
Submitted:
19 June 2023
Posted:
20 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Not in the history of transmissible illnesses has there been an infection as strongly associated with acute cerebrovascular disease as the novel human coronavirus, SARS-CoV-2. While the risk of stroke has known associations with other viral infections, such as influenza and human immunodeficiency virus, the risk of ischemic and hemorrhagic stroke related to SARS-CoV-2 is unprecedented. Furthermore, the coronavirus disease 2019 (COVID-19) pandemic has so profoundly impacted psychosocial behaviors and modern medical care that we have witnessed shifts in epidemiology and have adapted our treatment practices to reduce transmission, address delayed diagnoses, and mitigate gaps in health care. In this narrative review, we summarize the history and impact of the COVID-19 pandemic on cerebrovascular disease, and lessons learned regarding the management of patients as we endure this period of human history.
Keywords:
Coronavirus disease 2019
; COVID-19
; Stroke
; Cerebral vein thrombosis
; Intracranial hemorrhage
; Anticoagulation
; Mechanical thrombectomy
; Intravenous thrombolysis
Following the emergence of the novel human coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), there has been an explosion of research into the global epidemiologic impact and paradigm shifts in care related to the COVID-19 pandemic. As we move into the third year of the pandemic, with rapidly accumulating literature on the topic, we provide an update to prior reviews [1,2] on the association between COVID-19 and cerebrovascular disease.
1. History of COVID-19 and Its Variants
Now having infected more than 750 million persons, accounting for more than 6.9 million fatalities worldwide [3,4], the first cases of the novel human coronavirus disease 2019 (COVID-19) were reported in December 2019 in Wuhan, China. Initial manifestations of the SARS-CoV-2 infection included respiratory failure and multi-organ dysfunction, with a wide variety of neurological presentations. Neurological manifestations related to COVID-19 range from common symptoms of gustatory and olfactory dysfunction, headache, dizziness, to more severe neurological complications of cerebral venous thrombosis, seizures, posterior reversible encephalopathy syndrome, and stroke–with stroke occurring in 1.1%-1.5% of patients admitted with COVID-19 according to global reports [5,6].
Over time, new variants of SARS-CoV-2 were identified. Among them, the delta and omicron variants were sequenced in May and November 2021, respectively, and have been implicated in more severe clinical phenotypes of COVID-19. Following the emergence of the delta SARS-CoV-2 variant, there was an increased risk of neurological complications, including stroke and seizure, as well as an increase in anxiety disorders and heightened risk of early mortality [7,8]. During times when the omicron variant of SARS-CoV-2 was more prevalent, there were similarly high rates of neurological complications, while the hospitalization rates and duration of symptoms decreased when compared to the delta variant [9]. Compared to patients infected with the delta variant, those affected by omicron had a lower prevalence of the prototypical COVID-19 symptoms of fever, loss of smell, and persistent cough. However, omicron infected individuals had higher prevalence of sore throat, hoarse voice, as well as joint and muscle pain.
In addition to the significant concerns regarding the variable mortality and long-term complications of COVID-19, including the post-acute sequelae syndrome (“Long COVID”) [8], there were considerable concerns regarding higher levels of transmissibility (particularly with delta and omicron variants) and resistance of SARS-CoV-2 variants to vaccines under development [10,11]. By indirect comparisons of clinical trial data, vaccine efficacy for the omicron variant was lower than the delta variant for the ChAdOx1 nCoV-19 (AstraZeneca), BNT162b2 (Pfizer/BioNTech), and mRNA-1273 (Moderna) vaccines. Even with subsequent immunizations/boosters, vaccine effectiveness for the delta variant ranged from 72-95% in comparison to 46-68% for the omicron variant [11].
Given the high risk of thrombotic complications with acute SARS-CoV-2, including ischemic stroke and cerebral vein thrombosis, one might expect a rise in the worldwide incidence rate of ischemic stroke and cerebrovascular disease during the COVID-19 pandemic. However, for reasons that are summarized in the following sections, there was a global decline in stroke diagnoses during the early months of the pandemic, with other epidemiologic and paradigm changes as a consequence of the biological and psychosocial effects of COVID-19.
2. Direct and Indirect Relationships between COVID-19 and Cerebrovascular Disease
Never before has a virus been so strongly linked to a heightened risk of acute cerebrovascular disease. The risk of stroke has a known association with many transmissible infections, including those responsible for bronchitis, influenza, H. pylori, cytomegalovirus, and many others [12]. The inflammatory response to these infections is thought to trigger inflammation and endothelial dysfunction, culminating in vascular events such as ischemic stroke and myocardial infarction [13]. Among the more common infections, the ongoing human immunodeficiency virus pandemic has been associated with a 60% relative increase in the risk of stroke and grows over time, although the overall incidence of stroke with this virus is low (1.28% over a 5-year period) [14]. Influenza, by contrast, is associated with a small but significant early risk (maximal within the first 15 days of symptoms), which disappears within 2 months [15]. The temporal association between stroke and SARS-CoV-2 is similar more to the relationship between influenza and stroke in that there is a high early risk that likely falls with time. However, the risk of stroke is several-fold greater with SARS-CoV-2 than influenza [16].
Multiple mechanisms account for the unique association between SARS-CoV-2 and stroke (Figure 1). Some of these include increased thromboxane synthesis with associated platelet activation, rapid turnover of fibrinogen, endothelial dysfunction and inflammation, as well as thrombus formation following cardiac dysfunction. Following infection, the SARS-CoV-2 spike protein activates platelets via platelet angiotensin converting enzyme 2 (ACE2) receptors, resulting in heightened expression of platelet integrin αIIbβ3 and P-selectin, which facilitates degranulation and platelet aggregation [17]. The vascular endothelium is also highly susceptible to viremia given its surface expression of ACE2 receptors, which permits viral entry into endothelial cells leading to activation/disruption [18]. In parallel with these pathways responsible for platelet activation and endothelial dysfunction, SARS-CoV-2 indirectly activates factor X via inflammatory mediators (e.g., IL-6 and IL-8), which increase tissue factor expression–thereby activating the extrinsic pathway [19]. Further, 30-40% of patients with severe COVID-19 may develop myocardial ischemia, elevated troponins, and new heart failure with resultant ventricular dysfunction [20], potentially contributing to intracardiac thrombus formation and stroke or systemic embolism. There is also suggestion of elevated anticardiolipin IgA, and beta-2-glycoprotein IgG and IgM levels in patients with COVID-19 in several reports [21,22,23], but these serum findings are also found in patients with other acute infections (unrelated to SARS-CoV-2).
Among the multiple thrombotic complications of COVID-19, ischemic stroke has been reported in approximately 1.0-1.5% of all hospitalized individuals who test positive for SARS-CoV-2 [6], with twice as many patients having no identifiable mechanism of cerebral infarction (>40%) as compared to conventional stroke cohorts [24]. Further, in one early multinational cohort of 156 patients with stroke and COVID-19, nearly half (49.5%) presented with a proximal or medium vessel occlusion on initial neuroimaging–a nearly doubled risk compared to historic stroke cohorts with traditional mechanisms [25]. Even more concerning, when considering the “cryptogenic” mechanism of stroke as being directly related to SARS-CoV-2, the risk of early mortality may be five-fold greater when compared to patients with other suspected mechanisms of infarction, according to one case-control study (adjusted OR 5.16, 95% CI 1.41-18.87) [26].
