
Submitted:
14 June 2023
Posted:
14 June 2023
You are already at the latest version
Abstract
Current nutritional guidelines for stomach cancer survivors (SCS) mainly focus on the influence of surgical resection of the stomach, with limited guidance regarding a wider range of food options. We aimed to investigate the factors associated with healthier dietary changes in Korean adult SCS. This cross-sectional study assessed dietary pattern change after cancer treatment for 11 food categories, using a self-administered questionnaire. A ‘healthier dietary change’ was operationally defined as reduced consumption of red and processed meat, grains, salt, and burnt food, and increased consumption of poultry, fish, vegetables, fruits, legumes, and dairy products. Among a total of 624 SCS, approximately 60% of participants reported healthier directional dietary changes in three or more food categories, while 9.1% reported no changes. There was no significant difference in dietary habit changes between surgery types. Multivariable adjusted analysis showed that elderly and long-term survivors were inversely associated with a healthier dietary change. SCS with higher educational achievement and income were more likely to make healthier changes in their intake of processed meat, vegetables, fruits, burnt food, or salt. SCS with higher levels of fear of cancer recurrence, anxiety, or depression were more likely to follow healthier dietary changes for fish, meat, fruits, grains, or burnt food. Change in dietary pattern varied across different food items and was associated with various characteristics of SCS. It is crucial to repeatedly provide SCS with information about healthier dietary patterns, considering their sociodemographic, clinical, and psychological characteristics.
Keywords:
Stomach cancer survivor
; Dietary habit change
; Nutritional guideline
1. Introduction
Stomach cancer is globally ranked as the fifth in terms of cancer incidence and the fourth in terms of cancer mortality. The Eastern Asian population, in particular, exhibits a higher incidence of stomach cancer [1]. In Korea, 25,768 new cases of stomach cancer were registered in 2021 [2]. Notably, the 5-year survival rate of stomach cancer patients has remarkably improved from 43.9% in 1993-1995 to 77.5% in 2015-2019 [3]. This improvement can be attributed to advancements in early diagnosis and treatment strategy, leading to an increasing number of stomach cancer survivors (SCS). SCS often face challenges related to inadequate dietary and nutritional intake, primarily resulting from surgical resection of the stomach. Commonly reported health problems [4,5] of SCS include weight loss, dyspepsia, gastrointestinal reflux disease, dumping syndrome, anemia, and osteoporosis [6,7]. Some of these health issues are closely related to the malabsorption of essential minerals such as vitamins, calcium, and iron [8]. Consequently, SCS have unique dietary needs [4] emphasizing the need for evidence-based guidelines specifically tailored to SCS, addressing dietary consumptions. Such guidelines are crucial for maintaining optimal nutritional status, preventing the development of new diseases, reducing cancer-specific and overall mortality, and enhancing the quality of life of SCS.
Despite the growing body of evidence highlighting the need for dietary support among cancer survivors [9], it seems unclear whom to target and how to effectively recommend modification in dietary patterns. Current guidelines suggest that cancer survivors should follow a prudent and healthy dietary pattern, incorporating and adequate balance of macro- and micro-nutrient content derived from plant-based food characterized by a higher intake of fruits, vegetables, cereals, nuts, legumes, and nonfat dairy products [10]. Nutritional management of patients with stomach cancer mainly revolves around the extent of surgical resection of the stomach with the involvement of the esophageal or pyloric sphincter [11]. SCSs are often advised to eat smaller, more frequent meals or snacks than three times a day, restrict concentrated sweets and drink fluids between meals. However, comprehensive and specific professional information about healthy dietary intake after stomach cancer treatment has been scarcely available. Therefore, SCSs who are eager to change their dietary intake toward a healthier direction tend to resort to internet browsing or public media [12]. Regrettably, this approach often ends up with following unscientific advice that may be potentially harmful [13]. It is widely recognized that cancer survivors are likely to encounter multiple barriers that impact their adherence to nutritional recommendations, such as clinical, social, environmental, and structural barriers [14,15,16]. Therefore, helping survivors make sustainable behavior change to follow the guideline with consideration of barrier factors would be also important. However, there is a lack of evidence regarding which factors are associated with dietary behavioral change among SCS. Besides, given the difference in dietary patterns between Western and Asian people, the development of specific guidelines for desirable dietary intake of Asian cancer survivors would be necessary [17].
In this regard, we conducted this study to investigate how the Korean SCS change their dietary intake pattern after completion of cancer treatment. We also evaluated the factors associated with healthier dietary intake change of Korean SCS.
2. Materials and Methods
2.1. Study participants
Participants of this cross-sectional study were a total of 624 Korean adults (≥19 years) SCS who had completed primary cancer treatment. We recruited study participants at two university-affiliated hospitals between September 2014 and February 2017. The recruitment was irrespective of the time elapsed since the initial cancer diagnosis when they visited the hospitals for routine surveillance after cancer treatment or seeking consultations for health issues. These two hospitals are reported to provide medical services to around 20% of Korean cancer patients. Among the initially enrolled 689 SCS, we excluded 65 due to the following reasons: those who had multiple cancers (n=40); who had recurrent or metastatic cancer (n=7); and who did not receive surgery (n=2) or any treatment (n=8); who did not respond to questions asking dietary habits (n=8).
2.2. Dietary intake pattern
We assessed dietary pattern change across 11 specific food categories and meal size in total by using a self-administered questionnaire with five response levels (decreased a lot, decreased somewhat, not changed, increased somewhat, increased a lot). We asked study participants if there had been a change in the frequency of intake for 11 predetermined food items after cancer treatment. The 11 individual food categories included red meat (pork and beef), poultry (chicken and duck), processed meat (sausage, ham, and bacon), fish, vegetable, fruit, bean, dairy product, grain, salt, and burned food. We did not survey refined grains separately from whole grains. Additionally, participants were asked if there had been any changes in the overall meal size after cancer treatment.
In accordance with the cancer prevention recommendations of World Cancer Research Fund(WCRF)/ American Institute for Cancer Research (AICR) [18], we established the “healthier dietary change” as follows: 1) reduced consumption of red and processed meat, grains, salt, and burnt food 2) increased consumption of poultry, fish, vegetable, fruit, legume, and dairy product as valuable sources of protein and micronutrients. we set the decrease in grain intake as a healthier dietary change, given that Asians tend to daily consume extremely high-carbohydrate diets (>70% of energy) consisting of various refined grains like white rice and noodles [19,20], compared with the western population [21]. In addition, we calculated a dietary change score for each participant by tallying the total number of dietary changes toward a healthier direction across 11 individual food categories.
2.3. Other study variables
Cancer-related clinical information was obtained through a review of medical records, which includes age at cancer diagnosis, time since cancer diagnosis (< 1 year, 1-<5 years, 5-<10 years, and ≥ 10 years), cancer stage (I, II, III or IV), and cancer treatments received (surgery, chemotherapy, or radiotherapy). The surgical procedures encompassed various stomach operations, such as total gastrectomy, subtotal gastrectomy, wedge resection, and endoscopic submucosal dissection. We collected data on preoperative weight and height by reviewing medical records. Weight and height at the time of survey were measured to the nearest 0.1kg and 0.1cm, respectively. The measurements were taken with a standardized scale and stadiometer, while participants were wearing light clothing and no shoes. Subsequently, we calculated body mass index (BMI) as weight divided by height squared (kg/m2), which was categorized into four groups (< 18.5 kg/m2, 18.5-22.9 kg/m2, 23-24.9 kg/m2, and ≥ 25 kg/m2) [22].
