
Submitted:
21 June 2023
Posted:
23 June 2023
You are already at the latest version
Abstract
Esophageal cancer is a formidable challenge in the realm of cancer treatment. Conventional methods such as surgery, chemotherapy, and immunotherapy have demonstrated limited success rates in managing this disease. In response, targeted drug therapies have emerged as a promising strategy to improve outcomes for patients. These therapies aim to disrupt specific pathways involved in the growth and development of esophageal cancer cells. This review explores various drugs used to target specific pathways, including cetuximab and monoclonal antibodies (gefitinib) that target the epidermal growth factor receptor (EGFR), trastuzumab that targets human epidermal growth factor receptor 2 (HER-2), drugs targeting the vascular endothelial growth factor receptor (VEGFR), mTOR inhibitors, and cMET inhibitors. Additionally, the article discusses the impact of drug resistance on the effectiveness of these therapies, highlighting factors such as cancer stem cells, cancer-associated fibroblasts, immune-inflammatory cells, cytokines, hypoxia, and growth factors. While drug targeting approaches do not provide a complete cure for esophageal cancer due to drug resistance and associated side effects, they offer potential for improving patient survival rates.
Keywords:
Esophageal cancer
; Targeted drug therapies
; Pathway targeting
; Drug resistance
; Patient survival rates
1. Introduction
Esophageal carcinoma (EC) is a malignant disease with devastating effects. It is the ninth most common cancer and ranks as the sixth leading cause of cancer-related deaths worldwide [1]. EC, which includes esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC), is a kind of cancer that develops in the esophagus [2]. If it occurs in the middle or upper portion, EC can be fatal [3]. The male-to-female ratio is 3:1 for ESCC, while for EAC, it is 6:1. However, this ratio varies significantly across different geographical locations [4,5]. Cohort studies indicate that the incidence of esophageal cancer increases with age, with the typical age of onset being 65 to 70 years [6]. EC is characterized by progressive dysphagia and weight loss. Dysphagia often presents with vomiting of undigested food [7].
Tobacco smoking and excessive alcohol consumption, particularly when combined, are the primary risk factors for esophageal squamous cell cancer. EC is associated with gastroesophageal reflux disease and obesity [8]. A study suggests that squamous cell carcinoma is linked to an overrepresentation of C to A substitutions, which is more common among cigarette users [9]. Esophageal adenocarcinoma is associated with abnormalities in homologous recombination repair, a high mutational burden, or an aging-related C to A or T mutation pattern [10]. According to the World Health Organization, based on the Global Burden of Disease Study 2015, the estimated mortality rate from EC is 439,025 [11]. In 2018, there were approximately 500,000 cases of EC worldwide. Unfortunately, most patients are diagnosed at an advanced stage, resulting in a low overall survival rate of 20% at the end of five years [12]. However, multimodal therapy may lead to better outcomes as it has shown some improvement in overall survival [13]. Patients diagnosed with ESCC or EAC often present at an advanced stage, leaving limited treatment options. Chemotherapy is employed as a palliative approach for end-of-life cancer patients [14]. Unfortunately, there have been few significant clinical advancements in EC treatment over the past three decades, resulting in modest improvements in survival rates [15]. Chemotherapy has been a cornerstone in EC treatment, while molecular targeted therapy and immune checkpoint inhibitors have been investigated in preclinical and clinical trials [7,16,17]. Targeted molecular therapy serves as a vital adjunct to chemotherapy, although only a few targeted therapies are currently available in clinical practice [18]. Despite the initial success of targeted therapy in early-stage EC treatment, patients inevitably develop drug resistance during the course of treatment [19]. In addition to treatment resistance, recurrence and metastasis are the primary causes of treatment failure [20].
Several monoclonal antibodies and tyrosine kinase inhibitors (TKIs) have been discovered to date. These drugs can be used alone or in combination with conventional treatments to improve the prognosis of ESCC patients. This review primarily focuses on the utilization of different drug types to target signaling pathways (EGFR, HER2, VEGF, HGF/cMET, mTOR) associated with EC and inhibit their activity. Additionally, we address challenges related to targeting, such as cancer heterogeneity and the molecular mechanisms underlying drug resistance. Furthermore, we discuss the side effects of drugs used in targeting and present future prospects.
Drugs targeting the key signalling pathway
ESCC is believed to result from the dysregulation of cell signaling networks rather than individual mutations, as supported by recent research. There is an increasing consensus that mutations primarily affect signaling pathways rather than specific genes [21]. Therefore, targeting drugs towards these specific signaling pathways is crucial to reducing the risk of cancer. Numerous monoclonal antibodies and tyrosine kinase inhibitors have been discovered to date, which can be utilized alone or in combination with conventional treatments to improve the prognosis of esophageal cancer [22].(Figure 1)
Cetuximab and nimotuzumab are monoclonal antibodies that target the EGFR, while gefitinib and lapatinib are EGFR receptor tyrosine kinase inhibitors that bind to the RTK domain of EGFR, thereby downregulating signaling. Trastuzumab specifically targets HER-2 and increases the survival of patients. Ramucirumab is a monoclonal antibody that binds to VEGFR, while endostar and apatinib inhibit downstream signaling pathways. Rilotumumab inhibits the interaction of hepatocyte growth factor (HGF) with c-MET, and obinutuzumab blocks c-MET from binding to HGF. Rapamycin and everolimus inhibit mTOR signaling. All these drugs downregulate signaling, block esophageal cancer cell proliferation and division.
Drug targeting EGFR pathway
EGFR is a transmembrane growth factor receptor family that initiates signal transduction by activating a receptor-associated tyrosine kinase (RTKs) [23]. Upon ligand binding, this receptor triggers the formation of homodimers or heterodimers, which in turn activate the RAS-RAF-MEK-ERK-MAPK and PI3K-AKT-mTOR pathways, relaying downstream signals. Overexpression of EGFR contributes to carcinogenic effects [24,25]. Recently, several drugs with similar mechanisms have been discovered to block EGFR signaling, enabling successful treatment of EC [26]. Numerous monoclonal antibodies targeting EGFR have been designed, and inhibitors have been developed to inhibit EGFR signalling [27].
Anti EGFR monoclonal antibody
Anti-EGFR monoclonal antibodies have been widely explored and used in the treatment of different malignancies, including EC. However, their usefulness in the treatment of EC is still being studied. Anti-EGFR monoclonal antibodies, such as cetuximab and nimotuzumab, precisely target and bind to the EGFR protein, blocking its signaling pathways. They have the potential to limit tumor growth and enhance patient outcomes.
Cetuximab
Studies have evaluated the efficacy of cetuximab in combination with chemotherapy or radiation therapy for the treatment of EC. The results have been mixed, and the overall benefit of cetuximab in this context remains uncertain. Studies shows that when administered in conjugation with chemotherapy in other cancer, cetuximab gives improved results [28]. Cetuximab is effective in the treatment of advanced colorectal adenocarcinoma [29]. In addition, preclinical investigation indicates that cetuximab can overcome an essential mechanism of radio resistance[30]. Cetuximab also increases overall survival in patients with resectable ESCC without increasing toxicities or postoperative morbidity [31].
Nimotuzumab
The monoclonal antibody nimotuzumab has been utilized in cancer therapy due to its anti-EGFR activity [32]. Studies have demonstrated the effectiveness of nimotuzumab in combination with radiotherapy and chemotherapy for the treatment of EC [33]. The majority of these trials have reported positive outcomes. Phase I clinical trials involving patients with advanced EC utilized a combination of radiation therapy and nimotuzumab [34]. The trials determined that the maximum tolerated dosage was safe and tolerable. However, the ideal dose and frequency of nimotuzumab administration have yet to be established, although it has proven to be effective. Retrospective research suggests that nimotuzumab should be administered at a dosage of >200 mg per week [35]. In vitro studies have shown that nimotuzumab enhances the susceptibility of ESCC cells with high EGFR expression to radiation therapy. Additionally, nimotuzumab accelerates apoptosis in ESCC cells and inhibits the G2 phase of the ESCC cell cycle. In vivo, nimotuzumab inhibits EGFR phosphorylation and improves radiosensitivity in recurrent ESCC cells with EGFR overexpression [36].
