
Submitted:
27 June 2023
Posted:
28 June 2023
You are already at the latest version
Abstract
Assistance dogs provide significant benefits to older adult owners. However, despite protective legislation, aged care facilities continue to not allow owners to retain their dog on relocation. The purpose of the current study was to explore whether older adults should be allowed to retain their dog on relocation to an aged care facility, and what factors should impact this decision. Further, if allowed to retain their dog, what would be the best practice to allow for this. A deliberative democracy methodology was used, with a range of key stakeholders recruited. Focus groups were held, with follow up questionnaire to establish deliberation for all questions. Results indicated that with sufficient objective measurement, fair decisions can be made to ensure the welfare and wellbeing for owner and dog. Key policy and procedure changes would also be necessary to ensure ongoing support, such as training, care plans, and emergency directives. By ensuring sufficient policies and procedures are in place, training and support could lead to an ideal outcome where facilities could be at the forefront of a better future for aged care.
Keywords:
assistance dogs
; aged care
; older adults
; regulation
; support
1. Introduction
The use of assistance dogs can have a profound positive impact on the lives of their owners, with considerable focus in the recent research body. This impact is especially crucial for older adults who are also more likely to experience health declines, such as in vision and hearing, which warrant the use of an assistance dog. Further, it is important to note the benefits extend far beyond mere practical tasks, but also across mental, physical, and social health domains [1]. As such, it seems rational that older adults should be encouraged to acquire an assistance dog as a multi-faceted treatment and support. However, a number of actual and perceived barriers prevent or deter this age group from this acquisition, in particular the availability of suitable accommodation.
Current legislation, at state and federal levels, including the Guide, Hearing and Assistance Dogs Act 2009 [2] and Disability Discrimination Act 1992 [3], is designed to protect the rights of owners and their assistance dogs. This includes maintaining their right to sufficient accommodation, outlawing discrimination based on refusal as well as any condition that would lead to their separation. Despite this, it has been suggested that many aged care facilities in Australia continue to refuse to allow owners to relocate to the facility with their assistance dog, with one report finding as little as 18% allowing residents to keep an animal of any kind [4,5]. This is a considerable barrier not only in discouraging initial acquisition, but in their retention. The latter potentially contributes to significant distress for both owner and dog, with the loss or separation from an assistance dog creating distress greater than that of a companion dog [6].
Given this is an issue with the potential to affect a number of key stakeholders, it is important to consider the above through the lens of a wide range of people who are either directly or indirectly impacted, such as allied health staff, animal professionals, aged care staff, and assistance dog owners themselves. These individuals are likely to have competing interests and differing opinions, all of which should be harnessed for well-rounded discussion and solutions. Deliberative democracy involves providing participants with adequate information, before facilitating discussion that not only takes into consideration differing views but works to integrate the views of all participants based on a culmination of all participants’ perspectives [7]. This methodology has received support for use within the public policy sphere, with the opportunity to raise and consider alternative perspectives increasing the likelihood of policy acceptability and thus increased likelihood of successful implementation [8]. While traditionally these discussions would be held in person, the boom of online meeting software has allowed for the adaptation of online deliberative democracy. While this comes with possible technical difficulties, it has been found to lead to the same outcomes [9], with the benefits of improved scheduling and recording capabilities, and the ability to complete follow-ups with participants via email. This allows for increased capabilities to reach consensus on key issues.
The current study thus aims to use deliberative democracy to explore whether older adults with assistance dogs should be allowed to retain their dog when they relocate to an aged care facility, and what factors should impact this decision (e.g., dog size, care abilities). Further, if they were allowed to retain their dog, what would be the best practice to allow for an effective transition and continued support within the aged care facility.
2. Materials and Methods
2.1. Participants
Participants (N=18) were recruited via a convenient sample of existing professional networks. The authors selected professionals and consumers with a range of backgrounds and experiences, all of whom had relevant experience or involvement with older adults, aged care, or assistance animals (See ‘Table 1’). Potential participants were initially invited by direct email, and those who indicated interest were then sent participant information, consent form, and instructions to nominate their available dates and times via an online poll. The study was approved by the Research Ethics and Integrity Board at the University of Queensland (2022/HE001752), and informed consent was received from all participants prior to the commencement of the study.
2.2. Design
The current study used an adapted an exploratory deliberative democracy methodology with qualitative and quantitative findings. Qualitative data was collected during focus groups, which was summarized into key common points. Where deliberation of key points was not reached, or response priority was unclear, the points were developed into a questionnaire format for ranking, providing subsequent quantitative data.
2.3. Procedure
On receipt of consent forms and time availability from all participants, 3 focus online groups were held, with numbers kept as even as possible to allow for minimal group sizes to promote discussion and engagement from all participants (Group 1, n=6; Group 2, n=6; Group 3, n=5). While ideally this allocation would consider the spread by participant experience, availability needed to take precedence due to participant availability.
All focus groups followed an identical format, facilitated by PowerPoint slides containing all crucial information. Firstly, participants introduced themselves and their relevant background. Secondly, they were presented with background information on the issue (See ‘Appendix A’) to ensure all had a base-level understanding of the issue. Thirdly, participants were provided with a list of key assumptions for the subsequent case studies, to ensure the brevity and specificity of discussion across all groups. These included having them assume that in both case studies the assistance dog owner was:
- Healthy enough to care for their dog themselves
- Does not have cognitive functioning impairments
- Intends to relocate from their home to an aged care facility
- Previously lived alone
Fourthly, they were presented with 2 differing case studies and a list of questions. This not only guided the conversation and ensured relevant discussion, but also gave tangible examples for how the cases may or may not differ within their considerations. These included:
Case 1: Person A has a severe hearing impairment, for which she has a hearing dog to assist in alerting her to key sounds (e.g., the doorbell, kettle, and smoke alarm). She has owned her hearing dog for 5 years, which is a small terrier.
