
Submitted:
12 June 2023
Posted:
12 June 2023
You are already at the latest version
Abstract
Despite the high prevalence of epilepsy in individuals with autism spectrum disorder (ASD) there is little information regarding whether seizure characteristics and treatment effectiveness change across age. Using an on-line survey, seizure characteristics, effectiveness of antiepileptic treatments, comorbidities and ASD diagnosis were collected from individuals with ASD and seizures. We previously reported overall general patterns of treatment effectiveness but did not examine the effect of seizure characteristics or age on antiepileptic treatment effectiveness. Such information would improve the personalized medicine approach to the treatment of seizures in ASD. Survey data from 570 individuals with ASD and clinical seizures were analyzed. Seizure severity (seizure/week) decreased with age of onset of seizures, plateauing in adolescence, with a greater reduction in generalized tonic clonic (GTC) seizures with age. Seizure severity was worse in those with genetic disorders, neurodevelopmental regression (NDR) and poor sleep maintenance. Carbamazepine and oxcarbazepine were reported to be more effective when seizures started in later childhood while surgery and the Atkin’s/Modified Atkin’s Diet (A/MAD) were reported to be more effective when seizures started early in life. A/MAD and the ketogenic diet were reported to be more effective in those with NDR. Interestingly, atypical Landau-Kleffner syndrome was associated with mitochondrial dysfunction and NDR, suggesting a novel syndrome. These interesting findings need to be verified in independent, prospectively collected cohorts, but none-the-less these data provide some insight into novel relationships that may assist in a better understanding of epilepsy in ASD and providing insight into personalizing epilepsy care in ASD.
Keywords:
antiepileptic drugs
; age
; autism spectrum disorder
; epilepsy
; ketogenic diet
; mitochondrial dysfunction
; modified Atkins diet
; neurodevelopmental regression
; seizures
1. Introduction
Autism spectrum disorder (ASD) is a behaviorally defined disorder that is estimated to affect 2% or more of children in the United States [1]. Some of the most challenging aspects in medically managing children with ASD are the medical comorbidities associated with ASD. A recent retrospective analysis of medical claims data suggests that a subgroup of about 24% of children with ASD have an unusual high number of comorbid conditions [2] while other studies report an average of 4-5 comorbidities per child [3]. Comorbidities are wide ranging and include, intellectual disability, sensory sensitivity, immune problems such as allergic rhinitis [4], gastrointestinal (GI) abnormalities [5] such as irritable bowel syndrome [4], sleep problems [6], psychiatric conditions such as attention deficit hyperactivity disorder [7] and anxiety [8], metabolic conditions such as mitochondrial dysfunction (MD) [9] and cerebral folate deficiency (CFD) [10] and neurological conditions such seizures and epilepsy [11].
Epilepsy is one of the most common comorbid conditions associated with ASD. Individuals with ASD have a 3-to-22-fold increased risk for developing seizures as compared to the typically developing population [12] and clinical studies estimate that seizures co-occur in 25% [13] and 46% [14] of those with ASD. Recent systematic reviews estimate the prevalence of epilepsy in ASD to be 6.3% [15] and 12.1% [16]. Furthermore, up to 86% of those with ASD, many of them without clinical seizures, demonstrate subclinical epileptiform discharges (SEDs) on electroencephalograph (EEG) [17,18,19] and one study using magnetoencephalography has linked a unique pattern of SEDs to ASD diagnosis [20]. Thus, ASD appears to have a complex relationship with epilepsy.
Because there are a wide variety of treatments for seizures in ASD, including anti-epileptic drugs (AEDs), nutritional supplements, vitamins, special diets and other alternative medical treatments [17], we previously conducted an online survey where caretakers of individuals with ASD rated the perceived ability of standard and alternative treatment to improve or worsen seizures [18]. The analysis of the 733 respondents demonstrated that, in general, four AED and four non-AED treatments were beneficial for controlling seizures while not causing adverse effects on behavior, sleep and cognition.
Although the results from our previous study were interesting and informative, it only provided an assessment of potential treatments that would be generally helpful. However, as discussed below, we know that ASD has marked heterogeneity which might affect the response to seizure treatment. The influence of individual characteristics of individuals with ASD has not been investigated. Thus, in this article we use the previously collected survey data to examine the effect of important ASD and epilepsy characteristics on response to seizure treatment.
One of the possible reasons for the heterogeneity in response to epilepsy treatment in ASD may be the various medical comorbidities associated with seizures and epilepsy in ASD. For example, mitochondrial disease increases the prevalence of epilepsy in those with ASD [9]. This is significant since 5% of children with ASD have mitochondrial disease and 30% or more exhibit MD [9]. CFD is estimated to occur in 38% of those with ASD with 75% of those demonstrating epilepsy [10]. Additionally, many genetic syndromes associated with ASD are also associated with epilepsy [17], especially those genetic syndrome where gene variants affect synaptic plasticity, ion channels, neurotransmitter receptors and synaptic structure and function [21]. There is also evidence that seizure characteristics are associated with ASD characteristics. For example, children with ASD who experience neurodevelopmental regression (NDR) [22] have a worse prognosis if the NDR is heralded by a seizure [23].
There is some evidence that the types and severity of seizures may vary with age in ASD [24]. Thus, we hypothesized that the effectiveness of epilepsy treatments varies with age and believe this is due to the atypical course of brain development in ASD. For example, epilepsy in ASD is many times associated with genetic abnormalities which not uncommonly cause congenital brain malformation such as neuronal migration disorders [25]. Epilepsy in such disorders tends to start early in life [26], although studies do suggest this does depend on the location of the malformation, at least for focal cortical dysplasia [27]. Other data have demonstrated that brain growth is altered in those with ASD [28] with implication of differences in age-dependent neuronal synaptic development [29] and white matter organization [30]. Although many alternation in brain development are believe to occur in early childhood, other studies suggest alteration in brain maturation extend into adolescence [31]. Indeed, a recent study suggests age-dependent dysregulation in GABAergic and glutamate signaling pathways starting in adolescence and extending into adulthood [32]. Thus, given the dynamic changes in brain development across childhood, adolescence, and young adulthood, it is likely that different ages may be associated with different seizure characteristics and treatment responses.
Thus, we investigated variations in seizure characteristics, regression profiles, medical comorbidities, and treatment effectiveness in those with ASD using our previously collected survey data to examine variations in these characteristics, particularly with respect to age of seizure onset. As this survey was conducted in the past, it contains limitations with respect to the drugs and diagnostic criteria at the time. Despite this, we believe this data provides a starting point to understand seizure and epilepsy treatment in ASD in order to despite future prospective studies on seizure treatment in ASD.
2. Materials and Methods
2.1. Institutional Review Board Approval
This study was conducted in accordance with the Declaration of Helsinki and the Institutional Review Board of the University of Texas Health Science Center at Houston (The senior author’s primary institution at the time of the study). Since the survey was anonymous and did not contain any unique identifying information or protected health information, the study qualified for category 2 exempt status according to 45 CFR 46.101(b) and did not require full-board review. Information regarding Institutional Review Board approval and contact information was provided on the first page of the survey. The survey did not record any identifying information of the responder nor did it collect any protected health information identifiers, so data was automatically deidentified for analysis.
