
Submitted:
11 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
In Μay 2022, for the first time, multiple cases of mpox were reported in several non-endemic countries. The first ever case of the disease in Greece was confirmed on 8 June 2022 and a total of 88 cases were reported in the country until the end of April 2023. A multidisciplinary response team was established by the Greek National Public Health Organization (EODY) to monitor and manage the situation. EODY’s emergency response focused on enhanced surveillance, laboratory testing, contact tracing, medical countermeasures, and education of health care providers and the public. Even though management of cases was considered successful and the risk from the disease was down-graded, sporadic cases continue to occur. Here, we provide epidemiological and laboratory features of the reported cases to depict the course of the disease notification rate, that suggests measures for raising awareness as well as vaccination of high-risk groups of the population should be continued.
Keywords:
mpox
; virus
; outbreak
; response
; vaccination
; Orthopoxvirus
1. Introduction
Human mpox is a viral zoonosis caused by the mpox virus that was first recognized in 1958 at a Danish laboratory [1]). The first human cases were reported in the Democratic Republic of Congo in 1970 [2]. Since then, cases have been identified in West and Central Africa tropical regions [3], with Europe reporting only sporadic imported cases [4-6]. In May 2022, multiple non-travel related cases of mpox were reported for the first time in European countries, mainly among men having sex with men (MSM) [7]. On 23 July 2022, the Director General of WHO declared the multi-country outbreak of mpox to be a Public Health Emergency of International concern (PHEIC) [8]. In total, until 04 April 2023, 25,874 laboratory confirmed cases of the disease were recorded in 45 European Union/European Economic Area (EU/EEA) countries, including six deaths [9].
Within one week of the report of the first suspected case of mpox in Greece on June 8, the National Public Health Organization (EODY) launched an emergency response plan for mpox. We present epidemiological and laboratory features of identified mpox cases and describe the response of the Greek public health authorities depicting main lessons-learned and providing evidence for future public health strategies against the disease.
2. Materials and Methods
2.1. Surveillance and epidemiological investigation of cases
An enhanced mpox surveillance system was implemented. A notification form, an investigation form, and a form for recording close contacts of possible/confirmed cases were created. The ECDC case definition was used.
All laboratory confirmed mpox cases were investigated Investigation was performed via communication with the attending physicians and/or via interviews with the patients by specially trained personnel, using a structured epidemiological questionnaire. Data collected included sociodemographic, clinical, and behavioral data.
Data were used to describe cases in terms of person’s characteristics (age, sex), place (location), time and putative risk factors (recent travel, contact with other cases, sexual orientation, and HIV status). The number of cases by ISO week depicts the temporal distribution of the recorded cases in the country. ISO weeks system uses the week containing the first Thursday of the year as the first week of the year and weeks start with Monday and end on Sunday.
Exposure investigation covered the period of 21 days prior to symptom onset.
A contact tracing team was formed for identification and follow-up of close contacts aiming to interrupt transmission and support people at a higher risk of developing severe disease. Cases were prompted to identify contacts across a number of contexts, such as household, workplace, sexual contacts, healthcare, sports, social gatherings, and any other recalled interactions.
Contacts were notified on their exposure (preferably by the case ) and asked to self-monitor daily for the onset of signs or symptoms (including headache, fever, chills, sore throat, malaise, fatigue, rash, and lymphadenopathy) for a period of 21 days from the last contact with the probable or confirmed case or their contaminated materials during the infectious period.
Actions triggered by the notification of a suspected mpox case are summarized in Figure 1.
In parallel, close monitoring of data from other countries inside and outside Europe for continuous risk assessment was performed.
EODY suggested the inclusion of the disease in the Mandatory Notification System, however the update of the list of mandatory notifiable diseases in the respective law is pending.
2.2. Laboratory investigation
The Central Public Health Laboratory (CPHL) in Athens, the National Reference Lab for emerging viruses in Thessaloniki, Northern Greece, and the Clinical Virology Laboratory in Heraklion, Crete have been appointed by EODY, as the main laboratories for confirmation of suspected cases according to the ECDC case definition. Samples were also analyzed by the clinical microbiology laboratories of Attikon General University Hospital in Athens and the University Hospital of Larissa.
The recommended skin lesion material, including swabs of lesion surface or exudate and lesion crusts was collected from each case. DNA was extracted using commercial manual extraction kits (QIAamp DNA Mini Kit from QIAGEN, Hilden, Germany or genesig Easy, Primerdesign, UK).
