
Submitted:
26 June 2023
Posted:
27 June 2023
You are already at the latest version
Abstract
In May 2022, WHO reported an outbreak of Mpox in several European countries which were previously Mpox free. Mpox (formerly known as monkeypox) is a zoonotic viral disease endemic in Central and West Africa. The sudden emergence of Mpox outside Africa and its subsequent rapid spread lead the WHO to declare the outbreak as Public Health Emergency of International Concern. As of May 15, 2023, a total of 87,704 confirmed cases and 140 deaths had been reported from 111 countries and territories worldwide. Looking back on this outbreak one year later, several important questions have arisen. Here, we address these questions using the classic five Ws: What, When, Where, Who and Why? We discuss these questions and outline what needs to be done to prevent, or at least minimize, outbreaks from emerging and re-emerging viral infection.
Keywords:
Emerging and reemerging viral infections
; Mpox
; Mpox virus
; 5 Ws
1. Introduction
Emerging and re-emerging viral infections have plagued humans for centuries. They remain a constant threat and a stark reminder to our weakness in preventing outbreaks from these infections [1]. The 1918 influenza pandemic, the so called ‘Spanish Flu,’ and the more recent COVID-19 pandemic, serve as striking examples of the impact these infections can have on a society. It is estimated that the Spanish Flu killed in excess of 50 million people, whilst the COVID-19 killed almost 7 million before it was brought under control [2]. We had hardly recovered from COVID-19 pandemic, when in early May 2022, another virus re-emerged; the monkeypox virus (MPOX virus) [3,4,5].
Monkeypox virus was not a new virus, but its sudden emergence and rapid spread in countries not previously known to have the virus was alarming and prompted the WHO to declare the outbreak as Public Health Emergency of International Concern (PHEIC) [6]. In an effort to control the outbreak, WHO issued numerous recommendations, including, enhance disease surveillance, diagnosis and reporting, training and education, engagement and awareness campaigns targeting high risk groups, and prophylactic use of smallpox vaccine for high risk groups [7,8]. These measures helped in eventually controlling and ending the outbreak. Monkeypox, renamed Mpox by WHO, peaked in August 2022 and thereafter gradually declined, eventually leading to the lifting of the 10-month long Public Health Emergency on 11th May 2023 (Figure 1a) [9]. In this concise review, we address the re-emergence of the Mpox pandemic in the context of the 5 Ws, namely, What is Mpox? When did Mpox make its debut? Where did Mpox spread to? Who was most at risk of Mpox? and finally, Why did Mpox reemerged? By discussing these questions, we hope to reflect on what we have learnt from this outbreak and how we can be better prepared in the future.
2. What is Mpox?
Monkeypox (Mpox) is a viral disease caused by the monkeypox virus (Mpox virus) [11]. Mpox virus is a large, enveloped, dsDNA virus belonging to the genus Orthopoxvirus from the Poxviridae family. The most notable members of this family that can cause disease in humans, include, variola virus, vaccinia virus, molluscum contagiosum virus, orf virus, cowpox, and Mpox virus [12]. A common feature of these viruses is that they typically cause some form of skin infection, but with varying presentation and degree of severity. Moreover, with the exceptions of variola, the cause of the deadly smallpox, and molluscum contagiosum virus, the cause of molluscum contagiosum [12], all others commonly infect animals, with man being an incidental host [13,14].
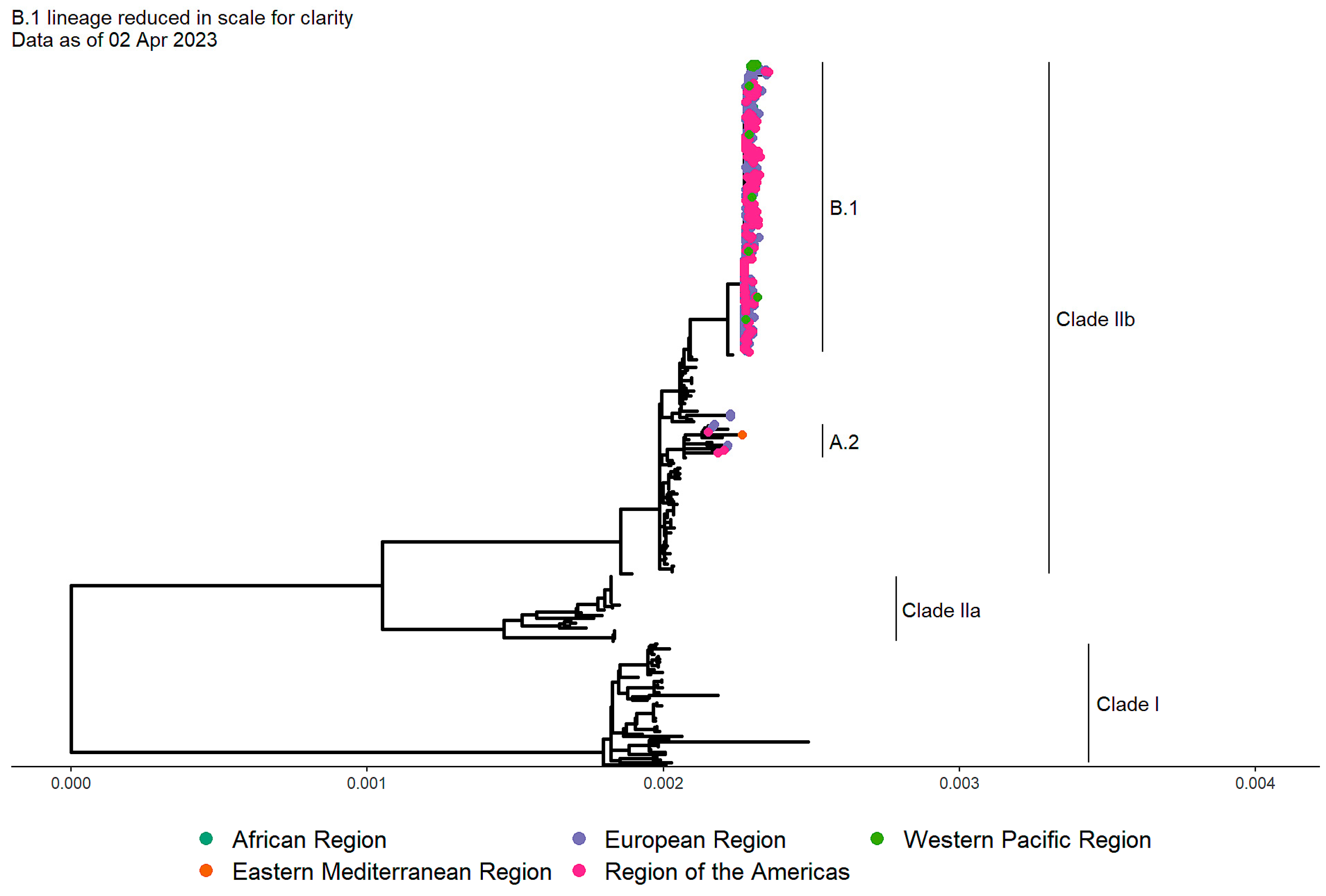
