
Submitted:
23 June 2023
Posted:
25 June 2023
You are already at the latest version
Abstract
Objective: The purpose of this study was to evaluate the surface texture and biofilm adhesion of veneered or CAD/CAM milled zirconia (partially stabilized with yttrium) after professional oral hygiene procedures.
Samples (4x4 mm, thickness 2 mm; n = 72) were separated from zirconia blanks (3Y-TZP-LA). One group was veenired with ceramics and the other group of samples was CAD/CAM milled. Each group had 2 subgroups: polished and glazed. The samples were subjected to simulated strokes of professional brushing using abrasive paste and ultrasonic scaling. Parameters of surface micromorphology and receptivity to biofilm were calculated before and after simulating the given methods of professional maintenance of oral hygiene. The characteristics of zirconia surface were evaluated by scanning electron microscopy (SEM). Microbial bacterial/fungal species (Staphylococcus aureus, Streptococcus sanguinis and Candida albicans) were used and cultured on the respective sterilized zirconia surfaces. The amount of biofilm formation on zirconia surface was quantified by colony forming unit (CFU) counts.
Results: SEM analysis showed the greatest change in surface microtopography after the use of ultrasonic scaling, in glazed zirconia samples. Less formation of colonies on the surface CAD/CAM milled zirconia restorations was observed.
Conclusion: Routine methods of professional maintenance of oral hygiene can damage the surface of glazed zirconia restorations.
Keywords:
Zirconia
; CAD/CAM
; ultrasonic scaling
; SEM
; surface micro topography
; microbial biofilm
Introduction
In recent decades, we have witnessed the intensive development of dental ceramic materials, especially in meeting the high aesthetic requirements of modern dentistry. In particular, zirconia stands out as a biomaterial of great interest.
Due to good mechanical properties (high hardness, strength, high wear resistance, corrosion resistance, modulus of elasticity similar to steel and increased fracture toughness) and aesthetic properties [1] this restorative material is widely used in prosthetic dentistry [2,3,4].
As dental ceramics develops, so do the methods of its technical production. Significant progress was made with the introduction of the CAD/CAM system, which describes the virtual design and the production of dental restorations using machine units [5].
In order to improve the mechanical properties tetragonal zirconium polycrystals (TZP) are strengthened by the use of certain elements such as yttrium (zirconium stabilized by yttrium ie YTZP). This form of material can be applied to high-strength single crown frames, bridges and implants using CAD/CAM techniques [6].
Zirconia partially stabilized by yttrium (YTZP) contains a highly crystalline phase and low translucency, which confers opacity [7]. To exclude the white opaque color of zirconia, transparent porcelain can be used to veneer the restorations. On the other hand, chipping of veneering porcelain has been reported as a major problem [8]. To overcome this clinical limitation, monolithic zirconia, in an anatomical form without veneers, is used.
Monolithic zirconia has adequate translucency and excellent mechanical properties, without failures due to chipping of the veneering ceramic [9]. Restorations made of this type of zirconia require decreasing clinical time and restoration costs.
Dental plaque causes an inflammatory reaction, which is associated with periodontal and peri-implant disease, with possible progressive bone loss around the tooth, but also around the implant. Early bacterial colonization is a condition and initial step in biofilm formation, leading to infection [10]. Studys reported high prevalence C. albicans and S. aureus rates for in saliva samples from elderly adults and hospitalized patients [11].
The clinical investigations showed that presence of C. albicans in peri-implantitis gingival zone was revealed [12]. C. albicans is associated with diseases such as peri-implantitis and periodontitis. This opportunistic pathogen is usually the cause of denture-associated stomatitis.
The oral streptococci are members of the indigenous microbiota mainly in the supragingival environment. S. sanguinis is commonly found in healthy periodontal individuals abesides it can contribute to the coaggregation of pathogenic bacteria, such as Porphyromonas gingivalis [13].
Bacterial adhesion to a substrate and initial biofilm formation is related to surface properties: roughness, hydrophobicity and interaction between existing microorganisms [14]. Streptococcus is one of the first colonizers of initial supragingival biofilm. Also, this microorganism is present in greater quantity in the first hours of oral biofilm formation. Microoganisms present in the oral cavity naturally tend to adhere to dental materials. Certain parts of the restorations are particularly susceptible to plaque accumulation because there is poor mechanical cleaning. These are the following surfaces: interface between tooth and restoration [15], the cervical third of the proximal surface, and along the gingival margin. This is a particularly sensitive topic, bearing in mind that zirconia is also used to make implant supported prosthetic restorations, where the implant, gingiva and zirconia are in contact [16].
In order to maintain patients’ oral hygiene, dentists use various manual (curettes) and machine instruments (ultrasonic scaling, brushes and pastes). The question arises whether these routine and recommended oral hygiene maintenance procedures damage the surface of zirconia restorations and increase surface roughness, thereby creating better conditions for the adhesion of microorganisms and thus the biofilm formation of [17,18,19].
The restoration surface roughness is extremely important because of the increased accumulation of plaque which affects the optical properties of the restoration and the wear of the opposing dentition [20].
On solid surfaces, the ability of microorganisms to aggregate and the environment are important factors in the formation of oral biofilm. It is certain that the finishing technique on ceramics significantly affects the surface properties of these materials and the formation of oral biofilm.
Accordingly, the aim of this study is to determine whether routine dental procedures, such as brushing and ultrasonic scaling, affect the surface microtopography and biofilm adhesion of veenired and CAD/CAM milled zirconia prosthetic restorations. Each group of zirconia samples had 2 subgroups: polished and glazed.
The surface microtopography and in vitro biofilm formation on zirconia samples surfaces will be analyzed before and after the oral hygiene maintenance treatmen.
The null hypothesis of this study was that different methods of professional oral hygiene (brushing and ultrasonic scaling) would not affect surface microtopography and biofilm adhesion on the tested zirconia samples.
Materials and methods
Sample preparation
The zirconia samples (n = 72) dimensions 4x4 mm and 2 mm thickness, were milled from the pre-sintered zirconia blanks (DD Bio ZX² color—High Translucent (3Y-TZP-LA, Dental Direkt, Dental Direkt GmbH, Germany) (Figure 1) by using a 5-Axis milling machine (K5, Vhf camfacture, Ammerbuch, Germany). Used burs in the CNC machine (Vhf camfacture, Ammerbuch, Germany), burs type: z200-r3d-40 (milling thickness 2 mm) and z100-r2d-40 (milling thickness 1 mm). Milling speed RPM 22000-25000 revolutions per minute. Then the samples were sintered at 1,450 °C for 2 h.
The first group of zirconia samples was veneered with IPS e. max Ceram ceramic (Ivoclar Vivadent, Schaan, Licheinstain), applied in layers. The sintering process was carried out in Programat P500 (Ivoclar Vivadent, Schaan, Licheinstain). This group of samples was divided into two subgroups:
Glazed (F1)—the samples were glazed with IPS e.max Ceram Glaze Powder (Ivoclar Vivadent, Schaan, Licheinstain).
