
Submitted:
05 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
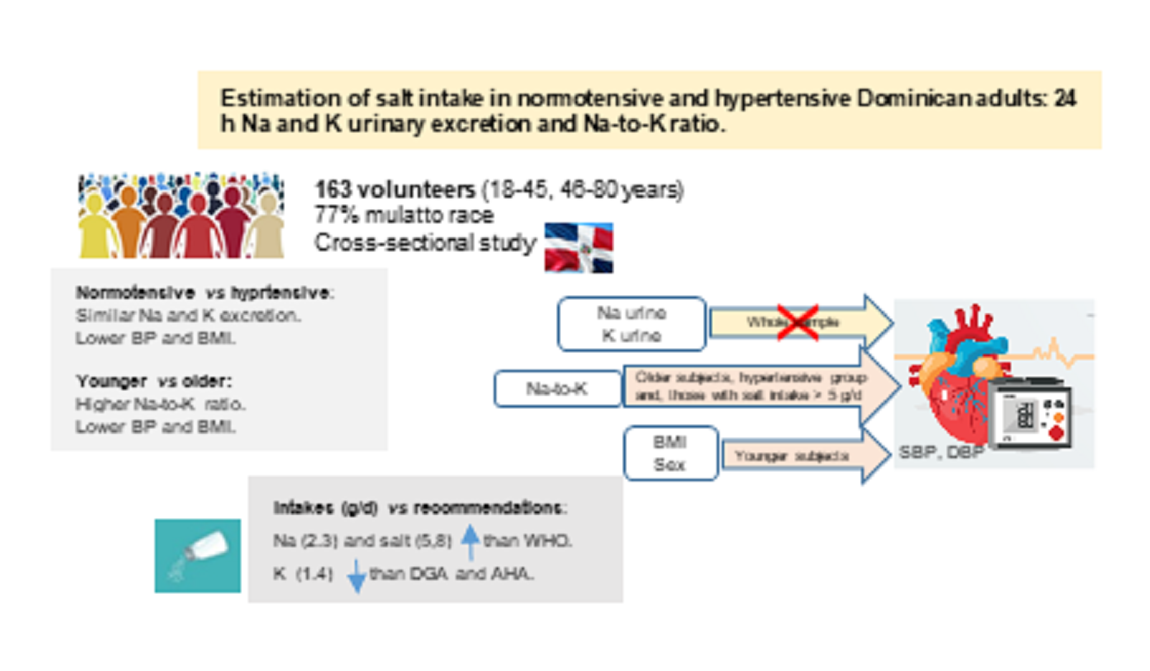
Higher salt (sodium) intake has been associated with a higher blood pressure (BP). The association degree may be influenced by factors such as age, origin and dietary components. This study aimed to evaluate the 24-hours urinary sodium (Na) and potassium (K) excretion in normotensive and hypertensive Dominicans adults and estimate their salt intake. 163 volunteers (18-45, 46-80 years) participated in a cross-sectional study. 24-hours Na and K urinary excretion were measured using an ion selective electrode technique. Na and K urinary excretion (99.4±46.5 and 35.0±17.5 mmol/24h) did not correlated with BP, except in the normotensive group in which K correlated with SBP (0.249, p=0.019). Na and K excretion were similar for normo- and hypertensive subjects. Na-to-K molar ratio (3.1±1.3) was higher in younger subjects (p=0.040). Na-to-K ratio was associated with DBP in the total group (r=0.153, p=0.052), in the hypertensive group (r=0.395, p<0.001) and in the older group with SBP (0.350, p=0.002) and DBP (0.373, p<0.001). In the older group, Na-to-K ratio and DBP correlated after controlling for subjects with hypertension controlled by treatment (r=0.236, p=0.041). The Na-to-K ratio correlated, when salt intake was over 5g/d (52.2%), with SBP (rho=0.219, p=0.044) and DBP (rho=0.259, p=0.017). Determinants of BP were age-dependent and in younger subjects were: sex (SBP, beta: 14.02±2.87, p<0.001) and body mass index (BMI) (beta:-12.07±3.72, p=0.001, beta:9.44±2.87, p=0.001, for SBP and DBP, respectively) and, in the olders, the Na-to-K ratio, for SBP (beta:6.7±2.4, p=0.005) and DBP (beta:3.8±1.1, p<0.001). The mean Na and salt intakes (2.3 and 5.8 g/d) were slightly higher and K intake lower (1.4 g/d) than WHO recommendations.
Keywords:
Dominicans
; Hypertensive
; Salt intake
; Sodium and potassium excretion
; Sodium-to-potassium ratio
Introduction
A large number of studies have been conducted on the association between sodium intake and cardiovascular morbidity-mortality [1,2,3], and, among other factors, a higher blood pressure (BP) has been associated with higher salt (sodium) intake [4,5] and ultimately with an increase in cardiovascular disease (CVD). However, although salt (sodium) intake is a determinant and modifiable factor of hypertension, the degree of correlation observed between the studies is inconsistent [1,3]. This could be due to the influence of other factors such as age, origin and other dietary components [6]. Some dietary components such as potassium can modify the effects of sodium intake as shown in the Dietary Approach to Stop Hypertension (DASH) study in the USA. That study demonstrated how a diet rich in potassium and calcium, together with different degrees of sodium intake (low, medium, high), correlated positively with lower BP [7]. Studies in recent years have focused on the excretion of potassium and sodium in urine after 24-h given that the sodium-potassium correlation in the diet would appear to be more important than strictly looking at the intake of sodium in terms of its effect on BP and resulting morbidity-mortality and on CVD [6,8,9,10,11,12,13,14], proposing urinary sodium and potassium excretion as surrogate measurements of their dietary intakes as an independent predictor of stroke [15,16].
The World Health Organization (WHO) recommends reducing sodium intake to less than 2 g/day (equivalent to 5 g salt) and increasing potassium intake (at least 3.5 g/day) to reduce BP and the risk of CVD, heart attack and coronary heart disease among adults, with or without hypertension [17]. While these recommendations do not stipulate the optimum sodium-to-potassium (Na-to-K) ratio, individual recommendations for these two elements lead to a ratio bellow 1. Although the scientific community generally recommends reducing salt /sodium intake for all populations, there are discrepancies in terms of the recommended amount [18,19,20,21,22,23]. The Dietary Guidelines for Americans (DGA) recommend no more than 2.3 g of sodium/day (5.75 g salt/d) while the American Heart Association (AHA) advocates a limit of less than 1.5 g of sodium/day (3.75 g salt/d), especially for those with high BP [24]. There is also disagreement regarding the impact of sodium on CVD as emerging evidence has shown that low sodium intake poses a greater risk for certain subgroups such as those with type 2 diabetes [25]. There are also differences in the degree of correlation between sodium and potassium intake and BP, the latter being higher in the case of hypertensive individuals with high salt intake and older adults [8].
It is estimated that the vast majority of the population consumes between 9 and 12 g of salt/day, i.e. approximately double the maximum recommended intake [21]. However, real intake could be even higher as many data have been obtained through dietary surveys which, due to their degree of variability, tend to underestimate true intake [25,26]. This variability is as much due to the dietary survey methodology employed (e.g. dietary note-taking, 24-h recall, food frequency questionnaire) as to the food composition tables/databases used. Hence, whenever possible, it is more reliable to base assessments on sodium excreted in urine after 24-h, the method currently considered the “gold standard” [3,23,27,28].
Salt intake in the region included within the Pan American Health Organization (PAHO) is estimated to be above 5 grams (2 g sodium) per day, varying between 8.5 and 15 g salt/person/day [29]. The PAHO therefore recommends reducing said consumption by 30% by 2025 in an attempt to prevent hypertension and CVD, the main causes of death in the region [29]. There is currently no data on salt intake in the Dominican Republic where recent studies have revealed a prevalence of hypertension of 32.3% [30]. To define factors impacting non-transmissible disease among adults, the PAHO/WHO, planned to conduct surveys in several countries, including the Dominican Republic by 2019 [31]. However, to the best of our knowledge, there are still no data on the salt intake among Dominicans. Our aims are to estimate the salt intake by means of the 24-h urinary sodium excretion in a group of normotensive and hypertensive Dominican adults and, to examine the association of urinary sodium and potassium excretion and sodium-to-potassium ratio with BP.
