
Submitted:
05 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
Background: Pneumocystis pneumonia (PCP) commonly affects immunocompromised individuals, whereas in immunocompetent persons, it occurs relatively rarely, and in most cases the Pneumocystis infection is detected as an asymptomatic colonization. The present study aimed to establish the prevalence of Pneumocystis jirovecii infection in human hosts with different immune status (immunocompromised and immunocompetent), using molecular diagnostic methods, and to compare their diagnostic value with that of classical staining methods. Methods: We used the collected to this moment data from a prospective study on the prevalence of pneumocystosis among the Bulgarian population. Clinical specimens (including throat secretion, induced sputum, tracheal aspirate, and bronchoalveolar lavage collected from 220 patients suspected of PCP (153 immunocompetent and 67 immunocompromised patients) were examined with staining microscopic methods and real-time PCR for detection of P. jirovecii. Results: DNA of the pathogen was detected in 38 (17%) specimens (32 immunocompromised patients and 6 immunocompetent subjects). From all 220 clinical samples examined by staining methods, only in five (2%) P. jirovecii cysts were detected by the Gomori's stain. All patients with PCP were treated with trimethoprim-sulfamethoxazole, but in ten of them (HIV- positive patients) the disease was with fatal outcome. Conclusions: This study is the first for the country including the main available laboratory methods for diagnosis of human pneumocystosis in Bulgaria. Regarding the etiological diagnosis of PCP, in our study the sensitivity of real-time PCR was higher compared to the staining methods. The choice of a method for sample collection and examination has an important role in the efficiency of the laboratory diagnostics.
Keywords:
Pneumocystis pneumonia
; immune status
; real-time PCR
; staining methods
1. Introduction
The first reports of the involvement of Pneumocystis in human pathology date back to the 1940s as a pathogen causing pneumonia in malnourished or premature infants. Until the 1980s, Pneumocystis pneumonia (PCP) in the elderly was considered as a rare but fatal infection mainly among patients with acute leukemia and other haematological malignancies [1]. In the 1980s, after the onset of the global epidemic of human immunodeficiency virus (HIV) infection, interest in PCP increased dramatically as it was one of the leading co-infections being the cause of death in patients with Acquired Immune Deficiency Syndrome (AIDS). Due to advances in access to antiretroviral therapy (ART) and routine prophylaxis against PCP, its incidence in the HIV-infected population has decreased in most industrialized countries. However, PCP still remains the most common opportunistic infection among AIDS patients in many countries [2,3,4].
Pneumocystis can be present in the respiratory system without leading to the clinical presentation of severe pneumonia. Detection of Pneumocystis in individuals without clinical symptoms is defined as colonization [5]. Pulmonary colonization with P. jirovecii is common in immunocompromised patients, but is less frequent among immunocompetent individuals with lung disease [6,7,8].
In Bulgaria, pneumocystosis has been the subject of scientific interest for years. P. jirovecii was found in young children with pneumonia and in patients with AIDS [9 – 11]. The first case of pneumocystosis associated with AIDS in our country was diagnosed at the National Center of Infectious and Parasitic Diseases [12,13,14]. In a study (covering the period 1986-2000) of the prevalence and features of different types of opportunistic infections in HIV-infected and AIDS patients in Bulgaria, Pneumocystis was detected in 26 (16.25%) of 160 patients by direct microscopic examination (staining methods and immunofluorescence assay). The clinical manifestation of pneumocystosis was represented by pneumonia with a disseminated type of infection in one case [15]. In another study conducted between 1993 and 2003, pneumocystosis was diagnosed in 6.06% of the examined (n=165) patients [16].
The present study aimed to establish the prevalence of pneumocystosis in different groups of immunocompromised and immunocompetent individuals using molecular diagnostic methods, and to compare their diagnostic value with that of classical staining methods.
2. Materials and Methods
2.1. Study design
This article is based on data from a prospective study on the prevalence of pneumocystosis among the Bulgarian population, beginning in January 2019.
2.2. Ethical considerations
The study was reviewed and approved by the Institutional review board (IRB) 00006384 and informed consent was obtained from the patients. No information that could reveal the identity of the patients who participated in the study was used.
2.3. Patients and samples
Clinical specimens (including throat secretion, induced sputum, tracheal aspirate, and bronchoalveolar lavage (BAL)) collected from a total of 220 patients suspected of having pneumocystosis (Group 1 - immunocompetent patients and Group 2 - patients with compromised immune system) were examined.
