
Submitted:
05 June 2023
Posted:
05 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
ACE2 impact on the severity of COVID-19 is widely discussed but still controversial. To estimate its role in aspects of the main risk factors and comorbidities, we involved post-COVID-19 patients in Ternopil region (Ukraine). Recruitment period was July 2020 to December 2021. Medical records, treatment modalities and outcomes were recorded and analyzed. Serum human ACE2 protein was measured with Cusabio ELISA kits (Houston, TX, USA). Statistical analysis was performed with SPSS21.0 software (SPSS Inc., Chicago, IL, USA). The level of ACE2 serum protein was significantly higher (p < 0.001) in patients with mild symptoms compared to more severe course of disease, and inversely had changed from 1 to 90 days after recovery. In patients with mild COVID-19, ACE2 level significantly decreased over time, while among critical patients, it increased by 34.1percent. Such results could be explained by ACE2 shedding from tissues into circulation. Loss of the membrane-bound form of the enzyme decreases the virus entry into cells. Our studies did not identify any sex-related ACE2 serum levels correlation. The most common comorbidities were hypertension, cardiovascular diseases, respiratory diseases and diabetes mellitus. All comorbidities except respiratory diseases contribute to the severity of disease and correlate with ACE2 blood serum level.
Keywords:
COVID-19
; ACE2
; severity
; post-COVID-19 patients
; comorbidity.
1. Introduction
As of May 10, 2023, more than 765 million confirmed cases of COVID-19, including around 7 million deaths, were reported. And as of May 8, 2023, a total of more than 13 billion vaccine doses have been administered (https://covid19.who.int/, accessed May 11, 2023). Since the first cases reported in Wuhan in 2019, the virus has spread to more than 200 countries. Finally, three years later WHO says that COVID-19 is no longer a global health emergency. But SARS-CoV-2 infection continues to spread. The virus is evolving and remains a global health threat but at a lower level of concern. This means that SARS-CoV-2 is still with us, however, it is no longer unusual or unexpected and does not meet the “extraordinary event” criterion. The main issue we will deal with, at least for the next couple of years, is post-COVID-19 condition, or post-acute sequelae of COVID-19, or long-COVID. It is a complex heterogeneous disorder that has affected the lives of millions of people globally [1,2,3,4].
The clinical spectrum of SARS-CoV-2 infection ranges from asymptomatic disease to critical illness and death [5,6]. Acute respiratory distress syndrome (ARDS) and respiratory failure are the leading causes of death, but damage to other organs and systems, including heart, liver and kidney, also contribute to mortality rates, especially in patients with comorbidity [7,8,9,10]. The virus spreads primarily through the respiratory tract, and lymphopenia and cytokine storms have been observed in severely ill patients [11,12].
The main entry gate for SARS-CoV-2 — Angiotensin Converting Enzyme 2 (ACE2) — was identified quite fast [13,14]. ACE2 receptors play an important role in the binding of virus and are located on the surface of many cells including respiratory epithelial and endothelial cells [14,15,16]. These receptors enable entry of the virus into target cells and may be linked to more severe progression of the disease [15,17]. It became an extremely important problem to study, because among the most common comorbidities associated with severe course of the disease are hypertension and other cardiovascular diseases (CVDs) [5,6,18]. The first-line drugs for hypertension treatment are ACE-inhibitors (ACEi, -prils) and Angiotensin II Receptor Blockers (ARBs, -sartans).
ACE and ACE2 are essential parts of the renin-angiotensin system (RAS), which maintains blood pressure and electrolyte balance and has been implicated in the pathogenesis of ARDS in COVID-19 patients. Due to that fact, at the early beginning of the pandemic controversy was observed regarding the impact of common antihypertensive treatments — ACEi and ARBs — on the severity of the SARS-CoV-2 infection. Potential benefit or harm were discussed very intensively. The virus has high affinity to the ACE2 receptors, and its expression is thought to be upregulated in ACEi users [19,20,21]. The increased expression of ACE2 may facilitate infection with COVID-19 and increase the viremia. One more important question: Does hypertension itself or ACEi use impact the severity of COVID-19?
The main risk factors that contribute to the severity course of coronavirus diseases are described in many studies. In addition to pre-existing comorbidities such as hypertension, diabetes mellitus, respiratory and cardiovascular diseases, old age, male sex, healthcare workers (due to higher exposed viral load and increased viral exposure time) and obesity are of the most interest [18,22,23,24,25,26].
Therefore, ACE2 is at the core of COVID-19 research and the aim of our study was to examine its role in the severity and outcomes of coronavirus infection in regard to aspects of the main risk factors and comorbidities.
2. Results
Among 577 involved persons, one third were healthcare workers — 197 (34.1 percent). Patients with mild COVID-19 (Home Quarantined with Mild symptoms (HQM) group) represented almost half of the cohort — 263 (45.6 percent). Hospitalized with Moderate course (HMO) group — 215 (37.3 percent) and Hospitalized oxygen-dependent patients with Severe symptoms (HSV) group — 82 (14.2 percent). Only 17 (2.9 percent) Hospitalized Critical patients in ICU departments with artificial ventilation (HCR) persons survived after time in the intensive care unit (ICU).
The numbers, represented in Table 1, correspond to the regular COVID-19 incidence rate and severity observed in Ukraine during the pandemic period in 2020–2021, the Delta wave of the pandemic (Table 1).