We collected information on sociodemographic and psychological factors by using a self-administered questionnaire. Marital status was assessed by determining whether the participant was living with their spouse/partner or not. Household monthly income was categorized into three groups (≥ 4,000,000 won, 2,000,000-3,999,999 won, or < 2,000,000 won). Educational achievement was categorized into three groups (≤ middle school, high school, ≥ college), considering the Korean education system. Smoking status was classified into three groups: never, ex-smoker, and current smoker. Alcohol consumption was classified into two groups: current and non-current drinking.
To evaluate the participant’s psychological status, we utilized the Korean version of the Hospital Anxiety and Depression Scale (HADS) to assess participants’ psychological status. The HADS is a validated self-rating report assessment comprising fourteen items designed to measure anxiety (HADS-A) and depression (HADS-D) [23]. We adopted HADS-A and HADS-D ≥8 as a cut-off value for detecting anxiety and depression [23]. The severity subscale of fear of cancer recurrence index (K-FCRI), known as the short form of FCRI, was employed to assess the fear of cancer recurrence. Cronbach’s alpha coefficient for the FCRI short-form Korean version was 0.77 [24], indicating good internal consistency. A score ≥13 on the severity subscale (short-form FCRI) was used as a cut-off score to determine clinically significant levels, following the recommendation by Simard et al. [25].
2.4. Statistical analysis
We investigated whether changes in dietary patterns after cancer diagnosis varied based on the age at cancer diagnosis and the time lapse after cancer diagnosis, using the chi-square test. Furthermore, we analyzed the association between healthier dietary pattern changes after cancer diagnosis with various sociodemographic, clinical, and psychological factors by estimating odds ratio (OR) and 95% confidence intervals (CI) from multiple logistic regression analysis. SPSS version 24 (IBM Corp., Armonk, NY, USA) and SAS software 9.4 (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses. A two-sided p-value of less than 0.05 (< 5%) was considered statistically significant for all analyses.
3. Results
3.1. Baseline characteristics
Out of the total 624 participants, 58% were male, and the mean age at the time of survey was 59.2 ± 9.9 years old. The mean age at cancer diagnosis was 52.5 ± 10.2 years old, and the mean duration since cancer diagnosis was 6.7 ± 3.0 years. Stage 1 stomach cancer occupied 67.8% of the cases. All participants underwent surgical treatment, with 28.7% also receiving chemotherapy and 12.2% receiving radiotherapy in addition. Biloth-1 subtotal gastrectomy was the most common type of surgery, followed by total gastrectomy (22.8%) and Biloth-2 subtotal gastrectomy. (Table 1).

Table 1.
Sociodemographic and clinical characteristics of study participants: 624 Korean stomach cancer survivors.
Table 1.
Sociodemographic and clinical characteristics of study participants: 624 Korean stomach cancer survivors.
| Sociodemographic characteristics | |
| Age | 59.2 ± 9.9 |
| < 55 years | 190 (30.4) |
| 55 - < 60 years | 129 (20.7) |
| 60 - < 65 years | 140 (22.4) |
| ≥ 65 years | 165 (26.4) |
| Male | 362 (58.0) |
| Live with spouse/ or partner | 530 (84.9) |
| Monthly household income | |
| < 2 million Won | 89 (14.3) |
| 2 - < 4 million Won | 134 (21.5) |
| ≥ 4 million Won | 217 (34.8) |
| Unknown | 184 (29.5) |
| Education achievement | |
| ≤ Middle school | 70 (11.2) |
| High school | 211 (33.8) |
| ≥ College | 189 (30.3) |
| Unknown | 154 (24.7) |
| Smoking status | |
| Never smoking |
352 (56.4) |
| Ex-smoking | 230 (36.9) |
| Current smoking | 30 (4.8) |
| Unknown | 12 (1.9) |
| Alcohol consumption | |
| Non-current drinking | 442 (70.8) |
| Current drinking | 182 (29.2) |
| Clinical characteristics | |
| Age at cancer diagnosis | 52.5 ± 10.2 |
| < 45 years | 138 (22.1) |
| 45 - < 55 years | 231 (37.0) |
| ≥ 55 years | 255 (40.9) |
| Lapse after diagnosis | 6.7 ± 3.0 |
| < 1 years | 14 (2.2) |
| 1 - < 5 years | 152 (24.4) |
| 5 - < 10 years | 395 (63.3) |
| ≥ 10 years | 63 (10.1) |
| Stage of Cancer | |
| Stage 0 | 7 (1.1) |
| Stage 1 | 423 (67.8) |
| Stage 2 | 102 (16.3) |
| Stage 3 | 60 (9.6) |
| Stage 4 | 9 (1.4) |
| Unknown | 23 (3.7) |
| Type of surgery received | |
| Total gastrectomy 14 |
142 (22.8) |
| Subtotal gastrectomy | 470 (75.3) |
| Biloth-1 subtotal gastrectomy | 328 (52.8) |
| Biloth-2 subtotal gastrectomy | 75 (12.0) |
| Pylorus preserving surgery | 63 (10.1) |
| Not specifically stated | 4 (0.6) |
| Wedge resection | 6 (1.0) |
| Endoscopic submucosal dissection | 3 (0.5) |
| Unknown | 3 (0.5) |
| Type of cancer treatment received | |
| Chemotherapy | 179 (28.7) |
| Radiotherapy | 76 (12.2) |
| Preoperative, body mass index | 23.8 ± 3.1 |
| < 18.5 kg/m2 | 13 (2.1) |
| 18.5 - 22.9 kg/m2 | 252 (40.4) |
| 23 - 24.9 kg/m2 | 140 (22.4) |
| ≥ 25 kg/m2 | 198 (31.7) |
| Unknown | 21 (3.4) |
| Psychological characteristics | |
| High fear of cancer recurrence (FCRI ≥ 13) | 206 (33.0) |
| Depression (HADS-D ≥ 8) | 270 (43.3) |
| Anxiety (HADS-A ≥ 8) | 91 (14.6) |
FCRI, Fear of Cancer Recurrence Inventory.
