
Submitted:
22 June 2023
Posted:
27 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
(1) Background: The COVID-19 pandemic has affected healthcare utilization rates on a global scale. This study aimed to analyze whether the COVID-19 pandemic affected the characteristics of first-visit patients with peripheral facial palsy visiting a Korean Medicine hospital and to observe characteristics changes in them. (2) Methods: This study analyzed the electronic medical records of 2,310 first-visit patients with peripheral facial palsy who visited the Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from January 1, 2019 to December 31, 2021 in terms of demographic characteristics, disease phase, residence locations, hospital visit route, and patient care type. (3) Results: There were significant relationships between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by disease phase (p=0.043), residence locations (p=0.003), residence locations in Seoul (p=0.003), and patient care types (p=0.003). (4) Conclusions: There were several differences in characteristics of first-visit patients with peripheral facial palsy visiting a Korean Medicine hospital during COVID-19 pandemic in terms of demographic characteristics, disease phase, residence locations, residence locations in Seoul, and patient care types.
Keywords:
COVID-19
; first-visit
; peripheral facial palsy
; Korean Medicine hospital
1. Introduction
The novel coronavirus disease (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in Wuhan, China, on 31 December 2019 [1]. The World Health Organization declared a COVID-19 pandemic on March 11, 2020. As of August 28th, 2022, SARS-CoV-2 infected approximately 598 million individuals and caused 6.4 million deaths worldwide [2]. The first confirmed case in South Korea was reported on January 20, 2020. As of September 6th, 2022, SARS-CoV-2 infected approximately 23,706,477 individuals and caused 27,193 deaths in South Korea [3].
The COVID-19 pandemic has affected healthcare utilization rates on a global scale. In South Korea, compared to the same period last year, patients using healthcare due to respiratory infections, digestive or intestinal infections and injury decreased by 51.9%, 31.3%, and 12.6%, respectively. In contrast, the number of patients with mood disorders, increased by 7.1%. Preventive measures, such as wearing masks, hand washing, and social distancing, are presumed to have led to these changes. In addition, the number of patients using Korean Medicine decreased by 12.5%. This decrease is presumed to be due to a reluctance of healthcare utilization in the case of not urgent situations during the COVID-19 pandemic [4]. As such, COVID-19 had a significant impact on all outpatients, including first-visit and revisit.
Facial nerve disorder is a disease with a high proportion in Korean Medicine, ranking 24th to 27th among the Korean Medicine common diseases over the past 10 years. The number of patients visiting Korean medical institutions due to facial nerve disorder has decreased gradually over the past decade; however, the decrease was rapid in 2020 when the COVID-19 pandemic occurred [5]. Several studies have suggested an association between COVID-19 and peripheral facial palsy. A higher occurrence of facial palsy was proposed during the COVID-19 pandemic than in the same period in the previous year [6]. Couple of cases of facial palsy after COVID-19 and facial nerve palsy as the initial clinical manifestations of COVID-19 infection have been reported [7,8,9]. However, various studies have proposed that there is no association between COVID-19 and peripheral facial palsy. Some studies have even argued that there is not enough evidence to attribute the increased prevalence of facial palsy to COVID-19 [10,11,12]. In addition, after the COVID-19 vaccine was introduced, there was a controversy regarding whether there was an association between COVID-19 vaccination and peripheral facial palsy [13,14,15,16,17,18,19].
Altogether, changes in the utilization of health care services due to COVID-19 and the association between the facial palsy and COVID-19 or the COVID-19 vaccine may have an influence on the patients with facial palsy. A few previous studies examined the utilization of Korean Medicine after the COVID-19 pandemic. The Korea Institute of Oriental Medicine published the results of its survey titled “Utilization of Korean Medicine and Consumption of Korean Medicine” in 2020 [20]. Several studies reported the trends of patients visiting Korean Medicine hospitals before and during the COVID-19 pandemic [21,22,23]. However, as far as we know, no previous study has investigated patients visiting a Korean Medicine hospital for a single disease, including facial palsy.
This study aimed to analyze how the COVID-19 pandemic affected the utilization of a Korean Medicine hospital by first-visit patients with peripheral facial palsy and to suggest future directions for facial palsy treatment in Korean Medicine hospitals. First, we investigate whether there is a change in the number of first-visit patients and in demographic characteristics in terms of age, sex, lesion site, and predisposing factors before and during COVID-19. Second, we determine if there is a difference in the distribution of disease phases before and during COVID-19. Third, we investigate if there is a difference by residence locations before and during COVID-19. Fourth, we determine whether there is change in patient care type before and during COVID-19.
2. Materials and Methods
2.1. Data Source and Ethics Statement
The data were collected from first-time patients who visited the Facial Palsy Center of Korean Medicine Hospital, Kyung Hee University Medical Center from January 01, 2019, to December 31, 2021. Since the first confirmed case of COVID-19 occurred in Korea in January 2020, the analysis was divided into the pre-COVID-19 period and the COVID-19 pandemic period based on January 2020. The COVID-19 pandemic period was divided into the first year and the second year, and whether there were differences in patient characteristics by years 2019, 2020, and 2021 were analyzed.
This study was approved by the Institutional Review Board of Kyung Hee university Korean Medicine hospital (IRB no: KOMCIRB 2022-01-001). Patient consent was not required due to the retrospective use of anonymous clinical data.
2.2. Inclusion and Exclusion Criteria
Patients with peripheral facial palsy (Bell’s palsy, Ramsay-Hunt syndrome, or sequelae of peripheral facial palsy) were included. Patients with non-peripheral facial palsy (central facial palsy, traumatic facial nerve injury, Guillain Barre syndrome, plastic surgery side effects, simple paresthesia, simple angular deviation) were excluded.
2.3. Extraction of Demographic and Clinical Characteristics
The following data were collected from electronical medical records at Kyung Hee university Korean Medicine hospital.