Age. The age of patients was significantly different and increased with the severity of disease (pANOVA < 0.001, χ2 – Pearson Chi-square test). The average age in HQM group was 44.82 ± 12.07 years, in HMO group — 54.10 ± 11.88 years, HSV — 58.73 ± 11.38 years and in HCR — 57.41 ± 11.41 years. According to the time after the last negative polymerase chain reaction (PCR) test, all patients were divided into two groups: 1) 0–45 days after, included 344 persons (59.6 percent), and 2) 46–90 days after, included 233 persons (40.4 percent).
The level of ACE2 serum protein was significantly higher (p < 0.001) in patients with mild course of the disease compared to more severe course, and even compared to seronegative clinically healthy persons (Table 2).
Severity. The serum level of ACE2 significantly decreased proportionally to COVID-19 severity. Its concentration was lower in HCR by 27.6 percent compared to HSV by 29.4 percent, and in HMO by 19.8 percent compared to HQM (p < 0.001). The concentration of ACE2 was higher in HMO [7.37 (5.75; 9.32) vs 6.49 (5.28; 7.25) ng/mL], compared to the HSR group. Moreover, the serum ACE2 in the HQM group was significantly higher than in control group by 16.3 percent (p < 0.001).
Sex difference. We observed the female prevalence (66.9 percent) in our cohort and there was no sex difference in ACE2 blood concentration among the observed groups. But the level of indices was different according to the severity of COVID-19 as well as in the general cohort (Table 3).
Post-COVID-19 time period. In patients with mild COVID-19, the level of ACE2 significantly decreased over time, while among critical patients who survived, we observed the opposite situation — it increased by 34.1 percent in the abovementioned time frame (Table 4). In other groups the tendency was the same.
BMI (body-mass index). We found that the proportion of patients with overweight and obesity increased directly proportionally from the HQM group to the HCR group. Among patients with mild COVID-19, 35.5 percent (93) had normal BMI, 36.3 percent (95) were overweight, and 26.3 percent (69) were obese; while in the HCR group only 5.9 percent had a normal weight, 11.7 percent were overweight and 82.4 percent were obese (Figure 1).
Detailed anthropometric data are presented in Table 5.
It is obvious that body weight and BMI were significantly higher in critical and oxygen-dependent patients compared to those with mild coronavirus diseases. The average body mass in HQM group was 76.02 ± 17.31 kg, while in HCR group was 93.41 ± 15.40 kg, and BMI increased from 27.17 ± 5.68 to 32.80 ± 4.91, respectively.
Among HQM patients, the level of ACE2 protein level was almost the same and did not differ, as well as for the severe and critical patients. But in HMO group, ACE2 level was higher by 33.7 percent in obese patients compared to those with normal weight.
The ACE2 serum protein level was significantly higher in all weight category patients (normal, overweight and obese) in HQM group compared to HMO and HSV patients (p < 0.05).
Data for obese persons is presented at Figure 2.
Pre-existing comorbidity. In the involved cohort the most common comorbidities were hypertension (246 patients or 42.8 percent), cardiovascular diseases (215 or 37.3 percent), respiratory diseases (73 or 12.5 percent) and diabetes mellitus (59 or 10.2 percent).
Hypertension and cardiovascular diseases. Significantly different ACE2 serum protein levels in patients with different COVID-19 severity were observed only in HQM patients with high blood pressure (absent (n = 150), 9.09 [7.83; 9.71] vs present (n = 50), 9.40 [8.84; 10.70]) and CVDs (absent (n = 119), 9.09 [8.36; 9.84] vs present (n = 36), 9.53 [8.36; 10.44]). We estimated statistical difference between groups absent and present for Mann-Whitney U test.
The multivariate analysis demonstrates the correlation between cardiovascular diseases (except hypertension) and ACE2 level (8.54 [6.62; 9.45] without vs 7.15 [5.62; 9.39] ng/mL in case of presence).
Respiratory diseases. The presence of respiratory diseases did not affect the ACE2 serum protein level.
Diabetes mellitus (DM). Most of the patients in the cohort had DM type II and ACE2 levels were significantly higher in all examined groups compared to patients with normal glycemia in the post-COVID-19 period (Table 7). It could be explained by the known fact that Metformin, the cornerstone of treatment of DM type II, also increases the ACE2 level.
3. Discussion
The severity of outcome in COVID-19 is greatly influenced by various comorbidities and unhealthy lifestyle. Since the beginning of the COVID-19 pandemic, the use of ACE-inhibitors and ARBs in hypertensive patients with COVID-19 has been controversial due to the proven role of RAS in regulating blood pressure mechanisms and the role of ACE2 receptors as an entry gate to SARS-CoV-2 [27]. Suppression of ren-in-angiotensin-aldosterone system is therefore a key strategy in the treatment of chronic cardiovascular and renal disease and is achieved by the administration of ACEi, ARBs and mineralocorticoid receptor antagonists, alone or in combination.
RAS operates via the classic ACE/Angiotensin (Ang) II/Ang II type 1(AT1) receptor axis and the non-classical ACE2/Ang 1–7/Mas receptor (MasR) axis. Classical pathway is associated with impairment of respiratory conditions, while non-classical plays a protec-tive role in COVID-19 complications as ARDS [19,28]. ACE2 as a carboxypeptidase con-verts the decapeptide angiotensin I (Ang I) to Ang (1–9) and the octapeptide Ang II to Ang (1–7) [29]. ACE2 possesses vasodilatory, anti-inflammatory and anti-fibrotic effects and is the main counter-balancer for the ACE/AngII/ AT1R pathway. It has a regulatory effect in the heart, kidney, lung and gastrointestinal tracts; regulates the homeostasis of amino ac-ids, the expression of peptides and local innate immune responses in the gut [30]. Bastolla et al. suggest that the main functional role of ACE2 may consist in reversing the inflam-mation process [27]. The roles of ACE and ACE2 have been investigated in an animal model of ARDS. ACE activity was enhanced in ARDS, whereas ACE2 activity was re-duced. It correlated with enhanced levels of Ang II and reduced levels of Ang (1–7) [30].
