
Submitted:
09 June 2023
Posted:
09 June 2023
Read the latest preprint version here
Abstract
Isokinetic testing of the knee joint is the “gold standard” in strength assessment in sport especially in soccer, where it is part of pre-season screening to establish norms in case of injuries. There are many devices on the market that make it difficult to use of normative data. Isokinetics literature in females’ soccer players is scarce in comparison to males. Furthermore, evaluation protocols strongly differ from each other, using different ranges of speeds, movement patterns and output data. Thus, it is difficult for the researcher and the clinician to choose a correct protocol for isokinetic evaluation in female soccer players. The indexes of isokinetic performance that are widely accepted are the hamstring/quadriceps (H/Q) ratio and dominant/non-dominant (D/ND) ratio as reference. In this review are highlighted some common features of isokinetic testing in female soccer players of different levels of qualification. From this study, it emerges that, for a reliable test, 3 reps at the speed of 60°/sec in knee flexion/extension is preferable due to the high reliability and that an optimal H/Q ratio in healthy female soccer players of different level of qualification and age is 50%, while the interlimb differences (D/ND) should be below 10%.
Keywords:
Female soccer
; isokinetics
; hamstring/quadriceps ratio
; dominant non dominant limb ratio
; errors in isokinetic dynamometry
Introduction.
Traditionally, female football (soccer) research has received less attention than research on male counterpart [1]. The reasons for this under consideration of female soccer are many, but mostly reside in social factors [1]. As consequence, research on female soccer players has been under funded and the availability of laboratories and instrumentation to perform research in females is scarce. Among research in female football, injuries on the knee and performance indicators have a special place. Strength is a basic physical quality which is largely investigated. Isokinetic testing is the most used tool for knee strength assessment in soccer and require expensive equipment, which are less affordable to female clubs.
Isokinetic testing provides useful information for performance and injury prevention and rehabilitation of the knee [2].
In sport performance testing, there are basically 3 basic factors to be considered: a) Validity (the protocol reproduce the functional task as closely as possible and this is the case of isokinetic testing, which reproduce the ball kicking; b) Reliability (the protocol gives similar result from day to day when no intervention is used; and Sensitivity: the protocol must be able to detect small, but significant, changes in performance [3]. Sensitivity of isokinetic machine is high [3], if the system is kept in proper working order. Thus, our review focuses on some factors which influence the reliability of isokinetic test.
As a preliminary consideration, must be noted that knee injuries are most common in females compared to males’ football players [4], and especially anterior knee pain is reported more often in females. Isokinetic pre-season and in-season screenings are a standard part of the functional screening of soccer’s players, and the reference values are used as landmarks in case of injuries, to quantify the extent of strength losses and to establish the return to play after rehabilitation [5]. Quantify the bilateral strength deficit is useful for insurance compensation procedures [6] as well to compare of the outcomes of different surgical methods, e.g. for the reconstruction of the anterior cruciate ligament [7]. Isokinetic measurements were first described in 1927, as a tool to measure the strength characteristic of isolated muscle fibers in the early physiological studies of muscle functions [8]. Isokinetic comes from Greek iso = same, and kinesis = motion. The first isokinetic dynamometer was developed by Levin and Wyman (1927) [8] for studying isolated giant muscle fibers taken from the jaw of the giant shark, a very powerful muscle, capable of a pressure of 4000 PSI (pound per square inch). The modern isokinetic devices work by mean of a servo-controlled mechanism in a closed loop with the tested subjects, in order to keep the contractions speed constant with a sampling and controlling rate of 100 Hz. There are basically two kinds of machines: ones who employ a circular motor (e.g. leg extension) where a leg extension arm is attached to a rotating shaft, thus measuring torque, and one who employ linear motors (e.g. leg press). Other type of isokinetic machine, use endless rotational motor, are thus capable to achieve very high angular velocities, and such machines can achieve 1000 degrees per second, useful for some fast rotatory movements, such as downhill cycling. Using small cranks on a stationary isokinetic bike it is possible to spin up to 300rpm for cadence training which is equal to 1800 degree/second. The availability of linear isokinetic machines allows the measurement of the strength/speed curves in-vivo during the functional exercise. The in-vivo strength/speed (or Hill’s curve) is important for understanding the athlete’s characteristics and adaptation to training. The idea was to cancel the influence of speed of movement (otherwise uncontrollable acceleration and deceleration phases) on muscle contraction, thus obtaining a twofold objective: eliminate the elastic component (pre-tensioning the muscle elastic structures) and obtaining pure strength curves [8,9]. Early isokinetic devices, controlled the contraction speed, using smoothing apparatus basically made of a valve embedded in a high viscosity fluid [8]. For many years, the use of isokinetic devices was limited to physiological studies performed for research purposes. Only lately, the isokinetic principle went out of laboratories and spread into clinical practice, because of its clinical and functional usefulness, and because of the capacity of provide a safe muscular contraction, without any jerk caused by the limb acceleration [9]. Isokinetic was made commercially available in the 1970 and diffused in sport medicine in the 1980, with the lowering of the cost of isokinetic dynamometers, but still are relatively expensive. Considering females muscle testing, it worth noting that the strength characteristics of males and females muscle are different. Males and females with the same muscle size show different levels of strength, being females’ quadriceps muscles weaker by a 12% to 24 % in comparison to male’s when normalized for muscle thickness [10]. Furthermore, knee injuries rate is higher in females than in males due to the morphological condition of “genus valgus” [11], in fact, the prevalence of knee injuries in females is further worsened by the presence of the valgus knee, which is a common feature in the female Asian biotype [12].