3.2. Distribution of Dietary habit change
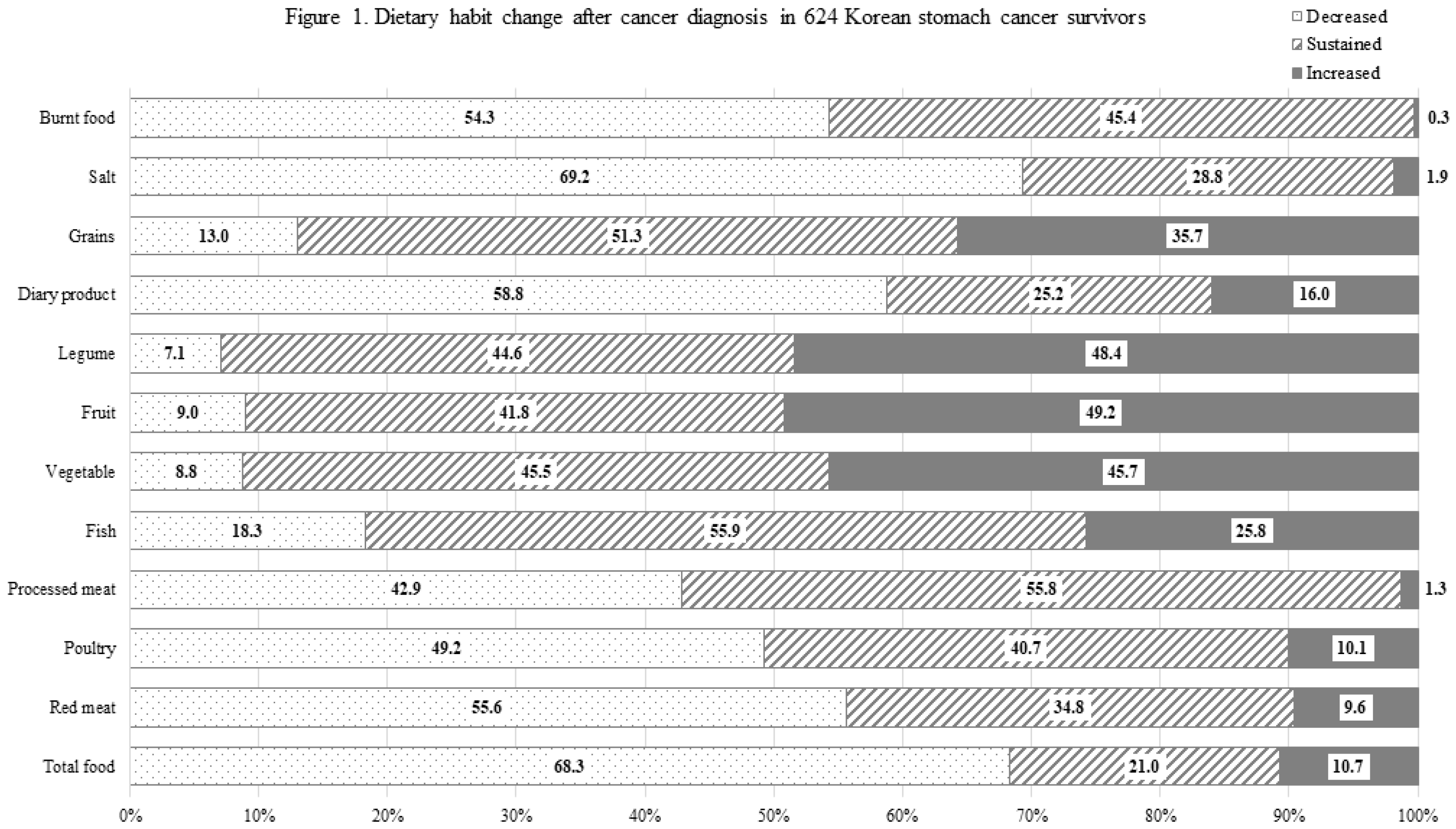
Approximately two-thirds (68.3%) of participants reported a reduction in their overall food consumption. Around half of the participants indicated a decrease in the intake of red meat, processed meat, poultry, dairy product, salt, and burnt food. Conversely, around half of the participants also reported an increase intake of vegetables, fruits, and legumes. The most common food category for which healthier dietary change was reported was salt, followed by red meat, burnt food, fruit, legume, vegetable, and processed meat (Figure 1). Around 60% experienced a shift towards a heathier dietary pattern in three or more categories of food, while 9.1% did not report any positive dietary change. With increasing age at cancer diagnosis, the number of food items changed into a healthier intake pattern tended to decrease (P trend<0.05) (Supplementary Figure S1). Reduction of total food intake was most common in SCS who received pylorus-preserving gastrectomy (79.4%), followed by total gastrectomy (73.9%), Biloth-2 subtotal gastrectomy (70.7%), and Biloth-2 subtotal gastrectomy (64.6%). There was no significant difference in dietary habit changes between surgery types. (Supplementary Table S1).
Figure 1.
Dietary habit change after cancer diagnosis in 624 Korean stomach cancer survivors.
3.3. Dietary habit change stratified by age and time lapse after cancer diagnosis
As the age at cancer diagnosis increased, a higher proportion of participants, especially female SCS, reduced vegetables and fruit intake. On the other hand, fewer participants, regardless of sex, reduced the intake of processed meat and burnt food as their age at cancer diagnosis increased. In males, the proportion of SCS who reduced salt intake decreased with an increase in age at cancer diagnosis. (Supplementary Table S2)
Regarding the time lapse after cancer diagnosis increased, more participants, particularly female SCS, maintained or increased their intake of vegetables, fruits, and legumes compared to the preoperative period. Conversely, as the time lapse after the cancer diagnosis increased, fewer participants reduced the intake of salt and grain, and this trend was evident only in male SCS. However, there were no significant changes in the intake of red meat, processed meat, poultry, fish, and burnt food with the increase in the time lapse after cancer diagnosis. (Supplementary Table S3)
3.4. Factors associated with dietary habit changes toward healthier directions
Table 2 presents the multivariable-adjusted association between changes in dietary patterns towards healthier directions after cancer diagnosis with various sociodemographic, clinical, and psychological factors. Each 1-year increase in age was inversely associated with the healthier dietary change in consumption of poultry, processed meat, vegetable, fruit, legume, and burnt food. Female SCS exhibited a decreased likelihood reducing burnt food intake compared to male SCS. SCS who were living with a spouse were less inclined to reduce grain intake compared to those without a spouse. SCS with higher levels of educational achievement were more likely to change their dietary habits towards healthier direction in terms of processed meat, vegetable, fruit, and burnt food, compared to those with lower education levels. Participants with higher incomes tended to change their dietary habits toward a healthier direction for the intake of vegetables, fruit, and salt.
As the time elapse after the cancer diagnosis increased, SCS were less likely to increase their intake of fish and less likely to reduce their intake of grains. SCS who underwent biloth-1 subtotal gastrectomy were more likely to increase their vegetable intake compared to those who had total gastrectomy. SCS who received chemotherapy were more likely to increase their poultry consumption, whereas those who received radiotherapy were less likely to increase their poultry consumption. Participants who were overweight or obese at cancer diagnosis showed a higher probability of reducing their intake of red meat, processed meat, and grains than the participants who were normal or underweight.
Furthermore, participants with higher FCR were more likely to increase their intake of fish and fruits compared to those with lower FCR. Participants with anxiety had a greater likelihood of reducing their grain consumption, while those with depression were more likely to reduce red meat, processed meat, and burnt food consumption.
Table 2.
Factors associated with the dietary habit change toward healthier direction: 624 Korean stomach cancer survivors.
Table 2.