Initially, during June 2022, a generic Orthopoxvirus real-time PCR assay (RealStar Orthopoxvirus PCR kit, altona Diagnostics), which targets genes common to other orthopoxviruses (e.g., smallpox, vaccinia), was used as a screening test or an in-house PCR protocol using the OPS3 and OPAs4 primers described by Panning et al [10], along with the CDC Non-Variola Orthopox Generic Real-Time PCR and subsequent Sanger sequencing. However, since early July, all the laboratories have been used a monkeypox–specific, real-time PCR test for the qualitative identification of DNA from Monkeypox virus in clinical samples (Viasure Monkeypox virus Real Time PCR Detection kit, Spain).
Whole genome sequencing analysis was performed in 2 samples; DNA was extracted from skin swab lesions samples by using the High Pure Viral Nucleic Acid Kit (Roche Life Sciences). Extracted DNA was quantified using a Qubit dsDNA High-Sensitivity Assay kit (Invitrogen, Thermo Fisher Scientific, MA, USA) following the protocol according to the manufacturer’s guidelines. One μg of DNA was used to prepare the library with the ligation Sequencing Kit- SQK-LSK109 and the Native Barcoding Expansion 1-12 (PCR-free) EXP-NBD104 (Oxford Nanopore Technologies), following the manufacturers’ protocol. The final library (~430 ng) was loaded to a FLO-MIN106 R9.4.1 flowcell on a MinIon Mk1C device, using Fast Accuracy Basecalling. The genome was assembled with Geneious Prime (https://www.geneious.com) using the MPXV sequence with GenBank accession number NC_063383 as reference.
The two sequences sampled in Greece were analyzed phylogenetically along with 36 reference sequences representative of all lineages (B.1, B.1.1, B.1.10, B.1.11, B.1.12, B.1.13, B.1.14, B.1.15, B.1.16, B.1.17, B.1.2, B.1.3, B.1.4, B.1.5, B.1.6, B.1.7, B.1.8, B.1.9) sampled during 01/05/2022 and 29/09/2022. Specifically, two high-quality sequences per lineage were selected and downloaded from the GISAID database [11] so as the sampling window per lineage to be at least 52 days (1.7 months). Multiple sequence alignment was performed using the MAFFT program (The CIPRES Science Gateway, version 3.3; https://www.phylo.org/). Phylogenetic analysis was performed with the HKY+F+I as an evolutionary model, and ultrafast bootstrap with 1000 replicates using the IQ-TREE, version 2.1.2 [12]. The phylogenetic tree was visualized using the FigTree (version 1.4) program.
2.3. Ethical considerations
EODY is authorized by the Greek law to process COVID-19 epidemiological data for public health purposes. No personal data was used. The study was conducted in accordance with the national and European Union regulations and approved by the Institutional Review Board of EODY (April 2023).
3. Results
3.1. Epidemiology
The first suspected monkeypox case in Greece was initially reported on June 08, 2022. By April 20, 2023, 88 cases were reported. Among them, 6 were travelers visiting Greece and the rest were Greek residents from 6 out of 13 NUTS-II regions (49 from the Attica region). All 88 cases were men; 82 of them (93.2%) self-identified as MSM. Cases median age was 37 years (16-62 years); all but one patient were adults.
The time distribution of laboratory-confirmed cases by week of symptom onset (ISO week) is shown in Figure 2.
The epidemic curve is compatible with person-to-person transmission up to week 38, however even though the outbreak was typically over in the country at around week 41, sporadic mpox cases were reported in weeks 44, 52 of 2022 and weeks 5 and 16 of 2023. These cases had not travelled outside the country during the incubation period. Their age ranged between 23 and 62 and two of them were self-identified as heterosexual.
Table 1 summarizes cases’ characteristics. Seventy-three cases were Greek (82.9%). Twenty-four cases reported travel to a country that had reported mpox cases during the incubation period (27.3%). Sexual contact was reported as the most likely way of transmission for 78 cases, 76 (97.4%) of them being self-identified as MSM. Of 88 cases, 13 reported having attended a large event with sexual contact or having sex in the context of parties (night club/private party/sauna or similar setting) before symptom onset. Among 37 cases with known HIV status, 26 (70,2%) were HIV-positive. Eight cases were health care workers.
The most frequently reported symptom was rash (88, 100%), followed by lymphadenopathy (69, 73.9%) and fever (65, 73.9%). A synchronous evolution of the skin rash was recorded in 52 cases (59.1%). The most frequent localization of the rash was the genital area (61.4%).
In total, fifteen cases (17.1%) were hospitalized, whereas no ICU admissions nor deaths were reported. Out of 84 cases with known smallpox vaccination status, only one case (1.2%) was vaccinated.
3.2. Laboratory findings
Of 238 suspected cases, 88 (52.7%) tested positive for MPXV DNA by PCR, with confirmation by Sanger sequencing in the first cases. From early July, the availability of an mpox –specific, real-time PCR test facilitated the confirmation of the suspected cases in the same day of sample arrival to the laboratories ensuring early diagnosis.
