
Submitted:
06 June 2023
Posted:
06 June 2023
You are already at the latest version
Abstract
This review article is aimed at exploring the possibility of developing an integrated approach in the management of the different needs of endometrial cancer (EC) patients seeking to become pregnant. Life preservation of the woman, health preservation of the baby, a precocious and – as much as possible – minimally invasive characterization of the health and fertility parameters of the patient, together with the concerns regarding the obstetric, neonatal, and adult health risks of the children conceived via assisted reproduction techniques (ART) are all essential aspects of the problem to be taken into consideration, yet the possibility to harmonize such needs through a concerted integrated approach is still highly challenging. This article aims to illustrate the main features of EC and how it affects the normal physiology of pre-menopausal women. Then, we focus on the prospect for a miR-based, molecular evaluation of patient health status, including both EC early diagnosis and staging and, similarly, the receptivity of the woman, discussing the possible evaluation of both aspects using a single specific panel of circulating miR in the patient, thus allowing a relatively fast, non-invasive way to perform such testing with a significantly reduced margin of error. Finally, the ethical and legal/regulatory complexities arising from such innovative techniques require not only a risk-benefit analysis; respect for patient autonomy and equitable health care access allocation are fundamental issues as well.
Keywords:
Endometrial cancer (EC)
; assisted reproduction techniques (ART)
; miR-based
; molecular evaluation
; ethical and legal/regulatory implications
1. Introduction
Assisted reproductive technology (ART) refers to a number of techniques allowing women to achieve pregnancy in a non (fully) natural way and include in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), gamete intrafallopian transfer (GIFT), and preimplantation genetic diagnosis (PGD) [1]. ART is a viable option not only in couples with a fertility impairment, but also in women diagnosed with cancer set to undergo chemotherapy; such therapeutical approach however not only affects fertility by impairing the viability of gametes but could also alter their genome introducing deleterious mutations in the embryo; as such, ART is a choice for EC patients as well to minimize those problems [2].
Endometrial cancer (EC) affects the lining of the uterus and is usually diagnosed in postmenopausal women, but about 5% of cases occur in women under 40, and approximately 20% of cases are diagnosed before menopause [3]. The most common type of endometrial cancer in premenopausal women is the estrogen-sensitive adenocarcinoma (type I carcinoma), which has a better prognosis than the more aggressive type II carcinoma. Several genes have been recognized in the last years playing a central role in EC development and growth [4,5] and, more recently, the epigenetics of EC has started to be unveiled. Micro RNA (miRNA or miR) are short molecules of non-coding endogenous RNA that function as post-transcriptional regulators of gene expression [6]. Also in EC, miR can play a role in the development and progression of cancer by modulating the expression of oncogenes and tumor suppressor genes. For example, some miRNAs have been reported to regulate the expression of PTEN, a tumor suppressor gene that is frequently mutated or deleted in endometrial cancer (see below). In addition, miR can also be associated with endometrial cancer risk factors, such as insulin resistance and hyperinsulinemia, which can trigger cell proliferation and angiogenesis [7]. In this perspective, it is crucial to understand the molecular bases of EC and how it influences women’s fertility; of similar importance is the evaluation of who, how and when can face oocyte preservation for ART application once EC is defeated.
Evaluation of female fertility is an important step for women who want to undergo ART or preserve their fertility after being diagnosed with endometrial cancer. A pelvic examination should be performed to assess the uterus and adnexa for masses or other abnormalities. The gold standard method for diagnosing endometrial cancer is hysteroscopy and endometrial biopsy, which have a high sensitivity and specificity. Other imaging techniques, such as ultrasound, magnetic resonance imaging (MRI), or computed tomography (CT), can be used to evaluate the extent of the disease and plan the treatment [8].
This review article is aimed at examining in depth all these aspects of the problem. We will discuss the etiopathogenesis of EC both from a clinical and a molecular point of view, with a special focus of epigenetic causes, and the use of circulating miR as diagnostic biomarkers. We will report the state-of-the-art in fertility evaluation by means of circulating miR as well, comparing the two set of data (circulating miR in EC and for fertility assessment) and highlight how these two sets largely do not overlap, providing the possibility to establish at the same time and with a minimally invasive test (a blood sample) both the health status of the patient and her possibility to undergo ART. Finally, we will provide an overview of the main ethical and legal aspects of the procreation in EC (and, more widely, in oncologic) patients.
In order to do that, the authors have set out to elucidate in a succinct and yet comprehensive fashion the underlying factors, determinants and dynamics at the root of EC, its clinical implications in terms of therapeutics and diagnostics, the prospects for fertility preservation in younger patients the prospect for a miR-based, molecular evaluation of patient health status, including both EC early diagnosis and staging and, similarly, the patient’s receptivity; finally, the ethical and legal/regulatory complexities have been weighed. For each one of the above-listed fundamental elements, 125 sources have been drawn upon, by using the search strings “endometrial cancer”, “fertility preservation”, “RNA-based molecular classification/evaluation”, “miRNA cancer diagnosis” through scientific databases PubMed/MedLine, PubMed Central, Scopus, ResearchGate, Web of Science. Only articles accounting for EC, infertility/fertility preservation, RNA-based diagnostic and therapeutic approaches and ethics peculiarities of such innovative techniques have been considered for the fundamental purpose of this review article.
2. Etiology and Pathogenesis of EC in Fertile Women: Clinical and Endocrinological Characteristics of EC
Endometrial cancer EC has long been known as one of the most widespread gynecologic cancer worldwide; it is also the most common neoplastic condition affecting the female genital tract in developed countries. The condition is localized to the uterus in most patients (reportedly as many as 67%) [9].
While uterine corpus cancer is currently the most common gynecologic malignancy, endometrial carcinomas constitute the majority of such diagnoses; sarcoma accounts for less than 10% of uterine corpus cancers. As many as 83% of uterine corpus cancers are endometrioid carcinomas. In addition, 4% to 6% of endometrial carcinomas consist of serous and papillary serous carcinomas, while clear cell carcinomas account for 1% to 2%. For a thorough analysis and better management and prevention of such conditions, it is worth drawing a distinction between type 1 endometrioid, type 2 serous endometrial carcinomas and other highly aggressive non-endometrioid carcinoma histotypes [10,11]
Abnormal uterine bleeding or postmenopausal bleeding constitute typical EC presentations. Diagnostic evaluation should be made available to any patient with EC risk factors, and that should include the assessment of clinical history, imaging, and endometrial sampling. Standard EC therapeutic pathways may entail hysterectomy,bilateral salpingo- oophorectomy,and surgical staging. Hysterectomy is instrumental in accurately assessing EC prognostic factors, such as stage, grade, myometrial invasion, lymphovascular space invasion, and lymph node status [12,13,14]
ECs has been found to begin as preinvasive intraepithelial lesions transitioning into full-blown invasive cancers affecting endometrial stroma; progressive penetration into the myometrium occurs through the lymphatic capillaries spreading cancerous cells into regional lymph nodes; the metastasizing process unfolds via vascular channels. Uterine cervix and stroma are likely affected by tumor progression through lymphatic channels, even if surface spread has been observed to take place from ECs manifesting in the lower uterine segment (LUS). LUS involvement in endometrial carcinoma has often been reported to result in lower survival rates and higher recurrence rates [15].
High levels of free-estrogens leading to endometrial hyperplasia have been linked to estrogen-secreting, ovarian tumors and polycystic ovaries (PCO); both conditions can adversely affect regular ovulation and menstruation. While anovulation obviously results in infertility, nulliparity is linked to a higher EC risk, even following adjustment for infertility [16].
Potential precursors of type I EC (which has been linked to a tumoral environment of excess estrogen) have been found to be atypical endometrial hyperplasia or endometrial intraepithelial neoplasia (EIN). Such dynamics often manifest at an early stage, with rather favorable outcomes. Serous, clear cell, mixed cell and undifferentiated histologies are all elements reportedly associated with type II ECs, which are estrogen independent and manifest at an already advanced stage with unfavorable prognosis [17]. Validation of prognostic elements for the establishment of genes or biomolecular factors is instrumental in terms of prognostic of outcomes [18].
Such clinical dynamics however entail medical as well as ethical and social concerns: fertility- sparing treatment (FST) can in fact forgo more radical care procedures by prioritizing the patient’s reproductive capabilities. Assisted reproductive technologies (ART) are often required to that end, which means that EC treatment in patients of reproductive age is uniquely challenging, due to the need to strike a balance between “competing interests” of cancer care and the determination of patients to maintain their reproductive potential. Early menarche and late menopause, with the higher levels of lifetime exposure to endogenous estrogens, have been found to lead to higher EC risks.
2.1. Challenges Arising from Fertility-Sparing Approaches in EC Patients
EC type and fundamental traits ought to be thoroughly assessed in order to choose the therapeutic pathway which best suits each patient, particularly when weighing a conservative management opportunity.
Fertility-sparing procedures therefore need to be weighed and counseled for when making treatment decisions. That is even more true in light of the potentially harmful psychological dynamics that may be triggered by the loss of fertility following aggressive therapeutic approaches. [19,20]
EC risk of extrauterine spread is an essential aspect to evaluate when assessing patient eligibility for fertility-sparing procedures. Only for patients who have interest to preserve their fertility and plan to conceive as soon as possible after remission should fertility-sparing be considered, in the absence of contraindication and favorable histopathological cancer make-up [21].
