
Submitted:
15 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
The information society has transformed human life. Technology is almost everywhere, including health and education. For example, years ago, speech and language therapy students required a long time and high-cost equipment to develop healthcare of the auditory and vestibular systems competencies. The high cost of the equipment permitted its practical use only in classes, hindering students’ autonomy in developing those competencies. That situation was a real issue, even more in times of pandemic where online education was essential. This article describes SAEF, an open-source software simulator for autonomously developing procedural audiology therapy competencies, user acceptance, and the validity of experiments and results. SAEF delivers immediate feedback and performance results. Obtained results permit validating students’ and educators’ acceptability of SAEF in audiology therapy education. Obtained results invite authors to continue developing simulator software solutions in other health education contexts. SAEF was developed using open-source technology to facilitate its accessibility, classification, and sustainability.
Keywords:
SAEF
; audiology competencies
; audiometry simulation
; speech language
; students.
1. Introduction
Hearing plays a fundamental role in children’s language and speech development, learning, and communication throughout the life course [1]. In this sense, hearing loss or hearing loss can affect a person’s quality of life in multiple areas, such as the social, educational, psychological, and work spheres, among others [2,3,4,5,6].
Data published in the World Hearing Report indicate that currently, 1.5 billion people live with some degree of hearing loss. At the same time, by the year 2050, it is estimated that around 2.5 billion people will have hearing loss [7]. Based on these figures and the magnitude of the problem, public health interventions have been proposed for those suffering from hearing loss and ear diseases to guarantee high-quality universal access in this area [7]. The interventions contemplate hearing checkups throughout life for groups at higher risk, where elder people, newborns, infants, and children in preschool and school stage stand out and people exposed to noise, medicines, and ototoxic chemicals.
Universal Health Coverage (UHC) establishes that for these interventions to be carried out, it is necessary to have strengthened health systems where there is access to safe and high-quality diagnostic equipment; as well as, there is personnel who have the necessary training in the required discipline [8]. In this same sense, since the 1980s, the World Health Organization (WHO) has proposed guiding universities and higher education institutions towards a new approach in the training of future health professionals, more focused on the process of learning and oriented to the development of competences where knowledge, skills, and attitudes highly linked to social reality are integrated and not superficial and rote learning [9].
In higher education, health sciences majors have sought innovations leading to a review of the teaching curriculum in their respective disciplines so that future graduates carry out a comprehensive approach focused on people and health rather than on medicine and disease [10,11]. Clinical simulation as a teaching methodology is introduced into the academic training of health career students, who, before having experiences with actual patients, obtain guided experiences that interactively emulate situations, environments, and problems similar to the contexts of healthcare establishments in a safe, controlled environment that ends with a reflection process [12].
One of the disciplines that perform the intervention related to hearing screening throughout life is speech therapy, which corresponds to the science in charge of the evaluation, diagnosis, rehabilitation, health promotion, and prevention of language, speech, swallowing, hearing, voice, and communication, as rescued from the proceedings of the XXV Congress of Speech Therapy, Phoniatrics and Audiology [13]. Likewise, speech therapy considers areas or dimensions of quality related to equity, access and opportunity, continuity, safety, technical quality, user satisfaction, efficacy, and efficiency [14]. For this reason, the importance of training health professionals with theoretical and procedural competencies also applies to this discipline.
Within speech and language therapy, there is an area of audiology in charge of promoting hearing health, prevention, evaluation, diagnosis, intervention, and monitoring of pathologies related to hearing. In audiology, one of the relevant aspects is audiometry, a delicate and precise procedure that must be applied with expertise by the professional. To achieve this expertise and thereby contribute to achieving quality in the service based on the health guarantee model, undergraduate students today have clinical simulation tools that allow them -in this safe environment described above- to recreate clinical evaluations in a controlled and standardized environment. Seeking to facilitate the development of competencies in the audiometry procedure and hearing loss classification in undergraduate students, SAEF (Audiometry Simulator for Speech-Language Students) is available as part of a Speech-Language Pathology project [15].
- RQ1 [Acceptability of SAEF] How do students and educators accept SAEF to develop audiometric examination procedural competencies and skills?
- RQ2 [Functional Validity of SAEF] How does SAEF functional validation allow the development of procedural competencies and skills with the audiometric examination?
This article summarizes the main features of SAEF, an open-source Java application, and looks to validate the user satisfaction and quality of experiments in SAEF. This work is organized as follows. The following section details the SAEF tool: source, goals, and evolution. Then, Section 3 describes the applied methodology: student characteristics, population and sample, data collection, and procedures for analysis. After, Section 4 details each applied survey together with their results. Section 5 summarizes the main positive impact of the tool SAEF on the students and related university community, overall for the autonomous learning by its use, without requiring an audiometer for developing audiology competencies, a relevant virtue, overall in pandemic time. In the end, Section 6 presents the main conclusions.
2. Audiometry Simulator SAEF
2.1. Procedure for the Search for hearing thresholds
The procedure for performing the hearing threshold search in SAEF was determined according to the guidelines of the American Speech-Language-Hearing Association [16], which recommends the following actions: 1) Begin the test with the best ear self-reported by the user (if both are identical, start by convention with the right ear). 2) Carry out the Down-Up procedure or the Hughson-Westlake descending method, modified to search for hearing thresholds [17]. 3) Begin the threshold search procedure by presenting a tone at 30 dB HL at 1000 Hz. 4) If the user does not respond to the tone sent, the stimulus intensity should be increased by 20 dB HL until a positive response is obtained response (Action only valid for a frequency of 1000 Hz). 5) If the user responds, reduce the tone level by 10 dB HL until they no longer respond. 6) When there is no response, increase the tone level by 5 dB HL until a response is obtained from the user. 6) Repeat the Down-10/Up-5 procedure until getting two responses in the upstroke. 7) After obtaining the threshold at 1000 Hz, continue with the following frequencies to be examined (125 to 8000 Hz; evaluating in the first instance the high frequencies (2000, 3000, 4000, 6000, and 8000 Hz) and later the low frequencies (500, 250 and 125 Hz). 9) Once the evaluation of the airway of the better ear is completed, the contralateral airway should be continued. 10) Continue with the bone pathway of the worst ear resulting from the airways already evaluated. 11) Evaluate the contralateral bone pathway.
2.2. SAEF
SAEF arises as a project of professors of the speech and language therapy major of a house of higher studies in Chile, given the scenario that there are existing and accessible solutions, but with various previously mentioned practical restrictions (language, cost, not entirely suitable with pedagogical approaches of the institution). For these reasons, a development team was formed with specialist professionals from the Information Technology (IT) area and professors from the health area, specifically from the Speech Pathology course at Santo Tomás University in Chile. Figure 1 and Figure 2 [15] show the principal and authentication interface for the simulation of a practical case of the original version of SAEF, respectively. Figure 2 shows a practical example of SAEF that only considers the evaluation of the airways.
The development team applied a modular development following a design science approach [18] to develop knowledge that professionals in the discipline concerned can apply to plan solutions to their field problems. Regarding software development, design science represents an incremental approach like evolutive and spiral [19] to satisfy required functionalities.
3. Methodology
Looking to answer RQ1 and RQ2, this work structures its methodology as follows: first, it describes the methodological characteristics of the study carried out; second, it provides details of the research participants; third, it specifies the instruments used for data collection; and finally, it describes the techniques used for the analysis of the collected data.
3.1. Study characteristics
The present study was based on quantitative methodology because the researchers collected data and evaluated hypotheses based on numerical measurement and statistical analysis. The design was cross-sectional and non-experimental because the measured variables were not manipulated, and the assessment was performed only once. This study employs a descriptive-comparative methodology first to demonstrate the usability of SAEF and, secondly, to determine the application’s validity according to audiology professors. Finally, this study compares the outcomes and the equipment employed.