Isokinetic testing can be performed in several joints and using different modalities of muscle contractions. Normally concentric (CON) and eccentric (ECC) mode of muscle contractions are employed and a wide range of speeds, normally from 1° to 500/sec for the knee joints. The so-called eccentric contraction, or contraction-in-lengthening (apparently a contradiction in terms), happens when a muscle contracts while it is stretched, thus resisting to the stretch in a controlled way. In this way was obtained the force/velocity curve using the first isokinetic dynamometer [8]. It is proven that eccentric “contraction” produces higher strength levels and strength gains in comparison to purely concentric contraction, thus, at least theoretically, it is worth to measure isokinetic strength. Laterality, or dominance, is another classical pillar of physical evaluation. Male professional soccer players of English premiere league, displayed the greatest level of asymmetry in isokinetic strength measures (5.9-12.7%) and lower levels of asymmetry in gait (1.6-7.7%)and jump (0.9-7.0%) . assessments [13]. From a psychological point of view, isokinetic testing is strictly depended from sincerity of effort [14]. In fact, studies on sincerity of effort in healthy young females, showed that a coefficient of variation lower than 10% between repeated strength curves is the optimal to ascertain the subject performed at his maximal capacities [14].
Left/Right, dominant, (D) and non-dominant (ND), knee extensors (EXT) and flexors (FLEX) strength and quadriceps/hamstrings (H/Q) ratios are widely used informative parameters of isokinetic testing that has been related with several performance parameters, occurrence of injuries and recovery [15]. It worth noting that the Dominant leg not necessarily coincide with the Right leg, and this factor can lead to negative values when looking at the side ratios. H/Q ratio is of special interest, because it reflected mainly of the effect of gravitation force during leg extension and flexion. In fact, there is an anti-gravity effect during the physical training, where gravitation acts against leg extensor muscle and, in turn, favorable to knee flexors, thus not stimulating the knee flexors, which in fact has to be trained with special “isolation exercise”. Leg flexors work in favor of the gravitational force are “weakened’ if not appropriately stimulated. On the opposite, gravitation train the strength in the quadriceps muscle in comparison to hamstrings muscles. It has been proposed that this unbalanced growth of anti-gravitational muscles, is, on the long run, can be detrimental to the safety of the knee [16] because of muscle imbalance and thus causing injuries. The gravitation effect is thus present during knee and flexion strength testing. In order to compensate for the measurement error due to the help of gravitational force during knee flexion, isokinetics devices were equipped with a gravitational compensation procedure, which in turn can be active (the isokinetic machine arm moves the limb trough the range of motion and weight it) or passive (the limb is dropped and the isokinetic machine arm weights it during the dropping) [17]. The obtained weight values for the tibial and foot segments are then subtracted from the torque produced by the machine electric engine to keep the speed constant and the values are subtracted from the test results. This way, the subject limb during testing effectively works in absence of gravitational force and the obtained H/Q ratios are cleared from the gravitational force. However, the assumption that H/Q imbalance necessarily relates to an injury, is controversial, and a recent study cast some doubt on the clinical relevance of H/Q and D/ND ratio for injury prevention [18], despite these recent findings, H/Q and D/ND ratio are still widely used. The reasons behind the usage of the ratio are they are because ratios are simply to understand, fast to measure and intuitively linked with muscle performance. Leg extension is of course linked to ball kicking speed [18]. There is also evidence that an increase in muscle tone and balance between knee extensors and flexors, also increases the knee’s stability [19]. However, the link between EXT/FLEX and perspective injury rate was questioned [19,20]. Isokinetic, being an artificial form of muscle work, not present in nature, but obtained with an “artifact”, the isokinetic device, presents in addition, several technical problems [21,22] and methodological [19,22] issues inherently linked to the isokinetic test itself, which sometimes are not considered and that can lead to erroneous or at least unexplainable results. The first gross source of error is the acceleration of the limb to “catch” the machine speed, which cause the torque overshoot (a sudden peak in strength), which happens when the limb “catches up” with the machine speed, and the “true” isokinetic phase in the range of motion, which shortens with the increasing speed [20,21,23]. Another factor which could deal to misinterpretation of the isokinetic test, is the different technology used, which does not allow a comparison between different system and sometime also between the same system, because of a poor calibration, or for the wearing of the mechanical part and of the measurement devices embedded in an isokinetic machines. In fact, isokinetic machine embeds electro goniometers, strain gauges and tachymeters, which easily worn with the usage. In addition, the measurement of other joint than knee is very problematic in terms of reliability [23]. These issues have been well known for long time, but still there are some misreporting in the literature about those topics and they might not be considered when testing, especially in females, which are less studied. Thus, the aim of this paper is to review the literature about isokinetic testing in female soccer players, in order to provide a survey of the available knowledge about testing protocols, but also to review the problems which can lead to misleading results detrimental for the interpretation of isokinetic data. Further, the reference values for H/Q, D/ND and L/R ratios and angles of occurrence of maximal strength will be reviewed in order to have a guideline for the interpretation of isokinetic testing in females.
Methods.
