
Submitted:
08 June 2023
Posted:
09 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: SARS-CoV-2 infection was first reported in 2019 and has since spread throughout the world. This is a cross-sectional study in cooperation with 118 Department of Pre-Hospital and Territorial Emergency (118 SET) of Taranto City and the University of Bari, Aldo Moro, and the School of Medicine from Italy. We conducted a study on how the COVID-19 epidemics evolved and how it was contained by different countermeasures by taking into account data showing socio-demographic and that older persons, as well as individuals with comorbidities and poor metabolic health, and people coming from economically depressed areas with lower quality of life in general, are more likely to develop severe COVID-19 infection.
Objective: Examine the association between county-level socio-demographic risk factors and COVID-19 incidence and mortality, determining the possible emo-biological markers, ferritin, and lymphocytes, that could be indicative of SARS-CoV-2 infection.
Methods: Descriptive cross-sectional study on 600 patients examined and treated at general hospital Ninh Thuan from January to September 2022.
Results: 33/600 patients were confirmed to be infected with SARS-CoV-2 (5.5%), males 4.8% and females 5.8%, the median age of infected patients is 36 years. Most infections were mild (75.8%). Our results revealed that the structure and the spatial arrangement of socio-demographic arrangements are important either as epidemiological determinants or as disease markers. Conclusion: Approximately 5.5% of patients infected with SARS-CoV-2 come to examination and treatment at the hospital, these findings suggested that possible infection rate in the burden of the COVID-19 pandemic, the sociodemographic risk factors, and their root causes must be addressed. In addition, lab results obtained from affected patients showed that lymphocytes and ferritin could be considered traits of mild COVID-19 infection.
Keywords:
COVID-19
; SARS-CoV-2
; socio-demographic analysis
; Ferritin
; Lymphocytes
; General hospital Ninh Thuan province
Introduction
Though COVID-19 has stopped spreading around the world, still we are facing post-infection consequences often extremely serious. More than 600 million confirmed of COVID-19 (F0), including 6.564.556 deaths, were reported to the World Health Organization (WHO), Southeast Asia with more than 60 million people infected and nearly 800.000 deaths and in Vietnam, there have been more than 11 million cases of infection with 43.000 deaths [1].
In the context of the ongoing pandemic, the spread of COVID-19 placed a significant burden on local health care systems and significantly contributed high to mortality rates. Timely and effective intervention were essential to reduce rates infection and death during the COVID-19 outbreak. Such interventions included rapid identification of the infections, followed by immediately applying of control measures, and daily monitoring procedures. An effective screening tool was based on blood test, and including some white blood cells, platelets, CRP, Ferritin [2,3].
Scientists and labs allover the World has conducted a huge number of researches on COVID-19, the described clinical and subclinical characteristics, epidemiological features were of big help in unsterstunding this pathology. In Ninh Thuan province in general and at the General Hospital of Ninh Thuan Province in particular, collected data and outcomes showed quite unique scenario. In general, though the reported rate of infection was high in the reality the confirmed infection numbers told a different story, numbers were relatively lower; we observed modest COVID-19 incidence despite consistent exposure at work or environmentally. Community and work contact was strongly associated with infections, however, though the high-risk exposure the estimated rate of COVID-19 patients coming for examination and treatment was no more than 14% as confirmed by similar studies around the world [4,5].
Therefore with this paper we have tried to answer to the following question, what was the actual rate of SARS-CoV-2 infection in patients who come for examination and treatment at General Hospital Ninh Thuan Province? To answer the above question, we conducted research on the topic following two objectives:
1. Determine prevalence of patients positive for SARS-CoV-2 at General Hospital of Ninh Thuan Province in 2022, with a general focus on the importance of socio-demographic patterns
2. Surveying concentration of some subclinical tests in patients positive for SARS-CoV-2 with a general focus on lynphocytes and ferritin patterns in low-medium sever infected patients.
Methods
Subjects of study
All patients hospitalized at General Hospital Ninh Thuan Province from January 1 to end September 2022.
Selection criteria: All patients hospitalized at General Hospital Ninh Thuan Province from January 1 to end September 2022, suspected of having COVID-19 are indicated for SARS-CoV-2 test (rapid test or RT-PCR).
Exclusion criteria: The patient was negative (rapid test or RT-PCR) at the following tests during patient follow-up
Methods
Study Design: Cross-sectional study
Sample size:
n: minimum sample size; Z2(1-α/2) = 1,96; p = 0,15 [5]; d = 0,03; The sample size we calculated is 544 but the actual number of patients studied is 600.
Sampling method: Convenience sample selection, consecutive.
Statistical analysis
SPSS 22.0 statistical software was used for all calculations. Qualitative variables are expressed as percentages (%). Use medians and percentile ranges (25 and 75) to describe quantitative variables that are not normally distributed.
Chi-square test or Fischer-exact test for categorical variables and student’s t-test or Mann Whitney U test for continuous variable as appropriate. P < 0.05 were considered as statistically significant.
Results
Association of Population socio-demographic condition and Health Care Measures With COVID-19 Incidence
Most of the population socio-demographic data such as age, sex or health care availability measures adopted by the Government bodies were significantly associated with lower COVID-19 incidence (Table 1, Table 2, Table 3 and Table 4). Age rate was significantly associated with COVID-19 incidence (IRR, 1.02; 95% CI, 1.01-1.02; P > 0.05). As expected, life expectancy was significantly associated with mortality, such that an additional year of life expectancy was associated with lower mortality rates (IRR, 0.95; 95% CI, 0.93-0.97; P > 0.05).
