Submitted:
27 June 2023
Posted:
27 June 2023
You are already at the latest version
Abstract
The current echocardiography reference values are derived primarily from populations in North America and Europe. It becomes necessary to study ethnically different groups of the population, which often have different living conditions, food habits and lifestyle. The aim of the study was to compare echocardiography indicators in urbanized patients with arterial hypertension of the Shor and non-indigenous ethnic groups living in the Gornaya Shoria region.
The study included patients with arterial hypertension: 58 Shors (20 men and 38 women) and 50 non-indigenous residents (15 men and 35 women) of Gornaya Shoria. All underwent an echocardiographic study with an assessment of the left heart parameters. We assessed the left ventricular hypertrophy (LVH) severity, LV geometry and diastolic function in the ethnic and sex groups.
Shor with hypertension no showed a significant difference in left ventricular dimensions compared to Caucasian. Severe abnormal LVH was associated in the Shors with glucose levels (OR 3.24, 95%CI 1.56-6.7, p=0,001), and in Caucasians with systolic (p=0.021) and diastolic (p=0.011) blood pressure, and heart rate (p=0.033). The Shor men were more likely to have normal LV diastolic function (p=0.029) and LV concentric remodeling (p=0.023), and less often to have normal LV geometry (p=0.015) compared to non-indigenous men.
Thus, this study can be useful in assessing the impact of the development of arterial hypertension, as well as the impact of changing the lifestyle of the Shors when moving to the city from rural areas on ethnic differences in echocardiography.
Keywords:
arterial hypertension
; echocardiography
; left ventricular hypertrophy
; Shors
1. Introduction
Detection of left ventricular hypertrophy (LVH) has important clinical and prognostic significance in patients with arterial hypertension [1,2]. Echocardiography is widely used and is considered the best method for this purpose. However, most data, on which the current worldwide-used ASE and EACVI recommended echocardiographic quantification values for the left ventricle are based, were obtained from Caucasian subjects in the United States and Europe [3]. Therefore, the use of published regulatory “control limits” remains limited as extending them to other racial and ethnic groups may not be applicable. For example, a systematic review has shown that left ventricular mass (LVM) reference ranges cannot be easily applied to the world's diverse multiracial population with cardiovascular disease [4]. If current ASE guidelines are used to define LVM as “normal,” then some patients may be misclassified [5-7]. This misclassification can lead to an underestimation of LVH and, ultimately, to inadequate treatment and underestimation of the predictive value of LVH in certain patients [8,9].
Moreover, even multicenter studies involving other regions and countries do not take the ethnic diversity of the inhabitants of these states into account. Some regions were even underrepresented in the largest-scale study of recent times - WASE- despite the inclusion of the countries of Africa, Asia and the Middle East [9]. A complete representation of the diversity of ethnic groups within each country wasn’t achieved in that study as well. Accordingly, further regional studies will be needed to address the issue of ethnic diversity within the country. Therefore, it becomes necessary to study ethnically different groups of the population, often characterized by differences in living conditions, dietary habits and lifestyle of both healthy persons and patients. Ultimately, this could allow the development of standards or correction factors for important indicators of echocardiography in each ethnic group. This was the basis for this study of one of the indigenous peoples native to the Gornaya Shoria region. Previous studies have shown differences in echocardiographic parameters of healthy individuals of the Shor nationality compared to Caucasians [11,12]. The aim of this study was to compare echocardiography indicators in patients with arterial hypertension from two ethnic groups living in the Gornaya Shoria region.
2. Methods
2.1. Patients
A one-stage study of the indigenous (Shors) and non-indigenous population living in Gornaya Shoria in the south of Western Siberia was carried out over 2017 and 2018. The Shors belong to the South Siberian segment of the Asian race [13]. They live in small indigenous ethnic communities, and the population is mainly concentrated in the south of Western Siberia. Their ancestors led a lifestyle centered on hunting, fishing, subsidiary livestock raising, primitive hand farming and gathering. In connection with intensive urbanization, the traditional Shor culture is gradually disappearing [14] in particular, there is a relocation of the Shors from the countryside to the cities.
The study was based on polyclinics 1 and 2, as well as the Topaz Rehabilitation Center (Myski). Recruitment of the studied indigenous-ethnicity and comparison groups was carried out by a continuous method, according to the lists provided by the administration of the Myski city, with persons over 18 years old. Mixed ethnicity persons were not included. The participants enrollment description is presented in Figure 1. The study included 270 adults (154 Shors and 116 non-indigenous people). The subjects were examined by a therapist during a visit to the city polyclinic. The questionnaires were surveyed using the Rose (chest pain) and Covey (anxiety) questionnaires; positive data from these questionnaires served as an exclusion criterion. Arterial blood pressure was measured in accordance with 2018 ESC/ESH guidelines for the management of arterial hypertension by an Omron automatic tonometer (Japan). Arterial hypertension was defined as systolic blood pressure of 140 mmHg or more, diastolic blood pressure of 90 mmHg or more, and / or taking antihypertensive medication. In this cohort, patients with arterial hypertension were identified (n=108, 58 the Shors and 50 non-indigenous subiects). Ethnic groups were matched for gender and age. Anthropometry included measurement of height, weight, waist and hip circumference, calculation of body surface area (BSA), body mass index (BMI). The lipid profile was analyzed, studies such as electrocardiography, color duplex scanning of the carotid and femoral arteries were carried out. The exclusion criteria included a history or instrumental data of other cardiovascular diseases (ischemic heart disease, heart failure, peripheral atherosclerosis, transient ischemic attacks and previous stroke). Written informed consent was obtained from each patient. The study protocol was in accordance with the ethical principles of the 1975 Declaration of Helsinki. The study design was approved by the Local Ethics Committee of the Research Institute for Complex Issues of Cardiovascular Diseases (Kemerovo, Russian Federation).
2.2. Echocardiography
All subjects underwent echocardiography on a Vivid S5 ultrasound system (General Electric) using a phased array sector probe. All measurements were carried out according to the current guidelines [15]. All echocardiographic examinations were performed by the same examiner (OA). Reported values of all echocardiographic parameters were obtained as the average value of 3 consecutive cardiac cycles. Structural parameters of the left and right heart were assessed using M-modal and B-modal scanning in standard positions. Al structural indicators were indexed to the BSA. The following left heart indicators were used: aortic diameter, index of the aortic diameter (DAi), end-diastolic and end-sistolic diameters (EDD and ESD), posterior wall thickness (TPWLV) and its index (TPWLVi), interventricular septum thickness (TIVS) and its index (TIVSi), end diastolic and end systolic volumes (EDV and ESV) of the LV, index of the end diastolic volume of the LV (LVEDVi). LV mass was calculated in B-mode at the end of diastole, and LV myocardial mass index (LVMi) was also calculated. The LV ejection fraction (LVEF) was determined by the Simpson method. In the section of 4 chambers at the end of diastole, the maximum transverse diameter of the left atrium (LA), its volume (LAV) and index (LAVi) were measured. In the pulse-wave Doppler mode, the velocity of early diastolic atrioventricular flows (E), the time of their deceleration (DTE), the flow rate of atrial systole (A), the ratio E / A were assessed. Using spectral tissue Doppler, the parameters of the regional function of the mitral valve annulus, related to the diastolic (e ', a', e '/ a') and systolic parts of the spectrum (s'), were measured. The indices of total LV performance were calculated as the ratio of the sums of isovolumic relaxation time and isometric filling time to the expulsion time. Using color M-modal scanning, we measured the propagation velocities of the early mitral flow (Vf) according to the slope of the brightest part of the spectrum.
