
Submitted:
09 June 2023
Posted:
12 June 2023
You are already at the latest version
Abstract
Background: The clinical outcomes of antiretroviral drugs may be modified by drug interactions; thus, it is important to update the drug interactions in people living with HIV. Aim: To update clinically relevant drug interactions in people living with HIV on antiretroviral therapy. Methods: A systematic review in Medline/PubMed database from July 2017 to December 2022, using the Mesh terms: Anti-retroviral agents and drug interactions or herb-drug interactions or food-drug interactions. Publications with drug interactions in humans, in English or Spanish, and with full text were retrieved. The clinical relevance of drug interaction was grouped into 5 levels according to gravity and probability of occurrence. Results: 361 articles were identified and 148 were included, which allowed the identification of 894 drug interaction pairs. Among these 894 drug pairs, 355 have not been identified previously; and 89 (25.1%) and 72 (20.2%) were of levels 1 and 2, respectively. In addition, for 197 (55.5%) pairs the mechanism was pharmacokinetic. The non-nucleoside reverse transcriptase inhibitors (NNRTIs) and the protease inhibitors (PIs) with 91 (25.6%) and 76 (21.4%) pairs, respectively were more frequent. Conclusions: In people living with HIV on antiretroviral therapy, we identify 355 new drug interaction pairs, of them 161 (45.3%) are assessed as levels 1 and 2 and thus, clinically relevant; a figure that is lower compared to 2014-2107 update. The pharmacokinetic mechanism is the most frequently identified. The non-nucleoside reverse transcriptase inhibitors (NNRTIs) and the protease inhibitors (PIs) are the antiretroviral groups with the highest number of clinically relevant drug interactions.
Keywords:
drug interactions
; antiretroviral agents
; HIV/AIDS
1. Introduction
The human immunodeficiency virus (HIV) is one of the main public health problems. According to the World Health Organization (WHO), 38.4 million got the HIV virus at the end of 2021, and around 650,000 people died from causes related to HIV/AIDS every year [1]. In recent years, remarkable advances have been made in the treatment of HIV; thus, currently most persons with HIV have a life expectancy similar to persons without HIV. According to the latest updates guidelines, it is recommended to start antiretroviral (ARV) therapy as soon as possible after HIV diagnosis, ideally within 7 days. Also, If they have an opportunistic infection, ARV therapy should be started shortly after initiation of treatment of the infection, and it is recommended within 2 weeks [2].
Currently, in persons living with HIV, the initial ARV therapy generally consists of two nucleoside reverse transcriptase inhibitors (NRTI) combined with a third active ARV drug, which may be an integrase strand transfer inhibitor (InSTI), a non-nucleoside reverse transcriptase inhibitor (NNRTI), or a protease inhibitor boosted with cobicistat (COBI) or ritonavir (RTV). InSTI such as bictegravir (BIC) or dolutegravir (DTG) are the preferred third ARV drug due among other factors, to low risk for drug-drug interactions. Also, the two-drug regimen, DTG plus lamivudine (3TC) may be recommended for initial treatment; and for patients who have achieved viral suppression, a long-acting injectable regimen of bimonthly injection of long-acting cabotegravir (CAB) and rilpivirine (RPV) may be used. Additionally, advances in ARV therapy have led to the availability of well-tolerated single-tablet regimens that are associated with a lower risk of drug interactions, as well as options for preexposure prophylaxis (PrEP), including oral medications such as tenofovir (TDF) plus emtricitabine (FTC) or CAB [2].
A drug interaction is an undesirable modification that is quantifiable in the magnitude or duration of effects related to the simultaneous or previous administration of other drugs, phytotherapeutics, foods, or by pathophysiological (special) conditions of the patient [3]. The identification, prevention, and resolution of clinically relevant drug interactions are critical aspect to contribute to getting the pharmacotherapy goals. Among other methods for evaluating the clinical relevance of interactions, a proposal based on the gravity of the effect on the patient's health (grave, moderate, and mild) and the probability of occurrence (defined, probable, and possible, according to the type of study that supporting the drug interaction) is considered appropriate. This proposed classification generates four levels of clinical relevance: level 1 (very high risk), level 2 (high), level 3 (medium), and level 4 (low) [3,4]. In addition, a new level of clinical relevance (level 5) has been proposed, which is characterized by the absence of effect on the patient's health (absence of gravity) documented in meta-analyses, systematic reviews, or clinical trials (defined probability), and therefore, has evidence of the absence of clinically relevant interactions [4].
Regarding clinically relevant drug interactions in persons with HIV, from 1995 to 2017 we identified four previously published reviews, which have been focused to identify drug interactions between ARV drugs, phytotherapeutics, and foods [5,6,7,8]. The most recent review updated the reported ARV interactions up to June 2017 [8]. However, due to the commercialization of new ARVs, guidelines, and expert recommendations updates, and mainly both the identification and reporting of new clinically relevant drug interactions or the generation of new knowledge about previously identified interactions, this information should be periodically updated. In addition, in 2017, a free software to facilitate the identification and assessment of the clinical relevance of ARV drug interactions (SIMARV®) was developed [9]; then a free mobile version (InterApp) was developed and available for mobile phones and tablets [10]. In this context, this systematic review aimed was to update clinically relevant drug interactions in persons living with HIV on antiretroviral therapy, regarding of drug interaction pairs between ARVs and other medications, phytotherapeutics, or foods from July 2017 to December 2022.
2. Materials and Methods
Similar to previously published reviews, a systematic review was conducted in the Medline/PubMed database, from 01/07/2017 to 31/12/2022, using the Mesh terms: Anti-retroviral agents AND Drug Interactions OR Herb-drug Interactions OR Food-drug Interaction. Articles published in English or Spanish, and with full-text access were identified.
Inclusion criteria: We included all articles containing clinically relevant information on drug interactions in humans using antiretroviral agents for the treatment of persons living with HIV/AIDS. Additionally, citation lists from identified articles were reviewed.
Exclusion criteria: We excluded the following types of articles: (a) preclinical or in vitro studies; (b) with theoretical concepts regarding drug interactions; (c) articles without specific ARV drug interactions; d) without relation with HIV; and (e) articles without full-text availability.
To ensure a systematic approach, three researchers reviewed the studies identified according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow chart via pre-determined eligibility criteria [11]. The titles and abstracts of all identified articles were screened for eligibility by two authors, and any discrepancies were resolved by the third author. Subsequently, to allow the synthesis and analysis of the results, the data was collected in a table with the following information: (a) article title, ARV assessed, (b) drug-related interaction, (c) clinical relevance level (according to the combination of gravity and probability of occurrence), (d) pharmacodynamic or pharmacokinetic mechanism, (e) comment, recommendation, and (f) reference. The information registered was proofread by another author.
Drug interaction pairs of identified ARV agents-drug interactions were classified into five levels, according to gravity (effect on patient’s health) and probability of occurrence (type of study that supports the interaction), following the combination of options as shown in Table 1 [3,4].
The probability of each ARV agent-drug interaction was determined and classified based on the type of study that supported the interaction: Possible: if the interaction was documented by results from less than three case reports; probable: if the interaction was documented by results from at least one observational study (cohort or case–control study) or at least three case reports; or Defined: if the interaction was documented by results from at least one meta-analysis, narrative systematic review, or randomized or non-randomized clinical trial. For its part, the gravity of the interaction was established as serious, moderate, or mild, based on the effect on the health of the patient caused by the interaction.
3. Results
From the search in PubMed/Medline database, 361 records were retrieved and reviewed in detail. From the 361 screened titles and abstracts, 115 were excluded. Thus, 246 articles were assessed for eligibility; among them, 98 were excluded and consequently, a total of 148 articles were included in the review (Figure 1).
A total of 894 drug interaction pairs between antiretroviral agents and other drugs were identified, of them 355 were new interactions and 539 were updates to previously identified. The assessed relevance levels, based on gravity and probability, for the new 355 pairs of antiretroviral agents-drug interactions, are shown in Table 2.
Among the 355 new drug interaction pairs, 161 (45.3%) were assessed as a higher risk of causing adverse drug outcomes linked to pharmacotherapy ineffectiveness or unsafety; in this sense 89 (25.1%) and 72 (20.2%) were assessed as level 1 and level 2, respectively. Table 3 and Table 4 provide detailed information for drug interaction pairs assessed as levels 1 and 2. Among ARV pharmacologic groups, the non-nucleoside reverse transcriptase inhibitors (NNRTIs) and the protease inhibitors (PIs) with 56 (15.8%) and 54 (15.2%) drug interaction pairs of levels 1 and 2, respectively were more frequent. Also, for the InSTIs pharmacologic group, 68 (19.2%) drug interaction pairs were identified, of them, 27 (7.6%) were evaluated as level 1 and 2; while 38 (10.7%) were assessed as level 5; thus, with evidence of lack of clinically relevant interactions (Table 5). In addition, for 197 (55.5%) of the 355 pairs, the pharmacokinetic mechanism to explain the drug interaction was the most frequent.
Globally, among 355 drug interaction pairs, 148 (42.0%) were assessed as level 5, 41 (11.5%) for NRTIs, and 38 (10.7%) for InSTI (Table 5). In addition, information regarding 51 drug interaction pairs with ARVs that are currently not in use in clinical practice was not presented: 41 corresponding to PIs (indinavir, nelfinavir, saquinavir and, tipranavir), and 10 corresponding to NRTIs (didanosine and stavudine).
Anticoagulants and antituberculosis, with 79 (22.3%) and 38 (10.7%), respectively were the pharmacologic groups with more drug interaction pairs. Also, there were a significant number of clinically relevant drug interactions associated with the use of illicit drugs, such as amphetamines, cocaine, ecstasy (MDMA), and ketamine; mainly by concomitant use of NNRTIs and elvitegravir/cobicistat (EVG/COBI) with 13 (3.7%) of these interactions. In addition, 6 (1.7%) drug interaction pairs with psychotropic drugs, particularly benzodiazepines were identified.
4. Discussion
Although current ARV therapy is simplified, safe, and effective, the combination of three ARV drugs (two in some patients), increases the risk of clinically relevant drug interactions, mainly in patients with one or more long-term diseases in addition to HIV. Currently, some systematic reviews, meta-analyses, and randomized clinical trials provide sufficient evidence that some drug interactions may cause negative health outcomes in patients living with HIV [3]. Overall, clinically relevant drug interactions occur in 20-30% of people living with HIV [67], mainly explained by a pharmacokinetics change linked to inhibition or induction of different enzymes and metabolic transporters, also including recently authorized ARV drugs [3,5,6,7,8,68].
The current review identified 148 articles with information that allowed to assess and classify the clinical relevance of 894 drug interaction pairs in people living with HIV on antiretroviral therapy. Among these 894 drug interaction pairs, 355 had not been previously identified [5,6,7,8]; which shows the need to make a periodic update on this topic through comprehensive reviews.