2.2. Survey
The survey was designed using the principles outlined by Keenan [16] and implemented with the SurveyMethods, Inc. website software (www.SurveyMethods.com). The survey was developed based on the consensus of an expert panel as part of the Elias Tembenis Seizures Think Tank specifically focusing on the treatment of seizure in ASD as described in our previous publication [18].
Basic information was collected including age, gender, ASD DSM-IV-TR based diagnosis and developmental profile, common associated comorbid medical conditions including genetic disorders, prematurity, intellectual disability (ID), MD, growth, sleep, GI disorders, allergies, and sensory disorders. The DSM-IV-TR was the current version during the data collection period. Since sensory symptoms were not included in the DSM-IV-TR diagnostic criteria, they are considered comorbidities in this study.
Specific information was obtained regarding seizure characteristics. The age at which seizures started was asked. Multiple seizure types could be indicated, including generalized tonic clonic (GTC), focal and absence. In addition, multiple epilepsy syndromes could also be indicated, including typical (LKS) or atypical (aLKS) Landau-Kleffner syndrome, SEDs, Lenox-Gastaut syndrome (LGS) and/or infantile spasms (IS). Seizure severity, as represented by the seizure frequency (seizures per week), was queried for periods in which the seizures were the worst and best controlled. Participants indicated whether the seizures resolved and, if so, the age at which the seizures resolved. If the seizures did not resolve, the patient was considered to have non-resolved epilepsy.
Following collection of this basic descriptive information, information on the effectiveness of a wide range of treatments was collected. The respondent rated each treatment that the individual with ASD used on a seven-point scale, including the effect on seizures, sleep, communication, behavior, attention, and mood. Any adverse effects could also be reported. Treatments were divided into AED treatment, other seizure treatments, dietary therapies, supplements and alternative therapies.
2.3. Participants
An invitation for the on-line survey was posted on the website and in email newsletters of multiple autism advocacy groups including the Autism Research Institute, Autism Speaks, Autism Society of America and over 30 other local and national ASD support groups for parents of individuals with ASD. A control survey which collected data on children with ASD without seizures was also included in our original study, but it not used in the analysis for the current study. The number of participants with clinical seizures and seizure characteristic information completed in the survey was 570.
2.4. Statistical Analysis
Ratings were converted into an ordinal scale ranging from 1 to 7 for analysis: substantial negative effect (1), a moderate negative effect (2), a mild negative effect (3), no effect (4), a mild positive effect (5), a moderate positive effect (6), and a substantial positive effect (7). Although the response scale was ordinal, the response distribution was found to be normally distributed allowing the use of parametric analyses for treatment ratings.
Several variables are used to describe seizure characteristics (see Supplementary Table S1 for a list of patient and seizure characteristics). Non-resolved epilepsy refers to individuals in which seizures were contining at the time of the survey. Duration of epilepsy refers to the number of years that the child experienced epilesy and was only relevent in those in which seizures resolved.
As this study was designed to look at the assocaition among variables, regression analysis was felt to be the best method for extracting such associations. Examining combinations of treatments would decrease the number of cases to the extent that a valid analysis could not be performed so each epilepsy treatment was examing seperately.
Other continous variables were also found to be normally distributed. Continuous dependent variables were analyzed using the generlized linear model with dichotmous variables for categorical factors and covariates for contiuous measures. Note that some individuals could have multiple seizure types and multiple ASD diagnoses, so the analysis provided a determination of these specific seizure types and ASD diagnosis independent of the whether other seizure types and ASD diagnosis were present. When independent variables were dichotmous factors, logistic regression was implemented.
The analysis on seizure treatments or patient charaterisic was conducted on the data from each seizure treatment or patient chracteristic individually. Thus, each treatment represents a separate dataset and the use of linear regression to analyze all factors at once eliminated the need for any post-hoc comparisons. Thus, no formal multiple comparison correction is necessary. However, because of the large number of variables being analyzed, alpha was set to p<=0.01 to be conservative.
3. Results
The general characteristics of children with clinical seizures overall and for specific epilepsy syndromes is provided in Supplementary Table S1. As seen from this table, most individuals with ASD were male (77.9%) with mean age of seizures onset in early childhood (5 y 11m) with a diagnosis of Autistic Disorder (71.7%).
The results are divided into several parts. First, the changes in seizure characteristics across the age of onset were examined. Second, the relationship between specific patient characteristics and seizures was examined. Third, the relation between treatment effectiveness ratings and patient characteristics, including age of onset, was examined. Fourth, rare epilepsy syndromes, specifically IS, LKS, aLKS and LGS were examined in detail. For our analysis, as stated above seizure severity is measured as seizures per week when seizures were under the worst and best control.
3.1. Seizure Characteristics across the age span
3.1.1. Seizure Severity vs. Age of Onset
Seizure severity when the seizures were under the worst control demonstrated a curvilinear relationship with age of onset such that seizure severity decreased with age of seizure onset, being most severe if starting in childhood and then decreasing and plateaued for those with seizure onset in adolescence [Linear: χ2(1)=17.73, p≤0.001; β=-0.434; Curvilinear: χ2(1)=6.70, p≤0.01; β=0.01]. However, for those with GTC seizures, this decrease with age of onset was accentuated [interaction with linear component: χ2(1)=6.65, p≤0.01; β=-0.129]. In other words, it appears that generalized GTC and non-GTC seizures are just as likely when seizures start early in life while non-GTC seizures seem to predominate as age of seizure onset increases.
For those who experienced NDR (27.7% of the sample), seizure severity when the seizures were under the worst control was more severe by about 1 seizure per week [χ2(1)=8.95, p≤0.01; β=1.188]. Similarly, for those who experienced absence seizures, seizure frequency was more severe by about 1 seizure every 4 days [χ2(1)=21.33, p≤0.001; β=1.657].
Seizure severity when the seizures were under the best control was not related to age but was worse in those who experienced absence seizures by about 1 seizure every 4 days [χ2(1)=21.33, p≤0.001; β=1.657] and better in those who experienced GTC seizures by about 1 seizure every week [χ2(1)=15.39, p≤0.001; β=-1.001].
Figure 1.
Seizure severity (as indexed by seizure frequency / week when seizures under the worse control) by age of onset of seizures for those with generalized seizures and those with non-generalized seizures. Size of the circle is proportional to the number of responders with the specific frequency.
Figure 1.
Seizure severity (as indexed by seizure frequency / week when seizures under the worse control) by age of onset of seizures for those with generalized seizures and those with non-generalized seizures. Size of the circle is proportional to the number of responders with the specific frequency.

3.1.2. Epilepsy Resolution
Non-resolved epilepsy (17.4% of the sample) was less likely if focal seizures were reported [χ2(1)=13.57, p≤0.001; β=-0.91 (-1.41,-0.44)].