Group 1 included a total of 153 individuals presenting with cough (n = 106), evidence of unspecified pneumonia (n = 23), shortness of breath (n = 4), respiratory failure (n = 3), hemoptysis (n = 3), bronchitis (n = 2), fatigue (n = 2), respiratory distress syndrome (n = 1), pharyngitis (n = 1), lung abscess (n = 1), and 7 with COVID-19 related pneumonia.
Group 2 consisted of 67 individuals - 47 with HIV infection and 20 on immunosuppressive therapy (including haematological disease, n = 7; interstitial pulmonary fibrosis, n = 3; nephrotic syndrome, n = 3; bronchiectasis, n = 3; solid organ transplantation, n = 2; asthma, n = 1, and disseminated lupus, n = 1).
2.4. Methods for detection of pathogen
2.4.1. Real-time PCR for qualitative and quantitative detection of P. jirovecii:
For extraction and purification of P. jirovecii DNA from clinical samples, PureLink™ Genomic DNA Mini Kit (Life Technologies Corporation, Carlsbad, CA 92008 USA) was used. Amplification of the gene encoding the mitochondrial large subunit of ribosomal RNA (mtL SU rRNA) was done by using RIDA®GENE kit (r-biofarm AG, Germany) according to the manufacturer's instructions.
2.4.2. Staining methods for detection of P. jirovecii:
Three staining methods for direct detection of P. jirovecii were applied. Six smears from each clinical material (throat secretion, induced sputum, tracheal aspirate, or bronchoalveolar lavage) of the PCP-suspected patient using clean glass microscope slides were prepared. After drying, two smears were stained by each of the three methods.
- Romanowski-Giemza staining (for trophozoites and cysts of P. jirovecii). Commercial Giemsa stain, modified solution (Sigma-Aldrich) was used. Dried thin smears were fixed with methyl alcohol for 5-10 minutes, dried, stained with a working solution of Giemsa stain for 20-22 minutes (the exposure was determined during the initial testing of the stain), washed with tap water and allowed to dry in a vertical position at room temperature.
- Toluidine blue staining (selective method for cysts of P. jirovecii). The thin smears from each clinical material were immersed for 5 minutes in sulfate reagent (prepared by mixing 25 ml diethyl ether and 25 ml concentrated sulfuric acid), rinsed with tap water, and stained with toluidine blue solution for 3 minutes. Differentiation was then performed in 2 shifts of isopropyl alcohol for 15-30 seconds, lightening with xylene and finally drying.
- Staining with methenamine-silver nitrate according to Gomori (for cysts of P. jirovecii). The method is considered the "gold standard" for microscopic visualization of P. jirovecii cysts. Microscopy Methenamine silver plating kit acc. to Gomori (Cat. No. 1.00820.0001; Merck KGaA, 64271 Darmstadt, Germany, Sigma-Aldrich Canada Co. or Millipore, Canada Ltd.) was used. The dried smears of the relevant clinical material were fixed for 30 minutes in 3.5% formalin and stained according to the manufacturer's protocol. The color of the cyst wall varies from gray to black (their surface membranes are visible).
- The samples were examined under a light microscope (Euromex IS.1153-Pli, The Netherlands) at 400x and 1000x magnification and visualized using color digital camera (Euromex DC.6000s, The Netherlands).
3. Results
We applied real-time PCR targeting the mtL SU rRNA gene of P. jirovecii for qualitative and quantitative detection of the pathogen from clinical specimens of the patients included in the study. P. jirovecii DNA was detected in the specimens of 38 (17%) out of 220 subjects examined. Positive PCR results were obtained in specimens of 6 patients with pneumonia of the 153 individuals of group 1. In group 2, amplification of a fragment of the target gene was obtained in 26 of the HIV-infected patients and 6 patients receiving suppressive therapy (Table 1).
Commercial kit RIDA®GENE Pneumocystis jirovecii (r-biofarm AG, Germany), containing standards with a certain number of copies of P. jirovecii (Standard A: 101 copies/µӏ, Standard B: 103 copies/µӏ, Standard B: 105 copies/µӏ; analytical sensitivity: ≥ 10 DNA copies per reaction) was used for pathogen load assessment in the tested samples. In the post-treatment period for Pneumocystis pneumonia, 4 patients of the immunocompromised group and 3 patients without immunosuppression were additionally tested in follow-up studies for assessment of their response to the therapy. The reason for these additional tests was the patient's continuing complaints of shortness of breath, cough, and ongoing fever. Except for one HIV-infected patient, in all others, we found that the control sample taken within one month after the end of therapy did not contain P. jirovecii DNA. The complaints of the patient with HIV infection, whose control sample had a positive PCR result one month after the examination of the primary clinical specimen (induced sputum), continued despite the prescribed etiological treatment. On the background of assigned secondary prophylaxis with TMP/SMX, a total of 9 control tests a month apart from each other were performed for monitoring the response of the treatment, and only in the last sample no DNA of the pathogen was detected [17].