Mpox is a relatively uncommon zoonotic disease with many clinical features similar to human smallpox, but typically milder [11]. The disease was first identified in laboratory monkeys and later discovered to also affect humans. Contrary to its name, neither monkeys or humans are the natural reservoir for the virus. The virus has been shown to infects a range of different animals, particularly rodents found in countries in Central and West Africa [15,16]. Two stains of Mpox virus have been identified to be circulating in different animal populations in the endemic countries in Africa; Congo Basin clade, and the West African clade. These clades have recently been renamed as Clade I and Clade II respectively [17]. Clade II is further divided into two subclades referred to as IIa and IIb. In the 2022 outbreak, sequence analysis of nearly 700 isolates from different countries around the world, revealed that all the sequences belonged to Clade IIb (Figure 2) [10]. It appears that this outbreak was not due to multiple zoonotic spillover events, but primarily due the sustained human-to-human transmission of lineage B.1 of the Clade IIb virus [10]. Although both clades, I and II, can be transmitted to humans through close contact with infected animals, or through consumption of their meat [18,19], Clade I appears to be associated with more severe diseases [20,21,22]. Person to person transmission usually occurs through close contact with infected bodily fluids, respiratory droplets, or contact with contaminated objects such as bedding or clothing [23,24,25]. In endemic countries, small isolated outbreaks are frequently reported. In most cases, these outbreaks are linked to contact with animals [24,26].
Although symptoms of Mpox can vary from person to person, most individuals typically present with prodromal symptoms of fever, headache, myalgias and lymphadenopathy. These symptoms generally last for 1-4 days before the appearance of a rash [27,28]. The rash may appear on the face, mouth, palms of the hands, soles of the feet, groin, genital and/or anal regions. Mpox can be confused with varicella (chickenpox) [29]. However, the latter is primarily a childhood disease in which the patients do not normally develop lymphadenopathy and the appearance of the rash on the palms and soles is rare [30]. The rash in Mpox progresses through different stages, from macular-papular to vesicular-pustular and finally to crusts (scabs), before falling off [31]. The disease is usually self-limited, with symptoms lasting for 2-4 weeks. Individual remaining infectious from the onset of clinical symptoms until the scabs fall off [11,31]. In healthy immunocompetent individuals, Mpox complications are uncommon, but can include rectal or perianal pain, secondary bacterial skin infections, pneumonia, and severe ocular problems [28,32].
3. When did Mpox make its debut?
Monkeypox was first identified in 1958 in a laboratory in Copenhagen, Denmark in monkeys imported from Singapore [33]. Subsequently, several other laboratories, including from the US, the Netherlands, and France reported outbreaks of Mpox in captive primates [34,35,36,37]. The outbreak in Philadelphia in 1959 was particularly notable since it involved a colony of some 2000 monkeys, at least 10% of which contracted the infection [35]. It was suspected that virus originated from a source in Africa, and subsequent studies confirmed that the virus was indeed present in some countries in Africa. Assessment of the prevalence of the virus in small mammals in the Democratic Republic of Congo (DRC), indicated that several animal species, such as the African striped squirrel, Lorrain dormouse, Emin's pouched rat, Red-legged sun squirrel, Rufous-nosed rat, and the Four-toed elephant shrew, were positive for anti-orthopoxvirus IgG antibodies [26,38]. Although the natural reservoir of Mpox virus still remains unknown, rodents are believed to be the most likely candidates [38]. During epidemiologic and clinical studies of Mpox virus in the DRC, other animals such as the Redless tree squirrel, Congo rope squirrel, and wild boar were also found to be positive [39,40]. Moreover, several different species of non-human primates have also been shown to be seropositive [41]. However, the seroprevalence in these animals is fairly low, and they are not the natural reservoir.
