
Submitted:
05 June 2023
Posted:
06 June 2023
You are already at the latest version
Abstract
Toxocarosis remains an important neglected parasitic infection representing one of the most common zoonotic infections caused by the parasite Toxocara canis or less frequently by Toxocara cati. The epidemiology of the disease is complex due to its transmission route by accidental ingestion of embryonated Toxocara eggs or larvae from tissues from domestic or wild paratenic hosts. Even though Toxocara infects about 1,4 billion people worldwide, global epidemiological data regarding the relationship between seropositivity and toxocarosis is limited. Although the vast majority of the infected individuals remains asymptomatic or experiences a mild disease, the infection is associated with important health and socioeconomic consequences, particularly in underprivileged, tropical, and subtropical areas. Toxocarosis is a disease with multiple clinical presentations, which are classified into five distinct forms: the classical visceral larva migrans, ocular toxocarosis, common toxocarosis, covert toxocarosis, and cerebral toxocarosis or neurotoxocarosis. Anthelmintic agents as for example albendazole or mebendazole is the recommended treatment, whereas a combination with topical or systemic corticosteroids for specific forms is suggested. Prevention strategies include educational programs, behavioural and hygienic changes, enhancement of the role of veterinarians, and anthelmintic regimens to control active infections.
Keywords:
Toxocara canis
; Toxocara cati
; Toxocarosis
; Parasitic infection
; Visceral larva migrans
; albendazole
1. Introduction
Human toxocarosis is an anthropozoonosis caused by the parasitic nematodes of the genus Toxocara, classified under the super-family of Ascaridoidea [1,2,3]. The term “toxocarosis” is used to designate the clinical spectrum of the human disease caused by the larval ascarids Toxocara canis, the roundworm of dogs, and less frequently Toxocara cati, the roundworm of cats [4]. In 1952, Beaver et al. (1952) presented the first defined cases of human visceral toxocarosis [5]; in the meanwhile, the infection was acknowledged as a cosmopolitan disease reported in approximately 100 countries [4,6]. In the natural definitive hosts (e.g., dogs and cats), the nematodes usually inhabit the digestive tract from where they are expelled into the environment as eggs with faeces [7], potentially spreading the infections to humans. Humans can be infected directly by animals or indirectly, that is, by ingestion of parasite eggs via consumption of contaminated vegetables and raw or undercooked meat [8,9,10]. Once ingested, eggs are converted to juvenile larvae, which hatch into the intestinal lumen, penetrate the intestinal wall, and migrate through the circulation in distal organs and systems leading to pleomorphic inflammatory and immune responses [11,12]. Due to the associated climate conditions, it probably represents the most common helminthiasis in tropical and subtropical areas. Moreover, reflecting children’s habit of putting their fingers in their mouths during their playing activities is considered an infection of childhood [13,14,15]. Reported seroprevalence of toxocarosis ranges between 2% and 37% in urban and rural areas of Europe and the USA, but may reach 93% in tropical regions [15,16,17,18,19]. Such variations can be explained predominantly by climate changes and hygiene conditions. The rate of infected dogs and the care of systemic administration of anthelmintics alongside children’s playing habits—which differ significantly between rural and urban areas—serve as an additional explanation of the observed variations [15,19,20]. Depending on the affected organs and symptoms, toxocarosis is classified into five differentiating forms. Visceral larva migrans and ocular toxocarosis represent the classical and most common clinical presentations, whereas covert toxocarosis, common toxocarosis, and neurotoxocarosis are further associated clinical syndromes [21,22]. The severity of the disease depends on various parameters, for example, the parasitic load, organs affected, host age, and immune responses of the affected individual [23,24,25]. The typical patient with toxocarosis will present a combination of general symptoms, for example, fever, fatigue, anorexia, malaise, and weight loss with symptoms of visceral origin—predominantly pulmonary—such as cough, dyspnea, and bronchospasm, hepatic, cardiac, gastrointestinal, cutaneous, and lymphatic [26,27,28,29,30]. Furthermore, it is well established that most human infections are asymptomatic or present non-specific signs and symptoms [10,21,31]. This last point in combination with the unfamiliarity of the disease among health care providers may explain the fact that although toxocarosis represents one of the most common helminthiases, the majority of the human infections remain undiagnosed resulting in a potential underestimation of its zoonotic impact on public health [10,21,31,32]. Despite the fact that the diagnosis of toxocarosis is mainly based on serological findings (i.e., primarily using ELISA), the recent identification of the sequent genome of T. canis as well as the transcriptomic analysis has opened new perspectives regarding our global understanding of this parasite [1,33,34]. In the present work, we focus on current developments related to the epidemiology, pathophysiology, diagnosis, treatment, management, and prevention of this neglected parasitic disease.
2. Terminology
In reference to the terminology of the disease and stimulated by the confusing use of “toxocariosis” and “toxocarosis”, based on the Standardized Nomenclature of Animal Parasitic Diseases (SNOAPAD) we encourage the use of the term “toxocarosis” to improve the clarity of scientific communication [26,35]. Moreover, clinicians should be cautious with the use of the terms “toxocarosis” and Toxocara infection, as “toxocarosis” refers to a symptomatic patient with abnormal laboratory tests, whereas “Toxocara infection” concerns clinically asymptomatic healthy individuals with positive anti-Toxocara antibodies [26].
3. Epidemiology
Toxocarosis represents the most common zoonotic helminth infection in industrialised countries [36] and is primarily caused by the ingestion of the eggs of nematode parasites of the genus Toxocara, commonly through the dog roundworm Toxocara canis and less frequently by the cat roundworm Toxocara cati [37,38].
The seroprevalence of toxocarosis varies worldwide. Tropical and subtropical areas present the highest values—even higher than 50 % [36]. Approximately 1.4 billion people are infected with or come into contact with Toxocara species worldwide [39]. In a meta-analysis by Rostrami et al. (2019), the global pooled seroprevalence of Toxocara was estimated at 19 % (95% CI 16.6–21.4 %). For Europe, its estimated impact appears to be around 18 % [40].
Infection tends to be more common in tropical regions due to the high humidity than in temperate regions, more common among rural populations with inadequate water supplies and poor housing than among urban populations, and more common in areas affected by poverty [41].
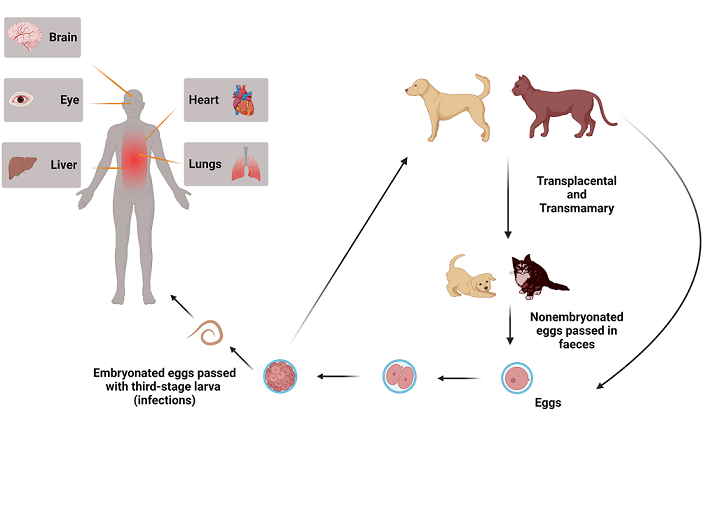
Usually, these parasites are transmitted directly to the human host via the faecal-oral route and can cause toxocariasis and associated complications, including allergic and neurologic disorders. Infected definitive hosts, such as dogs and cats, excrete the eggs in their faeces and, subsequently, under suitable conditions (i.e., humidity and temperature), they contaminate the environment, where they can remain infectious for many months or even years [7,42,43]. The eggs, which contain infective third-stage larvae, are accidentally ingested through contact with humans (e.g., via contaminated food such as raw vegetables or fruit, water or soil) (Figure 1). For example, consuming inadequately cooked or raw liver from infected animals has been associated with toxocarosis [44,45]. Another risk factor is human contact with dogs or cats, where embryonated eggs are found on the hair of these animals [7,42,43]. However, only a small number of embryonated eggs can be found on the host hair of well-cared animals [46]. Humans can also become infected by ingesting encysted third-stage larvae in raw or inadequately cooked meat or organs from paratenic hosts, such as rabbits, sheep, cattle, and chickens [44,45,47,48].
Figure 1.
Toxocara lifecycle.
