
Submitted:
19 June 2023
Posted:
20 June 2023
You are already at the latest version
Abstract
(1) Infective endocarditis is a severe inflammatory disease associated with substantial mortality and morbidity. Alkaline phosphatase (AP) levels have been shown to change significantly during sepsis additionally we previously found higher initial AP drop after cardiac surgery is associat-ed with unfavorable outcomes. Therefore, the course of AP after surgery for endocarditis is of special interest. (2) 314 patients with active isolated left-sided infective endocarditis at the De-partment of Cardiac Surgery (Medical University of Vienna, Austria) between 2009 and 2018 were enrolled in this retrospective analysis. Blood samples were analyzed at different time points (baseline, postoperative day 1-7, postoperative days 14, and 30). Patients were categorized ac-cording to relative alkaline phosphatase drop (≥30% vs. <30%). (3) The rate of postoperative renal replacement therapy with or without prior renal replacement therapy (7.4 vs. 21.8%; p=0.001 and 6.7 vs. 15.6%; p=0.015, respectively) and extracorporeal membrane oxygenation (2.2 vs. 19.0%; p=0.000) was observed after a higher initial alkaline phosphatase drop. Short-term (30-day mor-tality 3.0 vs. 10.6%; p=0.010) and long-term mortality (p=0.008) were significantly impaired after a higher initial alkaline phosphatase drop. (4) The higher initial alkaline phosphatase drop was accompanied by impaired short and long-term outcomes after cardiac surgery for endocarditis. Future risk assessment scores for cardiac surgery should consider alkaline phosphatase.
Keywords:
alkaline phosphatase
; cardiac surgery
; cardio-pulmonary bypass
; endocarditis
; kidney
1. Introduction
Infective endocarditis (IE) is a rare but severe manifestation of valvular disease associated with significant morbidity and mortality. [1] The Duke criteria are used for diagnostic purposes. [2] Besides extended antimicrobial therapy, surgery should be performed in case of heart failure, uncontrolled infection and in order to prevent embolism. If indicated, surgery should be performed as early as possible. [3,4]
Transient bacteremia, as it may occur after dental, gynecologic, gastrointestinal, or urologic procedures or even after daily activities such as brushing teeth, may lead to bacterial colonization of heart valves resulting in sepsis, causing a spectrum of end-organ damage. [5] With up to two-thirds developing acute kidney injury (AKI) in the setting of IE, end-organ damage of the kidney is one of the most common. [6] Renal inflammation and resulting hypoxia are considered to be the causative. [7] The binding of pathogen-associated molecular patterns (PAMPs) such as lipopolysaccharide (LPS) to toll-like receptor 4 leads to the further release of inflammatory mediators. [8] The pervasive alkaline phosphatase (AP) neutralizes LPS and converts proinflammatory molecules to anti-inflammatory ones (such as adenosine). [7,9,10] (Severely) elevated AP levels have been considered a surrogate parameter for infection or bacteremia. [11,12,13] Consequently, AP has been considered a treatment target for sepsis patients in improving AKI or survival (in animal models). [7,14,15]
Additionally, to the inflammatory process caused by endocarditis, cardiac surgery induces some systemic inflammation due to the heart-lung machine (HLM). In up to 30%, a systemic inflammatory response syndrome (SIRS) occurs, associated with an elevated risk of end-organ injury. [16,17,18] No sole mechanism is responsible, but various factors are considered contributing [7,19,20,21,22] Increased consumption of AP during cardiac surgery or extracorporeal membrane oxygenation is associated with a higher morbidity and mortality rate. [23,24,25,26]
This study aims to evaluate the AP metabolism in the setting of an inflammatory state in IE patients undergoing surgery. To our knowledge, no study evaluating the course of AP following cardiac surgery for IE has been published previously.
2. Results
Patient Population and Cut-off Values
After reviewing the exclusion criteria 314 patients were included in the retrospective analysis. According to an initial drop in AP of ≥ 30% (with an area under curve (AUC) 0.638; sensitivity 71%, specificity 53% for 1-year mortality) two groups were created– with 179 patients with an AP drop ≥ 30% and 135 patients with an AP drop < 30%. The selection of cut-off values was guided by previous research findings. [25,26] In the following sections, the first value always refers to the lower initial AP drop cohort.
Preoperative Characteristics
The higher initial AP drop cohort was at significantly higher surgical risk (EuroScore II 9.1 (15.9;3.5) vs. 16.1 (34.3;6.4) %; p=0.000), had a significantly higher rate of preoperative dialysis (5.9 vs. 13.4%; p=0.030) and prosthetic valve endocarditis (PVE) (20.0 vs. 40.2%; p=0.000). All other patient characteristics were similar among the cohorts (Table 1).
Procedural Data
A significantly higher rate of re-sternotomy (21.5 vs. 40.8%; p=0.000) and double valve replacement (8.9 vs. 22.9%; p=0.001) were observed after an initial higher AP drop. Surgical times were prolonged in the initial higher AP cohort: total surgery time (240 (300;195) vs. 348 (455;255) min; p=0.000), total cardiopulmonary bypass time (110 (155;90) vs. 162 (237;117) min; p=0.000) and total aortic cross clamp time (81 (113;62) vs. 111 (159;79) min; p=0.000). Procedural data is illustrated in Table 2.
Laboratory data
While AP values at baseline were significantly higher in the higher initial AP drop cohort (74 (96;62) vs. 93 (120;76) U/L; p=0.000), there was no significant difference at 30 days (116 (141;89) vs. 128 (172;99) U/L; p=0.089). Patients with the higher initial AP drop required a longer time to reach baseline values (days till baseline value surpassed: 4 (6;3) vs. 6 (7;4) days; p=0.000; baseline within 3 days: 43.7 vs. 33.0%; p=0.052; baseline within 5 days: 74.1 vs 60.3 %; p=0.011). The postoperative course of AP dependent on the initial AP drop is depicted in Figure 1. On postoperative day (POD) 30 AP levels were significantly higher compared to baseline in both cohorts (p=0.000 for both). Figure 2 illustrates the differences of AP levels at baseline to POD 1 and POD 30.