Factors associated with the dietary habit change toward healthier direction: 624 Korean stomach cancer survivors.
| Variable | Decreased Red meat |
Increased Poultry |
Decreased Processed meat |
Increased Fish |
Increased Vegetable |
Increased Fruit |
Increased Legume |
Increased Dairy product |
Decreased Grains |
Decreased Salt |
Decreased Burnt food |
| Sociodemographic characteristics | |||||||||||
| Age at the time of cancer diagnosis | |||||||||||
| < 45 years | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 45 - < 55 years | 1.37 (0.85, 2.19) |
0.77 (0.38, 1.54) |
0.68 (0.41, 1.11) |
1.77 (1.05, 2.98) |
0.68 (0.41, 1.11) |
0.87 (0.53, 1.44) |
0.69 (0.41, 1.13) |
1.44 (0.78, 2.66) |
0.78 (0.38, 1.59) |
1.16 (0.68, 1.98) |
0.96 (0.57, 1.62) |
| ≥ 55 years | 1.56 (0.92, 2.63) |
0.43 (0.19, 1.01) |
0.41 (0.24, 0.71) |
0.82 (0.45, 1.50) |
0.43 (0.24, 0.74) |
0.46 (0.26, 0.80) |
0.47 (0.27, 0.82) |
1.23 (0.61, 2.48) |
0.90 (0.42, 1.95) |
0.94 (0.53, 1.67) |
0.54 (0.31, 0.96) |
| Continuous, increase by 1 year | 1.01 (0.99, 1.04) |
0.96 (0.93, 0.99) |
0.97 (0.95, 0.99) |
0.99 (0.96, 1.01) |
0.97 (0.94, 0.99) |
0.96 (0.94, 0.98) |
0.96 (0.94, 0.98) |
0.99 (0.97, 1.02) |
0.99 (0.96, 1.02) |
0.99 (0.97, 1.01) |
0.97 (0.95, 0.99) |
| Female (vs. Male) | 1.01 (0.61, 1.66) |
0.94 (0.41, 2.12) |
1.01 (0.59, 1.73) |
1.22 (0.66, 2.26) |
0.86 (0.50, 1.49) |
0.76 (0.44, 1.30) |
1.15 (0.67, 1.97) |
0.91 (0.46, 1.82) |
1.14 (0.53, 2.45) |
1.35 (0.79, 2.29) |
0.54 (0.31, 0.93) |
| Live with spouse (vs. without spouse) | 1.05 (0.61, 1.80) |
0.77 (0.34, 1.70) |
1.51 (0.83, 2.74) |
1.03 (0.53, 1.98) |
1.16 (0.65, 2.09) |
1.07 (0.60, 1.92) |
1.01 (0.56, 1.83) |
0.61 (0.31, 1.19) |
0.44 (0.21, 0.91) |
1.02 (0.55, 1.86) |
0.90 (0.50, 1.63) |
| Education achievement | |||||||||||
| ≤ Middle school | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| High school | 1.08 (0.59, 1.99) |
0.91 (0.34, 2.42) |
1.07 (0.58, 1.99) |
1.28 (0.63, 2.59) |
1.99 (1.07, 3.73) |
1.55 (0.84, 2.86) |
1.55 (0.83, 2.88) |
1.57 (0.68, 3.64) |
0.34 (0.16, 0.73) |
1.25 (0.65, 2.39) |
1.92 (1.03, 3.56) |
| ≥ College | 1.01 (0.53, 1.94) |
1.33 (0.48, 3.74) |
2.49 (1.28, 4.84) |
2.15 (1.02, 4.53) |
2.64 (1.35, 5.18) |
2.16 (1.11, 4.20) |
1.07 (0.58, 1.99) |
1.56 (0.64, 3.79) |
0.30 (0.13, 0.70) |
1.29 (0.64, 2.62) |
1.90 (0.97, 3.71) |
| Monthly Household Income | |||||||||||
| < 2millions, Won | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 2 - < 4millions, Won | 1.34 (0.74, 2.44) |
1.56 (0.59, 4.12) |
1.79 (0.95, 3.36) |
1.70 (0.85, 3.38) |
2.17 (1.16, 4.04) |
2.18 (1.17, 4.07) |
1.55 (0.83, 2.88) |
1.71 (0.79, 3.70) |
1.44 (0.61, 3.42) |
2.07 (1.09, 3.96) |
1.39 (0.74, 2.62) |
| ≥ 4millions, Won | 1.35 (0.75, 2.45) |
0.89 (0.33, 2.42) |
1.76 (0.95, 3.29) |
1.12 (0.57, 2.23) |
1.20 (0.65, 2.20) |
1.11 (0.54, 2.29) |
1.07 (0.58, 1.99) |
1.20 (0.55, 2.61) |
1.79 (0.76, 4.22) |
2.03 (1.08, 3.81) |
1.28 (0.68, 2.40) |
| Smoking status | |||||||||||
| Never smoking | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Ex-smoking | 1.28 (0.78, 2.11) |
0.94 (0.40, 2.20) |
1.05 (0.62, 1.80) |
1.79 (0.99, 3.25) |
1.49 (0.87, 2.55) |
1.28 (0.75, 2.19) |
1.33 (0.78, 2.27) |
0.94 (0.47, 1.87) |
1.05 (0.49, 2.25) |
1.19 (0.70, 2.02) |
1.26 (0.73, 2.18) |
| Current smoking | 0.88 (0.37, 2.06) |
1.02 (0.20, 5.22) |
0.83 (0.33, 2.12) |
1.24 (0.45, 3.41) |
0.79 (0.14, 4.41) |
0.58 (0.23, 1.47) |
1.05 (0.42, 2.61) |
1.15 (0.36, 3.65) |
0.68 (0.17, 2.75) |
0.57 (0.24, 1.38) |
0.73 (0.28, 1.90) |
| Alcohol consumption | |||||||||||
| Non-current drinking | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Current drinking | 1.13 (0.75, 1.70) |
0.28 (0.12, 0.67) |
1.14 (0.74, 1.75) |
1.00 (0.63, 1.60) |
0.96 (0.62, 1.48) |
0.94 (0.61, 1.45) |
0.71 (0.46, 1.10) |
0.61 (0.34, 1.09) |
1.69 (0.92, 3.11) |
1.11 (0.71, 1.73) |
1.54 (0.98, 2.42) |
| Clinical characteristics | |||||||||||
| Lapse after diagnosis | |||||||||||
| < 5 years | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 5 - < 10 years | 1.24 (0.39, 3.98) |
0.52 (0.10, 2.85) |
0.93 (0.26, 3.42) |
0.26 (0.07, 0.95) |
2.06 (0.50, 8.56) |
1.10 (0.30, 4.08) |
0.87 (0.25, 3.07) |
0.42 (0.11, 1.60) |
0.30 (0.08, 1.14) |
1.41 (0.38, 5.25) |
2.30 (0.57, 9.29) |
| ≥ 10 years | 1.16 (0.37, 3.62) |
0.45 (0.09, 2.34) |
0.82 (0.23, 2.94) |
0.24 (0.07, 0.84) |
1.99 (0.49, 8.09) |
0.85 (0.23, 3.07) |
0.74 (0.22, 2.56) |
0.32 (0.09, 1.19) |
0.20 (0.05, 0.76) |
0.59 (0.17, 2.09) |
2.34 (0.59, 9.25) |
| Continuous, increase by 1 year | 1.01 (0.96, 1.08) |
0.93 (0.83, 1.04) |
0.98 (0.92, 1.05) |
0.95 (0.89, 1.02) |
1.03 (0.96, 1.10) |
0.96 (0.90, 1.02) |