The variability in treatment responses may be attributed to the heterogeneity of esophageal cancer, differences in patient populations, and the complex interplay of various molecular pathways involved in cancer growth. It's also important to consider that individual patient characteristics, such as EGFR expression levels and other genetic factors, can influence the response to anti-EGFR therapies. Anti-EGFR monoclonal antibodies are usually used in combination with chemotherapy or other agents. Some anti-EGFR monoclonal antibodies have been studied in EC, but further research is needed to fully understand their efficacy and optimal use in this particular cancer.
Anti EGFR tyrosine kinase inhibitor
Tyrosine kinase inhibitors (TKIs) are small oral drugs that prevent ATP from binding to the tyrosine kinase domain, thus inhibiting the autophosphorylation of EGFR and its subsequent signal transduction.
Gefitinib
Gefitinib is an orally administered selective and reversible EGFR tyrosine kinase inhibitor (TKI) [37]. By blocking downstream signaling of EGFR in cells, gefitinib inhibits the growth and progression of cancer [38]. The expression of galectin-3 was found to alter EGFR endocytosis and tumor development in the presence of gefitinib [39]. In a study conducted by Xu et al., it was observed that the combination of gefitinib with cisplatin or 5-fluorouracil (5-FU) improved the survival and quality of life in patients with advanced ESCC [40]. A primary cell line derived from an EC patient with significant EGFR polysomy exhibited high sensitivity to gefitinib [41].
Icotinib
The efficacy of icotinib, an EGFR tyrosine kinase inhibitor, was evaluated in ESCC cases with previous treatment and EGFR overexpression or amplification [42] Developed by Chinese scientists, icotinib is the first targeted small molecule drug designed as a novel anticancer therapy [43]. Preclinical studies have demonstrated that icotinib, an EGFR TKI, exhibits excellent specificity and selectivity towards its target, EGFR [42]. A study by Wang et al., icotinib was evaluated as a second-line treatment option for patients with advanced ESCC and EGFR overexpression or amplification. The results showed that icotinib led to a significant improvement in overall survival and progression-free survival compared to chemotherapy [44]. Another study by Li et al. investigated the efficacy and safety of icotinib in combination with radiotherapy for locally advanced ESCC. The combination therapy demonstrated promising results, with a higher overall response rate and longer median progression-free survival compared to radiotherapy alone [45].
Drug targeting HER2 pathway
The HER2 oncogene is responsible for encoding a transmembrane tyrosine kinase receptor belonging to the epidermal growth factor receptor (EGFR) family. It plays a crucial role in various cellular processes such as cell growth, migration, differentiation, proliferation, and survival [46]. The HER2 receptor consists of three domains: an extracellular domain, a lipophilic transmembrane domain, and an intracellular kinase domain. Ligand binding triggers kinase activation, leading to receptor dimerization [47]. HER2 receptor can be activated by HER2 mutations or overexpression, independent of ligand binding [48]. HER2 expression has been identified in several cancers, including esophageal and gastric, breast, and ovarian cancer. HER2-specific antibodies have been developed to disrupt HER signaling, employing two main mechanisms: receptor depletion from the cell surface and interference with heterodimerization [49,50].
Trastuzumab
Trastuzumab is an anti-HER2 monoclonal antibody that exhibits preclinical activities including antibody-dependent cell-mediated cytotoxicity (ADCC) and inhibition of growth stimulation [49]. Currently Trastuzumab, has emerged as a promising therapeutic option in the treatment of EC, particularly in HER2-positive cases. Recent research has focused on evaluating the efficacy of trastuzumab in combination with chemotherapy. It received approval from the Food and Drug Administration (FDA) in October 2010 for the treatment of patients with HER2-positive metastatic gastric or gastroesophageal (GE) adenocarcinoma who have not received prior treatment for metastatic disease. The approved regimen involves administering trastuzumab intravenously (IV) once every three weeks in combination with cisplatin and a fluopyrimidine (either capecitabine or 5-fluorouracil) [51].
The Trastuzumab for Gastric Cancer (ToGA) study, a landmark phase III clinical trial, demonstrated the benefit of adding trastuzumab to standard chemotherapy in HER2-positive advanced gastric or gastroesophageal junction cancer. Subsequent analyses of the ToGA study data have shown that the efficacy of trastuzumab extends to HER2-positive esophageal cancer as well. Patients with HER2-positive esophageal adenocarcinoma or squamous cell carcinoma treated with trastuzumab plus chemotherapy have shown improved overall survival and progression-free survival compared to those receiving chemotherapy alone [52].
Moreover, the phase III JACOB trial further supported the use of trastuzumab in HER2-positive esophagogastric cancer. This study demonstrated that trastuzumab, when combined with chemotherapy, led to a significant improvement in overall survival and progression-free survival compared to chemotherapy alone [53]. These studies highlight the importance of HER2-targeted therapy, specifically trastuzumab, in the management of HER2-positive EC. Initially marketed under the brand name Herceptin, comparable versions of trastuzumab, known as biosimilars, are now available under different names such as Ogivri, Herzuma, Ontruzant, Trazimera, and Kanjinti. These biosimilars have been developed to provide alternative treatment options while maintaining similar efficacy and safety profiles to the original drug.
Lapatinib
Lapatinib, also known as Tykerb or GlaxoSmithKline, is a reversible inhibitor of EGFR and HER2. It acts as a dual tyrosine kinase inhibitor by binding to the intracellular ATP binding site of these kinases, preventing their activation. In vitro and in vivo studies have shown that Lapatinib inhibits the growth of cancer cells overexpressing EGFR and/or HER2 by blocking downstream signaling pathways [54]. To eradicate ESCC cells expressing EGFR and/or HER2, Cetuximab and/or Herceptin-mediated ADCC has been utilized. The efficacy of this approach has been associated with the level of receptor expression intensity
Combining lapatinib with paclitaxel has been investigated by Guo et al, and they observed a synergistic effect on suppressing cell proliferation, as well as a significant decrease in ESCC cell invasion and migration. Treatment with lapatinib and paclitaxel led to a substantial decrease in the phosphorylation of downstream molecules MAPKs and AKT [55]. In vivo studies have shown that the combination of lapatinib and paclitaxel more effectively inhibits the growth of esophageal squamous carcinoma xenografts without increasing toxicity [56]. Furthermore, Hassan et al. evaluated the effect of Lapatinib and Foretinib on the expression of apoptosis-related proteins in OE33 esophageal adenocarcinoma xenografts in vivo [57]. Overall, these studies provide evidence for the potential of Lapatinib as a therapeutic agent in the treatment of esophageal cancer, particularly in cases involving EGFR and/or HER2 overexpression.
Drug targeting VEGF / VEGFR pathway
Signaling from vascular endothelial growth factor (VEGF) stimulates angiogenesis by promoting the migration and proliferation of endothelial cells [58]. VEGF receptor (VEGFR) is a specific receptor for VEGFs, and both tumors and stromal cells produce VEGFs that bind to VEGFR, acting in either an autocrine or paracrine manner [3]. The three main VEGF receptors, VEGFR1, VEGFR2, and VEGFR3, regulate signaling pathways that mediate the biological effects of VEGF [59].
Activation of VEGFR signaling leads to the activation of various intracellular proteins such as extracellular signal-regulated kinase 1/2 (ERK1/2), protein kinase A (PKA), and protein kinase B (PKB/AKT), which facilitate signal transduction and contribute to cell proliferation, migration, and survival [60]. The VEGF/VEGFR signaling pathway is a target for therapy in EC because VEGF production is closely associated with the development and prognosis of EC [61].
Ramucirumab
VEGFR-2 is inhibited by Ramucirumab, which is a fully humanized monoclonal antibody designed to bind to a ligand-binding epitope on VEGFR-2, thereby preventing VEGF ligands from interacting with this binding site [62]. In a phase I clinical study, it was observed that the concentration of VEGF A in the serum increased shortly after ramucirumab treatment and remained elevated for extended periods. However, the concentrations of VEGF 1 and VEGF 2 decreased immediately after ramucirumab therapy and returned to near-pretreatment levels [63]. Ramucirumab has been approved as an effective medication for advanced gastric or gastroesophageal junction (GEJ) adenocarcinoma, either as a monotherapy or in combination with paclitaxel in the second-line setting [64].
