
Submitted:
12 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
Background: There is poor evidence about sensitivity to chemotherapy according to microsatellite instability (MSI)/mismatch repair (MMR) status in endometrial cancer (EC).
Methodology: The RAME study is a retrospective analysis aiming to assess response to chemotherapy in MSI-high (h) /deficient (d) MMR and MSI- low (l)/proficient (p)MMR EC patients. Primary endpoints were recurrence-free survival (RFS) for patients with localized disease and progression-free survival (PFS) and overall survival (OS) in patients with advanced/recurrent disease.
Results: 312 patients treated between 2010-2022 in 4 high volume Multicenter Italian Trial in Ovarian cancer and gynecological malignancies (MITO) centers were selected. 239 patients had endometrioid EC (76.6%), 151 had FIGO stage I at diagnosis (48.9%) and 71 were MSI-h/dMMR (22.8%). Median age was 65 (range 31–91) years. Among patients with localized disease, median RFS was 100.0 months (95%CI 59.4–140.7) for MSI-l/pMMR and 120.9 months (60.0-181.8) for MSI-h/dMMR (p=0.39). Seventy-seven patients received first-line chemotherapy for advanced/recurrent disease. Patients with MSI-h/dMMR ECs had a significantly worse OS (p=0.039). In patients receiving platinum-based chemotherapy, no statistically significant difference in PFS (p=0.21) and OS (p=0.057) were detected, although PFS and OS were numerically longer in the MSI-l/pMMR population.
Conclusion: Patients with metastatic MSI-h/dMMR EC receiving first-line chemotherapy had a significantly worse OS.
Keywords:
Endometrial cancer
; microsatellite instability
; mismatch repair deficiency
; platinum-based chemotherapy
Introduction
Endometrial cancer (EC) is the most common gynaecological malignancy with increased incidence and disease-related mortality in recent years, especially in developed countries[1]. Approximately 3.1 percent of women will be diagnosed with uterine cancer at some point during their lifetime, based on 2017–2019 data[1]. Whereas early-stages EC are associated with an excellent 5-year relative survival rate (96%), this rate decreases to 18% in patients with advanced/metastatic disease[2,3]. Platinum based chemotherapy with carboplatin and paclitaxel is currently the standard of care in first line for metastatic EC, with an overall response rate (ORR) of 50-60%, a median progression-free survival (PFS) and an overall survival (OS) of 8 months and 15-20 months, respectively[4,5,6].
Historically EC was classified, according to the Bokhman classification[7], as type I (endometrioid) or type II (non-endometrioid). In 2013 The Cancer Genome Atlas (TGCA)[8,9,10,11] introduced a new classification based on molecular analysis: EC is no longer considered as a single entity, but the set of types of different tumours, each with a completely different prognosis. The new classification includes four subgroups: DNA polymerase epsilon (POLE)-mutated tumors; tumors with high microsatellite instability (MSI), or DNA mismatch repair mechanism (dMMR) deficiency, which identifies patients at risk for Lynch syndrome (LS)[12,13]; tumors with p53 alterations (p53-mutants), or copy-number high and tumors with no specific molecular profile (NSMP), or low copy-number.
The first two are distinguished by a defect in DNA repair, a high mutational rate, and a high neoantigen load. These two subgroups are also inflamed due to an abundance of tumor-infiltrating lymphocytes and increased expression of Programmed cell death protein 1 (PD-1) and PD-L1 as well as potentially more responsive to immune checkpoint inhibitors (ICIs)[14,15,16]. MMR is a highly conserved mechanism that restores DNA integrity by correcting single-base mismatches and insertion-deletion loops that can occur during DNA replication[17].
The last few years have witnessed the approvals of ICIs in the setting of advanced/metastatic EC previously treated with platinum based chemotherapy: dostarlimab on the basis of GARNET study[16] for MSI-h/dMMR, pembrolizumab on the basis of KEYNOTE-158[18], again for MSI-h/dMMR and pembrolizumab plus lenvatinib on the basis of KEYNOTE-775 trial[19] for MSI-l/pMMR. Recent research into the administration of ICIs in combination with chemotherapy has yielded very promising results. The ENGOT-EN6-NSGO/GOG-3031/RUBY trial[20] has provided strong data in terms of PFS and OS for the use of dostarlimab in combination with chemotherapy; furthermore, NRG-GY018 study[21] demonstrated that combining pembrolizumab with standard chemotherapy resulted in significantly longer PFS than chemotherapy alone in both the MSI-h/dMMR and MSI-l/dMMR cohorts. As a result, the combination of ICIs and carboplatin-paclitaxel is a new gold standard for advanced/metastatic EC.
It is now well established that immunotherapy in MSI-h/dMMR EC is the best option both in first line combined with chemotherapy and after failure of first-line carboplatin and paclitaxel and data from the recently completed PORTEC3 trial[22,23,24,25] suggested that adjuvant platinum-based chemotherapy had no benefit in MSI-h/dMMR EC.
However, limited data on the response to frontline carboplatin plus paclitaxel in EC are available[4].
We conducted a multicenter retrospective study with the aim of describing (i) RFS for patients with EC eligible at diagnosis for potentially curative treatment and treated with surgery, and (ii) PFS and OS in patients with advanced/recurrent disease, in particular in patient treated with platinum-based chemotherapy.