A survey of the existing literature was conducted in four different databases from inception to May 2023 (PubMed, Sport Discus, Ebsco, and Psychinfo) and on Google Scholar. The following keywords were used in different combinations: “isokinetics and females soccer players”, “female soccer players and isokinetics”, “isokinetics and knee and females and soccer”, “isokinetics and soccer and females”, “reliability of isokinetic systems”. The word “football” was also used instead of “soccer” and along this paper we use it interchangeability. The search strategies were combined, and duplicates were removed using Endnote X7 (Clarivate Analytics, previously Thomson Reuters, Philadelphia, PA, USA). The databases were queried in hierarchical order (e.g., first the broader database), starting from Google Scholar, followed by PubMed, Sport Discus, and Psychinfo. On Sport Discus only paper of higher level (level = advanced) was considered. All titles and abstracts were carefully read, and relevant articles were retrieved for review. In addition, the reference lists from both original and review articles retrieved were also reviewed. The eligibility criteria limited the search to studies performed on females’ soccer players with no previous history on injuries, e.g., pure functional or normative studies. The review complied with the PRISMA statement for a systematic review [24]. The inclusion criteria were studies related to isokinetics in healthy female soccer players of different levels of qualification, no presence of knee pathologies. The exclusion criteria were: (i) studies written in languages other than English, (ii) studies involving injured athletes. No limits were set concerning the year of publication. The inclusion or exclusion of articles was determined by applying the above criteria on the title and abstract as a first screening and on full texts as a second screening. and power in watts) but the ratios and when ratios were not reported, were calculated from the raw values We can generally observe that different devices for isokinetic testing were employed in the studies, with a high heterogeneity in the raw results. Thus, when considering interlimb and agonists/antagonist muscles ratios, we didn’t consider the absolute strength values (torque in newton meters, Nm or power, Watts, in one case) but the differences in %, using the formula: (Limb with higher strength – weaker limb) / Limb with higher strength x 100 and reported as % to allow a comparison between different test conditions.
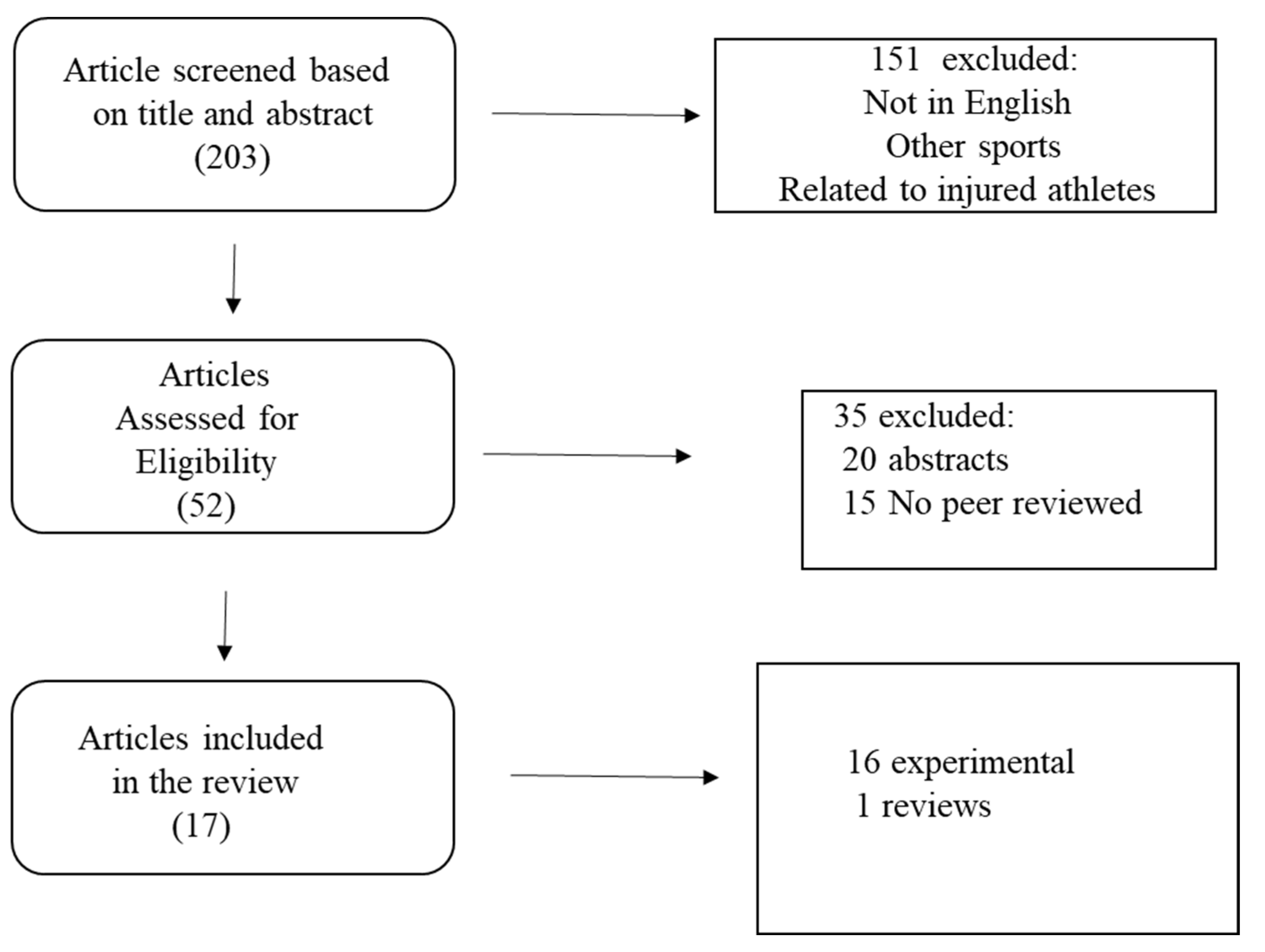
Figure 1.
