
Submitted:
26 June 2023
Posted:
27 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
This study examines the psychological repercussions of the COVID-19 pandemic on a medical team in an Israeli general hospital. The research explores the professional quality of life, burnout symptoms, secondary traumatic stress, and mindfulness among team members across three distinct phases of the pandemic. Analysis was conducted for different subgroups based on job roles and seniority, allowing for an evaluation of the phase-specific effects on the ProQOL (Professional Quality of Life) and mindfulness. Results align with established crisis trajectories, encompassing honeymoon/heroic phases, inventory, disillusionment, and recovery. The findings demonstrate a negative correlation between compassion satisfaction and burnout, as well as between mindfulness and burnout/secondary traumatic stress. Remarkably, male doctors exhibit a more pronounced negative impact on mindfulness compared to their female counterparts, primarily comprising healthcare workers. Temporal analysis reveals significant differences in compassion satisfaction and mindfulness, with baseline measurements being notably higher. Furthermore, the study sheds light on the vulnerability of male doctors, emphasizing the crucial role of hospital management in conveying the message and implementing effective measures to support professional quality of life. These findings underscore the necessity of prioritizing the well-being of medical professionals, particularly male doctors who face unique challenges in seeking assistance.
Keywords:
COVID-19
; Healthcare workers
; Medical doctors
; Compassion Satisfaction
; Burnout
; Secondary Traumatic Stress
; Coronavirus
; Mental health
; Mindfulness
1. Introduction
Crises, such as major public health events, for instance a pandemic, often have a significant impact on medical staff, and require them to make psychological adjustments. In December 2019, cases of pneumonitis of a new type of coronavirus infection (COVID-19) appeared in the Hubei Province, China. It has since spread rapidly in many countries and regions around the world, forcing the World Health Organization (WHO) to announce a COVID-19 pandemic on March 11 of 2020. During the pandemic, incidences of anxiety, depression, and post-traumatic stress disorder (PTSD) increased amongst Health Care Workers (HCWs), and quality of life was undermined by an increase in Burnout and Compassion Fatigue (CF), seen especially amongst women and nurses [1]. The psychological and physical impact has been reported to be especially high in HCWs, who face additional group-specific stressors [1,2,3,4,5]. HCWs face higher work demands and risks to their physical and mental integrity, in addition to high incidents of infection (25%-30% in the case of physicians, and 45%-55% in the case of nurses) [1], intense work-related stressors including long working hours, strict instructions and safety measures, a permanent need for concentration and vigilance, reduced social contact, and the performance of tasks that they may not have been prepared for[6]. Additionally, HCW’s are at risk of losing close colleagues, friends or infecting loved ones [7,8]. A rapid systematic review found that the rates of mental health disorder symptoms are high in HCWs (PTSD: 44.9%, depression: 27.2%, anxiety: 27.7%, and insomnia: 36.1%) [9]. Other reasons for the psychological suffering of HCWs may be associated with the uncertainty of a safe workplace, irritability, insomnia, sadness, demoralization, little time to rest, in addition to exhaustion due to the increasingly high number of cases[10,11]. Moreover, burnout, inadequate personal protective equipment, higher levels of CF and burnout may lead to higher levels of moral distress[1,5,12].
The risk of contracting the disease, the challenge of making difficult moral decisions about care priorities during the pandemic and poor working conditions have exposed HCWs to severe psychological stress leading to mental disorders such as anxiety (characterized by cognitive, somatic, emotional and behavioral components and is associated with social problems); depression (loneliness, sleep disturbances, difficulty concentrating, inability to initiate activities, sadness and feelings of rejection) [5,13] in addition to CF and burnout [3] Furthermore, factors such as a high-risk workplace, young age, and a history of psychological disorders can contribute to the development of anxiety, depression, and stress among HCWs[12,13,14,15,16], as-well as exposure to patient's death which is more likely to lead to secondary-traumatic stress (STS)[17] . Therefore, HCWs presented a high prevalence of mental disorders during the COVID-19 pandemic [18]. Many reports in the literature show that front-line professionals exposed and involved in the diagnosis and treatment of COVID-19 patients are more susceptible compared to people who are not dealing directly with these patients[2,15,17,19]. Recent studies have shown that frontline HCWs, especially nurses, may be experiencing the highest levels of anxiety [4,16,20], and STS [17] owing to the fact that they are responsible for the care of patients with COVID-19, and are more mentally overwhelmed by the lack of specific treatment guidelines and adequate support [3]. Moreover, studies show that a lack of social support increases the risk of depression and burnout [5].
A systematic review conducted upon Western frontline healthcare professionals reflecting variable levels of stress, anxiety, depression, sleep disturbance, and burnout in the population of healthcare professionals from different countries in Europe and the USA [21]. More intense symptoms were seen amongst frontline personnel, as well as amongst females and individuals in the nursing category [4,16,22,23]. Other factors which were found to aggravate stress are: suffering from chronic disease and a history of mental health issues [4,22,24], shorter work experience, and being single [25], having a worse perception [26] in addition to living in areas with a higher incidence of the disease [27].
Overall, the comparative results indicated greater anxiety among frontline professionals [12,25,28,29,30], with the most affected being the female nursing personnel working in the vicinity of COVID-19 patients, with 40% compared to the 15% of other categories [3,12,23]. Nurses showed poorer outcomes in terms of mental health and anxiety disorders compared to other healthcare professionals, as-well as high percentages of vicarious trauma (29.16) and burnout (29.16) [3,31,32]. In research carried out by [20], professional quality of life and mental health outcomes amongst HCWs were tested. According to the findings, female subjects showed higher stress levels, frontline staff reported higher Compassion Satisfaction (CS) levels and that burnout, secondary traumatization, first line activity and ICU were positively and significantly correlated with depression and anxiety. Other research showed that gender, age, anxiety, depression, and a history of past trauma were all risk factors for STS [4,16].
Burnout (BO) is a core aspect of reduced work-related psychological health and represents a severe, chronic strain response of the individual to enduring stress at work [33,34]. It is defined as high levels of emotional exhaustion, depersonalization, low personal accomplishment [34,35,36],frustration and feelings of powerlessness [32], loss of enthusiasm for work, psychological exhaustion, and indolence (a negative attitude, behaviors, and experience of guilt) [10].
With an increase in professional stress, burnout levels are higher. Persistent tension caused by work overload, lack of equipment, human resources, and lack of social support at work has been shown to correlate positively with burnout and can lead to psychological and\or physical distress. burnout is prevalent amongst HCWs, especially nurses (53.3%), compared to physicians, (42.5%) [10,37]. Moreover, burnout syndrome may increase the risk of medical errors and therefore patient safety which in turn compromises the quality of care in addition to decreased job satisfaction [35,38]. Physicians who had high levels of burnout and fatigue reported negligence of self-protection measures and an increase in the risk of infection. Moreover, negative consequences included depression, suicidal tendencies, medical illnesses [35,38], anxiety, lower satisfaction, and care quality [2]. More than half of physicians had experienced burnout [34,39].
Age (being younger), gender (being female), job category (nurses and physicians), work site (Specialized COVID-19 unit) [1,34], and perceived threat of COVID-19 [10] were all significantly associated with high levels of burnout, as-well as marital status, salary reduction, health problems and direct contact with infected people were susceptible to personal and work-related burnout [40]. Senior medical staff reported low levels of distress, while front-line workers reported high levels of resilience [11]. High exposure environment was associated with endorsement of PTSD symptoms, burnout, anxiety, and depression, whilst resilience showed less impact on the endorsement of PTSD symptoms.