3.1.3. Seizure Duration
Duration of epilepsy in those children in which epilepsy resolved (82.6% of the sample) was related to ASD diagnosis such that seizures continued 2.7 years and 3.8 years longer in Autistic Disorder and Asperger syndrome, respectively [χ2(1)=7.46, p≤0.01; β=2.68; χ2(1)=7.73, p≤0.01; β=3.80]. Duration was also longer by 2.6 years for those who experienced absence seizures [χ2(1)=10.39, p≤0.001; β=2.63].
3.2. Relation Between Patient Characteristics and Seizures
3.2.1. Neurodevelopmental Regression in Epilepsy
Risk of NDR increased with seizure frequency when seizures were at their worst control [χ2(1)=7.14, p≤0.01; OR 1.06 (1.02. 1.10)]. Seizure severity, seizure resolution, seizure type or ASD diagnosis were not related to any trigger variable.
3.2.2. Comorbidities and Epilepsy: General Medical Conditions
The relationship between seizure variables and the general medical conditions of prematurity, cerebral palsy, mitochondria disorder, microcephaly, macrocephaly, ID, genetic disorders and growth failure are reported in this section.
Age of seizure onset was 1.9 years earlier for those with mitochondrial [χ2(1)=6.18, p≤0.01; β=-1.872] disorders and 1.7 years later in those with macrocephaly [χ2(1)=6.00, p≤0.01; β=1.790].
Seizure severity when seizures were best controlled was more severe by 2.5 seizures per week for those with genetic disorders [χ2(1)=25.45, p≤0.001; β=2.492] and 1.7 seizures per week better in those with microcephaly [χ2(1)=6.508, p≤0.01; β=-1.622].
Seizure severity when seizures were worst controlled was higher by 3.1 seizures per week for those with genetic disorders [χ2(1)=16.87, p≤0.001; β=3.099].
Seizures were less likely to resolve in those with ID [χ2(1)=7.03, p≤0.01; OR=0.45 (0.25, 0.81)]. In those in which seizures resolved, failure to thrive was associated with 3.0 more years of epilepsy [χ2(1)=6.12, p≤0.01; β=2.967].
GTC seizures were less likely in those born premature [χ2(1)=7.46, p≤0.01; OR=0.52 (0.33, 0.83)] and those with mitochondrial disorders [χ2(1)=6.43, p≤0.01; OR=0.47 (0.26, 0.84)], and more likely in those with ID [χ2(1)=4.82, p≤0.05; OR=1.56 (1.05, 2.32)].
Focal seizures were more likely with ID [χ2(1)=10.84, p≤0.001; OR=1.89 (1.30, 2.77)].
3.2.3. Comorbidities and Epilepsy: Sleep
Poor sleep maintenance was associated with a diagnosis of Autistic disorder [χ2(1)=9.13, p≤0.01; OR=1.80 (1.23, 2.64)] and an increased seizure frequency when seizures were at their best control [χ2(1)=6.72, p≤0.01; OR=1.08 (1.02, 1.14)]. Insomnia, Sleep Apnea and restless leg syndrome were not associated with seizure variables.
3.2.4. Comorbidities and Epilepsy: Gastrointestinal Symptoms
NDR was more likely with a diagnosis of enteritis [χ2(1)=14.08, p≤0.001; OR=2.38 (1.51, 3.74)], lymphoid nodular hyperplasia [χ2(1)=6.86, p≤0.01; OR=3.56 (1.38, 9.19)], dysbiosis [χ2(1)=15.28, p≤0.001; OR=2.56 (1.60, 4.10)] and GERD [χ2(1)=8.75, p≤0.01; OR=1.90 (1.24, 2.91)]. Constipation was not related to seizure variables.
3.2.5. Comorbidities and Epilepsy: Sensory
Increase sensitivity to sounds [χ2(1)=7.25, p≤0.01; OR=2.34 (1.26, 4.36)], touch [χ2(1)=18.13, p≤0.001; OR=4.68 (2.30, 9.51)] and smell [χ2(1)=9.06, p≤0.01; OR=3.50 (1.55, 7.93)] was more likely n Asperger syndrome. Decrease touch sensitivity was less likely with older seizure onset [χ2(1)=6.05, p≤0.01; OR=0.83 (0.71, 0.96)]. Decreased sensitivity to taste was more likely in Autistic Disorder [χ2(1)=6.77, p≤0.01; OR=15.06 (1.95, 116.03)] or Asperger syndrome [χ2(1)=14.28, p≤0.001; OR=27.37 (4.92, 152.33)].
3.2.6. Comorbidities and Epilepsy: Allergies
NDR was less likely in individuals in which allergies were reported to affect seizure severity [χ2(1)=7.16, p≤0.01; OR=0.57 (0.38, 0.86)] but specific effects of allergies within each season was not related to seizure variables.
3.3. Treatment Effectiveness Ratings
3.3.1. Overall Treatment Effectiveness Ratings
Table 1 provides the overall effectiveness ratings for the perceived effect on seizure control for all treatments. Treatments with average ratings statistically above 4.0 (“no effect”) are provided in bold. Treatments which were statistically above “no effect” and had an average rating of at least “mild” improvement (rating 5 or more) include primidone, valproic acid and levertirecetam for the antiepileptic drugs, surgery and steriods for other seizure treatments and the ketogenic diet (KD) and the Atkin’s / modified Atkin’s diet (A/MAD) for diets.
3.3.2. Changes in Effectiveness Rating vs Age of Onset
The effectiveness ratings of carbamazepine [χ2(1)=6.46, p≤0.01; β=0.07] and oxcarbazepine [χ2(1)=19.09, p≤0.001; β=0.15] increased with age of onset. As seen in Figure 2A, for individuals with seizures that start early in life these AEDs, on average, demonstrated little effectiveness due to the wide variability in the effectiveness ratings. However, for those with seizure onset in late childhood and adolescence, fewer individuals rated these AEDs as negatively effecting seizures and more rated these AEDs as having a positive effect on seizures.
The effectiveness of surgery [χ2(1)=29.61, p≤0.001; β=-0.37] decreased with the age of seizure onset. As seen in Figure 2B, surgery was rated as very effective in those with seizures which started in infancy and younger childhood. The effectiveness of spironolactone decreased with the age of onset of the seizures [χ2(1)=20.68, p≤0.001; β=-0.41]. As seen in Figure 2B, those with seizures that started in early childhood, spironolactone was rated as having no effect while those with seizures that started in adolescence, spironolactone appeared to have a negative effect.
As seen in Figure 2C, the A/MAD was rated as having an excellent effectiveness in those with seizures which started in infancy and early childhood [χ2(1)=41.61, p≤0.001; β=-0.15]. As seen in Figure 2D, Taurine appears to have good effectiveness ratings for those with seizures which started early in life but did not have much of an effect if seizure started after early childhood [χ2(1)=8.89, p≤0.01; β=-0.26].