In addition to these cerebrovascular complications of SARS-CoV-2 infection, although it has not been explicitly studied, the psychosocial consequences of COVID-19 may also impact risk of cerebrovascular disease. Early avoidance of health care institutions in the setting of milder cerebrovascular events [27], delays (or cancellations) in primary care appointments [28], and other factors may have inadvertently affected control of vascular risk factors and heightened long-term stroke risk. Moreover, long-term consequences of COVID-19 include an increased risk of diabetes, congestive heart failure, coronary disease, and hypertension [29]–which can directly increase the risk of ischemic stroke–or fatigue, brain fog, and depression [30]–which can indirectly augment stroke risk by influencing activity, diet, and lifestyle preferences. The direct and indirect factors associated with stroke and disability following COVID-19 are illustrated in Figure 1.
3. Cerebral Vein Thrombosis
Beyond its effect on the cardiopulmonary system and the vascular endothelium, SARS-CoV-2 has been associated with a higher risk of venous thromboembolism and cerebral venous thrombosis (CVT) [31,32]. These thromboembolic events are not only disabling in and of themselves [33], but they are also thought of as biomarkers of more severe COVID-19 illness with greater morbidity and mortality. Results from one meta-analysis early in the course of the pandemic, including >8,000 patients with COVID-19 (21% of whom developed venous thromboembolism), indicated a 74% higher odds of mortality when venous thromboembolism occurred concomitantly with COVID-19 (odds ratio [OR] 1.74, 95% confidence interval [CI] 1.01-2.98) [34].
For a condition with a low historic incidence rate of 1-2 per 100,000 [35], CVT is over 10 times more common in patients infected with SARS-CoV-2 than in patients free of this infection [36,37]. In contrast to classic CVT which is more common in younger female patients and is generally associated with a favorable prognosis, CVT in patients with COVID-19 infection has been more common in older males without traditional risk factors and with greater morbidity and mortality than CVT associated with other conditions [38,39,40]. Along with other data regarding thrombotic risk of SARS-CoV-2, the risk of CVT gave rise to early recommendations for empiric anticoagulation among hospitalized patients with COVID-19, although evidence justifying these early recommendations was limited (see ‘Antithrombotic Strategies’).
The elevated incidence of CVT in hospitalized COVID-19 patients, coupled with their hypercoagulable state, provides compelling evidence of a causal link between COVID-19 infection and CVT. However, despite the fact that many studies have shown an increased incidence of CVT in patients with COVID-19 infections, the true incidence and prevalence of CVT among patients with COVID-19 remain unknown. Furthermore, these epidemiological and comparative studies before and during the COVID-19 pandemic years should be interpreted with caution as these incidences have not been estimated from the same population (e.g., CVT incidence was largely calculated among hospitalized COVID-19 patients and not the total COVID-19–positive population), and CVT risk factors may be confounded by known COVID-19 morbidity risk factors. For instance, one large multinational longitudinal cross-sectional study (n=217,560 COVID-19 patients, n=2,313 CVT patients) showed no significant differences in CVT volume or CVT in-hospital mortality overall between the first year of the COVID-19 pandemic compared to the pre-pandemic year [41]. Investigators from this study showed, however, that patients with CVT and COVID-19 had higher in-hospital mortality than COVID-negative patients (15.0% vs. 4.5%, p<0.01).
CVT has also been reported following certain SARS-CoV-2 vaccinations, mostly with the adenovirus vector-based vaccines (Ad26.COV2.S [Janssen/Johnson & Johnson] and ChAdOx1 [AstraZeneca]) [36,42]. The similarities between the clinical syndrome reported in these patients and spontaneous heparin-induced thrombocytopenia led investigators to identify circulating platelet-activating platelet factor 4 (PF4) antibodies in many of these patients [43]. The condition has been named vaccine-induced immune thrombotic thrombocytopenia and has preferentially affected young and middle-aged women without preexisting conditions [44]. These reports have prompted several countries to restrict the use of these vaccines, especially in younger patients. Although the relative morbidity of VITT is concerning, it remains a rare event, and the incidence of CVT among patients hospitalized with COVID-19 is significantly higher than VITT–related CVT [38]. Using publicly available data from Our World In Data, we have previously estimated across various age groups that the ChAdOx1 and Ad.26.COV2.S may be associated with >95% relative risk reduction for COVID-19-associated CVT as compared to the VITT-related COVID-19 [36]. For this reason, and for many other systemic and public health reasons, the advantages of SARS-CoV-2 vaccination by far exceed this risk of vaccination. Moreover, VITT and venous thromboembolic events have not been demonstrated in mRNA-based vaccines [45]. That said, the choice of one vaccine over another ought to be made at the patient level and considering the individualized risk of thrombotic events.
4. Antithrombotic Strategies
Given the high risk of thrombotic events associated with COVID-19, the safety and efficacy of anticoagulation has been explored in a number of randomized clinical trials [46]. More specifically, it has been thought that the prothrombotic state of COVID-19 may be mitigated with heparin, which has anti-factor Xa activity, anti-inflammatory effects, and potential antiviral effects against SARS-CoV-2 [47]. The RAPID clinical trial investigators evaluated the benefit of therapeutic heparin in critically ill patients with elevated D-dimer for the composite outcome of in-hospital mortality, invasive or non-invasive ventilation, or admission to an intensive care unit. The investigators found no significant advantage of anticoagulation over standard-of-care, however mortality was significantly lower with anticoagulation (OR 0.22, 95% CI 0.07-0.65) [48]. The HEP-COVID investigators also reported a benefit of therapeutic anticoagulation in patients with COVID-19 and elevated D-dimers for the outcome of venous or arterial embolism, and death due to any cause (relative risk 0.68; 95% CI 0.49-0.96). In this trial, the benefit was observed exclusively in non-critically ill patients [49]. Unfortunately, the risk of stroke was not reported in either RAPID or HEP-COVID. In the largest randomized clinical trial of non-critically ill patients with COVID-19, the ATTACC, ACTIV-4a, and REMAP-CAP investigators found that therapeutic anticoagulation with heparin increased the probability of patients surviving their hospitalization and being discharged with a reduced duration of need for intensive care (median adjusted OR of organ support-free days 1.27, 95% credible interval 1.03-1.58) [50]. Notably, this trial included all-comers with COVID-19, and the event rates for primary intracerebral hemorrhage were zero in both arms, and only 3 ischemic strokes occurred during hospitalization (2 with standard-of-care thromboprophylaxis, 1 with anticoagulation) [50]. The FREEDOM COVID Trialists also reported a survival advantage with therapeutic anticoagulation, although there was no benefit for the primary trial endpoint of all-cause mortality, requirement for intensive care unit–level of care, systemic thromboembolism, or ischemic stroke [51].