Methods
Patients
Patients with EC with known MSI/MMR status treated consecutively between January 2010 and January 2022 in four high volume MITO centers (Mauriziano Hospital, Candiolo Hospital, Bari Hospital and Reggio Emilia Hospital) were identified via a multicenter retrospective review of electronic case records. Eligibility criteria included adult patients with EC with any histology and stage of disease. Standardized chart review collected date of diagnosis, age at diagnosis, comorbidities, date of initial local therapy, adjuvant treatment, MMR/MSI status, date of first relapse, subsequent treatments and types. Data cut off was 30 April 2023. The study was approved by a central ethics committee, and informed consent was obtained from patients. Flow chart of the study is reported in Figure 1.
Efficacy endpoints
Primary endpoints of the study were RFS for patients with localized disease at diagnosis and treated with surgery; PFS and OS in patients with advanced/recurrent disease. In this setting, PFS and OS were calculated in the subgroup of patients receiving platinum based chemotherapy. Response was determined by local assessment from the clinician, according to computed tomography (CT)-scanner evaluation or positron emission tomography CT (PET-CT) evaluation. RFS was defined as the time from date of diagnosis to first recurrence. PFS was defined as the time from the date of start of first line therapy to disease progression or death. OS was defined as the time from the date of start of first line therapy to death.
MMR/MSI testing
The MMR/MSI status was assessed locally, according to one of the standard practices. Methods for determination included loss of 1 or more MMR protein expression by immunochemistry (IHC), or instability in 2 or more of five tumor repeat loci by polymerase chain reaction (PCR) assay.
Statistical analysis
Patients’ and tumor characteristics (age at diagnosis, comorbidities, histology, FIGO stage, surgery, MMR/MSI status and subsequent systemic treatment) were described (median for continuous variables and frequency for categorical variables). Median follow-up was estimated by using the reverse Kaplan-Meier method. RFS, PFS and OS were estimated by using the Kaplan-Meier method and median was reported with its 95% CI. The study cut-off date for the statistical analysis was April, 30th, 2023. Statistical analysis was performed by using IBM SPSS Statistics, version 28.0.1.0
Results
Between January 1st, 2010 and January 1st, 2022, we identified 317 patients with EC treated consecutively. The efficacy analysis was performed on 312 patients because of missing data of MMR/MSI status of 5 patients. All the patients’ characteristics are summarized in Table 1.
Median age was 65.3 (31.5–90.9) years, with no differences between the two groups analyzed (MSH-l/pMMR vs MSH-h/dMMR, p=0.26). The majority of patients were MSH-l/pMMR (77.2%, 241/312), mainly detected with immunohistochemistry (92%). Details of MMR status are reported in Table S1.
Most patients (71.2%, 22/312) had comorbidities: diabetes, hypertension and/or cardiopathy were the most frequent but with no differences between the two groups. Two-hundred and thirty-nine patients (76.6%) had endometrioid EC. Among MSH-l/pMMR, patients with endometrioid EC were 90.1% (p=0.002). At diagnosis nearly half of patients (48.9%) were FIGO stage I.
Among the 278 patients with no metastatic disease at diagnosis and treated with surgery, 171/278 (61.5%) underwent adjuvant therapy: 104/278 (37.4%) had radiotherapy, 96/278 had brachytherapy, 115/278 (41.4%) received chemotherapy and 6/278 (1.8%) received hormonal therapy. No differences between the two groups were highlighted among the different adjuvant treatments (respectively p=0.43 for RT, p=0.34 for BT, p=0.71 for chemotherapy, p=0.21 for HT). At a median FU of 58.2 months, the median RFS was 100.0 months (95%CI 59.4–140.7) for MSI-l/pMMR and 120.9 months (60.0-181.8) for MSI-h/dMMR 0.81, 95%CI 0.50-1.31, p=0.39). See Table 2 and Figure 2 for details.
Seventy-seven patients received first-line CT for advanced/recurrent disease, 76.6% (59/77) received platinum-based CT and 19.5% (15/77) were MSI-l/pMMR. Median age was 68.3 (39.8–87.2) years, with no differences between the MSH-l/pMMR and MSH-h/dMMR (p=0.72).
Median FU was 22.5 months. In this setting, median PFS was 10.3 months (95%CI 7.7-12.8) in MSI-l/pMMR and 6.3 months (95%CI 2.0-10.6) in MSI-l/pMMR (HR1.53, 95%CI 0.79 – 2.97, p=0.21). Median OS was 37.2 months (95%CI 28.0-46.4) for MSI-l/pMMR and median OS was 14.0 months (95%CI 1.0-27.1) for MSI-h/dMMR, with a significantly worse OS in MSI-h/dMMR patients (HR 2.26, 95% CI 1.04 – 4.92, p=0.039). (Table 3 and Figure 3A).
In the subgroup of patients receiving platinum-based CT, no statistically significant difference in PFS (p=0.21) and OS (p=0.057) were detected but PFS and OS were numerically longer in the MSI-l/pMMR population. Figure 3B.
Discussion
In this study we described a large series of 278 ECs treated for localized disease with surgery (± adjuvant treatments) and 77 advanced/metastatic ECs treated with first line chemotherapy, mainly platinum-based chemotherapy.
According to the literature, our series consists of about 20% of MSI-h/dMMR EC [24,26]. More than 90% of MSI-h/dMMR EC have endometroid histology. In the real life setting of this study, median age for advanced/metastatic EC was 68 years, slightly higher than that in major clinical trials investigating platinum-based chemotherapy in this setting (62 years in the Sovak et al. trial [27] and 65 years in the Pectasides D at al. trial[28]).
