
Submitted:
16 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
Despite evidence-based therapies, patients presenting with atherosclerosis involving more than one vascular bed, such as those with peripheral artery disease (PAD) and concomitant coronary artery disease (CAD), constitute a particular vulnerable group characterized by enhanced residual long-term risk for major adverse cardiac events (MACE), as well as major adverse limb events (MALE). The latter are progressively emerging as a hard outcome to be targeted, being correlated with increased mortality.
Antithrombotic therapy is the mainstay of secondary prevention in both patients with PAD or CAD however, the optimal intensity of such therapy is still topic of debate, particularly in the post-acute and long-term setting. Recent well powered randomized clinical trials (RCTs) have provided data in favor of a more intense antithrombotic therapy, such as prolonged dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor or a therapy with aspirin combined with an anticoagulant drug. Both approaches increase bleeding and patients selection is a key issue. The aim of this review is therefore to discuss and summarize the most updated available evidences for different strategies of anti-thrombotic therapies in patients with chronic PAD and CAD, particularly focusing on studies enrolling patients with both type of atherosclerotic disease and comparing a higher versus a lower intensity antithrombotic strategy. The final objective is to identify the optimal tailored approach in this setting, to achieve the greatest cardiovascular benefit and improving precision medicine.
Keywords:
Coronary artery disease
; Peripheral Artery Disease
; Polyvascular Diseae
; Anti-thrombotic therapy
; Personalized treatment
1. Introduction
Atherosclerosis is a lipid-driven chronic ubiquitous inflammatory disease of the arterial wall that leads to a broad spectrum of cardiovascular (CV) diseases [1]. Given the systemic nature of the disease the involvement of more than one vascular bed, known as polyvascular disease is frequent. Data from the REACH registry showed that approximately 10% of patients with coronary artery disease (CAD) present concomitant peripheral artery disease (PAD) and, viceversa, 60% of patients with PAD present concomitant CAD [2]. Particularly, PAD has been associated with more extensity and severity of CAD, including left main disease or more complex CAD [3]. Data from large randomized clinical trials, consistently showed that the co-existence of CAD and PAD is a particularly harmful association both in patients primarily randomized for CAD (Figure 1, Panel A) or PAD (Figure 1, Panel B), with a heightened risk of major adverse cardiovascular events (MACE), including myocardial infarction (MI), stroke and CV death, compared to CAD or PAD only [4]. In addition to an elevated risk of MACE, patients with PAD often require peripheral revascularization and lower extremity amputation, that are associated with increased morbidity and mortality [5].
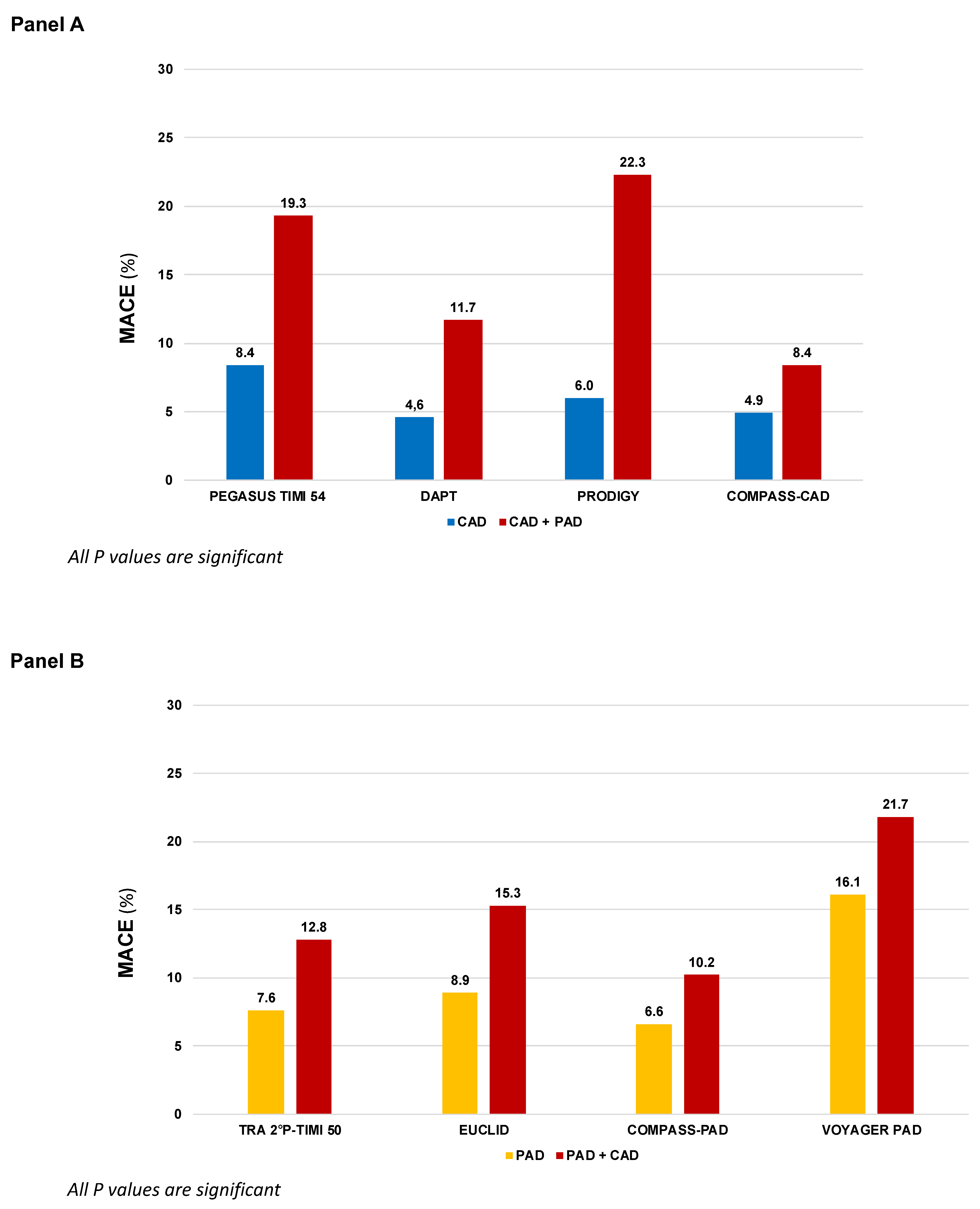
Figure 1.