Left ventricular hypertrophy was defined as LVMi > 95 g/ m2 for women and >115 g/m2 for men [15]. Relative wall thickness (RWT) was calculated using (IVSDd + PWDd) / LVEDd); concentric geometry was present when RWT> 0.42 [16]. LVMi and RWT were used to differentiate four types of left ventricular geometry: normal geometry (RWT ≤0.42 and normal LVMi), concentric remodeling (RWT>0.42 and normal LVMi), concentric hypertrophy (RWT>0.42 and increased LVMi), and eccentric hypertrophy (RWT ≤0.42 and increased LVMi). The severity of left ventricular hypertrophy was assessed according to the recommendations of Marwick TH et al. (Marwick TH, 2015). Mildly abnormal LVH was determined in women with LVMi within the range of 96-108 g / m2, in men - at 116-131 g / m2; moderately abnormal LVH - at 109-121 g / m2 and 132-148 g / m2; severely abnormal LVH - with LVMi ≥ 122 g / m2 and ≥ 149 g / m2, respectively.
The left ventricle diastolic function was assessed according to the 2009 ASE recommendations10. Normal LV diastolic function was considered at values of e ≥ 8 cm / s, lateral e ≥ 10 cm / s and left atrial volume index (LAVi) <34 ml / m2.In patients with e <8 cm / s or lateral e <10 cm / s and LAVi≥ 34 ml / m2, the grade of diastolic dysfunction from 1 to 3 was determined based on at least two indicators among the E / e (E ≤ 8, between 9 and 12 and ≥ 13 cm / s, respectively), the ratio E / A of mitral inflow (<0.8, between 0.8 and 1.2 and> 2, respectively) and DT (> 200, between 160 and 200 and <160 ms, respectively).
2.3. Statistical analysis
Statistical processing was performed using the standard Statistica 10.0 software package. The normality of the distribution was verified using the Shapiro - Wilk test. Since most of the quantitative characteristics were distributed asymmetrically, all quantitative variables were presented as the median, low and upper quartiles (ME [LQ, UQ]). Comparison of quantitative traits was carried out using the Kruskal - Wallis test. Qualitative and binary characteristics were compared using the χ2 (chi-square) test with Yates' correction for small samples. Intergroup differences were assessed using the Mann - Whitney test with Bonferroni's correction. Using logistic regression analysis, we studied the relationship of possible factors with severely abnormal LVH in all patients, and then separately in Shors and Caucasians. Multivariate regression analysis included variables for which the statistical significance in the univariate analysis was less than 0.1. After a preliminary assessment of the correlation between the identified predictors, several regression models were formed with the inclusion of independent factors. The level of statistical significance was taken as p <0.05.
3. Results
The groups were comparable in age (Table 1). According to the results of anthropometry, both body weight and BSA were lower in men and women of Shor ethnicity than in men and women of non-indigenous ethnicity (p = 0.0014 and p = 0.004). Among the representatives of the Shor urbanized population, persons with secondary specialized education (p = 0.013) were significantly less common, especially among men (p <0.01), while no significant differences between educational level of men and women within the Shor ethnic group was noted. Among the Shor men, there were significantly more people engaged in heavy physical and, generally, low-skilled labor than in all other groups (p = 0.01). Smoking was more prevalent among indigenous people (p = 0.003). The groups did not have significant differences in blood lipid spectrum parameters and in the level of office systolic and diastolic blood pressure, however, there was a tendency for the parameters to increase beyond the reference values in both groups. The Shor men and women had significantly lower urea and creatinine levels than the corresponding non-indigenous groups.
From the absolute echocardiographic parameters of the left heart (Table 2), no significant differences were found between the groups. The data of the longitudinal LV systolic function (Table 3) in the form of a systolic excursion of the septum (s'sept) were the highest in Shor men (p = 0.069), and the LV performance index was the lowest in them (p = 0.034). Also in this group, the minimum isovolumic relaxation time (p = 0.065) was noted.
The degree of LVH in patients is shown in Figure 2. No statistically significant difference was observed among men and women in both ethnic groups with different severity of LVH. At the same time, pronounced LVH was somewhat more common among Shors than among non-indigenous residents (27.6% and 16.0%, respectively, p = 0.03).
Despite similar data on the severity of LVH, normal LV geometry was less common among the Shors as a whole compared to non-indigenous population (p=0.163), and also among Shor men compared to non-indigenous men (p=0.023) (Figure 3). Accordingly, concentric LV remodeling was more common among Shors in general and among Shor men, although these differences did not reach statistical significance (p=0.364 and p=0.255, respectively). No significant ethnic differences in LV geometry were found in women.
Normal diastolic function of the left ventricle (Figure 4) was detected more often in Shor men than in men of non-indigenous nationality (p=0.029). Accordingly, grade 1 diastolic dysfunction was detected more often in non-indigenous men than in Shors (p=0.002). We did not reveal differences in the LV diastolic dysfunction prevalence in women of different ethnicities.
In univariate logistic regression analysis (Supplementary Table S1), the factor associated with severe abnormal LVH in the total sample was glucose (OR = 1.83, 95% CI 1.1-3.03, p=0.017), which remained an independent factor in the multiple logistic regression model (OR = 1.79, 95% CI 1.08-2.97, p =0.020). When carrying out univariate and multiple logistic regression analysis, the probable predictor associated with severe abnormal LVH in Shor patients was glucose level (OR = 3.31, 95% CI 1.6-6.85, p = 0.001 and OR = 3.24, 95% CI 1.56-6.70, p = 0.001, respectively). When carrying out univariate logistic regression analysis, the likely predictors associated with severe abnormal LVH in the group of Caucasian patients were SBP (OR = 1.04, 95% CI 1.0-1.08, p = 0.021), DBP (OR = 1.09, 95% CI 1.01-1.17, p = 0.011), heart rate (OR = 1.06, 95% CI 1.0-1.12, p = 0.033), and LDL cholesterol (OR = 1.99, 95% CI 1.04-3.79, p = 0.034). But in the multiple logistic regression model, none of these factors were independently associated with severe abnormal LVH.
4. Discussion
Our study has found no differences in the structural parameters of the left heart and the severity of left ventricular hypertrophy dependent on ethnicity of hypertensive patients. Normal geometry of the left ventricle was more common in non-indigenous men than in Shor men. At the same time, Shor men were more likely to have normal LV diastolic function compared to non-indigenous men. The LVH severity was associated with glucose levels in Shors, and with blood pressure and heart rate in Caucasians.