Search strategy.
Results
17 papers matched the inclusion criteria and were included in the review. Table 1 reports a summary of the findings.
A first observation can be made about the heterogeneity of the isokinetic machine that has been used. In fact, several different isokinetic systems were used. 8 out of 17 studies used a Biodex machine, followed by Cybex (3 studies) while Kin Com, Lido, Rev9000, Humac, Contrex and Isomed were employed in 1 study each. This heterogeneity makes absolute normative data difficult to be summarized. The isokinetic variables were collected mostly in Concentric (CON) mode, and less frequently in Eccentric (ECC) mode. We can hypothesize the reason for the preference of CON testing is because ECC reliability of the eccentric test is low, especially at the speed of 60°/sec, and eccentric contraction can be risky for the knee safety. This hypothesis is supported by literature which show poor reliability for eccentric testing [25]. Even at low contraction speed (60°/sec) isokinetic eccentric testing has been shown to have poor reliability [25]. Especially hamstring muscles testing showed a poor reliability of measurement and especially in female’s athletes [26]. In fact, for CON testing r was reported an ICC of 0.964 for EXT peak torque at 60°/sec on the Kin Com dynamometer [27], while on the Cybex 6000 was 0.84 [28]. Few studies exist on the comparability of measurement between isokinetic systems. Mostly of the available literature compares two isokinetic systems and no study on comparison of several machines exist. One study compared Kin Com and Lido isokinetic machine and found no difference in muscle strength (Nm) between the Biodex and Lido for CON FLEX and CON EXT [29]. Dominant (D) and Non-Dominant (ND) limb (D/ND) and Hamstring to Quadriceps (H/Q) ratio were calculated mostly using Peak Torque (PT, e.g the maximum torque registered along the range of motion), one paper measured peak power (W) and mean work (MW). Dominant limb was determined asking the kicking preference in all studies. 3 to 5 repetitions at slower speed (60°/sec) were measured, while at higher velocities 10 (180°sec) to 25 (300°/sec) repetitions were measured. Range of motion was in all cases 90° (from full knee extension to 90°of knee flexion). An important point is, the reliability of concentric test decrease with the increase of the speed because of the shortening of the “pure” isokinetic range of motion, due to the acceleration and deceleration [30].
The chosen test speeds in the paper we considered in this review, ranged from 30° to 300°/sec. Albeit some evidence in the literature suggest not to use speeds above 180°/sec because of limb acceleration and deceleration time, which reduce the true isokinetic phase [21], speeds above this limit were used in 12 studies of 17.
The differences between left and right limbs, which normally increase with increasing speeds, ranges from -1.7 % to 9.7 at 60°/sec up to 14.9% at 270°/sec in concentric leg extension and from 2% up to 8% in concentric knee flexion.
Three studies [31,32,33] show a small negative D/ND ratio. This fact can be explained by the presence of left sided players in the examined sample. No studied reported how the Dominant limb were determined. H/Q ratio varies between 44.9% at 60°sec (except for one study which found a 75% ratio - uncompensated for gravity) to 72% at 300°/sec [34]. Normalized values for kg of body weight were used only in two studies where young elite players presented a lower difference between D/ND leg [34,35]. One study found a small non-significant differences between under 17 and senior elite player in CON EXT (2.04 Nm/kg vs 2.10 Nm/kg) and 2.82 Nm/kg vs 2.06 Nm/kg, while a significant in CON FLEX difference was found at 60°/sec [36].
Very young (11-14 y.o.), elite soccer players, were found to have a H/Q ratio of 50% [37]. Olympic soccer players showed a H/Q ratio of 54% at 60°/sec and of 72% at 300/sec ° [38]. Three large studies in collegiate (196, and 138, and 101 players) reported an H/Q ratio of 59.6% and of 62% at 60°/sec [39,40] and a D/ND ratio of 7,8% and 6.46 % [41]. These H/Q values are higher than those found in another study in professional players which show a ratio of 44.9% at 60°/sec [42] and in collegiate who shows H/Q values at 60 °/sec equal to 49.5%, 54% and 46% [43,44,45], midway between Professional and young players. Professional players show small D/ND differences on the velocity’s spectrum of 60,180,240°/sec, with higher differences in the extensor muscles [28]. Healthy professional female players show a difference of 13% in EXT ECC at 60 ° and of 10% in CON EXT strength [46].
In our review, we found that there is a wide variation in the H/Q and N/ND ratio. H/Q at 60° sec is almost stable at around 50% through the literature (a little bit less for young athletes), while the N/ND in healthy females’ soccer players is quite small and below 10%. These can be reference values for healthy female soccer players. At higher speeds the H/Q values vary considerably among the different studies, and this is an index of lower reliability of the isokinetic test also at relatively fast speeds (120° and 180° /sec). We found the trend for PT values trough the speeds is in accord with the Hill’s force/velocity curve [47] (decrease of strength when the speed increased), we found some negative N/ND mean ratio in CON EXT and CON FLEX which is probably determined to the non-coincidence of Left and Right with ND and D leg. 12 of 17 studies didn’t report how they selected the Dominant limb, while the others selected the kicking limb as Dominant. Thus, limb dominance (laterality) must be carefully assessed before isokinetic testing. ECC values for knee EXT also increase with the speed and this is explainable with the difficulty to control high eccentric speeds which are less reliable. At low speeds (60°/sec) 46% to 60% H/Q ratios have been registered. As isokinetic testing is often assumed as the “golden standard” in knee strength evaluation, it quite surprising the lack of information on the used protocols. Also, the warmup procedure before isokinetic tests differed widely when described and sometimes were not reported. The protocols were sometimes poor described (e.g no rest time between series were reported, and no previous training schedule of athletes or menstrual cycle phase at the time of test were reported). These observations are in agreement with a recent study [48], which critically evidenced that, considering the available evidence, it need more investigations and an improving in standardization of methodology and analysis to optimize interpretation (e.g., within session and between session), adoption, and implementation of interlimb asymmetry testing, and subsequent appropriate interventions [48]. The same study also calls for a greater methodological rigor, to be applied in study design, data analysis, and interpretation of isokinetic (and other tests for asymmetry) and also when reviewing the current literature.