1.03 (0.96, 1.10) |
0.96 (0.88, 1.04) |
0.85 (0.75, 0.95) |
0.94 (0.88, 1.00) |
0.99 (0.92, 1.05) |
| Cancer stage | |||||||||||
| 0-1 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 2 | 1.23 (0.64, 2.34) |
0.49 (0.16, 1.45) |
1.60 (0.81, 3.16) |
0.65 (0.30, 1.43) |
1.25 (0.62, 2.55) |
1.26 (0.63, 2.53) |
1.29 (0.65, 2.58) |
1.23 (0.50, 3.04) |
2.80 (1.05, 7.47) |
1.64 (0.82, 3.27) |
1.15 (0.56, 2.35) |
| 3-4 | 0.67 (0.32, 1.38) |
0.51 (0.16, 1.69) |
0.86 (0.39, 1.86) |
0.78 (0.33, 1.83) |
0.75 (0.33, 1.69) |
0.96 (0.43, 2.14) |
1.56 (0.71, 3.42) |
1.13 (0.42, 3.08) |
2.92 (0.95, 8.99) |
2.07 (0.91, 4.70) |
1.01 (0.44, 2.33) |
| Surgery type* | |||||||||||
| Total gastrectomy | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Biloth-1 Subtotal gastrectomy | 0.87 (0.55, 1.36) |
0.76 (0.38, 1.55) |
1.17 (0.72, 1.88) |
0.67 (0.40, 1.10) |
1.69 (1.04, 2.74) |
1.17 (0.73, 1.89) |
1.46 (0.91, 2.36) |
0.90 (0.50, 1.62) |
0.71 (0.37, 1.36) |
1.02 (0.63, 1.65) |
0.97 (0.59, 1.58) |
| Biloth-2 Subtotal gastrectomy | 0.87 (0.47, 1.62) |
0.80 (0.29, 2.20) |
0.73 (0.38, 1.42) |
0.84 (0.42, 1.70) |
1.55 (0.80, 3.01) |
1.26 (0.65, 2.43) |
1.34 (0.69, 2.58) |
0.69 (0.28, 1.68) |
0.34 (0.11, 1.02) |
1.37 (0.68, 2.73) |
0.76 (0.39, 1.48) |
| Pylorus preserving surgery | 0.68 (0.35, 1.32) |
0.85 (0.28, 2.56) |
0.64 (0.31, 1.33) |
0.75 (0.34, 1.63) |
1.23 (0.59, 2.56) |
1.01 (0.49, 2.08) |
0.98 (0.48, 2.02) |
0.83 (0.34, 2.05) |
1.06 (0.41, 2.73) |
1.13 (0.54, 2.37) |
1.11 (0.53, 2.31) |
| Chemotherapy recipient (vs. non-chemotherapy recipient) |
1.17 (0.62, 2.19) |
3.06 (1.13, 8.29) |
0.89 (0.45, 1.73) |
1.38 (0.66, 2.91) |
1.45 (0.72, 2.93) |
1.49 (0.74, 2.99) |
0.87 (0.44, 1.72) |
0.65 (0.27, 1.57) |
0.44 (0.16, 1.21) |
0.63 (0.32, 1.22) |
0.88 (0.43, 1.77) |
| Radiotherapy recipient (vs. non-radiotherapy recipient) |
1.03 (0.55, 1.94) |
0.27 (0.09, 0.80) |
0.88 (0.45, 1.70) |
0.59 (0.28, 1.23) |
0.68 (0.35, 1.33) |
0.53 (0.27, 1.05) |
0.59 (0.30, 1.15) |
0.79 (0.32, 1.92) |
0.86 (0.33, 2.23) |
1.51 (0.74, 3.12) |
1.37 (0.68, 2.77) |
| Preoperative body mass index | |||||||||||
| < 23 kg/m2 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| 23 - 24.9 kg/m2 |
1.78 (1.13, 2.80) |
0.75 (0.34, 1.63) |
1.05 (0.64, 1.72) |
0.91 (0.53, 1.57) |
1.43 (0.87, 2.36) |
1.16 (0.71, 1.90) |
0.70 (0.43, 1.15) |
0.69 (0.37, 1.29) |
0.94 (0.45, 1.94) |
0.86 (0.53, 1.40) |
0.73 (0.44, 1.20) |
| ≥ 25 kg/m2 |
2.54 (1.66, 3.89) |
0.71 (0.34, 1.47) |
1.69 (1.08, 2.65) |
1.14 (0.70, 1.87) |
1.35 (0.85, 2.13) |
1.18 (0.75, 1.86) |
0.76 (0.49, 1.19) |
0.61 (0.34, 1.09) |
1.72 (0.94, 3.17) |
1.07 (0.68, 1.69) |
1.06 (0.66, 1.70) |
| Continuous, increase by 1 kg/m2 |
1.08 (1.01, 1.14) |
0.94 (0.85, 1.04) |
1.04 (0.98, 1.11) |
1.05 (0.97, 1.12) |
1.03 (0.97, 1.10) |
1.04 (0.98, 1.11) |
0.96 (0.90, 1.03) |
0.97 (0.90, 1.05) |
1.15 (1.05, 1.26) |
1.00 (0.94, 1.07) |
1.03 (0.96, 1.10) |
| Psychological characteristics | |||||||||||
| High fear of cancer recurrence, FCRI ≥13 (vs. FCRI <13) |
1.07 (0.71, 1.61) |
1.05 (0.55, 2.01) |
1.16 (0.76, 1.76) |
1.58 (1.01, 2.46) |
1.37 (0.90, 2.09) |
1.76 (1.15, 2.70) |
1.49 (0.98, 2.27) |
1.16 (0.96, 2.71) |
0.65 (0.35, 1.22) |
1.30 (0.82, 2.04) |
1.66 (1.06, 2.58) |
| Depression, HADS-D≥8 (vs. HADS-D <8) |
1.55 (1.07, 2.24) |
0.96 (0.53, 1.76) |
1.74 (1.19, 2.56) |
0.92 (0.60, 1.41) |
1.17 (0.79, 1.72) |
1.24 (0.84, 1.82) |
0.95 (0.65, 1.40) |
0.84 (0.51, 1.38) |
1.31 (0.763, 2.26) |
1.08 (0.72, 1.62) |
1.70 (1.14, 2.54) |
| Anxiety, HADS-A≥8 (vs. HADS-A <8) |
1.03 (0.60, 1.76) |
1.12 (0.50, 2.50) |
1.11 (0.64, 1.95) |
1.71 (0.98, 3.01) |
1.43 (0.81, 2.53) |
0.94 (0.53, 1.65) |
0.97 (0.56, 1.70) |
0.87 (0.44, 1.72) |
2.67 (1.32, 5.42) |
1.36 (0.72, 2.54) |
1.01 (0.56, 1.85) |
FCRI, Fear of Cancer Recurrence Inventory; HADS-D, Hospital Anxiety and Depression Scale-Depression; HADS-A, Hospital Anxiety and Depression Scale-Anxiety. * Not specifically stated subtotal gastrectomy (n=4), wedge resection (n=6), Endoscopic submucosal dissection (n=3) were not included in this analysis due to the small number. Data are presented as odd ratio and 95% confidence interval estimated by multiple logistic regression analysis after adjusting for the age at the time of cancer diagnosis, sex, living with spouse, education achievement, income, smoking status, alcohol consumption, lapse after diagnosis, cancer stage, surgery type, chemotherapy, radiotherapy, pre-op body mass index, Fear of Cancer Recurrence Inventory, Hospital Anxiety and Depression Scale-Depression, and Hospital Anxiety and Depression Scale-Anxiety. Bold values denote statistical significant at the p<0.05 level.