Although there was no statistic significant difference at baseline CRP values (3.9 (8.3;1.7) vs. 4.5 (11.7;1.5) mg/dL; p=0.456), a significantly higher value after 30 days in the higher initial AP drop cohort was observed (2.1 (5.7;0.7) vs. 4.6 (10.6;1.8) mg/dL; p=0.001). Laboratory values are provided in Table 3.
Adverse Events and mortality
An overview of adverse events and mortality is available in Table 4. A higher rate of revision due to bleeding (7.4 vs. 15.6%; p=0.027), postoperative renal replacement therapy with or without previous one (7.4 vs 21.8 %; p=0.001 and 6.7 vs. 15.6%; p=0.015), extracorporeal membrane oxygenation (2.2 vs. 19.0%; p=0.000) was seen after higher initial AP drop. While there was a strong trend towards prolonged hospitalization (p=0.054), a prolonged ICU stay was significantly more likely in the higher initial AP drop cohort (31.9 vs. 48.0%; p=0.004).
Short-term mortality (30day: 3.0 vs. 10.6; p=0.010; in-hospital: 5.9 vs. 17.3%; p=0.002; 1-year: 14.1 vs. 25.7%; p=0.012) and long-term mortality (p=0.008, see Figure 3) were significantly higher in the higher initial AP drop cohort.
ECMO – extracorporeal membrane oxygenation; prolonged hospital stay longer than 30days; prolonged ICU (intensive care unit) stay defined as more than 7 days; prolonged intubation defined as reintubated, longer as 48h, tracheostoma;
3. Discussion
In line with previous studies by Schaefer et al. (mitral valve patients with impaired left ventricular function) and Poschner et al. (postcardiotomy VA-ECMO patients), we were able to demonstrate a relation between higher initial AP drop and morbidity and mortality in patients undergoing cardiac surgery for left-sided IE. [25,26] Not only short-term (i.e., hospital mortality) but also long-term survival (over ten years) was significantly impaired following a higher initial AP drop (p=0.008).
Prosthetic valve endocarditis occurs in up to 20% of all endocarditis cases and is associated with a worse prognosis. [27,28] This finding could also be highlighted in our study cohort. Indeed, PVE was approximately twice as common in the higher initial AP drop cohort (40.2% vs. 20.0%; p=0.000). Even though preoperative AP levels were within the normal range in both cohorts, AP levels were significantly higher in the higher initial AP drop cohort (see Table 3). Interestingly, baseline AP values, as well as baseline CRP values, showed no significant difference in PVE versus native IE (baseline AP in PVE 87 (109; 71) vs. native 84 (113; 68) U/L; p=0.465; CRP in PVE 4.3 (12.6; 1.3) vs. native 4.2 (8.7; 1.8); p=0.617). Hence, we may conclude that PVE seems to be not related to a more pertinent systemic inflammation and that the significant impaired outcome was instead primarily due to the longer surgical times (total surgical time: PVE 389 (485;320) vs. native 245 (319;205) min; total cardiopulmonary bypass time PVE 192 (266;147) vs. native 118 (172;94) min and total aortic cross-clamp time PVE 121 (173;95) vs. native 82 (120;62) min all with a p=0.000). As demonstrated by Doenst T et al., Nissinen J et al., and others, longer operation times are an independent predictor of worse outcomes. [29,30]. Increased permeability in the gastrointestinal tract induced by HLM leads to a wash-in of endotoxins into the bloodstream, inducing the release of proinflammatory mediators. [20,22] AP-mediated dephosphorylation may convert a portion into anti-inflammatory substances. [31] This process leads to the consumption of systemic alkaline phosphatase. [23,32] Thus, prolonged duration of surgery is also likely to lead to an increased decrease in AP due to prolonged exposure to endotoxins and associated mediators.
Iso-forms of AP are present in the proximal tubule cells of the kidney. Without a complete understanding of the role of AP in the kidney, animal studies have demonstrated increased levels of AP in the urine after ischemia-reperfusion injury and administration of LPS, thus, suggesting injury to the proximal tubule brush border in these situations. [33,34] In the receiver operating characteristics (ROC) analysis in our cohort, the drop in alkaline phosphatase was associated with the need for postoperative dialysis with an AUC of 0.668. After an initial more significant drop, the need for postoperative dialysis was significantly more frequent (p=0.001). Interestingly, the rate of postoperative dialysis was significantly higher with and without preoperative dialysis in the cohort with a higher initial AP drop. This suggests that patients with and without injured renal parenchyma are significantly more likely to have AKI due to SIRS (represented by the higher AP drop). Patients with AKI have significantly worse outcomes after cardiac surgery. [35]
Zhang et al. highlighted the alkaline phosphatase on the surface membrane of neutrophils as a good tool for differentiating between SIRS patients with or without bacteremia. [36] Similarly, Kerner A. et al. and Tung C.B. et al. showed (severely) elevated AP levels as a surrogate parameter for bacteremia. [11,12] However, these findings could not be confirmed in this study. In 82.5% of the total cohort, positive blood cultures were present, which were associated with a significantly elevated CRP level (CRP positive BC 4.9 (11.9; 1.9) vs. negative BC 2.7 (5.7;0.8) mg/dL; p=0.001); however, without any differences in AP (AP positive BC 86 (114;70) vs. negative BC 79 (106;64) U/L; p=0.116).
An impaired barrier function of the gastrointestinal tract (GIT) leads to a wash-in of LPS. Hamarneh et al. demonstrated an impaired barrier function of the GIT in patients deprived of enteral feeding due to a loss of AP expression reversible to AP supplementation. [37] Given the critical state of IE patients, they often lack adequate enteral feeding. Hence, considering additionally the inflammatory state of endocarditis patients with the high rate of need for postoperative dialysis (and the likely even higher rate of any AKI) and the further AP consumption during cardiac surgery, supplementation of AP may be especially promising in IE patients. [8] Currently, clinical trials (e.g., APPIRED III – ClinicalTrial.gov NCT03050476) are evaluating the external administration of AP during (elective) cardiac surgery and are expected to reduce morbidity after cardiac surgery.