- 1)
- First visit date
- 2)
- Sex: male, female
- 3)
- Age groups: under 20 years, 20s-30s (20-39 years), 40s-50s (40-59 years), over 60 years
- 4)
- Lesion site: left, right
- 5)
- Predisposing factors: fatigue and overwork, insomnia, stress, on a diet, exposure to severe temperature difference, virus disease (i.e., cold, enteritis), Covid-19 vaccination, others
- 6)
- Disease phase: acute phase (within 7 days from onset), subacute phase (over 7 days and within 3 months from onset), chronic phase (over 3 months)
- 7)
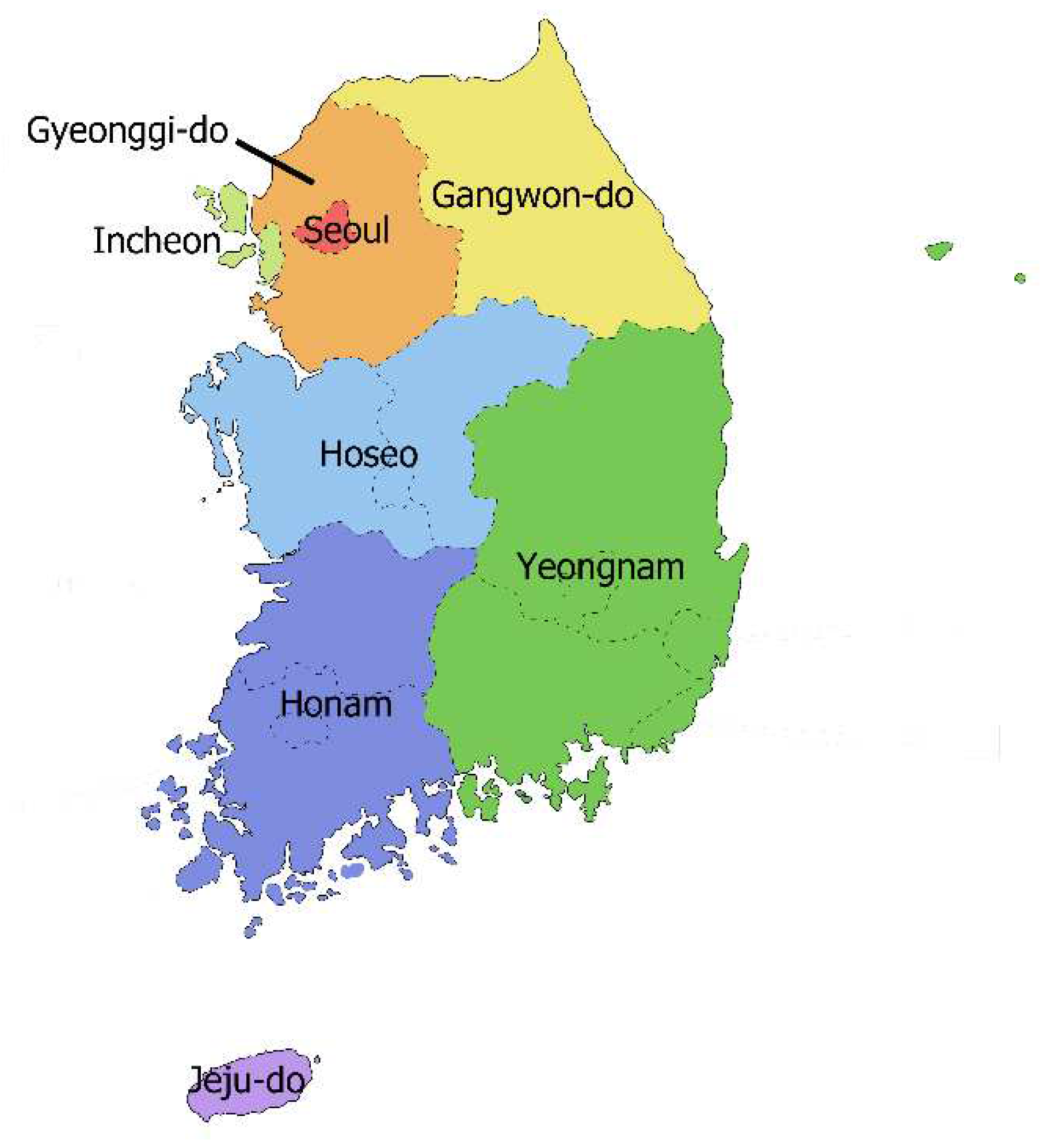
- Residence: Seoul, Gyeonggi-do, Incheon, Hoseo region (Chungchoeng-do, Daejeon, Sejong), Gangwon-do, Yeongnam region (Gyeongsang-do, Busan, Ulsan, Daegu), Honam region (Jeolla-do, Gwangju), Jeju-do, Foreign region (Figure A)
- 8)
- Residence in Seoul: northeastern region, northwestern region, inner city region, southeastern region, southwestern region
- 9)
- Hospital visit routes: ‘no treatment prior to visit’, ‘only Western Medicine treatment prior to visit’, ‘only Korean Medicine treatment prior to visit’, ‘both Western and Korean Medicine treatment prior to visit’
- 10)
- Patient care type: only outpatient care, both outpatient and inpatient care
2.4. Statistical Analysis
Statistical analysis was performed by using the Statistical Program for Social Science (SPSS), ver. 28.0.0.0. for windows. Chi-square test and Fisher's exact test were used to compare the frequencies and proportions of categorical variables, respectively, between the groups of first-visit patients with peripheral facial nerve palsy before and during the COVID-19 pandemic; annual analyses from 2019 to 2021 and from 2020 to 2021 were also conducted. Statistical significance was set at p <0.05. Monte Carlo simulation was used to calculate the p-value when data with too many variables were being analyzed and the p-value could not be calculated using SPSS.
3. Results
3.1. Total Numbers of Patients by Year
There were 2,381 patients who first visited the Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from January 01, 2019, to December 31, 2021. Sixty-six patients had central or secondary facial palsy, and five patients were excluded due to insufficient data. A total of 2,310 first-time patients were included in this study, and data were extracted from their medical records.
From January 1, 2019, to December 31, 2019, 897 patients visited the Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center. From January 1, 2020, to December 31, 2020, and from January 1, 2021, to December 31, 2021, 716 and 697 patients visited the hospital, respectively. The numbers of patients who visited the hospital in the years 2019, 2020, and 2021 are summarized in Figure 1. The monthly numbers of first-visit patients are presented to determine whether the COVID-19 pandemic waves overlapped with the timing of patient decline in Figure 2. However, the COVID-19 pandemic waves and periods of patient decline did not overlap.