3.3.3. Effectiveness Rating Across Seizure Types (GTC, Focal, Absence)
For those with GTC seizures, epilepsy surgery [χ2(1)=10.14, p≤0.001] and the A/MAD [χ2(1)=22.71, p≤0.001] were rated 1.89 (0.59) and 1.53 (0.32) points more effective while valproic acid [χ2(1)=6.00, p≤0.01] and steroids [χ2(1)=9.41, p≤0.01] were rated 0.56 (0.23) and 1.25 (0.41) points less effective, as compared to other treatments.
For those with focal seizures, spironolactone [χ2(1)=9.80, p≤0.01] was rated as 0.70 (0.22) points more effective while valproic acid [χ2(1)=8.64, p≤0.01] was rated 0.66 (0.22) points less effective, as compared to other treatments.
For absence seizures, steroids [χ2(1)=6.37, p≤0.01] and the KD [χ2(1)=14.35, p≤0.001] were rated 1.03 (0.41) and 1.38 (0.36) points more effective, respectively, while carbamazepine [χ2(1)=17.71, p≤0.001], surgery [χ2(1)=7.00, p≤0.01], spironolactone [χ2(1)=65.80, p≤0.001] were rated 1.28 (0.30), 1.57 (0.59), 1.94 (0.24) points less effective, respectively, as compared to other treatments.
3.3.4. Effectiveness Rating in Non-Resolved Seizures
For those with non-resolved epilepsy, levetiracetam [χ2(1)=8.07, p≤0.01] was rated as 1.15 (0.40) points more effective while phenytoin [χ2(1)=7.80, p≤0.01], surgery [χ2(1)=7.42, p≤0.01], GFCF diet [χ2(1)=8.50, p≤0.01], HBOT [χ2(1)=14.82, p≤0.001] and chelation [χ2(1)=7.31, p≤0.01] were rated as 1.31 (0.47), 2.61 (0.96), 0.53 (0.18), 1.42 (0.37) and 0.87 (0.25) points less effective, respectively.
3.3.5. Effectiveness Rating Across Seizure Severity
For seizure severity, as determined by seizures when they were under the worst control, surgery [χ2(1)=32.07, p≤0.001] was rated as 0.82 (0.15) points more effective for each increase in a seizure per week while zonisamide [χ2(1)=6.14, p≤0.01] and A/MAD [χ2(1)=13.72, p≤0.001] were rated as 0.13 (0.05) and 0.15 (0.04) points less effective for each increase in a seizure per week.
For seizure severity, as determined by seizures when they were under the best control, valproic acid [χ2(1)=17.49, p≤0.001], topiramate [χ2(1)=7.09, p≤0.01] and spironolactone [χ2(1)=55.26, p≤0.001] were rated as 0.15 (0.04), 0.11 (0.04) and 0.25 (0.03) points less effective for each increase in a seizure per week.
3.3.5. Effectiveness Rating Across Autism Diagnosis
Phenytoin [χ2(1)=7.88, p≤0.01] was rated as 1.71 (0.61) less effective when the diagnosis included PDD-NOS while gabapentin [χ2(1)=6.25, p≤0.01] was rated as 1.59 (0.63) less effective when the diagnosis included Asperger syndrome.
3.3.6. Effectiveness Rating with Neurodevelopmental Regression
The KD [χ2(1)=10.84, p≤0.001] and A/MAD [χ2(1)=48.98, p≤0.001] were 1.34 (0.41) and 2.70 (0.39) more effective when the child had a history of NDR.
3.3.7. Effectiveness Rating with Sex
Lamotrigine [χ2(1)=6.50, p≤0.01] and spironolactone [χ2(1)=57.18, p≤0.001] were 0.80 (0.31) and 2.18 (0.29) points more effective for individuals who were male.
3.4. Specific Epilepsy Syndromes
The survey captured patients with several epilepsy syndromes related to epilepsy including IS, LKS, aLKS and LGS. Thus, these groups were examined in detail.
3.4.1. Seizure Variables
Those with LKS were more likely to have a higher seizure severity as measured by seizure frequency at its worst control [χ2(1)=7.57, p≤0.01; OR 1.17 (1.05, 1.30)]. Those with aLKS were more likely to have NDR [χ2(1)=9.16, p≤0.01; OR 3.53 (1.56, 8.00)]. IS was less likely as age of seizure onset increased [χ2(1)=15.62, p≤0.001; OR 0.38 (0.23, 0.61)].
3.4.2. Comorbidities
Those with aLKS were more likely to have a mitochondrial disorder [χ2(1)=7.27, p≤0.01; OR 3.54 (1.41. 8.86)] while those with LGS were more likely to have a genetic syndrome [χ2(1)=8.25, p≤0.01; OR 5.50 (1.72. 17.58)] and ID [χ2(1)=7.99, p≤0.01; OR 4.97 (1.64. 15.10)].
3.4.3. Effectiveness of Treatments
Clonazepam [χ2(1)=6.65, p≤0.01] and zonisamide [χ2(1)=6.06, p≤0.01] were rated as 2.49 (0.97) and 2.76 (1.12) points less effective for those with aLKS. Felbamate [χ2(1)=7.41, p≤0.01] and A/MAD [χ2(1)=9.44, p≤0.01] were rated as 1.74 (0.64) and 1.90 (0.62) points more effective for LGS [χ2(1)=9.44, p≤0.01]. L-carnosine [χ2(1)=7.26, p≤0.01] was rated 1.35 (0.50) points better in those with IS.
4. Discussion
In this study, we used previously collected survey data to better understand how seizures are related to specific characteristics of individuals with ASD and better understand what factors might affect the effectiveness ratings of treatments for epilepsy.
4.1. Seizure Severity Improves with Age
Examining seizure severity across the age of seizure onset demonstrated that seizure frequency was much higher in children with early onset epilepsy, with seizure frequency decreasing significantly throughout childhood and plateauing in adolescence. Seizure severity appeared to be equally severe for those with GTC and non-GTC seizures early in life but the severity of GTC seizures drops to about half the severity of non-GTC seizures in adolescence. Earlier seizure onset was associated with mitochondrial disorders while relatively later onset seizures were associated with macrocephaly. Seizure severity was worse in those with genetic disorders, NDR and poor sleep maintenance.
4.2. Epilesy that does not resolve
Focal seizures and ID were associated with epilepsy that was less likely to resolve. In those in which seizures resolved, the number of years that the epilepsy lasted was longer in those that reported an Autistic Disorder or Asperger syndrome diagnosis, failure to thrive or those that reported absence seizures.
4.3. Effectiveness is Related to Age for some Treatments
Analysis of seizure treatments demonstrated interesting trends which are consistent with the epilepsy literature and other findings in this study. The data suggests that carbamazepine and oxcarbazepine, medications which primarily treat focal epilepsy, are rated as consistently having a more positive effect in older children and adolescents. Consistent with this, the data from this study also suggests that non-GTC seizures (which include focal seizures) are relatively more common in adolescents.
