
Submitted:
09 June 2023
Posted:
26 June 2023
You are already at the latest version
Abstract
Accidental soft tissue injuries are a frequent injury. We report a case involving a 37-year-old man with a soft tissue wound failing conservative treatment. The use of applied fibrin membranes and concentrated growth factors yielded a resolution of the injury in 16 months without need of skin grafting.
Keywords:
soft tissue injury
; fibrin membranes
; concentrated growth factors
1. Introduction
Accidental soft tissue injury represents the most common management challenges for hand surgeons [1]. The management of skin and soft tissue damage requires several steps, depending on the specifical nature of the lesion: i) analgesia reduces pain; ii) irrigation with Dakin’s solution or sterile isotonic solution reduces the development of infections; iii) tissue debridement, removing the devitalized tissue reduces the bacterial growth; iv) dressing and/or surgical closure reduce the time of healing [2].
Previously, we reported a series of 87 patients with wound lesions in which topical application of platelet gel resolved clinical symptoms reducing healing time [3,4,5,6].
Platelet-rich plasma (PRP) is an interesting therapeutic option for wounds and skin damage, because several growth factors are released by platelets: fibroblast growth factors, platelet-derived growth factor (PDGF), epidermal growth factor, insulin-like growth factor-1, transforming growth factor-β, vascular endothelial growth factor [7]. PRP favors the action of growth factors through the production of new epithelium, stimulation of granulomatous tissue formation, aggregation of fibroblasts, macrophages and other cells, and collagen production [8]. Nevertheless, PRP has antibacterial activity against Escherichia coli, Staphylococcus aureus, Candida albicans and Candida neoformans [9].
Fibrin sealants are a relatively recent therapeutic option in wound management. According to protocol TIME (Tissue, Inflammation/infection, Moisture imbalance and Epithelial edge advancement) for ulcer management, topical treatment has a crucial role in the recovery of this lesions. Fibrin seems to be an effective solution consequentially to its role in hemostasis, it acts in the healing process to promote collagen synthesis, angiogenesis, wound contraction and reepithelization. It is mainly used as sealant, adhesive and hemostatic [10].
Recently, we documented the effect of this treatment in three patients with chronic wound ulcers [11]. In the present case we report a case of successful application of fibrin membranes as a biologic wound dressing material for coverage of full thickness soft tissue loss.
2. Case report
A 37-year-old man presented to our ward of pain medicine for an accidental severe leg injury associated with skin and soft tissue loss (Figure 1A).
History revealed the use of recreational drugs without viral infections (e.g. HIV, HBV, HCV), or systemic diseases. At the exploration the patient experienced severe pain (visual analogue scale, VAS 10) with poor sensation; The skin of forearm was red with sign and symptoms of infection (Fever 38.2°C); bone, tendons and muscle were exposed. Interphalangeal joint flexion and extension of the last three fingers was not possible. Blood pressure was 120/78 mmHg, heart rate 85 beats/min, oxygen pressure saturation at room temperature 99%. Plain radiographs excluded the presence of bone fracture but revealed a severe soft tissue edema (Figure 2).
Initial treatment included wound debridement, wound dressings, systemic antibiotics (amoxicillin 1000 mg tid and azithromycin 500 mg od) and non-steroidal anti-inflammatory drugs (ibuprofen 600 mg bid). Seven days later, the infection of forearm improved. The patient consented to heterologous fibrin membrane treatment and 9 mL of heterologous blood obtained from the parents of the patient was analyzed for compatibility and sterility. About 1 week later, when the safety was showed, blood samples were taken from the parents to obtain PRP, in agreement with our previous study [11]. Briefly, blood samples were drawn in sterile Vacuette tubes (Greiner Bio-One, GmbH, Kremsmunster, Austria) without anticoagulant solutions and immediately centrifuged (Medifuge MF200, Silfradent srl, Forlì, Italy) at different velocities: 30” acceleration, 2’ 2,700 rpm, 4’ 2,400 rpm, 4’ 2,700 rpm, 3’ 3,000 rpm, and 36” deceleration and stop. Three blood fractions resulted: (1) the upper platelet poor plasma (PPP) layer; (2) the middle fibrin rich gel with aggregated platelets and concentrated growth factors (CGF); (3) the lower red blood cell (RBC) layer.