Secondary Traumatic Stress (STS) is considered a stressor for PTSD; it had been studied amongst HCWs involved in treatment of traumatically injured patients. STS includes a phenomena of compassion stress, that in turn, leads to feelings of fatigue and re-traumatization. The re-experiencing of trauma may lead to CF; inability to emphasize, support patients and to moral injury, due to the lack of actions (eg., the inability to help patients due to lack of resources) [2], or the emergence of ethical conflicts relating to rational decisions (eg. caring based on age or chronicity) [1]. Female HCWs showed significantly higher scores on the STS Intrusion subscale, in addition to subjects without children who exhibited higher scores on all STS subscales. STS was found to be positively correlated with the amount of time spent with the patient; exposure to patient's death; severity of symptoms of a friend or family member infected with COVID-19 [17].
Compassion Satisfaction (CS) represents the positive aspect of being a HCW, relating to empathy and QOC. CS is a possible factor that counterbalances the risks of CF, since stress and negative affect positively correlates with CF, whereas positive affect positively correlated with CS [32]. Findings from research that took place a couple of months after the beginning of the pandemic showed that CS seemed to be increasing, especially amongst nurses, due to the persistent media coverage that led to their perceived social recognition [41]. In accordance with the mentioned findings, research from the middle of the pandemic found high levels of CS (52.80%) as opposed to low levels of CF (41.80%) and burnout (36.04%) compared to prior research, [42], suggested that HCWs were able to find:
"Sense of value and meaning in the work they do, perhaps bolstered by the public's emphasis of the "essential" or even "heroic" nature of their roles". Moreover, CS was significantly and negatively correlated with CF and burnout, while burnout and CF were significantly and positively correlated. Regarding the 'heroic' nature, [43], agrees that the special circumstances caused by the pandemic have given nurses a chance to rediscover their motivation to provide care, and increased the visibility of nurse's work and social image.
Quality of Working Life (QoWL) can be seen as the way in which work is good for you in the widest context in which an employee would evaluate their job [44]. Poor patient outcomes decrease employee motivation, and decisions to leave the organization have been linked to poor working conditions [45]. Work engagement is a positive, fulfilling, affective motivational state of work-related well-being that is characterized by vigor, dedication, and absorption. Engaged employees have high levels of energy and identify strongly with their work [46].
Research on engagement revealed that engagement is a unique concept that is best predicted by job resources and demands (eg., autonomy – discretion to nursing staff in managing, coaching, performance feedback, training, continuing education) and personal resources (eg., optimism, self-efficacy, self-esteem) [36]. Studies have shown that work engagement is predictive of job performance and client satisfaction. A great deal of research supported the view that rudeness is a function of the social environment at work [47]. Thus, improving workplace social environments, in conjunction with a sincere commitment from management, may reduce rudeness and mistreatment. Rudeness may then lead to other positive employee outcomes, such as more positive work attitudes and less burnout, turnover intentions, and absenteeism.
Findings from research by [43], show factors such as resilience, empathy, and self-compassion influence whether the care by the HCW will be positive (and lead to CS) or negative (and lead to CF and\or burnout). Mean CS scores were higher in nurses, while CF and burnout scores were higher for physicians.
Mindfulness is described as the exercise of putting determined effort into paying attention to the current moment, experiencing it without judgement and acceptance. The goal of this exercise is for the individual to respond in a conscious, direct manner rather than automatically. Mindfulness has been associated with decreased levels of stress, anxiety, depression, improved mood, self-empathy, and empathy among medical students [48]. [49] found that components of mindfulness were positively associated with technical skills and the use of resources during simulation tasks, additionally [48] found that in a sample of medical students’ mindfulness was associated with lower levels of stress before beginning a task, and with stress being easier to manage during the task. [50] states that mindfulness has been found to be useful for preventing and managing stress and burnout, generating empathy and communication with patients in addition to being effective in treatment of anxiety.
2. Materials and Methods
Medical staff, comprising of MDs and health care workers (HCW),of the Shaare Zedek Medical Centre (Jerusalem, Israel) were asked to participate in an online survey regarding their quality of life as workers in the medical system. Between the months of September 2019 and July 2021, the survey was conducted in four different phases (T0-3). Overall, 1098 responses were recorded. Responses in which the participants had not fully completed the ProQOL questionnaire were removed. In addition, to ensure each participant had replied only once (i.e., independence of observations), the last four i.d. digits of the repliers were compared. Observations with the same four digits were marked as suspicious. In such cases we compared the rest of the demographic data. If they were identical, we randomly kept only one of the responses (while removing the others). Finally, the sample included 468 participants (T0: n = 295, T1: n = 80, T2: n= 51, T3: n = 42), of them 171 doctors and 297 HCW.
2.1. Materials
Demographics including gender, age, profession type (doctor or HCW), job type (daily or shift worker) and seniority (10+ years’ experience or under 10 years of experience).
The Professional Quality of Life questionnaire (ProQOL), a 30 item self-report measure of the positive and negative effects of working professionals each question answered on a Likert scale from 1 to 5.This measure includes 3 subscales comprised of 10 questions,that measure Compassion Satisfaction, CS ,burnout, and Secondary Traumatic Symptoms STS, The different subscales range for CS 0-22 low CS , 23-41 reasonable or medium CS and 42 and above high CS. For STS : 0-22 low STS , 23-41 Medium STS 42 and above high STS. For burnout 0-22 low burnout, 23-41 moderate burnout and 42 and above severe burnout.
The Mindful Attention Awareness scale (MAAS), a 5-scale, 15-item questionnaire designed to evaluate key aspects of mindfulness such as awareness and attention to the current moment.
Examples of questions: “I tend not to notice feelings of physical tension or discomfort until they really grab my attention.”, “It seems I am “running on automatic” without much awareness of what I’m doing.” [51].
Norms were not specified other than in a large U.S. adult sample the average MAAS score was 4.22 (S.D.=0.63); in a small cancer sample=4.27, S.D.=0.64.[52] and later [53] report on average scores for undergraduate students in the research were 3,85. Zen meditators scored an average of 4,38. So we assumed that 4 can be seen as average. So 1-3 low, 4 medium, 5-6 high mindfulness.
2.2. Statistical analysis
Analysis was performed for each subgroup of job & seniority separately to evaluate the phases effect within each subgroup on the ProQOL and Mindfulness..
The Shapiro & Wilk test was performed to verify if distribution of continuous variables is approximately normal, as all deviate from normal results are summarized using median & interquartile range [IQR]. Categorical variables a presented with counts and percentages.
To compare the differences in (ProQOL measures between the 4 phases a Kruskal Wallis test followed by Dunn’s post hoc test was performed
The ProQOL and mindfulness were categorized into 3 levels as detailed in the materials,to compare the distribution in each subgroup between phases a chi square test was applied
Stacked bar plots were used to represent the distribution of different categories of (ProQOL measures. The bars are stacked on top of each other, with the height of each bar representing the percentage of each category
To evaluate the correlation between ProQOL & Mindfulness measure the Pairwise Spearman correlations with 95% confidence intervals were calculated.