In the current update, we identified 355 new drug interaction pairs, among them 161 (45.3%) assessed as the most clinically relevant (levels 1 or 2). These figures were lower than reported in the update 2015-2017 [8]; in which 534 new drug interaction pairs were identified, of which 308 (64.2%) were assessed as levels 1 or 2 were reported. This reduction may be due to current guidelines [2] recommending, as first therapeutic options, regimes with more recent ARVs drugs, such as BIC (authorized in 2018) or CAB (authorized in 2021) which have less probability of pharmacokinetics interactions. In this sense, 38 (10.7%) of drug interaction pairs regarding InSTI have been assessed as level 5. Overall, second-generation InSTIs (CAB, BIC, and DTG), compared to PIs, have less probability to inhibit the metabolism of CYP450 isoenzymes, and therefore a lesser risk of clinically relevant drug-interactions interactions [2,69]. Similarly, for NRTIs, 41 (11.5%) of interaction pairs were assessed as level 5, which may be explained due to this ARV group are not metabolized by CYP450; for instance, zidovudine (AZT) and abacavir (ABC) are metabolized by glucuronidation, while 3TC, FTC, and TDF are mainly eliminated through the renal excretion [5,6,7,8].
The pharmacokinetic mechanism was the most frequent to explain the drug-interaction; thus in 197 (55.5%) of the 355 pairs no previously identified. The pharmacokinetics of ARV involves isoenzymes of the cytochrome P450 enzyme (CYP) family, such as CYP3A4, CYP2B6, and CYP2C9, as well as trans-carrier proteins, such as UGT1A1, OCT2, MATE1, OATP1B1, and glycoprotein P (P-gp), which increases the probability of pharmacokinetics drug interactions [70]. Some ARV drugs, especially PI and NNRTI are considered strong inhibitors or inducers of various isoenzymes of the CYP450 family as well as trans-carrier proteins, which increases the risk of significant clinical drug-interactions, and thereby the risk of do not achievement of therapeutic goals in patients living with HIV [67].
In the current review, the ARV groups with more clinically relevant drug-interactions were the NNRTI (15.8%) and the PIs (15.2%), likely due to their metabolism through the CYP450 family [71]. Similarly, a retrospective study found that the most frequently involved ARVs were the enhanced PI (49.3%), followed by NNRTIs (38.3%) [72]. However, these results are different from the findings in the 2015-2017 update, in which PIs were the predominant group with a percentage of 29.2% [8].
Drug abuse is an important consideration in people with HIV on ARV therapy, which requires an integrated approach based on evidence [2]. Currently, there is increasing awareness of the clinical relevance of cannabis-drug interactions [73], particularly with efavirenz (EFV) and EVG/COBI, as they can increase plasma levels of cannabis, prolong its clinical effects, and increase toxicity [32]. In addition, there are a significant number of clinically relevant drug interactions associated with the use of illicit drugs, such as amphetamines, cocaine, ecstasy (MDMA), and ketamine in combination with NNRTIs and elvitegravir/cobicistat, with the most serious combination being cocaine (Level 1) (32,33). Cocaine use can lead to an increase in plasma levels, which can be life-threatening due to the risk of rhabdomyolysis, arrhythmia, and cardiovascular collapse (33). Furthermore, a significant percentage of clinically relevant interactions were identified between psychotropic drugs, particularly benzodiazepines, which have the potential to cause dependence in patients. In combination with boosted PIs and EVG/COBI, the probability of respiratory depression, sedation, and muscle weakness is increased [13].
The method for assessing the clinical relevance of drug interactions used in this review is similar to used in previous reviews [5,6,7,8]; therefore, these results are useful to update and to synthesize the previous identified information regarding ARV drug-interactions. Thereby, the 355 newly identified drug interaction pairs will be used to update the mobile application for analyzing the clinical relevance of ARV drug-interactions (InterApp ARV) [10], which is an evolution of the SIMARV® software [9]. The application is freely accessible and can be downloaded for Android devices from the Play Store. (https://play.google.com/store/apps/details?id=co.com.pypudea.interapparv).
The results of this review may have some limitations; therefore, the results should be interpreted and used with caution. In this context, the main limitation is the search restriction to a single database, since the search was performed only in the PubMed/MEDLINE database, which may not identify other clinically relevant interactions. However, this situation could be minimized with the inclusion of publications identified as relevant in the references of the articles included.
5. Conclusions
From 2017 to 2022, in PubMed/Medline database we identify 361 records that may relate to drug interactions in patients living with HIV, among than 148 provide specific information for drug interactions in people living with HIV on antiretroviral therapy. Thus, the clinical relevance of 894 drug-interactions pairs is assessed, of them 355 are pairs not previously identified, a figure that is lower than the one reported in the update 2015-2017. Among the 355 newly identified drug-interactions pairs, 72 (20.2%) are assessed as level 2, while 89 (25.1%) as level 1, and thus with a high risk of causing adverse drug outcomes linked to ineffectiveness or unsafety of pharmacotherapy. Pharmacokinetics is the mechanism more frequently identified to explain the drug interactions. In addition, NNRTIs were the ARV drugs that had the highest number of clinically relevant interactions. Oral anticoagulants and antituberculosis medications were the drug groups that most frequently interacted with ARV, accounting for 20.6% and 12.7% of cases, respectively. In people living with HIV, a high frequency of clinically relevant drug interactions is associated with the use of illicit drugs, mainly cocaine, and with psychotropic drugs, particularly benzodiazepines.
Author Contributions
Database search, screening of articles, and extraction of information: M.R, M.C, and P.A; writing of the manuscript: M.C, M.R, and P.A. All authors have read and agreed to the published version of the manuscript.
Funding
The Pharmaceutical Promotion and Prevention Group received financial support from the Committee for Development Research (CODI) and sustainability program (2018–2019), Universidad de Antioquia.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within this article. In addition, data in Table 3 with footnote “c” the percentages of change were calculated with data contained within articles.
Acknowledgments
The authors acknowledge the members of the Research Group on Pharmaceutical Promotion and Prevention of the University of Antioquia for their comments and suggestions about the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. HIV/AIDS. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 10 February 2022).
- Gandhi RT, Bedimo R, Hoy JF, Landovitz RJ, Smith DM, Eaton EF, et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society-USA Panel. JAMA. 2023, 329, 63–84.
- Amariles P, Giraldo NA, Faus MJ. Interacciones medicamentosas: aproximación para establecer y evaluar su relevancia clínica. Med Clin (Barc). 2007, 129, 27–35.
- Amariles P, Madrigal-Cadavid J, Giraldo NA. Clinical relevance of drug interactions: Proposal to update the classification based on the severity and probability of its occurrence. Rev Chil Infectologia Organo Of Soc Chil Infectologia. 2021, 38, 304–5.
- Amariles, P.; Giraldo, N.; Faus, M. Interacciones medicamentosas en pacientes infectados con el VIH: aproximación para establecer y evaluar su relevancia clínica. Farm. Hosp. 2007, 31, 283–302. [Google Scholar] [CrossRef]
- Giraldo, N.; Amariles, P.; Gutiérrez, F.; Monsalve, M.; Faus, M. Aproximación para establecer y evaluar la relevancia clínica de las interacciones medicamentosas en pacientes infectados con virus de la inmunodeficiencia humana: actualización 2009. Farm. Hosp. 2010, 34, 90–93. [Google Scholar] [CrossRef]
- A Giraldo, N.; Amariles, P.; Marín, D.E.P.; Faus, M.J. Relevancia clínica de las interacciones medicamentosas en pacientes infectados con el virus de la inmunodeficiencia humana: actualización 2009-2014. 2016, 33, 36–53. [CrossRef]
- Osorio, T. L, Rivera C. M, Pino-Marín DE, Giraldo NA, Amariles P, Osorio T. L, et al. Relevancia clínica de las interacciones medicamentosas en pacientes infectados con el virus de la inmunodeficiencia humana: actualización 2015-2017. Rev Chil Infectol. 2019, 36, 475–89. [Google Scholar]
- Giraldo, N.; Amariles, P.; Monsalve, M.; Faus, M. Free software to analyse the clinical relevance of drug interactions with antiretroviral agents (SIMARV®) in patients with HIV/AIDS. Res. Soc. Adm. Pharm. 2017, 13, 831–839. [Google Scholar] [CrossRef]
- Amariles P, Madrigal Cadavid J, Granados J, Giraldo N. Interapp ARV: aplicación móvil para analizar la relevancia clínica de interacciones de antirretrovirales. Vitae. 2019, 26:S33-6.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372:n71.
- Hastain, N.V.; Santana, A.; Schafer, J.J. The Incidence and Severity of Drug Interactions Before and After Antiretroviral Therapy Simplification in Treatment-Experienced Patients With HIV Infection. Ann. Pharmacother. 2019, 54, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Marzolini, C.; Livio, F. Prescribing issues in elderly individuals living with HIV. Expert Rev. Clin. Pharmacol. 2019, 12, 643–659. [Google Scholar] [CrossRef] [PubMed]
- Tyrberg, E.; Edén, A.; Eriksen, J.; Nilsson, S.; Treutiger, C.J.; Thalme, A.; Mellgren. ; Gisslén, M.; Andersson, L.-M. Higher plasma drug levels in elderly people living with HIV treated with darunavir. PLOS ONE 2021, 16, e0246171. [Google Scholar] [CrossRef] [PubMed]
- Zautner, A.E.; Herchenröder, O.; El Moussi, A.; Schwarz, N.G.; Wiemer, D.F.; Groß, U.; Frickmann, H. Pharmaceutical interactions between antiretroviral and antimalarial drugs used in chemoprophylaxis. Acta Trop. 2018, 179, 25–35. [Google Scholar] [CrossRef]
- Haaland, R.E.; Otieno, K.; Martin, A.; Katana, A.; Dinh, C.; Slutsker, L.; Menendez, C.; Gonzalez, R.; Williamson, J.; Heneine, W.; et al. Short Communication: Reduced Nevirapine Concentrations Among HIV-Positive Women Receiving Mefloquine for Intermittent Preventive Treatment for Malaria Control During Pregnancy. AIDS Res. Hum. Retroviruses 2018, 34, 912–915. [Google Scholar] [CrossRef]
- Meintjes, G.; Brust, J.C.M.; Nuttall, J.; Maartens, G. Management of active tuberculosis in adults with HIV. Lancet HIV 2019, 6, e463–e474. [Google Scholar] [CrossRef]
- Chastain DB, Franco-Paredes C, Stover KR. Addressing Antiretroviral Therapy-Associated Drug-Drug Interactions in Patients Requiring Treatment for Opportunistic Infections in Low-Income and Resource-Limited Settings: Journal of Clinical Pharmacology. J Clin Pharmacol. 2017, 57, 1387–99.