| TABLE 1 | Demographic characteristics of the study population(N=600) | |||
| Characteristics | Frequency | (%) | ||
| Gender | ||||
| Male | 188 | 31.3 | ||
| Female | 412 | 68.7 | ||
| Age group | ||||
| 0 - 9 | 40 | 6.7 | ||
| 10 - 19 | 45 | 7.5 | ||
| 20 - 29 | 161 | 26.8 | ||
| 30 - 39 | 143 | 23.8 | ||
| 40 - 49 | 53 | 8.8 | ||
| 50 - 59 | 56 | 9.3 | ||
| 60 - 69 | 58 | 9.7 | ||
| 70 - 79 | 29 | 4.8 | ||
| ≥ 80 | 15 | 2.5 | ||
| Median age (25th - 75th): 32 (24 - 51) year old | ||||
| TABLE2 | Prevalenceof SARS-CoV-2 positivity | ||||
| Gender | Number tests | (+) | (%) |
OR (95% CI) |
P |
| Male | 188 | 9 | 4.8 | 0.8 (0.4 - 1.8) |
0.6 |
| Female | 412 | 24 | 5.8 | ||
| Total | 600 | 33 | 5.5 | ||
| TABLE3 | Prevalenceof SARS-CoV-2 positivityage group | ||
| Age group | Number tests | (+) | (%) |
| 0 - 9 | 40 | 2 | 5.0 |
| 10 - 19 | 45 | 1 | 2.2 |
| 20 - 29 | 161 | 6 | 3.7 |
| 30 - 39 | 143 | 12 | 8.4 |
| 40 - 49 | 53 | 4 | 7.5 |
| 50 - 59 | 56 | 1 | 1.8 |
| 60 - 69 | 58 | 4 | 6.9 |
| 70 - 79 | 29 | 2 | 6.9 |
| ≥ 80 | 15 | 1 | 6.7 |
| Total | 600 | 33 | 5.5 |
| TABLE 4 | Disease severity and treatment outcome (N=33) | |||
| Characteristics | Frequency | (%) | ||
| Disease severity | ||||
| Asymptomatic | 0 | 0.0 | ||
| Mild | 25 | 75.8 | ||
| Moderate | 7 | 21.2 | ||
| Severe | 1 | 3.0 | ||
| Critical | 0 | 0.0 | ||
| Treatment outcome | ||||
| Recover | 33 | 100 | ||
| Death | 0 | 0.0 | ||
Laboratory tests
In this study, the median white blood cell count in patients with COVID-19 was 4.600, lymphocytes 1.100, platelets 180.000, hemoglobin 12.2 g/dl, CRP > 10 mg% only 9.1%, ferritin 200 ng/mL. There was a statistically significant difference in the median number of WBC, lymphocytes, ferritin between the 2 groups, mild and moderate with severe (P < 0.05). Results of Chen et al, the whole blood count on admission of 3 (30%) moderate cases showed mild leucopenia, while white blood cell counts were normal or slightly increased above the upper limit of normal in all the severe cases, whereas lymphocyte counts were significantly lower in severe cases (0.7 × 109/L) than moderate cases (1.1 × 109/L). Lymphopenia (lymphocyte count <0.8 × 109/L) was developed in 8 (72.7%) severe cases and only 1 (10.0%) moderate case (P = 0.008). Overall, severe cases had increased WBC counts (P = 0.003) but lower lymphocyte counts (P = 0.049) [2]. Wang et al. showed that the median platelet count in patients with COVID-19 was 163 x 109 /L and there was no significant difference (P > 0.05) in the ICU and non-ICU groups [15]. Similar to us, Guan et al., the median hemoglobin in patients with COVID-19 was 13.4 g/dl and no difference was found between the severe and non-severe. However, CRP ≥ 10 mg/l accounts for 60.7% in study of Guan et al. our CRP > 10 mg% only accounts for 9.1% (Table 4) [15,16,17,18,19] The reason there is a difference here is because the author's research was conducted in the early stages of the COVID-19 epidemic, no patient was vaccinated COVID-19, at the same time, in this study of the author, there were many patients with severe disease, the mortality rate was 1.4% [16]. In our study, there was only 1 patient (3.0%) with severe severity and mortality rate of 0.0% (Table 3). Chen et al., ferritin concentration in severe cases was significantly higher than in moderate cases (P < 0.05) [2].
Prevalence of positive for SARS-CoV-2 in patients examined and treated at the Hospital
Females accounted for 68.7%, mostly in the age group of 20-29 years (26.8%) and 30-39 years old (23.8%).
The prevalence of patients positive for SARS-CoV-2 was 5.5% (95% CI: 0.3 - 7.6) in the overall sample. Prevalence positive in Female was 5.8% and Male was 4.8% (P > 0.05).
The positive prevalence was highest in the age group 30-39 (8.4%) and 40-49 years old (7.5%). The median age of the positive group was 36 years and the negative group was 32 years (IRR, 1.02; 95% CI, 1.01-1.02; P > 0.05).
The majority of COVID-19 patients had mild disease (75.8%), 1 patient was severe (3.0%) and no patient was in critical condition. The recover rate at Ninh Thuan Provincial General Hospital is 100%.
Concentrations of some laboratory tests
| TABLE 5 | Concentrations of some laboratory tests | |||||||||||
| Tests | Total(n=33) | Mild(n=25) | Moderate and Severe (n=8) | p | ||||||||
| White Blood Cell(/mm3) | ||||||||||||
| < 4000 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0.05 | |||||
| 4000 - 10.000 | 31 | 93.9 | 25 | 100 | 6 | 75.0 | ||||||
| > 10.000 | 2 | 6.1 | 0 | 0.0 | 2 | 25.0 | ||||||
| Median | 4.600 | 4.500 | 7.500 | <0.01 | ||||||||
| 25th - 75th | 4.400 - 5.000 | 4.300 - 4.600 | 6.000 - 13.500 | |||||||||
| Lymphocytes (/mm3) | ||||||||||||
| < 1.500 | 18 | 54.5 | 11 | 44.0 | 7 | 87.5 | 0.04 | |||||
| Median | 1.100 | 1.600 | 700 | <0.01 | ||||||||
| 25th - 75th | 800 - 2.000 | 1.100 - 2.000 | 625 - 800 | |||||||||
| Platelet Count(/mm3) | ||||||||||||
| < 150.000 | 20 | 60.6 | 14 | 56.0 | 6 | 75.0 | 0.3 | |||||
| Median | 180.000 | 180.000 | 205.000 | >0.05 | ||||||||
| 25th - 75th | 127.500 - 200.000 | 120.000 - 200.000 | 147.500 - 243.750 | |||||||||
| Hemoglobin (g/dl) | ||||||||||||
| Median | 12.2 | 12.2 | 12.6 | >0.05 | ||||||||
| 25th - 75th | 11.0 - 13.1 | 11.1 - 13.2 | 11 - 13 | |||||||||
| CRP (mg%) | ||||||||||||
| CRP > 10 | 3 | 9.1 | 1 | 4.0 | 2 | 25.0 | 0.1 | |||||
| CRP ≤ 10 | 30 | 90.9 | 24 | 96.0 | 6 | 75.0 | ||||||
| Ferritin (ng/mL) | ||||||||||||
| Median | 200 | 170 | 300 | <0.01 | ||||||||
| 25th - 75th | 150 - 275 | 145 - 256 | 273 - 348 | |||||||||
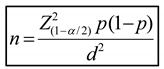
Figure 1.
Lymphocyte value determine disease severity.