Currently we know from two most important first line randomized trials (RUBY[20] and NRGY-018[21]) that the addition of an ICI to carboplatin plus paclitaxel in advanced/metastastic EC improves PFS both in the dMMR population (HR 0.28 and 0.30 respectively), and in pMMR population (HR 0.64 and 0.54, respectively) with a better PFS in the control arm of the pMMR population.
In our retrospective real-world population of relapsed patients, which is similar to 50% of the RUBY population, we confirm a worse performance of carboplatin plus paclitaxel in relapsed dMMR EC (PFS 6 months), in comparison with the pMMR population (PFS 12 months). If we consider the adjuvant setting, there is only preliminary evidence that MMR/MSI status in EC can predict benefit from chemotherapy also in the adjuvant setting [29].
Results from the PORTEC3 trial[22] confirmed a modest but statistically significant benefit of adjuvant chemotherapy in terms of RFS and OS in all comers but suggested that adjuvant platinum-based chemotherapy had limited benefit in MSI-h/dMMR EC.
A post-hoc analysis was carried out to evaluate these results according to the molecular classification: the p53-mutated tumors in immunochemistry presented an absolute benefit of adjuvant chemotherapy of 25% in terms of RFS, whereas there was no benefit for dMMR tumors[24,30].
RAINBO umbrella program is now ongoing to identify the best adjuvant treatment in EC. Eligible patients will be assigned to one of the four RAINBOW trials (ClinicalTrials.gov Identifier: NCT05255653) based on the molecular profile of their cancers: p53 abnormal EC patients to the p53abn-RED trial; MSI-h/dMMR EC patients to the MMRd-GREEN trial; no specific molecular profile EC patients to NSMP-ORANGE trial and POLE mutant EC patients to the POLEmut-BLUE trial. Results could clarify the role of adjuvant treatments in a prospective setting.
In our cohort of patients with localized disease, median RFS was 120 months in MSI-h/dMMR versus 100 months in MSI-l/pMMR without any clear statistically significant difference between the the two populations [27,28].
None of the patients in this retrospective study received ICIs, so that the data of response to chemotherapy are not influenced by previous exposure to immunotherapy.
Our data suggested a numerically better RFS in MSI-h/dMMR (although the difference was not statistically significant), but when these patients experienced recurrence or in MSI-h/dMMR de novo EC, prognosis is worse in terms of both PFS and OS.
Our retrospective study did not define a preplanned statistical power neither for RFS analysis in patients with localized stage nor for PFS and OS analyses in advanced disease.
The analysis is limited to describing a prognostic difference between the groups analyzed, and we cannot comment definitively on the predictive role of MMR/MSI status, since all the patients enrolled in our study were treated in clinical practice and we do not have a control group.
Although the present study contains all the limitations associated with its retrospective nature, our real world data confirm that MSI-h/dMMR EC s show a modest outcome when treated with chemotherapy in the relapsed setting. Conversely, pMMR patients seem to derive a greater benefit from carboplatin plus paclitaxel.
Conclusions
In conclusion, our study further confirms the need to incorporate ICIs in the MSI-h/dMMR EC population in line with the data from randomized phase III clinical trials. The optimal choice for relapsed pMMR EC patients is still to be defined, especially in patients with long RFS, where Carboplatin Paclitaxel may still be a treatment choice.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author contributions
Conceptualization, V.T. and G.V.; Methodology, M.D.M; Validation, V.T., L.P., E.G., V.Q., F.A., A.P., V.D.M., E.G., G.C., N.B., L.B., S. G., A.F., E.J., L.F., J.O.S.P.S., A.P., A.C., C.R., M.T., G.S., M.D.M., and G.V.; Formal Analysis, M.D.M.; Investigation, V.T., M.D.M, and G.V.; Data Curation, V.T., L.P., M.D.M, and G.V.; Writing – Original Draft Preparation, V.T., M.D.M, and G.V.; Writing – Review & Editing, V.T., L.P., E.G., V.Q., F.A., A.P., V.D.M., E.G., G.C., N.B., L.B., S. G., A.F., E.J., L.F., J.O.S.P.S., A.P., A.C., C.R., M.T., G.S., M.D.M., and G.V.; Supervision, V.T., M.D.M, and G.V.; Project Administration, L.B. and S.G.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Città della Scienza e della Salute di Torino (protocol code 0034941 and date of 25/03/2022)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Conflict of Interest
all authors declare no conflicts of interest
The abstract was submitted to ESGO Congress 2023.