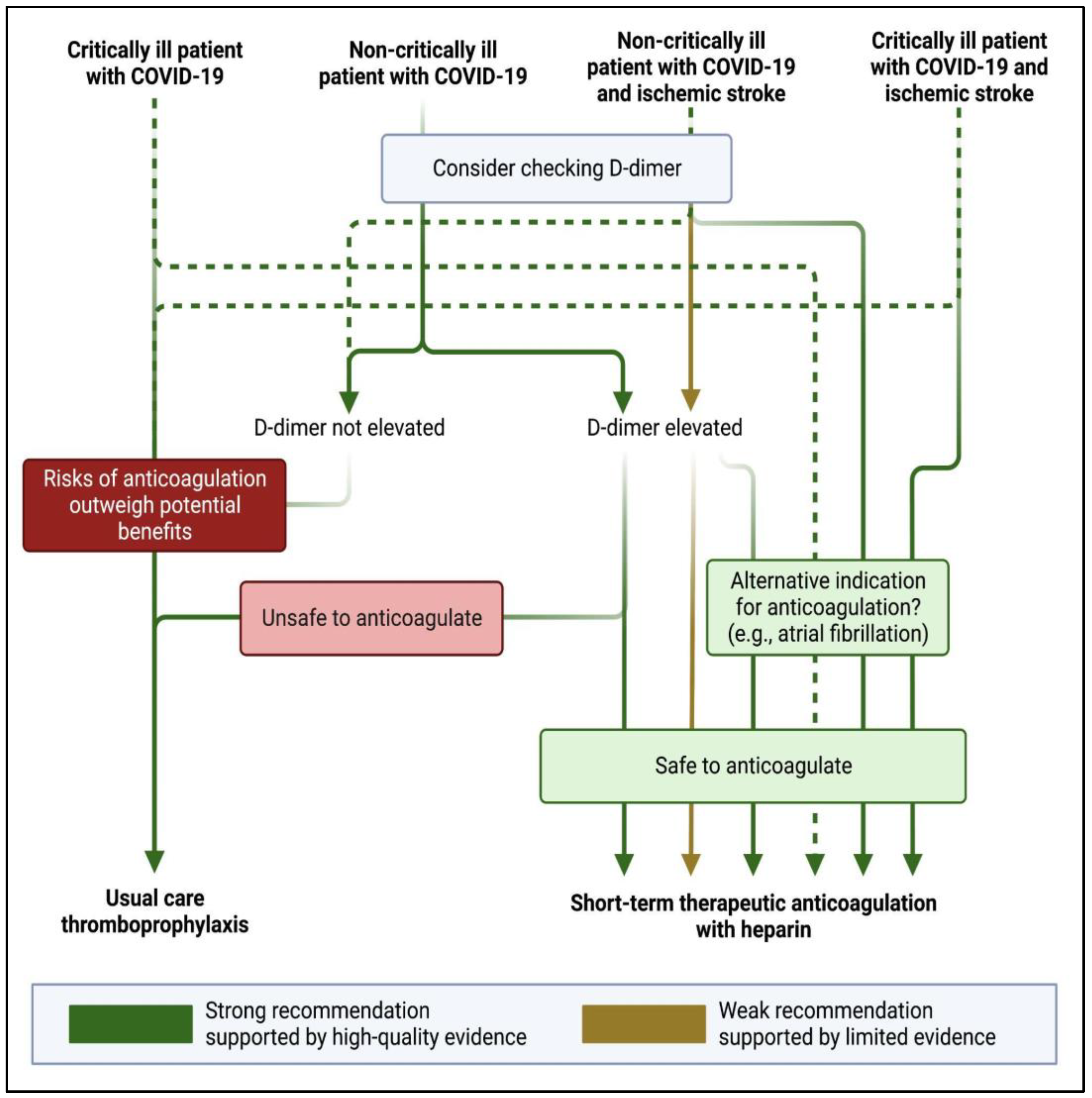
In a meta-analysis of available trial data, there was a significant benefit of therapeutic anticoagulation for the reduction in major thrombotic events (OR 0.47, 95% CI 0.24-0.90), but only in non-critically ill patients [52]. While there appears to be some benefit of short-term therapeutic anticoagulation with heparin, and a potential reduction in the risk of thromboembolism in certain patients with elevated D-dimer in non-critically ill patients, we cannot know whether therapeutic anticoagulation reduces the probability of ischemic stroke or increases the risk of hemorrhagic stroke in these patients. There are currently no ongoing trials looking into the benefit of treating patients with therapeutic anticoagulation post-discharge for patients with an ischemic stroke. In the absence of high quality data (and with no planned trials in a stroke population with COVID-19), many stroke providers believe it to be reasonable to consider (at least short-term) therapeutic anticoagulation in patients with ischemic stroke and COVID-19 especially if they are found in multiple vascular territories with an elevated D-dimer, suggesting an embolic phenomenon (Figure 2) [53,54]. In these situations, there is no specific D-dimer threshold high enough to warrant anticoagulation (or at which anticoagulation may be of benefit), although studies have identified heightened thrombotic events with D-dimer thresholds ranging from 1ug/mL [55] to 500ug/mL [56].
Although there is likely a benefit in primary prevention of major thrombotic events in select patients with COVID-19, there is unclear benefit for secondary prevention of ischemic stroke in COVID-19 patients. Furthermore, there are presently no guidelines or societal recommendations for these scenarios. The 2021 American Heart Association guidelines on secondary stroke prevention (published 15 months after the World Health Organization declared COVID-19 a pandemic) do not mention COVID-19 [57]. Presumably, the risk of subsequent arterial or venous thrombosis following ischemic infarction in a patient with COVID-19 (particularly a non-critically patient with elevated d-dimer) is high [58]. In patients with stroke and an indication for therapeutic anticoagulation (e.g., non-valvular atrial fibrillation), it is reasonable to treat with therapeutic anticoagulation as long as the risk of bleeding is outweighed by the benefit of anticoagulation. For most patients with stroke and COVID-19, but no alternative indication for anticoagulation, single antiplatelet (or short-term dual antiplatelet) therapy is safe and may be effective. For patients with embolic cryptogenic infarcts presumably due to COVID-19 hypercoagulability–particularly those with elevated D-dimer who are non-critically ill– short-term anticoagulation (30-60 days) with heparin and bridge to a direct oral anticoagulant can be considered, followed by antiplatelet monotherapy. For stroke patients with incidentally found SARS-CoV-2 by nasopharyngeal polymerase chain reaction, and no concern for hypercoagulable state, antiplatelet monotherapy (or short-term dual antiplatelet treatment, per guidelines [57]) is reasonable for secondary stroke prevention.
Any potential benefit of antithrombotic therapy must be weighed against the risk of hemorrhage. Among patients with COVID-19, there is a heightened risk of intracranial hemorrhage [59]. An international study showed patients with COVID-19 and acute ischemic stroke had higher rates of bleeding complications with revascularization treatment (intravenous thrombolysis or mechanical thrombectomy) and worse outcomes compared to contemporaneous patients who were being treated without COVID-19 [60]. Nonetheless, in the absence of a control group of patients who did not receive revascularization treatment, there is insufficient data regarding the risks of intravenous thrombolysis in acute ischemic stroke [61], therefore COVID-19 (or suspected COVID-19) should not be a contraindication to systemic thrombolysis. Furthermore, endovascular recanalization is not thought to be futile in patients with proximal large vessel occlusion who would otherwise meet criteria for thrombectomy [2]. While proximal intracranial occlusions are independent risk factors for poor outcomes and early mortality in the setting of COVID-19 [26,62], these patients should not be excluded from endovascular treatment [63]. One multicenter retrospective analysis of 575 patients with proximal intracranial occlusion (n=194 with COVID-19) reported lower rates successful recanalization (modified thrombolysis in cerebral infarction grade 3) in patients with COVID-19 versus non-COVID-19 patients (39.2% vs. 67.2%; adjusted OR 0.4, 95% CI 0.2-0.8, p<0.01) with higher rates of discharge with mRS >2 (79.8% vs. 66.7%; adjusted OR 2.6, 95% CI 1.1-5.8, p=0.03) with propensity score matching [64]. However, these patients still achieved better clinical outcomes than historic cohorts of non-COVID-19 patients with proximal occlusions treated medically.