The skin was cleaned (Figure 1B), cefepime was topically applied for 30 minutes, and then the fibrin rich gel (fraction 2) and the PPP (fraction 1) (Figure 1C) were applied. The wound was protected with an occlusive dressing.
At the follow-up (1 week later), the patient was pain-free without signs of infection (body temperature: 36.2 °C; heart rate 62 b/min). Wound was cleaned, cefepime was administered topically for 30 minutes and heterologous blood was taken for membranes. The follow-up was performed every week. At one-month no signs of infection or inflammation were present and cefepime was discontinued.
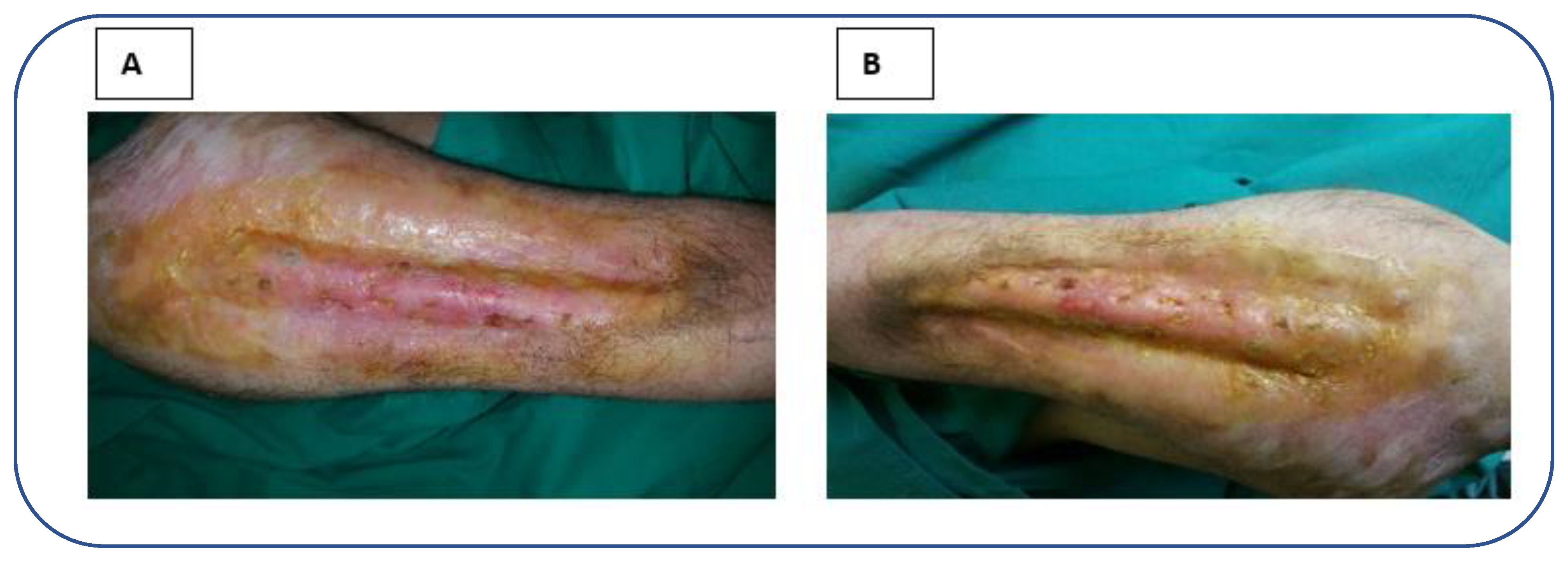
During a four-month follow-up the lesion improved (Figure 3A) and two months later (six months after the admission, Figure 3B), the patient achieved satisfactory cosmetic appearance of the reconstructed digit with complete functional restoration. The patient recovered thermal, pain and tactile sensitivity, evaluated using cold and hot water (thermal), a needle tip testing (pain) and cotton ball, bristle brush and strip of paper (tactile) testing, respectively. The patient signed the informed consent to publish this case and received a treatment in agreement with the Declaration of Helsinki.
