
Submitted:
06 June 2023
Posted:
07 June 2023
Read the latest preprint version here
Abstract
Knee osteoarthritis is the most popular type of osteoarthritis that causes extreme pain in elderly. Currently there is no cure for osteoarthritis. To lessen clinical symptoms, glucosamine was suggested. The primary goal of our study is to evaluate the efficacy and safety of glucosamine from recent studies. Electronic databases such as PubMed, Scopus, Cochrane were used to assess RCT. From the beginning through March 2023, the papers were checked, and if they fulfilled the inclusion criteria, they were then examined. WOMAC and VAS scales were considered as main outcome measure. A total of 15 studies were selected. Global pain was significantly decreased in comparison to placebo, as measured by the VAS index, with an overall effect size SMD of -7.41 ([95% CI] 14.31, 0.51). The WOMAC scale confirmed that pain, stiffness, and physical function had improved, however the effects were insufficient. A statistical update also revealed that there were no reports of serious medication interactions or significant adverse events. To summarize, glucosamine is more effective than a placebo at reducing pain in knee osteoarthritis patients. In long-term treatment, oral glucosamine sulfate 1500 mg/day is believed to be well tolerated.
Keywords:
Osteoarthritis
; Effectiveness
; Safety
; Glucosamine
; systematic review
1. Introduction
Around 58 million adults today have osteoarthritis (OA), a degenerative inflammatory disorder of the joint cartilage. By 2040, that number is expected to rise to 78.4 million [1]. Articular cartilage degeneration, subchondral bone remodeling, and synovial low-grade inflammation are anatomical features of OA [2]. This inflammation may result in discomfort, stiffness, and a decreased range of motion, which are finally referred to as arthritic joints [1]. Knee osteoarthritis is the most common type of osteoarthritis that affects the lower limb [3]. That is the location where impairment occurs the most frequently [3]. Mobility declines as a result of the usual symptoms of knee OA, including pain, joint contracture, misalignment, and muscle weakening [4]. These symptoms, may eventually raise your chance of being overweight, developing diabetes, and experiencing fractures [1]. Moreover, OA also affects younger people, proving that it is not just a disease of the elderly [2].
The use of both conservative therapy and surgical techniques has been made in the medical treatment of OA [5]. Lessening discomfort, enhancing function and quality of life, and reducing disability are the objectives of treating OA [5]. However, there are presently no disease-modifying therapies available for OA due to inadequate knowledge about the pathology. Also, the lack of a biomarker that is sensitive enough to enable detection in the early stages of the disease causes a delay in therapeutic management [2].
The American College of Rheumatology (ACR) and the Osteoarthritis Research Society International (OARSI) recommend patient education and self-management, land-based activity, and dietary weight management for those who are overweight or obese as the main therapy for knee OA [6]. Analgesia, which includes the use of paracetamol, topical and oral nonsteroidal anti-inflammatory medicines (NSAIDs), and opioid medications, continues to be the cornerstone of pharmaceutical treatment for symptomatic OA [7]. Nevertheless, they are accused of escalating the likelihood of unfavorable occurrences on gastrointestinal or cardiovascular systems , as they solely concentrate on symptomatic relief rather than curing the sickness [8].
This is why symptomatic slow-acting drugs (SYSADOAs), which can alleviate the clinical symptoms of OA with superior tolerance and safety profiles, have recently made waves [8]. One of these is glucosamine, a natural that ranks among the body’s most common monosaccharides [5]. For more than 50 years, it has been used as a medication to treat OA [2]. Most scientific societies in Europe, but not those in the United States, suggest glucosamine for the treatment of knee problems [2]. Glucosamine sulfate (GS) is one of two medications regarded as a first-line pharmacological treatment for slow-onset medium to long-term control of symptoms, following ESCEO advice for the prolonged use of SYSADOAs [9].
In Vietnam, Glucosamine is only indicated as a supporting role in the osteoarthritis therapy process for symptom reduction. Other locations than knee joint are not recommended to utilize glucosamine [10]. In addition, glucosamine is one of the two drugs listed in the health insurance coverage for mild-to-moderate osteoarthritis treatment [11].
Most recent findings from clinical research still demonstrate the controversial debate about glucosamine’s therapeutic effects. To expand the data supporting the safety and effectiveness of glucosamine in the treatment of osteoarthritis, we will conduct a systematic review of recent RCT in this study.
2. Materials and Methods
2.1. Search strategy
This study was designed according to PRISMA guidelines. To conduct our search, we utilized online scientific databases including PubMed, Cochrane and Scopus. We limited the search to articles from inception to March 2023. The following keywords were combined to retrieve the studies: “glucosamine” , “osteoarthritis”, “knee osteoarthritis” , “efficacy” , “effect” , “safety”, “placebo”, “randomized”, “double-blind”, “RCT” using Boolean connector. Additionally, further citations were discovered after screening reference lists of all obtained articles. The only participants in our search are human, and we exclusively use English-language articles.
2.2. Selection criteria
Studies were included if they met the following criteria: (1) the research was a randomized placebo-controlled trial with either a parallel or cross-over design either of efficacy or safety; (2) patients had a diagnosis of knee, hip, or hand osteoarthritis in minimum; (3) At least indicates comparison between oral glucosamine with chondroitin and placebo. (4) Sufficient data about pain, physical function, stiffness based on WOMAC index or VAS scale at the end of the treatment.
The other studies were excluded by: (1) Studies of non-randomized and/or uncontrolled trials; (2) Compare glucosamine in combination form to other drugs; (3) Lack of placebo control group for glucosamine; and (4) Unclear information about VAS or WOMAC index subscores at the end of treatment.