HGF/c-MET pathway
The c-MET (c-mesenchymal-epithelial transition) is a kinase receptor for hepatocyte growth factor (HGF) that has been implicated in carcinogenesis [65,66,67]. Upon interaction with HGF, c-MET activates several downstream signaling pathways, including the Phosphoinositide 3-kinase/threonine-protein kinase (PI3K/AKT) pathway, the Wnt pathway, and others [68,69,70]. In normal tissues, the HGF/c-MET receptor tyrosine kinase (RTK) pathway remains inactive; however, it becomes active in various malignancies [71]. Yang et al. observed higher c-Met protein expression in EC tissues compared to surrounding tissues. Increased c-Met expression was associated with clinical stage, depth of invasion, and lymph node metastasi [72].
Rilotumumab and Obinutuzumab
Rilotumumab and obinutuzumab are two drugs that target the HGF c-Met pathway. Rilotumumab is a fully humanized monoclonal antibody that inhibits the interaction between hepatocyte growth factor (HGF) and c-Met, thereby blocking c-Met activation and tumor development [73]. Obinutuzumab, on the other hand, is a humanized anti-MET antibody that prevents MET from binding to HGF [22]. Clinical studies involving gastric/adenocarcinoma patients who are MET-positive and treated with a combination of these drugs and chemotherapy have shown mixed results. Rilotumumab was found to be ineffective in effectively treating patients, and obinutuzumab did not significantly improve progression-free survival (PFS) or overall patient survival rates [74,75].
mTOR Pathway
The mammalian target of rapamycin (mTOR) is a serine-threonine kinase family that plays a crucial role in regulating the downstream signaling of the PI3K/AKT pathway. The mTOR signaling system influences various cellular processes, including cell survival, growth, proliferation, and motility, and it is interconnected with growth hormones, nutrition, and energy supply [76]. Dysregulation of mTOR is associated with cancer development. High levels of phosphorylated mTOR (p-mTOR) have been linked to a poor prognosis in ESCC, suggesting its potential as a therapeutic target [77]. Rapamycin, an mTORC1 inhibitor, is a drug that has been demonstrated to mimic the effects of calorie restriction and extend longevity [78]. Everolimus is another potent anticancer drug that inhibits mTOR activity [79]. Details description in Table 1
Factor associated with targeted therapy
Cancer heterogeneity
Cancer is a complex disease characterized by genetic variations known as cancer heterogeneity, which can differ among various tumor types and individuals [98]. heterogeneity in ESCC has been widely recognized, with studies demonstrating diverse molecular profiles within tumors. This heterogeneity can impact various aspects of ESCC, including tumor progression, treatment response, and patient outcomes [99]. Furthermore, heterogeneity exists within individual tumor cells, posing significant challenges in cancer treatment and potentially leading to drug resistance. In many cases, the majority of cancer cells within a tumor share common genetic alterations [21]. Understanding the extent of heterogeneity in ESCC can enhance the predictability of therapy.
Drug resistance
Drug resistance is defined as a decrease in the effectiveness of a drug, such as an antimicrobial or antineoplastic agent, in treating a medical condition [100].Various factors contribute to drug resistance in cancer treatment, including limitations in drug distribution, increased drug efflux, mutations in drug targets, DNA damage repair mechanisms, evasion of programmed cell death, and activation of alternative pro-tumorigenic signaling pathways [101].. The prevalence of drug resistance in esophageal cancer (EC) is rising, posing a significant barrier to effective therapy [102].
Growing evidence suggests that the interaction between tumor cells and the tumor microenvironment (TME) plays a crucial role in drug resistance. The TME includes not only cancer cells and cancer stem cells but also tumor-associated stromal cells (such as tumor-associated fibroblasts, immune and inflammatory cells, and endothelial cells) as well as non-cellular components (such as hypoxia, cytokines, acidity, extracellular matrix, and exosomes) [103]. Overall, drug resistance in EC poses a significant challenge in achieving optimal therapeutic outcomes for patients, and understanding the complex interplay between tumor cells and the TME is crucial for developing effective strategies to overcome resistance [104].
Cellular components involved in drug resistance
Cancer Stem Cells
Cancer stem cells (CSCs) are a small subset of cells within tumors that have the ability to initiate tumor formation and contribute to therapeutic resistance and cancer recurrence [105]. According to the stem cell theory of cancer, CSCs play a crucial role in tumor development and progression [106]. CSCs possess stem cell-like properties, including plasticity, self-renewal, dormancy, and drug resistance, and they can be identified by specific surface markers [107]. Several studies have demonstrated that cancer cells with stem cell-like characteristics exhibit higher resistance to chemotherapy [108].
In esophageal cancer (EC), CSCs employ various mechanisms to protect themselves from cytotoxic substances, particularly by enhancing the drug efflux process. One such mechanism involves a group of cells called side population (SP) cells, which are identified by flow cytometry and characterized by specific surface markers [109]. SP cells, which are enriched in CSCs, express high levels of ATP-binding cassette (ABC) transporters, such as ABCG5 and ABCG2, responsible for effluxing multiple drugs and conferring multidrug resistance [110]. Additionally, esophageal CSCs may hinder the drug influx process through the downregulation of Copper Uptake Protein 1 (CTR1), which is facilitated by p75 neurotrophin receptor (p75NTR) positive cells possessing stem cell-like characteristics and resistance to cisplatin [111,112].In summary, esophageal CSCs utilize specific membrane transporter distributions to maintain intracellular drug concentrations at safe levels and evade the cytotoxic effects of chemotherapy.
Cancer-Associated Fibroblasts
Cancer-associated fibroblasts (CAFs) are a type of cell found in the tumor microenvironment that contributes to tumorigenic properties by promoting extracellular matrix remodeling and secreting cytokines. Fibroblasts exist in varying quantities in different types of carcinomas and often represent the majority of the stromal cell population within the tumor [113]. The term "cancer-associated fibroblast" encompasses at least two distinct cell types: (1) fibroblasts that resemble the structural support cells found in normal epithelial tissues, and (2) myofibroblasts, which possess distinct biological roles and properties compared to tissue-derived fibroblasts [114].
CAFs, characterized by high levels of α-smooth muscle actin and fibroblast activation protein-α, are a significant component of the tumor stroma in the tumor microenvironment (TME) and play a crucial role in cancer development and resistance to medications [115]. In esophageal cancer (EC) and other malignancies, carcinogenesis is associated with persistent inflammation and mucosal damage. Normal fibroblasts undergo transformation into CAFs, which, in turn, confer drug resistance to neighboring EC cells by secreting soluble substances and enhancing pro-tumorigenic signals mediated by functional molecules such as microRNAs and lncRNAs [116,117]. Interleukin 6 (IL-6), a multifunctional cytokine involved in immunological and inflammatory responses, plays a role in cancer hallmarks, including treatment resistance. CAFs serve as crucial sources of IL-6 within the TME, leading to increased chemoresistance [118,119]. IL-6 derived from CAFs also contributes to chemoradiotherapy resistance in patients with esophageal adenocarcinoma (EAC).
However, CAFs in the tumor microenvironment have a significant impact on cancer development and drug resistance. Their secretion of soluble factors, including IL-6, and their ability to promote pro-tumorigenic signals contribute to the resistance of esophageal cancer cells to chemotherapy and chemoradiotherapy.
Inflammatory Immune cells
Tumor immune evasion is the ability of tumour cells to evade immunological responses by blocking T-cell activation [120]. These tumour cells build to programmed death ligand-1 and programmed death ligand-2 on the T-cell and inactivate them[121]. Cell surface inhibitors like PD-L1/2 and VISTA, as well as inhibitory receptors like PD-1, CTLA-4, T-cell immunoglobulin and mucin-domain containing-3 (TIM-3), and lymphocyte-activation gene 3 (LAG-3) are typically found in ECs[122]. Immune checkpoint drugs, such as nivolumab and pembrolizumab, have shown early promise in treating advanced or refractory EC[123]. In most studies, PD-L1 and PD-L2 are significantly expressed in a large number of ESCC patients (> 40%)[124]. The decreased level of tumor-infiltrating lymphocytes (TILs) has been linked to poor clinical outcomes in EC patients[125,126]. All these factors are responsible for the low response rate of immunotherapy.
