Submitted:
16 June 2023
Posted:
20 June 2023
You are already at the latest version
Abstract
Cancer is the most feared disease, with more than 1.6 million cases each year. Cancer can start almost anywhere in the human body, from the uncontrollable growth and multiplication of damaged cells. Cancerous tumors can spread into the human body (a process called metastasis) as a solid form usually, but the cancers of blood generally do not. Cancer treatment includes chemotherapy, surgery and radiations. In this article we will address inorganic compounds as a source of treatment, diagnosis, carriers of active substances.
Keywords:
cancer
; cisplatin
; selenium
; zinc
1. Introduction
The prevalence of sickness is rapidly rising due to the expanding population. Among the many threats to humankind, cancer is increasingly a major cause of death and mortality on a global scale. Nearly 15% of people worldwide die from cancer, making it the second leading cause of death, according to the World Health Organization [1]. In men, the prostate, lung and bronchus, colon and rectum, and urinary bladder have the largest percentages of cancer kinds. The breast, lung, and bronchi, colon, and rectum, uterine corpus, and thyroid are the areas of the female body where cancer is most common. According to this information, a significant amount of cancer in men and women is caused by prostate and breast cancer Blood cancer and malignancies of the brain and lymph nodes are the two cancers that affect youngsters at the highest rates [2,3]. Currently, surgery, radiotherapy, and chemotherapy are still the first-line cancer treatments that are prescribed as either a single therapy or in combination, patient-tailored to the tumor’s characteristics (such as type, stage, aggressiveness, and accessibility), the patient’s symptoms, and their health conditions. Immunotherapies are emerging as cutting-edge therapy to prime the patient’s immune system to effectively combat their cancer cells. Nonspecific distribution, insufficient medication concentration, and lax monitoring of pharmaceuticals reaching the tumor are the main issues with current cancer treatment procedures [4,5].
2. Materials and Methods
Initially, we searched research papers using keywords such as cancer, inorganic substances, cisplatin, zinc, and selenium. The publications that met these word criteria were then thoroughly scrutinized, and their conclusions were reported.
3. Results
3.1. Cisplatin
Cisplatin, also known as cis-diamminedichloroplatinum (II), is a coordination compound of metallic (platinum) with square planar geometry. At room temperature, it is a white or deep yellow to yellow-orange crystalline powder that is soluble in dimethylprimanide and N, N-dimethylformamide and only moderately soluble in water. Under normal conditions of pressure and temperature, cisplatin is stable, but it can gradually change into the trans-isomer over time. [4] Since it has demonstrated anticancer activity in a number of tumors, including ovarian cancer and solid tumors of the head and neck, cisplatin has received particular attention. Its cytotoxic capabilities were found in the 1960s, and by the end of the 1970s, it had established itself as a crucial component in the systemic treatment of malignancies. Cisplatin is one of the most effective chemotherapy medications available for treating cancer. It was the first platinum compound for cancer treatment to receive FDA approval in 1978 [6]. Despite the fact that majority of the patients receiving cisplatin initially respond well to its chemotherapy, some of them later relapse and develop resistance, which reduces the drug’s clinical value. Drug resistance may result from epigenetic changes at the cellular and molecular levels, including high levels of DNA damage repair (DDR), changes in DNA methylation progression, uprooted and poor regulation of mRNA expression levels, poor transcriptional regulation, and interference with apoptosis, according to evidence from tissue culture studies. The molecular cytotoxicity mechanisms of cisplatin includes cytotoxicity caused by losing one chloride ligand, attaching to DNA to create intra-strand DNA adducts, and preventing DNA synthesis and cell development. By stopping cisplatin-induced cell death by activating the ATM (ataxia telangiectasia mutated) pathway, the DNA lesions created by cisplatin-induced DNA damage stimulate DNA repair response via NER (nuclear excision repair system) [7].
3.1.1. Cisplatin in lung cancer
One of the most frequent fatal cancers is still lung cancer. 15% of all lung cancers are small cell lung cancers (SCLCs). The main medications for SCLC at the moment are platinum-based therapies. Because of its potent anticancer activity, cisplatin is frequently chosen in clinical trials; nonetheless, it has side effects that include nausea, vomiting, and kidney damage. Therefore, large-dose infusion is required in chemotherapy based on cisplatin and urine volumes should be monitored to prevent renal toxicity.
In the case of NSCLC, surgery is the predominant treatment, with adjuvant cisplatin-based chemotherapy being used in cases of stage II and III illness.
Due to poor medication delivery to the tumors, several potent therapeutic medicines tested in vitro did not provide any effects in vivo. Using protective substances such curcumin, berberine, resveratrol, and cinnamon, scientists have been effective in decreasing side effects or improving the anticancer efficacy of CP to get over this obstacle. To increase the bioavailability of medications, drug delivery systems incorporating micro- and nanocarriers are helpful. For instance, adding CP to a wide range of nanoparticles has proven to be effective in boosting drug effectiveness.
Selecting individuals with a suitable glomerular filtration rate (GFR) of >60 ml/min is the first step in preventing platinum-associated nephrotoxicity. GFR may be estimated using a variety of techniques, all of which are outside the purview of this review.
Serotonin receptor-3 (5-HT3) antagonists and corticosteroids have historically been used by clinicians to treat the possibly dose-limiting toxicity of emesis. Aprepitant, an oral neurokinin-1 (NK-1) receptor antagonist, has been part of the standard of treatment for patients receiving cisplatin ever since it was first introduced in 2003 for extremely emetic chemotherapy.
When used with dexamethasone and a 5-HT3 receptor antagonist, it enhances the likelihood that emesis will be completely controlled (i.e., there won’t be any vomiting and no need for rescue treatment) from around 50% to 75%. On delayed emesis in particular, a strong effect is noticeable. The Multinational Association of Supportive Care in Cancer (ESMO/MASCC) recommendations on nausea and vomiting were revised in 2010 to take these discoveries into account.
The most frequent cisplatin treatment dose-limiting issue is peripheral neurotoxicity. Paraesthesias and numbness are the primary symptoms of cisplatin neurotoxicity, and they often appear within the first few medication cycles. After a few treatment cycles, ataxia, paraesthesia, and loss of vibration perception may become evident. Peripheral neuropathy alterations may start after the treatment is finished and continue for 2.5 to 5.5 months after the cisplatin has been stopped. Monitoring with audiograms should be taken into consideration because the cumulative and potentially permanent ototoxicity brought on by cis-platin. Up to 31% of patients receiving a single dosage of cis- platin 50 mg/m2 have had ototoxicity, which is characterized by tinnitus and/or hearing loss in the high frequency range [7].