The fertility-sparing decision-making process needs to be weighed against the various EC risk factors, such asobesity and polycystic ovary syndrome; such factors are linked to infertility as well, hence any ART consideration may well be influenced by them. G1 and EEC are the malignancies for which fertility-sparing treatment is most often chosen. EC type II, on the other hand, often makes patients ineligible for conservative treatment, due to its high level of invasiveness and poor differentiation. Young women with G1, no myometrium and/or adnexal invasion, and without lymphvascular space involvement, are therefore deemed the best candidates for fertility preservation approaches [22,23]).
When outlining any such pathway, it is worth taking into account updated guidelines by scientific societies such as ESGO-ESHRE-ESGE, which issued specific, evidence-based guidance for fertility-sparing treatment of EC patients, by focusing on the fundamental traits of fertility-sparing treatment. Particularly relevant is the recommendation that EC patients undergoing fertility-sparing procedures be counseled and cared for by a multidisciplinary team relying on oncologists and fertility specialists [24].
Progestin therapies (e.g., medroxyprogesterone acetate, MPA), megestrol acetate (MA), and progesterone-releasing intrauterine device (IUD) are the most widespread and validated EC hormonal treatment (HT) options and constitute the bedrock of the conservative fertility-sparing armamentarium. Medroxyprogesterone (MPA) at 250-600mg daily and megestrol acetate (MA) at 160-480 mg daily are the most widely used regimens, and can rely on similar potency levels [25]. A 2016 meta-analysis by Qin et al., accounting for 25 sources comprising 445 women with early stage EC treated with an oral progestin, has found an 82.4% regression rate, a 25% relapse rate and a 28.8% pregnancy rate; such findings point to the high degree of safety of oral progestins for early stage EC patients who wish to have their fertility preserved [26].
Recent data have also pointed to the novel levonorgestrel intrauterine device (LNG-IUD) as a solid fertility preservation option as well [27]. Such a device in fact elicits a local hormonal surge in higher amounts, and has efficacy rates similar to oral formulation, although conclusive comparative studies are not yet available [28].
3. Discussion
Although gynecological cancers are most frequently diagnosed in post-menopausal patients, relatively substantial numbers of younger women of reproductive age are also affected. The importance of thorough counseling in such patients cannot be overstated, including a comprehensive discussion of long-term consequences on fertility of the various treatment options and fertility preservation as a viable prospect. EC diagnosis in reproductive age points to the risk of an hereditary condition hence counseling must address the genetic cancer risk evaluation in order to investigate possible genetic predisposition to cancer. Such broad-ranging principles notwithstanding, fertility-sparing pathways needs to be individually tailored, considering the high level of heterogeneity of gynecological cancers.
The chief surgical option for EC is hysterectomy, whereas fertility-sparing management in patients with EC or complex atypical hyperplasia is not deemed standard approach. Eligibility requirements are age under 40, complex atypical hyperplasia or grade 1 endometrial cancer limited to the endometrium. Accurate pretreatment staging is therefore essential and non-negotiable [29]
Gallos et al., in a meta-analysis involving 408 women with early stage EC who underwent fertility sparing treatment, found a 28% live birth rate, with patients undergoing ART achieving a 39.4% live birth rate, as opposed to 14.9% in the spontaneous conception group [30].
The preservation of fertility and procreative capabilities are ever-more relevant elements in terms of life quality after EC. Patients with no male partner or unwilling to freeze and store embryos can still preserve their oocytes. Such techniques, particularly those relying on freezing by vitrification, lowers the risk of incurring multiple pregnancies or ovarian hyperstimulation syndrome (OHSS). Compared to transfer from fresh embryo, no significant differences have been reported in terms of pregnancy rate per cycle and the clinical pregnancy rate per cycle [31].
The decision to store frozen oocytes, as opposed to embryos, can avoid or at least allay ethical and legal challenges often arising from cryopreseved embryos and their controversial status. Major improvements in overall outcomes of oocyte cryopreservation have been achieved through more effective cryopreservation techniques such as vitrification rather than the slow-freeze protocol, mostly thanks to the reduction of cellular damage arising from ice crystal formation [32]. Moreover, it is worth remarking that most endometrial cancers are estrogen-dependent, which questions the safety of pregnancy and the risk of cancer recurrence related to it.
The intersection of gonadotoxic therapy and reproduction raises ethical issues for both cancer and fertility specialists, including issues of experimental vs established therapies, the ability of minors to give consent, the welfare of expected children, and posthumous reproduction [33,34,35].
The newly-found possibility to theoretically focus both on the health status of the patient, including the definition of EC staging, and her fertility with a fast and minimally invasive approach, as described above, further contributes to enabling such patients to achieve motherhood, through a more effective management of an otherwise extremely adverse scenario.
3.1. Role of Circulating miRNA in EC: miR, ceRNET and Cancer Biology
Micro-RNAs (miRNA or miR) are a class of single stranded, non-coding RNAs (ncRNA) characterized by their short length – 20-25 nucleotides on average – and are part of the group of molecules collectively called ‘short non-coding RNAs’ (sncRNA). Their action is modulating gene expression by targeting messenger RNAs (mRNA) through sequence homology. Notably, the match between miR and its target is not always perfect, thus allowing the former to pair with multiple mRNA; this makes the discovery of their targets challenging and the identification of their function puzzling [36]. The binding occurs in most cases at the 3′UTR end of the mRNA, and the final effect is typically to inhibit mRNA function, either by impairing its translation or by promoting its degradation [37]. Consequently, many miR can be functionally considered gene expression silencers. It is estimated that more than 2,500 miR are encoded in the human genome, regulating over 60% of human genes [38], and several metabolic pathways are controlled by miR action, including those involved in cell cycle control. In fact, the central role of miR is now widely recognized in many cancers [39], including EC [40,41,42], where they control pivotal steps of tumor biology such as proliferation, apoptosis, and invasion. Interestingly, miR can exert either an oncogenic or an oncosuppressive action during cell cycle control, depending on several factors including (i) the role of the gene encoding the target mRNA, (ii) their own regulation, since miR as well can be up- or down-regulated in different patients; (iii) their expression in different tissues. In this perspective, EC is not an exception: recent systematic reviews highlighted the role of the dysregulation of more than 100 miR in the etiopathogenesis of EC [43,44]. Therefore, miR are also considered both valuable markers and very promising targets in cancer therapy [45]. However, the mechanism of action of miR on mRNA is neither simple nor straightforward. First, as said, because multiple miR can target the same mRNA and the same miR can target multiple mRNA. Second, because another heterogeneous class of non-coding RNA is involved as well in this control, called long non-coding RNAs (lncRNA). These molecules are longer ncRNA (200 nt or more), heterogeneous in several aspects (length, shape, cytological localization, genome localization) and able to bind to several miR at the same time, a phenomenon called ‘miR sponging’ [46]. In the last years hundreds of papers had been published describing single components of these control pathways, the sum of one lncRNA, one sncRNA and one target mRNA interacting with each other being called “axis”. In these axes, mRNA and lncRNA compete for miR binding, and multiple, interconnected axes create what it is now commonly known as a ceRNET (competing endogenous RNA network). In this network, nodes are ceRNAs (competing endogenous RNAs, i.e., lncRNA and mRNA), while miR represent their connections [47,48]. This complex epigenetic gene expression control allows a very fine tuning of cell cycle regulation; despite this organization should provide a certain redundancy able to confer robustness to mutation, nonetheless it also allows a single alteration to hit multiple metabolic pathways at the same time, hence the importance to identify and characterize ceRNET. These networks have been partially described in neurodegenerative diseases [49,50] and in a few cancers such as lung adenocarcinoma [51], intrahepatic cholangiocellular carcinoma [52], hepatocellular carcinoma [53], glioma [54], thyroid cancer [55], and breast cancer [56,57] while for most cancers only single axes had been described so far. Recently, a complex ceRNET involving the lncRNA encoded inside the X-linked chromosome inactivation center and involved in multiple organ cancerogenesis has been described [58].
Literature reports several ceRNA axes in EC [59] and a long list of simpler interactions has been described as well, describing only two components of each putative axis. Recently, ceRNET started to be described in EC as well. In 2019 Zhao and collaborators analyzed original data of EC RNA transcripts from The Cancer Genome Atlas (TCGA) database in search of prognostic biomarkers in endometrial carcinoma [60]. This study allowed the identification of 62 lncRNA, 26 miR, and 70 mRNA deregulated in EC. Of them, 10 lncRNA, 19 mRNA, and 4 miR were closely related to the survival of EC patients (P<0.05). In 2022 Cai and coworkers analyzed both the TCGA and the Clinical Proteomic Tumor Analysis Consortium (CPTAC) databases to reconstruct a lncRNA-mediated ceRNA network for uterine corpus endometrial carcinoma [61]. This work allowed identifying tens of these axes and the identification of six of them with a high prognostic value. In the same year, Song and collaborators again took advantage of the TGCA database to reconstruct a ceRNET including 5 deregulated lncRNA, 7 deregulated miR and 90 deregulated mRNA [62]. In Figure 1 we report two simplified examples of ceRNET in EC.
