
Submitted:
14 June 2023
Posted:
14 June 2023
You are already at the latest version
Abstract
The hypothesis that health status is the highest-ranking concept, followed by respiratory symptoms and dyspnea as the lowest-ranking concepts in subjects with chronic obstructive pulmonary disease (COPD) was tested in a real clinical setting with 157 subjects with stable COPD. Spearman's rank correlation coefficients for scores of health status using the COPD assessment test (CAT), respiratory symptoms using the COPD Evaluating Respiratory Symptoms (E-RS) and dyspnea using the Dyspnoea-12 (D-12) between any two were 0.6 to 0.7. Upon categorizing the patients as "abnormal" or "normal" according to the threshold, it was found that 30 patients (19.1%) had dyspnea, respiratory symptoms, and impaired the health status. Dyspnea was considered an important part of respiratory symptoms though seven patients had dyspnea but no respiratory symptoms. There were 10 patients who had respiratory symptoms without dyspnea but without health status problems. Furthermore, there were six patients who had both dyspnea and respiratory symptoms but whose health status was classified as fine. Thus, the hypothesis was correct in approximately 85% of cases.
Keywords:
COPD
; Dyspnea
; Health Status
; Respiratory Symptoms
; Surveys and Questionnaires
1. Introduction
During the last two decades, patient-reported outcomes (PROs) have been considered important in the evaluation of health care services, or as a primary or secondary endpoint of clinical trials, in the treatment of patients with chronic obstructive pulmonary disease (COPD) [1,2]. Since several tools have been reported in the literature, it may be difficult to understand how the conceptual framework from which each instrument derives differs between tools. Jones et al. developed the St. George’s Respiratory Questionnaire (SGRQ) and the COPD Assessment Test (CAT) for health status measurements in subjects with COPD [3,4,5,6,7]. Yorke et al. reported that the Dyspnoea-12 (D-12) provides a global score of severity of breathlessness and can measure dyspnea in a variety of diseases [8,9,10]. However, as dyspnea is obviously different from health status, it would not be easy to explain how dyspnea is relevant to health status [11].
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) launched a classification system in 2011 [12], called the revised 'combined COPD assessment' classification in which symptoms should be evaluated using the modified Medical Research Council (mMRC) dyspnea scale or the CAT. However, since the former is regarded as a tool for measuring dyspnea and the latter as a health status measure, the results may differ somewhat from what the symptoms really are they may be a little different from what the symptom should be. The discrepancy between the mMRC and the CAT score has since been widely debated [13,14,15,16,17,18,19,20]. Although some have attributed the discordance to the sensitivity of the tools’ measurement properties, it may not be surprising since dyspnea and health status differ conceptually.
On the other hand, Leidy et al. created a reliable and valid instrument for evaluating the severity of respiratory symptoms in stable COPD using 11 respiratory symptoms items from the 14-item Exacerbations of Chronic Pulmonary Disease Tool Patient-Reported Outcome (known as EXACT-PRO) [21,22,23,24]. This is the Evaluating Respiratory Symptoms in COPD (E-RS) [23,24], which was designed as a daily diary to be easily administered by clinical study subjects using a personal digital assistant or smartphone. The original developers of the CAT, D-12 and E-RS have mentioned that they derive from different conceptual frameworks, but theoretically, dyspnea may be included in respiratory symptoms, and this symptom may be one of the essential components of health status. Unfortunately, however, they are often undifferentiated and are used almost interchangeably in everyday clinical practice.
The GOLD states that chronic and progressive dyspnea is the most characteristic symptom of COPD, and cough with sputum production is present in up to 30% of patients. Hajiro et al. reported that, using stepwise multiple regression analyses, the Baseline Dyspnea Index (BDI) score, anxiety by the Hospital Anxiety Depression Scale (HAD), and maximal oxygen uptake (O2max) accounted for 61% of the variance in the SGRQ [11]. Therefore, health status is the highest-level concept, dyspnea is the lowest level concept, and respiratory symptoms are in between, which is the hypothesis that this study seeks to test. This hypothesis is depicted in Figure 1, in which dyspnea would be reflected in respiratory symptoms and respiratory symptoms in health status, since it can be commonly accepted that breathlessness is included in respiratory symptoms, and that this symptom is one of the essential components of health status in subjects with COPD. This may be helpful in solving the question of whether or not they can be used interchangeably, in subjects with COPD in clinical practice.
The aim of the present study was to ascertain whether the conceptual independence of health status, respiratory symptoms and dyspnea is maintained in the clinical practice of COPD. For this purpose, the authors examined whether the distribution of cases is consistent with the hypothesis when the cases are classified as "abnormal" or "normal" or "with (disability)" or "without (disability)" according to the respective thresholds based on the scores of the evaluation tools for the three concepts.
2. Materials and Methods
2.1. Participants
We recruited 157 consecutive patients with stable COPD who attended the outpatient clinic in the Department of Respiratory Medicine of the National Center for Geriatrics and Gerontology (NCGG) from September 2013 to February 2022. Inclusion criteria included being over 50 years of age, having a smoking history of more than 10 pack-years, having chronic fixed airflow limitation, attending the clinic regularly for more than half a year, having no uncontrolled comorbidities, and having no variation in treatment in the preceding four weeks. Chronic fixed airflow limitation was defined as a maximum ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of less than 0.7. All participants provided written informed consent, and the research was approved by the National Center for Geriatrics and Gerontology Institute’s Ethics Committee (No. 1138-3).
2.2. Measurements
Baseline pulmonary function measurements of the participants were taken on a single day, which included post-bronchodilator spirometry (CHESTAC-8800; Chest, Tokyo, Japan), residual volume (RV) measured by the closed-circuit helium method, and diffusing capacity for carbon monoxide (DLCO) assessed by the single-breath technique as reported by the American Thoracic Society and European Respiratory Society Task Force in 2005 [25]. Calculations of the predicted values for FEV1 and vital capacity were carried out as recommended by the Japan Respiratory Society [26].
2.3. Patient-Reported Measurements
Validated Japanese versions of the following patient-reported outcome measurement tools were used in the present study: the CAT to measure health status, D-12 to assess the severity of breathlessness and E-RS to analyze and quantify respiratory symptoms [27,28]. The St. George’s Respiratory Questionnaire (SGRQ) (version 2) and the Hyland Scale were also administered as a standard procedure. The former consists of 50 items divided into the three components of symptoms, activity, and impact, and a total score ranging from 0 to 100 is calculated [3,11]. Higher scores on the SGRQ indicate a more severe state of health. The latter is a global health scale with scores ranging from 0 to 100, where 0 = ‘might as well be dead' and 100 = 'perfect quality of life' [29,30].