4. Pathophysiology
Infection of the tissue triggers an inflammatory immune response in the body resulting in the clinical manifestations of the disease (usually nonspecific), for example, fever, headache, cough, and pain [49,50]. It is well recognized that specific “pathogen-associated molecular patterns” exist for any helminth infection. For Toxocara canis, these patterns are characterized by enhanced adaptive immune reactions and are primarily mediated by CD4+ T-helper type 2 cell (Th2) [51], also called type 2 immune response. The elevated CD4+ Th2 activity leads to the production and release of inflammatory mediators—especially interleukin (IL)-4, -5, -10, and -13—triggering the production of immunoglobulin (Ig)E antibodies and the differentiation of eosinophils [5]. It is well established that eosinophilia aims the destruction of the parasitic infection and that the eosinophilic chemotaxis is triggered apart from T-cell-mediated responses from IgE-associated reactivity and direct chemotactic properties of the parasites [52]. Experimental studies in mice have demonstrated a biphasic response with two peaks: an early peak at day 10 and a late peak at day 21. Interestingly, in CD4 T cell-deficient mice, only the early peak remains intact, the late peak is absent, leading to the conclusion that it is generated by the innate rather than the adaptive Type-2 response [53].
The pathophysiology of eosinophil-associated tissue and organ damage is complex. Isolated eosinophil accumulation cannot be the only explanation. Various clinical and experimental studies highlight the considerable contribution of pro-inflammatory and tissue-damaging properties of eosinophils to the pathogenesis of many eosinophil-related diseases and hypereosinophilic syndromes [54]. Indeed, eosinophils produce various deleterious products, for example, basic proteins, superoxides, and free radicals radicals [55]. The cardinal involvement of eosinophils in the development of tissue remodelling and fibrosis, in particular through their potent elaboration of remodelling and fibrogenic growth factors, such as IL-3, IL-5, and granulocyte-macrophage colony-stimulating factor, is supported by accumulating evidence [56,57,58]. More specifically, enhanced production of eosinophilopoietic cytokines leads to increased differentiation and uncontrolled proliferation. Subsequently, this magnifies migration, adhesion, and activation of the eosinophils [54,59]. Moreover, the intensive monoclonal proliferation of eosinophils from myeloid progenitor cells related to gene reorganization of oncogenic tyrosine kinase receptors may also play a fundamental role in the pathophysiology of hypereosinophilia and hypereosinophilic syndrome [60]. It is highlighted, however, that eosinophils of infected individuals are ineffective in killing the parasite [61], with experimental studies demonstrating that Toxocara canis shows an enhanced resistance against eosinophils [55].
Visceral larva migrans is the most common syndrome in infected individuals, especially children, with clinical signs including cough, myalgias, or skin manifestations (e.g., pruritus, eczema, panniculitis, and vasculitis.) Migrating larvae causes a host immune response, resulting in local inflammation associated with eosinophilia and increased production of cytokines and specific antibodies [16,49,62].
Furthermore, cardiac symptoms seem to be generated from the combination of direct larva invasion and enhanced immunological/hypersensitivity reactions—particularly associated to hypereosinophilia or immune responses induced by the presence of the parasites in tissues. These reactions can be strengthened during therapy with anthelmintics due to the release of antigens of the dying elminths [63], making steroids a well-considerable complementary therapy.
Regarding neurotoxocarosis, various factors have been suggested to contribute to its pathogenesis, including the abovementioned T helper type 2-driven immune response with subsequent production and release of IL-5 and IgE [19,64]. Moreover, further well-recognized mechanisms refer to the development of vasculitis, secondary to endothelial injury caused by cationic proteins released by eosinophils and IL-6 and the formation of immune complexes [65,66,67,68,69]. Furthermore, similarly to the pathophysiology of cardiac lesions release of helminth antigens—particularly from dying helminths during the therapy [63] —seems to play a cardinal role [66,70]. In addition, the—associated to chronic inflammation—release of major basic protein and eosinophilic cationic protein, and the production of anticardiolipin antibodies significantly contribute to the development of ischaemic lesions observed in this specific patients population [71,72]. Recognition and understanding of the associated pathophysiological mechanisms may improve clinical outcomes and therapeutic implications.
5. Clinical presentations
Historically, the first recorded mention of Toxocara canis dates back to 1782 when the German Parasitologist Paul Christian Friedrich Werner announced the discovery of this parasite as Lumbricus canis [73]. However, the recognition of the clinical importance took place many years after the first description, when Wilder discovered the presence of nematode larvae in removed enucleated eyes from children, who were falsely diagnosed with retinoblastoma [74]. The discovery of the nematode stimulated the identification of the parasite Toxocara canis by Beaver et al. [5]. Indeed, even though migrating ascarid larvae in human tissues were described during the first third of the 20th century [75,76,77], the definition of visceral toxocariasis as a clinical syndrome occurred in 1952 by Beaver et al. when the authors reported three patients suffering from various clinical manifestations including fever, anorexia, hepatomegaly, cough, eosinophilia, and anaemia [5]. Five years later, Toxocara canis was isolated in a liver biopsy of one of the patients, and the disease was defined as visceralis larva migrans syndrome [78]. Currently, human toxocarosis is classified into five clinical forms: the classical visceral larva migrans (VLM), ocular toxocarosis (OT), common toxocarosis (comT), covert toxocarosis (covT), and cerebral toxocarosis or neurotoxocarosis (NT). The possibility of symptomatic disease, its type and severity are associated with the parasite load, the duration of parasite migration, the migratory pathway, and the parasite-induced host immune responses [4,21,31,79,80].
5.1. Visceral larva migrans
Although visceral toxocarosis is a zoonotic disease of childhood affecting primarily children between 2 and 7 years old, it is documented that the proportion of individuals with antibodies to Toxocara species increases with age. Infections in adults have been described worldwide and are mainly caused by ingesting raw meat [45,81,82].
The clinical board of visceral toxocarosis is highly pleomorphic, affecting several organs and systems, including the liver, heart, lung, and skin, with the liver being described as the most affected organ [63,83,84,85,86,87,88,89]. The most common presenting symptoms include a combination of nonspecific manifestations, for example, fever, anorexia, fatigue, abdominal pain, and lymphadenopathy [90,91,92]. Hepatic toxocarosis is characterized by the formation of granulomatous nodules and hepatitis [83,84,85]. Visceral larva migrans hepatic nodules are described as small, oval, or elongated non-spherical lesions with fuzzy margins, and absent or insignificant rim enhancement on contrast-enhanced CT scan. Moreover, they may express cystic characteristics, making early and correct diagnosis difficult [93]. Indeed, it is reported that Toxocarosis-associated hepatic lesions may be misinterpreted as tumours or pyogenic abscesses [93,94].
Cardiac involvement represents an extremely rare, but occasionally fatal manifestation of visceral toxocarosis [63]. The severity of the illness ranges from asymptomatic to severe, and potentially lethal. The reported toxocarosis-associated cardiac presentations include myocarditis, heart failure, endocarditis and endocardial thrombosis, and pericarditis up to cardiac tamponade [63].
Pulmonary toxocarosis occur when the parasites migrate to the lungs and are associated with various symptoms, such as cough, dyspnea, and wheezing [95]. In the majority of the cases, the lung lesions involve more than three lobes with predilection of the subpleural region and the lower lung zone. Morphologically, there are two described radiologic patterns-ground-glass opacities (GGOs), solid nodules, consolidations, and linear opacities [96]. Rarely, toxocarosis may manifest as Loefler’s syndrome, characterized by pulmonary infiltrates and associated with peripheral eosinophilia [52]. Finally, the association between Toxocara species seropositivity and asthma has been widely discussed, with several studies indicating a pathophysiological relationship contributing to the development of asthmatic symptoms [88,97,98,99,100]. A meta-analysis of ten studies with 1530 participants highlighted a significantly higher Toxocara canis infection in asthmatic individuals [101].
Cutaneous larva migrans is endemic in tropical and subtropical regions and is caused by the invasion of Toxocara larvae to the epidermis [102]. However, due to the inability of the larvae to penetrate the skin’s basal membrane, they progress within the epidermis, making the disease self-limiting [103]. The associated skin, intensely pruritic lesions, called creeping eruptions, are typically erythematous, raised and vesicular, linear or serpentine [104]. The characteristic skin manifestations can resemble various other nosological entities such as thrombophlebitis, zoster, phytophotodermatitis, Mondor’s disease, lichen striatus, and other lichenoid eruptions of this type [105]. Other skin manifestations of cutaneous larva migrans include chronic urticaria, chronic pruritus, atopic dermatitis, and miscellaneous eczema in patients with Toxocara antibodies. Notably, isolated cutaneous toxocarosis without systemic symptoms may also occur, making the disease a diagnostic challenge [106,107].
5.2. Ocular larval toxocarosis
Ocular larval migrans (OLT) is a syndrome mainly affecting older children, adolescents, and adults, and shows clinical diversity, partly reflecting the age of the affected individual [32,110,111,112]. Ocular disease is associated to the migration of the parasites through the circulation into the posterior eye segment with subsequent local release of inflammatory responses [95,111]. The most prevalent form of the disease is the development of peripheral granuloma of the eye followed by granuloma of the posterior pole of the eye, commonly extending from the macular landscape to the central retinal periphery and is always accompanied by vitritis [112]. The disease occurs more frequently unilateral; however, bilateral ocular infestation has also been described [111]. The clinical manifestations include disturbed vision, ablatio of the macula, and heterotopia [61,113,114,115]. Children can also develop leukocoria, strabismus, photophobia, eye pain, or eye redness [32]. Moreover, in pediatric patients, OLT may be also manifested as optic nerve neuropathy, fulminant endophthalmitis or papillitis with or without glaucoma, and rarely as diffuse chorioretinitis due to migration of dying larvae [12,112].
