santos, C.; da Rocha Filgueiras, R.; Furtado Malard, P.; Rodrigues da Cunha Barreto-Vianna, A.; Nogueira, K.; da Silva Leite, C.; Maurício Mendes de Lima, E. Mesenchymal stem cells in osteotomy repair after tibial tuberosity advancement in dogs with cranial cruciate ligament injury. J. Exp. Orthop. 2018, 5(1), 1–8.
- Franco, G. G.; Minto, B. W.; Dreibi, R. M.; Costa Junior, J. S.; Dias, L. G. G. G. Percutaneous application of allogeneic adipose-derived mesenchymal stem cell in dogs submitted to minimally invasive plate osteosynthesis of the tibia. Acta Cir. Bras. 2021, 36. [CrossRef]
- Hoffer, M. J.; Griffon, D. J.; Schaeffer, D. J.; Johnson, A. L.; Thomas, M. W. Clinical applications of demineralized bone matrix: A retrospective and case-matched study of seventy-five dogs. Vet. Surg. 2008, 37(7), 639–647. [CrossRef]
Figure 1.
Radiographs of subjects treated with microfragmented adipose tissue (MFAT) immediately after tibial plateau levelling osteotomy (TPLO) (a and b) and after 8 weeks (c and d) show a significant degree of rounding of the distal step at the osteotomy site and callus formation (white arrow) with no osteotomy line visibility (black arrow). Radiographs of control group subject immediately after TPLO (e and f) and after 8 weeks (g and h) show a minimal degree of callus formation (white arrow) with osteotomy line visibility (black arrow).