A two-side p value less than 0.05 was considered to define statistical significance.
Analyses were carried out using R-4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) and IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0.1.1 Armonk, NY: IBM Corp .
3. Results
3.1. Participant characteristics
A total of 171 doctors & 297 health care staff were included in the analysis.
The median age of doctors was 40 IQR[34-50] and other staff 38 [31-46] p=0.009. Among doctors 40% female as compared to 91% female among HCW p<0.001 (see table 1).

Table 1.
Participants characteristics.
| Doctor (N=171) | HCW (N=297) | Total (N=468) | P value | |
|---|---|---|---|---|
| Age | 0.0009 | |||
| Median (IQR) | 40.0 (34.0, 50.0) | 38.0 (31.0, 46.0) | 38.0 (32.0, 48.8) | |
| Gender | < 0.001 | |||
| Male | 103 (60.2%) | 27 (9.1%) | 130 (27.8%) | |
| Female | 68 (39.8%) | 270 (90.9%) | 338 (72.2%) | |
| Seniority | 0.7013 | |||
| ≤10 years | 91 (53.2%) | 152 (51.2%) | 243 (51.9%) | |
| > 10 years | 80 (46.8%) | 145 (48.8%) | 225 (48.1%) |
3.2. General effects of phases among doctors & HCW
3.2.1. Compassion satisfaction
Pre Covid-19 approximately 50% of doctors and HCW reported high level of CS (score 42+) and the rest reported reasonable CS (score 23-41).
Among doctors a significant reduction in High CS levels was noted from 45.8% pre covid to 26.7% at phase 3(p=0.028) , while among HCW the rate of high CS remained stable from 49.2% to 44.4% at phase 3 (p=0.7616) .( see Figure 1.a)
Among doctors the median CS significantly decreased from 41 [37-45] at T0 to 38 [34.5-41] p=0.0233 while among HCW the median remains stable with median of 41 at all phases.
3.2.2. Burnout
There was no significant effect of the pandemic phases on burnout. Approximately 70% of both doctors and health care reported moderate burnout levels (scores 23-41) with no significant difference over time. (see Figure 1.b)
3.2.3. STS levels
The majority of both doctors and health care reports low stress level, and none reported high stress levels. It is noticeable that doctors STS decreased from T0 to T1 26% to 13% and then there is an increase of moderate stress at phase 2 from 26% at T0 to 38%, at T2, Among HCW slight decrease was noted from 21% pre covid-19 to 11%at phase 3.whilst doctors STS increased again to somewhat higher STS : T0 26% to 38% at T2 and 33% at T3. (See Figure 1.c)
3.2.4. Mindfulness
Among doctors at T0 mindfulness was reported low at 23% and T1 reduced to 5% and over time the percent of Mindfulness level (5-6) pre covid as compared to only 8% at phase 3 (p=0.1049). Among 41% reported high mindfulness pre Covid-19 41% and similar percent 46% at phases 3 (p=0.7756) . (See Figure 1.d ). When comparing male (doctors mainly) to female ( HCW mainly) there was a significant difference where male dropped from high level of mindfulness of 45% at T0 to nil at T3. (p=0.003) (see Figure 3d.)
Figure 1.
ProQOL & mindfulness distribution at 4 phases per job (doctors & HCW). Fig 1.a CS, Fig1.b burnout, Fig 1.c STS, Fig 1.d Mindfulness. The colors represent green normal level, orange moderate level, dark red extreme level.
Figure 1.
ProQOL & mindfulness distribution at 4 phases per job (doctors & HCW). Fig 1.a CS, Fig1.b burnout, Fig 1.c STS, Fig 1.d Mindfulness. The colors represent green normal level, orange moderate level, dark red extreme level.
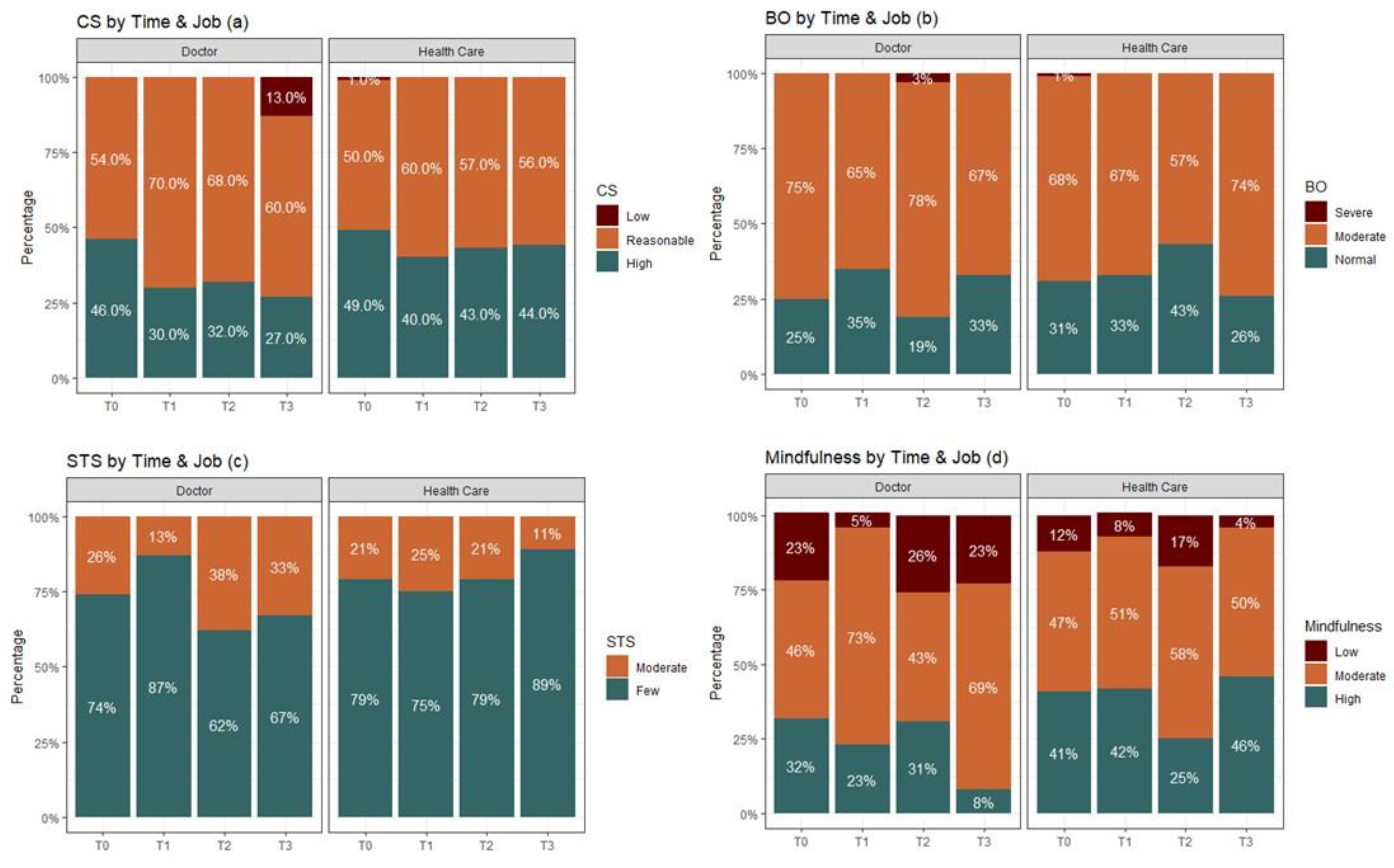
Figure 2.