The first human case of monkeypox was reported in 1970 in the DRC in 9 month-old-boy [42]. In addition to the rash, which lasted for about 2-weeks, the boy also developed otitis and enlarged, painful cervical nodes [42]. According to the boy’s father, the family ate monkeys from time to time. Monkey meat was considered a delicacy. Between 1970 and 1971, a total six cases of human Mpox were reported in Central and West African countries [43]. These countries are endemic for Mpox and sporadic outbreaks continue to be regularly reported [44,45]. The first largest outbreak outside of Africa occurred in the United States in 2003, and involved 71 confirmed or probable cases [46]. The outbreak was traced to infected animals (rope squirrels, giant pouched rats and dormice) that were imported from Ghana to Texas animals [18,47]. The infected animals had been housed with native prairie dogs, which subsequently became the source of the multi-state human Mpox outbreak in the United States [18,47]. The most recent outbreak of Mpox outside Africa occurred in May 2022 [3,4,5]. This was the largest outbreak of human Mpox in history and involved over 87000 cases. In contrast to the previous outbreaks, the pattern of spread of this outbreak was very different. Who was most affected and the factors which probably contributed this outbreak will be discussed in subsequent sections.
4. Where did Mpox spread to?
For more than 50 years (1970-2020), human Mpox remained primarily restricted to Africa. Most cases occurred in Central and West African countries, notably in DRC, Nigeria, Central African Republic, and the Republic of the Congo [44,48]. Cases usually occurred in rural or forested areas, typically involving animal-to-human transmission, and children under 15 years were most commonly affected [27,48]. Secondary human-to-human spread accounted for less than a third of the cases [49]. Although occasional sporadic cases were detected in a few countries outside Africa, they were primarily exported cases who contracted the infection in endemic countries before travelling [50,51]. Hence, these sporadic cases did not draw widespread attention and the disease remained largely neglected. However, all this change in the 2022 Mpox outbreak. There was a clear shift in the speed, pattern of transmission, and the demographics of the disease [52]. There was a sudden surge in cases in countries in the European and American continents, men were mostly affected, cases had no connection to endemic countries in Africa and the mode of transmission was human-to-human [5,11,52]. The first cases in this outbreak were reported on 7th May 2022 from UK in an individual who had returned from Nigeria [53]. The patient had developed a rash on the 29th April and flew back to London on 3-4th May [53]. By the 31st May, UK had 179 confirmed cases, whilst 17 EU member states reported 321 cases [54]. Highest number of cases were reported from Spain (120 cases), Portugal (96 cases), Netherlands (26 cases), Germany (21 cases) and Italy (14 cases) [54]. During this same period, the virus had also spread to several countries outside the EU, including Canada (26 cases), United States (15 cases), UAE (15 cases), Australia (2 cases), and Mexico (2 cases) [54].
Over the next 1-2 month, the virus continued to spread rapidly to countries which had previously been Mpox free. By 23th July 2022 (less than 3 months into the outbreak), a total of 16,836 cases were reported from 76 countries worldwide, triggering the Director-General of the WHO to declare the Mpox outbreak a Public Health Emergency of International Concern [55]. The outbreak peaked by the end of August 2022 and gradually started declining. By 15th May 2023, 1 year after the outbreak, over 87,000 cases had been reported from 111 countries [56]. In terms of mortality, a total of 140 deaths had been reported, and 113/130 (87%) of the deaths were in 104 locations with no previous evidence of Mpox infection in the population. More than 80% of 87,000 confirmed cases were reported from just 10 countries (Figure 1B); United States (30,243 cases), Brazil (10,948), Spain (7,555), France (4,146), Colombia (4,090), Mexico (4,020), Peru (3,800), United Kingdom (3,753), Germany (3,691), and Canada (1,496). The highest number of deaths were also from the Americas (117 cases) [10].
5. Who was at risk of getting Mpox?
Although everyone is potentially susceptible to infection with the Mpox virus, survey of confirmed or suspected cases over the last 50 years, indicated that certain groups were primary affected. People at highest risk tended to be those living in endemic rural communities [44,48], those in close contact with infected animals [27,48], people who hunted, ate, or handled infected wild animals [42,46], those who travelled to endemic regions [50,51], people who had not received the smallpox vaccine (which provides cross-protection) [57,58], and healthcare workers involved in diagnosing, treating, and caring for Mpox patients [59,60]. By contrast, in the 2022 Mpox outbreak, individuals in the European and American continents were primarily affected (Figure 1B). They had little or no connection with endemic regions or contact with infected animals. Notably, more than 95% (78,106/81,154) of cases were men with median age of 34 years (IQR: 29-41) [10]. Women accounted for less than 4%, and pregnant women accounted for only 58 cases [10]. The infection in this global outbreak was sustained by human-to-human transmission, resulting from sexual or intimate close contact with respiratory sections and mucocutaneous skin lesions of infected individuals [10]. Most of the cases were in gay, bisexual or men who have sex with men (MSM) living in urban areas in clustered social and sexual networks [10,61]. Sex workers and those engaged in high-risk behaviors, such as multiple sexual partners and having sex without using a condom were disproportionally affected. These individuals were also often infected with other sexually transmitted infections, including syphilis, gonorrhea and HIV [62,63].
In HIV patients, particularly those with CD4 T cell count less than 200/µL (i.e. AIDS stage of the disease), Mpox infection was reported to be more severe and associated with higher mortality [64,65]. These patients exhibited atypical features compared to the immunocompetent individuals in whom the disease was generally mild, self-limiting and rarely fatal. Although initial symptoms were similar all patients and included fever, headache, muscle aches and fatigue, followed by skin lesions and lymphadenopathy, in HIV patients, the skin lesions were more extensive, persistent, and prone to secondary infections (Figure 3) [66,67]. Additionally, these patients also frequently had disseminated infection involving other organs and tissues, including the lungs, oral/rectal mucosa, and eyes [65,66]. Thus, timely diagnosis, supportive care, and management of complications was essential for improving outcomes. Moreover, emphasizing on the importance of preventive measures, including adherence to anti-retroviral therapy and infection control practices, was helpful in reducing the risk of Mpox in this vulnerable population.