Materials and Methods
Subjects and Study Design
165 participants (18 - 80 years) were selected among patients who were contacted through the cardiology and internal medicine outpatient services of two hospitals in Santo Domingo (Dominican Republic), the Centro de Diagnóstico, Medicina Avanzada y Telemedicina (CEDIMAT) and the Centro Cardio-Neuro-Oftalmológico y Transplante (CECANOT), health care personnel and administrative staff and their relatives and acquaintances who expressed interest in participating in this study. Inclusion criteria were: age > 18 years and BP: normo and hypertension. Volunteers were asked to report information on the following exclusion criteria: diabetes or nephropathy with complications (e.g. renal, ocular), chronic diseases, pregnancy and consumption of restricted diets or avoidance of any food group. Two participants were excluded, one because of a very high triglyceride and microalbuminuria concentrations and, the other due to a lack of analytical blood and urine data. Thus, 163 participants (78 men, 85 women) took part in a cross-sectional study (October -November 2021): 88 normotensive and 75 hypertensive subjects. Classification as normo or hypertensive was done using systolic blood pressure (SBP) ≤ 140 mm Hg and / or diastolic blood pressure (DBP) ≤ 90 mm Hg as the cut-off point [32,33,34], in line with the criteria established by the European Society of Cardiology (ESC) and European Society of Hypertension (ESH) in their clinical practice guidelines [34].
The volunteers included in the study underwent fasted blood and 24-h urine sampling and blood pressure and anthropometric measurements. Three-day 24 hour dietary recalls were used for dietary assessment and will be published elsewhere along with two questionnaires, a general one about global health and dietary habits designed based on everyday food consumption in Dominican homes (the family food basket and a PAHO survey on knowledge, attitude and use of salt in food) [35].
The study was conducted in accordance with the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Consejo Nacional de Bioética en Salud (CONABIOS) (registry nº 022-2020, dated 9 December 2020). In the Dominican Republic, participant identity was preserved during the handling of samples and data in accordance with Law No. 172-13, G.O. and No. 10737 of 15 December 2013. Written informed consent was obtained from all subjects.
Anthropometric and Blood Pressure Measurements
Anthropometrical measurements included height, weight, waist and hip circumferences and bioimpedance analysis (Omrom HBF-514C-LA). Body weight (kg) was measured without shoes and with light clothing. Height was recorded to the nearest cm. using a scale (8023 Jiangsu Medical SH, Jiangsu Scale). Body mass index (BMI) was calculated as weight (kg) /height (m2).
BP (mm Hg) was taken using an automatic BP monitor (Omrom Hem-7320-LA) in quiet and temperature-controlled conditions. The cuff was placed on the right upper arm. BP was measured three times with at least five minutes between measurements.
Urine and Blood Samples
24-h urine samples were stored in two-liter plastic containers, with 10 g boric acid as preservative before transfer to the laboratory. Sodium, potassium, creatinine, microalbumin and endogenous creatinine clearance (ECC) were analysed and ECC was corrected by body surface area (ECC-c). 24-h sodium and potassium urinary excretion was analyzed using indirect potentiometry with the membrane ion-selective electrode technique using the AU5811 Beckman Coulter analyzer (Inc. Brea, CA, USA).
A fasted blood sample was obtained to analyze lipid profile (cholesterol, HDL- and LDL- cholesterol, VLDL, triglycerides), creatinine and glycaemia. Cholesterol was analyzed based on cholesterol dehydrogenase, HDL-cholesterol using direct polymer-polyanion measurement, triglyceride using an enzymatic method and the microalbumin with an immunoturbidimetric test. Creatinine was analyzed using the kinetic alkaline picrate method (modification of the Jaffe procedure kinetic method) and glucose by the hexokinase method. Endogenous creatinine clearance (ECC) and ECC-corrected by surface area (ECC-c) were calculated using the following formulas:
ECC = Creatinine in urine (mg/dL) x diuresis (mL urine 24-h) / creatinine in serum (mg/dL) x 1440
ECC-c = Creatinine in urine (mg/dL) x diuresis (mL urine 24-h) x 1.73 / creatinine in serum (mg/dL) x 1440 x body surface area
Body surface area = √ (weight (kg) x height (cm)) / 3600
To validate 24-h urine collection, a correlation between fat-free mass calculated from data obtained by electrical bioimpedance and that determined via urinary creatinine excretion was calculated. The fat-free mass was calculated using the formula [cited in 37]:
Fat-free mass (kg) = 7.38 + 0.02908 × urinary creatinine (mg/day)
All the analytical determinations in urine and blood were performed using an AU5821 Beckman Coulter analyzer (Inc. Brea, C.A., U.S.A.) in the Amadita P. de González S.A.S. Clinical Laboratory, which implemented and maintained a Quality Management System (ISO 9001:2015).
Statistical Analysis
To assess differences between normo and hypertensive subjects, the sample size was calculated on the basis of the urine sodium excretion data (140.5 ± 34.6 y 150.4 ± 38.8 mEq/d, respectively) using the G*Power Programme (Universität Düsseldorf, www.gpower.hhu.de/). A sample size of 77 subjects per group was necessary to obtain a difference in the urine sodium excretion (10 mEq/d) with 80 % power and an alpha error of 0.05.
Data are expressed as the mean and standard deviation and median. Normal data distribution of the data was assessed (Kolmogorov-Smirnov test). Correlations among urine and serum variables were established using Spearman’s rho correlation coefficient. All reported P-values are based on a two-sided test and a p value <0.05 was considered to indicate statistical significance. IBM® SPSS® Statistics for Windows, version 27.0 was used for all statistical calculations.
Partial correlation matrices for each age group controlled by BMI (3 categories: normal weight (18.5 – 25 kg/m2), overweight (25.1 – 30 kg/m2), and obesity (≥ 30.1 kg/m2), assessed the correlation between SBP and DBP with all other variables.
In each age group (18–45 and 46-80 years), the relationship between 24-h sodium and potassium excretion in urine and BP (SBP and DBP as dependent variables) was subjected to linear regression analysis considering sex, BMI (normal weight, overweight and obesity), urinary sodium, potassium, Na-to-K ratio, sodium-to-creatinine ratio and potassium-to-creatinine ratio as covariates.
A linear model was used to assess DBP and SBP -correlations, considering sex and BMI as fix factors and as covariate (in urine) Na-to-K ratio. The correlation matrix to assess the R value in the model was calculated by the correlation matrices of the original values of the variables and the values predetermined by the model.
Results
Participant characteristics are shown in Table 1 and a flow diagram for study participants in Figure 1. They were recruited at the hospitals CEDIMAT (n=85, 52.1%) and CECANOT (n=78, 47.9%), 78 men (47.9%) and 85 women (52.1%). The average age was 44.5 ± 14.6 y (age range: 18 – 80 y). By racial phenotypic the group was 76.7 % mix race (mulatto), 12.9% black, 9.2% white and 1.2% Asian. A similar number of hypertensive (46%) and normotensive (54%) subjects were included in the study. Most (82.7%) from the hypertensive group (n=75) were aware of their condition, being 62 of them being treated for hypertension (most frequently used: Amlodipino (19), Losartan (16), Candesartan (13), Valsartan (8), Bisoprolol (7), Enalapril (5)). From these participants treated with antihypertensives only 34 had their hypertension controlled. Only 12% of the participants were diabetics with no complications.
Table 2 shows data of BP, anthropometric measurements, biochemical data in 24-h urine (sodium, potassium, creatinine and ratios) and blood (lipid profile, creatinine and glycaemia) in the total sample as a whole and grouped by BP (normotensive and hypertensive). The urine sample was appropriate according validation by means of the correlation between muscle mass and urinary creatinine (r= 0.717).
P value between normo and hypertensive (Mann Whitney, Wilcoxon). bpm: beats per minute. 1 The sodium and potassium values used in this ratio were measured in millimoles.
SBP and DBP were higher in hypertensive than in normotensive subjects, as was the BMI (p<0.001), the waist-to-hip ratio, body fat and visceral fat (p<0.001). Muscle mass was lower than in the normotensive group (p=0.038). The 24-h urine sample showed no difference for the sodium or creatinine but significant differences were found for ECC-c, higher in normotensive (p=0.041) and microalbumin (higher in hypertensive, p=0.005). Blood test showed similar total cholesterol for both groups, but HDL-cholesterol was higher in the normotensive (p=0.002) and VLDL-cholesterol and triglycerides were higher in the hypertensive group (p=0.006 and p=0.004, respectively) as was the total cholesterol/HDL-cholesterol ratio and the glycaemia (p= 0.032 and p=0.01, respectively).
Urinary excretion of sodium, potassium and creatinine were similar between normo and hypertensive subjects. To validate 24-h urine collection, a correlation was drawn between fat-free mass calculated from data obtained by electrical bioimpedance (51.2 ± 12.5 kg) and that determined via urinary creatinine excretion (48.7 ± 16.6 kg) was calculated and a positive significant correlation was found (rho=0.717, p<0.001).