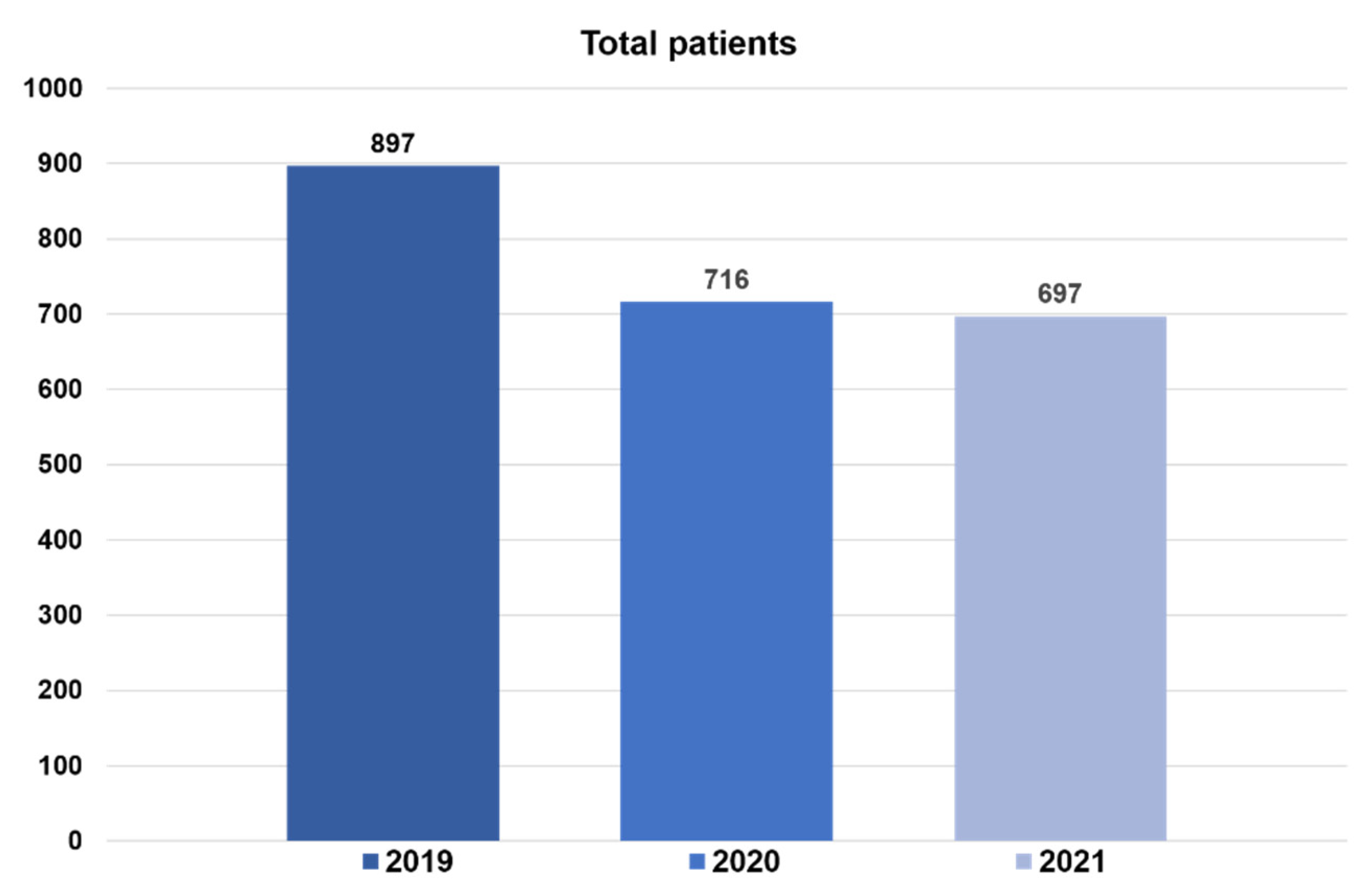

Figure A.
The number of first-visit patients visiting Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from 2019 to 2021
Figure A.
The number of first-visit patients visiting Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from 2019 to 2021
Figure B.
The monthly number of first-visit patients visiting Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from 2019 to 2021. Vertical dotted line indicates the start of the COVID-19 in South Korea. Shaded part indicates the 1st, 2nd, 3rd and 4th wave of COVID-19 pandemic.
Figure B.
The monthly number of first-visit patients visiting Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center from 2019 to 2021. Vertical dotted line indicates the start of the COVID-19 in South Korea. Shaded part indicates the 1st, 2nd, 3rd and 4th wave of COVID-19 pandemic.
3.2. Demographic Characteristics
The demographic characteristics of patients before and during COVID-19 were compared through percentages. The proportion of female patients increased by 2.9%, from 51.5% to 54.4% during the COVID-19 pandemic. The proportion of female patients continuously increased by 1.7%, from 51.5% to 53.2% in 2020 compared to that in 2019, and by 2.3%, from 53.2% to 55.5% in 2021 compared to that in 2020. The proportion of those under 20 and those in their 40s and 50s decreased during the COVID-19 pandemic compared to before COVID-19, while those in their 60s and older increased. There was no difference between the proportion of left and right lesions, and no characteristic changes and no tendency was found (Table 1).
Fatigue and overwork were the most common predisposing factors in the all years (63.3% in 2019, 58.2% in 2020, and 52.0% in 2021), followed by stress (51.8% in 2019, 49.4% in 2020, and 45.8% in 2021), and insomnia (46.6% in 2019, 44.9% in 2020, and 44.1% in 2021). The proportions of viral diseases, such as cold and enteritis, decreased during the COVID-19 pandemic (17.9% in 2019, 6.3% in 2020, and 1.8% in 2021). Additionally, the category of COVID-19 vaccination was newly included in 2021. A total of 24 patients complained of peripheral facial palsy after the COVID-19 vaccination (Table 2).
3.3. Disease Phase Distribution
The proportion of acute patients increased by 5.3%, from 48.7% before COVID-19 to 54.0% during the COVID-19 pandemic, the proportion of subacute patients decreased by 4.3%, from 36.5% to 32.2%, and the proportion of chronic patients decreased by 1.0%, from 14.8% to 13.8% (Table 3). There was a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by disease phase according to the chi-square analysis (p=0.043). There was a no relationship between the years from COVID-19 pandemic (i.e., 1st and 2nd year of COVID-19 pandemic) and the number of patients by disease phase (p=0.359).
3.4. Distribution of Residence Locations
The residence of patients who visited the hospital with facial paralysis was analyzed, and the proportion of residents in Seoul increased from 53.6% to 57.4% after the COVID-19 outbreak. The proportion of patients visiting from all regions except Seoul and Honam decreased during COVID-19. The proportions of patients visiting from Seoul were the highest in all years (53.6% in 2019, 57.4% in 2020, and 57.4% in 2021), followed by the proportions of those living in Gyeonggi (30.4% in 2019, 29.9% in 2020, and 29.3% in 2021) (Table 4). According to the chi-square analysis, there was a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by location of residence (p=0.003). And there was no relationship between the years of the COVID-19 pandemic (i.e., 1st and 2nd year of the COVID-19 pandemic) and the number of patients by location of residence.
In all the years, the proportions of visitors from the capital regions (Seoul, Gyeonggi-do, and Incheon) were the highest for the acute phase, followed by the subacute and chronic phase, whereas the proportions of visitors from the non-capital regions (Hoseo, Gangwon, Yeongnam, Honam, and Jeju) were the highest for the chronic phase, followed by the subacute and acute phases. In patients stratified by disease phase, there was a no relationship between the presence of the COVID-19 pandemic (i.e., before and during) and number of patients by location of residence (Table B1, Table B2 and Table B3).