3.1.2. Cisplatin in ovarian cancer
About 204,000 women worldwide are affected by epithelial ovarian cancer (EOC), which also causes about 125,000 deaths. Because it doesn’t show any symptoms until it has spread to the peritoneal cavity, when there is little chance of recovery, it is frequently referred to as the "silent killer."
Over the past 30 years, the management of advanced EOC has changed to include both chemotherapy and cytoreductive surgery (CRS). When combined with chemotherapy, CRS is thought to be effective because it eliminates large tumors that contain poorly oxygenated, non-proliferating cells that are either already resistant to chemotherapy or may become so in the future. This leaves behind smaller tumors that have a higher percentage of cells that are in the proliferative phase, making them more susceptible to chemotherapy. Previously, any nodule with a dimension of less than 2 cm was considered to have "optimal" residual disease at the conclusion of initial CRS for EOC; however, it is now known that patients with absolutely no macroscopic residual disease have the best prognosis.
One of the most potent medications used to treat ovarian cancer intraperitoneally is cisplatin. According to pharmacokinetic analyses of IP cisplatin, its high peritoneal clearance (43 ml/min) is a result of its large molecular weight. Early clinical trials demonstrating the safety and efficacy of IP treatment with cisplatin at recommended dosages (So-150 mg/m’) [8,9].
3.1.3. Cisplatin in head and neck cancer
Malignant tumors that originate in the upper aero-digestive tract, which includes the lips, mouth, tongue, nose, throat, vocal cords, and a portion of the esophagus and windpipe, are referred to as head and neck cancer (HNC). With an annual incidence rate of more than 500,000 cases, HNC is the eighth most common kind of cancer worldwide. It’s interesting to note that squamous cell carcinomas make up over 90% of head and neck cancers. Unfortunately, almost 50% of these cancers are already in a progressive stage when they are examined, necessitating treatment with a variety of methods (such as radiotherapy, chemotherapy, and surgery) in order to protect organs. First-line surgical chemo-radiation treatment for HNC often involves the use of cisplatin. The Radiation Therapy Oncology Group (RTOG) schedule, which combines conventional radiation with the administration of cisplatin at a dose of 100 mg/m2, is the most widely used treatment plan. According to the RTOG schedule, cisplatin can also be given at a preferred dose of 40 mg/m2 in addition to conventional or more intense radiation. Additionally, when treating locally advanced head and neck cancer, cisplatin in combination with the well-known chemotherapy such as drugs docetaxel and fluorouracil has been found to be more effective for induction therapy than cisplatin and fluorouracil alone [10,11].
The uses of platinum compounds and corresponding doses is presented in Table 1.
3.2. Arsenic Trioxide
Acute promyelocytic leukemia (APL) patients who have just been diagnosed as well as those who have relapsed have both responded favorably to treatment with arsenic trioxide. It generates complete remissions when used alone, with few side effects and barely any myelosuppression.
Some APL patients are not candidates for As2O3 treatment as the initial stage of treatment due to conditions such as PLZF/RAR gene positivity, moderate to severe liver or kidney dysfunction brought on by illnesses other than leukemia, relapse during continuous As2O3 maintenance treatment, or long-term exposure to arsenic.
Hemoglobin concentration, platelet count, bone marrow normoblast count, and band-cell count of peripheral WBC all show positive associations with therapeutic efficacy and prognosis. WBC count, peripheral juvenile blood cell count, myeloproliferation level, and lactic dehydrogenase (LDH) activity do not correlate.
Since 20% to 30% of patients with acute myelogenous leukemia relapse despite receiving all-trans retinoic acid and combination chemotherapy, the activity of arsenic trioxide in patients with APL is a significant finding.
The use of an As2O3 regimen may be advised in the clinical cases listed below:
1) APL that has not previously been treated or that has just been diagnosed
2) APL that is resistant to combination chemotherapy or all-trans retinoic acid (RA), has returned after a bone marrow transplant, or has recurrent illness;
3) APL in patients who cannot tolerate or should not get combination RA plus chemotherapy;
4) Maintenance therapy following complete remission (CR) from acute lymphoblastic leukemia;
5) CGL, some acute nonlymphocytic leukemia subtypes, and those with myelodysplastic syndromes (MDS), if they are accompanied by an excessive rise in promyelocytes.
Adults with APL get a daily injection of 10 ml of As2O3 (1 g/L), which is given intravenously over a 3–4-hour period in 250–500 ml of glucose solution (50 g/L) or normal saline.
The daily dosage for children with APL is 6 mg/m2 (or around 0.16 mg/kg). [12]
3.3. Zinc and compounds
The most prevalent malignant tumor in men is prostate cancer (PCa). Early-stage PCa can be successfully treated with curative treatment options such surgery and radiation therapy. However, hormonal ablation of metastatic cells can result in PCa cells losing their dependence on androgen, which would then result in a hormone-independent tumor with a very low chance of survival.
Human prostate gland glandular epithelial cells have the capacity to accumulate a significant amount of zinc, two to five times which of other tissues. Zinc buildup prevents mitochondrial aconitase activity, which prevents cells from oxidizing citrate. In order to chelate intracellular zinc, prostate cells can build up significant amounts of citrate. Malignant cells require low zinc concentrations to activate the citrate oxidation process, which increases their energy efficiency. In contrast, normal epithelial cells accumulate zinc, which inhibits the m-aconitase. Increasing the amount of circulating zinc that is accessible for cellular absorption would, in theory, be a successful strategy for treatment.