Our study found a significantly higher rate of ECMO implantation after a higher initial AP drop (2.2% vs. 19.0%; p=0.000), presumably due to the longer operation times and the higher preoperative risk found in this cohort. In-hospital mortality after postcardiotomy ECMO support is reported in up to two-thirds of patients. [38,39] The significantly worse outcome after a higher initial AP drop may thus be attributed to or at least influenced by the higher rate of ECMO implantation (30-day mortality 3.0% vs. 10.6%; p=0.010; in-hospital mortality 5.9% vs. 17.3%; p=0.002; 1-year mortality 14.1% vs. 25.7%; p=0.012). However, as already shown in previous work, ECMO support did not increase AP consumption, evident in reaching baseline values within five days in both studies. [25]
4. Materials and Methods
Patients
All patients who required valve surgery for isolated left-sided IE between January 2009 and October 2022 at the Department of Cardiac Surgery (Vienna General Hospital, Austria) were included into this retrospective data analysis. The ethics committee of the Medical University of Vienna approved this retrospective study (2101/2022). Modified Duke criteria were used for IE diagnosis. [40] Exclusion criteria included IE involvement of the right side, surgical valve repair, homograft implantation and missing laboratory values at baseline or on POD 1. After reviewing the exclusion criteria 314 patients were analyzed.
Laboratory Data
Blood samples were drawn at baseline and on each of the first seven POD as well as on POD 14 (±3) and 30 (±5). Baseline was defined as a preoperative blood draw within a maximum of 7 days prior surgery. The normal range of alkaline phosphatase is between 40 and 130 U/L and is determined as a routine parameter at our department. To determine the plasma concentrations of alkaline phosphatase, enzyme kinetic measurements are performed on native or heparinized blood samples.
Follow-Up
To evaluate the individual postoperative outcome and adverse events, the local patient documentation system AKIM was used. Additionally, federal statistics (Statistics Austria, Vienna, Austria) was used to determine the survival rates.
Statistical Analysis
Categorical variables are presented by numbers and percentages. For continuous variables, the mean ± standard deviation (SD) is reported if the data follows a normal distribution; otherwise, the median and interquartile range (IQR) are provided. The normal distribution assumption is tested using the Kolmogorov-Smirnov test. The patients were grouped according to the initial AP drop.
AP drop = 1 – AP POD 1 / AP Baseline
Cut-offs were determined using a ROC analysis for 1-year mortality. Furthermore, the first day when alkaline phosphatase returned or exceeded baseline level was determined.
The Mann-Whitney-U-Test was used to assess differences between the continuous variables with non-normal distributions. For the comparison of categorical variables, the chi-square test was applied. Differences between AP at Baseline and AP POD 1 and AP POD 30, respectively, were determined using the Wilcoxon signed-rank test. The findings are visually presented using boxplots. Survival was visualized with Kaplan Meier Curves and the differences between the groups were tested using the log rank test. All analyses were performed using SPSS version 27.0 (IBM Corp, Armonk, NY, USA). A two-sided p-value of less than 0.05 was considered to indicate statistical significance.
5. Conclusions
A significant higher morbidity and an impaired outcome after a higher initial drop of alkaline phosphatase at 30-days, 1-year and in the long-term survival was evident. Future risk assessment scores for cardiac surgery should consider alkaline phosphatase.
Author Contributions
Conceptualization, A.K., T.P., P.A., M.A., D.H., R.B., G.L., D.W.; methodology, A.K., T.P., D.W.; formal analysis, A.K., T.P., D.W.; data curation; A.K., T.P., A.S., L.A.; writing—original draft preparation.; A.K., T.P., D.W.; writing—review and editing, A.K., T.P., A.S., P.A., L.A., M.A., D.H., R.B., G.L., D.W.; visualization, A.K., T.P.; supervision, M.A., G.L., D.W.; project administration, T.P., D.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the local Ethics Committee (2101/2022).