6. Why did Mpox reemerged?
The world is effectively one global village and neglecting an outbreak in one part of the world, however remote and isolated, is not an option. The consequences of such neglect can be disastrous. The 2014 Ebola outbreak which infected over 28,000 individuals and claimed over 11,000 lives is a recent example [70]. Prior to the global 2022 Mpox outbreak, there were indications that the incidence of Mpox was increasing in some countries of Africa [58,71]. So, what contributed to its re-emergence and rapid spread outside Africa? Several factors are likely to be involved. (1) Increased human-animals contact: As human populations expand and encroach into previously uninhabited areas, there is increased contact with wild animals, increasing the risk of transmission. Some of the initial cases in the 2022 outbreak had travel history to endemic countries in Africa [53]. (2) Decreased vaccination coverage: Vaccination against smallpox, which provided some cross-protection against monkeypox, was discontinued in 1980 after smallpox was declared eradicated [72]. As a result, a large proportion of the population under the age of 45 became susceptible to Mpox, which in turn explains the increase in incidence of the disease observed in some African countries [57,58]. (3) Increase global travel: The ease and speed with which one can travel from one part of the world to another can facilitate the spread of infectious diseases. For the 2022 Mpox outbreak, travelling to and from large gatherings such Gay pride events or sex-on-site parties is believed to have played a role in the global spread of the infection [62,73]. Individuals in the LGBTQ communities was primarily affected. (4) The phylogenetic analysis of the Mpox virus indicated that the global 2022 Mpox outbreak was primarily driven by the B.1 stain from the Clade IIb lineage [74]. This particular strain of the virus appears to have evolved from the strain that caused an outbreak in Nigeria in 2018-2019 [75,76]. A number of single-nucleotide polymorphisms (SNPs) have been detected in this strain, which may account for its higher rate of human-to-human transmission [75].
Conclusion
The threat of emerging and re-emerging viral infections with pandemic potential is real [77,78]. It is not a question of if, but when the next pandemic will occur. We need to be prepared. The 2022 Mpox outbreak was brought under control within three months of its reemergence by advocating and implementing a combination of socio-behavioral changes and public health interventions [8,79]. These included, strategies involving public awareness and education, social and behavior campaigns aimed at high risk groups, rapid diagnosis and surveillance, and vaccinating those at high-risk and their contacts [80,81]. Although these strategies were effectively implemented in affluent Western countries, the same was not the case for most of the countries in the African continent. The mortality rate in the African continent was more than 300 times higher than the rest of the world [71]. It is essential to have sustainable and equitable global plans and policies which should include not only education and information sharing, but also equitable distribution of drugs and vaccines. The health disparities between the rich and poor countries are startling and if not addressed, will inevitably lead to further spillover of infectious diseases to other countries.
Author Contributions
Conceptualization, G.K. and N.P; formal analysis, G.K.; N.P.; writing—original draft preparation, G.K.; writing—review and editing, G.K.; N.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The Challenge of Emerging and Re-Emerging Infectious Diseases. Nature 2004, 430, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Morens, D.M.; Taubenberger, J.K. The Mother of All Pandemics Is 100 Years Old (and Going Strong)! Am J Public Health 2018, 108, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I.; et al. Community Transmission of Monkeypox in the United Kingdom, April to May 2022. Euro Surveill 2022, 27, 2200422. [Google Scholar] [CrossRef] [PubMed]
- Duque, M.P.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing Monkeypox Virus Outbreak, Portugal, 29 April to 23 May 2022. Euro Surveill 2022, 27, 2200424. [Google Scholar] [CrossRef]
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’Abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S.; et al. Epidemiological, Clinical and Virological Characteristics of Four Cases of Monkeypox Support Transmission through Sexual Contact, Italy, May 2022. Euro Surveill 2022, 27, 2200421. [Google Scholar] [CrossRef]
- WHO. WHO Director-General’s Statement at the Press Conference Following IHR Emergency Committee Regarding the Multi-Country Outbreak of Monkeypox - 23 July 2022 Available online:. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-the-press-conference-following-IHR-emergency-committee-regarding-the-multi--country-outbreak-of-monkeypox--23-july-2022 (accessed on 9 May 2023).
- Lewis, R.F.; Kuppalli, K.; Hoxha, A.; Doherty, M.C. Emergency Committee Recommendations on Mpox – What’s next? Bull World Health Organ 2023, 101, 300–300A. [Google Scholar] [CrossRef]
- Roper, R.L.; Garzino-Demo, A.; Del Rio, C.; Bréchot, C.; Gallo, R.; Hall, W.; Esparza, J.; Reitz, M.; Schinazi, R.F.; Parrington, M.; et al. Monkeypox (Mpox) Requires Continued Surveillance, Vaccines, Therapeutics and Mitigating Strategies. Vaccine 2023, S0264-410X(23)00393-6. [Google Scholar] [CrossRef]
- Wadman, M. WHO Ends Mpox Emergency Available online:. Available online: https://www.science.org/content/article/who-ends-mpox-emergency (accessed on 15 May 2023).
- WHO 2022-23 Mpox Outbreak: Global Trends. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 7 June 2023).