The age of participants ranged from 18 to 80 years and two age groups [18–45 y (51.5%) and 46-80 years (48.5%)] were established given that age was a confounding factor. The cut-off point for the age was set at 45 years based on other studies of representative populations and because 44% of Dominican adults in the age range 40 - 49 years have been described as hypertensive [39]. BP data, anthropometric measurements and biochemical data in 24-h urine and in blood samples of participants grouped by age are shown in table 2. Significant differences were found in BP and anthropometric and blood data between young and older subjects, similar to those obtained from the comparison between normo- and hypertensive subjects. However, comparisons between the two age groups showed more statistical differences in 24-h urine and creatinine excretion (higher in the younger group, p <0.001), ECC and ECC-c (higher in younger subjects, p<0.001), Na-to-K ratio (higher in younger subjects, p=0.04) and the K-to-creatinine ratio (higher in older subjects, p=0.013). However, there was no difference in the excretion of sodium or potassium or in the sodium-to-creatinine ratio.
Table 3 shows correlations between BP and variables in urine, blood and anthropometric measurements in the sample as a whole, and between the two age groups and between normotensive and hypertensive subjects. Sodium and potassium excretion did not show any correlation with BP except in normotensive subjects with the significant correlation between potassium and SBP. The Na-to-K ratio was found significanty correlated with DBP in the total group, in the older group with SBP and DBP and in the hypertensive subjects. In the older group the sodium-to-creatinine ratio was correlated with SBP. Anthropometric measurements, blood lipid profile and creatinine in serum and ECC-c showed several significant correlations in the group as a whole and in the age groups.
In a subgroup of participants with a salt intake higher than 5 g/day (n=85), the Na-to-K ratio showed a significative correlation with the SBP (rho=0.219, p=0.044) and DBP (rho=0.259, p=0.017).
In partial correlation matrix adjusted for blood pressure (normo and hypertensive groups), the correlation between Na-to-K ratio and DBP was significantly different (r=0.166, p=0.034).
The correlation between urinary excretion parameters and BP adjusted for controlled hypertension using antihypertensive treatment showed no significant differences in the total group and in the younger group. Instead, in the older group, there was a significant correlation between Na-to-K ratio and DBP (r=0.236, p=0.041).
In partial correlation matrices adjusted by BMI for each age group, the variable most closely correlating to BP (systolic and diastolic) was the Na-to-K ratio, especially in older group. In the same group, SBP also correlates significantly with the sodium-to-creatinine ratio, although this effect later disappears in the analysis using the general linear model for each age group.
BMI correlated with creatinine (rho=0.212, p=0.007) and ECC (rho=0.165, p=0.035) in urine. Assessment of these correlations by age group shows that in the younger group, BMI correlated with creatinine in urine (0.357, p <0.001) while in the older group, BMI correlated with ECC (0.260, p=0.021) and with sodium in urine (0.264, p=0.019). In the older group, sodium urinary excretion correlated with waist size (0.397, p<0.001), waist-hip size (0.379, p<0.001), visceral fat (0.374, p<0.001) and BMI (0.264, p=0.19)
A linear model was used for each age group to evaluate the predictive value of the BP variables analysed. The variables in the final model were sex, BMI and Na-to-K ratio (Table 4). Determinants of SBP and DBP were different for the two age groups. In the 18-45 group, sex and BMI showed significant effects on SBP and BMI impacted DBP. SBP was higher in men than in women (14 mmg Hg) and lower in normal weight (12.1 mm Hg) than in obese subjects, and lower in overweighted (10.7 mm Hg) than in obese subjects. DBP was lower in normal weight (9.4 mm Hg) than in obese subjects and lower in overweighted (5.1 mm Hg) than in obese subjects. In the 46-80 group, SBP and DBP were affected by the Na-to-K ratio and, for each unit increased, SBP increased by 6.7 mm Hg and DBP increased by 3.8 mm Hg.
The R coefficients for SBP were R= 0.575 (p=0.000) and R= 0.352 (p=0.001) for the younger and older groups, respectively. The R coefficients for the DBP were 0.377 (p=0.000) and R=0.392 (p=0.000) for the younger and older groups, respectively.
Table 5 shows the salt, sodium and potassium intakes estimated from the 24-h sodium and potassium urinary excretion for the entire sample and age and BP groupings. There was no significant difference between normo- and hypertensive subjects in terms of sodium intake but there was in terms of potassium intake in the group as a whole and in the older sub-group, potassium intake being higher in the normotensive subjects. In the older group, normotensive subjects exhibited lower sodium and higher potassium intake, leading to a lower Na-to-K ratio (p=0.011) than in their hypertensive counterparts.
Assuming that all of the sodium eliminated in urine (89 mmol/24h, median value for the entire sample) (Table 2) comes from dietary intake, this excretion indicates dietary salt intake of 5.8 ± 2.7 g (median: 5.2 g/d). Salt intake does not significantly correlated with BP but does correlated with the amount of sodium excreted in urine (rho= 1), potassium (rho= 0.652 p<0.001) and with the Na-to-K ratio (rho= 0.412, p<0.001).
In subjects whose dietary salt intake was over the 5 g/d recommended by the WHO (n=85, 52.2%), but not in those consuming less, the Na-to-K ratio correlated significantly with SBP (rho=0.219, p=0.044) and DBP (rho=0.259, p=0.017).
Discussion
To the best of our knowledge, there is no data on salt intake of Dominicans, a population with a prevalence of hypertension of 32.3% and obesity of 33.6 % and, this is the first study on salt intake in a group of Dominican adults, assessed by means of the “gold standard” method, the 24-h sodium excretion in urine [3,27,28]. A similar number of adults women and men participated (52 vs. 48% respectively), with a mean age of 44.5 (± 14.6) y. Most participants were mulatto (77%) and in a smaller proportion were black or white (13% and 9 %, respectively), representative of the Dominican population [40]. Most of the participants were non-diabetics (88 %), a percentage in line with diabetes data in Dominicans [30,41]. Only 17% of the participants were unaware that they had high BP, a small percentage compared with the 40.6% who did not know about their high BP according to a recent survey from the Dominican Government [30].
Urinary Sodium and Potassium Excretion
The median 24-h urinary sodium excretion in the total sample of 2046 mg/d (mean 2286 mg/d) was in the lower range of the 24-h sodium excretion reported in a systematic review that included more than 10.000 adults from the US and Europe (median: 3270 mg/24h, 10th to 90th percentile, 2099 to 4899) [3]. Urinary sodium excretion in our study was also bellow the lower interquartile reported for a representative sample of non-hypertensive Spanish adults (median: 2613, interquartile: 2480 – 4942 mg/d; mean 3062 mg/d) [26]. This sodium excretion was just half of the sodium excreted in a representative sample of the adult Irish population (4078 mg/d) and in a healthy adults sample in northern Greece (4220 mg/d) and was lower than the mean reported for men and women in Norway ( 3535 mg/d) [43], in the US (3291 mg/d by 24-h dietary recall and mean: 3608 mg/d, median: 3320 mg/d, by 24-h urinary sodium excretion) [14,44], in Greece university students (2803 mg/d) [12]. Urinary sodium excretion in this study was much lower than in China (4300 mg/d and 4700 mg/d) [16,45] and worldwide (42% from China) 4930 mg/d and Kazakhstan (6782 mg/d) [46].
Surprisingly, the median 24-h potassium excretion of 1209 mg/d (mean: 1365 mg/d) in this study was substantially lower than the mean reported in the previously mentioned data from the US and Europe (2535 mg/d, median range: 2067 - 3610) and lower than the median reported for men and women in Spain (2613 mg/d) and in Ireland (3290 mg/d) [5], and lower than the mean reported in Norway (3420 mg/d [43], in the US (2542 mg/d by 24-h dietary recall and 2155 mg/d by 24-h urinary sodium excretion) [14,44], in Greece (2152 mg/d and 3303 mg/d) [12,42], in Kazakhstan (2271 mg/d) and worldwide (42% from China) 2120 mg/d [8]. Potassium excretion was similar to that in the lower range of the distribution in the Chinese population (mean: 1600 mg/d, range: 1160- 1880) and lower the hypertensive Chinese adults (n=189 male; 2100 mg/d) [16].