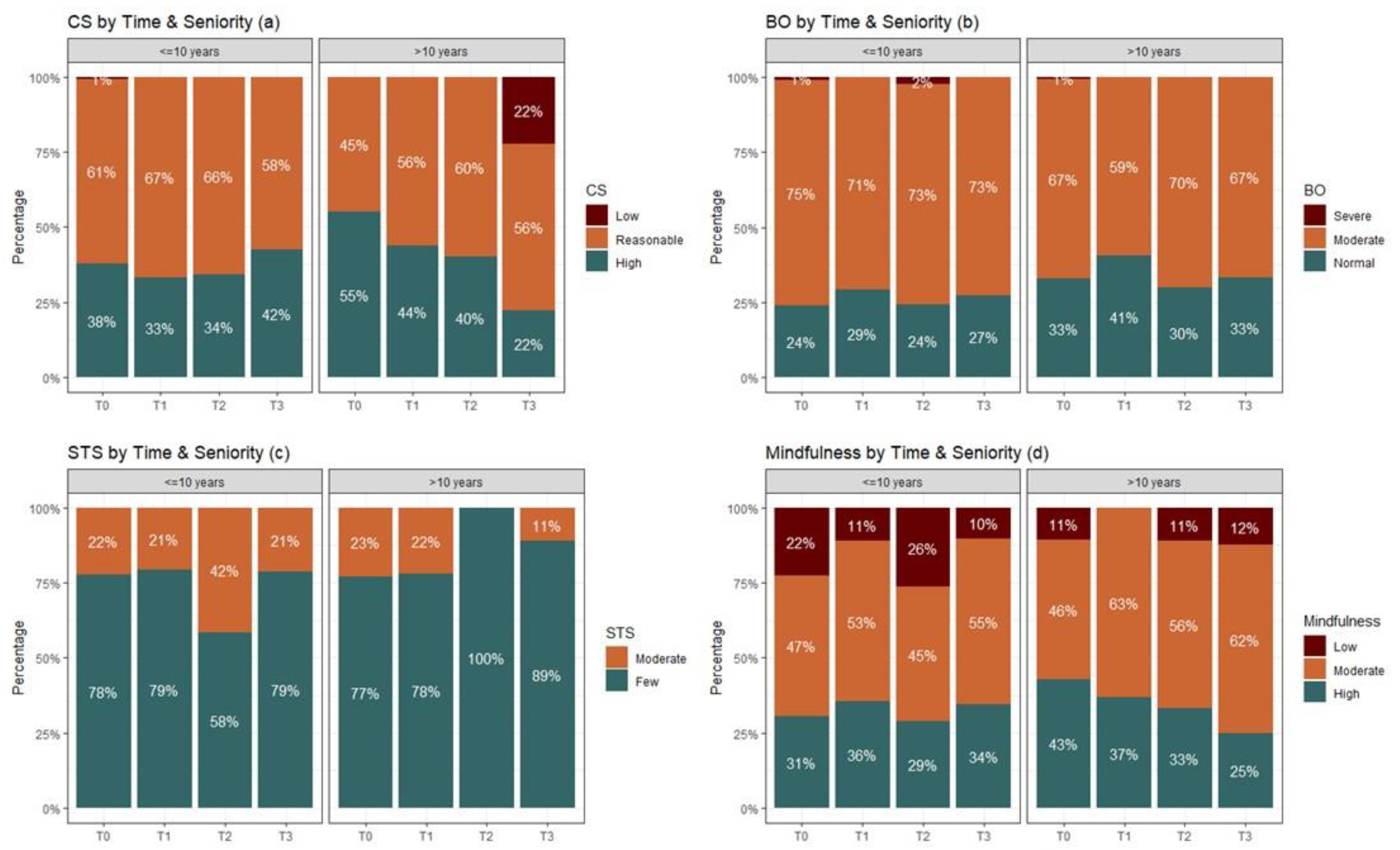
ProQOL & mindfulness distribution at 4 phases per seniority (<=10 years & >10 years). Fig 2.a CS, Fig2.b burnout, Fig 2.c STS, Fig 2d Mindfulness. The colors represent green normal level, orange moderate level, dark red extreme level.
Figure 2.
ProQOL & mindfulness distribution at 4 phases per seniority (<=10 years & >10 years). Fig 2.a CS, Fig2.b burnout, Fig 2.c STS, Fig 2d Mindfulness. The colors represent green normal level, orange moderate level, dark red extreme level.
3.3. Correlations between the ProQOL scales
For all ProQOL measures similar correlation were maintained during the pandemic phases and among doctors & HCW
3.3.1. CS
Strong negatively significantly correlated to burnout both among doctors and HCW r=-0.544 ,r= -0.601 respectively.
Mild (slight negative correlation to STS both among doctors and HCW r=-0.179 ,r= -0.149 respectively.
Mild (slight positive correlation to mindfulness both among doctors and HCW r=0.205 ,r= -0.280 respectively.
3.3.2. Burnout
Moderate positively significantly correlated to STS. among doctors and HCW r=0.475, and HCW r= 0.423 respectively.
Moderate negatively correlated to Mindfulness both among doctors and HCW r=-0.418 ,r= -0.380 respectively.
3.3.3. STS
Negatively significantly correlated to Mindfulness among doctors and HCW r=0.529 and moderate negative correlation among HS ,r= -0.337 respectively. (see table 2).
Table 2a.
Spearman pairwise correlations of mindfulness and ProQOL per job.
| Doctor | Health Care Workers | |||||||
|---|---|---|---|---|---|---|---|---|
| r | P value | 95% CI | r | P value | 95% CI | |||
| Lower | Upper | Lower | Upper | |||||
| CS - burnout | -0.544 | <0.001 | -0.644 | -0.425 | -0.601 | <0.001 | -0.671 | -0.520 |
| CS - STS | -0.179 | 0.019 | -0.325 | -0.025 | -0.149 | 0.010 | -0.262 | -0.033 |
| CS - Mindfulness | 0.205 | 0.009 | 0.048 | 0.353 | 0.280 | <0.001 | 0.162 | 0.390 |
| burnout - STS | 0.475 | <0.001 | 0.346 | 0.587 | 0.423 | <0.001 | 0.322 | 0.515 |
| burnout - Mindfulness | -0.418 | <0.001 | -0.540 | -0.277 | -0.380 | <0.001 | -0.481 | -0.269 |
| STS - Mindfulness | -0.529 | <0.001 | -0.634 | -0.404 | -0.337 | <0.001 | -0.442 | -0.223 |
Table 2b.