Case 2: Person B is blind, for which he has a guide dog to assist in his mobility. He previously used a cane but did not find this to be as effective. He has owned his guide dog for 5 years, which is a large Labrador.
Questions:
- What would an appropriate assistance dog policy for the aged care home look like?
- Should these policies differ across the two presented cases? Why/why not?
- Are there any other things that need to be implemented by aged care facilities to allow for owners to keep their assistance dog in the facility?
- Are there any relevant bodies that should be involved in ensuring these policies are being upheld?
- Is there any other information you would want to know about the cases that would affect your decision?
On completion of all focus groups, discussions were transcribed with identifying data removed. Data was summarized (See ‘2.4 Analysis’) and questions that did not have agreement had their various responses input into questionnaire format for ranking, using Qualtrics. This data was then collated and analysed through examination of the means and standard deviations from the Qualtrics data output.
2.4. Analysis
The initial focus group data was examined by the author, with key points identified and summarized, with similar or related responses combined for each question. For Questions 1 and 2, sufficient deliberation and agreement was achieved during the focus groups. For Question 3, two key subthemes were identified and included in the questionnaire as two independent answer lists for ranking by importance. Question 4 responses were input for ranking by importance with no subthemes. Finally, Question 5 had three key subthemes identified, which were input for independent ranking. Subsequent participant data from this questionnaire was then analysed using the Qualtrics output. Ranking was from 1 (most important) to the highest number, depending on the number of responses to rank (least important). Overall order of importance for each question or sub-question was established through the mean ranking response. That is, the lowest ranking mean was considered the most important response, the second lowest the second most important, and so on.
3. Results
The following will provide a summary of the results attained by question, with focus group qualitative data only for Questions 1 and 2 where deliberation was reached, and ranking was not necessary. The remainder of the questions include both the qualitative and quantitative results, with deliberation then established.
3.1. Question 1 - What Would an Appropriate Assistance Dog Policy for the Aged Care Home Look Like?
Five key subthemes were identified from the qualitative focus group data, including (1) Assessing and preparation for the future; (2) Where the owner has limited ability to care for the dog; (3) Where the owner is unable to care for the dog; (4) Consideration of others (staff, clients, visitors); and (5) Dog welfare and ability to complete tasks. The following are the key points identified for the development of appropriate policies for aged care facilities:
3.1.1. Assessing and Preparation for the Future
Assessing the ability of the person to care for their dog: aged care facilities should implement an objective testing protocol for whether the person is able to sufficiently care for the dog prior to relocation to the facility. This may require the development of a new assessment, or the direct use or adaption of an existing measure, such as the Companion-Dog Multi-Species Risk Management Tool (CAMSRMT) [10] or Safe Dog Friendly Eldercare (SAFE), which is currently under development [11]. This should also be readministered at regular intervals (annually; biannually) or after a significant event, such as hospitalization.
Assessing the welfare of the dog: aged care facilities in conjunction with owners should implement an objective protocol for whether the facility is appropriate for the dog prior to relocation and whether the dog’s welfare is continued to be supported. This would assess the suitability of the facility of the space itself (e.g., access to toileting facilities), whether the dog is coping and is sufficiently cared for (groomed, fed, seeing a vet regularly). Also, whether the dog is receiving sufficient stimulation and exercise to maintain health and prevent issues, such as obesity. This may require engagement by the issuing body to do initial and regular assessments. This should also be readministered at regular intervals (annually, biannually) or after a significant event, such as hospitalization.
General dog care plan: where someone is assessed as being able to keep their dog in the facility, there must be a care plan in place for relevant services including who and regularity (e.g., yearly veterinarian, monthly groomer), basic care (e.g., how food will be acquired), and any medication or other needs of the dog.
Dog risk management and emergency directive: aged care facilities in conjunction with owners should establish sufficient protocols to manage who will take care of the dog in case of short- or long-term inability to care for the dog, such as periods of illness or hospitalization, and where the dog should be placed in the case of death or incapacity of the person. This may include partner, friends, family, RSPCA, or the supplying organization (e.g., Guide Dogs Qld).
Policy perspective broadly: developed policies should include overarching policies for inclusion and risk assessment, but also include provision of case-by-case individual management and assessment for acceptance. These considerations should apply not just due to differences in the owner or dog, but to other factors such as room configuration, for example if the room is too small for a large dog but could accommodate a small dog.
3.1.2. Where the Owner has Limited Ability to Care for the Dog
The dog may still be able to be retained where a care plan can be made inclusive of additional help. This should specify what help is needed by the owner (feeding, walking, toileting, grooming, vet attendance) and who will provide this support (family/friends, or volunteers/staff with special training or experience). Other short-term assistance may also be specified in a care plan, such as foster carers or involvement of the dog issuing organization for temporary dog respite or crisis situations.
3.1.3. Where They are Unable to Care for the Dog
Aged care facilities should establish protocols to transition the patient into relocating to the facility without their dog. This may include slowly decreasing time with the dog and decreasing their reliance, having their own dog visit where possible or having a visiting therapy or companion dog they can engage with.