Conclusions.
Isokinetic testing is widely used in soccer, albeit few studies are available in females. Thus a limitation of our review is inherent to the topic, in fact, also in this field, females are underrepresented. Another limitation is several protocols were not clearly described. This paucity of information about isokinetic muscular performance in females, is explainable with social factors (e.g., less economic interests in female soccer players). In addition, the available literature used different isokinetic devices, different protocols of testing (speeds and number of repetitions, recovery) and the rationale for the choice of speeds are not reported. Also, in several studies how the dominant leg was chosen is unclear. There are some constants which emerge from the literature that can be summarized and can be useful for the practice and interpretation of isokinetic testing in females soccer players. We can conclude, that for clinical practice, an isokinetic test for the female’s soccer athletes at 60°/sec in concentric mode for EXT and FLEX is the most reliable, employing 3 reps. H/Q should be 50% (a little bit less for young athletes), while the N/ND in healthy females’ soccer players should be less than 10%. Several papers employed for research purposes employed high velocities, but previous literature show they are less reliable and do not add further information to the 60°/sec test. Limitations of our study are that in some papers, raw data, reliability and coefficients of variation in testing were not reported. These results can be helpful for establishing milestones in the process of training and rehabilitation and functional evaluation with an isokinetic machine. Isokinetic studies in women are quite sparse due to cultural and economic barriers, and beside further research, which are needed, social obstacle to the development of female soccer research must be removed.
Author Contributions
Cheng Zhan: conception of the study, data gathering and writing, data gathering and analysis, Antonio Cicchella, conception of the study, analysis and writing. All authors read and approved the final version of the manuscript and approve the manuscript in full.
Funding
This study was supported by the Education Research and Reform Cultivation Project of Tongji University.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Tongji University (approval code: tjdxsr029 22/12/2022.
Informed Consent
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are kept by the corresponding author for privacy reasons and will be given upon request.
Acknowledgments
The Authors thanks all the soccer players who participated in this study.
Conflicts of Interest
Authors declare no conflict of interests.
References
- Okholm Kryger, K.; Wang, A.; Mehta, R.; Impellizzeri, F.M.; Massey, A.; McCall, A. Research on women's football: a scoping review. Sci Med Footb. 2022,6,549-558. doi: 10.1080/24733938.2020.1868560. [CrossRef]
- Zeevi D. Isokinetic Muscle Testing. Interpretation and Clinical Applications. Churchill Livingstone, 2004.
- Currell, K.; Jeukendrup, A.E. Validity, reliability and sensitivity of measures of sporting performance. Sports Med. 2008,38, 297-316. doi: 10.2165/00007256-200838040-00003. [CrossRef]
- You, S.; Shen, Y.; Liu, Q.; Cicchella A. Patellofemoral Pain, Q-Angle, and Performance in Female Chinese Collegiate Soccer Players. Medicina (Kaunas) 2023,59,589. doi: 10.3390/medicina59030589. [CrossRef]
- Horn, T.; Brogden, C.; Greig, M. Isokinetic profiling of elite youth footballers: informing selection of a practicable and efficacious isokinetic screening test. Res Sports Med. 2023,31,125-136. doi: 10.1080/15438627.2021.1943392. [CrossRef]
- Herbawi, F.; Lozano-Lozano, M.; Lopez-Garzon, M.; Postigo-Martin, P.; Ortiz-Comino, L.; Martin-Alguacil, J.L.; Arroyo-Morales, M.; Fernandez-Lao, C. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. Int J Environ Res Public Health. 2022,19,6764. doi: 10.3390/ijerph19116764. [CrossRef]
- Chaney, G.K.; Krause, D.A.; Hollman, J.H.; Anderson, V.A.; Heider, S.E.; Thomez, S.; Vaughn, S.N.; Schilaty, N.D. Recurrence quantification analysis of isokinetic strength tests: A comparison of the anterior cruciate ligament reconstructed and the uninjured limb. Clin Biomech (Bristol, Avon) 2023,104,105929. doi: 10.1016/j.clinbiomech.2023.105929. [CrossRef]
- Levin, A.; Wyman, J. The Viscous Elastic Properties of Muscle. Proceedings of The Royal Society B: Biological Sciences 1927, 101, 218-243. doi: 10.1098/RSPB.1927.0014Corpus. [CrossRef]
- Hislop, H.J.; Perrine, J.J. The isokinetic concept of exercise. Phys Ther. 1967,47,114-7.