4. Discussion
To the best of our knowledge, the present study is the first to investigate the dietary pattern change among SCS after cancer treatment and its associated factors. Our findings revealed that nearly all SCS made dietary pattern changes toward healthier directions for at least one type of food, with over half of them modifying their diet for multiple food categories. Most SCS reported a reduction in total food consumption after their cancer diagnosis, which is consistent with previous finding [26]. A study of Australian cancer survivors from breast, colorectal, and hematological cancers found that 55% of the study participants made dietary changes after their cancer diagnosis [27]. In the Australian study, the most common changes included increased fruit and vegetable intake (36%), followed by reduced intake of red meat (25%), sugar (20%), fat (12%), and dairy product (7%) [27]. The direction of dietary pattern change in our study appears to be similar. However, the proportion of survivors with dietary change was notably higher in our study. We believe this difference could be attributed to the different distribution of cancer types between the two studies, considering the stomach’s significance as a major digestive organ. In fact, SCS exhibited a greater emphasis on calorie intake from potatoes, starches, legumes, seeds, vegetables, and fruits compared to other cancer survivors in previous Korean study [17].
The Continuous Update Project(CUP) conducted by WCRF/AICR argued the potential link between consumption of salt-preserved foods and an increased risk of stomach cancer [28]. The high concentration of sodium chloride in these foods can cause mucosal damage, leading to heightened susceptibility to mutagenesis or cancer development [29,30]. Additionally, a high salt intake may stimulate the colonization of Helicobacter pylori, which is known as the strongest risk factor for stomach cancer [31,32]. In our study, around 70% of SCS reported a reduction in salt intake, ranking it as the most commonly changed dietary item (Figure 1). However, another 30% did not decrease their salt intake and 1.9% even reported an increase in salt intake after their cancer diagnosis. Notably, higher income was strongly associated with a reduced salt intake. We presume that this inverse association between income and salt intake may reflect socioeconomic disparities in access to fresh food [33]. Interestingly, with a longer time lapse after the cancer diagnosis, SCS were significantly less likely to reduce salt intake. This finding indicates that as the duration of survival increases, cancer survivors became less keen on healthcare maintenance. A similar phenomenon has also been observed regarding smoking behaviors [34]. Therefore, it is crucial to consistently provide health education for desirable health behavior regardless of time lapse since a cancer diagnosis.
The WCRF recommends cancer patients limit their of red and processed meat, while encouraging the intake of poultry and fish as a valuable substitute [35]. Consumption of red and processed meat has been suggested to increase the risk of non-cardia stomach cancer [36], Primarily due to the presence of sodium nitrate and nitrite used as preservatives added in products like ham, bacon, and sausage. The compounds can react with amino acids to produce carcinogens such as N-nitro compounds in the stomach [37]. In our study, only 42.9% and 55.6% of SCS reported reducing their intake of processed meat and red meat, respectively, and preoperative overweight or obese patients were more likely to decrease such consumption. In addition, 49.2% of SCS reduced poultry intake, while the influence of poultry and fish on cancer risk is still inconclusive [28], given the role of processed meat and red meat as significant risk factors for colon cancer and atherosclerotic diseases, it is advisable to strongly recommend reducing consumption of processed meat and red meat for SCS, and promoting increased consumption of poultry and fish as a qualified protein sources for them.
There is only limited evidence suggesting that consuming little or no fruit may increase the risk of stomach cancer [38]. Citrus fruits have been proposed to potentially decrease the risk of stomach cardia cancer, perhaps because of their vitamin C content [39]. The effects of vegetables including dietary fiber, and legumes on stomach cancer risk are inconclusive [28]. Despite the lack of definite evidence, supporting the beneficial role of vegetables, fruits and legumes for overall health for SCS could still be encouraged. In our study, around 45% of SCS reported having increased vegetable, fruit, and legume intake, while the remaining 40% maintained as previously. Higher levels of education and income and higher fear of cancer recurrence were positively associated with these dietary changes.
The relationship between dairy products and stomach cancer has been scarcely evaluated. However, there is strong evidence that the consumption of dairy products is associated with decreased risk of colorectal cancer but an elevated risk of prostate cancer [18]. Since SCS may have an increased risk for colon cancer as a secondary cancer [40], increasing dairy product consumption may be regarded as a healthier diet in SCS. Notwithstanding, around 60% of SCS reported having reducing their dairy product intake, while only 16% increased their consumption in our study. This finding contrasts with an Australian study where only 7% of participants specifically avoided dairy product [27]. Therefore, it may be necessary to further encourage Korean SCS to increase dairy product intake.
Older adults generally tend to consume less fast food and more fruits and vegetables compared to younger adults [41]. However, our study found that older SCS at the time of cancer diagnosis were less likely to follow healthier directional dietary changes compared to younger SCS. As the age at cancer diagnosis increased, there was a decreasing likelihood to adopt healthier dietary habits by increasing the intake of poultry, vegetables, fruits, and legumes, while there was increasing likelihood of consuming more processed meat and burnt food, even after adjusting for education levels. This may be attributed to gastric resection having a worse influence on older SCSs than younger SCSs, leading to more frequent gastrointestinal problems such as indigestion, and decreased appetite with aging [42]. Thus, it is possible that the higher prevalence of gastrointestinal problems in older SCS explains their lower intake of vegetables and fruits compared to younger SCS. Therefore, healthcare professionals caring for older SCS should pay close attention to gastrointestinal symptoms and signs of malnutrition.
Interestingly, our finding that more of the subjects with higher education changed their dietary habit toward a healthier direction was consistent with the findings of other studies [16,43]. It is well established that individuals with higher socioeconomic status tend to adhere health recommendations better, likely due to the higher chance of health education and greater accessibility to healthcare [44,45]. Therefore, it may be needed to put special efforts to provide health information on healthier dietary intake to cancer survivors who may have limited chance of health education.
With increasing survival time, SCS was more likely to increase grain and salt intake in our study. Similarly, patients who have undergone sleeve gastrectomy for weight reduction reported initial difficulties in consuming certain foods such as red meat, rice, and pasta improved over time [16,46], particularly after 5 years [16,46]. Therefore, health professionals should be kept emphasize the importance of maintaining a healthy diet for long-term cancer survivors.
