
Submitted:
09 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
Over the last decade, the therapeutic scenario for advanced non-small-cell lung cancer (NSCLC) has undergone a major paradigm shift. Immune checkpoint inhibitors (ICIs) have shown a meaningful clinical and survival improvement in different settings of the disease. However, the real benefit of this therapeutic approach remains controversial in selected NSCLC subsets, such as those of the elderly with active brain metastases or oncogene-addicted mutations. This is mainly due to the exclusion or underrepresentation of these patient subpopulations in most of the pivotal phase III studies; this precludes the generalization of the ICI efficacy in this context. Moreover, no predictive biomarkers of ICI response exist that can help with patient selection for this therapeutic approach. Here, we critically summarize the current state of ICI efficacy in the most common “special” NSCLC subpopulations.
Keywords:
NSCLC
; Immunotherapy
; Immune Checkpoint Inhibitors
; Special populations
Introduction
In the last 15 years, one of the major advances in clinical oncology has been the introduction of immunotherapy (IO) in the treatment of a significant number of cancers, particularly lung cancer.
Since 2013, several randomized trials have shown the superiority of programmed cell death protein (PD)-1/PD-ligand(L)1 immune checkpoint inhibitors (ICIs) in terms of overall survival (OS) in both the first- and second-line treatments of metastatic non-small-cell lung cancer (NSCLC); in addition, several anti-PD1-PD-L1 drugs have become integrant or exclusive components of the treatment strategy of unresectable or metastatic advanced NSCLC [1,2,3,4] .
However, in all the randomized trials of ICIs ± chemotherapy vs. chemotherapy alone, in both first- and second-line treatments, the real clinical benefit in terms of OS at 5 years of follow up has resulted in being limited to a restricted number of patients; this has ranged between 16 and 20% of metastatic stage IV NSCLC patients [5,6]; to date, we do not have consistent reliable biomarkers to identify these patients beyond PD-L1 expression or mutational tumor burden (TMB), both of which present significant insufficiency and heterogeneity. For this reason, IO, in the absence of specific selective biomarkers, has been registered as the preferred treatment for several cancers of different histology, including melanoma, kidney cancer, lung cancer, gastrointestinal cancer, bladder cancer, head and neck cancer, and hepatocellular cancer [7], but despite this very broad label indication, it seems clear that IO is not fit for all comers; this is particularly true with NSCLC.
In several randomized clinical trials, IO has shown a significant clinical benefit in comparison to platinum-based chemotherapy in patients with metastatic NSCLC and PD-L1 expression over 50%; it has also been shown that there is a significant linear correlation in clinical outcome between the PD-L1 tumor proportion score (TPS) and the magnitude of benefit.
The combination of IO and chemotherapy in first-line treatment has been approved as the potential treatment of choice, but a recent FDA pooled analysis of 12 randomized clinical trials (RCTs) in patients with PD-L1 ≥ 50% has shown that first-line IO alone or in combination with chemotherapy yields a similar OS [8]; in the same pooled analysis, IO alone or in combination with chemotherapy or chemotherapy alone provided similar results regardless of the KRAS mutation status [9] .
Moreover, the efficacy of IO in the specific settings of NSCLC patients, in any line of treatment and regardless of biomarker expression, remains to be defined; never smokers, oncogene-addicted cancer patients, and autoimmune or immunosuppressive treatment-dependent patients do not benefit from IO in their significant clinical outcomes. On the basis of these considerations, it is highly relevant to define the role and the limitations of immunotherapy in these specific settings of NSCLC patients and to clarify the real value of IO in the treatment of lung cancer.
IO in never smoker and/or oncogene-addicted NSCLC patients
Since the discovery by Stanley Cohen (Nobel prize, 1986) of the epidermal growth factor receptor (EGFR), a number of studies and clinical trials have developed the paradigm of precision medicine based on targetable genomic alterations. Oncogenic DNA mutations and DNA tumor rearrangements are the basis for the molecular-driven therapy in lung adenocarcinoma. Since 2004, oncogene addiction has been demonstrated in terms of DNA mutations in the EGFR (exon 19-21); B-RAF (V600E); MET (exon 14 skip mutations); intragenic insertions in EGFR and ERB-B2 (exon 20); or fusion rearrangements in ALK, ROS1, RET, NTRK, and NRG1 in patients with lung adenocarcinoma. Proto-oncogenes induce cell proliferation and apoptosis inhibition through the activation of different specific tyrosine kinases (TKs). Therefore, a number of TKI inhibitors have been developed and approved as the preferred treatments for oncogene-addicted lung adenocarcinomas.
TKIs consist of oral small molecules and have shown superiority over chemotherapy in many randomized clinical trials; consequently, they represent the first line of treatment in EGFR, ALK, ROS1, and MET proto-oncogene-driven tumors, with a response rate ranging between 60 and 80% and a clear superiority in PFS and OS [10,11]. However, following years of critical evaluation of the results of TKI-based targeted therapies in all the specific subsets of lung adenocarcinomas, some concerns have been raised: despite their high activity, the complete response rate is usually less than 5%, and almost all the patients soon or later develop resistance to TKIs and experience progressive disease. In oncogene-addicted cancers, there is also a high propensity to develop brain metastases. Furthermore, a significant percentage (10-20%) of patients show primary resistance to TKIs, and patients apparently harboring the same molecular profile show a wide range of variations in performance status (PS) and in clinical phenotype. These two factors indicate the existence of high genomic heterogeneity, as was also suggested by a very different histotype and clinical phenotype inside the apparently identical molecular oncogene addiction. These observations were confirmed and substantiated by the seminal work of the Tracerx Consortium, which showed a large intratumor heterogeneity for somatic mutations, rearrangements, and gene amplifications in a prospective cohort study on the whole-exome sequencing of 100 early stages of resected NSCLC [12] .
This genomic heterogeneity and the chromosomal instability can explain the different clinical outcomes and the variable phenotypes that are present following the same treatment and in the same oncogene addiction. The definition of the genomic heterogeneity of the oncogene-addicted lung adenocarcinomas should be highly relevant in the development of alternative therapies after the failure of first-line TKIs. Currently, platinum-based chemotherapy is the only consistent second-line treatment; however, it is generally inadequate for patients with oncogene-addicted metastatic NSCLC. Immunotherapy seems to work poorly in oncogene-addicted tumors. In all the RCTs comparing IO and chemotherapy as both first- and second-line treatments, the forest plot analysis showed that oncogene addiction, mainly that of EGFR mutations and ALK rearrangements, and the never smoker status represented the variables that were more consistently associated with a chemotherapy benefit than IO [13,14]. The poor activity of IO in these situations can be explained by the absence of smoking exposure in all these cases, considering that the never smoker status accounts for most of the oncogene-addicted tumors. NSCLC in never smokers has long been considered a “different disease” [15], with a lower median age, a slight prevalence in females, widespread clinical dissemination despite good performance status (PS), and the increasing presence of oncogene addiction. In never smokers and in oncogene-addicted tumors, the number of somatic TMBs is lower, and the PD-L1 upregulation, which is often present, has a different biological role [16]. The tumor microenvironment is mostly poorly inflamed and results in a cold immune phenotype, which can explain the modest activity of IO [17].
The ICI treatment in oncogene-driven tumors has consistently yielded poor clinical results, and when combined with TKIs in EGFR, ALK, and ROS1 patients, it has been shown to have highly relevant toxicities, such as intestinal pneumonitis, liver failure, cutaneous dermatitis up to Stevens–Johnson syndrome, and systemic fever [18].
In the IMMUNOTARGET registry, in which data from 24 international institutions are collected, the overall response rate (ORR) to anti-PD-1 agents in 115 EGFR-mutated patients was 12%, and the median progression free survival (mPFS) was only 2.1 months; in the same registry, in 19 ALK-rearranged patients no activity at all was reported after TKI failure, with an mPFS of 2.5 months [15]. In the same study, the patient population harboring MET exon 14 skipping mutations, RET rearrangements, or BRAF mutations, showed modest activity, with an ORR of 16%, 6%, and 24%, and with a poor mPFS of 3.4, 2.1, and 3.1 months, respectively [19].
Furthermore, in a meta-analysis of randomized trials comparing different PD-L1 inhibitors to docetaxel as the control arm in second-line treatment after the failure of platinum-based chemotherapy, the never smoker patients with an activating EGFR mutation did not benefit from immunotherapy (HR: 1.05; 95 CI 0.70-1.55) [20] .
The poor activity of immunotherapy in EGFR-mutant patients has been confirmed in a prospective phase II study, in which pembrolizumab was used as the first-line treatment in EGFR-mutant patients, with PD-L1 TPS>10%. The trial was prematurely closed after enrolling 11 patients because of the lack of activity and the concern about safety that arose with the development of interstitial lung disease (ILD) and two reported deaths in the first 6 months of treatment [21] .
In a recent retrospective study performed at the Memorial Sloan Kettering Cancer Center and the Dana–Farber Cancer Institute, in 147 patients with MET exon 14 skipping alterations, of any stage, the response to pembrolizumab in 24 patients was poor (ORR: 17%), and the PFS was a very short 1.9 months, independently of PD-L1 expression and with a lower TMB in comparison with non-addicted NSCLC [22].
The idea to combine TKIs and IO to improve the outcome of oncogene-addicted patients has brought unexpected safety problems in both the concurrent and the sequential administration of ICIs and TKIs, with different toxicity profiles in EGFR-mutated and ALK-rearranged patients. Indeed, ILD, pneumonitis, liver toxicities, cutaneous erythema, and dermatitis have been reported at an increased rate in different trials of combination treatments with heterogeneous behavior, and most of the trials have been stopped due to the toxicities and lack of activity [23,24].
In daily practice, in addition to clinical trials, the sequential administration of IO and TKIs can occur on the basis of the overexpression of PD-L1 and delayed information regarding NGS mutational status. In this case, the prolonged half-lives of PD-1/PD-L1 inhibitors can induce enhanced toxicity, which can manifest at the beginning of TKI-based treatment [25]. We have reported an exon 19 EGFR-mutated young female, who developed systemic continuous fever, intestinal lung pneumonitis, and severe liver failure with Stevens–Johnson syndrome after sequential administration of ICIs and TKIs. She fully recovered after one month of supportive treatment [26].