References
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Son J, Chambers LM, Carr C, Michener CM, Yao M, Beavis A, Yen TT, Stone RL, Wethington SL, Fader AN et al. Adjuvant treatment improves overall survival in women with high-intermediate risk early-stage endometrial cancer with lymphovascular space invasion. Int J Gynecol Cancer 2020, 30, 1738–1747. [Google Scholar] [CrossRef] [PubMed]
- Miller DS, Filiaci VL, Mannel RS, Cohn DE, Matsumoto T, Tewari KS, DiSilvestro P, Pearl ML, Argenta PA, Powell MA et al. Carboplatin and Paclitaxel for Advanced Endometrial Cancer: Final Overall Survival and Adverse Event Analysis of a Phase III Trial (NRG Oncology/GOG0209). J Clin Oncol 2020, 38, 3841–3850. [Google Scholar] [CrossRef] [PubMed]
- Makker V, MacKay H, Ray-Coquard I, Levine DA, Westin SN, Aoki D, Oaknin A. Endometrial cancer. Nat Rev Dis Primers 2021, 7, 88. [Google Scholar] [CrossRef] [PubMed]
- Passarello K, Kurian S, Villanueva V. Endometrial Cancer: An Overview of Pathophysiology, Management, and Care. Semin Oncol Nurs 2019, 35, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Bokhman, JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol 1983, 15, 10–17. [Google Scholar] [CrossRef]
- Wilczyński M, Danielska J, Wilczyński J. An update of the classical Bokhman’s dualistic model of endometrial cancer. Prz Menopauzalny 2016, 15, 63–68. [Google Scholar]
- Talhouk A, McAlpine JN. New classification of endometrial cancers: the development and potential applications of genomic-based classification in research and clinical care. Gynecol Oncol Res Pract 2016, 3, 14. [Google Scholar] [CrossRef]
- Talhouk A, McConechy MK, Leung S, Li-Chang HH, Kwon JS, Melnyk N, Yang W, Senz J, Boyd N, Karnezis AN et al. A clinically applicable molecular-based classification for endometrial cancers. Br J Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef]
- Moore K, Brewer MA. Endometrial Cancer: Is This a New Disease? Am Soc Clin Oncol Educ Book 2017, 37, 435–442. [Google Scholar] [CrossRef]
- Zhao S, Chen L, Zang Y, Liu W, Liu S, Teng F, Xue F, Wang Y. Endometrial cancer in Lynch syndrome. Int J Cancer 2022, 150, 7–17. [Google Scholar] [CrossRef]
- Li Z, Cheng B, Liu S, Ding S, Liu J, Quan L, Hao Y, Xu L, Zhao H, Guo J et al. Non-classical phenotypes of mismatch repair deficiency and microsatellite instability in primary and metastatic tumors at different sites in Lynch syndrome. Front Oncol 2022, 12, 1004469. [Google Scholar] [CrossRef] [PubMed]
- Howitt BE, Shukla SA, Sholl LM, Ritterhouse LL, Watkins JC, Rodig S, Stover E, Strickland KC, D’Andrea AD, Wu CJ et al. Association of Polymerase e-Mutated and Microsatellite-Instable Endometrial Cancers With Neoantigen Load, Number of Tumor-Infiltrating Lymphocytes, and Expression of PD-1 and PD-L1. JAMA Oncol 2015, 1, 1319–1323. [Google Scholar] [CrossRef]
- Yen TT, Wang TL, Fader AN, Shih IM, Gaillard S. Molecular Classification and Emerging Targeted Therapy in Endometrial Cancer. Int J Gynecol Pathol 2020, 39, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Oaknin A, Gilbert L, Tinker AV, Brown J, Mathews C, Press J, Sabatier R, O’Malley DM, Samouelian V, Boni V et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficient/microsatellite instability-high (dMMR/MSI-H) or proficient/stable (MMRp/MSS) endometrial cancer: interim results from GARNET-a phase I, single-arm study. J Immunother Cancer 2022, 10. [Google Scholar]
- Meyer LA, Broaddus RR, Lu KH. Endometrial cancer and Lynch syndrome: clinical and pathologic considerations. Cancer Control 2009, 16, 14–22. [Google Scholar] [CrossRef] [PubMed]