As for sequence analysis obtained by analyzing the complete genome, a total of 372,658 raw reads were taken from sample MPXV-GR-386-2022 (collected on 22.07.2022), with sizes ranging from 60bp to about 42kb, and 99.8% (39,026 reads) were assigned for the assembly, presenting 72 nucleotide substitutions which resulted in 31 amino acid changes. For sample MPXV-GR-613-2022 (collected on 22.08.2022), a total of 486,023 raw reads were taken, with sizes ranging from 38bp to about 24kb, and 99.9% (27,997 reads) were assigned for the assembly, presenting 71 nucleotide substitutions, which resulted in 32 amino acid changes.
Both sequences belong to clade IIb of B.1 lineage (Nextclade v2.13.0), consistent with other sequences from the 2022 hMPXV outbreak.
Phylogenetic analysis using sequences from all previously described lineages suggested that one sequence was classified as B.1.1. and the other one was more closely related to B.1.11, although with a long branch (Figure 3).
The data for this study have been deposited in the European Nucleotide Archive (ENA) at EMBL-EBI under accession number PRJEB61234.
4. Response
A multi-disciplinary response team was formed to set the priorities towards this emerging public health threat. Public health specialists, epidemiologists, clinicians, veterinarians and representatives of non-governmental organizations collaborated for the effective response. A main consideration of the team was to protect the public, without discriminating against MSM or other groups of the population.
The basic pillars of action were to provide guidance for clinicians and the public and to implement control and prevention measures to minimize public health consequences. Information was sent to hospitals, health care centers and medical associations informing of the occurrence of cases, basic clinical manifestations and instructions on protection and hygiene measures. The importance of strict adherence to standard contact precautions, hand hygiene and barrier nursing through use of Personal Protective Equipment (PPE) including: gloves, face mask, gown and goggles, was stressed.
Patients with suspected mpox had to be isolated during the presumed and known infectious periods, that is during the prodromal and rash stages of the illness, respectively. Isolation continued until all of the lesions had resolved.
It was stressed that implementation of measures should not be delayed in anticipation of laboratory confirmation and all probable cases were treated as confirmed until laboratory investigation showed otherwise.
Guidance was provided on clinical management of possible and confirmed mpox cases. The European civil protection mechanism (rescEU) was successfully mobilized for treating a patient presented with non-healing corneal ulcer, who has fully recovered after receiving oral tecovirimat [13].
Finally, guidelines for biosafety issues as well as for samples’ collection, storage and transportation to the reference laboratories have been issued by the CPHL and uploaded to the EODY site.
In parallel, actions for the public took place. EODY issued a press release and uploaded Frequently Asked Questions at its official website, with the intention to minimize the effect of fake news spreading online. Efforts were made to reach people experiencing the highest risk of infection (via on site visits at gay bars, festivals etc.), whereas a dedicated mission was organized in a highly popular island touristic destination, aiming at sensitizing high risk groups, especially in view of the summer 2022 touristic season. In addition, a hotline was established by EODY, where both the public and health care professionals could address questions about the disease.
Finally, the necessary actions were taken for the national provision of JYNNEOS vaccines, and the country created a vaccine stock, for the disposal of which indications are finalized by the National Immunization Committee.
5. Discussion
In May 2022, non-travel related cases of mpox were reported to WHO from several non-endemic countries. In the following weeks the number of cases continued to increase worldwide leading to a global outbreak. Early cases were mostly-travel related, however by the end of May locally acquired infections and community transmission became predominant in all affected countries [14]. Epidemiological data suggested association of the early reported cases with an international LGBT+ Pride event on the island of Gran Canaria. These cases were then linked to transmission chains in several European countries [15-17].
In Greece, the burden of disease was lower compared to other European countries, however the course of the outbreak was compatible to the course in other European countries. Cases continue to be reported sporadically, with the last case reported on the 20th of April 2023. Further study is needed to investigate whether or not this is a result of ongoing transmission in the community that is not captured by the surveillance system. Studies on the percentage of asymptomatic cases of the disease are needed so that to have a clearer picture on the epidemiology of the disease.
Regarding the epidemiological characteristics of the reported cases, data were compatible with data from other countries [10]. Cases were all male, young adults. A relatively high percentage of HIV positive cases among cases with known HIV status was recorded, which underlines the need to test cases diagnosed with mpox for HIV and other sexually transmitted infections as well, taking into consideration that people with untreated HIV are more likely to have complications of mpox [18]. Even though in the literature the highest occupational risk associated with the mpox virus appears to apply to healthcare professionals (physicians, nurses, nursing assistants, emergency, medical technicians, therapists, pharmacists, students, laboratory workers) [19,20], no cases were identified among health care professionals that treated cases in Greece, despite the fact that they were not vaccinated against the virus.