To assess the severity of dyspnea, we used the D-12, which consists of twelve items (seven physical and five affective), each with a four-point grading scale (0-3), producing a Total Score (range 0-36, with higher scores representing more severe breathlessness) [8,9,10,28]. CAT is a questionnaire consisting of eight items scored from 0 to 5 in relation to cough, phlegm, chest tightness, breathlessness going up hills/stairs, activity limitations at home, confidence leaving home, sleep and energy [5,6,7,27]. CAT scores range from 0 to 40, with a score of zero indicating no impairment. The E-RS uses 11 respiratory symptom items from the 14-item EXACT-PRO, where scores range from 0 to 40, with higher scores indicating more severe symptoms [23,24]. The E-RS Total score represents the severity of the general respiratory symptoms. Three subscales were also used in this analysis. A Japanese translation has been created and provided by the original developers and they recommend using an electronic version to collect the answers. However, no electronic device with the Japanese version of the EXACT-PRO or E-RS was available, so all surveys were conducted using a paper-based method.
We reported in 2019 that, from the data obtained from 646 healthy non-smoking subjects, the reference values for the D-12, E-RS Total and CAT scores were considered to be ≤1, ≤4 and ≤9, respectively. These reference values were also used as the thresholds in the present study [31].
2.4. Statistical Methods
Score distributions of the tools were evaluated with the Shapiro-Wilk test and by inspection of histograms. Spearman’s rank correlation tests were used to examine relationships between two sets of data. The significance of between-group differences was determined by Kruskal-Wallis test and Steel-Dwass test. The relationships between three groups were also analyzed using a Venn diagram. All p values less than 0.05 were deemed to be statistically significant. The results are expressed as mean ± standard deviation (SD) with some exceptions in the tables.
3. Results
3.1. Subject Characteristics
A total of 157 consecutive patients (144 men) with COPD and a wide range of FEV1 (69.8±20.4%pred) participated. One hundred and twenty subjects were former smokers while 37 were current smokers. Their demographic details as well as the results of pulmonary function tests are listed in Table 1. Using the classification of severity of airflow limitation of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, 53 subjects (33.8%) were in Stage 1 (defined as FEV1≧80% predicted), 79 (50.3%) in Stage 2 (50%≦FEV1<80% predicted), 18 (11.5 %) in Stage 3 (30%≦FEV1<50% predicted) and 7 (4.5%) in Stage 4 (FEV1<30% predicted) (Table 2). Relatively few patients with severe or very severe COPD were involved in the present study.
3.2. S Distribution of Scores and Correlation between Tools
The hypothesis that the scores obtained are normally distributed was rejected in the D-12, CAT and E-RS including their subscales shown in Table 3 (Shapiro-Wilk test, all p < 0.001). They were skewed toward the milder ends, and a floor effect was observed in all scores. This effect was most pronounced for D-12 (47.8%) and least for the CAT (5.1%).
Regarding the interrelationships between the D-12 Total, CAT and E-RS Total scores, they were significantly correlated with each other (D-12 Total vs. CAT, Spearman’s correlation coefficient (Rs) =0.603, p<0.001; D-12 Total vs. E-RS Total, Rs=0.655, p<0.001; and CAT vs. E-RS Total, Rs=0.675, p<0.001) (Table 1). All of the correlation coefficients were below 0.7, or what is occasionally regarded as the level suggestive of conceptual equivalence. Scatterplots showing the relationships between tools are depicted in Figure 2.
3.3. Relationship between Tools Using the Thresholds.
The D-12 Total score was above the threshold in 43 out of the 157 participants (27.4%), and CAT and E-RS Total scores were higher than the thresholds in 61 (38.8%) and 65 (41.4%), respectively. This result conflicts with the study hypothesis that respiratory symptoms are one of the essential components of health status in subjects with COPD. Therefore, we subsequently analyzed the relationships between tools using a Venn diagram.
The actual number of patients with scores above the threshold is shown in the Venn diagram (Figure 3) (Table 4). Apart from patients who were negative for all three, the largest number were in the location that falls under D-12∩E-RS∩CAT, which included 30 patients (19.1%). The second most common was ∩E-RS∩CAT, and the third was ∩∩CAT. If the scores were distributed in complete accordance with the hypothesis, patients should not be distributed in positions ∩E-RS∩, D-12∩E-RS∩, D-12∩∩ or D-12∩∩CAT. However, in fact, a total of 23 patients (14.6%) fell into these categories.
Since the analysis using the Venn diagram revealed that the distribution of disability in actual cases was not necessarily distributed according to the hypothesis, the next step was to analyze the extent to which the three tools differed in their judgments. Concordant and discordant results between tools were examined using the threshold (Table 5). The numbers of those with higher scores on one instrument and lower scores on another were 28 (17.8%) between CAT and E-RS, 36 (22.9%) between E-RS and D-12 and 42 (26.8%) between CAT and D-12. If the D-12 score, which suggests the presence of dyspnea, is high, then the CAT score, which suggests impairment of health status, must also be high. However, in actual cases, 12 patients (7.6%) had high D-12 scores but normal CAT scores, a seemingly contradictory result. Likewise, the situation in which a lower-level concept is disturbed and shows abnormality, but a higher-level concept is not disturbed and does not show abnormality, would imply that the hypothesis is inconsistent with the assumption of correctness, which was the case for 16 (10.2%) for the relationship between CAT and E-RS, and for 7 (4.5%) in relation to E-RS and D-12.
4. Discussion
This is the first study to examine the hypothesis that in patients with COPD, the relationship between the concepts of dyspnea, respiratory symptoms, and health status is that health status is the highest concept, followed by respiratory symptoms and dyspnea as the lowest concepts, in a real clinical setting. The hypothesis is supported to some extent by the analysis of the scores of the tools that evaluate PROs designed to evaluate the three concepts. There is however some measurement error since the measuring properties of each tool are naturally related to the distribution of scores. For example, dyspnea is considered an important part of respiratory symptoms, but there were seven patients who had dyspnea but no respiratory symptoms. It would be expected that a patient with a cough and phlegm would be classified as having a problematic health condition, but there were 10 patients who had respiratory symptoms such as a cough and phlegm without dyspnea, but whose health condition was not problematic. There were also six patients who had both dyspnea and respiratory symptoms, but whose health status was classified as fine. This distribution of scores contradicting the hypothesis occurs in less than 15% of all cases and might be unavoidable in practical terms. In other words, it can be concluded that the hypothesis was correct in 85% of cases.