Organic substances known as Schiff bases have a variety of biological characteristics. The effectiveness of these compounds as chemotherapeutic agents is greatly influenced by the kind of metal and the complexity of the Schiff base. Researchers utilized the widely employed human prostate cell lines PC3 and PNT1A in biomedical research. According to a comparison of the microscopic pictures of the two cells, the Zn-SB complex was found to be dispersed throughout the cytoplasm of PC3 cells, in contrast to PNT1A cells, where it was restricted to the membrane. In contrast to PNT1A cells, which remained healthy after 12 hours of treatment, PC3 cells began to show membrane "blebbing," a sign of cell death through apoptosis . Regarding the innate immunity, it was discovered that cytotoxicity of natural killer cells, phagocytic activity of neutrophils, the possibility of immune cells to generate oxidants against pathogens and macrophages can be affected by zinc deficiency [14]. The function of adaptive immunity is also influenced by zinc deficiency, particularly the lymphocytes’ number and activity. Low levels of zinc cause thymic atrophy, which leads to an imbalance in the subsets of helper T cells. In addition, cytokine production affected by zinc deficiency leads to oxidative stress and inflammation. Even zinc border deficiency, the severity of which is often underestimated, affects different aspects of immunity. [16,17,18,19,20,21,22,23,24,25]. In Table 2 are summarizing some common zinc compounds used in cancer treatment, along with their typical doses.
3.4. Selenium and compounds
Various forms and doses of selenium have been used in clinical trials to evaluate selenium’s efficacy as a chemopreventive agent, with varying degrees of success. Instead of being directly cytotoxic agents, selenium species are currently being therapeutically assessed as modulators of medication responses. Both immune-suppressing and immune-boosting effects of selenium have been demonstrated. Some of selenium’s immune-stimulating qualities are caused, at least in part, by its role in promoting B cell activation and proliferation (as found in humans) and/or immune cell differentiation (as seen in mouse research).
Basal plasma Selenium levels in the participants are crucial for Seleneium’s prophylactic impact, based on researches on humans. Males with Se concentrations between 135 and 170 ng/mL had a 15%–25% lower risk of prostate cancer than those with plasma levels of Se around 60 ng/mL. Even more noticeably, their probability of developing advanced prostate cancer was decreased by 40%–50%. These findings suggested that Selenium may prevent the spread of prostate cancer metastases.
There has been considerable debate over the connection between Selenium level and cancer. The majority of studies show decreased Selenium levels in thyroid cancer patients. A high quantity of free radicals produced by oxidative stress might be linked to Selenium insufficiency in a number of disorders, including cancer. Thyroid tumor tissue samples show a much higher generation of ROS than healthy tissue. Selenium plays a significant role in the removal of ROS and is found in high amounts in the thyroid. Therefore, a change in its level could have an impact on the thyroid’s GPx1 and GPx3 antioxidant selenoproteins, which are sensitive to Se intake.
At various stages of tumor development, abnormal redox regulation is seen in cancer cells. To keep the redox equilibrium, tumor cells need antioxidant molecules such selenoproteins. Antioxidant protein expression rises in several cancer types while falling in others. Indeed, the expression of selenoproteins like the GPx gene differs significantly between normal and tumor cells. 15 selenoprotein genes were examined in two cohorts for colorectal cancer. In contrast to SePP and selenoprotein S, both selenoproteins TRx3 and GPx2 were increased in adenoma and cancer. The fact that GPx2 and TRx3 are target genes for Wnt signaling explains why their gene expression has risen. The majority of the colorectal cancer tissues have this signaling pathway active. The fact that certain selenoproteins appear to inhibit tumor cell development while others appear to promote it emphasizes how poorly understood the carcinogenesis pathways associated with the Selenium status are [26,27,28,29,30,31,32,33,34,35,36,37]. In Table 3 are summarizing some common zinc compounds used in cancer treatment, along with their typical doses.
3.5. Ruthenium
Ruthenium complexes, which provide distinct modes of action and a diverse range of activities, are already acknowledged as an efficient substitute for platinum complexes. There are many qualities of ruthenium such as:
Ruthenium complexes have the capacity to coordinate ligands that can modulate their activity and have the same kinetics of ligand substitution in aqueous medium as that of Pt (II) complexes.
They can exist in multiple oxidation states (II, III, and IV), all accessible under physiologic conditions, an advantage in the reducing environment of cancer tissues.
They have the potential to occupy a large number of spatial positions due to its octahedral coordination geometry, allowing for the exploration of more and different ligands than platinum complexes.
They exhibited lower toxicity compared to platinum compounds and were attributed to their ability to mimic iron binding to serum transferrin, with higher selectivity for their targets as a result of tumor-specific uptake as opposed to uptake by healthy tissues.
Two different mechanisms—energy-dependent endocytosis and active transport and energy-independent enhanced diffusion and passive diffusion—can be used by cells to absorb ruthenium complexes. For instance, researches using flow cytometry revealed that the ruthenium compounds penetrated the cell membrane and accumulated in the nucleus, causing cell cycle arrest and death in multiple tumor cells [38,39,40,41,42,43,44,45]. Ruthenium compounds have gained attention in cancer research as potential chemotherapeutic agents. In Table 4 are summarizing some common ruthenium compounds used in cancer treatment, along with their typical doses.
3.6. Copper
Because endogenous metal ions may result in less systemic toxicity, copper complexes are the most researched and used complexes for their antitumor properties. The characteristics of the ligands, which may also have antiproliferative activities, govern the features of the copper complexes. In order to demonstrate several anticancer processes, a number of Cu(II) complexes have been created with a range of ligands comprising N, S, or O. The ligands engage noncovalently with proteins or intercalate into the DNA molecule to neutralize the copper ion’s electrical charge and make it easier for the complex to pass across the cell membrane. Copper complexes have the ability to cause DNA cleavages through oxidative or hydrolytic processes. Recently, the copper (II) complex [Cu(C20H22NO3)2]*H2O was created, and the spectroscopic methods used to analyze it revealed that the complex attaches to the DNA of the calf thymus by partial intercalation and exhibits a static quenching process as the binding mechanism. A beneficial synergistic effect may be taking place since the cytotoxicity assay in cancer cell lines revealed increased cytotoxicity when compared to the Schiff base ligand.
Thiosemicarbazone ligands are copper compounds that have anticancer action by blocking enzymatic function and causing cell apoptosis. By concentrating on DNA and proteins, a Cu pro-drug created from thiosemicarbazone and based on the His146 residue in the IB subdomain of human serum albumin (HSA-PA) that has been mutated by palmitic acid (PA) can destroy cancer cells. Additionally, by substituting His146 for the leaving group and coordinating it with Cu2+ to form the HSA PA complex, the effective delivery of the Cu pro-drug was enhanced. The HSA-PA combination demonstrated improved tolerability, increased drug accumulation in the tumor, a greater ability to suppress tumor development, and less toxicity in surrounding tissues [46,47,48,49,50]. Copper compounds have been investigated for their potential role in cancer treatment. In Table 5 are summarizing some common copper compounds used in cancer research, along with their typical doses.