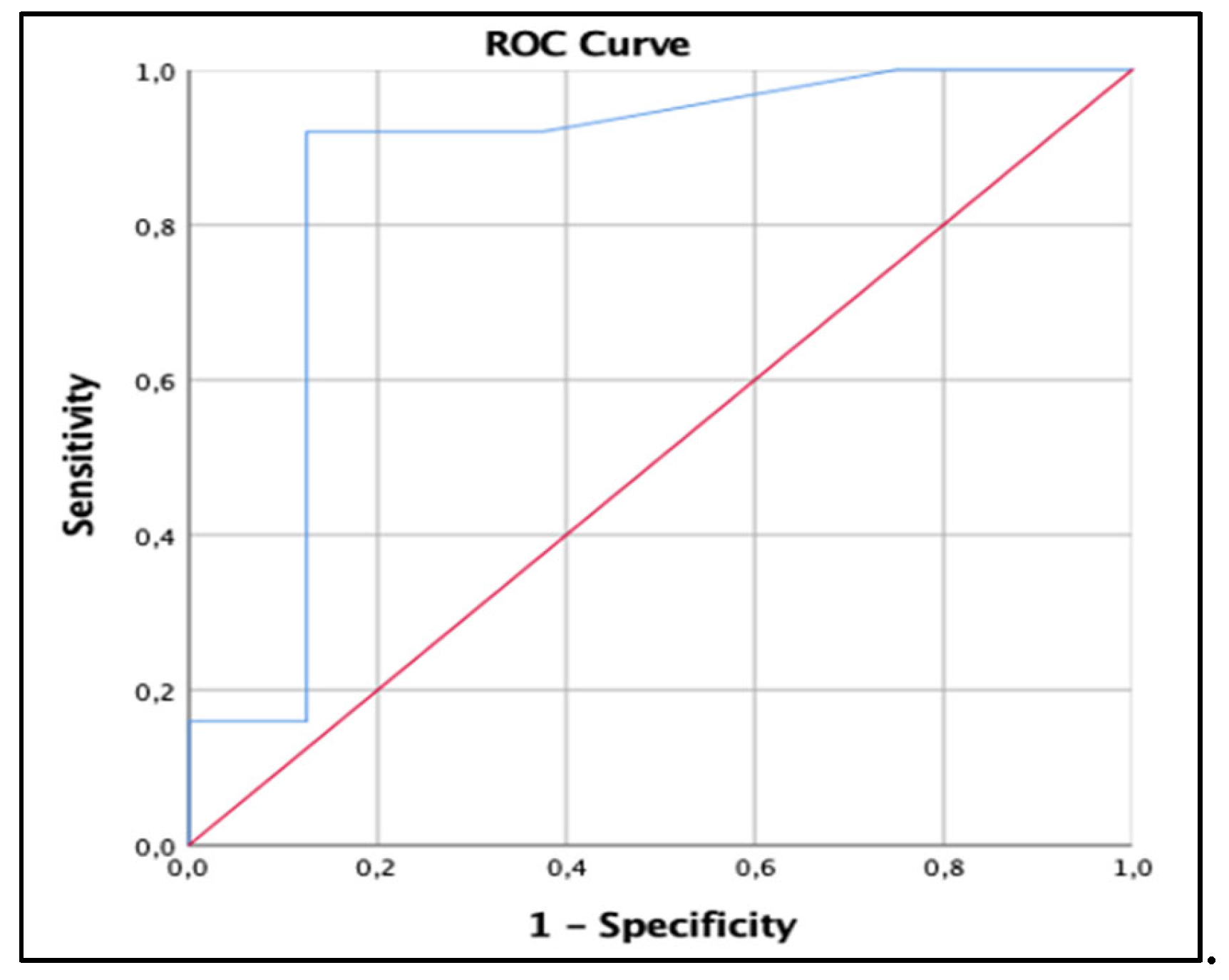
Figure 2.
Ferritin value determine disease severity.
The median white blood cell count in patients with COVID-19 was 4.600, lymphocytes 1.100, platelets 180.000, hemoglobin 12.2 g/dl, CRP > 10 mg% only 9.1%, ferritin 200 ng/mL. There was a statistically significant difference in the median number of WBC, lymphocytes, ferritin between the 2 groups, mild and moderate with severe (P < 0.05).
Discussion
Prevalence of positive for SARS-CoV-2, a socio-demographic point of view
This study aimed to determine the relationship between socio-demographic factors, the adherence to social recommendations and the effective rate of positive cases to COVID-19 during the pandemic in Ninh Thuan General Hospital of Ninh Thuan province, Vietnam. The results showed that positives were closely adherent to specific social-demographic traits of Vietnam together with the possible distancing recommendations ruled by the Central Government and Provincial Health bodies. Despite the high rate of adherence to social distancing recommendations in the whole population, low rates of infection were observed concomitantly to precise socio-demographic patterns that had a direct impact on the response to COVID-19 in terms of numbers of infections, such the age. According to the multiple linear regression model, age was the most important determinant of adherence to behavioral recommendations, followed by occupation, sex, awareness, and history of metabolic illness [20].
Therefore, the need for this analysis was also to determine the influences of socio-demographic variables in contributing to the increased number of COVID-19 cases in different "hotspot" areas of the world. With such information, the authorities may easily understand, develop and implement the needed measures to minimize and handle the increased number of cases in these areas. This would help in settling and plan the resources in more feasible way, such as the creation of quarantine sites, distribution of informative pamphlets and countermeasures to be adopted by the population, and the building of COVID-19 health-care spots to help contain and the spread the virus [20].
The socio-demographic planning plays a crucial role in revealing involving pattern of COVID-19 positive cases and deaths globally. The aging factor plays a crucial role in controlling COVID-19 deaths and spreading. For instance the high number of COVID-19 deaths and infection in Italy have to be associated with the demographic values where the median age of the population in Italy is 46.5 years with almost quarter is over the age of 65. Interesting, in accordance with the World Health Organization, age was at least during the first two waves of COVID-19 infection in Europe, a key factor [19,20]. More than 95% of people deceased were over 60, comorbidities are usually something related to old age therefore long-time illness and existing disease history are also found associated with COVID-19 deaths. A USA study found that occupations also have had a significance in explaining few aspects related to COVID-19 pandemic, as people with high-level social status with more often social interaction were more vulnerable to be infected to the virus [20].
Many studies have found people with metabolic condition such as diabetes to be at an increased risk of COVID-19 compared to individuals without diabetes. In general, at least during the first period of pandemic males and older adults were included among the risk factors associated with COVID-19; however, successively other results showed that the positive prevalence of SARS-CoV-2 in female (5.8%) and in male (4.8%) were almost equally distributed (P>0.05). Similarly, in Vietnam but not in Italy we also found no association between age and SARS-CoV-2. Our group in Italy during the same period of time showed compatible results with Setiadi et al., the oucomes showed that prevalence for COVID-19 was higher in the group > 60 years old (29.6%), followed by the group 41-60 years old (24.2%) and lowest observed in children under five years (11.0%) [6,7]. At the beginning of the pandemic, the elderly were the most vulnerable group to infection as the risk of infectivity increases with age [5,8,11,12]. As the pandemic progressed, many studies found evidence that younger adults likely contribute to community transmission of COVID-19. Different studies confirmed a switch in age trend primarily seen in youngsters and adult <65 that could be seen in the late stage of the COVID-19 pandemic[14,15]. Explanation may reside that these groups dominate the population size and case numbers at least in western countriesm China and south America. In particular, they are more engaged in social activities than other age groups. Some author found that during May-August 2020, the median age of COVID-19 cases in the US declined from 46 years in May to 37 years in July, and 38 years in August. People aged 20-29 years accounted for the largest proportion of total cases (> 20%) during June-August [13,14]. Our research, the median age of the positive group was 36 years and the negative group was 32 years (P > 0.05).