2.3. Data analysis & Outcome measure
In each article, the following date were extracted; (1) first author’s name, (2) year of publication, (3) study design, (4) site of OA, (5) number of participants in the intervention and control groups, (6) treatment duration, (7) type of outcome measure (VAS / WOMAC)
The main outcomes were the degree of pain, the improvement in function, and the stiffness score from baseline to the end of treatment. Safety was considered as secondary outcome. SMD divides the pooled SD of the differences between two interventions to represent the extent of the intervention impact in each study compared to the variability observed in that study [8]. In order to pool the data, outcomes measured on different scales were standardized. Standardized mean difference (SMD) estimations and 95% confidence intervals (95% CI) were used to present the results for the comparative effect between the glucosamine group and control group.
In this study, the effect size was transformed back to the different units of the WOMAC or Visual Analogue Scale (VAS), the most commonly used scale based on a media pooled SD of 2.5 cm to assess pain on the scale of 0 to 10 cm. Clinically substantial improvement was considered as a change of 2 points on the 0–10 scale [8]. Using traditional funnel plots, articles biases and small study effects were evaluated. Heterogeneity was assessed by I2 statistics. A two-sided p value of < 0.15 was considered statistically significant.
2.4. Risk of bias
To assess the methodological quality of the included studies, the Cochrane Risk of Bias Tool was utilized [8]. The criteria were scored as ‘yes’ (low risk of bias), ‘no’ (high risk of bias) or ‘unclear’ [12]. A study with a low risk of bias was defined as fulfilling six or more of the criteria items [12].
3. Results
3.1. Selection of study process
Combining these keywords “glucosamine,” “osteoarthritis,” “effect,” and “safety”, a total of 797 articles were identified through PubMed, Cochrane, Scopus databases, as shown on Figure 1. We then eliminated duplicates and examined the titles and abstracts of all the studies. Any papers that demonstrated a lack of relevance to our topic were disqualified. As a result, 53 publications were eligible to be reviewed. Through the evaluating process, those articles not fulfilling criteria included: unsuitable contents, non-English writing, and full-text unavailability. Additionally, we came across 1 article finding from references. Overall, 15 publications were deemed sufficient for data extraction.
Figure 1.
Flow diagram of study selection process.
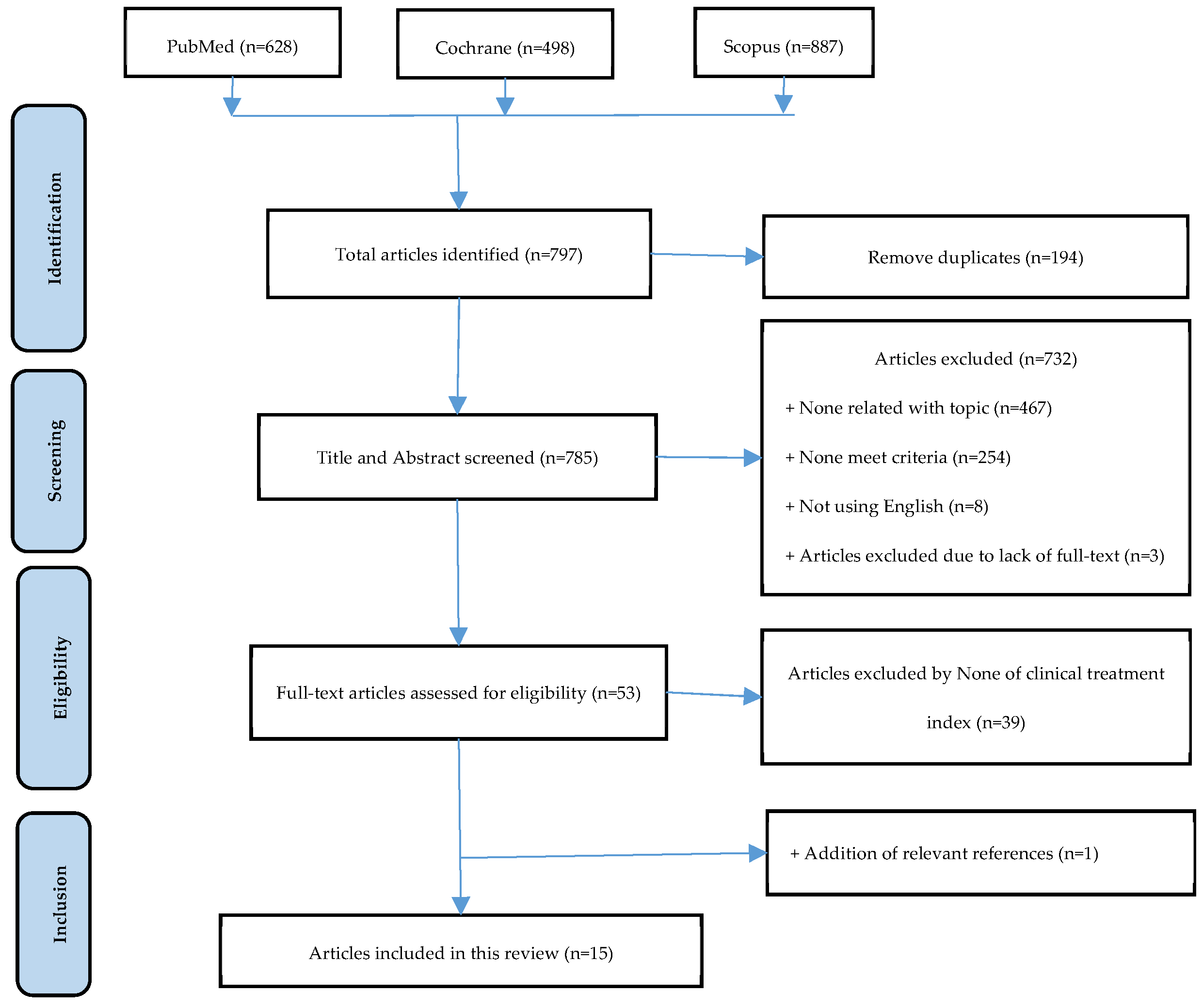

Table 1.