Figure 1.
Radiographs of subjects treated with microfragmented adipose tissue (MFAT) immediately after tibial plateau levelling osteotomy (TPLO) (a and b) and after 8 weeks (c and d) show a significant degree of rounding of the distal step at the osteotomy site and callus formation (white arrow) with no osteotomy line visibility (black arrow). Radiographs of control group subject immediately after TPLO (e and f) and after 8 weeks (g and h) show a minimal degree of callus formation (white arrow) with osteotomy line visibility (black arrow).
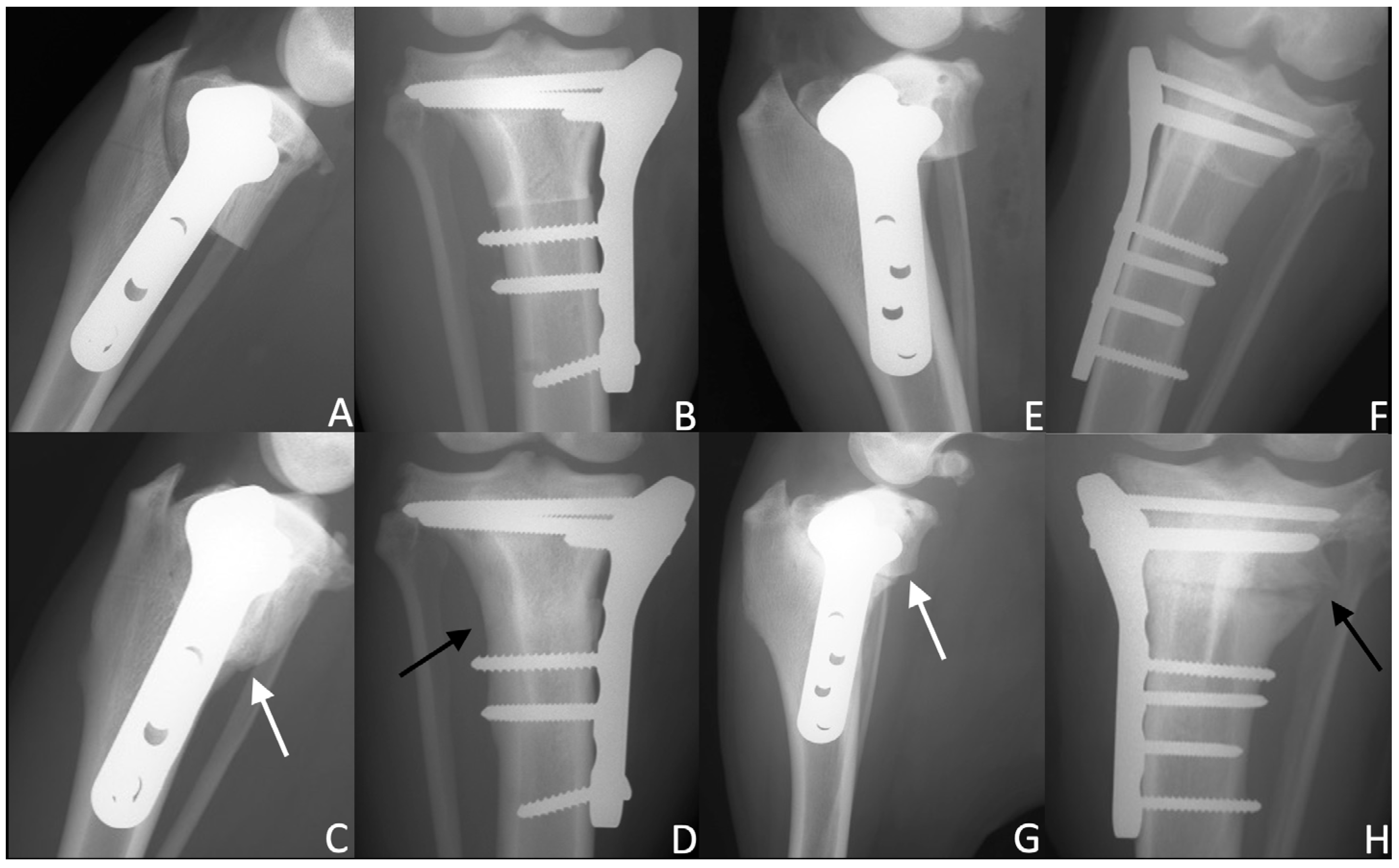
Figure 2.
This graph shows the radiographic healing based on the 12-point scoring system at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