Informed Consent Statement
Patient consent was waived given the retrospective nature of this study.
Conflicts of Interest
A.K. – non to declare; T.P. – Investigator of the APPIRED III study; A.S. – non to declare; P.A. – non toe declare; L.A. – non to declare; M.A. – Investigator of the APPIRED III study; D.H. – Investigator of the APPIRED III study; R.B. – CEO of Alloksys Life Sciences BV (Wageningen, Netherlands); G.L. – Investigator of the APPIRED III study; D.W. – Investigator of the APPIRED III study
References
- Pettersson, G.B.; Coselli, J.S.; Writing, C.; Pettersson, G.B.; Coselli, J.S.; Hussain, S.T.; Griffin, B.; Blackstone, E.H.; Gordon, S.M.; LeMaire, S.A.; et al. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J Thorac Cardiovasc Surg 2017, 153, 1241–1258.e1229. [Google Scholar] [CrossRef] [PubMed]
- Pierce, D.; Calkins, B.C.; Thornton, K. Infectious endocarditis: diagnosis and treatment. Am Fam Physician 2012, 85, 981–986. [Google Scholar] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Iung, B. 2015 ESC Guidelines on the management of infective endocarditis: a big step forward for an old disease. Heart 2016, 102, 992–994. [Google Scholar] [CrossRef]
- Holland, T.L.; Baddour, L.M.; Bayer, A.S.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr. Infective endocarditis. Nat Rev Dis Primers 2016, 2, 16059. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Pouvaret, A.; Maillard, N.; Berthelot, P.; Lutz, M.F.; Cazorla, C.; Tulane, C.; Fuzellier, J.F.; Verhoeven, P.O.; Fresard, A.; et al. Acute kidney injury in infective endocarditis: A retrospective analysis. Med Mal Infect 2019, 49, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.; Heemskerk, S.; Masereeuw, R.; Pickkers, P. Alkaline phosphatase: a possible treatment for sepsis-associated acute kidney injury in critically ill patients. Am J Kidney Dis 2014, 63, 1038–1048. [Google Scholar] [CrossRef]
- Hummeke-Oppers, F.; Hemelaar, P.; Pickkers, P. Innovative Drugs to Target Renal Inflammation in Sepsis: Alkaline Phosphatase. Front Pharmacol 2019, 10, 919. [Google Scholar] [CrossRef]
- Koyama, I.; Matsunaga, T.; Harada, T.; Hokari, S.; Komoda, T. Alkaline phosphatases reduce toxicity of lipopolysaccharides in vivo and in vitro through dephosphorylation. Clin Biochem 2002, 35, 455–461. [Google Scholar] [CrossRef]
- Poelstra, K.; Bakker, W.W.; Klok, P.A.; Kamps, J.A.; Hardonk, M.J.; Meijer, D.K. Dephosphorylation of endotoxin by alkaline phosphatase in vivo. Am J Pathol 1997, 151, 1163–1169. [Google Scholar]
- Kerner, A.; Avizohar, O.; Sella, R.; Bartha, P.; Zinder, O.; Markiewicz, W.; Levy, Y.; Brook, G.J.; Aronson, D. Association between elevated liver enzymes and C-reactive protein: possible hepatic contribution to systemic inflammation in the metabolic syndrome. Arterioscler Thromb Vasc Biol 2005, 25, 193–197. [Google Scholar] [CrossRef]
- Tung, C.B.; Tung, C.F.; Yang, D.Y.; Hu, W.H.; Hung, D.Z.; Peng, Y.C.; Chang, C.S. Extremely high levels of alkaline phosphatase in adult patients as a manifestation of bacteremia. Hepatogastroenterology 2005, 52, 1347–1350. [Google Scholar]
- Katasako, A.; Sasaki, S.; Raita, Y.; Yamamoto, S.; Tochitani, K.; Murakami, M.; Nishioka, R.; Fujisaki, K. Association between serum alkaline phosphatase and bacteraemia in haemodialysis outpatients: a multicentre retrospective cross-sectional study. BMJ Open 2022, 12, e058666. [Google Scholar] [CrossRef] [PubMed]
- Fawley, J.; Gourlay, D.M. Intestinal alkaline phosphatase: a summary of its role in clinical disease. J Surg Res 2016, 202, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Pickkers, P.; Heemskerk, S.; Schouten, J.; Laterre, P.F.; Vincent, J.L.; Beishuizen, A.; Jorens, P.G.; Spapen, H.; Bulitta, M.; Peters, W.H.; et al. Alkaline phosphatase for treatment of sepsis-induced acute kidney injury: a prospective randomized double-blind placebo-controlled trial. Crit Care 2012, 16, R14. [Google Scholar] [CrossRef] [PubMed]