All 220 clinical samples of patients suspected of having pneumocystosis from Groups 1 and 2 were examined by staining methods. In patients from Group 1, staining methods showed no evidence of P. jirovecii cysts, while in five of Group 2 patients, the presence of P. jirovecii cysts was detected only by the Gomori's methenamine silver stain (Table 1, Figure 1).
The results of Gomori's staining, quantification of DNA load, and PCR cycle (Ct value), in which a fluorescent signal was reported as a result of multiplication of the target region of DNA molecule in the test sample are presented in Table 2.
In some patients, we also performed a comparative study on the concentration of P. jirovecii DNA depending on the type of clinical specimen (Table 3).
4. Discussion
Cases of HIV-associated PCP are reported at fluctuating rates throughout the world. While the clinical manifestation of PCP in HIV-positive patients is well known and consists most often of the triad of dyspnea, fever, and cough, the presentation of PCP in HIV-negative patients is atypical and occurs suddenly with oxygen desaturation and rapid dead if left untreated [19]. This pathology is a serious public health problem not only because of the severity of the disease but also because PCP is a life-threatening condition in HIV-negative immunocompromised patients [18]. Another public health problem is the number of colonized patients in hospital wards, where other patients may be at high risk of infection or colonization [20].
According to the literature, the diagnosis of PCP or colonization depends on a complex algorithm based on the patient's medical history, laboratory and radiological data, treatment, and clinical evolution of the patient's condition. If a positive microscopic examination leads to a high probability of PCP, a negative quantitative PCR (qPCR) result cannot rule out the diagnosis, especially in HIV-negative patients. In most cases, qPCR is sensitive enough to allow the diagnosis of PCP in HIV patients, however, the presence of a gray area of Ct values prevents this analysis from becoming a reference method [21]. In the case of Ct value in the gray area, the physician will have to choose between prophylactic or active treatment according to the clinical parameters of the disease and the patient's condition [18].
With this study, we demonstrate that the use of real-time PCR can significantly improve the differential diagnosis in patients suspected of having P. jirovecii infection and to clarify the infection epidemiology in immunocompromised patients and those without immunosuppression.
Our data shows that of the 153 examined individuals without evidence of compromised immunity, 4% (n = 6) tested positive for P. jirovecii DNA. All of them were with severe pneumonia and PCP-specific radiological findings. While in 66.7% (n = 4) of them the condition can be explained by their infant (0 - 12 months) and child age (14 years), the remaining 33.3% (n = 2) were adults over 18 years old and the development of PCP was difficult to explain. The most significant risk factors for PCP in HIV-free patients are the use of glucocorticoids and the presence of cell-mediated immune defects, which lead to changes in lung surfactant, thus predisposing the patient to pneumonia [22]. There have been several reports of PCP in patients without underlying immunosuppressive disease. A study by Kano et al. described five patients who developed PCP without any underlying immunosuppressive conditions, and in their literature review, they identified only 11 other reported cases [23]. However, the exact mechanisms that lead to the development of PCP in patients without evidence of immunosuppressive status remain unclear [24].
From included in the study individuals with compromised immunity and lung pathology, 47.8% (n = 32) showed the presence of P. jirovecii DNA. Of them, 26 (38.8%) were HIV infected and 6 (8.96%) were with other immunosuppressive conditions (Table 1). The age distribution shows a prevalence of patients over 18 years of age (n = 29, 90.6%), while three of the patients (9.4%) were in the age group from 1 to 9 years. One of the children was HIV-positive, and two were non-HIV-infected. One child developed PCP symptoms on the background of oncohematological disease, and the other was on long-term corticosteroid therapy for nephrotic syndrome. In the group of immunocompromised patients, the distribution by sex showed a predominance of males (n = 26, 81.3%) compared to females (n = 6, 18.7%). In general, our data are similar to those in the literature for people at risk for developing PCP pneumonia [25].