The obtained results were somewhat unexpected for us. In the previous study, when comparing healthy people of Shor ethnicity and Caucasians, the differences in structural parameters were more noticeable, in particular, there was a significant increase in the indices of the end-diastolic diameter of the LV, left atrium and diameter of the pulmonary artery in men and women of Shor nationality relative to Caucasians. Moreover, there was a significant increase in the indices of the aorta diameter, of the LV posterior wall and interventricular septum thickness, and the mass of the left ventricular myocardium among indigenous women [11]. Such differences can be partly explained by the younger age of the examined healthy persons. Apparently, development of arterial hypertension and age-related changes leveled most of the initial ethnic differences in the compared cohorts. Similar data were obtained in the study of rural residents of Gornaya Shoria; it was shown that the LV myocardial mass index in the groups of hypertensive patients of the indigenous and non-indigenous population did not differ, although the absolute values of the end-diastolic size and LV myocardial mass were higher in Caucasians [17].
In previous studies, the following patterns were noted: LV myocardial mass was lower in healthy representatives of South Asia than in Caucasians and Afro-Caribbean in the SABER study [18]. A meta-analysis by Poppe KK et al., noted a significant geographic variability of LV myocardial mass values in healthy individuals. Lower values of LVMM were found in residents of Asia and South America compared with representatives of Europe and North America. The review also found that BSA indexing does not improve the relevance of recommended reference ranges for either sex and does not seem to account for differences between populations [19]. That study was limited by the lack of LV myocardial mass analysis in individual ethnic groups, since ethnicity was limited to definition at the country level, and the details of ethnic composition depended on the focus of a separate study.
The results of the EchoNoRMAL meta-analysis led to a proposition for standards for left ventricular indices in various ethnic groups [20]. Thus, the normative values of LVMM in men were lower in the Middle East, and even lower in South Asians as compared to Caucasians. On the other hand, LVMM values were lower in Caucasian women than in residents of different regions of Asia [20]. At the same time, studies in healthy individuals cannot be extended to cohorts of patients with various pathologies; this requires additional studies [15]. Different results of the echocardiography parameters comparing Shors and Caucasians among healthy individuals and hypertensive patients in our study are consistent with this statement.
In the WASE study, the protocol for assessing left ventricular parameters was standardized, with a wider representation of Asian countries (41.8% of subjects). That work found significant cross-country variations for all LV parameters reflecting LV size (size, mass, and volume), even after indexing body surface area, with LV end-diastolic and end-systolic volumes having the greatest variation. For both sexes, the largest volumes were recorded in Australia and the smallest were found in India. This finding suggests that, in addition to gender and body surface area, country-specific assessments of LV volumes should be considered (P <0.05 for all). While the differences in the main parameters of the LV were insignificant between Asians and Caucasians [10], the other races had the smallest values of the volumes and mass of the LV myocardium. One gets the impression that the representatives of the Shor nationality in this regard are closer to the indicators of the Asian ethnic groups.
Fewer studies have focused on comparing left ventricular diastolic function in individuals of different nationalities. Interestingly, the recently published results of the WASE study [21] have shown that Asians had lower e 'speeds, higher E / e' and lower LAVIs in almost all age groups compared to Caucasians. Similar findings were reported by Chahal et al. [22]: while comparing data from healthy Caucasians and Indian Asians living in London, Asians had a significantly lower e 'rate and a higher E / e' than whites with similar E and E / A rates. Lower indices of the main LV diastolic function parameters served as the basis for the development of separate standards for ethnic Asians in a recently published study [23]. Nevertheless, in our study, E / A rates was higher in Shors men than non-indigenous men of Gornaya Shoria with arterial hypertension, differences in diastolic function were noted in Shors and non-indigenous women; it is quite possible that the reason for this is leveling of the initial differences following the development of the pathological changes.
In rural residents of Gornaya Shoria, the LV hypertrophy prevalence in hypertensive patients was higher in the Shor group than in the non-indigenous (Caucasian) group. At the same time, various genetic associations with LV hypertrophy were established in different ethnic groups. Among the Shors, these were the MTHFR gene according to the log-additive mode of inheritance, the A / G genotype of the ADRB1 gene among persons with normal body weight, the I / D genotype of the ACE gene among men; among Caucasians, the D / D genotype of the ACE gene for the codominant mode of inheritance, the NOS3 gene for the log-additive mode of inheritance [17]. In addition to genetic factors, many factors affect LV myocardial mass, including age, sex, body size and composition, level of physical activity, blood pressure (de Simone G. 2005), and presence of other diseases (for example, diabetes mellitus). In healthy representatives of the Shor nationality living in rural areas, in addition to genetic factors, LVMM is also influenced by the traditional way of life, which includes hunting, gathering, and high physical activity in the middle mountains. In our sample, living in a city significantly changes the lifestyle of the Shors, and we have not identified any differences in the severity of LVH, only noting differences in the factors associated with the LVH presence. Our data are consistent with the opinion that the influence of environment seems to be critical in explaining most of the ethnic differences in LV mass when compared with genetic factors [24].
What is the clinical significance of this study? While previous studies have found ethnic differences in geographically diverse populations, the impact of changes in environment and socioeconomic status remains unknown. Consequently, it remains unclear whether the normal performance for a particular ethnic group living in their home area will be the same compared to people of the same ethnic group living in a culturally and economically different environment? Changes in the habitat often entail changes in diet, lifestyle and, as a result, in physique, which can affect the norms of echocardiography values based on indexing body surface area (de Simone G. 2005). In this light, the fact of leveling of ethnic differences in the frequency of detection of LV hypertrophy in arterial hypertension when examining a cohort of urban residents in comparison with previously identified patterns in rural residents is of undoubted interest. This can be a useful addition to studying of adaptation to changing environmental conditions due to the intensive industrial development of the Gornaya Shoria region, urbanization and food system transformation (Mihalina EV, 2019), as well as the possibility of influencing these mechanisms in order to improve the quality of life and prevent cardiovascular disease risk factors.
Study limitation
The data obtained in this study, due to the small size of the sample, cannot be generalized to the entire Shor population and give not a global, but a preliminary idea., When studying the urbanized Shor population in this work, the effect of obesity on the structural and functional parameters of the heart was not considered due to the small number of Shor men with increased body weight. Age at menopause in women was not considered, which may have influenced the study results in female ethnic groups. Echocardiographic studies by one operator excluded the possibility of assessing inter-operator reproducibility. In this work, we did not compare the age indicators of the structure and function of the ventricles, since the study groups were comparable in age. Also, we did not use more modern methods for assessing the state of the left heart (for example, 3D-echocardiography), but our results are quite consistent with real clinical practice, where patients with arterial hypertension are usually examined using routine transthoracic echocardiography.
5. Conclusion
In the present study, hypertensive urbanized Shors had no significant difference in left ventricular dimensions compared to Caucasian. The LVMM index did not differ between the ethnic groups; however, the severe abnormal LVH was associated with glucose level in the Shors, and with SBP, DBP, and heart rate in Caucasians. The Shor men were more likely to have normal LV diastolic function and LV concentric remodeling, while non-indigenous men had normal LV geometry more often. This study can be useful in assessing the impact of the development of arterial hypertension, as well as the impact of changing the lifestyle of the Shors when moving to the city from rural areas on ethnic differences in echocardiography.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Conflicts of Interest
No conflicting relationship exists for any author.