3.1.4. Consideration of Others (Staff, Clients, Visitors)
There is a clear need to consider the needs of staff, clients, and visitors, including dog allergies, fear or dislike of dogs, ethnic consideration, such as cultural beliefs of dogs being ‘dirty’. This may require some form of separation (e.g., a child gate on the doorway of the patient’s room), signage warning others of the presence of a dog, and training protocols and provision of information such as brochures about assistance dogs.
There is also a need to ensure the dog is kept at a hygienic standard to be around others, including being groomed, bathed, and nails cut so as not to damage anyone’s skin and minimize any infection and illness risks. This should tie into the ongoing assessment of the owner’s ability to care for the dog and ensuring the standard of the dog is maintained for its welfare.
Housing and restraint should be specified as part of OHS policies, such as: the dog must be on a leash when outside the person’s room, how it will be restrained within the room where needed (e.g., when moving beds or wheelchairs).
There could be an option for nominated additional staff training to be able to assist or provide information as a ‘champion’ for assistance dogs. This may also include specific identification, such as a paw emblem on their name tag.
3.1.5. Dog Welfare and Ability to Complete Tasks
Some dogs may be reactive to the environment (e.g., smells, sights, and sounds), or be not used to a lot of attention, causing unwanted behaviours (e.g., toileting on the floor) or may become distracted from their working tasks, or engage in risky behaviours (e.g., swallowing medication dropped on the floor). As such, the individual dog should be continually assessed for suitability and problem solving should guide any necessary policy or procedure changes.
Other visitors may bring their own dog or visiting dogs to the aged care facility, which could become disruptive to assistance dogs without the same level of control. This may entail policies around separating any visiting dogs and providing education to the visitors around assistance dogs.
Where the owner is ageing in place and is unable to go outside or engage in activities, there should be an assessment on the usefulness of the dog in terms of task completion. This should ideally be completed by the organization who issues the dog or training and provide a discussion around whether the dog could be retrained (e.g., to take the owner to a dining room or react to alternative sounds) or if it the dog should be retired or relocated.
3.2. Question 2 - Should These Policies Differ Across the Two Presented Cases? Why/Why Not?
All group participants unanimously agreed that any policies should not differ across the two case studies. It was noted that this could inadvertently introduce other discrimination issues and decisions should be made on a case-by-case basis and as objectively as possible.
3.3. Question 3 - Are There Any Other Things That Need to Be Implemented by Aged Care Facilities to Allow for Owners to Keep Their Assistance Dog in the Facility?
For Question 3, two key subthemes were identified, including (1) the physical environment; and (2) staff or training. Each subtheme contained multiple responses which were presented to the participants for ranking by importance. The following responses are presented by most to least important by mean ranking. For a summary of response statistics for Question 3, see Table 2. An additional yes/no question was also included in this section (see 3.3.3. Additional Question).
3.3.1. The Physical Environment
First important response: New aged care facilities should be built with dog retainment in mind, and established facilities should consider retrofitting wherever possible (possible government grants). This may include sufficient access to outdoors (e.g., a balcony with dog door, access to larger dog friendly outdoor space for exercise/toileting), ability to keep the dog within the room (particularly where the owner is not in the room, e.g., a child gate on the room’s door), and sufficient storage space for dog food and/or toys.
Second important response: Where a facility wants to maintain separation for those with fears or allergies, or has a sufficient amount of dogs, it could consider having dog specific floors/wards where and those that are dog free.
Third important response: Rooms should be configured to allow staff movement, emergency response or movement or equipment while keeping the dog safe or restrained where necessary.
Fourth important response: Where facilities have sufficient difficulties in housing an dog that cannot be adjusted (e.g., narrow corridors or rooms are too small), it must be acknowledged that they simply cannot allow the person to retain their dog. This is not just discrimination but introduces other legal issues. Where this is the case, the owner should consider an alternative facility.
3.3.2. Staff or Training
First important response: Facilities could engage dog care volunteers (e.g., vet students, community volunteers) to provide care for any dogs in the facility.
Second important response: Facilities could employ a person(s) at the facility specifically for dog care.
Third important response: Facilities could provide optional training for current staff to provide dog care.
3.3.3. Additional Question
Should the provision of dog care support (e.g., walking, feeding) be a pay-for-use service in an aged care facility? (Yes/No). Responses were n=11 (64.71%) for ‘Yes’ and n=6 (35.29%) for ‘No’ (See Figure 1).
3.4. Question 4 - Are There Any Relevant Bodies That Should Be Involved in Ensuring These Policies Are Being Upheld?
No subthemes were identified for this question, so all answers were presented for ranking by importance. For a summary of response statistics for Question 4, see Table 3.
First important response: Aged care bodies: E.g., Aged & Community Care Providers Association (ACCPA) and Catholic Health Australia (CHA), to assist in ensuring there are necessary plans and supports in place.
Second important response: Assistance dog organizations: E.g., Guide Dogs Qld and Lion Hearing Dogs, who may complete the regular assessments.
Third important response: Dog rights organizations: E.g., RSPCA, to ensure all facilities have advocacy resources and dog welfare is maintained.
3.5. Question 5 - Is There Any Other Information You Would Want to Know about the Cases That Would Affect Your Decision??
For Question 5, three key subthemes were identified, including (1) the person; (2) the dog; and (3) the owner-dog relationship. Each subtheme contained multiple responses which were presented to the participants for ranking by importance. For a summary of response statistics for Question 5, see Table 4.
3.5.1. The Person
First important response: How traumatic is it for people to give up their dog? Some people may really struggle, so need to have conversation at the early stages when getting dog and provide mental health support where needed on relinquishment.
Second important response: Why the person is relocating to an aged care facility. If it is due to difficulty caring for themselves or have become acutely unwell, they may experience difficulty caring for their dog.