Regarding the etiological diagnosis of Pneumocystis pneumonia, staining with methenamine-silver nitrate according to Gomori is considered as the "gold standard" for microscopic visualization of P. jirovecii cysts. However, our study gives us reason to consider that the real-time PCR is more useful for diagnostic purposes than the staining methods (Table 1). Patients with compromised immunity were more likely to have detectable cysts of the pathogen in obtained from them clinical specimens than those without immunosuppression. The data from our study prove the existence of a correlation between the levels of the pathogen load and the detectability of P. jirovecii cysts with staining methods (Table 2).
The choice of a method for sample collection and examination has an important role in the efficiency of the laboratory diagnostics. Results showed that various clinical specimens (induced sputum, tracheal aspirate, and BAL) can be tested to diagnose pneumocystosis. Our initial observations revealed that in infants and young children, the tracheal aspirate is a good enough clinical sample for genetic testing.
In Bulgaria, the first-line agent for the treatment of PCP is trimethoprim-sulfamethoxazole, regardless of the patient's immune status, while the use of additional drugs and oxygen therapy depends on the patient's condition and is in accordance with generally accepted international guidelines.
In the post-treatment period for Pneumocystis pneumonia, 4 patients in the immunocompromised group and 3 patients without immunosuppression had follow-up studies to assess their response to the therapy. The reason for this was continuing complaints such as shortness of breath, cough, and fever. With the exception of one HIV-infected patient, in all others, we found that the control sample taken within one month after the end of therapy did not contain P. jirovecii DNA.
Unfortunately, in ten of the patients (HIV-positive people) the disease was fatal. The mortality rate among people with PCP for the period studied by us was 26.3%, and our data are similar to the literature [26, 27].
5. Conclusions
This study is the first in the country including the main available laboratory methods for the diagnosis of human pneumocystosis in Bulgaria. Regarding the etiological diagnosis of PCP, based on our study, the sensitivity of real-time PCR is higher compared to the staining methods. The choice of a method for sample collection and examination plays an important role in the efficiency of the laboratory diagnostics.
Author Contributions
All authors (R.H., N.T., A.I., R.E., M.V., I.R., E.K., I.K., D.S., N.Y-P., I.S., V.L., N.Y.) were involved in drafting the article or revising it critically for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Bulgarian National Science Fund [grant number KP-06-N33/18, 2019] under the “Competition for financial support for basic research projects – 2019”.
Institutional Review Board Statement
Written consent was obtained according to the Declaration of Helsinki. The Institutional review board (IRB) 00006384 of the National Centre of Infectious and Parasitic Diseases (protocol number 2 from 11 May 2020) approved this retrospective study’s protocol.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kovacs, J.A.; Masur, H. Evolving health effects of Pneumocystis: one hundred years of progress in diagnosis and treatment. JAMA 2009, 301, 2578–2585. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Cattamanchi, A.; Davis, J.L.; Boon, S.D. , Kovacs, J.; Meshnick, S.; Miller, R.F.; Walzer, P.D.; Worodria, W.; Masur, H. HIV-Associated Pneumocystis Pneumonia. Proceedings of the American Thoracic Society 2011, 8, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Tasaka, S. Pneumocystis pneumonia in Human Immunodeficiency Virus-infected adults and adolescents: Current concepts and future directions. Clin. Med. Insights. Circ. Respir. Pulm. Med. 2015, 9, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Petrov, P.; Kurdova, R. Pneumocystosis. In Clinical parasitology and tropical medicine, 1st ed.; Petrov, P., Kurdova, R., Eds.; Publisher: East-West, Sofia, Bulgaria, 2016; pp. 198–205. (in Bulgarian) [Google Scholar]
- Morris, A.; Wei, K.; Afshar, K.; Huang, L. Epidemiology and clinical significance of Pneumocystis colonization. J. Infect. Dis. 2008, 197, 10–17. [Google Scholar] [CrossRef]
- Nevez, G.; Raccurt, C.; Vincent, P.; Jounieaux, V.; Dei-Cas, E. Pulmonary colonization with Pneumocystis carinii in human immunodeficiency virus-negative patients: assessing risk with blood CD4+ T cell counts. Clin. Infect. Dis. 1999, 29, 1331–1332. [Google Scholar] [CrossRef]
- Armbruster, C.; Pokieser, L.; Hassl, A. Diagnosis of Pneumocystis carinii pneumonia by bronchoalveolar lavage in AIDS patients. Acta Cytol. 1995, 39, 1089–1093. [Google Scholar]
- Sing, A.; Roggenkamp, A.; Autenrieth, I.B.; Heesemann, J. Pneumocystis carinii carriage in immunocompetent patients with primary pulmonary disorders as detected by single or nested PCR. J. Clin. Microbiol. 1999, 37, 3409–3410. [Google Scholar] [CrossRef]
- Koeva-Slavova, N.V. Peculiarities in the epidemiology and clinic of Pneumocystis pneumonia at NIIP in 1957-1960. Program and Abstracts of the National Paediatric Conference, Sofia, Bulgaria, 1960, Abstract pр.17-19. (in Bulgarian).