References
- Kawel-Boehm N, Kronmal R, Eng J, Folsom A, Burke G, Carr JJ, Shea S, Lima JAC, Bluemke DA. Left Ventricular Mass at MRI and Long-term Risk of Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis (MESA). Radiology. 2019;293(1):107-114. [CrossRef]
- Lertlaksameewilai P, Songsangjinda T, Kaolawanich Y, Yindeengam A, Krittayaphong R. Extracellular volume and left ventricular hypertrophy by cardiac magnetic resonance are independent predictors of cardiovascular outcome in obesity. Sci Rep. 2022;12(1):18758. [CrossRef]
- Lang RM, Mor-Avi V. One Size Does Not Fit All: A Cliché or a Hard Fact in Cardiac Chamber Quantification? JACC Cardiovasc Imaging. 2015 Jun;8(6):666-8. [CrossRef]
- Asch FM, Banchs J, Price R, Rigolin V, Thomas JD, Weissman NJ, Lang RM. Need for a Global Definition of Normative Echo Values-Rationale and Design of the World Alliance of Societies of Echocardiography Normal Values Study (WASE). J Am Soc Echocardiogr. 2019;32(1):157-162.e2. [CrossRef]
- Piskorz, D. Ethnicity and Left Ventricular Hypertrophy: Tools and Uncertainties. High Blood Press Cardiovasc Prev. 2018 Sep;25(3):291-294. [CrossRef]
- Wegener A, Kaagaard MD, Gomes LC, Holm AE, Matos LO, Lima KO, Vieira IVM, de Souza RM, Olsen FJ, Marinho CRF, Biering-Sørensen T, Silvestre OM, Brainin P. Reference values for left ventricular dimensions, systolic and diastolic function: a study from the Amazon Basin of Brazil. Int J Cardiovasc Imaging. 2021 Nov 22. [CrossRef]
- Sheng Y, Li M, Xu M, Zhang Y, Xu J, Huang Y, Li X, Yao G, Sui W, Zhang M, Zhang Y, Zhang C, Zhang Y, Zhang M. Left ventricular and atrial remodelling in hypertensive patients using thresholds from international guidelines and EMINCA data. Eur Heart J Cardiovasc Imaging. 2022 Jan 24;23(2):166-174. [CrossRef]
- Vidula MK, Chirinos JA. Adverse cardiac remodelling: discerning the normal from the pathologic using ethnic-specific echocardiographic thresholds. Eur Heart J Cardiovasc Imaging. 2022;23(2):175-176. [CrossRef]
- Cuspidi C, Tadic M. Left ventricular hypertrophy in hypertension: Need of ethnic-specific criteria. J Clin Hypertens (Greenwich). 2022 Nov;24(11):1530-1531. [CrossRef]
- Asch FM, Miyoshi T, Addetia K, Citro R, Daimon M, Desale S, Fajardo PG, Kasliwal RR, Kirkpatrick JN, Monaghan MJ, Muraru D, Ogunyankin KO, Park SW, Ronderos RE, Sadeghpour A, Scalia GM, Takeuchi M, Tsang W, Tucay ES, Tude Rodrigues AC, Vivekanandan A, Zhang Y, Blitz A, Lang RM; WASE Investigators. Similarities and Differences in Left Ventricular Size and Function among Races and Nationalities: Results of the World Alliance Societies of Echocardiography Normal Values Study. J Am Soc Echocardiogr. 2019 Nov;32(11):1396-1406.e2. [CrossRef]
- Arkhipov, O.G. , Suslova N.S., Sumin A.N. Structural and Functional Indicators of Echocardiography in Healthy Representatives of Indigenous and Non-organized Urbanized Population of Gornaya Shoria. The Siberian Medical Journal. 2019;34(1):152–161. (in Russian). [CrossRef]
- Sumin AN, Gomozova NS, Shcheglova AV, Arkhipov OG. Ethnic differences in right ventricular structure and function in urbanized hypertensive patients in the Gornaya Shoriya region. Sci Rep. 2023 Mar 21;13(1):4628. [CrossRef]
- Mulerova T, Ogarkov M, Uchasova E, Voevoda M, Barbarash O. A comparison of the genetic and clinical risk factors for arterial hypertension between indigenous and non-indigenous people of the Shoria Mountain Region. Clin Exp Hypertens. 2018;40(4):324-331. [CrossRef]
- Mihalina EV, Mulerova TA, Polikutina OM, Ogarkov MYu. Prevalence of coronary artery disease in the indigenous population of Gornaya Shoria (the results of epidemiological studies in 1998-2001 and 2013-2017). Complex Issues of Cardiovascular Diseases. 2019; 8 (4S): 15-21. (in Russ.). [CrossRef]
- Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2015; 16:233-270.
- Marwick TH, Gillebert TC, Aurigemma G, Chirinos J, Derumeaux G, Galderisi M, Gottdiener J, Haluska B, Ofili E, Segers P, Senior R, Tapp RJ, Zamorano JL. Recommendations on the Use of Echocardiography in Adult Hypertension: A Report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE). J Am Soc Echocardiogr. 2015 Jul;28(7):727-54. [CrossRef]
- Barbarash OL, Mulerova TA, Maksimov VN, Chigisova AN, Voevoda MI, Ogarkov MY. Left Ventricular Myocardial Hypertrophy as a Result of Arterial Hypertension Among Mountain Shoria Population. The Role of Genetic Polymorphism. Kardiologiia. 2018 Sep;58(9):37-46. (in Russian).
- Park CM, March K, Ghosh AK, Jones S, Coady E, Tuson C, Francis D, Mayet J, Tillin T, Chaturvedi N, Hughes AD. Left-ventricular structure in the Southall And Brent REvisited (SABRE) study: explaining ethnic differences. Hypertension. 2013 May;61(5):1014-20. [CrossRef]
- Poppe KK, Bachmann ME, Triggs CM, Doughty RN, Whalley GA. Geographic variation in left ventricular mass and mass index: a systematic review. J Hum Hypertens. 2012 Jul;26(7):420-9. [CrossRef]
- Echocardiographic Normal Ranges Meta-Analysis of the Left Heart Collaboration. Ethnic-Specific Normative Reference Values for Echocardiographic LA and LV Size, LV Mass, and Systolic Function: The EchoNoRMAL Study. JACC Cardiovasc Imaging. 2015 Jun;8(6):656-65. [CrossRef]
- Miyoshi T, Addetia K, Citro R, Daimon M, Desale S, Fajardo PG, Kasliwal RR, Kirkpatrick JN, Monaghan MJ, Muraru D, Ogunyankin KO, Park SW, Ronderos RE, Sadeghpour A, Scalia GM, Takeuchi M, Tsang W, Tucay ES, Tude Rodrigues AC, Vivekanandan A, Zhang Y, Blitz A, Lang RM, Asch FM; WASE Investigators. Left Ventricular Diastolic Function in Healthy Adult Individuals: Results of the World Alliance Societies of Echocardiography Normal Values Study. J Am Soc Echocardiogr. 2020 Oct;33(10):1223-1233. [CrossRef]
- Chahal NS, Lim TK, Jain P, Chambers JC, Kooner JS, Senior R. Ethnicity-related differences in left ventricular function, structure and geometry: a population study of UK Indian Asian and European white subjects. Heart. 2010 Mar;96(6):466-71. [CrossRef]
- Chang SN, Sung KT, Huang WH, Lin JW, Chien SC, Hung TC, Su CH, Hung CL, Tsai CT, Wu YW, Chiang FT, Yeh HI, Hwang JJ. Sex, racial differences and healthy aging in normative reference ranges on diastolic function in Ethnic Asians: 2016 ASE guideline revisited. J Formos Med Assoc. 2021;120(12):2160-2175. [CrossRef]
- de Simone, G. Left ventricular hypertrophy in blacks and whites: different genes or different exposure? Hypertension. 2005;46(1):23-4. [CrossRef]
Figure 1.