In the present study, Spearman's correlation coefficients of the scores for health status measured by the CAT, respiratory symptoms by E-RS and dyspnea by D-12 were between 0.6 and 0.7 for any two. In a similar study of a working population of 1,566 reported in 2019, the Spearman's correlation coefficient between D-12 and CAT was 0.398, between D-12 and E-RS it was 0.274 and between CAT and E-RS it was 0.446 [31], so it can be assumed that the correlation coefficient is quite good in subjects with COPD. However, the associations between dyspnea, respiratory symptoms and health status were significant but far below the level of conceptual similarity. This may be expected since the three PRO measurement tools were created by each developer from independent conceptual frameworks. Therefore, we believe that the three concepts must be distinguished and should not be used as complementary substitutes especially in a practical clinical setting. In addition, when the correlation coefficients of the CAT, E-RS and D-12 are compared with those of lung volume, airflow limitation, residual volume and diffusion capacity, the correlation coefficients of the first two are very similar, but there seems to be some distance between them and the D-12. While we cannot rule out the possibility that this is due to that conceptual factor, we suspect that it is rather related to the fact that the floor effect was quite advanced in the D-12. In any case, there are limitations to characterizing the three concepts by studying the distribution of scores and correlations.
We then proceeded with the analysis by classifying each concept into two options, "abnormal" or "normal" or "with disability" or "without," using a certain threshold value for each. In other words, we attempted to classify patients into 1) with or without dyspnea, 2) with or without respiratory symptoms, and 3) with or without impaired health status. However, this yes-or-no format approach is not inherently recommended as it carries the risk of false negatives or false positives. Standardized tools have been developed to avoid such measurement errors. The threshold values used in each tool are also important and may affect the results. For example, in the present study, the CAT threshold used was 10, which GOLD has historically advocated as the boundary between GOLD A and B and between GOLD C and D. However, our 2013 report recommended a threshold of 13.6 [32], and the Canadian Cohort Obstructive Lung Disease (CanCOLD) report by Pinto et al. in 2014 recommended 16 [33]. Since our 2019 report was based on 10, we used 10 as the threshold for the CAT in this analysis [31].
Here, it is necessary to verify to what extent it is correct to say that if there is no anomaly regarding one concept, the other concepts are not anomalous either if they are used in a complementary manner in a practical clinical setting. The question is to what extent the two tools agree or disagree on the results of the "abnormal" or "normal" or 'with disability' and 'without’ two-party classification using threshold values. Discordant results were observed in 28 (17.8%) to 42 (26.8%) patients, with the highest number between the CAT and D-12. It is understandable that there were many discrepancies between the conceptually most distant tools, but this may also involve differences in measurement characteristics. However, if the hypothesis is correct here, the condition of normal D-12 but abnormal CAT is not inconsistent with the hypothesis. Since the opposite situation, i.e., abnormal D-12 and normal CAT, is not allowed by the hypothesis, we can conclude that there was a measurement error in at least 12 (7.6%) of the subjects. Similarly, we believe there was a measurement error between the CAT and E-RS in 16 (10.2%) and between the E-RS and D-12 in 7 (4.5%). The same table is shown in the 2019 report for a working population of 1,566 people, where 1~4% of participants showed similar results [31], but the frequency is shown to be higher in the current study for COPD patients.
5. Conclusions
In COPD patients, the hypothesis that the relationship between the concepts of dyspnea, respiratory symptoms, and health status is that health status is the highest-level concept, followed by respiratory symptoms and dyspnea as the lowest level concepts, was tested for the first time in a clinical setting. The single correlation coefficients of the scores for health status by the CAT, respiratory symptoms by E-RS and dyspnea by D-12 ranged from 0.6 to 0.7 for any two. The distribution of scores showed a high degree of floor effect in the D-12. Correlations with physiological indices were similar for the CAT and E-RS. When each concept was analyzed by categorizing the patients as "abnormal" or "normal" or "with disability" or "without" according to the threshold, 30 patients (19.1%) were considered as core cases with dyspnea, respiratory symptoms, and impaired health status. Scores were distributed inconsistently with the hypothesis in less than 15% of the cases, for example, the seven patients who had dyspnea but no respiratory symptoms. In other words, we can conclude that the hypothesis was supported 85% of the time.
Author Contributions
KN contributed, as the principal investigator, to the design and concept of the study, the analysis of the results, and the writing of the manuscript. MK, RS, MM and AS contributed to acquisition of data. KN contributed to the statistical analysis. All authors have read and approved the final manuscript.
Funding
This study was partly supported by the Research Funding for Longevity Sciences (22-7) from the National Center for Geriatrics and Gerontology (NCGG), Japan.
Institutional Review Board Statement
The research was approved by the National Center for Geriatrics and Gerontology Institute’s Ethics Committee (No. 1138-3).
Informed Consent Statement
Written informed consent was obtained from all participants.