Our results demonstrate that post-COVID-19 patients with mild symptoms have higher ACE2 serum levels compared to those with severe infection. It is reflected in the studies of other researchers [27,31]. Our analysis strongly suggests that low serum ACE2 levels are a negative prognostic factor in the susceptibility to infection. Maza et al. also ob-served that high levels of serum ACE2 correlate with lower susceptibility to infection [32]. This phenomenon could be explained by the ACE2 shedding from tissue into circulation [33]. ADAM metallopeptidase domain 17 (ADAM17), also called tumor necrosis fac-tor-alpha converting enzyme (TACE), and transmembrane protease serine 2 (TMPRSS2) catalyzes ACE2 shedding from tissue into circulation. ACE2 shedding (ACE2 anchors onto the cell surface are not stable and can be shed from the membrane) might reduce ACE2 surface receptor expression. It finalizes in producing soluble ACE2, resulting in the loss of the membrane-bound form of the enzyme. That is why a higher level of soluble ACE2 in the serum demonstrates a lower ability to bind the virus and enter the cell [34,35].
Membrane-bound ACE2 is the main cellular receptor of SARS-CoV-2, and it is ex-pected that an increase in its level may enhance the infection. Nevertheless, ACE2 plays an important physiological role by downregulating the pro-inflammatory peptides, Ang II and bradykinin, and through this action, it protects the lungs from acute inflammation. Therefore, it was proposed by several authors that higher levels of ACE2 may alleviate the severity of SARS-CoV-2 infection. This hypothesis is supported by our results. However, our study is limited due to the lack of reflection on the levels and activity of the mem-brane-bound ACE2 receptor in pulmonary tissues or in other solid tissues.
Our studies did not identify any sex-related correlation of ACE2 serum level. As we know, ACE2 encoding gene is located on the X chromosome [36], and some studies have found a higher mortality level among men [36,37,38]. It could be explained by the higher number of involved females (67 percent of cohort). Women have increased serum ACE2 compared to men, and women seem to have milder symptoms of COVID-19. In addition, the tendency to lower levels of soluble ACE2 is observed in the aging population [39]. ACE2 levels are low in both sexes up to the age of 12 where upon it increases to a greater extent in males [31]. Also, hypertension and heart failure are likely associated with higher level of serum ACE2 activity in men compared to women [36].
ACE2 levels and SARS-CoV-2 infection severity correlates with BMI and obesity. More fat — more severe COVID-19 progress. There can be many reasons for the increased sus-ceptibility to COVID-19 among the obese and diabetics including for instance impaired immune response in these patient groups. Data are based on the measurements of serum protein levels of ACE2 in 5,457 individuals. Adipose tissue contains as many ACE2 re-ceptors as pulmonary tissues, and it was found that ACE2 expression in adipose tissue of mice is increased by high-fat diet [40]. Obesity, as well as DM, are associated with chronic low-grade inflammation that can aggravate systemic inflammation and influence the outcome in COVID-19.
We have found that the soluble ACE2 level was higher in patients with DM and should play the protective role, but it was not in this case. Clinical data by Prof. M. Hrebenyk demonstrated poor outcomes for COVID-19 patients with DM [41]. Such con-troversy could be explained by the late COVID-19 diagnosis in patients with DM and more severe endothelial dysfunction, caused by comorbidity. ACE2 is localized in the endothe-lial cells and smooth muscle cells of cardiovascular tissue, kidney, skin. So, that means it is a ubiquitous enzyme due to location in vessels throughout the whole body.
Patients with isolated DM postponed admission and/or physician’s consultation and diagnosis of COVID-19 in patients was the latest compared to other categories of patients (Table 8) (Hrebenyk et al. article is in the press).
4. Materials and Methods
Post-COVID-19 patients in the period 1–90 days after the last negative PCR test were involved in the study. Recruitment was performed in healthcare institutions of Ternopil region (Ukraine) between July 15, 2020, and December 28, 2021. Inclusion criteria included: positive PCR test for SARS-CoV-2, availability of medical records and collected vein blood samples as well as signed informed consent. Medical records, clinical manifestations, blood tests, BMI, treatment modalities and outcomes were recorded and analyzed. Final number of enrolled patients was 577, including 386 (66.9 percent) females and 191 (33.1 percent) males, average age (50.63 ± 13.08) years. According to the severity of COVID-19, all patients were divided into the following groups:
- HQM — Home Quarantined with Mild disease course
- HMO — Hospitalized with Moderate course
- HSV — Hospitalized oxygen-dependent patients with Severe symptoms
- HCR — Hospitalized Critical patients in ICU departments with artificial ventilation
As a comparison group, we used 30 seronegative patients with negative PCR test for SARS-CoV-2 and without any symptoms of respiratory illnesses at the time of examination.
Measurements of human ACE2 protein in blood serum were performed with Cusabio ELISA Kits (Houston, TX, USA).