3.5. Distribution of Residence Locations in Seoul
The proportion of patients from the northeastern region increased by 7.4%, from 59.7% to 67.1% during the COVID-19 pandemic. The proportions of patients visiting from the northeastern region showed a constant increase in the annual analyses: 59.7% in 2019, 66.9% in 2020, and 67.3% in 2021. The proportion of patients visiting from all regions except the northeastern and inner-city region decreased during COVID-19 (Table 5). There was a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and number of patients residing in Seoul (p=0.003). There was no relationship between the years from COVID-19 pandemic (i.e., 1st and 2nd year of COVID-19 pandemic) and the number of patients residing in Seoul (p=0.960).
3.6. Distribution of the Hospital Visit Routes
Both before COVID-19 and during the pandemic, the proportion of patients who visited hospitals after only Western medicine treatment was the highest, followed by after both Western and Korean Medicine treatment, after only Korean Medicine treatment, and after no treatment. (Table 6). There was no statistically significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by hospital visit route. And, there was no relationship between the years of COVID-19 pandemic (i.e., 1st and 2nd year of COVID-19 pandemic) and the number of patients by hospital visit route.
Regarding the proportions of visits by disease phase, the proportion of patients visiting the hospital after no treatment in all phases consistently decreased (Table C1, Table C2 and Table C3). In patients stratified by disease phase, there was no relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by hospital visit route.
3.7. Distribution of Patient Care Type
Compared to before COVID-19, the proportion of patients receiving only outpatient treatment during the COVID-19 pandemic has been steadily increasing year by year. In contrast, the proportion of outpatient and hospitalization patients decreased yearly (Table 7). There was a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during COVID-19) and the number of patients by patient care type (p=0.003). There was also a significant correlation between the time from COVID-19 (i.e., 2020 and 2021) and the number of patients by patient care type (p=0.016).
4. Discussion
Facial nerve palsy is a disease whose main symptom is paralysis of the facial muscles due to damage to the facial nerve [24]. Among them, peripheral facial palsy occurs mostly idiopathically (Bell's palsy) and also occurs with herpes zoster (Ramsay Hunt syndrome). It occurs secondary to other diseases, surgery, and trauma [25]. The most crucial treatment for peripheral facial palsy is to reduce the number of nerve fibers in the Wallerian degeneration state between about 2 and 14 days to help recovery of facial nerves. In Western medicine, early treatment with prednisolone significantly improves the chances of recovery [26]. And in Korean Medicine, acupuncture, herbal medicine, herbal acupuncture, and physical therapy are conducted to help quick recovery [27].
Regarding health service utilization in South Korea after the COVID-19 pandemic, the proportion of patients using Korean Medicine decreased by 12.5% compared to the last year [4]. The number of patients who visited Korean medical institutions for facial nerve disorders decreased gradually over the past decade but decreased rapidly in 2020 when the COVID-19 pandemic occurred [5]. This change in health service utilization is presumed to be due to new variations such as wearing masks, washing hands, social distancing, and concerns over COVID-19 infection in the hospital. The first-visit patient refers to a patient who has never been treated by a doctor in the same department at the same medical institution for the corresponding disease [28]. Unlike revisit patients, first-visit patients have not experienced the medical service of a hospital before, especially human factors such as skills, kindness, and detailed explanations of medical staff. Accordingly, they choose hospitals considering physical factors such as medical equipment, rest areas or convenience facilities, cleanliness of the environment, parking spaces, accessibility factors such as the location of the hospital, and efficiency factors such as waiting time, convenience of treatment procedure, collaborative practice more importantly [29].
In this study, we aimed to determine whether the COVID-19 pandemic affected the characteristics of first-visit patients with peripheral facial palsy visiting a Korean Medicine Hospital. The reason for limiting patients to first-visit patients is to observe the differences of health service utilization after COVID-19, excluding patient loyalty and trust from existing experiences in hospitals and medical staffs. In addition, since early treatment of peripheral facial palsy is important, we tried to confirm the specificity of the disease through first-time patients.
A total of 2,310 first-time patients visited the Facial Palsy Center, Korean Medicine Hospital, Kyung Hee University Medical Center for peripheral facial palsy from January 1, 2019, to December 31, 2021. From 2019 to 2020, the number of patients decreased by 20.2%, and from 2020 to 2021, it decreased by 2.7%. This decrease was particularly high between 2019 and 2020, possibly owing to a decrease in medical care utilization after the COVID-19 outbreak [4]. Considering the results of the survey that the number of patients using Korean Medicine decreased by 12.5% after the outbreak of COVID-19 and the results of the study that the number of first-time patients visiting the department of acupuncture and moxibustion at a Korean Medicine hospital in Daejeon decreased by 15.2%, this decrease was large. Moreover, we investigated whether a series of COVID-19 waves overlapped with the timing of patient decline by month, but it seems that there was no direct impact of a series of COVID-19 waves on the patient decline.
Overall, before COVID-19, the proportion of female patients was similar to that of male patients. Similarly, a previous study showed no difference in the incidence of peripheral facial palsy by sex [30]. During COVID-19, the proportion of female patients steadily increased with time. In contrast, the proportion of male patients persistently decreased. This is contrary to the results of a previous study that reported woman’s utilization of medical services decreased during the COVID-19 pandemic [31]. It seems that there was no effect by sex on first-visit patients with peripheral facial palsy during COVID-19.
The proportion of patients under 20 years and in their 40s-50s persistently decreased, and that of patients over 60 persistently increased during COVID-19. Patients in their 40s–50s accounted for the highest proportion in 2019 and 2020; however, those over 60 accounted for the highest proportion in 2021. These results are consistent with the findings of a previous study that showed that the medical utilization rate among those under the age of 18 and those in their 20s–40s decreased significantly during the COVID-19 pandemic, while the rate of medical utilization rate among those aged 60 and older slightly decreased [32]. This result can be attributed to several complex factors, such as the tendency of older adults to maintain medical care utilization despite the pandemic, underestimation of subjective health conditions, and increase in the number of the population aged over 65 years every year [22,33].
Analysis of the distribution of predisposing factors by year among patients in the acute phase revealed that fatigue and overwork were the most common factors in all the years, followed by stress and insomnia. Unlike previous surveys [31] that the psychology of stress, depression, and anxiety increased due to COVID-19, the proportion of psychological factors such as stress or insomnia did not increase. Characteristically, the proportions of viral diseases, such as colds and enteritis, plummeted during the COVID-19 pandemic. This result corresponds to a survey on public healthcare utilization in which the number of patients with colds and influenza decreased after wearing masks during the COVID-19 pandemic [4]. In addition, starting vaccination in Korea from February 2021, the category of COVID-19 vaccination was newly added and investigated in 2021. A total of 24 patients complained of peripheral facial palsy after the COVID-19 vaccination. There were no cases of COVID-19 as a predisposing factor for facial palsy because it was impossible for patients in the acute phase of COVID-19 to visit a Korean Medicine hospital owing to self-isolation or hospitalization at Western hospitals.