Low 24-h sodium and potassium urinary excretion was observed in the overall sample and no difference was found in terms of the age of the subjects, coinciding with findings from other studies [44], despite the fact that age could contribute to an increase in urinary sodium and potassium losses due to a decline in the glomerular filtration rate and an increased incidence of renal disease with advancing age. Lower potassium urinary concentration has been described in younger vs older subjects and higher sodium excretion in younger subjects and the opposite, higher sodium excretion in older subjects [48]. Race has been associated with potassium excretion and intake, both being lower in blacks than in whites [6]. Therefore, this variable may have been important in the results of this study considering the high percentage (77%) of mulatto subjects. Also, the very low K excretion could be related to lower consumption of potassium rich foods and, as reported in a group of Dominicans, the consumption of fruit and vegetables (major potassium food sources) was below the recommendations for Dominicans [49], Moreover, only a very limited variety of fruit and vegetables are most frequently consumed by Dominicans as can be deduced from a recent survey on the food intake in this country [50]. In addition, to dietary factors, sweat and faecal losses of these compounds should be taken into account for a more accurate estimate of their excretion. In sweat, the sodium losses has been estimated at approximately 10% under normal conditions and higher depending on the ambient temperature [53]. Instead, the potassium losses stays relatively constant, regardless of sweat rate and level of acclimatization [54]. Thus, this sodium loss could be greater in countries with a tropical climate such as the Dominican Republic (during the study the mean temperature was 32 ºC and the relative humidity was 86%) and could partially account for the lower sodium and potassium urinary excretion observed in this study compared to people from other countries.
The sodium excretion was similar in normotensive and hypertensive subjects, which contrast with the lower excretion in normotensive subjects described in others [38,48]. The potassium excretion was also similar in normotensive and hypertensive which does not coincide with the inverse association between the higher potassium intake (based on 24-h dietary recall) and BP at a higher threshold in the USA survey (NHANES 2018) [14]. As anticipated decades ago, potassium intake may be a major factor in the epidemiological differences of hypertension [6].
The Na-to-K ratio was approximately 3 and there was no difference in terms of BP levels but there was a difference according to age, the ratio being higher in the younger group as well as potassium-to-creatinine ratio, creatinine, ECC and ECC-c. This molar ratio is far from the recommended value of less than 1 (based on the sodium and potassium intake recommendations WHO [21], but is similar to the ratios described in individual cross-sectional studies of adults (from 2.2 to 3.8), with Na-to-K ratio greater than 2 [5.42,44] and lower than that found among in other populations such as in Kazakhstan (6.34) [46].
BP was higher in the older group as also has been described in other studies (i.e. [38]). Considering age and BP, the older normotensive subjects exhibited lower sodium intake and a higher potassium intake than in the older hypertensive group, which leads to a lower Na-to-K ratio intake (=1.22) than that in the other groups and closer to the target of 0.6 (based on Na and K intakes recommended by the WHO) [21]. According to a recent meta-analysis on cardiovascular risk in several prospective studies controlled for confounding factors, a higher sodium excretion, lower potassium excretion and higher Na-to-K ratio are associated with a higher cardiovascular risk [3]. Hence, the older normotensive subjects should have the lower cardiovascular risk compared with the older hypertensive group. While evidence on the effect that the Na-to-K ratio has on BP, highlights the benefits of reducing sodium and increasing potassium compared to sodium and potassium separately [11], in this study, the increase in K intake (which is extremely low) seems to be more necessary than a decrease in the Na intake. However, an increase in dietary potassium intake could not be advise for those with impaired kidney function who are in an advanced state of chronic kidney disease. Therefore, an education program to help lower the sodium-to-potassium ratio and individualized approaches to that end may help to minimize the gap between this ratio and the suggested levels [11].
The degree of correlation between the intake of sodium and potassium and BP is variable according to the literature but, in general, this correlation is higher in hypertensive people, in persons consuming high-sodium diets and in older persons [8,26], although no significative association has also been described [46]. In this study, BP did not correlate significantly with sodium and potassium excretion in the total sample, which coincide with the findings described in some studies [46,47], but stands in disagreement with the association between BP and sodium urinary excretion described in others [26,38]. Instead, the Na-to-K molar ratio correlated with SBP and DBP in the older group and with those with a high salt intake (> 5g/d). Similarly, that association has been shown in other studies [9,55].
Predictive BP variables were different depending on age group, sex and BMI for the younger group and, Na-to-K molar ratio for the older group. In the younger group, higher SBP was measured in men than in women, as also described recently in the Dominican Republic and other populations [26,43,48], and both SBP and DBP increased with body weight. This association between body weight and BP has been widely observed (i.e. [26]) and weight loss in overweight and obese individuals is one of the non-pharmacological interventions recommended for US adults with high BP [34].
In the older group, only the Na-to-K ratio was a determinant of SBP and DBP and for each unit increase in this ratio, there was an increase in 6.7 mm Hg in SBP and 3.8 mm Hg in DBP. Similar BP increments associated with the Na-to-K ratio have been reported in a study compiling data from eighteen countries (42% from China) [8]. Thus, the Na-to-K ratio seems to be a more important predictor of hypertension than either sodium or potassium intake alone, in agreement with other authors [3,5,9,11,14,16,44], in the older group.
Estimated Sodium, Salt and Potassium Intake: Comparison with Recommended Intake
The sodium 24-h urinary excretion (median in the entire sample: 89 mmol/24-h= 2046 mg/24-h) corresponded to a dietary salt intake of 5.8 g (median: 5.2 g, range: 1.34 to 14.2 g salt/day), which is quite a bit lower than the intake estimated from ten countries in the PAHO region (8.5 – 15 g/d, data from 2015) [29]. Our result is around half of the salt intake data obtained by 24-h sodium urinary excretion in Mesoamerica (3.5 and 3.8 g /day, equivalent to 8.9 - 9.8 g salt/day) [45,56]. This discrepancy between the estimated salt intake at a population level in the Region and our data in a group of Dominicans could be due to the origin / race of the population and their culinary habits, the salt intake assessment method and also the fact that a single 24-h urine collection may not reliably reflect an individual’s usual intake [23]. In Spain, a different geographical area and climate, in a representative sample or in northern Greece, 88.2 % and 94,4%, respectively had salt intakes above the recommended 5 g/d [26,42], a percentages considerably higher than the one found in the present study (52.2 %). In the Spanish population, sodium urinary excretion correlated with SBP and DBP, but in the present study, only the Na-to-K ratio is associated with BP in the older group.
The mean potassium intake in our study, 1.4 g/day (median 1.2 g/day), is far from the minimum of 3.5 g potassium/day (90 mmol/d) recommended by the WHO with the aim of reducing BP [21], and also by the EFSA for the adult population and the 4.7 g/d suggested by the DGA and by the AHA [22,24]. These sodium and potassium dietary intake recommendations (g) leads to a Na-to-K ratios of 0.32 [22], 0.5 and in the range 0.6 - 1 [21,23,57], which are approximately three times lower than the ones obtained in this study. Our data showed almost “normal” sodium but very low potassium urine excretions, thus a higher potassium consumption would lead to a better Na-to-K ratio and consequently to lower BP and to a lower risk of stroke associated to potassium intake below 3500 mg/d [53].
The median salt intake is higher, but closer to the maximum 5 g salt /d (under 2 g sodium/d) recommended by the WHO with the aim of reducing BP [58], and to the 5 g salt/day considered by the European Food Safety Authority as a safe and adequate intake for the general European adult population [23]. This is also higher than the 3.75 g salt/d (1.5 g sodium/day) estimated as adequate intake for the general population by the DGA but is lower than the 2.3 g sodium/day recommended by the AHA for the general population as part of a healthy diet [24].
Conclusions
Although neither sodium nor potassium urinary excretion were associated with BP, except the potassium in the normotensive group, the Na-to-K molar ratio (around 3) was associated with blood pressure in the older subjects (age 46 - 80), in hypertensive subjects and in subjects with a salt intake above 5 g/day. This Na-to-K ratio was lowest for the older normotensive group due to their relatively higher potassium intake.
There was no differences in the salt intake estimated in the normo and hypertensive Dominican subjects in this study, that, on average was slightly higher (5.8 g salt/d) than that recommended by WHO (5 g/d) [21,58]. Potassium intake was higher in normotensive subjects and was substantially lower than recommended (3.5 – 4.7 g/d, [21,59]).
BP determinants were age-dependent, i.e. sex and BMI in the younger group and the Na-to-K molar ratio in the older group. This study with the first data set on the salt intake in adult Dominicans may serve as the basis for a further study in a representative sample of the Dominican population and to define public health strategies based on age.
Funding
This study is funded by the Fondo Nacional de Innovación y Desarrollo Científico y Tecnológico (FONDOCyT), Ministerio de Educación Superior, Ciencia y Tecnología, Dominican Republic [grant. cod.: 2018-2019-2A2-233].