Statistical analysis was performed with SPSS 21.0 software (SPSS Inc., Chicago, IL, USA) using univariate and multivariate tests (Chi-square, Fisher’s exact test, Mann-Whitney U, one-way ANOVA and Kruskal-Wallis ANOVA tests). To present quantitative variables, the arithmetical average (Mean) and (±SD) standard deviation (normal distribution) or the median (Me) and [Lq; Uq] interquartile range (different from normal distribution) were calculated (Shapiro–Wilk test for normality). p < 0.05 was considered statistically significant.
5. Conclusions
The concentration of the blood ACE2 protein is time-dependent and normalized with the time flow after the last negative PCR test. We did not find any sex difference in the indices, which could be explained by lower numbers of involved critical and oxygen-dependent post-COVID-19 patients and women prevalence in the cohort. High BMI, comorbid pathologies such as hypertension, diabetes mellitus and cardiovascular pathology contribute to the severity of disease and correlate with the ACE2 blood serum level. ACE2 levels correlate with COVID-19 severity and its concentration decreased in oxygen-dependent and critical patients compared to the mild form of the disease.
Author Contributions
Conceptualization and Methodology, S.V. and M.K.; Software, K.K; Validation, S.V. and M.K.; Formal Analysis, K.K. and S.O.; Investigation, S.O., A.P., S.P. and Y.I.; Resources, S.V. and M.K.; Data Curation, S.O., A.P., S.P. and Y.I.; Writing – Original Draft Preparation, S.O.; Writing – Review & Editing, S.V. and M.K.; Supervision, S.V. and M.K.; Project Administration, S.V. and M.K.; Funding Acquisition, S.V. and M.K. All authors have read and agreed to the published version of the manuscript.
Funding
The study was supported by RECOOP Research Grant # 023 “Impacts of COVID-19 infection on patients with high blood pressure using angiotensin-converting enzyme inhibitors (ACEI), angiotensin-receptor blockers (ARBs)”, RECOOP Research Grant # 024 “Vascular Dysfunction in post-infected COVID-19 patients” and Ministry of Health of Ukraine Grant #0121U100305.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Bioethics Committee of the I. Horbachevsky Ternopil National Medical University, Protocol N 59 of 06/05/2020.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We thank Cedars-Sinai Medical Center’s International Research and Innovation in Medicine Program and the RECOOP HST Association for their support. We appreciate Ternopil region Primary Care Facilities and local healthcare authorities for supporting the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; Lin, K.; Mansur, R.B.; Ho, R.C.; Rosenblat, J.D.; Miskowiak, K.W.; Vinberg, M.; Maletic, V.; McIntyre, R.S. Fatigue and Cognitive Impairment in Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; Jafari, A.; Sasannia, F.; Ashrafi, S.; Nazeri, M.; Nasiri, S.; Shahisavandi, M. Long COVID Syndrome-Associated Brain Fog. J. Med. Virol. 2022, 94, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.T.; Porcher, R.; Pane, I.; Ravaud, P. Course of Post COVID-19 Disease Symptoms over Time in the ComPaRe Long COVID Prospective e-Cohort. Nat. Commun. 2022, 13, 1812. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; Iotti, G.; Latronico, N.; Lorini, L.; Merler, S.; Natalini, G.; Piatti, A.; Ranieri, M.V.; Scandroglio, A.M.; Storti, E.; Cecconi, M.; Pesenti, A. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; Cookingham, J.; Coppa, K.; Diefenbach, M.A.; Dominello, A.J.; Duer-Hefele, J.; Falzon, L.; Gitlin, J.; Hajizadeh, N.; Harvin, T.G.; Hirschwerk, D.A.; Kim, E.J.; Kozel, Z.M.; Marrast, L.M.; Mogavero, J.N.; Osorio, G.A.; Qiu, M.; Zanos, T.P. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and Diabetes as High-Risk Factors for Severe Coronavirus Disease 2019 (Covid-19). Diabetes Metab. Res. Rev. 2021, 37, e3377. [Google Scholar] [CrossRef]
- Ahmed, S.; Zimba, O.; Gasparyan, A.Y. Thrombosis in Coronavirus Disease 2019 (COVID-19) through the Prism of Virchow’s Triad. Clin. Rheumatol. 2020, 39, 2529–2543. [Google Scholar] [CrossRef]
- Su, H.; Yang, M.; Wan, C.; Yi, L.X.; Tang, F.; Zhu, H.Y.; Yi, F.; Yang, H.C.; Fogo, A.B.; Nie, X.; Zhang, C. Renal Histopathological Analysis of 26 Postmortem Findings of Patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Li, X.; Ma, X. Acute Respiratory Failure in COVID-19: Is It “Typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef]