3.2. Population and sample
This work used a non-probabilistic or directed sample of homogeneous participants; the selected units have characteristics in common or similar features. In this case, students and professors of the Santo Tomás University, Chile’s speech-language pathology program interacted with SAEF as users. Additionally, students and professors who were studying and teaching the subject of Audiology in a theoretical or practical way, respectively, in the house of studies aforementioned. There were no exclusion criteria. The participants were recruited through the extended invitation of subject coordination, and the student and professor users voluntarily participated in the study. All participants signed informed consent.
The sample consisted of 43 users, divided into 31 students and 12 professors from different Chilean cities: Iquique, Viña del Mar, Santiago, Talca, Concepción, Osorno, and Puerto Montt. The 31 students answered the survey according to the TAM model (Theoretical Extension of the Technology Acceptance Model) [20], while the 12 professors answered the survey aimed at the technical validation of the audiometric procedure. In times of pandemic, the direct use of TAM or its extensions represents a standard for measuring the acceptance of technology in contexts such as health [21], education [22], and the government [23].
3.3. Data collection instruments
Through the Google Forms platform, the student users received the scale of measurements and reliability based on the theoretical extension of the Technology Acceptance Model, as shown in Table 1. This scale includes 26 statements about the usability and usefulness of a technological resource in terms of social influence and cognitive instrumental processes. The 26 statements are distributed in 9 categories: Intent of Use, Perceived utility, Perceived ease of use, Subjective norm, Volunteering, User interface, Job relevance, Output quality, and Results Demonstrability. The user had to answer how much they agree or disagree with each of the statements according to the following Likert scale: 1 = Totally disagree, 2 = Quite disagree, 3 = Disagree, 4 = Not at all in agreement - I do not disagree, 5 = Agree, 6 = Somewhat agree, 7 = Totally agree. The scale was applied in 3 moments: immediately after the training on using SAEF, after one month of use, and finally, three months after the planned period of use.
A survey was applied to the teaching users to validate the audiometric Procedure technique and the subject’s learning results (see Table 2). This survey was prepared by the authors following the recommendations of ASHA [24] that guide the Procedure for the execution of the search for hearing thresholds. The user had to answer how much they agree or disagree with each of the statements regarding whether SAEF actually emulates each of the proposed steps according to the following Likert scale: 1 = Totally disagree, 2 = Disagree, 3 = Neither agree nor disagree, 4 = Agree, 5 = Totally agree. Three categories classify the surveyed statements: Hearing threshold, Student performance, and Procedure carried out based on learning results. The final SAEF version considers each feedback provided by SAEF on student performance and its usefulness in achieving the learning outcomes.
3.4. Analysis procedure
After administrating the TAM scale and the technical validation survey, a database was created to be analyzed using the SPSS statistical package, version 21.0. Descriptive statistics were used to present the results of the TAM scale responses. On the other hand, the Friedman test [25] was used to compare the results of each TAM scale question at the three moments of application and Cronbach’s alpha test [26] to determine the level of agreement between the experts and the reliability of the scale used. For all analyses, this work used a significance level of 0.05. The Friedman Test test permits determining if statistically significant differences exist between three or more dependent samples [27].
4. Results
For the analysis of the scale of measurements and reliability based on the theoretical extension of the Technology Acceptance Model, Table 3 presents the results of the responses in a descriptive manner. Favorable responses were calculated: those found to be at or above the acceptance threshold (this article considers the last three values of the scale: 5 = Agree, 6 = Fairly agree, 7 = Totally agreement). Table 3 shows the acceptability of SAEF v.2 at each of the moments in which the survey was applied, for which the total responses considered favorable were divided by the total responses for all evaluations. Notably, the number of participants who answered the questions in the three evaluation moments was not constant. Hence, the proportions show slight variations in the numerator and denominator.
Table 4 compares the users’ acceptability of SAEF (questions of Table 1) using the TAM scale through the Friedman test [26,28]. These results are for the three moments of the test application: immediately after the training on the use of SAEF (Acceptability T1), after one month of the use of SAEF (Acceptability T2), and three months after the use of SAEF (Acceptability T3). This table presents the changes that exceeded the critical threshold of significance of 0.05 [29].
On the other hand, in the analysis of the technical validation of the audiometric procedure and the learning results of the subject, the level of agreement among the experts on the aspects evaluated using Cronbach’s alpha, a technique widely used for this purpose [26,30], reached a value of 0.62. Although this value is considered low for reliability analysis, the nature of the questions explains the lower result concerning the optimum for the test. Analyzing the evaluators’ agreement was to explore if the answers needed to be more diverse, which was not the case.
It is important to remark on the evolution in the users’ acceptability of SAEF in the surveyed times: 0.701653846 in Acceptability T1, 0.754230769 in Acceptability T2, and 0.800423077 in Acceptability T3. Like the research of cite Abbas et al. [31], Alamri et al. [32], and Lozano et al. [33], we can apply the t-student test to validate these results. In this case, we define the next question: ¿Can students’ satisfaction increase with using SAEF over time? Hence, the null hypothesis is that student satisfaction does not increase during the time, whereas the alternative hypothesis is that student satisfaction increases during the time. With a confidence level of 95%, = . Table 5 and Table 6 show the t-student results that reject the null hypothesis and accept the alternative one.
Figure 3 illustrates the acceptability evolution for each of the nine categories.
Considering that the survey applied to professionals uses a Likert-type scale, the results of the questions reflect the level of acceptance, that is, answers whose value is 4 or 5 according to the scale: 1. Strongly disagree; 2. Disagree; 3. Neither agree nor disagree; 4. Agree; 5. Strongly agree. Table 7 presents details of the percentages of the responses "Agree" and "Strongly agree" of the professors’ participants based on the aspects related to the (1) Hearing threshold search procedure, (2) Student performance feedback and (3) Procedures carried out based on learning results. Figure 4 summarizes those results. We can appreciate a high acceptability percentage in each evaluated aspect: 100% in the Hearing threshold search procedure, 84.71666667% in the Student performance feedback, and 97% in the Procedures carried out based on learning results.
Figure 5, Figure 6 and Figure 7 show some of the functional and interface improvements made that are part of SAEF version 2 [34]. Specifically, Figure 5 offers optimization from the point of view of user interface design to include an option to select the difficulty level, and Figure 6 permits selecting the case to work, functionalities did not present in SAEF v.1. SAEF v.1 performed a random assignment of case studies without considering the level of difficulty. As Figure 7 shows, the interface of SAEF v.2 improved the visual aspects to be more attractive to users, along with optimizing the distribution of elements to provide more remarkable similarity to the actual instrument. SAEF v.2 offers a better response display and validity for the last user action performed. Patient response latency times were also adjusted and parameterized to allow the student to decide on the following examination procedure. SAEF v.2 continues to be a Java application thanks to its wide diffusion due to its cross-platform execution and open source and its compatibility with multiple tools, including MySQL.
5. Discussion
The results show that students and professors users in the area accept SAEF. Specifically, SAEF demonstrated high acceptance in the constructs of intention to use, perceived usefulness, perceived ease of use, subjective norm, volunteering, image, job relevance, output quality, and results from demonstrability. In addition, this article shows statistically significant differences in the aspects of ease of use and demonstrability of the results, representing a high-satisfaction user experience using SAEF. Those results allow positive answering RQ1 and RQ2. These results align with what was indicated by Venkatesh and Bala [35], who theorize that two factors determine an individual’s behavioral intention to use a system: perceived ease of use and perceived utility. These factors represent the belief that using the system will be effortless and that using the system will improve their work and educational performance [36].