3.2. Using Circulating miR for EC Diagnosis
According to recent advances in its histopathological and molecular characterization, EC can be classified in at least four different classes [71,72]; in addition, adequate biomarkers may be also used as valuable prognostic tools [73] and miR might account for promising tools during patients’ evaluation, as recently noted [74]. The accurate characterization of each patient is fundamental for their management, especially in those cases in which it is desirable to preserve fertility [75,76]; in this perspective, the use of adequate biomarkers and their early detection, possibly with a fast and minimally invasive approach, is a central issue. It has also been shown that it is possible to characterize EC according to the expression of different miR – and, consequently, their ceRNET-related characteristics [40,41,42]. Many studies have detected extracellular/circulating miR in biological fluids, such as plasma and serum, cerebrospinal fluid, saliva, breast milk, urine, tears, colostrum, peritoneal fluid, bronchial lavage, seminal fluid, and ovarian follicular fluid (see [77] and references therein). In these fluids miR can be either detected inside extracellular vesicles (exosomes, microvesicles, apoptotic bodies) or floating in association with proteins such as Ago2. Interestingly, miR stability in body fluids is far higher than inside cells [78,79]. The reason why miR – which are generated inside cells – are present in body fluids is still an open question. Two main hypotheses are under investigation: they are merely a byproduct of extensive cell death (mainly apoptosis and necrosis) connected to tumor biology (passive mechanism), or they fulfil long-distance, cell-cell communication (active mechanism).
The identification of deregulated miR in EC patients is running and the discovery of new ceRNA axes is relatively frequent. A meta-analysis published in 2019 by Delangle and co-workers [80] identified the deregulation in the expression levels of 261 miRs in EC, including 133 onco-miRs, 110 miR onco-suppressors, and 18 miRs with discordant functions. However, the possibility to use circulating miR to achieve this characterization is still at its beginning and has been only poorly explored in EC. In 2022 Bloomfield and collaborators performed a systematic review analyzing literature in search of circulating miR in serum and plasma of EC patients [81]. Their analysis allowed to identify 33 significantly deregulated miR, 27 showing up- and 4 down-regulation, while the remaining 2 (miR-21 and miR-204) showed contradictory expression values depending on the study considered (Table 1). These works show that adequate combinations of miR expression values may be used as prognostic markers, able to help in defining EC histological type and grade, tumor size, FIGO stage, lymph node involvement, and survival rate, thus demonstrating the miR role in decision making for patients’ management [80]. Interestingly, a simple one-to-one comparison of the two sets of data reported above indicates that almost half (16/33) of the described circulating miR are also deregulated in EC specimen. As shown in Table 1, while in most cases the up- or down-regulation match in both reports, in a few cases (miR-9, miR-99a, miR-100 and miR-199b) they are discordant. Considering the two hypotheses described above, concordant regulation might indeed be thought as a passive mechanism due to cell death and consequent release of cellular debris in the blood stream, but the discordant results might allow to think of an active mechanism which, if further supported by data, might shed light on some new and interesting features of miR biology in EC. In any case, the relatively high level of match (ca. 50%) between the miR identified in the two works strongly support the use of circulating miR in the characterization of EC patients, allowing a minimally invasive diagnostic approach, as indeed also shown in a recent meta-analysis based on 21 studies [82].
Eismann and coworkers in 2017 showed that the circulating miR excreted in vitro by EC cell lines are also dependent on exogenous environmental stress, such as hypoxia and acidosis [83]. In their work, the authors showed that hypoxia caused the downregulation of miR-15a, miR-20a, miR-20b and miR-128-1 in Ishikawa cells (type I EC) and upregulation of miR-21 in EFE-184 cells (type I EC), while acidosis caused the upregulation of the oncogenic miR-125b in AN3-CA cell (type II EC), while in Ishikawa cells (type I EC) miR with tumor suppressive function were found altered in divergent directions, either up- (let-7a) and down- (miR-22) regulated. These data show that, at least in type I EC cells, hypoxia promotes the downregulation of secreted miR with tumor suppressive and anti-angiogenetic function and the contemporary upregulation of secreted miRNAs with tumor and angiogenesis promoting function. Instead, acidosis caused upregulation of tumor promoting miR in type II EC. Collectively, these data suggest that the miR profile not only might be used to identify EC in patients, but also to evaluate the status of the tumor microenvironment and its changes over time.
3.3. Profiling the miR Transcriptome for the Evaluation of Endometrial Receptivity
To date, only a minor proportion of studies analyzed the expression levels of miR in healthy women to evaluate their potential receptivity.
In 2017, Altmae and collaborators performed a meta-analysis using as a ‘bait’ a meta-signature of endometrial receptivity involving 57 mRNA genes as putative receptivity markers [84]. Searching for putative regulators and using the robust rank aggregation (RRA) method [85], they identified 19 miR with 11 corresponding up-regulated meta-signature genes. Of them, three (miR-30c-1, miR-130b and miR-449c-5p) are also linked to human EC [86,87,88]. Drissennek and collaborators performed a retrospective analysis of the miRNome of endometrium samples collected during the implantation window and associated with the receptivity status and the pregnancy outcome (implantation failure, early embryo miscarriage, and live birth at term) in patients with a positive or negative b-hCG [89]. They identified 11 miR associated with the endometrial receptivity status (9 downregulated); of them, miR-455-3p being also a putative tumor suppressor. They also identified the overexpression of miR-152-3p and miR-155-5p in receptive endometrium associated with implantation failure, both involved also in the etiopathogenesis of several types of cancer. Unfortunately, additional validation tests did not allow to have more reliable results on other miR identified during the study, including circulating miR. Additional studies identified more miR involved in these processes, such as miR-135b [90], let-7-a [91], miR-21 [92], miR-22 [93], miR-23b and miR-145 [94], miR-30b/d [95,96], miR-148a-3p [97], miR-181a/b [98,99], miR-194-3p [100], miR-200a [101,102], miR-429, miR-4668 and miR-5088 [103] and miR-494 [95]. Only a few studies investigated circulating miR related to women fertility, but they allowed identifying miR-25, miR-27a, miR-31, miR-93, miR-106b, miR-146a, miR-152 and miR-155 (reviewed in [104]).
It is noteworthy to underline that, among all these fertility-related miR, only miR-21, miR-27a, miR-146a and miR-135b are present in Table 1, i.e., circulating miR related to EC. If further validated, these data would allow to characterize the presence of EC and the fertility status of the patients using sharply different miR panels, without ambiguity and with just one blood sample.
3.4. RNA-Based Diagnostics and Therapeutics: Are Innovations Set to Outpace Bioethics Precepts?
The potential of RNA-based measurements are potentially applicable through a wide array of medical areas, e.g., diagnosing diseases, prognosis and therapeutic selection. Currently, among the most promising clinical applications, it is worth mentioning not only cancer research [105], but also infectious diseases, transplant medicine and fetal monitoring [106]. RNA sequencing (RNA-seq) has enabled us to detect a remarkably wide host of RNA species, such as mRNA, non-coding RNA, pathogen RNA, chimeric gene fusions, transcript isoforms and splice variants. RNS-seq has also led to the possibility of quantifying known, pre-defined RNA species and rare RNA transcript variants. Not only can differential expression and detection of novel transcripts be feasible, but so can the detection of mutations and germline variation be achieved through RNA-seq, possibly involving hundreds to thousands of expressed genetic variants, which enhances our ability to evaluate allele-specific expression of these variants. Since the mechanisms governing RNA for diagnostics and therapeutics were first discovered and explored in the late 1990s, RNA interference (RNAi, a mechanism for gene silencing underpinned by short interfering RNAs, siRNA, and discovered in 1997 by Mello) [107,108] therapeutics has been developing remarkably fast, and our understanding of such highly complex processes and interactions has deepened considerably ever since [109]. Clinical trials have already begun. Still, such therapies relying on “gene-silencing” are even more controversial than diagnostic applications, since they may be viewed as akin to gene-editing/genetic engineering. It has been literally decades that such techniques have been developing and eliciting spirited debates among scientists, bioethicists, policy- and law-makers centered around how to best harness the potential of such breakthroughs to the benefit of potentially billions of human beings [110]. The hope and dream that diseases could one day be vanquished through the deliberate and targeted manipulation or editing of genes are the driving force behind the Human Genome Project [111,112], through which the complete human DNA sequence was first outlined and mapped in 2003. Such a fundamental principle at the core of which lies disease treatment via genetic modification dates back to the 1960s, i.e., when it was first observed that viral DNA had the ability to trigger cellular modulation during an infection. Early efforts aimed at gene modification date back to the 1970s [113,114]; recombinant DNAs (rDNAs) was used for that purpose, i.e., a combination of more than one DNA sequence from one or more species. Primary transfection methods were viral infection or calcium phosphate. Such innovations gradually bore fruit in the form of cell line development, genetically modified animals and even the creation of human proteins such as insulin in bacteria [115]. By the late 1970s, messenger RNA (mRNA) in vitro had been transfected by liposomes; this gave rise to rabbit globin expressed in mouse lymphocytes [116]. mRNA sequences in the cell cytoplasm, in order to inhibit protein translation or to induce exon skipping were targeted by newly developed antisense oligonucleotides (ASOs) [117]. Not surprisingly, it was back then that such fast-moving progress ignited a broad-ranging discourse encompassing genetic engineering in terms of its ethical, social, political and even economic implications. As a result, regulations limiting the different “tiers” of gene-editing were drafted and enacted. Later major developments are constituted by zinc finger nuclease (ZFN) to cleave a target DNA and two decades later TALEN and CRISPR/Cas9. Hence, it stands to reason that before such novel and potentially revolutionary therapeutic approaches can become mainstream from the standpoint of clinical applications, it is of utmost importance to discuss the legal and ethical issues arising from their use [118]. An analysis of the ethically relevant features of RNAi therapies is therefore essential for the purpose of producing a comprehensive risk-benefit analysis. Ethically relevant traits such as siRNA delivery and the specificity of silencing effects cannot be brushed aside. Furthermore, the future development of RNAi-based therapeutic options ought to take into account and respect patient autonomy by considering the risks of generating infection-competent viruses or possibly introducing genetic changes in germ line cells. Just as importantly, issues relative to justice in care delivery, such as equal access as opposed to private acquisition, and the right to participate in clinical trials should also be prioritized. The sheer scale of progress made in ncRNA research applied to cancer, and our ever-greater understanding of tumor biology, which will lay the groundwork for the development of new ‘smart’ drugs tailored to a patient-oriented approach, is poised to enable us to minimize adverse side effects and improving the patient prospects for recovery [119]. Having said that, the risk which needs confronting is that innovative biomedical techniques may outpace our ethical, legal and regulatory frameworks, leading to “grey areas” similar to those found in genome editing research and artificial intelligence. In addition, assisted reproductive technologies and fertility preservation also pose complex and challenging issues from the ethics and legal perspectives. Fertility preservation should only be offered to patients with endometrial cancer stage Ia grade 1 (G1), who present without myometrial invasion or where the cancer has invaded less than 50% of the myometrium, with no evidence of pathological lymph nodes or no evidence of synchronous or metachronous ovarian tumor [16]. The most common fertility-sparing treatment for endometrial cancer is hormonal therapy with progestins, which can induce regression or stabilization of the tumor. However, this treatment has several limitations, such as low response rate, high recurrence rate, lack of standardization, and potential adverse effects on the fetus. Therefore, patients who opt for fertility preservation should be carefully selected and counseled about the risks and benefits of this approach. They should also be monitored closely during and after the treatment and advised to undergo definitive surgery after completing their childbearing. ART can offer an alternative or complementary option for women who want to conceive after being treated for endometrial cancer. However, ART also poses some ethical dilemmas, such as the safety and efficacy of the procedures, the potential harm to the mother and the child, the disposal or donation of surplus embryos [120], and the access and affordability of the services [121,122]. Moreover, some ART techniques involve genetic testing or manipulation of the embryos, which raise further ethical questions about the respect for human dignity, autonomy, and diversity [123,124]. Undoubtedly, ART can provide hope and opportunity for women who want to have children after being diagnosed with EC. However, ART also involves medical, legal, and ethical challenges that require careful consideration and multidisciplinary collaboration. Therefore, patients who are interested in ART should be informed and supported by a team of experts who can help them make informed decisions that are consistent with their values and preferences [125].