In our study, the acute phase was the period within seven days of onset, the subacute phase was more than seven days and within three months after onset, and the chronic phase was more than three months after onset [34]. As the number of patients with various viral infections significantly decreased due to preventive measures during COVID-19, we aimed to confirm whether the proportion of patients in the acute phase decreased. During the COVID-19 pandemic, compared to pre-pandemic, the proportion of patients in the acute phase increased and decreased in the subacute and chronic phases. The proportion of patients in acute phase continuously increased, indicating that there was no effect of the decrease in viral infection. Given that the proportion of patients in acute phase continues to increase, we can assume that the perception that patients in acute phase need to visit a hospital as soon as possible for treatment continuously increased regardless of the pandemic situation. In contrast, the proportion of patients in subacute and chronic phases decreased, possibly due to reduced availability of non-urgent care in medical care during COVID-19 [4]. The decrease in patients in the chronic phase was smaller than in the subacute phase. This is presumed to be due to a tendency of chronic patients with sequelae of facial palsy after moderate or severe facial nerve damage to visit higher institutions after receiving treatment at primary medical institutions. Analysis of the proportion of patients by disease phase revealed a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients stratified by disease phase (p=0.043).
The patient residence was analyzed to see any changes in the regional distribution of patients visiting hospitals after social distancing. During the COVID-19 pandemic, the proportion of patients residing in Seoul increased, and the proportion of patients visiting from outside Seoul decreased, likely related to the avoidance of long-distance visits due to social distancing. Additional analyzes were performed to determine if there were differences in patient proportions between residences according to disease stage. In all patient groups by disease phase, the proportions of patients residing in Seoul and other capital regions (Seoul, Gyeonggi-do, Incheon) increased during COVID-19. We can assume that intention to avoid long-distance visits due to social distancing appear in all patient groups by disease phase. Interestingly, the proportions of patients were the highest in the acute phase, followed by the subacute and chronic phases in Seoul and other capital regions (Seoul, Gyeonggi-do, Incheon), while the proportions of patients were the highest in the chronic phase, followed by the subacute and acute phases in the non-capital regions (Hoseo, Gangwon, Yeongnam, Honam, and Jeju). Patients generally visit medical facilities in regions other than their residence locations for various reasons, such as preference for hospital depending on the severity of the disease, recommendations from medical staffs or surrounding people, dissatisfaction with existing hospitals, psychological factors, and preference for specific medical facilities and medical staff [35]. Considering that the treatment of facial palsy does not involve complicated techniques, the medical service levels among various Korean Medicine clinics and hospitals can be considered to be similar; hence, for subacute and chronic patients rather than acute patients, the current results can be attributed to psychological factors, such as dissatisfaction with existing hospitals or choice associated with no regret. However, in patients stratified by disease phase, there was no statistically significant relationship between presence of the COVID-19 pandemic (i.e., before and during) and the number of patients by location of residence.
During the COVID-19 pandemic, the proportion of residents in the northeast area of Seoul increased from 59.7% to 67.1%. It is estimated that the location of the hospital, which is included in the northeastern region, has produced this result. Similar to changes in the distribution of patients' residences, the tendency to avoid long-distance visits due to social distancing may have played a role. There was a statistically significant correlation between the COVID-19 pandemic (before and after) and the number of patients residing in Seoul (p=0.003).
From 2019 to 2021, in all years, there was no change in the order of the proportion of hospital visit routes, regardless of COVID-19. And there was no statistically significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients stratified by hospital visit. Characteristically, the proportion of patients visiting the hospital after no treatment in all phases consistently decreased. In particular, the proportion of patients in the acute phase who visited the hospital after no treatment decreased from 2019 to 15.1%, 14.6%, and 10.9% annually. This shows that despite the COVID-19 pandemic, awareness that patients with acute facial paralysis should receive appropriate treatment quickly is increasing, such as prompt treatment such as taking steroids within three days of onset is recommended in the case of peripheral facial paralysis [36].
To determine whether COVID-19 has changed the types of patient care among patients in the acute phase, we investigate the proportion of patients who received only outpatient treatment and patients who receive both outpatient and inpatient treatment in the Korean Medicine hospital. The proportion of patients who received both outpatient and inpatient treatment persistently decreased, but the proportion of patients who received only outpatient treatment persistently increased during COVID-19. This decrease is similar to a previous study [37], which showed a decrease in the number of people visiting medical institutions for hospitalization during the COVID-19 epidemic. Several complicating factors may have played a role in this process. In the early days of the COVID-19 epidemic in South Korea, the epidemic spread rapidly in medical and living facilities [38], so inpatients had higher anxiety about infection than outpatients [37]. In addition, the fact that facial paralysis reduces the quality of life and interferes with social life, but it is not life-threatening [39], and the inconvenience of having to undergo a COVID-19 PCR test before hospitalization may also have had an impact. There was a significant relationship between the presence of the COVID-19 pandemic (i.e., before and during) and the number of patients who received only outpatient treatment (Kyung Hee University Korean Medicine Hospital) (p=0.003). And there was a significant relationship between the time from COVID-19 (i.e., 2020 and 2021) and the number of patients by patient care type (p=0.016). Unlike other analyzed items, there was a difference between the first and second years of COVID-19. The prolonged COVID-19 pandemic seems to have continuously affected the type of patient care.
This study has some limitations. Study data collection ended on December 31, 2021, before the end of the COVID-19 outbreak. Since this study analyzed the data of a single Korean Medicine hospital were analyzed in this study, the results cannot be generalized to all Korean Medicine hospitals. Because patients infected with COVID-19 cannot visit Korean medical institutions during the initial quarantine period, the analysis of patients with facial palsy due to COVID-19 was limited. In addition, COVID-19 vaccination began in 2021, which limits the interpretation of the study results, and further research on the relationship between facial paralysis and COVID-19 vaccination is needed.
However, this study is meaningful in that it evaluated the proportion of first-visit patients with peripheral facial palsy who visited Korean Medicine hospitals before COVID-19 and during COVID-19 for three years in various aspects. This study may serve as a reference for policy decision-making and research on peripheral facial palsy.
Author Contributions
Conceptualization, Y.L., S.L. and Y.-S.K.; formal analysis, Y.L., S.L. and Y.-S.K.; funding acquisition, S.L.; investigation, Y.L and S.L.; methodology, Y.L., S.L., and Y.-S.K.; project administration, Y.L. and S.L.; resources, Y.L. and S.L.; software, Y.L.; supervision, Y.-S.K.; validation, S.L. and Y.-S.K.; .; visualization, Y.L., S.L. and Y.-S.K.; writing—original draft preparation, Y.L.; writing—review and editing, S.L. and Y.-S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a grant from the Korea Institute of Oriental Medicine [KSN1823211]
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Kyung Hee university Korean Medicine hospital (KOMCIRB 2022-01-001, on January 17, 2022).