The Covid-19 pandemic accentuated the need for virtual tools to teach certain content and procedures in different disciplines [37,38,39]. From the same perspective, Information and Communication Technologies have transformed teaching-learning processes in higher education, incorporating technological resources as pedagogical and didactic elements for professors and students. However, evaluating the quality of these technologies is crucial since their incorporation does not guarantee the success of the teaching processes and the consequent development of competencies defined in the study programs [40]. In this sense, the TAM model used in this research aims to predict the acceptance of a system and diagnose design problems. That model represents a robust, solid, and detailed model to predict users’ acceptance of information technology [41].
Finally, regarding other applications similar to SAEF, as reported in Orellana et al. [15], there are no freely accessible digital tools to develop speech-language pathology skills, specifically for developing audiometric examination procedural skills. In this way, SAEF represents a tremendous academic contribution to the Santo Tomás University in Chile and other study houses that would like access to this application. The authors plan to develop a web and mobile version of SAEF. Those versions would expand the case studies and include a ranking of time of use and efficiency for developing the cases.
6. Conclusions
The following conclusions may be drawn from the SAEF validation findings and the examination of the used instruments.
- SAEF is compliant from the user’s perspective, and users accept all of its features, including the output quality, demonstrability of results, subjective norm, perceived utility, perceived ease of use, image, and work relevance.
- After some time of usage, the SAEF’s most notable features point to the software’s easy-to-understand interface. The SAEF system is simple to use and doesn’t need much thought, and users may readily explain how it works to other users.
- According to the evaluation by subject-matter experts, SAEF accurately replicates the audiometry technique by international standards and adheres to the learning outcomes of the topic.
- The new SAEF v.2 has functional and interface upgrades that give even more striking parallels to the instrument.
- SAEF represents a sustainable open-source Java application currently applied for developing speech and language therapy competencies in students in Chile and Ecuador. Due to its open-source nature, SAEF does not require special permissions, and we can massify its use without restrictions.
In conclusion, SAEF provides a reliable open-source simulator that is ideal for educational and training purposes for determining audiometric competency utilizing real-world study scenarios. Additionally, it offers user satisfaction and effective audiologist competence development.
References
- Morgan, S.D.; Zeng, F.G.; Clark, J. Adopting change and incorporating technological advancements in audiology education, research, and clinical practice. American Journal of Audiology 2022, 31, 1052–1058. [Google Scholar] [CrossRef]
- Sharma, A.; Glick, H. Cortical Neuroplasticity in Hearing Loss: Why It Matters in Clinical Decision-Making for Children and Adults: Observing changes in brain processing–and adjusting our intervention strategies accordingly. The Hearing Review 2018, 25, 20–25. [Google Scholar]
- Idstad, M.; Engdahl, B. Childhood sensorineural hearing loss and educational attainment in adulthood: Results from the HUNT study. Ear and Hearing 2019, 40, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.; Bhattacharyya, N. Association of hearing loss with decreased employment and income among adults in the United States. Annals of Otology, Rhinology & Laryngology 2012, 121, 771–775. [Google Scholar]
- Linszen, M.M.; Brouwer, R.M.; Heringa, S.M.; Sommer, I.E. Increased risk of psychosis in patients with hearing impairment: review and meta-analyses. Neuroscience & Biobehavioral Reviews 2016, 62, 1–20. [Google Scholar]
- Shukla, A.; Harper, M.; Pedersen, E.; Goman, A.; Suen, J.J.; Price, C.; Applebaum, J.; Hoyer, M.; Lin, F.R.; Reed, N.S. Hearing loss, loneliness, and social isolation: a systematic review. Otolaryngology–Head and Neck Surgery 2020, 162, 622–633. [Google Scholar] [CrossRef]
- WHO. World Health Organization. https://www.who.int/, 2022. Accessed: 2023-05-27.
- Corvalan, C.; Villalobos Prats, E.; Sena, A.; Campbell-Lendrum, D.; Karliner, J.; Risso, A.; Wilburn, S.; Slotterback, S.; Rathi, M.; Stringer, R.; others. Towards climate resilient and environmentally sustainable health care facilities. International Journal of Environmental Research and Public Health 2020, 17, 8849. [Google Scholar] [CrossRef]
- Ghanbari, M.K.; Behzadifar, M.; Doshmangir, L.; Martini, M.; Bakhtiari, A.; Alikhani, M.; Bragazzi, N.L. Mapping research trends of universal health coverage from 1990 to 2019: bibliometric analysis. JMIR Public Health and Surveillance 2021, 7, e24569. [Google Scholar] [CrossRef]
- Sandoval-Barrientos, S.; Arntz-Vera, J.; Flores-Negrin, C.; Trunce-Morales, S.; Pérez-Carrasco, A.; López-Uribe, J.; Velásquez-Scheuch, J. Propuesta de formación interprofesional en 4 programas de licenciatura de profesionales sanitarios. Educación Médica 2019, 20, 25–32. [Google Scholar] [CrossRef]
- Vila, L.E.; Dávila Quintana, D.; Mora, J.G. Competências para a inovação nas universidades da América Latina: uma análise empírica. Revista Iberoamericana de Educación Superior 2010, 1, 5–23. [Google Scholar]
- Villca, S. Simulación clínica y seguridad de los pacientes en la educación médica. Revista Ciencia, Tecnología e Innovación 2018, 16, 75–88. [Google Scholar] [CrossRef]
- Vega Rodríguez, Y.E.; Torres Rodríguez, A.M.; del Campo Rivas, M.N. Análisis del Rol del Fonoaudiólogo (a) en el Sector Salud en Chile. Ciencia & trabajo 2017, 19, 76–80. [Google Scholar]
- Angelopoulou, E.; Papachristou, N.; Bougea, A.; Stanitsa, E.; Kontaxopoulou, D.; Fragkiadaki, S.; Pavlou, D.; Koros, C.; Değirmenci, Y.; Papatriantafyllou, J.; others. How Telemedicine Can Improve the Quality of Care for Patients with Alzheimer’s Disease and Related Dementias? A Narrative Review. Medicina 2022, 58, 1705. [Google Scholar] [CrossRef] [PubMed]
- Orellana, A.M.; Oyarzún-Díaz, P.A.; Briones-Rojas, C.; Vidal-Silva, C.L. Prototipo de simulador de audiometría para estudiantes de fonoaudiología de la Universidad Santo Tomás, Chile. Formación universitaria 2020, 13, 3–10. [Google Scholar] [CrossRef]
- Campbell, J.; Graley, J.; Meinke, D.; Vaughan, L.; Aungst, R.; Madison, T. Guidelines for manual pure-tone threshold audiometry. Rockville, MD: American Speech-Language-Hearing Association (ASHA) 2005, 20, 297–301. [Google Scholar]
- Katz, J. Handbook of clinical audiology, 2015.
- Larsen, K.R.; Lukyanenko, R.; Mueller, R.M.; Storey, V.C.; VanderMeer, D.; Parsons, J.; Hovorka, D.S. Validity in design science research. Designing for Digital Transformation. Co-Creating Services with Citizens and Industry: 15th International Conference on Design Science Research in Information Systems and Technology, DESRIST 2020, Kristiansand, Norway, December 2–4, 2020, Proceedings 15. Springer, 2020, pp. 272–282.
- Narang, P.; Mittal, P. Software Development Methodologies: Trending from Traditional to DOSE-An Empirical Study. 2022 IEEE Delhi Section Conference (DELCON). IEEE, 2022, pp. 1–6.