4. Conclusions
As infertility after cancer has become a recognized survivorship issue, oncologists should be prepared to discuss the negative impact of cancer therapy on reproductive potential with their female patients in the same way as any other risks of cancer treatment are discussed. Furthermore, patients interested in fertility preservation should be promptly referred to a reproductive medicine expert to offer timely and appropriate counseling and improve success of fertility preservation. Reproductive endocrinologists should collaborate with oncologists and molecular biologists, updating them regarding available technologies and facilitating consultations with patients newly diagnosed with cancer. To further these alliances, education about fertility preservation, as well as ethical and legal aspects tailored to country-specific laws, should be incorporated into training programs for oncology and reproductive endocrinology. Just as importantly, the breakthrough constituted by RNA-based diagnostics and therapeutics need to rely on as broad a consensus as possible, in order to reconcile the amazing opportunities created by such techniques with the core values that must guide scientific research and medical practice at all times.
Author Contributions
Conceptualization, R.P., A.P. and S.Z.; methodology, R.P., G.C. and G.G.; validation, R.P., A.P., G.G., and S.Z.; formal analysis, R.P., G.G. and S.Z.; investigation, R.P., A.P., G.C. G.G. and S.Z.; resources, R.P., C.G., A.P., G.G. and S.Z.; data curation, R.P., G.G. and S.Z.; writing—original draft preparation, R.P., C.G., A.P., G.G. and S.Z.; writing—review and editing, R.P., C.G., A.P., G.G. and S.Z.; visualization, R.P., C.G., A.P., G.G. and S.Z.; supervision, R.P., C.G., A.P., G.G. and S.Z.; project administration, R.P., C.G., A.P., G.G. and S.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schenker, J.G. Ethical Dilemmas in Assisted Reproductive Technologies, Berlin, Boston: De Gruyter, 2011. [CrossRef]
- Knez, J.; Al Mahdawi, L.; Takač, I.; Sobočan, M. The Perspectives of Fertility Preservation in Women with Endometrial Cancer. Cancers 2021, 13, 602. [Google Scholar] [CrossRef] [PubMed]
- Creasman, W.T.; Odicino, F.; Maisonneuve, P.; Beller, U.; Benedet, J.L.; Heintz, A.P.; Ngan, H.Y.; Pecorelli, S. Carcinoma of the Corpus Uteri. Int J Gynaecol Obstet 2003, 83 (Suppl 1), 79–118. [Google Scholar] [CrossRef] [PubMed]
- Makker, V.; MacKay, H.; Ray-Coquard, I.; Levine, D.A.; Westin, S.N.; Aoki, D.; Oaknin, A. Endometrial Cancer. Nat Rev Dis Primers 2021, 7, 88. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Broaddus, R.R. Endometrial Cancer. N Engl J Med 2020, 383, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Sidorkiewicz, I.; Jóźwik, M.; Niemira, M.; Krętowski, A. Insulin Resistance and Endometrial Cancer: Emerging Role for microRNA. Cancers (Basel) 2020, 12, 2559. [Google Scholar] [CrossRef]
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial Cancer. The Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J Clin 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.-B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II Endometrial Cancers: Have They Different Risk Factors? J Clin Oncol 2013, 31, 2607–2618. [Google Scholar] [CrossRef] [PubMed]
- Soslow, R.A.; Tornos, C.; Park, K.J.; Malpica, A.; Matias-Guiu, X.; Oliva, E.; Parkash, V.; Carlson, J.; McCluggage, W.G.; Gilks, C.B. Endometrial Carcinoma Diagnosis: Use of FIGO Grading and Genomic Subcategories in Clinical Practice: Recommendations of the International Society of Gynecological Pathologists. Int J Gynecol Pathol 2019, 38 (Suppl 1), S64–S74. [Google Scholar] [CrossRef] [PubMed]
- Andreano, A.; Rechichi, G.; Rebora, P.; Sironi, S.; Valsecchi, M.G.; Galimberti, S. MR Diffusion Imaging for Preoperative Staging of Myometrial Invasion in Patients with Endometrial Cancer: A Systematic Review and Meta-Analysis. Eur Radiol 2014, 24, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Beddy, P.; Moyle, P.; Kataoka, M.; Yamamoto, A.K.; Joubert, I.; Lomas, D.; Crawford, R.; Sala, E. Evaluation of Depth of Myometrial Invasion and Overall Staging in Endometrial Cancer: Comparison of Diffusion-Weighted and Dynamic Contrast-Enhanced MR Imaging. Radiology 2012, 262, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Gullo, G.; Cucinella, G.; Chiantera, V.; Dellino, M.; Cascardi, E.; Török, P.; Herman, T.; Garzon, S.; Uccella, S.; Laganà, A.S. Fertility-Sparing Strategies for Early-Stage Endometrial Cancer: Stepping towards Precision Medicine Based on the Molecular Fingerprint. Int J Mol Sci 2023, 24, 811. [Google Scholar] [CrossRef]
- Merickel, C.R.; Dennison, E.; Moghadamfalahi, M. The Significance of Lower Uterine Segment Involvement in the Surgical Management of Endometrial Carcinoma. Am J Clin Pathol 2012, 138, A155–A155. [Google Scholar] [CrossRef]
- Dumesic, D.A.; Lobo, R.A. Cancer Risk and PCOS. Steroids 2013, 78, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Tanos, P.; Dimitriou, S.; Gullo, G.; Tanos, V. Biomolecular and Genetic Prognostic Factors That Can Facilitate Fertility-Sparing Treatment (FST) Decision Making in Early Stage Endometrial Cancer (ES-EC): A Systematic Review. Int J Mol Sci 2022, 23, 2653. [Google Scholar] [CrossRef]
- Mahdy, H.; Casey, M.J.; Crotzer, D. Endometrial Cancer. [Updated 2022 Sep 26]. In StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Uterine Cancer, Ed.; National Cancer Institute: Bethesda, MD, USA, 2021. [Google Scholar]
- Mutlu, L.; Manavella, D.D.; Gullo, G.; McNamara, B.; Santin, A.D.; Patrizio, P. Endometrial Cancer in Reproductive Age: Fertility-Sparing Approach and Reproductive Outcomes. Cancers 2022, 14, 5187. [Google Scholar] [CrossRef] [PubMed]
- Giampaolino, P.; Cafasso, V.; Boccia, D.; Ascione, M.; Mercorio, A.; Viciglione, F.; Palumbo, M.; Serafino, P.; Buonfantino, C.; De Angelis, M.C.; et al. Fertility-Sparing Approach in Patients with Endometrioid Endometrial Cancer Grade 2 Stage IA (FIGO): A Qualitative Systematic Review. Biomed Res Int 2022, 2022, 4070368. [Google Scholar] [CrossRef]
- Wei, J.; Zhang, W.; Feng, L.; Gao, W. Comparison of Fertility-Sparing Treatments in Patients with Early Endometrial Cancer and Atypical Complex Hyperplasia: A Meta-Analysis and Systematic Review. Medicine (Baltimore) 2017, 96, e8034. [Google Scholar] [CrossRef]
- Obermair, A.; Baxter, E.; Brennan, D.J.; McAlpine, J.N.; Muellerer, J.J.; Amant, F.; Van Gent, M.D.J.M.; Coleman, R.L.; Westin, S.N.; Yates, M.S.; et al. Fertility-Sparing Treatment in Early Endometrial Cancer: Current State and Future Strategies. Obstet Gynecol Sci 2020, 63, 417–431. [Google Scholar] [CrossRef]
- Gonthier, C.; Douhnai, D.; Koskas, M. Lymph Node Metastasis Probability in Young Patients Eligible for Conservative Management of Endometrial Cancer. Gynecol Oncol 2020, 157, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Rodolakis, A.; Scambia, G.; Planchamp, F.; Acien, M.; Di Spiezio Sardo, A.; Farrugia, M.; Grynberg, M.; Pakiž, M.; Pavlakis, K.; Vermeulen, N.; et al. ESGO/ESHRE/ESGE Guidelines for the Fertility-Sparing Treatment of Patients with Endometrial Carcinoma. Facts Views Vis ObGyn 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, J.-X. Fertility-Preserving Treatment in Women with Early Endometrial Cancer: The Chinese Experience. Cancer Manag Res 2018, 10, 6803–6813. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Yu, Z.; Yang, J.; Cao, D.; Yu, M.; Wang, Y.; Shen, K. Oral Progestin Treatment for Early-Stage Endometrial Cancer: A Systematic Review and Meta-Analysis. Int J Gynecol Cancer 2016, 26, 1081–1091. [Google Scholar] [CrossRef] [PubMed]