3.7. Vanadium
Vanadium compounds’ main molecular targets for their anticancer effects include caspases, which can cause cell cycle arrest and cell death, the breakdown of cellular metabolism through the production of ROS, GSH depletion, alterations in cellular organelles, and various signal transduction pathways. A metal ion is sandwiched between two cyclopentadienyl rings in the metallocene vanadocene. The first vanadocene that produced intriguing results in preclinical research was vanadocene dichloride. In vitro tests of this compound against a variety of tumor cells revealed high efficacy. Vanadocene dichloride also showed anticancer effects in in vivo experiments. Some vanadocene derivatives have cytotoxic effects on T-lymphocytic leukemia cells, with DNA damage and p53 activation as the underlying mechanisms. Vanadocenes, on the other hand, function efficiently against human testicular cell lines [51,52,53,54]. Vanadium compounds have been studied for their potential anticancer properties, although their use in cancer treatment is still primarily in the experimental and preclinical stages. As such, there is limited information available on the specific doses used in human cancer treatment. In Table 6 are described some common vanadium compounds that have been investigated and their potential usage in cancer.
3.8. Osmium
Ruthenium’s heavier congeners, osmium complexes (Os(II) and Os(III) complexes), have slower kinetics than ruthenium and are substitution-inert. Osmium compounds have been widely used because of their ability to target mitochondrias, increase the production of ROS, oxidize NADH to NAD+, interfere with cell cycle progression in cancer cells, and disrupt redox signaling pathways. Osmium analogs of ruthenium anticancer drugs including RAPTA-C, NAMI-A, and KP1019 have been created in recent years. In addition, there has been progress to develop metal–chemotherapy drug complexes based on rhodium, osmium, palladium, ruthenium, and iridium noble metals similar to cisplatin (Pt-based). Similar to Rh, there has been limited literature reporting the theranostic application of Osmium nanostructures since 2010. In an in vitro study, Osmium NSs (spherical, core–shell, and nanorods) were found to be optothermal. The additional layer of silica not only improved the stability profile of NSs, but also increased the overall temperature and thermal conductivity within the NSs and system when exposed to a laser source. More recently, Osmium–tellurium nanorods were explored for enzymatic activity and were found to exhibit excellent photothermal, photocatalytic, and photodynamic activity to act as a penta-modal treatment profile against hepatocellular carcinoma. The formulation reduced hypoxia by generating O2, and reduced bone marrow and other organ toxicity by delivering the drug within the tumor [55,56]. Osmium compounds have shown promise in cancer research due to their potential cytotoxic effects. However, their use in cancer treatment is still in the experimental stage, and there is limited information available on specific doses used in human cancer therapy. In Table 7 are some common osmium compounds that have been investigated and their potential usage in cancer.
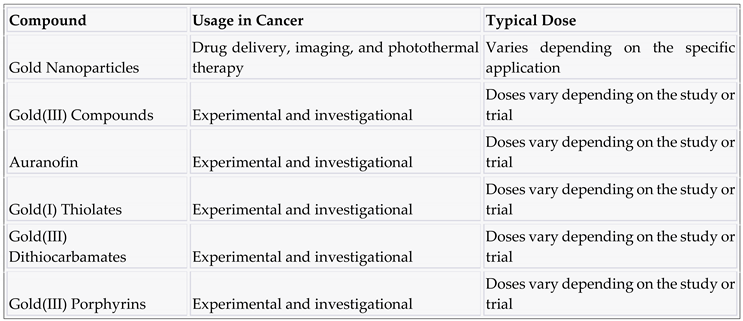
3.9. Gold and compounds
Due to its bacteriostatic, anticorrosive, and antioxidative qualities, gold is a multipurpose substance that has been used in medical applications for generations. Gold nanoparticles can absorb light at particular wavelengths, resulting in photoacoustic and photothermal properties, making them potentially useful for hyperthermic cancer treatments and medical imaging applications. This phenomenon is known as localized plasmon surface resonance (LPSR), and it has been demonstrated that colloidal gold exhibits it. Gold nanoparticles may have their LPSR photochemical activities changed by varying their size and shape, which also affects their photothermal and photoacoustic characteristics. This enables the use of various light wavelengths, such as light in the near-infrared spectrum. Gold could be produced in a nanoscale structure and passively distributed through the body. This allows the material to concentrate in tumors, which are known for their leaky blood arteries, and be safely eliminated through the urine system. Thermal stress causes tumors to become radiosensitized, which increases their propensity to react to radiation and raises cancer survival rates. Studies of metastatic head and neck squamous cell malignancies have shown this to be true, with intense radiation therapy combined with hyperthermia improving results without increasing toxicity. Traditional methods of inducing hyperthermia, however, are not the best since they are not highly effective and cause the body to produce heat in an untargeted manner throughout. The outcome is the creation of significant undesired side effects. Light is a preferable external stimulus than other techniques because it can be concentrated, adjusted, and remotely controlled. Better targeted treatments are made possible by this ease of concentration and control, which results in less harm to healthy tissues.
Recent developments in the multifunctional design of gold nanoparticles enable the regulated and targeted administration of many desired medications as well as the formation of localized heat in close proximity to cancer tissues. Gold nanoparticles can be used for photothermal therapy (PTT) to treat cancer because they have a number of advantages, including the ability to target the local tumor area while minimizing non-specific distribution, the ability to be activated by near-infrared (NIR) laser light, which allows them to penetrate deeply into biological tissues, and the ability to be modulated to create cancer PTT and drug delivery systems with multiple functions [57,58,59,60,61,62].
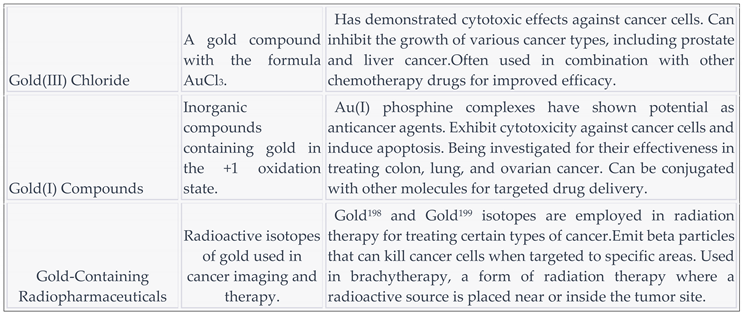
Gold compounds have been investigated for their potential applications in cancer treatment. In Table 8 are summarizing some common gold compounds used in cancer research, along with their potential usage and typical doses.