Non-cellular components
Cytokines
Cytokines are markers for metastasis and angiogenesis, the primary causes of cancer death [127]. Cytokines released by the immune cells help activate several downstream pathways like JAT/STAT, NF-kβ, delta-notch to mediate various cancer characteristic traits [128]. In patients having esophagectomy, STAT3 activation by its principal inducers, IL-6 and IL-6R, has been linked to a poor prognosis [129]. IL-6 is produced by TME stromal cells like CAFs and confers chemoresistance on EC cells through various mechanisms [118,130]. EC cells treated with cisplatin produce more IL-6, enhancing STAT3 phosphorylation and conferring cancer markers, such as apoptosis evasion and chemoresistance [131]. The p65 component of NF-kβ is overexpressed and activated in EC specimens, and its link to 5-fluorouracil resistance has been confirmed in cultivated EC cell lines [132]. Downregulation of IL-1 receptor antagonist (IL-1RA) expression in EC is linked to tumour development and poor prognosis [133].
Hypoxia
Hypoxia is an abnormally low amount of oxygen tension that occurs in most malignant tumors [134]. Many hypoxia-inducible genes, such as hypoxia-inducible transcription factor (HIF), a dimeric protein composed of a constitutively active component (HIF-1) and an oxygen-sensitive subunit (HIF-1), are expressed when cancer cells are exposed to hypoxia[135]. In the EC, HIF-1 expression is linked to venous invasion, VEGF expression, and microvessel density [136]. Recent discovered state that a new lncRNA called EMS was hypoxia-induced and overexpressed in human EC tumour tissues and cell lines. Importantly, in the ECA-109 cell line, EMS expression was needed for hypoxia-mediated drug resistance to DDP [137].
Growth factors
Growth factors are responsible for the proliferation and differentiation of the cell. IGF-1 prevents apoptosis generated by various pharmacologic agents in EC, including cisplatin, 5-fluorouracil, and camptothecin (Liu et al., 2002). IGF-1, partly produced by Id1, can upregulate survivin expression via the PI3K/Akt and casein kinase 2 signaling pathways, inhibiting Smac/DIABLO release and activating caspases responsible for 5-fluorouracil-driven cell death [138]. In SLMT-1/CDDP1R cells(cisplatin/CDDP resistance), overexpression of IGFBP5 using an IGFBP5 expression vector reduced cisplatin resistance by 41%. As a result of recent findings, it is concluded that IGFBP5 suppression is one of the methods by which ESCC cells acquire cisplatin resistance[139]. IGF2 is involved in the regulation of EC chemoresistance. Although blocking the IGF2 receptor IGF1R can sensitize ESCC cells to 5-FU therapy, the function and mechanism of IGF2 in 5-FU chemoresistance have remained unknown[42]. By comparing the genome-wide gene profiles of the sensitivity and resistant xenografts, a recent study includes a cetuximab-sensitive ESCC tumour model that developed resistance to cetuximab as a result of FGFR2 gene amplification and overexpression [140]. In addition, although the mechanism is uncertain, FGFR inhibitors can decrease FGF-mediated lapatinib resistance[141].
Conclusion
In this review, we comprehensively discuss the latest advancements in drug targeting for EC. These drugs primarily aim to disrupt the various pathways involved in cell proliferation and differentiation, which contribute to the development of EC. Their mechanisms of action involve binding to specific receptors within these pathways, thereby inhibiting ligand binding or blocking downstream signaling. Notably, inhibitors targeting VEGFR (ramucirumab) and HER-2 (trastuzumab) have demonstrated improved survival outcomes and prognoses in advanced esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC). These medications are typically administered in combination with chemotherapy, radiotherapy, and immunotherapy. Combination therapy has been shown to impact the tumor microenvironment, enhance tumor cell response to targeted therapies, and improve disease control. Despite the extension of patients' lives achieved through targeted therapy, complete recovery remains elusive due to the emergence of medication resistance. Drug resistance in EC is a multifaceted process involving cancer cells, cancer stem cells (CSCs), tumor-associated stromal cells, hypoxia, immune-inflammatory cells, cytokines, growth factors, and other factors. Overcoming this challenge may lie in the future development of combination therapies, although adverse events associated with such treatments cannot be entirely avoided. Therefore, addressing the side effects of targeted therapy remains an important aspect to be resolved. Ongoing research efforts are focused on identifying and developing new targeted drugs to improve the treatment outcomes of EC. Further investigation is warranted to overcome drug resistance and effectively manage the side effects associated with targeted therapies in EC treatment.
Author Contributions
Conceptualization, B.L and H.K.V; methodology, P.P. and H.K.V; data curation, P.P. and H.K.V; writing—original draft preparation, P.P. and H.K.V; writing—review and editing, P.P, H.K.V and B.L supervision, B.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable as this is a review article.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
We do not have any conflict of interest.
References
- Collaboration, G.B.o.D.C., Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncology, 2017. 3(4): p. 524-548.
- Liu, K., et al., Etiology, cancer stem cells and potential diagnostic biomarkers for esophageal cancer. Cancer Lett, 2019. 458: p. 21-28. [CrossRef]
- Yang, Y.M., et al., Advances in targeted therapy for esophageal cancer. Signal Transduct Target Ther, 2020. 5(1): p. 229. [CrossRef]
- Edgren, G., et al., A global assessment of the oesophageal adenocarcinoma epidemic. Gut, 2013. 62(10): p. 1406. [CrossRef]
- Xie, S.-H. and J. Lagergren, A global assessment of the male predominance in esophageal adenocarcinoma. Oncotarget, 2016. 7(25): p. 38876-38883. [CrossRef]
- Lagergren, J. and P. Lagergren, Oesophageal cancer. 2010. 341: p. c6280.
- Smyth, E.C., et al., Oesophageal cancer. Nat Rev Dis Primers, 2017. 3: p. 17048.
- Tong, C., et al., Causes, Risk Factors and Outcomes of Patients Readmitted to the Intensive Care Unit After Esophageal Cancer Surgery: A Retrospective Cohort Study. World J Surg, 2021. 45(7): p. 2167-2175. [CrossRef]
- Lagergren, J., et al., Oesophageal cancer. The Lancet, 2017. 390(10110): p. 2383-2396.
- Secrier, M., et al., Mutational signatures in esophageal adenocarcinoma define etiologically distinct subgroups with therapeutic relevance. Nat Genet, 2016. 48(10): p. 1131-41. [CrossRef]
- Rahmani, H., et al., Burden of esophageal cancer in Iran during 1995-2015: Review of findings from the Global Burden of Disease studies. Medical journal of the Islamic Republic of Iran, 2018. 32: p. 55-55. [CrossRef]
- Lagergren, J., et al., Oesophageal cancer. Lancet, 2017. 390(10110): p. 2383-2396.
- Schweigert, M., A. Dubecz, and H.J. Stein, Oesophageal cancer--an overview. Nat Rev Gastroenterol Hepatol, 2013. 10(4): p. 230-44.