- Falcone, F.; Laurelli, G.; Losito, S.; Di Napoli, M.; Granata, V.; Greggi, S. Fertility Preserving Treatment with Hysteroscopic Resection Followed by Progestin Therapy in Young Women with Early Endometrial Cancer. J Gynecol Oncol 2017, 28, e2. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.; Obermair, A.; Gebski, V.; Janda, M. Efficacy of Oral or Intrauterine Device-Delivered Progestin in Patients with Complex Endometrial Hyperplasia with Atypia or Early Endometrial Adenocarcinoma: A Meta-Analysis and Systematic Review of the Literature. Gynecologic Oncology 2012, 125, 263–270. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-Up. Ann Oncol 2016, 27, 16–41. [Google Scholar] [CrossRef]
- Gallos, I.D.; Yap, J.; Rajkhowa, M.; Luesley, D.M.; Coomarasamy, A.; Gupta, J.K. Regression, Relapse, and Live Birth Rates with Fertility-Sparing Therapy for Endometrial Cancer and Atypical Complex Endometrial Hyperplasia: A Systematic Review and Metaanalysis. Am J Obstet Gynecol 2012, 207, 266.e1–266.e12. [Google Scholar] [CrossRef]
- Gullo, G.; Scaglione, M.; Cucinella, G.; Chiantera, V.; Perino, A.; Greco, M.E.; Laganà, A.S.; Marinelli, E.; Basile, G.; Zaami, S. Neonatal Outcomes and Long-Term Follow-Up of Children Born from Frozen Embryo, a Narrative Review of Latest Research Findings. Medicina (Kaunas) 2022, 58, 1218. [Google Scholar] [CrossRef]
- Gullo, G.; Perino, A.; Cucinella, G. Open vs. Closed Vitrification System: Which One Is Safer? Eur Rev Med Pharmacol Sci 2022, 26, 1065–1067. [Google Scholar] [CrossRef]
- Zaami, S.; Stark, M.; Signore, F.; Gullo, G.; Marinelli, E. Fertility Preservation in Female Cancer Sufferers: (Only) a Moral Obligation? The European Journal of Contraception & Reproductive Health Care 2022, 27, 335–340. [Google Scholar] [CrossRef]
- Fertility Preservation and Reproduction in Patients Facing Gonadotoxic Therapies: An Ethics Committee Opinion. Fertil Steril 2018, 110, 380–386. [CrossRef] [PubMed]
- Robertson, J.A. Cancer and Fertility: Ethical and Legal Challenges. Journal of the National Cancer Institute Monographs 2005, 2005, 104–106. [Google Scholar] [CrossRef]
- Riolo, G.; Cantara, S.; Marzocchi, C.; Ricci, C. MiRNA Targets: From Prediction Tools to Experimental Validation. Methods Protoc 2021, 4, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Naeli, P.; Winter, T.; Hackett, A.P.; Alboushi, L.; Jafarnejad, S.M. The Intricate Balance between MicroRNA-Induced MRNA Decay and Translational Repression. FEBS J 2022. [Google Scholar] [CrossRef] [PubMed]
- Friedman, R.C.; Farh, K.K.H.; Burge, C.B.; Bartel, D.P. Most Mammalian MRNAs Are Conserved Targets of MicroRNAs. Genome Res 2009, 19, 92. [Google Scholar] [CrossRef]
- Shu, J.; Resende E Silva, B.V.; Gao, T.; Xu, Z.; Cui, J. Dynamic and Modularized MicroRNA Regulation and Its Implication in Human Cancers. Scientific Reports 2017 7:1 2017, 7, 1–17. [Google Scholar] [CrossRef]
- Kumar, S.; Gonzalez, E.A.; Rameshwar, P.; Etchegaray, J.-P. Non-Coding RNAs as Mediators of Epigenetic Changes in Malignancies. Cancers (Basel) 2020, 12, 3657. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Perelli, F.; Zaami, S.; Piergentili, R.; Mattei, A.; Vizzielli, G.; Scambia, G.; Straface, G.; Restaino, S.; Signore, F. Towards Personalized Medicine: Non-Coding Rnas and Endometrial Cancer. Healthcare (Switzerland) 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Piergentili, R.; Zaami, S.; Cavaliere, A.F.; Signore, F.; Scambia, G.; Mattei, A.; Marinelli, E.; Gulia, C.; Perelli, F. Non-Coding Rnas as Prognostic Markers for Endometrial Cancer. Int J Mol Sci 2021, 22, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Klicka, K.; Grzywa, T.M.; Klinke, A.; Mielniczuk, A.; Włodarski, P.K. The Role of MiRNAs in the Regulation of Endometrial Cancer Invasiveness and Metastasis—A Systematic Review. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Donkers, H.; Bekkers, R.; Galaal, K.; Donkers, H.; Bekkers, R.; Galaal, K. Diagnostic Value of MicroRNA Panel in Endometrial Cancer: A Systematic Review. Oncotarget 2020, 11, 2010–2023. [Google Scholar] [CrossRef]
- Sayed, S.R. El; Cristante, J.; Guyon, L.; Denis, J.; Chabre, O.; Cherradi, N. MicroRNA Therapeutics in Cancer: Current Advances and Challenges. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Piergentili, R.; Basile, G.; Nocella, C.; Carnevale, R.; Marinelli, E.; Patrone, R.; Zaami, S. Using NcRNAs as Tools in Cancer Diagnosis and Treatment—The Way towards Personalized Medicine to Improve Patients’ Health. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Salmena, L.; Poliseno, L.; Tay, Y.; Kats, L.; Pandolfi, P.P. A CeRNA Hypothesis: The Rosetta Stone of a Hidden RNA Language? Cell 2011, 146, 353–358. [Google Scholar] [CrossRef]
- Karreth, F.A.; Pandolfi, P.P. CeRNA Cross-Talk in Cancer: When Ce-Bling Rivalries Go Awry. Cancer Discov 2013, 3, 1113–1121. [Google Scholar] [CrossRef]
- Moreno-García, L.; López-Royo, T.; Calvo, A.C.; Toivonen, J.M.; de la Torre, M.; Moreno-Martínez, L.; Molina, N.; Aparicio, P.; Zaragoza, P.; Manzano, R.; et al. Competing Endogenous Rna Networks as Biomarkers in Neurodegenerative Diseases. Int J Mol Sci 2020, 21, 1–42. [Google Scholar] [CrossRef]
- Nuzziello, N.; Liguori, M. The MicroRNA Centrism in the Orchestration of Neuroinflammation in Neurodegenerative Diseases. Cells 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Mao, Q.; Chen, B.; Wang, L.; Ma, W.; Liang, Y.; Zhang, T.; Dong, G.; Xu, L.; Jiang, F. The TWIST1-Centered Competing Endogenous RNA Network Promotes Proliferation, Invasion, and Migration of Lung Adenocarcinoma. Oncogenesis 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Yu, S.; Xiong, J.; Long, J.; Zheng, Y.; Sang, X. CeRNA Regulatory Network-Based Analysis to Study the Roles of Noncoding RNAs in the Pathogenesis of Intrahepatic Cholangiocellular Carcinoma. Aging (Albany NY) 2020, 12, 1047. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Liu, J. Bin; Deng, J.; Zou, D.Z.; Wu, J.J.; Cao, Y.H.; Yin, J.; Ma, Y.S.; Da, F.; Li, W. The Role of CeRNA-Mediated Diagnosis and Therapy in Hepatocellular Carcinoma. Hereditas 2021, 158. [Google Scholar] [CrossRef]
- Cen, L.; Liu, R.; Liu, W.; Li, Q.; Cui, H. Competing Endogenous RNA Networks in Glioma. Front Genet 2021, 12. [Google Scholar] [CrossRef]
- Morovat, P.; Morovat, S.; Hosseinpour, M.; Moslabeh, F.G.Z.; Kamali, M.J.; Samadani, A.A. Survival-Based Bioinformatics Analysis to Identify Hub Long Non-Coding RNAs along with LncRNA-MiRNA-MRNA Network for Potential Diagnosis/Prognosis of Thyroid Cancer. J Cell Commun Signal 2022. [Google Scholar] [CrossRef]
- Yang, S.; Wang, X.; Zhou, X.; Hou, L.; Wu, J.; Zhang, W.; Li, H.; Gao, C.; Sun, C. NcRNA-Mediated CeRNA Regulatory Network: Transcriptomic Insights into Breast Cancer Progression and Treatment Strategies. Biomed Pharmacother 2023, 162. [Google Scholar] [CrossRef] [PubMed]