Third important response: Any relevant factors around their visual/hearing abilities, including severity and comorbidities, and available alternatives (e.g., blind cane).
Fourth important response: Whether they have any family/friends who are nearby or visit who are able to assist them with the care of their dog, or to take the dog in crisis.
3.5.2. The Dog
First important response: The overall manners and any problematic behaviours of the dog to assess suitability.
Second important response: Is it self-trained or provided by an organisation? This may affect who is able to follow up on dog welfare.
Third important response: Breed specific issues – what are the different needs of the breed e.g. exercise, socialisation, stimulation, behavioural anomalies etc to consider.
Fourth important response: Age of the dog – if they have had it for 5+ years it may be heading towards retirement. This may require a discussion with the dog providing organisation.
Fifth important response: Availability or someone to physically pick up the dog in an emergency e.g., managing a Labrador if they become sick.
3.5.3. The Owner-Dog Relationship
First important response: What is the cost to them if they are separated? Consideration for transition time – if losing the dog will make them deteriorate quicker then it could have higher offset or needs.
Second important response: Anything in particular about the person and dog, such as the context of where they came from (e.g. from a house vs apartment) and what they would need to relocate. This would allow transition into aged care to be tailored.
4. Discussion
The current study aimed to use deliberative democracy to explore whether older adults with assistance dogs should be allowed to retain their dog when they relocate to an aged care facility, and what factors should impact this decision (e.g., dog size, care abilities). Further, if they were allowed to retain their dog, what would be the best practice to allow for an effective transition and continued support within the aged care facility.
The question of whether older adults should be allowed to retain their dog when they relocate to an aged care facility is deceivingly complex. At first glance it seems like a simple yes, particularly given the numerous and far-reaching benefits highlighted in the research [1] and the legislation which is designed to prevent separation in the context of accommodation provision [2,3]. However, the results indicated that there is much to consider from the perspective of the owner, the dog, and the aged care facility to protect the best interests, safety, and wellbeing of all involved. Further, this needs to be grounded in sufficient policies and procedures based on objective measurement to minimise discrimination or ageist assumptions. Specifically, it was found that assessment should begin prior to relocation and be an ongoing process, including whether the owner is able to care for the dog, whether the dog’s welfare is maintained, and initially whether the aged care facility is sufficiently and safely able to house the dog. While this seems daunting, the discussion highlighted some tools, such as the CAMSRMT or SAFE [9,10], can be easily implemented. Further, many aged care facilities already maintain care plans for residents, which could be adapted to include dog care. So, while this may take some time to initially establish, ongoing assessment and record keeping would be achievable with minimal time or financial burden to the aged care facility.
On consideration of what factors should impact the decision, all participants unanimously agreed that policies should not differ across the case studies. This was noted to prevent any other inadvertent discrimination, and to encourage decisions made on a case-by-case basis guided by objectivity. However, it was later raised that there were a number of factors that would influence this decision from a person, dog, and owner-dog perspective. The most important person factor was ‘how traumatic is it for people to give up their dog?’. While there may be some who see their dog as a tool that is no longer necessary, research suggests that this may indeed be traumatic [6] and could be established through a discussion with the owner. Other factors alluded to how unwell the person is, severity of illnesses or disability, comorbidities, and availability of friends/family to assist. These are all important factors for all parties involved, which could be addressed by the aforementioned initial and ongoing assessments and having a sufficient care plan in place. It was also noted that alternatives could be considered, such as the cane. But taking this example, it has been found that those who have used a guide dog for a prolonged period may not be as proficient with a cane due to lack of practice so may not be easily implemented [12]. Considerations around the dog, such as manners and behaviours, training, and breed issues should also be assessed for suitability. While ideally factors such as dog size should not prevent an owner from relocation with their dog, it must be considered that some facilities simply cannot accommodate due to limited physical space. Thinking about the owner-dog relationship again the most important factor deliberated was the cost of separation. Not just because this loss could be profound [6], but because losing their dog could also lead to a quicker deterioration of health. Given that the health of older adults without dogs has been found to be related to faster deterioration of health, it is reasonable to consider that the compounding issue of grief could lead to further health deterioration [13].
The third part of the study’s aim is predictably the most in-depth; considering what would be the best practice to allow for an effective transition and continued support within the aged care facility. However, it is arguably the most crucial, as it has the potential to guide best practices for future policies within aged care facilities, to facilitate owners in keeping their assistance dog wherever possible. Further, it became evident during the discussions that these policies should not just look at what to do where the owner is able to keep their dog, but also what needs to be put in place where they cannot. As already mentioned, the first step would be to ensure policies outline objective assessments to assess suitability. Thus, the following will discuss further policies and procedures in the context of where owners have the ability or limited ability to care for their dog, and where they are unable to keep their dog, followed by other key considerations.