5.3. Neurotoxocarosis or cerebral toxocarosis
The invasion of Toxocara canis through the blood-brain barrier into the central nervous system (i.e., brain and spinal cord) may potentially result in one other form of the disease, that is, neurotoxocarosis or cerebral toxocarosis [26]. Autopsy findings of patients with cerebral toxocarosis have demonstrated the presence of parasites in various areas of the central nervous system, for example, the leptomeninges, the cerebellum, the gray and white matter of the brain, and the spinal cord [116,117,118,119,120]. Interestingly, in most patients, the clinical picture and necropsy findings did not correlate, given that neurological manifestations were absent in many cases. The question, therefore, arises as to whether the localization of the parasites into the central nervous system is of clinical significance. However, taking into account that between 1951 and 2015 only 100 cases of NT were reported [27] in combination with the high incidence of non-specific symptoms [121], an issue that remains open is whether neurotoxocarosis is, indeed, a rare disease or a disease that diverts clinical attention.
In contrast to visceral larval migrans, NT is mainly a disease of adulthood, as children younger than 18 years are restrictively affected [27,122]. The clinical spectrum of NT is wide and comprises various clinical entities, for example, meningitis, encephalitis, meningoencephalitis, myelitis, encephalomyelitis, meningomyelitis, and meningoencphalomyelitis. The associated, described clinical symptoms include fever headache, epileptic seizures, weakness, mental confusion, autonomic dysfunction, sensory and motor disturbances, and paraparesis [6,16,27,123,124,125,126,127,128].Moreover, accumulating evidence suggests that Toxocara infections are causally associated with the development of epilepsy in children [4], however, taking into account the high prevalence of epilepsy and the high seroprevalence of Toxocara such an association becomes questionable [20,129].
Blood eosinophilia is not an indispensable finding, presented in approximately 65% of the patients, whereas IgE appears universally increased [121]. Cerebrospinal fluid pleocytosis has been observed in 40 to 64% of the patients [27,121] with eosinophilic predominance. Other cerebrospinal fluid (CSF) findings include increased protein concentration and hypoglycorrhachia [27].
Imaging findings on computer tomography (CT) or magnetic resonance imaging [130] are not pathognomonic and include single or multiple cortical, subcortical, or white matter hyperintense alterations [25,121]. Homogenous or punctate enhancement after administration of contrast agent, multiple, or single ring-enhancing lesions, and focal meningeal contrast enhancement is described in a minority of the published cases [121].
5.4. Covert and common toxocarosis
In 1987, Taylor and co-workers proposed additionally to visceral larva migrans and ocular toxocarosis the presence of another form of toxocarosis, namely covert toxocarosis, affecting children and presenting as a combination of several signs and symptoms including pulmonary manifestations, for example, cough, pneumonia, and wheezing, pharyngitis, limb pains, cervical lymphadenitis, abdominal pain, hepatomegaly, vomiting, headaches, lethargy, and, sleep and behaviour disturbances. Eosinophilia is not an obligatory laboratory abnormality, as it is observed in only 50% of the cases [22,79].
Common toxocarosis, initially observed in French adults, is characterized by a combination of symptoms, including asthenie, cutaneous manifestations, for example, pruritus and rash, dyspnea, and abdominal pain associated with blood eosinophilia, elevated levels of total serum IgE, and enhanced titers of anti-Toxocara antibodies [79].
6. Diagnosis of toxocariasis in humans
The fact that the human intestine is not colonised by adult worms causes diagnostic problems [131]. As a rule, neither Toxocara eggs nor larvae or other parasite stages are excreted in the human stool [132], which makes stool examination unhelpful. Direct detection of larvae in biopsies or punctates is invasive and, in addition, rarely successful and should be only performed when indicated [133]. In addition, it is difficult to distinguish between larvae of Toxocara and other ascarids, especially if the larvae degenerate or if only parts of the larva can be recovered from tissues [134]. In general, the diagnosis of toxocarosis should be based on history, clinical examination, and laboratory findings (leukocytosis and eosinophilia) and can be confirmed by serology [134]. There are several enzyme-linked immunosorbent assays (ELISA) that detect human IgG antibodies to Toxocara excretory antigens/secretory antigens (TES) of third-stage larvae of Toxocara canis. Reliability varies depending on the test and clinical presentation. For example, the sensitivity and specificity of the Toxocara enzyme immunoassay for visceral larva migrans are reported to be between 78% and 92% [10,135]. It should be noted that the amount and type of antibodies cannot distinguish between acute and chronic infection [136]. The results must be interpreted in conjunction with the clinical symptoms and exposure to Toxocara. However, a negative test can exclude VLM, although it should be noted that ocular and neurological toxocarosis can occur even with negative serology. A further complicating factor is the cross-reactivity of the ELISA test with other parasite antigens. In addition, the test can remain positive for years after therapy. In unclear cases, positive ELISA tests can be confirmed by Western blot [137]. The Western blot, which is more expensive and labour-intensive, has a higher sensitivity and specificity when compared to the ELISA [136,138]. Specific detection of total anti-Toxocara IgG antibodies and subclasses (e.g. IgG1, IgG2, IgG3 and IgG4) is also possible [139]. In addition, IgE- and IgM- based on ELISAs can be used to monitor the effectiveness of treatment. Molecular techniques have high analytical specificity and shorter turnaround times than other diagnostic methods. Polymerase chain reaction (PCR)-based assays using a variety of genetic markers (e.g. ITS-1 and ITS-2 regions of rDNA) have now been developed and have enabled the identification and phylogenetic analysis of T. canis, T. cati, and others ascarids [140].
6. Treatment
The therapeutic approach to toxocarosis represents a medical challenge. As abovementioned, it should be differentiated between asymptomatic Toxocara infection in a seropositive patient without symptoms and toxocarosis (e.g., a manifest infection) [26]. Due to the self-limited nature of the disease, it is suggested that treatment should be evaluated in symptomatic patients with severe manifestations [141].
Traditionally, the therapy of human toxocarosis has relied on the use of anthelmintics and anti-inflammatory drugs [136]. Anthelmintics, also known as antihelminthics, are a group of therapeutic regimens and chemical compounds broadly used in the treatment of parasitic infections. The group of anthelmintic drugs include a variety of pharmaceutical agents, for example, benzimidazoles (albendazole, mebendazole, thiabendazole, and triclabendazole), ivermectin, nitazoxanide, praziquantel, pyrantel pamoate and niclosamide [142]. Albendazole has been the cornerstone for the first-line treatment of human toxocarosis for many decades. The preference for albendazole in relation to other antihelmintic agents could be explained based on its relatively safe profile with limited side effects, its wide availability in most countries, and the lower absorption rate of mebendazole outside the gastrointestinal tract [143,144,145,146]. Albendazole is characterized by its high potency against a variety of infections caused by many nematodes and some trematodes, and protozoa [142].
Visceral larval migrans
Albendazole at 400 mg twice a day for five days is the current recommended dose for adults [134]. However, doses of 10 up to 15mg/kg/day taken orally twice daily have also been reported with sufficient therapeutic rate [50,146]. In some patients with VLM disease, a repetition of the treatment may be necessary. Treatment response could be assessed by clinical investigation and the observation of improvement in eosinophilia and serological tests performed over a time period of at least 4 weeks [50]. Even though side effects of the therapy (e.g., constipation, diarrhoea, vomiting, epigastric pain, lethargy, headache, and leucopenia) are usually mild [147], severe drug-associated reactions may also occur. These include hepatotoxicity, commonly induced by higher doses of albendazole, neurologic manifestations, and hematologic abnormalities, such as cytopenias. It should be noted, however, that in predisposed individuals, even therapeutic doses of albendazole may cause liver toxicity, in both adults and children [148,149,150,151,152,153]. Serious, underlying diseases, such as immunosuppression, have been a cause of death under treatment with albendazole, but this is extremely rare [147].
Mebendazole is an alternative treatment option, with low extraintestinal absorption and rapid first-pass metabolism as major disadvantages [79,134,154]. Traditionally, it has been used as second-line therapy [79,134]. Three randomized trials have investigated the efficacy of MBZ in treating common/covert toxocariasis. In these studies, mebendazole was administrated at 25 mg/kg b/w daily for 7 days [145] or 20–25 mg/kg b/w daily for 3 weeks [144]. In a double-blind, placebo-controlled, randomised study investigating the efficacy of mebendazole versus placebo, Magnaval and Charlet used a discontinuous regimen (10-15 mg/kg b/w daily for 3 consecutive days weekly for 6 weeks) and found similar efficacy of mebendazole versus placebo [155]. However, continuous administration at higher doses resulted in a greater cure rate, control of clinical symptoms, and normalization of laboratory abnormalities, particularly blood eosinophilia [144,145]. Similarly to albendazole, mebendazole has mild side effects, for example, skin abscess, granulocytopenia, arthritis, pruritus and, alopecia. However, in high doses, it can cause anaemia and liver damage [154,156,157,158].