- Mitjà, O.; Ogoina, D.; Titanji, B.K.; Galvan, C.; Muyembe, J.-J.; Marks, M.; Orkin, C.M. Monkeypox. Lancet 2023, 401, 60–74. [Google Scholar] [CrossRef]
- Pauli, G.; Blümel, J.; Burger, R.; Drosten, C.; Gröner, A.; Gürtler, L.; Heiden, M.; Hildebrandt, M.; Jansen, B.; Montag-Lessing, T.; et al. Orthopox Viruses: Infections in Humans. Transfus Med Hemother 2010, 37, 351–364. [Google Scholar] [CrossRef]
- Buller, R.M.; Palumbo, G.J. Poxvirus Pathogenesis. Microbiological Reviews 1991, 55, 80–122. [Google Scholar] [CrossRef]
- Lewis-Jones, S. Zoonotic Poxvirus Infections in Humans. Curr Opin Infect Dis 2004, 17, 81. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.M.; Anderson, S.A. Qualitative Assessment of Risk for Monkeypox Associated with Domestic Trade in Certain Animal Species, United States. Emerg Infect Dis 2006, 12, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Yuan, Y.; Jiang, L.; Liu, Y.; Liu, Y.; Zhang, L. Animal Host Range of Mpox Virus. J Med Virol 2023, 95, e28513. [Google Scholar] [CrossRef] [PubMed]
- WHO Monkeypox: Experts Give Virus Variants New Names Available online:. Available online: https://www.who.int/news/item/12-08-2022-monkeypox--experts-give-virus-variants-new-names (accessed on 7 June 2023).
- Reed, K.D.; Melski, J.W.; Graham, M.B.; Regnery, R.L.; Sotir, M.J.; Wegner, M.V.; Kazmierczak, J.J.; Stratman, E.J.; Li, Y.; Fairley, J.A.; et al. The Detection of Monkeypox in Humans in the Western Hemisphere. N Engl J Med 2004, 350, 342–350. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Carroll, D.S.; Olson, V.A.; Hughes, C.; Galley, J.; Likos, A.; Montgomery, J.M.; Suu-Ire, R.; Kwasi, M.O.; Jeffrey Root, J.; et al. A Silent Enzootic of an Orthopoxvirus in Ghana, West Africa: Evidence for Multi-Species Involvement in the Absence of Widespread Human Disease. Am J Trop Med Hyg 2010, 82, 746–754. [Google Scholar] [CrossRef]
- Chen, N.; Li, G.; Liszewski, M.K.; Atkinson, J.P.; Jahrling, P.B.; Feng, Z.; Schriewer, J.; Buck, C.; Wang, C.; Lefkowitz, E.J.; et al. Virulence Differences between Monkeypox Virus Isolates from West Africa and the Congo Basin. Virology 2005, 340, 46–63. [Google Scholar] [CrossRef]
- Likos, A.M.; Sammons, S.A.; Olson, V.A.; Frace, A.M.; Li, Y.; Olsen-Rasmussen, M.; Davidson, W.; Galloway, R.; Khristova, M.L.; Reynolds, M.G.; et al. A Tale of Two Clades: Monkeypox Viruses. J Gen Virol 2005, 86, 2661–2672. [Google Scholar] [CrossRef]
- Americo, J.L.; Earl, P.L.; Moss, B. Virulence Differences of Mpox (Monkeypox) Virus Clades I, IIa, and IIb.1 in a Small Animal Model. PNAS 2023, 120, e2220415120. [Google Scholar] [CrossRef]
- Colavita, F.; Antinori, A.; Nicastri, E.; Focosi, D.; Girardi, E.; Vaia, F.; Maggi, F. Monkeypox Virus in Human Body Sites and Fluids: Evidence for Transmission. Lancet Infect Dis 2023, 23, 6–8. [Google Scholar] [CrossRef]
- Nolen, L.D.; Osadebe, L.; Katomba, J.; Likofata, J.; Mukadi, D.; Monroe, B.; Doty, J.; Kalemba, L.; Malekani, J.; Kabamba, J.; et al. Introduction of Monkeypox into a Community and Household: Risk Factors and Zoonotic Reservoirs in the Democratic Republic of the Congo. Am J Trop Med Hyg 2015, 93, 410–415. [Google Scholar] [CrossRef]
- Besombes, C.; Gonofio, E.; Konamna, X.; Selekon, B.; Gessain, A.; Berthet, N.; Manuguerra, J.-C.; Fontanet, A.; Nakouné, E. Intrafamily Transmission of Monkeypox Virus, Central African Republic, 2018. Emerg Infect Dis 2019, 25, 1602–1604. [Google Scholar] [CrossRef] [PubMed]
- Hutson, C.L.; Lee, K.N.; Abel, J.; Carroll, D.S.; Montgomery, J.M.; Olson, V.A.; Li, Y.; Davidson, W.; Hughes, C.; Dillon, M.; et al. Monkeypox Zoonotic Associations: Insights from Laboratory Evaluation of Animals Associated with the Multi-State US Outbreak. Am J Trop Med Hyg 2007, 76, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Jezek, Z.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Human Monkeypox: Clinical Features of 282 Patients. J Infect Dis 1987, 156, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Núñez, I.; García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Toledo-Salinas, C.; Carbajal-Sandoval, G.; Sosa-Laso, L.; García-Rodríguez, G.; Cortés-Alcalá, R.; Torre, A. de la; Fragoso-Saavedra, S.; et al. Epidemiological and Clinical Characteristics of Patients with Human Monkeypox Infection in Mexico: A Nationwide Observational Study. Lancet Reg Health Am 2023, 17, 100392. [Google Scholar] [CrossRef] [PubMed]
- Rasizadeh, R.; Shamekh, A.; Shiri Aghbash, P.; Bannazadeh Baghi, H. Comparison of Human Monkeypox, Chickenpox and Smallpox: A Comprehensive Review of Pathology and Dermatological Manifestations. Curr Med Res Opin 2023, 1–10. [Google Scholar] [CrossRef]
- McCollum, A.M.; Damon, I.K. Human Monkeypox. Clinical Infectious Diseases 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending After Effect of Smallpox Eradication? Front Trop Dis 2022, 3. [Google Scholar] [CrossRef]