- Coperchini, F.; Chiovato, L.; Croce, L.; Magri, F.; Rotondi, M. The Cytokine Storm in COVID-19: An Overview of the Involvement of the Chemokine/Chemokine-Receptor System. Cytokine Growth Factor Rev. 2020, 53, 25–32. [Google Scholar] [CrossRef]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines Including Interleukin-6 in COVID-19 Induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef]
- (Kai, H.; Kai, M. Interactions of Coronaviruses with ACE2, Angiotensin II, and RAS Inhibitors—Lessons from Available Evidence and Insights into COVID-19. Hypertens. Res. 2020, 43, 648–654. [Google Scholar] [CrossRef]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The Vascular Endothelium: The Cornerstone of Organ Dysfunction in Severe SARS-CoV-2 Infection. Crit. Care 2020, 24, 353. [Google Scholar] [CrossRef]
- Amraei, R.; Rahimi, N. COVID-19, Renin-Angiotensin System and Endothelial Dysfunction. Cells 2020, 9, 1652. [Google Scholar] [CrossRef]
- Long, B.; Brady, W.J.; Koyfman, A.; Gottlieb, M. Cardiovascular Complications in COVID-19. Am. J. Emerg. Med. 2020, 38, 1504–1507. [Google Scholar] [CrossRef]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F. M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; Nicklin, S.A.; Marian, A.J.; Nosalski, R.; Murray, E.C.; Guzik, B.; Berry, C.; Touyz, R.M.; Kreutz, R.; Dao, W.W.; Bhella, D.; Sagliocco, O.; Crea, F.; Thomson, E.C.; McInnes, I.B. COVID-19 and the Cardiovascular System: Implications for Risk Assessment, Diagnosis, and Treatment Options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of Comorbidities and Its Effects in Coronavirus Disease 2019 Patients: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- South, A.M.; Tomlinson, L.; Edmonston, D.; Hiremath, S.; Sparks, M.A. Controversies of Renin-Angiotensin System Inhibition during the COVID-19 Pandemic. Nat. Rev. Nephrol. 2020, 16, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Chary, M.A.; Barbuto, A.F.; Izadmehr, S.; Hayes, B.D.; Burns, M.M. COVID-19: Therapeutics and Their Toxicities. J. Med. Toxicol. 2020, 16, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Khashkhusha, T.R.; Chan, J.S.K.; Harky, A. ACE Inhibitors and COVID-19: We Don’t Know Yet. J. Card. Surg. 2020, 35, 1172–1173. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Poland, G. Influenza Immunization and COVID-19. Vaccine 2020, 38, 6078–6079. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; Zhang, Y.; Song, J.; Wang, S.; Chao, Y.; Yang, Z.; Xu, J.; Zhou, X.; Chen, D.; Xiong, W.; Xu, L.; Zhou, F.; Jiang, J.; Bai, C.; Zheng, J.; Song, Y. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Verma, R.; Lohana, P.; Lohana, A.; Ramphul, K. Acute Myocardial Infarction in COVID-19 Patients. A Review of Cases in the Literature. Arch. Med. Sci Atheroscler. Dis. 2021, 6, e169–e175. [Google Scholar] [CrossRef] [PubMed]
- Rojas-García, M.; Vázquez, B.; Torres-Poveda, K.; Madrid-Marina, V. Lethality Risk Markers by Sex and Age-Group for COVID-19 in Mexico: A Cross-Sectional Study Based on Machine Learning Approach. BMC Infect. Dis. 2023, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- (Hamer, M.; Gale, C.R.; Kivimäki, M.; Batty, G.D. Overweight, Obesity, and Risk of Hospitalization for COVID-19: A Community-Based Cohort Study of Adults in the United Kingdom. Proc. Natl. Acad. Sci. USA 2020, 117, 21011–21013. [Google Scholar] [CrossRef] [PubMed]
- Bastolla, U.; Chambers, P.; Abia, D.; Garcia-Bermejo, M.-L.; Fresno, M. Is Covid-19 Severity Associated With ACE2 Degradation? Front. Drug Discov. 2022, 1, 5. [Google Scholar] [CrossRef]
- Chen, F.; Chen, Y.; Ke, Q.; Wang, Y.; Gong, Z.; Chen, X.; Cai, Y.; Li, S.; Sun, Y.; Peng, X.; Ji, Y.; Zhang, T.; Wu, W.; Cui, L.; Wang, Y. ApoE4 Associated with Severe COVID-19 Outcomes via Downregulation of ACE2 and Imbalanced RAS Pathway. J. Transl. Med. 2023, 21, 103. [Google Scholar] [CrossRef]
- Lee, S.H.; Lee, Y.H.; Jung, S.W.; Kim, D.J.; Park, S.H.; Song, S.J.; Jeong, K.H.; Moon, J.Y.; Ihm, C.-G.; Lee, T.W.; Kim, J.S.; Sohn, I.S.; Lee, S-Y.; Kim, D-O.; Kim, Y.G. Sex-Related Differences in the Intratubular Renin-Angiotensin System in Two-Kidney, One-Clip Hypertensive Rats. Am. J. Physiol. Renal Physiol. 2019, 317, F670–F682. [Google Scholar] [CrossRef]
- Pouremamali, A.; Babaei, A.; Malekshahi, S.S.; Abbasi, A.; Rafiee, N. Understanding the Pivotal Roles of ACE2 in SARS-CoV-2 Infection: From Structure/Function to Therapeutic Implication. Egypt J. Med. Hum. Genet. 2022, 23, 103. [Google Scholar] [CrossRef]