The duration of antithrombotic treatment in patients with stroke presumably due to COVID-19 is unclear. While the severity of COVID-19 is mediated, in part, by many vascular risk factors (such as diabetes and chronic obstructive pulmonary disease) which predispose to cerebrovascular events, COVID-19 has been implicated as a unique mechanism of cerebral infarction irrespective of this clinical history. For these patients who survive COVID-19 and have no other cause of stroke, it is unclear what–if any benefit–may be gained from lifelong antithrombotic treatment. Such ill-defined benefit from long-term antiplatelet or anticoagulant therapy following COVID-19-associated stroke is much like the unclear advantage of long-term antithrombotic therapy in cervical artery dissection. The 2021 Guidelines from the American Heart Association have recommended anticoagulation for patients in a hypercoagulable state [57]. However, this is dependent on the cause of the patient’s hypercoagulable state and it is still unclear whether oral anticoagulation with direct oral anticoagulants or vitamin K antagonists offer differential protection from thrombotic events when compared to heparin.
5. COVID-19 Impact on Stroke Systems of Care
For many reasons, the COVID-19 pandemic has led to a decline in new diagnoses of acute cerebrovascular disease [5,6,65,66,67], myocardial infarction [68,69], and other acute medical conditions [70]. Some of this epidemiologic shift was driven by the abrupt change in medical-seeking behaviors of patients (who became avoidant of health care institutions due to fear of contracting SARS-CoV-2) [71,72,73]. But there is also compelling evidence that declines in other transmissible infections, such as influenza [74], mediate declines in vascular events [2,12]. Despite the greater risk of ischemic stroke due to SARS-CoV-2 than infections like influenza [16], the significantly lower incidence rate of other communicable respiratory and gastrointestinal infections during the COVID-19 pandemic [75,76] (which may be more common than SARS-CoV-2) likely displaced any rise in stroke rate due to SARS-CoV-2.
Early in the course of COVID-19, as health care systems adapted to contact and respiratory precautions, several major barriers to acute stroke care emerged [1]. First, there was a dramatic change in available emergency medical services with fewer available first responders in the community. Second, while the overall number of patients treated in emergency departments fell steeply [76], safety precautions implemented in emergency departments led to bottlenecks in acute care for many conditions, including stroke. While data do not indicate consistent delays in neurodiagnostic testing (e.g., due to needs for frequent decontamination of equipment), resource limitations and precautions have been associated with delays in intravenous thrombolysis according to several large analyses [77,78], mechanical thrombectomy [79], with expected deleterious effects on clinical outcomes [80].
As stated previously, SARS-CoV-2 has been directly related to large vessel intracranial occlusions [26,81], which are amenable to endovascular treatment. Access to endovascular treatment centers and time to recanalization therapy do not seem to have been adversely affected by the COVID-pandemic [82,83], despite the precautions necessary to maintain safety of patients and providers. Pandemic preparedness campaigns and early guidance from multiple vascular societies may have influenced the stability of treatment times and specialist availability [63,84,85]. In addition, many non-urgent endovascular cases were rescheduled to reduce unnecessary patient exposure in health care settings [2,86], with concomitant increases in endovascular treatment (over open surgical treatment) of other acute conditions–such as ruptured intracranial aneurysms [67,87].
In addition to these collateral effects on acute intervention and stabilization of patients with stroke during the COVID-19 pandemic, we also witnessed changes in patient and family education, disposition planning, and post-discharge follow-up. With implementation of contact precautions, many family members were prohibited from entering health care facilities. Therefore, much of stroke education was provided to patients in person–or caregivers via telephone, when possible. While it has not been well studied, the limited bandwidth of providers during this time and these changes in education and counseling may have negatively impacted patient and caregiver teaching. Further compounding the (potentially suboptimal) education difficulties during the COVID-19 pandemic was the reduction in patient time spent with rehabilitation specialists. A large number of stroke [88,89] and non-stroke [90,91] patients admitted during the pandemic who were potentially eligible for discharge to acute inpatient rehabilitation facilities were discharged more frequently to home (with fewer available therapy services). This disposition derailment may be due to a number of collateral effects of the pandemic. First, discharges to home may be preferred by patients, caregivers, and providers because they can be planned more quickly than arranging a discharge to an inpatient facility. Second, discharges to home (which may be faster) can reduce the exposure of patients to hospital and rehabilitation facility staff–and other patients–potentially carrying SARS-CoV-2. And finally, during the pandemic, discharges to post-acute care institutions were delayed due to a decline in availability of rehabilitation and nursing facilities [92]. At follow-up, in-person contact with health care providers and hospital staff was quickly restricted. While telemedicine appointments became a new standard of care and reduced the exposure of patients and caregivers to SARS-CoV-2, these virtual services increased accessibility of patients to specialty providers across great distances. Furthermore, telemedicine reduced consumption of personal protective equipment [93]. That said, the (practically obligatory) transition from in-person to telemedical visits was fraught with early difficulties regarding reimbursement for services and limitations of physical assessments–many of which have been assuaged over time.
6. Future Directions
To say that the COVID-19 pandemic has altered the epidemiology of stroke and transformed the manner in which we care for our patients would be an understatement. As we endure through this pandemic, we would be remiss to ignore the lessons learned along the way. Our deeper understanding of the relationship between transmissible infections and ischemic stroke should reinforce the value of primary care, attention to basic hygienic interventions, and vaccinations. The successes of telemedicine in providing subspecialty care to rural areas and to patients with limited mobility or access to providers has the potential to reduce many disparities. And while there is much we have learned for the better, we have also grown more cautious to accept published information as fact. Early reports seeking to dispel myths of stroke due to COVID-19 [94], or misleading statements pertaining to risks of COVID-19 vaccination [95], have caused us to question social media, journalism, and even scientific peer review. Further, such misinformation campaigns have sowed a public sense of mistrust of medical providers so deep that it may take a generation (or more) to rectify. With that in mind, let us accept and embrace this journey to rehabilitate the public perspective of health care providers and clinical science. As patient advocates, we have a renewed obligation to leverage all resources available to us–ranging from the scientific method to social media–to promote the dissemination of accurate information and improve the wellbeing of our patients and communities.
Author Contributions
“Conceptualization, J.E.S. and T.N.N..; investigation, J.E.S., S.D., M.A., M.P., S.Y., T.N.N.; resources, T.N.N.; data curation, S.D., M.A., M. P.; writing—original draft preparation, J.E.S., S.D., M.A., M. P.; writing—review and editing, S.Y., T.N.N.; supervision, J.E.S., T.N.N. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegler JE, Abdalkader M, Michel P, Nguyen TN. Therapeutic Trends of Cerebrovascular Disease during the COVID-19 Pandemic and Future Perspectives. J. Stroke. 2022, 24, 179–188. [CrossRef]
- Rana A, Nguyen TN, Siegler JE. Stroke and neurointervention in the COVID-19 pandemic: a narrative review. Expert Rev. Med. Devices 2021, 18, 523–531. [CrossRef] [PubMed]
- Mathieu E, Ritchie H, Rodés-Guirao L, Appel C, Giattino C, Hasell J, Macdonald B, Dattani S, Beltekian D, Ortiz-Ospina E, et al. Coronavirus Pandemic (COVID-19). Our World in Data. 2020 [cited 2023 May 18];Available from: https://ourworldindata.org/covid-cases.
- WHO Coronavirus (COVID-19) dashboard. [cited 2023 Jun 13];Available from: https://covid19.who.int/.
- Nogueira RG, Qureshi MM, Abdalkader M, Martins SO, Yamagami H, Qiu Z, Mansour OY, Sathya A, Czlonkowska A, Tsivgoulis G, et al. Global Impact of COVID-19 on Stroke Care and IV Thrombolysis. Neurology 2021, 96, e2824–e2838.