Polished (F2)—the samples were polished with polishing rubber (Edenta AG, Switzerland). The order of rubber use is from the coarsest blue, the medium pink and the finest yellow.
The second group, after the CAD/CAM milling process, was divided into two subgroups:
Glassed (C1)—the samples were glazed with IPS e.max Ceram Glaze Powder (Ivoclar Vivadent, Schaan, Licheinstain).
Polished (C2)—the samples were polished with polishing rubber (Edenta AG, Switzerland). The order of rubber use is from the coarsest blue, the medium pink and the finest yellow.
Samples of both groups: zirconia veneered and zirconia milled were divided into 3 subgroups:
- 0-
- no treatment (control samples),
- 1-
- exposed to brushing (with a professional dental cleaning brush and abrasive paste, Super Polish, Kerr),
- 2-
- exposed to ultrasonic scaling (with a ultrasonic scaler incorporated in a dental unit).
Surface characteristics of zirconia surface
Scanning electron microscopy (SEM)
A scanning electron microscope (Scanning Electron Microscope, Model JSM-6390, JEOL, USA, Inc.) was used to observe the surface morphology of different zirconia group samples. The samples were gold sputtered and the analyzing procedures were carried out at 150× magnification.
Biofilm formation assay
Microbial biofilms of each bacterial/fungal species were formed on the surfaces on different zirconia samples. The following strains were used: Staphylococcus aureus ATCC 11632, Streptococcus sanguinis ATTC 10556 and Candida albicans ATCC 10231. Each strain was formed on 16 samples (4 control—untreated material (F1, F2, C1, C2) and 12 samples treated with ultrasonic scaling (treatment 60s) and brush (treatment 60s) (F1a/b; F2a/b; C1a/b; C2a/b). Following procedure [22], with some modification, the sample (dimensions 4x4x2mm) were placed in 200 μL of medium at 37 °C for 24 h. For S. aureus and S. sanguinis biofilm formation, Triptic soya broth with 2% glucose (Torlak, Belgrade, Serbia) was used and for the C. albicans biofilm Yeast extract Pepton Dextrose (YPD) medium (HiMedia, India).
Since only one surface of the samples was treated with ultrasonic scaling and brushing, after incubation, the biofilm was removed mechanically with alcohol from all other surfaces. Then, the samples were washed with sterile PBS and placed in sterile plastic tubes containing 500 μL sterile PBS. Each tube was treated in an ultrasonic bath (40kHz for 10min), in order to remove the biofilm from the desired surface. The dilutions were seeded on Plate Counting Agar (PCA) (Neogen, UK) and incubated at 37 °C for 24 h. After 24 h the colonies were counted on Microprocessor colony counter (Supertek) and the results were presented as Colony-Forming Units (CFU)/plate [23].
Statistical analysis
Data were analysed and graphically presented by means of the program Microsoft (Excel Spreadsheet, Software Microsoft 365). The average values and the standard deviations were calculated for colony-forming units (CFU).
Results
SEM imaging
Figure 2 and Figure 3 show the morphological appearance of the zirconia samples surface before and after routine methods for professional maintenance of oral hygiene.
Veneered and polished zirconia samples (F1) had a slightly irregular surface, with microcracks and visible particles on the surface. Barely visible horizontal lines may indicate the direction of polishing. However, veneered and polished zirconia after ultrasonic scaling (F1a) showed an uneven surface with pores and grooves of various sizes, cavities and chipping-type defects. On the venneered zirconia samples, treated with brushing (F1b), small surface defects and groovelike formations were evident. On the contrary, venneered zirconia glazed samples (F2), showed a relatively regular surface texture with whitish particles, without voids. The veneered and glazed samples, treated with ultrasonic scaling (F2a) showed the most surface irregularities in the form of large defects. The layered breaking of the material was evident. On the side of the defects, remained a porous surface. On the surface of veneered and glazed samples after brushing (F2b), there were visible protrusions and traces of the brushing. The entire surface was undulating with round-topped particules (Figure 2).
F1—zirconia veneered and polished samples; F1a—zirconia veneered and polished samples treated with ultrasonic scaling; F1b—zirconia veneered, polished and brushed samples; F2—zirconia veneered and glazed samples; F2a—zirconia veneered and glazed samples treated with ultrasonic scaling; F2b—zirconia veneered, glazed and brushed samples.
SEM examination of the CAD/CAM milled and polished zirconia samples (C2) revealed an eroded surface that was created by the sample making manufacturing technique. These changes are in the form of two types of traces, one coarser and the other finer. CAD/CAM milled and polished zirconia samples treated with ultrasonic scaling (C2a), showed a rough surface in the form of parallel scratches. Visible irregularities were those created by the effect of ultrasonic scaling- rougher and others created by the effect of milling–mild. As for the CAD/CAM milled and polished zirconia samples after brushing (C2b), there were slight traces, which were probably the result of the action of the brush. In the case of CAD/CAM milled and glazed zirconia samples (C1), a slightly smoother surface layer with pale dimples and poured glaze drops can be described. On the surface of CAD/CAM milled and glazed zirconia after ultrasonic scaling (C1a), extreme irregularities in the form of scratches and defects are visible. In the case of CAD/CAM milled and glazed zirconia after brushing (C1b), a porous surface with black and white holes was observed. The black holes have an uneven bottom and are not covered with glaze, only their edges are glazed. Probably the tip of the bristles of the brush broke off parts of the glaze.
C2—zirconia milled and polished samples; C2a—zirconia milled and polished samples treated with ultrasonic scaling; C2b—zirconia milled, polished and brushed samples; C1—zirconia milled and glazed samples; C1a—zirconia milled and glazed samples treated with ultrasonic scaling; C1b—zirconia milled, glazed and brushed samples.
Biofilm formation on different zirconia samples
This study determined potential of S. aureus, S. sanguinis and C. albicans to form biofilm on different zirconia samples. The results of microbial biofilm formed on the control and test samples were presented in Figure 4, Figure 5 and Figure 6. In case of S. aureus biofilm, zirconia veneered and polished samples (F1, control) were the ones with the lowest obtained CFUs. Compared S. aureus biofilm formation between zirconia veneered and zirconia milled samples, showed that CFUs of S. aureus were higher on the veneered samples (Figure 4). Among veneered samples, on the glazed ones treated with brush and abrasive paste (F2b), the lowest number of S. aureus colonies was detected. While, among zirconia milled samples, the glazed ones treated with ultrasonic scaling (C1a) had the lowest CFUs.
F1—zirconia veneered and polished samples; F1a—zirconia veneered, polished samples treated with ultrasonic scaling; F1b—zirconia veneered, polished and brushed samples; F2—zirconia veneered and glazed samples; F2a—zirconia veneered and glazed samples treated with ultrasonic scaling; F2b—zirconia veneered, glazed and brushed samples; C2—zirconia milled and polished samples; C2a—zirconia milled and polished samples treated with ultrasonic scaling; C2b—zirconia milled, polished and brushed samples; C1—zirconia milled and glazed samples; C1a—zirconia milled and glazed samples treated with ultrasonic scaling; C1b—zirconia milled, glazed and brushed samples.