Data Availability Statement
Anonymized participant data will be available upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ekstrom, M.; Sundh, J.; Larsson, K. Patient reported outcome measures in chronic obstructive pulmonary disease: Which to use? Expert. Rev. Respir. Med. 2016, 10, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Jahagirdar, D.; Kroll, T.; Ritchie, K.; Wyke, S. Patient-reported outcome measures for chronic obstructive pulmonary disease : The exclusion of people with low literacy skills and learning disabilities. Patient 2013, 6, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. The St. George's Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.; Harding, G.; Wiklund, I.; Berry, P.; Leidy, N. Improving the process and outcome of care in COPD: Development of a standardised assessment tool. Prim. Care Respir. J. 2009, 18, 208–215. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Jones, P.W.; Brusselle, G.; Dal Negro, R.W.; Ferrer, M.; Kardos, P.; Levy, M.L.; Perez, T.; Soler Cataluna, J.J.; van der Molen, T.; Adamek, L.; et al. Properties of the COPD assessment test in a cross-sectional European study. Eur. Respir. J. 2011, 38, 29–35. [Google Scholar] [CrossRef]
- Jones, P.W.; Tabberer, M.; Chen, W.H. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT) scores. BMC Pulm. Med. 2011, 11, 42. [Google Scholar] [CrossRef]
- Yorke, J.; Moosavi, S.H.; Shuldham, C.; Jones, P.W. Quantification of dyspnoea using descriptors: Development and initial testing of the Dyspnoea-12. Thorax 2010, 65, 21–26. [Google Scholar] [CrossRef]
- Yorke, J.; Swigris, J.; Russell, A.M.; Moosavi, S.H.; Ng Man Kwong, G.; Longshaw, M.; Jones, P.W. Dyspnea-12 is a valid and reliable measure of breathlessness in patients with interstitial lung disease. Chest 2011, 139, 159–164. [Google Scholar] [CrossRef]
- Yorke, J.; Armstrong, I. The assessment of breathlessness in pulmonary arterial hypertension: Reliability and validity of the Dyspnoea-12. Eur. J. Cardiovasc. Nurs. 2014, 13, 506–514. [Google Scholar] [CrossRef]
- Hajiro, T.; Nishimura, K.; Tsukino, M.; Ikeda, A.; Koyama, H.; Izumi, T. Comparison of discriminative properties among disease-specific questionnaires for measuring health-related quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Vestbo, J.; Hurd, S.S.; Agusti, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Adamek, L.; Nadeau, G.; Banik, N. Comparisons of health status scores with MRC grades in COPD: Implications for the GOLD 2011 classification. Eur. Respir. J. 2013, 42, 647–654. [Google Scholar] [CrossRef]
- Rhee, C.K.; Kim, J.W.; Hwang, Y.I.; Lee, J.H.; Jung, K.S.; Lee, M.G.; Yoo, K.H.; Lee, S.H.; Shin, K.C.; Yoon, H.K. Discrepancies between modified Medical Research Council dyspnea score and COPD assessment test score in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 1623–1631. [Google Scholar] [CrossRef]
- Tsiligianni, I.G.; Alma, H.J.; de Jong, C.; Jelusic, D.; Wittmann, M.; Schuler, M.; Schultz, K.; Kollen, B.J.; van der Molen, T.; Kocks, J.W. Investigating sensitivity, specificity, and area under the curve of the Clinical COPD Questionnaire, COPD Assessment Test, and Modified Medical Research Council scale according to GOLD using St George's Respiratory Questionnaire cutoff 25 (and 20) as reference. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 1045–1052. [Google Scholar] [CrossRef]
- Mittal, R.; Chhabra, S.K. GOLD Classification of COPD: Discordance in Criteria for Symptoms and Exacerbation Risk Assessment. COPD 2017, 14, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.L.; Lin, C.H.; Wang, C.C.; Chan, M.C.; Hsu, J.Y.; Hang, L.W.; Perng, D.W.; Yu, C.J.; Wang, H.C.; Taiwan Clinical Trial Consortium for Respiratory, D. Comparison between COPD Assessment Test (CAT) and modified Medical Research Council (mMRC) dyspnea scores for evaluation of clinical symptoms, comorbidities and medical resources utilization in COPD patients. J. Formos. Med. Assoc. 2019, 118, 429–435. [Google Scholar] [CrossRef]
- Moya-Alvarez, V.; Quevedo-Marin, J.L.; Ji, Z.; Navarro-Jimenez, C.; Jimenez-Garcia, R.; Lopez-de-Andres, A.; Perez-Trullen, A.; de Miguel-Diez, J. Variation in Assignment of the COPD Patients into a GOLD Group According to Symptoms Severity. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1987–1995. [Google Scholar] [CrossRef]
- Casanova, C.; Marin, J.M.; Martinez-Gonzalez, C.; de Lucas-Ramos, P.; Mir-Viladrich, I.; Cosio, B.; Peces-Barba, G.; Solanes-Garcia, I.; Aguero, R.; Feu-Collado, N.; et al. Differential Effect of Modified Medical Research Council Dyspnea, COPD Assessment Test, and Clinical COPD Questionnaire for Symptoms Evaluation Within the New GOLD Staging and Mortality in COPD. Chest 2015, 148, 159–168. [Google Scholar] [CrossRef]
- Ertan Yazar, E.; Niksarlioglu, E.Y.; Yigitbas, B.; Bayraktaroglu, M. How to Utilize CAT and mMRC Scores to Assess Symptom Status of Patients with COPD in Clinical Practice? Medeni. Med. J. 2022, 37, 173–179. [Google Scholar] [CrossRef]
- Leidy, N.K.; Wilcox, T.K.; Jones, P.W.; Murray, L.; Winnette, R.; Howard, K.; Petrillo, J.; Powers, J.; Sethi, S.; Group, E.-P.S. Development of the EXAcerbations of Chronic Obstructive Pulmonary Disease Tool (EXACT): A patient-reported outcome (PRO) measure. Value Health 2010, 13, 965–975. [Google Scholar] [CrossRef]
- Leidy, N.K.; Wilcox, T.K.; Jones, P.W.; Roberts, L.; Powers, J.H.; Sethi, S.; Group, E.-P.S. Standardizing measurement of chronic obstructive pulmonary disease exacerbations. Reliability and validity of a patient-reported diary. Am. J. Respir. Crit. Care Med. 2011, 183, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Leidy, N.K.; Murray, L.T.; Monz, B.U.; Nelsen, L.; Goldman, M.; Jones, P.W.; Dansie, E.J.; Sethi, S. Measuring respiratory symptoms of COPD: Performance of the EXACT- Respiratory Symptoms Tool (E-RS) in three clinical trials. Respir. Res. 2014, 15, 124. [Google Scholar] [CrossRef] [PubMed]
- Leidy, N.K.; Sexton, C.C.; Jones, P.W.; Notte, S.M.; Monz, B.U.; Nelsen, L.; Goldman, M.; Murray, L.T.; Sethi, S. Measuring respiratory symptoms in clinical trials of COPD: Reliability and validity of a daily diary. Thorax 2014, 69, 443–449. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Sasaki, H.; Nakamura, M.; Kida, K.; Kambe, M.; Takahashi, K.; Fujimura, M. Reference values for spirogram and blood gas analysis in Japanese adults. J Jpn Respir Soc 2001, 39, S1–S17. [Google Scholar]
- Tsuda, T.; Suematsu, R.; Kamohara, K.; Kurose, M.; Arakawa, I.; Tomioka, R.; Kawayama, T.; Hoshino, T.; Aizawa, H. Development of the Japanese version of the COPD Assessment Test. Respir. Investig. 2012, 50, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Oga, T.; Nakayasu, K.; Taniguchi, H.; Ogawa, T.; Watanabe, F.; Arizono, S.; Kusunose, M.; Sanda, R.; Shibayama, A.; et al. Comparison between tools for measuring breathlessness: Cross-sectional validation of the Japanese version of the Dyspnoea-12. Clin. Respir. J. 2021, 15, 1201–1209. [Google Scholar] [CrossRef]
- Hyland, M.E.; Sodergren, S.C. Development of a new type of global quality of life scale, and comparison of performance and preference for 12 global scales. Qual. Life Res. 1996, 5, 469–480. [Google Scholar] [CrossRef]
- Nishimura, K.; Oga, T.; Ikeda, A.; Hajiro, T.; Tsukino, M.; Koyama, H. Comparison of health-related quality of life measurements using a single value in patients with asthma and chronic obstructive pulmonary disease. J. Asthma 2008, 45, 615–620. [Google Scholar] [CrossRef]
- Nishimura, K.; Oga, T.; Nakayasu, K.; Ogasawara, M.; Hasegawa, Y.; Mitsuma, S. How different are COPD-specific patient reported outcomes, health status, dyspnoea and respiratory symptoms? An observational study in a working population. BMJ Open 2019, 9, e025132. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Mitsuma, S.; Kobayashi, A.; Yanagida, M.; Nakayasu, K.; Hasegawa, Y.; Jones, P.W. COPD and disease-specific health status in a working population. Respir. Res. 2013, 14, 61. [Google Scholar] [CrossRef] [PubMed]
- Pinto, L.M.; Gupta, N.; Tan, W.; Li, P.Z.; Benedetti, A.; Jones, P.W.; Bourbeau, J.; Can, C.s.g. Derivation of normative data for the COPD assessment test (CAT). Respir. Res. 2014, 15, 68. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The hypothesis of the present study. Considering health status, respiratory symptoms, and dyspnea in subjects with COPD, health status is hypothesized to be the highest concept and dyspnea is the lowest. We aimed to examine how different they are and to determine whether or not they can be used interchangeably.