- Fink, D.L.; Callaby, H.; Luintel, A.; Beynon, W.; Bond, H.; Lim, E.Y.; Gkrania-Klotsas, E.; Heskin, J.; Bracchi, M.; Rathish, B.; et al. Clinical Features and Management of Individuals Admitted to Hospital with Monkeypox and Associated Complications across the UK: A Retrospective Cohort Study. Lancet Infect Dis 2023, 23, 589–597. [Google Scholar] [CrossRef]
- Magnus, P. von; Andersen, E.K.; Petersen, K.B.; Birch-Andersen, A. A Pox-Like Disease in Cynomolgus Monkeys. Acta Pathologica Microbiologica Scandinavica 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Prier, J.E.; Sauer, R.M.; Malsberger, R.G.; Sillaman, J.M. Studies on a Pox Disease of Monkeys. II. Isolation of the Etiologic Agent. Am J Vet Res 1960, 21, 381–384. [Google Scholar]
- Cho, C.T.; Wenner, H.A. Monkeypox Virus. Bacteriol Rev 1973, 37, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Arita, I.; Henderson, D.A. Smallpox and Monkeypox in Non-Human Primates. Bull World Health Organ 1968, 39, 277–283. [Google Scholar]
- Parker, S.; Buller, R.M. A Review of Experimental and Natural Infections of Animals with Monkeypox Virus between 1958 and 2012. Future Virol 2013, 8, 129–157. [Google Scholar] [CrossRef] [PubMed]
- Doty, J.B.; Malekani, J.M.; Kalemba, L.N.; Stanley, W.T.; Monroe, B.P.; Nakazawa, Y.U.; Mauldin, M.R.; Bakambana, T.L.; Liyandja Dja Liyandja, T.; Braden, Z.H.; et al. Assessing Monkeypox Virus Prevalence in Small Mammals at the Human–Animal Interface in the Democratic Republic of the Congo. Viruses 2017, 9, 283. [Google Scholar] [CrossRef] [PubMed]
- Hutin, Y.J.; Williams, R.J.; Malfait, P.; Pebody, R.; Loparev, V.N.; Ropp, S.L.; Rodriguez, M.; Knight, J.C.; Tshioko, F.K.; Khan, A.S.; et al. Outbreak of Human Monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerging infectious diseases 2001, 7, 434–438. [Google Scholar] [CrossRef]
- Khodakevich, L.; Jezek, Z.; Kinzanzka, K. Isolation of Monkeypox Virus from Wild Squirrel Infected in Nature. Lancet 1986, 1, 98–99. [Google Scholar] [CrossRef]
- Radonić, A.; Metzger, S.; Dabrowski, P.W.; Couacy-Hymann, E.; Schuenadel, L.; Kurth, A.; Mätz-Rensing, K.; Boesch, C.; Leendertz, F.H.; Nitsche, A. Fatal Monkeypox in Wild-Living Sooty Mangabey, Côte d’Ivoire, 2012. Emerg Infect Dis 2014, 20, 1009–1011. [Google Scholar] [CrossRef]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A Human Infection Caused by Monkeypox Virus in Basankusu Territory, Democratic Republic of the Congo. Bull World Health Organ 1972, 46, 593–597. [Google Scholar]
- Lourie, B.; Bingham, P.G.; Evans, H.H.; Foster, S.O.; Nakano, J.H.; Herrmann, K.L. Human Infection with Monkeypox Virus: Laboratory Investigation of Six Cases in West Africa. Bull World Health Organ 1972, 46, 633–639. [Google Scholar]
- Durski, K.N.; McCollum, A.M.; Nakazawa, Y.; Petersen, B.W.; Reynolds, M.G.; Briand, S.; Djingarey, M.H.; Olson, V.; Damon, I.K.; Khalakdina, A. Emergence of Monkeypox - West and Central Africa, 1970-2017. MMWR Morb Mortal Wkly Rep 2018, 67, 306–310. [Google Scholar] [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review. PLoS Negl Trop Dis 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- CDC Update: Multistate Outbreak of Monkeypox --- Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin, 2003 Available online:. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5227a5.htm (accessed on 23 May 2023).
- Sale, T.A.; Melski, J.W.; Stratman, E.J. Monkeypox: An Epidemiologic and Clinical Comparison of African and US Disease. J Am Acad Dermatol 2006, 55, 478–481. [Google Scholar] [CrossRef] [PubMed]
- McCollum, A.M.; Shelus, V.; Hill, A.; Traore, T.; Onoja, B.; Nakazawa, Y.; Doty, J.B.; Yinka-Ogunleye, A.; Petersen, B.W.; Hutson, C.L.; et al. Epidemiology of Human Mpox - Worldwide, 2018-2021. MMWR Morb Mortal Wkly Rep 2023, 72, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Shchelkunov, S.N.; Totmenin, A.V.; Babkin, I.V.; Safronov, P.F.; Ryazankina, O.I.; Petrov, N.A.; Gutorov, V.V.; Uvarova, E.A.; Mikheev, M.V.; Sisler, J.R.; et al. Human Monkeypox and Smallpox Viruses: Genomic Comparison. FEBS Lett 2001, 509, 66–70. [Google Scholar] [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’Connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two Cases of Monkeypox Imported to the United Kingdom, September 2018. Euro Surveill 2018, 23, 1800509. [Google Scholar] [CrossRef]
- Ng, O.T.; Lee, V.; Marimuthu, K.; Vasoo, S.; Chan, G.; Lin, R.T.P.; Leo, Y.S. A Case of Imported Monkeypox in Singapore. Lancet Infect Dis 2019, 19, 1166. [Google Scholar] [CrossRef]
- Kumar, R.; Singh, S.; Singh, S.K. A Systematic Review of 5110 Cases of Monkeypox: What Has Changed Between 1970 and 2022? Cureus 2022, 14, e30841. [Google Scholar] [CrossRef]
- ECDC Communicable Disease Threats Report, 8-14 May 2022, Week 19 Available online:. Available online: https://www.ecdc.europa.eu/en/publications-data/communicable-disease-threats-report-8-14-may-2022-week-19 (accessed on 1 June 2023).