The nutritional management for individuals who have stomach cancer depends on which part of the stomach was surgically removed or altered [47]. If the pyloric sphincter is affected, it can lead to symptoms such as reflux and rapid food transit through the stomach. Thus, we assumed that the type of surgery would be associated with dietary changes. However, apart from vegetable intake, we did not find significant differences in dietary pattern changes among the various surgical types. This may be partly explained by post-surgical complications like gastrointestinal reflux disease. There also might be a difference in the change of the amount of one portion or the frequency of eating according to surgery type, which we did not investigate in this study.
A balanced and healthy diet has been shown beneficial for relieving cancer survivors’ FCR [48]. In our study, SCS with higher fear of cancer recurrence, anxiety, and depression were more likely to change their dietary intake toward a healthier direction. This finding is compatible with the finding of a Duchy study of colorectal cancer survivors that those who experienced symptoms of anxiety or depression were more likely to express a need for dietary support than those who without such symptoms (27.6% and 28.7%, respectively) [49]. These findings suggest that psychological difficulties of cancer survivors including fear, anxiety, and depression, may serve as motivators for pursuing healthier dietary intake. However, it is crucial to implement strategies that further encourage healthier dietary intake among SCS who suffer from psychological difficulty.
There were several limitations that should be acknowledged in our study. First, we were unable to include a non-cancer group for comparison, which limited our ability to assess differences in dietary habits between cancer survivors and people without cancer. Second, the study was based on a self-reported survey, so there could be recall bias. Third, the evaluation of dietary habit changes was based on tendency rather than precise quantitative measures. Fourth, as a quantitative study, we were unable to investigate the underlying reasons behind the observed associations. Finally, it is a cross-sectional study that hinders accurate causal association. Despite this limitation, our study first attempted to elucidate the factors associated with healthy dietary change in SCS. In addition, we also took into consideration a comprehensive range of variables including socioeconomic and psychological factors in addition to cancer-related factors.
5. Conclusions
The present study confirmed that the majority of SCSs have a strong desire to adopt their dietary pattern toward a healthier direction after the cancer diagnosis. However, as time passes since cancer diagnosis, SCS became less inclined to maintain healthier dietary patterns for certain food items. The changes in dietary patterns differed by depending on the specific food items and were associated with various characteristics of the SCS. Therefore, healthcare professionals responsible for the care of stomach cancer patients should consistently and repeatedly provide evidence-based information regarding healthier dietary patterns after the cancer diagnosis. Additionally, they should take into account the sociodemographic, clinical, and psychological characteristics of the patients to tailor the dietary recommendations effectively.
Supplementary Materials
The following supporting information can be downloaded, Supplementary Table S1. Dietary change after cancer diagnosis according to the subtype of surgical treatment: 608 Korean gastric cancer survivors, Supplementary Table S2. Dietary habit change after cancer diagnosis stratified by sex and age at the cancer diagnosis, Supplementary Table S3. Dietary habit change after cancer diagnosis stratified by sex and lapse after cancer diagnosis.
Author Contributions
Conceptualization, J.P. and Y-M.S.; methodology, J.P. and Y-M.S; formal analysis, J.P. and Y-M.S; investigation, J.P., J.K., and Y-M.S.; resources, D.W.S., J.S., B.C., and Y-M.S; data curation, D.W.S., J.S., B.C., and Y-M.S; writing—original draft preparation, J.P.; writing—review and editing, J.P., J.K., D.W.S, J.S., B.C., and Y-M. S.; visualization, J.P.; supervision, Y-M.S.; funding acquisition, Y-M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (2014R1A2A2A01002705). The funding source had no involvement in the study design, data collection, data analysis, or data interpretation of this study.
Institutional Review Board Statement
The Institutional Review Board (IRB) of Samsung Medical Center (SMC 2013-07-133) and Seoul National University Hospital (H-1407-066-595) approved the study protocol.
Informed Consent Statement
Written informed consent was obtained from all of the participants.
Conflicts of Interest
All of the authors have nothing to declare.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209-49. [CrossRef]
- Jung KW, Won YJ, Hong S, Kong HJ, Im JS, Seo HG. Prediction of Cancer Incidence and Mortality in Korea, 2021. Cancer Res Treat. 2021;53:316-22. [CrossRef]
- Kang MJ, Won YJ, Lee JJ, Jung KW, Kim HJ, Kong HJ, et al. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2019. Cancer Res Treat. 2022;54:330-44. [CrossRef]
- Carrillo GM, Santamaría NP. Life after a gastrectomy: Experience of patients with gastric cancer. Enferm Clin (Engl Ed). 2019;29:27-33. [CrossRef]
- Rha SY, Lee HJ, Lee J. Unmet needs in the physical and daily living domain mediates the influence of symptom experience on the quality of life of gastric cancer patients. Support Care Cancer. 2020;28:1419-31. [CrossRef]
- Jeong SM, Shin DW, Lee JE, Jin SM, Kim S. Increased Risk of Osteoporosis in Gastric Cancer Survivors Compared to General Population Control: A Study with Representative Korean Population. Cancer Res Treat. 2019;51:530-7. [CrossRef]
- Seo GH, Kang HY, Choe EK. Osteoporosis and fracture after gastrectomy for stomach cancer: A nationwide claims study. Medicine (Baltimore). 2018;97:e0532.
- Jones LW, Demark-Wahnefried W. Diet, exercise, and complementary therapies after primary treatment for cancer. The Lancet Oncology. 2006;7:1017-26. [CrossRef]
- Pekmezi DW, Demark-Wahnefried W. Updated evidence in support of diet and exercise interventions in cancer survivors. Acta Oncol. 2011;50:167-78. [CrossRef]
- Rock CL, Thomson CA, Sullivan KR, Howe CL, Kushi LH, Caan BJ, et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J Clin. 2022;72:230-62. [CrossRef]
- Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, Schwartz AL, et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin. 2012;62:243-74. [CrossRef]
- Ghelfi F, Tieri M, Gori S, Nicolis F, Petrella MC, Filiberti A, et al. Do cancer patients change their diet in the e-health information era? A review of the literature and a survey as a proposal for the Italian population. Food Res Int. 2018;104:59-68. [CrossRef]
- Helft PR, Hlubocky F, Daugherty CK. American oncologists’ views of internet use by cancer patients: a mail survey of American Society of Clinical Oncology members. J Clin Oncol. 2003;21:942-7. [CrossRef]
- Ryu SW, Son YG, Lee MK. Motivators and barriers to adoption of a healthy diet by survivors of stomach cancer: A cross-sectional study. Eur J Oncol Nurs. 2020;44:101703. [CrossRef]
- Tollosa DN, Tavener M, Hure A, James EL. Adherence to multiple health behaviours in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv. 2019;13:327-43. [CrossRef]
- Moazzen S, Cortés-Ibañez FO, van Leeuwen BL, Alizadeh BZ, de Bock GH. Assessment of Diet Quality and Adherence to Dietary Guidelines in Gastrointestinal Cancer Survivors: A Cross-Sectional Study. Nutrients. 2020;12. [CrossRef]
- Hoang T, Lee J, Kim J, Park B. Food Intake Behavior in Cancer Survivors in Comparison With Healthy General Population; From the Health Examination Center-based Cohort. J Cancer Prev. 2019;24:208-16. [CrossRef]
- Continuous Update Project Expert Report 2018. Recommendations and Public Health and Policy Implications. World Cancer Research Fund/American Institute for Cancer Research. 2018.