Characteristic of included studies.
| References | Study design |
OA site | Intervention | N in control group |
N in glucosamine group |
Follow-up (months) | *Age | Outcome |
|---|---|---|---|---|---|---|---|---|
| Giordano et al., 2009 [13] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 30 | 30 | 3 | 57.2 ± 7.2 58.0 ± 8.3 |
WOMAC, VAS |
| Rozendaal et al., 2008 [14] | Randomized, placebo-controlled, blinded trial |
Hip | GS vs P | 111 | 111 | 24 | 63.1 ± 9.5 63.7 ± 8.5 |
WOMAC, VAS |
| Herrero-Beaumont et al., 2007 [15] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 104 | 106 | 6 | 63.4 ± 6.9 64.5 ± 7.2 |
WOMAC |
| Fransen et al., 2015 [16] | Randomized, placebo-controlled, double-blind trial |
Knee | GS vs GS+CS vs CS vs P |
151 | 152 | 24 | 61.2 ± 7.7 60.6 ± 8.1 |
WOMAC |
| Hughes et al., 2002 [17] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 40 | 40 | 6 | **62.28 ± 9.12 | WOMAC,VAS, McGill pain questionnaire |
| Pavelka et al., 2002 [18] | Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 101 | 101 | 36 | 61.2 ± 7.2 63.5 ± 6.9 |
WOMAC |
| Sawitzke et al., 2010 [19] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs CS vs GS+CS vs celecoxib vs P |
134 | 131 | 24 | 56.7 ± 10.5 56.9 ±9.8 |
WOMAC |
| Reginster et al., 2001 [20] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 106 | 106 | 36 | 66.0 ± 8.1 65.5 ± 7.5 |
WOMAC |
| Rindone et al., 2000 [21] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 49 | 49 | 2 | 63 ± 12 64 ± 11 |
VAS |
| Kwoh et al., 2014 [22] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS + P | 103 | 98 | 6 | 52.17±6.05 52.29±6.72 |
WOMAC |
| McAlindon et al., 2004 [23] |
Randomized, placebo-controlled, double-blind trial |
Knee | GH vs P | 104 | 101 | 3 | ND ND |
WOMAC |
| Madhu et al., 2013 [24] |
Randomized, placebo-controlled, single-blind trial |
Knee | GS vs P vs NR-INF-02 vs NR-INF-02 + GS |
30 | 30 | 1,5 (42 days) | 56.80±7.99 56.77±9.98 |
WOMAC, VAS, CGIC |
| Petersen et al., 2011 [25] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs ibuprofen vs P |
12 | 12 | 3 | 62.2±3.4 63.1±4.7 | VAS |
| Frestedt et al., 2008 [26] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P vs Aquamin vs GS + aquamin |
16 | 19 | 3 | 59.2 ± 8.3 58.9 ± 7.4 |
WOMAC, 6-MWD |
| Clegg et al., 2006 [27] |
Randomized, placebo-controlled, double-blind trial |
Knee | GH vs CS vs GH+CS vs P vs Celecoxib | 313 | 317 | 6 | 58.6 ± 10.2 58.2 ± 9.8 |
WOMAC |
| Cibere et al., 2004 [28] |
Randomized, placebo-controlled, double-blind trial |
Knee | GS vs P | 66 | 71 | 6 | 64(40–83)a 65(43–88)a |
WOMAC, EQ-5D |
| Nieman et al., 2013 [29] |
Randomized, placebo-controlled, double-blind trial |
KneeHip Ankles Shoulders Hand | GS vs P | 51 | 101 | 2 | 57.6 ± 0.9 58.3 ± 0.8 |
WOMAC, VAS, SF-36, 6-MWD |
* Abbreviations: ND: no data; GS: glucosamine sulfate; GH: glucosamine hydrochloride; CS: chondroitin sulfate; P: placebo; *Age: the upper number indicates Glucosamine group; the lower number indicates Placebo group; ** representative for both glucosamine and placebo group; a median (IQR); IQR: interquartile range.
The study’s data were compiled from 17 randomized, placebo-controlled articles. In which there were 10 articles using the double blind method. The study included 2859 subjects who completed the study. Of these, 1428 were in the control group and 1431 were in the Glucosamine group. Clinical studies were published between 2000-2015. The studies were followed up from 1.5 to 36 months. The dose of glucosamine used in these clinical studies is 1500 mg/day. In the studies we have synthesized, we used 2 forms of glucosamine: glucosamine sulfate and glucosamine hydrochloride [22], or used both forms [28]. These studies were focused mainly on Knee and used WOMAC scale as primary outcome measure.
3.2. Risk of bias assessment
Evaluation on Methodological quality was summarized in Table 2. Low risk of bias for selective outcome reporting was confirmed in most of included studies, aside from Nieman et al., 2013 trial.
3.3. Efficacy of Glucosamine on Knee osteoarthritis
According to VAS scale (Table 3), Glucosamine showed improvement versus placebo with the overall difference −7.41 ([95% CI] −14.31, −0.51) significantly, judging at the global pain.