- Nguyen TN, Qureshi MM, Klein P, Yamagami H, Mikulik R, Czlonkowska A, Abdalkader M, Sedova P, Sathya A, Lo HC, et al. Global Impact of the COVID-19 Pandemic on Stroke Volumes and Cerebrovascular Events: A 1-Year Follow-up. Neurology 2023, 100, e408–e421. [CrossRef] [PubMed]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [CrossRef]
- Moghimi N, Di Napoli M, Biller J, Siegler JE, Shekhar R, McCullough LD, Harkins MS, Hong E, Alaouieh DA, Mansueto G, et al. The Neurological Manifestations of Post-Acute Sequelae of SARS-CoV-2 infection. Curr. Neurol. Neurosci. Rep. 2021, 21, 44.
- Menni C, Valdes AM, Polidori L, Antonelli M, Penamakuri S, Nogal A, Louca P, May A, Figueiredo JC, Hu C, et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: a prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624.
- Kläser K, Molteni E, Graham M, Canas LS, Österdahl MF, Antonelli M, Chen L, Deng J, Murray B, Kerfoot E, et al. COVID-19 due to the B.1.617.2 (Delta) variant compared to B.1.1.7 (Alpha) variant of SARS-CoV-2: a prospective observational cohort study. Sci. Rep. 2022, 12, 1–17.
- Collie S, Champion J, Moultrie H, Bekker L-G, Gray G. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 494–496. [CrossRef]
- Grau AJ, Urbanek C, Palm F. Common infections and the risk of stroke. Nat. Rev. Neurol. 2010, 6, 681–694. [CrossRef]
- Lindsberg PJ, Grau AJ. Inflammation and infections as risk factors for ischemic stroke. Stroke 2003, 34, 2518–2532. [CrossRef] [PubMed]
- Rasmussen LD, Engsig FN, Christensen H, Gerstoft J, Kronborg G, Pedersen C, Obel N. Risk of cerebrovascular events in persons with and without HIV: a Danish nationwide population-based cohort study. AIDS 2011, 25, 1637–1646. [CrossRef] [PubMed]
- Boehme AK, Luna J, Kulick ER, Kamel H, Elkind MSV. Influenza-like illness as a trigger for ischemic stroke. Ann. Clin. Transl. Neurol. 2018, 5, 456–463. [CrossRef]
- Merkler AE, Parikh NS, Mir S, Gupta A, Kamel H, Lin E, Lantos J, Schenck EJ, Goyal P, Bruce SS, et al. Risk of Ischemic Stroke in Patients With Coronavirus Disease 2019 (COVID-19) vs Patients With Influenza. JAMA Neurol. 2020. [CrossRef]
- Zhang S, Liu Y, Wang X, Yang L, Li H, Wang Y, Liu M, Zhao X, Xie Y, Yang Y, et al. SARS-CoV-2 binds platelet ACE2 to enhance thrombosis in COVID-19. J. Hematol. Oncol. 2020, 13, 120. [CrossRef]
- Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, Mehra MR, Schuepbach RA, Ruschitzka F, Moch H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418.
- Page EM, Ariëns RAS. Mechanisms of thrombosis and cardiovascular complications in COVID-19. Thromb. Res. 2021, 200, 1–8. [CrossRef]
- Sandoval Y, Januzzi JL Jr, Jaffe AS. Cardiac troponin for assessment of myocardial injury in COVID-19: JACC review topic of the week. J. Am. Coll. Cardiol. 2020, 76, 1244–1258. [CrossRef]
- Zhang Y, Xiao M, Zhang S, Xia P, Cao W, Jiang W, Chen H, Ding X, Zhao H, Zhang H, et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38.
- Rothstein A, Oldridge O, Schwennesen H, Do D, Cucchiara BL. Acute Cerebrovascular Events in Hospitalized COVID-19 Patients. Stroke 2020, 51, e219–e222.
- Harzallah I, Debliquis A, Drénou B. Lupus anticoagulant is frequent in patients with Covid-19. J. Thromb. Haemost. 2020, 18, 2064–2065. [CrossRef] [PubMed]
- Siegler JE, Cardona P, Arenillas JF, Talavera B, Guillen AN, Chavarría-Miranda A, de Lera M, Khandelwal P, Bach I, Patel P, et al. Cerebrovascular events and outcomes in hospitalized patients with COVID-19: The SVIN COVID-19 Multinational Registry. Int. J. Stroke 2021, 16, 437–447. [CrossRef] [PubMed]
- Lakomkin N, Dhamoon M, Carroll K, Singh IP, Tuhrim S, Lee J, Fifi JT, Mocco J. Prevalence of large vessel occlusion in patients presenting with acute ischemic stroke: a 10-year systematic review of the literature. J. Neurointerv. Surg. 2019, 11, 241–245. [CrossRef]
- Ramos-Araque ME, Siegler JE, Ribo M, Requena M, López C, de Lera M, Arenillas JF, Pérez IH, Gómez-Vicente B, Talavera B, et al. Stroke etiologies in patients with COVID-19: the SVIN COVID-19 multinational registry. BMC Neurol. 2021, 21, 43. [CrossRef]
- Siegler JE, Heslin ME, Thau L, Smith A, Jovin TG. Falling stroke rates during COVID-19 pandemic at a comprehensive stroke center. J. Stroke Cerebrovasc. Dis. 2020, 29, 104953. [CrossRef] [PubMed]
- Krist AH, DeVoe JE, Cheng A, Ehrlich T, Jones SM. Redesigning Primary Care to Address the COVID-19 Pandemic in the Midst of the Pandemic. Ann. Fam. Med. 2020, 18, 349–354. [CrossRef]
- Daugherty SE, Guo Y, Heath K, Dasmariñas MC, Jubilo KG, Samranvedhya J, Lipsitch M, Cohen K. Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study. BMJ 2021, 373, n1098.
- Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615.
- Knight R, Walker V, Ip S, Cooper JA, Bolton T, Keene S, Denholm R, Akbari A, Abbasizanjani H, Torabi F, et al. Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales. Circulation 2022, 146, 892–906.
- Abdalkader M, Shaikh SP, Siegler JE, Cervantes-Arslanian AM, Tiu C, Radu RA, Tiu VE, Jillella DV, Mansour OY, Vera V, et al. Cerebral Venous Sinus Thrombosis in COVID-19 Patients: A Multicenter Study and Review of Literature. J. Stroke Cerebrovasc. Dis. 2021, 30, 105733. [CrossRef]
- Klein P, Shu L, Nguyen TN, Siegler JE, Omran SS, Simpkins AN, Heldner M, Havenon A de, Aparicio HJ, Abdalkader M, et al. Outcome Prediction in Cerebral Venous Thrombosis: The IN-REvASC Score. J. Stroke Cerebrovasc. Dis. 2022, 24, 404–416.
- Malas MB, Naazie IN, Elsayed N, Mathlouthi A, Marmor R, Clary B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100639.
- Otite FO, Patel S, Sharma R, Khandwala P, Desai D, Latorre JG, Akano EO, Anikpezie N, Izzy S, Malik AM, et al. Trends in incidence and epidemiologic characteristics of cerebral venous thrombosis in the United States. Neurology 2020, 95, e2200–e2213. [CrossRef] [PubMed]
- Siegler JE, Klein P, Yaghi S, Vigilante N, Abdalkader M, Coutinho JM, Abdul Khalek F, Nguyen TN. Cerebral Vein Thrombosis With Vaccine-Induced Immune Thrombotic Thrombocytopenia. Stroke 2021, 52, 3045–3053. [CrossRef]
- Dakay K, Cooper J, Bloomfield J, Overby P, Mayer SA, Nuoman R, Sahni R, Gulko E, Kaur G, Santarelli J, et al. Cerebral Venous Sinus Thrombosis in COVID-19 Infection: A Case Series and Review of The Literature. J. Stroke Cerebrovasc. Dis. 2021, 30, 105434. [CrossRef] [PubMed]
- McCullough-Hicks ME, Halterman DJ, Anderson D, Cohen K, Lakshminarayan K. High Incidence and Unique Features of Cerebral Venous Sinus Thrombosis in Hospitalized Patients With COVID-19 Infection. Stroke 2022, 53, e407–e410.