Acknowledgments
The authors wish to thank quality assistance of Dr Patricia González from the Amadita P. de González S.A.S. Clinical Laboratory in the blood and urine analysis, and Belkis Billini and Albania Arredondo for assisting with the samples collection. The authors thank Francisco Felipe, coordinator of medical department of CECANOT, for his support in the physicians training for volunteer recruitment and, CEDIMAT staff for their support in this study. The authors wish to thank Laura Barrios and Belén Garzón-García from the Secretaría General Adjunta de Informática of the CSIC for the statistical study assessment.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- McGuire: S. Institute of Medicine. 2013. Sodium intake in populations: Assessment of evidence. Adv Nutr 2014, 5, 19–20. [CrossRef]
- Kong, Y.W.; Baqar, S.; Jerums, F.; Ekinci, E.I. Sodium and its role in cardiovascular disease - the debate continues. Front Endocrinol 2016, 7, 164. [CrossRef]
- Ma, Y.; He, F.J.; Sun, Q.I.; Changzheng, Y.; Kieneker, L.M.; Curhan, G.C.; et al. Urinary sodium and potassium excretion and cardiovascular risk. N Engl J Med 2022, 386, 252–263. [CrossRef]
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. Brit Med J 2013; 3: 346, 1325. [CrossRef]
- Morrissey, E.; Giltinan, M.; Kehoe, L.; Nugent, A.P.; McNulty, B.A.; Flynn, A.; et al. Sodium and potassium intakes and their ratio in adults (18-90 y): Findings from the Irish National Adult Nutrition Survey. Nutrients 2020, 12, 938. [CrossRef]
- Langford, H.G. Dietary potassium and hypertension: epidemiologic data. Ann Intern Med 1983, 98, 770–772. [CrossRef]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium collaborative Research Group. N Engl J Med 2001, 34, 3–10. [CrossRef]
- Mente, A.; Martin, J.; O’Donnell, M.J.; Rangarajan, S.; McQueen, M.J.; Poirier, P.; et al. for the PURE investigators. Association of urinary sodium and potassium excretion with blood pressure. N Engl J Med 2014, 371, 601–611. [CrossRef]
- Perez, V.; Chang, E.T. Sodium-to-potassium ratio and blood pressure, hypertension, and related factors. Adv Nutr 2014, 5, 712–741. [CrossRef]
- Park, J.; Kwock, C.K.; Yan, Y.J. The effect of the sodium to potassium ratio on hypertension prevalence: A propensity score matching approach. Nutrients 2016, 8, 482. [CrossRef]
- Iwahori, T.; Miura, K.; Ueshima, H. Time to consider use of the sodium-to-potassium ratio for practical sodium reduction and potassium increase. Nutrients 2017, 8, 700. [CrossRef]
- Athanasatou, A.; Kandyliari, A.; Malisova, O.; Pepa, A.; Kapsokefalou, M. Sodium and Potassium Intake from Food Diaries and 24-h Urine Collections from 7 Days in a Sample of Healthy Greek Adults. Front Nutr 2018, 5, 13. [CrossRef]
- Nohara-Shitama, Y.; Adachi, H.; Enomoto, M.; Fukami, A.; Kumagai, E.; Nakamura, S.; et al. Twenty-four-hour urinary potassium excretion, but not sodium excretion, is associated with all-cause mortality in a general population. J Am Heart Assoc 2018, 7, e007369. [CrossRef]
- Bhagavathula, A.S.; Refaat, S.A.; Bentley, B.L.; Rahmani, J. Association between intake of sodium, potassium, sodium-to-potassium ratio, and blood pressure among US adults. Int J Vitam Nutr Res 2021, 1-9. [CrossRef]
- Willey, J.; Gardener, H.; Cespedes, S.; Cheung, Y.K.; Sacco, R.L.; Elkind, M.S.V. Dietary sodium to potassium ratio and risk of stroke in a multiethnic urban population. The Northern Manhattan Study. Stroke 2017, 48, 2979–2983. [CrossRef]
- Liu, W.; Huang, X.; Liu, X.; Wang, L.; Chen, Z.; Ortega, D.; et al. Urinary sodium and potassium excretion and cerebrovascular health: a multimodal imaging study. Eur J Nutr 2021, 60, 4555–4563. [CrossRef]
- WHO. World Health Organization. Hypertension. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 20 February 2023.
- American Diabetes Association, Bantle, J.P.; Wylic-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G.; Franz, M.J.; et al. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care 2008, 31, S61–S78. [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO). CKD Work Group, KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013, 3, 1–150.
- WHO. Sodium intake for adults and children. Geneve: WHO, 2012. Available online: https://apps.who.int/iris/bitstream/handle/10665/77985/9789241504836_eng.pdf (accessed on 20 February 2023).
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015 – 2020 Dietary Guidelines for Americans. 8th Edition. December 2015. Available online: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2015 (accessed on 20 February 2023).
- EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods and Food Allergens), Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, H.; Kearney, J.; Maciuk, A.; et al. Scientific Opinion on the dietary reference values for sodium. EFSA J 2019, 17, 5778.
- 24. AHA, American Heart Association. Available online: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/sodium/how-much-sodium-should-i-eat-per-day (accessed on 20 February 2023).
- Aparicio, A.; Rodríguez-Rodríguez, E.; Cuadrado-Soto, E.; Navia, B.; López-Sobaler, A.M.; Ortega, R.M. Estimation of salt intake assessed by urinary excretion of sodium over 24 h in Spanish subjects aged 7-11 years. Eur J Nutr 2017, 56, 171–178. [CrossRef]
- Ortega, R.M.; López-Sobaler, A.M.; Ballesteros, J.M.; Pérez-Farinós, N.; Rodríguez-Rodríguez, E.; Aparicio, A.; et al. Estimation of salt intake by 24 h urinary sodium excretion in a representative sample of Spanish adults. Brit J Nutr 2011, 105, 787–794. [CrossRef]
- World Health Organization. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting, 5–7 October 2006, Paris, France. Geneva: WHO, 2007.
- WHO/PAHO regional expert group for cardiovascular disease prevention through population-wide dietary salt reduction. Protocol for population level sodium determination in 24-hour urine samples. May, 2010. Available online: https://www.paho.org/hq/dmdocuments/2013/24h-urine-Protocol-eng.pdf (accessed on 20 February 2023).
- PAHO. Mapping Dietary Salt/Sodium Reduction Policies and Initiatives in the Region of the Americas. Washington, D.C.: Pan American Health Organization; 2021.
- MISPAS. Ministerio de Salud Pública y Asistencia Social, Gobierno de la República Dominicana. 1era Jornada Nacional de Hipertensión Arterial: Prevención de diabetes y obesidad. Informe de resultados. Santo Domingo D.N. Octubre, 2021.
- PAHO (PanAmerican Health Organization). Plan of Action for the Prevention and Control of Noncommunicable Diseases in the Americas 2013-2019. Washington, DC: OPS, 2014. Available online: https://www.paho.org/hq/dmdocuments/2014/NCD-SP-low.pdf (accessed on 20 February 2023).
- 32. Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.Z.; Azizi, M.; Burnier, M.; et al. Guía ESC/ESH 2018 sobre el diagnóstico y tratamiento de la hipertensión arterial. Rev Esp Cardiol 2019, 72, 160e1–e78.
- PAHO. Hypertension. Available online: https://www.paho.org/en/topics/hypertension (accessed on 20 February 2023).
- Whelton, P.K.; Caarey, R.M.; Mancia, G.; Kreutz, R.; Bundy, J.D.; Williams, B. Harmonization of the American College of Cardiology/ American Heart Association and European Society of Cardiology / European Society of Hypertension Blood Pressure /Hypertension Guidelines. Eur Heart J 2022, 43, 3302–3311. [CrossRef]
- PAHO. Consumers International. Cuestionario sobre conocimiento, actitud, comportamiento acerca de la sal dietética y la salud. Available at: https://www.paho.org/hq/dmdocuments/2013/Knowledge-behaviour-questionaire-salt-Spa.pdf Accessed: 2 March 2023.