- O’Malley DM, Bariani GM, Cassier PA, Marabelle A, Hansen AR, De Jesus Acosta A, Miller WH, Safra T, Italiano A, Mileshkin L et al. Pembrolizumab in Patients With Microsatellite Instability-High Advanced Endometrial Cancer: Results From the KEYNOTE-158 Study. J Clin Oncol 2022, 40, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Makker V, Colombo N, Casado Herráez A, Santin AD, Colomba E, Miller DS, Fujiwara K, Pignata S, Baron-Hay S, Ray-Coquard I et al. Lenvatinib plus Pembrolizumab for Advanced Endometrial Cancer. N Engl J Med 2022, 386, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Mirza MR, Chase DM, Slomovitz BM, dePont Christensen R, Novák Z, Black D, Gilbert L, Sharma S, Valabrega G, Landrum LM et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N Engl J Med 2023. [Google Scholar]
- Eskander RN, Sill MW, Beffa L, Moore RG, Hope JM, Musa FB, Mannel R, Shahin MS, Cantuaria GH, Girda E et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. N Engl J Med 2023. [Google Scholar]
- de Boer SM, Powell ME, Mileshkin L, Katsaros D, Bessette P, Haie-Meder C, Ottevanger PB, Ledermann JA, Khaw P, Colombo A et al. Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): final results of an international, open-label, multicentre, randomised, phase 3 trial. Lancet Oncol 2018, 19, 295–309. [Google Scholar] [CrossRef]
- Stelloo E, Bosse T, Nout RA, MacKay HJ, Church DN, Nijman HW, Leary A, Edmondson RJ, Powell ME, Crosbie EJ et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer; a TransPORTEC initiative. Mod Pathol 2015, 28, 836–844. [Google Scholar] [CrossRef] [PubMed]
- León-Castillo A, de Boer SM, Powell ME, Mileshkin LR, Mackay HJ, Leary A, Nijman HW, Singh N, Pollock PM, Bessette P et al. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer: Impact on Prognosis and Benefit From Adjuvant Therapy. J Clin Oncol 2020, 38, 3388–3397. [Google Scholar] [CrossRef] [PubMed]
- de Boer SM, Wortman BG, Bosse T, Powell ME, Singh N, Hollema H, Wilson G, Chowdhury MN, Mileshkin L, Pyman J et al. Clinical consequences of upfront pathology review in the randomised PORTEC-3 trial for high-risk endometrial cancer. Ann Oncol 2018, 29, 424–430. [Google Scholar] [CrossRef]
- Soumerai TE, Donoghue MTA, Bandlamudi C, Srinivasan P, Chang MT, Zamarin D, Cadoo KA, Grisham RN, O’Cearbhaill RE, Tew WP et al. Clinical Utility of Prospective Molecular Characterization in Advanced Endometrial Cancer. Clin Cancer Res 2018, 24, 5939–5947. [Google Scholar] [CrossRef]
- Sovak MA, Dupont J, Hensley ML, Ishill N, Gerst S, Abu-Rustum N, Anderson S, Barakat R, Konner J, Poyner E et al. Paclitaxel and carboplatin in the treatment of advanced or recurrent endometrial cancer: a large retrospective study. Int J Gynecol Cancer 2007, 17, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Pectasides D, Xiros N, Papaxoinis G, Pectasides E, Sykiotis C, Koumarianou A, Psyrri A, Gaglia A, Kassanos D, Gouveris P et al. Carboplatin and paclitaxel in advanced or metastatic endometrial cancer. Gynecol Oncol 2008, 109, 250–254. [Google Scholar] [CrossRef]
- Zighelboim I, Goodfellow PJ, Gao F, Gibb RK, Powell MA, Rader JS, Mutch DG. Microsatellite instability and epigenetic inactivation of MLH1 and outcome of patients with endometrial carcinomas of the endometrioid type. J Clin Oncol 2007, 25, 2042–2048. [Google Scholar] [CrossRef]
- van den Heerik ASVM, Horeweg N, de Boer SM, Bosse T, Creutzberg CL. Adjuvant therapy for endometrial cancer in the era of molecular classification: radiotherapy, chemoradiation and novel targets for therapy. Int J Gynecol Cancer 2021, 31, 594–604. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study. *Data cut off 30 April 2023.
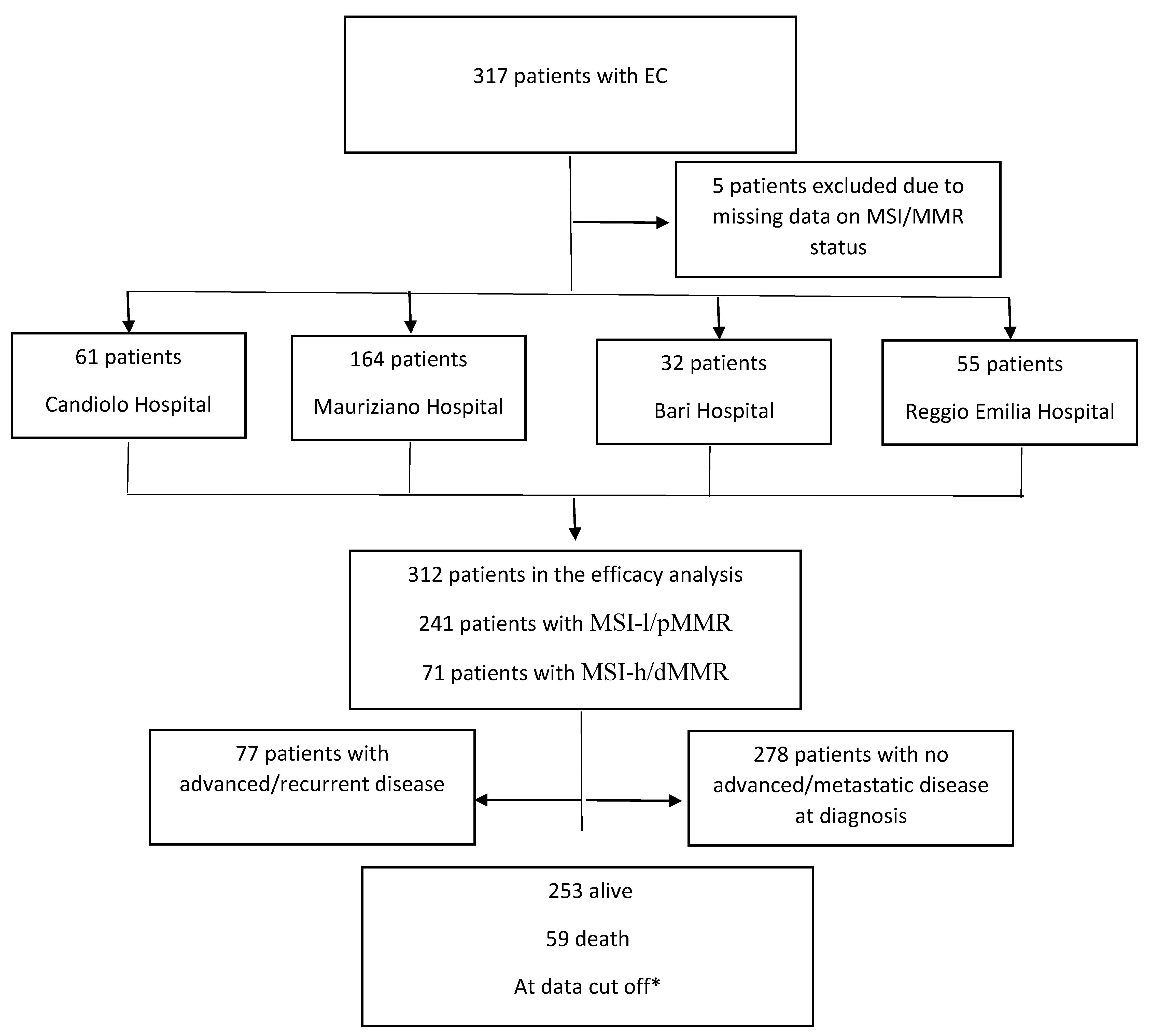
Figure 2.