Surgery and A/MAD treatments appeared to be rated as primarily effective for those with seizures that started early in life. Children with early onset epilepsy tends to have neuronal migration and postmigration organizational abnormalities [26]. Such abnormalities are not uncommonly refractory to medications and may requiring surgical intervention [33,34]. This could explain why surgery tends to help with epilepsy that starts early in life in individuals with ASD. The A/MAD and KD appeared to be effective treatments, especially for seizures that started early in life. Further definition of this subgroup could indicate those in which dietary interventions should be started early in treatment.
4.4. Potential Mechanisums of Low Carbohydrate Diets
The A/MAD has many therapeutic mechanisms. Both the A/MAD and KD are believed to be helpful for treating underlying mitochondrial dysfunction [35] and data from this study suggests that those with mitochondrial dysfunction have seizure onset earlier in life. In addition, the KD and A/MAD were rated as more favorable in those with NDR, another factor which is associated with both classic mitochondrial disease [9,36] and mitochondrial dysfunction [37,38] in ASD. Further, NDR was associated with multiple GI pathological conditions. This is compelling as GI abnormalities are believed to be the result of a disrupted microbiome in ASD [39,40] and some of the therapeutic actions of the A/MAD may occur through normalization of the microbiome [41].
4.5. Effectiveness is Related to Seizure Severity for some Treatments
Interestingly, several treatments were rated as not effective for more severe seizures. For example, the effectiveness ratings of zonisamide, A/MAD, valproic acid and topiramate was inversely proportional to the seizure frequency while phenytoin, surgery, GFCF, HBOT and chelation were rated lower in those with epilepsy which did not resolve. The caveat to these findings is these treatments, such as surgery, are only prescribed when seizures are very severe and refractory which is also associated with a lower rate of successful control seizures. Thus, the ratings may be biased due to the underlying individuals to which they were prescribed.
4.6. Epilepsy Syndrome may Require Specific Treatments
Analysis of specific epilepsy syndromes revealed some interesting trends. Consistent with known characteristics of syndromes, those with LGS were more likely to have a genetic syndrome. ID and IS were associated with early onset of seizures. Interestingly, aLKS was associated with both mitochondrial dysfunction and NDR, suggesting that aLKS may be associated with an underlying characteristic of a subset of ASD children with NDR and mitochondrial abnormalities. While the greater effectiveness of Felbamate and A/MAD for LGS is not surprising, the lower rated effectiveness of Clonazepam and zonisamide for aLKS and higher rating of L-carnosine for IS were novel findings.
4.7. Identifying Patient Comorbidities Could Aid Treatment
The findings from this study demonstrate the unique characteristics of epilepsy in ASD and the potential ASD specific treatments that could be useful in ASD. For example, poor sleep maintenance, a common issue in children with ASD, was associated with increased seizure severity. Sleep is an important comorbidity to address as improvement in sleep can improve behavior [6] and quality of life for the whole family [42] as well as improve seizure control [43]. NDAR was also associated with increased seizure severity. Although the reason for NDAR remains enigmatic, both mitochondrial disease [9] and MD [37] have been linked to NDR in ASD and CFD, which appears to be not uncommon in ASD, is also associated with NDR [10]. Both of these metabolic disorders are treatable, so an investigation as to whether they are underlying comorbidities in individuals with ASD and epilepsy may provide an effective treatment pathway.
4.8. Study Limitations
This paper had some limitations. Data for this study was collected using an online survey which might lead to selection bias. Diagnoses of ASD and seizure disorders were not confirmed with standard clinical instruments. The collected data was retrospective in nature. Each treatment was considered in isolation as if it was given in a controlled fashion. It is possible that a caretaker other than the child’s parent filled out the survey. Finally, only 6% of children in the survey had a genetic condition, which may be an undersampling of this group. This study is limited by the self-reported nature of the study and the fact that newer AED and ASD treatments were not included in the study.
5. Conclusions
This study has revealed some interesting trends in the relationship between seizures onset, age, and ASD characteristics. A better understanding of the factors which modulate epilepsy severity in individuals with ASD will no doubt improve the ability to personalize treatment. Overall, the results suggest that multiple patient characteristics related to the effectiveness of seizure treatments, and those characteristics may be useful in guiding choice of treatments for each patient. Future research should focus on defining specific subgroups, if possible, to help better define diagnostic and treatment guidelines for those with ASD.
It is important to note that this paper focuses on the effect of treatments on seizure frequency. However, as discussed in detail in our previous paper, AED treatments generally worsen other symptoms, whereas non-AED treatments tended to improve other symptoms. So, it is important to consider both effects on seizure frequency on effect on other symptoms when considering treatments for a patient.
Further prospective clinical studies would be helpful to confirm and expand on these findings. Once these relationships are better understood, it may be possible to design an algorithm for selecting the most promising treatments for children with ASD and epilepsy in a personalized precision fashion in order to optimize outcomes.
Supplementary Materials
Supplementary Table 1: Patient Characteristics.
Author Contributions
Conceptualization: B.S.G., J.G, J.A., D.A.R. and R.E.F. methodology: J.A., R.E.F. formal analysis: B.S.G., R.E.F. writing—original draft preparation: B.S.G. and R.E.F. review and editing: B.S.G., J.G, J.A., D.A.R. and R.E.F. All authors have read and agreed to the published version of the manuscript.
Funding
The review did not receive any financial or grant support from any sources.
Institutional Review Board Statement
The study qualified for category 2 exempt status according to 45 CFR 46.101(b) as determined by the Institutional Review Board of the University of Texas Health Science Center at Houston.
Informed Consent Statement
Information regarding except status was provided on the first page of the survey before any information was entered into the survey.
Data Availability Statement
All data are presented within the article.
Conflicts of Interest
Dr Frye is funded by the BRAIN Foundation (Pleasanton, CA) to study mitochondrial dysfunction in individuals with ASD and epilepsy. The other authors declared no conflicts of interest.
References
- Maenner, M.J.; Shaw, K.A.; Baio, J.; EdS; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill Summ 2020, 69, 1-12. https://doi.org/10.15585/mmwr.ss6904a1. [CrossRef]
- Vargason, T.; Frye, R.E.; McGuinness, D.L.; Hahn, J. Clustering of co-occurring conditions in autism spectrum disorder during early childhood: A retrospective analysis of medical claims data. Autism research : official journal of the International Society for Autism Research 2019, 12, 1272-1285. https://doi.org/10.1002/aur.2128. [CrossRef]
- Soke, G.N.; Maenner, M.J.; Christensen, D.; Kurzius-Spencer, M.; Schieve, L.A. Prevalence of Co-occurring Medical and Behavioral Conditions/Symptoms Among 4- and 8-Year-Old Children with Autism Spectrum Disorder in Selected Areas of the United States in 2010. Journal of autism and developmental disorders 2018, 48, 2663-2676. https://doi.org/10.1007/s10803-018-3521-1. [CrossRef]
- Brondino, N.; Fusar-Poli, L.; Miceli, E.; Di Stefano, M.; Damiani, S.; Rocchetti, M.; Politi, P. Prevalence of Medical Comorbidities in Adults with Autism Spectrum Disorder. Journal of general internal medicine 2019, 34, 1992-1994. https://doi.org/10.1007/s11606-019-05071-x. [CrossRef]
- Holingue, C.; Newill, C.; Lee, L.C.; Pasricha, P.J.; Daniele Fallin, M. Gastrointestinal symptoms in autism spectrum disorder: A review of the literature on ascertainment and prevalence. Autism research : official journal of the International Society for Autism Research 2018, 11, 24-36. https://doi.org/10.1002/aur.1854. [CrossRef]
- Rossignol, D.A.; Frye, R.E. Psychotropic Medications for Sleep Disorders in Autism Spectrum Disorders. In Handbook of Autism and Pervasive Developmental Disorder: Assessment, Diagnosis, and Treatment, Matson, J.L., Sturmey, P., Eds.; Springer International Publishing: Cham, 2022; pp. 1191-1217.