3. Discussion
We report the clinical efficacy of fibrin membranes plus growth factors in the treatment of a traumatic non-healing ulcer.
The use of topical treatment reduces surgery offering a conservative strategy, with less stress and economic expense for patients and health care systems. Nevertheless, topical treatment is often a fundamental complement after surgery [2,10].
Fibrin sealants are biocompatible products. There are two main types of fibrin sealants: homologous and heterologous. Homologous type is the most diffused and validated in clinical studies, but has high costs [10].
Fibrin has been used in different wound management setting and in association to other components including keratinocytes, fibroblasts and platelets [10].
Kirsner et al. [12], in a phase II clinical trial, highlighted the efficacy of a spray (0.5 × 10⁶ cells/mL every 2 weeks) containing neonatal keratinocytes, fibroblasts and fibrin sealant in 228 venous ulcers patients. Wound area was significantly reduced in the treatment group respect to the control one. Few adverse events (AE) were reported, including skin ulceration and cellulitis.
Asadi et al. [13], in 10 patients affected by refractory ulcer, documented an improvement of symptoms after topical treatment with PRP, fibrin glue and collagen matrix. In this study, 9 of 10 patients completely recovered, showing relevant benefits in epithelization, vascularization, and granulation tissue development, without the development of AE.
Despite these interesting results, some concerns about homologous fibrin sealants remains (e.g. high costs and risk of infection). Therefore, scientists are testing heterologous fibrin in experimental animals [10], even if to date only few clinical trials have been performed.
Gatti and colleagues [14], observed a good clinical response in 13 patients with venous ulcer managed with heterologous fibrin, essential fatty acids and Unna’s boot. The main advantages of heterologous fibrin were the decrease of pain, the easily of application, the absence of both infection and AE.
Abbade et al. [15], highlighted a clinical improvement in 10 patients managed with heterologous fibrin, a gauze soaked in fatty acids and Unna’s boot, without the development of AE. The same group described the development of local AE related to this treatment (ulcer pain, peri-ulcer eczema, the opening of new ulcers, peri-ulcer maceration, peri-ulcer pruritus, critical colonization, and increased ulcerated area) in 31 patients [16].
A long-date debate animates the scientific community concerning PRP use. Despite its current application (autologous and allogenic) in stimulating tissue growth and regeneration, consensus remains controversial. Several clinical studies in non-healing ulcers demonstrated a certain grade of efficacy of this treatment [13].
A longitudinal single arm trial by Mohammadi et al. [17], in 100 diabetic patients with foot ulcer documented the efficacy of PRP gel preparation in the improvement of wound area.
Suthar et al. [18], showed in 24 patients with non-healing ulcers of different etiologies, that subcutaneous PRP, followed by topical administration led to wound size reduction, without the development of autoimmunity or infections.
Burgos-Alonso et al.[19], in a randomized pilot study, in 12 patients with leg wounds due to venous insufficiency showed the efficacy of autologous PRP (reduction of ulcer size 3.9 cm2 for week) compared to standard of care (time of healing 10-12 weeks).
Nolan et al. [20], performed a randomized clinical trial (RCT) in 18 diabetic foot ulcer patients, divided in three arms: autologous fat grafting, autologous fat grafting plus PRP and routine care. Although, no clinical difference was shown between these groups, increased graft survival in PRP arm was documented, increasing micro-vascularization. It is not clear if reduced apoptosis or increased proliferation are responsible for this beneficial effect. However, the increased angiogenesis related to PRP use has been highlighted as a determinant factor to revert the ulcer [7].