- Al-Fares, A.; Pettenuzzo, T.; Del Sorbo, L. Extracorporeal life support and systemic inflammation. Intensive Care Med Exp 2019, 7, 46. [Google Scholar] [CrossRef] [PubMed]
- Giacinto, O.; Satriano, U.; Nenna, A.; Spadaccio, C.; Lusini, M.; Mastroianni, C.; Nappi, F.; Chello, M. Inflammatory Response and Endothelial Dysfunction Following Cardiopulmonary Bypass: Pathophysiology and Pharmacological Targets. Recent Patents on Inflammation & Allergy Drug Discovery 2019, 13, 158–173. [Google Scholar] [CrossRef]
- Squiccimarro, E.; Labriola, C.; Malvindi, P.G.; Margari, V.; Guida, P.; Visicchio, G.; Kounakis, G.; Favale, A.; Dambruoso, P.; Mastrototaro, G.; et al. Prevalence and Clinical Impact of Systemic Inflammatory Reaction After Cardiac Surgery. Journal of Cardiothoracic and Vascular Anesthesia 2019, 33, 1682–1690. [Google Scholar] [CrossRef]
- Montesinos, M.C.; Takedachi, M.; Thompson, L.F.; Wilder, T.F.; Fernandez, P.; Cronstein, B.N. The antiinflammatory mechanism of methotrexate depends on extracellular conversion of adenine nucleotides to adenosine by ecto-5'-nucleotidase: findings in a study of ecto-5'-nucleotidase gene-deficient mice. Arthritis Rheum 2007, 56, 1440–1445. [Google Scholar] [CrossRef]
- Neuhof, C.; Wendling, J.; Dapper, F.; Bauer, J.; Zickmann, B.; Jochum, M.; Tillmanns, H.; Neuhoft, H. Endotoxemia and cytokine generation in cardiac surgery in relation to flow mode and duration of cardiopulmonary bypass. Shock 2001, 16 (Suppl. 1), 39–43. [Google Scholar] [CrossRef]
- Paparella, D.; Yau, T.M.; Young, E. Cardiopulmonary bypass induced inflammation: pathophysiology and treatment. An update. European Journal of Cardio-Thoracic Surgery: Official Journal of the European Association for Cardio-Thoracic Surgery 2002, 21, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Riddington, D.W.; Venkatesh, B.; Boivin, C.M.; Bonser, R.S.; Elliott, T.S.; Marshall, T.; Mountford, P.J.; Bion, J.F. Intestinal permeability, gastric intramucosal pH, and systemic endotoxemia in patients undergoing cardiopulmonary bypass. JAMA 1996, 275, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.; Tong, S.; Hauck, A.; Lawson, D.S.; Jaggers, J.; Kaufman, J.; da Cruz, E. Alkaline phosphatase activity after cardiothoracic surgery in infants and correlation with post-operative support and inflammation: a prospective cohort study. Crit Care 2012, 16, R160. [Google Scholar] [CrossRef]
- Davidson, J.A.; Urban, T.T.; Tong, S.; Maddux, A.; Hill, G.; Frank, B.S.; Watson, J.D.; Jaggers, J.; Simoes, E.A.F.; Wischmeyer, P. Alkaline Phosphatase Activity and Endotoxemia After Infant Cardiothoracic Surgery. Shock 2019, 51, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Poschner, T.; Schaefer, A.K.; Hutschala, D.; Goliasch, G.; Riebandt, J.; Distelmaier, K.; Bernardi, M.H.; Andreas, M.; Brands, R.; Aref, T.; et al. Impact of Venoarterial Extracorporeal Membrane Oxygenation on Alkaline Phosphatase Metabolism after Cardiac Surgery. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- Schaefer, A.K.; Hutschala, D.; Andreas, M.; Bernardi, M.H.; Brands, R.; Shabanian, S.; Laufer, G.; Wiedemann, D. Decrease in serum alkaline phosphatase and prognostic relevance in adult cardiopulmonary bypass. Interact Cardiovasc Thorac Surg 2020, 31, 383–390. [Google Scholar] [CrossRef]
- Vongpatanasin, W.; Hillis, L.D.; Lange, R.A. Prosthetic heart valves. N Engl J Med 1996, 335, 407–416. [Google Scholar] [CrossRef]
- Wang, A.; Athan, E.; Pappas, P.A.; Fowler, V.G., Jr.; Olaison, L.; Pare, C.; Almirante, B.; Munoz, P.; Rizzi, M.; Naber, C.; et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA 2007, 297, 1354–1361. [Google Scholar] [CrossRef]
- Doenst, T.; Borger, M.A.; Weisel, R.D.; Yau, T.M.; Maganti, M.; Rao, V. Relation between aortic cross-clamp time and mortality--not as straightforward as expected. Eur J Cardiothorac Surg 2008, 33, 660–665. [Google Scholar] [CrossRef]