In the absence of molecular information, a wise recommendation is to not start immunotherapy in never smokers or former infrequent smokers with high TPS. A lack of activity and unexpected enhanced toxicity has similarly been shown when combining ICIs and anti-ALK TKIs, mainly with liver dose-limiting toxicity for both current and sequential administration [27].
According to these data, immunotherapy seems to have no role in the treatment of oncogene-addicted patients. Recently, however, in EGFR-mutated patients who failed first-line TKIs, a randomized trial has shown a significant PFS and OS benefit with the second-line combination of atezolizumab and carboplatin paclitaxel bevacizumab (PCB) vs. PCB alone (HR: 0.61 in PFS; HR: 0.31 in OS). This finding suggests an important potential interaction between immunotherapy and anti-angiogenesis [28], which may represent an important treatment achievement, with the caveat that it is the result of a post hoc subgroup analysis.
IO in elderly NSCLC patients
Owing to the aging population and the progress in cancer treatment, the aged population with advanced NSCLC is increasing globally [29]. Conventionally, the elderly population includes those aged ≥70 years; around half of all patients with advanced NSCLC are within this population. By using the cutoff of 75 years, these patients represent around one-third of the overall NSCLC population.
In recent years, the concept of elderly has changed from a purely chronological evaluation to a more complex one which also considers the biological age and the functional and social status of the subjects. In this regard, several scales have been developed that can assess specific aspects, including function, comorbidities, quality of life, cognition, and emotional state [30], and a comprehensive geriatric assessment on decision making and treatment allocation is usually included in the multidisciplinary evaluation of elderly NSCLC patients.
The introduction of ICIs in NSCLC patients led to the reconsideration of the treatment paradigm in the elderly subpopulation, who, before the immunotherapy era, were often only candidated to best supportive care due to their ineligibility for chemotherapy.
However, though ICIs have demonstrated a better safety profile compared to chemotherapy, major concerns have been raised about their efficacy in elderly subjects. Indeed, immune senescence has been proposed as a process which favors cancer occurrence in older patients, but it can also limit the efficacy and impair the safety of anticancer treatments [28]. Nowadays, we know that aging may foster many mechanisms that affect the immune system. These include a reduction in the bone marrow functions; a decrease in the size of other organs, such as the thymus, lymph nodes, and spleen; a reduction in the antigenic diversity of immune cells; a decrease in co-stimulatory molecule expression on T lymphocytes; and a reduction in the antibody production in B lymphocytes. Moreover, “inflammaging”, a low-grade chronic inflammation state, is frequent with advanced age, and it is related to the increase in pro-inflammatory cytokines [31,32]. Conversely, Erbe and colleagues found biomarkers within a multi-omics database that were associated with an ICI response (such as TMB, ICI-related gene expression in selected tumors, and more immune-stimulatory signaling TME) and were particularly enriched in tumors from older patients compared to those of their younger counterparts [33]. Moreover, the assumption that ICI therapy has potentially reduced efficacy in the elderly has gradually faded away in the light of the results generated in second-line, randomized clinical studies. Indeed, single-agent anti-PD-1 (nivolumab and pembrolizumab) and anti-PD-L1 (atezolizumab) demonstrated prolonged OS and long-term survival compared with docetaxel in platinum-refractory patients, including the subset of older patients aged more than 65 years. Based on these results, ICI treatment was also firmly established as a further line of treatment in the elderly population. However, in these studies OS was not improved in the restricted cohort of older patients aged more than 75 years; the negative results could possibly have been affected by the small number of patients.
To further support the efficacy of ICIs in elderly patients, a meta-analysis of 17 randomized controlled trials that compared ICIs (nivolumab, pembrolizumab, or atezolizumab) to standard therapy (chemotherapy or targeted therapy) was conducted. The authors found comparable survival outcomes between younger patients and those older than 65 years [34]. A subsequent pooled analysis, including some of those trials, confirmed the same results with regard to the subgroup of patients aged > 75 years. The rates of severe toxicity in this pooled analysis were not different in this age subgroup, but its small number of patients could still have influenced that finding. We should presume that these very old patients were carefully selected according to performance status; thus, they do not really represent the real-life population of NSCLC patients older than 75 years [35]. Nevertheless, in a retrospective Japanese study, the enrolled 131 elderly NSCLC patients (aged ≥ 75 years) receiving a subsequent line of ICI monotherapy achieved an efficacy and safety level similar to that usually observed in younger patients [36].
Soon after, the use of ICIs rapidly moved to the frontline setting of NSCLC treatment. As for the second line, a restriction for age was not planned in the trials on first-line ICIs versus chemotherapy, which included the study of pembrolizumab monotherapy for patients with PD-L1 expression ≥ 50% (Keynote-024); the studies of pembrolizumab plus platinum-based chemotherapy (Keynote-189, Keynote-407); and the study of atezolizumab plus platinum-based chemotherapy and bevacizumab (IMPower150) [1,2,37]. In these trials, the authors described no differences in terms of efficacy when using the cutoff of 65 years of age, but data on patients older than 75 years were not specifically reported.
A real-life study included a larger group of NSCLC patients older than 70 years (N=110), but the number of patients older than 80 years was still small (N=16). Age did not significantly influence either survival or toxicity in the patients receiving first- or second-line ICI-based therapy. The multivariate survival analysis of this study highlighted the performance status and the number of metastatic sites as independent prognostic factors [38].
In a study including three cohorts of NSCLC patients treated with immunotherapy (N=665), high TMB made it possible to predict the durable clinical benefit only in patients aged less than 65 years [39]. This finding suggests that immune senescence processes could limit the neoantigen immunogenicity associated with a high TMB.
Overall, though efficacy was mainly confirmed across the data, some concerns still remain with regard to IO–chemotherapy combinations, especially in octogenarians. In this regard, a panel of experts agreed on the need to expand clinical research with robust real-world studies in the elderly NSCLC patients. Currently, there is an ongoing phase III trial comparing atezolizumab plus carboplatin–paclitaxel vs. carboplatin–paclitaxel specifically in elderly patients (aged 70-89 years) with advanced NSCLC (ClinicalTrial ID: NCT03977194).
IO in poor performance status (PS) patients
The Eastern Cooperative Oncology Group (ECOG) PS is a scale used to estimate the impact of a malignancy on a patient’s daily living abilities, and it helps in the determination of the appropriate treatment and prognosis. It has scores ranging from 0 to 5, where 0 is the best and 5 means that the patient has died.
A poor PS may be induced by tumor burden and/or comorbidities. It is commonly believed that cancer patients with tumor-related poor PS could benefit from treatments which induce a rapid tumor response. If poor PS is mainly caused by comorbidities, therapy cannot change it.
Around one-third of the patients diagnosed with NSCLC have a poor PS (PS: 2–4) [40]. For those patients with metastatic NSCLC and a PS of 3–4 simultaneously, best supportive care is deemed to be the standard of care because of the unfavorable risk–benefit ratio of chemotherapy and a short life expectancy (2–4 months from diagnosis).
Before the advent of targeted therapy and immunotherapy, chemotherapy was allowed for PS 2 patients when less toxic regimens were used [41,42]. The observation of the fast improvement of PS in patients treated with TKIs, also known as the “Lazarus response”, allowed the clinical practice to change. So, the metastatic NSCLC patients with activating oncogene mutations could receive a target therapy irrespective of their PS status [43,44].
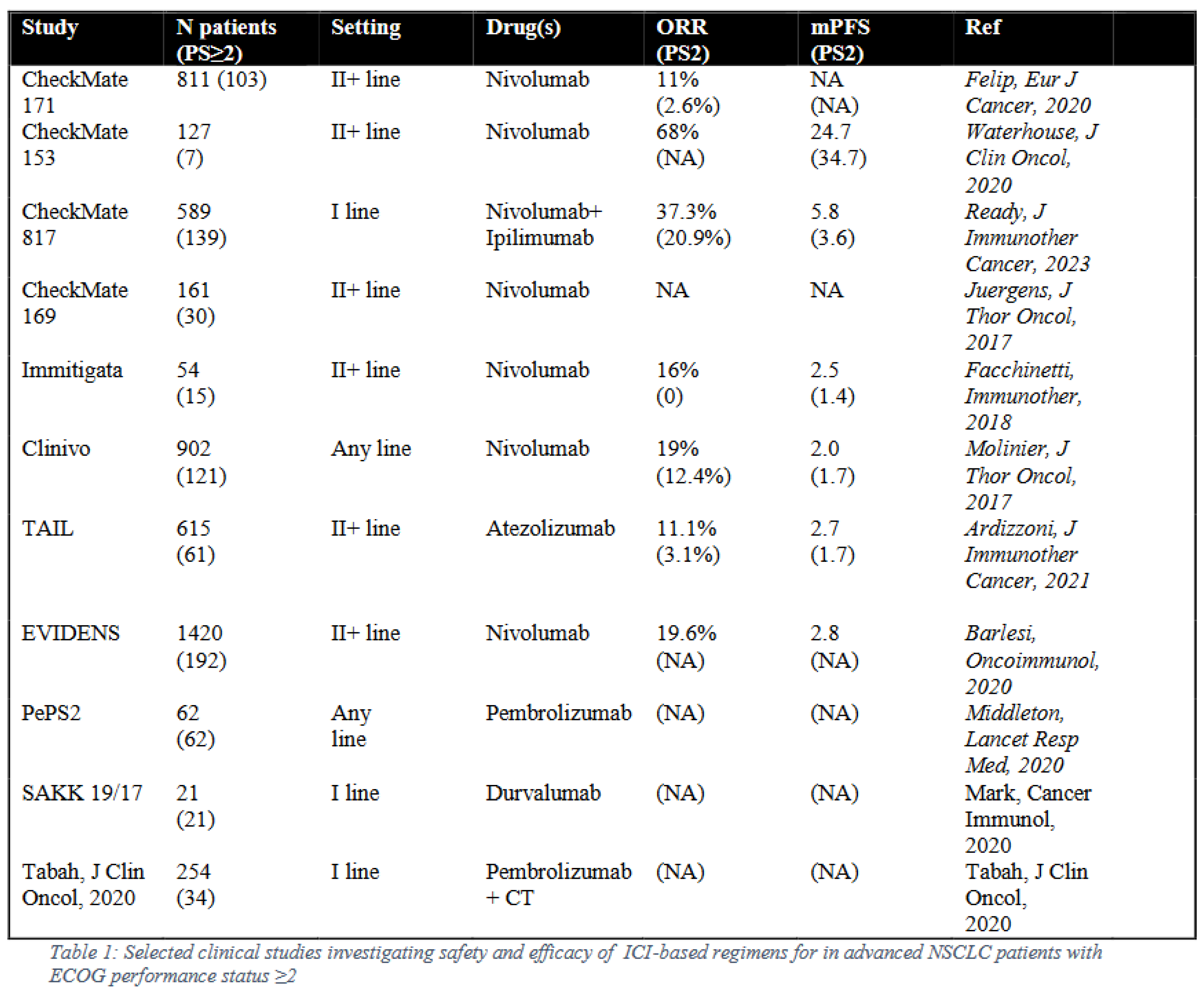
Data on the efficacy of ICIs in NSCLC patients with poor PS are limited and usually come from heterogeneous meta-analyses and small phase II or expanded access trials. Regarding the prospective trials, some studies include PS 2 patients, such as in the PePS2 trial with pembrolizumab, the CheckMate 171 and CheckMate 153 trials with nivolumab, and the CheckMate 817 trial with nivolumab plus ipilimumab [45,46,47,48] (Table 1). The PePS2 trial included only patients with PS 2. In the other trials, PS 2 patients were enrolled together with elderly patients and PS ≤1 patients affected by comorbidities; so, the final results were less specific with regard to the PS 2 patients. However, these trials found grade 3–4 treatment-related adverse events in the PS 2 patients that were similar to those observed in the PS ≤1 patients. Conversely, the OS was worse in the PS 2 patients compared to that of the overall population.