MACE incidence according to different antithrombotic strategies in patients randomized in large clinical trials primarily based on coronary artery disease (Panel A) or peripheral artery disease (Panel B). COMPASS: Cardiovascular Outcomes for People Using Anticoagulation Strategies; CAD: Coronary artery disease; PAD: Peripheral artery disease; DAPT: Dual antiplatelet therapy; EUCLID: Examining Use of Ticagrelor in Peripheral Artery Disease; PEGASUS-TIMI 54: Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54; TRA 2P–TIMI 50: Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events – Thrombolysis in Myocardial Infarction 50; PRODIGY: Prolonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study; VOYAGER-PAD: Vascular Outcomes Study of ASA (acetylsalicylic acid) Along with Rivaroxaban in Endo-vascular or Surgical Limb Revascularization for PAD.
Figure 1.
MACE incidence according to different antithrombotic strategies in patients randomized in large clinical trials primarily based on coronary artery disease (Panel A) or peripheral artery disease (Panel B). COMPASS: Cardiovascular Outcomes for People Using Anticoagulation Strategies; CAD: Coronary artery disease; PAD: Peripheral artery disease; DAPT: Dual antiplatelet therapy; EUCLID: Examining Use of Ticagrelor in Peripheral Artery Disease; PEGASUS-TIMI 54: Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54; TRA 2P–TIMI 50: Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events – Thrombolysis in Myocardial Infarction 50; PRODIGY: Prolonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study; VOYAGER-PAD: Vascular Outcomes Study of ASA (acetylsalicylic acid) Along with Rivaroxaban in Endo-vascular or Surgical Limb Revascularization for PAD.
Beyond controlling modifiable cardiovascular risk factors, antithrombotic therapy is the mainstay of secondary prevention both in chronic PAD and chronic coronary syndrome (CCS). However, the optimal antithrombotic strategy in term of duration and intensity is still debated, particularly in the long-term. Recent evidences supported a long-term dual antiplatelet therapy strategy (DAPT) with aspirin and a P2Y12 or an approach combing an antiplatelet agent and an anticoagulant drug, at the cost of increased risk of bleeding [6,7].
The aim of this review is therefore, to discuss and summarize the most updated available evidences derived from large RCTs, investigating different strategies of anti-thrombotic therapies in patients with CAD and PAD (Table 1), in order to identify the optimal tailored approach to achieve the greatest cardiovascular benefit and improving precision medicine.

Table 1.
Trials comparing in patients with peripheral artery disease and/or chronic coronary syndrome a higher versus lower intense antithrombotic regimen.
Table 1.
Trials comparing in patients with peripheral artery disease and/or chronic coronary syndrome a higher versus lower intense antithrombotic regimen.