- Nissinen, J.; Biancari, F.; Wistbacka, J.O.; Peltola, T.; Loponen, P.; Tarkiainen, P.; Virkkila, M.; Tarkka, M. Safe time limits of aortic cross-clamping and cardiopulmonary bypass in adult cardiac surgery. Perfusion 2009, 24, 297–305. [Google Scholar] [CrossRef]
- Coleman, J.E. Structure and mechanism of alkaline phosphatase. Annu Rev Biophys Biomol Struct 1992, 21, 441–483. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.A.; Urban, T.T.; Baird, C.; Tong, S.; Woodruff, A.; Twite, M.; Jaggers, J.; Simoes, E.A.F.; Wischmeyer, P. Alkaline Phosphatase in Infant Cardiopulmonary Bypass: Kinetics and Relationship to Organ Injury and Major Cardiovascular Events. J Pediatr 2017, 190, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Coux, G.; Trumper, L.; Elias, M.M. Renal function and cortical (Na(+)+K(+))-ATPase activity, abundance and distribution after ischaemia-reperfusion in rats. Biochim Biophys Acta 2002, 1586, 71–80. [Google Scholar] [CrossRef]
- Khundmiri, S.J.; Asghar, M.; Khan, F.; Salim, S.; Yusufi, A.N. Effect of reversible and irreversible ischemia on marker enzymes of BBM from renal cortical PT subpopulations. Am J Physiol 1997, 273, F849–F856. [Google Scholar] [CrossRef]
- Corredor, C.; Thomson, R.; Al-Subaie, N. Long-Term Consequences of Acute Kidney Injury After Cardiac Surgery: A Systematic Review and Meta-Analysis. J Cardiothorac Vasc Anesth 2016, 30, 69–75. [Google Scholar] [CrossRef]
- Zhang, C.Y.; Zhang, H.H.; Zhao, S.L.; Wu, H.Y.; Li, H.N.; Li, W.; Yang, J. Clinical value of alkaline phosphatase on the surface membrane of neutrophils for prediction of bacteremia in patients with systemic inflammatory response syndrome. Diagn Microbiol Infect Dis 2021, 100, 114105. [Google Scholar] [CrossRef] [PubMed]
- Hamarneh, S.R.; Mohamed, M.M.; Economopoulos, K.P.; Morrison, S.A.; Phupitakphol, T.; Tantillo, T.J.; Gul, S.S.; Gharedaghi, M.H.; Tao, Q.; Kaliannan, K.; et al. A novel approach to maintain gut mucosal integrity using an oral enzyme supplement. Ann Surg 2014, 260, 706–714. [Google Scholar] [CrossRef]
- Biancari, F.; Dalen, M.; Fiore, A.; Ruggieri, V.G.; Saeed, D.; Jonsson, K.; Gatti, G.; Zipfel, S.; Perrotti, A.; Bounader, K.; et al. Multicenter study on postcardiotomy venoarterial extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg 2020, 159, 1844–1854. [Google Scholar] [CrossRef]
- Khorsandi, M.; Dougherty, S.; Bouamra, O.; Pai, V.; Curry, P.; Tsui, S.; Clark, S.; Westaby, S.; Al-Attar, N.; Zamvar, V. Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: a systematic review and meta-analysis. J Cardiothorac Surg 2017, 12, 55. [Google Scholar] [CrossRef]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000, 30, 633–638. [Google Scholar] [CrossRef]
Figure 1.
Alkaline phosphatase blood values dependent in the initial AP drop at baseline, on each consecutive day until POD 7 as well as on POD 14 and POD30.
Figure 1.
Alkaline phosphatase blood values dependent in the initial AP drop at baseline, on each consecutive day until POD 7 as well as on POD 14 and POD30.
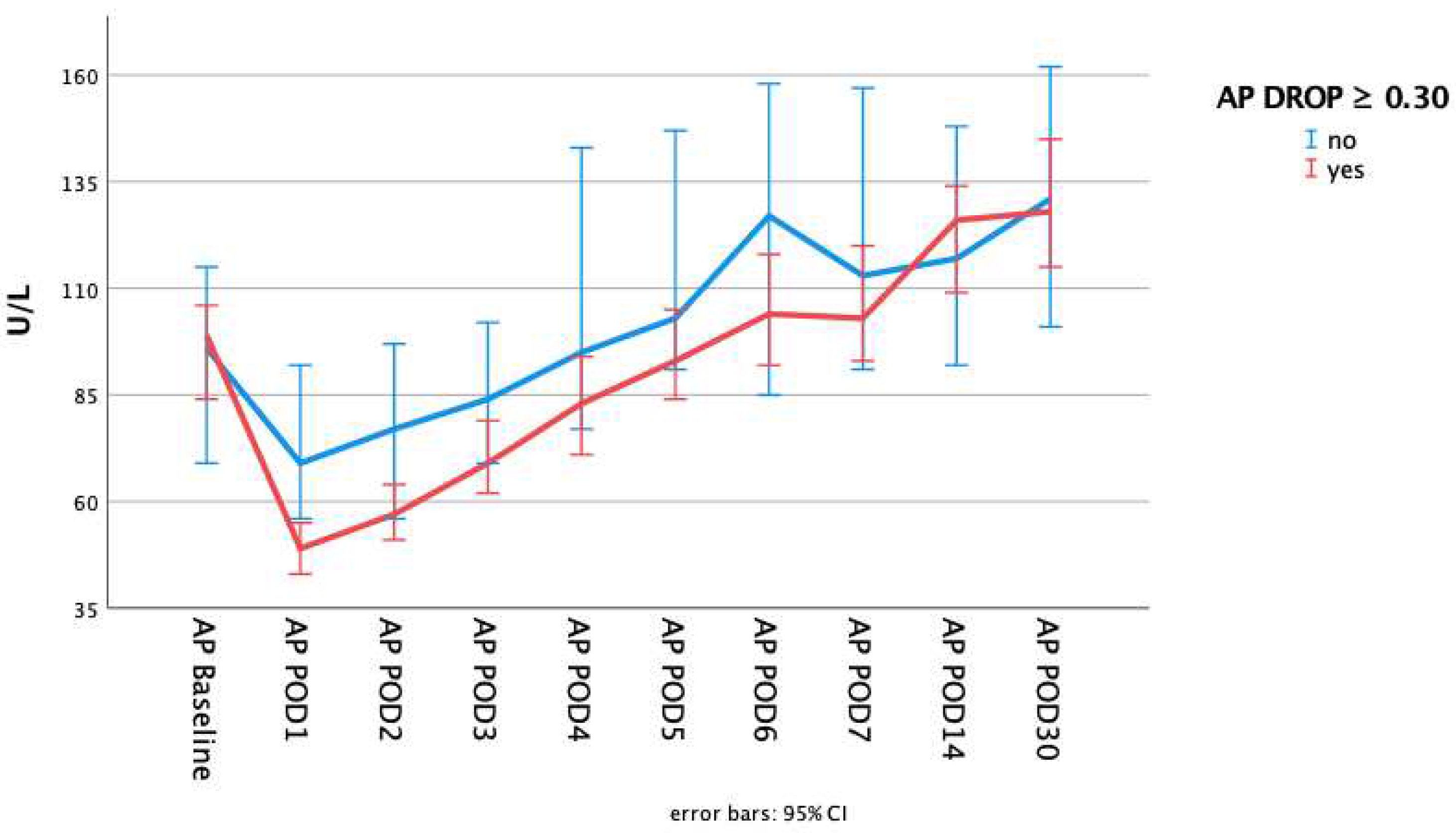
Figure 2.
Comparison of alkaline phosphatase levels at baseline to different postoperative timepoints dependent on the initial drop of alkaline phosphatase. P-values calculated for the difference in alkaline phosphatase between the timepoints using Wilcoxon signed rank test. (a) Comparison AP baseline to POD 1 (b) Comparison AP baseline to POD 30.
Figure 2.
Comparison of alkaline phosphatase levels at baseline to different postoperative timepoints dependent on the initial drop of alkaline phosphatase. P-values calculated for the difference in alkaline phosphatase between the timepoints using Wilcoxon signed rank test. (a) Comparison AP baseline to POD 1 (b) Comparison AP baseline to POD 30.
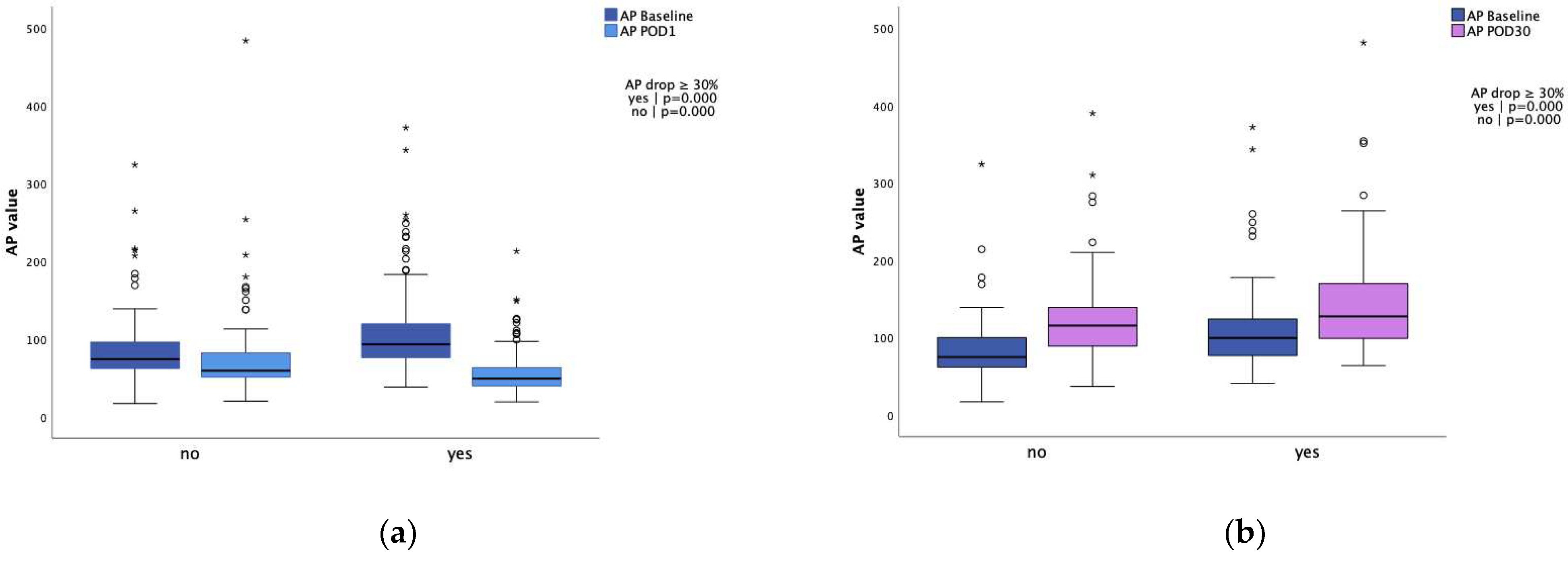
Figure 3.
10-year survival. Long-term survival comparison dependent on initial drop of alkaline phosphatase. P-value calculated using log-rank test.
Figure 3.
10-year survival. Long-term survival comparison dependent on initial drop of alkaline phosphatase. P-value calculated using log-rank test.