- Baldini T, Asioli GM, Romoli M, Carvalho Dias M, Schulte EC, Hauer L, Aguiar De Sousa D, Sellner J, Zini A. Cerebral venous thrombosis and severe acute respiratory syndrome coronavirus-2 infection: A systematic review and meta-analysis. Eur. J. Neurol. 2021. [CrossRef]
- Hinduja A, Nalleballe K, Onteddu S, Kovvuru S, Hussein O. Impact of cerebral venous sinus thrombosis associated with COVID-19. J. Neurol. Sci. 2021, 425, 117448. [CrossRef]
- Nguyen TN, Qureshi MM, Klein P, Yamagami H, Abdalkader M, Mikulik R, Sathya A, Mansour OY, Czlonkowska A, Lo H, et al. Global Impact of the COVID-19 Pandemic on Cerebral Venous Thrombosis and Mortality. J. Stroke Cerebrovasc. Dis. 2022, 24, 256–265.
- Tu TM, Yi SJ, Koh JS, Saffari SE, Hoe RHM, Chen GJ, Chiew HJ, Tham CH, Seet CYH, Yong MH, et al. Incidence of Cerebral Venous Thrombosis Following SARS-CoV-2 Infection vs mRNA SARS-CoV-2 Vaccination in Singapore. JAMA Netw Open 2022, 5, e222940. [CrossRef] [PubMed]
- Sánchez van Kammen M, Aguiar de Sousa D, Poli S, Cordonnier C, Heldner MR, van de Munckhof A, Krzywicka K, van Haaps T, Ciccone A, Middeldorp S, et al. Characteristics and Outcomes of Patients With Cerebral Venous Sinus Thrombosis in SARS-CoV-2 Vaccine-Induced Immune Thrombotic Thrombocytopenia. JAMA Neurol. 2021, 78, 1314–1323.
- Greinacher A, Thiele T, Warkentin TE, Weisser K, Kyrle PA, Eichinger S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021. [CrossRef]
- Nicholson M, Goubran H, Chan N, Siegal D. No apparent association between mRNA COVID-19 vaccination and venous thromboembolism. Blood Rev. 2022, 56, 100970. [CrossRef] [PubMed]
- Bikdeli B, Talasaz AH, Rashidi F, Bakhshandeh H, Rafiee F, Rezaeifar P, Baghizadeh E, Matin S, Jamalkhani S, Tahamtan O, et al. Intermediate-Dose versus Standard-Dose Prophylactic Anticoagulation in Patients with COVID-19 Admitted to the Intensive Care Unit: 90-Day Results from the INSPIRATION Randomized Trial. Thromb. Haemost. 2022, 122, 131–141.
- Buijsers B, Yanginlar C, Maciej-Hulme ML, de Mast Q, van der Vlag J. Beneficial non-anticoagulant mechanisms underlying heparin treatment of COVID-19 patients. EBioMedicine 2020, 59, 102969. [CrossRef]
- Sholzberg M, Tang GH, Rahhal H, AlHamzah M, Kreuziger LB, Áinle FN, Alomran F, Alayed K, Alsheef M, AlSumait F, et al. Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with covid-19 admitted to hospital: RAPID randomised clinical trial. BMJ 2021, 375, n2400.
- Spyropoulos AC, Goldin M, Giannis D, Diab W, Wang J, Khanijo S, Mignatti A, Gianos E, Cohen M, Sharifova G, et al. Efficacy and Safety of Therapeutic-Dose Heparin vs Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620.
- Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [CrossRef] [PubMed]
- Stone GW, Farkouh ME, Lala A, Tinuoye E, Dressler O, Moreno PR, Palacios IF, Goodman SG, Esper RB, Abizaid A, et al. Randomized Trial of Anticoagulation Strategies for Noncritically Ill Patients Hospitalized With COVID-19. J. Am. Coll. Cardiol. 2023, 81, 1747–1762.
- Sholzberg M, da Costa BR, Tang GH, Rahhal H, AlHamzah M, Baumann Kreuziger L, Ní Áinle F, Almarshoodi MO, James PD, Lillicrap D, et al. Randomized trials of therapeutic heparin for COVID-19: A meta-analysis. Res Pract Thromb Haemost 2021, 5, e12638.
- Simonetto M, Wechsler PM, Merkler AE. Stroke Treatment in the Era of COVID-19: a Review. Curr. Treat. Options Neurol. 2022, 24, 155–171. [CrossRef] [PubMed]
- Cappellari M, Zini A, Sangalli D, Cavallini A, Reggiani M, Sepe FN, Rifino N, Giussani G, Guidetti D, Zedde M, et al. Thrombolysis and bridging therapy in patients with acute ischaemic stroke and Covid-19. Eur. J. Neurol. 2020, 27, 2641–2645. [CrossRef] [PubMed]
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020, 395, 1054–1062. [CrossRef] [PubMed]
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [CrossRef] [PubMed]
- Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, Kamel H, Kernan WN, Kittner SJ, Leira EC, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467.
- Yamakawa M, Kuno T, Mikami T, Takagi H, Gronseth G. Clinical Characteristics of Stroke with COVID-19: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 105288. [CrossRef]
- Lang CN, Dettinger JS, Berchtold-Herz M, Utzolino S, Bemtgen X, Zotzmann V, Schmid B, Biever PM, Bode C, Müller-Peltzer K, et al. Correction to: Intracerebral Hemorrhage in COVID-19 Patients with Pulmonary Failure: A Propensity Score-Matched Registry Study. Neurocrit. Care 2021, 34, 1112. [CrossRef]
- Marto JP, Strambo D, Ntaios G, Nguyen TN, Herzig R, Czlonkowska A, Demeestere J, Mansour OY, Salerno A, Wegener S, et al. Safety and Outcome of Revascularization Treatment in Patients With Acute Ischemic Stroke and COVID-19: The Global COVID-19 Stroke Registry. Neurology 2023, 100, e739–e750.
- Sasanejad P, Afshar Hezarkhani L, Arsang-Jang S, Tsivgoulis G, Ghoreishi A, Barlinn K, Rahmig J, Farhoudi M, Sadeghi Hokmabadi E, Borhani-Haghighi A, et al. Safety and Outcomes of Intravenous Thrombolytic Therapy in Ischemic Stroke Patients with COVID-19: CASCADE Initiative. J. Stroke Cerebrovasc. Dis. 2021, 30, 106121.
- Dmytriw AA, Dibas M, Phan K, Efendizade A, Ospel J, Schirmer C, Settecase F, Heran MKS, Kühn AL, Puri AS, et al. Acute ischaemic stroke associated with SARS-CoV-2 infection in North America. J. Neurol. Neurosurg. Psychiatry 2022, 93, 360–368. [CrossRef]
- Nguyen TN, Abdalkader M, Jovin TG, Nogueira RG. Mechanical thrombectomy in the era of the COVID-19 pandemic: emergency preparedness for neuroscience teams: a guidance statement from the Society of vascular …. Stroke Available from: https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.120.030100. 2020.