| Trial | First Author, year | Population | Total N | Proportion with both CAD and PAD |
Comparison | Median FUP |
|---|---|---|---|---|---|---|
| Single antiplatelet therapy (more vs. less potent) | ||||||
| CAPRIE | CAPRIE Steering Committee, 1996 | Recent MI (N=6,302) or Symptomatic LE PAD (N=6,452) or Ischemic stroke (N=6,431) |
19,185 | N.A. | Clopidogrel 75 mg vs. Asprin 325 |
22.9 |
| EUCLID | Hiatt WR, 2017 Berger J, 2018 |
Symptomatic LE PAD | 13,885 | 29.0% | Ticagrelor 90 mg b.i.d vs. Clopidogrel 75 mg |
30 |
| DAPT vs. Single antiplatelet therapy | ||||||
| CHARISMA | Bhatt DL, 2006 Cacoub P, 2009 |
CCS (N=5,835) or LE PAD (N=2,838) or Ischemic stroke/TIA (N=4,290) or multiple atherosclerotic risk factors (N=3,284) |
15,603 | N.A. | Clopidogrel 75 mg + Aspirin 75-162 mg vs. Aspirin 75-162 mg |
28 |
| PRODIGY | Valgimigli M, 2012 Franzone A, 2016 |
CCS (N=505) or ACS (N=1,465) |
1,970 | 12.5% | Clopidogrel 75 mg + Aspirin 80-160 mg for 24 months vs. 6 months |
28 |
| DAPT | Secemsky EA, 2017 | Patients free from ischemic and bleeding events 12 months after coronary stenting | 11,648 | 5.57% | Continued thienopyridine (clopidogrel 75 mg or prasugrel 10 mg) + Aspirin therapy for an additional 18 months vs. Aspirin 100 mg | 18 |
| TRA-2°P-TIMI 50 | Morrow D, 2012 Magnani G, 2015 Qamar A, 2020 |
Stable MI (N=17,779) or LE PAD (N=3,787) or Ischemic stroke (N=4,883) |
26,449 | 76.3% of 6,136 patients with PAD regardless of stratum |
Vorapaxar 2.5 mg vs. Placebo | 30 |
| PEGASUS TIMI-54 | Bonaca MP, 2015 & 2016 | Stable MI | 21,162 | CAD + PAD 5.2% |
Ticagrelor 60 or 180 mg b.i.d. + Aspirin 75-150 mg o.d. vs. or Aspirin 75-150 mg o.d. | 33 |
| Therapy with aspirin combined with an anticoagulant drug | ||||||
| COMPASS | Eikelboom JW, 2017 Connolly S, 2018 Anand SS, 2018 |
Stable CAD (N=24,828) or [Symptomatic LE PAD or carotid artery disease or ABI <0.9 with CAD (N=7,470)] |
27,395 | COMPASS-CAD: 17.9% COMPASS-PAD: 44.1% |
Rivaroxaban 2.5 b.i.d. + Aspirin 100 mg or Rivaroxaban 5 mg b.i.d. vs. Aspirin 100 mg |
23 |
| VOYAGER-PAD | Bonaca MP, 2020 | LE PAD with recent peripheral revascularization | 6,564 | PAD + CAD 23.6% | Rivaroxaban 2.5 mg b.i.d + Aspirin 100 mg vs. Aspirin 100 mg | 28 |
ACS: acute coronary syndrome; CAPRIE: Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events artery disease; BID: Twice a day; CAD: Coronary artery disease; CCS: Chronic coronary syndrome; CHARISMA: Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance; COMPASS: Cardiovascular Outcomes for People Using Anticoagulation Strategies; DAPT: Dual antiplatelet therapy; EUCLID: Examining Use of Ticagrelor in Peripheral Artery Disease; FUP:Follow-up; LE-PAD: Lower-extremity peripheral artery disease; OD: Once daily; MI: Myocardial infarction; PEGASUS-TIMI 54: Prevention of Cardiovascular Events in Patients with Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin–Thrombolysis in Myocardial Infarction 54; SAPT: Single antiplatelet therapy; TIA. Transient ischemic attack; TRA 2P–TIMI 50: Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events – Thrombolysis in Myocardial Infarction 50; PRODIGY: Prolonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study; VOYAGER-PAD: Vascular Outcomes Study of ASA (acetylsalicylic acid) Along with Rivaroxaban in Endo-vascular or Surgical Limb Revascularization for PAD.
2. Single Antiplatelet Strategy
Single antiplatelet therapy with aspirin is still the most frequently used antiplatelet drug in both chronic CAD and PAD, with a class I recommendation, level of evidence A, in secondary prevention of CCS and in symptomatic PAD patients [6,7,8,9]. Clopidogrel monotherapy has been studied in the Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events (CAPRIE) enrolling a broad population with stable atherosclerotic cardiovascular disease (ASCVD). In this trial, clopidogrel monotherapy reduced ischaemic events compared with aspirin monotherapy [10]. In a post-hoc analysis of patients with symptomatic PAD, clopidogrel was associated with an additional one fourth risk reduction of MACE compared to aspirin (HR 0.76, 95% CI: 0.64–0.91, p=0.003) [11] and the European PAD guidelines suggests clopidogrel as the preferred antiplatelet drug (Class IIb, Level of evidence C) [7]. Although the efficacy of clopidogrel has been confirmed in an extensive meta-analysis including PAD patients who underwent revascularization [12], more recent evidences did not corroborate the superiority of clopidogrel over aspirin as SAPT in PAD patients [13]. This may be partially traced back to the so called “antiplatelet non-responsiveness”, a condition of high on-treatment platelet reactivity present in up to 50% of patients with critical limb ischemia and associated to a significantly increased CV events risk [14]. More recently, in the Examining Use of Ticagrelor in Peripheral Artery Disease (EUCLID) trial, enrolling 13,185 patients with symptomatic PAD, more potent P2Y12 inhibition with ticagrelor monotherapy, did not reduce MACE (HR 1.02, 95% CI: 0.92–1.13, p=0.65) or lower-limb revascularization (HR 0.95, 95% CI: 0.87–1.05, p=0.30) compared to clopidogrel, with a similar rate of major bleeding (HR 1.10, 95% CI: 0.84–1.43, p=0.49) [15]. The use of SAPT with ticagrelor may be therefore reserved to PAD patients who are non-responders to clopidogrel. Although neutral, the EUCLID trial is of clinical utility, raising awareness of a higher CV risk in the subgroup of PAD patients with concomitant CAD (N=4032, 29%), that had higher composite rates of CV death, MI, and ischemic stroke (15.3% vs. 8.9%, HR 1.50, 95% CI: 1.13–1.99; p=0.005) compared to those without CAD (Figure 1, Panel B).