- Rosli, M.S.; Saleh, N.S.; Ali, A.M.; Abu Bakar, S.; Mohd Tahir, L. A Systematic Review of the Technology Acceptance Model for the Sustainability of Higher Education during the COVID-19 Pandemic and Identified Research Gaps. Sustainability 2022, 14, 11389. [Google Scholar] [CrossRef]
- AlQudah, A.A.; Al-Emran, M.; Shaalan, K. Technology acceptance in healthcare: A systematic review. Applied Sciences 2021, 11, 10537. [Google Scholar] [CrossRef]
- Sukendro, S.; Habibi, A.; Khaeruddin, K.; Indrayana, B.; Syahruddin, S.; Makadada, F.A.; Hakim, H. Using an extended Technology Acceptance Model to understand students’ use of e-learning during Covid-19: Indonesian sport science education context. Heliyon 2020, 6, e05410. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Chen, J.; Liu, Z. Government responsiveness and public acceptance of big-data technology in urban governance: Evidence from China during the COVID-19 pandemic. Cities 2022, 122, 103536. [Google Scholar] [CrossRef]
- ASHA. American Speech-Language-Hearing Association (ASHA). https://www.asha.org/, 2022. Accessed: 2022-12-27.
- Kouriati, A.; Moulogianni, C.; Kountios, G.; Bournaris, T.; Dimitriadou, E.; Papadavid, G. Evaluation of Critical Success Factors for Enterprise Resource Planning Implementation Using Quantitative Methods in Agricultural Processing Companies. Sustainability 2022, 14, 6606. [Google Scholar] [CrossRef]
- Luna-Krauletz, M.D.; Juárez-Hernández, L.G.; Clark-Tapia, R.; Súcar-Súccar, S.T.; Alfonso-Corrado, C. Environmental education for sustainability in higher education institutions: design of an instrument for its evaluation. Sustainability 2021, 13, 7129. [Google Scholar] [CrossRef]
- Pereira, D.G.; Afonso, A.; Medeiros, F.M. Overview of Friedman’s test and post-hoc analysis. Communications in Statistics-Simulation and Computation 2015, 44, 2636–2653. [Google Scholar] [CrossRef]
- Pacces, A.M. Will the EU Taxonomy Regulation Foster Sustainable Corporate Governance? Sustainability 2021, 13, 12316. [Google Scholar] [CrossRef]
- Ashraf, H.; Waris, A.; Jamil, M.; Gilani, S.O.; Niazi, I.K.; Kamavuako, E.N.; Gilani, S.H.N. Determination of optimum segmentation schemes for pattern recognition-based myoelectric control: a multi-dataset investigation. IEEE Access 2020, 8, 90862–90877. [Google Scholar] [CrossRef]
- Coskun, S. Zero Waste Management Behavior: Conceptualization, Scale Development and Validation—A Case Study in Turkey. Sustainability 2022, 14, 12654. [Google Scholar] [CrossRef]
- Abbas, J.; Aman, J.; Nurunnabi, M.; Bano, S. The impact of social media on learning behavior for sustainable education: Evidence of students from selected universities in Pakistan. Sustainability 2019, 11, 1683. [Google Scholar] [CrossRef]
- Alamri, M.M.; Almaiah, M.A.; Al-Rahmi, W.M. Social media applications affecting Students’ academic performance: A model developed for sustainability in higher education. Sustainability 2020, 12, 6471. [Google Scholar] [CrossRef]
- Lozano-Díaz, A.; Fernández-Prados, J.S. Educating digital citizens: An opportunity to critical and activist perspective of sustainable development goals. Sustainability 2020, 12, 7260. [Google Scholar] [CrossRef]
- Orellana, A.M.; Oyarzún-Díaz, P.A.; Briones-Rojas, C.; Vidal-Silva, C.L. Validation and optimization of the prototype of audiometry simulator for speech therapy students ASST in pandemic times. Formación universitaria 2023, 16, 3–12. [Google Scholar]
- Venkatesh, V.; Bala, H. Technology acceptance model 3 and a research agenda on interventions. Decision sciences 2008, 39, 273–315. [Google Scholar] [CrossRef]
- Lim, T.L.; Lee, A.S.H. Extended TAM and TTF Model: A Framework for the 21 st Century Teaching and Learning. 2021 International Conference on Computer & Information Sciences (ICCOINS). IEEE, 2021, pp. 339–334.
- Crawford, J.; Cifuentes-Faura, J. Sustainability in higher education during the COVID-19 pandemic: A systematic review. Sustainability 2022, 14, 1879. [Google Scholar] [CrossRef]
- Imran, M.; Hina, S.; Baig, M.M. Analysis of Learner’s Sentiments to Evaluate Sustainability of Online Education System during COVID-19 Pandemic. Sustainability 2022, 14, 4529. [Google Scholar] [CrossRef]
- Faura-Martínez, U.; Lafuente-Lechuga, M.; Cifuentes-Faura, J. Sustainability of the Spanish university system during the pandemic caused by COVID-19. Educational Review 2022, 74, 645–663. [Google Scholar] [CrossRef]
- Avendaño, W.R.; Luna, H.O.; Rueda, G. Educación virtual en tiempos de COVID-19: percepciones de estudiantes universitarios. Formación universitaria 2021, 14, 119–128. [Google Scholar] [CrossRef]
- Rahimi, B.; Nadri, H.; Afshar, H.L.; Timpka, T. A systematic review of the technology acceptance model in health informatics. Applied clinical informatics 2018, 9, 604–634. [Google Scholar] [CrossRef]
Figure 1.
SAEF First Version Authentication Screen

Figure 2.
SAEF First Version Main Screen
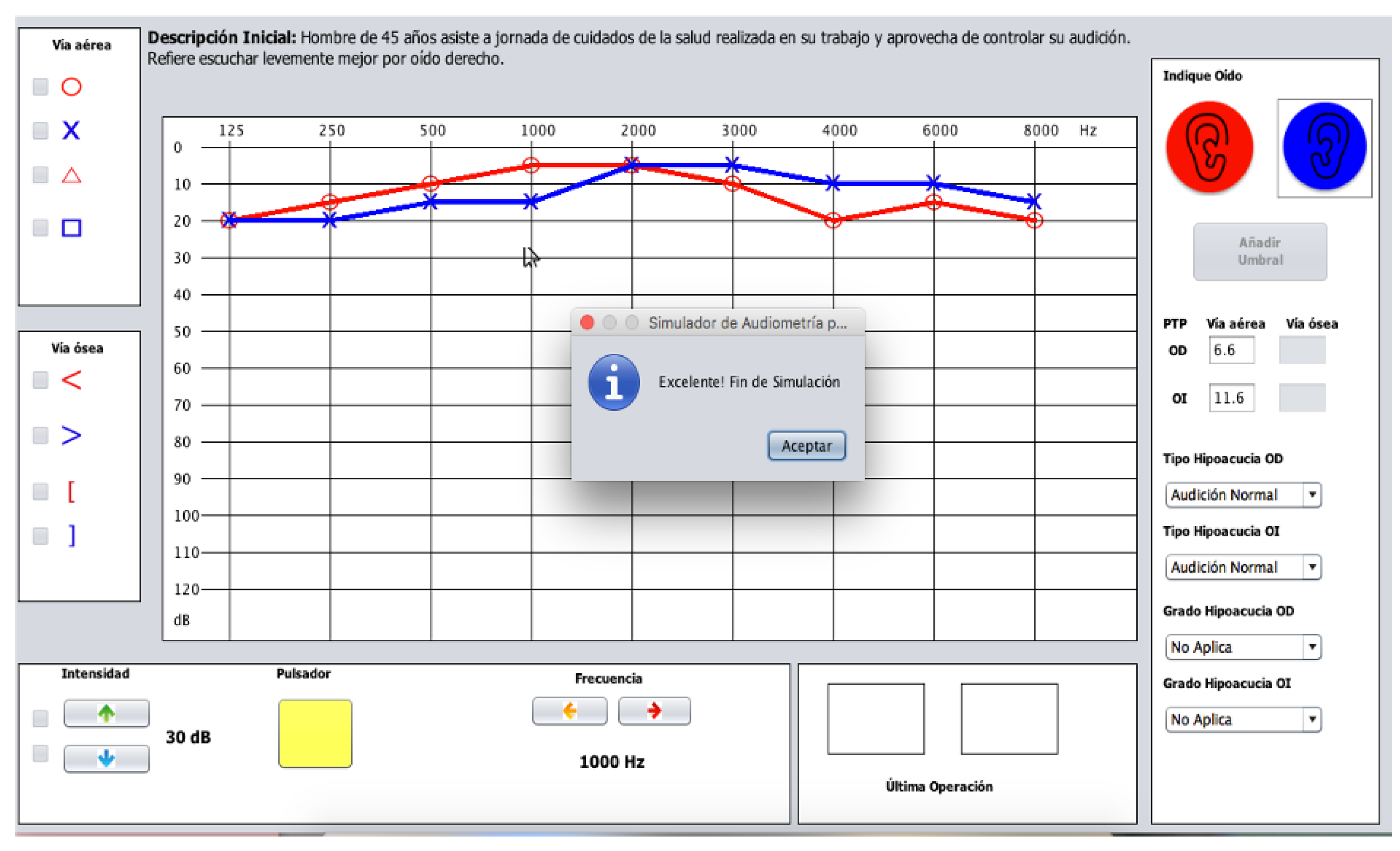
Figure 3.