RFS by MSI/MMR status. Blue line MSI-l/pMMR, green line MSI-h/dMMR. RFS was 83.9% at 1 year, 73.1% at 2 years, 69.2% at 3 years, 58.8% at 5 years and 46% at 10 years.
Figure 2.
RFS by MSI/MMR status. Blue line MSI-l/pMMR, green line MSI-h/dMMR. RFS was 83.9% at 1 year, 73.1% at 2 years, 69.2% at 3 years, 58.8% at 5 years and 46% at 10 years.
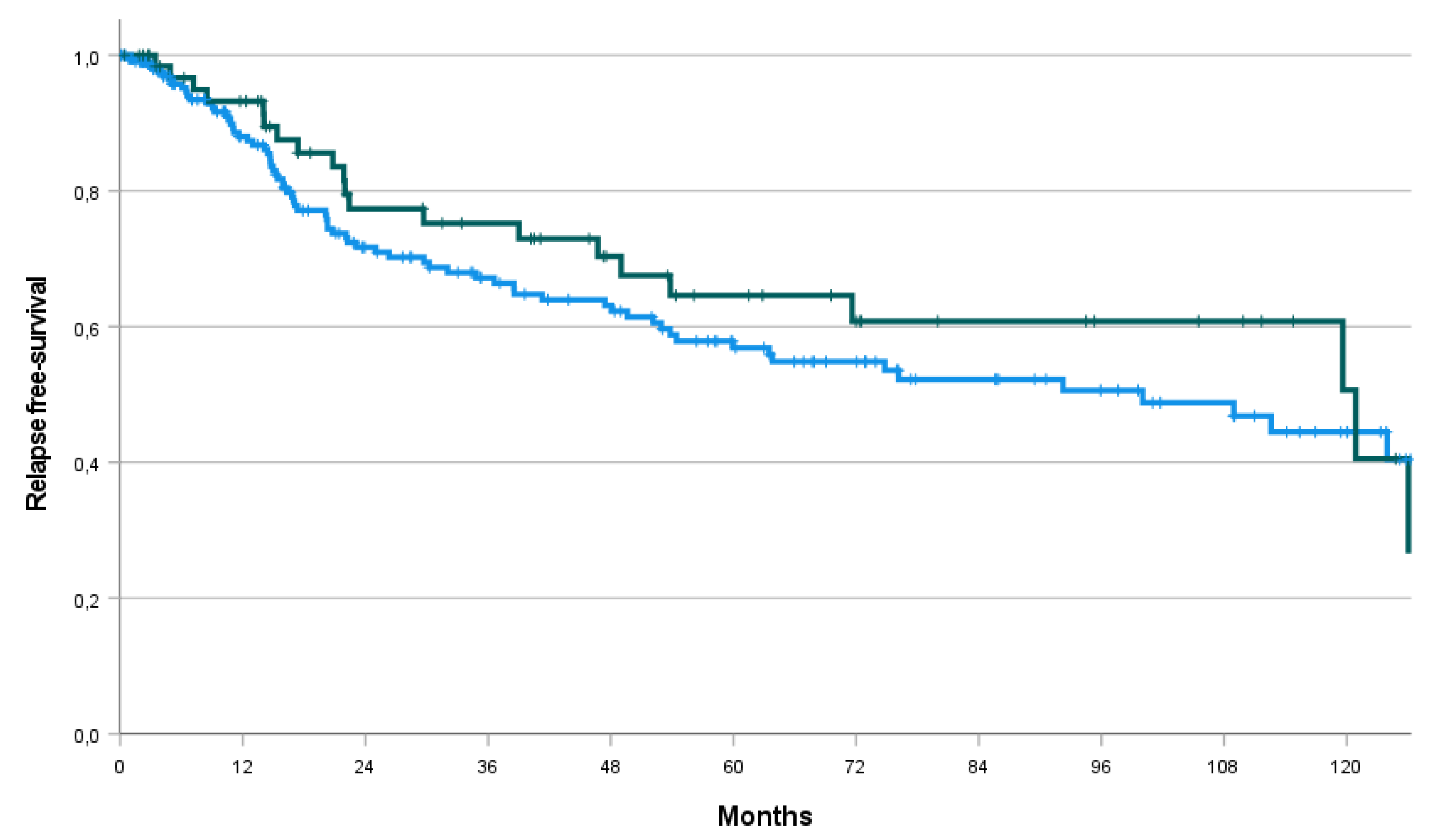
Figure 3.
A: PFS and OS by MSI/MMR status. B: PFS and OS by MSI/MMR status in patient receiving platinum based chemotherapy as first line of treatment. Blue line MSI-l/pMMR, green line MSI-h/dMMR.
Figure 3.
A: PFS and OS by MSI/MMR status. B: PFS and OS by MSI/MMR status in patient receiving platinum based chemotherapy as first line of treatment. Blue line MSI-l/pMMR, green line MSI-h/dMMR.