Figure 2.
This graph shows the radiographic healing based on the 12-point scoring system at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
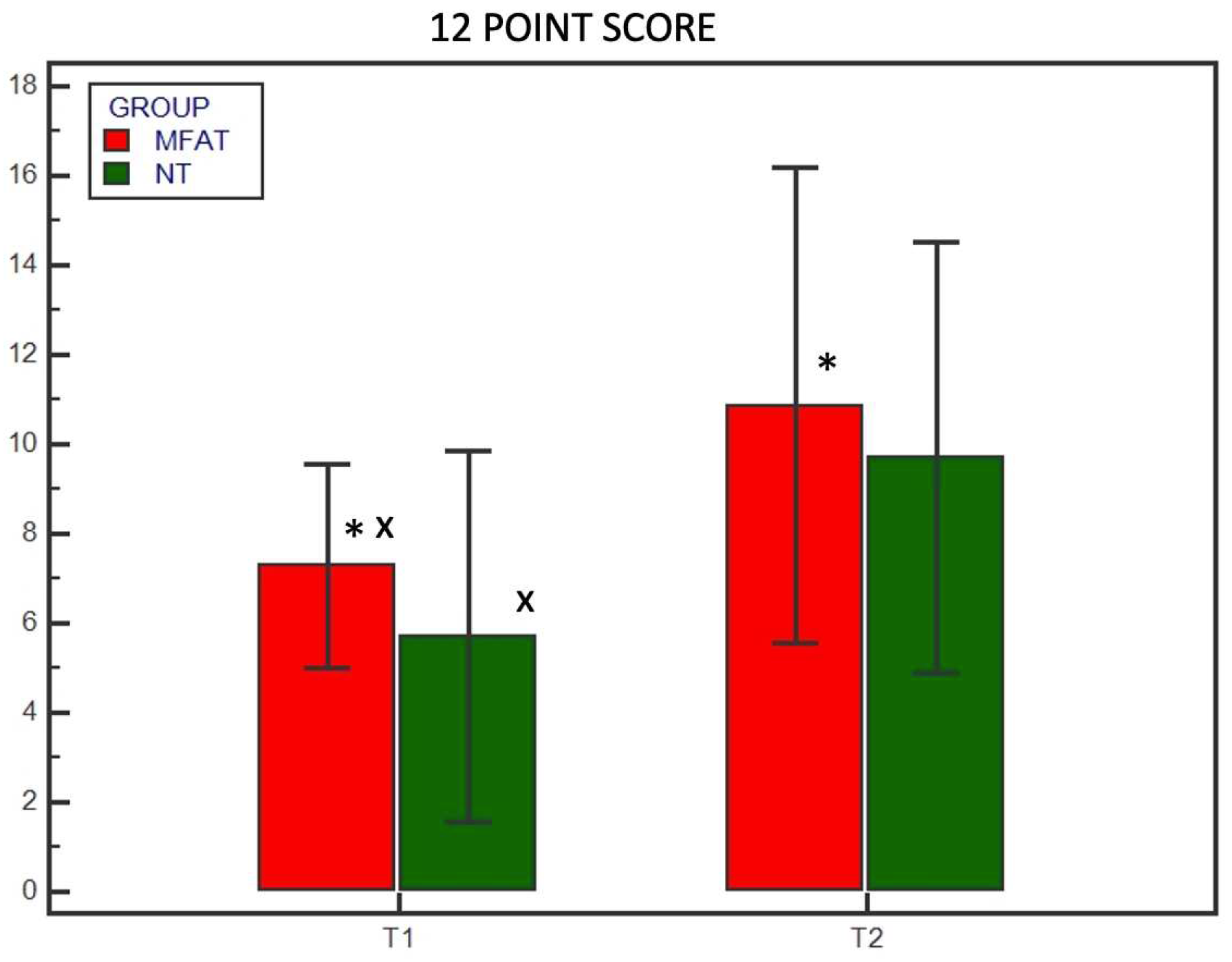
Figure 3.
This graph shows the radiographic healing based on the 5-point scoring system at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
Figure 3.
This graph shows the radiographic healing based on the 5-point scoring system at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
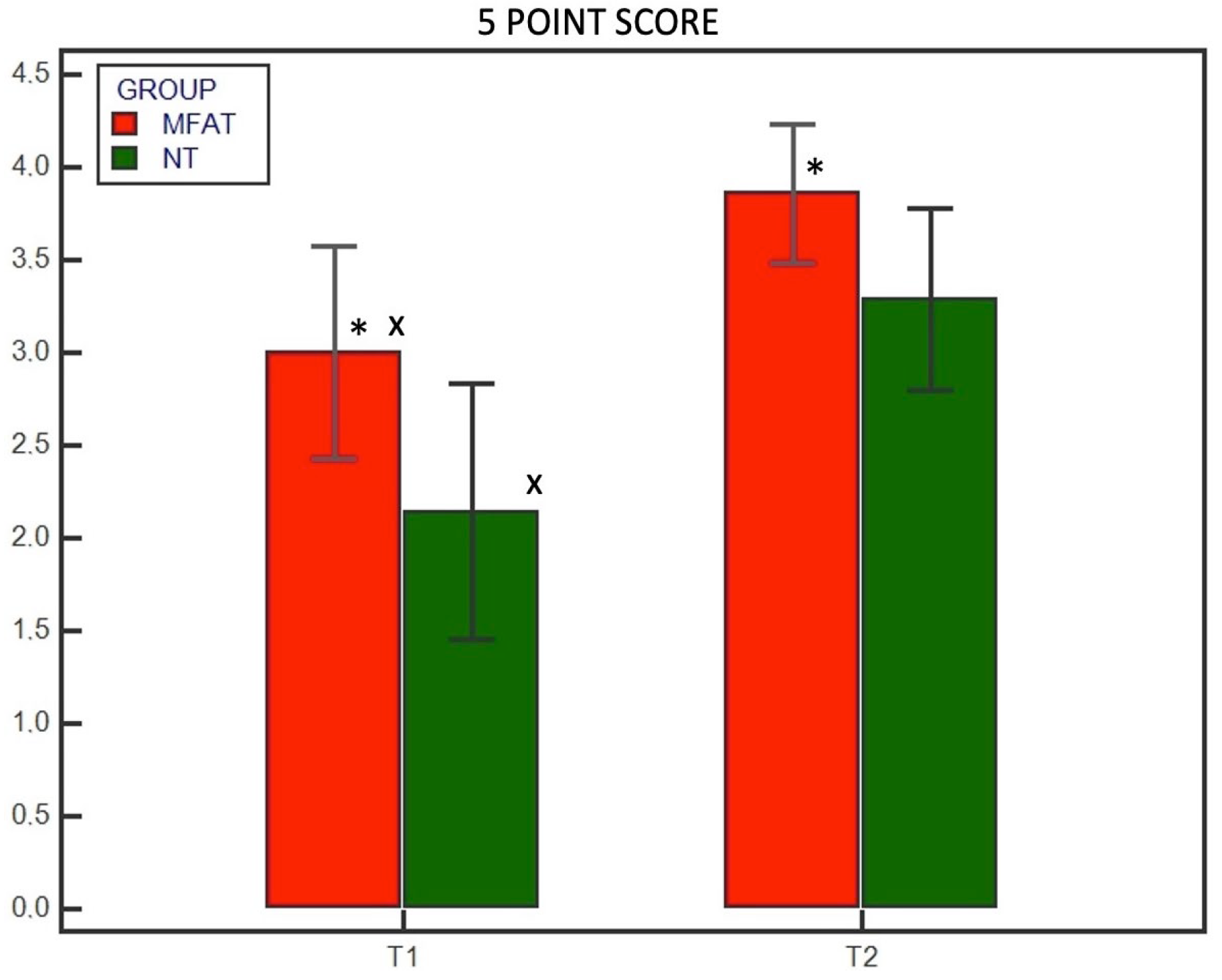
Figure 4.
This graph shows the degree of rounding of the distal step at the osteotomy site at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