- Kataoka, R.; Spitz, R.W.; Wong, V.; Bell, Z.W.; Yamada, Y.; Song, J.S.; Hammert, W.B.; Dankel, S.J.; Abe, T.; Loenneke, J.P. Sex segregation in strength sports: Do equal-sized muscles express the same levels of strength between sexes? Am J Hum Biol. 2023,35, e23862. doi: 10.1002/ajhb.23862. [CrossRef]
- Sprouse, B.; Alty, J.; Kemp, S.; Cowie, C.; Mehta, R.; Tang, A.; Morris, J.; Cooper, S.; Varley, I. The football Association Injury and Illness Surveillance Study: The Incidence, Burden and Severity of Injuries and Illness in Men’s and Women’s International Football. Sport. Med. 2020, 28, 1–20. [CrossRef]
- Harvey, W.F.; Niu, J.; Zhang, Y.; McCree, P.I.; Felson, D.; Nevitt, M.; Xu, L.; Aliabadi, P.; Hunter, D.J. Knee alignment differences between Chinese and Caucasian subjects without osteoarthritis. Ann. Rheum. Dis. 2008, 67, 1524–1528. [CrossRef]
- Nicholson, G.; Bennett, T.; Thomas, A.; Pollitt, L.; Hopkinson, M.; Crespo, R.; Robinson, T.; Price, R.J. Inter-limb asymmetries and kicking limb preference in English premier league soccer players. Front Sports Act Living. 2022,4, 982796. doi: 10.3389/fspor.2022.982796. [CrossRef]
- Almosnino, S.; Dvir, Z.; Bardana, D.D.; Diaconescu, E.D.; Stevenson, J.M. Ascertaining maximal voluntary effort production during isokinetic knee strength testing of anterior cruciate ligament-reconstructed patients. Am J Phys Med Rehabil. 2014,93,169-81. doi: 10.1097/PHM.0000000000000041. [CrossRef]
- Pieters, D.; Witvrouw, E.; Wezenbeek, E.; Schuermans, J. Value of isokinetic strength testing for hamstring injury risk assessment: Should the 'strongest' mates stay ashore? Eur J Sport Sci. 2022 ,22, 257-268. doi: 10.1080/17461391.2020.1851774. [CrossRef]
- Lutz, F.D.; Cleary, C.J.; Moffatt, H.M.; Sullivan, V.E.; LaRoche, D.P.; Cook, S.B. Comparison of the H/Q Ratio Between the Dominant and Nondominant Legs of Soccer Players: A Meta-Analysis. Sports Health. 2022,19417381221095096. doi: 10.1177/19417381221095096. [CrossRef]
- Dvir, Z.; Müller, S. Multiple-Joint Isokinetic Dynamometry: A Critical Review. Journal of Strength and Conditioning Research 34, 587-601. doi: 10.1519/JSC.0000000000002982. [CrossRef]
- Claudino, J.G.; Cardoso Filho, C.A.; Bittencourt, N.F.N., Gonçalves, L.G.; Couto, C.R.; Quintão, R.C.; Reis, G.F.; de Oliveira Júnior, O.; Amadio, A.C.; Boullosa, D.; Serrão, J.C. Eccentric Strength Assessment of Hamstring Muscles with New Technologies: A Systematic Review of Current Methods and Clinical Implications. Sports Med Open. 2021, 7,10. doi: 10.1186/s40798-021-00298-7. [CrossRef]
- Möck, S.; Happ, K.; Wirth, K. The evaluation of strength imbalances as risk factor for contactless injuries of the knee and thigh: a critical review. J Sports Med Phys Fitness. 2023,63,685-695. doi: 10.23736/S0022-4707.23.14501-4. [CrossRef]
- Winter, D.A.; Wells, R.P.; Orr, G.W. Errors in the use of isokinetic dynamometers. Eur J Appl Physiol Occup Physiol. 1981,46,397-408. doi: 10.1007/BF00422127. [CrossRef]
- Green B, Bourne MN, Pizzari T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: a systematic review and meta-analysis. Br J Sports Med. 2018 Mar;52(5):329-336. doi: 10.1136/bjsports-2017-098101. [CrossRef]
- Schwartz, F.P.; Bottaro, M.; Celes, R.S.; Brown, L.E.; Nascimento, F.A. The influence of velocity overshoot movement artifact on isokinetic knee extension tests. J Sports Sci Med. 2010,9,140-6.
- Brown, L.; Whitehurst, M.; Findley, B.W.; Gilbert, R.; Buchalter, D.N. Isokinetic load range during shoulder rotation exercise in elite male jounior players. J. Strength Cond. Res. 1995,9,160–164.