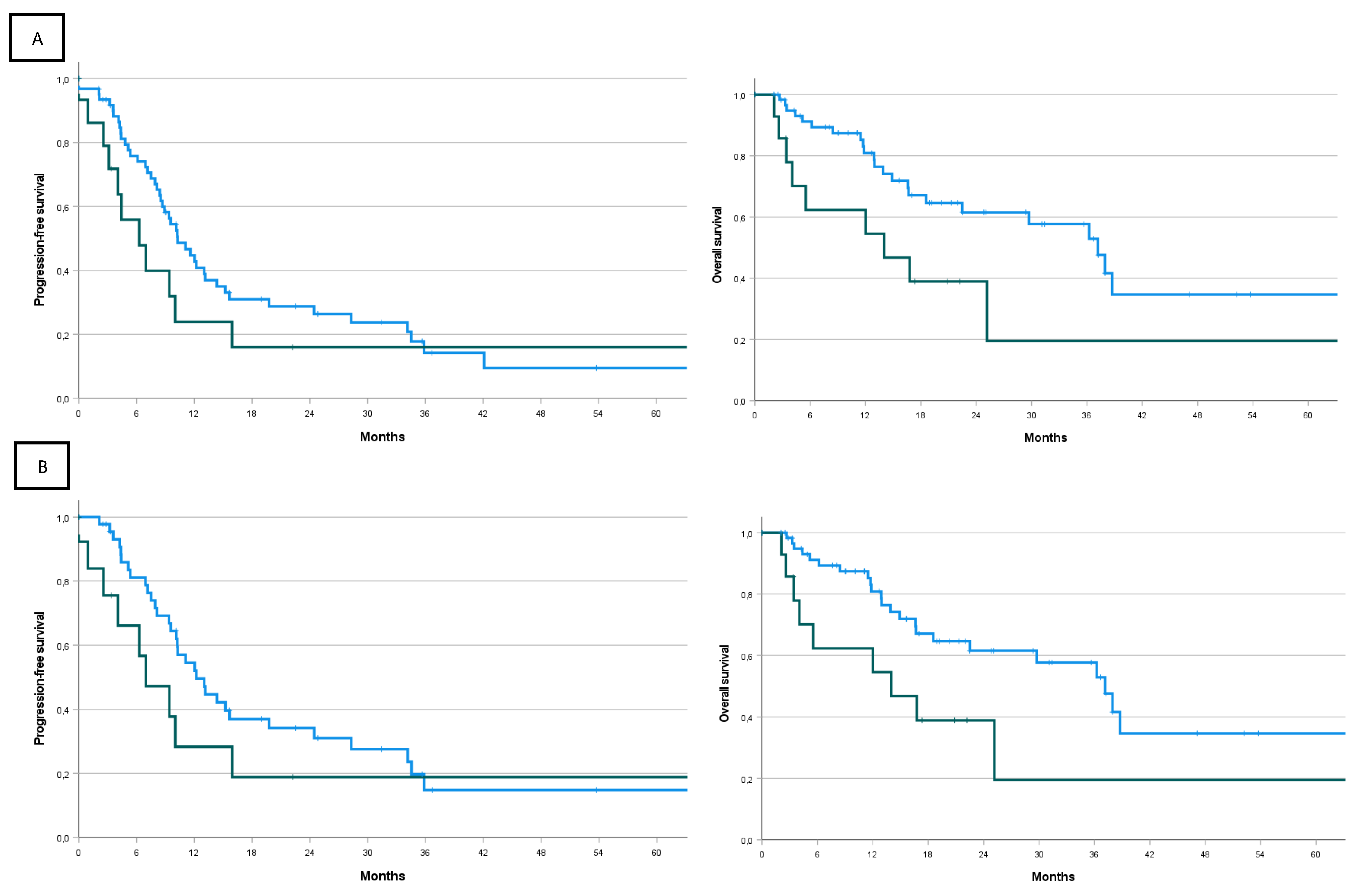

Table 1.
Patients’ characteristics at diagnosis.
| All patients | MSI-l/pMMR patients | MSI-h/dMMR patients | p-value | |
|---|---|---|---|---|
| Center (N. of patients) | 312 | 241/312 (77.2%) | 71/312 (22.8%) | |
| -Mauriziano | 164 (52.6%) | 132 (54.8%) | 32 (45.1%) | |
| -Candiolo | 61 (19.6%) | 44 (18.3%) | 17 (23.9%) | |
| - Reggio Emilia | 55 (17.6%) | 40 (16.6%) | 15 (21.1%) | |
| -Bari | 32 (10.3) | 25 (10.4%) | 7 (9.9%) | |
| Median age at diagnosis(years, CI) | 65.3 (31.5–90.9) | 65.3 (31.5-90.9) | 64.6 (42.4-89.8) | p=0.26 |
| Comorbidities | p=0.66 | |||
| -Yes | 222 (71.2%) | 170 (70.5%) | 52(73.1%) | |
| -No | 90(28.8%) | 71(29.5%) | 19(26.8%) | |
| Diabetes | p=0.57 | |||
| -Yes | 42 (13.5%) | 31 (12.9%) | 11 (15.5%) | |
| -No | 270 (86.5%) | 210 (87.1%) | 60 (84.5%) | |
| Hypertension | p=0.73 | |||
| -Yes | 135 (43.3%) | 103 (42.7%) | 32 (45.1%) | |
| -No | 177 (56.7%) | 138 (57.3%) | 39 (54.9%) | |
| Cardiopathy | p=0.95 | |||
| Yes | 27 (8.7%) | 21 (8.7%) | 6 (8.5%) | |
| No | 285 (91.3%) | 220 (91.3%) | 65(91.5%) | |
| Hystology | p=0.002 | |||
| Endometrioid | 239 (76.6%) | 175 (72.6%) | 64 (90.1%) | |
| Other | 73 (23.4%) | 66 (27.4%) | 7 (9.9%) | |
| FIGO stage at diagnosis | p=0.43 | |||
| I | 151 (48.4%) | 115 (47.7%) | 36 (50.7%) | |
| II | 32 (10.3%) | 23 (9.5%) | 9 (12.7%) | |
| III | 93(29.8%) | 73 (30.3%) | 20 (28.2%) | |
| IV | 33 (10.6%) | 28 (11.6%) | 5 (7.0%) | |
| Missing data | 3 (0.9%) | 2 (0.8%) | 1 (1.4%) |
N= number, MSI-h= high microsatellite instability; dMMR= mismatch repair deficiency; MSI-l= low microsatellite instability; pMMR= mismatch repair proficient; FIGO= International Federation of Gynecology and Obstetrics; CI=confidence interval.