- Song S, Lee JE, Song WO, Paik HY, Song Y. Carbohydrate intake and refined-grain consumption are associated with metabolic syndrome in the Korean adult population. J Acad Nutr Diet. 2014;114:54-62. [CrossRef]
- Park S, Ahn J, Kim NS, Lee BK. High carbohydrate diets are positively associated with the risk of metabolic syndrome irrespective to fatty acid composition in women: the KNHANES 2007-2014. Int J Food Sci Nutr. 2017;68:479-87. [CrossRef]
- Kang Y, Lee K, Lee J, Kim J. Grain Subtype and the Combination of Grains Consumed Are Associated with the Risk of Metabolic Syndrome: Analysis of a Community-Based Prospective Cohort. J Nutr. 2020;150:118-27. [CrossRef]
- Pan WH, Yeh WT. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: an extension of Asian-Pacific recommendations. Asia Pac J Clin Nutr. 2008;17:370-4.
- Beekman E, Verhagen A. Clinimetrics: Hospital Anxiety and Depression Scale. J Physiother. 2018;64:198. [CrossRef]
- Shin J, Goo A, Ko H, Kim JH, Lim SU, Lee HK, et al. Validation Study for the Korean Version of Fear of Cancer Recurrence Inventory. J Korean Med Sci. 2017;32:1792-9. [CrossRef]
- Simard S, Savard J. Screening and comorbidity of clinical levels of fear of cancer recurrence. J Cancer Surviv. 2015;9:481-91. [CrossRef]
- Park B, Lee J, Kim J. Imbalanced Nutrient Intake in Cancer Survivors from the Examination from the Nationwide Health Examination Center-Based Cohort. Nutrients. 2018;10. [CrossRef]
- Tan SY, Wong HY, Vardy JL. Do cancer survivors change their diet after cancer diagnosis? Support Care Cancer. 2021;29:6921-7.
- Continuous Updated Project Diet, Nutrition Physical Activity and Stomach Cancer. World Cancer Research Fund/American Institute for Cancer Research. Revised 2018.
- Charnley G, Tannenbaum SR. Flow cytometric analysis of the effect of sodium chloride on gastric cancer risk in the rat. Cancer Res. 1985;45:5608-16.
- Fang X, Wei J, He X, An P, Wang H, Jiang L, et al. Landscape of dietary factors associated with risk of gastric cancer: A systematic review and dose-response meta-analysis of prospective cohort studies. Eur J Cancer. 2015;51:2820-32. [CrossRef]
- Fox JG, Dangler CA, Taylor NS, King A, Koh TJ, Wang TC. High-salt diet induces gastric epithelial hyperplasia and parietal cell loss, and enhances Helicobacter pylori colonization in C57BL/6 mice. Cancer Res. 1999;59:4823-8.
- Gaddy JA, Radin JN, Loh JT, Zhang F, Washington MK, Peek RM, Jr., et al. High dietary salt intake exacerbates Helicobacter pylori-induced gastric carcinogenesis. Infect Immun. 2013;81:2258-67. [CrossRef]
- Costa BVL, Menezes MC, Oliveira CDL, Mingoti SA, Jaime PC, Caiaffa WT, et al. Does access to healthy food vary according to socioeconomic status and to food store type? an ecologic study. BMC Public Health. 2019;19:775. [CrossRef]
- Walker MS, Vidrine DJ, Gritz ER, Larsen RJ, Yan Y, Govindan R, et al. Smoking relapse during the first year after treatment for early-stage non-small-cell lung cancer. Cancer Epidemiol Biomarkers Prev. 2006;15:2370-7. [CrossRef]
- Food, Nutrition, Physical Activity, and Prevention of Cancer: a Global perspective. World Cancer Research Fund/American Institute for Cancer Research. 2007.
- Doyle C, Kushi LH, Byers T, Courneya KS, Demark-Wahnefried W, Grant B, et al. Nutrition and physical activity during and after cancer treatment: an American Cancer Society guide for informed choices. CA Cancer J Clin. 2006;56:323-53. [CrossRef]
- Iqbal A. Effect of Food on Causation and Prevention of Gastric Cancer. Journal of Cancer Prevention & Current Research. 2017;8. [CrossRef]
- Fruits and vegetables, IARC Handbooks of Cancer Prevention Volume 8. Lyon, France: International Agency for Research on Cancer, World Health Organization; 2003:384.
- Wang Q, Chen Y, Wang X, Gong G, Li G, Li C. Consumption of fruit, but not vegetables, may reduce risk of gastric cancer: results from a meta-analysis of cohort studies. Eur J Cancer. 2014;50:1498-509. [CrossRef]
- Zheng G, Sundquist K, Sundquist J, Chen T, Försti A, Hemminki A, et al. Second Primary Cancers After Gastric Cancer, and Gastric Cancer as Second Primary Cancer. Clin Epidemiol. 2021;13:515-25. [CrossRef]
- Nicklett EJ, Kadell AR. Fruit and vegetable intake among older adults: a scoping review. Maturitas. 2013;75:305-12. [CrossRef]
- Nakazono M, Aoyama T, Komori K, Watanabe H, Kano K, Nagasawa S, et al. The Comparison of the Dietary Intake Loss Between Elderly and Non-Elderly Patients After Gastrectomy for Gastric Cancer. J Gastrointest Cancer. 2023;54:35-43. [CrossRef]
- Thorpe MG, Milte CM, Crawford D, McNaughton SA. Education and lifestyle predict change in dietary patterns and diet quality of adults 55 years and over. Nutr J. 2019;18:67. [CrossRef]
- McMaughan DJ, Oloruntoba O, Smith ML. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front Public Health. 2020;8:231. [CrossRef]
- Zajacova A, Lawrence EM. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu Rev Public Health. 2018;39:273-89. [CrossRef]
- Ruiz-Tovar J, Bozhychko M, Del-Campo JM, Boix E, Zubiaga L, Muñoz JL, et al. Changes in Frequency Intake of Foods in Patients Undergoing Sleeve Gastrectomy and Following a Strict Dietary Control. Obes Surg. 2018;28:1659-64. [CrossRef]
- Brown J, Byers T, Thompson K, Eldridge B, Doyle C, Williams AM. Nutrition during and after cancer treatment: a guide for informed choices by cancer survivors. CA Cancer J Clin. 2001;51:153-87; quiz 89-92. [CrossRef]
- Séguin Leclair C, Lebel S, Westmaas JL. Can Physical Activity and Healthy Diet Help Long-Term Cancer Survivors Manage Their Fear of Recurrence? Front Psychol. 2021;12:647432.
- Ramp D, Mols F, Ezendam N, Beijer S, Bours M, Winkels R, et al. Psychological distress and lower health-related quality of life are associated with need for dietary support among colorectal cancer survivors with overweight or obesity. Support Care Cancer. 2021;29:7659-68. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