Protocol flowchart.
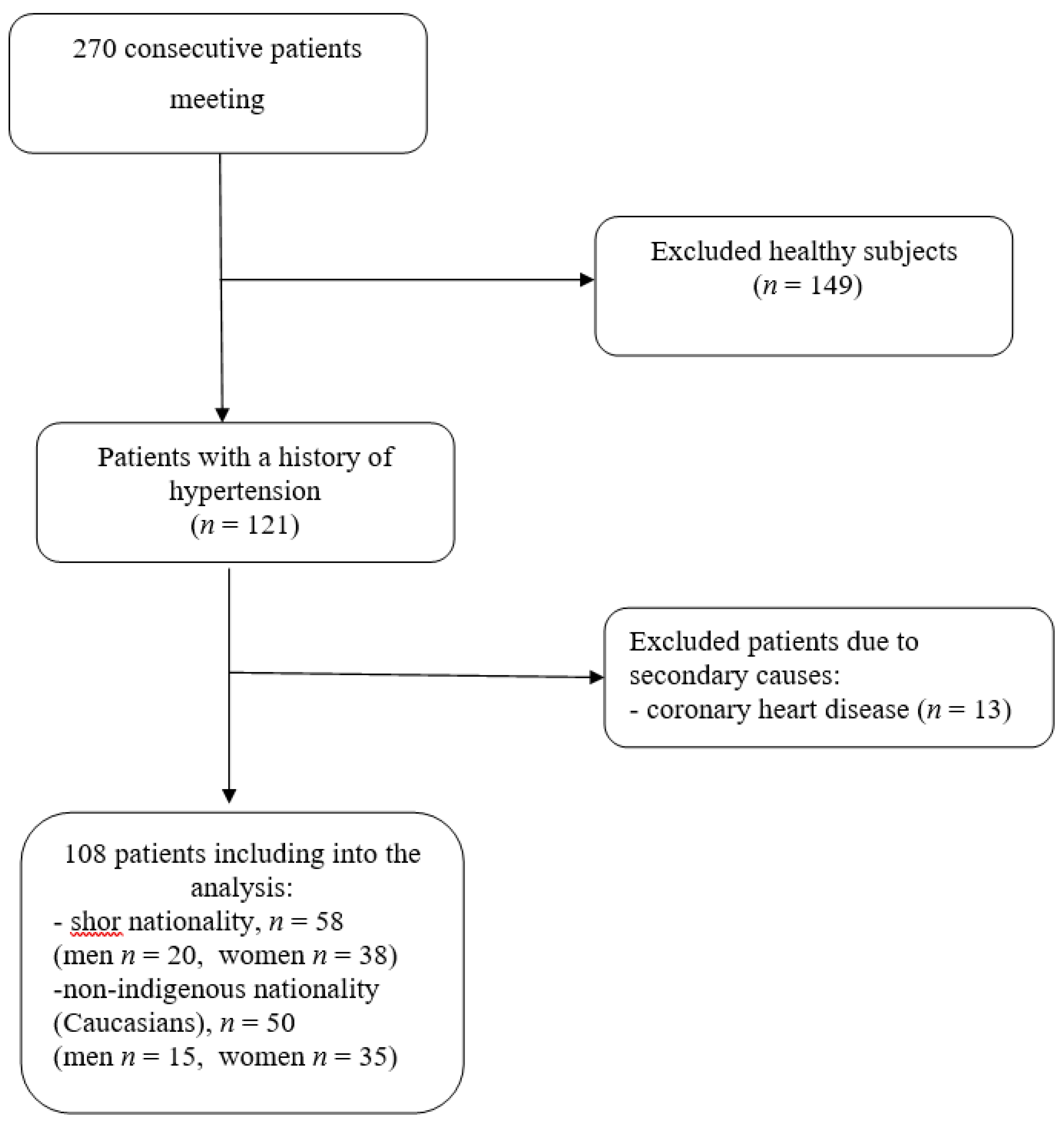
Figure 2.
The severity of LVH in patients of different ethnic groups. LVH – left ventricular hypertrophy.
Figure 2.
The severity of LVH in patients of different ethnic groups. LVH – left ventricular hypertrophy.