A meta-analysis summarized the outcomes of the retrospective studies of first-line immunotherapy in NSCLC patients with poor PS (PS ≥ 2). In the selected studies, the patients with poor PS showed worse outcomes in comparison to those with good PS. In the group with poor PS, the ORR was 30.9% (vs. 55.2% in the PS ≤1 patients), and the disease control rate (DCR) was 41.5% (vs. 71.5% in the PS ≤1 patients). Similarly, both the PFS and OS were worse in the patients with poor PS in comparison to those with a good PS [49].
The “Lazarus response” was also anecdotally described in patients with very poor PS (PS ≥ 3), who were treated with immunotherapy [50,51]. An initial PS ≥ 3 improved to 0 after only one month of ICI-based therapy, with a follow-up after more than 24 months and a major tumor response. On the basis of these observations, pembrolizumab could be considered a valid option in critically ill patients with advanced NSCLC and PD-L1 expression ≥ 50%.
As PS 2 patients represent a heterogeneous population, the main challenge involves knowing how to identify the patients who can really benefit from ICI treatment. This aim could be reached through the identification of ad hoc predictive biomarkers, such as PD-L1, TMB [52], the lung immune prognostic index, inflammatory markers, LDH, and steroids exposure49, in addition to those already utilized in the clinical practice.
Recently, clinical trials for PS 2 NSCLC patients have been launched and are currently ongoing (ClinicalTrial ID: NCT03620669; Clinical trial ID:NCT04108026).
IO in NSCLC with brain metastases
The occurrence of brain metastases (BM) is relatively frequent in selected solid tumors, such as lung cancer, breast cancer, and melanoma. It is estimated that up to 40% of lung cancer patients will experience metastatic spreading to the central nervous system (CNS) in the course of their disease [53]. Unfortunately, the prognosis and survival of patients with BM remains poor; the presence of extracranial metastases or leptomeningeal disease, primary disease control, age, and performance status represent the most relevant prognostic factors [54]. No treatments have demonstrated real efficacy for non-addicted lung cancer patients with BM in the pre-immunotherapy era; consistently, the therapeutic options are largely palliative and include surgical resection, whole-brain radiation therapy (WBRT), or stereotactic radiosurgery (SRS) [55], though both WBRT and, to a lower degree, SRS have certain limitations, such as radiation neurotoxicity and cognitive deterioration [56,57,58]. In contrast to radiotherapy, chemotherapy is rarely utilized due to its well-known limitation in effectively crossing the blood–brain barrier (BBB), except for in the case of very limited drugs [59]. Due to the lack of effective treatment together with the poorer prognosis, in the last decade the BM patient population has usually been excluded from clinical trials with chemotherapeutic agents, as well as those with immune checkpoint inhibitors (ICIs) [60]. More recently, growing scientific evidence has identified CNS as immunologically distinct rather than as an immune-isolated compartment [61]. The inflammatory TME of BM has been shown to be active in the majority of patients with a dense infiltration of tumor-infiltrating lymphocytes (TILs), which often express immunosuppressive factors such as PD-L1 [62]. This evidence and the availability of effective immunotherapeutic strategies [63,64] targeting CTLA-4, PD-1, and PD-L1 have prompted their use in patients with BM [65], particularly those with negative driver genes [66]. In this regard, Cohen JV et al. suggested that ICIs and active T cells could penetrate the BBB [67], which is necessary for ICIs to work.
Limited data are currently available on the clinical efficacy of ICIs in NSCLC patients with BM. The data generated in this scenario are mostly retrospective; they are real-world data and preferentially generated in pretreated BM.
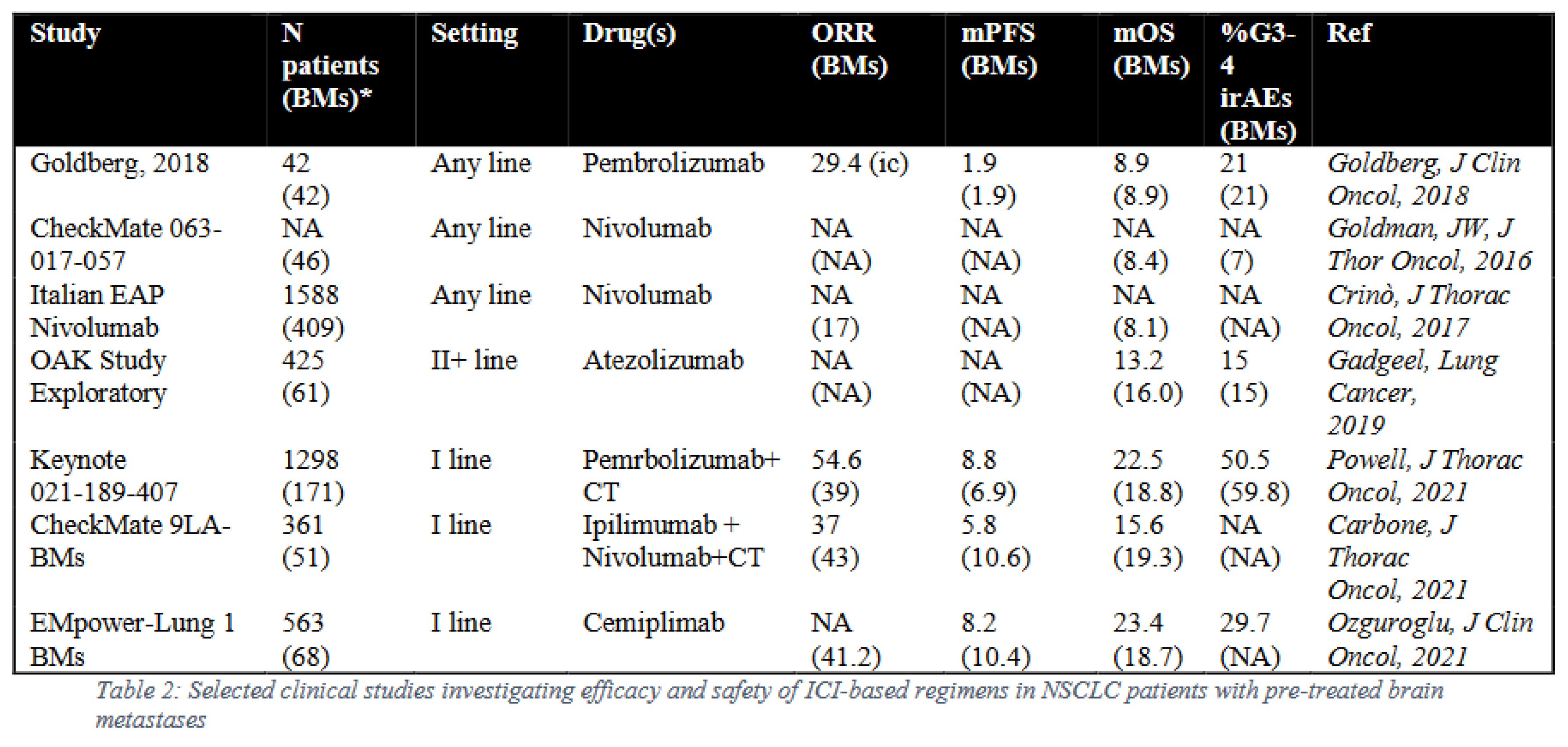
In a prospective phase II trial, pembrolizumab induced an intracranial (ic) ORR in 10 out of 34 (29.4%) PD-L1 positive patients, while no objective responses were observed in the five PD-L1 negative patient subsets [68]. The median OS among all the patients was 8.9 months, and 31% of the patients were alive at 2 years34.
A pooled analysis from the three CheckMate (CM) studies (the phase II CM-063, and the phases III CM-017 and CM-057) explored the role of nivolumab in second-line NSCLC patients with pretreated BM. The results showed an improvement in survival in the patients treated with nivolumab (8.4 months) as compared to those treated with chemotherapy (docetaxel) (6.2 months). Supporting the efficacy of ICIs in this patient population, in the 409 NSCLC patients with BM treated with nivolumab within the Italian expanded access program (EAP), the ORR and DCR were 17% and 40%, respectively [69]. Additionally, in the OAK study, an exploratory analysis performed in a cohort of NSCLC patients with no active BM [70] showed an improvement in survival with atezolizumab compared with docetaxel (16 months versus 11.9 months, respectively). Moreover, atezolizumab led to a prolonged time to the radiologic identification of new symptomatic BM compared with the docetaxel arm [71].