In the most of veneered zirconia samples S. sanguinis was detected in the lowest number (Figure 5). The exception among the veneered zirconia samples were polished samples, treated with ultrasonic scaling (F1a) and glazed and brushed samples (F2b). While, among zirconia milled samples the polished ones and treated with brush (C2b) had the lowest CFUs.
F1—zirconia veneered and polished samples; F1a—zirconia veneered and polished samples treated with ultrasonic scaling; F1b—zirconia veneered, polished and brushed samples; F2—zirconia veneered and glazed samples; F2a—zirconia veneered and glazed samples treated with ultrasonic scaling; F2b—zirconia veneered, glazed and brushed samples; C2—zirconia milled and polished samples; C2a—zirconia milled and polished samples treated with ultrasonic scaling; C2b—zirconia milled, polished and brushed samples; C1—zirconia milled and glazed samples; C1a—zirconia milled and glazed samples treated with ultrasonic scaling; C1b—zirconia milled, glazed and brushed samples.
Regarding C. albicans biofilm, veneered samples showed the higher CFUs then milled ones (Figure 6). Among veneered zirconia samples, the lowest number of C. albicans colonies were detected on the polished zirconia samples treated with ultrasonic scaling (F1a). While, among zirconia milled samples the polished ones treated with ultrasonic scaling (C2a) had the lowest CFUs.
F1—zirconia veneered and polished samples; F1a—zirconia veneered and polished samples treated with ultrasonic scaling; F1b—zirconia veneered, polished and brushed samples; F2—zirconia veneered and glazed samples; F2a—zirconia veneered and glazed samples treated with ultrasonic scaling; F2b—zirconia veneered, glazed and brushed samples; C2—zirconia milled and polished samples; C2a—zirconia milled and polished samples treated with ultrasonic scaling; C2b—zirconia milled, polished and brushed samples; C1—zirconia milled and glazed samples; C1a—zirconia milled and glazed samples treated with ultrasonic scaling; C1b—zirconia milled, glazed and brushed samples.
Overall, the amount of formed biofilm depends on the type of samples, surface properties and different sample treatment (ultrasonic scaling/brushing). Also, based on the data obtained by counting colonies, it can be concluded that the density of biofilm on different samples also depends on the biofilm-forming species of bacteria/fungi.
Discussion
This in vitro study investigated the effects of professional oral hygiene treatments on surface microtopography and microbial biofilm adhesion on zirconia obtained by different techniques (CAD/CAM milled and veenered). Both forms of zirconia had a surface treated differently: glazed and polished.
Based on the results of this study, the null hypothesis was rejected because the microtopography of the samples surface and biofilm formation were different, depending on the oral hygiene maintenance treatment.
In this research, ultrasonic scaling and brushing were performed to simulate professional plaque control. These methods are part of supportive therapy after prosthetic treatment. There is a recommendation that they, including control of oral hygiene, be carried out at least once every 6 months after prosthetic and periodontal treatment [24]. According to previously reported data [21], the time required for the treatment of one tooth with an ultrasonic scaling scaler during periodontal therapy is ranged from 0.35 to 3.90 min. Based on these findings, ultrasonic scaling was performed for 1 min and repeated 10 times, imitating the procedure carried out over 5 years.
The microtopography properties of the tested zirconia samples were qualitatively evaluated by SEM. Observation with a SEM microscope was performed at a 150x magnification. This magnification allowed us to see comprehensive changes on the surface of the tested samples. Other researches performed the analysis at a higher magnification [25,26,27]. In this case, higher magnification, wouldn’t show the changes on the surface caused by applied ultrasonic scaling and brushing techniques, described in this experiment, on such an obvious and striking way.
In this study, the biggest damage to the surface was caused by the ultrasonic scaling treatment, especially on the glazed surface of zirconia samples, which can be explained by the glassy structure of the glaze, which is literally broken by gentle vibration using ultrasound.
Some studies reported a significant increase in surface roughness after scaling [24,28], while others did not [27]. This discrepancy could be attributed to the unequal duration of scaling in previous studies and to the differently treated surface and type of ceramics.
Disruption of the surface topography by brushing has been reported in other studies [26,29,30], but in this study it is particularly pronounced in glazed zirconia samples. Damage caused by brushing was less but not insignificant, especially when we know that the microtopography of the surface of ceramic restorations is related to the formation of biofilm [31,32].
Biofilm has several stages in its formation. It represents dense micro-communities, which have the ability to adapt to changes in the environment by changing their gene expression patterns. The formation and composition of the biofilm is influenced by the method of adhesion to the surface. Each microorganism has its own unique method (binding using flagella, saws, proteins or polysaccharides). The initial phase of attachment of microorganisms is the key phase for the formation of a biofilm, and this process can further go in two directions: the microorganisms can continue to stick to the surface and to each other, or they can return to their free form (planktonic). It can be said that microorganisms have created a unique way to survive by forming a biofilm [33].
It has been proven that biofilm is formed on all surfaces in the oral cavity, both natural tissues and artificial materials. It is the microorganisms from the biofilm with their products that affect the inflammatory processes in the mouth and the durability of dental restorations. Scanning electron microscopy (SEM) showed a significant difference in the formation of biofilm on different materials and tooth enamel, and this is related to the roughness of the surface of the examined materials [34].
Biofilm adhesion is influenced by several factors. Most often these are the surface characteristics of the material, such as: surface microtopography and roughness, surface free energy, chemical characteristics [35].
Bacterial adhesion on the surface of 3Y-TZP subjected to ultrasonic scaling and brushing was evaluated using S. aureus, S. sanguinis and C. albicans, which are known as initial colonizers among the microorganisms who compose dental plaque [36]. Therefore, these three representative microorganisms were chosen in this study.
Results of studies showed that glazed surfaces of monolithic zirconia samples have a greater roughness and tend to accumulate more biofilm [37].
S. aureus showed the highest adhesion on veneered and polished zirconia samples after ultraconic scaling. While S. sanguis mostly adhered to zirconia surfaces after ultrasonic scaling. It is obvious that the defects created after the action of ultrasonic scaling favor the retention of microorganisms.
When microorganisms were compared to each other, a greater growth of Streptococcus was observed independent of the surface type. Also, a greater formation of colonies on glazed surfaces were observed in comparison to polished surfaces, corroborating a previous study [37].
C. albicans adhered more to the vennered zirconia samples, but there was no difference in fungal adhesion between the groups of polished and glazed samples, which is confirmed by the results [38] and [25].
Surface texture and microtopography play an important role in microbial adhesion. Certain studies have shown that many micrometer- and nanometer-scale topographic patterns (created by processing techniques or otherwise) of various shapes and sizes inhibit biofilm formation compared to flat surfaces of the same material [39]. In this study, however, the highest bacterial adhesion is on the surface of the zirconia samples with the most drastic defects after ultrasonic scaling, which can be explained by the depth and rough edges of the defects that retain microorganisms.