Cathegories of SAEF acceptability
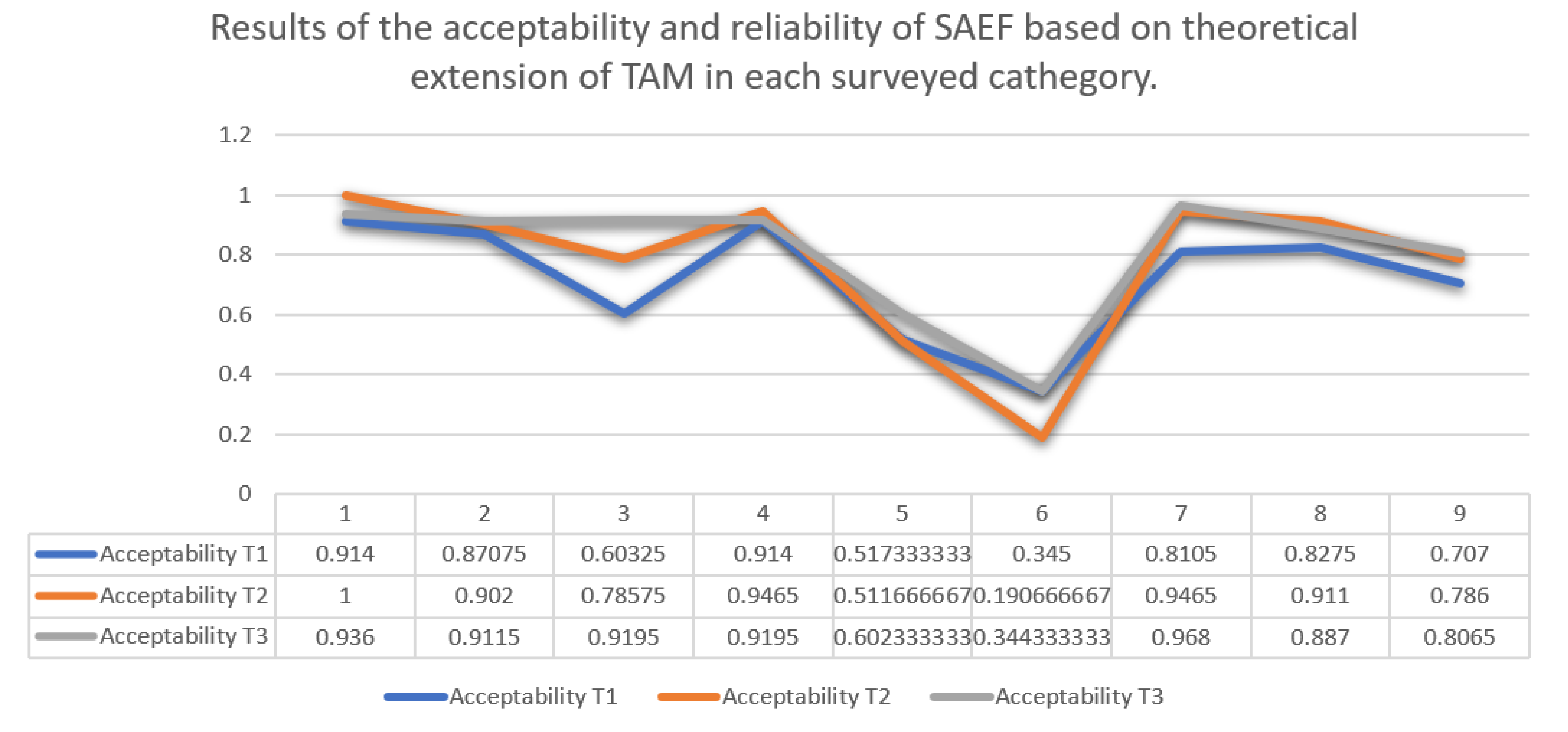
Figure 4.
Summary of percentage of responses of technical validation acceptability of SAEF
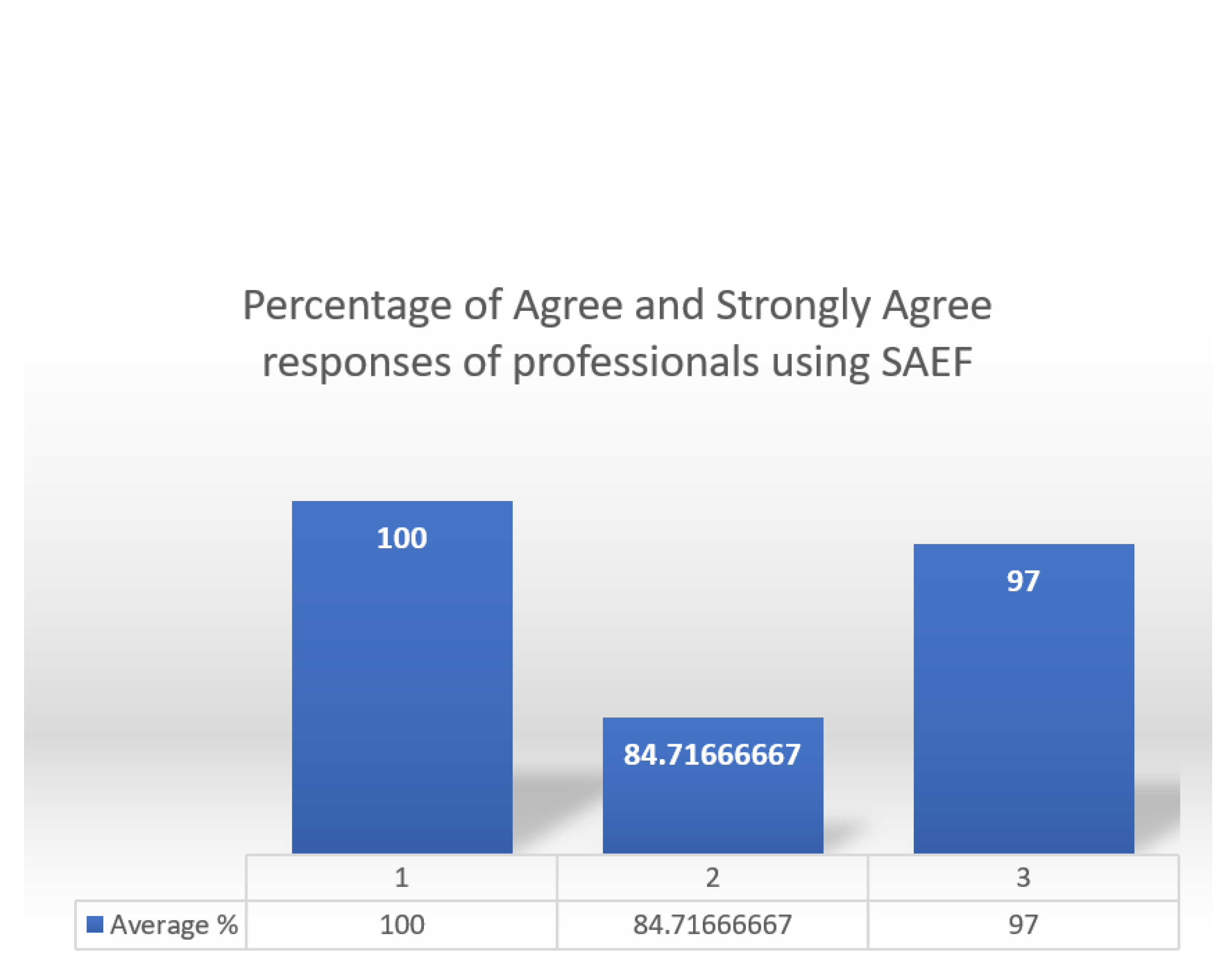
Figure 5.