- Gamcheva, C.S. Study on pneumocystosis in infancy. PhD Thesis, National Center of Infectious and Parasitic Diseases, Sofia, Bulgaria, 1980. (in Bulgarian). [Google Scholar]
- Kurdova, R. Contemporary problems of opportunistic parasitoses and their diagnosis, In Proceedings of the IV national seminar on the topic: Modern methods for immunodiagnostics in the field of infectology, Sofia, Bulgaria,1999; Abstract, pр. 4-5. (in Bulgarian). (in Bulgarian).
- Dikov, I.; Plochev, K.; Topov, J.; et al. First case of AIDS in Bulgaria in a Bulgarian citizen. Epidemic Microbiol. Infect. Dis. 1999, 1, 35–38 (in Bulgarian). (in Bulgarian). [Google Scholar]
- Dikov, I.; Plochev, K.; Duhovnikova, T.; et al. Clinical and laboratory studies on the HIV-infectious process in Bulgaria. Modern Medicine 1989, 10, 15–18 (in Bulgarian). (in Bulgarian). [Google Scholar]
- Kurdova-Mincheva, R.; Tsvetanov, J.; Dikov, I. Pneumocystosis in a patient who died of AIDS - electron microscopy. Epidemic Microbiol. Inf. Dis. 1990, 27, 31–38 (in Bulgarian). (in Bulgarian). [Google Scholar]
- Kurdova, R.; Jordanova, D. Opportunistic parasitoses and HIV infection in Bulgaria. Infectology 2000, 37, 16–19 (in Bulgarian). (in Bulgarian). [Google Scholar]
- Kurdova, R.; Marinova, T.; Jordanova, D.; Ivanova, M.; Tzvetkova, N.; Rainova, I. Opportunistic parasitic diseases associated with HIV infection in Bulgaria. In Proceedings of the IX European Multicolloquium of Parasitology, Valencia, Spain, 2004; 1009(P); pp. 435–440. [Google Scholar]
- Tsvetkova, N.D.; Harizanov, R.N.; Ivanova, A.I.; Strashimirov, D.T.; Grozdeva, R.S.; Yancheva-Petrova, N.S. Recurrent Pneumocystis jirovecii pneumonia in an HIV-infected patient: A case report. GSC Advanced Research and Reviews 2021, 7, 083–086. [Google Scholar] [CrossRef]
- Sokulska, M.; Kicia, M.; Wesołowska, M.; Hendrich, A.B. Pneumocystis jirovecii - from a commensal to pathogen: clinical and diagnostic review. Parasitol. Res. 2015, 114, 3577–3585. [Google Scholar] [CrossRef] [PubMed]
- Fauchier, T.; Hasseine, L.; Gari-Toussaint, M.; Casanova, V.; Marty, P. M.; Pomares, C. Detection of Pneumocystis jirovecii by Quantitative PCR To Differentiate Colonization and Pneumonia in Immunocompromised HIV-Positive and HIV-Negative Patients. J. Clin. Microbiol. 2016, 54, 1487–1495. [Google Scholar] [CrossRef]