One of the most important factors in the formation of oral biofilm is surface roughness, which is correlated with bacterial adhesion. Surface finishing protocols like grinding directions, pressure, water coolants, in one hand and treatment during routine maintenance of oral hygiene, in the other hand, can affect the roughness of the surface of zirconia prosthetic restorations [40].
In the treatment of periodontal disease, patients are offered modern surgical procedures, after which it is recommended to make prosthetic ceramic restorations in order to maintain the achieved therapeutic results. Furthermore, patients are scheduled for regular hygiene procedures that include the use of ultrasound, brushes and abrasive paste. This experiment has shown that these routine hygiene procedures should be carried out very carefully, as they can damage the surface of the prosthetic restoration.
The strength of this study is that CAD/CAM ceramics with different surfaces were compared after simulated clinical ultrasonic scaling and brushing procedures. Moreover, the corresponding SEM measurements provided us with extensive data on the surface properties of the zirconia samples.
Finally, it should be pointed out that the results of this in vitro study are based on data on viable counts (microbial growth), which may show inhomogeneous results, probably due to the general problem of achieving reproducibility in microbial tests and reliably determining the true value of viable cells. Estimation of cell count by CFU, as used in this experiment, usually underestimates the number of viable cells present in the sample, as clumps of microbial cells can be miscounted as single colonies. This can be problematic for statistical analysis. It should also be noted that in this experiment, not all conditions prevailing in the oral cavity were simulated, such as: the influence of saliva, rinsing effects or changes in pH. Therefore, it would be necessary to prove the results under in vivo conditions as well.
Conclusion
This work has shown that, after ultrasonic scaling and brushing, the resulting mechanical damage favors greater adhesion of microorganisms and that is in contrast to maintaining the achieved therapeutic results in the surgical treatment of periodontal disease. That is why it is recommended to apply ultrasonic scaling and brushing with the greatest care, especially on surfaces that are glazed, because this experiment proved that these routine hygiene procedures damage glazed surfaces of prosthetic zirconia restorations more than the polished zirconia surfaces.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank for the financial support, Serbian Ministry of Education, Science and Technological Development (Contract No. 451-03-9/2021-14/200007). The authors are grateful to DDS_Dental Lab and Jelačić Dental Lab for the laboratory support. The authors respectfully thank Prof Vladimir Pavlović, for his dedication help on SEM.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gomes, A.L.; Montero, J. Zirconia implant abutments: A review. Med Oral Patol Oral Cir Bucal 2011, 16, e50–e55. [Google Scholar] [CrossRef] [PubMed]
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Hisbergues, M.; Vendeville, S.; Vendeville, P. Zirconia: Established facts and perspectives for a biomaterial in dental implantology. Journal of Biomedical Materials Research. Part B, Applied Biomaterials 2009, 88, 519–529. [Google Scholar] [CrossRef]
- Lee, B.C.; Jung, G.Y.; Kim, D.J.; Han, J.S. Initial bacterial adhesion on resin, titanium and zirconia in vitro. Journal of Advanced Prosthodontics 2011, 3, 81–84. [Google Scholar] [CrossRef]
- Saravi, B.; Vollmer, A.; Hartmann, M.; Lang, G.; Kohal, R.-J.; Boeker, M.; Patzelt, S.B.M. Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Materials 2021, 14, 2672. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, I.F.A.; Santos Marques, T.M.S.; Araújo, F.M.; Azevedo, L.F.; Donato, H.; Correia, A. Clinical Performance of CAD/CAM Tooth-Supported Ceramic Restorations: A Systematic Review. Int. J. Periodontics Restor. Dent. 2018, 38, e68–e78. [Google Scholar] [CrossRef]
- Vitti, R.P.; Catelan, A.; Amaral, M.; Pacheco, R.R. Zirconium in dentistry. Advanced Dental Biomaterials 2019, 317–345. [Google Scholar]
- Cantner, F.; Cacaci, C.; Mücke, T.; Randelzhofer, P.; Hajtó, J.; Beuer, F. Clinical performance of tooth- or implant-supported veneered zirconia single crowns: 42-month results. Clin Oral Investig 2019, 23, 4301–4309. [Google Scholar] [CrossRef]
- de Matos, J.D.M.; Lopes, G.R.S.; Queiroz, D.A.; Nakano, L.J.N.; Ribeiro, N.C.R.; Barbosa, A.B.; Anami, L.C.; Bottino, M.A. Dental Ceramics: Fabrication Methods and Aesthetic Characterization. Coatings 2022, 12, 1228. [Google Scholar] [CrossRef]
- Vieira Colombo, A.P.; Magalhães, C.B.; Hartenbach, F.A.; Martins do Souto, R.; Maciel da Silva-Boghossian, C. Periodontal-disease-associated biofilm: A reservoir for pathogens of medical importance. Microb Pathog. 2016, 94, 27–34. [Google Scholar] [CrossRef]
- Offenbacher, S.; Barros, S.P.; Singer, R.E.; Moss, K.; Williams, R.C.; Beck, J.D. Periodontal disease at the biofilm–gingival interface. Journal of periodontology 2007, 78, 1911–1925. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Lang, N.P. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontology 2000 2010, 53, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Pita, P.P.C.; Rodrigues, J.A.; Ota-Tsuzuki, C.; Miato, T.F.; Zenobio, E.G.; Giro, G.; Figueiredo, L.C.; Gonçalves, C.; Gehrke, S.A.; Cassoni, A. Oral streptococci biofilm formation on different implant surface topographies. BioMed Res. Int. 2015, 2015, 159625. [Google Scholar] [CrossRef]
- Li, J.; Helmerhorst, E.J.; Leone, C.W.; Troxler, R.F.; Yaskell, T.; Haffajee, A.D.; Socransky, S.S.; Oppenheim, F.G. Identification of early microbial colonizers in human dental biofilm. Journal of Applied Microbiology 2004. [Google Scholar] [CrossRef]
- Øilo, M.; Bakken, V. Biofilm and dental biomaterials. Materials 2015, 8, 2887–2900. [Google Scholar] [CrossRef]
- Cinquini, C.; Alfonsi, F.; Marchio, V.; Gallo, F.; Zingari, F.; Bolzoni, A.R.; Romeggio, S.; Barone, A. The Use of Zirconia for Implant-Supported Fixed Complete Dental Prostheses: A Narrative Review. Dent. J. 2023, 11, 144. [Google Scholar] [CrossRef] [PubMed]