The WOMAC scale is divided into 3 subscales: pain, physical function and stiffness (Table 5, Table 6, Table 7 respectively). On knee joint, all of 3 categories though there was favorable in statistical change but did not contribute considerable benefit, as the effect size indicated − 0.04 ([95% CI] − 0.13, 0.06) for pain (Table 5), − 0.07 ([95% CI] − 0.17, 0.03) for physical function (Table 6) and -0.30, ([95% CI] 0.82, 0.21) for stiffness (Table 7) respectively. It can also be noted that Glucosamine did not affect the total WOMAC score, with the SMD -2.27 ([95% CI] −5.21, 0.66).
Table 3.
Weighted mean difference and 95% confidence intervals for the effect of glucosamine versus placebo on visual analogue scale [5].
Table 3.
Weighted mean difference and 95% confidence intervals for the effect of glucosamine versus placebo on visual analogue scale [5].
| Study and year | Glucosamine | Placebo | Std. Mean Difference |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | IV, Random, 95% CI | |
| Clegg et al., 2006 | -16 | 26.9 | 317 | -16.6 | 25.2 | 313 | 4.5% | 0.60 [-3.47, 4.67] |
| Fransen et al., 2015 | -8.6 | 24.5 | 152 | -7.2 | 33.8 | 151 | 4.1% | -1.40 [-8.05 , 5.25 ] |
| Giodarno et al., 2009 | -16.6 | 22.4 | 30 | 0.3 | 10.8 | 30 | 3.7% | -16.90 [-25.80,-8.00] |
| Madhu et al., 2013 | -31.7 | 19 | 24 | -15.5 | 18.3 | 29 | 3.5% | -16.20 [-26.31, -6.09] |
| Petersen et al., 2011 | -16.8 | 17.3 | 12 | -1.9 | 10.7 | 12 | 3.3% | -14.90 [-26.41, -3.39] |
| Rindone et al., 2000 | -15 | 26.6 | 49 | -15 | 23.4 | 49 | 3.6% | 0.00 [ -9.92, 9.92] |
| Subtotal (95% Cl) | 584 | 584 | 22.6% |
-7.41 [-14.31, -0.51] |
||||
Table 4.
Weighted mean difference and 95% confidence intervals for the effect of glucosamine versus placebo on total WOMAC index [5].
Table 4.
Weighted mean difference and 95% confidence intervals for the effect of glucosamine versus placebo on total WOMAC index [5].
| Study and year | Glucosamine | Placebo | Std. Mean Difference |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | IV, Random, 95% CI | |
| Cibere et al., 2004 | 3.2 | 15.5 | 71 | 3.4 | 18.1 | 66 | 9.7% | -0.20 [-5.86, 5.46] |
| Frestedt et al., 2008 | -10.5 | 15 | 14 | -5.9 | 16.9 | 9 | 3.8% | -4.60 [-18.15, 8.95] |
| Herrero-Beaumont et al., 2007 | -17.3 | 13.3 | 78 | -11.7 | 14.3 | 70 | 11.0% | -5.60 [-10.06, -1.14] |
| Kwoh et al., 2014 | -15.1 | 19.3 | 98 | -19.1 | 20.1 | 103 | 9.9% | 4.00 [-1.45, 9.45] |
| Madhu et al., 2013 | -23.4 | 17.1 | 24 | -9.3 | 11.4 | 29 | 7.3% | -14.10 [-22.0, -6.10] |
| McAlindon et al., 2004 | 7.8 | 13.1 | 101 | 7.8 | 13.5 | 104 | 11.9% | 0.00 [-3.64, 3.64] |
| Pavelka et al., 2002 | -7.7 | 7.1 | 66 | -4.7 | 5.9 | 55 | 13.2% | -3.00 [-5.32, -0.68] |
| Regisnter et al., 2001 | -0.2 | 19.2 | 68 | -0.6 | 19.6 | 71 | 8.8% | 0.40 [-6.05, 6.85] |
| Subtotal (95% Cl) | 520 | 507 | 75.6% |
-2.27 [-5.21, 0.66] |
||||
Table 5.
Changes in WOMAC pain sub-score in patients treated with glucosamine versus placebo [4].
Table 5.
Changes in WOMAC pain sub-score in patients treated with glucosamine versus placebo [4].
| Study and year | Glucosamine | Placebo | Std. Mean Difference |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | IV, Fixed, 95% CI | |
| McAlindon et al., 2004 | -2 | 3.4 | 101 | -2.5 | 3.8 | 104 | 12.7% | 0.14 [-0.14, 0.41] |
| Cibere et al., 2004 | -25 | 98 | 71 | -28 | 104 | 66 | 8.5% | 0.03 [-0.31, 0.36] |
| Clegg et al., 2006 | -82.9 | 115.4 | 317 | -86.1 | 114.2 | 313 | 39.1% | 0.03 [-0.13, 0.18] |
| Herreo-Beaumont et al., 2007 | -2.7 | 3.15 | 106 | -1.8 | 4.16 | 104 | 12.9% | -0.24 [-0.51, 0.03] |
| Frestedt et al., 2008 | -12.3 | 16.26 | 19 | -2.9 | 22.16 | 16 | 2.1% | -0.48 [-1.15, 0.02] |
| Nieman et al., 2013 | -2.4 | 2.8 | 49 | -0.9 | 2.86 | 51 | 6.0% | -0.53 [-0.92, -0.13] |
| Fransen et al., 2015 | -22 | 3.55 | 152 | -2.1 | 3.45 | 151 | 18.8% | 0.03 [-0.20, 0.25] |
| Total | 815 | 805 | 100.0% | -0.04 [-0.13, 0.06] |
||||
|
Heterogeneity: Chi2 = 12.33, df = 6 (P = 0.05); I2 = 51% Test for overall effect: Z = 0.74 (P=0.46) | ||||||||
Table 6.