Where owners are allowed to keep their dogs, it is important to consider the ongoing needs, safety, and welfare of the dog and owner, as well as what to do where unexpected factors arise. It should also be considered that even when the owner is able to care for their dog it may not provide the same utility. Thus, there may be the possibility for retraining (e.g., retraining a hearing dog to alert the owner to a new set of sounds). Nevertheless, key points raised and deliberated were the need for a general animal care plan, and an animal risk management and emergency directive. The general animal care plan should be developed in conjunction with the owner, to establish services needed and any care that should be undertaken by the owner. Where the owner is fully capable, this should be a relatively simple process that can be reviewed periodically as needed, or where an unexpected event occurs (e.g., health deterioration). Where the owner has limited capacity to care for their dog, this plan could include additional assistance depending on their needs, and who will provide that assistance (e.g., a professional or friends/family). This may also include who to contact where temporary respite is needed. It was raised that some aged care facilities have additional services available to residents on a pay-per-use basis. Interestingly, the majority of participants agreed that the provision of dog care support (e.g., walking, feeding) should be a pay-for-use service in an aged care facility. Given that many owners may require assistance, of only periodically, and the limited funding abilities of many aged care facilities, this could be a simple answer to provide a necessary service at no extra cost to the facility. Alternatively, it was raised that there were three other possibilities, including the recruitment of volunteers, which would be no extra cost, the employment of an animal care staff member (particularly where there is a significant amount of dogs in the facility), or additional training to current staff to provide dog care. An animal risk management and emergency directive should also be included as part of policy, again developed in conjunction with the owner. This would prevent any confusion over where the dog should be relocated, whether temporarily or permanently, in the case of illness, hospitalisation, or death. This would not only provide peace of mind to staff, but also to owners.
An overlooked factor raised in the discussions was what to do where owners are assessed as unable to keep their dog. We know that this is often associated with a period of grief, loss, and distress [6]. As such, there should be policy protocols in place not only for those facing separation from their assistance dog, but even those facing separation from a companion animal. This could include a transition through decreasing their time with the dog, which would also allow alternatives to be explored and practiced (e.g., cane use). Alternately, having their dog visiting periodically (where possible, such as where family adopt the dog), or having an aged care visiting companion or therapy dog that they are encouraged to engage with. The latter might be a positive decision for the broader facility, with many benefits highlighted in the literature for dog assisted therapy in aged care [14].
Much of the focus thus far has been on the owner and dog, but it is crucial that policies and procedures should also take into consideration others within the aged care facility, such as staff, other residents, and visitors. A myriad of reasons were raised as to why others may not want to be around dogs, such as allergies or fears, so physical separation, signage, training protocols and assistance dog information would be important. Also, some visitors may bring their own dog to the facility that could interfere with an assistance dog. This also ties into the point that housing and restraint should be considered as part of policy, such as ensuring the dog is kept in the owner’s room where possible, and always leashed when outside the room. This was also raised on discussion of other factors that should be considered by aged care facilities. Namely, where many dogs are in a facility a dedicated dog-friendly floor or wing could be considered, and rooms should be configured to allow staff movement while the dog is restrained. Though it must be acknowledged that for some facilities there is just not sufficient space to maintain a dog safely or comfortably. This should thus be a key consideration as part of the initial assessment. Ideally new aged care facilities should be built with animals in mind, and older facilities could consider retrofitting (e.g., adding more access to outdoor spaces). The latter of which would highly benefit from government support, with the provision of grants, particularly to encourage facilities with limited budgets. This was unsurprisingly noted as the most important factor when considering physical space. It was also raised that the dog must be kept at a hygienic standard to manage any risks of injury (such as from long claws) or infection. This should be tied back into the policies and procedures in the dog care plan, whereby the dog receives sufficient ongoing care.
Where staff have identified a sufficient reason why they cannot be around a dog (such as allergies), other staff should be able to work with the owner instead. However, for all other staff, policies should inform sufficient training, whether mandatory or optional, on assistance dogs. It was further suggested this could include staff opting to become a ‘champion’ for assistance dogs, with specific identification like a paw emblem on their name badge. While a very different cause, the use of this idea has previously been successful in the LGBT+ space, with the use of ally training and identification (such as rainbow badges) helping provide a safe, accepting space with spreading of education [15]. Thus, this may similarly work to encourage acceptance and support of assistance dogs in the facility, and further spread education around assistance dog use and etiquette to other residents and visitors.
Given all this, the obvious question that remains is ‘which relevant bodies should be involved in ensuring these policies are upheld?’ In order of importance from the data, aged care bodies, assistance dog organisations and dog rights organisations. This is a logical order, particularly given their relative direct involvement already. But it is important to note all should be involved to a degree. Aged care bodies would already be involved at a policy level working with aged care facilities, and thus would likely assist in policy implementation support for this case. While assistance dog organisations may not be as involved in the policies, they would often be already in contact with the owner and could be instrumental in ongoing assessment of the owner’s ability to care for the dog, the necessity of the dog (may no longer have practical utility), and the welfare of the dog. The latter leads on to dog rights organisations, who may be required where the welfare of the dog is not assessed by an assistance dog organisation, or where the dog needs to be re-homed.
5. Conclusions
The question of whether older adult assistance dog owners should be able to keep their dog on relocation to an aged care facility is a deceivingly complex one. However, by inputting sufficient objective assessments in place for the person, dog, and facility, there is an opportunity to make a logical decision based on the best interests of all involved. Where possible, owner and dog should be kept together, as the law supports. Though it is important to have periodic follow-up assessments, care plans, and sufficient policies and procedures to ensure continued safety and welfare.
Policies need to take into consideration the necessity for case-by-case decision making, but also be clear in what should be done where an owner can or cannot keep their dog. And where they can, ensure that this guides procedures that maximise the safety, health, and wellbeing of all involved, not just the owner and dog, but staff, visitors and beyond. Any facilities who are willing to implement these policies and procedures, thus allowing owners and their dog to remain together, would be at the forefront of a better future for aged care.