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [CrossRef]
- Tredinnick, T.J; Duncan, P.W. Reliability of Measurements of Concentric and Eccentric Isokinetic Loading. Physical Therapy 1988, 68, 656–659. Doi:10.1093/ptj/68.5.656. [CrossRef]
- Claudino, J.G.; Cardoso, Filho C.A.; Bittencourt, N.F.N.; Gonçalves, L.G.; Couto, C.R.; Quintão R.C.; Reis, G.F.; de Oliveira Júnior O.; Amadio, A.C.; Boullosa, D.; Serrão, J.C. Eccentric Strength Assessment of Hamstring Muscles with New Technologies: a Systematic Review of Current Methods and Clinical Implications. Sports Med Open. 2021,7,10. doi: 10.1186/s40798-021-00298-7. [CrossRef]
- Li, R.C.; Wu, Y.; Maffulli, N.; et al. Eccentric and concentric isokinetic knee flexion and extension: a reliability study using the Cybex 6000 dynamometer. British Journal of Sports Medicine 1996, 30,156-160. [CrossRef]
- Steiner, L.A.; Harris, B.A.; Krebs, D.E. Reliability of eccentric isokinetic knee flexion and extension measurements. Archives of Physical Medicine and Rehabilitation 1993, 74, 1327-1335. Doi: 10.1016/0003-9993(93)90088-R. [CrossRef]
- Lund, H.; Søndergaard, K.; Zachariassen, T.; Christensen, R.; Bülow, P.; Henriksen, M.; Bartels, E.M.; Danneskiold-Samsøe, B.; Bliddal, H. Learning effect of isokinetic measurements in healthy subjects, and reliability and comparability of Biodex and Lido dynamometers. Clin Physiol Funct Imaging 2005,25,75-82. doi: 10.1111/j.1475-097X.2004.00593. x. [CrossRef]
- Feiring, D.C.; Ellenbecker, T.S.; Derscheid, G.L. Test-retest reliability of the biodex isokinetic dynamometer. J Orthop Sports Phys Ther. 1990,11, 298-300. doi: 10.2519/jospt.1990.11.7.298. [CrossRef]
- Brígido-Fernández, I.; García-Muro San José, F.; Charneco-Salguero, G.; Cárdenas-Rebollo, J.M.; Ortega-Latorre, Y.; Carrión-Otero, O.; Fernández-Rosa, L. Knee Isokinetic Profiles and Reference Values of Professional Female Soccer Players. Sports (Basel). 2022,10,204. doi: 10.3390/sports10120204. [CrossRef]
- Zhang, Q.; Léam, A.; Fouré, A.; Wong, D.P.; Hautier, C.A. Relationship Between Explosive Strength Capacity of the Knee Muscles and Deceleration Performance in Female Professional Soccer Players. Front Physiol. 2021,12,723041. doi: 10.3389/fphys.2021.723041. [CrossRef]
- Parpa, K.; Michaelides, M.A. The Effect of Transition Period on Performance Parameters in Elite Female Soccer Players. Int J Sports Med. 2020, 41,528-532. doi: 10.1055/a-1103-2038. [CrossRef]
- Eustace, S.J.; Morris, R.; Tallis, J.; Page, R.M.; Greig, M. The influence of angle-specific torque of the knee flexors and extensors on the angle-specific dynamic control ratio in professional female soccer players. J Sports Sci. 2022,40,1235-1242. doi: 10.1080/02640414.2022.2061251. [CrossRef]
- Manson, S. A.; Brughelli, M.; Harris, N.K. Physiological Characteristics of International Female Soccer Players. Journal of Strength and Conditioning Research 2014, 28, 308-318. doi: 10.1519/JSC.0b013e31829b56b1. [CrossRef]
- Hannon, J.P.; Wang-Price, S.; Garrison, J.C.; Goto, S.; Bothwell, J.M.; Bush, C.A. Normalized Hip and Knee Strength in Two Age Groups of Adolescent Female Soccer Players. J Strength Cond Res. 2022, 36, 207-211. doi: 10.1519/JSC.0000000000003420. [CrossRef]
- Chrisman, S.P.; O'Kane, J.W.; Polissar, N.L.; Tencer, A.F.; Mack, C.D.; Levy, M.R.; Schiff, M.A. Strength and jump biomechanics of elite and recreational female youth soccer players. J Athl Train. 2012,47,609-15. doi: 10.4085/1062-6050-47.6.01. [CrossRef]
- Andrade, M. dos S.; De Lira, C.A.; Koffes, Fde C.; Mascarin, N.C.; Benedito-Silva, A.A.; Da Silva AC. Isokinetic hamstrings-to-quadriceps peak torque ratio: the influence of sport modality, gender, and angular velocity. J Sports Sci. 2012, 30,547-53. doi: 10.1080/02640414.2011.644249. [CrossRef]
- Risberg, M.A.; Steffen, K.; Nilstad, A.; Myklebust, G.; Kristianslund, E.; Moltubakk, M.M.; Krosshaug, T. Normative Quadriceps and Hamstring Muscle Strength Values for Female, Healthy, Elite Handball and Football Players. J Strength Cond Res. 2018,32,2314-2323. doi: 10.1519/JSC.0000000000002579. [CrossRef]
- Knapik, J.J.; Bauman, C.L.; Jones, B.H.; Harris, J.M.; Vaughan, L. Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. Am J Sports Med. 1991, 19, 76-81. doi: 10.1177/036354659101900113. [CrossRef]
- Vargas, V.Z.; Motta, C.; Peres, B.; Vancini, R.L.; Andre Barbosa De Lira, C.; Andrade, M.S. Knee isokinetic muscle strength and balance ratio in female soccer players of different age groups: a cross-sectional study. Phys Sportsmed. 2020, 48,105-109. doi: 10.1080/00913847.2019.1642808. [CrossRef]
- Ostenberg, A; Roos, E.; Ekdahl, C.; Roos, H. Isokinetic knee extensor strength and functional performance in healthy female soccer players. Scand J Med Sci Sports. 1998,257-64. doi: 10.1111/j.1600-0838. 1998.tb00480. x. [CrossRef]
- Rosene, J.M.; Fogarty, TD.; Mahaffey, B.L. Isokinetic Hamstrings: Quadriceps Ratios in Intercollegiate Athletes. J Athl Train. 2001, 36, 378-383.