3. Dual Antiplatelet Therapy
Aspirin, through the inhibition of the cyclooxygenase 1, and prasugrel, ticagrelor or clopidogrel, blocking the platelet receptor for adenosine diphosphate P2Y12, reduce the production of thromboxane A2 and inhibit platelets activation and aggregation [16]. DAPT is the standard therapy in the acute phase post-ACS, however duration and type of treatment in patients with stable CAD or PAD is still subject of ongoing debate.
In the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization Management and Avoidance (CHARISMA) trial, 15,603 patients with established CV disease or high risk profile were randomly assigned either to DAPT with aspirin and clopidogrel or aspirin alone. Although the overall trial was neutral, in the subgroup of patients with prior MI, the addition of clopidogrel to aspirin significantly reduced the primary endpoint of CV death, MI, or stroke (HR 0.77, 95% CI: 0.62–0.98; p=0.03) [17]. In PAD patients (n=3,096), MACE were not significantly reduced (HR 0.85, 95% CI: 0.66–1.08; p=0.18), and there was a numerically lower rate of peripheral arterial bypass surgery (p=0.07) with similar risk of leg amputation, at the cost of increased moderate bleeding (HR 1.36, 95% CI: 1.03–1.79; p=0.03) [18]. The use of DAPT with ticagrelor, in patients with prior MI, was examined in the Prevention of Cardiovascular Events TIMI 54 in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin-Thrombolysis in Myocardial Infarction 54 (PEGASUS-TIMI 54). Patients with prior MI and PAD present a double CV risk than those with PAD alone (8.4% vs. 19.3%, placebo group, p < 0.001, Figure 1, Panel A). The combination of aspirin and ticagrelor 60 mg twice daily (the approved dose) compared to aspirin alone, provided in 1,143 patients with concomitant PAD an absolute risk reduction for MACE of 4.1% and a significant reduction in risk of MALE (HR 0.65, 95% CI: 0.44–0.95, p=0.026) with no differences in TIMI major bleeding (HR 1.18, 95% CI: 0.29–4.70;p=0.82) compared to patients without PAD [19]. Subgroup analyses from the Dual Antiplatelet Therapy (DAPT) and Prolonging Dual Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia Study (PRODIGY) trials provided information regarding extended use of DAPT after coronary stenting in patients with PAD. In the DAPT trial, extended DAPT (clopidogrel or prasugrel plus aspirin for 30 vs. 12 months) was associated with consistent ischemic benefit among patients with (HR: 0.63; 95%CI: 0.32-1.22) and without PAD (HR: 0.53; 95% CI: 0.42, 0.66, p for interaction=0.63) [20], while in the PRODIGY trial, there was a significant interaction based on PAD. Prolonged versus shorter DAPT duration was associated with a greater reduction in MACE, in patients with PAD (16.1% vs. 27.3%; HR, 0.54;95%CI, 0.31-0.95 P =0.03) compared with those without PAD (9.3% vs. 7.4%; HR, 1.28; 95%CI, 0.92-1.77; P = 0.15, p for interaction 0.01) [21]. Based on these overall evidences the current guidelines for CCS recommends a prolonged DAPT regimen in post-MI patients with a high risk of ischaemic events, such as those with concomitant PAD, and without high bleeding risk, if they have tolerated the DAPT regimen for 1 year [6].
Finally, the inhibition thrombin-induced platelet aggregation through PAR-1 with vorapaxar has been investigated in the Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events – Thrombolysis in Myocardial Infarction (TRA-2°P-TIMI 50) which enrolled a broad population of patients with ASCVD [22]. Consistently with the other studies, patients with both CAD and PAD presented with higher risk of MACE (12.8% vs. 7.6%), More interestingly, there was significant heterogeneity in the magnitude of benefit of vorapaxar therapy in PAD patients with CAD, that experienced a greater benefit in term of MACE reduction compared to those with PAD alone (number needed to treat 45 vs. 1000) [23]. In the FDA approved population (patients with CAD or PAD without history of stroke/transient ischemic attack) the benefit of vorapaxar was associated with increased bleeding, leading to a class IIB recommendation in the current American Guidelines [24]. The overall findings highlight the clinical importance of identifying subgroups of patients that derive greater benefit from a more intense antithrombotic approach.