- Mosteller, R.D. Simplified calculation of body-surface area. N Engl J Med 1987, 317, 1098. [CrossRef]
- Kawasaki, T.; Itoh, K.; Uezono, K.; Sasaki, H. A simple method for estimating 24 h urinary sodium and potassium excretion from second morning voiding urine specimen in adults. Clin Exp Pharmacol Physiol, 1993,20,7-14. [CrossRef]
- Oh, J.; Lee, J.; Koo, H.S.; Kim, S.; Chin, H.J. Estimated 24-hour urine sodium excretion is correlated with blood pressure in korean population: 2009-2011 Korean National Health and Nutritional Examination Survey. J Korean Med Sci 2014, 29, S109–S116. [CrossRef]
- Pichardo, R.; González, A.R.; Ramírez, W.; et al. Estudio de los factores de riesgo cardiovascular y síndrome metabólico en la República Dominicana. EFRICARD II. Rev Domin Cardiol 2012, 1, 36–55. Available online: https://static.elsevier.es/cardio/static/premio_cardio/revista-dominicana-cardiologia.pdf (accessed on 20 February 2023).
- Paulino-Ramirez, R.; Oakley, E.; Vega, B.; Vilar, M.G.; Mencía-Ripley, A.; Tapia, L.; et al. Diversidad genética en ADN mitocondrial en la República Dominicana: Implicaciones para la historia y demografía de La Española. CLÍO 2019, 88, 193–206.
- Consejo de Ministros de Salud de Centroamérica y República Dominicana (COMISCA), INCAP / OPS-OMS. Instituto de Nutrición de Centro América y Panamá / organización Panamericana de la salud / organización mundial de la salud / consejo de Ministros de Salud de Centroamérica y República dominicana. Estrategia regional para la reducción del consumo de sal y sodio en Centroamérica y República Dominicana. Enero 2019. Available online: http://www.incap.int/index.php/es/noticias/145-estrategia-regional-para-la-reduccion-del-consumo-de-sal-y-sodio-en-centroamerica-y-republica-dominicana (Accessed on 20 February 2023).
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.A.; Cappucio, F.P. Sodium and Potassium Intake in Healthy Adults in Thessaloniki Greater Metropolitan Area—The Salt Intake in Northern Greece (SING) Study, Nutrients, 2017; 9:417. [CrossRef]
- Meyer, H.E.; Johansson, L.; Eggen, A.E.; Johansen, H.; Holvik, K. Sodium and potassium intake assessed by spot and 24-h urine in the population-based TromsØ study 201-2016. Nutrients 2019, 11, 1619. [CrossRef]
- Cogswell, M.W.; Loria, C.M.; Terry, A.L.; Zhao, L.; Wang, C.-Y.; Chen, T-C.; et al. Estimated 24-hour urinary sodium and potassium excretion in US adults. JAMA 2018, 319, 1209–1220. [CrossRef]
- Sun, Y.; Zhang, P.; Li, Y.; He, F.J.; Wu, J.; Xu, J.; et al. Association of sodium, potassium and sodium-to-potassium ratio with urine albumin excretion among the general Chinese population. Nutrients 2021, 13, 3456. [CrossRef]
- Trieu, K.; Ospanova, F.; Tazhibayev, S.; Jewell, J.; Breda, J.; Santos, J.A.; et al. Sodium and potassium intakes in the Kazakhstan population estimated using 24-h urinary excretion: evidence for national action. Eur J Nutr 2021, 60, 1537–1546. [CrossRef]
- Moliterno, P.; Álvarez-Vaz, R.; Pécora, M.; Luzardo, L.; Borgarello, K.; Olascoaga, A.; et al. Blood pressure in relation to 23-hour urinary sodium and potassium excretion in a Uruguayan population sample. Int J Hypertens 2018, 6956078. [CrossRef]
- Huang, F.; Yu, P.; Yuan, Y.; Li, Q.; Lin, F.; Gao, Z.; et al. The relationship between sodium excretion and blood pressure, urine albumin, central retinal arteriolar equivalent. BMC Cardiovasc Disord 2016, 16, 194. [CrossRef]
- Durán-Cabral, M.; Fernández-Jalao, I.; Estévez-Santiago, R.; Olmedilla-Alonso, B. Assessment of individual carotenoid and vitamin A dietary intake in overweight and obese Dominican subjects. Nutr Hosp 2017, 34, 407–415. [CrossRef]
- Del Rosario, P. El consumo de alimentos en República Dominicana. Instituto Dominicano de Investigaciones Agropecuarias y Forestales (IDIAF). Santo Domingo, DO. 2021.
- Johnson, C.; Mohan, S.; Rogers, K.; Shivashankar, R.; Thout, S.R.; Gupta, P.; et al. Mean dietary salt intake in urban andrural areas in India: A population survey of 1395 persons. J Am Heart Assoc 2017, 6, e004547.
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6: 4651-4662. [CrossRef]
- Mannheimer, B.; Sterea-Grossu, A.; Falhammar, H.; Calissendorff, J.; Skov, J.; Lindh, J.D. Current and future burdens of heat-related hyponatremia: A nationwide register-based study. J Clin Endocrinol Metab 2022, 107, e2388–e2393. [CrossRef]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), Turck, D.; Bresson, J-L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; et al. Scientific opinion on dietary reference values for potassium. EFSA J. 2016, 14, 459.
- Huang. L.; Wang, H.; Wang, Z.; Wang, Y.; Zhang, B.; Ding, G. Associations of dietary sodium, potassium, and sodium to potassium ratio with blood pressure – regional disparities in China. Nutrients 2020, 12, 366.
- López, P.; Pérez, W. Situación del consumo de sal y sodio en Centroamérica y República Dominicana. INCAP. Notas Técnicas PP/NT/079. 2018. Available online: http://www.incap.int/index.php/es/publicaciones-destacadas/218-situacion-consumo-sal-sodio-2018 (accessed on 20 February 2023).
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), Bresson, J.L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; et al. Scientific opinion on dietary reference values for potassium. EFSA J 2016, 14, 4592.
- WHO, 2020. Salt reduction. Key facts (29 April 2020). Available online: https://www.who.int/news-room/fact-sheets/detail/salt-reduction (accessed on 20 February 2023).
- AHA, American Heart Association. How potassium can help control high blood pressure. Available online: https://www.heart.org/en/health-topics/high-blood-pressure/changes-you-can-make-to-manage-high-blood-pressure/how-potassium-can-help-control-high-blood-pressure (accessed on 20 February 2023).
Figure 1.
Flow diagram for study participants.
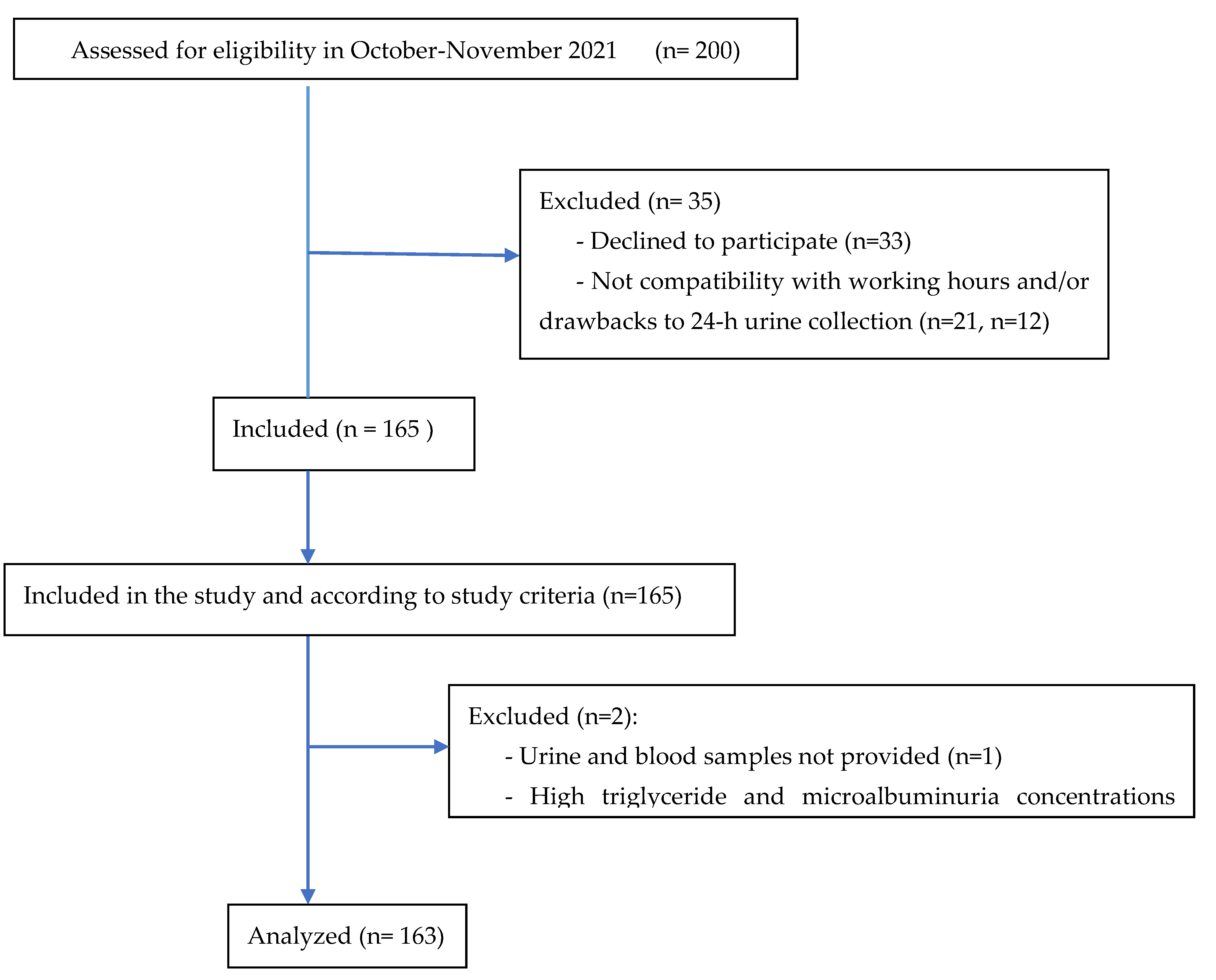

Table 1.