Changes in Western Ontario and McMaster Universities Osteoarthritis Index physical function sub-score in patients treated with glucosamine versus placebo [4].
Table 6.
Changes in Western Ontario and McMaster Universities Osteoarthritis Index physical function sub-score in patients treated with glucosamine versus placebo [4].
| Study and year | Glucosamine | Placebo | Std. Mean Difference |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | IV, Fixed, 95% CI | |
| McAlindon et al., 2004 | -5.2 | 9.5 | 101 | -4.6 | 9.6 | 104 | 12.9% | -0.06 [-0.34, 0.21] |
| Cibere et al., 2004 | -58 | 270 | 71 | -63 | 318 | 66 | 8.6% | 0.02 [-0.32, 0.35] |
| Clegg et al., 2006 | -222.3 | 388.3 | 317 | -227.4 | 362.7 | 313 | 39.7% | 0.01 [-0.14, 0.17] |
| Herreo-Beaumont et al., 2007 | -9.2 | 10.51 | 106 | -5.5 | 11.45 | 104 | 13.1% | -0.34 [-0.61, -0.06] |
| Frestedt et al., 2008 | -10.6 | 16.31 | 19 | -7 | 23.55 | 16 | 2.2% | -0.18 [-0.84, 0.49] |
| Nieman et al., 2013 | -8.2 | 9.34 | 36 | -3 | 9.34 | 36 | 4.4% | -0.55 [-1.02, -0.08] |
| Fransen et al., 2015 | -3.9 | 12.68 | 152 | -3.9 | 12.85 | 151 | 19.1% | 0.00 [-0.23, 0.23] |
| Total | 802 | 790 | 100.0% | -0.07 [-0.17, 0.03] |
||||
|
Heterogeneity: Chi2 = 9.48, df = 6 (P=0.15); I2 = 51% Test for overall effect: Z = 1.45 (P =0.15) | ||||||||
Table 7.
The weighted mean difference and 95% confidence intervals for the effect of glucosamine on WOMAC subscale for pain stiffness [5].
Table 7.
The weighted mean difference and 95% confidence intervals for the effect of glucosamine on WOMAC subscale for pain stiffness [5].
| Study and year | Glucosamine | Placebo | Std. Mean Difference |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Total | Mean | SD | Total | Weight | IV, Fixed, 95% CI | |
| Clegg et al., 2006 | -1.4 | 2.1 | 317 | -1.5 | 2.1 | 313 | 19.3% | 0.10 [-0.23, 0.43] |
| Frestedt et al., 2008 | -0.8 | 1.9 | 14 | -0.5 | 1.5 | 9 | 8.6% | -0.30 [-1.70, 1.10] |
| Giordano et al., 2009 | -1 | 0.3 | 30 | 0 | 0.3 | 30 | 20.4% | -1.00 [-1.15, -0.85] |
| McAlindon et al., 2004 | 0.7 | 1.6 | 101 | 0.8 | 1.5 | 104 | 18.4% | -0.10 [-0.52, 0.32] |
| Pavelka et al., 2002 | -0.3 | 1.5 | 66 | 0.1 | 0.7 | 55 | 18.5% | -0.40 [-0.81, 0.01] |
| Regisnter et al., 2001 | 0 | 2.3 | 68 | 0 | 2.2 | 71 | 14.8% | 0.00 [-0.75, 0.75] |
| Total | 596 | 582 | 100.0 % | -0.30 [-0.82, 0.21] |
||||
|
Heterogeneity: Tau2 = 0.33; Chi2 = 51.22, df = 5 (P<0.00001); I2 = 90% Test for overall effect: Z = 1.15 (P = 0.25) | ||||||||
3.4. Safety
3.4.1. Adverse events
Table 8 displayed the safety and tolerability outcomes including patients withdrawn because of adverse events. There was no discernible difference between glucosamine and placebo in terms of the frequency of adverse events. In which, incidence of adverse events of using glucosamine was slightly lower than using placebo.
3.4.2. Drug interactions
Most studies showed no serious drug interactions exist [31,32]. However, there were some studies stating that using glucosamine with warfarin may increase the anticoagulation effect, but still further research is required for more information [33,34,35]. On the other hand, there was also a theory that glucosamine reduced effectiveness of diabetes medications [32,34].
4. Discussion
Our search tends to focus on studies using those two indexes because they are the most frequently used to assess the effects of glucosamine. Notably, measuring pain intensity is a commonality between WOMAC and VAS. Nevertheless, based on our research, their results showed a sizable gap. At the end of the follow-up, the VAS score had significantly improved, but the positive change in WOMAC pain was too slight to be influential. Additionally, neither the overall WOMAC score nor any of its subscales established a discernible clinical improvement. It is important to remember that the VAS global pain was thought to have better assay sensitivity than the WOMAC pain subscale, which exhibited valuable authenticity as a primary result measure [36]. Even though glucosamine has been found to mitigate discomfort, the scores in the placebo group also improved. This improvement could be the result of the arthritis’ normal progression or the effects of a placebo. Other musculoskeletal structures have been affected by this issue as well.