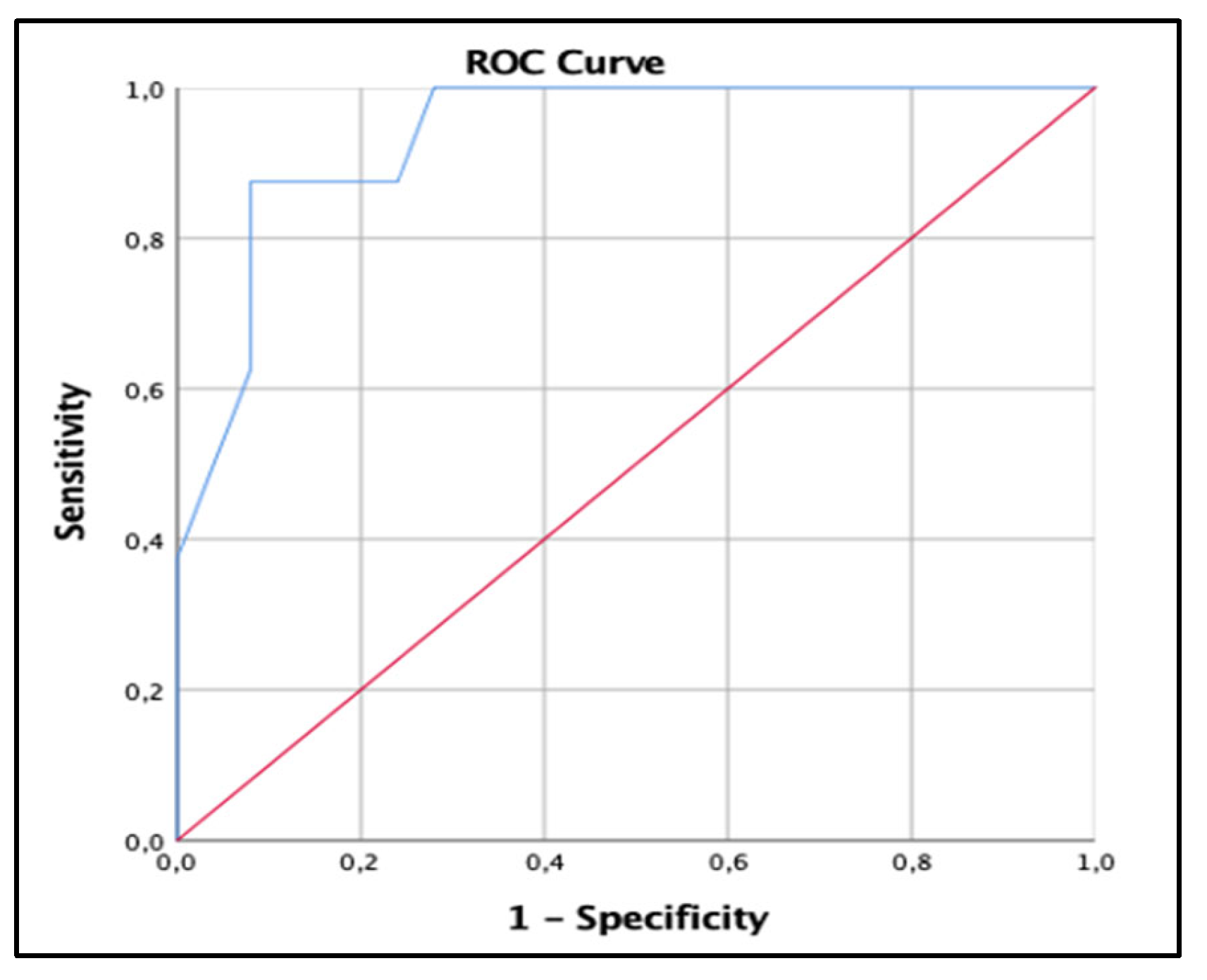
Despite its small land surface area, Vietnam it’s one of the world’s most density populated area. However, the Ninh Thuan region is one of the lowest densely populated in Vietnam, with just 178.000 person/sq km in 2021 with a total population of 679,467, the region's female and male population is practically equivalent. More than half of the population, are under the age of 38 and from the working class, fishing and agriculture. Even though international migration is low, migrants to big cities such as Ho Chi Minh City, Danang and Hue outnumber those from outside the area [21]. We agreed on the fact that despite those studies’ important advancements, most of them included participants irrespectively of their potential symptomatology, the specific prevalence of different COVID-19 variants, the associated symptoms (e.g., cough, fatigue, aches, ageusia, anosmia or fever), and the country’s population average age. We have to point-out that the average age between the different areas play a key role in assessing and understanding the data. Vietnam for instance, has a young population if compared to both Germany and Italy, more than half of the people living in Vietnam are under 35 years old, very close to USA population which seem to under 38 years old. Due to this, the sociodemographic and clinical characteristics of individuals diagnosed with COVID-19, the general outcomes may explain current conflicting findings (fig.3,4,5) [21].
In this study, the prevalence of patients positive for SARS-CoV-2 was 5.5% (95% CI: 0.3 - 7.6) in the overall sample (Table 2). Situation worldwide told sometimes different stories [5]. Setiadi et al, in Indonesia, of the 64,364 swab specimens tested, 15.7% (n = 10,130) were positive for SARS-CoV-2 [6]. Balzanelli et al, Jacob et al., respectively in Italy and Germany, the prevalence in symptomatic patients monitored in their hospitals facilities were approximately the same 13.8% and 17% respectively [4,5,6,7,8]. Meanwhile, the results of Mani et al. In Seattle-USA, the positive rate of SARS-CoV-2 was 5.3% [9], similar to ours in Vietnam (5.5%).
In this study, the general distribution of affected patients showed that female accounted for 68.7% and male was 31.3%, mostly in the age group of 20-29 years old (26.8%) and 30-39 years old (23.8%), median age is 32 years , prevalence and some related factors in symptomatic patients monitored at general hospitals in Germany, female accounted for 54.7% and mean age was 44.6 years. In the other hand, our group in Italy showed quite different scenario, the patients reporting the COVID-19 infection symptoms were divided into these age groups indicating a net majority of males compared to female (74 vs 26%), 0-9 years (1.70%), 10-19 years (3.80 %), 20-34 years (13.19 %), 35-59 years (36.66 %), 60-69 years (14.29 %), 70-79 years (15.08 %), 80-89 years (11.99%), ≥ 90 years (3.30%) [5].
Figure 3.
Vietnam population average age.
Figure 4.
USA population average age.