Spearman pairwise correlations of mindfulness and ProQOL per Seniority.
| Seniority | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1 <=10 | 2 >10 | |||||||
| r | P value | 95% CI | r | P value | 95% CI | |||
| Lower | Upper | Lower | Upper | |||||
| CS - burnout | -0.571 | <0.001 | -0.652 | -0.476 | -0.575 | <0.001 | -0.659 | -0.478 |
| CS - STS | -0.235 | <0.001 | -0.354 | -0.109 | -0.052 | 0.437 | -0.185 | 0.083 |
| CS - Mindfulness | 0.299 | <0.001 | 0.171 | 0.418 | 0.187 | 0.007 | 0.048 | 0.320 |
| burnout - STS | 0.436 | <0.001 | 0.325 | 0.536 | 0.436 | <0.001 | 0.320 | 0.539 |
| burnout - Mindfulness | -0.439 | <0.001 | -0.542 | -0.323 | -0.356 | <0.001 | -0.473 | -0.226 |
| STS - Mindfulness | -0.413 | <0.001 | -0.519 | -0.294 | -0.413 | <0.001 | -0.523 | -0.289 |
For doctors, the difference between over 10 years and under 10 years on STS showed that more doctors with less than 10 years reported more STS p=0.008.
Figure 3.
ProQOL & mindfulness distribution at 4 phases per Gender difference. Fig 3.a CS, Fig3.b burnout, Fig 3.c STS, Fig 3d Mindfulness.
Figure 3.
ProQOL & mindfulness distribution at 4 phases per Gender difference. Fig 3.a CS, Fig3.b burnout, Fig 3.c STS, Fig 3d Mindfulness.
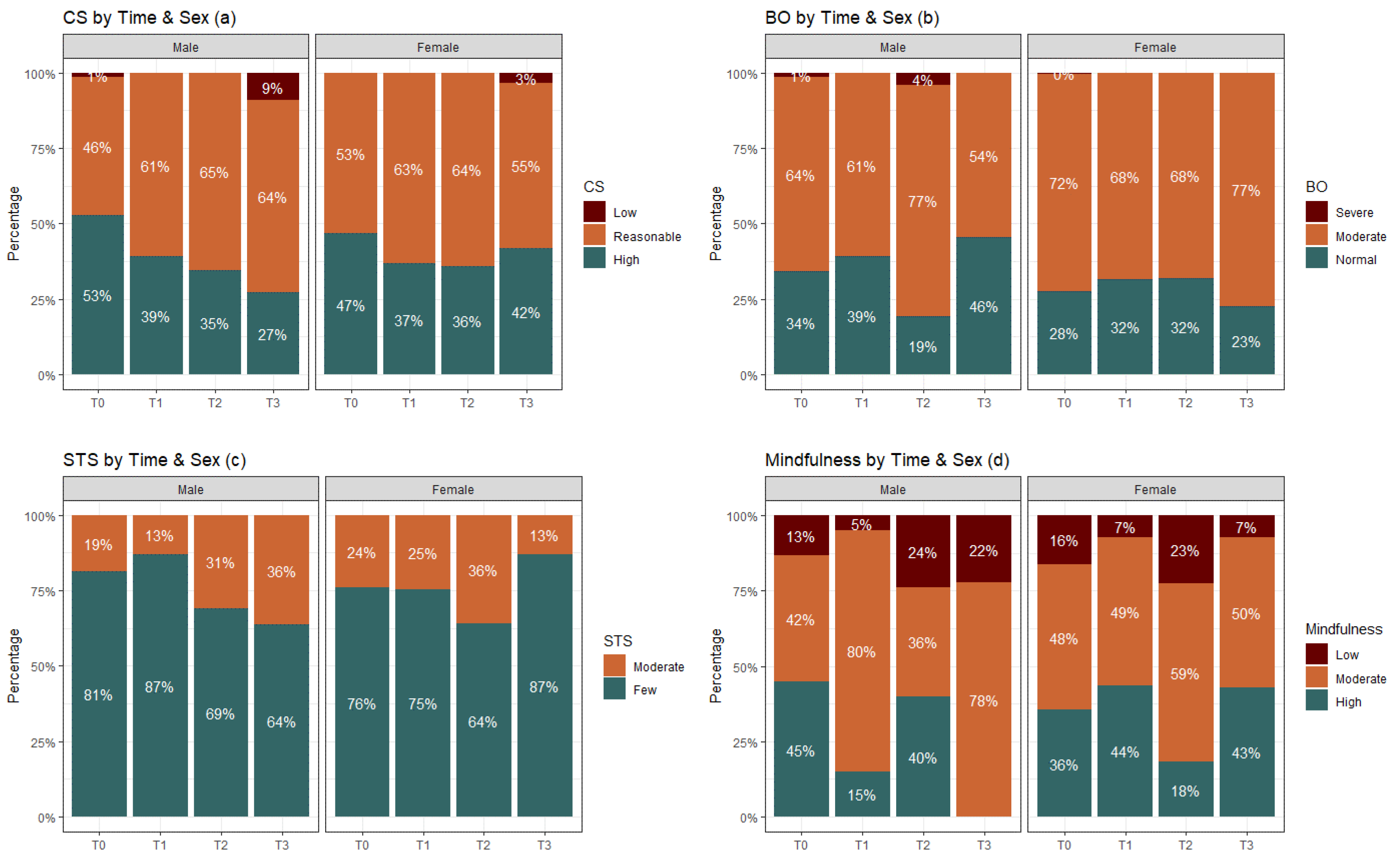
The difference in mindfulness between male and female (in our case doctors and HCW) indicate that for male compared to female the level of high mindfulness dropped p=0.003.
4. Discussion
Overall, the current study found that compassion satisfaction was negatively correlated with burnout, and mindfulness was negatively correlated with burnout and secondary traumatic stress. The impact of time on compassion satisfaction revealed a significant difference between T0 (pre Covid-19) and the other times, with T0 being the highest for doctors and thereafter decreasing, while for health care workers (HCW) compassion satisfaction remained stable. Additionally, an impact of time on mindfulness was found. Doctor's high levels of mindfulness dropped from T0 to T3 whilst for HCW it regains its T0 level at T3, returning to high levels of mindfulness.
For doctors, there is a noticeable decrease in CS from the time before COVID-19 to the first lockdowns and onwards, and they maintain this level throughout the lockdowns. However, in measurement number three, which took place immediately after the start of the vaccinations, but also coincided with a significant increase in the number of dead (from 2281 deceased to 3813 deceased and an almost double- increase in confirmed cases from 297,526 to 523,931) , a further decrease in the feeling of satisfaction from compassion is evident, and moreover, for the first time, a group of low CS also appears. It is possible that we are seeing a manifestation of attrition here. In the HCW group there is no change in the CS level throughout all the measurements.
The fluctuations in the burnout level are maintained throughout the course of the pandemic. At the same time, from the histograms, it appears that the attrition levels among doctors are higher compared to HCW, especially during the second lockdown. Perhaps when the realization that COVID-19 is not an event limited in time and the number of deaths in Israel and in the world brought awareness to the severity of the pandemic (a phase known as the disillusionment stage). In Israel it increased almost 10 times from 289 deceased to 2281 deceased.
The same trend is maintained in the STS levels, throughout the lockdowns, but again it seems that specifically among the doctors there are higher markers of symptoms of mental stress starting from the second closure compared to HCW.
This phenomenon also repeats itself in mindfulness when doctors in the third lockdown have a sharp drop in the high levels of mindfulness (theoretically at least the protective level) from a pre-Covid situation where 32% of the doctors reported a high level of mindfulness dropping to only 8% in the high level during the third lockdown.
This picture, even if it does not reach statistical significance (see the limitations of the study), points to the group of doctors as the one that reacted more acutely compared to the rest of the HCW. This is a unique picture, since in most studies the HCWs were found to have a higher severity of reactions.