Figure 4.
This graph shows the degree of rounding of the distal step at the osteotomy site at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
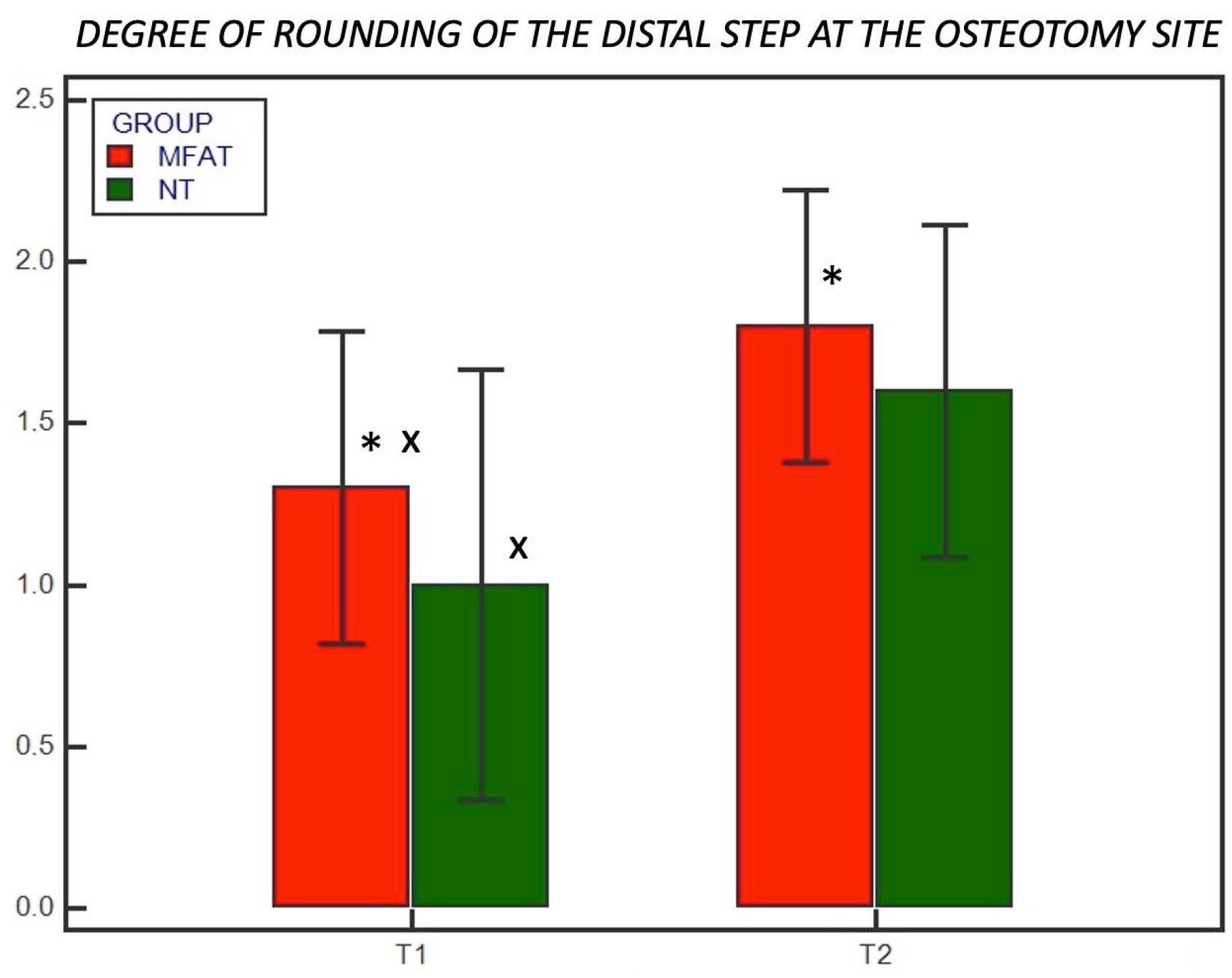
Figure 5.
This graph shows the subjective degree of callus formation at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
Figure 5.
This graph shows the subjective degree of callus formation at T1 (4 weeks) and T2 (8 weeks) for the microfragmented adipose tissue (MFAT) group (red) and the control (NT) group (green). ∗ indicates a significant difference between the groups (p < 0.05); x indicates a significant difference within the same group between T1 and T2 (p < 0.05).