- Gal, S. Le.; Pougnet, L.; Damiani, C.; Fréalle, E.; Guéguen, P.; Virmaux, M.; Ansart, S.; Jaffuel, S.; Couturaud, F.; Delluc, A.; Tonnelier, J.-M.; Castellant, P.; Le Meur, Y.; Le Floch, G.; Totet, A.; Menotti, J.; Nevez, G. Pneumocystis jirovecii in the air surrounding patients with Pneumocystis pulmonary colonization. Diagn. Microbiol. Infect. Dis. 2015, 82, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Mühlethaler, K.; Bögli-Stuber, K.; Wasmer, S.; von Garnier, C. , Dumont, P.; Rauch, A.; Mühlemann, K.; Garzoni, C. Quantitative PCR to diagnose Pneumocystis pneumonia in immunocompromised non-HIV patients. Eur. Respir. J. 2012, 39, 971–978. [Google Scholar] [CrossRef]
- Chabé, M.; Dei-Cas, E.; Creusy, C.; Fleurisse, L; Respaldiza, N.; Camus, D.; Durand-Joly, I. Immunocompetent hosts as a reservoir of Pneumocystis organisms: Histological and RT-PCR data demonstrate active replication. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 89–97. [CrossRef]
- Cano, S.; Capote, F.; Pereira, A.; Calderon, E.; Castillo, J. Pneumocystis carinii pneumonia in patients without predisposing illnesses: acute episode and follow-up of five cases. CHEST 1993, 104, 376–381. [Google Scholar] [CrossRef]
- Ide, H.; Yamaji, Y.; Tobino, K.; Okahisa, M.; Murakami, K.; Goto, Y.; Sueyasu, T.; Nishizawa, S.; Yoshimine, K.; Munechika, M.; Oya, M.; Hiraki, Y. Pneumocystis jirovecii Pneumonia in an Immunocompetent Japanese Man: A Case Report and Literature Review. Case Rep. Pulmonol. 2019, 2019, 1–5. [Google Scholar] [CrossRef]
- Dunbar, A.; Schauwvlieghe, A.; Algoe, S.; van Hellemond, J. J.; Reynders, M.; Vandecasteele, S.; Boelens, J.; Depuydt, P.; Rijnders, B. Epidemiology of Pneumocystis jirovecii Pneumonia and (Non-)use of Prophylaxis. Front. Cell. Infect. Microbiol. 2020, 15, 10:224. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.J.; Lueck, C.; Ziesing, S.; Stoll, M.; Haller, H.; Gottlieb, J.; Eder, M.; Welte, T.; Hoeper, M.M.; Scherag, A.; David, S. Clinical course, treatment and outcome of Pneumocystis pneumonia in immunocompromised adults: a retrospective analysis over 17 years. Crit. Care 2018, 22, 307. [Google Scholar] [CrossRef]
- Shoji, K.; Michihata, N.; Miyairi, I.; Matsui, H.; Fushimi, K.; Yasunaga, H. Recent epidemiology of Pneumocystis pneumonia in Japan. J. Infect. Chemother. 2020, 26, 1260–1264. [Google Scholar] [CrossRef]
Figure 1.