The difference in seniority was seen in the STS where doctors with less than 10 years showed more STS than those with 10 years and above (p=0.008) but the fact that it did not play a difference in the other measures maybe an indication that COVID 19 met both senior and junior staff unprepared and ignorant to what are the features, course of development and potential remedy to COVID 19.
These results could be due to what is called the disillusionment phase in the known trajectories following major and prolonged crises. In the immediate aftermath of a disaster there is an initial phase of high energy used for survival, rescue, and repair, altruism is high in this stage among aid workers. Over time, limits of resources become apparent, and people become fatigued and discouraged by the enormous demands that are needed for restoration [54]. This could be reflected in the lowering levels of mindfulness and CS seen over time.
Our study suggests that doctors, mainly men, showed more signs of fatigue in the different time phases than nurses, mostly women it reached a statistical level in mindfulness where male (doctors mainly) level of high mindfulness dropped from 45% at T0 to nil. Whereas for female, most of the HCW ,high level of mindfulness at T0 is 45% and at T3 it was 36% This is a novel result since other research during the pandemic found that women were reporting a larger impact psychologically when compared to men [55,56,57]. Only studies mentioned doctors' worse reaction, high emotional exhaustion than nursing staff [58]. Studies found that the majority of HCWs show negative impact to their mental health during this challenging time [31,59], indicating that nurses showed more negative effects compared to doctors [31,55]. Other studies found that women have higher emotional sensitivity when they are presented with aversive situations, and that women’s moral reasoning is directed toward others [60]. This may also reflect social gender norms. [61] states that masculine social norms of being strong, unemotional, pragmatic, and independent don’t allow masculine men to care for themselves during times of distress, leading to low levels of self-compassion compared to qualities related to nurturing, caring, and self-sacrifice which were associated with feminine gender norms, which may have led women to put patients’ needs before their own, more so than men, generating higher levels of CS. Studies have shown that men who follow masculine gender norms show heightened psychological distress [61]. Using post hoc interview with the team another possible explanation may be possible, that is the normal delineation of role and procedures carried by medical doctors and nursing staff was nullified in the case of COVID 19 patient care. Whereas nursing staff are used to care and do routine nursing jobs, doctors found themselves facing nonspecific care tasks very similar to the nursing staff, no heroic medicine, and a rather passive position of waiting and seeing. This is supported by the latest Ministry of Health survey of burnout following Covid in Israeli hospitals 42% of the doctors (mostly men) reported above 4 level of burnout (on a 0-5 scale) whereas only 36% of nursing staff (mostly women) reported above 4 level of burnout.
Prior experience with widespread events such as the COVID-19 pandemic emphasized that support for HCWs enables them to be aware and elaborate upon their emotions and this in turn leads to more emphatic communication with patients in addition to higher adeptness and focus during stressful times [59]. Compared to doctors, nurses prioritize having a supportive supervisor and prefer team-based work environments [62] which may lead to nurses having a wider support system. [59] suggest that a lack of emotional recognition stemming from improper support may influence HCWs own sense of wellbeing, leading to disengagement, distress, and burnout. One other possible explanation to our findings may stem from the fact that doctors have higher status in the healthcare system, which is reflected in their workload, work schedule and the challenges they are presented with. Compared to doctors, nurses are often seen as having a lower status or less power. Since they have less control over many aspects of their work, they are likely to experience different challenges when it comes to compassion. This may suggest that nurses experience overall less barriers to their compassion compared to doctors [63]. Perhaps doctors are more symptomatic since they are the professionals that make the final decisions [55]. Moreover, as stated earlier, preparedness for dealing with the COVID-19 pandemic played an important factor. Research by [64] found negative results concerning the psychological health of frontline doctors in Jordan. Only 28.2% of doctors in the study felt satisfied with the infection control policy at their institution, and only 19.8% felt safe at their workplace. More than 90% of doctors were concerned about transmitting the virus to noninfected patients or their families. This study also found that the more knowledge a doctor has about the virus, the higher anxiety was regarding dealing with cases. In the phases of Covid 19 that our study covered, information on treatment protocol and virus containment methods were lacking and at the same time constant changes of regulation and protocols from MOH were sent daily, adding to the confusion and helplessness of those who usually see themselves as the leaders and source of authority and knowledge in the wards.
4.1. Limitations
The main limitation of this study is the different responses we received in the 4 phases. It is mostly to do with the pandemic itself that is whereas during the pre-Covid, staff were relatively in their routine and participation was rather easy, as time passed, the workload and distress have risen under Covid we can see less participation, in some cases due to fatigue in other because hospital staff were overwhelmed with tasks and were less responsive. The overall size of responses in the different phases made it difficult to achieve clear results that with a bigger sample may reach statistical significance.
4.2. Recommendations
We recommend continuing and measure the long term effect of Covid on doctors and Health Care Workers. Once Covid 19 subsided, most hospitals went very quickly to "business as usual " into their usual overload of work with very little time for processing, support and self-nurturing tools. Developing in service programs to alleviate distress burnout on the one hand but as importantly to train in mindfulness and other self-nurturing and resilience building methods is crucial.
4.3. Contribution to the field
Our main contribution is the finding that male doctors are vulnerable and in the current study more than the Health Care Workers mainly nursing staff and female. This sheds a light on a very sensitive issue of MDs and specifically male MDs who find it hard to receive help.