A systematic review and meta-analysis of the existing randomized trials of PRP use in chronic wounds by Meznerics and colleagues [21] concludes that PRP is an effective method in this setting offering great advantages. Concerning ulcer etiologies they found a higher efficacy in venous ulcers, whereas diabetic ones had worse outcomes. This could be related to i) the pathogenesis of diabetic ulcers; ii) the PRP administration (commonly through injection).
A low number of studies were made using PPP. Setta and colleagues [22] recruited 24 patients with diabetic ulcers, dividing them in two groups managed respectively with PPP and PRP. The wound healing was significantly faster in PRP group vs PPP one.
The efficacy of topical application of platelet gel in patients with skin lesions has been previously documented [3,4,5,6]. Jiritano et al. [3], and Serraino et al.[6] , documented the effect of autologous PRP application in the prevention of surgical infections. Similarly, Serra et al., [5] in a diabetic patient, reported the efficacy and the safety of PRP in wound healing, without the development of infections.
In the present case, we report the efficacy and the safety of PRP in a patient with traumatic non-healing ulcer that usually received a surgical treatment.
Few studies were made on this topic in acute setting and trauma.
Kazakos et al.[23], in 59 patients with acute wounds (open fractures, closed fractures with skin necrosis and friction burns) documented that the wound healing rate was significantly faster at week 1, 2 and 3 in patients (n. 27) treated with topical application of PRP gel vs patients (n.32) treated with conventional dressing (p=0.003, p<0.001 and p<0.001, respectively). Moreover, the authors reported that the mean time to plastic reconstruction in PRP-treated patients was 21.26 days vs 40.6 days in dressing-treated patients. These data suggest that PRP gel treatment represents an effective aid in the treatment of acute wounds trauma.
Similarly, Moneib et al. [24] documented in 40 patients with chronic venous leg ulcers that a 6-week treatment with autologous PRP (1 administration/week) induced a significant improvement in the ulcer size respect to a 6-week treatment with compression and dressing (4.92 ± 11.94 cm and 0.13 ± 0.27 cm, respectively).
Fibrin sealants may offer a comfortable solution and effective solution. However, cost-benefit ratio must improve, especially for homologous preparation. Heterologous fibrin sealants are less expensive but increase the risk of immunogenicity[10]. Conversely, PRP is an optimal choice, considering its provenience from the patient and the absence of immunogenicity. Nevertheless, long period treatment may make this treatment uncomfortable for patients, according to the necessity of blood sampling. Therefore allogenic PRP is another possible option showing good clinical efficacy [13].
In our study we used heterologous blood because we need high quantity of blood for a long time, obtaining a good clinical efficacy without the development of AE or autoimmunity.
In conclusion, in the present case we documented that PRP represents an efficacy and safety treatment for soft tissue wounds or damages. However, larger randomized clinical trials are needed to have more solid data about its usage.
References
- Baum, C.L.; Arpey, C.J. Normal cutaneous wound healing: Clinical correlation with cellular and molecular events. Dermatologic Surg. 2005, 31, 674–686. [Google Scholar] [CrossRef]
- Rapp, J.; Plackett, T.; Crane, J.; Lu, J.; Hardin, D.; Loos, P.; Kelly, R.; Hall, M.A.; Murray, C.; Keenan, S.; et al. Burn Wound Management in Prolonged Field Care Available online:. Available online: https://jts.amedd.army.mil/assets/docs/cpgs/Wound_Management_PFC_24_Jul_2017_ID62.pdf (accessed on Feb 4, 2023).