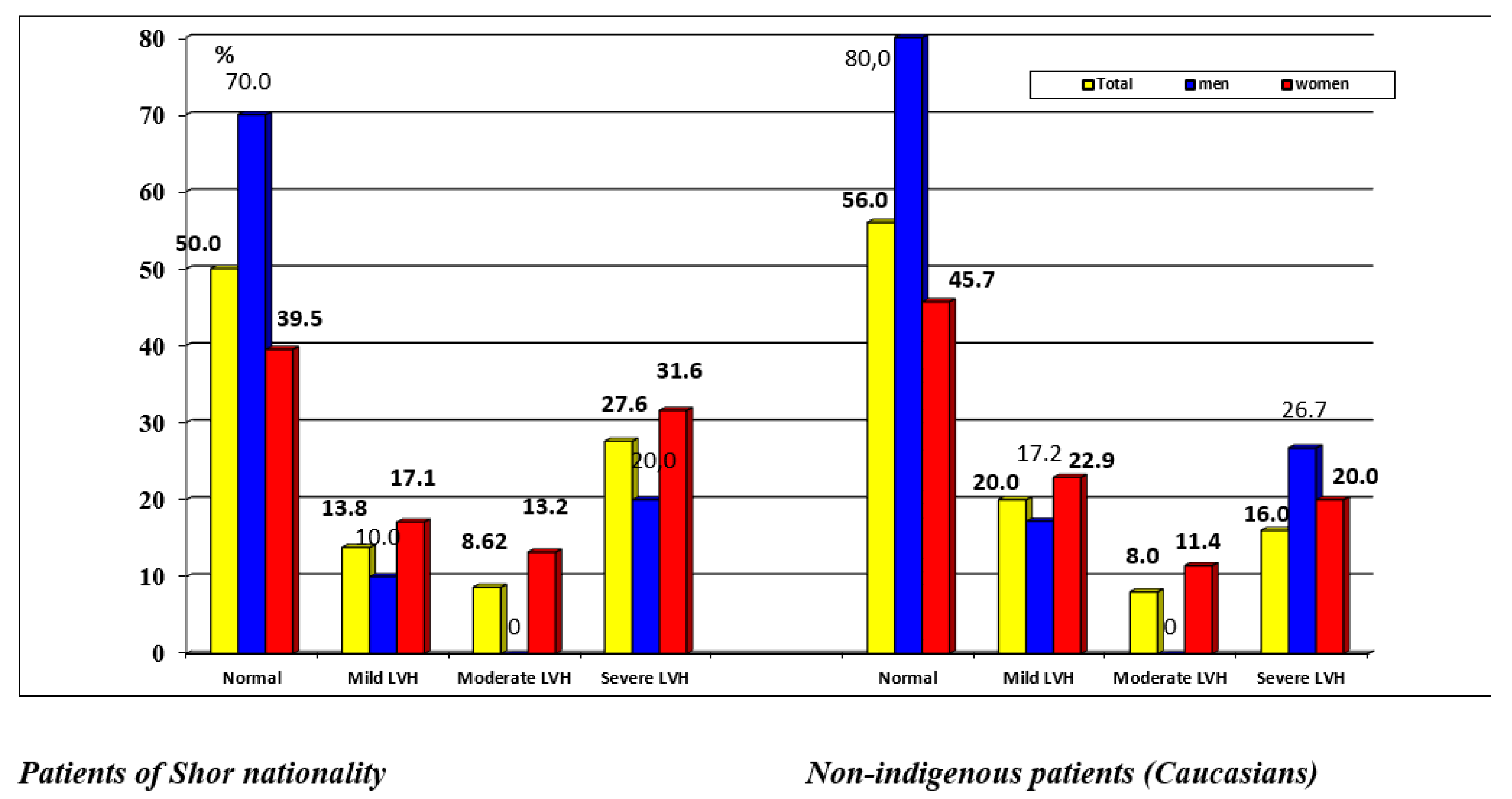
Figure 3.
Left ventricular remodeling in patients of different ethnic groups. Normal – normal left ventricular geometry, ELVH – eccentric left ventricular hypertrophy, CLVH – concentric left ventricular hypertrophy, CR - concentric left ventricular remodeling, * - p<0.05 compared with Shor men.
Figure 3.
Left ventricular remodeling in patients of different ethnic groups. Normal – normal left ventricular geometry, ELVH – eccentric left ventricular hypertrophy, CLVH – concentric left ventricular hypertrophy, CR - concentric left ventricular remodeling, * - p<0.05 compared with Shor men.
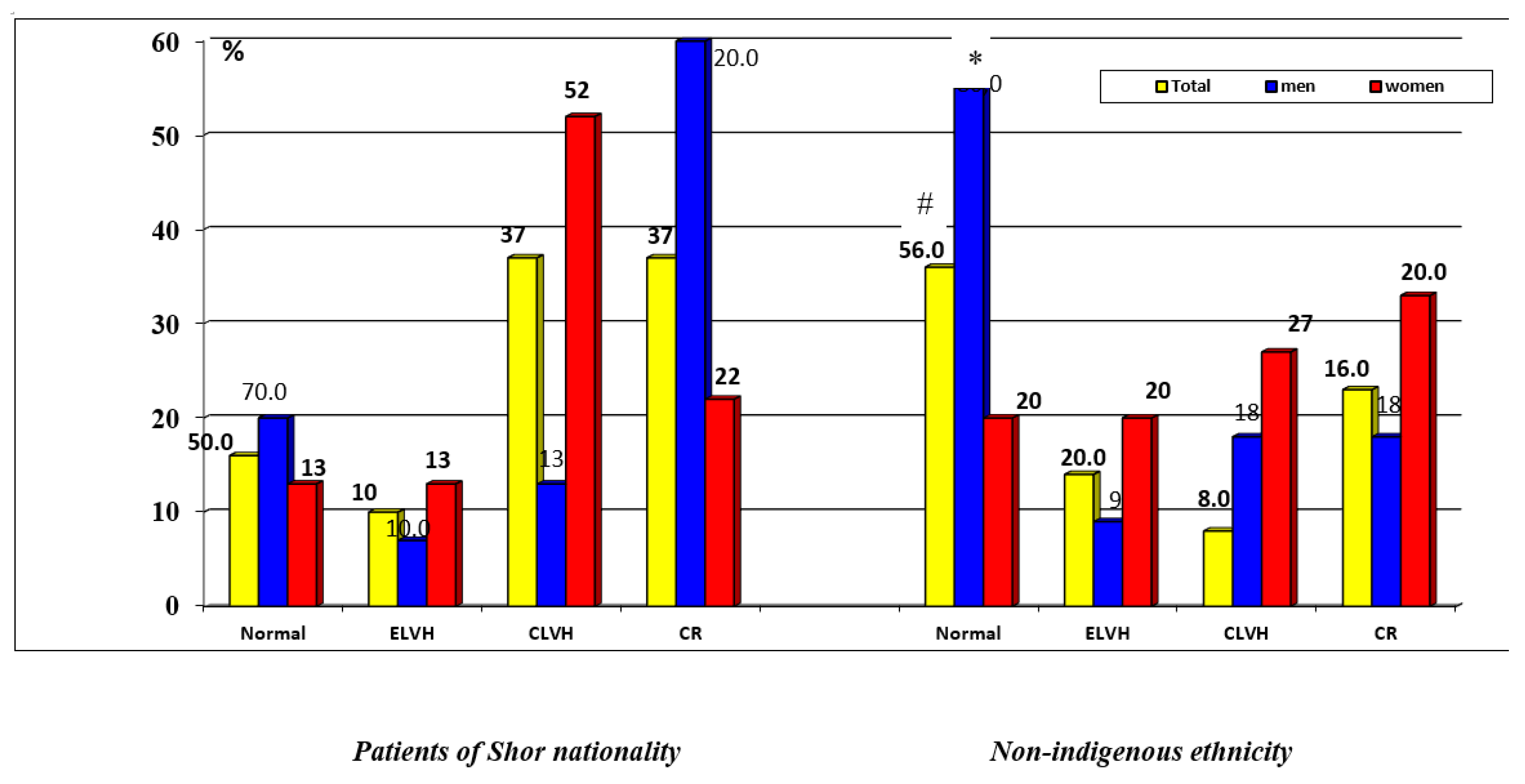
Figure 4.
Detection frequency of left ventricular diastolic dysfunction in patients of different ethnic groups. * P<0.05 compared with Shor men.
Figure 4.
Detection frequency of left ventricular diastolic dysfunction in patients of different ethnic groups. * P<0.05 compared with Shor men.