Sputum smear of HIV+ patient, stained with methenamine-silver nitrate (according to Gomori). A cluster of black-stained oval and rounded cysts of P. jirovecii (arrow). Light microscopy, magnification 1000x.
Figure 1.
Sputum smear of HIV+ patient, stained with methenamine-silver nitrate (according to Gomori). A cluster of black-stained oval and rounded cysts of P. jirovecii (arrow). Light microscopy, magnification 1000x.
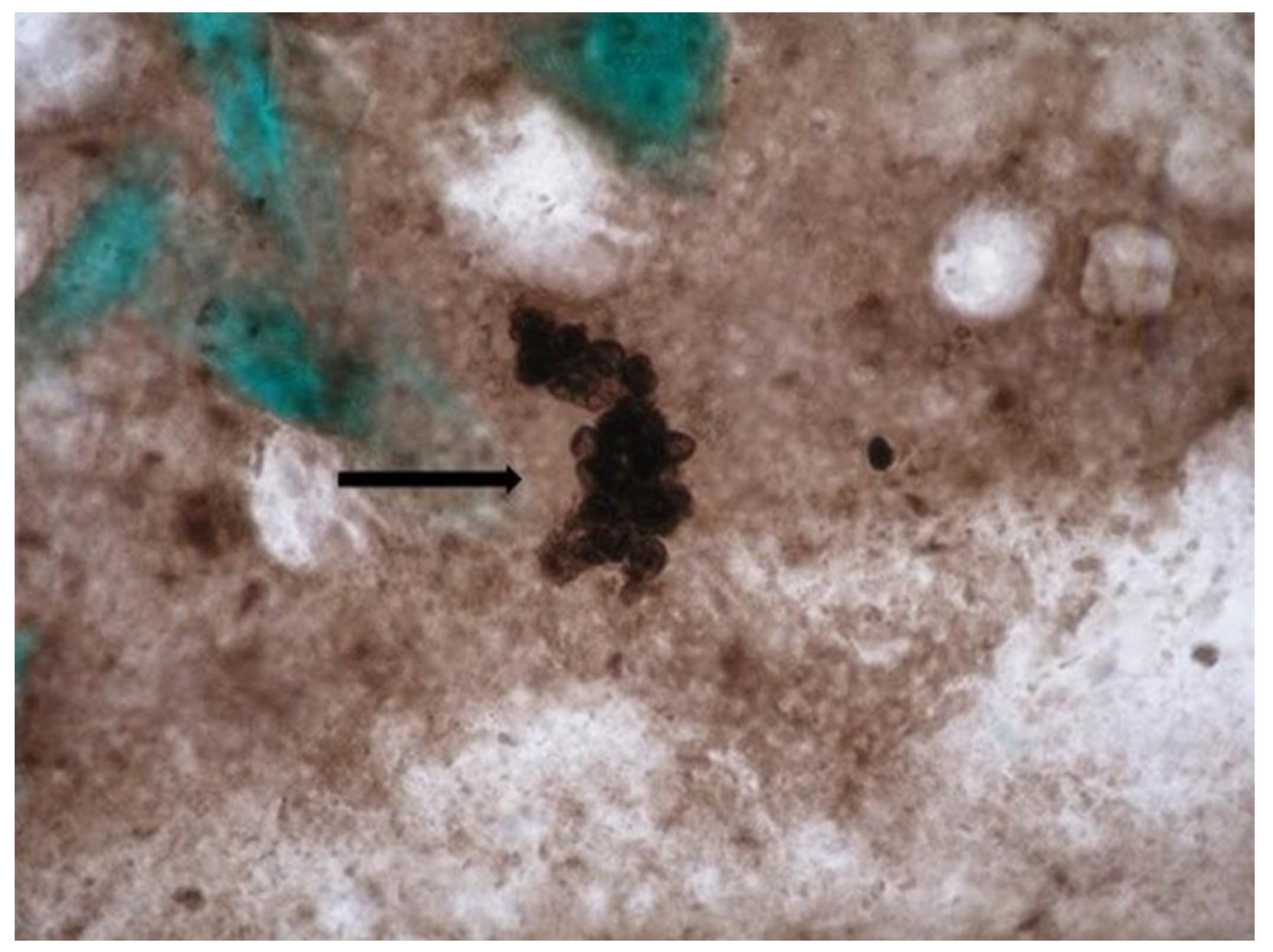

Table 1.
Demographic, immunological and clinical data for study participants.
| Demographic data | Age groups (range) | Gender | Total N (%) |
||||
|---|---|---|---|---|---|---|---|
| 0-12 months |
1-9 years |
10-18 years |
> 18 years | Male sex | Female sex | ||
| No of cases | 25 | 36 | 31 | 128 | 137 | 83 | 220 |
|
Real-time PCR positive |
3 | 2 | 2 | 31 | 32 | 6 | 38 (17.3%) |
|
Real-time PCR negative |
22 | 34 | 29 | 97 | 105 | 77 | 182 (82.7%) |
|
Light microscopy(RG1/ TB2/ GMS3), positive |
0 | 0 | 0 | 5 | 5 | 0 | 5 (2.3%) |
|
Light microscopy, negative |
25 | 36 | 31 | 123 | 132 | 83 | 215 (97.7%) |
| Groups distributed by immunological status and clinical presentation (primary diagnosis) | |||||||
| Group 1 - patients without data of immunosuppression | 23 | 34 | 26 | 70 | 86 | 67 | 153 |
| pneumonia | 7 | 1 | 1 | 14 | 16 | 7 | 23 (15%) |
| respiratory distress syndrome | 0 | 0 | 1 | 0 | 1 | 0 | 1 (0.7%) |
| pharyngitis | 0 | 0 | 0 | 1 | 1 | 0 | 1 (0.7%) |
| respiratory failure | 1 | 0 | 0 | 2 | 1 | 2 | 3 (1.9%) |
| dyspnea | 0 | 0 | 1 | 3 | 1 | 3 | 4 (2.6%) |
| pulmonary abscess | 0 | 0 | 0 | 1 | 1 | 0 | 1 (0.7%) |
| bronchitis | 0 | 1 | 0 | 1 | 0 | 0 | 2 (1.3%) |
| fatigue | 0 | 0 | 0 | 2 | 2 | 0 | 2 (1.3%) |
| hemoptysis | 0 | 0 | 0 | 3 | 1 | 2 | 3 (1.9%) |
| cough | 15 | 32 | 23 | 36 | 56 | 50 | 106 (69.3%) |
| COVID-19 | 0 | 0 | 0 | 7 | 4 | 3 | 7 (4.6%) |
|
Real-time PCR positive |
3 | 0 | 1 | 2 | 6 | 0 | 6 (3.9%) |
|
Real-time PCR negative |
20 | 34 | 25 | 68 | 80 | 67 | 147 (96.1%) |
|
Light microscopy, positive |
0 | 0 | 0 | 0 | 0 | 0 | 0 |
|
Group 2 - patients with compromised immune system |
2 | 2 | 5 | 58 | 51 | 16 | 67 |
| HIV infection | 0 | 1 | 0 | 46 | 42 | 5 | 47 (70%) |
| hematological malignancy | 1 | 0 | 1 | 5 | 4 | 3 | 7 (10.5%) |
| interstitial pulmonary fibrosis | 0 | 0 | 0 | 3 | 2 | 1 | 3 (4.5%) |
| nephrotic syndrome | 0 | 1 | 2 | 0 | 1 | 2 | 3 (4.5%) |
| solid organ transplantation | 1 | 0 | 1 | 0 | 2 | 0 | 2 (3%) |