- Jiritano, F.; Serraino, G.F.; Rossi, M.; Dominijanni, A.; Brescia, A.; Renzulli, A. Ventricular assist device driveline infection: Treatment with platelet-rich plasma. Ann. Thorac. Surg. 2013, 96, e37–e38. [Google Scholar] [CrossRef]
- Serra, R.; Buffone, G.; De Franciscis, A.; Mastrangelo, D.; Vitagliano, T.; Greco, M.; De Franciscis, S. Skin grafting followed by low-molecular-weight heparin long-term therapy in chronic venous leg ulcers. Ann. Vasc. Surg. 2012, 26, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Serra, R.; Buffone, G.; Dominijanni, A.; Molinari, V.; Montemurro, R.; de Franciscis, S. Application of platelet-rich gel to enhance healing of transmetatarsal amputations in diabetic dysvascular patients. Int. Wound J. 2013, 10, 612–615. [Google Scholar] [CrossRef]
- Serraino, G.F.; Dominijanni, A.; Jiritano, F.; Rossi, M.; Cuda, A.; Caroleo, S.; Brescia, A.; Renzulli, A. Platelet-rich plasma inside the sternotomy wound reduces the incidence of sternal wound infections. Int. Wound J. 2015, 12, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Rechichi, M.; Ferrise, M.; Romano, F.; Gallelli, L.; Toschi, V.; Dominijanni, A.; Meduri, A. Autologous platelet-rich plasma in the treatment of refractory corneal ulcers: A case report. Am. J. Ophthalmol. Case Reports 2020, 20, 100838. [Google Scholar] [CrossRef] [PubMed]
- Tsachiridi, M.; Galyfos, G.; Andreou, A.; Sianou, A.; Sigala, F.; Zografos, G.; Filis, K. Autologous platelet-rich plasma for nonhealing ulcers: A comparative study. Vasc. Spec. Int. 2019, 35, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Yaltirik, M.; Koray, M.; Kocaelli, H.; Ofluoglu, D. Platelet-Rich Plasma in Trauma Patients Available online:. Available online: https://www.intechopen.com/chapters/63335 (accessed on Feb 4, 2023).
- Abbade, L.P.F.; Ferreira, R.S.; Dos Santos, L.D.; Barraviera, B. Chronic venous ulcers: A review on treatment with fibrin sealant and prognostic advances using proteomic strategies. J. Venom. Anim. Toxins Incl. Trop. Dis. 2020, 26, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Romano, F.; Paolino, F.M.; Rizzo, B.A.; Russo, A.; Southworth, S.; Serra, R.; Gallelli, L. The use of growth factors, CD34+ cells and fibrin for the management of chronic venous ulcers. Int. Wound J. 2016, 13, 1011–1013. [Google Scholar] [CrossRef] [PubMed]
- Kirsner, R.S.; Marston, W.A.; Snyder, R.J.; Lee, T.D.; Cargill, D.I.; Slade, H.B. Spray-applied cell therapy with human allogeneic fi broblasts and keratinocytes for the treatment of chronic venous leg ulcers: A phase 2, multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2012, 380, 977–985. [Google Scholar] [CrossRef]
- Asadi, M.; Alamdari, D.H.; Rahimi, H.R.; Aliakbarian, M.; Jangjoo, A.; Abdollahi, A.; Bahar, M.M.; Azadmand, A.; Forghani, N.; Sadegh, M.N.; et al. Treatment of life-threatening wounds with a combination of allogenic platelet-rich plasma, fibrin glue and collagen matrix, and a literature review. Exp. Ther. Med. 2014, 8, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.A.N.; Vieira, L.M.; Barraviera, B.; Barraviera, S.R.C.S. Treatment of venous ulcers with fibrin sealant derived from snake venom. J. Venom. Anim. Toxins Incl. Trop. Dis. 2011, 17, 226–229. [Google Scholar] [CrossRef]
- Abbade, L.; Barraviera, S.R.C.S.; Silvares, M.R.; Seabra Ferreira Junior, R.; Carneiro, M.T.R.; Medolago, N.B.M.; Barraviera, B. A new fibrin sealant derived from snake venom candidate to treat chronic venous ulcers. J. Am. Acad. Dermatol. 2015, 72, AB271. [Google Scholar] [CrossRef]