- Abdollahzadeh, R.; Daraei, A.; Mansoori, Y.; Sepahvand, M.; Amoli, M.M.; Tavakkoly-Bazzaz, J. Competing Endogenous RNA (CeRNA) Cross Talk and Language in CeRNA Regulatory Networks: A New Look at Hallmarks of Breast Cancer. J Cell Physiol 2019, 234, 10080–10100. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, C.; Di Palo, A.; Russo, A.; Potenza, N. The LncRNAs at X Chromosome Inactivation Center: Not Just a Matter of Sex Dosage Compensation. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Shetty, A.; Venkatesh, T.; Kabbekodu, S.P.; Tsutsumi, R.; Suresh, P.S. LncRNA-MiRNA-MRNA Regulatory Axes in Endometrial Cancer: A Comprehensive Overview. Arch Gynecol Obstet 2022, 306, 1431–1447. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Ren, C.; Yao, Y.; Wang, Q.; Li, F.; Li, Y.; Jiang, A.; Wang, G. Identifying Prognostic Biomarkers in Endometrial Carcinoma Based on CeRNA Network. J Cell Biochem 2020, 121, 2437–2446. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Cui, J.; Wang, Z.; Wu, H. Comprehensive Bioinformatic Analyses of LncRNA-Mediated CeRNA Network for Uterine Corpus Endometrial Carcinoma. Transl Cancer Res 2022, 11, 1994–2012. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Chu, P.; Li, P.; Li, F. Construction of Endometrial Carcinoma CeRNA Network and Screening of Key Genes Based on TCGA Database. Comput Math Methods Med 2022, 2022. [Google Scholar] [CrossRef]
- Guo, C.; Song, W.Q.; Sun, P.; Jin, L.; Dai, H.Y. LncRNA-GAS5 Induces PTEN Expression through Inhibiting MiR-103 in Endometrial Cancer Cells. J Biomed Sci 2015, 22. [Google Scholar] [CrossRef]
- Xin, W.; Gao, X.; Zhao, S.; Zhao, P.; Yu, H.; Wu, Q.; Hua, K. LncRNA RP11-395G23.3 Suppresses the Endometrial Cancer Progression via Regulating MicroRNA-205-5p/PTEN Axis. Am J Transl Res 2020, 12, 4422. [Google Scholar]
- Xin, W.; Zhao, S.; Han, X.; Zhao, P.; Yu, H.; Gao, X.; Li, P.; Wu, Q.; Ding, J.; Hua, K. LncRNA LA16c-313D11.11 Modulates the Development of Endometrial Cancer by Binding to and Inhibiting MicroRNA-205-5p Function and Indirectly Increasing PTEN Activity. Int J Oncol 2020, 57, 355–363. [Google Scholar] [CrossRef]
- Tian, C.; Su, J.; Ma, Z.; Wu, Y.; Ma, H. LncRNA NBAT1 Inhibits Cell Metastasis and Promotes Apoptosis in Endometrial Cancer by Sponging MiR-21-5p to Regulate PTEN. Comput Math Methods Med 2022, 2022. [Google Scholar] [CrossRef]
- Li, Z.; Yu, Z.; Meng, X.; Zhou, S.; Xiao, S.; Li, X.; Liu, S.; Yu, P. Long Noncoding RNA GAS5 Impairs the Proliferation and Invasion of Endometrial Carcinoma Induced by High Glucose via Targeting MiR-222-3p/P27. Am J Transl Res 2019, 11, 2413. [Google Scholar]
- Shen, J.; Feng, X.; Wang, H.; Wang, Y.; Zhou, Y. Long Non-Coding RNA NNT-AS1 Positively Regulates NPM1 Expression to Affect the Proliferation of Estrogen-Mediated Endometrial Carcinoma by Interacting. J Cancer 2022, 13, 112–123. [Google Scholar] [CrossRef]
- Zhou, Y.X.; Wang, C.; Mao, L.W.; Wang, Y.L.; Xia, L.Q.; Zhao, W.; Shen, J.; Chen, J. Long Noncoding RNA HOTAIR Mediates the Estrogen-Induced Metastasis of Endometrial Cancer Cells via the MiR-646/NPM1 Axis. Am J Physiol Cell Physiol 2018, 314, C690–C701. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, S.; Zong, Z.H.; Guan, X.; Zhao, Y. CircRNA WHSC1 Targets the MiR-646/NPM1 Pathway to Promote the Development of Endometrial Cancer. J Cell Mol Med 2020, 24, 6898–6907. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A Clinically Applicable Molecular-Based Classification for Endometrial Cancers. Br J Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef]
- Paleari, L.; Pesce, S.; Rutigliani, M.; Greppi, M.; Obino, V.; Gorlero, F.; Vellone, V.G.; Marcenaro, E. New Insights into Endometrial Cancer. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Njoku, K.; Barr, C.E.; Crosbie, E.J. Current and Emerging Prognostic Biomarkers in Endometrial Cancer. Front Oncol 2022, 12. [Google Scholar] [CrossRef]
- Ravegnini, G.; Gorini, F.; De Crescenzo, E.; De Leo, A.; De Biase, D.; Di Stanislao, M.; Hrelia, P.; Angelini, S.; De Iaco, P.; Perrone, A.M. Can MiRNAs Be Useful Biomarkers in Improving Prognostic Stratification in Endometrial Cancer Patients? An Update Review. Int J Cancer 2022, 150, 1077. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. International Journal of Gynecologic Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Aimagambetova, G.; Terzic, S.; Laganà, A.S.; Bapayeva, G.; la Fleur, P.; Terzic, M. Contemporary Fertility-Sparing Management Options of Early Stage Endometrioid Endometrial Cancer in Young Nulliparous Patients. J Clin Med 2022, 11, 196. [Google Scholar] [CrossRef]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front Endocrinol (Lausanne) 2018, 9. [Google Scholar] [CrossRef]
- Javidi, M.A.; Ahmadi, A.H.; Bakhshinejad, B.; Nouraee, N.; Babashah, S.; Sadeghizadeh, M. Cell-Free MicroRNAs as Cancer Biomarkers: The Odyssey of MiRNAs through Body Fluids. Medical Oncology 2014, 31, 1–11. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating MicroRNAs as Stable Blood-Based Markers for Cancer Detection. Proc Natl Acad Sci U S A 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Delangle, R.; De Foucher, T.; Larsen, A.K.; Sabbah, M.; Azaïs, H.; Bendifallah, S.; Daraï, E.; Ballester, M.; Mehats, C.; Uzan, C.; et al. The Use of MicroRNAs in the Management of Endometrial Cancer: A Meta-Analysis. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef]
- Bloomfield, J.; Sabbah, M.; Castela, M.; Mehats, C.; Uzan, C.; Canlorbe, G. Clinical Value and Molecular Function of Circulating MicroRNAs in Endometrial Cancer Regulation: A Systematic Review. Cells 2022, 11. [Google Scholar] [CrossRef]
- Gao, J.; Fan, Y.Z.; Gao, S.S.; Zhang, W.T. Circulating MicroRNAs as Potential Biomarkers for the Diagnosis of Endometrial Cancer: A Meta-Analysis. Reproductive Sciences 2023, 30, 464–472. [Google Scholar] [CrossRef]
- Eismann, J.; Hirschfeld, M.; Erbes, T.; Rücker, G.; Jäger, M.; Ritter, A.; Weiss, D.; Gitsch, G.; Mayer, S. Hypoxia-and Acidosis-Driven Aberrations of Secreted MicroRNAs in Endometrial Cancer in Vitro. Oncol Rep 2017, 38, 993–1004. [Google Scholar] [CrossRef]
- Altmäe, S.; Koel, M.; Võsa, U.; Adler, P.; Suhorutšenko, M.; Laisk-Podar, T.; Kukushkina, V.; Saare, M.; Velthut-Meikas, A.; Krjutškov, K.; et al. Meta-Signature of Human Endometrial Receptivity: A Meta-Analysis and Validation Study of Transcriptomic Biomarkers. Sci Rep 2017, 7. [Google Scholar] [CrossRef]
- Kolde, R.; Laur, S.; Adler, P.; Vilo, J. Robust Rank Aggregation for Gene List Integration and Meta-Analysis. Bioinformatics 2012, 28, 573–580. [Google Scholar] [CrossRef]
- Wu, W.; Lin, Z.; Zhuang, Z.; Liang, X. Expression Profile of Mammalian MicroRNAs in Endometrioid Adenocarcinoma. Eur J Cancer Prev 2009, 18, 50–55. [Google Scholar] [CrossRef]
- Chung, T.K.H.; Cheung, T.H.; Huen, N.Y.; Wong, K.W.Y.; Lo, K.W.K.; Yim, S.F.; Siu, N.S.S.; Wong, Y.M.; Tsang, P.T.; Pang, M.W.; et al. Dysregulated MicroRNAs and Their Predicted Targets Associated with Endometrioid Endometrial Adenocarcinoma in Hong Kong Women. Int J Cancer 2009, 124, 1358–1365. [Google Scholar] [CrossRef]
- Boren, T.; Xiong, Y.; Hakam, A.; Wenham, R.; Apte, S.; Wei, Z.Z.; Kamath, S.; Chen, D.T.; Dressman, H.; Lancaster, J.M. MicroRNAs and Their Target Messenger RNAs Associated with Endometrial Carcinogenesis. Gynecol Oncol 2008, 110, 206–215. [Google Scholar] [CrossRef]
- Drissennek, L.; Baron, C.; Brouillet, S.; Entezami, F.; Hamamah, S.; Haouzi, D. Endometrial MiRNome Profile According to the Receptivity Status and Implantation Failure. Hum Fertil (Camb) 2022, 25, 356–368. [Google Scholar] [CrossRef]
- Riyanti, A.; Febri, R.R.; Zakirah, S.C.; Harzif, A.K.; Rajuddin, R.; Muharam, R.; Asmarinah, A.; Wiweko, B. Suppressing HOXA-10 Gene Expression by MicroRNA 135b During the Window of Implantation in Infertile Women. J Reprod Infertil 2020, 21, 217. [Google Scholar]
- Li, Q.; Liu, W.; Chiu, P.C.N.; Yeung, W.S.B. Mir-Let-7a/g Enhances Uterine Receptivity via Suppressing Wnt/β-Catenin Under the Modulation of Ovarian Hormones. Reproductive Sciences 2020, 27, 1164–1174. [Google Scholar] [CrossRef]