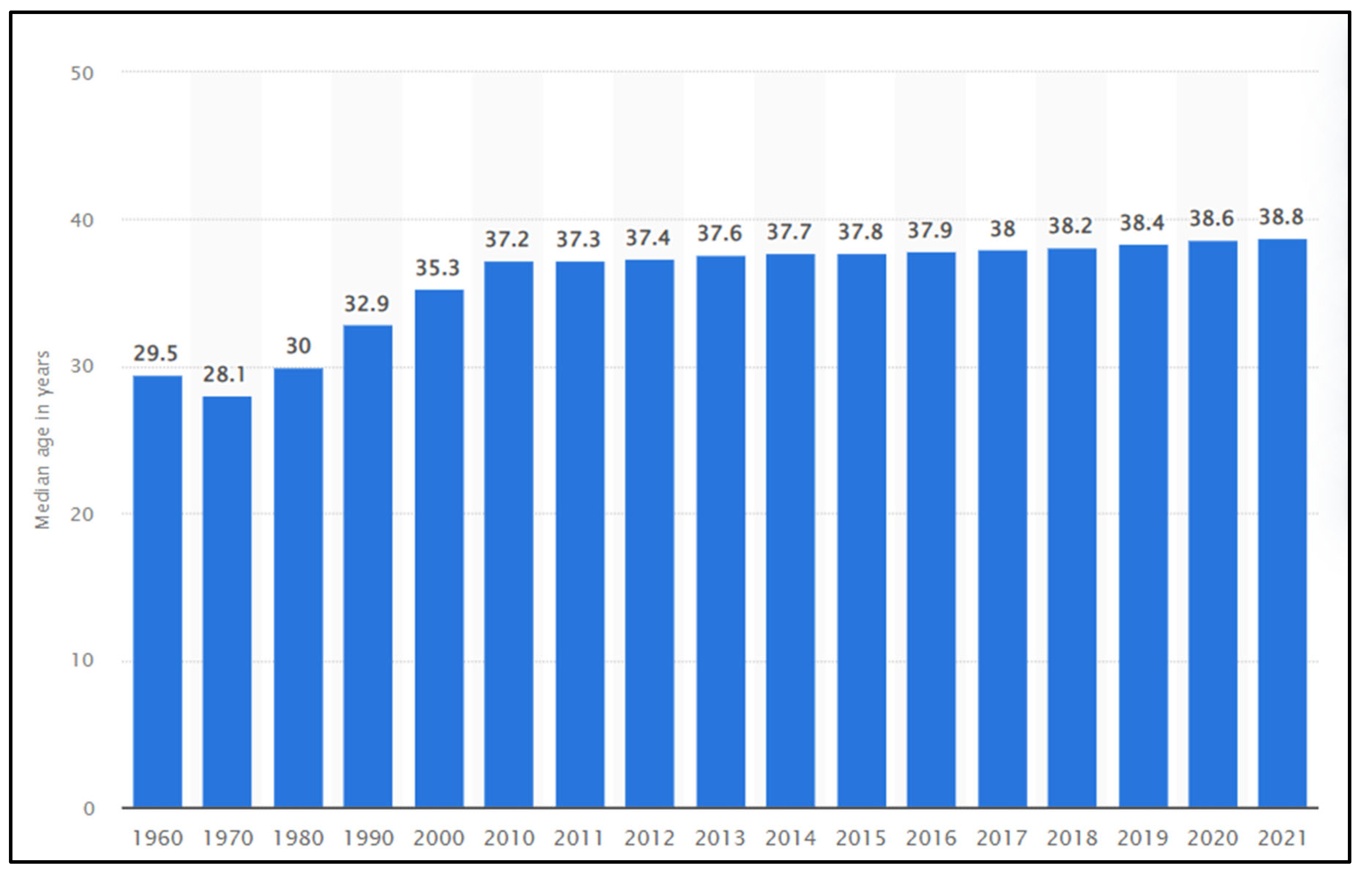
Figure 5.
.Italian population average age.
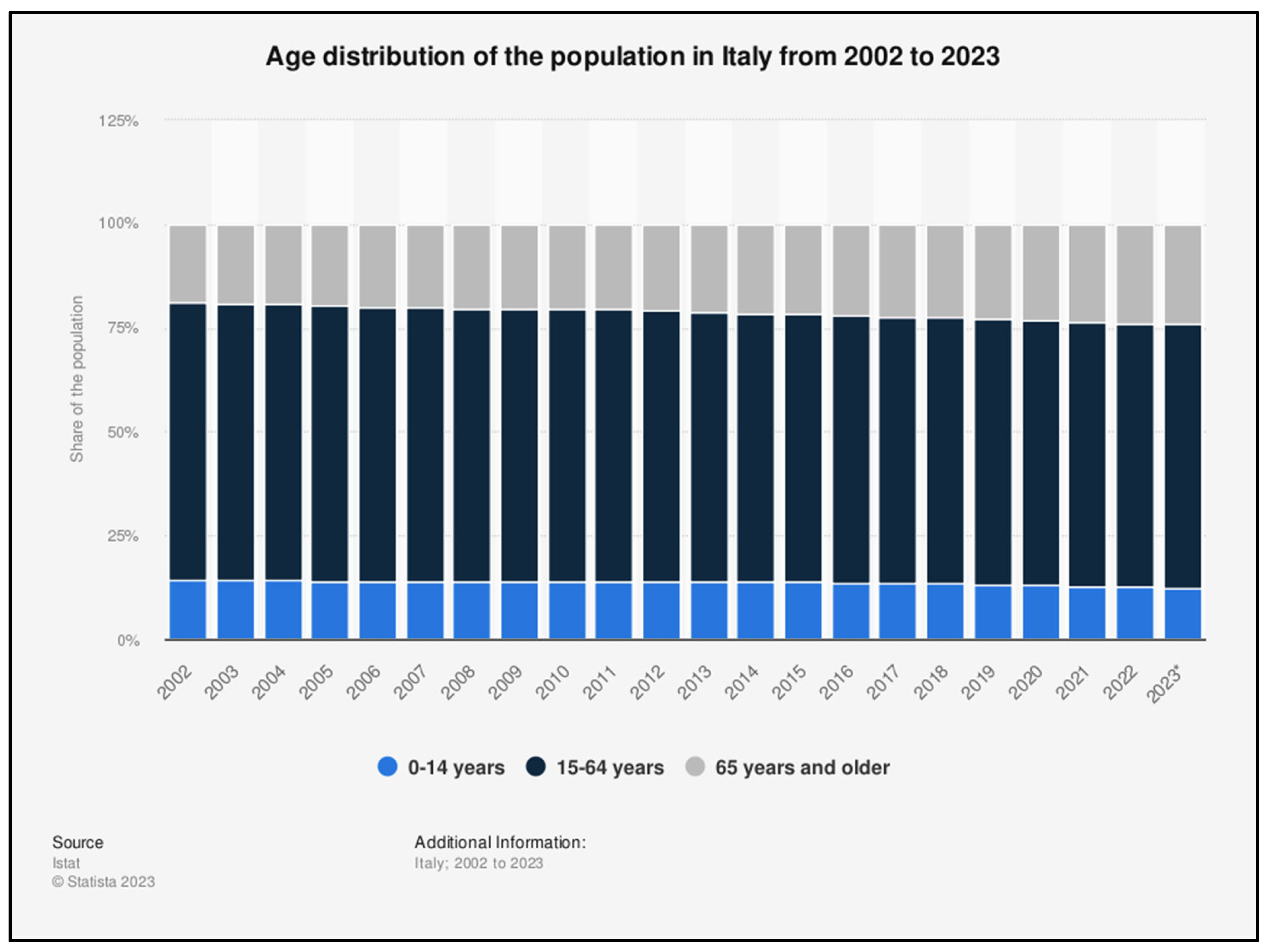
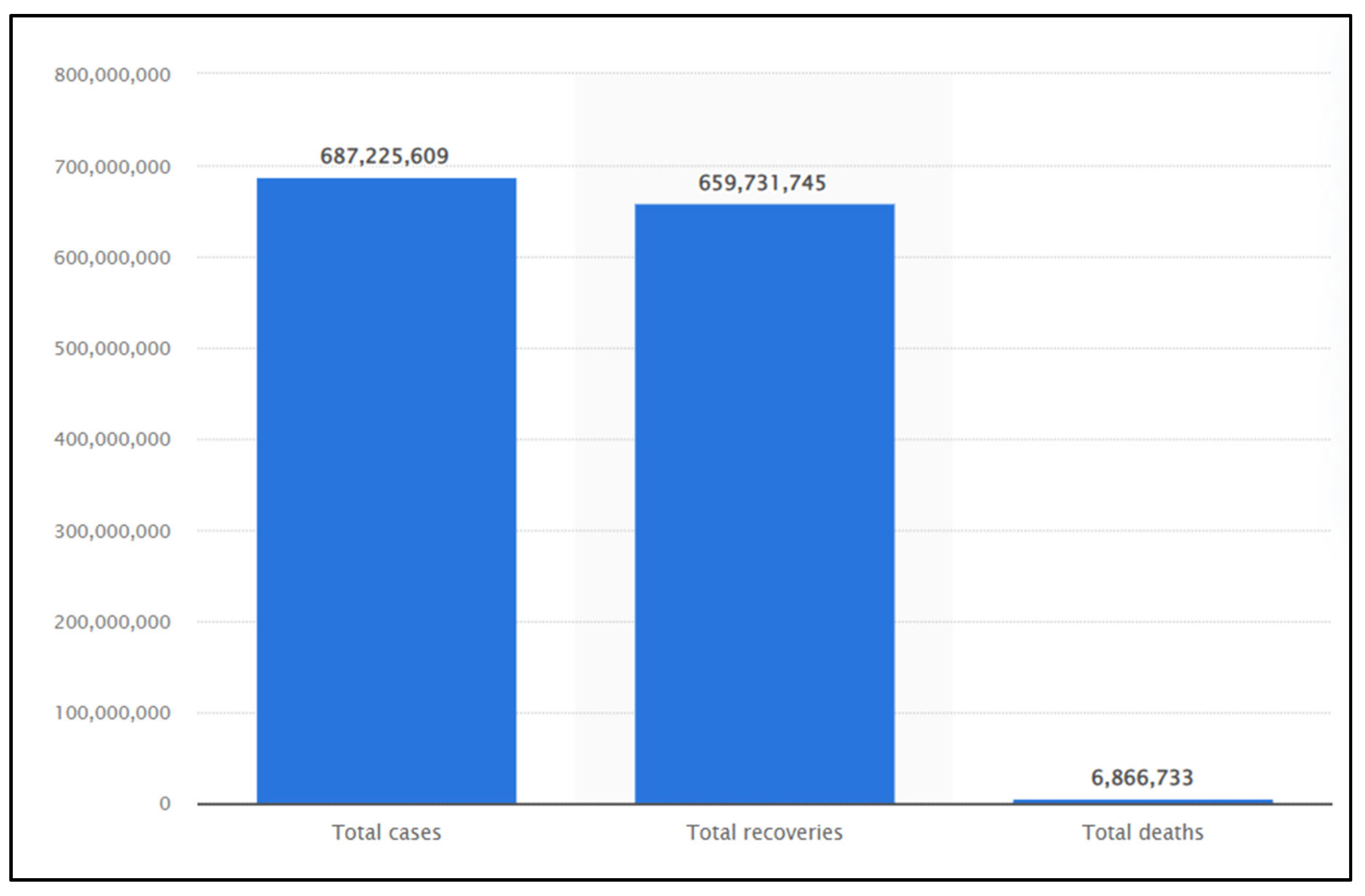
Figure 6.
Number of coronavirus (COVID-19) cases, recoveries, and deaths worldwide as of May 2023.
Interpretation of the findings
This Vietnamese study showed that, approximately, one in twenty symptomatic patients tested for COVID-19 was actually diagnosed with COVID-19. It is difficult to compare this finding with previous studies' results, as most of these studies included symptomatic and asymptomatic participants, were conducted in other settings and countries, and were conducted independently from different COVID-19 variants. That being said, if we compare these results with those from other studies we may conclude that numbers refer to a condition often overestimated as many were the cases of false positive and false negative. For instance, a U.S. study of 3,477 symptomatic healthcare workers reported that 5.3% of the sample had COVID-19. Another study using samples from 2,203 individuals from Germany collected in May–June 2020 found that none of the throat swabs taken was positive for SARS-CoV-2 [4,22]. Worldwide the numbers seem to confirm this trend with 680 million people affected vs 670 million recovered with a rate of mortality of almost 7 million (8,56%), in Asia only the 217 million c.ca infected with a mortality of 1.5 million c.ca (4.56%) (fig.6) [1].
With the correct proportions the current study showed that the prevalence of COVID-19 infected individuals appears to be relatively low, being 33 out of 600. These findings highlight two main points; (i), the age, the younger the lesser are the possibility to catch the infection; (ii), the important role played by general awareness campaign either in prevention adopted measures or, (iii), in earlier diagnosing procedure conducted by the health authorities in the Ninh Thuanh province in particular and in Vietnam in general, stressing out the the crucial role of implementing preventive measures in controlling the transmission of the virus in the communities and hospitals.