Author Contributions
Conceptualization, A.S., N.P. and M.M.; methodology, A.S., N.P. and M.M.; formal analysis, A.S.; investigation, A.S.; data curation, A.S.; writing—original draft preparation, A.S.; writing—review and editing, A.S. and N.P.; visualization, A.S.; supervision, N.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Research Ethics and Integrity Board at the University of Queensland (2022/HE001752).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Associate Professor Margaret McAndrew and Professor Elizabeth Beattie for her valuable input and advice on the deliberative democracy process.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A - Background Information
The federal Disability Discrimination Act 1992 [1] and state acts, such as the Guide, Hearing and Assistance Dogs Act 2009 [2] ensure that certified assistance dogs and their owners maintain access rights. This includes accommodation and incorporates both refusal and stipulations that would require owner-dog separation. Despite this, many aged care facilities continue to disallow owners to retain their assistance dog and proving disability to obtain an assistance dog while in aged care has considerable barriers [3]. A report by the Dog Welfare League Australia (AWLA) found that of 2,933 aged care facilities reviewed, only 18% considered allowing residents to keep an animal [4]. While this did not pertain specifically to assistance dogs, it is indicative of the difficulties with relocating to an aged care facility with an animal.
Assistance dog ownership has been found to be highly beneficial for older adults, not just from a practical perspective, but across social, mental, and physical health domains [5]. As such, it is ideal that older adults do not avoid obtaining an assistance dog due to concerns over future retention in the case of relocation into aged care. Further, for those who already own an assistance dog, that they do not need to experience feelings of loss associated with not only the separation itself, but the loss of the relationship and benefits the dog provided [5]. Particularly as they are already likely experiencing compounding losses downsizing, losing their home, and in some cases their autonomy, this situation can be quite devastating.
Consideration of the dog itself is also often overlooked when they are required to be relinquished. In the case of assistance dogs, owners are generally able to contact their provider to return the dog [7]. However, where the dog is self-trained by the owner, in the absence of a suitable friend or family member, they may need to be relinquished to a shelter, such as the RSPCA. Additionally, the process of relinquishment is not only upsetting to the owner but may be considerably distressing and confusing to the dog itself.
While there is little research on the reasons aged care facilities may prohibit assistance dogs, it can be extrapolated that they are the same reasons as for companion dogs. These include: the age of the owner, lack of support funding and staff to assist in dog maintenance, and health and safety concerns [4,8]. It is often assumed that the advanced age of the owner can affect their ability to provide sufficient care to their dog, or that their dog will out-live them. However, it has been argued that lack of sufficient dog care or the death of an owner could happen at any age, for a range of reasons, such as unexpected death or illness, or competing life interests [8]. Thus, suitability of continued ownership should be based on the health and abilities of the owner, rather than age, which is discriminatory.
On consideration of the aged care facility’s lack of support funding and staff who are able to assist, where owners are able to care for the dogs themselves there should be limited assistance required. Further, assistance dogs provide practical supportive utility, such as mobility and sound alerting, and dogs broadly have been found to improve mental and physical health aspects when introduced into aged care facilities [9]. As such, it is possible that the owner would require less support from staff from a practical perspective, as well as less emotional and physical support requirements. This may also impact the amount of funding required due to maintained health.
Health and safety concerns in any aged care setting are of the upmost importance, both for staff and residents. While some free-roaming companion dogs may cause issues such as a trip hazard, assistance dogs are specifically trained and, thus, less likely to create these issues. Zoonotic illnesses, parasites, and contamination related issues are possible. However, these can be limited through regular dog vaccination, hygiene practices, and cleaning [10]. It is also important to note that the potential benefits for the owner outweigh these limited risks.
Overall, the current antidiscrimination legislation is designed to protect assistance dog owners and allow them the same access to sufficient care and accommodation. While aged care facilities often do not allow dogs of any kind, a reconsideration of these rules for assistance dogs is crucial, particularly, as it can have the ramification of older adults deciding not to obtain an assistance dog if they expect to need to re-locate to an aged care facility in the future, despite the significant benefits of ownership.
Adapted from: Salmon, A. J., Driscoll, C., Paterson, M., Harpur, P, & Pachana, N. A. (2022). Issues regarding the welfare of assistance dogs. Dogs, Under Review.
References
- Australian Government. Disability Discrimination Act 1992. Available online: https://www.legislation.gov.au/Details/C2016C00763 (Accessed on 30 September 2022).
- Guide, Hearing and Assistance Dogs Act 2009. Available online: https://www.legislation.qld.gov.au/view/pdf/2010-02-24/act-2009-004 (Accessed on 25 September 2022).
- Harpur, P.; Pachana, N. My dog, my support, and my new home in a retirement village: Disability discrimination, assistance dogs and old age. Elder L Rev, 2018, 11; https://doi.org/http://dx.doi.org/10.2139/ssrn.3258054
- Dog Welfare League Australia. Pets in Aged Care National Snapshot. 2018. Available online: https://www.awla.org.au/wp-content/uploads/2018/04/Pets-in-Aged-Care-Snapshot.pdf (Accessed on 25 September 2022).
- Salmon, A. J.; Pachana, N. A. A systematic review of the effect of assistance dog ownership on practical support, health, and wellbeing: Implications for older adults. Clinical Gerontologist, 2022, 1-26; https://doi.org/https://doi.org/10.1080/07317115.2022.2100728
- Yamamoto, M.; Hart, L. A. (2019). Separation from assistance dogs: the complicated psychological burden during loss of the relationship. In Pet Loss, Grief, and Therapeutic Interventions. Routledge: UK; pp. 188-208.
- Department of Veteran Affairs. Assistance Dogs. 2022. Available online: https://www.dva.gov.au/health-and-treatment/care-home-or-aged-care/services-support-you-home/assistance-dogs#when-you-need-to-return-an-assistance-dog (Accessed on 25 September 2022).