Other anthelmintic agents, such as ivermectin, should be avoided in the treatment of human toxocarosis due to their very low cure rate [143,159,160].
While the recommendations for treating other forms of VLM are clear, the evidence regarding cardiac toxocarosis is restricted and limited to case reports. In a systematic review, Kuenzli et al. (2016) analyzed 24 cases of cardiac toxocariasis. Given the potentially lethal nature of the disease, and based on the fact that in cases who received therapy for 2 to 3 weeks a relapse was observed, the authors suggested higher doses of albendazole (15mg/kg or 800-1000mg/day) for a duration of 3 to 4 weeks. Moreover, to avoid severe dose-dependent side effects—specifically, hepatotoxicity and myelosuppression—prolonged therapy (e.g., for more than 3–4 weeks) should be carefully evaluated [63]. Based on the pathophysiology of heart disease representing a combination between direct larval toxicity and damage through activated immunological and hypersensitivity mechanisms, which can be potentially exacerbated after a successful treatment due to the release of antigens of destroyed larvae, the additional administration of corticosteroids reflects a meaningful consideration. However, their therapeutic relevance remains poorly understood and needs further evaluation. The administration of corticosteroids should be evaluated in patients with inflammatory reactions and is associated with a rapid resolution of clinical signs and symptoms. The suggested dose is 1 mg/kg body weight for one week which should be subsequently tapered according to the clinical course and laboratory parameters (e.g., blood eosinophilia) [63].
Ocular toxocarosis
The diagnosis of OT represents a diagnostic challenge, something that may explain the limited existing data regarding the therapy of ocular toxocarosis [146]. Even though some published cases of OT showed a favourable outcome when anthelmintic drugs were combined with corticosteroids, the role of such drugs, for example, albendazole and thiabendazole, remains unclear [146,161,162,163,164]. However, the therapy of OT is based on anthelmintic drugs in combination with corticosteroids or surgical interventions, depending on previous ocular comorbidities and grade of inflammation [165,166,167]. In a retrospective study of OT presenting with uveitis and retinochoroidal granulomas, Barisani-Asenbauer and co-authors (2001) showed the resolve of the inflammatory process and elimination of the granulomas in patients who received 800mg albendazole daily for two weeks combined with corticosteroids [168]. Systemic or topical corticosteroids are used to control intraocular inflammation and related symptoms, but their potency to resolve structural retinal complications is limited [161]. Surgical treatment may be necessary in cases with epiretinal membrane, persistent vitreous opacity, and retinal detachment [95,115,169,170]. Alternative treatments, such as cryotherapy [171,172] and photocoagulation photocoagulation [173,174], may be considerable therapy modalities in specific patients; however, more research towards this direction is necessary.
Neurotoxocarosis
Unfortunately, due to the rarity of cerebral toxocarosis [27], no controlled studies have taken place towards this direction. However, knowledge from other parasitic infections of the central nervous system, for example, neurocysticercosis, indicates that combining albendazole with corticosteroids may represent an effective therapeutic option [175]. The duration of therapy should be at least three weeks. In some cases, repetition may be needed and is facilitated by the efficient penetration of albendazole into the central nervous system (CNS) with no significant toxicity [176,177]. Moreover, pharmacokinetic studies have shown that corticosteroids elevate the concentrations of albendazole in plasma by 50% [178]. The suggested dose of albendazole is 10–15 mg/kg daily, which should be administered until complete resolution of the clinical symptoms and normalization of the MRI, generally over a time period of 21 to 28 [134,176,179,180].
Although there are no recommendations regarding the utility of corticosteroids in the treatment of cerebral toxocarosis, about 90% of the patients receive corticosteroids in combination with antihelminthic medication to eliminate inflammation and control hypersensitivity/immunological reactions associated with the degeneration of larvae following the treatment of NT. Moreover, some patients with myelitis have been treated with corticosteroids-monotherapy. In the vast majority of cases, a clinical and radiological improvement is reported, including in patients with spinal cord lesions managed with corticosteroids alone [121,181].
7. Prevention
Despite that notable progress has been achieved in the prevention, control, and elimination of zoonotic diseases [182], the remarkable expansion of the dog and cats population-and particularly feral and stray animals-contributes to the increased risk of human infection with Toxocara in combination with other factors, for example, climate changes and massive migration [182,183,184]. In the Special Issue regarding a United States (US) perspective on significant pet-related parasitic diseases, Paul and coauthors (2010) refer to synergistic work between various disciplines to maintain human, animal, and environmental health as one health approach [185]. Until today there is an effective way to eradicate environmental contamination with Toxocara [186], toxocarosis, however, is preventable through environmental and ecological modifications. Primary, prevention goals are the reduction of the parasitic load and the risk of zoonotic transmission [187]. A significant contribution in this direction is raising clinicians' awareness regarding the signs and symptoms of the disease as well as the education and behavioural changes of the general population on how to avoid parasitic infections. In addition, the role of veterinarians in preventing zoonotic diseases should be stressed. Deworming pets regularly, particularly new kittens and puppies-even when asymptomatic-represents one of the main preventive measures. Moreover, waste deposits in areas in which children play should be strongly avoided [32]. Furthermore, weight must be given to educating the general population regarding the collection and hygienic disposition of pet faeces, before the eggs become infective [188]. In addition, collective actions regarding stray dogs and cats with deworming at 2-3 weeks of age and two times a year for adults as well as municipal orders to prevent pet dogs from entering parks and playgrounds may also contribute to the elimination of the disease [27]. Modifications in human behavioural characteristics, that is, hand hygiene, careful washing of vegetables, and avoiding raw or undercooked meat, represent further preventive challenges [27].
8. Conclusions
Even though toxocarosis represents one of the most common zoonoses worldwide, its diagnosis remains a challenge due to the unfamiliarity of clinicians with its wide clinical spectrum, its diagnostic approaches, and the available treatment options, especially in non-endemic areas. In this work, we aim to address common questions about the aetiology, epidemiology and transmission, clinical manifestations, laboratory and radiologic findings, diagnosis, treatment and, prevention of infections caused by Toxocara spp. The disease should be suspected in patients presenting with organ involvement, for example, liver, lungs and, heart, accompanied by blood eosinophilia and elevated immunoglobulin E, with or without cutaneous manifestations. Serology assays are considered the most useful method for the detection of toxocarosis in patients with suspected clinical disease. In symptomatic patients, anthelmintic drugs such as albendazole with or without corticosteroids are the recommended treatment of choice. Prevention strategies should involve multiple disciplines and should include educational programs, behavioural and hygienic changes, enhancement of the role of veterinarians, and municipal orders. Further research is needed in order to better understand the pathophysiology and natural history of the disease, especially in less common or less recognized forms, such as common or covert toxocarosis, ocular, and neurotoxocarosis.
Author Contributions
Conceptualization, M.Z. and A.E.; methodology, M.Z.; software, J.KR.; validation, M.Z., A.E. and J.KR.; formal analysis, M.Z.; investigation, M.Z.; resources, M.Z.; data curation, M.Z.; writing—original draft preparation, K.H.; S.N. and M.Z.; writing—review and editing, M.Z. and A.E.; visualization, J.KR.; supervision, M.Z.; project administration, A.E.; funding acquisition, J.KR. All authors have read and agreed to the published version of the manuscript.
Funding
No funding.
Informed Consent Statement
No specific consent was obtained for this study.