Table 9.
Gold compounds used in cancer treatment and their typical doses.
In Table 10 are presenting a gold compound and application in cancer therapy.
4. Discussion
It is crucial to look for fresh cancer treatment options while keeping in mind the wellbeing of oncological sufferers and the dynamic advancement of contemporary anti-cancer remedies. The most recent methods for treating sick tissues using newer technology and materials are discussed in this study. Metal complexes, which are organic molecules, have unquestionably demonstrated anti-cancer action.
However, it is unknown how the rise in temperature and the formation of active forms affect the active substances deposited on the surface of photothermal carriers. The use of photothermal therapy in the treatment of cancer appears to be an appropriate direction to reduce the development of diseases. Nanoparticles possess great potential for future clinical applications in imaging, diagnosis and therapeutics.
5. Conclusions
One of the major issues facing society in the ensuing decades is the fight against cancer. Research on the issue is very important in light of the anticipated rise in the incidence of cancer and the repercussions, including high death rates and major social and economic effects. The main objective of the problem as it is described is to enhance the quality of life of cancer patients by reducing the adverse effects of the medication used. It is important to keep in mind from an economic standpoint that cancer disorders result in both direct expenses (because to their diagnosis and treatment) and indirect costs.
Author Contributions
Alina Stefanache came up with the idea and participated in writing of the manuscript. Ionut Iulian Lungu performed all literature surveys. Denisa Florina Diaconu and Ioana Babarus analyzed the interpretation of literature. All authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- IARC. Monographs Evaluate the Carcinogenicity of Occupational Exposure as a Firefighter; International Agency for Research on Cancer (IARC), the Cancer Agency of the World Health Organization; WHO: Lyon, France, 2022; p. 2. [Google Scholar]
- Gavas, S.; Quazi, S.; Karpiński, T.M. Nanoparticles for cancer therapy: Current progress and challenges. Nanoscale Res. Lett. 2021, 16, 173. [Google Scholar] [CrossRef] [PubMed]
- Persano, F.; Leporatti, S. Current Overview of inorganic nanoparticles for the treatment of central nervous system (CNS) diseases. Curr. Nanomater. 2020, 5, 92–110. [Google Scholar] [CrossRef]
- Mousa, M.; Evans, N.D.; Oreffo, R.O.; Dawson, J.I. Clay nanoparticles for regenerative medicine and biomaterial design: A review of clay bioactivity. Biomaterials 2018, 159, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; Kim, J.; Christophi, C.A.; Kales, S.N. Cancer Incidence and Mortality in Firefighters: A State-of-the-Art Review and Meta-َAnalysis. Asian Pac. J. Cancer Prev. 2019, 20, 3221–3231. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.D.; Li, M.; Yuan, Y.; Mao, N.; Pan, L.Y. Biological comparison of ovarian cancer resistant cell lines to cisplatin and Taxol by two different administrations. Oncol. Rep. 2007, 17, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Takakura, M.; Nakamura, M.; Kyo, S.; Hashimoto, M.; Mori, N.; Ikoma, T.; Mizumoto, Y.; Fujiwara, T.; Urata, Y.; Inoue, M. Intraperitoneal administration of telomerase-specific oncolytic adenovirus sensitizes ovarian cancer cells to cisplatin and affects survival in a xenograft model with peritoneal dissemination. Cancer Gene Ther. 2010, 17, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Nounamo, B.; Liem, J.; Cannon, M.; Liu, J. Myxoma Virus Optimizes Cisplatin for the Treatment of Ovarian Cancer In Vitro and in a Syngeneic Murine Dissemination Model. Mol. Ther. Oncolytics 2017, 6, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Qin, ; Qiu, H; Zhang, M.; Zhang, F.; Yang, H.; Yang, L.; Jia, L.; Qin, K.; Jia, L.; Dou, X.; et al. Soluble CD40 ligands sensitize the epithelial ovarian cancer cells to cisplatin treatment. Biomed. Pharmacother. 2016, 79, 166–175. [CrossRef] [PubMed]
- De Brito, R.V.; Mancini, M.W.; Palumbo, M.d.N.; de Moraes, L.H.O.; Rodrigues, G.J.; Cervantes, O.; Sercarz, J.A.; Paiva, M.B. The Rationale for “Laser-Induced Thermal Therapy (LITT) and Intratumoral Cisplatin” Approach for Cancer Treatment. Int. J. Mol. Sci. 2022, 23, 5934. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.; Aouida, M.; Alhaj Sulaiman, A.; Madhusudan, S.; Ramotar, D. Can Cisplatin Therapy Be Improved? Pathways That Can Be Targeted. Int. J. Mol. Sci. 2022, 23, 7241. [Google Scholar] [CrossRef] [PubMed]