Author Contributions
Designing the study, coordinating the collection of data during Covid (when hospitals were out of bound for outsiders) advised on the computation and partner in the discussion, S.M. (deputy medical manager of the Sharie Zedek medical center); part of the designing team and the original statistician, I.D.; literature review and editing, R.E.; head of the team, advisor on design and statistics and the writer of the discussion, M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We wish to thank the staff of Sharie Zedek Medical center in Jerusalem for taking the time even under the stress of COVID 19 and for endurance and compassionate support for the many patients and families they cared for during COVID 19. Special thanks to Mr. David Mizrachi for hos outstanding help.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moreno-Mulet, C.; Sansó, N.; Carrero-Planells, A.; López-Deflory, C.; Galiana, L.; García-Pazo, P.; Borràs-Mateu, M.M.; Miró-Bonet, M. The Impact of the COVID-19 Pandemic on ICU Healthcare Professionals: A Mixed Methods Study. Int. J. Environ. Res. Public. Health 2021, 18, 9243. [Google Scholar] [CrossRef] [PubMed]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational Burnout Syndrome and Post-Traumatic Stress among Healthcare Professionals during the Novel Coronavirus Disease 2019 (COVID-19) Pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; Santos, J.A.A. Fear of COVID-19, Psychological Distress, Work Satisfaction and Turnover Intention among Frontline Nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Arpacioglu, S.; Gurler, M.; Cakiroglu, S. Secondary Traumatization Outcomes and Associated Factors Among the Health Care Workers Exposed to the COVID-19. Int. J. Soc. Psychiatry 2021, 67, 84–89. [Google Scholar] [CrossRef]
- Sunjaya, D.K.; Herawati, D.M.D.; Siregar, A.Y.M. Depressive, Anxiety, and Burnout Symptoms on Health Care Personnel at a Month after COVID-19 Outbreak in Indonesia. BMC Public Health 2021, 21, 227. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Pérez, V.; Arango, C. Psychiatry in the Aftermath of COVID-19. Rev. Psiquiatr. Salud Ment. 2020, 13, 105–110. [Google Scholar] [CrossRef]
- Selman, L.E.; Chao, D.; Sowden, R.; Marshall, S.; Chamberlain, C.; Koffman, J. Bereavement Support on the Frontline of COVID-19: Recommendations for Hospital Clinicians. J. Pain Symptom Manage. 2020, 60, e81–e86. [Google Scholar] [CrossRef]
- Wallace, C.L.; Wladkowski, S.P.; Gibson, A.; White, P. Grief During the COVID-19 Pandemic: Considerations for Palliative Care Providers. J. Pain Symptom Manage. 2020, 60, e70–e76. [Google Scholar] [CrossRef]
- Killikelly, C.; Lenferink, L.I.M.; Xie, H.; Maercker, A. Rapid Systematic Review of Psychological Symptoms in Health Care Workers COVID-19. J. Loss Trauma 2021, 26, 638–655. [Google Scholar] [CrossRef]
- Manzano García, G.; Ayala Calvo, J.C. The Threat of COVID-19 and Its Influence on Nursing Staff Burnout. J. Adv. Nurs. 2021, 77, 832–844. [Google Scholar] [CrossRef]
- Dobson, H.; Malpas, C.B.; Burrell, A.J.; Gurvich, C.; Chen, L.; Kulkarni, J.; Winton-Brown, T. Burnout and Psychological Distress amongst Australian Healthcare Workers during the COVID-19 Pandemic. Australas. Psychiatry 2021, 29, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Ferry, A.V.; Wereski, R.; Strachan, F.E.; Mills, N.L. Predictors of UK Healthcare Worker Burnout during the COVID-19 Pandemic. QJM Int. J. Med. 2021, 114, 374–380. [Google Scholar] [CrossRef]
- Mokhtari, R.; Moayedi, S.; Golitaleb, M. COVID-19 Pandemic and Health Anxiety among Nurses of Intensive Care Units. Int. J. Ment. Health Nurs. 2020, 29, 1275–1277. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Shahin, S.Y.; Bugshan, A.S.; Almulhim, K.S.; AlSharief, M.S.; Al-Dulaijan, Y.A.; Siddiqui, I.; al-Qarni, F.D. Knowledge of Dentists, Dental Auxiliaries, and Students Regarding the COVID-19 Pandemic in Saudi Arabia: A Cross-Sectional Survey. BMC Oral Health 2020, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Smallwood, N.; Willis, K. Mental Health among Healthcare Workers during the COVID -19 Pandemic. Respirology 2021, 26, 1016–1017. [Google Scholar] [CrossRef] [PubMed]
- Orrù, G.; Marzetti, F.; Conversano, C.; Vagheggini, G.; Miccoli, M.; Ciacchini, R.; Panait, E.; Gemignani, A. Secondary Traumatic Stress and Burnout in Healthcare Workers during COVID-19 Outbreak. Int. J. Environ. Res. Public. Health 2021, 18, 337. [Google Scholar] [CrossRef]
- Da Silva Neto, R.M.; Benjamim, C.J.R.; De Medeiros Carvalho, P.M.; Neto, M.L.R. Psychological Effects Caused by the COVID-19 Pandemic in Health Professionals: A Systematic Review with Meta-Analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110062. [Google Scholar] [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The Prevalence of Anxiety and Depression among Healthcare Workers during the COVID-19 Pandemic: An Umbrella Review of Meta-Analyses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to Sars-Cov-2 (Covid-19). Int. J. Environ. Res. Public. Health 2020, 17, 6180. [Google Scholar] [CrossRef]
- Danet Danet, A. Psychological Impact of COVID-19 Pandemic in Western Frontline Healthcare Professionals. A Systematic Review. Med. Clínica Engl. Ed. 2021, 156, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Cipolotti, L.; Chan, E.; Murphy, P.; Harskamp, N.; Foley, J.A. Factors Contributing to the Distress, Concerns, and Needs of UK Neuroscience Health Care Workers during the COVID-19 Pandemic. Psychol. Psychother. Theory Res. Pract. 2021, 94, 536–543. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological Distress, Coping Behaviors, and Preferences for Support among New York Healthcare Workers during the COVID-19 Pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maiorano, T.; Vagni, M.; Giostra, V.; Pajardi, D. COVID-19: Risk Factors and Protective Role of Resilience and Coping Strategies for Emergency Stress and Secondary Trauma in Medical Staff and Emergency Workers—An Online-Based Inquiry. Sustainability 2020, 12, 9004. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, Anxiety, Stress Levels of Physicians and Associated Factors in Covid-19 Pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Man, M.A.; Toma, C.; Motoc, N.S.; Necrelescu, O.L.; Bondor, C.I.; Chis, A.F.; Lesan, A.; Pop, C.M.; Todea, D.A.; Dantes, E.; et al. Disease Perception and Coping with Emotional Distress During COVID-19 Pandemic: A Survey Among Medical Staff. Int. J. Environ. Res. Public. Health 2020, 17, 4899. [Google Scholar] [CrossRef]
- Romero, C.S.; Delgado, C.; Catalá, J.; Ferrer, C.; Errando, C.; Iftimi, A.; Benito, A.; De Andrés, J.; Otero, M. ; The PSIMCOV group* COVID-19 Psychological Impact in 3109 Healthcare Workers in Spain: The PSIMCOV Group. Psychol. Med. 2022, 52, 188–194. [Google Scholar] [CrossRef]
- Dosil Santamaría, M.; Ozamiz-Etxebarria, N.; Redondo Rodríguez, I.; Jaureguizar Albondiga-Mayor, J.; Picaza Gorrochategi, M. Psychological Impact of COVID-19 on a Sample of Spanish Health Professionals. Rev. Psiquiatr. Salud Ment. Engl. Ed. 2021, 14, 106–112. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Stojanov, A.; Malobabic, M.; Milosevic, V.; Stojanov, J.; Vojinovic, S.; Stanojevic, G.; Stevic, M. Psychological Status of Patients with Relapsing-Remitting Multiple Sclerosis during Coronavirus Disease-2019 Outbreak. Mult. Scler. Relat. Disord. 2020, 45, 102407. [Google Scholar] [CrossRef]