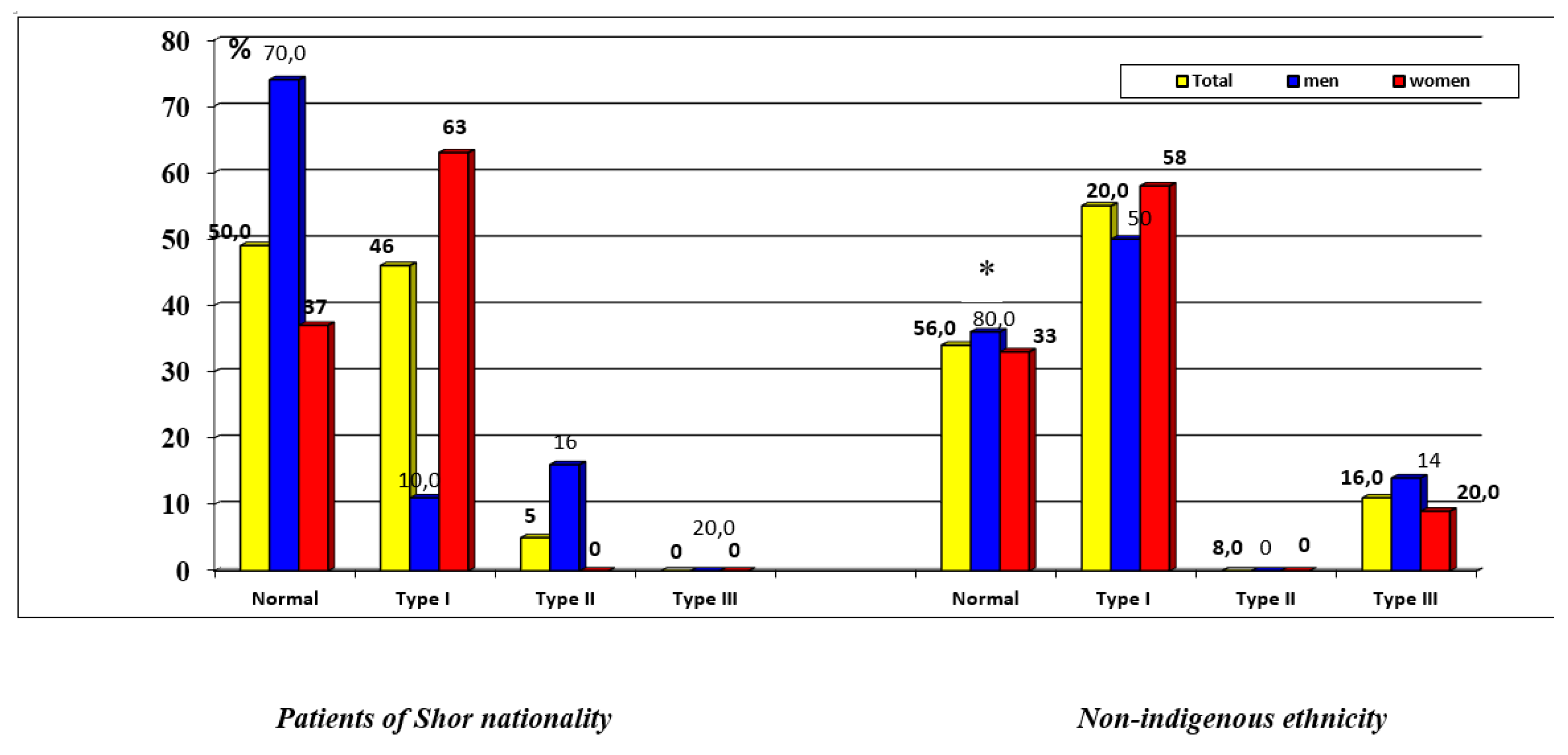

Table 1.
General characteristics of hypertensive patients of various ethnic groups.
| Patients of Shor nationality (n=58) | Patients with non-indigenous ethnicity (n=50) | Н | p | |||
|---|---|---|---|---|---|---|
| men (n=20) | women (n=38) | men (n=15) | women (n=35) | |||
| Age (years) | 51.5 [45-55] | 48 [43-53] | 52 [41-55] | 51 [44-55] | 2.11 | 0.27 |
| Weight (kg) | 65 [60-69] | 71 [64-80] ^ | 75 [65-90] * | 79 [67-88] | 10.77 | 0.005 |
| Height (cm) | 161 [157.5-166.5] | 156.5 [154-162] ^ | 169 [166-171] * | 160 [157-164] + | 28.93 | 0.036 |
| BSA (m2) | 1.7 [1.64-1.8] | 1.75 [1.7-1.8] ^ | 1.8 [1.7-1.9] * | 1.8 [1.7-1.9] | 9.63 | 0.004 |
| BMI (kg / m2) | 24.61[22.29-27.36] | 29.14 [26.48-32.79] ^ | 26.89[23.22-31.24] | 31.16 [26.98-33.79] | 15.48 | 0.0014 |
| Obesity | 0 (0%) | 2 (5.3%) | 2 (13.3%) | 3 (8.57%) | 2.87 | 0.41 |
| Elementary education | 2 (10%) | 2 (5.3%) | 0 (0%) | 1 (2.86%) | 0.43 | 0.5 |
| Secondary education | 9 (45%) | 14 (36.84%) | 1 (6.66%) * | 11 (31.43%) | 6.3 | 0.09 |
| Vocational education | 8 (40%) | 20 (52.6%) | 14 (93.3%) * | 20 (57.14%) + | 10.65 | 0.013 |
| Higher education | 1 (5%) | 2 (5.3%) | 0 (0%) | 3 (8.57%) | 1.49 | 0.68 |
| Hard physical labor | 16 (80%) | 20 (52.6%) ^ | 8 (53.3%) | 16 (45.7%) | 0.45 | 0.5 |
| Smoking | 14 (24.1%) | 9 (23.7%) ^ | 4 (26.6%) * | 5 (14.3%) | 11.54 | 0.003 |
| Cholesterol (mmol / L) | 6.65 [5.2-7.3] | 6.4 [5.9-6.9] | 6.4 [5.4-6.9] | 6.4 [5.9-7.4] | 1.47 | 0.73 |
| LDL (mmol / l) | 2.5 [2.0-3.9] | 2.9 [2.3-3.7] | 2.9 [2.5-4.1] | 3.8 [3.1-4.1] | 14.93 | 0.83 |
| HDL (mmol / L) | 1.2 [1.1-1.5] | 1.12 [0.96-1.59] | 1.05 [0.92-1.2] | 1.06 [0.94-1.2] | 6.28 | 0.21 |
| Glucose (mmol / L) | 5.14 [4.37-5.9] | 4.7 [4.2-5.5] | 5.8 [5.1-6.2] | 5.9 [5.1-6.1] | 12.85 | 0.33 |
| SBP (mm Hg) | 140 [125-150] | 140 [130-150] | 150 [130-160] | 140 [130-150] | 4,2 | 0.97 |
| DBP (mm Hg) | 80 [80-80] | 80 [80-80] | 80 [80-100] | 80 [80-90] | 6,9 | 0,44 |
Table 2.
Structural parameters of echocardiography in hypertensive patients of various ethnic groups.
Table 2.