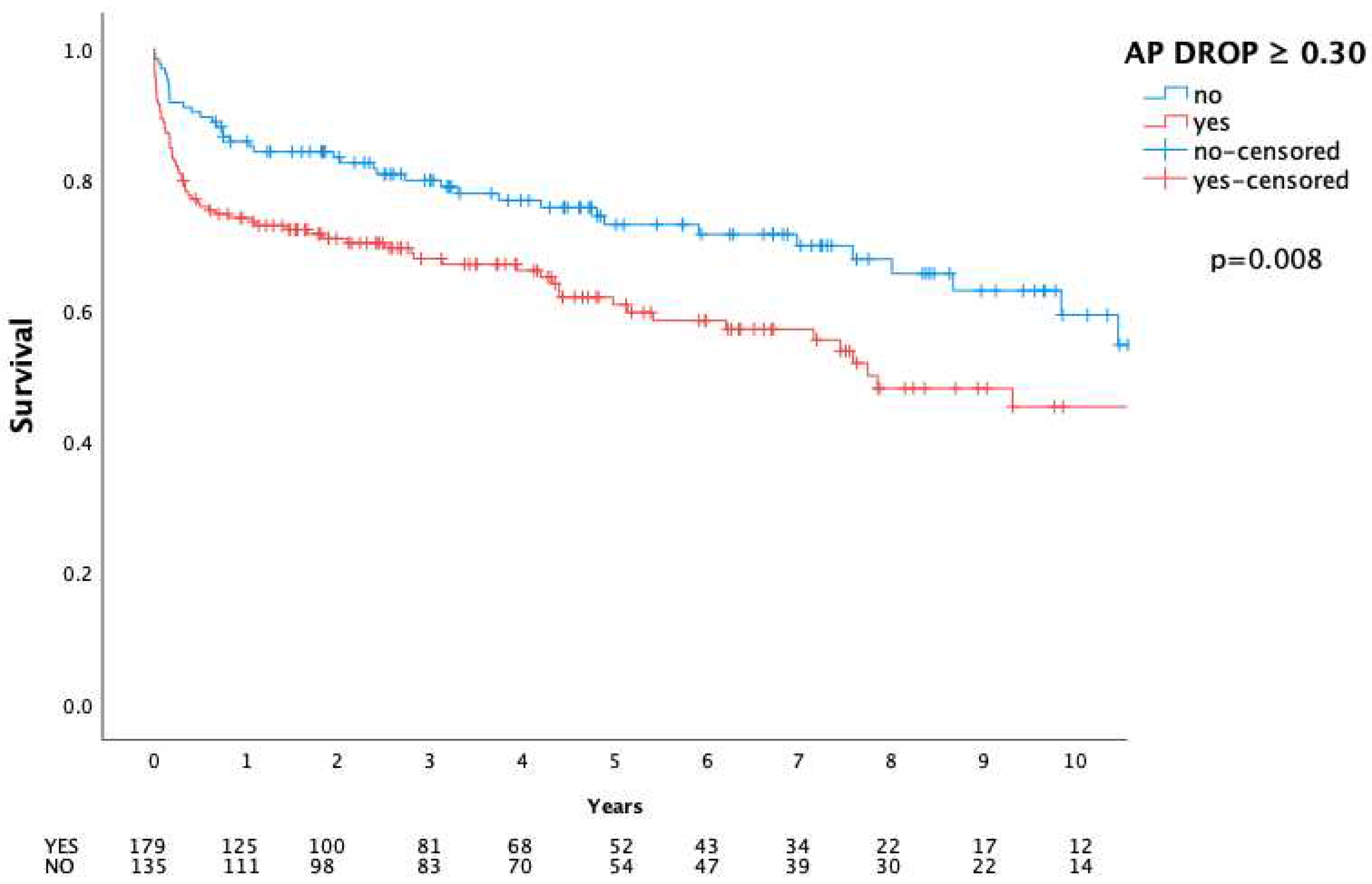

Table 1.
Preoperative characteristics.
| Overall n=314 |
AP drop < 30% n=135 |
AP drop ≥ 30% n=179 |
p-valueª | ||
|---|---|---|---|---|---|
| Age | 62 (70;48) | 59 (69;45) | 62 (70;49) | 0.230 | |
| Female | 85 (27.1) | 37 (27.4) | 48 (26.8) | 0.907 | |
| BMI | 25.3 (28.9;22.8) | 25.1 (28.9;22.9) | 25.6 (28.7;22.5) † | 0.703 | |
| EuroScore II | 11.7 (26.4;5.5) | 9.1 (15.9;3.5) | 16.1 (34.3;6.4) | 0.000* | |
| NYHA III | 78 (24.8) | 34 (25.2) | 44 (24.6) | 0.902 | |
| NYHA IV | 89 (28.3) | 35 (25.9) | 54 (30.2) | 0.409 | |
| LVEF | 60 (60;55) | 60 (60;55) | 60 (60;55) | 0.042* | |
| Hypertension | 200 (63.7) | 79 (58.5) | 121 (67.6) | 0.098 | |
| Atrial fibrillation | 90 (28.7) | 38 (28.1) | 52 (29.1) | 0.861 | |
| IDDM | 15 (4.8) | 6 (4.4) | 9 (5.0) | 0.810 | |
| Preoperative dialysis | 32 (10.2) | 8 (5.9) | 24 (13.4) | 0.030* | |
| Cancer | 19 (6.1) | 10 (7.4) | 9 (5.0) | 0.381 | |
| h/o stroke | 123 (39.2) | 55 (40.7) | 68 (38.0) | 0.621 | |
| Modified Duke Criteria | |||||
| Major criteria | Positive BC | 259 (82.5) | 107 (79.3) | 152 (84.9) | 0.192 |
| Vegetation | 266 (84.7) | 114 (84.4) | 152 (84.9) | 0.908 | |
| Annular abscess | 131 (41.7) | 55 (40.7) | 76 (42.5) | 0.760 | |
| Minor criteria | IV drug abuse | 24 (7.6) | 11 (8.1) | 13 (7.3) | 0.770 |
| Fever > 38°C | 201 (64.0) | 81 (60) | 120 (67.0) | 0.198 | |
| Vascular phenomena | 161 (51.3) | 67 (49.6) | 94 (52.5) | 0.613 | |
| Immunologic phenomena | 19 (6.1) | 11 (8.1) | 8 (4.5) | 0.176 | |
| PVE | 99 (31.5) | 27 (20.0) | 72 (40.2) | 0.000* | |
| Preoperative ventilation | 142 (45.2) | 64 (47.4) | 78 (43.6) | 0.499 | |
| Preoperative inotropic support | 88 (28.0) | 32 (23.7) | 56 (31.3) | 0.139 | |
| CPR | 13 (4.1) | 5 (3.7) | 8 (4.5) | 0.736 | |
| Lactate value | 0.9 (1.3;0.7) | 0.8 (1.2;0.7) | 1.0 (1.3;0.7) | 0.013* |
All values are referred in median (Q3;Q1) or in total number (n) and percentage (%) if not stated otherwise | † normal distributed, median taken for better comparison | ª If not stated otherwise, the Mann-Whitney U Test and Pearson’s chi-squared test, respectively, were used; values marked with an asterisk (*) achieved statistically significance | age [years]; BC – blood culture; BMI – body mass index [kg/m2]; CPR – cardiopulmonary resuscitation; lactate [mmol/l]; EuroSCORE II: European System for Cardiac Operative Risk Evaluation [%]; h/o – history of; IDDM – insulin dependent diabetes mellitus; IV – intravenous; NYHA – new york heart association classification; LVEF – left ventricular ejection fraction [%]; PVE – prosthetic valve endocarditis.