Acknowledgments
Figure 1 created with BioRender.com
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gasser, R.B.; et al. Harnessing the Toxocara Genome to Underpin Toxocariasis Research and New Interventions. Adv Parasitol 2016, 91, 87–110. [Google Scholar] [PubMed]
- Mizgajska-Wiktor, H.; Jarosz, W. [A comparison of soil contamination with Toxocara canis and Toxocara cati eggs in rural and urban areas of Wielkopolska district in 2000-2005]. Wiad Parazytol 2007, 53, 219–25. [Google Scholar] [PubMed]
- Gawor, J.; Borecka, A. The contamination of the environment with Toxocara eggs in Mazowieckie voivodship as a risk of toxocarosis in children. Wiad Parazytol 2004, 50, 237–41. [Google Scholar] [PubMed]
- Fan, C.K.; et al. Cerebral Toxocariasis: Silent Progression to Neurodegenerative Disorders? Clin Microbiol Rev 2015, 28, 663–86. [Google Scholar] [CrossRef] [PubMed]
- Beaver, P.C.; et al. Chronic eosinophilia due to visceral larva migrans; report of three cases. Pediatrics 1952, 9, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.K.; Liao, C.W.; Cheng, Y.C. Factors affecting disease manifestation of toxocarosis in humans: genetics and environment. Vet Parasitol 2013, 193, 342–52. [Google Scholar] [CrossRef]
- Overgaauw, P.A.; van Knapen, F. Veterinary and public health aspects of Toxocara spp. Vet Parasitol 2013, 193, 398–403. [Google Scholar] [CrossRef]
- Morimatsu, Y.; et al. A familial case of visceral larva migrans after ingestion of raw chicken livers: appearance of specific antibody in bronchoalveolar lavage fluid of the patients. Am J Trop Med Hyg 2006, 75, 303–6. [Google Scholar] [CrossRef]
- Choi, G.Y.; et al. Acute drug-induced hepatitis caused by albendazole. J Korean Med Sci 2008, 23, 903–5. [Google Scholar] [CrossRef]
- Rubinsky-Elefant, G.; et al. Human toxocariasis: diagnosis, worldwide seroprevalences and clinical expression of the systemic and ocular forms. Ann Trop Med Parasitol 2010, 104, 3–23. [Google Scholar] [CrossRef]
- Schantz, P.M.; Glickman, L.T. Toxocaral visceral larva migrans. N Engl J Med 1978, 298, 436–9. [Google Scholar] [CrossRef] [PubMed]
- Despommier, D. Toxocariasis: clinical aspects, epidemiology, medical ecology, and molecular aspects. Clin Microbiol Rev 2003, 16, 265–72. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, O.; et al. [Meningoencephalitis caused by Toxocara canis]. Ann Med Interne (Paris) 1998, 149, 391–2. [Google Scholar]
- Gueglio, B.; et al. Epidemiologic approach to human toxocariasis in western France. Parasitol Res 1994, 80, 531–6. [Google Scholar] [CrossRef]
- Moiyadi, A.; et al. Visceral larva migrans presenting as multiple intracranial and intraspinal abscesses. Neuropathology 2007, 27, 371–4. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J.; Auer, H. Neurotoxocarosis. Rev Inst Med Trop Sao Paulo 2007, 49, 279–87. [Google Scholar] [CrossRef] [PubMed]
- Kazek, B.; et al. The cerebral form of toxocarosis in a seven-year-old patient. Folia Neuropathol 2006, 44, 72–6. [Google Scholar] [PubMed]
- Poulsen, C.S.; et al. Differential serodiagnostics of Toxocara canis and Toxocara cati--is it possible? Parasite Immunol 2015, 37, 204–7. [Google Scholar] [CrossRef] [PubMed]
- Bachli, H.; Minet, J.C.; Gratzl, O. Cerebral toxocariasis: a possible cause of epileptic seizure in children. Childs Nerv Syst 2004, 20, 468–72. [Google Scholar] [CrossRef]
- Quattrocchi, G.; et al. Toxocariasis and epilepsy: systematic review and meta-analysis. PLoS Negl Trop Dis 2012, 6, e1775. [Google Scholar] [CrossRef]
- Smith, H.; et al. How common is human toxocariasis? Towards standardizing our knowledge. Trends Parasitol 2009, 25, 182–8. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.R.; et al. Clinical features of covert toxocariasis. Scand J Infect Dis 1987, 19, 693–6. [Google Scholar] [CrossRef] [PubMed]
- Noh, Y.; et al. Meningitis by Toxocara canis after ingestion of raw ostrich liver. J Korean Med Sci 2012, 27, 1105–8. [Google Scholar] [CrossRef]
- Radman, N.E.; et al. Human toxocarosis. Its seroprevalence in the city of La Plata. Mem Inst Oswaldo Cruz 2000, 95, 281–5. [Google Scholar] [CrossRef]
- Xinou, E.; et al. CT and MR imaging findings in cerebral toxocaral disease. AJNR Am J Neuroradiol 2003, 24, 714–8. [Google Scholar] [PubMed]
- Auer, H.; Walochnik, J. Toxocariasis and the clinical spectrum. Adv Parasitol 2020, 109, 111–130. [Google Scholar] [CrossRef]
- Deshayes, S.; Bonhomme, J.; de La Blanchardiere, A. Neurotoxocariasis: a systematic literature review. Infection 2016, 44, 565–74. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, C.N. The epidemiology and public health importance of toxocariasis: a zoonosis of global importance. Int J Parasitol 2013, 43, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Pelloux, H.; Faure, O. [Toxocariasis in adults]. Rev Med Interne 2004, 25, 201–6. [Google Scholar] [CrossRef]
- Cianferoni, A.; et al. Visceral larva migrans associated with earthworm ingestion: clinical evolution in an adolescent patient. Pediatrics 2006, 117, e336–9. [Google Scholar] [CrossRef]
- Chen, J.; et al. Advances in molecular identification, taxonomy, genetic variation and diagnosis of Toxocara spp. Infect Genet Evol 2012, 12, 1344–8. [Google Scholar] [CrossRef]
- Woodhall, D.M.; Fiore, A.E. Toxocariasis: A Review for Pediatricians. J Pediatric Infect Dis Soc 2014, 3, 154–9. [Google Scholar] [CrossRef]
- Li, M.W.; et al. The complete mitochondrial genomes for three Toxocara species of human and animal health significance. BMC Genomics 2008, 9, 224. [Google Scholar] [CrossRef]
- Zhu, X.Q.; et al. Genetic blueprint of the zoonotic pathogen Toxocara canis. Nat Commun 2015, 6, 6145. [Google Scholar] [CrossRef] [PubMed]
- Kassai, T.; et al. Standardized nomenclature of animal parasitic diseases (SNOAPAD). Vet Parasitol 1988, 29, 299–326. [Google Scholar] [CrossRef] [PubMed]
- Strube, C.; et al. Seroprevalence of human toxocarosis in Europe: A review and meta-analysis. Adv Parasitol 2020, 109, 375–418. [Google Scholar]
- Petithory, J.C. Can Ascaris suum cause visceral larva migrans? Lancet 1996, 348, 689. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, W.; et al. Optimized DNA-based identification of Toxocara spp. eggs in soil and sand samples. Parasit Vectors 2021, 14, 426. [Google Scholar]
- Ma, G.; et al. Global and regional seroprevalence estimates for human toxocariasis: A call for action. Adv Parasitol 2020, 109, 275–290. [Google Scholar]
- Fakhri, Y.; et al. Toxocara eggs in public places worldwide - A systematic review and meta-analysis. Environ Pollut 2018, 242(Pt B), 1467–1475. [Google Scholar] [CrossRef]
- Azam, D.; et al. Temperature and the development and survival of infective Toxocara canis larvae. Parasitol Res 2012, 110, 649–56. [Google Scholar] [CrossRef] [PubMed]
- Roddie, G.; et al. Contamination of dog hair with eggs of Toxocara canis. Vet Parasitol 2008, 152, 85–93. [Google Scholar] [CrossRef] [PubMed]
- El-Tras, W.F.; Holt, H.R.; Tayel, A.A. Risk of Toxocara canis eggs in stray and domestic dog hair in Egypt. Vet Parasitol 2011, 178, 319–23. [Google Scholar] [CrossRef] [PubMed]
- Salem, G.; Schantz, P. Toxocaral visceral larva migrans after ingestion of raw lamb liver. Clin Infect Dis 1992, 15, 743–4. [Google Scholar] [CrossRef]
- Yoshikawa, M.; et al. A familial case of visceral toxocariasis due to consumption of raw bovine liver. Parasitol Int 2008, 57, 525–9. [Google Scholar] [CrossRef]
- Keegan, J.D.; Holland, C.V. Contamination of the hair of owned dogs with the eggs of Toxocara spp. Vet Parasitol 2010, 173, 161–4. [Google Scholar] [CrossRef] [PubMed]
- Taira, K.; et al. Zoonotic risk of Toxocara canis infection through consumption of pig or poultry viscera. Vet Parasitol 2004, 121, 115–24. [Google Scholar] [CrossRef] [PubMed]
- Dutra, G.F.; et al. Risk of infection by the consumption of liver of chickens inoculated with low doses of Toxocara canis eggs. Vet Parasitol 2014, 203, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.R.; et al. The expanded spectrum of toxocaral disease. Lancet 1988, 1, 692–5. [Google Scholar] [CrossRef]
- Pawlowski, Z. Toxocariasis in humans: clinical expression and treatment dilemma. J Helminthol 2001, 75, 299–305. [Google Scholar] [CrossRef]
- Del Prete, G.F.; et al. Purified protein derivative of Mycobacterium tuberculosis and excretory-secretory antigen(s) of Toxocara canis expand in vitro human T cells with stable and opposite (type 1 T helper or type 2 T helper) profile of cytokine production. J Clin Invest 1991, 88, 346–50. [Google Scholar] [CrossRef]
- Sil, A.; et al. Loeffler's Syndrome and Multifocal Cutaneous Larva Migrans: Case report of an uncommon occurrence and review of the literature. Sultan Qaboos Univ Med J 2023, 23, 104–108. [Google Scholar] [CrossRef]
- Takamoto, M.; et al. Occurrence of interleukin-5 production by CD4- CD8- (double-negative) T cells in lungs of both normal and congenitally athymic nude mice infected with Toxocara canis. Immunology 1995, 85, 285–91. [Google Scholar]
- Ackerman, S.J.; Bochner, B.S. Mechanisms of eosinophilia in the pathogenesis of hypereosinophilic disorders. Immunol Allergy Clin North Am 2007, 27, 357–75. [Google Scholar] [CrossRef] [PubMed]