- Hakkola, J.; Hukkanen, J.; Turpeinen, M.; Pelkonen, O. Inhibition and induction of CYP enzymes in humans: an update. Arch. Toxicol. 2020, 94, 3671–3722. [Google Scholar] [CrossRef]
- Cerrone, M.; Bracchi, M.; Wasserman, S.; Pozniak, A.; Meintjes, G.; Cohen, K.; Wilkinson, R.J. Safety implications of combined antiretroviral and anti-tuberculosis drugs. Expert Opin. Drug Saf. 2019, 19, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Boyle, A.; Moss, C.E.; Marzolini, C.; Khoo, S. Clinical Pharmacodynamics, Pharmacokinetics, and Drug Interaction Profile of Doravirine. Clin. Pharmacokinet. 2019, 58, 1553–1565. [Google Scholar] [CrossRef] [PubMed]
- Freise, K.J.; Hu, B.; Salem, A.H. Impact of ritonavir dose and schedule on CYP3A inhibition and venetoclax clinical pharmacokinetics. Eur. J. Clin. Pharmacol. 2018, 74, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Mutiti, C.S.; Kapungu, N.N.; Kanji, C.R.; Stadler, N.; Stingl, J.; Nhachi, C.; Hakim, J.; Masimirembwa, C.; Thelingwani, R.S. Clinically relevant enantiomer specific R- and S-praziquantel pharmacokinetic drug-drug interactions with efavirenz and ritonavir. Pharmacol. Res. Perspect. 2021, 9, e00769. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.A.; Tseng, A.; Cooper, R. Managing drug interactions in HIV-infected adults with comorbid illness. Can. Med Assoc. J. 2014, 187, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Chary, A.; Nguyen, N.N.; Maiton, K.; Holodniy, M. A review of drug-drug interactions in older HIV-infected patients. Expert Rev. Clin. Pharmacol. 2017, 10, 1329–1352. [Google Scholar] [CrossRef]
- Patel, R.C.; Stalter, R.M.; Thomas, K.K.; Tamraz, B.; Blue, S.W.; Erikson, D.W.; Kim, C.J.; Kelly, E.J.; Nanda, K.; Kourtis, A.P.; et al. A pharmacokinetic and pharmacogenetic evaluation of contraceptive implants and antiretroviral therapy among women in Kenya and Uganda. AIDS 2019, 33, 1995–2004. [Google Scholar] [CrossRef]
- Neary, M.; A Chappell, C.; Scarsi, K.K.; Nakalema, S.; Matovu, J.; Achilles, S.L.; A Chen, B.; Siccardi, M.; Owen, A.; Lamorde, M. Effect of patient genetics on etonogestrel pharmacokinetics when combined with efavirenz or nevirapine ART. J. Antimicrob. Chemother. 2019, 74, 3003–3010. [Google Scholar] [CrossRef]
- Kosloski, M.P.; Oberoi, R.; Wang, S.; Viani, R.M.; Asatryan, A.; Hu, B.; Ding, B.; Qi, X.; Kim, E.J.; Mensa, F.; et al. Drug-Drug Interactions of Glecaprevir and Pibrentasvir Coadministered With Human Immunodeficiency Virus Antiretrovirals. J. Infect. Dis. 2019, 221, 223–231. [Google Scholar] [CrossRef]
- Starbird, L.E.; Hong, H.P.; Sulkowski, M.S.; Farley, J.E.P. Management of the Patient With HIV/Hepatitis C Drug Interactions: A Guide for Nurses and Nurse Practitioners. J. Assoc. Nurses AIDS Care 2020, 31, 241–248. [Google Scholar] [CrossRef] [PubMed]
- El-Sherif, O.; Back, D. Drug Interactions of Hepatitis C Direct-Acting Antivirals in the HIV-Infected Person. Curr. HIV/AIDS Rep. 2015, 12, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Sabourin, A.A.; Patel, T.; Saad, S.; Renner, E.; Mouland, E.; Adie, S.; Ha, N.B. Management of anticoagulation in patients with human immunodeficiency virus/acquired immunodeficiency virus. Thromb. Res. 2021, 200, 102–108. [Google Scholar] [CrossRef]
- Chen, G.-L.; Lin, S.-Y.; Lo, H.-Y.; Wu, H.-C.; Lin, Y.-M.; Chen, T.-C.; Chu, C.-Y.S.; Lee, W.-C.; Chen, Y.-H.; Lu, P.-L. Clinical impact of recreational drug use among people living with HIV in southern Taiwan. J. Microbiol. Immunol. Infect. 2020, 54, 952–962. [Google Scholar] [CrossRef] [PubMed]
- Castro-Granell V, Garin N, Jaén Á, Cenoz S, Galindo MJ, Fuster-RuizdeApodaca MJ. Prevalence, beliefs and impact of drug-drug interactions between antiretroviral therapy and illicit drugs among people living with HIV in Spain. Torti C, editor. PLOS ONE. 2021, 16, e0260334.
- Ryom, L.; Cotter, A.; De Miguel, R.; Béguelin, C.; Podlekareva, D.; Arribas, J.; Marzolini, C.; Mallon, P.; Rauch, A.; Kirk, O.; et al. 2019 update of the European AIDS Clinical Society Guidelines for treatment of people living with HIV version 10.0. HIV Med. 2020, 21, 617–624. [Google Scholar] [CrossRef]
- O’kelly, B.B.M.B.B.M.; Murtagh, R.; Lambert, J.S. Therapeutic Drug Monitoring of HIV Antiretroviral Drugs in Pregnancy: A Narrative Review. Ther. Drug Monit. 2020, 42, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Scarsi, K.K.; Havens, J.P.; Podany, A.T.; Avedissian, S.N.; Fletcher, C.V. HIV-1 Integrase Inhibitors: A Comparative Review of Efficacy and Safety. Drugs 2020, 80, 1649–1676. [Google Scholar] [CrossRef]
- Burgess, M.J.; Kasten, M.J.; Zeuli, J.D. Management of HIV/AIDS in older patients–drug/drug interactions and adherence to antiretroviral therapy. HIV/AIDS - Res. Palliat. Care, 7. [CrossRef]
- Nachega, J.B.; Hsu, A.J.; Uthman, O.A.; Spinewine, A.; Pham, P.A. Antiretroviral therapy adherence and drug–drug interactions in the aging HIV population. AIDS 2012, 26, S39–S53. [Google Scholar] [CrossRef] [PubMed]
- Devanathan, A.S.; Anderson, D.J.; Cottrell, M.L.; Burgunder, E.M.; Saunders, A.C.; Kashuba, A.D. Contemporary Drug–Drug Interactions in HIV Treatment. Clin. Pharmacol. Ther. 2019, 105, 1362–1377. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo D, Giacomelli A, Pagani G, Filice C, Gervasoni C. Ritonavir/Cobicistat-Induced Cushing Syndrome in HIV Patients Treated With Non-Oral Corticosteroids: A Call for Action? Am J Med Sci. 2021, 361, 137–9.
- Flynn, P.M.; Abrams, E.J. Response to correspondence entitled: Perinatal HIV and response to vaccination. AIDS 2019, 33, 1675–1677. [Google Scholar] [CrossRef] [PubMed]
- Canetti, D.; Spagnuolo, V. An evaluation of cabotegravir for HIV treatment and prevention. Expert Opin. Pharmacother. 2020, 22, 403–414. [Google Scholar] [CrossRef]
- Ford, S.L.; Sutton, K.; Lou, Y.; Zhang, Z.; Tenorio, A.; Trezza, C.; Patel, P.; Spreen, W. Effect of Rifampin on the Single-Dose Pharmacokinetics of Oral Cabotegravir in Healthy Subjects. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef]
- Hostench-Junoy N, Ramírez-Montoya M, Arefai-Refai B, Estal-Jiménez J, Santana-Rodríguez ZJ, Costa-Pérez L. Acute Ischemia of Lower Extremities Caused by Ergotamine Toxicity due to Pharmacologic Interaction With Cobicistat in an HIV-Positive Patient. Ann Vasc Surg. 2022, 80:392.e1-392.e6.
- Manzardo, C.; Tuset, M.; Miró, J.M.; Gatell, J.M. Interacciones graves o potencialmente letales entre antirretrovirales y otros medicamentos. Enfermedades Infecc. Y Microbiol. Clin. (english Ed.) 2015, 33, e15–e30. [Google Scholar] [CrossRef]
- Tseng A, Seet J, Phillips EJ. The evolution of three decades of antiretroviral therapy: challenges, triumphs and the promise of the future: Three decades of antiretroviral therapy. Br J Clin Pharmacol. 2015, 79, 182–94.
- Hiransuthikul, A.; Janamnuaysook, R.; Himmad, K.; Kerr, S.J.; Thammajaruk, N.; Pankam, T.; Phanjaroen, K.; Mills, S.; Vannakit, R.; Phanuphak, P.; et al. Drug-drug interactions between feminizing hormone therapy and pre-exposure prophylaxis among transgender women: the iFACT study. J. Int. AIDS Soc. 2019, 22, e25338. [Google Scholar] [CrossRef] [PubMed]
- Ribera E, Podzamczer D. Mecanismo de acción, farmacología e interacciones de dolutegravir. Enfermedades Infecc Microbiol Clínica. 2015, 33:2-8.
- Dooley KE, Sayre P, Borland J, Purdy E, Chen S, Song I, et al. Safety, Tolerability, and Pharmacokinetics of the HIV Integrase Inhibitor Dolutegravir Given Twice Daily With Rifampin or Once Daily With Rifabutin: Results of a Phase 1 Study Among Healthy Subjects. J Acquir Immune Defic Syndr. 2013, 62.