Most cases identified themselves as MSM. Clinical presentation involved predominantly genital, perineal or perianal lesions, with inguinal lymphadenopathy sexual transmission being the main mode of transmissionas described in other studies [16, 21].
Historically, in terms of its genomic and evolutionary characteristics, two distinct clades of MPXV had been identified in different geographical regions of Africa. The “Central African” clade, with a case-fatality rate of 1–12%, found in central Africa and the Congo Basin, and the “West African” clade which is less virulent, with case-fatality rate less than 0·1% that found in west Africa [22,23]. However, Happi et al [24] proposed a novel classification of MPXV that is non-discriminatory and non-stigmatizing for specific nations and geographic regions which has been accepted by WHO. According to the new classification, clade I corresponds to the prior “Central African clade”, while clade II with its two subgroupings IIa and IIb corresponds to the prior “West African clade”. Subclade IIb includes genomes associated with the most recent outbreaks in humans (hMPXV), including the current MPXV outbreak. Moreover, the different outbreaks occurring in recent years have reshaped the genomic landscape of subclade IIb leading to a further divergence of lineages (A, A.1, A.1.1, A.1.1, B.1) [25]. The new lineage B.1 of clade IIb has been identified in the 2022 global outbreak [23, 25] and up to now several different B.1.1 lineages have been recognized. The two MPXV strains from Greece fall into B.1.1 and B.1.11 lineages. Although most B.1 lineages appear as widely distributed, some are predominantly present only in certain countries. For instance, the majority of B.1.6 genomes originate from Peru, B.1.4 from Canada and B.1.11 mostly from the USA [25].
We consider that the level of preparedness and the response deployed to the international signals were successful, as diagnostic laboratory capacity was adequate from the early stages of the outbreak, clinical doctors were sensitized, and high-risk groups of the population have been informed. Special efforts during summer, in an extremely high touristic season for Greece, are deemed successful, given the fact that the number of cases reported from popular islands that hosted events for the MSM community was not high. In parallel, we did not receive any reports from EWRS / IHR about tourists travelling to Greece having been infected by the disease. On the other hand, the low number of reported cases may also be attributed to an underreporting of probable cases to a degree that is not easy to be estimated.
To further strengthen the disease surveillance, the necessary steps to integrate mpox in the mandatory notification system have been undertaken, with the relevant law amendment been rooted. In addition, it is deemed important to remind clinicians – especially targeting those who do not work directly in STI clinics– of the need to be aware of mpox symptoms and the possibility that cases may reappear.
A main challenge in the response was contact tracing, as most of the cases could not share contact details of their sexual partners, either because they did not have this information, or they did not want to share with public health authorities.
Another challenge in the management of the outbreak was that testing criteria were not always met and, in several cases, samples were tested even though the pre-test probability to actually be positive was extremely low. Systematic effort should be made to reinforce testing where it is most needed, targeting clinical settings that serve the population at highest risk. The probability of integrating mpox testing in existing HIV and STI programmes should be explored.
The identification of sporadic domestic cases in Greece and other countries [9], after the end of the outbreak depicts the need for strengthening surveillance and retaining a well-coordinated plan to prevent a resurge of cases, focusing mainly on raising awareness among high-risk population groups, preparing health care units, and assuring testing availability especially as the new summer high-touristic season for Greece approaches.
Author Contributions
Conceptualization, K.M.; methodology, N.S., K.T., K.G.; software, M.T. and G.P.; validation, A.K., and S.P.; formal analysis, M.T. and G.P.; investigation, S.P(2), S.P.(3). E.V., E.G.K. K.P. E.M., Z.F., G.S, E.P.; resources, S.S, G.S.; data curation, M.T., writing—original draft K.M., K.T., K.G.; writing—review and editing, K.M., S.P., V.P., A.P., T.Z.; visualization, G.P.; supervision, D.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of EODY (date of approval: 14 April 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available upon request.
Acknowledgments
The NGS study was supported by the European Union's Horizon 2020 research and innovation programme under grant agreements No. 874735 (VEO).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Parker S., Buller R.M. A review of experimental and natural infections of animals with monkeypox virus between 1958 and 2012. Futur. Virol. 2013; 8:129–157. [CrossRef]
- Ladnyj ID, Ziegler P, Kima E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull World Health Organ 1972; 46:593–7.