Figure 1.
The hypothesis of the present study. Considering health status, respiratory symptoms, and dyspnea in subjects with COPD, health status is hypothesized to be the highest concept and dyspnea is the lowest. We aimed to examine how different they are and to determine whether or not they can be used interchangeably.
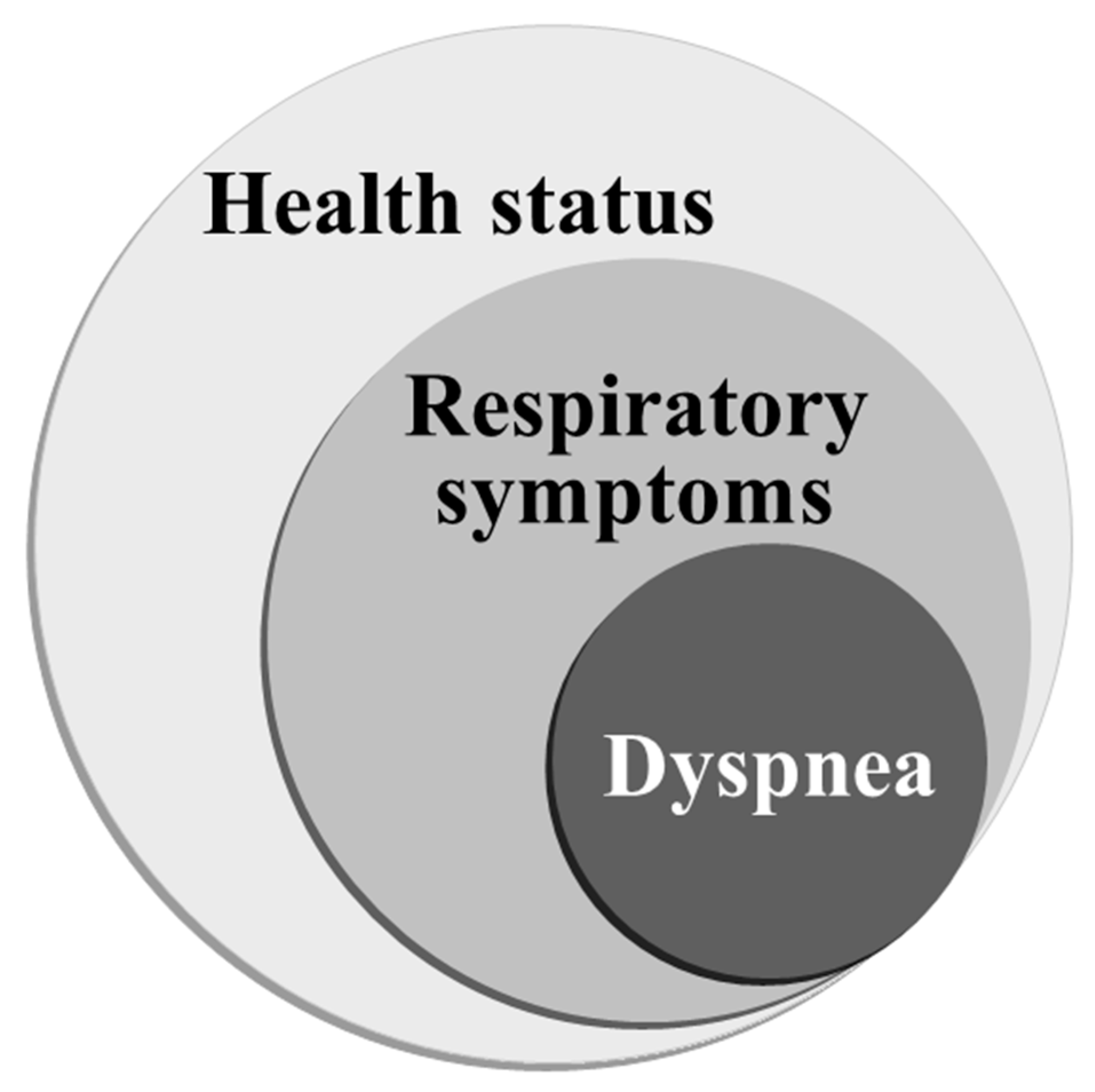
Figure 2.
Scatterplots showing the relationships between the D-12 (Dyspnoea-12) Total score, CAT (COPD assessment test) score and E-RS (Evaluating Respiratory Symptoms in COPD) Total score in subjects with COPD.
Figure 2.
Scatterplots showing the relationships between the D-12 (Dyspnoea-12) Total score, CAT (COPD assessment test) score and E-RS (Evaluating Respiratory Symptoms in COPD) Total score in subjects with COPD.