- Kitareewan, S.; Roebuck, B.D.; Demidenko, E.; Sloboda, R.D.; Dmitrovsky, E. Lysosomes and Trivalent Arsenic Treatment in Acute Promyelocytic Leukemia. Gynecol. Oncol. 2007, 99, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Jurcic, J.G.; Soignet, S.L.; Maslak, P. Diagnosis and treatment of acute promyelocytic leukemia. Curr. Oncol. Rep. 2007, 9, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Ramaekers, B.L.T.; Riemsma, R.; Grimm, S.; Fayter, D.; Deshpande, S.; Armstrong, N.; Witlox, W.; Pouwels, X.; Duffy, S.; Worthy, G.; et al. Arsenic Trioxide for Treating Acute Promyelocytic Leukaemia: An Evidence Review Group Perspective of a NICE Single Technology Appraisal. Pharmacoeconomics 2018, 37, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Antman, K.H. Introduction: The History of Arsenic Trioxide in Cancer Therapy. Oncologgist 2001, 6, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Paek, H.J.; Lee, Y.J.; Chung, H.E.; Yoo, N.H.; Lee, J.A.; Kim, M.K.; Lee, J.K.; Jeong, J.; Choi, S.J. Modulation of the pharmacokinetics of zinc oxide nanoparticles and their fates in vivo. Nanoscale 2013, 5, 11416–11427. [Google Scholar] [CrossRef] [PubMed]
- Varadharajaperumal, P.; Muthuswamy, S.; Thiruvengadam, S.; Muthuswamy, S.; Mahalingam, S. Biosynthesised Drug-Loaded Silver Nanoparticles: A Vivid Agent for Drug Delivery On Human Breast Carcinoma. Biosci. Biotechnol. Res. Commun. 2021, 14, 1839–1846. [Google Scholar] [CrossRef]
- Sadhukhan, P.; Kundu, M.; Chatterjee, S.; Ghosh, N.; Manna, P.; Das, J.; Sil, P.C. Targeted delivery of quercetin via pH-responsive zinc oxide nanoparticles for breast cancer therapy. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 100, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Anderson, D.; Dhawan, A. Zinc oxide nanoparticles induce oxidative DNA damage and ROS-triggered mitochondria mediated apoptosis in human liver cells (HepG2). Apoptosis 2012, 17, 852–870. [Google Scholar] [CrossRef] [PubMed]
- Baky, N.A.; Faddah, L.M.; Al-Rasheed, N.M.; Al-Rasheed, N.M.; Fatani, A.J. Induction of inflammation, DNA damage and apoptosis in rat heart after oral exposure to zinc oxide nanoparticles and the cardioprotective role of α-lipoic acid and vitamin E. Drug Res. 2013, 63, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Chuang, H.C.; Juan, H.T.; Chang, C.N.; Yan, Y.H.; Yuan, T.H.; Wang, J.S.; Chen, H.C.; Hwang, Y.H.; Lee, C.H.; Cheng, T.J. Cardiopulmonary toxicity of pulmonary exposure to occupationally relevant zinc oxide nanoparticles. Nanotoxicology 2014, 8, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Sun, K.; Wang, Y.; Dong, S.; Wang, C.; Liu, L.; Wu, Y. Role of Cyt-C/caspases-9,3, Bax/Bcl-2 and the FAS death receptor pathway in apoptosis induced by zinc oxide nanoparticles in human aortic endothelial cells and the protective effect by alpha-lipoic acid. Chem. Biol. Interact. 2016, 258, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Wahab, R.; Siddiqui, M.A.; Saquib, Q.; Dwivedi, S.; Ahmad, J.; Musarrat, J.; Al-Khedhairy, A.A.; Shin, H.S. ZnO nanoparticles induced oxidative stress and apoptosis in HepG2 and MCF-7 cancer cells and their antibacterial activity. Colloids Surf. B 2014, 117, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Bai, D.P.; Zhang, X.F.; Zhang, G.L.; Huang, Y.F.; Gurunathan, S. Zinc oxide nanoparticles induce apoptosis and autophagy in human ovarian cancer cells. Int. J. Nanomed. 2017, 12, 6521–6535. [Google Scholar] [CrossRef] [PubMed]
- Lungu, I.I.; Babarus, I.; Oniciuc, L.; Stefanache, A. A Review of Essential Microelements in the Immune System. International Journal of Immunology 2022, 10(1), 1–4. [Google Scholar]
- Chasteen, T.G.; Bentley, R. Biomethylation of selenium and tellurium: Microorganisms and plants. Chem. Rev. 2003, 103, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Cerwenka, E.A.J.; Cooper, W.C. Toxicology of selenium and tellurium and their compounds. Arch. Environ. Health. 1961, 3, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Garberg, P.; Engman, L.; Tolmachev, V.; Lundqvist, H.; Gerdes, R.G.; Cotgreave, I.A. Binding of tellurium to hepatocellular selenoproteins during incubation with inorganic tellurite: Consequences for the activity of selenium-dependent glutathione peroxidase. Int. J. Biochem. Cell. Biol. 1999, 31, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Kessi, J.; Ramuz, M.; Wehrli, E.; Spycher, M.; Bachofen, R. Reduction of selenite and detoxification of elemental selenium by the phototrophic bacterium Rhodospirillum rubrum. Appl. Environ. Microbiol. 1999, 65, 4734–4740. [Google Scholar] [CrossRef] [PubMed]