- Speaker Abstracts. J Int AIDS Soc. 2018, 21, e25093. [CrossRef] [PubMed]
- Eke, A.C.; Mirochnick, M. Ritonavir and cobicistat as pharmacokinetic enhancers in pregnant women. Expert Opin. Drug Metab. Toxicol. 2019, 15, 523–525. [Google Scholar] [CrossRef] [PubMed]
- Podany, A.T.; Scarsi, K.K.; Fletcher, C.V. Comparative Clinical Pharmacokinetics and Pharmacodynamics of HIV-1 Integrase Strand Transfer Inhibitors. Clin. Pharmacokinet. 2016, 56, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Chandiwana, N.C.; Chersich, M.; Venter, W.F.; Akpomiemie, G.; Hill, A.; Simmons, B.; Lockman, S.; Serenata, C.M.; Fairlie, L.; Moorhouse, M.A. Unexpected interactions between dolutegravir and folate: randomized trial evidence from South Africa. AIDS 2020, 35, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Bukkems, V.E.; Smolders, E.J.; Jourdain, G.; Burger, D.M.; Colbers, A.P.; Cressey, T.R. ; PANNA Network and iTAP Study Group Effect of Pregnancy and Concomitant Antiretrovirals on the Pharmacokinetics of Tenofovir in Women With HIV Receiving Tenofovir Disoproxil Fumarate-Based Antiretroviral Therapy Versus Women With HBV Receiving Tenofovir Disoproxil Fumarate Monotherapy. J. Clin. Pharmacol. 2020, 61, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.N.; Gufford, B.T.; Lu, J.B.L.; Bushman, L.R.; Anderson, P.L.; Bergstrom, R.F.; Desta, Z.; Gupta, S.K. Inhibitory Effects of Probenecid on Pharmacokinetics of Tenofovir Disoproxil Fumarate and Emtricitabine for On-Demand HIV Preexposure Prophylaxis. Clin. Pharmacol. Ther. 2019, 107, 1200–1208. [Google Scholar] [CrossRef]
- Ewing, A.C.; King, C.C.; Wiener, J.B.; Chasela, C.S.; Hudgens, M.G.; Kamwendo, D.; Tegha, G.; Hosseinipour, M.C.; Jamieson, D.J.; Van der Horst, C.; et al. Effects of concurrent exposure to antiretrovirals and cotrimoxazole prophylaxis among HIV-exposed, uninfected infants. AIDS 2017, 31, 2455–2463. [Google Scholar] [CrossRef]
- Ippolito, M.M.; Jacobson, J.M.; Lederman, M.M.; Winterberg, M.; Tarning, J.; A Shapiro, T.; Flexner, C. Effect of Antiretroviral Therapy on Plasma Concentrations of Chloroquine and Desethyl-chloroquine. Clin. Infect. Dis. 2018, 67, 1617–1620. [Google Scholar] [CrossRef]
- van der Laan, L.E.; Garcia-Prats, A.J.; Schaaf, H.S.; Tikiso, T.; Wiesner, L.; de Kock, M.; Winckler, J.; Norman, J.; McIlleron, H.; Denti, P.; et al. Pharmacokinetics and Drug-Drug Interactions of Lopinavir-Ritonavir Administered with First- and Second-Line Antituberculosis Drugs in HIV-Infected Children Treated for Multidrug-Resistant Tuberculosis. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef]
- Ramachandran, G.; Kumar, A.H.; Kannan, T.; Sridhar, R.; Guha, S.; Kadam, D.; Gangadevi, N.P.; Rajapandian, T. Pharmacokinetics of rifabutin during atazanavir/ritonavir co-administration in HIV-infected TB patients. Indian J. Tuberc. 2018, 66, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Shieh, E.; A Marzinke, M.; Fuchs, E.J.; Hamlin, A.; Bakshi, R.; Aung, W.; Breakey, J.; Poteat, T.; Brown, T.; Bumpus, N.N.; et al. Transgender women on oral HIV pre-exposure prophylaxis have significantly lower tenofovir and emtricitabine concentrations when also taking oestrogen when compared to cisgender men. J. Int. AIDS Soc. 2019, 22, e25405. [Google Scholar] [CrossRef] [PubMed]
- Havens, J.P.; Podany, A.T.; Scarsi, K.K.; Fletcher, C.V. Clinical Pharmacokinetics and Pharmacodynamics of Etravirine: An Updated Review. Clin. Pharmacokinet. 2019, 59, 137–154. [Google Scholar] [CrossRef]
- Serrano López De Las Hazas, JI. Interacciones farmacológicas de los nuevos antirretrovirales. Farm Hosp. 2011, 35, 36–43. [Google Scholar] [CrossRef]
- Thurman, A.R.; Schwartz, J.L.; Brache, V.; Chen, B.A.; Chandra, N.; Kashuba, A.D.; Weiner, D.H.; Mauck, C.; Doncel, G.F. Effect of Hormonal Contraception on Pharmacokinetics of Vaginal Tenofovir in Healthy Women: Increased Tenofovir Diphosphate in Injectable Depot Medroxyprogesterone Acetate Users. Am. J. Ther. 2019, 80, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Hodge, D.; Back, D.J.; Gibbons, S.; Khoo, S.H.; Marzolini, C. Pharmacokinetics and Drug–Drug Interactions of Long-Acting Intramuscular Cabotegravir and Rilpivirine. Clin. Pharmacokinet. 2021, 60, 835–853. [Google Scholar] [CrossRef]
- Trezza C, Ford SL, Gould E, Lou Y, Huang C, Ritter JM, et al. Lack of effect of oral cabotegravir on the pharmacokinetics of a levonorgestrel/ethinyl oestradiol-containing oral contraceptive in healthy adult women: Effect of cabotegravir on combined oral contraceptives. Br J Clin Pharmacol. 2017, 83, 1499–505.
- Wang, S.C.; Kaur, G.; Schulman-Marcus, J.; Purga, S.; Mookherjee, S.; Miller, C.; Sidhu, M.S.; Rosenson, R.S. Implementation of Cholesterol-Lowering Therapy to Reduce Cardiovascular Risk in Persons Living with HIV. Cardiovasc. Drugs Ther. 2020, 36, 173–186. [Google Scholar] [CrossRef]
- Lozano F, Domingo P. [Antiretroviral therapy for HIV infection]. Enferm Infecc Microbiol Clin. 2011, 29, 455–65.
- Burgess S, Partovi N, Yoshida EM, Erb SR, Azalgara VM, Hussaini T. Drug Interactions With Direct-Acting Antivirals for Hepatitis C: Implications for HIV and Transplant Patients. Ann Pharmacother. 2015, 49, 674–87.
- Zhao, A.V.; Crutchley, R.D.; Guduru, R.C.; Ton, K.; Lam, T.; Min, A.C. A clinical review of HIV integrase strand transfer inhibitors (INSTIs) for the prevention and treatment of HIV-1 infection. Retrovirology 2022, 19, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Rathbun, R.C.; Liedtke, M.D. Antiretroviral Drug Interactions: Overview of Interactions Involving New and Investigational Agents and the Role of Therapeutic Drug Monitoring for Management. Pharmaceutics 2011, 3, 745–781. [Google Scholar] [CrossRef]
- Al Sayed, H.A.H.; Sharif-Askari, N.S.; Rahimi, M.R. Clinically significant drug interactions between antiretroviral and co-prescribed drugs in HIV infected patients: retrospective cohort study. Med. Pharm. Rep. 2022, 95, 260–266. [Google Scholar] [CrossRef]
- Jiménez-Guerrero L, Núñez-Núñez M, Castañeda-Macías I, Sandoval-Fernández del Castillo S, Jiménez-Guerrero L, Núñez-Núñez M, et al. Interacciones potenciales en una cohorte de pacientes VIH positivos de edad avanzada. Farm Hosp. 2018, 42, 163–7.
- Lopera, V.; Rodríguez, A.; Amariles, P. Clinical Relevance of Drug Interactions with Cannabis: A Systematic Review. J. Clin. Med. 2022, 11, 1154. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) [11] - flow diagram for the systematic review of the clinical relevance of drug interactions in people living with human immunodeficiency virus.
Figure 1.
Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) [11] - flow diagram for the systematic review of the clinical relevance of drug interactions in people living with human immunodeficiency virus.
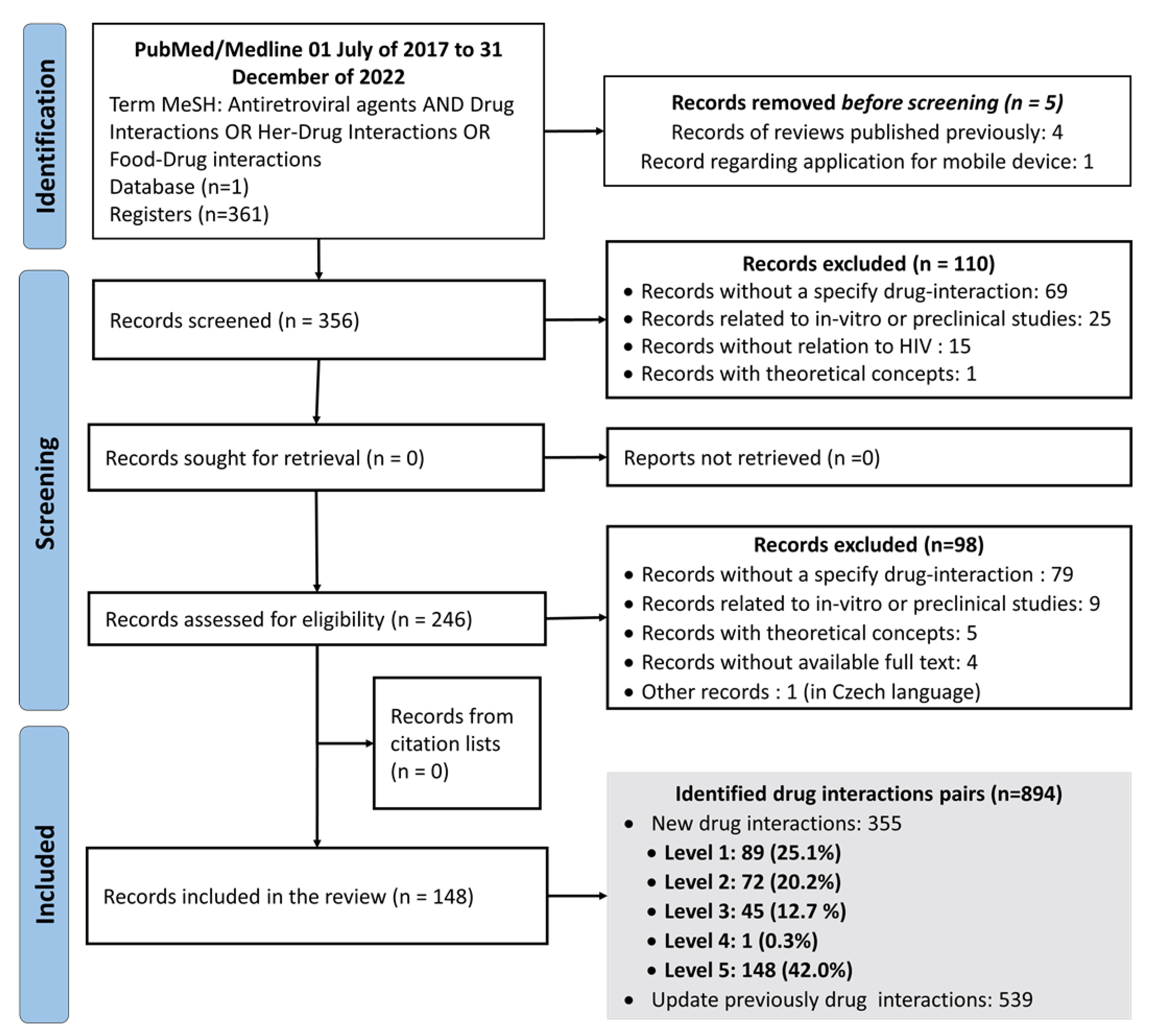

Table 1.
Levels of the clinical relevance of drug interactions according to the combination of gravity and probability of occurrence [3,4].
| Probability | |||
|---|---|---|---|
| Gravity | Defined | Probable | Possible |
| Grave | 1 (very high risk) | 1 (very high risk) | 2 (high risk) |
| Moderate | 2 (high risk) | 2 (high risk) | 3 (medium risk) |
| Minor | 3 (medium risk) | 3 (medium risk) | 4 (low risk) |
| Lack of gravity | 5 (riskless) | N/A | N/A |
N/A: No aplicable.
Table 2.