| long-term use of inhaled corticosteroids due to bronchiectasis and asthma | 0 | 0 | 0 | 4 | 0 | 4 | 4 (6%) |
| disseminated lupus | 0 | 0 | 1 | 0 | 0 | 1 | 1 (1.5%) |
|
Real-time PCR positive |
0 | 2 | 1 | 29 | 26 | 6 | 32 (47.8%) |
|
Real-time PCR negative |
2 | 0 | 4 | 29 | 25 | 10 | 35 (52.2%) |
|
Light microscopy, positive |
0 | 0 | 0 | 5 (GMS3) | 5 | 0 | 5 (7.5%) |
|
Light microscopy, negative |
2 | 2 | 5 | 53 | 46 | 16 | 62 (92.5%) |
¹RG - Romanowski-Gimza staining; ²TC- toluidine blue staining; ³GMS - Gomori's methenamine silver stain.
Table 2.
Comparison of data from studies with the Gomori's methenamine silver stain and the real-time PCR (the specific target gene of Pneumocystis jirovecii is mtL SU rRNA) of 5 patients with positive results by both techniques.
Table 2.
Comparison of data from studies with the Gomori's methenamine silver stain and the real-time PCR (the specific target gene of Pneumocystis jirovecii is mtL SU rRNA) of 5 patients with positive results by both techniques.
| Patients | Staining method Specimen type - induced sputum |
Real-time quantitative PCR | Ct | |
|---|---|---|---|---|
| GMS |
P. jirovecii DNA concentration (copies/µӏ) |
|||
| In 1µl of the reaction solution | In 200 µӏ of the initial sample | |||
| P1 HIV+ | Clusters of cysts | 5,035 х 105 | 1,007 х 108 | 18.074 |
| P2 HIV+ | Clusters of cysts | 4,669 x 105 | 9,338 x 107 | 18.176 |
| P3 HIV+ | Single cysts | 2,179 х 101 | 4,358 х 103 | 31.566 |
| P4 HIV+ | Single cysts | 5,790 х 101 | 1,158 х 104 | 30.254 |
| P5 HIV+ | Single cysts | 4,703 х 102 | 9,406 х 104 | 27.441 |
Table 3.
Concentration of P. jirovecii DNA depends on the type of clinical specimen.
| Type of clinical specimen | Patients/age group | Real-time quantitative PCR |
Ct |
|
|---|---|---|---|---|
| Concentration of P. jirovecii DNA (copies/µl) | ||||
| In 1µl of the reaction solution | In 200 µӏ of the initial sample | |||
| Tracheal aspirate | A 4-month-old baby with pneumonia | 0,8123 х 103 | 0,162480 х 106 | 35.37 |
| A 6-month-old baby with severe interstitial pneumonia | 359,6 х 103 | 71,92 х 106 | 26.67 | |
| Bronchoalveolar lavage | A 60-year-old man with interstitial pulmonary fibrosis | 1,265 х 103 | 253 х 106 | 24.87 |
| A 45-year-old man with bilateral interstitial pneumonia | 87,52 х 103 | 17,504 х 106 | 29.69 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