- Fatehi Hassanabad, A., et al., Esophageal carcinoma: Towards targeted therapies. Cell Oncol (Dordr), 2020. 43(2): p. 195-209. [CrossRef]
- Lu, R.-M., et al., Development of therapeutic antibodies for the treatment of diseases. Journal of Biomedical Science, 2020. 27(1): p. 1. [CrossRef]
- van Hagen, P., et al., Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med, 2012. 366(22): p. 2074-84. [CrossRef]
- Tong, Y., et al., Tumor-Secreted Exosomal lncRNA POU3F3 Promotes Cisplatin Resistance in ESCC by Inducing Fibroblast Differentiation into CAFs. Mol Ther Oncolytics, 2020. 18: p. 1-13. [CrossRef]
- Mao, C., et al., Mechanisms of Pharmaceutical Therapy and Drug Resistance in Esophageal Cancer. 2021. 9(22). [CrossRef]
- Hong, Y. and Z.Y. Ding, PD-1 Inhibitors in the Advanced Esophageal Cancer. Front Pharmacol, 2019. 10: p. 1418. [CrossRef]
- Aref, D. and S. Croul, Medulloblastoma: recurrence and metastasis. CNS oncology, 2013. 2: p. 377-385. [CrossRef]
- Kang, X., et al., Personalized targeted therapy for esophageal squamous cell carcinoma. World J Gastroenterol, 2015. 21(25): p. 7648-58. [CrossRef]
- Yang, Y.-M., et al., Advances in targeted therapy for esophageal cancer. Signal Transduct Target Ther, 2020. 5(1): p. 229. [CrossRef]
- Lyons, T.G. and G.Y. Ku, Systemic therapy for esophagogastric cancer: targeted therapies. Chin Clin Oncol, 2017. 6(5): p. 48. [CrossRef]
- Chong, C.R. and P.A. Jänne, The quest to overcome resistance to EGFR-targeted therapies in cancer. Nat Med, 2013. 19(11): p. 1389-400. [CrossRef]
- Ciardiello, F. and G. Tortora, EGFR Antagonists in Cancer Treatment. 2008. 358(11): p. 1160-1174. [CrossRef]
- Martinelli, E., et al., Anti-epidermal growth factor receptor monoclonal antibodies in cancer therapy. Clinical and experimental immunology, 2009. 158(1): p. 1-9. [CrossRef]
- Verma, H.K., et al., A Retrospective Look at Anti-EGFR Agents in Pancreatic Cancer Therapy. Curr Drug Metab, 2019. 20(12): p. 958-966. [CrossRef]
- Lv, Z.-C., J.-Y. Ning, and H.-B. Chen, Efficacy and toxicity of adding cetuximab to chemotherapy in the treatment of metastatic colorectal cancer: a meta-analysis from 12 randomized controlled trials. Tumour biology : the journal of the International Society for Oncodevelopmental Biology and Medicine, 2014. 35. [CrossRef]
- Sotelo, M.J., et al., Role of cetuximab in first-line treatment of metastatic colorectal cancer. World J Gastroenterol, 2014. 20(15): p. 4208-19. [CrossRef]
- Cunningham, D., et al., Cetuximab Monotherapy and Cetuximab plus Irinotecan in Irinotecan-Refractory Metastatic Colorectal Cancer. New England Journal of Medicine, 2004. 351(4): p. 337-345. [CrossRef]
- Huang, Z.H., et al., Cetuximab for esophageal cancer: an updated meta-analysis of randomized controlled trials. BMC Cancer, 2018. 18(1): p. 1170. [CrossRef]
- Xu, S., et al., Treatment outcome of nimotuzumab plus chemotherapy in advanced cancer patients: a single institute experience. Oncotarget, 2016. 7(22): p. 33391-407. [CrossRef]
- Han, X., et al. Nimotuzumab Combined with Chemotherapy is a Promising Treatment for Locally Advanced and Metastatic Esophageal Cancer. Medical science monitor : international medical journal of experimental and clinical research, 2017. 23, 412-418. [CrossRef]
- Zhao, K.-l., et al., A phase I dose escalation study of Nimotuzumab in combination with concurrent chemoradiation for patients with locally advanced squamous cell carcinoma of esophagus. Investigational New Drugs, 2012. 30(4): p. 1585-1590. [CrossRef]
- Bai, S.-X., et al., Clinical efficacy and safety of nimotuzumab plus chemotherapy in patients with advanced colorectal cancer: a retrospective analysis. The Journal of international medical research, 2020. 48(1): p. 300060519895858. [CrossRef]
- Yu, Y., et al., Nimotuzumab, an EGFR-targeted antibody, promotes radiosensitivity of recurrent esophageal squamous cell carcinoma. Int J Oncol, 2020. 56(4): p. 945-956. [CrossRef]
- Cui, G., et al., Galectin-3 knockdown increases gefitinib sensitivity to the inhibition of EGFR endocytosis in gefitinib-insensitive esophageal squamous cancer cells. Med Oncol, 2015. 32(4): p. 124. [CrossRef]
- Petty, R.D., et al., Gefitinib and EGFR Gene Copy Number Aberrations in Esophageal Cancer. J Clin Oncol, 2017. 35(20): p. 2279-2287. [CrossRef]
- Liu, W., et al., Galectin-3 regulates intracellular trafficking of EGFR through Alix and promotes keratinocyte migration. The Journal of investigative dermatology, 2012. 132(12): p. 2828-2837. [CrossRef]
- Xu, Y., et al., Gefitinib single drug in treatment of advanced esophageal cancer. J Cancer Res Ther, 2016. 12(Supplement): p. C295-c297. [CrossRef]
- Drenckhan, A., et al., Esophageal carcinoma cell line with high EGFR polysomy is responsive to gefitinib. Langenbeck's Archives of Surgery, 2014. 399(7): p. 879-888. [CrossRef]
- Huang, J., et al., Icotinib in Patients with Pretreated Advanced Esophageal Squamous Cell Carcinoma with EGFR Overexpression or EGFR Gene Amplification: A Single-Arm, Multicenter Phase 2 Study. Journal of Thoracic Oncology, 2016. 11(6): p. 910-917. [CrossRef]
- Sun, J., et al., Icotinib inhibits the proliferation of hepatocellular carcinoma cells in vitro and in vivo dependently on EGFR activation and PDL1 expression. Onco Targets Ther, 2018. 11: p. 8227-8237. [CrossRef]
- Wang, X., et al., Predictive value of EGFR overexpression and gene amplification on icotinib efficacy in patients with advanced esophageal squamous cell carcinoma. Oncotarget, 2016. 7(17): p. 24744-51. [CrossRef]
- Luo, H., et al., Icotinib With Concurrent Radiotherapy vs Radiotherapy Alone in Older Adults With Unresectable Esophageal Squamous Cell Carcinoma: A Phase II Randomized Clinical Trial. JAMA Netw Open, 2020. 3(10): p. 19440.
- Budi, H.S., et al., Human epidermal growth factor receptor 2 (HER2)-specific chimeric antigen receptor (CAR) for tumor immunotherapy; recent progress. Stem Cell Research & Therapy, 2022. 13(1): p. 40. [CrossRef]
- Won, E., Y.J. Janjigian, and D.H. Ilson, HER2 directed therapy for gastric/esophageal cancers. Curr Treat Options Oncol, 2014. 15(3): p. 395-404. [CrossRef]
- Swain, S.M., M. Shastry, and E. Hamilton, Targeting HER2-positive breast cancer: advances and future directions. Nature Reviews Drug Discovery, 2023. 22(2): p. 101-126. [CrossRef]
- Gerson, J.N., et al., Perspectives of HER2-targeting in gastric and esophageal cancer. Expert Opin Investig Drugs, 2017. 26(5): p. 531-540. [CrossRef]
- Swain, S.M., et al., Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med, 2015. 372(8): p. 724-34. [CrossRef]
- Won, E., Y. Janjigian, and D.J.C.T.O.i.O. Ilson, HER2 Directed Therapy for Gastric/Esophageal Cancers. 2014. 15(3): p. 395-404. [CrossRef]
- Bang, Y.J., et al., Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet, 2010. 376(9742): p. 687-97. [CrossRef]
- Tabernero, J., et al., Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol, 2018. 19(10): p. 1372-1384. [CrossRef]
- Mimura, K., et al., Lapatinib inhibits receptor phosphorylation and cell growth and enhances antibody-dependent cellular cytotoxicity of EGFR- and HER2-overexpressing esophageal cancer cell lines. Int J Cancer, 2011. 129(10): p. 2408-16. [CrossRef]
- Shiraishi, K., et al., Lapatinib acts on gastric cancer through both antiproliferative function and augmentation of trastuzumab-mediated antibody-dependent cellular cytotoxicity. Gastric cancer : official journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association, 2012. 16. [CrossRef]
- Guo, X.-f., et al., Lapatinib in combination with paclitaxel plays synergistic antitumor effects on esophageal squamous cancer. Cancer Chemotherapy and Pharmacology, 2018. 82(3): p. 383-394. [CrossRef]
- Hassan, M.S., et al., Combination effect of lapatinib with foretinib in HER2 and MET co-activated experimental esophageal adenocarcinoma. Sci Rep, 2019. 9(1): p. 019-54129.
- Chai, J., M.K. Jones, and A.S. Tarnawski, Serum response factor is a critical requirement for VEGF signaling in endothelial cells and VEGF-induced angiogenesis. Faseb j, 2004. 18(11): p. 1264-6. [CrossRef]
- Meng, L., et al., Survivin is critically involved in VEGFR2 signaling-mediated esophageal cancer cell survival. Biomed Pharmacother, 2018. 107: p. 139-145. [CrossRef]
- Whittaker, S., R. Marais, and A.X. Zhu, The role of signaling pathways in the development and treatment of hepatocellular carcinoma. Oncogene, 2010. 29(36): p. 4989-5005. [CrossRef]
- Cheung, A., W. Xu, and B. Li, The potential of targeted antiangiogenesis therapies in the treatment of esophageal cancer. Gastrointestinal Cancer: Targets and Therapy, 2015. 2015. [CrossRef]
- Khan, U. and M.A. Shah, Ramucirumab for the treatment of gastric or gastro-esophageal junction cancer. Expert Opin Biol Ther, 2019. 19(11): p. 1135-1141. [CrossRef]
- Spratlin, J.L., et al., Phase I pharmacologic and biologic study of ramucirumab (IMC-1121B), a fully human immunoglobulin G1 monoclonal antibody targeting the vascular endothelial growth factor receptor-2. J Clin Oncol, 2010. 28(5): p. 780-7.