- Franza, F.; Basta, R.; Pellegrino, F.; Solomita, B.; Fasano, V. The Role of Fatigue of Compassion, Burnout and Hopelessness in Healthcare: Experience in the Time of COVID-19 Outbreak. Psychiatr. Danub. 2020, 32, 10–14. [Google Scholar]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public. Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among Healthcare Professionals during COVID-19 Pandemic: A Cross-Sectional Study. Int. Arch. Occup. Environ. Health 2021, 94, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Dimitriu, M.C.T.; Pantea-Stoian, A.; Smaranda, A.C.; Nica, A.A.; Carap, A.C.; Constantin, V.D.; Davitoiu, A.M.; Cirstoveanu, C.; Bacalbasa, N.; Bratu, O.G.; et al. Burnout Syndrome in Romanian Medical Residents in Time of the COVID-19 Pandemic. Med. Hypotheses 2020, 144, 109972. [Google Scholar] [CrossRef]
- Cotel, A.; Golu, F.; Pantea Stoian, A.; Dimitriu, M.; Socea, B.; Cirstoveanu, C.; Davitoiu, A.M.; Jacota Alexe, F.; Oprea, B. Predictors of Burnout in Healthcare Workers during the COVID-19 Pandemic. Healthcare 2021, 9, 304. [Google Scholar] [CrossRef]
- Chor, W.P.D.; Ng, W.M.; Cheng, L.; Situ, W.; Chong, J.W.; Ng, L.Y.A.; Mok, P.L.; Yau, Y.W.; Lin, Z. Burnout amongst Emergency Healthcare Workers during the COVID-19 Pandemic: A Multi-Center Study. Am. J. Emerg. Med. 2021, 46, 700–702. [Google Scholar] [CrossRef]
- Etesam, F.; Akhlaghi, M.; Vahabi, Z.; Akbarpour, S.; Sadeghian, M.H. Comparative Study of Occupational Burnout and Job Stress of Frontline and Non-Frontline Healthcare Workers in Hospital Wards during COVID-19 Pandemic. Iran. J. Public Health 2021. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Hasan, O.; Dyrbye, L.N.; Sinsky, C.; Satele, D.; Sloan, J.; West, C.P. Changes in Burnout and Satisfaction With Work-Life Balance in Physicians and the General US Working Population Between 2011 and 2014. Mayo Clin. Proc. 2015, 90, 1600–1613. [Google Scholar] [CrossRef]
- Duarte, I.; Teixeira, A.; Castro, L.; Marina, S.; Ribeiro, C.; Jácome, C.; Martins, V.; Ribeiro-Vaz, I.; Pinheiro, H.C.; Silva, A.R.; et al. Burnout among Portuguese Healthcare Workers during the COVID-19 Pandemic. BMC Public Health 2020, 20, 1885. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion Fatigue, Burnout, Compassion Satisfaction and Perceived Stress in Healthcare Professionals during the COVID-19 Health Crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef]
- Dwyer, M.; Alt, M.; Brooks, J.; Katz, H.; Poje, A. Burnout and Compassion Satisfaction: Survey Findings of Healthcare Employee Wellness During COVID-19 Pandemic Using ProQOL. Kans. J. Med. 2021, 14, 121–127. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Carmona-Rega, M.I.; Sánchez-Ruiz, M.J.; Ortega-Galán, Á.M. Professional Quality of Life, Self-compassion, Resilience, and Empathy in Healthcare Professionals during COVID-19 Crisis in Spain. Res. Nurs. Health 2021, 44, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Van Laar, D.; Edwards, J.A.; Easton, S. The Work-Related Quality of Life Scale for Healthcare Workers: WRQoL Scale for Healthcare Workers. J. Adv. Nurs. 2007, 60, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Opollo, J.G.; Gray, J.; Spies, L.A. Work-Related Quality of Life of Ugandan Healthcare Workers: Work-Related Quality of Life in Uganda. Int. Nurs. Rev. 2014, 61, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Schaufeli, W.B.; Leiter, M.P.; Taris, T.W. Work Engagement: An Emerging Concept in Occupational Health Psychology. Work Stress 2008, 22, 187–200. [Google Scholar] [CrossRef]
- Aquino, K.; Thau, S. Workplace Victimization: Aggression from the Target’s Perspective. Annu. Rev. Psychol. 2009, 60, 717–741. [Google Scholar] [CrossRef]
- Łoś, K.; Chmielewski, J.; Cebula, G.; Bielecki, T.; Torres, K.; Łuczyński, W. Relationship between Mindfulness, Stress, and Performance in Medical Students in Pediatric Emergency Simulations. GMS J. Med. Educ. 384Doc78 2021. [Google Scholar] [CrossRef]
- Chmielewski, J.; Łoś, K.; Łuczyński, W. Mindfulness in Healthcare Professionals and Medical Education. Int. J. Occup. Med. Environ. Health 2021, 34, 1–14. [Google Scholar] [CrossRef]
- Sanders, C. The Role of Mindfulness in Medical Practice. Pract. Manag. 2019, 29, 34–36. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The Benefits of Being Present: Mindfulness and Its Role in Psychological Well-Being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Brown, K.W. Validation of the Mindful Attention Awareness Scale in a Cancer Population. J. Psychosom. Res. 2005, 58, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.; Lamis, D.A.; Bagge, C.L.; Freedenthal, S.; Barnes, S.M. The Mindful Attention Awareness Scale: Further Examination of Dimensionality, Reliability, and Concurrent Validity Estimates. J. Pers. Assess. 2016, 98, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Johanson, M.M.; Guchait, P. Employees Intent to Leave: A Comparison of Determinants of Intent to Leave versus Intent to Stay. Int. J. Hosp. Manag. 2009, 28, 374–381. [Google Scholar] [CrossRef]
- Dosil, M.; Ozamiz-Etxebarria, N.; Redondo, I.; Picaza, M.; Jaureguizar, J. Psychological Symptoms in Health Professionals in Spain After the First Wave of the COVID-19 Pandemic. Front. Psychol. 2020, 11, 606121. [Google Scholar] [CrossRef]
- Hashem, Z.; Zeinoun, P. Self-Compassion Explains Less Burnout Among Healthcare Professionals. Mindfulness 2020, 11, 2542–2551. [Google Scholar] [CrossRef]
- Mohammadpour, M.; Ghorbani, V.; Khoramnia, S.; Ahmadi, S.M.; Ghvami, M.; Maleki, M. Anxiety, Self-Compassion, Gender Differences and COVID-19: Predicting Self-Care Behaviors and Fear of COVID-19 Based on Anxiety and Self-Compassion with an Emphasis on Gender Differences. Iran. J. Psychiatry 2020. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Burnout Syndrome Among Hospital Healthcare Workers During the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 579563. [Google Scholar] [CrossRef]
- Barello, S.; Graffigna, G. Caring for Health Professionals in the COVID-19 Pandemic Emergency: Toward an “Epidemic of Empathy” in Healthcare. Front. Psychol. 2020, 11, 1431. [Google Scholar] [CrossRef]
- Mercadillo, R.E.; Díaz, J.L.; Pasaye, E.H.; Barrios, F.A. Perception of Suffering and Compassion Experience: Brain Gender Disparities. Brain Cogn. 2011, 76, 5–14. [Google Scholar] [CrossRef]
- Yarnell, L.M.; Neff, K.D.; Davidson, O.A.; Mullarkey, M. Gender Differences in Self-Compassion: Examining the Role of Gender Role Orientation. Mindfulness 2019, 10, 1136–1152. [Google Scholar] [CrossRef]
- Degeling, P.; Kennedy, J.; Hill, M. Mediating the Cultural Boundaries between Medicine, Nursing and Management - the Central Challenge in Hospital Reform. Health Serv. Manage. Res. 2001, 14, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Dev, V.; Fernando, A.T.; Kirby, J.N.; Consedine, N.S. Variation in the Barriers to Compassion across Healthcare Training and Disciplines: A Cross-Sectional Study of Doctors, Nurses, and Medical Students. Int. J. Nurs. Stud. 2019, 90, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Suleiman, A.; Bsisu, I.; Guzu, H.; Santarisi, A.; Alsatari, M.; Abbad, A.; Jaber, A.; Harb, T.; Abuhejleh, A.; Nadi, N.; et al. Preparedness of Frontline Doctors in Jordan Healthcare Facilities to COVID-19 Outbreak. Int. J. Environ. Res. Public. Health 2020, 17, 3181. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