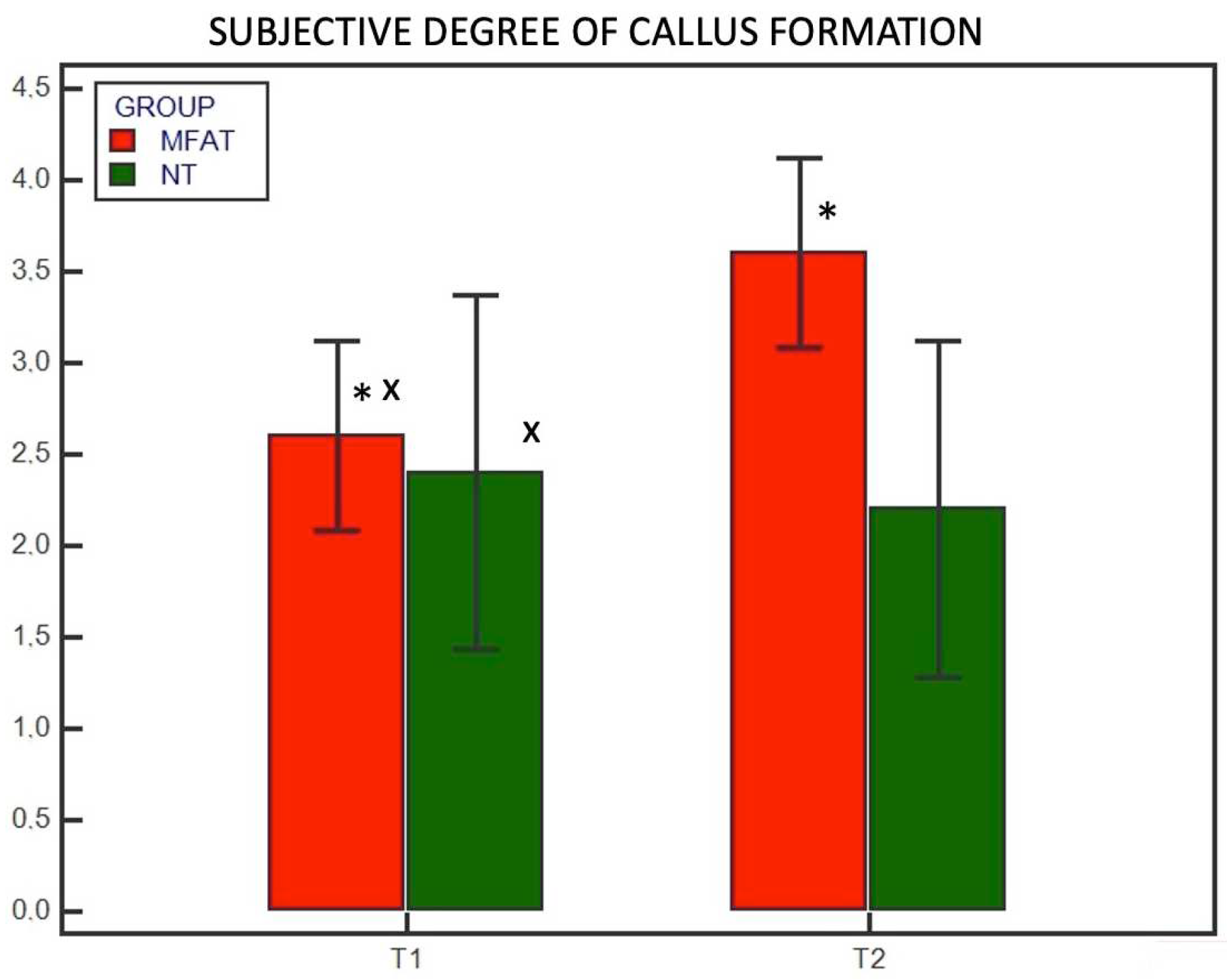

Table 1.
The 12-point scoring system with the specific parameters evaluated for bone healing.
| 12-point scoring system | |
| Cortical continuity (0–4) | 0 = no cortical continuity 1 = one continuous cortex 2 = two continuous cortices 3 = three continuous cortices 4 = four continuous cortices |
| Osteotomy line visibility (0–2) |
0 = osteotomy line visibility 1 = osteotomy line barely visible 2 = no osteotomy line visible |
| Subjective degree of callus formation or remodelling (0–4) |
0 = none 1 = minimal 2 = moderate 3 = remodelled 4 = healed |
|
Degree of rounding of the distal step at the osteotomy site (0–2) |
0 = none 1 = mild 2 = significant |
Table 2.
The 5-point scoring system with the percentage of bone healing associated with each score.
| 5-point scoring system | |
| 0 | No healing |
| 1 | 1%– 25% healing |
| 2 | 26%– 50% healing |
| 3 | 51%– 75% healing |
| 4 | 76%– 100% healing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