- Sors, T.G.; Ellis, D.R.; Salt, D.E. Selenium uptake, translocation, assimilation and metabolic fate in plants. Photosynth. Res. 2005, 86, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Harada, T.; Takahashi, Y. Origin of the difference in the distribution behavior of tellurium and selenium in a soil-water system. Geochim. Cosmochim. Ac. 2009, 72, 1281–1294. [Google Scholar] [CrossRef]
- Fernández-Llamosas, H.; Castro, L.; Blázquez, M.L.; Díaz, E.; Carmona, M. Speeding up bioproduction of selenium nanoparticles by using Vibrio natriegens as microbial factory. Sci. Rep. 2017, 7, 16046. [Google Scholar] [CrossRef]
- Geering, H.R.; Cary, E.E.; Jones, L.H.P.; Allaway, W.H. Solubility and redox criteria for the possible forms of selenium in soils. Soil Sci. Soc. Am. Proc. 1968, 32, 35–47. [Google Scholar] [CrossRef]
- Kieliszek, M.; Błazejak, S.; Gientka, I.; Bzducha-Wróbel, A. Accumulation and metabolism of selenium by yeast cells. Appl. Microbiol. Biotechnol. 2015, 99, 5373–5382. [Google Scholar] [CrossRef]
- Jiménez-Lamana, J.; Abadálvaro, I.; Bierla, K.; Laborda, F.; Szpunar, J.; Lobinski, R. Detection and characterization of biogenic selenium nanoparticles in selenium-rich yeast by single particle ICPMS. J. Anal. At. Spectrom. 2018, 33, 452–460. [Google Scholar] [CrossRef]
- Grones, J.; Macor, M.; Siekel, P.; Bilska, V. Capability of Escherichia coli and Lactobacillus spp. to accumulate selenium in a biologically utilisable form. Bull. Food Res. 1999, 38, 45–53. [Google Scholar]
- Macor, M.; Grones, J. Genetic basis of selenium incorporation into proteins in bacterial cells. Bull. Food Res. 2001, 40, 101–118. [Google Scholar]
- Bergamo, A.; Gaiddon, C.; Schellens, J.H.M.; Beijnen, J.H.; Sava, G. Approaching tumour therapy beyond platinum drugs: Status of the art and perspectives of ruthenium drug candidates. J. Inorg. Biochem. 2012, 106, 90–99. [Google Scholar] [CrossRef]
- Moreira, T.; Francisco, R.; Comsa, E.; Duban-Deweer, S.; Labas, V.; Teixeira-Gomes, A.-P.; Combes-Soia, L.; Marques, F.; Matos, A.; Favrelle-Huret, A.; et al. Polymer ‘ruthenium-cyclopentadienyl’ conjugates—New emerging anti-cancer drugs. Eur. J. Med. Chem. 2019, 168, 373–384. [Google Scholar] [CrossRef]
- Dougan, S.J.; Sadler, P.J. The design of organometallic ruthenium arene anticancer agents. Chimia 2007, 61, 704–715. [Google Scholar] [CrossRef]
- Murray, B.S.; Babak, M.V.; Hartinger, C.G.; Dyson, P.J. The development of RAPTA compounds for the treatment of tumors. Coord. Chem. Rev. 2016, 306, 86–114. [Google Scholar] [CrossRef]
- Motswainyana, W.M.; Ajibade, P.A. Anticancer Activities of Mononuclear Ruthenium(II) Coordination Complexes. Adv. Chem. 2015, 2015, 859730. [Google Scholar] [CrossRef]
- Valente, A.; Garcia, M.H.; Marques, F.; Miao, Y.; Rousseau, C.; Zinck, P. First polymer ‘ruthenium-cyclopentadienyl’ complex as potential anticancer agent. J. Inorg. Biochem. 2013, 127, 79–81. [Google Scholar] [CrossRef]
- Côrte-Real, L.; Karas, B.; Gírio, P.; Moreno, A.; Avecilla, F.; Marques, F.; Buckley, B.T.; Cooper, K.R.; Doherty, C.; Falson, P.; et al. Unprecedented inhibition of P-gp activity by a novel ruthenium-cyclopentadienyl compound bearing a bipyridine-biotin ligand. Eur. J. Med. Chem. 2019, 163, 853–863. [Google Scholar] [CrossRef]
- Pierroz, V.; Joshi, T.; Leonidova, A.; Mari, C.; Schur, J.; Ott, I.; Spiccia, L.; Ferrari, S.; Gasser, G. Molecular and Cellular Characterization of the Biological Effects of Ruthenium(II) Complexes Incorporating 2-Pyridyl-2-pyrimidine-4-carboxylic Acid. J. Am. Chem. Soc. 2012, 134, 20376–20387. [Google Scholar] [CrossRef]
- Tsvetkov, P.; Coy, S.; Petrova, B.; Dreishpoon, M.; Verma, A.; Abdusamad, M.; Rossen, J.; Joesch-Cohen, L.; Humeidi, R.; Spangler, R.D.; et al. Copper induces cell death by targeting lipoylated TCA cycle proteins. Science 2022, 375, 1254–1261. [Google Scholar] [CrossRef]
- Koizumi, M.; Fujii, J.; Suzuki, K.; Inoue, T.; Inoue, T.; Gutteridge, J.M.; Taniguchi, N. A marked increase in free copper levels in the plasma and liver of LEC rats: An animal model for Wilson disease and liver cancer. Free Radic. Res. 1998, 28, 441–450. [Google Scholar] [CrossRef]
- Siddiqui, M.A.; Alhadlaq, H.A.; Ahmad, J.; Al-Khedhairy, A.A.; Musarrat, J.; Ahamed, M. Copper oxide nanoparticles induced mitochondria mediated apoptosis in human hepatocarcinoma cells. PLoS ONE 2013, 8, e69534. [Google Scholar] [CrossRef]
- Polishchuk, E.V.; Merolla, A.; Lichtmannegger, J.; Romano, A.; Indrieri, A.; Ilyechova, E.Y.; Concilli, M.; De Cegli, R.; Crispino, R.; Mariniello, M.; et al. Activation of autophagy, observed in liver tissues from patients with wilson disease and from ATP7B-deficient animals, protects hepatocytes from copper-induced apoptosis. Gastroenterology 2019, 156, 1173–1189.e5. [Google Scholar] [CrossRef]