4. Therapy with Aspirin Combined with an Anticoagulant Drug
Beside platelets activation and aggregation, coagulation is the other key player in thrombus formation. Atherosclerotic plaque rupture exposes tissue factor, which initiates the coagulation cascade and triggers, through the activation of factor X to factor Xa, thrombin generation and fibrin formation. Both thrombin and factor Xa, through the protease-activated receptors (PARs), enhanced platelet activation, with a continuous cross-talking between the coagulation and platelet pathway. Furthermore, is now well established that in patients with acute coronary syndromes a hypercoagulable state persists for a prolonged period after clinical stabilization and it is associated with worse CV outcome [25,26,27]. Finally, factor Xa and thrombin modulate a number of inflammation pathways, which further supports their contributing role in atherogenesis and its thrombotic complications [28].
Thus, hypothesizing a synergistic effect, a strategy combining an oral anticoagulant on top of a single antiplatelet agent has been investigated in studies enrolling patients with ASCVD. Particularly, the combination of aspirin with a low-dose of the selective direct factor Xa inhibitor rivaroxaban at the dosage of 2.5 mg b.i.d., showed to reduce the rates of cardiovascular death and all-cause death (2.9% versus 4.5%; HR, 0.68; 95% CI, 0.53–0.87) compared with placebo in the ATLAS ACS 2-TIMI 51 trial (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome 2–Thrombolysis in Myocardial Infarction 51), enrolling 15 526 patients with acute coronary syndromes [29].
This strategy was therefore tested in the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial enrolling patients (N=27,395) with established coronary or peripheral artery disease (included carotid artery disease). Participant subjects have been randomized to rivaroxaban 5 mg OD alone, rivaroxaban 2.5 mg BID plus aspirin and aspirin alone. The trial has been stopped earlier owing to overwhelming proof of efficacy of rivaroxaban 2.5 mg BID plus aspirin, which provided a 24%relative risk reduction of MACE (rivaroxaban plus aspirin vs. aspirin alone: HR 0.76, 95% CI 0.66–0.86, P < 0.001; rivaroxaban versus aspirin: HR 0.90, 95% CI 0.79–1.03, P = 0.12) driven by reductions in the rate of CV death and stroke. All cause of death was significantly reduced by 18% in the rivaroxaban 2.5 mg plus aspirin arm (HR 0.82, 95% CI 0.71–0.96; P = 0.01). Major bleeding, according to a modified International Society on Thrombosis and Haemostasis (ISTH) classification occurred more frequently in patients in the rivaroxaban plus aspirin group than in those receiving aspirin alone (3.1% versus 1.9%; HR 1.70, 95% CI 1.40–2.05, P < 0.001), driven by gastrointestinal bleeding, with no significant differences in fatal bleeding or intracranial bleeding [30].
A subgroup analysis of 6,391 patients with lower extremity PAD demonstrated that aspirin plus a low-dose rivaroxaban, compared to aspirin alone, reduced peripheral vascular outcome by 24% (5.5% versus 7.1%; P = 0.03), MALE by 43% (1.5% versus 2.6%; P = 0.01) and amputation by 58% (0.5% versus 1.2%; P = 0.01), at the cost of a significant increase in major bleeding (2.0% versus 3.2%; P = 0.02), without difference in intracranial or fatal bleeding [5]. These findings have been confirmed, in the Vascular Outcomes Study of ASA (acetylsalicylic acid) Along with Rivaroxaban in Endovascular or Surgical Limb Revascularization for PAD (peripheral artery disease) (VOYAGER-PAD) trial, enrolling 6,564 patients who underwent infrainguinal percutaneous or surgical revascularization and were randomized within 10 days after revascularization, to rivaroxaban 2.5 mg twice daily plus aspirin or to placebo plus aspirin [31]. Thus, the use of a combination of low-dose rivaroxaban plus aspirin in PAD patients has been confirmed across a broad spectrum of disease. The consensus document from the ESC working group on aorta and peripheral vascular diseases recommends therefore rivaroxaban 2.5 mg bid (the so-called “vascular-dose”) on top of low-dose aspirin in stable patients with chronic symptomatic PAD or undergoing revascularization (surgical or endovascular) for lower extremities PAD without conditions at high risk of bleeding.
5. A Practical Approach
Although antithrombotic therapy is the cornerstone of both CAD and PAD, the optimal strategy is still debated, particularly when these conditions are associated. Available evidences suggest that the higher is the burden of atherosclerosis the higher is the benefit of a high intensity antithrombotic therapy. The price to be paid is an increased of major bleeding, primarily of gastrointestinal origin, without excess in intracranial or fatal bleeding. Therefore, in accordance with the most recent ESC guidelines [6], the first step for a practical approach in selecting the optimal antithrombotic in patients with stable CAD or PAD, is the evaluation of the bleeding risk (Figure 2). Only patients at low bleeding risk should be considered for a regimen of high intensity antithrombotic therapy. In this contest two factors, anemia at baseline and a previous history of bleeding requiring hospitalization, have emerged as useful characteristic to identify patients at increased risk of bleeding [32]. Those patients should be considered for SAPT, always taking into account that bleeding risk changes over time and periodic re-assessment is mandatory [33].