- Hjerppe, J.; Rodas, S.; Korvala, J.; Pesonen, P.; Kaisanlahti, A.; Özcan, M.; Suojanen, J.; Reunanen, J. Surface Roughness and Streptococcus mutans Adhesion on Metallic and Ceramic Fixed Prosthodontic Materials after Scaling. Materials 2021, 14, 1027. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, M.; Gyr, S.; Astasov-Frauenhoffer, M.; Zitzmann, N.U.; Fischer, J.; Rohr, N. Influence of different zirconia surface treatments on biofilm formation in vitro and in situ. Clin Oral Implants Res. 2022, 33, 424–432. [Google Scholar] [CrossRef]
- Chen, H.L.; Yang, S.; Yu, P.; Wu, J.; Guan, H.; Wu, Z. Comparison of bacterial adhesion and biofilm formation on zirconia fabricated by two different approaches: An in vitro and in vivo study. Advances in Applied Ceramics 2020, 119, 323–331. [Google Scholar] [CrossRef]
- Alves, L.M.M.; Contreras, L.P.C.; Bueno, M.G.; Campos, T.M.B.; Bresciani, E.; Valera, M.C. The wear performance of glazed and polished full contour zirconia. Braz Dent J 2019, 30, 511–518. [Google Scholar] [CrossRef]
- Tunkel, J.; Heinecke, A.; Flemmig, T.F. A systematic review of efficacy of machine-driven and manual subgingival debridement in the treatment of chronic periodontitis. J Clin Periodontol. 2002, 29 (Suppl. 3), 72–81. [Google Scholar] [CrossRef]
- Ivanovic, V.; Popovic, D.; Petrovic, S.; Rudolf, R.; Majerič, P.; Lazarevic, M.; Djordjevic, I.; Lazic, V.; Radunovic, M. Unraveling the Antibiofilm Activity of a New Nanogold Resin for Dentures and Epithesis. Pharmaceutics 2022, 14, 1513. [Google Scholar] [CrossRef] [PubMed]
- Brugger, S.D.; Baumberger, C.; Jost, M.; Jenni, W.; Brugger, U.; et al. Automated Counting of Bacterial Colony Forming Units on Agar Plates. PLoS ONE 2012, 7, e33695. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, K.; Nakamura, K.; Harada, A.; Shirato, M.; Inagaki, R.; Örtengren, U.; Kanno, T.; Niwano, Y.; Egusa, H. Surface properties of dental zirconia ceramics affected by ultrasonic scaling and low-temperature degradation. PLoS ONE 2018, 13, e0203849. [Google Scholar] [CrossRef]
- Zupancic Cepic, L.; Dvorak, G.; Piehslinger, E.; Georgopoulos, A. In vitro adherence of Candida albicans to zirconia surfaces. Oral Dis. 2020, 26, 1072–1080. [Google Scholar] [CrossRef]
- Lee, W.F.; Iwasaki, N.; Peng, P.W.; Takahashi, H. Effect of toothbrushing on the optical properties and surface roughness of extrinsically stained high-translucency zirconia. Clin Oral Investig. 2022, 26, 3041–3048. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.H.; Han, J.S.; Luke Yeo, I.S.; Yoon, H.I.; Lee, J. Effects of ultrasonic scaling on the optical properties and surface characteristics of highly translucent CAD/CAM ceramic restorative materials: An in vitro study. Ceramics International. 2019, 45, 14594–14601. [Google Scholar] [CrossRef]
- Yoon, H.I.; Noh, H.M.; Park, E.J. Surface changes of metal alloys and high-strength ceramics after ultrasonic scaling and intraoral polishing. J. Adv. Prosthodont. 2017, 9, 188–194. [Google Scholar] [CrossRef]
- Sulaiman, T.A.; Camino, R.N.; Cook, R.; Delgado, A.J.; Roulet, J.F.; Clark, W.A. Time-lasting ceramic stains and glaze: A toothbrush simulation study. J Esthet Restor Dent. 2020, 32, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Fiorin, L.; Oliveira, P.E.B.S.; Silva, A.O.d.; Faria, A.C.L.; Macedo, A.P.; Ribeiro, R.F.; Rodrigues, R.C.S. Wear Behavior of Monolithic Zirconia after Staining, Glazing, and Polishing Opposing Dental Restorative Materials: An In Vitro Study. Coatings 2023, 13, 466. [Google Scholar] [CrossRef]
- Yuan, J.C.C.; Barão, V.A.R.; Wee, A.G.; Alfaro, M.F.; Afshari, F.S.; Sukotjo, C. Effect of brushing and thermocycling on the shade and surface roughness of CAD-CAM ceramic restorations. The Journal of prosthetic dentistry 2018, 119, 1000–1006. [Google Scholar] [CrossRef]
- Kreve, S.; Dos Reis, A.C. Effect of surface properties of ceramic materials on bacterial adhesion: A systematic review. J Esthet Restor Dent. 2022, 34, 461–472. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, G.; Kaplan, H.B.; Kolter, R. Annual Rewiev of Microbiology. 2000, 54, 49–79. [Google Scholar] [CrossRef] [PubMed]
- Engel, A.S.; Kranz, H.T.; Schneider, M.; Tietze, J.P.; Piwowarcyk, A.; Kuzius, T.; Arnold, W.; Naumova, E.A. Biofilm formation on different dental restorative materials in the oral cavity. BMC Oral Health 2020, 20, 162. [Google Scholar] [CrossRef]
- Song, F.; Koo, H.; Ren, D. Effects of material properties on bacterial adhesion and biofilm formation. J. Dent. Res. 2015, 94, 1027–1034. [Google Scholar] [CrossRef]
- Karygianni, L.; Jähnig, A.; Schienle, S.; Bernsmann, F.; Adolfsson, E.; Kohal, R.J.; Chevalier, J.; Hellwig, E.; Al-Ahmad, A. Initial Bacterial Adhesion on Different Yttria-Stabilized Tetragonal Zirconia Implant Surfaces in Vitro. Materials 2013, 6, 5659–5674. [Google Scholar] [CrossRef]
- Dal Piva, A.M.O.; Contreras, L.P.C.; Ribeiro, F.C.; Anami, L.C.; Camargo, S.E.A.; Jorge, A.O.C.; Bottino, M.A. Monolithic Ceramics: Effect of Finishing Techniques on Surface Properties, Bacterial Adhesion and Cell Viability. Oper Dent 2018, 43, 315–325. [Google Scholar] [CrossRef]
- de Carvalho, I.H.G.; da Silva, N.R.; Vila-Nova, T.E.L.; de Fatima, D.; de Almeida, L.; Veríssimo, A.H.; de Melo, R.M.; Zhang, Y.; de Assunção, E.; Souza, R.O. Effect of finishing/polishing techniques and aging on topography, C. albicans adherence, and flexural strength of ultra-translucent zirconia: An in situ study. Clin Oral Investig. 2022, 26, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Tsoi, J.K.-H.; Matinlinna, J.P.; Chen, Z. Influence of Grit-Blasting and Hydrofluoric Acid Etching Treatment on Surface Characteristics and Biofilm Formation on Zirconia. Coatings 2017, 7, 130. [Google Scholar] [CrossRef]
- Lee, D.H.; Mai, H.N.; Thant, P.P.; Hong, S.H.; Kim, J.; Jeong, S.M.; Lee, K.W. Effects of different surface finishing protocols for zirconia on surface roughness and bacterial biofilm formation. J Adv Prosthodont 2019, 11, 41–47. [Google Scholar] [CrossRef]
Figure 1.
Zirconia disc (98 mm diameter, 2 mm thick).

Figure 2.