In our study, the majority of COVID-19 patients had mild disease (75.8%), 1 patient was severe (3.0%) and no patient was in critical condition (Table 3). Because most of the infections were mild, the rate of patients recover at Ninh Thuan General Hospital is very high (100%). This result is consistent with the current situation, though almost all patients have received the 2nd and 3rd dose of COVID-19 vaccine, still most of the critically ill patients are elderly, accompanied by underlying disease, the median age of patients in our study was young (36 years), so a high cure rate is appropriate.
The second results came out from the present study was the characterization of possible adjunctive markers that may refer to COVID-19 infection, therefore those blood markers that could be significantly associated in regarding the differences involved with the disease tendency. There are major physiognomic related differences in the human immune system response against SARS-CoV-2 at various stages of the infection (e.g., virus entry, virus sensing, and innate immune response...), and towards the different types of its variants, these differences may result in a higher risk of COVID-19 or more persistent detection of viral RNA in different individuals independently from the gender, age or factors.
From a clinical perspective, previous researches have also shown that compliance with preventive public measures is lower in men than in women, which may at least partially explain the relationship between sex and COVID-19 diagnosis observed in this study. Finally, several age-related changes such as immunosenescence, inflammation, and a dysregulated renin-angiotensin system may increase COVID-19 susceptibility in older adults compared to their younger counterparts. Furthermore, in line with previous research, there was a positive association between male sex, older age and the severity degree of the disease. Although the strength of the association between the different parameters such as the gender, the possible presence of specific genetic make-up such as the single nucleotide polymorphisms (SNPs) and the diagnosis of COVID-19 was considered a strong determinant variable (i.e., OR 1.04) [20,21,22,23].