- Mortaz, E.; Jamaati, H.; Roofchayee, N. D.; Sheikhzade, H.; Mirenayat, M.; Sadeghi, M.; Lookzadeh, S.; Dezfuli, N.K.; Folkerts, G.; Mumby, S.; Garssen, J.; Adcock, I.M. Decreased Serum Levels of Angiotensin Converting Enzyme (ACE)2 and Enhanced Cytokine Levels with Severity of COVID-19: Normalisation upon Disease Recovery. Heliyon 2022, 8, e08957. [Google Scholar] [CrossRef]
- Maza, M.; Úbeda, M.; Delgado, P.; Horndler, L.; Llamas, M.A.; van Santen, H.M.; Alarcón, B.; Abia, D.; García-Bermejo, L.; Serrano-Villar, S.; Bastolla, U.; Fresno, M. ACE2 Serum Levels as Predictor of Infectability and Outcome in COVID-19. Front. Immunol. 2022, 13, 836516. [Google Scholar] [CrossRef]
- Florescu, S.; Stanciu, D.; Zaharia, M.; Kosa, A.; Codreanu, D.; Fareed, K.; Kidwai, A.; Kaye, C.; Coutts, A.; MacKay, L.; et al. Effect of Angiotensin-Converting Enzyme Inhibitor and Angiotensin Receptor Blocker Initiation on Organ Support–Free Days in Patients Hospitalized With COVID-19: A Randomized Clinical Trial. JAMA 2023, 329, 1183–1196. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, H.; An, Y. ACE2 Shedding and the Role in COVID-19. Front. Cell. Infect. Microbiol. 2022, 11, 789180. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; Guan, L.; Wei, Y.; Li, H.; Wu, X.; Xu, J.; Tu, S.; Zhang, Y.; Chen, H.; Cao, B. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.M.; Mehta, J.L. Hypothesis: Sex-Related Differences in ACE2 Activity May Contribute to Higher Mortality in Men Versus Women With COVID-19. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 114–118. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S.; Cannarella, R.; Condorelli, R.A.; Torre, F.; Aversa, A.; Calogero, A.E. Sex-Specific SARS-CoV-2 Mortality: Among Hormone-Modulated Ace2 Expression, Risk of Venous Thromboembolism and Hypovitaminosis D. Int. J. Mol. Sci. 2020, 21, 2948. [Google Scholar] [CrossRef] [PubMed]
- Bienvenu, L.A.; Noonan, J.; Wang, X.; Peter, K. Higher Mortality of COVID-19 in Males: Sex Differences in Immune Response and Cardiovascular Comorbidities. Cardiovasc. Res. 2020, 116, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, H.C.; Sukumaran, V.; Al-Ruweidi, M.K.A.A.; Shurbaji, S. Do Changes in ACE-2 Expression Affect SARS-CoV-2 Virulence and Related Complications: A Closer Look into Membrane-Bound and Soluble Forms. Int. J. Mol. Sci. 2021, 22, 6703. [Google Scholar] [CrossRef] [PubMed]
- Emilsson, V.; Gudmundsson, E.F.; Aspelund, T.; Jonsson, B.G.; Gudjonsson, A.; Launer, L.J.; Lamb, J.R.; Gudmundsdottir, V.; Jennings, L.L.; Gudnason, V. Serum Levels of ACE2 Are Higher in Patients with Obesity and Diabetes. Obes. Sci. Pract. 2021, 7, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Hrebenyk, M.; Maslii, S.; Shevchuk, O.; Korda, M.; Vari, S.G. Impact of High Blood Pressure and Antihypertensive Treatment on COVID-19 Severity (Retrospective Observational Study in Ternopil Region, Ukraine). In Materials of 17th RECOOP Bridges in Life Sciences, Video Conference; Prague, Check Republic, 2022, pp 72–73.
Figure 1.
The distribution of patients according to severity of COVID-19 and BMI index (χ2 = 61.23; p < 0.001, χ2 – Pearson Chi-square test). * - the indices were significantly different compared to HQM group, p < 0.05. HQM – Home Quarantined with Mild COVID-19 course, HMO – Hospitalized with Moderate course, HSV – Hospitalized oxygen-dependent patients with Severe symptoms, HCR – Hospitalized Critical patients in ICU departments with artificial ventilation.
Figure 1.
The distribution of patients according to severity of COVID-19 and BMI index (χ2 = 61.23; p < 0.001, χ2 – Pearson Chi-square test). * - the indices were significantly different compared to HQM group, p < 0.05. HQM – Home Quarantined with Mild COVID-19 course, HMO – Hospitalized with Moderate course, HSV – Hospitalized oxygen-dependent patients with Severe symptoms, HCR – Hospitalized Critical patients in ICU departments with artificial ventilation.

Figure 2.
ACE2 serum protein level in obese patients (Median, ng/mL) in different COVID-19 severity groups. * — significantly different compared to HQM group, p < 0.05. # — significantly different compared to HMO group, p < 0.05. HQM — Home Quarantined with Mild COVID-19 course. HMO — Hospitalized with Moderate course. HSV — Hospitalized oxygen-dependent patients with Severe symptoms. HCR — Hospitalized Critical patients in ICU departments with artificial ventilation
Figure 2.