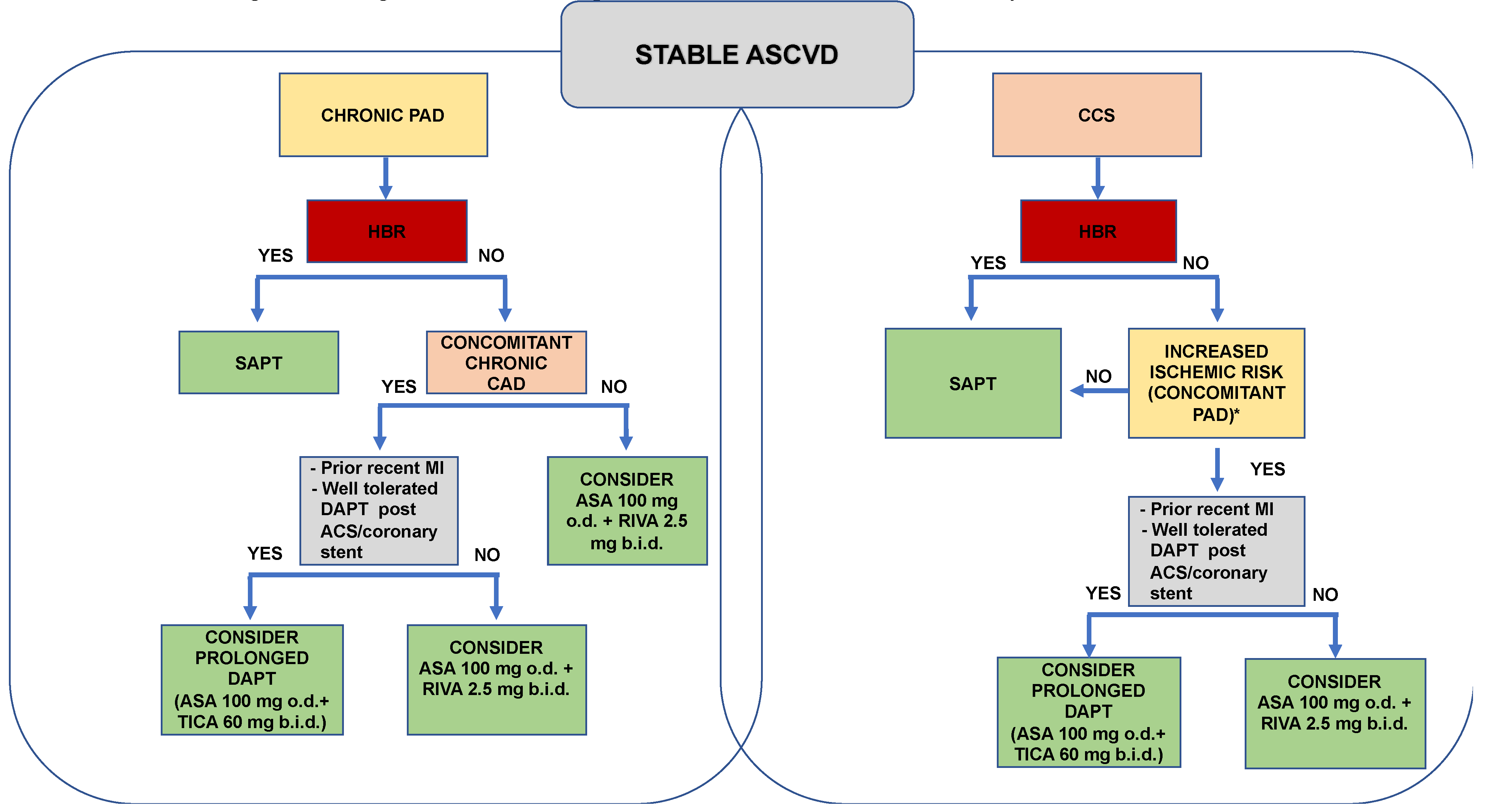
Figure 2.
Selecting antithrombotic therapy in patients with stable CAD and PAD: a practical approach.
Figure 2.
Selecting antithrombotic therapy in patients with stable CAD and PAD: a practical approach.
High bleeding risk (HBR) defined as history of intracerebral haemorrhage or ischaemic stroke, history of other intracranial pathology, recent gastrointestinal bleeding or anaemia due to possible gastrointestinal blood loss, other gastrointestinal pathology associated with increased bleeding risk, liver failure, bleeding diathesis or coagulopathy, extreme old age or frailty, or renal failure requiring dialysis or with eGFR <15 mL/min/1.73 m2. CCS: Chronic coronary syndrome; PAD: peripheral artery disease; DAPT: Dual antiplatelet therapy; SAPT: Single antiplatelet therapy; RIVA: Rivaroxaban; TICA: Ticagrelor; ASA: Aspirin; o.d.: once daily; b.i.d.: twice a day; Myocardial infarction; ACS: Acute coronary syndrome.