At the present is generally accepted that individuals are differentially affected by COVID-19. Although pre-existing disorders have been studied extensively, little is known how much the genetic background may influence on the predisposition to the disease. The rapid progression of the infection accompanied by a sudden clinical decay seemed a prerogative of certain subjects rather than others [20,21,22,23]. The excessive uncontrolled inflammatory responses mainly determined by the overexpression of typical inflammatory factors and markers such as the IL-6, IFNγ and TNF-α were common clinical traits of this infection. There was little or none homogeneity among patients and among the unpredictability of the events this trait drove the attention towards the possible role of single nucleotide polymorphisms (SNPs) of those genes involved in the immune regulatory mechanism. In fact, the disease grade of severity was soon observed in connection to several gene carrying specific SNPs [23,24,25].
For instance, while the IL6 174 G/G genotype indicates an overexpression of IL6 expression, the G/C is mainly related to a moderate IL6 expression. In addition, it is known that IL6 may become completely unmanageable in the presence of low circulatory level of IL10 as consequence of IL6 genes down-expression, indicated by SNPs with the genotype A/A, which characterize the SARS-CoV-2 “cytokine storm”. Thus, the SNPs' analysis may also play a strong role in the diverse degree of infection and the differences in individual's responses to Sars-CoV-2 [23,24,25].
Hyperferritinaemia has been considered an indicator of inflammatory processes in different disorders. Hyperferritinaemia may be due to leakage from damaged intracellular stores, and once released from tissue stores, ferritin loses the inner iron content allowing the rise of free iron which also favors growth of many viruses [26,27,28,29].
Iron metabolism and immune response to SARS-CoV-2 have not been fully described although several line of evidence demonstrated their involvement in Covid-19 pathogenesis. Our research, showed that the median ferritin in patients with COVID-19 was 200 ng/mL, there was a statistically significant difference in the median ferritin concentration between the two groups (P < 0.05), AUC=0.9, P<0.001 . Many studies confirmed the high presence of the ferritin concentration with moderate and severe disease in patients with COVID-19, our results showed a cutoff of 266 ng/ml, the sensitivity was 88% and the specificity was 92% [26].
Lymphopenia and specific T cell lineage affection are characteristic features of Covid-19 and have been correlated with poorer prognosis [27,28,29]. In previous coronavirus outbreaks, such as SARS, the peak of viral load occurred 7 days after symptoms development, followed by elevation in IL-6 and IL-8, low lymphocyte count, high neutrophils count and subsequent neutrophils pulmonary infiltrates. This description suggests that clinical symptoms might be mediated by the immune system deregulation rather than direct viral damage [12,30]. The distribution of different subtypes of T cells in peripheral blood of symptomatic critical and non-critical Covid-19 patients has been described [30,31,32].
In our experience, the majority of patients affected by COVID-19 shared a quite common scenario characterized by important high levels of IL-6 and CRP presented with increased serum fibrinogen and troponin with low levels of eGFR and hemoglobin and hematocrit, with slightly high levels of RDW (suggestive of iron anemia) [30,31,32].
Different studied demonstrated the capacity of Sars-CoV-2 virus to disrupt the coordination between the two branches of the immune system, innate and adaptive immune responses. The affected patients' immune profiles showed low levels of B-lymphocytes, low levels of T-regs CD4+CD25+, high levels of T CD8+CD38+DR, high levels of T-suppressor CD8+CD57+, high levels of T-NK CD3+CD56+ (higher than NP, NN, and NA). High levels of neutrophils, low levels of lymphocytes, low levels of T-mature CD3, low levels of CD4, low ratio < 1 CD4/CD8, low levels of naïve CD4 [30,31,32].
Conclusion
In this cross-sectional study, a wide range of sociodemographic risk factors, including age and environmental factors, were significantly associated with COVID-19 incidence and mortality. To address inequities in the burden of the COVID-19 pandemic, these social variabilities and their root causes must be addressed. Approximately 5.5% of patients infected with SARS-CoV-2 come to examination and treatment at hospital. Lymphocytes and ferritin were valuable in determining moderate and severe disease in patients with SARS-CoV-2 infection.
Author Contributions
T.L.H., T.L.V., T.L.Q., H. L.T., D.D.T. And M.G.B. conceptualization, final editing, and harmonization; C.G.I., K.C.D.N. and R.L. drew the figures; K.C.D.N. and C.G.I. drafted the manuscript in cooperation; writing, review and editing, C.G.I., M.G.B., F.I.; visualization, M.G.B., L.S., V.D.L. and R.D.P.; validation, C.G.I., M.G.B., P.D. and K.C.D.N.; supervising, C.G.I., M.G.B., P.D.; project administration, F.I, R.D.P and L.S. All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Applicable.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard 2022. https://covid19.who.int/.
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H. Clinical and immunological features of severe and moderate coronavirus disease 2019. The Journal of clinical investigation 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, J.; Yang, Y.; Ma, H.; Li, Z.; Zhang, J.; Cheng, J.; Zhang, X.; Zhao, Y.; Xia, Z. The potential role of IL-6 in monitoring severe case of coronavirus disease 2019. MedRxiv. 2020:2020.2003. 2001.20029769..
- Jacob, L.; Koyanagi, A.; Smith, L.; Haro, J.M.; Rohe, A.M.; Kostev, K. Prevalence of and factors associated with COVID-19 diagnosis in symptomatic patients followed in general practices in Germany between March 2020 and March 2021. International journal of infectious diseases 2021, 111, 37–42. [Google Scholar] [CrossRef]
- Balzanelli, G.M.; Distratis, P.; Aityan, K.S.; Amatulli, F.; Catucci, O.; Cefalo, A.; et al. Clinical Features in Predicting COVID-19. Biomed J Sci & Tech Res 29(5)-2020. BJSTR extension. MS.ID.0048743.
- de Lusignan, S.; Dorward, J.; Correa, A.; Jones, N.; Akinyemi, O.; Amirthalingam, G.; Andrews, N.; Byford, R.; Dabrera, G.; Elliot, A. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. The Lancet Infectious Diseases 2020, 20, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Setiadi, W.; Rozi, I.E.; Safari, D.; Daningrat, W.O.D.; Johar, E.; Yohan, B.; Yudhaputri, F.A.; Lestari, K.D.; Oktavianthi, S.; Myint, K.S.A. Prevalence and epidemiological characteristics of COVID-19 after one year of pandemic in Jakarta and neighbouring areas, Indonesia: A single center study. Plos one 2022, 17, e0268241. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.; Distratis, P.; Catucci, O.; Amatulli, F.; Cefalo, A.; Lazzaro, R.; Aityan, K.S.; Dalagni, G.; Nico, A.; De Michele, A.; Mazza, E.; Tampoia, M.; D'Errico, P.; Pricolo, G.; Prudenzano, A.; D' Ettorre, E.; Di Stasi, C.; Morrone, L.F.P.; Nguyen, K.C.D.; Pham, H.V.; Inchingolo, F.; Tomassone, D.; Gargiulo Isacco, C. Clinical and diagnostic findings in COVID-19 patients: an original research from SG Moscati Hospital in Taranto Italy. J Biol Regul Homeost Agents. 2021, 35, 171–183, https://www.statista.com/statistics/1087466/covid19-cases-recoveries-deaths-worldwide/. [Google Scholar] [CrossRef] [PubMed]
- Statista-2023, https://www.statista. 1087.