A meta-analysis summarized the outcomes of the three first-line studies (Keynote (KN)-021, KN-189, and KN-407) in the NSCLC patient subpopulation with stable BM compared to those receiving only chemotherapy. Interestingly, the patients who received pembrolizumab alone or combined with chemotherapy received a benefit in terms of mOS (18.8 months vs. 7.6 months, HR 0.48), mPFS (6.9 months vs. 4.1 months, HR 0.44), and ORR (39% vs. 17.7%), regardless of PD-L1 status [72]. Similarly, the results generated in the CM-9LA study showed an improvement in mOS (19.3 vs. 6.8 months), mPFS (10.6 vs. 4.1 months), and ORR (43% vs. 24%) in patients with pretreated BM who had received a platinum-based regimen combined with nivolumab plus ipilimumab compared to those who received only chemotherapy [73]. These results were comparable to the results generated in the IMPower-Lung1 study, in which NSCLC patients with no active BM receiving cemiplimab had a better mPFS compared with those treated with chemotherapy (18.7 months vs. 7.4 months) [74] (Table 2).
Despite these intriguing findings, the efficacy of immunotherapy in BM currently remains controversial due to the limited sample size and long-term efficacy data in the above clinical trials and to the use of various immunotherapy regimens for which there is no comparison of effectiveness.
In order to overcome these limitations, Chu and colleagues [75] performed a comprehensive meta-analysis which included a total of 3160 participants from 46 trials. The results showed an improvement in PFS (HR = 0.48) and OS (HR = 0.64) for the immunotherapy-based regimen compared with non-immunotherapy in NSCLC patients with BM; This was probably due to the well-known synergy between ICIs and chemotherapy and/or radiotherapy. Additionally, no significant differences in PFS (HR = 0.97, 95% CI: 0.40-2.35), OS (HR = 0.69, 95% CI: 0.23-1.15); extracranial overall response rate (odds ratios (OR)= 0.75, 95%CI: 0.28-2.01); intracerebral overall response rate (OR = 1.27, 95%CI: 0.65-2.47); intracerebral disease control rate (OR = 1.52, 95%CI: 0.80-2.91); or extracranial disease control rate (OR= 0.99, 95%CI: 0.26-3.81) were observed between ICIs combined with RT and ICI monotherapy. In this regard, future studies should be addressed toward the investigation of both the sequencing of IO and RT and the optimal interval between ICIs and cranial RT in the treatment of BM from NSCLC, in view of their potential influence on the efficacy of ICIs combined with RT. Indeed, the evidence supports concurrent ICIs combined with RT rather than sequential ICIs combined with RT in terms of a decreased incidence of recurrence. Furthermore, an interval shorter than 2 weeks between ICIs and RT was associated with a longer OS and PFS. Finally, dual ICIs combined with CT or ICIs combined with CT provided a better PFS and OS than ICIs alone.
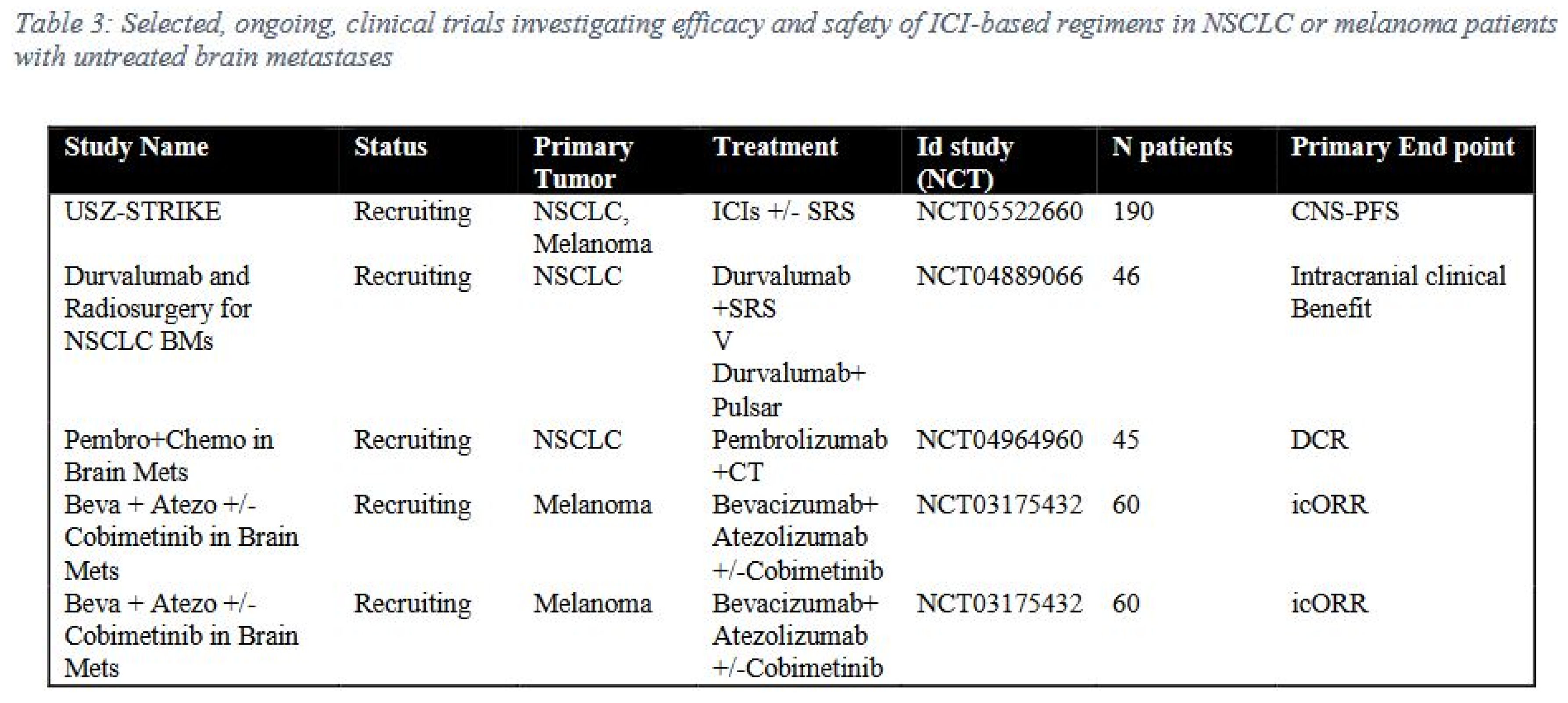
An intriguing, relevant aspect concerns the efficacy of ICIs in NSCLC patients with active BM, for whom limited data are currently available. The data generated in this scenario are mostly retrospective and based on real-world data. However, the evidence shown in metastatic melanoma patients with active BM strongly support the efficacy of ICI treatment, especially in the combination regimen; it has become the new standard of care for metastatic melanoma patients with BM [76,77]. In this regard, and seeking to expand the potential efficacy of ICI treatment in NSCLC patients with active BM, a variety of prospective clinical trials are currently ongoing (Table 3).
An additional major concern is the appropriate evaluation of the radiologic response of brain metastases during treatment with immunotherapy. Indeed, immunotherapy may significantly affect the imaging features of BM as well as the brain parenchyma, hindering a correct neuroradiological interpretation of post-treatment findings. Consistently, atypical responses, such as initial disease progression or the appearance of new lesions followed by a clinical response and pseudo-progression, can be observed in the course of immunotherapy and can be misinterpreted as tumor recurrence or progression [78]. This aspect is also more relevant for patients receiving radiotherapy for BM and immunotherapy. Therefore, it is crucial for neuroradiologists to be more comprehensively familiar with the treatment response criteria and treatment-induced changes in brain lesions [79,80,81]. With the aim of standardizing the radiologic evaluation of BM, novel criteria have been proposed and incorporated into the immunotherapy RANO (iRANO) criteria [82,83], providing recommendations for the interpretation of neuroradiological changes in the course of this therapeutic approach [82]. Moreover, PET-based imaging, especially with amino acid tracers, provides information on tumor metabolism and is currently under investigation with regard to the proper differentiation of neoplastic tissues from non-specific, treatment-related changes [84,85,86,87].
In conclusion, the results of ICI-based treatment in NSCLC patients with BM may soon lead to significant changes in their comprehensive management; thus, the role of surgery and radiotherapy to treat BM may be revisited. Indeed, in selected cases, the ICI-based regimen alone could represent the first, optimal therapeutic choice, though its use requires a careful patient evaluation due to the lack of well-defined selection criteria. Prospective clinical data to corroborate the efficacy of ICI treatment in NSCLC patients with BM are awaited; in the daily practice scenario, a multidisciplinary interaction is mandatory for the optimal management of lung patients with BM and must undoubtedly include a neuroradiologist to support the treating physicians in evaluating clinical response and neurological side effects.
Biomarkers of tumor immunogenicity
Currently, PD-L1 expression is the most studied predictive biomarker of ICIs targeting the PD-1/PD-L1 axis [88]. Metastatic NSCLC patients achieved a better OS benefit from pembrolizumab in comparison to chemotherapy when their tumors expressed PD-L1 ≥ 50% [1]. Some data also highlighted that the higher the PD-L1 expression level, the greater the benefit from anti-PD-1/PD-L1, particularly when used as a monotherapy [89]. Despite these findings, PD-L1 expression has great limitations as a biomarker, given that the benefit from immunotherapy is also observed in those patients bearing PD-L1 negative tumors. For this reason, the research on further biomarkers is ongoing.
TMB represents the total amount of DNA mutation per megabase. Only nonsynonymous tumor mutations are considered. This amount is supposed to be related to the generation of neoantigens that T lymphocytes can recognize as non-self. A higher number of neoantigens could enhance the efficacy of ICI-based therapy. TMB is independent of PD-L1 expression [90]. However, a high TMB is more related to the efficacy of the combination of nivolumab plus ipilimumab in NSCLC patients with negative PD-L1 [91]. Moreover, the combination of the CTLA-4 inhibitor tremelimumab plus the PD-L1 inhibitor durvalumab did not improve OS in comparison with chemotherapy, but a better OS was observed in the patients with a high TMB in the ctDNA; these patients were treated with this combination immunotherapy [92]. In the B-F1RST phase 2 trial, blood-based TMB was evaluated as a predictive biomarker for first-line monotherapy with atezolizumab in advanced NSCLC patients. TMB ≥ 16 was associated with higher tumor responses, which further increased at higher TMB cutoffs. The OS was also better with TMB ≥ 16 in an exploratory analysis of this trial [93]. In a meta-analysis by Ma et al., including almost three thousand patient tumor responses, the PFS and OS were improved in the group of patients with a high TMB in comparison to those with a low TMB [94]. However, the use of TMB as a biomarker is still limited by its heterogeneity across the various NSCLC subtypes and variable detection assays and the lack of cutoff standardization.