Summary of new 355 antiretroviral drug interactions pairs.
| Total of drug interaction pairs, n (%) | 355 (100%) | |||||
|---|---|---|---|---|---|---|
| Pharmacokinetic mechanism | 197 (55.5%) | |||||
|
111 (31.2%) | |||||
|
66 (18.6%) | |||||
|
18 (5.1%) | |||||
|
1 (0.3%) | |||||
|
1 (0.3%) | |||||
| Pharmacodynamic mechanism | 6 (1.7%) | |||||
|
6 (1.7%) | |||||
| Pharmacokinetic/pharmacodynamic mechanism | 4 (1.1%) | |||||
| Enzyme inhibition/synergism | 2 (0.5%) | |||||
| Enzyme induction/synergism | 2 (0.5%) | |||||
| Evidence of no clinically relevant interactions | 148 (42.0%) | |||||
| Level of the clinical relevance of drug interaction | ||||||
| Level 1 | Level 2 | Level 3 | Level 4 | Level 5 | Total, n (%) | |
| 89 (25.1%) | 72 (20.2%) | 45 (12.7%) | 1 (0.3%) | 148 (42.0%) | 355 (100.0%) | |
Table 3.
New drug interactions with protease inhibitors and non-nucleoside reverse transcriptase inhibitors Level 1 and 2.
Table 3.
New drug interactions with protease inhibitors and non-nucleoside reverse transcriptase inhibitors Level 1 and 2.
| Pharmacological group or drugs affected | Antiretroviral agent | Gravity/Probability | Comments/Suggestions |
|---|---|---|---|
| Alpha-1 adrenergic receptor antagonist | |||
| Silodosin [12] | ATV/RTV, DRV/RTV, FPV/RTV, LPV/RTV | (Moderate/Probable): Level 2 | Boosted PIs may increase silodosin plasma levels through the inhibition of CYP3A4 metabolism. To monitor silodosin safety parameters, a dose adjustment may be necessary. |
| Anesthetic/Anxiolytic/Benzodiazepine | |||
| Midazolam [13] | ATV/RTV | (Grave/Defined): Level 1 | Boosted PIs may increase midazolam plasma levels, increasing the probability of respiratory depression, sedation, and muscle weakness. The use of this combination is not recommended. If necessary, parenteral midazolam should be used with close clinical monitoring or use safer alternatives such as lorazepam or propofol. |
| Triazolam [13] | ATV/RTV | (Grave/Defined): Level 1 | Boosted PIs may increase triazolam plasma levels, increasing the probability of respiratory depression, sedation, and muscle weakness. The use of this combination is not recommended, safer alternatives such as oxazepam, lorazepam or temazepam should be used. |
| Antiasthmatic/ Glucocorticoid | |||
| Budesonide [14] | ATV | (Grave/Defined): Level 1 | ATV may increase the budesonide plasma levels, enhancing the side effects produced by steroids. To monitor budesonide safety parameters, a dose adjustment may be necessary. |
| Antimalarial | |||
| Atovaquone [15] | EFV, ETR | (Moderate/Defined): Level 2 | NNRTIs may decrease the AUC and Cmax of atovaquone by inducing glucuronidation. To monitor atovaquone effectiveness parameters, a dose adjustment may be necessary. |
| Mefloquine [16] | NVP | (Moderate/Defined): Level 2 | Mefloquine may decrease NVP plasma levels. Caution is recommended in case of using NVP concomitantly with mefloquine, closely monitor, a dose adjustment may be necessary. |
| Proguanil [15] | EFV, ETR | (Moderate/Defined): Level 2 | NNRTIs may decrease proguanil AUC and Cmax. To monitor proguanil effectiveness parameters, a dose adjustment may be necessary. |
| Antimicrobial/ Antileprotic | |||
| Clofazimine [17] | EFV | (Grave/Defined): Level 1 | The use of EFV and clofazimine may generate QT interval prolongation in the ECG. Heart function should be closely monitored by ECG. |
| Antimicrobial/ Antituberculosis | |||
| Moxifloxacin [17] | EFV | (Grave/Defined): Level 1 | EFV may decrease the AUC of moxifloxacin by 30 %, increasing the development of resistance and the risk of virological failure. Levofloxacin is suggested instead of moxifloxacin when used concomitantly with EFV. |
| Rifabutin [18] | ATV, DRV, FPV, LPV/RTV | (Moderate/Defined): Level 2 | Rifabutin may reduce PIs plasma levels by induction of CYP3A4, causing decreased virological response. It is recommended to adjust the dose of rifabutin to 150 mg daily. |
| Rifabutin [19] | DOR | (Moderate/Defined): Level 2 | Rifabutin may decrease DOR plasma levels by induction of CYP3A4. To monitor rifabutin effectiveness parameters, a dose adjustment may be necessary. |
| Rifabutin [18,20] | EFV, ETR | (Grave/Defined): Level 1 | Rifabutin may induce CYP3A4 and increase EFV and ETR metabolism, causing decrease in their plasma levels and virological response. These combinations are not recommended given the risk of reducing viral susceptibility and developing resistance. |
| Rifampicin (17,18,20] | DRV/RTV | (Grave/Defined): Level 1 | Rifampicin may significantly decrease DRV/RTV plasma levels by 57 %, increasing the development of resistance and the risk of virological failure. Alternatively, it suggests using rifabutin 150 mg daily. |
| Rifampicin [19,20,21] | DOR | (Grave/Defined): Level 1 | Rifampicin may induce CYP3A4, causing decrease DOR plasma levels by 88 %. To monitor rifabutin effectiveness parameters, a dose adjustment may be necessary. |
| Rifampicin [16,20] | RPV | (Grave/Defined): Level 1 | Rifampicin may decrease RPV plasma levels, increasing the risk of virological failure and development of resistance, therefore, this combination is contraindicated. In this sense, rifabutin 300 mg daily and double dose of RPV is recommended. |
| Antineoplastic | |||
| Venetoclax [22] | RTV | (Moderate/Probable): Level 2 | RTV (doses of 50 mg and 100 mg) may inhibit CYP3A4 resulting in an increase of venetoclax Cmax 2.3 to 2.4 times compared with venetoclax alone and AUC 6.1 and 8.1 times, respectively. After completing the gradual increase in dose, venetoclax dose reductions of at least 75 % are recommended when administered concomitantly with potent CYP3A inhibitors to maintain venetoclax exposures within the therapeutic range established for the treatment of lymphocytic leukemia chronic. |
| Antiparasitic/ Anthelmintic | |||
| Praziquantel [23] | EFV | (Moderate/Defined): Level 2 | EFV may decrease praziquantel plasma levels up to 4 times the risk of therapeutic failure. To monitor praziquantel effectiveness parameters, a dose adjustment may be necessary, but not exceed the maximum. |
| Antiplatelet agent | |||
| Ticagrelor [13] | ATV/RTV, DRV/RTV, FPV/RTV, LPV/RTV | (Grave/Defined): Level 1 | Boosted PIs may increase ticagrelor plasma levels, increasing the risk of bleeding. The use of ticagrelor with boosted PIs is not recommended. Other antiplatelet agents are suggested as an alternative. |
| Antiulcer/Anti-H2 | |||
| Famotidine [19] | RPV | (Moderate/Defined): Level 2 | Famotidine may decrease RPV plasma levels, increasing the risk of virological failure and development of resistance, by increasing gastric pH. To monitor RPV effectiveness parameters. This combination may be used as long as doses are temporarily separated, i.e., RPV can be given 4 h before or 12 h after anti-H2. |
| Antiulcer/Proton Pump Inhibitor | |||
| Lansoprazole [24,25] | RPV | (Grave/Defined): Level 1 | Proton pump inhibitors may increase gastrointestinal pH and affect RPV absorption by decreasing its plasma levels. Avoid this combination or use esomeprazole by spacing your intake in 10 hours with RPV. |
| Omeprazole [13, 19] | |||
| Pantoprazole [24,25] | |||
| Rabeprazole [24,25] | |||
| Atypical antipsychotic | |||
| Ziprasidone [25] | EFV | (Moderate/Defined): Level 2 | EFV may decrease ziprasidone plasma levels. To monitor ziprasidone effectiveness parameters, a dose adjustment may be necessary. |
| Contraceptive | |||
| Etonogestrel (Oral contraceptive) [26] | NVP | (Grave/Defined): Level 1 | NVP may reduce etonogestrel plasma levels (Cmin decrease by 39 % and AUC of 0-24 weeks by 37 %), significantly decreasing the contraceptive effect. Etonogestrel implants are not recommended for women receiving long-term treatment with NVP. The patient should be informed of the need to use a barrier method as a complementary method of planning or to seek a safer contraceptive alternative. |
| Levonorgestrel (Implant) [26,27] | EFV | (Grave/Defined): Level 1 | EFV may significantly reduce plasma levonorgestrel concentrations by 61 %, and the contraceptive effect can be decreased. Levonorgestrel implants are not recommended for women receiving long-term treatment with EFV. The patient should be informed of the need to use a barrier method as a complementary method of planning or to seek a safer contraceptive alternative. |
| Direct acting antiviral | |||
| Glecaprevir/Pibrentasvir [28-30] | ATV/RTV, DRV/RTV, FPV/RTV | (Grave/Defined): Level 1 | Boosted PIs increase glecaprevir/pibrentasvir plasma levels. Administration of glecaprevir/pibrentasvir with boosted PIs regimens is completely contraindicated. |
| Glecaprevir/Pibrentasvir [28-30] | EFV | (Grave/Defined): Level 1 | EFV may reduce glecaprevir/pibrentasvir plasma levels. Administration of glecaprevir/pibrentasvir with EFV is completely contraindicated. |
| Grazoprevir/Elbasvir [28-30] | NVP | (Grave/Defined): Level 1 | NVP may decrease grazoprevir/elbasvir plasma levels. Administration of grazoprevir/elbasvir with NVP is completely contraindicated. |
| Sofosbuvir/Velpatasvir/ Voxilaprevir [28-30] | ATV/RTV | (Grave/Defined): Level 1 | ATV/RTV may increase voxilaprevir plasma levels up to 4 times. Concomitant administration between ATV/RTV and voxilaprevir-containing regimens is contraindicated. |
| Sofosbuvir/Velpatasvir/ Voxilaprevir [28-30] | EFV | (Grave/Defined): Level 1 | EFV may decrease voxilaprevir plasma levels. Concomitant administration between EFV and voxilaprevir-containing regimens is contraindicated. |
| Direct acting oral anticoagulant | |||
| Edoxaban [13,31] | ATV | (Moderate/Defined): Level 2 | ATV may increase edoxaban plasma levels by inhibition of Pg-P. The use of these drugs is not recommended, therefore other oral anticoagulants should be considered as an alternative, or if it combination is necessary, a dose adjustment should be made. |
| Edoxaban [13,31] | ATV/RTV, DRV/RTV, FPV/RTV, LPV/RTV | (Moderate/Defined): Level 2 | Boosted PIs may increase edoxaban plasma levels. To monitor edoxaban safety parameters. It is recommended to reduce the dose of edoxaban from 60 mg to 30 mg daily. |
| Edoxaban [13,31] | ETR | (Grave/Defined): Level 1 | ETR may increase edoxaban plasma levels, increasing the risk of bleeding. The use of this combination is not recommended, other anticoagulants are suggested. |
| Edoxaban [13,31] | FPV | (Grave/Defined): Level 1 | FPV may increase/decrease edoxaban plasma levels, increasing the risk of bleeding and thrombus formation, respectively. The use of this combination is not recommended. |
| Drugs of abuse | |||
| Amphetamine [32] | LPV/RTV | (Grave/Possible): Level 2 | LPV/RTV may inhibit amphetamine metabolism, leading to increased plasma levels and toxicity. Warn patients about the risks of this combination. |
| Cocaine [33] | RPV | (Grave/Defined): Level 1 | RPV may inhibit cocaine metabolism, leading to increased plasma levels and toxicity. Warn patients about the risks of this combination. Cocaine overdose is life-threatening due to rhabdomyolysis, arrhythmia, and cardiovascular collapse. |
| Heroin [32] | ETR | (Grave/Possible): Level 2 | Heroin may decrease ETR plasma levels, resulting in a no suppressed viral load. Warn patients of the risk of using this combination. |
| Ketamine [32] | ETR | (Grave/Possible): Level 2 | Ketamine may decrease ETR plasma levels, resulting in a no suppressed viral load. Warn patients of the risk of using this combination. |
| Tetrahydrocannabinol (THC) [32] | EFV | (Grave/Possible): Level 2 | EFV may increase THC plasma levels, prolong its clinical effects and increase toxicity. Warn patients about the risks of this combination. |
| Tetrahydrocannabinol (THC) [32] | ETR | (Grave/Possible): Level 2 | THC may decrease ETR plasma levels, increasing the risk of faster HIV progression, neurocognitive impairment and immune dysfunction in people with HIV. Warn patients of the risk of using this combination. |
| Mineralocorticoid | |||
| Eplerenone [13] | ATV/RTV, DRV/RTV, FPV/RTV, LPV/RTV | (Grave/Defined): Level 1 | Boosted PIs may increase eplerenone plasma levels, increasing the risk of hyperkalemia. The use of this combination is not recommended. |
| Oral anticoagulant/Anti vitamin K | |||
| Warfarin [31] | DRV | (Moderate/Defined): Level 2 | PIs may increase warfarin plasma levels, increasing the risk of bleeding. To monitor warfarin safety parameters, a dose adjustment may be necessary. |
| Special condition | |||
| Pregnancy [34,35] | ATV, DRV | (Grave/Defined): Level 1 | Pregnancy may decrease PIs exposure. Using ritonavir-enhanced IPs in women who become pregnant while on ART treatment. |
| Pregnancy [34] | DOR | (Grave/Defined): Level 1 | Pregnancy may decrease DOR exposure. Currently, its use is not recommended in women who become pregnant while on ART treatment. |
ART: antiretroviral therapy; ATV: atazanavir; ATV/RTV: atazanavir/ritonavir; AUC: area under the curve; Cmax: maximum concentration; Cmin: minimum concentration; CYP: cytochrome; DRV: darunavir; DRV/RTV: darunavir/ritonavir; DOR: doravirine; ECG: electrocardiogram; EFV: efavirenz; ETR: etravirine; FPV: fosamprenavir; FPV/RTV: fosamprenavir/ritonavir; HIV: human immunodeficiency virus; LPV/RTV: lopinavir/ritonavir; NNRTIs: non-nucleoside reverse transcriptase inhibitors; NVP: nevirapine; Pg-P: P-Glycoprotein; PIs: protease inhibitors; RPV: rilpivirine; RTV: ritonavir; THC: tetrahydrocannabidiol.