- Dizitzer, Y.; Meiri, G.; Flusser, H.; Michaelovski, A.; Dinstein, I.; Menashe, I. Comorbidity and health services' usage in children with autism spectrum disorder: a nested case-control study. Epidemiol Psychiatr Sci 2020, 29, e95. https://doi.org/10.1017/S2045796020000050. [CrossRef]
- Foldes, S.T.; Jensen, A.R.; Jacobson, A.; Vassall, S.; Foldes, E.; Guthery, A.; Brown, D.; Levine, T.; Tyler, W.J.; Frye, R.E. Transdermal Electrical Neuromodulation for Anxiety and Sleep Problems in High-Functioning Autism Spectrum Disorder: Feasibility and Preliminary Findings. J Pers Med 2021, 11. https://doi.org/10.3390/jpm11121307. [CrossRef]
- Rossignol, D.A.; Frye, R.E. Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis. Molecular psychiatry 2012, 17, 290-314. https://doi.org/10.1038/mp.2010.136. [CrossRef]
- Rossignol, D.A.; Frye, R.E. Cerebral Folate Deficiency, Folate Receptor Alpha Autoantibodies and Leucovorin (Folinic Acid) Treatment in Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. J Pers Med 2021, 11. https://doi.org/10.3390/jpm11111141. [CrossRef]
- Anukirthiga, B.; Mishra, D.; Pandey, S.; Juneja, M.; Sharma, N. Prevalence of Epilepsy and Inter-Ictal Epileptiform Discharges in Children with Autism and Attention-Deficit Hyperactivity Disorder. Indian journal of pediatrics 2019, 86, 897-902. https://doi.org/10.1007/s12098-019-02977-6. [CrossRef]
- Volkmar, F.R.; Nelson, D.S. Seizure disorders in autism. J Am Acad Child Adolesc Psychiatry 1990, 29, 127-129. https://doi.org/10.1097/00004583-199001000-00020. [CrossRef]
- Hara, H. Autism and epilepsy: a retrospective follow-up study. Brain Dev 2007, 29, 486-490. https://doi.org/10.1016/j.braindev.2006.12.012. [CrossRef]
- Hughes, J.R.; Melyn, M. EEG and seizures in autistic children and adolescents: further findings with therapeutic implications. Clin EEG Neurosci 2005, 36, 15-20. https://doi.org/10.1177/155005940503600105. [CrossRef]
- Strasser, L.; Downes, M.; Kung, J.; Cross, J.H.; De Haan, M. Prevalence and risk factors for autism spectrum disorder in epilepsy: a systematic review and meta-analysis. Dev Med Child Neurol 2018, 60, 19-29. https://doi.org/10.1111/dmcn.13598. [CrossRef]
- Lukmanji, S.; Manji, S.A.; Kadhim, S.; Sauro, K.M.; Wirrell, E.C.; Kwon, C.S.; Jetté, N. The co-occurrence of epilepsy and autism: A systematic review. Epilepsy Behav 2019, 98, 238-248. https://doi.org/10.1016/j.yebeh.2019.07.037. [CrossRef]
- Frye, R.E.; Rossignol, D.; Casanova, M.F.; Brown, G.L.; Martin, V.; Edelson, S.; Coben, R.; Lewine, J.; Slattery, J.C.; Lau, C.; et al. A review of traditional and novel treatments for seizures in autism spectrum disorder: findings from a systematic review and expert panel. Front Public Health 2013, 1, 31. https://doi.org/10.3389/fpubh.2013.00031. [CrossRef]
- Frye, R.E.; Sreenivasula, S.; Adams, J.B. Traditional and non-traditional treatments for autism spectrum disorder with seizures: an on-line survey. BMC Pediatr 2011, 11, 37. https://doi.org/10.1186/1471-2431-11-37. [CrossRef]
- Precenzano, F.; Parisi, L.; Lanzara, V.; Vetri, L.; Operto, F.F.; Pastorino, G.M.G.; Ruberto, M.; Messina, G.; Risoleo, M.C.; Santoro, C.; et al. Electroencephalographic Abnormalities in Autism Spectrum Disorder: Characteristics and Therapeutic Implications. Medicina 2020, 56, 419.
- Lewine, J.D.; Andrews, R.; Chez, M.; Patil, A.A.; Devinsky, O.; Smith, M.; Kanner, A.; Davis, J.T.; Funke, M.; Jones, G.; et al. Magnetoencephalographic patterns of epileptiform activity in children with regressive autism spectrum disorders. Pediatrics 1999, 104, 405-418. https://doi.org/10.1542/peds.104.3.405. [CrossRef]
- Specchio, N.; Di Micco, V.; Trivisano, M.; Ferretti, A.; Curatolo, P. The epilepsy-autism spectrum disorder phenotype in the era of molecular genetics and precision therapy. Epilepsia 2022, 63, 6-21. https://doi.org/10.1111/epi.17115. [CrossRef]
- Barger, B.D.; Campbell, J.M.; McDonough, J.D. Prevalence and onset of regression within autism spectrum disorders: a meta-analytic review. Journal of autism and developmental disorders 2013, 43, 817-828. https://doi.org/10.1007/s10803-012-1621-x. [CrossRef]
- Tuchman, R.F.; Rapin, I. Regression in pervasive developmental disorders: seizures and epileptiform electroencephalogram correlates. Pediatrics 1997, 99, 560-566. https://doi.org/10.1542/peds.99.4.560. [CrossRef]
- Liu, X.; Sun, X.; Sun, C.; Zou, M.; Chen, Y.; Huang, J.; Wu, L.; Chen, W.X. Prevalence of epilepsy in autism spectrum disorders: A systematic review and meta-analysis. Autism 2022, 26, 33-50. https://doi.org/10.1177/13623613211045029. [CrossRef]
- Juric-Sekhar, G.; Hevner, R.F. Malformations of Cerebral Cortex Development: Molecules and Mechanisms. Annu Rev Pathol 2019, 14, 293-318. https://doi.org/10.1146/annurev-pathmechdis-012418-012927. [CrossRef]
- Simmons, R.; Martinez, A.B.; Barkovich, J.; Numis, A.L.; Cilio, M.R.; Glenn, O.A.; Gano, D.; Rogers, E.E.; Glass, H.C. Disorders of Neuronal Migration/Organization Convey the Highest Risk of Neonatal Onset Epilepsy Compared With Other Congenital Brain Malformations. Pediatr Neurol 2022, 127, 20-27. https://doi.org/10.1016/j.pediatrneurol.2021.11.005. [CrossRef]