Structural parameters of echocardiography in hypertensive patients of various ethnic groups.
| Patients of Shor nationality (n=58) |
Patients with non-indigenous ethnicity (n=50) |
Н | р | |||
|---|---|---|---|---|---|---|
| men (n=20) | women (n=38) | men (n=15) | women (n=35) | |||
| Aorta (mm) | 35.5 [33-37] | 37 [36-38] | 38 [37-38] | 37 [35-38] | 8.14 | 0.06 |
| Aorta index (mm/m2) | 29.5 [25.4-31] | 26 [24-30] | 28.3 [22.9-31.2] | 25.6 [22.2-30] | 4.14 | 0.1 |
| TPW (mm) | 11 [11.0-12.0] | 12 [11.0-13.0] | 11 [11.0-12.0] | 11 [11.0-13.0] | 1.25 | 0.38 |
| TPWi (mm/m2) | 9.06 [8.5-10.3] | 8.6 [7.2-10.3] | 8.8 [6.6-9.7] | 8.5 [7.5-9.6] | 3.7 | 0.15 |
| TIVS (mm) | 12 [11.0-13.0] | 12.5 [11.0-13.0] | 11 [11.0-12.0] | 12.0 [10.0-13.0] | 3.99 | 0.18 |
| TIVSi (mm/m2) | 9.8 [7.9-10.7] | 9.08 [8.09-10.4] | 8.8 [6.6-9.7] | 8.3 [7.2-9.5] | 8.7 | 0.39 |
| LVM (g) | 173.5 [155.5-193] | 176 [159-214] | 182 [167-196] | 185 [161-205] | 0.98 | 0.53 |
| LVMi (g/m2) | 141.9[119.7-164.2] | 132 [114-162] | 127.4 [105-147] | 134 [108.4-154] | 1.74 | 0.37 |
| EDD (mm) | 50 [48-53] | 53 [48-54] | 55.5 [53-56] | 51 [49-55] | 4.65 | 0.30 |
| EDV (ml) | 109.5 [103-122] | 132 [100-142] | 135 [127-150] | 124 [104-150] | 6.05 | 0.15 |
| LVEDVi (ml/m2) | 89.4 [84-98] | 86.7 [73.5-110] | 102 [77.9-120] | 89.8 [79.5-104.6] | 1.46 | 0.46 |
| LVEF % | 66 [62-69] | 65 [63-68] | 67 [64-70] | 67 [64-70] | 3.18 | 0.52 |
| LA (mm) | 38 [35-39] | 38 [37-40] | 39 [37-40] | 39 [37-40] | 4.43 | 0.26 |
| LAV (ml) | 81 [50-89] | 79 [57-88] | 89 [68-91] | 81 [66-89] | 4.12 | 0.68 |
| LAVi (ml/m2) | 63.2 [41.9-72.5] | 54.5 [44.5-62.5] | 64.3 [47.8-69.7] | 53.1 [40.4-66.4] | 3.46 | 0.14 |
| PA (mm) | 21 [20-21] | 21 [20-22] | 22 [20-22] | 21 [20-22] | 3.88 | 0.16 |
| PAi (mm/m2) | 17.2 [15-18] | 15.7 [13.9-17.9] ^ | 15.3 [12.6-17.6] | 15.4 [13-17.4] | 5.47 | 0.05 |
| RA (mm) | 32 [31.5-35] | 35 [32-36] ^ | 35 [33-38] * | 35 [32-38] | 7.59 | 0.04 |
| RAS (cm2) | 11.5 [11.5-14.4] | 14.4 [11.5-16.3] | 15.4 [12-17.5] | 14.2 [11.5-17] | 5.35 | 0.067 |
| RASi (cm2/m2) | 10 [8.4-11.7] | 10.3 [8.7-11.7] | 10.7 [9.3-12] | 9.3 [7.6-11.5] | 2.56 | 0.78 |
Table 3.
Indicators of diastolic function in patients with arterial hypertension of various ethnic groups.
Table 3.
Indicators of diastolic function in patients with arterial hypertension of various ethnic groups.
| Patients of Shor nationality (n=58) |
Patients with non-indigenous ethnicity (n=50) |
H | р | |||
|---|---|---|---|---|---|---|
| men (n=20) | women (n=38) | men (n=15) | women (n=35) | |||
| IVRT (msec) | 68 [60-81] | 81 [74-90] | 80 [67-104] | 89 [70-100] | 7.23 | 0.065 |
| E (cm/sec) | 76 [64-89.5] | 62.5 [56-76] | 69 [57-94] | 61.5 [53-76] | 4.74 | 0.112 |
| A (cm/sec) | 59.1 [47.1-73.1] | 71.3 [57.5-82.0] | 68.5 [48.2-83.0] | 72.7 [58.7-82.0] | 4.50 | 0.213 |
| Е/А | 1.3 [1.1-1.54] | 0.87 [0.75-1.15] | 0.99 [0.63-1.28] | 0.81 [0.71-1.27] | 4.70 | 0.016 |
| DT (msec) | 171.5 [148-200] | 203.5 [163-222] | 163 [115-222] | 177 [137-214] | 3.71 | 0.295 |
| Vf (cm/sec) | 47 [42-50.5] | 47 [35-53] | 42 [39-54] | 48 [39-60] | 1.94 | 0.585 |
| е' (cm/sec) | 12.0 [10-13] | 11.5 [9.0-13.0] | 11.0 [10.0-14.0] | 11.0 [9.0-14.0] | 0.581 | 0.901 |
| а' (cm/sec) | 9.4 [6.5-12.0] | 10.8 [8.2-12.8] | 9.4 [6.7-12.03] | 10.0 [9.2-12.6] | 2.380 | 0.497 |
| е'/ а' | 1.36 [0.77-1.7] | 1.0 [0.87-1.33] | 1.04 [0.79-1.73] | 1.2 [0.9-1.6] | 1.715 | 0.634 |
| s' (cm/sec) | 9.5 [9.0-12.0] | 9.0 [7.0-10.7] | 9.0 [7.8-13.0] | 10.0 [8.0-12.0] | 2.064 | 0.559 |
| е'sept (cm/sec) | 9.5 [9.0-12.0] | 9.8 [7.0-12.0] | 9.0 [8.0-11.0] | 10.0 [7.8-11.0] | 1.371 | 0.712 |
| е' sept/ а' sept | 1.0 [0.73-1.2] | 0.97 [0.7-1.1] | 1.06 [0.6-1.3] | 0.95 [0.73-1.3] | 0.914 | 0.822 |
| s' sept (cm/sec) | 10.3 [10.0-11.3] | 9.0 [8.0-10.0] ^ | 9.0 [8.0-11.0] | 9.0 [8.0-11.0] | 7.11 | 0.069 |
| Е/е' | 0.37 [0.30-0.44] | 0.30 [0.26-0.41] ^ | 0.37 [0.29-0.47] | 0.32 [0.28-0.47] | 2.68 | 0.44 |
| Tei index | 0.37 [0.29-0.44] | 0.49 [0.40-0.58] ^ | 0.49 [0.42-0.73] * | 0.50 [0.39-0.64] | 8.646 | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