- ECDC Epidemiological Update: Monkeypox Multi-Country Outbreak Available online:. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-monkeypox-multi-country-outbreak-0 (accessed on 1 June 2023).
- WHO. WHO Director-General Declares the Ongoing Monkeypox Outbreak a Public Health Emergency of International Concern. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 24 July 2022).
- 56. WHO 2022-23 Mpox (Monkeypox) Outbreak: Global Trends. https://worldhealthorg.shinyapps.io/mpx_global/ (retrieved 30 April 2023), 30 April.
- Reynolds, M.G.; Damon, I.K. Outbreaks of Human Monkeypox after Cessation of Smallpox Vaccination. Trends Microbiol 2012, 20, 80–87. [Google Scholar] [CrossRef]
- Rimoin, A.W.; Mulembakani, P.M.; Johnston, S.C.; Lloyd Smith, J.O.; Kisalu, N.K.; Kinkela, T.L.; Blumberg, S.; Thomassen, H.A.; Pike, B.L.; Fair, J.N.; et al. Major Increase in Human Monkeypox Incidence 30 Years after Smallpox Vaccination Campaigns Cease in the Democratic Republic of Congo. Proc Natl Acad Sci U S A 2010, 107, 16262–16267. [Google Scholar] [CrossRef]
- Pinto, P.; Costa, M.A.; Gonçalves, M.F.M.; Rodrigues, A.G.; Lisboa, C. Mpox Person-to-Person Transmission-Where Have We Got So Far? A Systematic Review. Viruses 2023, 15, 1074. [Google Scholar] [CrossRef]
- Choi, Y.; Jeon, E.; Kim, T.; Choi, S.J.; Moon, S.M.; Song, K.-H.; Kim, H.B.; Kim, E.S. Case Report and Literature Review of Occupational Transmission of Monkeypox Virus to Healthcare Workers, South Korea. Emerg Infect Dis 2023, 29, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Angelo, K.M.; Smith, T.; Camprubí-Ferrer, D.; Balerdi-Sarasola, L.; Menéndez, M.D.; Servera-Negre, G.; Barkati, S.; Duvignaud, A.; Huber, K.L.B.; Chakravarti, A.; et al. Epidemiological and Clinical Characteristics of Patients with Monkeypox in the GeoSentinel Network: A Cross-Sectional Study. The Lancet Infectious Diseases 2023, 23, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries — April–June 2022. N Engl J Med 2022, 387, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Ogoina, D.; Iroezindu, M.; James, H.I.; Oladokun, R.; Yinka-Ogunleye, A.; Wakama, P.; Otike-Odibi, B.; Usman, L.M.; Obazee, E.; Aruna, O.; et al. Clinical Course and Outcome of Human Monkeypox in Nigeria. Clin Infect Dis 2020, 71, e210–e214. [Google Scholar] [CrossRef]
- Miller, M.J. Severe Monkeypox in Hospitalized Patients — United States, August 10–October 10, 2022. MMWR Morb Mortal Wkly Rep 2022, 71. [Google Scholar] [CrossRef]
- Mitjà, O.; Alemany, A.; Marks, M.; Mora, J.I.L.; Rodríguez-Aldama, J.C.; Silva, M.S.T.; Herrera, E.A.C.; Crabtree-Ramirez, B.; Blanco, J.L.; Girometti, N.; et al. Mpox in People with Advanced HIV Infection: A Global Case Series. The Lancet 2023, 0. [Google Scholar] [CrossRef]
- Boesecke, C.; Monin, M.B.; van Bremen, K.; Schlabe, S.; Hoffmann, C. Severe Monkeypox-Virus Infection in Undiagnosed Advanced HIV Infection. Infection 2022, 50, 1633–1634. [Google Scholar] [CrossRef]
- Uysal, F. Detection of Monkeypox Disease from Human Skin Images with a Hybrid Deep Learning Model. Diagnostics (Basel) 2023, 13, 1772. [Google Scholar] [CrossRef]