- Dent, L.A.; et al. Interleukin-5 transgenic mice show enhanced resistance to primary infections with Nippostrongylus brasiliensis but not primary infections with Toxocara canis. Infect Immun 1999, 67, 989–93. [Google Scholar] [CrossRef]
- Kay, A.B. The role of eosinophils in the pathogenesis of asthma. Trends Mol Med 2005, 11, 148–52. [Google Scholar] [CrossRef]
- Kay, A.B.; Phipps, S.; Robinson, D.S. A role for eosinophils in airway remodelling in asthma. Trends Immunol 2004, 25, 477–82. [Google Scholar] [CrossRef]
- Gomes, I.; et al. Eosinophil-fibroblast interactions induce fibroblast IL-6 secretion and extracellular matrix gene expression: implications in fibrogenesis. J Allergy Clin Immunol 2005, 116, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J Allergy Clin Immunol 2012, 130, 607–612. [Google Scholar] [CrossRef]
- van Balkum, M.; et al. Hypereosinophilia: a diagnostic challenge. Neth J Med 2018, 76, 431–436. [Google Scholar] [PubMed]
- Gillespie, S.H. Human toxocariasis. J Appl Bacteriol 1987, 63, 473–9. [Google Scholar] [CrossRef]
- Pivetti-Pezzi, P. Ocular toxocariasis. Int J Med Sci 2009, 6, 129–30. [Google Scholar] [CrossRef]
- Kuenzli, E.; et al. Toxocariasis-associated cardiac diseases--A systematic review of the literature. Acta Trop 2016, 154, 107–20. [Google Scholar] [CrossRef] [PubMed]
- Hoffmeister, B.; et al. Cerebral toxocariasis after consumption of raw duck liver. Am J Trop Med Hyg 2007, 76, 600–2. [Google Scholar] [CrossRef] [PubMed]
- Dousset, V.; Sibon, I.; Menegon, P. [Case no 6. Cerebral vasculitis due to Toxocara canis (or catis) origin]. J Radiol 2003, 84, 89–91. [Google Scholar] [PubMed]
- Lompo, L.D.; et al. [Toxocara canis cerebral vasculitis revealed by iterative strokes]. Rev Neurol (Paris) 2012, 168, 533–7. [Google Scholar] [CrossRef]
- Fellrath, J.M.; Magnaval, J.F. Toxocariasis after slug ingestion characterized by severe neurologic, ocular, and pulmonary involvement. Open Forum Infect Dis 2014, 1, ofu063. [Google Scholar] [CrossRef]
- Hamidou, M.A.; et al. Systemic vasculitis with lymphocytic temporal arteritis and Toxocara canis infection. Arch Intern Med 2002, 162, 1521–4. [Google Scholar] [CrossRef]
- de Boysson, H.; et al. Vasculitis secondary to anti-C1q antibodies induced by Toxocariasis. Infection 2015, 43, 755–8. [Google Scholar] [CrossRef]
- Maiga, Y.; et al. [Presentation of cerebral toxocariasis with mental confusion in an adult: case report and review of the literature]. Bull Soc Pathol Exot 2007, 100, 101–4. [Google Scholar]
- Ardiles, A.; et al. [Toxocariasis in an adult manifested as hypereosinophilic syndrome with predominant neurological involvement Clinical case]. Rev Med Chil 2001, 129, 780–5. [Google Scholar] [PubMed]
- Oujamaa, L.; et al. [Cerebral vasculitis secondary to Toxocara canis and Fasciola hepatica co-infestation]. Rev Neurol (Paris) 2003, 159, 447–50. [Google Scholar] [PubMed]
- Stiles, C.W. The determination of generic types, and a list of roundworm genera with their original and type species, in Bulletin 79, C.W. Stiles, Hassall, A., Editor. 1905, Bureau of Animal Industry, United States Department of Agriculture. p. 1–150.
- Wilder, H.C. Nematode endophthalmitis. Trans Am Acad Ophthalmol Otolaryngol 1950, 55, 99–109. [Google Scholar] [PubMed]
- Chandler, A.C. The helminthic parasites of cats in Calcutta and the relation of cats to human helminthic infections. Indian Journal of Medical Research 1925, 23, 213–227. [Google Scholar]
- Fülleborn, F. Askarisinfektion durch Verzehren eingekapselter Larven und übergelungene intrauterine Askarisinfektion. Arch. Schiffs-u. Tropen-Hyg. 1921, 25, 367–375. [Google Scholar]
- Schwartz, Some parasites of dogs and cats transmissible to human beings and domesticated animals. Vet. Alumni Quart. 1932. Ohio State Univ..
- Nichols, R.L. The etiology of visceral larva migrans I. Diagnostic morphology of infective second-stage Toxocara larvae. J Parasitol 1956, 42, 349–62. [Google Scholar]
- Magnaval, J.F.; et al. Highlights of human toxocariasis. Korean J Parasitol 2001, 39, 1–11. [Google Scholar] [CrossRef]
- Moreira, G.M.; et al. Human toxocariasis: current advances in diagnostics, treatment, and interventions. Trends Parasitol 2014, 30, 456–64. [Google Scholar] [CrossRef]
- Akao, N.; Ohta, N. Toxocariasis in Japan. Parasitol Int 2007, 56, 87–93. [Google Scholar] [CrossRef]
- Raistrick, E.R.; Hart, J.C. Ocular toxocariasis in adults. Br J Ophthalmol 1976, 60, 365–70. [Google Scholar] [CrossRef] [PubMed]
- Stoicescu, R.M.; Mihai, C.M.; Giannakopoulou, A.D. Marked hypereosinophilia in a toddler: a case report. J Med Life 2011, 4, 105–8. [Google Scholar]
- Musso, C.; et al. Prevalence of Toxocara-induced liver granulomas, detected by immunohistochemistry, in a series of autopsies at a Children's Reference Hospital in Vitoria, ES, Brazil. Virchows Arch 2007, 450, 411–7. [Google Scholar] [CrossRef] [PubMed]
- Hartleb, M.; Januszewski, K. Severe hepatic involvement in visceral larva migrans. Eur J Gastroenterol Hepatol 2001, 13, 1245–9. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.; et al. Myocarditis associated with visceral larva migrans due to Toxocara canis. Intern Med 2002, 41, 706–8. [Google Scholar] [CrossRef]
- Enko, K.; et al. Fulminant eosinophilic myocarditis associated with visceral larva migrans caused by Toxocara canis infection. Circ J 2009, 73, 1344–8. [Google Scholar] [CrossRef]
- Aghaei, S.; et al. Toxocara spp. infection and risk of childhood asthma: A systematic review and meta-analysis. Acta Trop 2018, 182, 298–304. [Google Scholar] [CrossRef]
- Humbert, P.; et al. Skin manifestations associated with toxocariasis: a case-control study. Dermatology 2000, 201, 230–4. [Google Scholar] [CrossRef]
- Marx, C.; et al. Toxocariasis of the CNS simulating acute disseminated encephalomyelitis. Neurology 2007, 69, 806–7. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J. Visceral and ocular larva migrans. Semin Neurol 1993, 13, 175–9. [Google Scholar] [CrossRef]
- Keller, M.; Pavia, A.T.; Byington, C.L. Possible intrafamilial transmission of Toxocara causing eosinophilic meningitis in an infant. Pediatr Infect Dis J 2008, 27, 849–50. [Google Scholar] [CrossRef] [PubMed]
- Mukund, A.; et al. Eosinophilic abscesses: a new facet of hepatic visceral larva migrans. Abdom Imaging 2013, 38, 774–7. [Google Scholar] [CrossRef] [PubMed]
- Raffray, L.; Le Bail, B.; Malvy, D. Hepatic visceral larva migrans presenting as a pseudotumor. Clin Gastroenterol Hepatol 2013, 11, e42. [Google Scholar] [CrossRef]
- Woodhall, D.; et al. Ocular toxocariasis: epidemiologic, anatomic, and therapeutic variations based on a survey of ophthalmic subspecialists. Ophthalmology 2012, 119, 1211–7. [Google Scholar] [CrossRef]
- Lee, K.H.; Kim, T.J.; Lee, K.W. Pulmonary Toxocariasis: Initial and Follow-Up CT Findings in 63 Patients. AJR Am J Roentgenol 2015, 204, 1203–11. [Google Scholar] [CrossRef]
- Sharghi, N.; et al. Environmental exposure to Toxocara as a possible risk factor for asthma: a clinic-based case-control study. Clin Infect Dis 2001, 32, E111–6. [Google Scholar] [CrossRef]
- Buijs, J.; Egbers, M.W.; Nijkamp, F.P. Toxocara canis-induced airway eosinophilia and tracheal hyporeactivity in guinea pigs and mice. Eur J Pharmacol 1995, 293, 207–15. [Google Scholar] [CrossRef]
- Pinelli, E.; Aranzamendi, C. Toxocara infection and its association with allergic manifestations. Endocr Metab Immune Disord Drug Targets 2012, 12, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Desowitz, R.S.; Rudoy, R.; Barnwell, J.W. Antibodies to canine helminth parasites in asthmatic and nonasthmatic children. Int Arch Allergy Appl Immunol 1981, 65, 361–6. [Google Scholar] [CrossRef]
- Li, L.; et al. Asthma and toxocariasis. Ann Allergy Asthma Immunol 2014, 113, 187–92. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Barankin, B.; Hon, K.L.E. Cutaneous Larva Migrans. Recent Pat Inflamm Allergy Drug Discov 2017, 11, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Caumes, E. Treatment of cutaneous larva migrans. Clin Infect Dis 2000, 30, 811–4. [Google Scholar] [CrossRef]
- Brenner, M.A.; Patel, M.B. Cutaneous larva migrans: the creeping eruption. Cutis 2003, 72, 111–5. [Google Scholar]
- Del Giudice, P.; et al. Autochthonous Cutaneous Larva Migrans in France and Europe. Acta Derm Venereol 2019, 99, 805–808. [Google Scholar] [CrossRef]
- Gavignet, B.; et al. Cutaneous manifestations of human toxocariasis. J Am Acad Dermatol 2008, 59, 1031–42. [Google Scholar] [CrossRef]
- Bahnea, R.G.; et al. [Cutaneous manifestations on toxocariasis cases hospitalized in the Paediatric Diseases Clinic of Iasi, between 2005-2008]. Rev Med Chir Soc Med Nat Iasi 2009, 113, 428–31. [Google Scholar]
- Rayes, A.A.; et al. Human toxocariasis and pyogenic liver abscess: a possible association. Am J Gastroenterol 2001, 96, 563–6. [Google Scholar] [CrossRef]
- Smith, H.V. Antibody reactivity in human toxocariasis., in Toxocara and Toxocariasis: Clinical, Epidemiological, and Molecular Perspectives, J.W. Lewis, Maizels, R. M., Editor. 1993, Institute of Biology and the British Society for Parasitology: London, UK. p. 91-109.