Table 4.
New drug interactions with nucleoside reverse transcriptase inhibitors, integrase inhibitors and pharmacokinetic extender Level 1 and 2.
Table 4.
New drug interactions with nucleoside reverse transcriptase inhibitors, integrase inhibitors and pharmacokinetic extender Level 1 and 2.
| Pharmacological group or drugs affected | Antiretroviral agent | Gravity/Probability | Comments/Suggestions |
|---|---|---|---|
| Alpha-1 adrenergic receptor antagonist | |||
| Silodosin [12] | EVG/COBI | (Moderate/Probable): Level 2 | EVG/COBI may increase silodosin plasma levels by inhibition of CYP3A4. To monitor silodosin safety parameters, a dose adjustment may be necessary. |
| Anesthetic/Anxiolytic/ Benzodiazepine | |||
| Clonazepam [13] | EVG/COBI | (Moderate/Defined): Level 2 | EVG/COBI may increase benzodiazepines plasma levels. To monitor benzodiazepines safety parameters. It is recommended to use the lowest dose and for a short period of time. |
| Diazepam [13] | |||
| Midazolam [13] | (Grave/Defined): Level 1 | EVG/COBI may increase midazolam plasma levels, increasing the probability of respiratory depression, sedation, and muscle weakness. The use of this combination is not recommended. If necessary, parenteral midazolam should be used with close clinical monitoring or use safer alternatives such as lorazepam or propofol. | |
| Triazolam [13] | (Grave/Defined): Level 1 | EVG/COBI may increase triazolam plasma levels, increasing the probability of respiratory depression, sedation, and muscle weakness. The use of this combination is not recommended, safer alternatives such as oxazepam, lorazepam or temazepam should be used. | |
| Antacids | |||
| Aluminum hydroxide [13,36] | BIC, CAB, RAL | (Moderate/Defined): Level 2 | Antacids may produce chelation and affect InSTIs absorption, mainly antacids containing Ca2+, Al3+, Mg2+ and Fe2+. InSTIs may be given together with antacids containing calcium when taken along with food, but not on an empty stomach because food increases InSTIs exposure. Moreover, any antacid containing aluminum or magnesium should be administered at least 2 h after or 6 h before administration of InSTIs. |
| Calcium carbonate [13,36] | |||
| Ferrous fumarate [13,36] | |||
| Magnesium hydroxide [13,36] | |||
| Aluminum hydroxide [13,24,25,37,38] | DTG | (Moderate/Defined): Level 2 | Antacids may produce chelation and affect DTG absorption, mainly antacids containing polyvalent cations such as Mg2+, Al3+, Fe2+, Ca2+ and Zn2+. To administer DTG 2 hours before or 6 h after antacids. |
| Calcium carbonate [13,24,25,37,38] | |||
| Ferrous fumarate [13,24,25,37,38] | |||
| Magnesium hydroxide [13,24,25,37,38] | |||
| Zinc Gluconate [13,24,25,37,38] | |||
| Aluminum hydroxide [13] | EVG/COBI | (Moderate/Defined): Level 2 | Antacids may produce chelation and affect EVG absorption, mainly antacids containing polyvalent cations such as Mg2+, Al3+, Fe2+, Ca2+ and Zn2+. To separate EVG/COBI for 4 h from antacids. |
| Calcium carbonate [13] | |||
| Ferrous fumarate [13] | |||
| Magnesium hydroxide [13] | |||
| Zinc Gluconate [13] | |||
| Antiarrhythmic | |||
| Dofetilide [39] | DTG | (Grave/Defined): Level 1 | DTG administration causes a 70-90 % increase in dofeltilde plasma levels. Concomitant use is not recommended. |
| Antiasthmatic/Glucocorticoid | |||
| Budesonide [12] | EVG/COBI | (Moderate/Probable): Level 2 | EVG/COBI may increase budesonide and fluticasone plasma levels by inhibition of CYP3A4. To monitor budesonide and fluticasone safety parameters, a dose adjustment may be necessary. |
| Fluticasone [12,13] | |||
| Mometasone [12,13] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may increase mometasone plasma levels, and even lead to the appearance of Cushing's Syndrome. To monitor mometasone safety parameters and cortisol levels. To suspend treatment if necessary and use beclomethasone as an alternative. |
| Triamcinolone (injectable) [12,13,40] | EVG/COBI | (Grave/Probable): Level 1 | EVG/COBI may increase triamcinolone plasma levels by generating adrenal suppression. Do not co-administer unless the benefit outweighs the risk of systemic effect. Safer alternatives should be considered. |
| Anticoagulant/Anti vitamin K | |||
| Warfarin [31] | BIC, DTG, EVG/COBI | (Grave/Defined): Level 1 | InSTIs may increase warfarin plasma levels. To monitor warfarin safety parameters, especially INR, a dose adjustment may be necessary. |
| Anticonvulsant | |||
| Valproic acid [41] | DTG | (Grave/Possible): Level 2 | Valproic acid may decrease DTG plasma levels by inducing the metabolism of the enzymes UGT1A1 and CYP3A4, P-gp protein and BCRP transporter. Closely monitor DTG effectiveness parameters, because it may lead to increased resistance and increased viral load. In addition, other anticonvulsant alternatives such as levetiracetam are suggested. |
| Antidiabetic/Biguanide | |||
| Metformin [20] | BIC | (Moderate/Probable): Level 2 | BIC may increase metformin plasma levels by 39 % dose-dependent, through inhibition of MATE 1 and OCT2. Additionally, there have been cases of lactic acidosis and loss of glycemic control when the metformin dose was reduced empirically in combination with BIC. Efficacy and safety monitoring is recommended and dose adjustment may be required. Preferably start with low doses and increase according to the patient’s response. |
| Antidiabetic/Sulphonylurea | |||
| Chlorpropamide [39] | 3TC | (Moderate/Defined): Level 2 | 3TC administration may cause a significant reduction in exposure to chlorpropamide. It is advisable to strictly control blood glucose levels in diabetic patients treated concomitantly with these drugs. |
| Antimalarial | |||
| Artemether/Lumefantrine [39] | DTG | (Moderate/Defined): Level 2 | Artemether/Lumefantrine may decrease DTG exposure by 40 %. To monitor DTG effectiveness parameters, a dose adjustment may be necessary. |
| Artesunate/Amodiaquine [39] | DTG | (Moderate/Defined): Level 2 | Artesunate/Amodiaquine may decrease DTG exposure by 25-45 %. To monitor DTG effectiveness parameters, a dose adjustment may be necessary. |
| Atovaquone [15] | AZT | (Moderate/Defined): Level 2 | Atovaquone may increase the AUC of AZT. To monitor AZT effectiveness parameters, a dose adjustment may be necessary. |
| Antimicrobial/Oxazolidinone | |||
| Linezolid [17] | AZT | (Grave/Defined): Level 1 | The concomitant use of AZT and linezolid can produce hematologic toxicity, since it may generate suppression of the bone marrow. Avoid the concomitant use of AZT and linezolid due to the risk of hematological toxicity. |
| Antimicrobial/Sulfonamide | |||
| Trimethoprim/Sulfamethoxazole [39] | 3TC | (Moderate/Defined): Level 2 | Trimethoprim administration causes a 40% increase in 3TC plasma levels. There is no need to adjust the dose of 3TC in patients with normal renal function; the dose may be reduced in patients with renal failure. |
| Antimicrobial/Antituberculosis | |||
| Bedaquiline [17] | COBI | (Grave/Defined): Level 1 | COBI may significantly increase bedaquiline exposure. Closely monitor cardiac function using the ECG. |
| Rifabutin [17,20] | ABC, COBI | (Grave/Defined): Level 1 | Rifabutin may induce CYP3A4 and increase ABC and COBI metabolism, causing a decrease in plasma levels and virological response. It is not recommended given the risk of reducing viral susceptibility and the development of resistance associated with therapeutic ARV drug levels. |
| Rifampicin [19,20] | ATV/COBI | (Grave/Defined): Level 1 | Rifampicin may induce CYP3A4 and increase ATV/COBI metabolism, causing decrease in plasma levels and virological response. Administration of rifampicin with ATV/COBI is completely contraindicated. |
| Rifampicin [17,20,36] | BIC | (Grave/Defined): Level 1 | Rifampicin may induce BIC metabolism, causing a significant decrease in plasma levels (46-61 %), resulting in a loss of therapeutic effect. Dose recommendations for co-administration of BIC and rifampicin have not been established, however, the combination is contraindicated. |
| Rifampicin [36,40,42,43] | CAB | (Grave/Defined): Level 1 | Rifampicin may induce CAB metabolism, causing a 60 % decrease in oral CAB AUC, resulting in loss of therapeutic effect. Additionally, oral rifampicin may decrease exposure to intramuscular CAB by 44 %. Dose recommendations for co-administration of CAB and rifampin have not been established, however, the combination is contraindicated. |
| Rifampicin [17] | EVG/COBI | (Grave/Probable): Level 1 | Rifampicin may decrease EVG/COBI plasma levels, causing risk of reduced viral susceptibility and development of resistance. Simultaneous use between EVG/COBI and rifampicin is not recommended. |
| Antimigraine | |||
| Ergotamine/Dipyrone/Caffeine [44] | TDF/FTC/EVG/COBI | (Grave/Possible): Level 2 | COBI may increase plasma ergotamine concentrations by inhibiting CYP3A4, increasing the probability of ergotism: High blood pressure, nervousness, hallucinations, seizures, gastrointestinal and muscle disorders, as well as the appearance of acute ischemia of the lower extremities. To monitor ergotamine safety parameters. Rapid initiation of treatment is important to reduce the risk of ischemic sequelae. |