Table 2.
Characteristics of the 278 patients included in the analysis of RFS (data cut off 30/APR/2023).
Table 2.
Characteristics of the 278 patients included in the analysis of RFS (data cut off 30/APR/2023).
| Whole series (N=278) |
MSI-l/pMMR patients (N=212) |
MSI-h/dMMR patients (N=94) |
p value | |
|---|---|---|---|---|
| N. of patients with event (recurrence or death) | 94 (XXX%) | 73/94 (77.6%) | 21/94 (22.3%) | |
| Adjuvant Therapy | p=0.20 | |||
| Yes | 171/278 (61.5%) | 126/212 (54.9%) | 45/66 (68.2%) | |
| No | 107/278 (38.5%) | 86/212 (40.6%) | 21/66 (31.8%) | |
| Radiotherapy | p=0.34 | |||
| Yes | 104/278 (37.4%) | 76/212 (35.8%) | 28/66 (42.4%) | |
| No | 174/278 (62.6%) | 136/212 (64.2%) | 38/66 (57.6%) | |
| Brachitherapy | p=0.34 | |||
| Yes | 96/278 (34.5%) | 70/212 (33.0%) | 26/66 (39.4%) | |
| No | 182/278 (65.5%) | 142/212 (67.0%) | 40/66 (60.6%) | |
| Chemotherapy | p=0.71 | |||
| Yes | 115/278 (41.4%) | 89/212 (42.0%) | 26/66 (39.4%) | |
| No | 163/278 (58.6%) | 123/212 (58.0%) | 40/66 (60.6%) | |
| Hormonotherapy | p=0.21 | |||
| Yes | 5/278 (1.8%) | 5/212 (2.4%) | 0/66 (0%) | |
| No | 273/278 (98.2%) | 207/212 (97.6%) | 66/66 (100%) | |
| RFS Median (months, CI) |
112.6 (78.4 – 146.8) | 100.0 (59.4 – 140.7) | 120.9 (60.0 – 181.8) | p=0.39 |
| Rate at 1 year | 89.3% | 88.0% | 93.2% | |
| Rate at 2 years | 73.1% | 71.7% | 77.4% | |
| Rate at 3 years | 69.2% | 67.2% | 75.2% | |
| Rate at 5 years | 58.8% | 56.9% | 64.6% | |
| Rate at 10 years | 46.0% | 44.5% | 50.7% |
N= number, RFS= recurrence free survival; CI=confidence interval.
Table 3.
Characteristics of the patients (N=77) treated with chemotherapy as first-line treatment for advanced/metastatic disease. N= number; PFS= progression free survival; OS= overall survival; CI=confidence interval; CT= chemotherapy.
Table 3.
Characteristics of the patients (N=77) treated with chemotherapy as first-line treatment for advanced/metastatic disease. N= number; PFS= progression free survival; OS= overall survival; CI=confidence interval; CT= chemotherapy.
| All comers | MSI-l/pMMR patients | MSI-h/dMMR patients | p value | |
|---|---|---|---|---|
| N. of patients | 77 | 62 (80.5%) | 15 (19.5%) | |
| Median age at advanced/metastatic disease (years, CI) | 68.3 (39.8–87.3) | 67.9 (39.8-86.0) | 71.0 (56.8-87.2) | p=0.72 |
| First line CT | ||||
| platinum-based | 59 (76.6%) | 46 (74.2%) | 13 (86.7%) | |
| liposomal doxorubicin | 12/77 (15.6%) | 11/62 (17.4%) | 1/15 (6.7%) | |
| other | 6/77 (6.8%) | 5/62 (8.1%) | 1/15 (6.7%) | |
| PFS (months, CI) | 10.0 (8.51– 11.55) | 10.3 (7.7 – 12.8) | 6.3 (2.0 – 10.6) | p=0.21 |
| Rate at 6 months | 72.0% | 75,8% | 55.8% | |
| Rate at 1 year | 40.8% | 44.7% | 23.9% | |
| Rate at 2 years | 26.3% | 28.8% | 16.0% | |
| Rate at 3 years | 14.3% | 14.2% | 16.0% | |
| Rate at 5 years | 10.7% | 9.5% | 16.0% | |
| OS (months, CI) | 36.3 (20.9-51.6) | 37.2 (28.0 – 46.4) | 14.0 (1.0 – 27.1) | p=0.039 |
| Rate at 6 months | 85.8% | 91.2% | 62.3% | |
| Rate at 1 year | 77.5% | 80.9% | 62.3% | |
| Rate at 2 years | 56.9% | 61.6% | 39.0% | |
| Rate at 3 years | 50.7% | 57.7% | 19.5% | |
| Rate at 5 years | 32.4% | 34.7% | 19.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