Informed Consent Statement
Patient consent of this retrospective chart review study was waived and approved by the Kyung Hee university Korean Medicine hospital. To protect the privacy of the patients, all records and documentation were de-identified immediately following extraction and were not used for other studies.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
We would like to thank Editage (www.editage.co.kr) for editing and reviewing this manuscript for English language.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A. Classification of Administrative Districts of South Korea Used in the Study
Figure A.
South Korea Administrative District Classification. Seoul is the capital of Korea, and this oriental clinic is located.
Figure A.
South Korea Administrative District Classification. Seoul is the capital of Korea, and this oriental clinic is located.
Appendix B. The Proportion of Residence by Disease Stage before and during COVID-19

Table B1.
The proportion of residence locations before and during COVID-19 in acute patients.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Seoul | 264 (60.4%) | 253 (66.9%) | 239 (62.1%) | 492 (64.5%) | 0.6564 | |
| Geonggi | 123 (28.1%) | 97 (25.7%) | 116 (30.1%) | 213 (27.9%) | ||
| Incheon | 15 (3.4%) | 7 (1.9%) | 11 (2.9%) | 18 (2.4%) | ||
| Ho-seo | 8 (1.8%) | 5 (1.3%) | 4 (1.0%) | 9 (1.2%) | ||
| Gwang Won | 6 (1.4%) | 7 (1.9%) | 6 (1.6%) | 13 (1.7%) | ||
| Yeongnam | 14 (3.2%) | 6 (1.6%) | 6 (1.6%) | 12 (1.6%) | ||
| Honam | 4 (0.9%) | 3 (0.8%) | 2 (0.5%) | 5 (0.7%) | ||
| Jeju | 1 (0.2%) | 0 (0.0%) | 1 (0.3%) | 1 (0.1%) | ||
| Foreign region | 2 (0.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
Table B2.
The proportion of residence locations before and during COVID-19 in subacute patients.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Seoul | 157 (48.0%) | 113 (46.5%) | 111 (52.4%) | 224 (49.2%) | 0.110 | |
| Geonggi | 109 (33.3%) | 85 (35.0%) | 61 (28.8%) | 146 (32.1%) | ||
| Incheon | 14 (4.3%) | 15 (6.2%) | 9 (4.2%) | 24 (5.3%) | ||
| Ho-seo | 8 (2.4%) | 7 (2.9%) | 9 (4.2%) | 16 (3.5%) | ||
| Gwang Won | 12 (3.7%) | 6 (2.5%) | 10 (4.7%) | 16 (3.5%) | ||
| Yeongnam | 10 (3.1%) | 6 (2.5%) | 4 (1.9%) | 10 (2.2%) | ||
| Honam | 8 (2.4%) | 10 (4.1%) | 8 (3.8%) | 18 (4.0%) | ||
| Jeju | 4 (1.2%) | 1 (0.4%) | 0 (0.0%) | 1 (0.2%) | ||
| Foreign region | 5 (1.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
Table B3.
The proportion of residence locations before and during COVID-19 in chronic patients
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Seoul | 60 (45.1%) | 45 (47.4%) | 50 (50.0%) | 95 (48.7%) | 0.766 | |
| Geonggi | 41 (30.8%) | 32 (33.7%) | 27 (27.0%) | 59 (30.3%) | ||
| Incheon | 3 (2.3%) | 0 (0.0%) | 3 (3.0%) | 3 (1.5%) | ||
| Ho-seo | 5 (3.8%) | 6 (6.3%) | 4 (4.0%) | 10 (5.1%) | ||
| Gwang Won | 9 (6.8%) | 4 (4.2%) | 6 (6.0%) | 10 (5.1%) | ||
| Yeongnam | 9 (6.8%) | 3 (3.2%) | 6 (6.0%) | 9 (4.6%) | ||
| Honam | 3 (2.3%) | 5 (5.3%) | 3 (3.0%) | 8 (4.1%) | ||
| Jeju | 2 (1.5%) | 0 (0.0%) | 1 (1.0%) | 1 (1.5%) | ||
| Foreign region | 1 (0.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
Appendix C. The Proportion of Hospital Visit Routes by Disease Stage before and during COVID-19
Table C1.
The proportion of hospital visit routes before and during COVID-19 in acute patients.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| After no treatment | 66 (15.1%) | 55 (14.6%) | 42 (10.9%) | 97 (12.7%) | X2=4.768 0.190 |
|
| After only Western Medicine treatment | 216 (49.4%) | 212 (56.1%) | 213 (55. 3%) | 425 (55.7%) | ||
| After only Korean Medicine treatment | 60 (13.7%) | 45 (11.9%) | 42 (10.9%) | 87 (11.4%) | ||
| After both Western and Korean Medicine treatment | 95 (21.7%) | 66 (17.5%) | 88 (22.9%) | 154 (20.2%) | ||
Table C2.
The proportion of hospital visit routes before and during COVID-19 in subacute patients.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| After no treatment | 6 (1.8%) | 4 (1.6%) | 2 (0.9%) | 6 (1.3%) | X2=5.544 0.136 |
|
| After only Western Medicine treatment | 130 (39.8%) | 93 (38.3%) | 72 (34.0%) | 165 (36.3%) | ||
| After only Korean Medicine treatment | 24 (7.3%) | 10 (4.1%) | 10 (4.7%) | 20 (4.4%) | ||
| After both Western and Korean Medicine treatment | 167 (51.1%) | 136 (56.0%) | 128 (60.4%) | 264 (58.0%) | ||
Table C3.
The proportion of hospital visit routes before and during COVID-19 in chronic patients.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| After no treatment | 7 (5.3%) | 3 (3.2%) | 0 (0.0%) | 3 (1.5%) | X2=6.466 0.091 |
|
| After only Western Medicine treatment | 24 (18.0%) | 13 (13.7%) | 13 (13.0%) | 26 (13.3%) | ||
| After only Korean Medicine treatment | 18 (13.5%) | 22 (23.2%) | 16 (16.0%) | 38 (19.5%) | ||
| After both Western and Korean Medicine treatment | 84 (63.2%) | 57 (60.0%) | 71 (71.0%) | 128 (65.6%) | ||
References
- Sweeny K; Rankin K; Cheng X; Hou L; Long F; Meng Y; et al. Flow in the time of COVID-19: Findings from China. PloS one 2020, 15, e0242043.
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 6 september 2022).