- Abbade, L.P.F.; Barraviera, S.R.C.S.; Silvares, M.R.C.; Lima, A.B.B. d. C.O.; Haddad, G.R.; Gatti, M.A.N.; Medolago, N.B.; Rigotto Carneiro, M.T.; dos Santos, L.D.; Ferreira, R.S.; et al. Treatment of Chronic Venous Ulcers With Heterologous Fibrin Sealant: A Phase I/II Clinical Trial. Front. Immunol. 2021, 12, 1–16. [Google Scholar] [CrossRef]
- Mohammadi, M.H.; Molavi, B.; Mohammadi, S.; Nikbakht, M.; Mohammadi, A.M.; Mostafaei, S.; Norooznezhad, A.H.; Ghorbani Abdegah, A.; Ghavamzadeh, A. Evaluation of wound healing in diabetic foot ulcer using platelet-rich plasma gel: A single-arm clinical trial. Transfus. Apher. Sci. 2017, 56, 160–164. [Google Scholar] [CrossRef]
- Suthar, M.; Gupta, S.; Bukhari, S.; Ponemone, V. Treatment of chronic non-healing ulcers using autologous platelet rich plasma: a case series. J. Biomed. Sci. 2017, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Burgos-Alonso, N.; Lobato, I.; Hernández, I.; Sebastian, K.S.; Rodríguez, B.; March, A.G.; Perez-Salvador, A.; Arce, V.; Garcia-Alvarez, A.; Gomez-Fernandez, M.C.; et al. Autologous platelet-rich plasma in the treatment of venous leg ulcers in primary care: A randomised controlled, pilot study. J. Wound Care 2018, 27, S20–S24. [Google Scholar] [CrossRef]
- Nolan, G.S.; Smith, O.J.; Heavey, S.; Jell, G.; Mosahebi, A. Histological analysis of fat grafting with platelet-rich plasma for diabetic foot ulcers—A randomised controlled trial. Int. Wound J. 2022, 19, 389–398. [Google Scholar] [CrossRef]
- Meznerics, F.A.; Fehérvári, P.; Dembrovszky, F.; Kovács, K.D.; Kemény, L.V.; Csupor, D.; Hegyi, P.; Bánvölgyi, A. Platelet-Rich Plasma in Chronic Wound Management: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Clin. Med. 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Saad Setta, H.; Elshahat, A.; Elsherbiny, K.; Massoud, K.; Safe, I. Platelet-rich plasma versus platelet-poor plasma in the management of chronic diabetic foot ulcers: A comparative study. Int. Wound J. 2011, 8, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Kazakos, K.; Lyras, D.N.; Verettas, D.; Tilkeridis, K.; Tryfonidis, M. The use of autologous PRP gel as an aid in the management of acute trauma wounds. Injury 2009, 40, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Moneib, H.A.; Youssef, S.S.; Aly, D.G.; Rizk, M.A.; Abdelhakeem, Y.I. Autologous platelet-rich plasma versus conventional therapy for the treatment of chronic venous leg ulcers: A comparative study. J. Cosmet. Dermatol. 2018, 17, 495–501. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient’s admission conditions and management. 1A: skin lesion was very severe at admission, with consistent tissue damage and bone exposure; 1B: lesion cleansed. Then cefepime was topically applied for 30 minutes. Finally, the fibrin rich gel was applied; 1C: platelet poor plasma was applied, and the wound was protected with an occlusive dressing. After seven days the patient returned for scheduled examination.
Figure 1.
Patient’s admission conditions and management. 1A: skin lesion was very severe at admission, with consistent tissue damage and bone exposure; 1B: lesion cleansed. Then cefepime was topically applied for 30 minutes. Finally, the fibrin rich gel was applied; 1C: platelet poor plasma was applied, and the wound was protected with an occlusive dressing. After seven days the patient returned for scheduled examination.