Most of our collected articles utilized Glucosamine sulfate rather than Glucosamine hydrochloride. Despite inconsistent findings across studies, there was a tendency that glucosamine sulfate portrayed a noticeable and clinically meaningful impact on OA at high dose [37]. According to hypothesis, glucosamine works by modifying the O-GlcNAcylation pathway, a reversible post-translational modification similar to phosphorylation that regulates protein activity, location, or stability depending on the availability of glucose. This is done by attaching N-Acetylglucosamine to the serine or threonine residues of cytosolic or nuclear proteins [37].
Our research showed that glucosamine was more effective than placeto at lessening pain. This differentiated with earlier meta-analyses that yielded conflicting findings about the symptomatic efficacy of glucosamine in treating knee osteoarthritis [8,12]. It should be highlighted that the glucosamine modifying-therapeutic effects were centered mostly in the short-term RCTs, since long-term ones found no superior advantage versus placebo [14,16,19]. Given that osteoarthritis is a chronic illness, glucosamine should be evaluated over a longer period of time to ascertain how it affects the human body. On the other hand, one of the key reason that influences one’s decision to look for medications is pain degree [38]. As a result, our study result could perhaps help individuals with knee osteoarthritis enhance their quality of life.
Using oral glucosamine sulfate (1500 mg/day) has no significant difference in the frequency of adverse events compared to placebo. Besides, adverse events reported in the glucosamine group were slightly lower than the placebo group with RR = 0.99 (95% CI 0.66, 1.23) as shown in Table 8. According to Table 9, most adverse events were affected in the gastrointestinal tract (including abdominal pain, diarrhea, dyspepsia). There were no serious adverse events reported over a period of 3-4 months based on the study duration of the majority studies. On the other hand, in another trial lasting 2-3 years of using Glucosamine, there were also no serious adverse events occurring [39]. Some people withdrew from the study due to serious adverse events were not related to the study treatment, mostly because of pre-existing or concurrent diseases.
Glucosamine has no serious drug interactions. However, using warfarin and glucosamine together may boost the anticoagulant impact according to several studies, although additional research is required. A different hypothesis suggested that glucosamine decreased the efficiency of diabetes medicines. If patients are currently using diabetes drugs or warfarin, they should inform the doctor, in case drug interactions occur.
Majority of our articles are limited within 6 months (12/17 articles). Observation on joint space narrowing was not mentioned. We focus on symptomatic effect, assessed by VAS and WOMAC indexes, rather than structural effect of glucosamine. In addition, restriciton of time might attribute to incomplete data for long-term efficacy and safety of glucosamine. Overall, most research have small sample sizes, which could limit the ability to comprehend the outcomes that have been displayed [38]. Ultimately, potential sources of inter-study heterogeneity that could have impacted our findings included the severity of OA, different formulations and the duration of therapies.
5. Conclusions
Glucosamine did show significant decreasement in global pain based on VAS scores in knee osteoarthritis patients. Besides, Glucosamine is safe. It doesn’t cause serious side effects and has no serious drug interactions. However, further studies of glucosamine are needed in patients who are taking warfarin or diabetic medicines. At the same time, doctors should also inform patients about possible interactions when using these drugs together.
References
- Colletti, A.; Cicero, A.F.G. Nutraceutical Approach to Chronic Osteoarthritis: From Molecular Research to Clinical Evidence. Int J Mol Sci 2021, 22, 12920. [Google Scholar] [CrossRef] [PubMed]
- Conrozier, T.; Lohse, T. Glucosamine as a Treatment for Osteoarthritis: What If It’s True? Front Pharmacol 2022, 13, 820971. [Google Scholar] [CrossRef] [PubMed]
- Gregori, D.; Giacovelli, G.; Minto, C.; Barbetta, B.; Gualtieri, F.; Azzolina, D.; Vaghi, P.; Rovati, L.C. Association of Pharmacological Treatments With Long-term Pain Control in Patients With Knee Osteoarthritis. JAMA 2018, 320, 2564–2579. [Google Scholar] [CrossRef]
- Ogata, T.; Ideno, Y.; Akai, M.; Seichi, A.; Hagino, H.; et al. Effects of glucosamine in patients with osteoarthritis of the knee: a systematic review and meta-analysis. Clin Rheumatol 2018, 37, 2479–2487. [Google Scholar] [CrossRef]
- Simental-Mendía, M.; Sánchez-García, A.; Vilchez-Cavazos, F.; Acosta-Olivo, C.A.; Peña-Martínez, V.M.; Simental-Mendía, L.E. Effect of glucosamine and chondroitin sulfate in symptomatic knee osteoarthritis: a systematic review and meta-analysis of randomized placebo-controlled trials. Rheumatol Int 2018, 38, 1413–1428. [Google Scholar] [CrossRef]
- Smedslund, G.; Kjeken, I.; Musial, F.; Sexton, J.; Østeråsa, N. Interventions for osteoarthritis pain: A systematic review with network meta-analysis of existing Cochrane reviews. Osteoarthr Cartil Open 2022, 4, 100242. [Google Scholar] [CrossRef]
- Ghouri, A.; Conaghan, P.G. Update on novel pharmacological therapies for osteoarthritis. Ther Adv Musculoskelet Dis 2019, 11, 1759720X19864492. [Google Scholar] [CrossRef]
- Zhu, X.; Sang, L.; Wu, D.; Rong, J.; Jiang, L. Effectiveness and safety of glucosamine and chondroitin for the treatment of osteoarthritis: a meta-analysis of randomized controlled trials. J Orthop Surg Res 2018, 13, 170. [Google Scholar] [CrossRef]
- Bruyère, O.; Altman, R.D.; Reginster, J.-Y. Efficacy and safety of glucosamine sulfate in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin Arthritis Rheum 2016, 45, S12–S17. [Google Scholar] [CrossRef]
- Notes need to know about glucosamine. Available online: http://bachmai.gov.vn/tin-tuc-va-su-kien/thong-tin-thuoc-menuleft-124/6734-mot-so-dieu-can-biet-ve-glucosamin.html (accessed on 31 March 2023).