- Mani, N.S.; Budak, J.Z.; Lan, K.F.; Bryson-Cahn, C.; Zelikoff, A.; Barker, G.E.; Grant, C.W.; Hart, K.; Barbee, C.J.; Sandoval, M.D. Prevalence of coronavirus disease 2019 infection and outcomes among symptomatic healthcare workers in Seattle, Washington. Clinical Infectious Diseases 2020, 71, 2702–2707. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Coronavirus disease 2019 (COVID-19): Situation report, 51. Retrieved , 2020, from https://apps.who.int/iris/handle/10665/331475. In.; 2020a. . 2 May.
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; Felix, S.E.B.; Tie, Y.; Fullerton, K.E. Coronavirus disease 2019 case surveillance-United States, January 22–may 30, 2020. Morbidity and Mortality Weekly Report 2020, 69, 759. [Google Scholar] [CrossRef] [PubMed]
- Boehmer, T.K.; DeVies, J.; Caruso, E.; van Santen, K.L.; Tang, S.; Black, C.L.; Hartnett, K.P.; Kite-Powell, A.; Dietz, S.; Lozier, M. Changing age distribution of the COVID-19 pandemic-United States, May–August 2020. Morbidity and Mortality Weekly Report 2020, 69, 1404. [Google Scholar] [CrossRef]
- Dudel, C.; Riffe, T.; Acosta, E.; van Raalte, A.; Strozza, C.; Myrskylä, M. Monitoring trends and differences in COVID-19 case-fatality rates using decomposition methods: Contributions of age structure and age-specific fatality. PLOS one 2020, 15, e0238904. [Google Scholar] [CrossRef]
- Ferre, J.; Abou Rafeh, A. COVID-19 and Older Persons: A Defining Moment for an Informed, Inclusive and Targeted Response. 2020.
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.; Fu, H. Estimates of the severity of coronavirus disease 2019: a model-based analysis. The Lancet infectious diseases 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Liu, Y.; Gu, Z.; Xia, S.; Shi, B.; Zhou, X.-N.; Shi, Y.; Liu, J. What are the underlying transmission patterns of COVID-19 outbreak? An age-specific social contact characterization. EClinicalMedicine 2020, 22, 100354. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. jama 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Guan W-j Ni Z-y Hu, Y.; Liang W-h Ou C-q He J-x Liu, L.; Shan, H.; Lei C-l Hui, D.S. Clinical characteristics of coronavirus disease 2019 in China. New England journal of medicine 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Sannigrahi, S.; Pilla, F.; Basu, B.; Basu, A.S.; Molter, A. Examining the association between socio-demographic composition and COVID-19 fatalities in the European region using spatial regression approach. Sustainable Cities and Society. 2020, 62.102418. ISSN 2210-6707. [CrossRef]
- Government News of the Socialist Republic of Viet Nam. https://en.baochinhphu.vn/viet-nams-population-increases-by-nearly-1-million-in-2022-111230104160334712.htm.
- Tomczyk, S.; Hönning, A.; Hermes, J.; Grossegesse, M.; Hofmann, N.; Michel, J.; et al. Longitudinal SARS-CoV-2 seroepidemiological investigation among healthcare workers at a tertiary care hospital in Germany. BMC Infect Dis. 2022, 22, 80. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; Pham, V.H.; Tran, T.C.; Dipalma, G.; Bianco, A.; Serlenga, E.M.; Aityan, S.K.; Pierangeli, V.; Nguyen, K.C.D.; Inchingolo, F.; Tomassone, D.; Gargiulo Isacco, C. Analysis of Gene Single Nucleotide Polymorphisms in COVID-19 Disease Highlighting the Susceptibility and the Severity towards the Infection. Diagnostics (Basel). 2022, 12, 2824. [Google Scholar] [CrossRef]
- Balzanelli, M.G.; Distratis, P.; Lazzaro, R.; Cefalo, A.; Catucci, O.; Aityan, S.K.; Dipalma, G.; Vimercati, L.; Inchingolo, A.D.; Maggiore, M.E.; et al. The Vitamin D, IL-6 and the eGFR Markers a Possible Way to Elucidate the Lung-Heart-Kidney Cross-Talk in COVID-19 Disease: A Foregone Conclusion. Microorganisms. 2021, 9, 1903. [Google Scholar] [CrossRef]
- Martens, P.J.; Gysemans, C.; Verstuyf, A.; Mathieu, A.C. Vitamin D's Effect on Immune Function. Nutrients. 2020, 12, 1248. [Google Scholar] [CrossRef]
- Kaushal, K.; Kaur, H.; Sarma, P.; Bhattacharyya, A.; Sharma, D.J.; et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J Crit Care. 2022, 67, 172–181. [Google Scholar] [CrossRef]
- Edeas, M.; Saleh, J.; Peyssonnaux, C. Iron: innocent bystander or vicious culprit in COVID-19 pathogenesis? Int J Infect Dis. 2020. [CrossRef]
- Colafrancesco, S.; Alessandri, C.; Conti, F.; Priori, R. COVID-19 gone bad: a new character in the spectrum of the hyperferritinemic syndrome? Autoimmun Rev. 2020, 19, 102573. [Google Scholar] [CrossRef] [PubMed]
- Drakesmith, H.; Prentice, A. Viral infection and iron metabolism. Nat Rev Microbiol. 2008, 6, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China, Clinical Infectious Diseases 2020, 71, 762–768.
- Velavan, T.P.; Meyer, C.G. Mild versus severe COVID-19: laboratory markers. Int J Infect Dis. 2020, 95, 304–7. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.G.; Distratis, P.; Dipalma, G.; Vimercati, L.; Catucci, O.; Amatulli, F.; Cefalo, A.; Lazzaro, R.; Palazzo, D.; Aityan, S.K.; Pricolo, G.; Prudenzano, A.; D'Errico, P.; Laforgia, R.; Pezzolla, A.; Tomassone, D.; Inchingolo, A.D.; Pham, V.H.; Iacobone, D.; Materi, G.M.; Scarano, A.; Lorusso, F.; Inchingolo, F.; Nguyen, K.C.D.; Gargiulo Isacco, C. Immunity Profiling of COVID-19 Infection, Dynamic Variations of Lymphocyte Subsets, a Comparative Analysis on Four Different Groups. Microorganisms. 2021, 9, 2036. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