Personal and anthropometric characteristics of the participants (n=163).
| Age (years) | 44.5 ± 14.6 (18 – 80) |
| Sex | Men 78 / women 85 |
| Race | Mix-race (mulatto) 125 / Black 21 / White 15 / Asian 2 |
| Diabetes | No 143 (87.7%) / yes 20 (12.3%) |
| Normotensive / Hypertensive | 88 / 75 |
Table 2.
Blood pressure and biochemical data in 24-h urine and blood. Mean ±SD [median].
| Total sample (n=163) | Normotensive (n=88) |
Hypertensive (n=75) |
P value | 18–45 years (n=84) (normotensive=64, hypertensive=20) |
46–80 years (n=79) (normotensive=24, hypertensive=55) |
P value |
||
| Systolic blood pressure (mm Hg) | 126.2 ± 21.1 [123.3] | 116.3 ± 11.8 [115.8] | 138.0 ± 23.4 [135] |
0.000 | 119.3 ± 15.5 [120.2] |
133.7 ± 23.6 [128.6] |
<0.001 | |
| Diastolic blood pressure (mm Hg) | 81.2 ± 11.2 [81.0] |
76.6 ± 7.3 [76.6] |
86.7 ± 12.5 [87.3] |
<0.001 | 78.7 ± 10.6 [77.6] |
84.0 ± 11.2 [83.6] |
0.001 | |
| Heart rate (bpm) | 71.3 ± 10.2 [71.6] |
71.0 ± 9.8 [70.8] |
71.5 ± 10.8 [72.0] |
0.826 | 72.2 ±10.7 [73.0] |
70.2 ± 9.7 [69.3] |
0.077 | |
| Anthropometric measurementes | ||||||||
| Height (cm) | 166.3 ± 10.0 [165.5] | 167.8 ± 10.6 [166.2] | 164.6 ± 9.1 [164.1] | 0.072 | 169.2 ± 10.3 [169.0] |
163.2 ± 8.8 [162.0] |
<0.001 | |
| Weight (kg) | 80.6 ± 16.0 [79.7] |
79.0 ± 17.6 [77.8] |
82.4 ± 13.9 [83.1] |
0.054 | 81.8 ± 18.1 [79.1] |
79.4 ± 13.4 [80.0] |
0.717 | |
| BMI (kg/m2) | 29.1 ± 4.8 [28.6] |
27.9 ± 4.7 [27.1] |
30.5 ± 4.6 [30.4] |
<0.001 | 28.4 ± 4.8 [27.4] |
29.9 ± 4.7 [29.6] |
0.031 | |
| Waist (cm) | 95.9 ± 12.3 [95.0] |
92.7 ± 12.0 [92.8] |
99.5 ± 11.7 [99.0] |
<0.001 | 93.0 ± 12.2 [92.8] |
98.9 ± 11.8 [98.0] |
<0.001 | |
| Hip (cm) | 107.5 ± 9.0 [107.0] | 106.3 ± 9.4 [104.0] | 108.9 ± 8.5 [109.0] | 0.015 | 106.5 ± 9.2 [104.2] |
108.4 ± 8.8 [108.5] |
0.081 | |
| Waist - hip ratio | 0.89 ± 0.08 [0.89] |
0.87 ± 0.07 [0.87] |
0.91 ± 0.07 [0.92] |
<0.001 | 0.87 ± 0.07 [0.88] |
0.91 ± 0.08 [0.91] |
0.002 | |
| Body fat (%) | 36.3 ± 9.8 [35.4] |
34.8 ± 9.6 [33.3] |
38.1 ± 9.8 [40.3] |
0.019 | 34.1 ± 9.7 [31.5] |
38.7 ± 9.4 [40.0] |
0.002 | |
| Visceral fat (%) | 10.6 ± 4.2 [10.0] |
9.2 ± 3.8 [9.0] |
12.1 ± 4.0 [11.5] |
<0.001 | 9.3 ± 4.0 [9.0] |
11.8 ± 3.9 [11.0] |
<0.001 | |
| Muscle mass (%) | 28.5 ± 5.9 [28.0] |
29.4 ± 6.4 [28.8] |
27.4 ± 5.1 [27.6] |
0.038 | 30.0 ± 6.2 [30.9] |
26.9 ± 5.3 [25.9] |
<0.001 | |
| Urine (24-h) | ||||||||
| Volume (mL) | 1775.2 ± 819.1 [1740.0] | 1709.4 ± 842.7 [1680] | 1833.4 ± 777.2 [1780] | 0.257 | 1732.0 ± 839.2 [1575.0] | 1821.0 ± 800.0 [1850] | 0.367 | |
| Creatinine (mmol) | 12.4 ± 5.3 [11.5] |
13.3 ± 5.3 [11.5] |
11.5 ± 3.5 [11.5] |
0.493 | 14.8 ± 8.3 [14.1] |
12.0 ± 3.6 [11.2] |
<0.001 | |
| Endogenus creatinine clearance (ECC) (mL/min) | 108.7 ±35.7 [105.3] | 113.5 ± 37.1 [115.3] | 103.4 ± 33.4 [101.9] | 0.089 | 118.0 ±35.8 [120.7] |
98.8 ± 33.0 [97.1] |
<0.001 | |
| ECC corrected by surface area (ECC-c) (mL/min) | 100.9 ± 30.6 [102.3] | 105.4 ± 30.1 [105.6] | 96.3 ± 30.3 [96.9] | 0.041 | 107.7 ± 30.5 [109.3] |
93.6 ± 29.2 [93.1] |
<0.001 | |
| Sodium (mmol) | 99.4 ± 46.5 [89.0] |
100.8 ± 47.3 [96.5] | 97.9 ± 46.1 [84.5] | 0.670 | 105.4 ± 46.8 [98.5] |
92.9 ± 45.5 [81.0] |
0.058 | |
| Potassium (mmol) | 35.0 ± 17.5 [31.0] |
37.8 ± 20.2 [33.2] |
31.8 ± 13.1 [29.0] | 0.123 | 35.2 ± 17.6 [31.0] |
34.8 ± 17.5 [31.2] |
0.976 | |
| Sodium : potassium ratio 1 | 3.1 ± 1.3 [2.9] |
3.0 ± 1.3 [2.9] |
3.2 ± 1.3 [3.0] |
0.255 | 3.3 ± 1.3 [3.1] |
2.9 ± 1.1 [2.9] |
0.040 | |
| Na : creatinine ratio | 9.1 ± 6.1 [7.4] |
9.4 ± 7.0 [6.8] |
8.8 ± 4.8 [7.8] |
0.562 | 9.1 ± 6.7 [6.4] |
9.1 ± 5.4 [8.0] |
0.273 | |
| K : creatinine ratio | 3.2 ± 2.3 [2.7] |
3.5 ± 2.8 [2.7] |
2.9 ± 1.5 [2.6] |
0.067 | 3.0 ±2.3 [2.4] |
3.5 ± 2.4 [3.0] |
0.013 | |
| Microalbumin (mg) | 10.4 ± 27.9 [4.8] |
7.0 ± 16.2 [4.3] |
14.4 ± 37.0 [5.5] |
0.005 | 11.0 ±33.8 [4.5] |
9.7 ± 20.0 [5.2] |
0.616 | |
| Blood | ||||||||
| Cholesterol (mg/dL) | 193.0 ± 47.4 [189.7] | 194.8 ± 48.0 [190.5] | 190.6 ± 47.3 [189.6] | 0.687 | 188.4 ± 44.5 [185.2] |
198.3 ± 50.3 [198.7] |
0.258 | |
| HDL-cholesterol (mg/dL) | 48.8 ± 14.6 [46.5] |
51.4 ± 13.3 [49.1] |
45.9 ± 15.7 [42.8] | 0.002 | 50.6 ± 12.7 [48.7] |
47.2 ± 16.5 [44.6] |
0.051 | |
| LDL-chol.(mg/dL) | 122.2 ± 42.6 [42.6] | 123.4 ± 43.9 [122.5] | 120.7 ± 41.3 [125.5] | 0.844 | 118.3 ± 42.8 [121.0] |
126.7 ± 42.3 [127.0] |
0.338 | |
| VLDL-cholesterol (mg/dL) | 21.9 ± 11.1 [19.5] |
20.2 ± 10.8 [17.9] |
24.0 ± 11.2 [20.6] | 0.006 | 19.6 ± 11.2 [14.6] |
24.5 ± 10.5 [22.3] |
<0.001 | |
| Triglycerides (mg/dL) | 111.6 ± 60.6 [97.3] |
101.0 ± 54.2 [89.3] | 120.1 ± 55.8 [103.0] | 0.004 | 98.0 ± 56.2 [73.2] |