- Bilerte, M.; Bozorg, G.; Millross, A. The issues of housing the elderly with their companion dogs in care homes. The Student Journal of Professional Practice and Academic Research, 2019, 1, 1-45. https://journals.northumbria.ac.uk/index.php/sjppar/article/view/875/1278
- Crowley-Robinson, P.; Fenwick, D. C.; Blackshaw, J. K. A long-term study of elderly people in nursing homes with visiting and resident dogs. Applied Dog Behaviour Science, 1996, 47(1-2), 137-148; https://doi.org/https://doi.org/10.1016/0168-159101017-3
- Murthy, R.; Bearman, G.; Brown, S.; Bryant, K.; Chinn, R.; Hewlett, A.; George, B. G.; Goldstein, E. J.; Holzmann-Pazgal, G.; Rupp, M. E. Dogs in healthcare facilities: recommendations to minimize potential risks. Infection Control & Hospital Epidemiology, 2015, 36, 495-516; https://doi.org/10.1017/ice.2015.15
References
- Salmon, A. J.; Pachana, N. A. A systematic review of the effect of assistance dog ownership on practical support, health, and wellbeing: Implications for older adults. Clinical Gerontologist 2022, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Guide, Hearing and Assistance Dogs Act 2009. Available online: https://www.legislation.qld.gov.au/view/pdf/2010-02-24/act-2009-004 (accessed on 01 February 2023).
- Australian Government. Disability Discrimination Act 1992. Available online: https://www.legislation.gov.au/Details/C2016C00763 (accessed on 01 February 2023).
- Dog Welfare League Australia. Pets in Aged Care National Snapshot. 2018. Available online: https://www.awla.org.au/wp-content/uploads/2018/04/Pets-in-Aged-Care-Snapshot.pdf (accessed on 01 February 2023).
- Salmon, A.; Driscoll, C.; Paterson, M.; Harpur, P.; Pachana, N. A. Issues regarding the welfare of assistance dogs. Dogs 2022, 12, 3250. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Hart, L. A. Separation from assistance dogs: The complicated psychological burden during loss of the relationship. In Pet Loss, Grief, and Therapeutic Interventions. [CrossRef]
- Chambers, S. Deliberative democratic theory. Annual Review of Political Science 2003, 6, 307–326. [Google Scholar] [CrossRef]
- Degeling, C.; Carter, S. M.; Rychetnik, L. Which public and why deliberate? – A scoping review of public deliberation in public health and health policy research. Social Science & Medicine 2015, 131, 114–121. [Google Scholar] [CrossRef]
- Grönlund, K.; Himmelroos, S. The challenge of deliberative democracy online – A comparison of face-to-face and virtual experiments in citizen deliberation. Information Polity 2009, 14, 187–201. [Google Scholar] [CrossRef]
- Young, J. N.; Burton, D.; Milanese, E. The Companion-Dog Multi-Species Risk Management Tool (CAMSRMT), Society for Companion Dog Studies. http://www.scas.org.uk/the-companion-dog-multispecies-risk-management-toolkit-camsrmt/. (accessed on 01 April 2023).
- Young, J. N. Society for Companion Dog Studies Confirms Successful Applicants for 2020 Research Funding Round. https://www.scas.org.uk/society-for-companion-dog-studies-confirms-successful-applicants-for-2020-research-funding-round/. (accessed on 01 April 2023).
- Lloyd, J.; Budge, C.; La Grow, S.; Stafford, K. The end of the partnership with a guide dog: Emotional responses, effects on quality of life and relationships with subsequent dogs. Frontiers in Veterinary Science 2021, 8, 1–10. [Google Scholar] [CrossRef]
- Raina, P.; Waltner-Toews, D.; Bonnett, B.; Woodward, C.; Abernathy, T. Influence of companion dogs on the physical and psychological health of older people: An analysis of a one-year longitudinal study. Journal of the American Geriatrics Society 1999, 47, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Franklin, M. A.; Parnell, T.; Versi, N.; Pope, R. Dog assisted therapy for older adults in aged care facilities: A rapid review. Internet Journal of Allied Health Sciences and Practice 2022, 20, 14. [Google Scholar] [CrossRef]
- Hafford-Letchfield, T.; Simpson, P.; Willis, P. B.; Almack, K. Developing inclusive residential care for older lesbian, gay, bisexual and trans (LGBT) people: An evaluation of the Care Home Challenge action research project. Health & Social Care in the Community 2018, 26, e312–e320. [Google Scholar]
Figure 1.
Summary of responses for additional question “Should the provision of dog care support (e.g., walking, feeding) be a pay-for-use service in an aged care facility?”.
Figure 1.
Summary of responses for additional question “Should the provision of dog care support (e.g., walking, feeding) be a pay-for-use service in an aged care facility?”.