Microsatellite instability (MSI) is the genomic consequence of the mismatch repair deficiency (dMMR). Microsatellites are short tandem repeats present throughout the genome. The instantaneous dissociation of the DNA strand during replication can change microsatellite lengths, which should be corrected by the mismatch repair system. MSI severity can be categorized into three groups: microsatellite stable (MSS), MSI low (MSI-L), and MSI high (MSI-H) [95,96]. MSI and dMMR involve high tumor immunogenicity; thus some authors have hypothesized that they have a role as predictive biomarkers for ICI-related outcomes. The combined results of the study on ICI efficacy emerged in MSI-H tumors, irrespective of the tumor types [97]. These findings led the FDA to approve pembrolizumab for the treatment of patients with advanced solid tumors when an MSI-H or dMMR status was present. Prospective randomized studies focused on NSCLC are needed in order to better identify further applications for these biomarkers.
Biomarkers of tumor immune microenvironment
The presence of CD8+ cytotoxic T lymphocytes infiltrating the tumor stroma (TILs) is a requirement for ICI anti-tumor action. Some studies have already shown the favorable prognostic role of TILs in NSCLCs [98,99]. These findings led to the hypothesis that these cells could also represent a predictive biomarker of ICI efficacy [100]. Various approaches were used to address this aim. Among these, RNA sequencing and immunohistochemistry staining of NSCLC samples of patients treated with anti–PD-1 showed that high CD8A and CD274 mRNA expressions were associated with longer PFS [101].
In the KEYNOTE-001 phase I trial, the tumor responses to pembrolizumab were associated with a higher quantity of TILs in the baseline tumor biopsies. For this purpose, the biopsy slices were stained for CD8 [102]. Other authors used multiplexed quantitative immunofluorescence to characterize both PD-L1 expression and TILs and their state of activation; they were also characterized in relation to their mutational status. NSCLC tissues bearing a KRAS mutation were more inflamed because of a greater quantity of active TILs. However, EGFR mutant tumors hosted inactive TILs. Moreover, activated TILs were related to a higher PD-L1 expression only in tumors without EGFR or KRAS mutations [103]. Some authors also used the gene expression signature of CD8+ T lymphocytes in correlation with a radiomic signature for the detection of CD8+ TILs. The aim of this association was an indirect estimation of the presence of TILs through a computed tomography scan to predict the responses to ICI-based therapy [104]. A new technique is under development using CD8 PET imaging with the 89Zr-Df-IAB22M2C radioisotope to visualize the distribution of CD8+ T cells in the whole body or in tumor sites and potentially to predict an early tumor response to immunotherapy [105].4.3.
Biomarkers of host immune system
Currently, a lot of evidence is available regarding systemic inflammation markers in peripheral blood as prognostic or predictive factors, particularly in metastatic NSCLC patients treated with ICI-based therapy. The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were the most studied. These biomarkers are based on the association between tumor development and increased inflammation and can be easily extracted from routine blood tests. So, these markers are usually available worldwide and are highly reproducible with no further costs [106,107]. Many studies on this topic were carried out; then, these studies were summarized in some meta-analyses, which confirmed that NLR and PLR may be considered prognostic factors in metastatic NSCLC patients treated with ICI-based therapy [108,109]. The former, by Tan et al., suggested that high baseline NLR predicted a worse PFS and OS, but this result was not confirmed for PLR. The latter, by Platini et al., found that both biomarkers were prognostic in the same setting.
Peripheral blood inflammatory markers were combined with other parameters to obtain prognostic scores in order to predict outcomes in metastatic NSCLC patients treated with ICIs. These scores included further laboratory variables, e.g., the derived NLR (dNLR), calculated with the formula [neutrophils/leucocytes – neutrophils], lactate dehydrogenase (LDH), albumin, and C-reactive protein, as well as clinical variables, e.g., ECOG PS or tumor stage. Twenty-two combined scores were studied on the basis of baseline values used only for prognosis. Some of these also showed a predictive value for ICI-based therapy in both pretreated patients and in the first-line setting or treatment monitoring [110].
Among these prognostic scores, the lung immune prognostic index (LIPI) was the most studied in metastatic NSCLC patients. It includes two parameters, the dNLR (cutoff: 3) and LDH (cutoff: above the limit of normal). The presence or absence of each factor defines a score for the prognostic stratification, which is categorized into three groups: good LIPI for both factors under the cutoff; intermediate LIPI for one factor above the cutoff; and poor LIPI for both factors above the cutoff [111]. Some subgroup analyses of randomized trials and a pooled analysis including the above prognostic score confirm its prognostic role in patients treated with both ICI and chemotherapy, but not the predictive usefulness [112,113].
The presence or activation of suppressive cells can also limit the efficacy of ICIs. Myeloid-derived suppressor cells (MDSCs) are the most studied and showed a prognostic role both in treatments with chemotherapy and in those with ICIs. MDSCs are immature myeloid cells, which usually increase with tumor progression and are related to systemic chronic inflammation. MDSCs interact with the host immune system through various mechanisms: the inhibition of T cell function via the depletion of some fundamental amino acids in the proliferation of T lymphocytes; the interference of the PD-1/PD-L1 signaling pathway with T cell viability and relative migration; the production of nitric oxide (NO) and reactive oxygen species (ROS), which induces T cell apoptosis; the transition of CD4+ T cells into regulatory T cells (Tregs) via TGF-β; the repolarization of macrophages towards an M2 phenotype; the impairment of natural killer (NK) cell function via direct cell–cell contact; and the reduction in IFN-γ production [114,115,116,117].
MDSCs can be grouped into two subpopulations: polymorphonuclear cells (PMN-MDSCs), characterized by CD11b + CD14- CD15 + or CD11b + CD14-CD66b +, and monocytic cells (M-MDSC), as CD11b + CD14 + HLA-DR-/lowCD15 cells. These surface markers have a great limitation in that they cannot help to distinguish normal monocytes from M-MDSCs and neutrophils from PMN-MDSCs. A unique pattern of markers specific for MDSCs is not currently available [118]. However, these cells have the advantage that they can be studied in the peripheral blood as circulating markers.
A recent meta-analysis highlighted that NSCLC patients with high circulating M-MDSC levels achieved a statistically significant shorter PFS and OS than patients with low levels, irrespective of treatment. The statistical significance was not reached for PMN-MDSCs [119]. Among the 14 studies summarized in this meta-analysis, three considered NSCLC patients treated with immunotherapy and included one study on PMN-MDSCs, one on M-MDSCs, one on both cell subpopulations. The first one achieved a better OS when the circulating PMN-MDSCs were higher [120]. In the second one, the OS was worse, with high circulating M-MDSCs [121]. In the latter, a worse OS was associated with high PMN- and M-MDSCs [122]. Given that these cells could also be targeted through various strategies, the research on MDSCs treated with ICI-based therapy is still ongoing [123].
Conclusions
In the last few years, we have witnessed an impressive therapeutic paradigm shift in NSCLC with the appearance of the IO-based regimen in all clinical settings. However, the role of IO regimens has not been fully established for a significant proportion of patients, particularly elderly patients with cases complicated by BM and/or TKI-resistant driver gene mutations; it remains a challenge to treat these patients. The knowledge on the applicability of immunotherapy in “special” NSCLC populations is mostly derived from studies with other purposes. The various studies discussed in this paper highlight how ICI-based therapy is not precluded in these patients.
A broader understanding of immune and inflammatory responses will fully allow the definition of the real benefit of IO-based treatment in “special” NSCLC populations, as will the ad hoc design of combined/sequential therapies. The availability of predictive/prognostic biomarkers could help to select patients for whom immunotherapy would actually be beneficial rather than those patients belonging to a “special population”. Currently, we have some data on the biomarkers of tumor immunogenicity (i.e., TMB and MSI), the tumor immune microenvironment (i.e., TILs), and the host immune system (i.e., NLR, PLR, LIPI, and MDSCs). Additionally, the identification of validated biomarkers via multi-omics approaches will also be mandatory for the better selection of NSCLC patients for IO therapy.
Contributors
Lucio Crinò and Luana Calabrò contributed equally as the final authors of this work. Giuseppe Bronte, Lucio Crinò, Luana Calabrò, Donato Michele Cosi, and Chiara Magri wrote the text. Giuseppe Bronte, Antonio Frassoldati, Lucio Crinò, and Luana Calabrò revised the text and provided comments. All authors provided comments on the initial version and approved the final draft of the manuscript.
Ethics approval and consent to participate
Not applicable.
Acknowledgments
The work was supported in part by grants awarded to Luana Calabrò from the FONDAZIONE AIRC under 5 per Mille 2018 – ID 21073 program.
Conflicts of Interest
Calabrò L. has served as consultant or advisor to Bristol-Myers Squibb, Merck Sharp and Dohme, and has received compensated educational activities from Bristol Myers Squibb, Astrazeneca, and Sanofi. The other authors declare no relevant conflict of interests.
References
- M. Reck et al., “Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer,” (in eng), N Engl J Med, vol. 375, no. 19, pp. 1823-1833, Nov 10 2016. [CrossRef]
- L. Gandhi et al., “Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer,” (in eng), N Engl J Med, vol. 378, no. 22, pp. 2078-2092, May 31 2018. [CrossRef]
- L. Paz-Ares et al., “Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer,” (in eng), N Engl J Med, vol. 379, no. 21, pp. 2040-2051, Nov 22 2018. [CrossRef]
- H. Borghaei et al., “Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer,” (in eng), N Engl J Med, vol. 373, no. 17, pp. 1627-39, Oct 22 2015. [CrossRef]
- M. C. Garassino et al., “Keynote-189 5-year update: First line pembrolizumab+pemetrexed and platinum vs placebo+pemetrexed and platinum for metastatic non squamous non-small-cell lung cancer “ vol. 33(sup) ed. Ann.Oncol., 2022.