ACE2 serum protein level in obese patients (Median, ng/mL) in different COVID-19 severity groups. * — significantly different compared to HQM group, p < 0.05. # — significantly different compared to HMO group, p < 0.05. HQM — Home Quarantined with Mild COVID-19 course. HMO — Hospitalized with Moderate course. HSV — Hospitalized oxygen-dependent patients with Severe symptoms. HCR — Hospitalized Critical patients in ICU departments with artificial ventilation
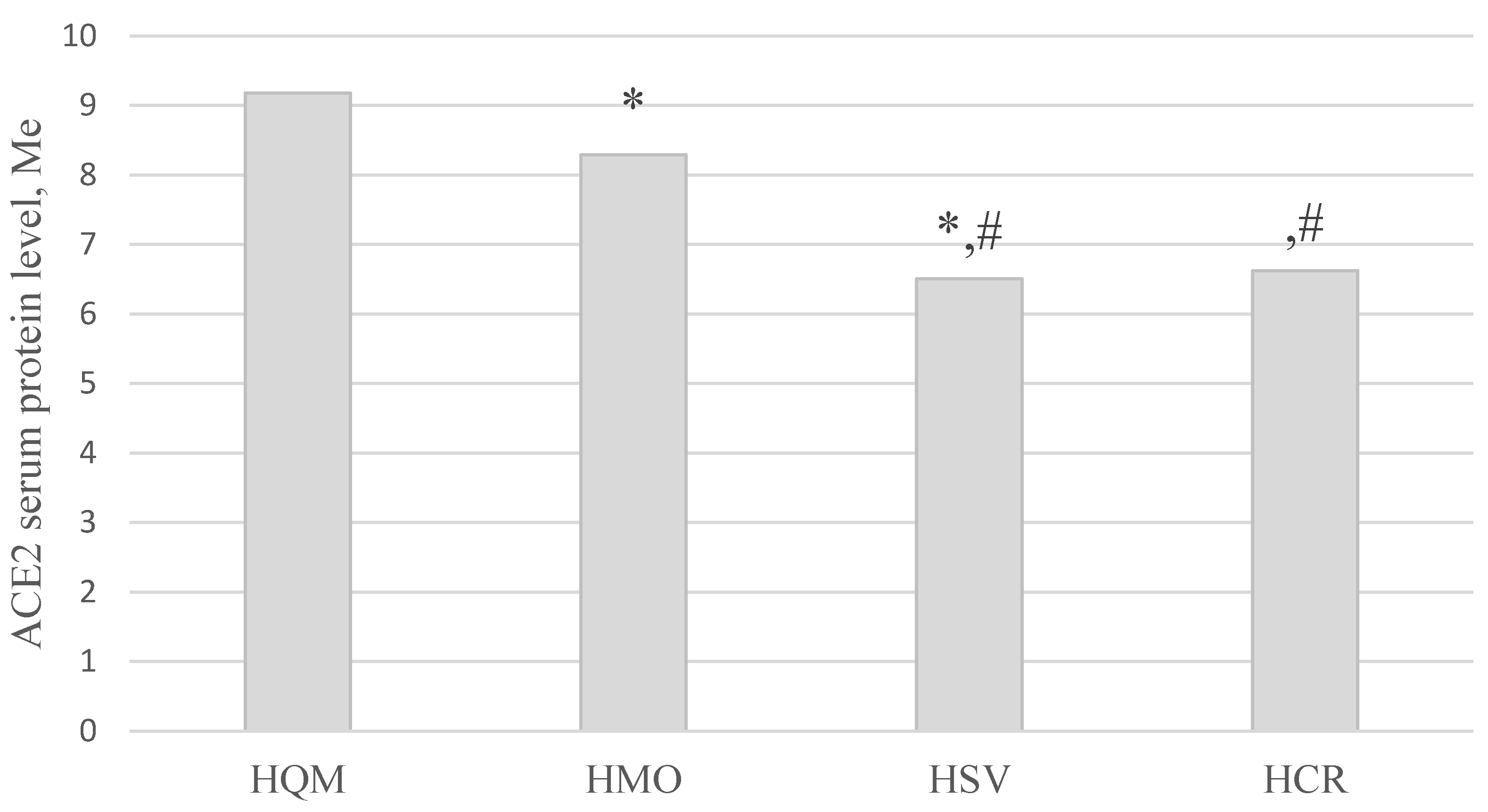

Table 1.
Post-COVID-19 patients in the period 1–90 days after the last negative polymerase chain reaction (PCR) test.
Table 1.
Post-COVID-19 patients in the period 1–90 days after the last negative polymerase chain reaction (PCR) test.
| 0–45 days after the last negative PCR (59.6%) | 46–90 days after the last negative PCR (40.4%) | ||||||
|---|---|---|---|---|---|---|---|
| 344 | 233 | ||||||
| Total number | Females (66.9%) | Males (33.1%) | Average age | Seronegative patients (control) | |||
| 577 | 386 | 191 | 50.63 ± 13.08 years | 30 | |||
| Patients based on COVID-19 severity were divided into groups | |||||||
| HQM (45.6%) | HMO (37.3%) | HSV (14.2%) | HCR (2.9%) | ||||
| 263 | 215 | 82 | 17 | ||||
Table 2.
ACE2 level depending on COVID-19 severity (Me [Lq; Uq]) with control comparison.
| Groups | ACE2, ng/mL n = 440 |
|
|---|---|---|
| n | Me [Lq; Uq] | |
| HQM (1) | 155 | 9.19 [8.36; 10.05] |
| HMO (2) | 156 | 7.37 [5.75; 9.32] |
| HSV (3) | 82 | 6.49 [5.28; 7.25] |
| HCR (4) | 17 | 6.65 [5.35; 7.35] |
| Control group (5) | 30 | 7.69 [6.82; 9.09] |
| Kruskal-Wallis test | H = 104.53; p < 0.001* | |
| Multiple groups comparisons | p1-2, 1-3, 1-4, 1-5 < 0.001*, p2-3 < 0.05*, p 3-5 < 0.05* | |
1 Note: * – statistically significant results.
Table 3.
Sex differences in ACE2 level in study groups (Me [Lq; Uq]).
| Group | ACE2, ng/mL; n = 410 | ||
| M | F | ||
| HQM (A) | n | 54 | 101 |
| Me [Lq; Uq] |
9.05 [8.19; 10.70] |
9.22 [8.53; 9.94] |
|
| HMO (B) | n | 60 | 96 |
| Me [Lq; Uq] | 7.65 [6.32; 9.53] |
6.93 [5.61; 9.04] |
|
| HSV (C) | n | 41 | 41 |
| Me [Lq; Uq] |
6.67 [4.95; 7.25] |
6.05 [5.33; 7.17] |
|
| HCR (D) | n | 9 | 8 |
| Me [Lq; Uq] |
6.60 [5.35; 6.88] |
7.05 [5.47; 7.41] |
|
| Kruskal-Wallis test | H = 41.35, p < 0.001* |
H = 60.93, p < 0.001* |
|
| Multiple groups comparisons | p A-B, A-C, A-D, B-C < 0.05* | p A-B, A-C, A-D < 0.05* | |
1 Note. * – statistically significant results. 2 Note. M – males; F – females.
Table 4.