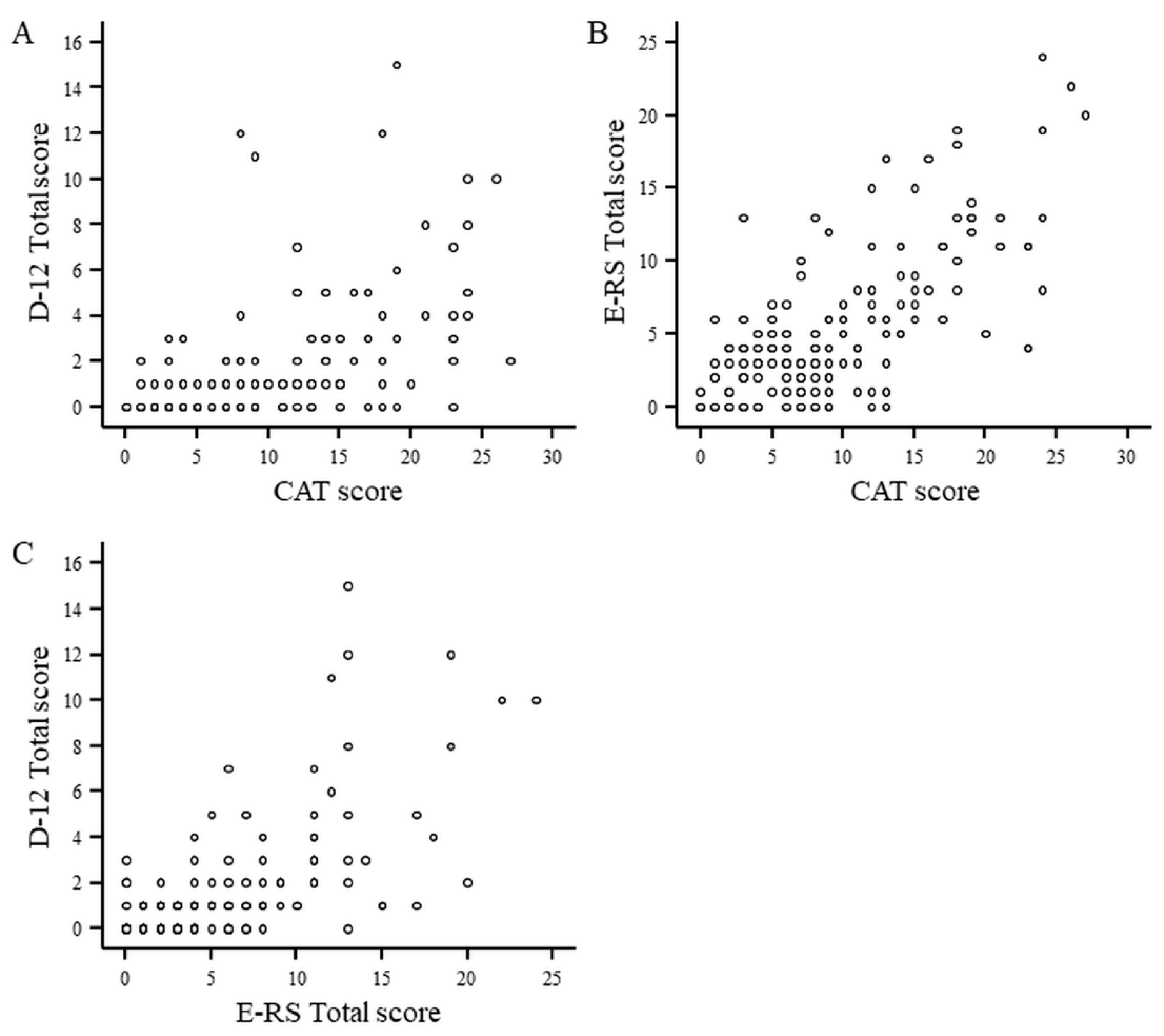
Figure 3.
Three-circle Venn diagram representing the relationships between the D-12 Total, CAT and E-RS Total scores. Each reveals the number of positive patients with scores above threshold values.
Figure 3.
Three-circle Venn diagram representing the relationships between the D-12 Total, CAT and E-RS Total scores. Each reveals the number of positive patients with scores above threshold values.
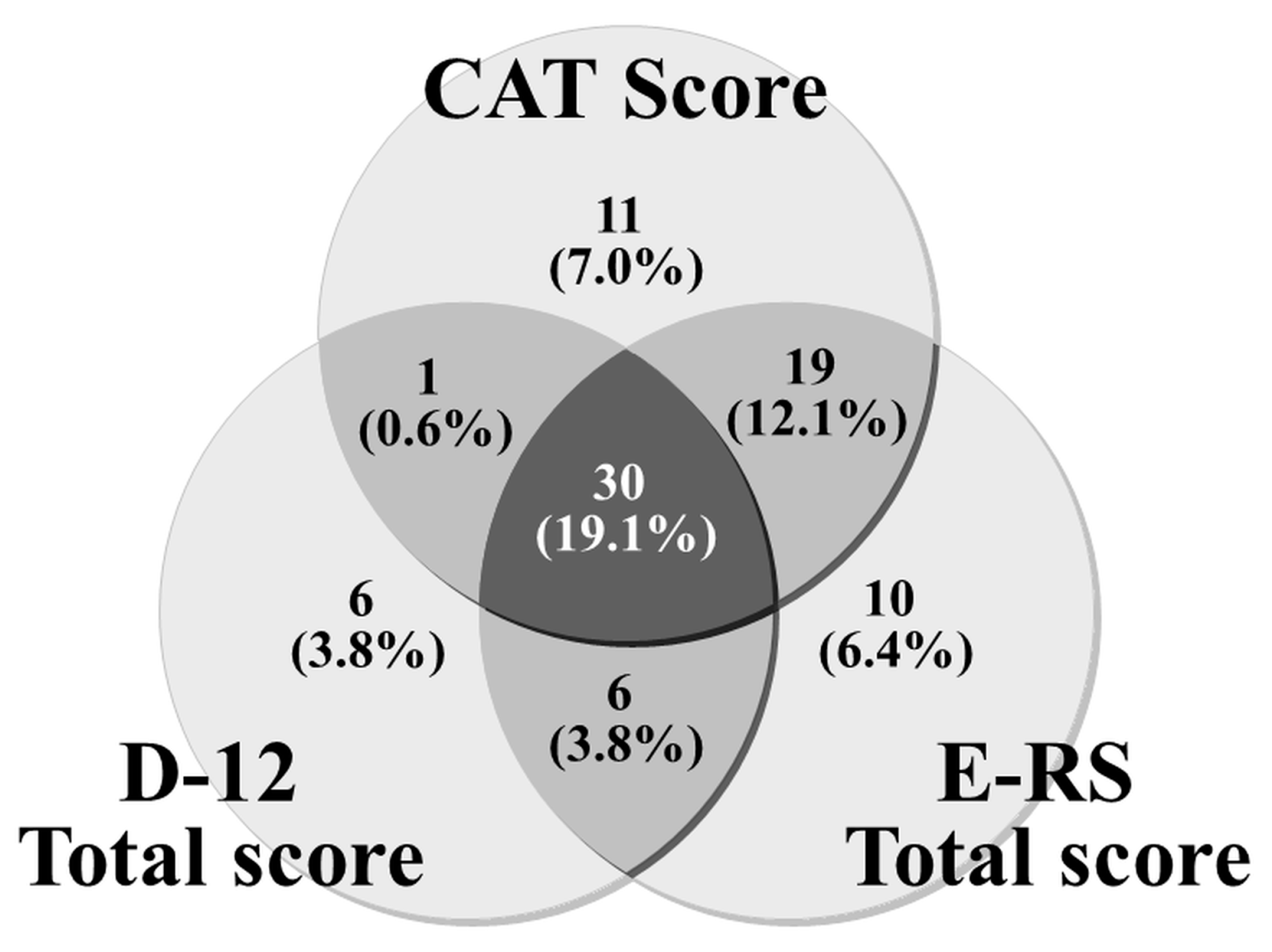

Table 1.