| Antineoplastic | |||
| Methotrexate [42] | CAB | (Grave/Defined): Level 1 | CAB can inhibit OAT1 and OAT3 causing increased methotrexate plasma levels. This combination requires strict vigilance, because methotrexate is a drug with a narrow therapeutic index. |
| Vinblastine [25] | AZT | (Grave/Defined): Level 1 | AZT may increase the probability of hematologic toxicity with the use of vinblastine. This combination is not recommended due to the possibility of serious adverse effects. |
| Antiplatelet agents | |||
| Clopidogrel [13] | EVG/COBI | (Grave/Defined): Level 1 | Boosted ARVs may alter clopidogrel antiplatelet effect. Co-administration of clopidogrel with boosted regimens is not possible. Use alternative antiplatelet agents or non-boosted regimens. |
| Ticagrelor [13] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may increase ticagrelor plasma levels, increasing the risk of bleeding. The use of ticagrelor with boosted ARVs is not recommended. Other antiplatelet agents are suggested as an alternative. |
| Antiulcer/Proton Pump Inhibitor | |||
| Omeprazole [12] | EVG/COBI | (Grave/Probable): Level 1 | EVG/COBI may increase omeprazole plasma levels by inhibition of CYP3A4. To monitor omeprazole safety parameters, a dose adjustment may be necessary. |
| Antiviral/Purine Analogue | |||
| Ribavirin [45,46] | AZT | (Grave/Defined): Level 1 | Concomitant use between AZT and ribavirin increases the probability of development of bone medulla suppression, associated with the appearance of severe hematological toxicity and increased risk of anemia. This combination is not recommended due to serious adverse effects. |
| Atypical antipsychotic | |||
| Quetiapine [12] | EVG/COBI | (Moderate/Probable): Level 2 | EVG/COBI may increase quetiapine plasma levels by inhibition of CYP3A4. To monitor quetiapine safety parameters, a dose adjustment may be necessary. |
| Direct-acting antiviral | |||
| Grazoprevir/Elbasvir [29] | COBI | (Grave/Defined): Level 1 | COBI may increase grazoprevir plasma levels. The administration of grazoprevir/elbasvir with COBI is completely contraindicated. |
| Direct oral anticoagulant | |||
| Apixaban [13,31] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may inhibit CYP3A4, causing increased apixaban plasma levels. The use of this combination is not recommended. |
| Dabigatran [13,31] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may increased dabigatran plasma levels by inhibition of Pg-P. The use of this combination is not recommended. Other anticoagulants are suggested as an alternative. |
| Edoxaban [13,31] | ATV/COBI | (Grave/Defined): Level 1 | ATV/COBI may increased edoxaban plasma levels. It is not recommended to use this combination; it is suggested to use other anticoagulants as an alternative. |
| Edoxaban [13,31] | DRV/COBI | (Moderate/Defined): Level 2 | DRV/COBI may increase plasma concentrations of edoxaban by inhibition of P-gp. It is recommended to monitor edoxaban safety parameters, especially in patients with renal damage. |
| Edoxaban [13,31] | EVG/COBI | (Moderate/Defined): Level 2 | EVG/COBI may inhibit CYP3A4, causing increase edoxaban plasma levels. To monitor edoxaban safety parameters. It is recommended to reduce the dose of edoxaban from 60 mg to 30 mg. |
| Rivaroxaban [13,31] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may inhibit CYP3A4, causing increase rivaroxaban plasma levels. The use of this combination is not recommended. |
| Disease | |||
| Severe renal impairment (36) | DTG | (Grave/Defined): Level 1 | Severe kidney failure can decrease DTG plasma levels. Caution is recommended in certain populations, for example, those with resistance associated with the use of InSTIs. |
| Drugs abuse | |||
| Amphetamine [32] | EVG/COBI | (Moderate/Probable): Level 2 | EVG/COBI may increase plasma levels of abused drugs, prolong their clinical effects and increase toxicity. Warn patients about the risks of these combinations. |
| Cannabis [32] | |||
| Ecstasy (MDMA) [32] | |||
| Heroin [32] | |||
| Ketamine [32] | |||
| Methamphetamine [32] | |||
| Cocaine [33] | EVG/COBI | (Grave/Probable): Level 1 | Simultaneous administration of cocaine and EVG/COBI may reduce cocaine metabolism, leading to increased plasma levels and toxicity. Warn patients about the risks of this combination. Cocaine overdose is life-threatening due to rhabdomyolysis, arrhythmia, and cardiovascular collapse. |
| Feminizing Hormone Therapy (FHT) | |||
| Estradiol Valerate/Cyproterone Acetate [47] | TDF/FTC | (Moderate/Probable): Level 2 | TDF exposure was reduced by 12 % in the presence of FHT, suggesting that it may potentially affect the effectiveness of PrEP among transgender women. To monitor TDF effectiveness parameters. |
| Mineralocorticoid | |||
| Eplerenone [13] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may increase eplerenone plasma levels, increasing the risk of hyperkalemia. The use of this combination is not recommended. |
| PI | |||
| Ritonavir [19,25,48-50] | DTG | (Moderate/Defined): Level 2 | Ritonavir may significantly reduce DTG plasma levels. To monitor DTG effectiveness parameters, a dose adjustment may be necessary. |
| Special conditions | |||
| Pregnancy [34] | BIC | (Grave/Defined): Level 1 | Pregnancy may decrease BIC exposure. This drug is not currently recommended in women who become pregnant while on ART treatment. |
| Pregnancy [34,36,51,52] | EVG/COBI | (Grave/Defined): Level 1 | Pregnancy may decrease the AUC of EVG and COBI by 24 % and 44 %, respectively, during the second trimester. Additionally, pregnancy may decrease the AUC of COBI by 59 % during the third trimester. This scheme should not be used during pregnancy. If women become pregnant during treatment with COBI it should be changed to an alternative treatment regimen such as ritonavir. |
| Pregnancy [34] | TDF/FTC/RAL | (Grave/Defined): Level 1 | Pregnancy may decrease TDF/FTC/RAL exposure. This scheme is not currently recommended in women who become pregnant while on ART treatment. |
| Pregnancy [36,51,52] | CAB | (Grave/Possible): Level 2 | Three cases of pregnancy were reported in patients who were using CAB. CAB is not recommended during pregnancy. However, more studies are needed to prove the effectiveness of this drug in pregnancy. |
| Pregnancy [34,36,53] | DTG | (Moderate/Defined): Level 2 | Exposure to DTG in pregnancy may be associated with an increased risk of neural tube defects in fetus. Additionally, a decrease in DTG exposure between 10-50 % has been demonstrated compared to postpartum plasma levels. The use of DTG should be avoided, especially in the first trimester of pregnancy, however, some studies claim that it can be administered without dose adjustment during pregnancy, if it is taken with food to increase absorption. |
| Pregnancy [54] | TDF | (Moderate/Defined): Level 2 | Pregnancy may decrease exposure and TDF plasma levels. Monitor viral load continuously. |
| Statins | |||
| Lovastatin [13] | EVG/COBI | (Grave/Defined): Level 1 | EVG/COBI may increase lovastatin and simvastatin plasma levels, increasing the risk of myopathies, rhabdomyolysis and even death. These combinations are not recommended. Safer alternatives such as pravastatin or fluvastatin should be used. |
| Simvastatin [13] | |||
| Tricyclic antidepressant drugs | |||
| Amitriptyline [13] | EVG/COBI | (Moderate/Defined): Level 2 | EVG/COBI may increase plasma levels of tricyclic antidepressants. It is recommended to start with low doses of antidepressant and adjust the dose according to the patient’s response, monitoring safety parameters. |
| Clomipramine [13] | |||
| Imipramine [13] | |||
| Uricosuric agent | |||
| Probenecid [55] | TDF/FTC | (Grave/Possible): Level 2 | Probenecid increases the AUC of TDF and FTC by 64 % and 62 %, respectively. Administer this combination with caution. |
ARV: antiretroviral; ATV/COBI: atazanavir/cobicistat; AUC: area under the curve; AZT: zidovudine; BCRP: breast cancer resistant protein; BIC: bictegravir; CAB: cabotegravir; COBI: cobicistat; CYP: cytochrome; DRV/COBI: darunavir/cobicistat; DTG: dolutegravir; ECG: electrocardiogram; EVG: elvitegravir; EVG/COBI: elvitegravir/cobicistat; INR: International Normalized Ratio; InSTIs: integrase inhibitors; MATE 1: toxin extrusion proteins and multiple drugs; NRTIs: nucleoside reverse transcriptase inhibitors; OAT1/OAT3: organic anion transporters; OCT2: organic cation transporters; P-gp: P-Glycoprotein; PrEP: pre-exposure prophylaxis; RAL: raltegravir; TDF: tenofovir disoproxil-fumarate; TDF/FTC: tenofovir disoproxil-fumarate/emtricitabine; TDF/FTC/EVG/COBI: tenofovir disoproxil-fumarate/emtricitabine/elvitegravir/cobicistat; TDF/FTC/RAL: tenofovir disoproxil-fumarate/emtricitabine/raltegravir; UGT1A1: uridinadifosfatoglucoronosiltransferasa; 3TC: lamivudine.
Table 5.
New drug interaction pairs with evidence for lack of clinically relevant interactions (Level 5).
Table 5.