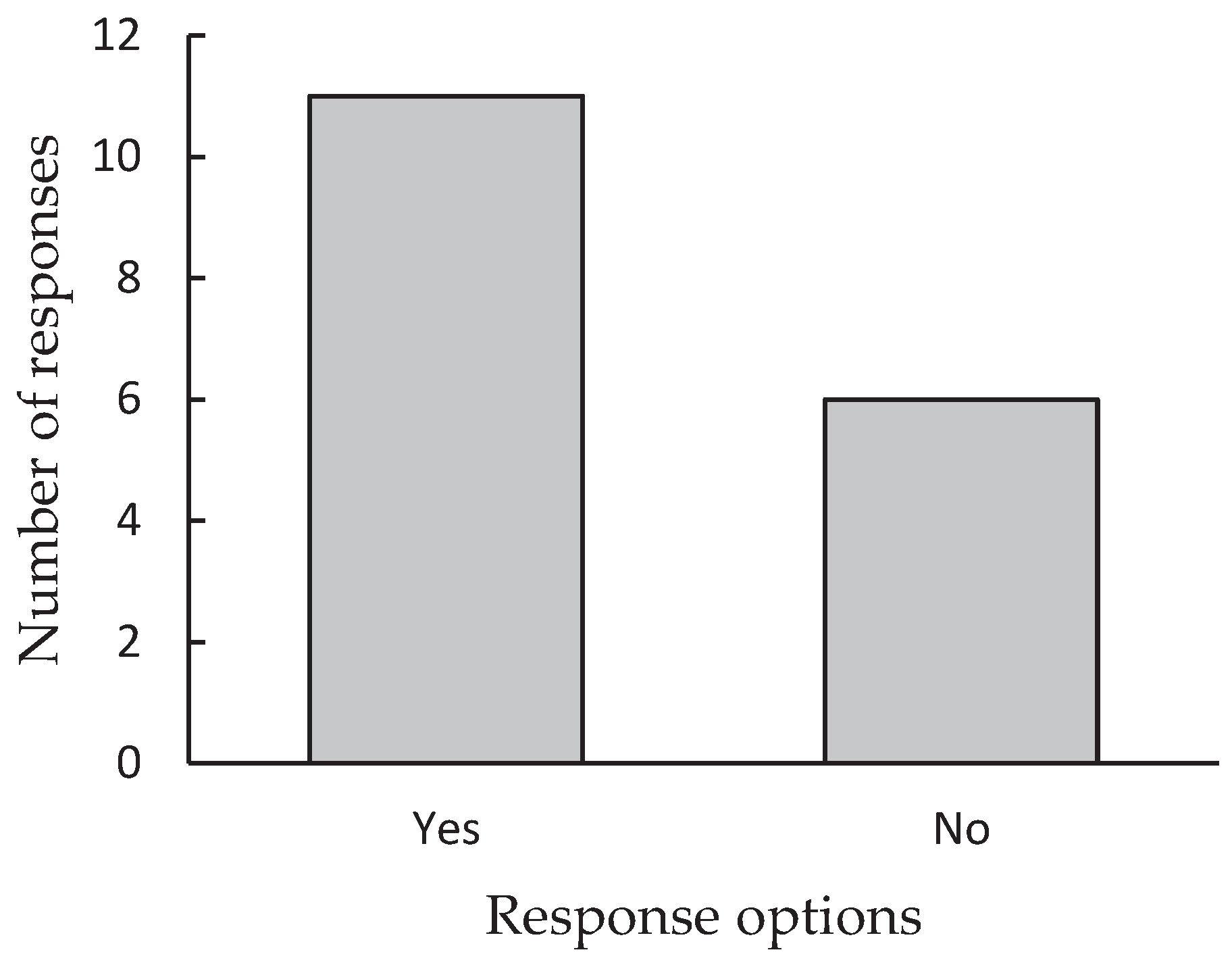

Table 1.
Relevant position or background of participants.
| Participant # | Position/Background |
|---|---|
| 1 | Guide dog facilitator and dog trainer; worked in aged care; and former professor of nursing |
| 2 | Representative from Vision Australia |
| 3 | Hearing dog user |
| 4 | Representative from an aged care facility |
| 5 | Geropsychologist |
| 6 | Animal therapy director; audiologist |
| 7 | Representative from the RSPCA |
| 8 | Representative from the UQ Business School |
| 9 | Veterinarian with an interest in older adults |
| 10 | Veterinarian with an interest in older adults |
| 11 | Assistance dog trainer |
| 12 | Researcher in companion dogs in aged care |
| 13 | Organizational psychologist with an interest in aged care |
| 14 | Hearing in nursing homes |
| 15 | RSPCA researcher |
| 16 | RSPCA dog adoption specialist |
| 17 | Occupational therapist with a PhD in dementia |
| 18 | Psychology student and nursing home services consumer |
Table 2.
Summary of ranked response statistics by importance for Question 3.
| Sub-response | Importance Rank | M (SD) |
|---|---|---|
| Physical environment | 1st | 2.00 (1.03) |
| 2nd | 2.27 (1.00) | |
| 3rd | 2.33 (0.87) | |
| 4th | 3.40 (1.02) | |
| Staff and training | 1st | 1.88 (0.83) |
| 2nd | 2.00 (0.84) | |
| 3rd | 2.12 (0.76) |
Table 3.
Summary of ranked response statistics by importance for Question 4.
| Importance Rank | M (SD) |
| 1st | 1.77 (0.58) |
| 2nd | 1.85 (0.86) |
| 3rd | 2.38 (0.84) |
Table 4.
Summary of ranked response statistics by importance for Question 5.
| Sub-response | Importance Rank | M (SD) |
|---|---|---|
| Person factors | 1st | 2.20 (1.28) |
| 2nd | 2.47 (0.88) | |
| 3rd | 2.60 (1.20) | |
| 4th | 2.73 (1.00) | |
| Dog factors | 1st | 1.82 (1.04) |
| 2nd | 2.53 (1.33) | |
| 3rd | 3.35 (1.33) | |
| 4th | 3.59 (1.14) | |
| 5th | 3.71 (1.23) | |
| Owner-dog relationship factors | 1st | 1.40 (0.49) |
| 2nd | 1.60 (0.49) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