- Dinning, W.J.; et al. Toxocariasis: a practical approach to management of ocular disease. Eye (Lond) 1988, 2 ( Pt 5), 580–2. [Google Scholar] [CrossRef]
- Stewart, J.M.; Cubillan, L.D.; Cunningham, E.T. Prevalence, clinical features, and causes of vision loss among patients with ocular toxocariasis. Retina 2005, 25, 1005–13. [Google Scholar] [CrossRef] [PubMed]
- Krasny, J.; Sach, J. Forms of Ocular Larval Toxocariasis in Childhood. A Review. Cesk Slov Oftalmol 2022, 2, 1001–1009. [Google Scholar] [PubMed]
- Good, B.; et al. Ocular toxocariasis in schoolchildren. Clin Infect Dis 2004, 39, 173–8. [Google Scholar] [CrossRef]
- Shields, J.A. Ocular toxocariasis. A review. Surv Ophthalmol 1984, 28, 361–81. [Google Scholar] [CrossRef]
- Small, K.W.; et al. Surgical management of retinal traction caused by toxocariasis. Am J Ophthalmol 1989, 108, 10–4. [Google Scholar] [CrossRef]
- Moore, M.T. Human Toxocara canis encephalitis with lead encephalopathy. J Neuropathol Exp Neurol 1962, 21, 201–18. [Google Scholar] [CrossRef]
- Beautyman, W.; et al. Review of a case previously reported as showing an ascarid larva in the brain. J Pathol Bacteriol 1966, 91, 271–3. [Google Scholar] [CrossRef]
- Schochet, S.S. Human Toxocara canis encephalopathy in a case of visceral larva migrans. Neurology 1967, 17, 227–9. [Google Scholar] [CrossRef]
- Hill, I.R.; Denham, D.A.; Scholtz, C.L. Toxocara canis larvae in the brain of a British child. Trans R Soc Trop Med Hyg 1985, 79, 351–4. [Google Scholar] [CrossRef]
- Mikhael, N.Z.; et al. Toxocara canis infestation with encephalitis. Can J Neurol Sci 1974, 1, 114–20. [Google Scholar] [CrossRef]
- Sanchez, S.S.; Garcia, H.H.; Nicoletti, A. Clinical and Magnetic Resonance Imaging Findings of Neurotoxocariasis. Front Neurol 2018, 9, 53. [Google Scholar] [CrossRef]
- Vidal, J.E.; Sztajnbok, J.; Seguro, A.C. Eosinophilic meningoencephalitis due to Toxocara canis: case report and review of the literature. Am J Trop Med Hyg 2003, 69, 341–3. [Google Scholar] [CrossRef]
- Caldera, F.; et al. Toxocara encephalitis presenting with autonomous nervous system involvement. Infection 2013, 41, 691–4. [Google Scholar] [CrossRef]
- Ruttinger, P.; Hadidi, H. MRI in cerebral toxocaral disease. J Neurol Neurosurg Psychiatry 1991, 54, 361–2. [Google Scholar] [CrossRef] [PubMed]
- Singer, O.C.; et al. Severe meningoencephalomyelitis due to CNS-Toxocarosis. J Neurol 2011, 258, 696–8. [Google Scholar] [CrossRef] [PubMed]
- Quinnell, R.J. Genetics of susceptibility to human helminth infection. Int J Parasitol 2003, 33, 1219–31. [Google Scholar] [CrossRef] [PubMed]
- Ota, K.V.; et al. Radiologic surveillance for retinoblastoma metastases unexpectedly showed disseminated toxocariasis in liver, lung, and spinal cord. Can J Ophthalmol 2010, 45, 185–6. [Google Scholar] [CrossRef]
- Lee, J.Y.; et al. Toxocariasis might be an important cause of atopic myelitis in Korea. J Korean Med Sci 2009, 24, 1024–30. [Google Scholar] [CrossRef] [PubMed]
- Moshe, S.L.; et al. Epilepsy: new advances. Lancet 2015, 385, 884–98. [Google Scholar] [CrossRef]
- Sack, U.; et al. Multiplex analysis of cytokines in exhaled breath condensate. Cytometry A 2006, 69, 169–72. [Google Scholar] [CrossRef]
- Wendler, H. [The visceral larva migrans syndrome due to Toxocara canis]. Munch Med Wochenschr 1972, 114, 1634–40. [Google Scholar]
- Kazacos, K.R. Visceral and ocular larva migrans. Semin Vet Med Surg Small Anim 1991, 6, 227–35. [Google Scholar]
- Sumner, D.; Tinsley, E.G. Encephalopathy due to visceral larva migrans. J Neurol Neurosurg Psychiatry 1967, 30, 580–4. [Google Scholar] [CrossRef]
- Chen, J.; et al. Toxocariasis: a silent threat with a progressive public health impact. Infect Dis Poverty 2018, 7, 59. [Google Scholar] [CrossRef]
- Jones, J.L.; et al. Toxoplasma gondii and Toxocara spp. co-infection. Am J Trop Med Hyg 2008, 78, 35–9. [Google Scholar] [CrossRef]
- Fillaux, J.; Magnaval, J.F. Laboratory diagnosis of human toxocariasis. Vet Parasitol 2013, 193, 327–36. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; et al. Application of the western blotting procedure for the immunodiagnosis of human toxocariasis. Parasitol Res 1991, 77, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Roig, J.; et al. Acute eosinophilic pneumonia due to toxocariasis with bronchoalveolar lavage findings. Chest 1992, 102, 294–6. [Google Scholar] [CrossRef] [PubMed]
- Watthanakulpanich, D.; et al. Application of Toxocara canis excretory-secretory antigens and IgG subclass antibodies (IgG1-4) in serodiagnostic assays of human toxocariasis. Acta Trop 2008, 106, 90–5. [Google Scholar] [CrossRef] [PubMed]
- Li, M.W.; et al. PCR tools for the verification of the specific identity of ascaridoid nematodes from dogs and cats. Mol Cell Probes 2007, 21, 349–54. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.-F.; Glickman, L.T.; Dorchies, P. La toxocarose, une zoonose helminthique majeure. Rev Med Vet. 1994, 145, 611–627. [Google Scholar]
- in LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2012: Bethesda (MD).