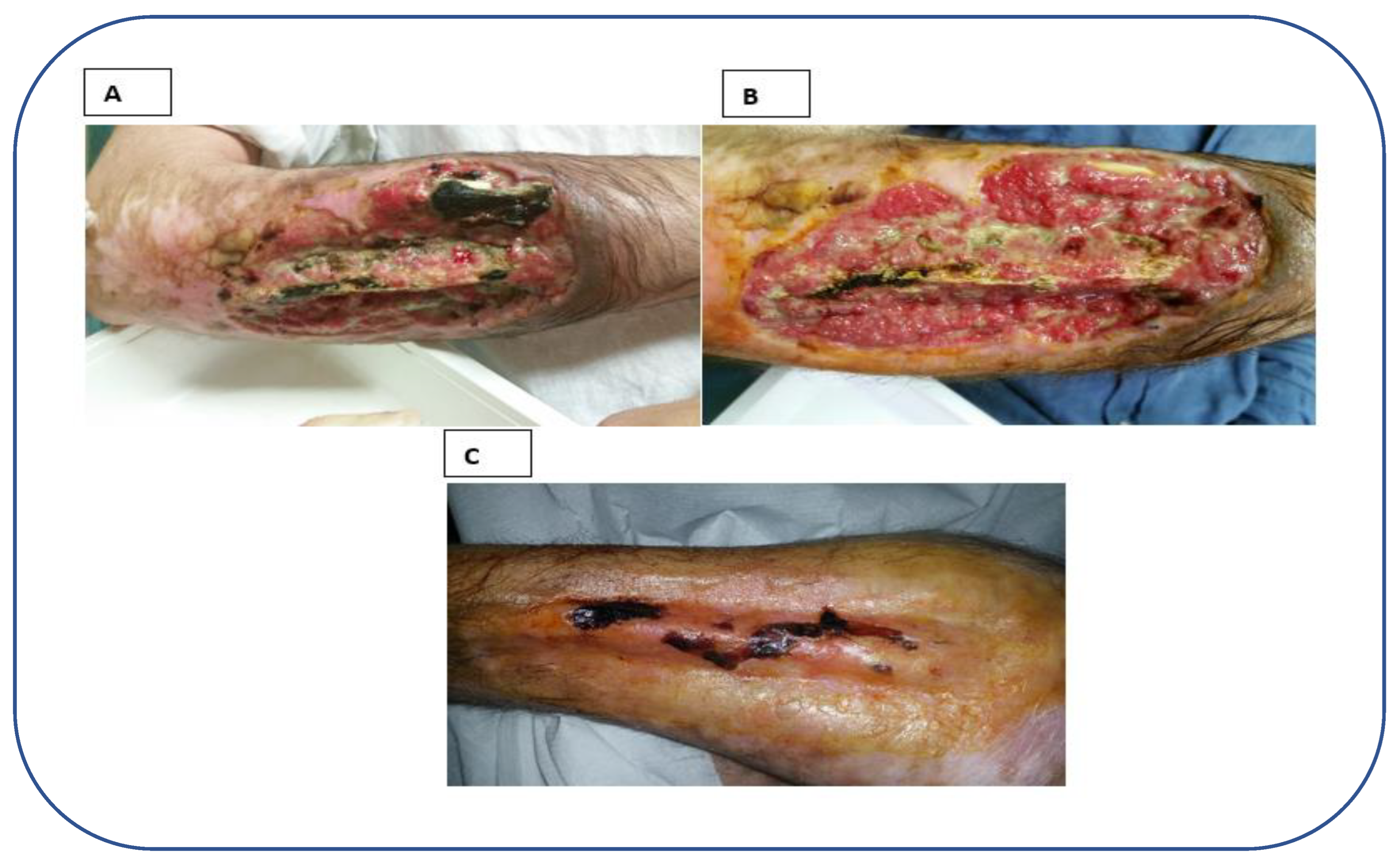
Figure 2.
Radiograms of patient’s right arm. Despite soft tissue oedema and disruption, no relevant bone involvement was documented.
Figure 2.
Radiograms of patient’s right arm. Despite soft tissue oedema and disruption, no relevant bone involvement was documented.

Figure 3.
Follow-up at 4 (A) and 6 (B) months after the first admission.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