- Coronavirus (COVID-19), Republic of Korea. Available online: http://ncov.kdca.go.kr/?brdId=1&brdGubun=11&ncvContSeq=&contSeq=&board_id=&gubun= (accessed on 6 september 2022).
- Changes in people’s medical usage behavior due to COVID-19. Available online: http://www.alioplus.go.kr/news/newsDetail.do;jsessionid=623l2hH4RmlgHPOwKwIq1SZQ.node21?brdSeq=10340 (accessed on 6 september 2022).
- Health Insurance Review and Assessment Service. Healthcare Bigdata Hub. Available online: http://opendata.hira.or.kr/op/opc/olapHthInsRvStatInfo.do (accessed on 6 september 2022).
- Codeluppi L; Venturelli F; Rossi J; Fasano A; Toschi G; Pacillo F; et al. Facial palsy during the COVID-19 pandemic. Brain Behav 2021, 11, e01939.
- Kerstens J; Deschuytere L; Schotsmans K; Maréchal E. Bilateral peripheral facial palsy following asymptomatic COVID-19 infection: a case report. Acta Neurologica Belgica 2021, 121, 815-6.
- Al-Kaisy M; Eid MM. Bell’s Palsy Caused by SARS-CoV-2. Case Rep. Acute Med 2021, 4, 91-4.
- Lima MA; Silva MTT; Soares CN; Coutinho R; Oliveira HS; Afonso L; et al. Peripheral facial nerve palsy associated with COVID-19. JNV 2020, 26, 941-4.
- Finsterer J; Scorza FA; Scorza CA; Fiorini AC. Attributing increased prevalence of facial palsy to SARS-CoV-2 requires evidence. Brain Behav 2020, 11, e01996. doi: 10.1002/brb3.1996.
- Mutlu A; Kalcioglu MT; Gunduz AY; Bakici B; Yilmaz U; Cag Y. Does the SARS-CoV-2 pandemic really increase the frequency of peripheral facial palsy? Am. J. Otolaryngol 2021, 42, 103032.
- Martin-Villares C; Alba JR; Gonzalez-Gimeno MJ. Data from 235 Cases of Bell's Palsy during COVID-19 Pandemic: Were There Clusters of Facial Palsy? Neuroepidemiology 2021, 55, 495.
- Colella G; Orlandi M; Cirillo N. Bell’s palsy following COVID-19 vaccination. J. Neurol 2021, 268, 3589-91.
- Martin-Villares C; Vazquez-Feito A; Gonzalez-Gimeno MJ; de la Nogal-Fernandez B. Bell’s palsy following a single dose of mRNA SARS-CoV-2 vaccine: a case report. J. Neurol 2022, 269, 47-8.
- Obermann M; Krasniqi M; Ewers N; Fayad J; Haeberle U. Bell’s palsy following COVID-19 vaccination with high CSF antibody response. Neurol. Sci. 2021, 42, 4397-9.
- Shibli R; Barnett O; Abu-Full Z; Gronich N; Najjar-Debbiny R; Doweck I, et al. Association between vaccination with the BNT162b2 mRNA COVID-19 vaccine and Bell's palsy: a population-based study. Lancet Reg. Health Eur 2021, 11, 100236.
- Klein NP; Lewis N; Goddard K; Fireman B; Zerbo O; Hanson KE; et al. Surveillance for adverse events after COVID-19 mRNA vaccination. Jama 2021, 326, 1390-9.
- Renoud L; Khouri C; Revol B; Lepelley M; Perez J; Roustit M; et al. Association of facial paralysis with mRNA COVID-19 vaccines: a disproportionality analysis using the World Health Organization pharmacovigilance database. JAMA Intern. Med. 2021, 181, 1243-5.
- Shemer A; Pras E; Einan-Lifshitz A; Dubinsky-Pertzov B; Hecht I. Association of COVID-19 vaccination and facial nerve palsy: a case-control study. JAMA Otolaryngol Head Neck Surg 2021, 147, 739-43.
- 2020 Korean Medicine Utilization Survey. Available online: https://www.koms.or.kr/main.do (accessed on 6 september 2022).
- Cha HJ; Kim BS; Sung KJ; Lee YR; Choi HK; Kim MJ; et al. Statistical Analysis of Outpatients Trends at Korean Medicine Hospitals of Daejeon University by Region before and after COVID-19. JKM 2021, 42, 26-43.
- Lee JE; Shin YJ; Shin SH. Comparative Analysis of Patients Visiting Department of Korean Internal Medicine in a Korean Medicine Hospital Before and During COVID-19-From July 2018 to June 2021 at Wonkwang University Jeonju Korean Medicine Hospital. J Int Korean Med 2021, 42, 1255-68.
- Lee YR; Cha HJ; Choi HK; Kim MJ; Kim BS; Sung KJ; et al. Statistical analysis of patients visiting department of acupuncture and moxibustion in Korean medicine hospital before and after COVID-19-Focusing on a Korean medicine hospital in Daejeon. JKM 2021, 42, 31-49.
- Kwon NH; Shin YJ; Kim CY; Koh PS; Yi WI; Joh BJ; et al. Comparative clinical study between Oriental medical and oriental-western medical treatment on bell’s palsy. Journal of Korean Acupuncture & Moxibustion Society 2008, 25, 19-28.
- Lee DH. Clinical efficacy of electroneurography in acute facial paralysis. J Audiol Otol 2016, 20, 8.
- Kim MW, Kim J. Early stage steroid treatment for acute facial paralysis in Korea. Korean J Otorhinolaryngol-Head Neck Surg 2016, 59, 346-52.
- Clinical practice Guideline of Korean Medicine for Facial palsy. Available online: https://nikom.or.kr/nikom/index.do (accessed on 6 september 2022).
- 2022 Health Insurance Health Insurance Medical Care Benefit. Available online: https://repository.hira.or.kr/handle/2019.oak/2964 (accessed on 6 september 2022).
- Yang JH. A Comparative Study on Hospital Choice Factors between First-visit and Revisit patients in General Hospitals. J. Digit. Converg 2017, 15, 231-8.
- Peitersen E. Bell's palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta oto-laryngologica 2002, 122, 4-30.
- Oh JY; Cho SJ; Choi JS. Changes in Health Care Utilization during the COVID-19 Pandemic. Health Policy and Management 2021, 31, 508-17.
- Shin JW; Moon SJ; Jeong SH. COVID-19 and medical care service utilization experience. Health and welfare Issue & Focus 2021, 400, 1-8.
- Han SH; Kang JK; Hong JS. A Study of Factors Related to the Subjective Health Status of Elderly Population in Korea. Health Policy and Management 2021, 31, 56-64.
- Valls-Solé J. Facial palsy, postparalytic facial syndrome, and hemifacial spasm. J. Mov. Disord 2002, 17, S49-S52.