- Wiwattanadittakul, N.; Suwannachote, S.; You, X.; Cohen, N.T.; Tran, T.; Phuackchantuck, R.; Tsuchida, T.N.; Depositario-Cabacar, D.F.; Zelleke, T.; Schreiber, J.M.; et al. Spatiotemporal distribution and age of seizure onset in a pediatric epilepsy surgery cohort with cortical dysplasia. Epilepsy Res 2021, 172, 106598. https://doi.org/10.1016/j.eplepsyres.2021.106598. [CrossRef]
- Yankowitz, L.D.; Herrington, J.D.; Yerys, B.E.; Pereira, J.A.; Pandey, J.; Schultz, R.T. Evidence against the "normalization" prediction of the early brain overgrowth hypothesis of autism. Mol Autism 2020, 11, 51. https://doi.org/10.1186/s13229-020-00353-2. [CrossRef]
- Guang, S.; Pang, N.; Deng, X.; Yang, L.; He, F.; Wu, L.; Chen, C.; Yin, F.; Peng, J. Synaptopathology Involved in Autism Spectrum Disorder. Front Cell Neurosci 2018, 12, 470. https://doi.org/10.3389/fncel.2018.00470. [CrossRef]
- Li, M.; Wang, Y.; Tachibana, M.; Rahman, S.; Kagitani-Shimono, K. Atypical structural connectivity of language networks in autism spectrum disorder: A meta-analysis of diffusion tensor imaging studies. Autism research : official journal of the International Society for Autism Research 2022, 15, 1585-1602. https://doi.org/10.1002/aur.2789. [CrossRef]
- O'Hearn, K.; Lynn, A. Age differences and brain maturation provide insight into heterogeneous results in autism spectrum disorder. Front Hum Neurosci 2022, 16, 957375. https://doi.org/10.3389/fnhum.2022.957375. [CrossRef]
- Zhang, P.; Omanska, A.; Ander, B.P.; Gandal, M.J.; Stamova, B.; Schumann, C.M. Neuron-specific transcriptomic signatures indicate neuroinflammation and altered neuronal activity in ASD temporal cortex. Proc Natl Acad Sci U S A 2023, 120, e2206758120. https://doi.org/10.1073/pnas.2206758120. [CrossRef]
- Licchetta, L.; Vignatelli, L.; Toni, F.; Teglia, A.; Belotti, L.M.B.; Ferri, L.; Menghi, V.; Mostacci, B.; Di Vito, L.; Bisulli, F.; et al. Long-term Outcome of Epilepsy and Cortical Malformations Due to Abnormal Migration and Postmigrational Development: A Cohort Study. Neurology 2022, 99, e23-e32. https://doi.org/10.1212/wnl.0000000000200352. [CrossRef]
- Guerrini, R.; Dobyns, W.B.; Barkovich, A.J. Abnormal development of the human cerebral cortex: genetics, functional consequences and treatment options. Trends Neurosci 2008, 31, 154-162. https://doi.org/10.1016/j.tins.2007.12.004. [CrossRef]
- Frye, R.E. Mitochondrial Dysfunction in Autism Spectrum Disorder: Unique Abnormalities and Targeted Treatments. Semin Pediatr Neurol 2020, 35, 100829. https://doi.org/10.1016/j.spen.2020.100829. [CrossRef]
- Shoffner, J.; Hyams, L.; Langley, G.N.; Cossette, S.; Mylacraine, L.; Dale, J.; Ollis, L.; Kuoch, S.; Bennett, K.; Aliberti, A.; et al. Fever plus mitochondrial disease could be risk factors for autistic regression. Journal of child neurology 2010, 25, 429-434. https://doi.org/10.1177/0883073809342128. [CrossRef]
- Singh, K.; Singh, I.N.; Diggins, E.; Connors, S.L.; Karim, M.A.; Lee, D.; Zimmerman, A.W.; Frye, R.E. Developmental regression and mitochondrial function in children with autism. Ann Clin Transl Neurol 2020, 7, 683-694. https://doi.org/10.1002/acn3.51034. [CrossRef]
- Rose, S.; Niyazov, D.M.; Rossignol, D.A.; Goldenthal, M.; Kahler, S.G.; Frye, R.E. Clinical and Molecular Characteristics of Mitochondrial Dysfunction in Autism Spectrum Disorder. Mol Diagn Ther 2018, 22, 571-593. https://doi.org/10.1007/s40291-018-0352-x. [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome 2017, 5, 10. https://doi.org/10.1186/s40168-016-0225-7. [CrossRef]
- Qureshi, F.; Adams, J.; Hanagan, K.; Kang, D.W.; Krajmalnik-Brown, R.; Hahn, J. Multivariate Analysis of Fecal Metabolites from Children with Autism Spectrum Disorder and Gastrointestinal Symptoms before and after Microbiota Transfer Therapy. J Pers Med 2020, 10. https://doi.org/10.3390/jpm10040152. [CrossRef]
- Lim, J.M.; Letchumanan, V.; Tan, L.T.; Hong, K.W.; Wong, S.H.; Ab Mutalib, N.S.; Lee, L.H.; Law, J.W. Ketogenic Diet: A Dietary Intervention via Gut Microbiome Modulation for the Treatment of Neurological and Nutritional Disorders (a Narrative Review). Nutrients 2022, 14. https://doi.org/10.3390/nu14173566. [CrossRef]
- Tilford, J.M.; Payakachat, N.; Kuhlthau, K.A.; Pyne, J.M.; Kovacs, E.; Bellando, J.; Williams, D.K.; Brouwer, W.B.; Frye, R.E. Treatment for Sleep Problems in Children with Autism and Caregiver Spillover Effects. Journal of autism and developmental disorders 2015, 45, 3613-3623. https://doi.org/10.1007/s10803-015-2507-5. [CrossRef]
- Nobili, L.; Beniczky, S.; Eriksson, S.H.; Romigi, A.; Ryvlin, P.; Toledo, M.; Rosenzweig, I. Expert Opinion: Managing sleep disturbances in people with epilepsy. Epilepsy Behav 2021, 124, 108341. https://doi.org/10.1016/j.yebeh.2021.108341. [CrossRef]
Figure 2.
Changes in effectiveness ratings as a function of age of seizure onset for (A) antiepileptic drugs, (B) other seizure treatments, (C) dietary treatments and (D) supplements. Size of the circle is proportional to the number of responders with the specific frequency.
Figure 2.
Changes in effectiveness ratings as a function of age of seizure onset for (A) antiepileptic drugs, (B) other seizure treatments, (C) dietary treatments and (D) supplements. Size of the circle is proportional to the number of responders with the specific frequency.