- Fillyaw, M.; Bevins, T.; Fernandez L. Importance of correcting isokinetic peak torque for the effect of gravity when calculating knee flexor to extensor muscle ratios. Phys Ther. 1986, 66,23-31. doi: 10.1093/ptj/66.1.23. [CrossRef]
- Westing, S.H.; Seger, J.Y. Eccentric and concentric torque-velocity characteristics, torque output comparisons, and gravity effect torque corrections for the quadriceps and hamstring muscles in females. Int J Sports Med. 1989,10,175-80. doi: 10.1055/s-2007-1024896. [CrossRef]
- Jones, P.A. Isokinetics strength profile of female soccer players: between limb comparisons. John J. McMahon & Philip Graham-Smith ed. 38th International Society of Biomechanics in Sport Conference, Physical conference cancelled, Online Activities: July 20-24, 2020.
- Hill, A.V. The heat of shortening and dynamics constants of muscles. Proc. R. Soc. Lond. B. London: Royal Society. 1938, 126 (843): 136–195. doi:10.1098/rspb.1938.0050. [CrossRef]
- Bishop, C.; de Keijzer, K.L.; Turner, A.N.; Beato, M. Measuring Interlimb Asymmetry for Strength and Power: A Brief Review of Assessment Methods, Data Analysis, Current Evidence, and Practical Recommendations. J Strength Cond Res. 2023, 37,745-750. doi: 10.1519/JSC.0000000000004384. [CrossRef]

Table 1.
Summary of isokinetics testing of the knee in female soccer players.
| Author | Device | Age (years ± sd) | N | Level | Speed (deg/sec) | Results |
|---|---|---|---|---|---|---|
| Fillyaw 1986 | Cybex | 19 | 27 | collegiate | 60,240 | H/Q PT CON EXT: 54%, 51% |
| Jones 2020 | Kin Com | 21.2 ± 4.1 | 21 | prof | 60 | D/ND PT: CON EXT: 9.54%; CON FLEX: 10.95%. |
| EXT ECC: 9.92%; FLEX ECC: 13.05% | ||||||
| Ostenberg 1998 | Cybex II | 20.3 ± 4.1 | 101 | collegiate | 60,180 | D/ND PT CON EXT: 7.8 %, 6.46% |
| Brigido Fernandez 2022 | Isomed 2000 | 21.9 ± 4.19 | 68 | prof | 60, 180, 240 | D/ND CON FLEX: 8.2%, 6% ,6.5 % |
| D/ND CON EXT 5.6%, 3%, 3,6 % | ||||||
| H/Q CON: 52%, 57%, 62% | ||||||
| Westing 1989 | Lido | 20 | 20 | collegiate | 60,120,180,240,360 | H/Q CON: 46%,44%,45%,47%,50% |
| Knapik 1991 | Biodex | 18.9 | 138 | collegiate | 30 | H/Q CON:62% |
| Chrisman 2012 | Biodex 3 | 11-14 | 92 | young | 180, 300 | H/Q CON: 50% |
| D/ND CON EXT: 14% (elite), 22 % (recreational). | ||||||
| Rosene 2001 | Biodex Pro | 19.3± 1.3 | 10 | collegiate | 60,120,180 | HQ CON: 49.5%,57.8%,58.1 % |
| D/ND CON TW: 53.8%,57.7%, 55.2 % | ||||||
| Eustace 2022 | Biodex 4 | 21.30 ± 4.44 year | 52 | prof | 60 | PT CON: APT higher in seniors. |
| Vargas 2019 | Biodex 4 | 18.21 ± 0.41ƚ | 19 | prof | 60,240 | H/Q: P CON EXT 44,9 % and 28% |
| 240 | H/Q PT ECC EXT: 35.4% | |||||
| 240 | H/Q W CON EXT: 36.1% | |||||
| Hannon 2022 | Biodex 4 | 1-14, 15-18 | 64 | young | 60,180 | D/ND PT CON EXT: 3.5% (11-14 ) and 3.2 % (14-18) |
| PT CON FLEX: 6% (11-14) AND 2% (15-18). | ||||||
| H/Q EXT CON = 50% | ||||||
| Zhang 2021 | Contrex | 24.7±4.2 | 14 | prof | 30 (ECC),60,240 | MEAN PT D/ND: EXT : - 1.17% , -0.35%, -1.17% |
| FLEX: 0.5%,2.1%, -3.4% | ||||||
| Parpa 2020 | Humac | 23.6±4.3 | 18 | prof | 60 | D/ND: EXT: - 2.1%; FLEX: 1.96 % |
| H/Q CON EXT= 1.3% R; 1 % L | ||||||
| Eustace 2019 | Biodex 4 | 21.31 ± 4.51 | 17 | elite | 60,180,270 | D/ND CON EXT: -2,4%, 0.22%, -2% |
| 16.91 ± 1.16 17 | 17 | young | D/ND: -1,7.8; 5.3 % | |||
| D/ND ECC EXT: 14.9%, 6.6%,9.7 % | ||||||
| Manson 2014 | Cybex Norm | 19-36 | 15 | pro | 60 | H/Q PT CON: 25% |
| H/Q ECC PT: 10 % | ||||||
| Risberg 2018 | Rev 9000 | 29 ±4 | 196 | collegiate | 60 | H/Q CON: 59.6% |
| Andrade 2012 | Biodex | 21.3±5.5 | 17 | olympic | 60,300 | H/Q CON:54%, 72% |
H/Q: hamstrings/quadriceps ratio; D: dominant leg; ND: non-dominant leg; ECC: eccentric contraction; CON: concentric contraction; PT: peak torque; MW: maximum work;W: power; APT: angle at peak torque; L: left; R: right; EXT: extension; FLEX: flexion; Speeds are in concentric mode, if not differently specified.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