- Yan, Q.; Yan, G.; Zhang, C.; Wang, Z.; Huang, C.; Wang, J.; Zhou, J.; Liu, Y.; Ding, L.; Zhang, Q.; et al. MiR-21 Reverses Impaired Decidualization through Modulation of KLF12 and NR4A1 Expression in Human Endometrial Stromal Cells. Biol Reprod 2019, 100, 1395–1405. [Google Scholar] [CrossRef]
- Ma, H.L.; Gong, F.; Tang, Y.; Li, X.; Li, X.; Yang, X.; Lu, G. Inhibition of Endometrial Tiam1/Rac1 Signals Induced by MiR-22 up-Regulation Leads to the Failure of Embryo Implantation during the Implantation Window in Pregnant Mice. Biol Reprod 2015, 92, 152–153. [Google Scholar] [CrossRef]
- Revel, A.; Achache, H.; Stevens, J.; Smith, Y.; Reich, R. MicroRNAs Are Associated with Human Embryo Implantation Defects. Human Reproduction 2011, 26, 2830–2840. [Google Scholar] [CrossRef]
- Moreno-Moya, J.M.; Vilella, F.; Martínez, S.; Pellicer, A.; Simón, C. The Transcriptomic and Proteomic Effects of Ectopic Overexpression of MiR-30d in Human Endometrial Epithelial Cells. Mol Hum Reprod 2014, 20, 550–566. [Google Scholar] [CrossRef]
- Altmäe, S.; Martinez-Conejero, J.A.; Esteban, F.J.; Ruiz-Alonso, M.; Stavreus-Evers, A.; Horcajadas, J.A.; Salumets, A. MicroRNAs MiR-30b, MiR-30d, and MiR-494 Regulate Human Endometrial Receptivity. Reprod Sci 2013, 20, 308–317. [Google Scholar] [CrossRef]
- Zhang, Q.; Ni, T.; Dang, Y.; Ding, L.; Jiang, J.; Li, J.; Xia, M.; Yu, N.; Ma, J.; Yan, J.; et al. MiR-148a-3p May Contribute to Flawed Decidualization in Recurrent Implantation Failure by Modulating HOXC8. J Assist Reprod Genet 2020, 37, 2535–2544. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhang, H.; Jiang, Y.; Xue, B.; Diao, Z.; Ding, L.; Zhen, X.; Sun, H.; Yan, G.; Hu, Y. MicroRNA-181a Is Involved in the Regulation of Human Endometrial Stromal Cell Decidualization by Inhibiting Krüppel-like Factor 12. Reproductive Biology and Endocrinology 2015, 13, 1–9. [Google Scholar] [CrossRef]
- Graham, A.; Holbert, J.; Nothnick, W.B. MiR-181b-5p Modulates Cell Migratory Proteins, Tissue Inhibitor of Metalloproteinase 3, and Annexin A2 during in Vitro Decidualization in a Human Endometrial Stromal Cell Line. Reproductive Sciences 2017, 24, 1264–1274. [Google Scholar] [CrossRef]
- Pei, T.; Liu, C.; Liu, T.; Xiao, L.; Luo, B.; Tan, J.; Li, X.; Zhou, G.; Duan, C.; Huang, W. MiR-194-3p Represses the Progesterone Receptor and Decidualization in Eutopic Endometrium From Women With Endometriosis. Endocrinology 2018, 159, 2554–2562. [Google Scholar] [CrossRef]
- Jimenez, P.T.; Mainigi, M.A.; Word, R.A.; Kraus, W. Le; Mendelson, C.R. MiR-200 Regulates Endometrial Development During Early Pregnancy. Molecular Endocrinology 2016, 30, 977–987. [Google Scholar] [CrossRef]
- Haraguchi, H.; Saito-Fujita, T.; Hirota, Y.; Egashira, M.; Matsumoto, L.; Matsuo, M.; Hiraoka, T.; Koga, K.; Yamauchi, N.; Fukayama, M.; et al. MicroRNA-200a Locally Attenuates Progesterone Signaling in the Cervix, Preventing Embryo Implantation. Molecular Endocrinology 2014, 28, 1108–1117. [Google Scholar] [CrossRef]
- Shi, C.; Shen, H.; Fan, L.J.; Guan, J.; Zheng, X.B.; Chen, X.; Liang, R.; Zhang, X.W.; Cui, Q.H.; Sun, K.K.; et al. Endometrial MicroRNA Signature during the Window of Implantation Changed in Patients with Repeated Implantation Failure. Chin Med J (Engl) 2017, 130, 566–573. [Google Scholar] [CrossRef]
- Shekibi, M.; Heng, S.; Nie, G. MicroRNAs in the Regulation of Endometrial Receptivity for Embryo Implantation. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Sonu, R.J.; Jonas, B.A.; Dwyre, D.M.; Gregg, J.P.; Rashidi, H.H. Optimal Molecular Methods in Detecting P190 (BCR-ABL) Fusion Variants in Hematologic Malignancies: A Case Report and Review of the Literature. Case Rep Hematol 2015, 2015, 458052. [Google Scholar] [CrossRef]
- Byron, S.A.; Van Keuren-Jensen, K.R.; Engelthaler, D.M.; Carpten, J.D.; Craig, D.W. Translating RNA Sequencing into Clinical Diagnostics: Opportunities and Challenges. Nat Rev Genet 2016, 17, 257–271. [Google Scholar] [CrossRef]
- Rocheleau, C.E.; Downs, W.D.; Lin, R.; Wittmann, C.; Bei, Y.; Cha, Y.H.; Ali, M.; Priess, J.R.; Mello, C.C. Wnt Signaling and an APC-Related Gene Specify Endoderm in Early C. Elegans Embryos. Cell 1997, 90, 707–716. [Google Scholar] [CrossRef]
- Setten, R.L.; Rossi, J.J.; Han, S.-P. The Current State and Future Directions of RNAi-Based Therapeutics. Nat Rev Drug Discov 2019, 18, 421–446. [Google Scholar] [CrossRef]
- Ebbesen, M.; Jensen, T.G.; Andersen, S.; Pedersen, F.S. Ethical Perspectives on RNA Interference Therapeutics. Int J Med Sci 2008, 5, 159–168. [Google Scholar] [CrossRef]
- Kim, B.; Park, J.-H.; Sailor, M.J. Rekindling RNAi Therapy: Materials Design Requirements for In Vivo siRNA Delivery. Adv Mater 2019, 31, e1903637. [Google Scholar] [CrossRef]
- Green, E.D.; Watson, J.D.; Collins, F.S. Human Genome Project: Twenty-Five Years of Big Biology. Nature 2015, 526, 29–31. [Google Scholar] [CrossRef]
- Morris, P.J. From Mendel to the Human Genome Project. N C Med J 2013, 74, 477. [Google Scholar]
- Friedmann, T. A Brief History of Gene Therapy. Nat Genet 1992, 2, 93–98. [Google Scholar] [CrossRef]
- Jackson, D.A.; Symons, R.H.; Berg, P. Biochemical Method for Inserting New Genetic Information into DNA of Simian Virus 40: Circular SV40 DNA Molecules Containing Lambda Phage Genes and the Galactose Operon of Escherichia Coli. Proc Natl Acad Sci U S A 1972, 69, 2904–2909. [Google Scholar] [CrossRef]
- Goeddel, D.V.; Kleid, D.G.; Bolivar, F.; Heyneker, H.L.; Yansura, D.G.; Crea, R.; Hirose, T.; Kraszewski, A.; Itakura, K.; Riggs, A.D. Expression in Escherichia Coli of Chemically Synthesized Genes for Human Insulin. Proc Natl Acad Sci U S A 1979, 76, 106–110. [Google Scholar] [CrossRef]
- Dimitriadis, G.J. Translation of Rabbit Globin mRNA Introduced by Liposomes into Mouse Lymphocytes. Nature 1978, 274, 923–924. [Google Scholar] [CrossRef]
- Schoch, K.M.; Miller, T.M. Antisense Oligonucleotides: Translation from Mouse Models to Human Neurodegenerative Diseases. Neuron 2017, 94, 1056–1070. [Google Scholar] [CrossRef]
- Chan, J.J.; Tay, Y. Noncoding RNA:RNA Regulatory Networks in Cancer. Int J Mol Sci 2018, 19, 1310. [Google Scholar] [CrossRef]
- Tian, Z.; Liang, G.; Cui, K.; Liang, Y.; Wang, Q.; Lv, S.; Cheng, X.; Zhang, L. Insight Into the Prospects for RNAi Therapy of Cancer. Front Pharmacol 2021, 12, 644718. [Google Scholar] [CrossRef]
- Montanari Vergallo, G.; Zaami, S.; Bruti, V.; Signore, F.; Marinelli, E. How the legislation in medically assisted procreation has evolved in Italy. Med Law 2017, 36, 5–28. [Google Scholar]
- Ethics Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org Cross-Border Reproductive Care: An Ethics Committee Opinion. Fertil Steril 2022, 117, 954–962. [Google Scholar] [CrossRef]
- Marinelli, S.; Cucinella, G.; Basile, G. COVID-19 and Female Fertility: The Flaws of Italian Law 40/2004 on Assisted Procreation in Pandemic Times. Acta Biomed 2022, 93, e2022316. [Google Scholar] [CrossRef]
- Ghoshal, R. Assisted Reproductive Technologies: Conundrums and Challenges. Indian J Med Ethics 2018, 3, 95–98. [Google Scholar] [CrossRef]
- Frith, L.; Blyth, E. Assisted Reproductive Technology in the USA: Is More Regulation Needed? Reprod Biomed Online 2014, 29, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.N.; Ke, R.W. Ethical Considerations in the Field of Assisted Reproductive Technology. Minerva Endocrinol 2018, 43, 80–86. [Google Scholar] [CrossRef]
Figure 1.