Veneered zirconia samples (polished and glazed) surface before and after ultrasonic scaling and brushing.
Figure 2.
Veneered zirconia samples (polished and glazed) surface before and after ultrasonic scaling and brushing.
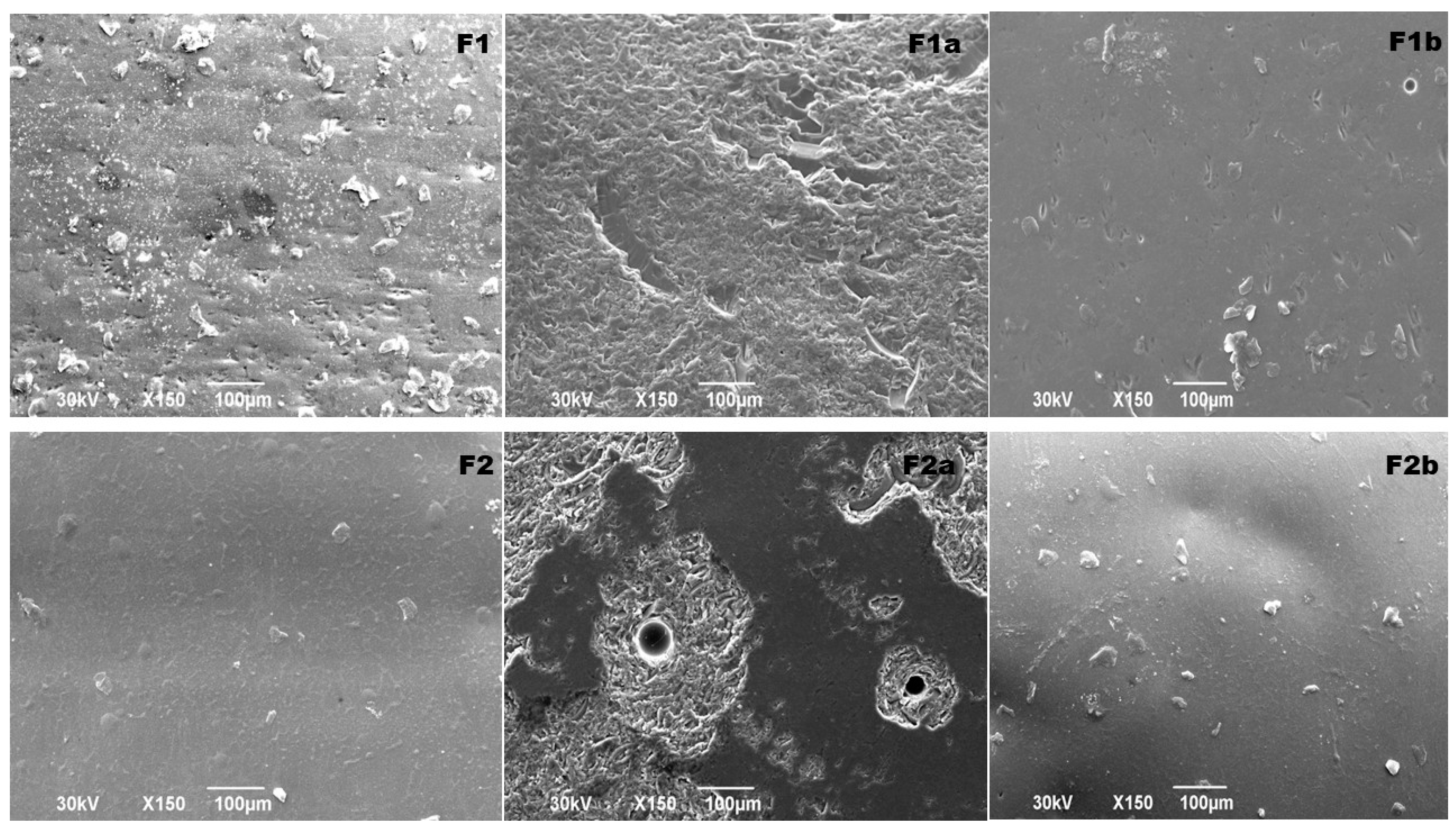
Figure 3.
CAD/CAM milled (polished and glazed) zirconia samples surface before and after ultrasonic scaling and brushing.
Figure 3.
CAD/CAM milled (polished and glazed) zirconia samples surface before and after ultrasonic scaling and brushing.
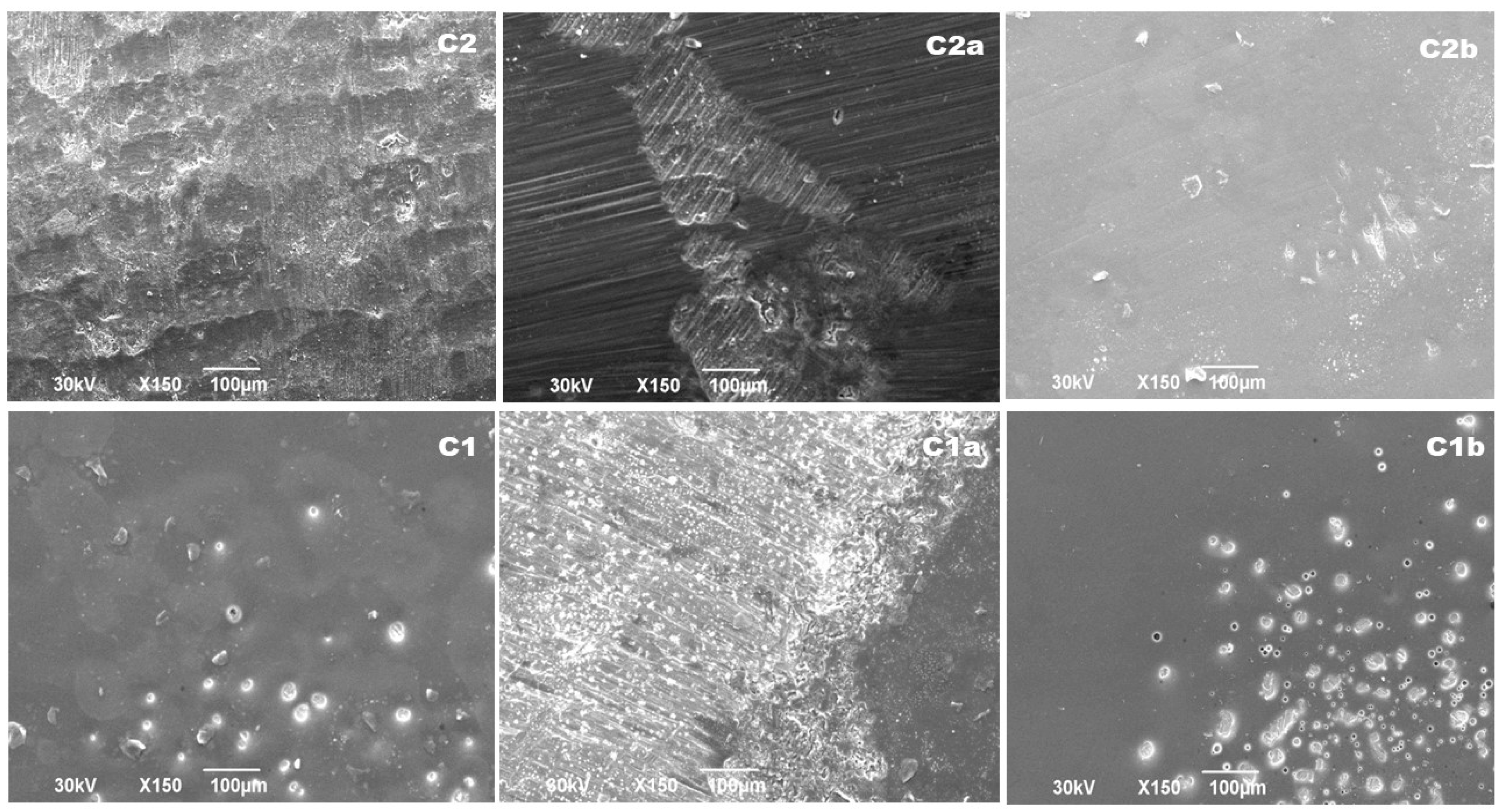
Figure 4.