- Jabbour P, Dmytriw AA, Sweid A, Piotin M, Bekelis K, Sourour N, Raz E, Linfante I, Dabus G, Kole M, et al. Characteristics of a COVID-19 Cohort With Large Vessel Occlusion: A Multicenter International Study. Neurosurgery 2022, 90, 725–733. [CrossRef]
- Siegler JE, Heslin ME, Thau L, Smith A. Falling stroke rates during COVID-19 pandemic at a Comprehensive Stroke Center: Cover title: Falling stroke rates during COVID-19. J. Stroke Cerebrovasc. Dis. Available from: https://www.sciencedirect.com/science/article/pii/S105230572030361X?casa_token=yXSRnHGlRDsAAAAA:mBl3lMpc1HjgqUiSzc4APwrhkY21fiZjCKEzuNVcWA3s76EPwUjET1RoNRki8hZFBMhxPKhCHuM. 2020.
- SVIN COVID-19 Global SAH Registry. Global impact of the COVID-19 pandemic on subarachnoid haemorrhage hospitalisations, aneurysm treatment and in-hospital mortality: 1-year follow-up. J. Neurol. Neurosurg. Psychiatry Available from: http://dx.doi.org/10.1136/jnnp-2022-329200. 2022. [CrossRef]
- Nguyen TN, Haussen DC, Qureshi MM, Yamagami H, Fujinaka T, Mansour OY, Abdalkader M, Frankel M, Qiu Z, Taylor A, et al. Decline in subarachnoid haemorrhage volumes associated with the first wave of the COVID-19 pandemic. Stroke Vasc Neurol 2021, 6, 542–552. [CrossRef] [PubMed]
- Solomon MD, McNulty EJ, Rana JS, Leong TK, Lee C, Sung S-H, Ambrosy AP, Sidney S, Go AS. The Covid-19 Pandemic and the Incidence of Acute Myocardial Infarction. N. Engl. J. Med. 2020, 383, 691–693.
- 69. Nogueira RG, Etter K, Nguyen TN, Ikeme S, Wong C, Frankel M, Haussen DC, Del Rio C, McDaniel M, Sachdeva R, et al. Changes in the care of acute cerebrovascular and cardiovascular conditions during the first year of the covid-19 pandemic in 746 hospitals in the USA: retrospective analysis. BMJ Med 2023, 2, e000207.
- Rosenthal MG, Fakhry SM, Morse JL, Wyse RJ, Garland JM, Duane TM, Slivinski A, Wilson NY, Watts DD, Shen Y, et al. Where did all the appendicitis go? Impact of the COVID-19 pandemic on volume, management, and outcomes of acute appendicitis in a nationwide, multicenter analysis. Ann. Surg. Open 2021, 2, e048.
- Gale R, Eberlein S, Fuller G, Khalil C, Almario CV, Spiegel BMR. Public Perspectives on Decisions About Emergency Care Seeking for Care Unrelated to COVID-19 During the COVID-19 Pandemic. JAMA Netw Open 2021, 4, e2120940. [CrossRef]
- Zhao J, Li H, Kung D, Fisher M, Shen Y, Liu R. Impact of the COVID-19 Epidemic on Stroke Care and Potential Solutions. Stroke Available from: https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.120.030225. 2020.
- Czeisler MÉ, Marynak K, Clarke KEN, Salah Z, Shakya I, Thierry JM, Ali N, McMillan H, Wiley JF, Weaver MD, et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns - United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [CrossRef] [PubMed]
- Olsen SJ, Winn AK, Budd AP, Prill MM, Steel J, Midgley CM, Kniss K, Burns E, Rowe T, Foust A, et al. Changes in Influenza and Other Respiratory Virus Activity During the COVID-19 Pandemic - United States, 2020-2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1013–1019. [CrossRef] [PubMed]
- Cassell K, Zipfel CM, Bansal S, Weinberger DM. Trends in non-COVID-19 hospitalizations prior to and during the COVID-19 pandemic period, United States, 2017–2021. Nat. Commun. 2022, 13, 1–8.
- Hartnett KP, Kite-Powell A, DeVies J, Coletta MA, Boehmer TK, Adjemian J, Gundlapalli AV, National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits - United States, January 1, 2019-May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704.
- Siegler JE, Zha AM, Czap AL, Ortega-Gutierrez S, Farooqui M, Liebeskind DS, Desai SM, Hassan AE, Starosciak AK, Linfante I, et al. Influence of the COVID-19 Pandemic on Treatment Times for Acute Ischemic Stroke: The Society of Vascular and Interventional Neurology Multicenter Collaboration. Stroke 2020, STROKEAHA120032789.
- Alonso de Leciñana M, Castellanos M, Ayo-Martín Ó, Morales A, Stroke Group - Spanish Society of Neurology. Stroke care during the COVID-19 outbreak in Spain: the experience of Spanish stroke units. Stroke Vasc Neurol 2021, 6, 267–273. [CrossRef] [PubMed]
- Rivera R, Amudio C, Cruz JP, Brunetti E, Catalan P, Sordo JG, Echeverria D, Badilla L, Chamorro A, Gonzalez C, et al. The impact of a two-year long COVID-19 public health restriction program on mechanical thrombectomy outcomes in a stroke network. J. Stroke Cerebrovasc. Dis. 2023, 32, 107138. [CrossRef] [PubMed]
- Jillella DV, Nahab F, Nguyen TN, Abdalkader M, Liebeskind DS, Vora N, Rai V, Haussen DC, Nogueira RG, Desai S, et al. Delays in thrombolysis during COVID-19 are associated with worse neurological outcomes: the Society of Vascular and Interventional Neurology Multicenter Collaboration. J. Neurol. 2022, 269, 603–608.
- Khandelwal P, Al-Mufti F, Tiwari A, Singla A, Dmytriw AA, Piano M, Quilici L, Pero G, Renieri L, Limbucci N, et al. Incidence, Characteristics and Outcomes of Large Vessel Stroke in COVID-19 Cohort: An International Multicenter Study. Neurosurgery 2021, 89, E35–E41. [CrossRef]
- Czap AL, Zha AM, Sebaugh J, Hassan AE, Shulman JG, Abdalkader M, Nguyen TN, Linfante I, Starosciak AK, Ortega-Gutierrez S, et al. Endovascular thrombectomy time metrics in the era of COVID-19: observations from the Society of Vascular and Interventional Neurology Multicenter Collaboration. J. Neurointerv. Surg. 2022, 14, neurintsurg–2020–017205.
- Raymaekers V, Demeestere J, Bellante F, De Blauwe S, De Raedt S, Dusart A, Jodaitis L, Lemmens R, Loos C, Noémie L, et al. The impact of COVID-19 on acute stroke care in Belgium. Acta Neurol. Belg. 2021, 121, 1251–1258.
- Stroke Council Leadership A. Temporary Emergency Guidance to US Stroke Centers During the Coronavirus Disease 2019 (COVID-19) Pandemic: On Behalf of the American Heart Association …. Stroke. 2020;Available from: https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.120.030023?casa_token=-gS7ZSAmrEQAAAAA:gLTFfX0gdo0YH3A2aoiUnMsrSBsKplk3HPGqYOTpgcBfEpc2akSNLyDjW6Sw884P5IWhFU3SzxjJbnY. g: from: https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.120.030023?casa_token=-gS7ZSAmrEQAAAAA, 1161.
- Nguyen TN, Jadhav AP, Dasenbrock HH, Nogueira RG, Abdalkader M, Ma A, Cervantes-Arslanian AM, Greer DM, Daneshmand A, Yavagal DR, et al. Subarachnoid hemorrhage guidance in the era of the COVID-19 pandemic - An opinion to mitigate exposure and conserve personal protective equipment. J. Stroke Cerebrovasc. Dis. 2020, 29, 105010.