For patients at low bleeding risk, the following step is the evaluation of the ischemic risk. Patients with CAD, especially with multivessel disease, and concomitant PAD have been categorized to be at high ischemic risk and a more intense antithrombotic regimen with DAPT or DAT may be therefore considered in this group. Particularly, in patients with CAD or PAD, who experienced a recent MI and have well-tolerated the “bleeding stress-test” of the 1-year period of DAPT following the acute event, a prolonged DAPT therapy may be considered over a strategy combining aspirin and an anticogulant. Based on the results of the PEGASUS TIMI 54 trial ticagrelor 60 mg b.i.d, should be the preferred option [19,34].
6. Conclusions
Based on the overall results of RCTs and subgroup analyses of patients with coronary and peripheral artery disease, antithrombotic therapy should be individualized considering the clinical presentation, burden of the atherosclerotic disease, together with the bleeding-ischemic balance. A stepwise selection may be useful for clinician to identify those patients who benefit the most from a more intense antithrombotic therapy. Further data regarding subgroup of patients with PAD in large RCTs of CAD and, above of all, RCTs randomizing primarily patients with PAD are needed, in order to further define the optimal antithrombotic therapy in this setting and improving precision medicine.
References
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Suárez, C.; Zeymer, U.; Limbourg, T.; Baumgartner, I.; Cacoub, P.; Poldermans, D.; Röther, J.; Bhatt, D.L.; Steg, P.G.; Investigatorsa, R.R. Influence of polyvascular disease on cardiovascular event rates. Insights from the REACH Registry. Vasc. Med. 2010, 15, 259–265. [Google Scholar] [CrossRef]
- Cotter, G.; Cannon, C.P.; McCabe, C.H.; Michowitz, Y.; Kaluski, E.; Charlesworth, A.; Milo, O.; Bentley, J.; Blatt, A.; Krakover, R.; et al. OPUS-TIMI 16 Investigators. Prior peripheral arterial disease and cerebrovascular disease are independent predictors of adverse outcome in patients with acute coronary syndromes: are we doing enough? Results from the Orbofiban in Patients with Unstable Coronary Syndromes-Thrombolysis In Myocardial Infarction (OPUS-TIMI) 16 study. Am. Hear. J. 2003, 145, 622–627. [Google Scholar] [CrossRef]
- Hess, C.N.; Bonaca, M.P. Contemporary Review of Antithrombotic Therapy in Peripheral Artery Disease. Circ. Cardiovasc. Interv. 2020, 13, e009584. [Google Scholar] [CrossRef] [PubMed]
- Aronow, W.; Ss, A.; F, C.; Jw, E.; J, B.; L, D.; V, A.; Mt, A.; Krh, B.; K, K.; et al. Faculty Opinions recommendation of Major adverse limb events and mortality in patients with peripheral artery disease: the compass trial. J Am Coll Cardiol. 2018, 71, 2306. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; et al.; ESC Scientific Document Group 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018, 39, 763–816. [Google Scholar]
- Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002, 324, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.S.; Kranty, M.J.; Kittelson, J.M.; et al. Aspirin for the prevention of cardiovascualr events in patients with peripheral artery disease: a meta-analysis of randomized trials. JAMA 2009, 301, 1909–1919. [Google Scholar] [CrossRef]
- CAPRIE Steering Committee. CAPRIE Steering Committee A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef]
- Ferreiro, J.L.; Bhatt, D.L.; Ueno, M.; et al. Impact of smoking on long-term outcomes in patients with atherosclerotic vascular disease treated with aspirin or clopidogrel: insights from the CAPRIE trial (Clopidogrel Versus Aspirin in Patients at Risk of Ischemic Events). J Am Coll Cardiol. 2014, 63, 769–777. [Google Scholar] [CrossRef]
- Bauersachs, R.; Wu, O.; Briere, J.-B.; Bowrin, K.; Borkowska, K.; Jakubowska, A.; Taieb, V.; Toumi, M.; Huelsebeck, M. Antithrombotic Treatments in Patients with Chronic Coronary Artery Disease or Peripheral Artery Disease: A Systematic Review of Randomised Controlled Trials. Cardiovasc. Ther. 2020, 2020, 1–11. [Google Scholar] [CrossRef]
- Hess, C.N.; Hiatt, W.R. Antithrombotic Therapy for Peripheral Artery Disease in 2018. JAMA 2018, 319, 2329–2330. [Google Scholar] [CrossRef]