Table 2.
Procedural data.
| Overall n=314 |
AP drop < 30% n=135 |
AP drop ≥ 30% n=179 |
p-valueª | |
|---|---|---|---|---|
| Urgent operation | 262 (83.4) | 118 (87.4) | 144 (80.4) | 0.100 |
| Emergency operation | 49 (15.6) | 16 (11.9) | 33 (18.4) | 0.111 |
| Salvage operation | 3 (1.0) | 1 (0.7) | 2 (1.1) | 0.734 |
| Full sternotomy | 303 (96.5) | 128 (94.8) | 175 (97.8) | 0.159 |
| Re-sternotomy | 102 (32.5) | 29 (21.5) | 73 (40.8) | 0.000* |
| Isolated AVR | 168 (53.5) | 84 (62.2) | 84 (46.9) | 0.007* |
| Isolated MVR | 93 (29.6) | 39 (28.9) | 54 (30.2) | 0.806 |
| Double valve replacement | 52 (16.9) | 12 (8.9) | 41 (22.9) | 0.001* |
| Surgery time | 276 (390;220) | 240 (300;195) | 348 (455;255) | 0.000* |
| CPB | 139 (204;104) | 110 (155;90) | 162 (237;117) | 0.000* |
| ACC | 100 (144;70) | 81 (113;62) | 111 (159;79) | 0.000* |
All values are referred in median (Q3;Q1) or in total number (n) and percentage (%) | ª If not stated otherwise, the Mann-Whitney U Test and Pearson’s chi-squared test, respectively, were used; values marked with an asterisk (*) achieved statistically significance | ACC – aortic cross clamp time in minutes; AVR – aortic valve replacement; CPB – cardiopulmonary bypass in minutes; MVR – mitral valve replacement.
Table 3.
Laboratory data.
| Overall n=314 |
AP drop < 30% n=135 |
AP drop ≥ 30% n=179 |
p-valueª | |
|---|---|---|---|---|
| Baseline AP value | 85 (112;69) | 74 (96;62) | 93 (120;76) | 0.000* |
| Baseline CRP value | 4.2 (10.7;1.6) | 3.9 (8.3;1.7) | 4.5 (11.7;1.5) | 0.456 |
| AP Drop | 32.5 (45.2;23.0) | 21.4 (25.8;11.5) | 42.7 (54.7;36.4) | 0.000* |
| First day baseline AP value surpassedå | 5 (7;4) | 4 (6;3) | 6 (7;4) | 0.000* |
| Baseline within 3 days | 118 (37.6) | 59 (43.7) | 59 (33.0) | 0.052 |
| Baseline within 5 days | 208 (66.2) | 100 (74.1) | 108 (60.3) | 0.011* |
| 30day AP value∫ | 121 (157;95) | 116 (141;89) | 128 (172;99) | 0.089 |
| 30day CRP valueç | 3.4 (7.8;1.1) | 2.1 (5.7;0.7) | 4.6 (10.6;1.8) | 0.001* |
All values are referred in median (Q3;Q1) or in total number (n) and percentage (%) |ª If not stated otherwise, the Mann-Whitney U Test and Pearson’s chi-squared test, respectively, were used; values marked with an asterisk (*) achieved statistically significance | AP in U/L | AP Drop – defined as 1 – AP POD 1 / AP Baseline | CRP – C-reactive protein in mg/dL. å available for 254 patients (overall), 115 (AP drop < 30%) and 139 (AP drop ≥ 30%) ∫ available for 140 patients (overall), 62 (AP drop < 30%) and 78 (AP drop ≥ 30%). ç available for 159 patients (overall), 71 (AP drop < 30%) and 88 (AP drop ≥ 30%).
Table 4.
Adverse events and mortality.
| Overall n=314 |
AP drop < 30% n=135 |
AP drop ≥ 30% n=179 |
p-valueª | ||
|---|---|---|---|---|---|
| Bleeding revision | 38 (12.1) | 10 (7.4) | 28 (15.6) | 0.027* | |
| Need for any renal replacement therapy |
49 (15.6) | 10 (7.4) | 39 (21.8) | 0.001* | |
| Need for any renal replacement therapy without preoperative | 37 (11.8) | 9 (6.7) | 28 (15.6) | 0.015* | |
| Need for ECMO | 37 (11.8) | 3 (2.2) | 34 (19.0) | 0.000* | |
| Prolonged intubation | 107 (34.1) | 38 (28.1) | 69 (38.5) | 0.054 | |
| Prolonged ICU stay | 129 (41.1) | 43 (31.9) | 86 (48.0) | 0.004* | |
| Prolonged hospital stay | 62 (19.7) | 22 (16.3) | 40 (22.3) | 0.182 | |
| Mortality | |||||
| 30 day | 23 (7.3) | 4 (3.0) | 19 (10.6) | 0.010* | |
| In-hospital | 39 (12.4) | 8 (5.9) | 31 (17.3) | 0.002* | |
| 1 year | 65 (20.7) | 19 (14.1) | 46 (25.7) | 0.012* |
All values are referred in median (Q3;Q1) or in total number (n) and percentage (%) |ª If not stated otherwise, the Mann-Whitney U Test and Pearson’s chi-squared test, respectively, were used; values marked with an asterisk (*) achieved statistically significance |.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