- Parker S., Nuara A., Buller R.M., Schultz D.A. Human monkeypox: An emerging zoonotic disease. Future Microbiol. 2007; 2:17–34. [CrossRef]
- Vaughan A, Aarons E, Astbury J, Balasegaram S, Beadsworth M, Beck CR, et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveill. 2018 Sep;23(38):1800509. PMID: 30255836; PMCID: PMC6157091. [CrossRef]
- Hobson G, Adamson J, Adler H, Firth R, Gould S, Houlihan C, et al. Family cluster of three cases of mpox imported from Nigeria to the United Kingdom, May 2021. Euro surveillance: bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2021;26(32).
- Vaughan A., Aarons E., Astbury J., Brooks T., Chand M., Flegg P., Hardman A., Harper N., Jarvis R., Mawdsley S., et al. Human-to-Human Transmission of Mpox Virus, United Kingdom, October 2018. Emerg. Infect. Dis. 2020; 26:782–785.
- WHO. Mpox outbreak 2022. Overview. Available online: https://www.who.int/emergencies/situations/monkeypox-oubreak-2022 (accessed on 15/05/2023).
- WHO. WHO Director-General declares the ongoing monkeypox outbreak a Public Health Emergency of International Concern. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 15/05/2023).
- Joint ECDC-WHO Regional Office for Europe Mpox Surveillance Bulletin. Available online: https://monkeypoxreport.ecdc.europa.eu/ (accessed on 15/05/2023).
- Panning M. Asper M et al. Rapid Detection and Differentiation of Human Pathogenic Orthopox Viruses by a Fluorescence Resonance Energy Transfer Real-Time PCR Assay. 2004; Clin Chem 50:4:702-708. [CrossRef]
- Khare, S., et al (2021) GISAID’s Role in Pandemic Response. China CDC Weekly, 3(49): 1049-1051. PMCID: 8668406. [CrossRef]
- B.Q. Minh, H.A. Schmidt, O. Chernomor, D. Schrempf, M.D. Woodhams, A. von Haeseler, R. Lanfear (2020) IQ-TREE 2: New models and efficient methods for phylogenetic inference in the genomic era. Mol. Biol. Evol., 37:1530-1534. [CrossRef]
- Androudi S, Kaufman AR, Kouvalakis A, Mitsios A, Sapounas S, Al-Khatib D, Schibler M, Pineda R 2nd, Baglivo E. Non-Healing Corneal Ulcer and Uveitis Following Monkeypox Disease: Diagnostic and Therapeutic Challenges. Ocul Immunol Inflamm. 2023 May 4:1-6. Epub ahead of print. PMID: 37140328. [CrossRef]
- Selb R, Werber D, Falkenhorst G, et al. A shift from travel-associated cases to autochthonous transmission with Berlin as epicentre of the monkeypox outbreak in Germany, May to June 2022. Euro Surveill. 2022;27:2200499. [CrossRef]
- Perez Duque M, Ribeiro S, Martins JV, et al. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. Euro Surveill. 2022;27:2200424. [CrossRef]
- Iñigo Martínez J, Gil Montalbán E, Jiménez Bueno S, et al. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Euro Surveill. 2022;27:2200471.
- Antinori A, Mazzotta V, Vita S, et al. Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Euro Surveill. 2022;27:2200421. [CrossRef]
- European Centre for Disease Prevention and Control. Public health considerations for mpox in EU/EEA countries. Stockholm: ECDC; 2023.
- Nörz D., Pfefferle S., Brehm T.T., Franke G., Grewe I., Knobling B., Aepfelbacher M., Huber S., Klupp E.M., Jordan S., et al. Evidence of Surface Contamination in Hospital Rooms Occupied by Patients Infected with Monkeypox, Germany, June 2022. Eurosurveillance. 2022;27:2200477. [CrossRef]
- Rao A.K., Petersen B.W., Whitehill F., Razeq J.H., Isaacs S.N., Merchlinsky M.J., Campos-Outcalt D., Morgan R.L., Damon I., Sánchez P.J., et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR US Dep. Health Hum. Serv. Cent. Dis. Control. Prev. 2022;71:734–742. [CrossRef]
- Velavan TP, Meyer CG. Monkeypox 2022 outbreak: An update. Trop Med Int Health. 2022 Jul;27(7):604-605. [CrossRef]
- Chen N, Li G, Liszewski MK, et al. Virulence differences between monkeypox virus isolates from west Africa and the Congo Basin.Virology 2005; 340: 46–63. [CrossRef]
- Likos AM, Sammons SA, Olson VA, et al. A tale of two clades: monkeypox viruses. J Gen Virol 2005; 86: 2661–72. [CrossRef]
- Happi C, Adetifa I, Mbala P, et al. Urgent need for a non-discriminatory and non-stigmatizing nomenclature for monkeypox virus. PLoS Biol 2022; 20: e3001769. [CrossRef]
- Luna N, Munoz M, et al. Monkeypox virus (MPXV) genomics: A mutational and phylogenomic analyses of B.1 lineages. Travel Medicine and Infectious Disease 2023:52. [CrossRef]
Figure 1.