- Wilke, H., et al., Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol, 2014. 15(11): p. 1224-35. [CrossRef]
- Konstorum, A. and J.S. Lowengrub, Activation of the HGF/c-Met axis in the tumor microenvironment: A multispecies model. Journal of theoretical biology, 2018. 439: p. 86-99. [CrossRef]
- Boromand, N., et al., Clinical and prognostic value of the C-Met/HGF signaling pathway in cervical cancer. J Cell Physiol, 2018. 233(6): p. 4490-4496. [CrossRef]
- Granito, A., E. Guidetti, and L. Gramantieri, c-MET receptor tyrosine kinase as a molecular target in advanced hepatocellular carcinoma. J Hepatocell Carcinoma, 2015. 2: p. 29-38. [CrossRef]
- Arnold, L., J. Enders, and S.M. Thomas, Activated HGF-c-Met Axis in Head and Neck Cancer. Cancers (Basel), 2017. 9(12). [CrossRef]
- Stanley, A., et al., Synergistic effects of various Her inhibitors in combination with IGF-1R, C-MET and Src targeting agents in breast cancer cell lines. Sci Rep, 2017. 7(1): p. 3964. [CrossRef]
- Lam, B.Q., L. Dai, and Z. Qin, The role of HGF/c-MET signaling pathway in lymphoma. J Hematol Oncol, 2016. 9(1): p. 135. [CrossRef]
- Krause, D.S. and R.A. Van Etten, Tyrosine kinases as targets for cancer therapy. N Engl J Med, 2005. 353(2): p. 172-87. [CrossRef]
- Yang, Y.M., et al., Advances in targeted therapy for esophageal cancer. Signal Transduct Target Ther, 2020. 5(1): p. 020-00323. [CrossRef]
- Van Der Steen, N., et al., Chapter 2 - Targeting the Hepatocyte Growth Factor Receptor to Overcome Resistance to Targeted Therapies, in Targeting Cell Survival Pathways to Enhance Response to Chemotherapy, D.E. Johnson, Editor 2019, Academic Press. p. 25-60.
- Shah, M., et al., METGastric: A phase III study of onartuzumab plus mFOLFOX6 in patients with metastatic HER2-negative (HER2-) and MET-positive (MET+) adenocarcinoma of the stomach or gastroesophageal junction (GEC). J Clin Oncol, 2015. 33. [CrossRef]
- Catenacci, D.V.T., et al., Rilotumumab plus epirubicin, cisplatin, and capecitabine as first-line therapy in advanced MET-positive gastric or gastro-oesophageal junction cancer (RILOMET-1): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol, 2017. 18(11): p. 1467-1482. [CrossRef]
- Pópulo, H., J.M. Lopes, and P. Soares, The mTOR signalling pathway in human cancer. International journal of molecular sciences, 2012. 13(2): p. 1886-1918. [CrossRef]
- Hirashima, K., et al., Phosphorylated mTOR Expression is Associated with Poor Prognosis for Patients with Esophageal Squamous Cell Carcinoma. Annals of Surgical Oncology, 2010. 17(9): p. 2486-2493. [CrossRef]
- Harrison, D.E., et al., Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature, 2009. 460(7253): p. 392-395. [CrossRef]
- Hasskarl, J., Everolimus. Recent Results Cancer Res, 2018. 211: p. 101-123.
- Huang, Z.-H., et al., Cetuximab for esophageal cancer: an updated meta-analysis of randomized controlled trials. BMC Cancer, 2018. 18. [CrossRef]
- Yang, X., et al., Radiotherapy combined with nimotuzumab for elderly esophageal cancer patients: A phase II clinical trial. Chinese journal of cancer research = Chung-kuo yen cheng yen chiu, 2021. 33(1): p. 53-60. [CrossRef]
- Guan, Y.-S., Q. He, and M. Li, Icotinib: Activity and clinical application in Chinese patients with lung cancer. Expert opinion on pharmacotherapy, 2014. 15. [CrossRef]
- Soularue, É., et al., Efficacy and safety of trastuzumab in combination with oxaliplatin and fluorouracil-based chemotherapy for patients with HER2-positive metastatic gastric and gastro-oesophageal junction adenocarcinoma patients: A retrospective study. Bulletin du cancer, 2015. 102. [CrossRef]
- Nolting, M., T. Schneider-Merck, and M. Trepel, Lapatinib. Recent Results Cancer Res, 2014. 201: p. 125-43.
- Kawai, S., et al., Retrospective observational study of salvage line ramucirumab monotherapy for patients with advanced gastric cancer. BMC Cancer, 2020. 20. [CrossRef]
- Han, H.S., et al., Ramucirumab plus paclitaxel as second-line treatment in patients with advanced gastric or gastroesophageal junction adenocarcinoma: a nationwide real-world outcomes in Korea study (KCSG-ST19-16). Ther Adv Med Oncol, 2021. 13: p. 17588359211042812. [CrossRef]
- Ling, Y., et al., Endostar, a novel recombinant human endostatin, exerts antiangiogenic effect via blocking VEGF-induced tyrosine phosphorylation of KDR/Flk-1 of endothelial cells. Biochem Biophys Res Commun, 2007. 361: p. 79-84. [CrossRef]
- Li, Y., et al., Efficacy and Safety of Endostar Combined with Chemotherapy in Patients with Advanced Solid Tumors. Asian Pacific journal of cancer prevention : APJCP, 2010. 11: p. 1119-23.
- Adnane, L., et al., Sorafenib (BAY 43-9006, Nexavar), a dual-action inhibitor that targets RAF/MEK/ERK pathway in tumor cells and tyrosine kinases VEGFR/PDGFR in tumor vasculature. Methods Enzymol, 2006. 407: p. 597-612.
- Janjigian, Y., et al., Phase II Trial of Sorafenib in Patients with Chemotherapy Refractory Metastatic Esophageal and Gastroesophageal (GE) Junction Cancer. PloS one, 2015. 10(8):e0134731. [CrossRef]
- Roviello, G., et al., Apatinib: A novel receptor tyrosine kinase inhibitor for the treatment of gastric cancer. Cancer Lett, 2016. 372(2): p. 187-91. [CrossRef]
- Hu, L., et al., Apatinib enhances the radiosensitivity of the esophageal cancer cell line KYSE-150 by inducing apoptosis and cell cycle redistribution. Oncol Lett, 2019. 17(2): p. 1609-1616. [CrossRef]
- Metibemu, D.S., et al., Exploring receptor tyrosine kinases-inhibitors in Cancer treatments. Egyptian Journal of Medical Human Genetics, 2019. 20(1): p. 35. [CrossRef]
- Huang, J., et al., Anlotinib for previously treated advanced or metastatic esophageal squamous cell carcinoma: A double-blind randomized phase 2 trial. Cancer medicine, 2021. 10. [CrossRef]
- Shen, G., et al., Anlotinib: a novel multi-targeting tyrosine kinase inhibitor in clinical development. Journal of Hematology & Oncology, 2018. 11(1): p. 120. [CrossRef]
- Paplomata, E., A. Zelnak, and R. O'Regan, Everolimus: side effect profile and management of toxicities in breast cancer. Breast Cancer Res Treat, 2013. 140(3): p. 453-62. [CrossRef]
- Xie, J., X. Wang, and C.G. Proud, mTOR inhibitors in cancer therapy. F1000Research, 2016. 5: p. F1000 Faculty Rev-2078. [CrossRef]
- Meacham, C.E. and S.J. Morrison, Tumour heterogeneity and cancer cell plasticity. Nature, 2013. 501(7467): p. 328-337. [CrossRef]
- Dinh, H.Q., et al., Integrated single-cell transcriptome analysis reveals heterogeneity of esophageal squamous cell carcinoma microenvironment. Nature Communications, 2021. 12(1): p. 7335. [CrossRef]
- Alfarouk, K.O., et al., Resistance to cancer chemotherapy: failure in drug response from ADME to P-gp. Cancer Cell International, 2015. 15(1): p. 71. [CrossRef]
- Luan, S., et al., Advances in Drug Resistance of Esophageal Cancer: From the Perspective of Tumor Microenvironment. 2021. 9(623). [CrossRef]
- Yang, W., et al., Molecular mechanisms and clinical implications of miRNAs in drug resistance of esophageal cancer. Expert Rev Gastroenterol Hepatol, 2017. 11(12): p. 1151-1163. [CrossRef]
- Hanahan, D. and R.A. Weinberg, Hallmarks of cancer: the next generation. Cell, 2011. 144(5): p. 646-74. [CrossRef]
- Adhikari, S., et al., The paradigm of drug resistance in cancer: an epigenetic perspective. Biosci Rep, 2022. 42(4). [CrossRef]
- Yu, Z., et al., Cancer stem cells. The International Journal of Biochemistry & Cell Biology, 2012. 44(12): p. 2144-2151.