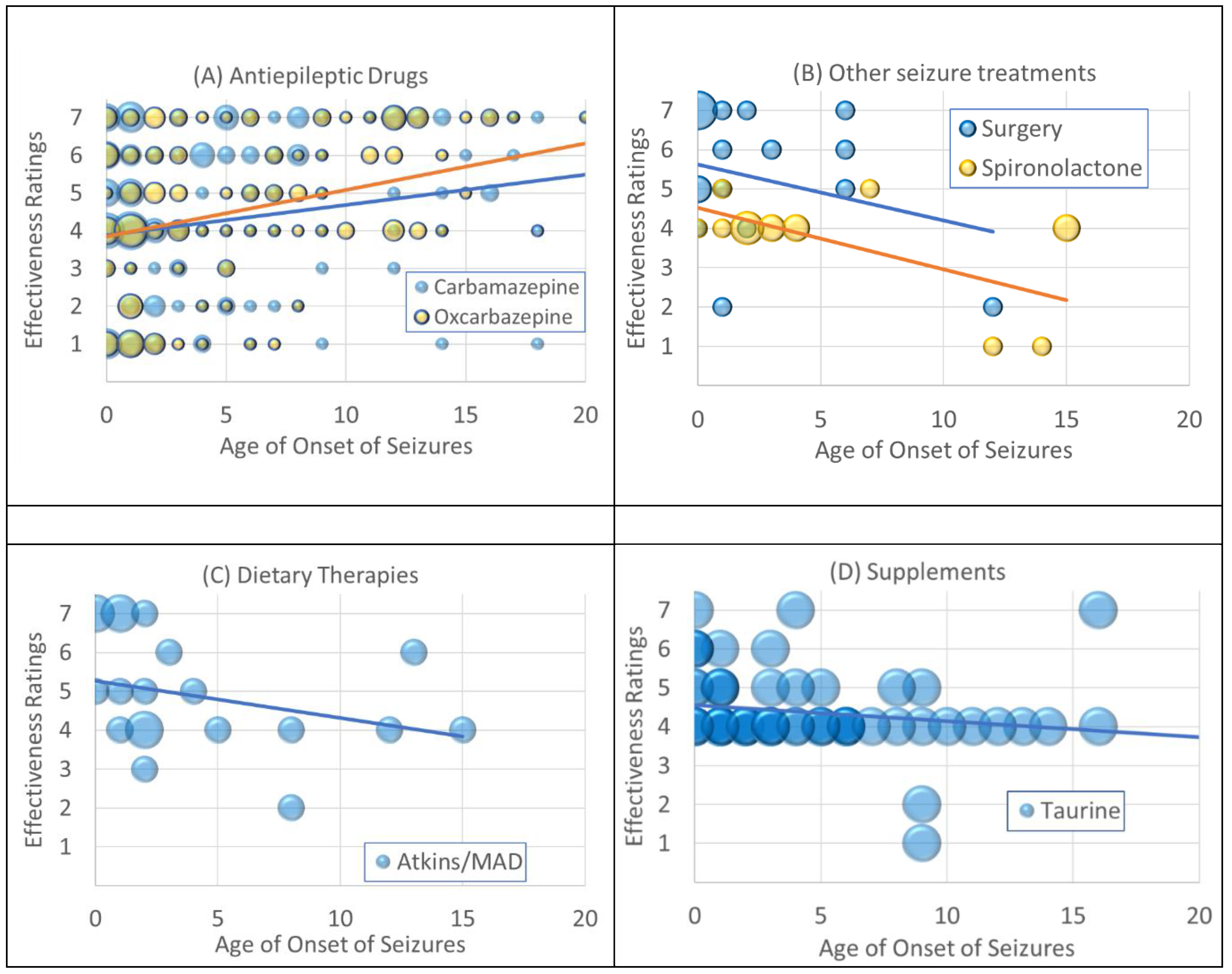

Table 1.
Average (Standard Error) Effectiveness of surveyed treatment for their effects on seizures. Treatments are organized by average effectiveness. Effectiveness rating statistically greater than 4 (no effect) are bold; Effectiveness scale: 1 = substantial negative effect, 4 = no effect, 7 = substantial positive effect.
Table 1.
Average (Standard Error) Effectiveness of surveyed treatment for their effects on seizures. Treatments are organized by average effectiveness. Effectiveness rating statistically greater than 4 (no effect) are bold; Effectiveness scale: 1 = substantial negative effect, 4 = no effect, 7 = substantial positive effect.
| Antiepileptic Drugs | Other seizure treatments | Supplements | ||||||
|---|---|---|---|---|---|---|---|---|
| Treatment | N | Effectiveness | Treatment | N | Effectiveness | Treatment | N | Effectiveness |
| Primidone | 7 | 5.29 (0.64) | Surgery | 17 | 5.41 (0.40) | GABA | 47 | 4.51 (0.158) |
| Valproic Acid | 247 | 5.21 (0.12) | Steroids | 33 | 5.09 (0.25) | Vitamin B6 | 82 | 4.51 (0.12) |
| Levetiracetam | 151 | 5.07 (0.14) | VNS | 25 | 4.80 (0.34) | Magnesium | 96 | 4.49 (0.08) |
| Lamotrigine | 171 | 4.91 (0.14) | IVIG | 15 | 4.27 (0.40) | L-carnosine | 29 | 4.41 (0.15) |
| Phenobarbital | 78 | 4.90 (0.21) | Neurofeedback | 14 | 4.21 (0.40) | Vit B12 | 111 | 4.37 (0.09) |
| Topiramate | 141 | 4.81 (0.13) | TMS/DCS | 2 | 4.00 (0.00) | Taurine | 60 | 4.35 (0.13) |
| Felbamate | 28 | 4.68 (0.33) | Spironolactone | 14 | 3.71 (0.32) | DMG | 50 | 4.30 (0.125) |
| Zonisamide | 58 | 4.67 (0.23) | CoQ10 | 69 | 4.29 (0.08) | |||
| Carbamazepine | 149 | 4.65 (0.16) | Diet therapies | Bacopa | 4 | 4.25 (0.25) | ||
| Oxcarbazepine | 125 | 4.59 (0.18) | Treatment | N | Effectiveness | Glutathione | 66 | 4.24 (0.10) |
| Tiagabine | 7 | 4.57 (0.30) | Ketogenic | 48 | 5.38 (0.21) | L-carnitine | 101 | 4.24 (0.09) |
| Phenytoin | 66 | 4.52 (0.19) | Atkins/MAD | 20 | 5.00 (0.33) | 5-HTP | 33 | 4.15 (0.13) |
| Ethosuximide | 27 | 4.44 (0.32) | SCD | 34 | 4.74 (0.21) | Alternative therapies | ||
| Clonazepam | 86 | 4.41 (0.19) | GFCF | 154 | 4.59 (0.08) | Treatment | N | Effectiveness |
| Vigabatrin | 10 | 4.40 (0.50) | HBOT | 44 | 4.39 (0.19) | |||
| Gabapentin | 43 | 3.79 (0.27) | Pioglitazone | 6 | 4.33 (0.21) | |||
| Chelation | 62 | 4.08 (0.16) | ||||||
| Minocycline | 1 | 4.00 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