- Magnaval, J.F. Apparent weak efficacy of ivermectin for treatment of human toxocariasis. Antimicrob Agents Chemother 1998, 42, 2770. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F. Comparative efficacy of diethylcarbamazine and mebendazole for the treatment of human toxocariasis. Parasitology 1995, 110 ( Pt 5), 529–33. [Google Scholar] [CrossRef]
- Magnaval, J.F.; Charlet, J.P. [Comparative efficacy of thiabendazole and mebendazole in the treatment of toxocariasis]. Therapie 1987, 42, 541–4. [Google Scholar] [PubMed]
- Sturchler, D.; et al. Thiabendazole vs. albendazole in treatment of toxocariasis: a clinical trial. Ann Trop Med Parasitol 1989, 83, 473–8. [Google Scholar] [CrossRef] [PubMed]
- Horton, J. Albendazole: a review of anthelmintic efficacy and safety in humans. Parasitology 2000, 121, S113–32. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.L.; Smith, P.G. Albendazole in hydatid disease--hepatocellular toxicity. Trans R Soc Trop Med Hyg 1987, 81, 343–4. [Google Scholar] [CrossRef] [PubMed]
- Ben Fredj, N.; et al. Albendazole-induced associated acute hepatitis and bicytopenia. Scand J Infect Dis 2014, 46, 149–51. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, B.O.; Haznedaroglu, I.C.; Coplu, L. Albendazole-induced amegakaryocytic thrombocytopenic purpura. Ann Pharmacother 1998, 32, 842. [Google Scholar] [CrossRef] [PubMed]
- Polat, C.; et al. Dual treatment of albendazole in hepatic hydatidosis: New therapeutic modality in 52 cases. J Gastroenterol Hepatol 2005, 20, 421–5. [Google Scholar] [CrossRef]
- Bilgic, Y.; et al. Albendazole Induced Recurrent Acute Toxic Hepatitis: A Case Report. Acta Gastroenterol Belg 2017, 80, 309–311. [Google Scholar]
- Marin Zuluaga, J.I.; et al. Albendazole-induced granulomatous hepatitis: a case report. J Med Case Rep 2013, 7, 201. [Google Scholar] [CrossRef]
- Dayan, A.D. Albendazole, mebendazole and praziquantel. Review of non-clinical toxicity and pharmacokinetics. Acta Trop 2003, 86, 141–59. [Google Scholar] [CrossRef] [PubMed]
- Magnaval, J.F.; Charlet, J.P. Etude double aveugle de l’efficacité du mébendazole dans le traitement de la toxocarose humaine. Therapie 1992, 47, 145–148. [Google Scholar] [PubMed]
- Braithwaite, P.A.; Thomas, R.J.; Thompson, R.C. Hydatid disease: the alveolar variety in Australia. A case report with comment on the toxicity of mebendazole. Aust N Z J Surg 1985, 55, 519–23. [Google Scholar] [PubMed]
- Miskovitz, P.F.; Javitt, N.B. Leukopenia associated with mebendazole therapy of hydatid disease. Am J Trop Med Hyg 1980, 29, 1356–8. [Google Scholar] [CrossRef] [PubMed]
- Puente, S.; et al. Imported Mansonella perstans infection in Spain. Infect Dis Poverty 2020, 9, 105. [Google Scholar] [CrossRef] [PubMed]
- Boussinesq, M.; Prod, J.; Chippaux, J.P. Onchocerca volvulus: striking decrease in transmission in the Vina valley (Cameroon) after eight annual large scale ivermectin treatments. Trans R Soc Trop Med Hyg 1997, 91, 82–6. [Google Scholar] [CrossRef]
- Marti, H.; et al. A comparative trial of a single-dose ivermectin versus three days of albendazole for treatment of Strongyloides stercoralis and other soil-transmitted helminth infections in children. Am J Trop Med Hyg 1996, 55, 477–81. [Google Scholar] [CrossRef]
- Ahn, S.J.; Ryoo, N.K.; Woo, S.J. Ocular toxocariasis: clinical features, diagnosis, treatment, and prevention. Asia Pac Allergy 2014, 4, 134–41. [Google Scholar] [CrossRef]
- Inagaki, K.; et al. Case Report: Ocular Toxocariasis: A Report of Three Cases from the Mississippi Delta. Am J Trop Med Hyg 2019, 100, 1223–1226. [Google Scholar] [CrossRef]
- Rubin, M.L.; et al. An intraretinal nematode (a case report). Trans Am Acad Ophthalmol Otolaryngol 1968, 72, 855–66. [Google Scholar]
- Seong, S.; et al. A case of ocular toxocariasis successfully treated with albendazole and triamcinolon. Korean J Parasitol 2014, 52, 537–40. [Google Scholar] [CrossRef]
- Hrˇckova, G. Novel approaches to immunoprophylaxis in toxocariasis, in Toxocara: the enigmatic parasite, C.V. Holland, Smith, H.V., Editor. 2006, CAB International: Oxfordshire. p. 174–194.
- Martinez-Pulgarin, D.F.; et al. Ocular toxocariasis: new diagnostic and therapeutic perspectives. Recent Pat Antiinfect Drug Discov 2015, 10, 35–41. [Google Scholar] [CrossRef]
- Frazier, M.; Anderson, M.L.; Sophocleous, S. Treatment of ocular toxocariasis with albendezole: a case report. Optometry 2009, 80, 175–80. [Google Scholar] [CrossRef]
- Barisani-Asenbauer, T.; et al. Treatment of ocular toxocariasis with albendazole. J Ocul Pharmacol Ther 2001, 17, 287–94. [Google Scholar] [CrossRef] [PubMed]
- Giuliari, G.P.; Ramirez, G.; Cortez, R.T. Surgical treatment of ocular toxocariasis: anatomic and functional results in 45 patients. Eur J Ophthalmol 2011, 21, 490–4. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; et al. Clinical features and course of ocular toxocariasis in adults. PLoS Negl Trop Dis 2014, 8, e2938. [Google Scholar] [CrossRef]
- el Matri, L.; et al. [Toxocara canis in apparently bilateral ocular site]. J Fr Ophtalmol 1990, 13, 303–8. [Google Scholar]
- Choi, K.D.; et al. Toxocara optic neuropathy: clinical features and ocular findings. Int J Ophthalmol 2018, 11, 520–523. [Google Scholar] [PubMed]
- Gass, J.D.; Braunstein, R.A. Further observations concerning the diffuse unilateral subacute neuroretinitis syndrome. Arch Ophthalmol 1983, 101, 1689–97. [Google Scholar] [CrossRef]
- Zygulska-Machowa, H.; Ziobrowski, S. [A case of ocular toxocariasis treated by xenon photocoagulation]. Klin Oczna 1987, 89, 213–4. [Google Scholar]
- Garcia, H.H. Neurocysticercosis. Neurol Clin 2018, 36, 851–864. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, O.; et al. Eosinophilic meningomyelitis in toxocariasis: case report and review of the literature. Clin Neurol Neurosurg 2005, 107, 432–8. [Google Scholar] [CrossRef] [PubMed]
- Graeff-Teixeira, C.; da Silva, A.C.; Yoshimura, K. Update on eosinophilic meningoencephalitis and its clinical relevance. Clin Microbiol Rev 2009, 22, 322–48, Table of Contents. [Google Scholar] [CrossRef] [PubMed]
- Sotelo, J.; Jung, H. Pharmacokinetic optimisation of the treatment of neurocysticercosis. Clin Pharmacokinet 1998, 34, 503–15. [Google Scholar] [CrossRef] [PubMed]
- Hombu, A.; et al. Treatment of larva migrans syndrome with long-term administration of albendazole. J Microbiol Immunol Infect 2019, 52, 100–105. [Google Scholar] [CrossRef]
- Jabbour, R.; Atweh, L.A.; Atweh, S. Migration of Toxocara canis into the spinal cord in poorly treated patients. Neurology 2015, 84. [Google Scholar] [CrossRef]
- Goffette, S.; et al. Eosinophilic pleocytosis and myelitis related to Toxocara canis infection. Eur J Neurol 2000, 7, 703–6. [Google Scholar] [CrossRef]
- Wang, J.L.; et al. Major parasitic diseases of poverty in mainland China: perspectives for better control. Infect Dis Poverty 2016, 5, 67. [Google Scholar] [CrossRef]
- Matsangos, M.; et al. Health Status of Afghan Refugees in Europe: Policy and Practice Implications for an Optimised Healthcare. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Deplazes, P.; et al. Role of pet dogs and cats in the transmission of helminthic zoonoses in Europe, with a focus on echinococcosis and toxocarosis. Vet Parasitol 2011, 182, 41–53. [Google Scholar] [CrossRef]
- Paul, M.; King, L.; Carlin, E.P. Zoonoses of people and their pets: a US perspective on significant pet-associated parasitic diseases. Trends Parasitol 2010, 26, 153–4. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.C. Ascarid infections of cats and dogs. Vet Clin North Am Small Anim Pract 1987, 17, 1307–39. [Google Scholar] [CrossRef]
- Chomel, B.B. Control and prevention of emerging parasitic zoonoses. Int J Parasitol 2008, 38, 1211–7. [Google Scholar] [CrossRef] [PubMed]
- Action to reduce human health hazards arising from animals. WHO Chron 1978, 32, 307–10.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