Current SAEF -Authentication Screen
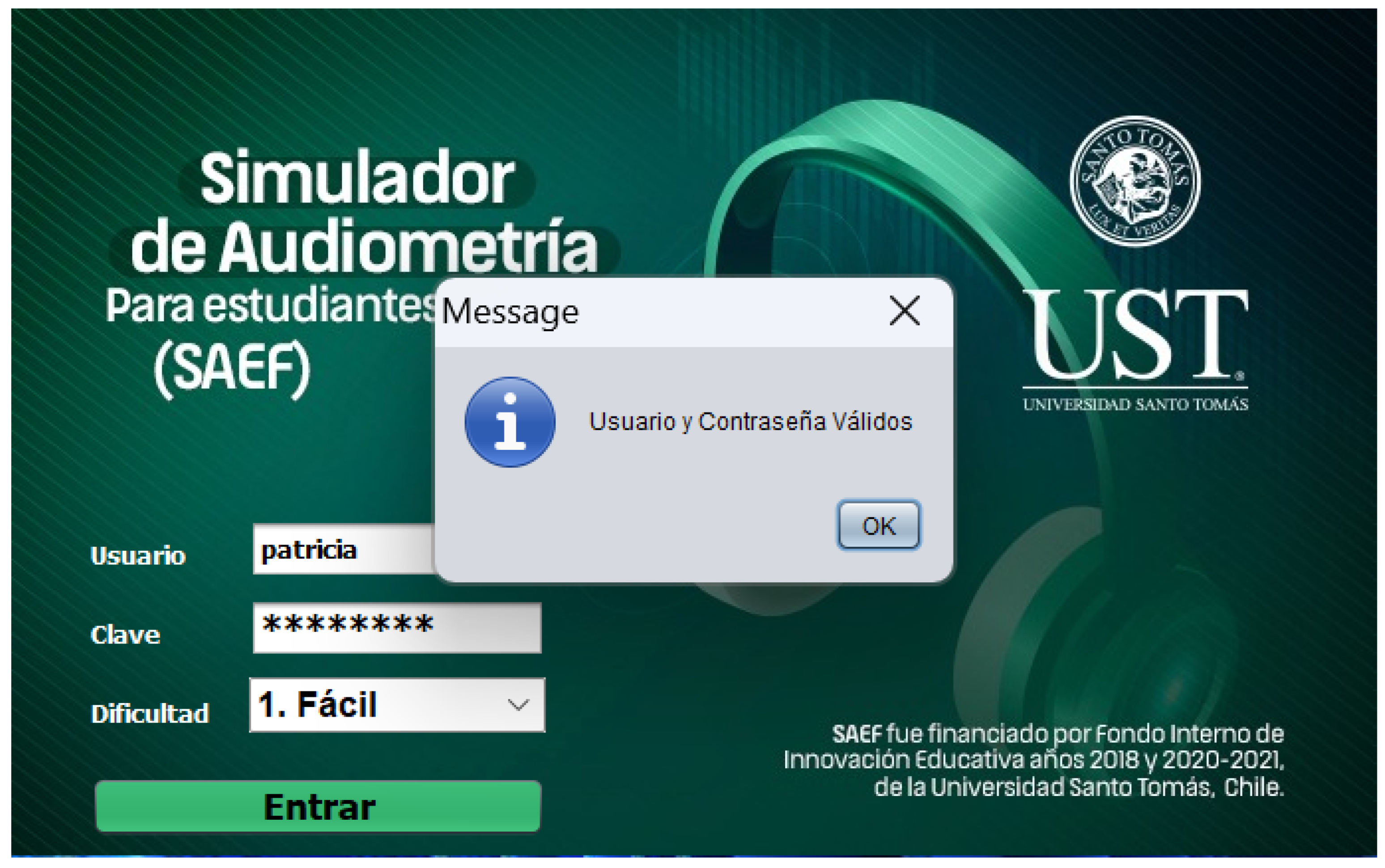
Figure 6.
Current SAEF -Selecting Case
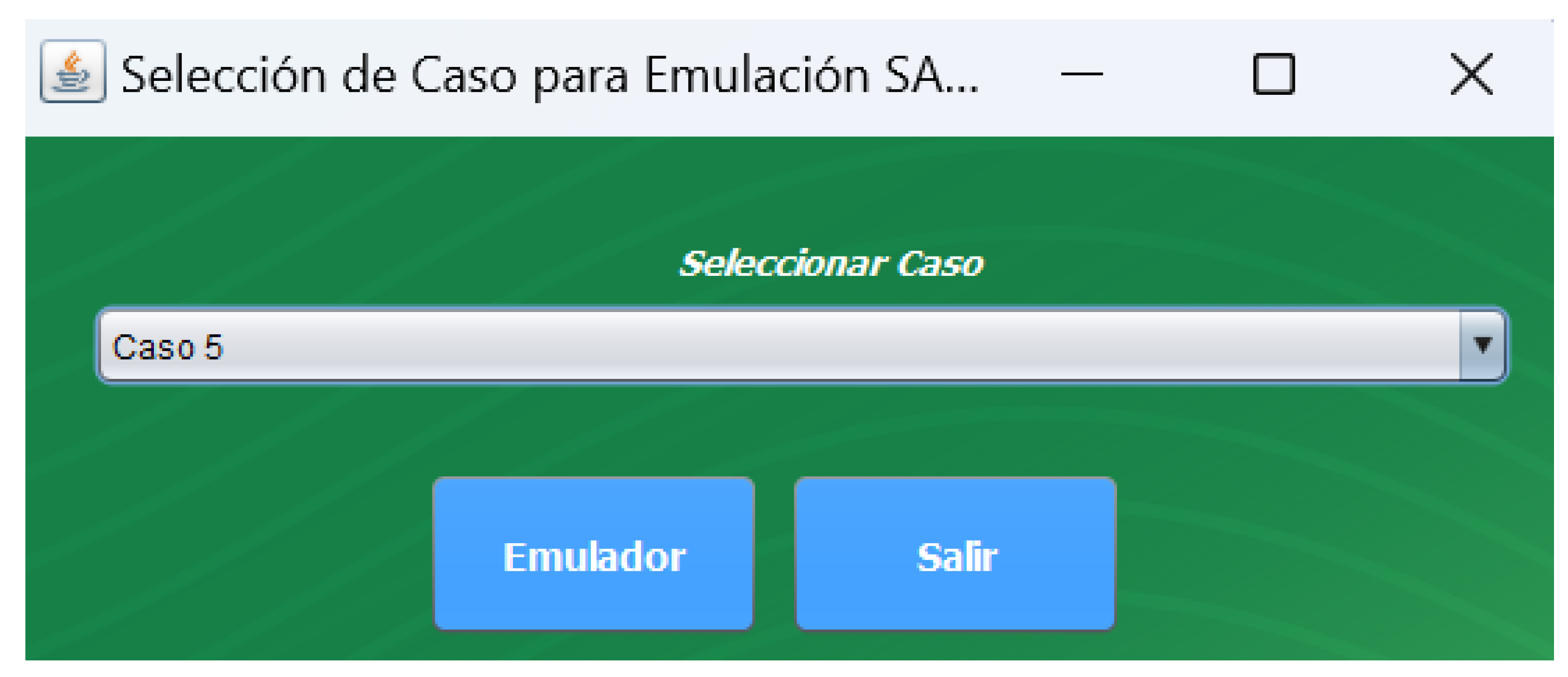
Figure 7.