- Kim SH; Lee HJ; Lee KS; Shin HW. Factors Affecting Patient Moving for Medical Service Using Multi-level Analysis. Korean J Hosp Manag 2014, 19, 9-20.
- Garro A; Nigrovic LE. Managing peripheral facial palsy. Annals of Emergency Medicine 2018, 71, 618-24.
- Shin JW; Jo BH; Choi BR; Kim HN; Moon SJ; Jin JH, et al. 2020 Medical service experience survey. Sejong: KIHASA 2020, 231-266.
- Yoon GJ. Infectious diseases and public health care examined through the COVID-19 response. Health and welfare Issue & Focus 2020, 377, 1-11.
- Lee SM; Yang SP; Kim ES; Lee MJ; Park JM; Nam DW; et al. Admission care for Bell's palsy patients: a qualitative report on patient experiences. J Acupunct Res 2013, 30, 11-23.
Table 1.
The proportion of demographic characteristics.
| Before COVID-19 | During COVID-19 | ||||
|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | ||
| Sex | |||||
| Male | 435 (48.5%) | 335 (46.8%) | 310 (44.5%) | 645 (45.6%) | |
| Female | 462 (51.5%) | 381 (53.2%) | 381 (55.5%) | 768 (54.4%) | |
| Age | |||||
| Under 20 | 42 (4.7%) | 24 (3.4%) | 22 (3.2%) | 46 (3.3%) | |
| 20s-30s | 210 (23.4%) | 191 (26.7%) | 164 (23.5%) | 355 (25.1%) | |
| 40s-50s | 362 (40.4%) | 266 (37.2%) | 242 (34.7%) | 508 (36.0%) | |
| Over 60 | 283 (31.5%) | 235 (32.8%) | 269 (38.6%) | 504 (35.7%) | |
| Lesion Site | |||||
| Left | 468 (52.2%) | 350 (48.9%) | 351 (50.4%) | 712 (50.4%) | |
| Right | 429 (47.8%) | 366 (51.1%) | 346 (49.6%) | 701 (49.6%) | |
Table 2.
The proportion of predisposing factors for peripheral facial palsy.
| Before COVID-19 | During COVID-19 | |||
|---|---|---|---|---|
| 2019 | 2020 | 2021 | ||
| Fatigue and overwork | 198 (63.3%) | 184 (58.2%) | 118 (52.0%) | |
| Insomnia | 146 (46.6%) | 142 (44.9%) | 100 (44.1%) | |
| Stress | 162 (51.8%) | 156 (49.4%) | 104 (45.8%) | |
| On a diet | 12 (3.8%) | 9 (2.8%) | 8 (3.5%) | |
| Exposure to severe temperature differences | 66 (21.1%) | 43 (13.6%) | 35 (15.4%) | |
| Virus disease (ex. cold, enteritis) | 56 (17.9%) | 20 (6.3%) | 4 (1.8%) | |
| Surgery and injury | 14 (4.8%) | 9 (2.8%) | 7 (3.1%) | |
| COVID-19 vaccination | - | - | 24 (10.6%) | |
| Others | 2 (0.6%) | 6 (1.9%) | 15 (6.6%) | |
Table 3.
The proportion of disease phase before and during COVID-19.
| Before COVID-19 | During COVID-19 | P-Value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Acutephase | 437 (48.7%) | 378 (52.8%) | 385 (55.2%) | 763 (54.0%) | X2=6.286 0.043 |
|
| Subacute phase | 327 (36.5%) | 243 (33.9%) | 212 (30.4%) | 455 (32.2%) | ||
| Chronic phase | 133 (14.8%) | 95 (13.3%) | 100 (14.3%) | 195 (13.8%) | ||
Table 4.
The proportion of residence locations before and during COVID-19.
| Before COVID-19 | During COVID-19 | P-Value | |||||
|---|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | ||||
| Seoul | 481 (53. 6%) | 411 (57.4%) | 400 (57.4%) | 811 (57.4%) | X2=23.741 0.003 |
||
| Geonggi | 273 (30.4%) | 214 (29.9%) | 204 (29.3%) | 418 (29.6%) | |||
| Incheon | 32 (3.6%) | 22 (3.1%) | 23 (3.3%) | 45 (3.2%) | |||
| Ho-seo | 21 (2.3%) | 18 (2.5%) | 17 (2.4%) | 35 (2.5%) | |||
| Gwang Won | 27 (3.0%) | 17 (2.4%) | 22 (3.2%) | 39 (2.8%) | |||
| Yeongnam | 33 (3.7%) | 15 (2.1%) | 16 (2.3%) | 31 (2.2%) | |||
| Honam | 15 (1.7%) | 18 (2.5%) | 13 (1.9%) | 31 (2.2%) | |||
| Jeju | 7 (0.8%) | 1 (0.1%) | 2 (0.3%) | 3 (0.2%) | |||
| Foreign region | 8 (0. 9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
Table 5.
The proportion of residence locations in Seoul before and during COVID-19.
| Before COVID-19 | During COVID-19 | P-Value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Northeastern region | 287 (59.7%) | 275 (66.9%) | 269 (67.3%) | 544 (67.1%) | X2=23.741 0.003 |
|
| Northwestern region | 33 (6.9%) | 25 (6.1%) | 27 (6.8%) | 52 (6.4%) | ||
| Inner-city region | 30 (6.2%) | 29 (7.1%) | 25 (6.3%) | 54 (6.7%) | ||
| Southeastern region | 50 (10.4%) | 22 (5.4%) | 31 (7.6%) | 53 (6.5%) | ||
| Southwestern region | 81 (16.8%) | 60 (14. 6%) | 48 (12.0%) | 108 (13.3%) | ||
Table 6.
The proportion of hospital visit routes before and during COVID-19.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| After no treatment | 79 (8.8%) | 62 (8.7%) | 44 (6.4%) | 106 (7.5%) | X2=18.840 0.277 |
|
| After only Western Medicine treatment | 370 (41.2%) | 318 (44.4%) | 298 (42.8%) | 616 (43.6%) | ||
| After only Korean Medicine treatment | 102 (11.4%) | 77 (10.8%) | 68 (9.8%) | 145 (10.3%) | ||
| After both Western and Korean Medicine treatment | 346 (38.6%) | 259 (36.2%) | 287 (41.2%) | 546 (38.6%) | ||
Table 7.
The proportion of patient care type before and during COVID-19.
| Before COVID-19 | During COVID-19 | P-value | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Total | |||
| Only outpatient treatment | 250 (57.2%) | 246 (65.1%) | 288 (74.8%) | 534 (70.0%) | X2=23.741 0.003 |
|
| Both outpatient and inpatient treatment | 187 (42.8%) | 132 (34.9%) | 97 (25.2%) | 229 (30.0%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