ACE2 serum level (ng/mL) is a time-dependent index (Me [Lq; Uq])..
| Group | 0–45 days | 46–90 days |
|---|---|---|
| HQM | 9.41 [8.85; 10.88] | 8.94 [7.43; 9.54]* |
| HCR | 5.16 [4.75; 6.34] | 6.92 [6.60; 7.41]* |
Note. * – statistically significant results (p < 0.05).
Table 5.
Anthropometrical parameters of persons recruited in the study depending on the COVID-19 severity.
Table 5.
Anthropometrical parameters of persons recruited in the study depending on the COVID-19 severity.
| Parameters | HQM (1) | HMO (2) | HSV (3) | HCR (4) | Statistical significance |
| Weight, kg | 76.02 ± 17.31 |
83.24# ± 14.88 |
88.70# ± 18.04 |
93.41# ± 15.40 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.001* |
| Height, cm | 166.43 ± 13.35 |
168.25 ± 9.26 |
168.99 ± 9.67 |
168.76 ± 9.58 |
pANOVA = 0.186 |
| BMI, kg/m2 | 27.17 ± 5.68 |
29.45# ± 4.76 |
31.01# ± 5.29 |
32.80# ± 4.91 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.001* |
| WC, cm | 90.91 ± 14.92 |
99.66# ± 13.49 |
106.63# ± 12.38 |
109.29# ± 9.58 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.001* p2-3 < 0.001* p2-4 = 0.031* |
| HC, cm | 105.24 ± 11.46 |
109.12# ± 9.48 |
111.35# ± 10.33 |
114.06# ± 11.71 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.01* |
| WHtR | 0.54 ± 0.09 |
0.59# ± 0.08 |
0.63# ± 0.07 |
0.65# ± 0.06 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.001* p2-3 = 0.002* p2-4 = 0.038* |
| WHR | 0.86 ± 0.10 |
0.91 ± 0.09 |
0.96 ± 0.08 |
0.96 ± 0.09 |
pANOVA < 0.001* p1-2; p1-3; p1-4 < 0.001* p2-3 = 0.001* |
| AO (WC ≥ 94 cm [M], ≥ 80 cm [W])* | 179 (69.65%) |
186 (88.57%) |
76 (96.20%) |
17 (100.00%) |
χ2 = 45.79; p < 0.001* |
| AO (WHtR ≥ 0.5) | 175 (67.83%) |
185 (88.94%) |
77 (97.47%) |
17 (100.00%) |
χ2 = 55.02; p < 0.001* |
| AO (WHR ≥0.90 [M]; ≥0.85 [W]) | 137 (53.31%) |
158 (75.24%) |
72 (91.14%) |
17 (100.00%) |
χ2 = 58.18; p < 0.001* |
1Note: AO – abdominal obesity; WC – waist circumference; HC – hip circumference; WHtR – waist to height ratio; WHR – waist-hip ratio; M – men; W – women. 2Note: * – statistically significant results. 3Note: # – statistical difference between groups HMO, HSV, HCR and HQM (p < 0.05).
Table 7.
ACE2 level in patients with diabetes mellitus depending on the COVID-19 severity. ACE2, ng/mL (Me [Lq; Uq]).
Table 7.
ACE2 level in patients with diabetes mellitus depending on the COVID-19 severity. ACE2, ng/mL (Me [Lq; Uq]).
| Group | Diabetes Mellitus | ||
|---|---|---|---|
| absent | present | ||
| HQM (A) | n | 150 | 5 |
| Me [Lq; Uq] |
9.18 [8.35; 9.9]) |
11.16 # [9.53; 12.77] |
|
| HMO (B) | n | 138 | 18 |
| Me [Lq; Uq] |
7.11 [5.57; 9.26]) |
8.21 # [7.19; 9.57] |
|
| HSV (C) | n | 62 | 20 |
| Me [Lq; Uq] |
6.20 [4.90; 7.06] |
7.14 # [5.67; 8.96] |
|
| HCR (D) | n | 13 | 4 |
| Me [Lq; Uq] |
6.34 [4.97; 6.88] |
7.37 # [7.26; 7.41] |
|
| Kruskal-Wallis test | H = 98.02 p < 0.001* |
H = 11.92 p = 0.008* |
|
| Multiple groups comparisons | p A-B, A-C, A-D, B-C < 0.05* |
p A-C < 0.05* | |
1Note. * – statistically significant results compared to different severity of disease. 2Note. # – statistically significant results compared to groups with absent or present diabetes mellitus.
Table 8.
Admission and/or physician’s consultation and diagnosis of COVID-19 in patients.
| COVID-19 | 1 — HP, n = 338 |
2 — HP + DM, n = 88 |
3 — DM, N = 17 |
4 — No HP, No DM, n = 500 | p < 0,05 |
| Diagnosis | 5.58 ± 0.42 | 4.80 ± 0.38 | 8.33 ± 1.60 | 5.01 ± 0,34 | р1-3 = 0.037, р2-3 = 0.0003, р3-4 = 0.018 |
1 HP – Hypertension, DM – Diabetes mellitus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