- Clavijo, L.C.; Al-Asady, N.; Dhillon, A.; Matthews, R.V.; Caro, J.; Tun, H.; Rowe, V.; Shavelle, D.M. Prevalence of high on-treatment (aspirin and clopidogrel) platelet reactivity in patients with critical limb ischemia. Cardiovasc. Revascularization Med. 2018, 19, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, W.R.; Fowkes, F.G.R.; Heizer, G.; Berger, J.S.; Baumgartner, I.; Held, P.; Katona, B.G.; Mahaffey, K.W.; Norgren, L.; Jones, W.S.; et al. EUCLID Trial Steering Committee and Investigators. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease. New Engl. J. Med. 2017, 376, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Bhatt, D.L.; Eikelboom, J.W.; Fox, K.A.A.; Geisler, T.; Gibson, C.M.; Gonzalez-Juanatey, J.R.; James, S.; Lopes, R.D.; Mehran, R.; et al. Dual-pathway inhibition for secondary and tertiary antithrombotic prevention in cardiovascular disease. Nat. Rev. Cardiol. 2020, 17, 242–257. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Fox, K.A.; Hacke, W.; et al.; CHARISMA Investigators Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006, 354, 1706–1717. [Google Scholar] [CrossRef] [PubMed]
- Cacoub, P.P.; Bhatt, D.L.; Steg, P.; Topol, E.J.; Creager, M.A. ; for the CHARISMA Investigators Patients with peripheral arterial disease in the CHARISMA trial. Eur. Hear. J. 2009, 30, 192–201. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bhatt, D.L.; Storey, R.F.; et al. Faculty Opinions recommendation of Ticagrelor for prevention of ischemic events after myocardial infarction in patients with peripheral artery disease. J Am Coll Cardiol. 2016, 67, 2719–2728. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Yeh, R.W.; Kereiakes, D.J.; et al.; Dual Antiplatelet Therapy Study Investigators Extended Duration Dual Antiplatelet Therapy After Coronary Stenting Among Patients With Peripheral Arterial Disease: A Subanalysis of the Dual Antiplatelet Therapy Study. JACC Cardiovasc Interv. 2017, 10, 942–954. [Google Scholar] [CrossRef]
- Franzone, A.; Piccolo, R.; Gargiulo, G.; et al. Prolonged vs Short Duration of Dual Antiplatelet Therapy After Percutaneous Coronary Intervention in Patients With or Without Peripheral Arterial Disease: A Subgroup Analysis of the PRODIGY Randomiyed Clinical Trial. JAMA Cardiol 2016, 1, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Creager, M.A.; Olin, J.; et al. Peripheral Revascularization in Patients With Peripheral Artery Disease With Vorapaxar: Insights From the TRA 2°P-TIMI 50 Trial. JACC Cardiovasc Interv. 2016, 9, 2157–2164. [Google Scholar] [CrossRef]
- Qamar, A.; A Morrow, D.; A Creager, M.; Scirica, B.M.; Olin, J.W.; A Beckman, J.; A Murphy, S.; Bonaca, M.P. Effect of vorapaxar on cardiovascular and limb outcomes in patients with peripheral artery disease with and without coronary artery disease: Analysis from the TRA 2°P-TIMI 50 trial. Vasc. Med. 2020, 25, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Matsushita, K.; Aboyans, V.; et al.; American Heart Association Council on Epidemiology and Prevention; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; Council on Lifestyle and Cardiometabolic Health; Council on Peripheral Vascular Disease; and Stroke Council Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e171–e191. [Google Scholar] [CrossRef] [PubMed]
- Merlini, P.A.; Bauer, K.A.; Oltrona, L.; Ardissino, D.; Cattaneo, M.; Belli, C.; Mannucci, P.M.; Rosenberg, R.D. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation 1994, 90, 61–68. [Google Scholar] [CrossRef]
- Ardissino, D.; Merlini, P.A.; Bauer, K.A.; Galvani, M.; Ottani, F.; Franchi, F.; Bertocchi, F.; Rosenberg, R.D.; Mannucci, P.M. Coagulation activation and long-term outcome in acute coronary syndromes. Blood 2003, 102, 2731–2735. [Google Scholar] [CrossRef]
- Weitz, J.I. Insights into the role of thrombin in the pathogenesis of recurrent ischaemia after acute coronary syndrome. Thromb. Haemost. 2014, 112, 924–931. [Google Scholar] [CrossRef]
- Mega, J.L.; Braunwald, E.; Wiviott, S.D.; Bassand, J.-P.; Bhatt, D.L.; Bode, C.; Burton, P.; Cohen, M.; Cook-Bruns, N.; Fox, K.A.A.; et al. ATLAS ACS 2–TIMI 51 Investigators. Rivaroxaban in Patients with a Recent Acute Coronary Syndrome. N. Engl. J. Med. 2012, 366, 9–19. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; et al. ; COMPASS Investigators. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N Engl J Med. 2017, 377, 1319–1330. [Google Scholar]
- Bonaca, M.P.; Bauersachs, R.M.; Anand, S.S.; et al. Rivaroxaban in Peripheral Artery Disease after Revascularization. N Engl J Med. 2020, 382, 1994–2004. [Google Scholar] [CrossRef]
- Magnani, G.; Ardissino, D.; Im, K.; Budaj, A.; Storey, R.F.; Steg, P.G.; Bhatt, D.L.; Cohen, M.; Ophius, T.O.; Goudev, A.; et al. Predictors, Type, and Impact of Bleeding on the Net Clinical Benefit of Long-Term Ticagrelor in Stable Patients With Prior Myocardial Infarction. J. Am. Hear. Assoc. 2021, 10, e017008. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Im, K.; Magnani, G.; Bansilal, S.; Dellborg, M.; Storey, R.F.; Bhatt, D.L.; Steg, P.G.; Cohen, M.; Johanson, P.; et al. Patient selection for long-term secondary prevention with ticagrelor: insights from PEGASUS-TIMI 54. Eur. Hear. J. 2022, 43, 5037–5044. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