Actions triggered by the notification of a suspected mpox case.
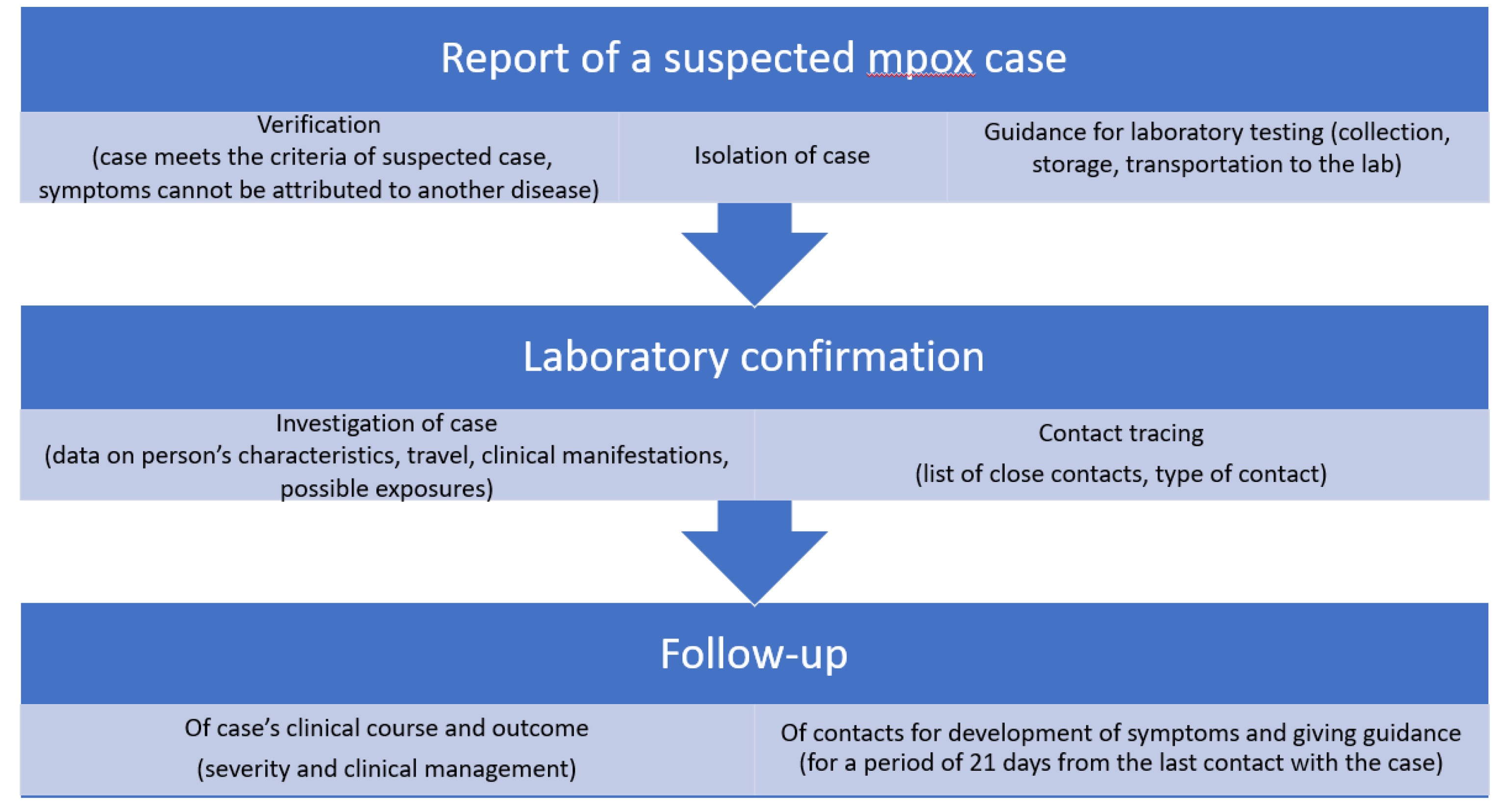
Figure 2.
Number of confirmed cases of Mpox by week of symptom onset in Greece, from 2 June 2022 to 18 April 2023.
Figure 2.
Number of confirmed cases of Mpox by week of symptom onset in Greece, from 2 June 2022 to 18 April 2023.