- S. Novello et al., “Pembrolizumab Plus Chemotherapy in Squamous Non-Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study,” (in eng), J Clin Oncol, p. Jco2201990, Feb 3 2023. [CrossRef]
- R. Falcone et al., “Oncologic Drugs Approval in Europe for Solid Tumors: Overview of the Last 6 Years,” (in eng), Cancers (Basel), vol. 14, no. 4, Feb 11 2022. [CrossRef]
- O. Akinboro et al., “Outcomes of anti-PD-(L1) therapy in combination with chemotherapy versus immunotherapy (IO) alone for first-line (1L) treatment of advanced non-small cell lung cancer (NSCLC) with PD-L1 score 1-49%: FDA pooled analysis,” Journal of Clinical Oncology, vol. 39, pp. 9001-9001, 2021. [CrossRef]
- E. C. Nakajima et al., “Outcomes of first-line immune checkpoint inhibitors with or without chemotherapy according to KRAS mutational status and PD-L1 expression in patients with advanced NSCLC: FDA pooled analysis,” Journal of Clinical Oncology, vol. 40, no. 16_suppl, pp. 9001-9001, 2022. [CrossRef]
- R. Rosell et al., “Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial,” (in eng), Lancet Oncol, vol. 13, no. 3, pp. 239-46, Mar 2012. [CrossRef]
- D. Cortinovis, M. Abbate, P. Bidoli, S. Capici, and S. Canova, “Targeted therapies and immunotherapy in non-small-cell lung cancer,” (in eng), Ecancermedicalscience, vol. 10, p. 648, 2016. [CrossRef]
- M. Jamal-Hanjani et al., “Tracking the Evolution of Non-Small-Cell Lung Cancer,” (in eng), N Engl J Med, vol. 376, no. 22, pp. 2109-2121, Jun 1 2017. [CrossRef]
- R. S. Herbst et al., “Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial,” (in eng), Lancet, vol. 387, no. 10027, pp. 1540-1550, Apr 9 2016. [CrossRef]
- S. Sun, J. H. Schiller, and A. F. Gazdar, “Lung cancer in never smokers--a different disease,” (in eng), Nat Rev Cancer, vol. 7, no. 10, pp. 778-90, Oct 2007. [CrossRef]
- J. Mazieres et al., “Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry,” (in eng), Ann Oncol, vol. 30, no. 8, pp. 1321-1328, Aug 1 2019. [CrossRef]
- E. Smolle, K. Leithner, and H. Olschewski, “Oncogene addiction and tumor mutational burden in non-small-cell lung cancer: Clinical significance and limitations,” (in eng), Thorac Cancer, vol. 11, no. 2, pp. 205-215, Feb 2020. [CrossRef]
- G. Wang et al., “Impacts of Cigarette Smoking on the Tumor Immune Microenvironment in Esophageal Squamous Cell Carcinoma,” (in eng), J Cancer, vol. 13, no. 2, pp. 413-425, 2022. [CrossRef]
- A. Somasundaram, M. A. Socinski, and L. C. Villaruz, “Immune Checkpoint Blockade in Oncogene-Driven Non-Small-Cell Lung Cancer,” (in eng), Drugs, vol. 80, no. 9, pp. 883-892, Jun 2020. [CrossRef]
- C. K. Lee et al., “Clinical and Molecular Characteristics Associated With Survival Among Patients Treated With Checkpoint Inhibitors for Advanced Non-Small Cell Lung Carcinoma: A Systematic Review and Meta-analysis,” (in eng), JAMA Oncol, vol. 4, no. 2, pp. 210-216, Feb 1 2018. [CrossRef]
- A. Lisberg et al., “A Phase II Study of Pembrolizumab in EGFR-Mutant, PD-L1+, Tyrosine Kinase Inhibitor Naïve Patients With Advanced NSCLC,” (in eng), J Thorac Oncol, vol. 13, no. 8, pp. 1138-1145, Aug 2018. [CrossRef]
- J. K. Sabari et al., “PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers,” (in eng), Ann Oncol, vol. 29, no. 10, pp. 2085-2091, Oct 1 2018. [CrossRef]
- G. R. Oxnard et al., “TATTON: A multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer,” (in eng), Ann Oncol, vol. 31, no. 4, pp. 507-516, Apr 2020. [CrossRef]
- J. C. Yang et al., “Osimertinib Plus Durvalumab versus Osimertinib Monotherapy in EGFR T790M-Positive NSCLC following Previous EGFR TKI Therapy: CAURAL Brief Report,” (in eng), J Thorac Oncol, vol. 14, no. 5, pp. 933-939, May 2019. [CrossRef]
- A. J. Schoenfeld et al., “Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib,” (in eng), Ann Oncol, vol. 30, no. 5, pp. 839-844, May 1 2019. [CrossRef]
- C. Gianni et al., “Case Report: Stevens-Johnson Syndrome and Hepatotoxicity Induced by Osimertinib Sequential to Pembrolizumab in a Patient With EGFR-Mutated Lung Adenocarcinoma,” in Front Pharmacol, vol. 12. Switzerland: Copyright © 2021 Gianni, Bronte, Delmonte, Burgio, Andrikou, Monti, Menna, Frassineti and Crinò., 2021, p. 672233.
- J. J. Lin et al., “Increased Hepatotoxicity Associated with Sequential Immune Checkpoint Inhibitor and Crizotinib Therapy in Patients with Non-Small Cell Lung Cancer,” (in eng), J Thorac Oncol, vol. 14, no. 1, pp. 135-140, Jan 2019. [CrossRef]
- M. Reck et al., “Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): Key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial,” (in eng), Lancet Respir Med, vol. 7, no. 5, pp. 387-401, May 2019. [CrossRef]
- R. Ferrara, L. Mezquita, E. Auclin, N. Chaput, and B. Besse, “Immunosenescence and immunecheckpoint inhibitors in non-small cell lung cancer patients: Does age really matter?,” (in eng), Cancer Treat Rev, vol. 60, pp. 60-68, Nov 2017. [CrossRef]
- K. D. Miller et al., “Cancer treatment and survivorship statistics, 2022,” (in eng), CA Cancer J Clin, vol. 72, no. 5, pp. 409-436, Sep 2022. [CrossRef]
- S. Zuccarino et al., “Exploring Cost-Effectiveness of the Comprehensive Geriatric Assessment in Geriatric Oncology: A Narrative Review,” (in eng), Cancers (Basel), vol. 14, no. 13, Jun 30 2022. [CrossRef]
- J. E. Rodriguez et al., “Immunosenescence, inflammaging, and cancer immunotherapy efficacy,” (in eng), Expert Rev Anticancer Ther, vol. 22, no. 9, pp. 915-926, Sep 2022. [CrossRef]
- J. Serrano-López and B. Martín-Antonio, “Inflammaging, an Imbalanced Immune Response That Needs to Be Restored for Cancer Prevention and Treatment in the Elderly,” (in eng), Cells, vol. 10, no. 10, Sep 28 2021. [CrossRef]
- R. Erbe et al., “Evaluating the impact of age on immune checkpoint therapy biomarkers,” (in eng), Cell Rep, vol. 36, no. 8, p. 109599, Aug 24 2021. [CrossRef]
- R. Elias, A. Giobbie-Hurder, N. J. McCleary, P. Ott, F. S. Hodi, and O. Rahma, “Efficacy of PD-1 & PD-L1 inhibitors in older adults: A meta-analysis,” (in eng), J Immunother Cancer, vol. 6, no. 1, p. 26, Apr 4 2018. [CrossRef]
- S. Marur et al., “FDA analyses of survival in older adults with metastatic non-small cell lung cancer in controlled trials of PD-1/PD-L1 blocking antibodies,” (in eng), Semin Oncol, vol. 45, no. 4, pp. 220-225, Aug 2018. [CrossRef]
- O. Yamaguchi et al., “Efficacy and safety of immune checkpoint inhibitor monotherapy in pretreated elderly patients with non-small cell lung cancer,” (in eng), Cancer Chemother Pharmacol, vol. 85, no. 4, pp. 761-771, Apr 2020. [CrossRef]
- M. A. Socinski et al., “Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC,” (in eng), N Engl J Med, vol. 378, no. 24, pp. 2288-2301, Jun 14 2018. [CrossRef]
- G. Galli et al., “Efficacy and safety of immunotherapy in elderly patients with non-small cell lung cancer,” (in eng), Lung Cancer, vol. 137, pp. 38-42, Nov 2019. [CrossRef]
- Y. Wu, J. Xu, Y. Wang, L. Wang, W. Lv, and J. Hu, “The predictive value of tumor mutation burden for immune checkpoint inhibitors therapy in non-small cell lung cancer is affected by patients’ age,” (in eng), Biomark Res, vol. 8, p. 9, 2020. [CrossRef]
- R. C. Lilenbaum, J. Cashy, T. A. Hensing, S. Young, and D. Cella, “Prevalence of poor performance status in lung cancer patients: Implications for research,” (in eng), J Thorac Oncol, vol. 3, no. 2, pp. 125-9, Feb 2008. [CrossRef]
- G. Bronte et al., “What can platinum offer yet in the treatment of PS2 NSCLC patients? A systematic review and meta-analysis,” (in eng), Crit Rev Oncol Hematol, vol. 95, no. 3, pp. 306-17, Sep 2015. [CrossRef]
- G. L. Banna et al., “Oral Metronomic Vinorelbine in Advanced Non-small Cell Lung Cancer Patients Unfit for Chemotherapy,” (in eng), Anticancer Res, vol. 38, no. 6, pp. 3689-3697, Jun 2018. [CrossRef]
- A. Inoue et al., “First-line gefitinib for patients with advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutations without indication for chemotherapy,” (in eng), J Clin Oncol, vol. 27, no. 9, pp. 1394-400, Mar 20 2009. [CrossRef]
- E. Iwama et al., “Alectinib for Patients with ALK Rearrangement-Positive Non-Small Cell Lung Cancer and a Poor Performance Status (Lung Oncology Group in Kyushu 1401),” (in eng), J Thorac Oncol, vol. 12, no. 7, pp. 1161-1166, Jul 2017. [CrossRef]
- E. Felip et al., “CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations,” (in eng), Eur J Cancer, vol. 127, pp. 160-172, Mar 2020. [CrossRef]