Biofilm formation of Staphylococcus aureus ATCC 11632 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
Figure 4.
Biofilm formation of Staphylococcus aureus ATCC 11632 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
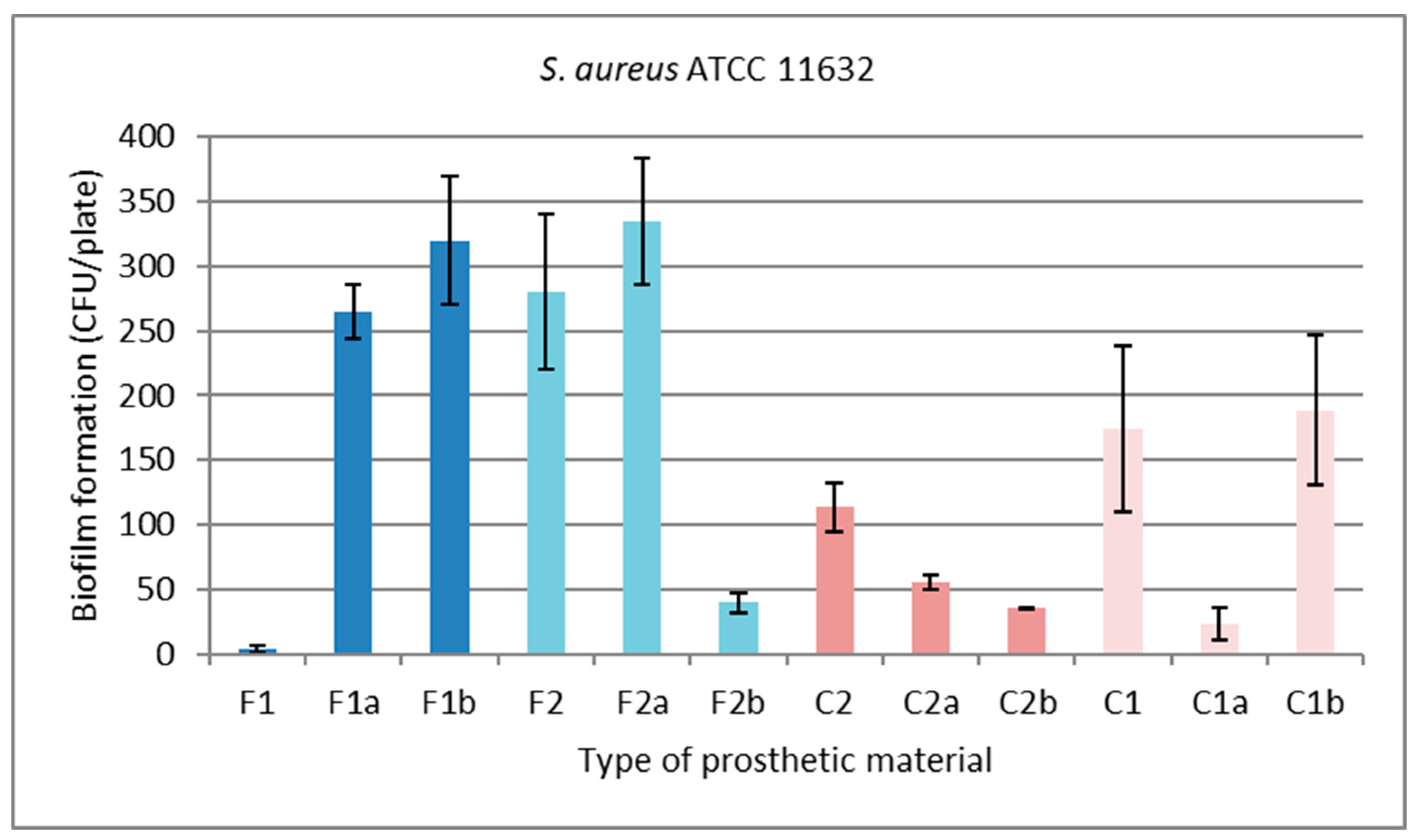
Figure 5.
Biofilm formation of Streptococcus sanguinis ATCC 10556 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
Figure 5.