- Abdalkader M, Sathya A, Malek AM, Fifi JT, Norbash AM, Wakhloo AK, Nguyen TN. Roadmap for Resuming Elective Neuroendovascular Procedures Following the First COVID-19 Surge. J. Stroke Cerebrovasc. Dis. 2020, 29, 105177. [CrossRef] [PubMed]
- Nguyen TN, Qureshi MM, Klein P, Yamagami H, Mikulik R, Etminan N, Abdalkader M, Mansour OY, Czlonkowska A, Lo H, et al. Global impact of the COVID-19 pandemic on subarachnoid haemorrhage hospitalisations, aneurysm treatment and in-hospital mortality: 1-year follow-up. J. Neurol. Neurosurg. Psychiatry Available from: https://scholarworks.bwise.kr/skku/handle/2021.sw.skku/98710. 2022.
- Thau L, Siegal T, Heslin ME, Rana A, Yu S, Kamen S, Chen A, Vigilante N, Gallagher S, Wegner K, et al. Decline in Rehab Transfers Among Rehab-Eligible Stroke Patients During the COVID-19 Pandemic. J. Stroke Cerebrovasc. Dis. 2021, 30, 105857. [CrossRef] [PubMed]
- Ortega-Gutierrez S, Farooqui M, Zha A, Czap A, Sebaugh J, Desai S, Jadhav A, Vora N, Rai V, Jovin TG, et al. Decline in mild stroke presentations and intravenous thrombolysis during the COVID-19 pandemic: the Society of vascular and Interventional Neurology multicenter collaboration. Clin. Neurol. Neurosurg. 2021, 201, 106436.
- Roberts P, Wertheimer J, Park E, Nuño M, Riggs R. Identification of Functional Limitations and Discharge Destination in Patients With COVID-19. Arch. Phys. Med. Rehabil. 2021, 102, 351–358. [CrossRef]
- Maltser S, Trovato E, Fusco HN, Sison CP, Ambrose AF, Herrera J, Murphy S, Kirshblum S, Bartels MN, Bagay L, et al. Challenges and Lessons Learned for Acute Inpatient Rehabilitation of Persons With COVID-19: Clinical Presentation, Assessment, Needs, and Services Utilization. Am. J. Phys. Med. Rehabil. 2021, 100, 1115–1123.
- Spanko, A. Nursing home industry projects $34B in revenue losses, 1,800 closures or mergers due to COVID. Skilled Nursing News. 2021 [cited 2023 May 1];Available from: https://skillednursingnews.com/2021/02/nursing-home-industry-projects-34b-in-revenue-losses-1800-closures-or-mergers-due-to-covid/. 1 May.
- Hubert GJ, Corea F, Schlachetzki F. The role of telemedicine in acute stroke treatment in times of pandemic. Curr. Opin. Neurol. 2021, 34, 22–26. [CrossRef]
- Miller A, Segan S, Rehmani R, Shabsigh R, Rahme R. Letter: Dismantling the Apocalypse Narrative: The Myth of the COVID-19 Stroke. Neurosurgery 2020, 87, E703–E704. [CrossRef]
- Chavda VP, Chen Y, Dave J, Chen Z-S, Chauhan SC, Yallapu MM, Uversky VN, Bezbaruah R, Patel S, Apostolopoulos V. COVID-19 and vaccination: myths vs science. Expert Rev. Vaccines 2022, 21, 1603–1620.
Figure 1.
Direct and indirect effects of COVID-19 on cerebrovascular disease. COVID-19 denotes coronavirus disease 2019. Figure generated using biorender.com.
Figure 1.
Direct and indirect effects of COVID-19 on cerebrovascular disease. COVID-19 denotes coronavirus disease 2019. Figure generated using biorender.com.
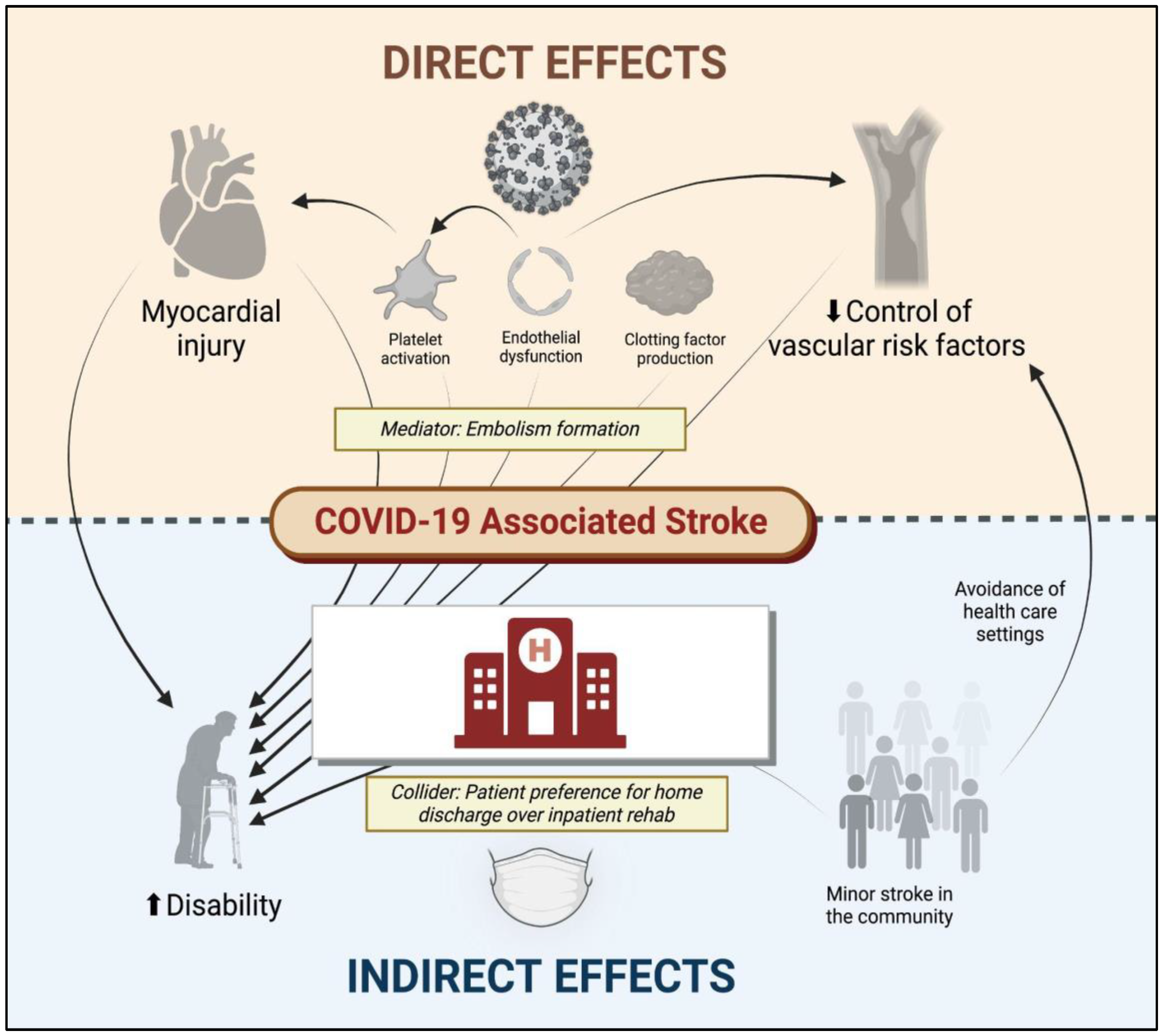
Figure 2.
Antithrombotic recommendations in patients with COVID-19. COVID-19 denotes coronavirus disease 2019. Figure generated using biorender.com.
Figure 2.
Antithrombotic recommendations in patients with COVID-19. COVID-19 denotes coronavirus disease 2019. Figure generated using biorender.com.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