122.5 ± 52.7 [111.3] |
<0.001 | |
| Total cholesterol / HDL-chol. | 4.3 ± 2.2 [4.1] |
4.0 ± 1.2 [3.8] |
4.7 ± 3.0 [4.3] |
0.032 | 3.9 ± 1.3 [3.8] |
4.8 ± 2.9 [4.5] |
0.008 | |
| LDL-chol / HDL-chol. | 2.8 ± 2.0 [2.6] |
2.6 ± 1.0 [2.4] |
3.1 ± 2.6 [2.8] |
0.140 | 2.5 ± 1.1 [2.3] |
3.1 ± 2.5 [2.8] |
0.030 | |
| Creatinine (mg/dL) | 0.92 ± 0.28 [0.87] |
0.88 ± 0.22 [0.85] |
0.96 ± 0.34 [0.92] | 0.137 | 0.94 ± 0.29 [0.93] |
0.90 ± 0.28 [0.85] |
0.267 | |
| Glucaemia (mg/dL) | 103.5 ± 31.1 [97.1] | 97.5 ± 25.1 [95.8] |
110.5 ± 35.9 [99.4] | 0.010 | 95.1 ± 14.5 [93.3] |
112.4 ± 40.4 [100.4] |
0.001 | |
Table 3.
Significant correlations [(rho, (p)] between blood pressure and the anthropometric measurements, variables in urine and blood in the total group and in participants grouped according age.
Table 3.
Significant correlations [(rho, (p)] between blood pressure and the anthropometric measurements, variables in urine and blood in the total group and in participants grouped according age.
| Total group (n=163) | 18 - 45 years (n=84) 46-80 years (n= 79) | Normotensive Hypertensive | |||||||
| SBP | DBP | SBP | DBP | SBP | DBP | SBP DBP | |||
| Waist – hip index | 0.432 (<0.001) | 0.259 (<0.001) | 0.508 (<0.001) | 0.316 (0.003) | 0.249 (0.027) | ||||
| BMI | 0.367 (<0.001) | 0.261 (<0.001) | 0.374 (<0.001) | 0.326 (0.002) | 0.264 (0.019) | ||||
| Body fat | 0.196 (0.013) | ||||||||
| Muscle mass | 0.333 (0.002) | ||||||||
| Visceral fat | 0.492 (<0.001) | 0.293 (<0.001) | 0.559 (<0.001) | 0.318 (0.003) | 0.294 (0.009) | ||||
| Sodium | |||||||||
| Potassium | 0.249 (0.019) | ||||||||
| Soldium /Potassium 1 | 0.153 (0.052) | 0.350 (0.002) | 0.373 (<0.001) | 0.395 (<0.001) | |||||
| Sodium/ creatinine | 0.241 (0.032) | ||||||||
| Potassium / creatinine | |||||||||
| Creatinine 24h-urine | 0.429 (<0.001) | ||||||||
| Microalbumin | 0.219 (0.005) | 0.187 (0.017) | 0.262 (0.016) | 0.269 (0.013) | |||||
| HDL-cholesterol | -0.230 (0.003) | - 0.357 (<0.001) | |||||||
| LDL-cholesterol | 0.155 (0.049) | ||||||||
| VLDL | 0.269 (<0.001) | 0.203 (0.010) | 0.216 (0.049) | ||||||
| TG | 0.282 (<0.001) | 0.217 (0.005 ) | 0.226 (0.038) | 0.243 (0.026) | |||||
| Chol. (total) /HDL | 0.303 (<0.001) | 0.373 (<0.001) | |||||||
| LDL / HDL | 0.259 (<0.001) | 0.333 (0.002) | |||||||
| Creatinine (serum) | 0.326 (<0.001) | 0.507 (<0.001) | 0.239 (0.034) | ||||||
| CCE-c | - 0.195 (0.013) | - 0.185 (0.018) | |||||||
Table 4.
General lineal model. Blood pressure (dependent variable) in model: (intersection), sex, BMI, sodium-to-potassium ratio.
Table 4.
General lineal model. Blood pressure (dependent variable) in model: (intersection), sex, BMI, sodium-to-potassium ratio.
| Systolic blood pressure | ||||||
| beta | S.E. | p | 95% CI | |||
| 18-45 years | Constant | 114.4 | 4.8 | 0.000 | 105.0 , 123.8 | |
| Sex (man) | 14.02 | 2.87 | < 0.001 | 8.40 , 19.64 | ||
| Sex (woman) | 0 | |||||
| BMI -normoweight | -12.07 | 3.72 | 0.001 | -19.35 , -4.79 | ||
| BMI - overweight | - 10.7 | 3.2 | <0.001 | -16.95 , -4.49 | ||
| BMI- obese | 0 | |||||
| 46- 80 years | Constant | 118.6 | 7.7 | 0.000 | 103.6 , 133.6 | |
| Sodium-to-potassium ratio | 6.7 | 2.4 | 0.005 | 2.07 , 11.34 |
||
| Diastolic blood pressure | ||||||
| beta | S.E. | P | 95% IC | |||
| 18-45 years | Constant | 78.3 | 3.7 | 0.000 | 71.1 , 85.5 | |
| BMI-normoweight | -9.44 | 2.87 | 0.001 | - 3.8 , 10.8 | ||
| BMI-overweight | -5.1 | 2.5 | 0.039 | -9.9 , -0.26 | ||
| BMI- obese | 0 | |||||
| 46- 80 years | Constant | 73.4 | 3.6 | 0.000 | 66.4 , 80.4 | |
| Sodium-to-potassium ratio | 3.8 | 1.1 | < 0.001 | 1.6 , 5.9 | ||
CI: confidence interval.
Table 5.
Dietary intake of salt, sodium and potassium expressed in g/day. Mean ± SD, [median].
| Sodium intake (g/day) | Salt intake (g/day) | Potassium intake (g/day) | Dietary Na : K (g) | |
| Total sample (n=163) Normotensive (n=88) Hypertensive (n=75) |
2.29 ± 1.07 [2.05] 2.32 ± 1.09 [2.22] 2.25 ± 1.06 [1.94] |
5.8 ± 2.7 [5.2] 5.9 ± 2.8 [5.6] 5.7 ± 2.7 [4.9] |
1.37 ± 0.68 [1.21] 1.47 ± 0.79 [1.30] a 1.24 ± 0.51 [1.17] |
1.7 1.6 1.82 |
| Aged 18-45 years Normotensive (n=64) Hypertensive (n=20) |
2.45 ± 1.12 [2.36] 2.32 ± 0.94 [2.16] |
6.2 ± 2.9 [6.0] 5.9 ± 2.4 [5.5] |
1.43 ± 0.73 [1.24] 1.19 ± 0.52 [1.03] |
1.7 2 |
| Aged 46- 80 years Normotensive (n= 24) Hypertensive (n= 55) |
1.95 ± 0.92 [1.85] 2.22 ± 1.10 [1.91] |
5.0 ± 2.3 [4.7] 5.6 ± 2.8 [4.8] |
1.60 ± 0.94 [1.36] b 1.26 ± 0.52 [1.20] |
1.22 1.76 |
Significant differences between normo and hypertensive: a p=0.025, b p=0.039.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