Biofilm formation of Streptococcus sanguinis ATCC 10556 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
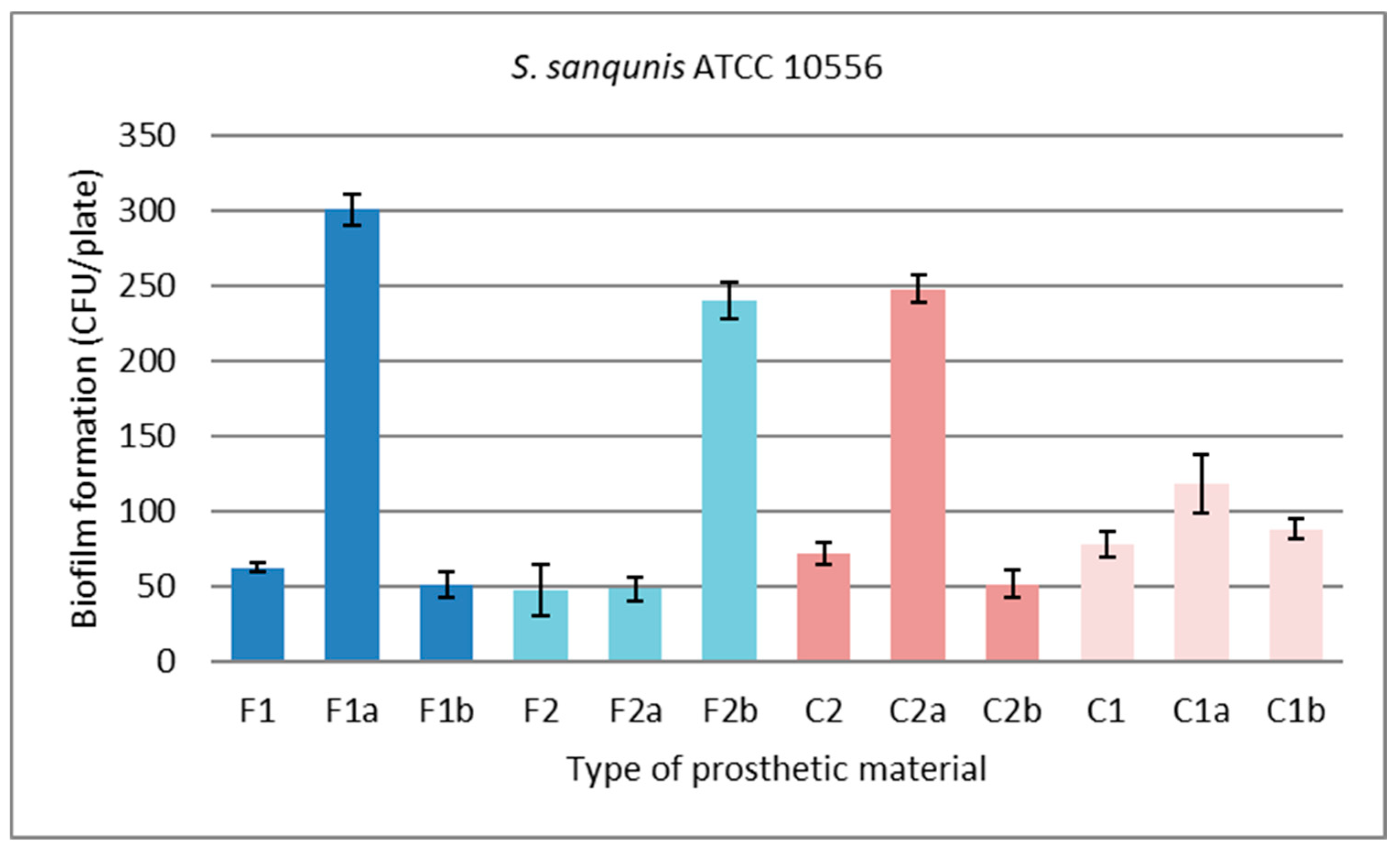
Figure 6.
Biofilm formation of Candida albicans ATCC 10556 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
Figure 6.
Biofilm formation of Candida albicans ATCC 10556 on different zirconia samples. The error bars indicate standard deviations. The data were presented as mean ± SD of two replicates.
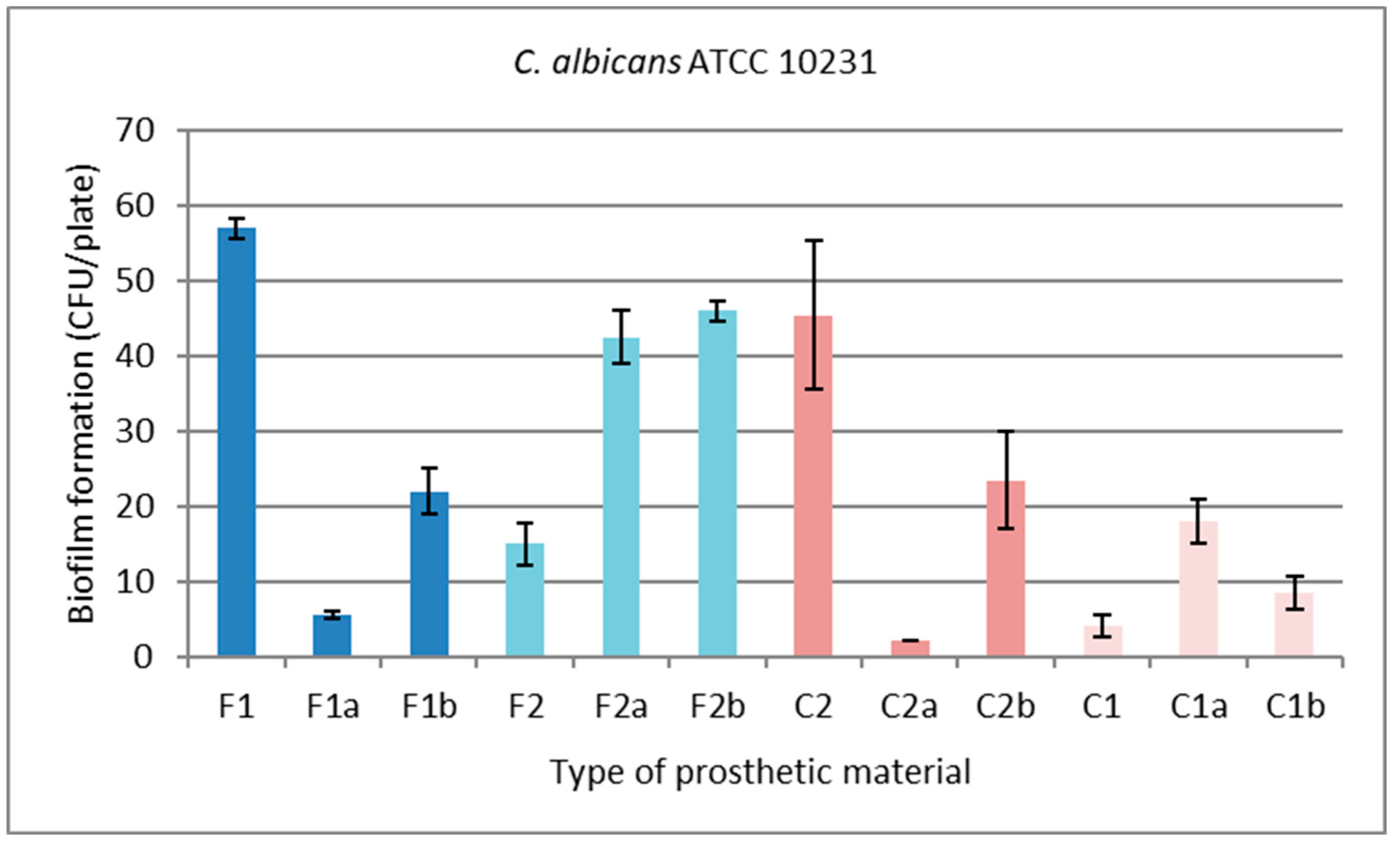

Table 1.
Samples used in the study
| Material Name | Material Code | |
|---|---|---|
| veneered zirconia | Polished | F1 |
| polished treated with ultrasonic scaling | F1a | |
| polished treated with a brushing | F1b | |
| Glazed | F2 | |
| glazed treated with ultrasonic scaling | F2a | |
| glazed treated with brushing | F2b | |
| CAD/CAM milled zirconia | Polished | C2 |
| polished treated with ultrasonic scaling | C2a | |
| polished treated with brushing | C2b | |
| Glazed | C1 | |
| glazed treated with ultrasonic scaling | C1a | |
| glazed treated with brushing | C1b | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