- G. Middleton et al., “Pembrolizumab in patients with non-small-cell lung cancer of performance status 2 (PePS2): A single arm, phase 2 trial,” (in eng), Lancet Respir Med, vol. 8, no. 9, pp. 895-904, Sep 2020. [CrossRef]
- D. R. Spigel et al., “Safety, Efficacy, and Patient-Reported Health-Related Quality of Life and Symptom Burden with Nivolumab in Patients with Advanced Non-Small Cell Lung Cancer, Including Patients Aged 70 Years or Older or with Poor Performance Status (CheckMate 153),” (in eng), J Thorac Oncol, vol. 14, no. 9, pp. 1628-1639, Sep 2019. [CrossRef]
- F. Barlesi et al., “OA04.02 CheckMate 817: First-Line Nivolumab + Ipilimumab in Patients with ECOG PS 2 and Other Special Populations with Advanced NSCLC,” Journal of Thoracic Oncology, vol. 14, no. 10, pp. S214-S215, 2019. [CrossRef]
- F. Facchinetti, M. Di Maio, F. Perrone, and M. Tiseo, “First-line immunotherapy in non-small cell lung cancer patients with poor performance status: A systematic review and meta-analysis,” (in eng), Transl Lung Cancer Res, vol. 10, no. 6, pp. 2917-2936, Jun 2021. [CrossRef]
- J. Pluvy et al., “Lazarus syndrome in nonsmall cell lung cancer patients with poor performance status and major leukocytosis following nivolumab treatment,” (in eng), Eur Respir J, vol. 50, no. 1, Jul 2017. [CrossRef]
- E. M. McLoughlin et al., “Rapid Response to Pembrolizumab in a Critically Ill Mechanically Ventilated Patient with New Diagnosis of NSCLC,” (in eng), J Thorac Oncol, vol. 14, no. 9, pp. e193-e195, Sep 2019. [CrossRef]
- R. Veluswamy et al., “Immunotherapy Outcomes in Individuals With Non-Small Cell Lung Cancer and Poor Performance Status,” (in eng), JNCI Cancer Spectr, vol. 6, no. 2, Mar 2 2022. [CrossRef]
- D. N. Cagney et al., “Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study,” (in eng), Neuro Oncol, vol. 19, no. 11, pp. 1511-1521, Oct 19 2017. [CrossRef]
- A. S. Achrol et al., “Brain metastases,” (in eng), Nat Rev Dis Primers, vol. 5, no. 1, p. 5, Jan 17 2019. [CrossRef]
- M. C. Chamberlain, C. S. Baik, V. K. Gadi, S. Bhatia, and L. Q. Chow, “Systemic therapy of brain metastases: Non-small cell lung cancer, breast cancer, and melanoma,” (in eng), Neuro Oncol, vol. 19, no. 1, pp. i1-i24, Jan 2017. [CrossRef]
- R. A. Patchell et al., “A randomized trial of surgery in the treatment of single metastases to the brain,” (in eng), N Engl J Med, vol. 322, no. 8, pp. 494-500, Feb 22 1990. [CrossRef]
- J. P. Sheehan, M. H. Sun, D. Kondziolka, J. Flickinger, and L. D. Lunsford, “Radiosurgery for non-small cell lung carcinoma metastatic to the brain: Long-term outcomes and prognostic factors influencing patient survival time and local tumor control,” (in eng), J Neurosurg, vol. 97, no. 6, pp. 1276-81, Dec 2002. [CrossRef]
- W. A. Castrucci and J. P. Knisely, “An update on the treatment of CNS metastases in small cell lung cancer,” (in eng), Cancer J, vol. 14, no. 3, pp. 138-46, May-Jun 2008. [CrossRef]
- Q. T. Ostrom, C. H. Wright, and J. S. Barnholtz-Sloan, “Brain metastases: Epidemiology,” (in eng), Handb Clin Neurol, vol. 149, pp. 27-42, 2018. [CrossRef]
- H. L. Kaufman et al., “The promise of Immuno-oncology: Implications for defining the value of cancer treatment,” (in eng), J Immunother Cancer, vol. 7, no. 1, p. 129, May 17 2019. [CrossRef]
- D. F. Quail and J. A. Joyce, “The Microenvironmental Landscape of Brain Tumors,” (in eng), Cancer Cell, vol. 31, no. 3, pp. 326-341, Mar 13 2017. [CrossRef]
- A. S. Berghoff, V. A. Venur, M. Preusser, and M. S. Ahluwalia, “Immune Checkpoint Inhibitors in Brain Metastases: From Biology to Treatment,” (in eng), Am Soc Clin Oncol Educ Book, vol. 35, pp. e116-22, 2016. [CrossRef]
- Rotte, “Combination of CTLA-4 and PD-1 blockers for treatment of cancer,” (in eng), J Exp Clin Cancer Res, vol. 38, no. 1, p. 255, Jun 13 2019. [CrossRef]
- A. C. Tan, A. B. Heimberger, A. M. Menzies, N. Pavlakis, and M. Khasraw, “Immune Checkpoint Inhibitors for Brain Metastases,” (in eng), Curr Oncol Rep, vol. 19, no. 6, p. 38, Jun 2017. [CrossRef]
- X. Wang, G. Guo, H. Guan, Y. Yu, J. Lu, and J. Yu, “Challenges and potential of PD-1/PD-L1 checkpoint blockade immunotherapy for glioblastoma,” (in eng), J Exp Clin Cancer Res, vol. 38, no. 1, p. 87, Feb 18 2019. [CrossRef]
- J. C. Soria, A. Marabelle, J. R. Brahmer, and S. Gettinger, “Immune checkpoint modulation for non-small cell lung cancer,” in Clin Cancer Res, vol. 21, no. 10). United States: ©2015 American Association for Cancer Research., 2015, pp. 2256-62.
- J. V. Cohen and H. M. Kluger, “Systemic Immunotherapy for the Treatment of Brain Metastases,” (in eng), Front Oncol, vol. 6, p. 49, 2016. [CrossRef]
- S. B. Goldberg et al., “Pembrolizumab for management of patients with NSCLC and brain metastases: Long-term results and biomarker analysis from a non-randomised, open-label, phase 2 trial,” (in eng), Lancet Oncol, vol. 21, no. 5, pp. 655-663, May 2020. [CrossRef]
- L. Crinò et al., “Nivolumab and brain metastases in patients with advanced non-squamous non-small cell lung cancer,” (in eng), Lung Cancer, vol. 129, pp. 35-40, Mar 2019. [CrossRef]
- A. Rittmeyer et al., “Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial,” (in eng), Lancet, vol. 389, no. 10066, pp. 255-265, Jan 21 2017. [CrossRef]
- S. M. Gadgeel et al., “Atezolizumab in patients with advanced non-small cell lung cancer and history of asymptomatic, treated brain metastases: Exploratory analyses of the phase III OAK study,” (in eng), Lung Cancer, vol. 128, pp. 105-112, Feb 2019. [CrossRef]
- S. F. Powell et al., “Outcomes With Pembrolizumab Plus Platinum-Based Chemotherapy for Patients With NSCLC and Stable Brain Metastases: Pooled Analysis of KEYNOTE-021, -189, and -407,” (in eng), J Thorac Oncol, vol. 16, no. 11, pp. 1883-1892, Nov 2021. [CrossRef]
- M. Reck et al., “First-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update,” (in eng), ESMO Open, vol. 6, no. 5, p. 100273, Oct 2021. [CrossRef]
- A. Sezer et al., “Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial,” (in eng), Lancet, vol. 397, no. 10274, pp. 592-604, Feb 13 2021. [CrossRef]
- X. Chu et al., “The Long-Term and Short-Term Efficacy of Immunotherapy in Non-Small Cell Lung Cancer Patients With Brain Metastases: A Systematic Review and Meta-Analysis,” (in eng), Front Immunol, vol. 13, p. 875488, 2022. [CrossRef]
- A. M. Di Giacomo et al., “Immunotherapy of brain metastases: Breaking a “dogma”,” (in eng), J Exp Clin Cancer Res, vol. 38, no. 1, p. 419, Oct 17 2019. [CrossRef]
- A. M. Di Giacomo et al., “Primary Analysis and 4-Year Follow-Up of the Phase III NIBIT-M2 Trial in Melanoma Patients With Brain Metastases,” (in eng), Clin Cancer Res, vol. 27, no. 17, pp. 4737-4745, Sep 1 2021. [CrossRef]
- N. Galldiks et al., “Imaging challenges of immunotherapy and targeted therapy in patients with brain metastases: Response, progression, and pseudoprogression,” (in eng), Neuro Oncol, vol. 22, no. 1, pp. 17-30, Jan 11 2020. [CrossRef]
- A. T. Kessler and A. A. Bhatt, “Brain tumour post-treatment imaging and treatment-related complications,” (in eng), Insights Imaging, vol. 9, no. 6, pp. 1057-1075, Dec 2018. [CrossRef]
- M. Nowosielski and A. Radbruch, “The emerging role of advanced neuroimaging techniques for brain metastases,” (in eng), Chin Clin Oncol, vol. 4, no. 2, p. 23, Jun 2015. [CrossRef]
- J. E. Villanueva-Meyer, M. C. Mabray, and S. Cha, “Current Clinical Brain Tumor Imaging,” (in eng), Neurosurgery, vol. 81, no. 3, pp. 397-415, Sep 1 2017. [CrossRef]
- H. Okada et al., “Immunotherapy response assessment in neuro-oncology: A report of the RANO working group,” (in eng), Lancet Oncol, vol. 16, no. 15, pp. e534-e542, Nov 2015. [CrossRef]
- M. Chamberlain et al., “Leptomeningeal metastases: A RANO proposal for response criteria,” (in eng), Neuro Oncol, vol. 19, no. 4, pp. 484-492, Apr 1 2017. [CrossRef]
- N. L. Albert et al., “Response Assessment in Neuro-Oncology working group and European Association for Neuro-Oncology recommendations for the clinical use of PET imaging in gliomas,” (in eng), Neuro Oncol, vol. 18, no. 9, pp. 1199-208, Sep 2016. [CrossRef]
- S. Kebir et al., “Dynamic O-(2-[18F]fluoroethyl)-L-tyrosine PET imaging for the detection of checkpoint inhibitor-related pseudoprogression in melanoma brain metastases,” in Neuro Oncol, vol. 18, no. 10). England, 2016, pp. 1462-4. [CrossRef]
- K. J. Langen, N. Galldiks, E. Hattingen, and N. J. Shah, “Advances in neuro-oncology imaging,” (in eng), Nat Rev Neurol, vol. 13, no. 5, pp. 279-289, May 2017. [CrossRef]