- Melgosa Ramos, F.J.; Parra Civera, M.; Pons Fuster, J.J. Skin Lesions Due to Monkeypox Virus in a Well-Controlled HIV Patient. Med Clin (Engl Ed) 2022, 159, e87–e88. [Google Scholar] [CrossRef]
- Coltart, C.E.M.; Lindsey, B.; Ghinai, I.; Johnson, A.M.; Heymann, D.L. The Ebola Outbreak, 2013–2016: Old Lessons for New Epidemics. Philos Trans R Soc Lond B Biol Sci 2017, 372. [Google Scholar] [CrossRef] [PubMed]
- Tomori, O.; Ogoina, D. Monkeypox: The Consequences of Neglecting a Disease, Anywhere. Science 2022, 377, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Strassburg, M.A. The Global Eradication of Smallpox. Am J Infect Control 1982, 10, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Vusirikala, A.; Charles, H.; Balasegaram, S.; Macdonald, N.; Kumar, D.; Barker-Burnside, C.; Cumiskey, K.; Dickinson, M.; Watson, M.; Olufon, O.; et al. Epidemiology of Early Monkeypox Virus Transmission in Sexual Networks of Gay and Bisexual Men, England, 2022. Emerg Infect Dis 2022, 28, 2082–2086. [Google Scholar] [CrossRef]
- Gao, L.; Shi, Q.; Dong, X.; Wang, M.; Liu, Z.; Li, Z. Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global. Trop Med Infect Dis 2023, 8, 76. [Google Scholar] [CrossRef]
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Phylogenomic Characterization and Signs of Microevolution in the 2022 Multi-Country Outbreak of Monkeypox Virus. Nat Med 2022, 28, 1569–1572. [Google Scholar] [CrossRef]
- Falendysz, E.A.; Lopera, J.G.; Rocke, T.E.; Osorio, J.E. Monkeypox Virus in Animals: Current Knowledge of Viral Transmission and Pathogenesis in Wild Animal Reservoirs and Captive Animal Models. Viruses 2023, 15, 905. [Google Scholar] [CrossRef]
- Gao, G.F. From “A”IV to “Z”IKV: Attacks from Emerging and Re-Emerging Pathogens. Cell 2018, 172, 1157–1159. [Google Scholar] [CrossRef]
- Fauci, A.S. It Ain’t Over Till It’s Over…but It’s Never Over — Emerging and Reemerging Infectious Diseases. N Engl J Med 2022, 387, 2009–2011. [Google Scholar] [CrossRef]
- Kirby, T. From Early Alarm to Gradual Control of Monkeypox. Lancet HIV 2022. [Google Scholar] [CrossRef]
- Vairo, F.; Leone, S.; Mazzotta, V.; Piselli, P.; Carli, G.D.; Lanini, S.; Maggi, F.; Nicastri, E.; Gagliardini, R.; Vita, S.; et al. The Possible Effect of Sociobehavioral Factors and Public Health Actions on the Mpox Epidemic Slowdown. International Journal of Infectious Diseases 2023, 130, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Strathdee, S.A.; Crago, A.-L.; Shannon, K. Harm Reduction and Rights-Based Approaches to Reduce Monkeypox Transmission among Sex Workers. Lancet Infect Dis 2023, 23, e43–e46. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Weekly confirmed cases of Mpox, and (B) Cumulative confirmed cases from 2nd May 2022 to 15th May 2023 (based on WHO data)[10].
Figure 1.
(A) Weekly confirmed cases of Mpox, and (B) Cumulative confirmed cases from 2nd May 2022 to 15th May 2023 (based on WHO data)[10].
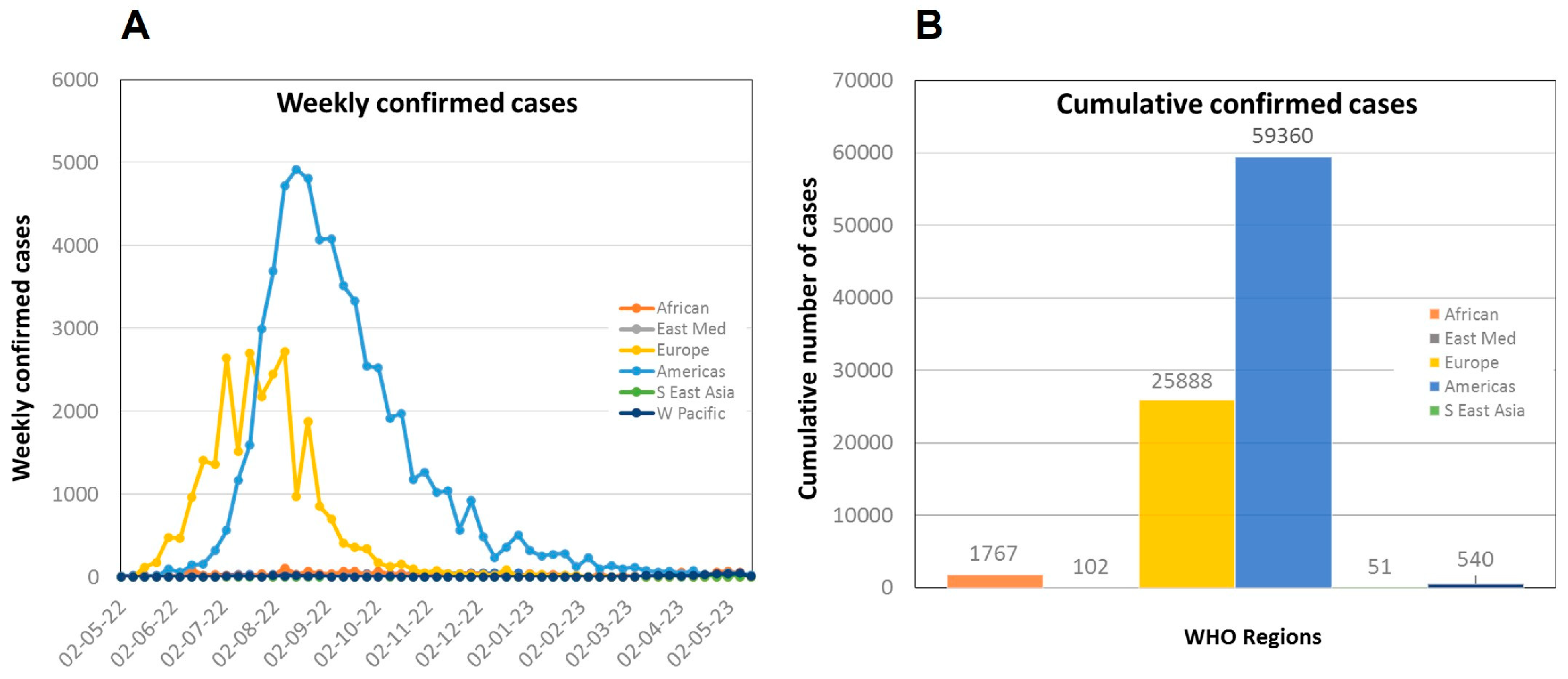
Figure 2.
Phylogenetic tree of Mpox virus isolates from the 2022 outbreak [10].
Figure 2.
Phylogenetic tree of Mpox virus isolates from the 2022 outbreak [10].

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