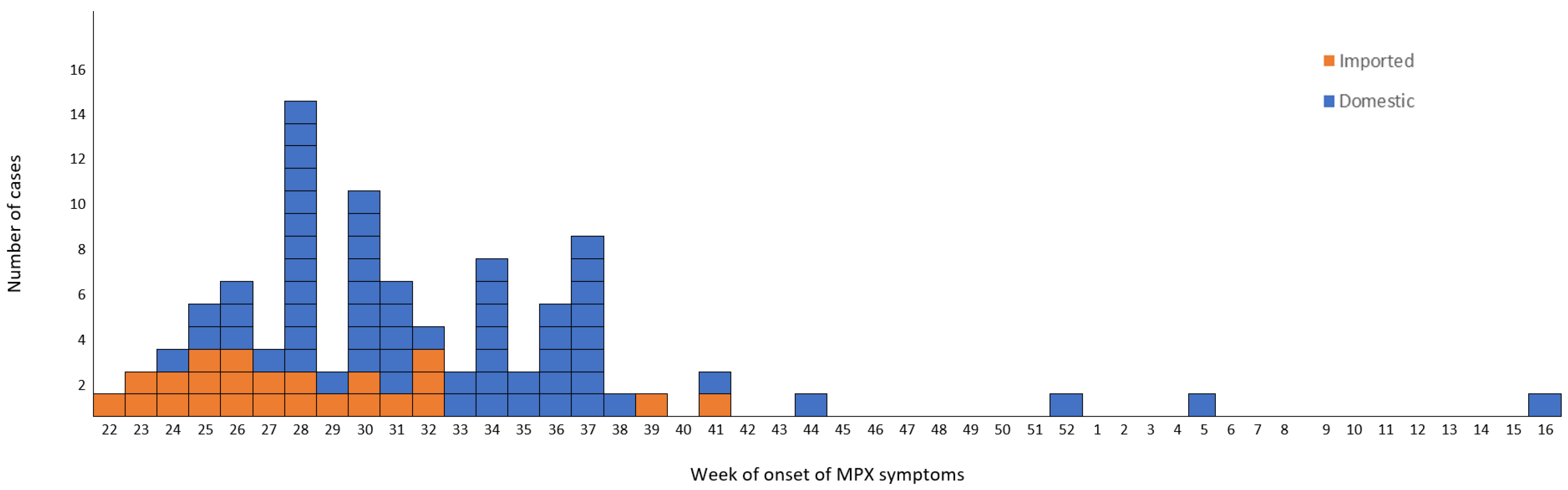
Figure 3.
Phylogenetic tree of Greek MPXV genomes using reference sequences representative of all lineages from GISAID database.
Figure 3.
Phylogenetic tree of Greek MPXV genomes using reference sequences representative of all lineages from GISAID database.
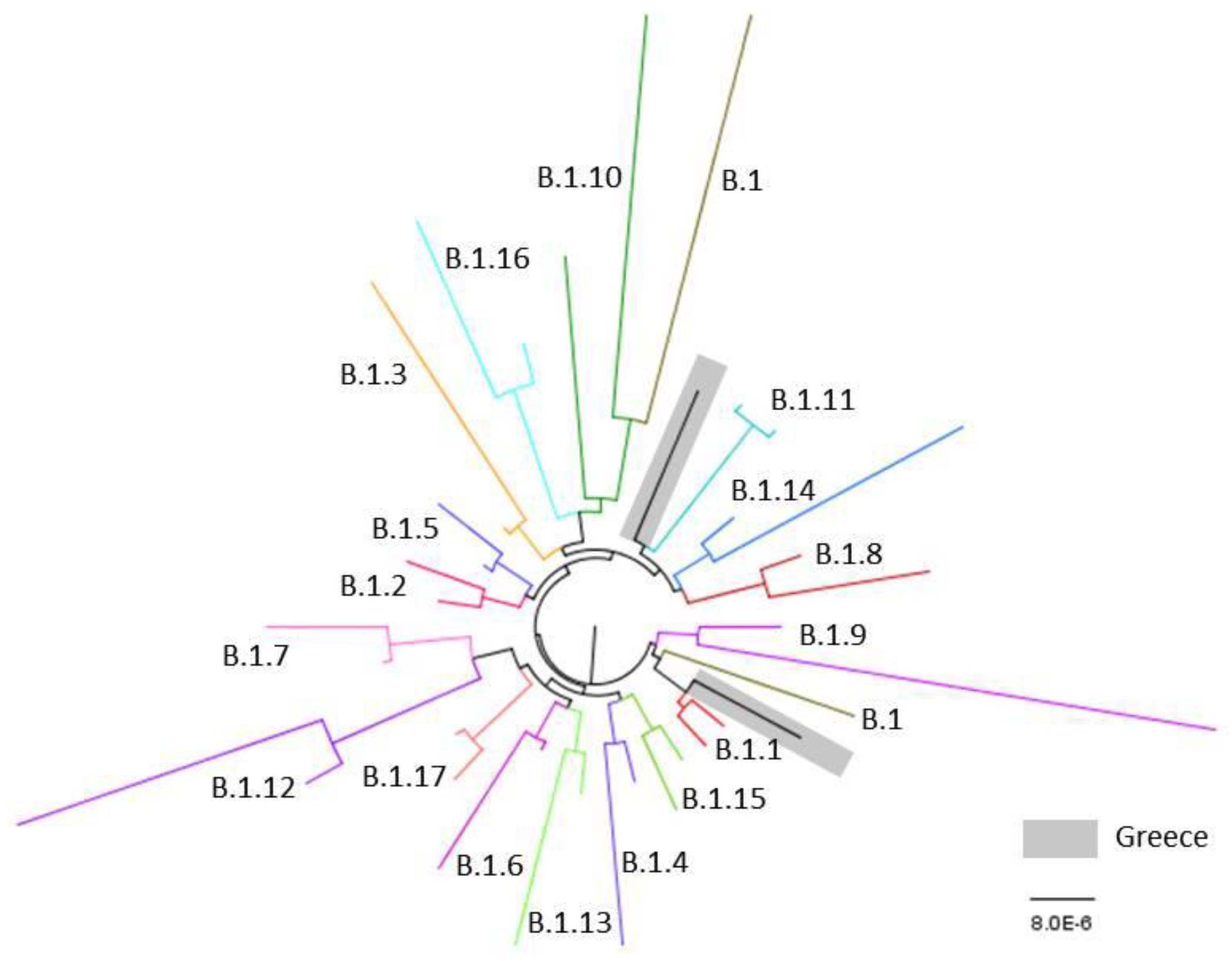

Table 1.
Demographic, epidemiological and clinical characteristics of mpox cases, Greece, June.
| Characteristic | n | % |
|---|---|---|
| Age groups, yrs | ||
| 0-17 | 1 | 1.1 |
| 18-30 | 24 | 27.3 |
| 31-40 | 33 | 37.5 |
| 41-50 | 23 | 26.1 |
| 51-60 | 5 | 5.7 |
| >60 | 2 | 2.3 |
| Gender | ||
| Male | 88 | 100.0 |
| Place of residence (NUTS II Region) | ||
| Regional Area of Attica | 49 | 55.7 |
| Central Macedonia | 22 | 25.0 |
| Crete | 4 | 4.5 |
| Thessaly | 4 | 4.5 |
| South Aegean Sea | 2 | 2.3 |
| Ionian Islands | 1 | 1.1 |
| Travelers/Tourists | 6 | 6.8 |
| Nationality | ||
| Greek | 73 | 83.0 |
| Other | 15 | 17.0 |
| - African | 1 | 1.1 |
| - American | 2 | 2.3 |
| - Asia | 3 | 3.4 |
| - Europe | 9 | 10.2 |