- MOH. Circular No. 20/2022/TT-BYT. 2022. Ha Noi.
- Runhaar, J.; Rozendaal, R.M.; Middelkoop, M.v.; Bijlsma, H.J.W.; Doherty, M.; et al. Subgroup analyses of the effectiveness of oral glucosamine for knee and hip osteoarthritis: a systematic review and individual patient data meta-analysis from the OA trial bank. Ann Rheum Dis 2017, 76, 1862–1869. [Google Scholar] [CrossRef]
- Giordano, N.; Fioravanti, A.; Papakostas, P.; Montella, A.; Giorgi, G.; Nuti, R. The efficacy and tolerability of glucosamine sulfate in the treatment of knee osteoarthritis: A randomized, double-blind, placebo-controlled trial. Curr Ther Res Clin Exp 2009, 70, 185–196. [Google Scholar] [CrossRef]
- Rozendaal, R.M.; Koes, B.W.; Osch, G.J.V.M.v.; Uitterlinden, E.J.; Garling, E.H.; et al. Effect of glucosamine sulfate on hip osteoarthritis: a randomized trial. Ann Intern Med 2008, 148, 268–277. [Google Scholar] [CrossRef]
- Herrero-Beaumont, G.; Ivorra, J.A.R.; Trabado, M.D.C.; Blanco, F.J.; Benito, P.; et al. Glucosamine sulfate in the treatment of knee osteoarthritis symptoms: a randomized, double-blind, placebo-controlled study using acetaminophen as a side comparator. Arthritis Rheum 2007, 56, 555–567. [Google Scholar] [CrossRef]
- Fransen, M.; Agaliotis, M.; Nairn, L.; Votrubec, M.; Bridgett, L.; et al. Glucosamine and chondroitin for knee osteoarthritis: a double-blind randomised placebo-controlled clinical trial evaluating single and combination regimens. Ann Rheum Dis 2015, 74, 851–858. [Google Scholar] [CrossRef]
- Hughes, R.; Carr, A. A randomized, double-blind, placebo-controlled trial of glucosamine sulphate as an analgesic in osteoarthritis of the knee. Rheumatology (Oxford) 2002, 41, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Pavelká, K.; Gatterová, J.; Olejarová, M.; Machacek, S.; Giacovelli, G.; Rovati, L.C. Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Arch Intern Med 2002, 162, 2113–2123. [Google Scholar] [CrossRef]
- Sawitzke, A.D.; Shi, H.; Finco, M.F.; Dunlop, D.D.; Harris, C.L.; et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis 2010, 69, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.Y.; Deroisy, R.; Rovati, L.C.; Lee, R.L.; Lejeune, E.; et al. Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet 2001, 357, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Rindone, J.P.; Hiller, D.; Collacott, E.; Nordhaugen, N.; Arriola, G. Randomized, controlled trial of glucosamine for treating osteoarthritis of the knee. West J Med 2000, 172, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Kwoh, C.K.; Roemer, F.W.; Hannon, M.J.; Moore, C.E.; Jakicic, J.M.; Guermazi, A.; Green, S.M.; Evans, R.W.; Boudreau, R. Effect of oral glucosamine on joint structure in individuals with chronic knee pain: a randomized, placebo-controlled clinical trial. Arthritis Rheumatol 2014, 66, 930–939. [Google Scholar] [CrossRef]
- McAlindon, T.; Formica, M.; LaValley, M.; Lehmer, M.; Kabbara, K. Effectiveness of glucosamine for symptoms of knee osteoarthritis: results from an internet-based randomized double-blind controlled trial. Am J Med 2004, 117, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Madhu, K.; K Chanda, M.J.S. Safety and efficacy of Curcuma longa extract in the treatment of painful knee osteoarthritis: a randomized placebo-controlled trial. Inflammopharmacology 2013, 21, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.G.; Beyer, N.; Hansen, M.; Holm, L.; Aagaard, P.; Mackey, A.L.; Kjaer, M. Nonsteroidal anti-inflammatory drug or glucosamine reduced pain and improved muscle strength with resistance training in a randomized controlled trial of knee osteoarthritis patients. Arch Phys Med Rehabil 2011, 92, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Frestedt, J.L.; Walsh, M.; Kuskowski, M.A.; Zenk, J.L. A natural mineral supplement provides relief from knee osteoarthritis symptoms: a randomized controlled pilot trial. Nutr J 2008, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Clegg, D.O.; Reda, D.J.; Harris, C.L.; Klein, M.A.; O’Dell, J.R.; et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med 2006, 354, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Cibere, J.; Kopec, J.A.; Thorne, A.; Singer, J.; Canvin, J.; et al. Randomized, double-blind, placebo-controlled glucosamine discontinuation trial in knee osteoarthritis. Arthritis Rheum 2004, 51, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C.; Shanely, R.A.; Luo, B.; Dew, D.; Meaney, M.P.; Sha, W. A commercialized dietary supplement alleviates joint pain in community adults: a double-blind, placebo-controlled community trial. Nutr J 2013, 12, 154. [Google Scholar] [CrossRef]
- Noack, W.; Fischer, M.; Förster, K.K.; Rovati, L.C.; Setnikar, I. Glucosamine sulfate in osteoarthritis of the knee. Osteoarthritis Cartilage 1994, 2, 51–59. [Google Scholar] [CrossRef]
- MOH. Drugbank. .