Baseline Characteristics in 157 Subjects with COPD and Spearman’s Rank Correlation Coefficients with the Scores of the Patient-Reported Outcome Measures.
Table 1.
Baseline Characteristics in 157 Subjects with COPD and Spearman’s Rank Correlation Coefficients with the Scores of the Patient-Reported Outcome Measures.
| mean | SD | max. | min. | Correlations (Rs) with | |||||
|---|---|---|---|---|---|---|---|---|---|
| D-12 Total score |
CAT score |
E-RS Total score |
|||||||
| Age | Years | 75.1 | 6.8 | 89.0 | 51.0 | - | - | - | |
| BMI | kg/m2 | 22.7 | 3.3 | 35.7 | 14.0 | - | - | - | |
| Cumulative Smoking | pack-years | 57.7 | 30.9 | 204.0 | 10.0 | - | - | - | |
| SVC | % pred. | 95.7 | 18.1 | 145.9 | 56.7 | -0.250** | -0.207** | -0.203* | |
| FEV1 | % pred. | 69.8 | 20.4 | 132.5 | 21.8 | -0.340*** | -0.335*** | -0.381*** | |
| FEV1/FVC | % | 56.3 | 10.8 | 69.9 | 22.4 | -0.251** | -0.311*** | -0.391*** | |
| RV1) | % pred. | 125.1 | 63.7 | 718.9 | 28.4 | - | 0.189* | 0.214** | |
| RV/TLC1) | % | 44.9 | 9.7 | 85.1 | 18.1 | - | 0.242** | 0.258** | |
| DLco2) | % pred. | 53.4 | 20.6 | 163.9 | 8.0 | -0.183* | -0.285*** | -0.248** | |
| PaO23) | mmHg | 79.2 | 8.9 | 101.8 | 56.6 | -0.188* | -0.301*** | -0.289*** | |
| SGRQ Total Score | (0-100) | 22.8 | 15.3 | 63.1 | 0.9 | 0.602*** | 0.667*** | 0.636*** | |
| SGRQ Symptoms | (0-100) | 37.9 | 20.0 | 85.3 | 0.0 | 0.508*** | 0.549*** | 0.586*** | |
| SGRQ Activity | (0-100) | 32.1 | 23.6 | 87.2 | 0.0 | 0.553*** | 0.616*** | 0.578*** | |
| SGRQ Impact | (0-100) | 13.1 | 13.1 | 55.2 | 0.0 | 0.533*** | 0.553*** | 0.519*** | |
| Hyland Scale score | (0-100) | 66.6 | 16.0 | 100 | 20.0 | -0.381*** | -0.513*** | -0.437*** | |
| D-12 Total score | (0-36) | 1.5 | 2.6 | 15.0 | 0.0 | NA | 0.603*** | 0.655*** | |
| CAT score | (0-40) | 9.1 | 6.7 | 27.0 | 0.0 | 0.603*** | NA | 0.675*** | |
| E-RS Total score | (0-40) | 5.2 | 5.2 | 24.0 | 0.0 | 0.655*** | 0.675*** | NA | |
***: p < 0.001, **: p < 0.01, *: p < 0.05; 1) n=156, 2) n=154, 3) one patient receiving oxygen. Missing values of correlation coefficients indicate no statistically significant relationship. D-12, Dyspnoea-12; CAT, the COPD Assessment Test; E-RS, Evaluating Respiratory Symptoms in COPD; SGRQ, the St. George’s Respiratory Questionnaire; NA, not available. The numbers in parentheses denote possible score range.
Table 2.
Comparison of Patient Characteristics and the Scores Obtained from Patient-Reported Outcomes at Baseline by Airflow Limitation Severity in 157 Subjects with COPD.
Table 2.
Comparison of Patient Characteristics and the Scores Obtained from Patient-Reported Outcomes at Baseline by Airflow Limitation Severity in 157 Subjects with COPD.