Examples of ceRNET in EC. The reported examples are only for exemplification purposes, they are not exhaustive of EC-related ceRNET identified so far. As described in text, in these networks, nodes are ceRNA (competing endogenous RNAs, i.e., a lncRNA or a mRNA), while miR represent their connections. As a rule, in these axes the regulation of lncRNA and mRNA are concordant, i.e., they are both either up- or down-regulated thanks to the inhibitory action of lncRNA over miR and the contemporary inhibitory action of miR over mRNA. In these schemes, circles represent mRNA, rectangles represent lncRNA. According to the definition reported in the text, a ceRNET is identified when one axis (lncRNA + miR + mRNA) share at least a node or a connection with another axis. In panel A, the two top axes share both a connection (miR-646) and a node (NPM1) and at the same time this node (NPM1) is shared with the lower axis. In panel B, a more complex situation is depicted: the two top axes share both a connection (miR-205-5p) and a node (PTEN) which is shared with two additional axes; one of these PTEN-linked axes (PTEN/miR103/GAS5) is in turn connected with an additional axis, sharing the node identified by GAS5. Bibliographic sources for these schemes are reported in the references list [63,64,65,66,67,68,69,70].
Figure 1.
Examples of ceRNET in EC. The reported examples are only for exemplification purposes, they are not exhaustive of EC-related ceRNET identified so far. As described in text, in these networks, nodes are ceRNA (competing endogenous RNAs, i.e., a lncRNA or a mRNA), while miR represent their connections. As a rule, in these axes the regulation of lncRNA and mRNA are concordant, i.e., they are both either up- or down-regulated thanks to the inhibitory action of lncRNA over miR and the contemporary inhibitory action of miR over mRNA. In these schemes, circles represent mRNA, rectangles represent lncRNA. According to the definition reported in the text, a ceRNET is identified when one axis (lncRNA + miR + mRNA) share at least a node or a connection with another axis. In panel A, the two top axes share both a connection (miR-646) and a node (NPM1) and at the same time this node (NPM1) is shared with the lower axis. In panel B, a more complex situation is depicted: the two top axes share both a connection (miR-205-5p) and a node (PTEN) which is shared with two additional axes; one of these PTEN-linked axes (PTEN/miR103/GAS5) is in turn connected with an additional axis, sharing the node identified by GAS5. Bibliographic sources for these schemes are reported in the references list [63,64,65,66,67,68,69,70].
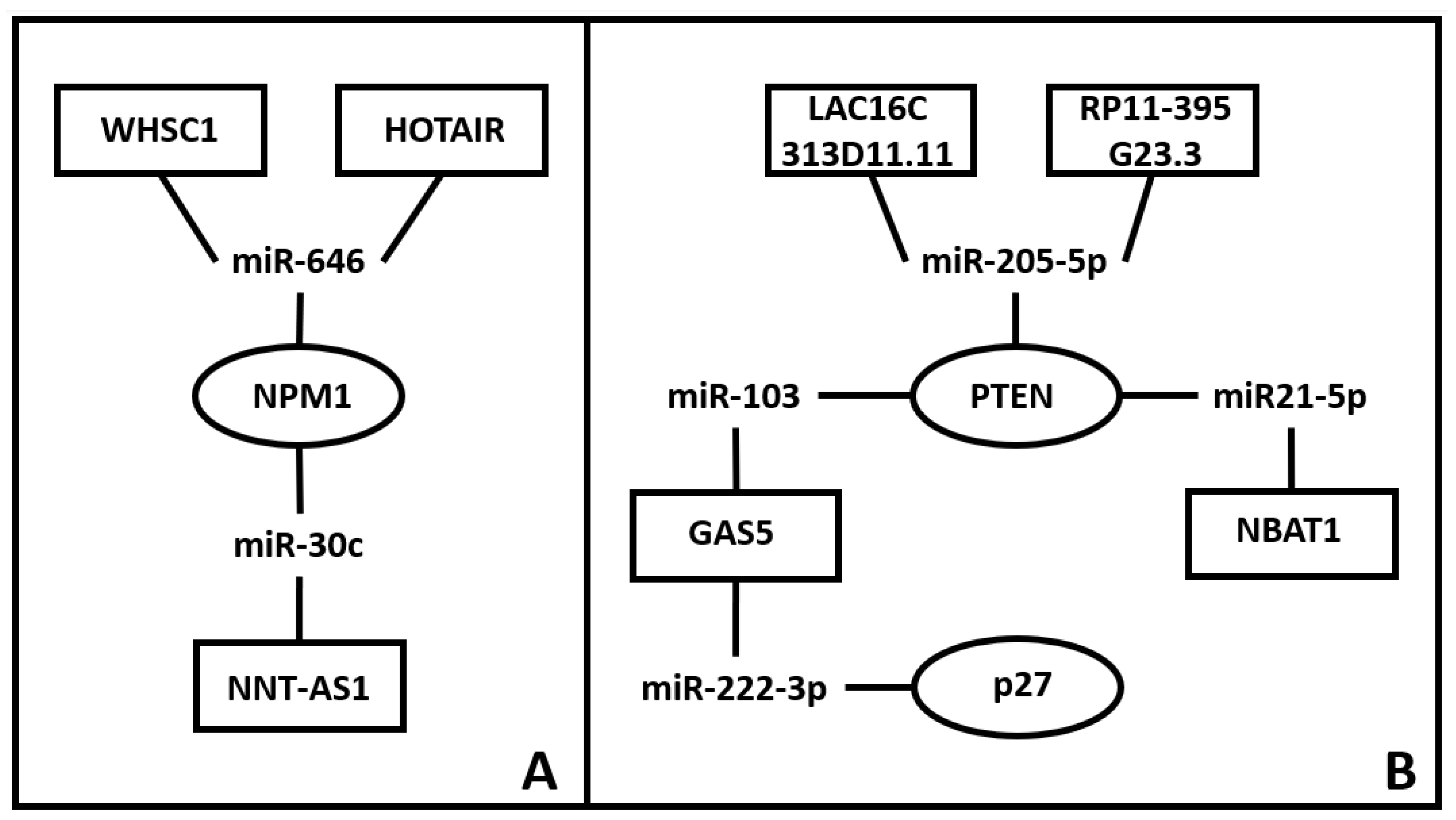

Table 1.
deregulated miR in EC. Column 1: circulating miR in EC patients [81]; column 2: up- or down-regulation of circulating miR, according to Bloomfield and collaborators [81]; column 3: up- or down-regulation of miR from EC specimen and matching circulating miR, retrieved from the work of Delangle and co-workers [80]. Double arrows represent inconclusive results; extr is for extracellular (i.e., serum/plasma derived) miR, intr is for intracellular (i.e., specimen-derived) miR.
Table 1.
deregulated miR in EC. Column 1: circulating miR in EC patients [81]; column 2: up- or down-regulation of circulating miR, according to Bloomfield and collaborators [81]; column 3: up- or down-regulation of miR from EC specimen and matching circulating miR, retrieved from the work of Delangle and co-workers [80]. Double arrows represent inconclusive results; extr is for extracellular (i.e., serum/plasma derived) miR, intr is for intracellular (i.e., specimen-derived) miR.
| miR name | extr. | intr. |
|---|---|---|
| 9 | ↓ | ↑ |
| 15b | ↑ | |
| 20b-5p | ↑ | |
| 21 | ↑↓ | ↓ |
| 27a | ↑ | ↑ |
| 29b | ↓ | |
| 30a-5p | ↓ | ↓ |
| 92a | ↑ | |
| 99a | ↑ | ↓ |
| 100 | ↑ | ↓ |
| 135b | ↑ | ↑ |
| 141 | ↑ | ↑ |
| 142-3p | ↑ | ↑↓ |
| 143-3p | ↑ | |
| 146a-5p | ↑ | |
| 150-5p | ↑ | |
| 151a-5p | ↑ | |
| 186 | ↑ | |
| 195-5p | ↑ | |
| 199b | ↑ | ↓ |
| 200a | ↑ | ↑ |
| 203 | ↑ | ↑ |
| 204 | ↑↓ | ↓ |
| 205 | ↑ | ↑ |
| 222 | ↑ | |
| 223 | ↑ | ↑ |
| 301b | ↓ | |
| 423-3p | ↑ | |
| 449 | ↑ | ↑ |
| 484 | ↑ | |
| 887-5p | ↑ | |
| 1228 | ↑ | |
| 1290 | ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