- Walcher, L., et al., Cancer Stem Cells—Origins and Biomarkers: Perspectives for Targeted Personalized Therapies. 2020. 11(1280). 1280. [CrossRef]
- Batlle, E. and H. Clevers, Cancer stem cells revisited. Nat Med, 2017. 23(10): p. 1124-1134. [CrossRef]
- Zhao, J., Cancer stem cells and chemoresistance: The smartest survives the raid. Pharmacol Ther, 2016. 160: p. 145-58. [CrossRef]
- Luan, S., et al., Advances in Drug Resistance of Esophageal Cancer: From the Perspective of Tumor Microenvironment. Frontiers in Cell and Developmental Biology, 2021. 9. [CrossRef]
- Li, H., et al., The PTEN/PI3K/Akt pathway regulates stem-like cells in primary esophageal carcinoma cells. Cancer biology & therapy, 2011. 11(11): p. 950-958. [CrossRef]
- Tong, D., et al., p75 neurotrophin receptor: A potential surface marker of tongue squamous cell carcinoma stem cells. Molecular medicine reports, 2017. 15(5): p. 2521-2529. [CrossRef]
- Galluzzi, L., et al., Molecular mechanisms of cisplatin resistance. Oncogene, 2012. 31(15): p. 1869-1883. [CrossRef]
- Sahai, E., et al., A framework for advancing our understanding of cancer-associated fibroblasts. Nature Reviews Cancer, 2020. 20(3): p. 174-186. [CrossRef]
- Hanahan, D. and Robert A. Weinberg, Hallmarks of Cancer: The Next Generation. Cell, 2011. 144(5): p. 646-674. [CrossRef]
- Kalluri, R., The biology and function of fibroblasts in cancer. Nat Rev Cancer, 2016. 16(9): p. 582-98. [CrossRef]
- Tong, Y., et al., Tumor-Secreted Exosomal lncRNA POU3F3 Promotes Cisplatin Resistance in ESCC by Inducing Fibroblast Differentiation into CAFs. Molecular therapy oncolytics, 2020. 18: p. 1-13. [CrossRef]
- Tanaka, K., et al., miR-27 is associated with chemoresistance in esophageal cancer through transformation of normal fibroblasts to cancer-associated fibroblasts. Carcinogenesis, 2015. 36(8): p. 894-903. [CrossRef]
- Qiao, Y., et al., IL6 derived from cancer-associated fibroblasts promotes chemoresistance via CXCR7 in esophageal squamous cell carcinoma. Oncogene, 2018. 37(7): p. 873-883. [CrossRef]
- Verma, H.K., G. Falco, and L.V.K.S. Bhaskar, Molecular Signaling Pathways Involved in Gastric Cancer Chemoresistance, in Theranostics Approaches to Gastric and Colon Cancer, G.S.R. Raju and L.V.K.S. Bhaskar, Editors. 2020, Springer Singapore: Singapore. p. 117-134. [CrossRef]
- Juneja, V.R., et al., PD-L1 on tumor cells is sufficient for immune evasion in immunogenic tumors and inhibits CD8 T cell cytotoxicity. J Exp Med, 2017. 214(4): p. 895-904. [CrossRef]
- Zhao, J. and J. Huang, Breast cancer immunology and immunotherapy: targeting the programmed cell death protein-1/programmed cell death protein ligand-1. Chin Med J (Engl), 2020. 133(7): p. 853-862.
- Huang, T.-X. and L. Fu, The immune landscape of esophageal cancer. Cancer communications (London, England), 2019. 39(1): p. 79-79. [CrossRef]
- Hong, Y. and Z.-Y.J.F.i.p. Ding, PD-1 inhibitors in the advanced esophageal cancer. 2019. 10: p. 1418. [CrossRef]
- Dhupar, R., et al., Targeting Immune Checkpoints in Esophageal Cancer: A High Mutational Load Tumor. Ann Thorac Surg, 2017. 103(4): p. 1340-1349. [CrossRef]
- Yagi, T., et al., Tumour-associated macrophages are associated with poor prognosis and programmed death ligand 1 expression in oesophageal cancer. Eur J Cancer, 2019. 111: p. 38-49. [CrossRef]
- Däster, S., et al., Low expression of programmed death 1 (PD-1), PD-1 Ligand 1 (PD-L1), and Low CD8+ T Lymphocyte infiltration identify a subgroup of patients with gastric and esophageal adenocarcinoma with severe prognosis. 2020. 7: p. 144. [CrossRef]
- Bielenberg, D.R. and B.R.J.C.J. Zetter, The contribution of angiogenesis to the process of metastasis. 2015. 21(4): p. 267. [CrossRef]
- Nisar, S., et al., Exploring dysregulated signaling pathways in cancer. 2020. 26(4): p. 429-445. [CrossRef]
- Leu, C.-M., et al., Interleukin-6 acts as an antiapoptotic factor in human esophageal carcinoma cells through the activation of both STAT3 and mitogen-activated protein kinase pathways. 2003. 22(49): p. 7809-7818. [CrossRef]
- Ebbing, E.A., et al., Stromal-derived interleukin 6 drives epithelial-to-mesenchymal transition and therapy resistance in esophageal adenocarcinoma. Proc Natl Acad Sci U S A, 2019. 116(6): p. 2237-2242. [CrossRef]
- Sugimura, K., et al., Let-7 expression is a significant determinant of response to chemotherapy through the regulation of IL-6/STAT3 pathway in esophageal squamous cell carcinoma. Clin Cancer Res, 2012. 18(18): p. 5144-53.
- Hatata, T., et al., Immunohistochemical study of nuclear factor-κB expression in esophageal squamous cell carcinoma: prognostic significance and sensitivity to treatment with 5-FU. 2012. 25(8): p. 716-722.
- Chen, S., et al., IL-1RA suppresses esophageal cancer cell growth by blocking IL-1α. 2019. 33(6): p. e22903.
- Muz, B., et al., The role of hypoxia in cancer progression, angiogenesis, metastasis, and resistance to therapy. Hypoxia (Auckland, N.Z.), 2015. 3: p. 83-92. [CrossRef]
- Brown, A., S. Kumar, and P.B. Tchounwou, Cisplatin-Based Chemotherapy of Human Cancers. J Cancer Sci Ther, 2019. 11(4).
- Kimura, S., et al., Expression of hypoxia-inducible factor (HIF)-1alpha is associated with vascular endothelial growth factor expression and tumour angiogenesis in human oesophageal squamous cell carcinoma. Eur J Cancer, 2004. 40(12): p. 1904-12. [CrossRef]
- Zhu, Z.J., et al., Hypoxia induces chemoresistance of esophageal cancer cells to cisplatin through regulating the lncRNA-EMS/miR-758-3p/WTAP axis. Aging (Albany NY), 2021. 13(13): p. 17155-17176.
- Li, B., et al., Id1-induced IGF-II and its autocrine/endocrine promotion of esophageal cancer progression and chemoresistance--implications for IGF-II and IGF-IR-targeted therapy. Clin Cancer Res, 2014. 20(10): p. 2651-62.