Current SAEF -Main Screen
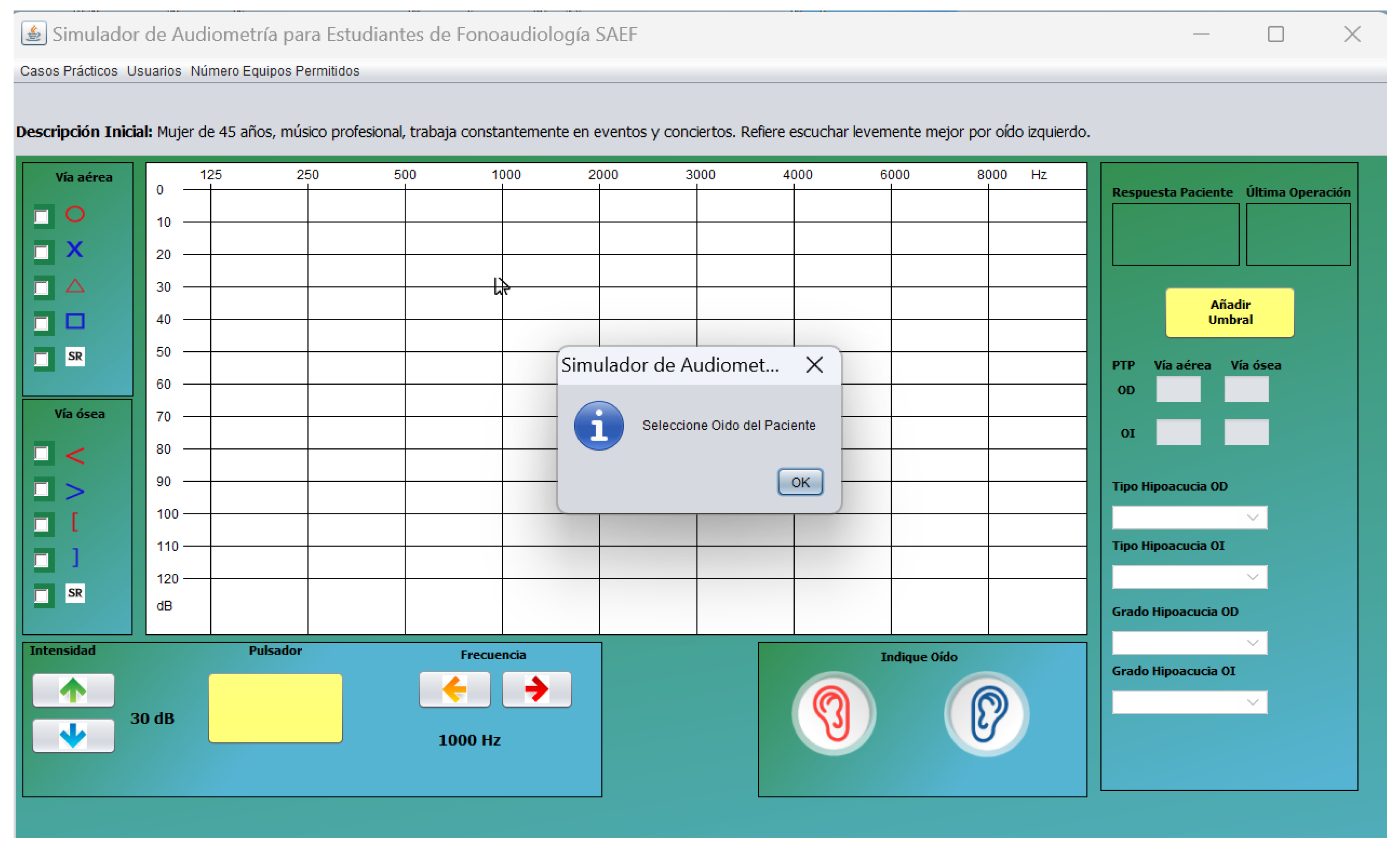

Table 1.
Items and scale to measure the acceptability of SAEF according to the scale of measurements and reliability based on a theoretical extension of TAM.
Table 1.
Items and scale to measure the acceptability of SAEF according to the scale of measurements and reliability based on a theoretical extension of TAM.
| Ítems | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Intent of use | |||||||
| 1. Assuming I have access to the system, I intend to use it. | |||||||
| 2. Since I have access to the system, I predict I will use it. | |||||||
| Perceived utility | |||||||
| 3. Using the system improves my performance at work. | |||||||
| 4. Using the system at work increases my productivity. | |||||||
| 5. Using the system improves my effectiveness in my work. | |||||||
| 6. I find the system useful in my work. | |||||||
| Perceived ease of use | |||||||
| 7. My interaction with the system is clear and understandable. | |||||||
| 8. Interacting with the system does not require much mental effort. | |||||||
| 9. I find the system easy to use. | |||||||
| 10. I find it easy to make the system do what I want it to do. | |||||||
| Subjective norm | |||||||
| 11. The people who influence my behavior think that I should use the system. |
|||||||
| 12. People who are important to me think that I should use the system. |
|||||||
| Volunteering | |||||||
| 13. My use of the system is voluntary. | |||||||
| 14. My supervisor does not require me to use the system. | |||||||
| 15. Although it can be useful, the use of the system is certainly not mandatory in my work. |
|||||||
| User interface | |||||||
| 16. People in my organization who use the system have more prestige than those who don’t. |
|||||||
| 17. The people in my organization who use the system are high profile. |
|||||||
| 18. Having the system is a symbol of rank (status) in my organization. |
|||||||
| Job relevance | |||||||
| 19. In my work, the use of the system is important. | |||||||
| 20. In my work, the use of the system is relevant. | |||||||
| Output quality | |||||||
| 21. The output of the system is of high quality. | |||||||
| 22. I have no problem with the quality of the system output. | |||||||
| Demonstrability of results | |||||||
| 23. I have no difficulty telling others about the results of using the system. |
|||||||
| 24. I think that I could communicate to others the consequences of using the system. |
|||||||
| 25. The results of using the system are evident to me. | |||||||
| 26. You would have difficulty explaining why using the system may or may not be beneficial. |
Table 2.