- A. Dimitrakopoulou-Strauss, “Monitoring of patients with metastatic melanoma treated with immune checkpoint inhibitors using PET-CT,” (in eng), Cancer Immunol Immunother, vol. 68, no. 5, pp. 813-822, May 2019. [CrossRef]
- A. Salmaninejad et al., “PD-1/PD-L1 pathway: Basic biology and role in cancer immunotherapy,” (in eng), J Cell Physiol, vol. 234, no. 10, pp. 16824-16837, Aug 2019. [CrossRef]
- K. Nosaki et al., “Safety and efficacy of pembrolizumab monotherapy in elderly patients with PD-L1-positive advanced non-small-cell lung cancer: Pooled analysis from the KEYNOTE-010, KEYNOTE-024, and KEYNOTE-042 studies,” (in eng), Lung Cancer, vol. 135, pp. 188-195, Sep 2019. [CrossRef]
- M. D. Hellmann et al., “Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden,” (in eng), N Engl J Med, vol. 378, no. 22, pp. 2093-2104, May 31 2018. [CrossRef]
- M. Reck et al., “Nivolumab plus ipilimumab versus chemotherapy as first-line treatment in advanced non-small-cell lung cancer with high tumour mutational burden: Patient-reported outcomes results from the randomised, open-label, phase III CheckMate 227 trial,” (in eng), Eur J Cancer, vol. 116, pp. 137-147, Jul 2019. [CrossRef]
- N. A. Rizvi et al., “Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial,” (in eng), JAMA Oncol, vol. 6, no. 5, pp. 661-674, May 1 2020. [CrossRef]
- E. S. Kim et al., “Blood-based tumor mutational burden as a biomarker for atezolizumab in non-small cell lung cancer: The phase 2 B-F1RST trial,” (in eng), Nat Med, vol. 28, no. 5, pp. 939-945, May 2022. [CrossRef]
- X. Ma, Y. Zhang, S. Wang, and J. Yu, “Predictive value of tumor mutation burden (TMB) with targeted next-generation sequencing in immunocheckpoint inhibitors for non-small cell lung cancer (NSCLC),” (in eng), J Cancer, vol. 12, no. 2, pp. 584-594, 2021. [CrossRef]
- H. Ellegren, “Microsatellites: Simple sequences with complex evolution,” (in eng), Nat Rev Genet, vol. 5, no. 6, pp. 435-45, Jun 2004. [CrossRef]
- K. Imai and H. Yamamoto, “Carcinogenesis and microsatellite instability: The interrelationship between genetics and epigenetics,” (in eng), Carcinogenesis, vol. 29, no. 4, pp. 673-80, Apr 2008. [CrossRef]
- D. T. Le et al., “Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade,” (in eng), Science, vol. 357, no. 6349, pp. 409-413, Jul 28 2017. [CrossRef]
- Y. Geng et al., “Prognostic Role of Tumor-Infiltrating Lymphocytes in Lung Cancer: A Meta-Analysis,” (in eng), Cell Physiol Biochem, vol. 37, no. 4, pp. 1560-71, 2015. [CrossRef]
- D. Q. Zeng et al., “Prognostic and predictive value of tumor-infiltrating lymphocytes for clinical therapeutic research in patients with non-small cell lung cancer,” (in eng), Oncotarget, vol. 7, no. 12, pp. 13765-81, Mar 22 2016. [CrossRef]
- Z. Y. Dong et al., “Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma,” (in eng), Clin Cancer Res, vol. 23, no. 12, pp. 3012-3024, Jun 15 2017. [CrossRef]
- J. D. Fumet et al., “Prognostic and predictive role of CD8 and PD-L1 determination in lung tumor tissue of patients under anti-PD-1 therapy,” (in eng), Br J Cancer, vol. 119, no. 8, pp. 950-960, Oct 2018. [CrossRef]
- P. C. Tumeh et al., “Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC,” (in eng), Cancer Immunol Res, vol. 5, no. 5, pp. 417-424, May 2017. [CrossRef]
- M. I. Toki et al., “Immune Marker Profiling and Programmed Death Ligand 1 Expression Across NSCLC Mutations,” (in eng), J Thorac Oncol, vol. 13, no. 12, pp. 1884-1896, Dec 2018. [CrossRef]
- R. Sun et al., “A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: An imaging biomarker, retrospective multicohort study,” (in eng), Lancet Oncol, vol. 19, no. 9, pp. 1180-1191, Sep 2018. [CrossRef]
- M. D. Farwell et al., “CD8-Targeted PET Imaging of Tumor-Infiltrating T Cells in Patients with Cancer: A Phase I First-in-Humans Study of (89)Zr-Df-IAB22M2C, a Radiolabeled Anti-CD8 Minibody,” (in eng), J Nucl Med, vol. 63, no. 5, pp. 720-726, May 2022. [CrossRef]
- W. M. Brueckl, J. H. Ficker, and G. Zeitler, “Clinically relevant prognostic and predictive markers for immune-checkpoint-inhibitor (ICI) therapy in non-small cell lung cancer (NSCLC),” (in eng), BMC Cancer, vol. 20, no. 1, p. 1185, Dec 3 2020. [CrossRef]
- Y. Katayama et al., “Significance of inflammatory indexes in atezolizumab monotherapy outcomes in previously treated non-small-cell lung cancer patients,” (in eng), Sci Rep, vol. 10, no. 1, p. 17495, Oct 15 2020. [CrossRef]
- Q. Tan, S. Liu, C. Liang, X. Han, and Y. Shi, “Pretreatment hematological markers predict clinical outcome in cancer patients receiving immune checkpoint inhibitors: A meta-analysis,” (in eng), Thorac Cancer, vol. 9, no. 10, pp. 1220-1230, Oct 2018. [CrossRef]
- H. Platini et al., “Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Prognostic Markers for Advanced Non-Small-Cell Lung Cancer Treated with Immunotherapy: A Systematic Review and Meta-Analysis,” (in eng), Medicina (Kaunas), vol. 58, no. 8, Aug 8 2022. [CrossRef]
- S. E. Rebuzzi et al., “Prognostic scores including peripheral blood-derived inflammatory indices in patients with advanced non-small-cell lung cancer treated with immune checkpoint inhibitors,” (in eng), Crit Rev Oncol Hematol, vol. 179, p. 103806, Nov 2022. [CrossRef]
- L. Mezquita et al., “Association of the Lung Immune Prognostic Index With Immune Checkpoint Inhibitor Outcomes in Patients With Advanced Non-Small Cell Lung Cancer,” (in eng), JAMA Oncol, vol. 4, no. 3, pp. 351-357, Mar 1 2018. [CrossRef]
- D. Kazandjian, Y. Gong, P. Keegan, R. Pazdur, and G. M. Blumenthal, “Prognostic Value of the Lung Immune Prognostic Index for Patients Treated for Metastatic Non-Small Cell Lung Cancer,” (in eng), JAMA Oncol, vol. 5, no. 10, pp. 1481-1485, Oct 1 2019. [CrossRef]
- A. M. Hopkins, G. Kichenadasse, A. Y. Abuhelwa, R. A. McKinnon, A. Rowland, and M. J. Sorich, “Value of the Lung Immune Prognostic Index in Patients with Non-Small Cell Lung Cancer Initiating First-Line Atezolizumab Combination Therapy: Subgroup Analysis of the IMPOWER150 Trial,” (in eng), Cancers (Basel), vol. 13, no. 5, Mar 9 2021. [CrossRef]
- F. De Sanctis, S. Solito, S. Ugel, B. Molon, V. Bronte, and I. Marigo, “MDSCs in cancer: Conceiving new prognostic and therapeutic targets,” (in eng), Biochim Biophys Acta, vol. 1865, no. 1, pp. 35-48, Jan 2016. [CrossRef]
- J. Duraiswamy, G. J. Freeman, and G. Coukos, “Therapeutic PD-1 pathway blockade augments with other modalities of immunotherapy T-cell function to prevent immune decline in ovarian cancer,” (in eng), Cancer Res, vol. 73, no. 23, pp. 6900-12, Dec 1 2013. [CrossRef]
- A. Stiff et al., “Nitric Oxide Production by Myeloid-Derived Suppressor Cells Plays a Role in Impairing Fc Receptor-Mediated Natural Killer Cell Function,” (in eng), Clin Cancer Res, vol. 24, no. 8, pp. 1891-1904, Apr 15 2018. [CrossRef]
- D. Sarhan et al., “Adaptive NK Cells with Low TIGIT Expression Are Inherently Resistant to Myeloid-Derived Suppressor Cells,” (in eng), Cancer Res, vol. 76, no. 19, pp. 5696-5706, Oct 1 2016. [CrossRef]
- V. Bronte et al., “Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards,” (in eng), Nat Commun, vol. 7, p. 12150, Jul 6 2016. [CrossRef]
- G. Bronte, L. Calabrò, F. Olivieri, A. D. Procopio, and L. Crinò, “The prognostic effects of circulating myeloid-derived suppressor cells in non-small cell lung cancer: Systematic review and meta-analysis,” (in eng), Clin Exp Med, Nov 19 2022. [CrossRef]
- A. Passaro et al., “Gr-MDSC-linked asset as a potential immune biomarker in pretreated NSCLC receiving nivolumab as second-line therapy,” (in eng), Clin Transl Oncol, vol. 22, no. 4, pp. 603-611, Apr 2020. [CrossRef]
- G. Bronte et al., “High Levels of Circulating Monocytic Myeloid-Derived Suppressive-Like Cells Are Associated With the Primary Resistance to Immune Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer: An Exploratory Analysis,” (in eng), Front Immunol, vol. 13, p. 866561, 2022. [CrossRef]
- J. Koh et al., “MDSC subtypes and CD39 expression on CD8(+) T cells predict the efficacy of anti-PD-1 immunotherapy in patients with advanced NSCLC,” (in eng), Eur J Immunol, vol. 50, no. 11, pp. 1810-1819, Nov 2020. [CrossRef]
- P. De Cicco, G. Ercolano, and A. Ianaro, “The New Era of Cancer Immunotherapy: Targeting Myeloid-Derived Suppressor Cells to Overcome Immune Evasion,” (in eng), Front Immunol, vol. 11, p. 1680, 2020. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