New drug interaction pairs with evidence for lack of clinically relevant interactions (Level 5).
| Pharmacological group or drugs affected | Antiretroviral agent | Comments/Suggestions |
|---|---|---|
| Anesthetic/Anxiolytic/ Benzodiazepine | ||
| Diazepam [40,45,46] | AZT, TDF | Plasma levels of either drug is not affected. These combinations are safe and do not require dose adjustment. |
| Midazolam [40] | CAB | CAB does not modify the pharmacokinetics of midazolam. It is a safe combination, therefore, does not require dose adjustment. |
| Triazolam [45,46] | TDF | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Anticoagulant/Anti vitamin K | ||
| Warfarin [31] | 3TC | No significant changes in plasma levels of 3TC and warfarin are generated. This combination is safe and does not require dose adjustment. |
| Warfarin [25,31,38] | MVC | No significant changes in plasma levels of MVC and warfarin are generated. This combination is safe and does not require dose adjustment. |
| Warfarin [31] | TDF/FTC/RPV | No significant changes in plasma levels of RPV and warfarin are generated. This combination is safe and does not require dose adjustment. |
| Antifungal | ||
| Clotrimazole [56] | NVP | No significant changes in plasma levels of NVP and clotrimazole are generated. This combination is safe and does not require dose adjustment. |
| Voriconazole [19,56] | BIC | No significant changes in plasma levels of BIC and voriconazole are generated. This combination is safe and does not require dose adjustment. |
| Antimalarial | ||
| Chloroquine [57] | EFV | EFV does not change chloroquine plasma levels. This combination is safe and does not require dose adjustment. |
| Antimicrobial/Antituberculosis | ||
| Ethambutol [58] | LPV/RTV | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Ethionamide [58] | LPV/RTV | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Levofloxacin [17,58] | EFV | No significant changes in plasma levels of EFV and levofloxacin are generated. This combination is safe and requires no dose adjustment. |
| Pyrazinamide [58] | LPV/RTV | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Rifabutin [17,59] | ATV/RTV | No significant changes in plasma levels of ATV/RTV and rifabutin are generated. This combination is safe and does not require dose adjustment. |
| Rifabutin [17,59] | BIC | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Terizidone [58] | LPV/RTV | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Antiplatelet agent | ||
| Acetylsalicylic acid [13] | EVG/COBI | There are no significant changes in plasma levels of EVG/COBI and acetylsalicylic acid. This combination is safe and requires no dose adjustment. |
| Conjugated estrogens | ||
| Estradiol [60] | TDF/FTC | The use of conjugated estrogens for the GAHT reduces from 24-32 % in the AUC of TDF and FTC, but there is no statistically significant reduction in plasma levels of TDF/FTC and estradiol. The combination of TDF and FTC on demand (2+1+1) and GAHT may result in plasma levels too low for reliable prevention of HIV infection. |
| Direct acting oral anticoagulant | ||
| Apixaban [25,31,38] | ABC, ABC/AZT, ABC/3TC, BIC, BIC/TAF/FTC, DTG, DTG/ABC/3TC, EFV, MVC, TFV/FTC, TDF/FTC/RPV, T-20, 3TC | There are no significant changes in the plasma levels of apixaban and the ARVs mentioned. These combinations are safe and do not require dose adjustment. |
| Dabigatran [25,31,38] | ABC, ABC/AZT, ABC/3TC, BIC, BIC/TAF/FTC, DTG, DTG/ABC/3TC, EFV, MVC, TFV/FTC, TDF/FTC/RPV, T-20, 3TC | There are no significant changes in the plasma levels of dabigatran and the ARVs mentioned. These combinations are safe and do not require dose adjustment. |
| Edoxaban [25,31,38] | ABC, ABC/AZT, ABC/3TC, BIC, BIC/TAF/FTC, DTG, DTG/ABC/3TC, EFV, MVC, TFV/FTC, TDF/FTC/RPV, T-20, 3TC | There are no significant changes in the plasma levels of edoxaban and the ARVs mentioned. These combinations are safe and do not require dose adjustment. |
| Rivaroxaban [25,31,38] | ABC, ABC/AZT, ABC/3TC, BIC, BIC/TAF/FTC, DTG, DTG/ABC/3TC, EFV, MVC, TFV/FTC, TDF/FTC/RPV, T-20, 3TC | There are no significant changes in the plasma levels of rivaroxaban and the ARVs mentioned. These combinations are safe and do not require dose adjustment. |
| Disease | ||
| Mild to moderate hepatic impairment [36] | DTG, EVG, RAL | No significant differences have been observed in the exposures of InSTIs in people with mild to moderate liver impairment. Dose adjustment is not required in patients with mild to moderate liver impairment. |
| Drugs of abuse | ||
| Amphetamine [32] | ABC, DTG, NVP, RAL, RPV | There are no changes in the plasma levels of the ARVs mentioned. No dose adjustment is required. |
| Cannabis [32] | ABC, NVP, RAL, RPV | There are no changes in the plasma levels of the ARVs mentioned. No dose adjustment is required. |
| Ecstasy (MDMA) [32] | ||
| Methamphetamine [32] | ||
| Heroin [32] | ABC, RAL, RPV | There are no changes in the plasma levels of the ARVs mentioned. No dose adjustment is required. |
| Ketamine [32] | ||
| Nitrates | ABC, EFV, EVG/COBI, NVP, RAL, RPV | There are no changes in the plasma levels of the ARVs mentioned. No dose adjustment is required. |
| Attachment inhibitor | ||
| Fostemsavir [61] | ETR | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Injectable contraceptive | ||
| Medroxyprogesterone [62] | AZT | AZT does not reduce plasma levels of medroxyprogesterone (progestin). This combination is safe and does not require dose adjustment. |
| Medroxyprogesterone [63] | TDF (Topical) | Medroxyprogesterone affects the systemic and mucosa pharmacokinetics of TDF (topical) in healthy women. However, TDF administered topically for HIV-1 prevention in women resulted in high and protective mucosal concentrations with or without use of medroxyprogesterone. This combination is safe and requires no dose adjustment. |
| NNRTI | ||
| Etravirine [61] | CAB | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Rilpivirine [64] | CAB | Intramuscular administration of CAB has a low probability of pharmacokinetic interaction with rilpivirine. This combination is safe and does not require dose adjustment. |
| Oral contraceptive | ||
| Ethinylestradiol/Levonorgestrel [65] | CAB | There are no significant changes in plasma levels of CAB and ethinylestradiol/levonorgestrel. This combination is safe and requires no dose adjustment. |
| Ethinylestradiol [45,46,65] | TDF | There are no significant changes in plasma levels of TDF and ethinylestradiol. This combination is safe and requires no dose adjustment. |
| Ethinylestradiol/Levonorgestrel [63] | TDF (Topical) | Ethinylestradiol/Levonorgestrel affects the systemic and mucosa pharmacokinetics of TDF (topical) in healthy women. However, TDF administered topically for HIV-1 prevention in women resulted in high and protective mucosal concentrations with or without use of oral contraceptives. This combination is safe and requires no dose adjustment. |
| PI | ||
| Atazanavir [19] | BIC | Plasma levels of either drug is not affected. This combination is safe and does not require dose adjustment. |
| Special condition | ||
| Adults < 74 years [36] | BIC | There are no changes in plasma levels of BIC in adults < 74 years. Dose adjustment is not required in these patients. |
| Adults > 65 years [36] | EVG | There are no changes in plasma levels of EVG in adults > 65 years. Dose adjustment is not required in these patients. |
| Dialysis [36] | DTG, EVG, RAL | InSTIs are highly bound to plasma proteins (albumin and alpha-1 acid glycoprotein, 83-99 %) and are not significantly eliminated by dialysis (hemodialysis or peritoneal dialysis). Dose adjustment is not required in patients receiving hemodialysis or peritoneal dialysis. |
| Statin | ||
| Lovastatin [45,66] | DOR, RPV | There are no changes in the plasma levels of NNRTIs and lovastatin. These combinations are safe and do not require dose adjustment. |
| Pitavastatin [45,66] | ATV, DRV, LPV/RTV | There are no changes in the plasma levels of PIs and pitavastatin. These combinations are safe and do not require dose adjustment. |
| Pitavastatin [45,66] | ATV/RTV, DRV/RTV, FPV/RTV | There are no changes in the plasma levels of boosted PIs and pitavastatin. These combinations are safe and do not require dose adjustment. |
| Pitavastatin [45,66] | DOR, EFV, NVP | There are no changes in the plasma levels of NNRTIs and pitavastatin. These combinations are safe and do not require dose adjustment. |
| Pitavastatin [45,66] | EVG/COBI | There are no changes in the plasma levels of EVG/COBI and pitavastatin. These combinations are safe and do not require dose adjustment. |
| Pravastatin [45,66] | DOR, RPV | DOR and RPV do not affect the pharmacokinetics of pravastatin. These combinations are safe and do not require dose adjustment. |
| Rosuvastatin [45,66] | DOR, EFV, NVP, RPV | There are no changes in the plasma levels between NNRTIs and rosuvastatin. These combinations are safe and do not require dose adjustment. |
| Simvastatin [45,66] | DOR, NVP, RPV | There are no changes in the plasma levels between NNRTIs and simvastatin. These combinations are safe and do not require dose adjustment. |
| Thiazide antihypertensive | ||
| Hydrochlorothiazide [13] | ATV/RTV, DRV/RTV, FPV/RTV, LPV/RTV | There are no changes in the plasma levels between boosted PIs and hydrochlorothiazide. These combinations are safe and does not require dose adjustment. |
| Hydrochlorothiazide [13] | EVG/COBI | There are no changes in the plasma levels of EVG/COBI and hydrochlorothiazide. This combination is safe and do not require dose adjustment. |
ABC: abacavir; ABC/AZT: abacavir/zidovudine; ABC/3TC: abacavir/lamivudine; ARV: antiretroviral; ATV/RTV: atazanavir/ritonavir; AZT: zidovudine; BIC: bictegravir; BIC/TAF/FTC: bictegravir/tenofovir alafenamide/emtricitabine; CAB: cabotegravir; DOR: doravirine; DRV: darunavir; DRV/RTV: darunavir/ritonavir; DTG: dolutegravir; DTG/ABC/3TC: dolutegravir/abacavir/lamivudine; EFV: efavirenz; ETR: etravirine; EVG: elvitegravir; EVG/COBI: elvitegravir/cobicistat; FPV/RTV: fosamprenavir/ritonavir; GAHT: gender-affirmation hormone therapy; HIV: human immunodeficiency virus; InSTIs: integrase inhibitors; LPV/RTV: lopinavir/ritonavir; MVC: maraviroc; NNRTIs: non-nucleoside reverse transcriptase inhibitors; NVP: nevirapine; PIs: protease inhibitors; RAL: raltegravir; RPV: rilpivirine; TAF: tenofovir alafenamide; TDF: tenofovir disoproxil-fumarate; TDF/FTC: tenofovir disoproxil-fumarate/emtricitabine; TDF/FTC/RPV: tenofovir disoproxil-fumarate/emtricitabine/rilpivirine; T-20: enfuvirtide; 3TC: lamivudine.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