- Chan, D., et al., Expression of Insulin-Like Growth Factor Binding Protein-5 (IGFBP5) Reverses Cisplatin-Resistance in Esophageal Carcinoma. Cells, 2018. 7(10). [CrossRef]
- Zhang, Y., et al., Resistance to cetuximab in EGFR-overexpressing esophageal squamous cell carcinoma xenografts due to FGFR2 amplification and overexpression. J Pharmacol Sci, 2014. 126(1): p. 77-83. [CrossRef]
- Saito, S., et al., The role of HGF/MET and FGF/FGFR in fibroblast-derived growth stimulation and lapatinib-resistance of esophageal squamous cell carcinoma. 2015. 15(1): p. 1-12. [CrossRef]
Figure 1.
Schematic representation of medications targets the pathway and prevents downstream signaling.
Figure 1.
Schematic representation of medications targets the pathway and prevents downstream signaling.
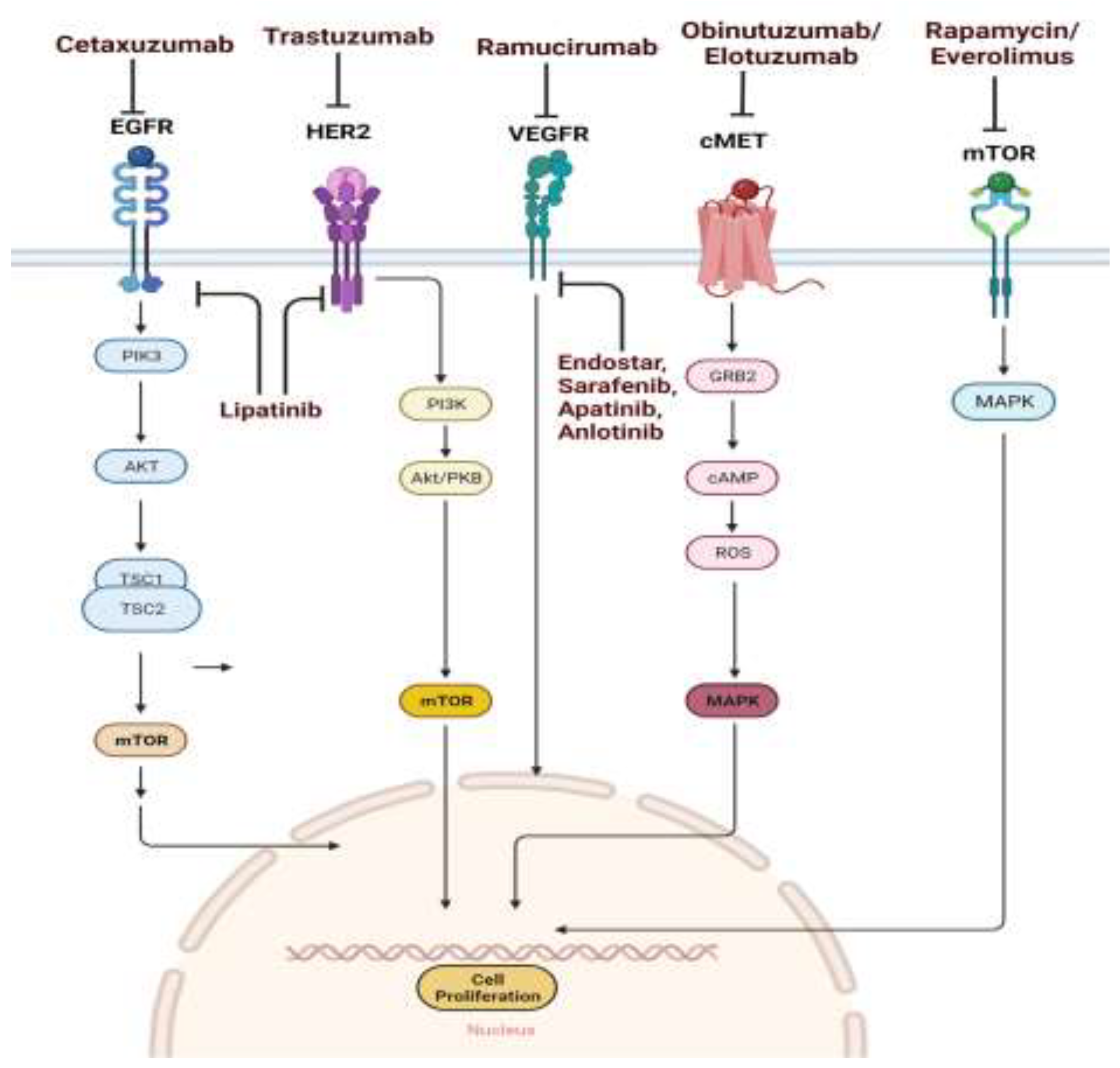

Table 1.
Summary of Drugs Targeting Pathways in Esophageal Cancer: Mode of Action, Findings, and Side Effects.
Table 1.
Summary of Drugs Targeting Pathways in Esophageal Cancer: Mode of Action, Findings, and Side Effects.
| Drugs Name | Targeting Pathway | Mode of Action | Findings | Side Effects | Reference | |
|---|---|---|---|---|---|---|
| Cetuximab | EGFR | Anti EGFR monoclonal antibody | Effective in combination with chemotherapy, Increase survival rate in resectable ESCC patient | Hypomagnesamia | [31,80] | |
| Nimotazumab | EGFR | Anti EGFR monoclonal antibody | Nimotazumab + radiotherapy= used in phage I clinical trial,Stop G2 phasr of ESCC cell cycle | esophagitis, pneumonitis, leukopenia, gastrointestinal reaction, thrombocytopenia, radiothermitis and fever | [36,81] | |
| Gefinitib | EGFR | Anti EGFR-RTK inhibitor | Gefinitib + 5-FU= increase survival rate of advance ESCC patient | Dry skin, Itching, rash, acne, mouth sores, and weakness,diarrhoea skin toxicity,fatigue | [40] | |
| Icotinib | EGFR | Anti EGFR-RTK inhibitor | Rash and diarrhea | [42,82] | ||
| Transtuzumab | HER2 | Monoclonal anti HER2 antibody | used in combination with cisplatin + fluopyrimidine (either capecitabine or 5-fluorouracil) for patient with HER2-positive metastatic gastric or GE adenocarcinoma | Fever and chills, cough,and.headache | [47,83] | |
| Lapatinib | Dual RTK inhibitor. Bind to ATP binding site and inhibit kinase activity | Lapatinib + paclitaxel = supress cell prlifetation and decrease ESCC cell migration,invasion | Face redness, dizziness, headache, shortness of breath, and anxiety | [56,84] | ||
| Ramucirumab | VEGF | Monoclonal antibody,block binding of VEGF to VEGFR | Ramucirumab + paclitaxel = used in 2nd line treatment of advanced GEJ adenocarcinoma | Hypertension, thromboembolism, rash, diarrhoea, and myelosuppression | [85,86] | |
| Endastar | VEGF | Supress the signaling of VEGFR and inhibit endothelial growth and migration | Endostar in combination with chemotherapy decline tumour weight | Nausea, vomiting, fever etc. | [87,88] | |
| sarofenib | VEGF | Inhibit VEGFR2 | Reduce development of EAC and GEJ in phase II clinical trial | fatigue, weakness, redness of the skin, hair loss, itching, dry or peeling skin, and a lack of appetite etc. | [89,90] | |
| Apatinib | VEGF | Inhibit RTK-VEGFR2 receptor | Having anti esohageal cancer effect | Diarrhea ,nausea, vomiting, dry skin etc | [91,92] | |
| Anlotinib | VEGF | Inhibit RTK-VEGFR2/3 receptor | Increase disease controle rate in pretreated advanced ESCC patients | thrombocytopenia and neutropenia,hypercholesterolemia, dermal toxicity hypertriglyceridemia | [93,94,95] | |
| Rilotumumab | HGF-c-MET | Inhibit interaction of HGF with c-MET | rilotumumab cant not effectively treat the pateients | Nausea, vomiting, fever etc. | [75] | |
| Obinautuzumab | HGF-c-MET | Block MET from binding to HGF | Obinutuzumab can not improve the patient survival rate | decrease in the number of WBC and platelets cause nfection and bleeding. Fever; Tiredness and weakness, headache; Hair loss | [22] | |
| Rapamysin and Everolimuzs | m-TOR | Inhibit m-TOR | Decrease cell proliferation and grwth | Stomatitis, rash, tiredness, hyperglycemia, hyperlipidemia,ect.. | [96,97] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