- Tadini-Buoninsegni, F.; Smeazzetto, S. Mechanisms of charge transfer in human copper ATPases ATP7A and ATP7B. IUBMB Life 2017, 69, 218–225. [Google Scholar] [CrossRef]
- Pessoa, J.C.; Etcheverry, S.; Gambino, D. Vanadium compounds in medicine. Coord. Chem. Rev. 2015, 301–302, 24–48. [Google Scholar] [CrossRef]
- Crans, D.C. Fifteen years of dancing with vanadium. Pure Appl. Chem. 2005, 77, 1497–1527. [Google Scholar] [CrossRef]
- Niu, X.; Xiao, R.; Wang, N.; Wang, Z.; Zhang, Y.; Xia, Q.; Yang, X. The molecular mechanisms and rational design of anti-diabetic vanadium compounds. Curr. Top. Med. Chem. 2016, 16, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Tamrakar, A.K.; Maurya, C.K.; Rai, A.K. PTP1B inhibitors for type 2 diabetes treatment: A patent review (2011–2014). Expert Opin. Ther. Pat. 2014, 24, 1101–1115. [Google Scholar] [CrossRef]
- Heidari, A.; Schmitt, K.; Henderson, M.; Besana, E. Drug delivery systems (DDSs) of osmium nanoparticles on human gum cancer cells, tissues and tumors treatment under synchrotron radiation. Dent. Oral Maxillofac. Res. 2019, 5, 1–18. [Google Scholar] [CrossRef]
- Kang, S.; Gil, Y.-G.; Yim, G.; Min, D.-H.; Jang, H. Osmium–Tellurium Nanozymes for Pentamodal Combinatorial Cancer Therapy. ACS Appl. Mater. Interfaces 2021, 13, 44124–44135. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.R.K.; Wu, Y.; Ghosh, D.; Do, B.H.; Chen, K.; Dawson, M.R.; Fang, N.; Sulchek, T.A.; El-Sayed, M.A. Nuclear Membrane-Targeted Gold Nanoparticles Inhibit Cancer Cell Migration and Invasion. ACS Nano 2017, 11, 3716. [Google Scholar] [CrossRef]
- Cheheltani, R.; Ezzibdeh, R.M.; Chhour, P.; Pulaparthi, K.; Kim, J.; Jurcova, M.; Hsu, J.C.; Blundell, C.; Litt, H.I.; Ferrari, V.A.; et al. Tunable, biodegradable gold nanoparticles as contrast agents for computed tomography and photoacoustic imaging. Biomaterials 2016, 102, 87–97. [Google Scholar] [CrossRef]
- Her, S.; Jaffray, D.A.; Allen, C. Gold nanoparticles for applications in cancer radiotherapy: Mechanisms and recent advancements. Adv. Drug Deliv. Rev. 2017, 109, 84–101. [Google Scholar] [CrossRef]
- Singh, P.; Pandit, S.; Mokkapati, V.; Garg, A.; Ravikumar, V.; Mijakovic, I. Gold Nanoparticles in Diagnostics and Therapeutics for Human Cancer. Int. J. Mol. Sci. 2018, 19, 1979. [Google Scholar] [CrossRef]
- Luo, D.; Wang, X.; Zeng, S.; Ramamurthy, G.; Burda, C.; Basilion, J.P. Prostate-specific membrane antigen targeted gold nanoparticles for prostate cancer radiotherapy: Does size matter for targeted particles? Chem. Sci. 2019, 10, 8119–8128. [Google Scholar] [CrossRef]
- Tomić, S.; Đokić, J.; Vasilijić, S.; Ogrinc, N.; Rudolf, R.; Pelicon, P.; Vučević, D.; Milosavljević, P.; Janković, S.; Anžel, I.; et al. Size-Dependent Effects of Gold Nanoparticles Uptake on Maturation and Antitumor Functions of Human Dendritic Cells In Vitro. PLoS ONE 2014, 9, e96584. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Uses of platinum compounds and corresponding doses.
| Compound | Usage in Cancer | Typical Dose |
|---|---|---|
| Cisplatin | Testicular, ovarian, bladder, lung, head and neck cancers | 20-100 mg/m² every 3-4 weeks |
| Carboplatin | Ovarian, lung, and other types of cancers | 4-6 mg/mL/min every 3-4 weeks |
| Oxaliplatin | Colorectal cancer | 85-130 mg/m² every 2-3 weeks |
| Nedaplatin | Lung, ovarian, and head and neck cancers | 80-120 mg/m² every 3-4 weeks |
| Satraplatin | Prostate, ovarian, and other types of cancers | 80-120 mg/m² every 5-6 weeks |
| Lobaplatin | Lung, ovarian, and other types of cancers | 25-50 mg/m² every 3-4 weeks |
| Heptaplatin | Lung, gastric, and other types of cancers | 100-300 mg/m² every 3-4 weeks |
| Spiroplatin | Ovarian, cervical, and other types of gynecological cancers | 70-100 mg/m² every 3-4 weeks |
| Proplatine | Ovarian, bladder, and other types of cancers | 60-120 mg/m² every 3-4 weeks |
Table 2.
Zinc compounds used in cancer treatment and their typical doses.
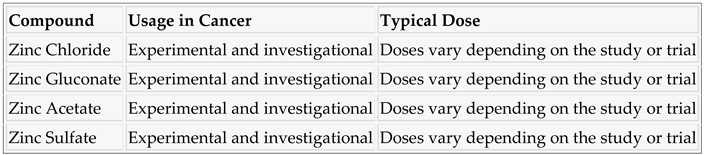
Table 3.
Selenium compounds used in cancer treatment and their typical doses.
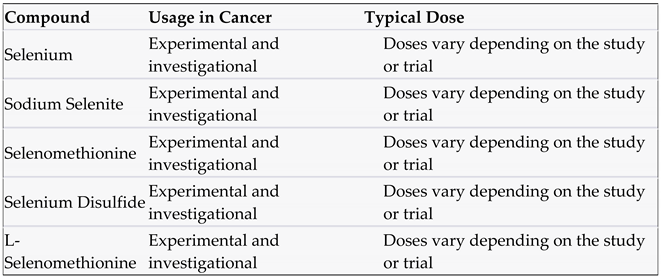
Table 4.
Ruthenium compounds used in cancer treatment and their typical doses.
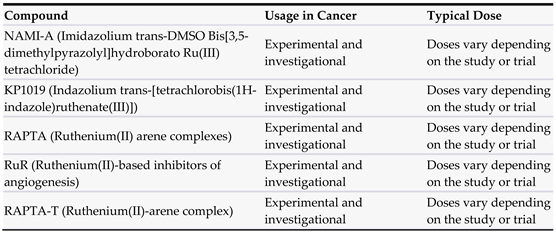
Table 5.
Copper compounds used in cancer treatment and their typical doses.
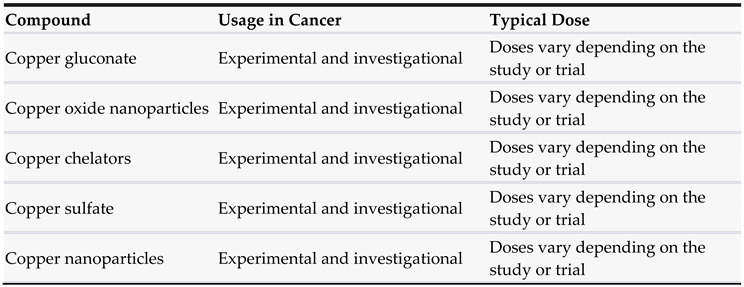
Table 6.
Vanadium compounds used in cancer treatment and their typical doses.
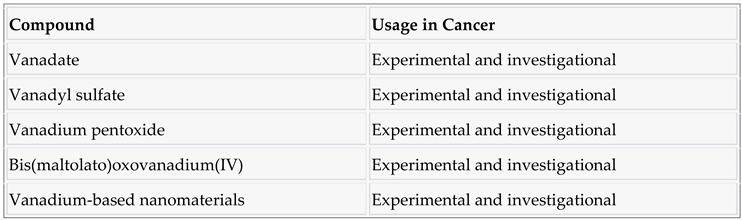
Table 7.
Osmium compounds used in cancer treatment and their typical doses.

Table 10.
Gold compound in cancer therapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