| Stage 1 (n=53) | Stage 2 (n=79) | Stage 3+4 (n=25) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| mean | SD | mean | SD | mean | SD | ||||||||||
| Age | years | 75.5 | ± | 6.6 | 74.8 | ± | 7.0 | 74.7 | ± | 6.7 | |||||
| BMI | kg/m2 | 23.1 | ± | 2.8 | 22.9 | ± | 3.6 | 21.4 | ± | 3.1 | |||||
| Cumulative Smoking | pack-years | 47.4** | ± | 23.3 | 63.5 | ± | 34.0 | 61.4 | ± | 30.5 | |||||
| SVC | % pred. | 109.7*** | ± | 12.6 | 92.0§§§ | ± | 15.8 | 77.8¶¶¶ | ± | 13.0 | |||||
| FEV1 | % pred. | 91.7*** | ± | 10.1 | 64.9§§§ | ± | 9.1 | 38.7¶¶¶ | ± | 8.7 | |||||
| FEV1/FVC | % | 63.7*** | ± | 4.9 | 56.4§§§ | ± | 8.4 | 40.2¶¶¶ | ± | 9.2 | |||||
| RV1) | % pred. | 108.5 | ± | 31.5 | 122.0§§§ | ± | 47.4 | 169.3¶¶ | ± | 119.0 | |||||
| RV/TLC1) | % | 39.3*** | ± | 7.3 | 45.4§§§ | ± | 8.8 | 54.7¶¶¶ | ± | 8.7 | |||||
| DLco2) | % pred. | 58.9* | ± | 14.3 | 53.5§§§ | ± | 23.1 | 41.4¶ | ± | 19.3 | |||||
| PaO23) | mmHg | 81.7 | ± | 8.9 | 79.2§§ | ± | 8.9 | 74.4¶ | ± | 6.9 | |||||
| SGRQ Total Score | (0-100) | 15.0** | ± | 9.9 | 22.7§§§ | ± | 14.3 | 40.0¶¶¶ | ± | 13.9 | |||||
| SGRQ Symptoms | (0-100) | 31.2 | ± | 16.3 | 37.0§§§ | ± | 19.9 | 54.9¶¶¶ | ± | 17.9 | |||||
| SGRQ Activity | (0-100) | 20.4** | ± | 19.0 | 31.7§§§ | ± | 21.4 | 58.1¶¶¶ | ± | 18.2 | |||||
| SGRQ Impact | (0-100) | 7.1* | ± | 7.7 | 13.3§§§ | ± | 12.7 | 25.1¶¶ | ± | 15.1 | |||||
| Hyland Scale Score | (0-100) | 72 | ± | 15 | 67§§§ | ± | 15 | 54¶¶ | ± | 14 | |||||
| D-12 Total Score | (0-36) | 0.8 | ± | 1.8 | 1.4§§§ | ± | 2.3 | 3.7¶¶ | ± | 3.9 | |||||
| CAT Score | (0-40) | 7.0 | ± | 5.4 | 8.3§§§ | ± | 6.1 | 16.3¶¶¶ | ± | 6.7 | |||||
| E-RS Total Score | (0-40) | 3.4 | ± | 3.5 | 4.8§§§ | ± | 5.0 | 10.2¶¶¶ | ± | 6.0 | |||||
| in comparison between Stage 1 and Stage 2 (Steel-Dwass test), ***: p < 0.001, **: p < 0.01, *: p < 0.05 | |||||||||||||||
| in comparison between Stage 2 and Stage 3+4 (Steel-Dwass test), §§§: p < 0.001, §§: p < 0.01, §: p < 0.05 | |||||||||||||||
| in comparison between Stage 1 and Stage 3+4 (Steel-Dwass test), ¶¶¶: p < 0.001, ¶¶: p < 0.01, ¶: p < 0.05 | |||||||||||||||
| 1) n=156, 2) n=154, 3) one patient receiving oxygen. SGRQ, the St. George’s Respiratory Questionnaire; D-12, Dyspnoea-12; CAT, the COPD Assessment Test; E-RS, Evaluating Respiratory Symptoms in COPD. The numbers in parentheses denote possible score range. | |||||||||||||||
Table 3.
Internal Consistency and Score Distribution in the Questionnaires.
| Patient-reported outcomes | possible score range |
items | score distribution | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n) | Mean | SD | median | 75th percentile |
25th percentile |
max. | min. | floor effect |
ceiling effect |
|||
| D-12 Total score | 0-36 | 12 | 1.5 | 2.6 | 1.0 | 2.0 | 0.0 | 15.0 | 0.0 | 47.8% | 0% | |
| D-12 Physical score | 0-21 | 7 | 1.4 | 2.1 | 1.0 | 2.0 | 0.0 | 10.0 | 0.0 | 48.4% | 0% | |
| D-12 Affective score | 0-15 | 5 | 0.2 | 0.9 | 0.0 | 0.0 | 0.0 | 5.0 | 0.0 | 93.6% | 0% | |
| CAT score | 0-40 | 8 | 9.1 | 6.7 | 8.0 | 13.0 | 3.0 | 27.0 | 0.0 | 5.1% | 0% | |
| E-RS Total score | 0-40 | 11 | 5.2 | 5.2 | 4.0 | 8.0 | 1.0 | 24.0 | 0.0 | 19.7% | 0% | |
| RS-Breathlessness | 0-17 | 5 | 2.3 | 3.2 | 0.0 | 4.0 | 0.0 | 15.0 | 0.0 | 50.3% | 0% | |
| RS-Cough & Sputum | 0-11 | 3 | 1.9 | 1.7 | 2.0 | 3.0 | 0.0 | 7.0 | 0.0 | 32.5% | 0% | |
| RS-Chest Symptoms | 0-12 | 3 | 1.0 | 1.6 | 0.0 | 2.0 | 0.0 | 6.0 | 0.0 | 60.5% | 0% | |
D-12, Dyspnoea-12; CAT, COPD Assessment Test; E-RS, Evaluating Respiratory Symptoms in COPD.
Table 4.
Morbidity Distribution in the Venn Diagram.
| Real-world clinic n (%) |
on the hypothesis | |||||
|---|---|---|---|---|---|---|
| D-12 | ∩ | E-RS | ∩ | CAT | 30 (19.1%) | present, a centrical position |
| ∩ | E-RS | ∩ | CAT | 19 (12.1%) | possible | |
| ∩ | ∩ | CAT | 11 (7.0%) | possible | ||
| ∩ | E-RS | ∩ | 10 (6.4%) | no | ||
| D-12 | ∩ | E-RS | ∩ | 6 (3.8%) | no | |
| D-12 | ∩ | ∩ | 6 (3.8%) | no | ||
| D-12 | ∩ | ∩ | CAT | 1 (0.6%) | no | |
| ∩ | ∩ | 74 (47.1%) | present |
D-12, Dyspnoea-12; CAT, COPD Assessment Test; E-RS, Evaluating Respiratory Symptoms in COPD.
Table 5.
Concordant and Discordant Results between Tools Using the Thresholds.
| COPD assessment test (CAT) and Evaluating Respiratory Symptoms in COPD (E-RS) | |||
| E-RS Total Score | |||
| 0-4 | 5 or more | ||
| CAT Score | 0-9 | 80 (51.0%) | 16 (10.2%) |
| 10 or more | 12 (7.6%) | 49 (31.2%) | |
| COPD assessment test (CAT) and Dyspnoea-12 (D-12) | |||
| D-12 Total Score | |||
| 0-1 | 2 or more | ||
| CAT Score | 0-9 | 84 (53.5%) | 12 (7.6%) |
| 10 or more | 30 (19.1%) | 31 (19.7%) | |
| Evaluating Respiratory Symptoms in COPD (E-RS) and Dyspnoea-12 (D-12) | |||
| D-12 Total Score | |||
| 0-1 | 2 or more | ||
| E-RS Total Score | 0-4 | 85 (54.1%) | 7 (4.5%) |
| 5 or more | 29 (18.5%) | 36 (22.9%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