Items and scale used for validation of the technique of the audiometric procedure, feedback and learning results.
Table 2.
Items and scale used for validation of the technique of the audiometric procedure, feedback and learning results.
| Items | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Hearing threshold search procedure | |||||
| 1. It allows starting with the best ear self-reported by the patient or, if both ears are believed to be identical, starting by convention in the right ear. |
|||||
| 2. It allow you to perform a "Down-up" procedure or descending method to search for hearing thresholds. |
|||||
| 3. It allows starting the threshold search procedure by presenting a tone at 30 dB HL at the frequency of 1000 Hz. |
|||||
| 4. As there is no response to the initial tone, it allows the intensity of the stimulus to be increased by 20 dB HL until a response is obtained (action only valid for the frequency of 1000 Hz). |
|||||
| 5. If the patient responds, it allows you to reduce the tone level by 10 dB until the patient no longer responds. |
|||||
| 6. When there is no response, it allows the examiner to increase the tone level by 5 dB until a response is obtained. |
|||||
| 7. The hearing threshold is obtained from 2 responses in ascending runs. |
|||||
| 8. After evaluating 1000 Hz, the software allows you to continue with the evaluation of the following frequencies (125 to 8000 Hz), evaluating the highest frequencies and later the low frequencies. |
|||||
| 9. It allows starting the procedure at the next frequency, increasing 30 dB to the threshold obtained at the next frequency. |
|||||
| 10. Once the evaluation of the airway of the better ear is completed, it is possible to continue with the contralateral airway. Subsequently, the bone pathway of the worst ear resulting from the airways is already evaluated; and finally, evaluate the contralateral bone pathway. |
|||||
| Student performance feedback. | |||||
| 11. The program provides information on student performance. | |||||
| 12. The information provided is useful for individual feedback. | |||||
| 13. The program provides feedback to the student on her performance at different stages of the procedure. |
|||||
| 14. The program allows the student to make diagnostic decisions regarding the results obtained in the audiometry. |
|||||
| 15. The analysis of the information delivered by the program helps to identify general aspects of the group/course that must be reinforced. |
|||||
| 16. In general, the program is useful for the professors regarding feedback on student performance |
|||||
| Procedures carried out based on learning results | |||||
| 17. The program is a useful tool to achieve learning outcomes: Apply descending audiometric technique to obtain hearing thresholds. |
|||||
| 18. The program is a useful tool to achieve the following learning outcome: Classify hearing loss according to audiometric findings. |
|||||
| 19. In general, the program is a useful complement to the development of the subject. |
Table 3.
Results of the acceptability and reliability of SAEF based on a theoretical extension of TAM.
Table 3.
Results of the acceptability and reliability of SAEF based on a theoretical extension of TAM.
| Question | Acceptability T1 | Acceptability T2 | Acceptability T3 |
|---|---|---|---|
| 1 | .931 | 1 | .936 |
| 2 | .897 | 1 | .936 |
| 3 | .862 | .929 | .903 |
| 4 | .793 | .786 | .839 |
| 5 | .931 | .964 | .936 |
| 6 | .897 | .929 | .968 |
| 7 | .793 | .964 | .968 |
| 8 | .586 | .786 | .968 |
| 9 | .586 | .786 | .903 |
| 10 | .448 | .607 | .839 |
| 11 | .966 | .964 | .936 |
| 12 | .862 | .929 | .903 |
| 13 | .966 | .964 | .903 |
| 14 | .172 | .214 | .355 |
| 15 | .414 | .357 | .549 |
| 16 | .345 | .286 | .323 |
| 17 | .345 | .143 | .323 |
| 18 | .345 | .143 | .387 |
| 19 | .828 | 1 | 1 |
| 20 | .793 | .893 | .936 |
| 21 | .862 | .929 | .903 |
| 22 | .793 | .893 | .871 |
| 23 | .862 | .929 | 1 |
| 24 | .793 | .929 | .903 |
| 25 | .828 | .857 | .968 |
| 26 | .345 | .429 | .355 |
Table 4.
Comparison of acceptability of the new version of SAEF according to moments of application of the TAM Scale.
Table 4.
Comparison of acceptability of the new version of SAEF according to moments of application of the TAM Scale.
| Item | n | gl | p | |
|---|---|---|---|---|
| 7. My interaction with the system is clear and understandable. | 28 | 7.253 | 2 | .027 |
| 8. Interacting with the system does not require much mental effort. | 28 | 9.172 | 2 | .010 |
| 9. I find the system easy to use. | 28 | 6.090 | 2 | .048 |
| 23. I have no difficulty telling others about the results of using the system. | 28 | 7.014 | 2 | .030 |
Table 5.
t-Test: Paired Sample T1 - T2
| Mean | 0.701653846 | 0.754230769 |
| Variance | 0.058437835 | 0.085445145 |
| Observations | 26 | 26 |
| Pearson Correlation | 0.943311282 | |
| Hypothesized Mean Difference | 0 | |
| df | 25 | |
| t Stat | -2.607746847 | |
| P(T=t) one-tail | 0.007577472 | |
| t Critical one-tail | 1.708140761 | |
| P(T=t) two-tail | 0.015154944 | |
| t Critical two-tail | 2.059538553 |
Table 6.
t-Test: Paired Sample T2 - T3
| Acceptability T2 | Acceptability T3 | |
|---|---|---|
| Mean | 0.754230769 | 0.800423077 |
| Variance | 0.085445145 | 0.057671454 |
| Observations | 26 | 26 |
| Pearson Correlation | 0.950741471 | |
| Hypothesized Mean Difference | 0 | |
| df | 25 | |
| t Stat | -2.399369238 | |
| P(T=t) one-tail | 0.012099974 | |
| t Critical one-tail | 1.708140761 | |
| P(T=t) two-tail | 0.024199948 | |
| t Critical two-tail | 2.059538553 |
Table 7.
Percentage of response of agreement and total agreement in technical validation of SAEF v.1 according to experts.
Table 7.
Percentage of response of agreement and total agreement in technical validation of SAEF v.1 according to experts.
| Developed aspect by SAEF procedure | Validated aspect | Percentage |
|---|---|---|
| - It lets start for better hearing. | 1 | 100 |
| - It allows descending method. | 1 | 100 |
| - It lets start with 30 dB at 1000 Hz frequency. | 1 | 100 |
| - It allows increasing 20 dB HL if there is no initial response. | 1 | 100 |
| - Allows you to reduce the tone level by 10 dB when there is a response. |
1 | 100 |
| - Allows increasing by 5 dB until response is obtained. | 1 | 100 |
| - It allows to obtain from 2 answers in ascending races. | 1 | 100 |
| - It allows you to continue with the following frequencies. | 1 | 100 |
| - It allows starting the next frequency by adding 30 dB to the previous threshold. |
1 | 100 |
| - It allows continuing with the contralateral airway. | 1 | 100 |
| - It provides information on student performance. | 2 | 83.3 |
| - The information provided is useful for individual feedback. | 2 | 83.3 |
| - It allows feedback to the student on the performance of it. | 2 | 83.3 |
| - It allows the student to make diagnostic decisions. | 2 | 91.7 |
| - It makes it possible to identify general aspects of the group/course that must be reinforced. |
2 | 91.7 |
| - It is useful for the professor regarding feedback to students. | 2 | 75 |
| - Allows to achieve learning outcome: Apply descending audiometric technique to obtain hearing thresholds. |
3 | 100 |
| - It allows to achieve learning results: Classify hearing loss according to audiometric findings. |
3 | 91 |
| - It is a useful complement for the development of the subject. | 3 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