- Williams, C.; Ampat, G. Glucosamine Sulfate; StatPearls: Treasure Island (FL), 2023. [Google Scholar]
- Drug interaction report Glucosamine and Warfarin. Available online: https://www.drugs.com/interactions-check.php?drug_list=1182-0,2311-0 (accessed on 31 March 2023).
- Dahmer, S.; Schiller, R.M. Glucosamine. Am Fam Physician 2008, 78, 471–476. [Google Scholar]
- Knudsen, J.F.; Sokol, G.H. Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and MedWatch database. Pharmacotherapy 2008, 28, 540–548. [Google Scholar] [CrossRef]
- Costa, B.R.d.; Saadat, P.; Basciani, R.; Agarwal, A.; Johnston, B.C.; Jüni, P. Visual Analogue Scale has higher assay sensitivity than WOMAC pain in detecting between-group differences in treatment effects: a meta-epidemiological study. Osteoarthritis Cartilage 2021, 29, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Herrero-Beaumont, G.; Largo, R. Glucosamine and O-GlcNAcylation: a novel immunometabolic therapeutic target for OA and chronic, low-grade systemic inflammation? Ann Rheum Dis 2020, 79, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, G.; Nedeljkovic, B.; Trajkovic, G.; Rasic, D.; Mirkovic, Z.; Pajovic, S.; Grbic, R.; Sipetic, S.; Vujcic, I. Pain, Physical Function, Radiographic Features, and Quality of Life in Knee Osteoarthritis Agricultural Workers Living in Rural Population. Pain Res Manag 2019, 7684762. [Google Scholar] [CrossRef]
- Lee, Y.H.; Woo, J.-H.; Choi, S.J.; Ji, J.D.; Song, G.G. Effect of glucosamine or chondroitin sulfate on the osteoarthritis progression: a meta-analysis. Rheumatol Int 2010, 30, 357–363. [Google Scholar] [CrossRef] [PubMed]
Table 2.
Risk of bias following Cochrane criteria.
| No. | References | Low / High |
|---|---|---|
| 1 | Clegg et al., 2006 [27] | Low |
| 2 | Fransen et al., 2015 [16] | Low |
| 3 | Giodarno et al., 2009 [13] | Low |
| 4 | Madhu et al., 2013 [24] | Low |
| 5 | Petersen et al., 2011 [25] | Low |
| 6 | Rindone et al., 2000 [21] | Low |
| 7 | Cibere et al., 2004 [28] | Low |
| 8 | Frestedt et al., 2008 [26] | Low |
| 9 | Herrero-Beaumont et al.,2007 [15] | Low |
| 10 | Kwoh et al., 2014 [22] | Low |
| 11 | McAlindon et al., 2004 [23] | Low |
| 12 | Pavelka et al., 2002 [18] | Low |
| 13 | Regisnter et al., 2001 [20] | Low |
Table 8.
Relative risk, 95% confidence intervals and weight of adverse events (including patients withdrawn caused of adverse events) comparison between glucosamine and placebo [8].
Table 8.
Relative risk, 95% confidence intervals and weight of adverse events (including patients withdrawn caused of adverse events) comparison between glucosamine and placebo [8].
| Study ID | Relative risk (RR) 95% CI |
Weight % |
|---|---|---|
| Reginster et al., 2001 | 1.07 [0.70, 1.65] | 14.26 |
| Pavelka et al., 2002 | 1.05 [0.46, 2.39] | 6.57 |
| McAlindon et al., 2004 | 0.50 [0.07, 3.75] | 1.83 |
| Clegg et al., 2006 | 0.71 [0.31, 1.60] | 8.97 |
| Herrero-Beaumont et al., 2007 | 0.54 [0.19, 1.57] | 6.18 |
| Rozendaal et al., 2008 | 2.29 [0.26, 20.13] | 0.71 |
| Fransen et al., 2015 | 7.33 [0.96, 56.00] | 0.33 |
| Kwoh 2014 | 0.39 [0.13, 1.20] | 3.53 |
| Subtotal (I 2 = 24.3%, p = 0.236) | 0.90 [0.66, 1.23] | 42.37 |
Table 9.
Frequency of adverse events reported in patients using Glucosamine Sulphate.
| Study ID | Glucosamine sulphate (N) | Adverse events | ||||||
|---|---|---|---|---|---|---|---|---|
| GI | CV | CNS | MU | Skin | Infections | Others | ||
|
Pavelkaet al., 2002 [18] |
101 | 25 | 23 | ND | 30 | 10 | 29 | 14 |
| Noack et al., 1994 [30] |
126 | 5 | 0 | 2 | 0 | 1 | 0 | 0 |
| Reginster et al., 2001 [20] | 106 | 27 | 21 | 31 | ND | ND | ND | 4 |
| McAlindon et al., 2004 [23] | 101 | 4 | ND | 2 | 5 | ND | ND | 7 |
| Herrero-Beaumont et al., 2007 [15] |
106 | 11 | ND | 3 | 10 | ND | 12 | 8 |
| Rozendaal et al., 2008 [14] | 111 | 58 | 21 | 66 | ND | ND | ND | 7 |
| Hughes et al., 2002[17] | 39 | 0 | ND | 1 | 9 | 0 | 1 | 8 |
* Abbreviations: ND: no data; GI: gastrointestinal; CV: cardiovascular; CNS: central nervous system; MU: musculoskeletal.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