| HIV status | ||
| Negative | 11 | 12.5 |
| Positive | 26 | 29.5 |
| Unknown Travel history during the incubation period |
51 | 58.0 |
| Yes | 24 | 27.3 |
| Νο | 64 | 72.7 |
| Possible route of transmission | ||
| Sexual contact | 78 | 88.6 |
| Unknown | 10 | 11.4 |
| Prior smallpox vaccination | ||
| Vaccinated | 1 | 1.1 |
| Not vaccinated | 83 | 94.3 |
| Unknown | 4 | 4.6 |
| Clinical symptoms | ||
| Rash | 88 | 100.0 |
| Lymphadenopathy | 69 | 78.4 |
| Fever | 65 | 73.9 |
| Fatigue | 52 | 59.1 |
| Headache | 34 | 38.6 |
| Myalgia | 32 | 36.4 |
| Back pain | 23 | 26.1 |
| Itching | 5 | 5.7 |
| Pain | 3 | 3.4 |
| Evolution of skin lesions | ||
| Synchronous | 52 | 59.1 |
| Asynchronous | 33 | 37.5 |
| Unknown | 3 | 3.4 |
| Localisation of the skin lesions | ||
| Genital | 54 | 61.4 |
| Arms | 24 | 27.3 |
| Face | 22 | 25.0 |
| Anal-perianal | 20 | 22.7 |
| Legs | 14 | 15.9 |
| Mouth | 13 | 14.8 |
| Trunk | 9 | 10.2 |
| Thorax | 9 | 10.2 |
| Palms | 5 | 5.7 |
| Soles | 4 | 4.5 |
| Head | 2 | 2.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



